Robin Hill1,2, Brendan Healy3, Lois Holloway1,4,Zdenka Kuncic1, David Thwaites1 and Clive Baldock5
1 Institute of Medical Physics, School of Physics, University of Sydney, Australia2 Chris O’Brien Lifehouse, Sydney, Australia3 International Atomic Energy Agency, Vienna, Austria4 Cancer Therapy Centre, Liverpool Hospital, Sydney, Australia5 Faculty of Science, Macquarie University, Sydney, Australia
Received 5 September 2013, revised 27 January 2014Accepted for publication 30 January 2014Published 28 February 2014
AbstractThis topical review provides an up-to-date overview of the theoretical andpractical aspects of therapeutic kilovoltage x-ray beam dosimetry. Kilovoltagex-ray beams have the property that the maximum dose occurs very close tothe surface and thus, they are predominantly used in the treatment of skincancers but also have applications for the treatment of other cancers. Inaddition, kilovoltage x-ray beams are used in intra operative units, within animalirradiators and in on-board imagers on linear accelerators and kilovoltagedosimetry is important in these applications as well. This review covers bothreference and relative dosimetry of kilovoltage x-ray beams and providesrecommendations for clinical measurements based on the literature to date.In particular, practical aspects for the selection of dosimeter and phantommaterial are reviewed to provide suitable advice for medical physicists. Anoverview is also presented of dosimeters other than ionization chambers whichcan be used for both relative and in vivo dosimetry. Finally, issues related tothe treatment planning and the use of Monte Carlo codes for solving radiationtransport problems in kilovoltage x-ray beams are presented.
Keywords: kilovoltage x-ray beams, dosimetry, ionization chambers, phantoms,Monte Carlo methods
3. Reference dosimetry of kilovoltage x-ray beams 1883.1. Primary standards for low energy x-ray beams 1883.2. Ionization chamber dosimetry 1883.3. Air kerma calibrations 1893.4. IAEA TRS-398 protocol 1913.5. Comparisons of reference dosimetry protocols 1913.6. Quality audits 192
4. Relative dosimetry of kilovoltage x-ray beams 1924.1. 1D dosimeters 1924.2. 2D dosimetry—radiochromic film 1954.3. 3D dosimetry—gel dosimeters 1964.4. Relative dosimetry measurements 197
5. Backscatter factors 2035.1. Monte Carlo calculations 2035.2. Published BSFs and uncertainties 2045.3. Measured BSFs 204
6. Phantom materials 2066.1. Testing for water equivalence 2076.2. Solid phantom dosimetry for kilovoltage x-ray beams 2086.3. Effective atomic numbers of solid phantoms 2106.4. Effects of different phantom materials on BSF 211
7. Treatment planning 2127.1. Manual calculations 2127.2. Computer calculations 2127.3. Dose to other tissues 2137.4. Shielding and interface effects 213
8. Monte Carlo methods for radiation transport 2158.1. EGSnrc 2158.2. Geant4 2168.3. MCNP 2178.4. PENELOPE 217
9. Conclusions and future perspectives 217Acknowledgments 218References 218
1. Introduction
X-rays were first discovered by Wilhelm Roentgen in 1895 for which he was awarded the firstNobel prize for physics in 1901 (Roentgen 1895). In a relatively short time, it was discoveredthat ionizing radiation could be used to treat various benign and malignant medical conditionswhich prompted the rapid development of x-ray units. Therapeutic kilovoltage x-ray units
R184
Phys. Med. Biol. 59 (2014) R183 Topical Review
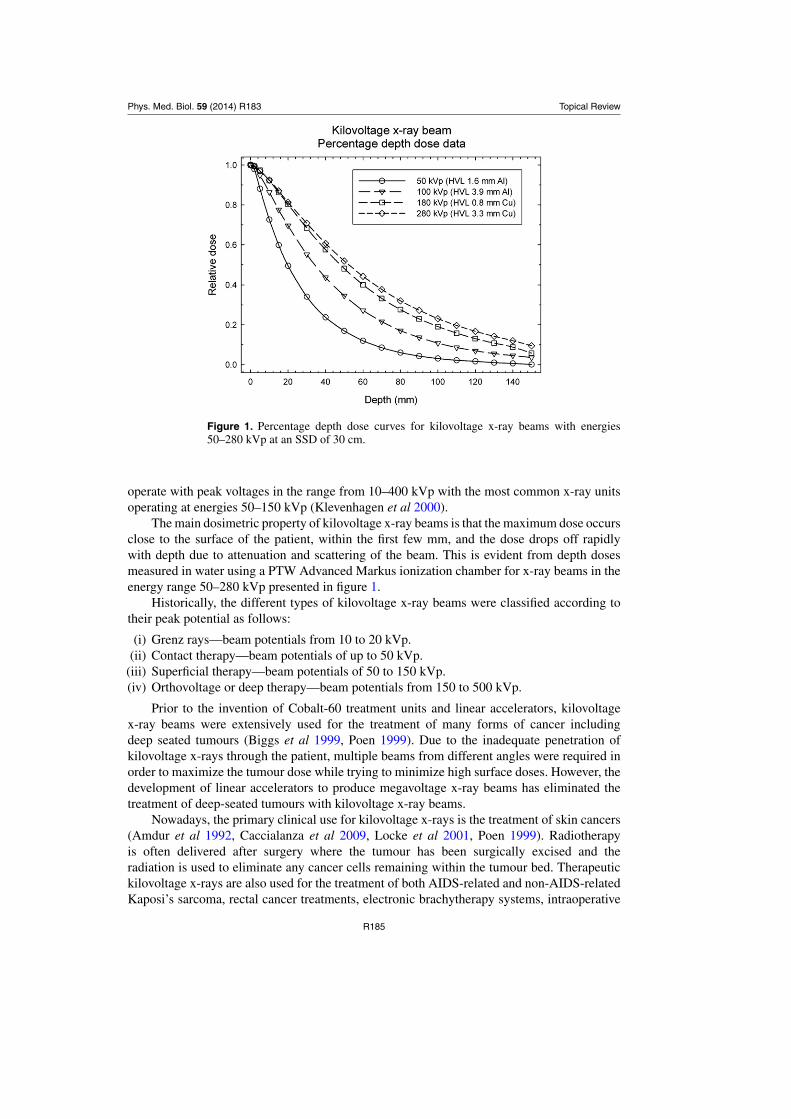
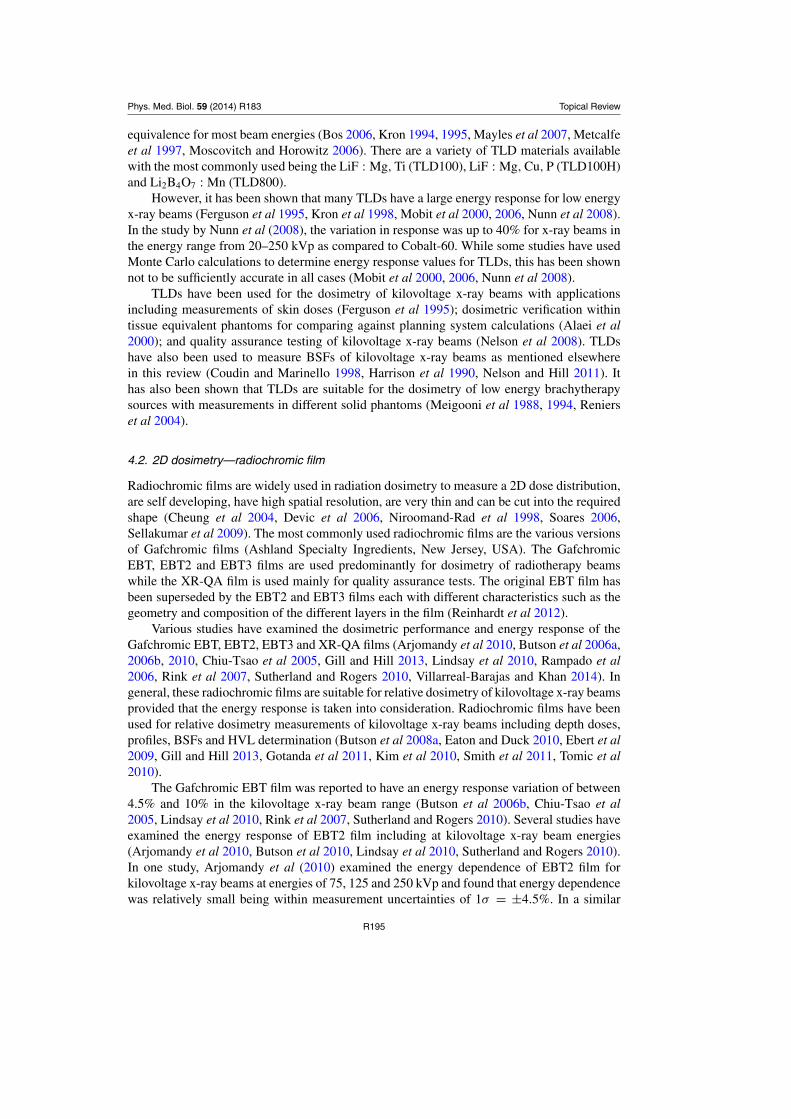
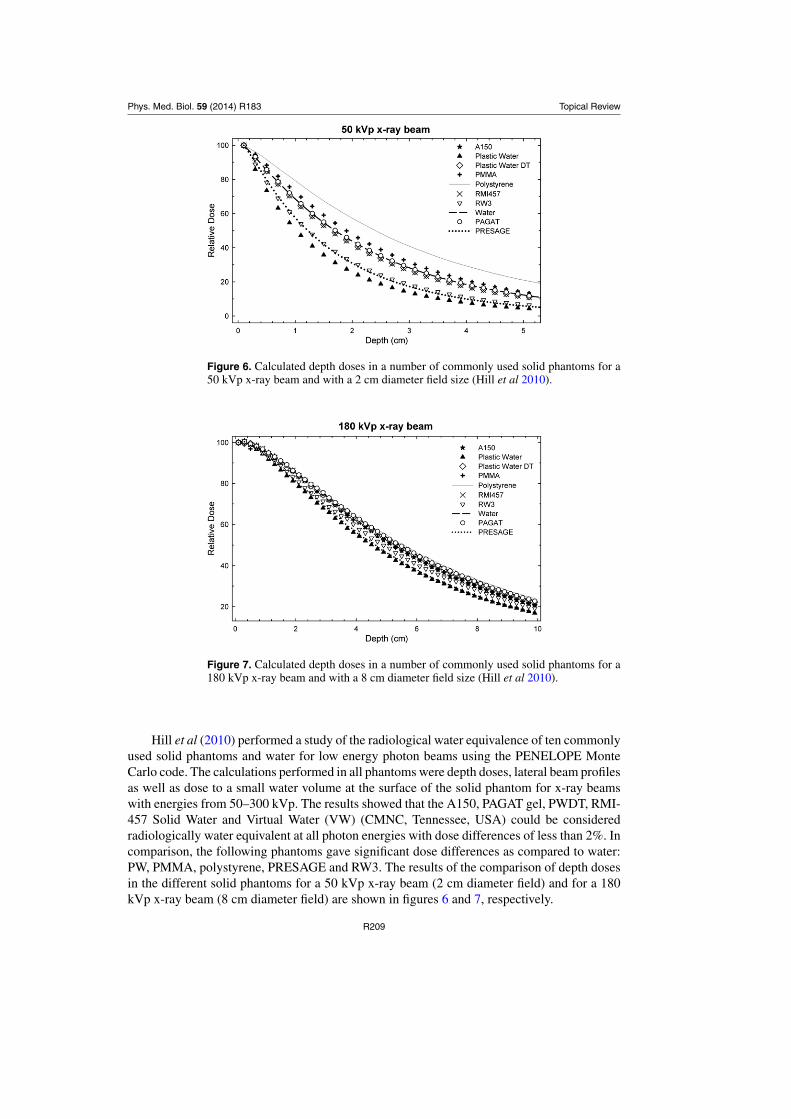
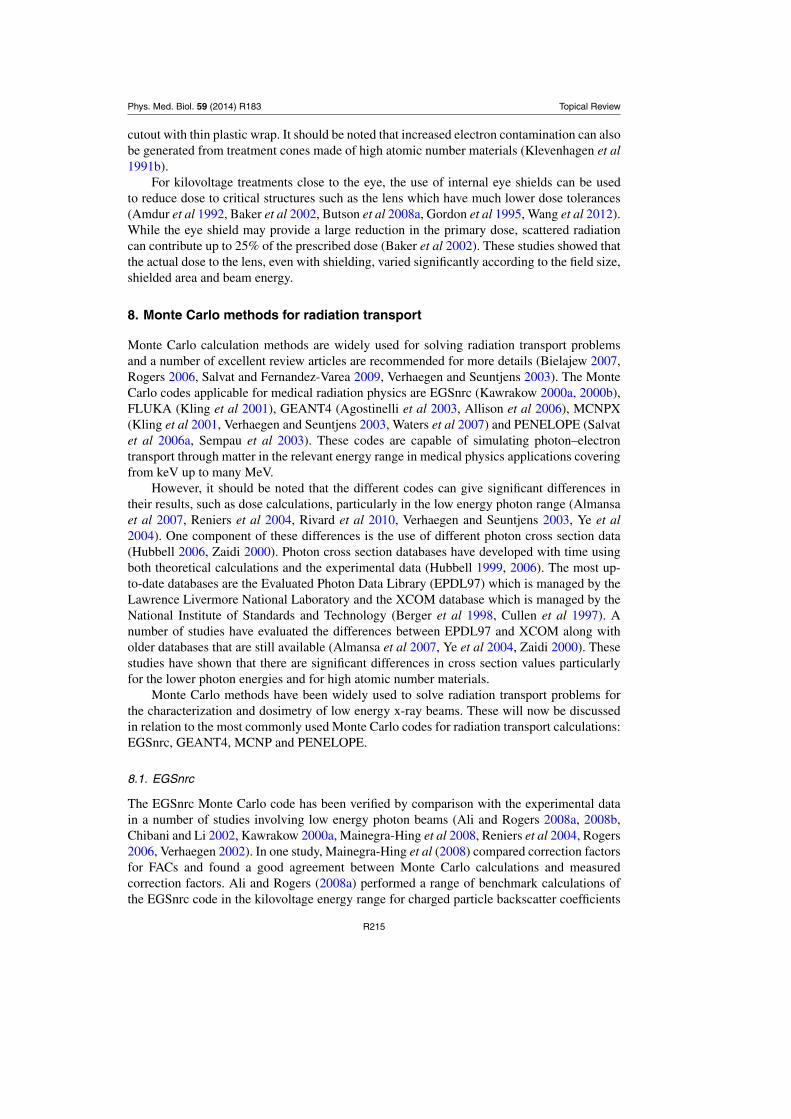
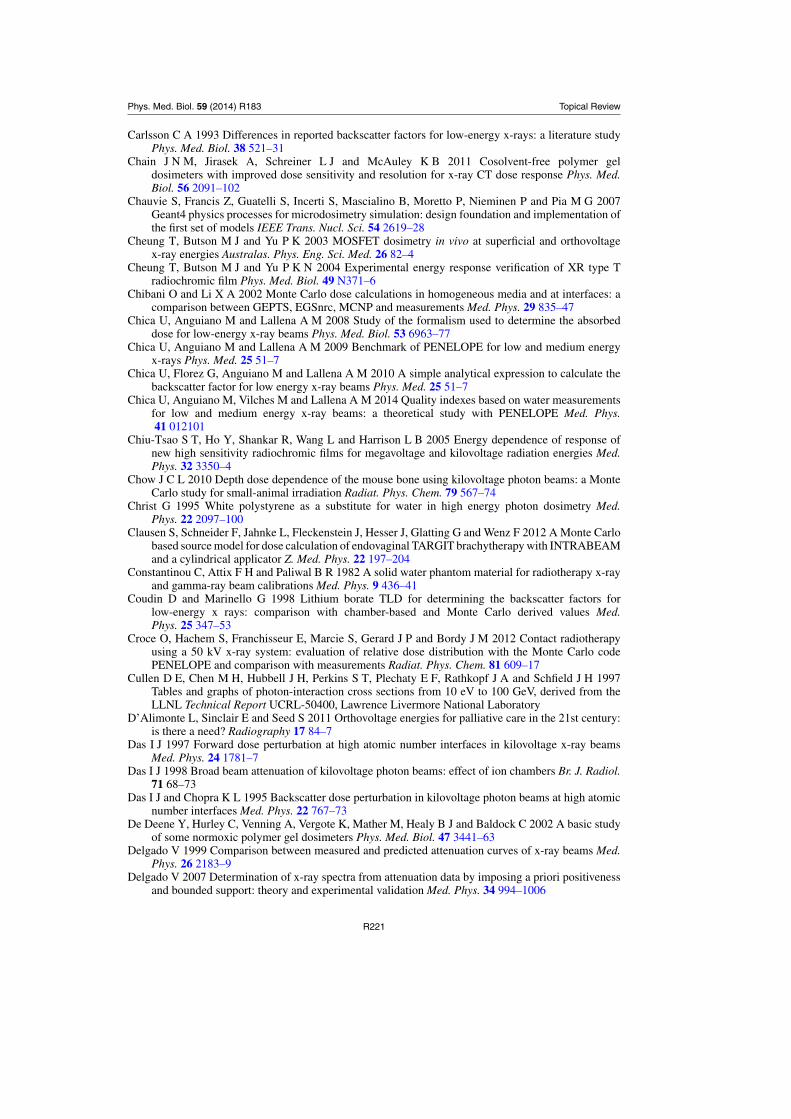
Figure 1. Percentage depth dose curves for kilovoltage x-ray beams with energies50–280 kVp at an SSD of 30 cm.
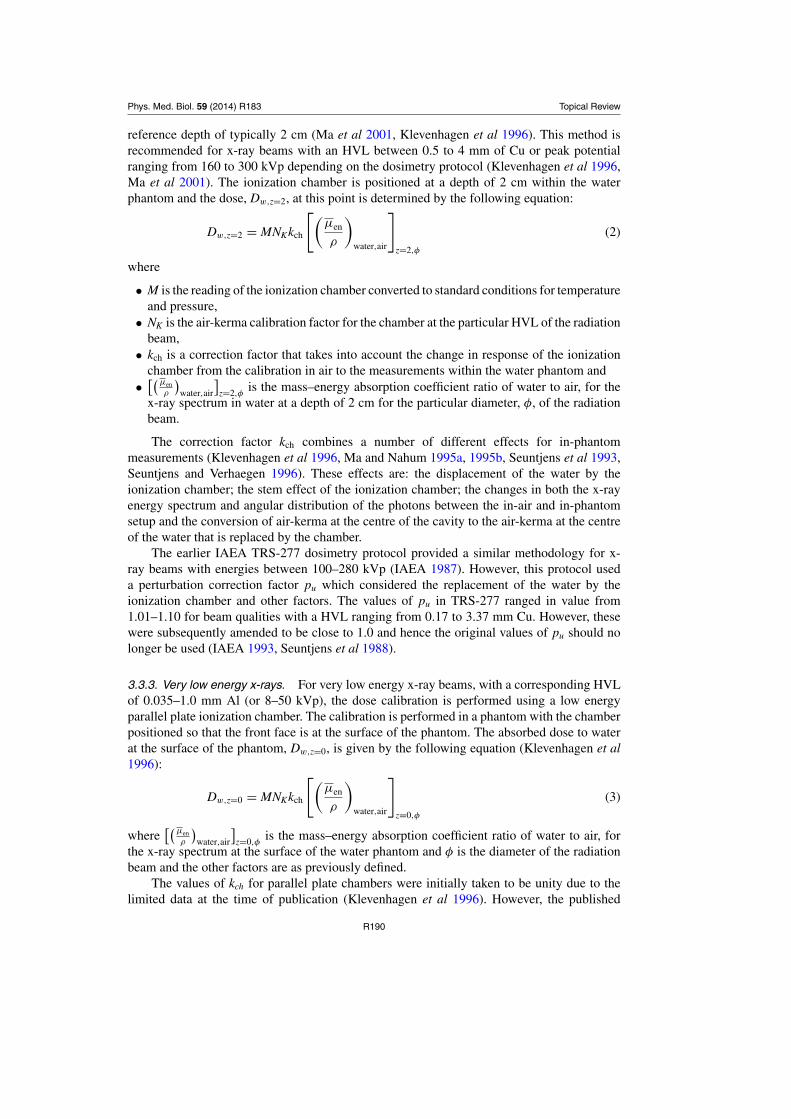
operate with peak voltages in the range from 10–400 kVp with the most common x-ray unitsoperating at energies 50–150 kVp (Klevenhagen et al 2000).
The main dosimetric property of kilovoltage x-ray beams is that the maximum dose occursclose to the surface of the patient, within the first few mm, and the dose drops off rapidlywith depth due to attenuation and scattering of the beam. This is evident from depth dosesmeasured in water using a PTW Advanced Markus ionization chamber for x-ray beams in theenergy range 50–280 kVp presented in figure 1.
Historically, the different types of kilovoltage x-ray beams were classified according totheir peak potential as follows:
(i) Grenz rays—beam potentials from 10 to 20 kVp.(ii) Contact therapy—beam potentials of up to 50 kVp.
(iii) Superficial therapy—beam potentials of 50 to 150 kVp.(iv) Orthovoltage or deep therapy—beam potentials from 150 to 500 kVp.
Prior to the invention of Cobalt-60 treatment units and linear accelerators, kilovoltagex-ray beams were extensively used for the treatment of many forms of cancer includingdeep seated tumours (Biggs et al 1999, Poen 1999). Due to the inadequate penetration ofkilovoltage x-rays through the patient, multiple beams from different angles were required inorder to maximize the tumour dose while trying to minimize high surface doses. However, thedevelopment of linear accelerators to produce megavoltage x-ray beams has eliminated thetreatment of deep-seated tumours with kilovoltage x-ray beams.
Nowadays, the primary clinical use for kilovoltage x-rays is the treatment of skin cancers(Amdur et al 1992, Caccialanza et al 2009, Locke et al 2001, Poen 1999). Radiotherapyis often delivered after surgery where the tumour has been surgically excised and theradiation is used to eliminate any cancer cells remaining within the tumour bed. Therapeutickilovoltage x-rays are also used for the treatment of both AIDS-related and non-AIDS-relatedKaposi’s sarcoma, rectal cancer treatments, electronic brachytherapy systems, intraoperative
R185
Phys. Med. Biol. 59 (2014) R183 Topical Review
radiotherapy, palliative radiotherapy and keloid treatments (Avanzo et al 2012, Clausen et al2012, Croce et al 2012, D’Alimonte et al 2011, Eaton and Duck 2010, Eaton et al 2012, Eaton2012, Gerard et al 2011, Perez et al 2004, Poen 1999, Rong and Welsh 2010, Schneider et al2009). More recently, there has been increased use of kilovoltage x-ray beams inside smallanimal irradiators as used for radiation dosimetry and radiobiology studies (Arndt et al 2011,Bazalova et al 2009, Chow 2010, McKerracher and Thwaites 2006, Newton et al 2011, Pidikitiet al 2011, Thomas et al 2011, Verhaegen et al 2011).
Kilovoltage x-ray beam dosimetry provides a number of challenges which are not presentfor megavoltage x-ray beams (Nahum 1996). Firstly, as most dosimeters have a relatively largedimension in the depth direction, the rapid fall off of dose with depth means there can be asignificant dose gradient over the measuring volume of the dosimeter. Another issue is thatdosimeter response is sensitive to the materials used in its construction. For low energy x-raybeams, the photoelectric effect is a dominant interaction process and the photoelectric crosssection has a strong dependence on the atomic number of the material. The third challengeis that ionization chambers do not act as Bragg–Gray cavities in the kilovoltage x-ray energyrange and so cavity theory cannot be used for reference dosimetry (Ma and Nahum 1991).
In this review paper, we discuss a range of aspects of the dosimetry for therapeutickilovoltage x-ray beams as used in the radiation oncology. It is noted that there is an overlapwith dosimetry of imaging kilovoltage beams which have become more important given thewide availability of planar and cone beam CT imaging systems in the radiation therapy.However, the primary focus of this review paper is the dosimetry of therapeutic kilovoltagex-ray beams.
2. Beam quality specification
2.1. Half-value layer
Knowledge of the beam quality is a precursor to any reference dosimetry (or absolute dosecalibration) of kilovoltage x-ray beams. Direct measurement of the x-ray beam spectrum is adifficult task and not readily achievable in the clinic (Ma et al 2001, Seuntjens et al 1987a). Incurrent dosimetry protocols, the beam quality is specified in terms of the half-value layer (HVL)in combination with the peak generating voltage (kVp) (Andreo et al 2000, Klevenhagen et al1996, Grimbergen et al 1997, Ma et al 2001). The HVL is defined in terms of the thicknessof absorber (typically high purity aluminium or copper) which reduces the air-kerma rate bya factor of one half (Klevenhagen et al 1996). Many of the parameters used in the referencedosimetry calculations are defined as a function of the HVL.
A Farmer type ionization chamber is typically recommended for HVL measurement andabsolute calibration except for lower energy x-ray beams (typically less than 50 kVp), where alow energy parallel-plate chamber is recommended (Klevenhagen et al 1996, Ma et al 2001).The air-kerma calibration of the ionization chamber used for the HVL measurement shouldvary smoothly and by less than 5% over the energy range concerned.
According to dosimetry protocols, the HVL should be measured under scatter free andnarrow beam conditions. Scatter free conditions are achieved by placing the ionization chamberat a distance from the source, ensuring distances from detector to walls, floor or ceiling aremaximized and placing the absorber at half the distance between the source and detector.The source-detector distance is typically 80–100 cm, and where possible should be consistentwith the source-detector distance used by the primary or secondary standards dosimetry labwhen they perform their calibrations. Narrow beam geometry can be achieved either by usinga small size applicator or a lead sheet with a small cutout. The size of the collimated beam
R186
Phys. Med. Biol. 59 (2014) R183 Topical Review
should be such that it covers the ionization chamber with a small margin around the chamberof 5–10 mm, for instance.
Good practice in HVL measurement includes exposing a piece of film behind the detectorto ensure the ionization chamber is correctly positioned in the radiation field and ensuringthe chamber axis is perpendicular both to the filament-target direction of the x-ray tube andthe beam central axis to avoid the heel effect. During beam commissioning, it is commonto measure both the first and second HVLs for each radiation beam for quality assurancepurposes.
2.2. Other beam quality specifiers
The beam quality for a kilovoltage x-ray beam cannot be completely described by the HVLonly (Ma et al 2001). It has been demonstrated that for clinical x-ray beams with the samemeasured HVL, the beams had a wide range of beam potentials and vice versa. This limitationhas been addressed in the NCS reference dosimetry protocol by listing parameters in termsof both HVL and kVp (Grimbergen et al 1997). However, to date there has not been anyalternative beam specifier found to replace the HVL.
Several beam quality specifiers were investigated by Rosser (1998) as an alternativequality index that would correlate with the ratio of mass–energy absorption coefficients ofwater to air at 2 cm depth in water,
!"µenρ
#water,air
$z=2,φ
. The three parameters investigated werethe HVL, the mean energy at a depth of 2 cm and the ratio of the doses at depths of 2 and 5 cmin water. The ratio of doses showed the best correlation but has not been widely implementedwith the HVL still the dominant beam quality specifier.
More recently, Chica et al (2014) investigated the relationship between ionization chambercalibration factors and the ratios of absorbed doses at two depths in water by using Monte Carlocalculations. They found that the relationship was almost linear. Therefore, the determination ofsuperior beam quality specifiers for kilovoltage x-ray beams requires additional investigation.
2.3. X-ray spectral determination
The direct measurement of the primary and/or scattered x-ray beam spectra is a difficultprocess and requires specialist equipment (Birch and Marshall 1979, Mainardi and Bonzi2008, Seuntjens et al 1987a, Tucker et al 1991a). However, if beam spectra information isrequired, it is usually sufficient to use either published spectral data or an analytical calculation(Birch and Marshall 1979, Chica et al 2008, Ma and Seuntjens 1999, Poludniowski 2007,Poludniowski and Evans 2007, Poludniowski et al 2009, Tucker et al 1991b).
Alternatively, one can determine the primary x-ray spectra by using Monte Carlocalculations. However, this involves determining a complete model of the x-ray unit andrequires a good knowledge of the geometry and materials in the x-ray tube (Ali and Rogers2008a, 2008c, Mainegra-Hing and Kawrakow 2006, Mesbahi and Zakariaee 2013, Munck AfRosenschold et al 2008, Omrane et al 2003).
A number of studies have also investigated methods to derive primary x-ray beam spectrafrom the measured transmission data (Archer and Wagner 1988a, 1988b, Delgado 1999, 2007,Du et al 2006, Mainardi and Bonzi 2008, Sidky et al 2005, Waggener et al 1999). Thederivation of the spectra requires the use of mathematical techniques to solve what is a verydifficult mathematical problem (Sidky et al 2005). Nevertheless, many of these studies gaveresults that were in a reasonably good agreement with either measured beam spectra, publisheddata or Monte Carlo calculations.
R187
Phys. Med. Biol. 59 (2014) R183 Topical Review
3. Reference dosimetry of kilovoltage x-ray beams
3.1. Primary standards for low energy x-ray beams
For low energy x-ray beams, the free-air ionization chamber (FAC) is considered the referenceinstrument for the determination of air-kerma (Attix 2004, Burns and Buermann 2009, Lyeet al 2010b, Mayles et al 2007, Rapp et al 2013, Snow et al 2013). It is known as a FAC becauseit relies on the principle that the walls of the chamber do not influence the measurement ofcharge. This requires that the FAC has a sufficiently large size for the air cavity and largerthan the range of electrons in air. The FAC can be used to directly measure air-kerma (orexposure) as the size of the ionization chamber is such that charged particle equilibrium isachieved (Buhr et al 2012, Burns and Buermann 2009, Mayles et al 2007). Due to the largesize and complex use of the FAC, they are predominantly found in primary standard dosimetrylaboratories (PSDLs) but are too bulky and difficult to use in radiotherapy clinics.
Water calorimeters are used by a number of national standard laboratories as the absorbeddose primary standards for either Cobalt-60 or megavoltage x-ray beams (Seuntjens and Duane2009). However, there has been recent work in developing water calorimeters for use withkilovoltage x-ray beams (de Prez and de Pooter 2008, Krauss et al 2012, Rapp et al 2013).It is expected that absorbed dose standards for kilovoltage x-ray beams will continue to beestablished in standards laboratories around the world.
3.2. Ionization chamber dosimetry
In the clinic, the Farmer type cylindrical ionization chamber is considered to be the goldstandard for reference dosimetry of radiotherapy x-ray beams including kilovoltage x-raybeams (Attix 2004, Mayles et al 2007). The main reason for this is that the Farmer chamberhas an energy response variation within 2–3% for beam energies ranging from 50–300 kVp(Andreo et al 2000, Mayles et al 2007). In addition, Farmer chambers are robust, easy to use,stable in their response and can be used for a wide range of dosimetry measurements (Mayleset al 2007). This is supported by the reference dosimetry protocols which state that the goldstandard dosimeter for kilovoltage x-ray beam dosimetry is the Farmer chamber (Andreo et al2000, Aukett et al 2005, IPSM 1991, Klevenhagen et al 1996, Ma et al 2001). However, forthe very low energy x-ray beams, typically less than 50 kVp, the gold standard detector isa low energy x-ray parallel plate ionization chamber (Andreo et al 2000, Klevenhagen et al1996)
For megavoltage x-ray beams, the absorbed dose to a medium such as water can bemeasured with an ionization chamber by the use of Bragg–Gray or Spencer-Attix cavitytheory (Attix 2004, Mayles et al 2007). However, the Bragg–Gray principle does not apply forkilovoltage x-ray beams as the range of secondary electrons within the medium is very small(Mayles et al 2007). It was shown by Ma and Nahum (1991) that for beam energies less than240 kV, up to 30% of the ionization within the air cavity was due to photon interactions thatoccurred within the air itself and not from the surrounding medium.
For these reasons, the determination of absorbed dose to water for kilovoltage x-ray beamsis based on using an ionization chamber calibrated in terms of air-kerma, Kair, or exposure X .It should be noted that PSDLs no longer provide calibration factors in terms of exposure butrather in terms of air-kerma.
Since the absorbed dose is almost equal to the kerma in the medium for kilovoltage x-raybeams, one is able to assume charge particle equilibrium (CPE) and directly relate the kermain air to the dose in air and finally convert this to the dose in the water. The different methodsof calibration will now be discussed in more detail.
R188
Phys. Med. Biol. 59 (2014) R183 Topical Review
3.3. Air kerma calibrations
The FAC is the standard used for the determination of air-kerma of low and medium energyx-rays (Ma et al 2001, Buhr et al 2012, Burns and Buermann 2009, Burns and Kessler 2009,Lye et al 2010b). The user provides an ionization chamber which is calibrated against thestandard FAC and the standards lab determines the air-kerma calibration factor, NK , as afunction of x-ray beam energy for that particular ionization chamber. Air-kerma calibrationshave been implemented in various reference dosimetry protocols for kilovoltage x-ray beams(Aukett et al 2005, DIN 1988, 1996, Grimbergen et al 1997, Klevenhagen et al 1996, Ma et al2001, Mayles et al 2007).
The two most commonly used air-kerma calibration protocols are those published in theTask Group 61 report from the American Association of Physicists in Medicine (AAPM) andthe Code of Practice from the Institution of Physics and Engineering in Medicine and Biology(IPEMB) (Klevenhagen et al 1996, Ma et al 2001). Both of these protocols recommend air-kerma calibrations for kilovoltage x-ray beams in the energy range from 40–300 kVp andprovide a list of parameters required for use in the calibration.
There are two methods for performing air-kerma calibrations being the in-air method andthe in-phantom method. These methods will now be discussed in more detail.
3.3.1. The in-air calibration method. For kilovoltage x-ray beams, CPE exists at the surface ofa water phantom and so one can determine the absorbed dose by taking in-air measurements andapplying backscatter factors (BSFs) (Aukett et al 2005, Grimbergen et al 1997, Klevenhagenet al 1996, Ma et al 2001, Mayles et al 2007). In this method, the absorbed dose is determinedby placing the ionization chamber at the end of the applicator, free-in-air, to first measureKair. This is converted to the dose at the surface of a water phantom by using two factors: themass–energy absorption coefficient of water to air in air and the BSF.
The following equation is used to determine the dose at the surface of a water phantomDw,z=0:
Dw,z=0 = MNKBw
%&µen
ρ
'
water,air
(
air
(1)
where
• M is the reading of the ionization chamber converted to standard conditions for temperatureand pressure,
• NK is the air-kerma calibration factor of the ionization chamber for the particular HVL ofthe radiation beam,
• Bw is the BSF in water for the particular HVL, field size and source to surface distance(SSD) and
•!"µen
ρ
#water,air
$air is the mass–energy absorption coefficient ratio of water to air for the
primary x-ray spectrum only which is also known as the condition of free-in-air.
This calibration method can be used over a wide energy range from 40 to 300 kVpdepending on the particular protocol being used (Aukett et al 2005, Klevenhagen et al 1996,DIN 1988, Ma et al 2001). It should be noted that the earlier IAEA TRS-277 dosimetryprotocol provided a similar methodology for kilovoltage x-ray beams with energies less than100 kVp but uses slightly different nomenclature (IAEA 1987).
3.3.2. The in-phantom calibration method. The in-phantom method for reference dosimetryof kilovoltage x-ray beams involves the determination of the dose in a water phantom at a
R189
Phys. Med. Biol. 59 (2014) R183 Topical Review
reference depth of typically 2 cm (Ma et al 2001, Klevenhagen et al 1996). This method isrecommended for x-ray beams with an HVL between 0.5 to 4 mm of Cu or peak potentialranging from 160 to 300 kVp depending on the dosimetry protocol (Klevenhagen et al 1996,Ma et al 2001). The ionization chamber is positioned at a depth of 2 cm within the waterphantom and the dose, Dw,z=2, at this point is determined by the following equation:
Dw,z=2 = MNKkch
%&µen
ρ
'
water,air
(
z=2,φ
(2)
where
• M is the reading of the ionization chamber converted to standard conditions for temperatureand pressure,
• NK is the air-kerma calibration factor for the chamber at the particular HVL of the radiationbeam,
• kch is a correction factor that takes into account the change in response of the ionizationchamber from the calibration in air to the measurements within the water phantom and
•!"µen
ρ
#water,air
$z=2,φ
is the mass–energy absorption coefficient ratio of water to air, for thex-ray spectrum in water at a depth of 2 cm for the particular diameter, φ, of the radiationbeam.
The correction factor kch combines a number of different effects for in-phantommeasurements (Klevenhagen et al 1996, Ma and Nahum 1995a, 1995b, Seuntjens et al 1993,Seuntjens and Verhaegen 1996). These effects are: the displacement of the water by theionization chamber; the stem effect of the ionization chamber; the changes in both the x-rayenergy spectrum and angular distribution of the photons between the in-air and in-phantomsetup and the conversion of air-kerma at the centre of the cavity to the air-kerma at the centreof the water that is replaced by the chamber.
The earlier IAEA TRS-277 dosimetry protocol provided a similar methodology for x-ray beams with energies between 100–280 kVp (IAEA 1987). However, this protocol useda perturbation correction factor pu which considered the replacement of the water by theionization chamber and other factors. The values of pu in TRS-277 ranged in value from1.01–1.10 for beam qualities with a HVL ranging from 0.17 to 3.37 mm Cu. However, thesewere subsequently amended to be close to 1.0 and hence the original values of pu should nolonger be used (IAEA 1993, Seuntjens et al 1988).
3.3.3. Very low energy x-rays. For very low energy x-ray beams, with a corresponding HVLof 0.035–1.0 mm Al (or 8–50 kVp), the dose calibration is performed using a low energyparallel plate ionization chamber. The calibration is performed in a phantom with the chamberpositioned so that the front face is at the surface of the phantom. The absorbed dose to waterat the surface of the phantom, Dw,z=0, is given by the following equation (Klevenhagen et al1996):
Dw,z=0 = MNKkch
%&µen
ρ
'
water,air
(
z=0,φ
(3)
where!"µen
ρ
#water,air
$z=0,φ
is the mass–energy absorption coefficient ratio of water to air, forthe x-ray spectrum at the surface of the water phantom and φ is the diameter of the radiationbeam and the other factors are as previously defined.
The values of kch for parallel plate chambers were initially taken to be unity due to thelimited data at the time of publication (Klevenhagen et al 1996). However, the published
R190
Phys. Med. Biol. 59 (2014) R183 Topical Review
addendum to the IPEMB protocol includes updated kch values of up to 1.10, based on latercalculations and these are now the recommended values to be used in such calibrations (Aukettet al 2005, Ipe et al 2001, Perrin et al 2001).
3.4. IAEA TRS-398 protocol
The IAEA published an updated reference dosimetry protocol, TRS-398, entitled ‘AbsorbedDose Determination in External Beam Radiotherapy: An International Code of Practice forDosimetry based on Standards of Absorbed Dose to Water’ (Andreo et al 2000). This dosimetryprotocol is based on a standard of absorbed dose to water and is applied to a wide range ofradiation beams including kilovoltage x-ray beams (Seuntjens et al 1999).
The formalism in the TRS-398 protocol is such that the absorbed dose to water, Dw,Q, fora radiation beam of quality Q is given by the following equation:
Dw,Q = MQND,w,Q0 kQ,Q0 (4)
where MQ is the dosimeter reading corrected for the influence quantities such as air temperatureand pressure to their reference values, ND,w,Q0 is the calibration factor for the dosimeter interms of absorbed dose to water for a reference beam quality Q0 and kQ,Q0 is a correctionfactor which accounts for the effects of the difference between the reference beam quality Q0
and the actual clinical beam quality Q (Andreo et al 2000).However, the main issue in adopting the TRS-398 protocol for kilovoltage x-ray beams is
that absorbed dose to water calibrations are not generally available for low and medium energyx-ray beams (Andreo et al 2000, Mayles et al 2007). The number of standards laboratories thathave implemented absorbed dose to water calibrations to date is limited (de Prez and de Pooter2008, Seuntjens and Duane 2009, Krauss et al 2012). However, according to the TRS-398protocol, it is possible to derive calibration factors in terms of absorbed dose to water usingair-kerma calibration factors and one of the published air-kerma calibration protocols.
3.5. Comparisons of reference dosimetry protocols
A number of studies have investigated the different dosimetry protocols as well as thedifferences in dose when using them (Chica et al 2008, Jhala et al 2009, Munck Af Rosenscholdet al 2008, Nisbet et al 1999, Peixoto and Andreo 2000, Williams and Thwaites 2000, Yooet al 2002).
Peixoto and Andreo (2000) compared four dosimetry protocols for kilovoltage x-raybeams (DIN, IAEA TRS-277, IPEMB and NCS) using a Farmer type ionization chamber.For the x-ray beam energies for which direct comparisons could be made, they found thatthe agreement was within ±1% except at the extremes for beam energy. This agreement wasexpected due to the consistency of the various correction factors used within the protocols.
However, greater differences in dose have been reported when changing to a newercalibration protocol. Yoo et al (2002) found differences of up to 5% when they implementedthe AAPM TG-61 protocol over an older method, with the differences attributed to the use ofmore recent correction factors. Larger differences have also been reported in the adoption ofthe IAEA TRS-398 protocol and attributed to issues in determining depth doses and publishedperturbation factors (Jhala et al 2009, Munck Af Rosenschold et al 2008).
It has been reported that using generic BSFs and mass–energy absorption coefficientsleads to greater uncertainty in the absorbed dose of more than 5% (Chica et al 2008, Munck AfRosenschold et al 2008). Determination of machine specific values can reduce the uncertaintyin dose but does require extensive calculations using Monte Carlo methods (Knight and Nahum1994).
R191
Phys. Med. Biol. 59 (2014) R183 Topical Review
Based on these comparisons, the use of an air-kerma or absorbed dose to water calibrationmethod should follow one of the more recently published dosimetry protocols. This will ensurereliability and accuracy in dosimetry and lead to consistency in the delivery of radiation dosesto patients (Andreo et al 2000). The use of the older dosimetry protocols with the older datahas the potential to cause inconsistent and inaccurate radiation dose delivery.
3.6. Quality audits
Quality audits are very useful as an independent check of dose calibrations of radiotherapybeams (Nisbet et al 1998, Thwaites et al 1995, Thwaites 1996, Van Dyk 1999). Dosimetryaudits have been performed on megavoltage x-ray and electron beams for many years throughorganizations such as the IAEA (Van Dyk 1999). These audits have been useful for identifyinggross errors with beam calibration and are often required prior to the participation in clinicaltrials.
There have been a number of audits of kilovoltage x-ray beams (Austerlitz et al 2008,Burton et al 2008, Eaton et al 2013, Nisbet et al 1998, Palmer et al 2011). Some audits did notfind any significant dose calibration issues, with dose differences of less than 3% (Nisbet et al1998, Palmer et al 2011). However, the study by Austerlitz et al (2008) found dose differencesof up to 25% for some kilovoltage x-ray beams. The cause of these dose differences wereincorrect dose calibrations, incorrect HVL measurements, out of date calibration factors forequipment and insufficient quality assurance testing on the x-ray units.
Therefore, it is recommended that the last step in the commissioning of a new kilovoltagetherapy x-ray unit is an independent dosimetry audit of all x-ray beams. This process isalso recommended after recommissioning an older x-ray unit. This could be achieved by anindependent dose calibration using equipment with independent calibration factors.
4. Relative dosimetry of kilovoltage x-ray beams
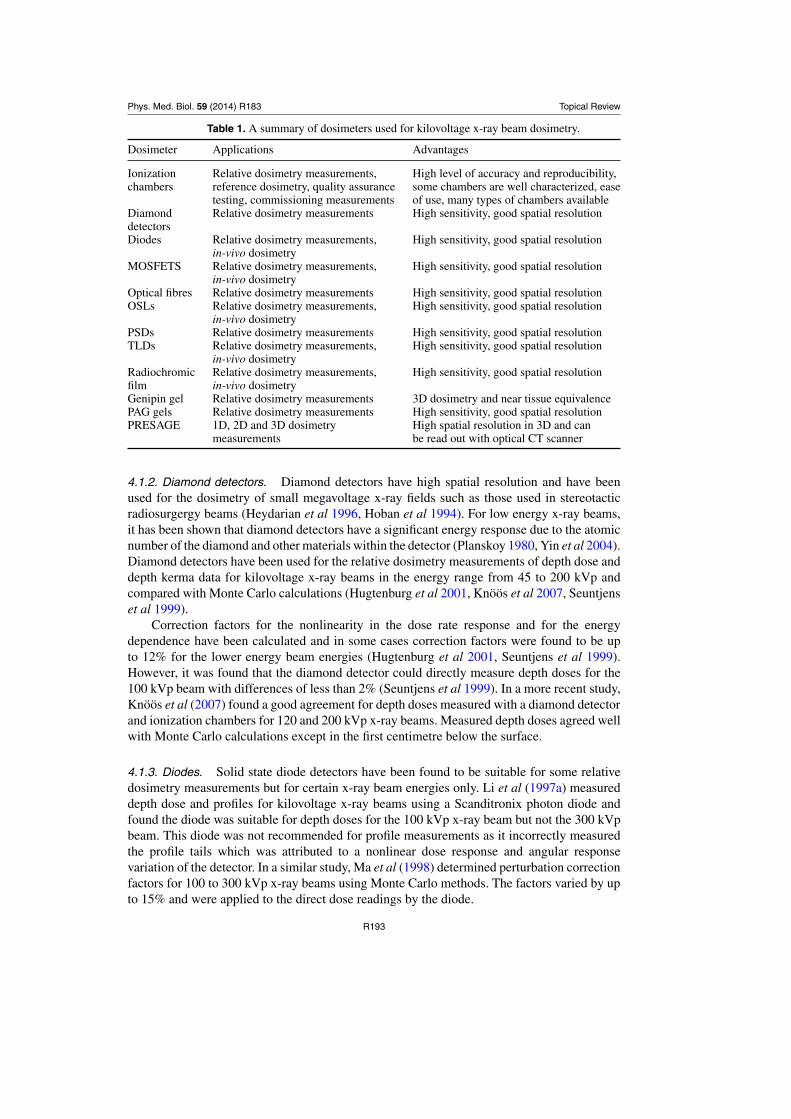
In this section, a range of different dosimeters will be examined for their suitability for thedosimetry of kilovoltage x-ray beams. A summary of the different dosimeters available foruse in radiotherapy is presented in table 1.
4.1. 1D dosimeters
4.1.1. Ionization chambers. Ionization chambers are commonly used to measure the radiationdose from an ionizing radiation beam (Attix 2004, Johns and Cunningham 1983, Khan 1994).There are a variety of different ionization chambers with different physical characteristics andapplications.
(i) Thimble-shaped cylindrical chambers with a small air cavity used for reference andrelative dosimetry.
(ii) Small cylindrical chambers with a small air cavity used for scanning radiation beams inwater phantoms.
(iii) Pinpoint cylindrical chambers used for scanning very small radiation beams.(iv) Parallel plate chambers designed primarily for electron beam dosimetry.(v) Thin window parallel plate chambers designed primarily for dosimetry of very low energy
x-ray beams.
R192
Phys. Med. Biol. 59 (2014) R183 Topical Review
Table 1. A summary of dosimeters used for kilovoltage x-ray beam dosimetry.
Dosimeter Applications Advantages
Ionization Relative dosimetry measurements, High level of accuracy and reproducibility,chambers reference dosimetry, quality assurance some chambers are well characterized, ease
testing, commissioning measurements of use, many types of chambers availableDiamond Relative dosimetry measurements High sensitivity, good spatial resolutiondetectorsDiodes Relative dosimetry measurements, High sensitivity, good spatial resolution
in-vivo dosimetryMOSFETS Relative dosimetry measurements, High sensitivity, good spatial resolution
in-vivo dosimetryOptical fibres Relative dosimetry measurements High sensitivity, good spatial resolutionOSLs Relative dosimetry measurements, High sensitivity, good spatial resolution
in-vivo dosimetryPSDs Relative dosimetry measurements High sensitivity, good spatial resolutionTLDs Relative dosimetry measurements, High sensitivity, good spatial resolution
in-vivo dosimetryRadiochromic Relative dosimetry measurements, High sensitivity, good spatial resolutionfilm in-vivo dosimetryGenipin gel Relative dosimetry measurements 3D dosimetry and near tissue equivalencePAG gels Relative dosimetry measurements High sensitivity, good spatial resolutionPRESAGE 1D, 2D and 3D dosimetry High spatial resolution in 3D and can
measurements be read out with optical CT scanner
4.1.2. Diamond detectors. Diamond detectors have high spatial resolution and have beenused for the dosimetry of small megavoltage x-ray fields such as those used in stereotacticradiosurgergy beams (Heydarian et al 1996, Hoban et al 1994). For low energy x-ray beams,it has been shown that diamond detectors have a significant energy response due to the atomicnumber of the diamond and other materials within the detector (Planskoy 1980, Yin et al 2004).Diamond detectors have been used for the relative dosimetry measurements of depth dose anddepth kerma data for kilovoltage x-ray beams in the energy range from 45 to 200 kVp andcompared with Monte Carlo calculations (Hugtenburg et al 2001, Knoos et al 2007, Seuntjenset al 1999).
Correction factors for the nonlinearity in the dose rate response and for the energydependence have been calculated and in some cases correction factors were found to be upto 12% for the lower energy beam energies (Hugtenburg et al 2001, Seuntjens et al 1999).However, it was found that the diamond detector could directly measure depth doses for the100 kVp beam with differences of less than 2% (Seuntjens et al 1999). In a more recent study,Knoos et al (2007) found a good agreement for depth doses measured with a diamond detectorand ionization chambers for 120 and 200 kVp x-ray beams. Measured depth doses agreed wellwith Monte Carlo calculations except in the first centimetre below the surface.
4.1.3. Diodes. Solid state diode detectors have been found to be suitable for some relativedosimetry measurements but for certain x-ray beam energies only. Li et al (1997a) measureddepth dose and profiles for kilovoltage x-ray beams using a Scanditronix photon diode andfound the diode was suitable for depth doses for the 100 kVp x-ray beam but not the 300 kVpbeam. This diode was not recommended for profile measurements as it incorrectly measuredthe profile tails which was attributed to a nonlinear dose response and angular responsevariation of the detector. In a similar study, Ma et al (1998) determined perturbation correctionfactors for 100 to 300 kVp x-ray beams using Monte Carlo methods. The factors varied by upto 15% and were applied to the direct dose readings by the diode.
R193
Phys. Med. Biol. 59 (2014) R183 Topical Review
A stereotactic diode was used to measure total scatter factors in a small animal irradiatorwhich used an x-ray beam operating at 250 kVp and with an HVL of 0.45 mm Cu (Pidikitiet al 2011). These output factors agreed with those measured using an ionization chamber andGafchromic EBT2 to within 3% for collimators greater than 5 mm diameter.
4.1.4. MOSFETS. Metal oxide semiconductor field-effect transistors (MOSFETS) are usedin radiation dosimetry and possess several desirable features such as small size, being ableto provide real time dose rate information and instantaneous dose readouts (Rosenfeld 2006).Several studies have shown that MOSFETs do have a large variation in energy response forlow energy x-ray beams (Kron et al 1998, Lian et al 2011). One solution is the determinationof correction factors using Monte Carlo calculations (Lian et al 2011).
In one study, Cheung et al (2003) compared in vivo dosimetry measurements usingMOSFETs against calculated doses and TLD measurements for a wide range of kilovoltage x-ray beams. The MOSFETS gave an average dose difference of 5.6% as compared to calculateddoses. In a similar study, Ehringfeld et al (2005) examined the dosimetric characteristicsof MOSFETs for x-ray beams in the energy range 80–220 kVp. They found the agreementbetween TLD and MOSFET measured doses were generally within 3% but indicated thatenergy correction factors may be required.
4.1.5. Optical fibres. Issa et al (2011) investigated the thermoluminescence (TL) properties ofGe-doped silica optical fibres for the dosimetry of kilovoltage x-ray beams. These fibres providegood spatial resolution for radiation dosimetry measurements. The maximum difference indepth doses obtained from the optical fibres and a Farmer ionization chamber was 2.1% forthe 90 kVp x-ray beam and 1.5% for 300 kVp x-ray beam. Similar agreement was also foundin the measured depth doses as compared to the BJR25 reported data. This indicates a goodenergy response for the optical fibres and potential use in kilovoltage x-ray beam dosimetry.
4.1.6. Optically stimulated luminescence dosimeters. Optically stimulated luminescence(OSL) dosimeters are now commonly used in radiation dosimetry particularly for personnelmonitoring and in vivo dosimetry (Akselrod et al 2006, Yukihara and McKeever 2008). OSLshave an easy to read dosimetry system and are quite small in size. The most commonly usedmaterial for OSLs is Al2O3.
Reft (2009) performed a study on the energy and dose response of an OSL system forradiation radiation beams including kilovoltage x-rays. He found that the response of Al2O3
dosimeters was up to 3.5 times greater for the 125 kVp x-ray beam as compared to the 6MVx-ray beam and attributed this predominantly to the relatively high atomic number of theOSL compared to water. This means the use of OSL dosimeters requires calibration in similarenergy x-ray beams as those used for measurement.
4.1.7. Plastic scintillator detectors. Plastic scintillator detectors (PSDs) have found anapplication in the radiation therapy due to their small size and other dosimetric properties(Beddar 2006). One study has investigated the suitability of PSDs for relative dosimetrymeasurements in kilovoltage x-ray beams for beams with energies ranging from 80–150 kVp(Lessard et al 2012). They found that that the PSDs had a high-energy dependence whichwas corrected using mass–energy-absorption coefficients determined using Monte Carlocalculations with measured x-ray spectra information. An over-response of up to 3% wasfound in the measured PDDs at depth due to beam hardening even with correction factorsapplied.
4.1.8. TLDs. Thermoluminescent dosimeters (TLDs) are widely used in radiation dosimetrymeasurements and have the properties of being small in size, reusable and near tissue
R194
Phys. Med. Biol. 59 (2014) R183 Topical Review
equivalence for most beam energies (Bos 2006, Kron 1994, 1995, Mayles et al 2007, Metcalfeet al 1997, Moscovitch and Horowitz 2006). There are a variety of TLD materials availablewith the most commonly used being the LiF : Mg, Ti (TLD100), LiF : Mg, Cu, P (TLD100H)and Li2B4O7 : Mn (TLD800).
However, it has been shown that many TLDs have a large energy response for low energyx-ray beams (Ferguson et al 1995, Kron et al 1998, Mobit et al 2000, 2006, Nunn et al 2008).In the study by Nunn et al (2008), the variation in response was up to 40% for x-ray beams inthe energy range from 20–250 kVp as compared to Cobalt-60. While some studies have usedMonte Carlo calculations to determine energy response values for TLDs, this has been shownnot to be sufficiently accurate in all cases (Mobit et al 2000, 2006, Nunn et al 2008).
TLDs have been used for the dosimetry of kilovoltage x-ray beams with applicationsincluding measurements of skin doses (Ferguson et al 1995); dosimetric verification withintissue equivalent phantoms for comparing against planning system calculations (Alaei et al2000); and quality assurance testing of kilovoltage x-ray beams (Nelson et al 2008). TLDshave also been used to measure BSFs of kilovoltage x-ray beams as mentioned elsewherein this review (Coudin and Marinello 1998, Harrison et al 1990, Nelson and Hill 2011). Ithas also been shown that TLDs are suitable for the dosimetry of low energy brachytherapysources with measurements in different solid phantoms (Meigooni et al 1988, 1994, Renierset al 2004).
4.2. 2D dosimetry—radiochromic film
Radiochromic films are widely used in radiation dosimetry to measure a 2D dose distribution,are self developing, have high spatial resolution, are very thin and can be cut into the requiredshape (Cheung et al 2004, Devic et al 2006, Niroomand-Rad et al 1998, Soares 2006,Sellakumar et al 2009). The most commonly used radiochromic films are the various versionsof Gafchromic films (Ashland Specialty Ingredients, New Jersey, USA). The GafchromicEBT, EBT2 and EBT3 films are used predominantly for dosimetry of radiotherapy beamswhile the XR-QA film is used mainly for quality assurance tests. The original EBT film hasbeen superseded by the EBT2 and EBT3 films each with different characteristics such as thegeometry and composition of the different layers in the film (Reinhardt et al 2012).
Various studies have examined the dosimetric performance and energy response of theGafchromic EBT, EBT2, EBT3 and XR-QA films (Arjomandy et al 2010, Butson et al 2006a,2006b, 2010, Chiu-Tsao et al 2005, Gill and Hill 2013, Lindsay et al 2010, Rampado et al2006, Rink et al 2007, Sutherland and Rogers 2010, Villarreal-Barajas and Khan 2014). Ingeneral, these radiochromic films are suitable for relative dosimetry of kilovoltage x-ray beamsprovided that the energy response is taken into consideration. Radiochromic films have beenused for relative dosimetry measurements of kilovoltage x-ray beams including depth doses,profiles, BSFs and HVL determination (Butson et al 2008a, Eaton and Duck 2010, Ebert et al2009, Gill and Hill 2013, Gotanda et al 2011, Kim et al 2010, Smith et al 2011, Tomic et al2010).
The Gafchromic EBT film was reported to have an energy response variation of between4.5% and 10% in the kilovoltage x-ray beam range (Butson et al 2006b, Chiu-Tsao et al2005, Lindsay et al 2010, Rink et al 2007, Sutherland and Rogers 2010). Several studies haveexamined the energy response of EBT2 film including at kilovoltage x-ray beam energies(Arjomandy et al 2010, Butson et al 2010, Lindsay et al 2010, Sutherland and Rogers 2010).In one study, Arjomandy et al (2010) examined the energy dependence of EBT2 film forkilovoltage x-ray beams at energies of 75, 125 and 250 kVp and found that energy dependencewas relatively small being within measurement uncertainties of 1σ = ±4.5%. In a similar
R195
Phys. Med. Biol. 59 (2014) R183 Topical Review
study, Butson et al (2010) found that EBT2 film had energy response variations of up to 6.5%for x-ray beams with energies from 50 kVp to 10 MV. These energy response variations weretaken into account by calibrating the film with the same or similar x-ray beam energies as usedfor the measurements.
Gafchromic EBT and EBT2 films have been used to measure BSFs in the energy rangefrom 50 to 280 kVp (Butson et al 2007, Kim et al 2010, Smith et al 2011). The measured BSFswere compared to Monte Carlo calculations and/or published BSFs and gave differences ofup to 3%. These results indicate that Gafchromic films are suitable for the direct measurementof BSFs of kilovoltage x-ray beams.
The Gafchromic EBT3 film has been found to be suitable for the measurement of relativeoutput factors for x-ray beams in the energy range from 50–125 kVp (Gill and Hill 2013).They found that the agreement between output factors measured with EBT3 film and a parallelplate ionization chamber was generally better than 2%, with larger differences of up to 3.3%for the smallest field size.
Fletcher and Mills (2008) measured depth doses for 50 and 100 kVp x-ray beams usingvarious dosimeters including several ionization chambers, a Wellhoefer photon diode andGafchromic EBT film. Measured depth doses were compared to BEAMnrc Monte Carlocalculations and used an analytical program to generate the primary x-ray beam spectra. Theyfound the agreement between the EBT film and Monte Carlo was quite good for both the 50and 100 kVp x-ray beams. The maximum difference was up to 8% at depth but with the dosesnormalized at a depth of 20 mm.
Radiochromic films have found an application in relative dosimetry measurements ofintraoperative x-ray units (Croce et al 2012, Eaton and Duck 2010, Ebert et al 2009). Theseunits produce very low energy x-ray beams typically 50 kVp and some radiochromic filmsused for measurements showed significant nonlinearity, particularly the XR-QA film (Ebertet al 2009).
4.3. 3D dosimetry—gel dosimeters
The majority of radiation dosimeters can only provide dose information at a point or within a2D plane. This limitation has been overcome through the development of different chemicaldosimeters that contain ferrous sulphate (Fricke gel) or polyacrylamide gels (PAGs) (Baldocket al 2010). These gel dosimeters have the advantage that they can be made into any shapedvolume and so be used to measure 3D dose distributions.
Many of these gel dosimeters contain a large proportion of water in their composition andare radiologically water equivalent for high energy photon beams (Brown et al 2008b, Kealland Baldock 1999, Kron et al 1993). The water equivalence of different gel dosimeters hasalso been examined for low energy photon beams (Boudou et al 2004, Pantelis et al 2004,Trapp et al 2002, Venning et al 2005b).
4.3.1. Genipin gels. The genipin dosimeter uses genipin which is extracted from the fruitof Gardenia jasminoides Ellis (Yao et al 2004). Genipin gelatin or genipin gel is a blueradiochromic gel which bleaches quantitatively after exposure to ionizing radiation (Jordan2009).
Gorjiara et al (2011b) characterized the radiological properties of genipin gel for clinicalkilovoltage x-ray beams in the energy range from 50 to 300 kVp. For energies below 150 keV,the photoelectric absorption cross sections were 3% greater than water due to the dependenceon the atomic number. However, the calculated depth dose curves for genipin gel agree to within1% as compared to those in water. This indicates that genipin gel has excellent radiologicalwater equivalence for low energy x-ray beams.
R196
Phys. Med. Biol. 59 (2014) R183 Topical Review
4.3.2. Polyacrylamide gels. PAG dosimeters are made of radiation sensitive chemicals whichpolymerize when exposed to ionizing radiation (Baldock et al 2010, De Deene et al 2002).The development of different formulations of PAGs and readout techniques have led to awide variety of dosimeters each with particular advantages and disadvantages (Babic andSchreiner 2006, Baldock et al 1999, Brindha et al 2004, Chain et al 2011, De Deene et al2002, Gustafsson et al 2004, Senden et al 2006, Venning et al 2005a).
In one study, Venning et al (2005b) compared the radiological properties of several PAGsand water for photons over a wide energy range by calculating the photon cross section data.The photon cross section ratios for the PAGs as compared to water were generally better than3% of unity except for photon energies less than 100 keV where there were differences of upto 6%.
4.3.3. PRESAGE dosimeter. The PRESAGE dosimeter is a 3D dosimetry material consistingof an optically clear polyurethane matrix, containing a leuco dye that exhibits a radiochromicresponse when exposed to ionizing radiation (Adamovics and Maryanski 2006, Guo et al 2006).Exposure to ionizing radiation causes changes in the optical absorbance of the PRESAGEdosimeter, which can then be used to determine the absorbed dose distribution. PRESAGE hasa number of advantages over other 3D dosimeters which include being insensitive to oxygen,having a solid form which means it can be designed to the required shape and that it is lightabsorbing rather than scattering which allows readout by optical CT scanner (Adamovics andMaryanski 2006, Baldock et al 2010, Guo et al 2006).
Brown et al (2008b) studied the radiological water equivalence of PRESAGE bydetermining the photon and electron interaction cross section data. They found that the mass–energy absorption coefficient ratio of PRESAGE to water was up to 5% more than unity inthe energy range 10 to 100 keV and attributed this to the presence of high atomic numbermaterials within the PRESAGE. In a more recent study, Gorjiara et al (2011a) investigatedthe radiological water equivalence of different formulations of PRESAGE by Monte Carlomethods. While the radiological water equivalence for low energy x-ray beams was better forthe new formulations, correction factors were still required to convert the dose measured inthe PRESAGE dosimeter to dose in water.
PRESAGE dosimeters have also been used for the dosimetry of kilovoltage x-ray beamsfor animal irradiators (Newton et al 2011, Thomas et al 2011). The x-ray units were generallyoperated at higher kilovoltage beam energies and the PRESAGE dosimeter was found toprovide accurate 3D dosimetry as compared to ionization chambers and radiochromic film.
4.4. Relative dosimetry measurements
Relative dosimetry data of kilovoltage x-ray beams is measured for the commissioning of thex-ray unit, beam data collection for quality assurance testing, reference dosimetrymeasurements and treatment planning calculations. This data typically includes depth doses,profiles, relative output factors both for applicators and lead cutouts as well as BSFs.
Farmer type cylindrical ionization chambers are often considered the gold standarddosimeter for kilovoltage x-ray beam dosimetry in the radiotherapy clinic (Aukett et al 1996,BJR Report 25 1996, Das 1998, Evans et al 2001, Healy et al 2005, Hill et al 2005, 2007,Ismail et al 2011, Jurado et al 2005, Klevenhagen 1982, Kurup and Glasgow 1993, Li et al1997a, 1997b, Podgorsak et al 1990, 1998).
There are however a number of limitations in using Farmer chambers for radiationdosimetry measurements. Some Farmer chambers are not water-proof, particularly those usedfor reference dosimetry and calibrated by a primary or secondary standards laboratory (Andreoet al 2000). A water proof sheath can be used on the Farmer chamber for measurements in
R197
Phys. Med. Biol. 59 (2014) R183 Topical Review
water but care must be taken in the selection of an appropriate sheath (Ma et al 2001, Ma andSeuntjens 1997). The other limitation is that the Farmer chamber is quite large, typically witha radius of 3 mm. This means the minimum depth of measurement is equal to the radius ofthe chamber or that surface dose measurements have a part of the Farmer chamber positionedabove the phantom surface (Ma et al 2001). This will lead to increased uncertainty in the dosemeasurements close to and at the phantom surface. It should be noted that many of the studieslisted immediately above do not provide details of the minimum depth used and/or the useof any corrections applied if a part of the Farmer chamber was positioned partially above thephantom surface.
For these reasons, there have been a number of studies into the use of different dosimetersfor the relative dosimetry of kilovoltage x-ray beams. These have included parallel plateionization chambers, small volume ionization chambers, solid state detectors such as diodesand diamonds and radiochromic film.
4.4.1. Protocol recommendations. Reference dosimetry protocols for kilovoltage x-raybeams provide some recommendations on the particular choice of detector for relativedosimetry (Andreo et al 2000, Aukett et al 2005, Klevenhagen et al 1996, Ma et al 2001).
The IPEMB dosimetry protocol for kilovoltage x-ray beams contains no recommendationsfor relative dosimetry measurements (Klevenhagen et al 1996). However, the addendum tothis protocol recommends relative dosimetry measurements should only be made with anionization chamber with an air-kerma calibration factor, NK , that varies by no more than ±5%over the energy range corresponding to an HVL of 0.15–4.0 mm Cu (Aukett et al 2005). Theaddendum also states that this requirement would usually be met by cylindrical ionizationchambers but not necessarily by parallel plate chambers designed for electron beams. Theserecommendations are based on two studies which compared different ionization chambers bycalculating dose ratios over a range of depths for a range of x-ray beam energies (Aukett et al1999, Rosser 1996). However, dose ratios are not typically used in radiation dosimetry and itshould be noted that taking ratios of small dose values can lead to large dose ratio differenceswhile the actual doses difference can be quite small.
The AAPM TG-61 protocol states that a well designed cylindrical ionization chamberusually has a flat energy response for kilovoltage beams in the energy range 40–300 kVp (Maet al 2001). However, this is limited to the minimum depth of measurement being the outerradius of the chamber. The AAPM protocol also states that some parallel plate chambers, asdesigned for electron beams, are suitable for depth dose measurements with uncertainties ofless than 3% (Li et al 1997a). Depth-dependent correction factors may be required for someionization chambers when used for depth dose measurements. However, published work bysome of the authors of the protocol found that the correction factors were quite small forsome detectors such as the NACP plane parallel plate ionization chamber (Ma et al 1998,Seuntjens et al 1999).
The IAEA TRS-398 protocol has two sets of recommendations for kilovoltage x-raybeams depending on the beam energy (Andreo et al 2000). Low-energy kilovoltage x-raybeams are defined as x-ray beams with a potential of up to 100 kVp or a measured HVL ofup to 3 mm Al while medium-energy kilovoltage x-ray beams have a beam potential greaterthan 80 kVp or a measured HVL greater than 2 mm Al. In the low-energy section, the protocolrecommends that ‘depth-dose distribution can be measured by using the same chamber as thatused for reference dosimetry and a water-equivalent phantom’ (Andreo et al 2000). The IAEATRS-398 protocol also states that the published depth dose data are not likely to match theclinical x-ray beam for both the kVp and the HVL and recommend that the data be measuredfor each clinical beam. They suggest that for the medium-energy x-ray beams, measurement
R198
Phys. Med. Biol. 59 (2014) R183 Topical Review
of the depth doses using either a scanning ionization chamber or parallel plate chambers wouldintroduce uncertainties of no more than several per cent (Andreo et al 2000).
4.4.2. Detector comparisons. There has been a number of studies examining the suitabilityof different detectors for relative dosimetry measurements of kilovoltage x-ray beams (Aukettet al 1996, Gerig et al 1994, Hill et al 2009, Knoos et al 2007, Li et al 1997a, 1998, MunckAf Rosenschold et al 2008, Snow et al 2013). These detectors include Farmer type chambers,parallel plate ionization chambers as designed primarily for electron beams, scanning thimblechambers and solid state detectors such as diode and diamond detectors. Many of thesedetectors have the potential of better spatial resolution for either depth dose or lateral profilemeasurements.
Gerig et al (1994) measured the relative dosimetry data for x-ray beams in the energy range100–300 kVp on a Pantak DXT300 x-ray unit and compared with the published data (BJRSupplement 17). They used an NACP parallel plate chamber for depth doses and a ScanditronixRK scanning chamber for the profiles. They found the agreement with the published depthdose data were very good except for the 300 kVp beam which was attributed to differences inthe beam quality and design of the x-ray unit.
Aukett et al (1996) reported on commissioning two DXT300 Therapax kilovoltage x-rayunits in two different centres. Depth dose and relative output factors were measured witha variety of Farmer, thimble and parallel plate ionization chambers. Comparisons betweendifferent detectors showed differences in dose of up to 4% at a depth of 2 cm and attributedthis to issues with measuring the dose accurately at the surface. Much larger differences indose of up to 44% were observed as compared to the previously published dosimetry data.However, the published data were for x-ray units with different beam characteristics to thoseused in the study (BJR Report 25 1996, Niroomand-Rad et al 1987).
In two comprehensive studies, Li et al (1997a), 1998) investigated nine different detectorsfor the relative dosimetry of x-ray beams in the energy range 50–300 kVp. They found that thePTW N22342, PTW Markus and Scanditronix NACP parallel plate chambers could be usedto measure depth doses with an uncertainty of less than 3% without applying any correctionfactors. While the Farmer chamber was considered the gold-standard, it could only be usedwith a minimum depth of 1 cm. They also found a good agreement in profile measurementsbetween the Farmer, NACP and RK scanning ionization chambers.
A later study by the same group involved measurements of depth doses and profilesfor highly filtered beams in the energy range 40–60 kVp and comparison with Monte Carlocalculations (Li et al 1998). The result of this work was that the PTW Markus and PTWN23342 parallel plate chambers gave doses within 2% for a 50 kVp x-ray beam while theNACP chamber gave results that were up to 10% greater for depths less than 0.3 cm.
In two studies, Knoos et al (2007), Munck Af Rosenschold et al (2008) comparedthe following dosimeters: the FC65-G Farmer chamber, NACP-02 parallel plate chamber(Wellhofer-Scanditronix, Germany) and PTW Roos parallel plate chambers and PTW diamonddetector (PTW-Freiburg, Freiburg). In the first study, they undertook measurements of depthdoses and profiles of 120 and 200 kVp x-ray beams. The Farmer chamber was used for thedepth dose measurements except for depths less than 0.7 cm where the NACP chamber wasused in order to avoid collisions with the applicator. The BEAMnrc Monte Carlo system wasused to calculate both depth doses and profiles in a water phantom for both x-ray beams. Theagreement between measured and calculated depth doses was better than 1% except near thewater surface where there were differences of up to 2%. The second study involved measuringdoses at the surface and at 2 cm depth and included the PTW Roos chamber (Munck AfRosenschold et al 2008). They found differences of less than 2% between all dosimeters for
R199
Phys. Med. Biol. 59 (2014) R183 Topical Review
the relative doses measured at 2 cm depth compared to the surface doses for both 120 and200 kV x-ray beams.
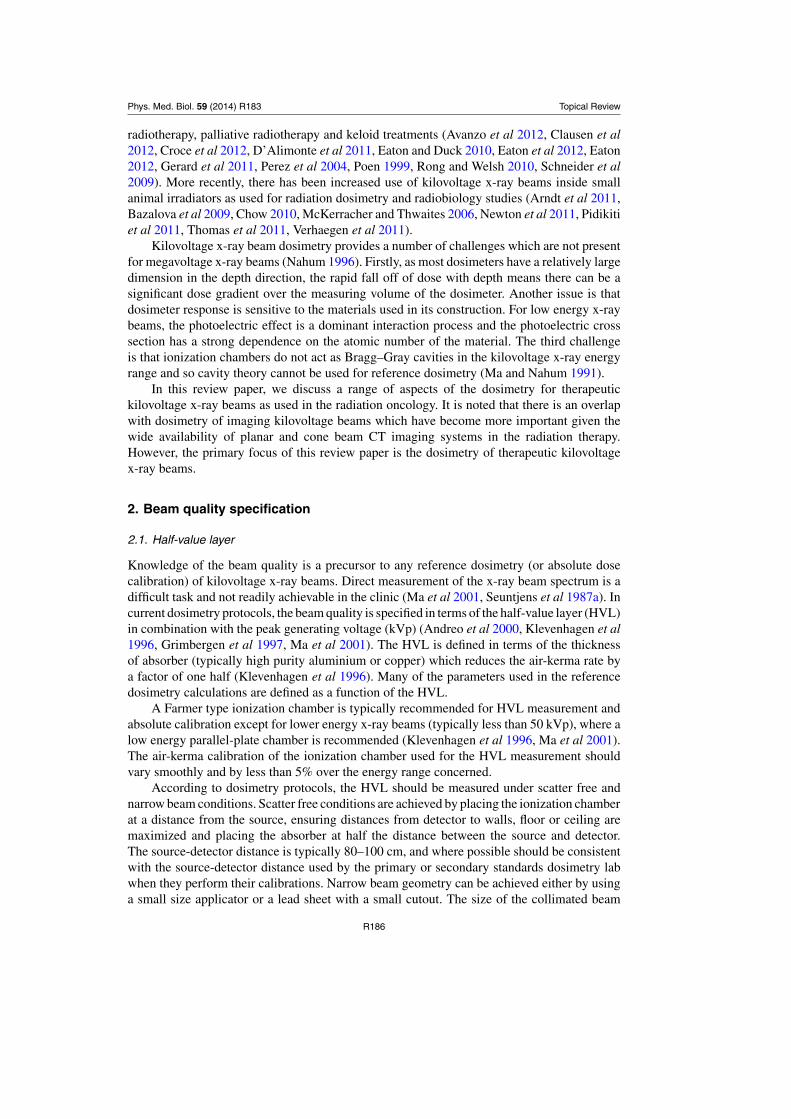
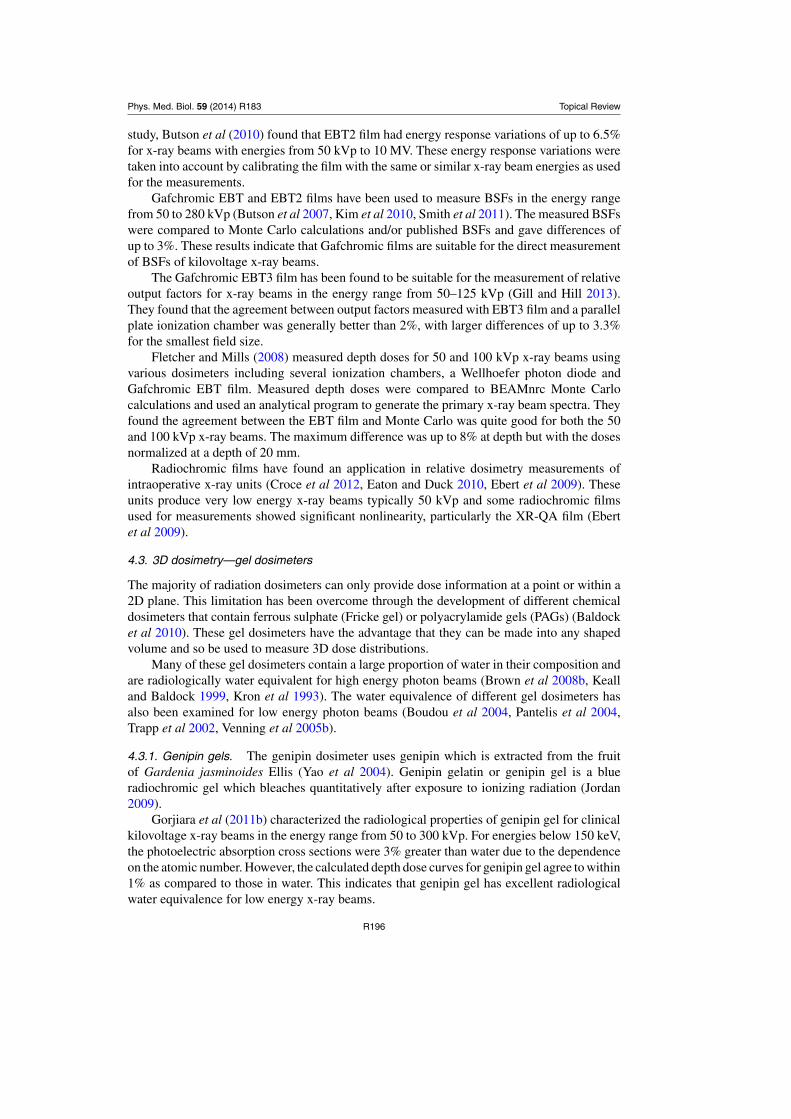
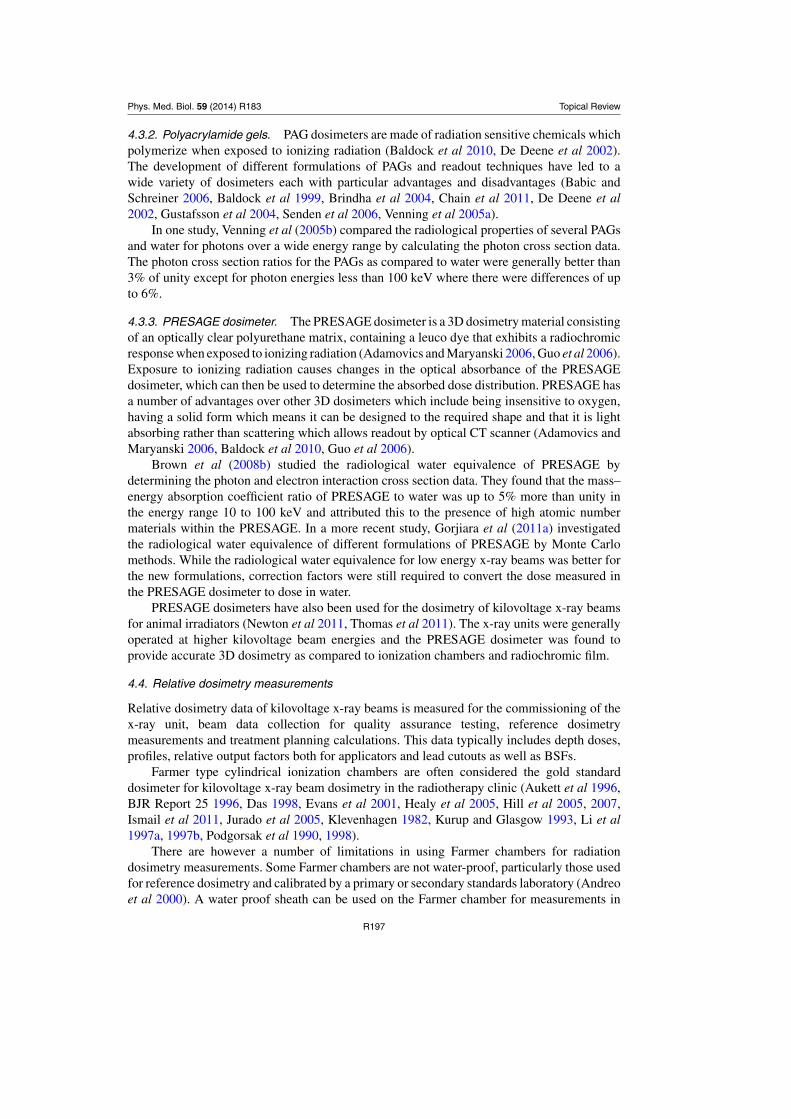
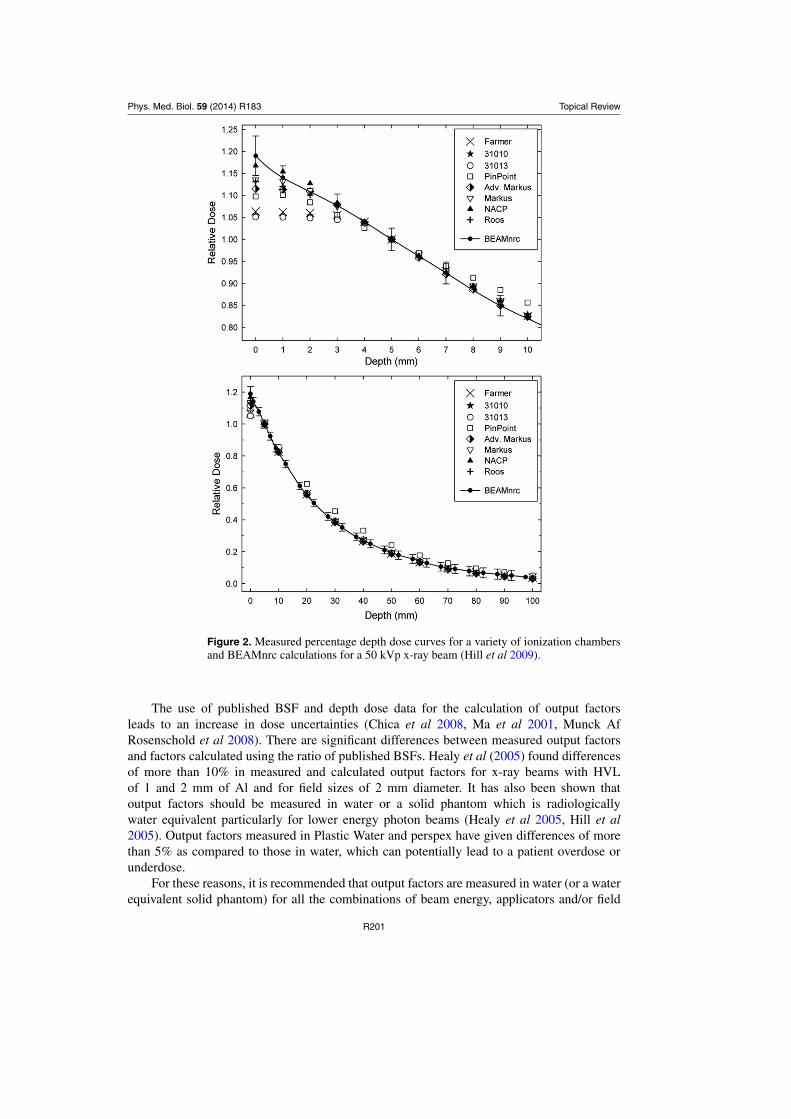
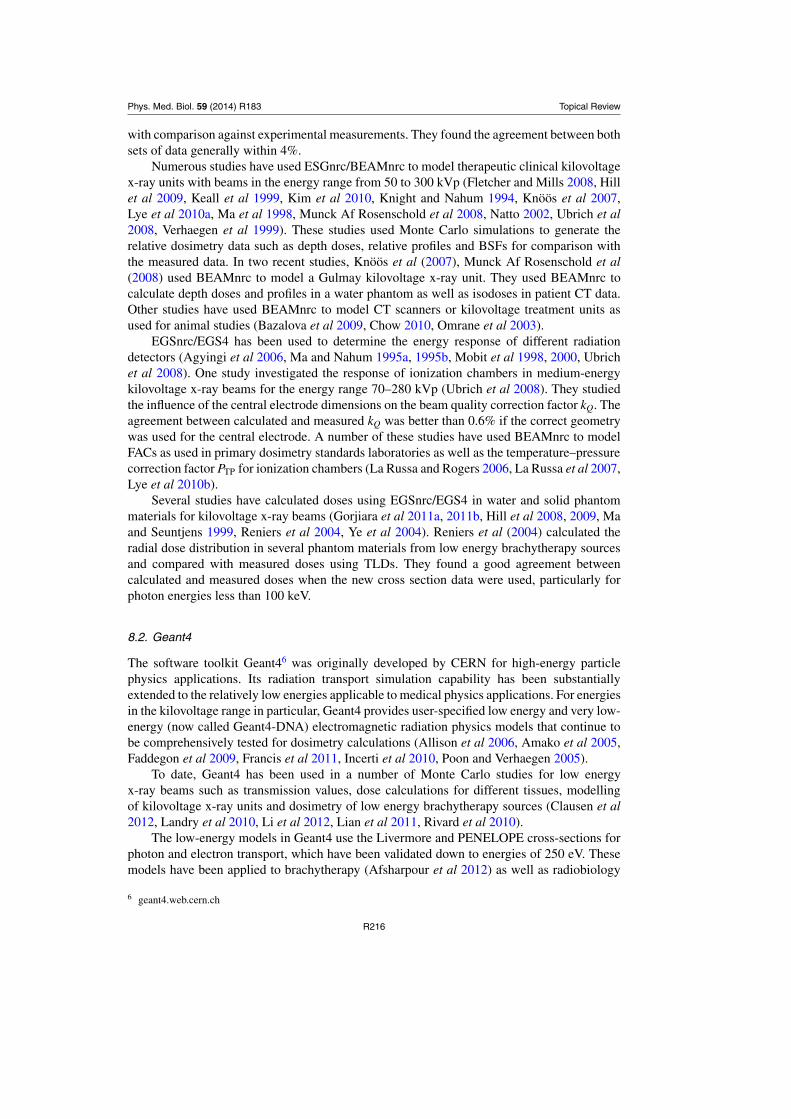
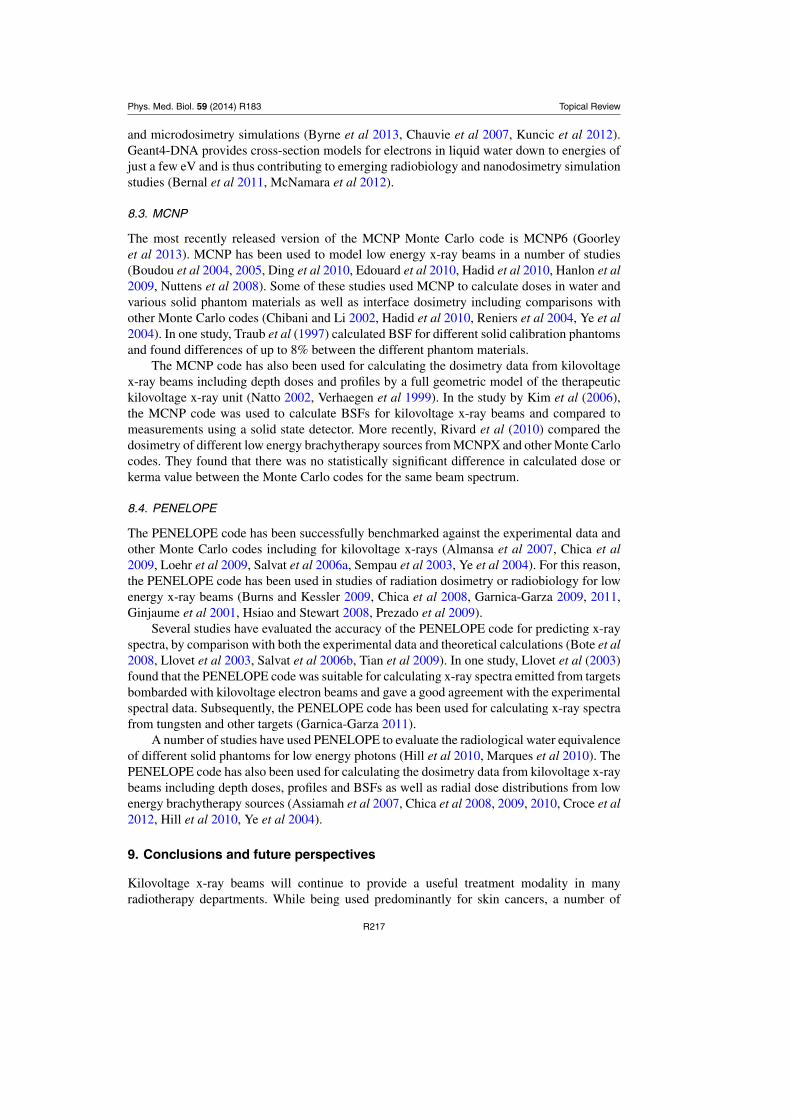
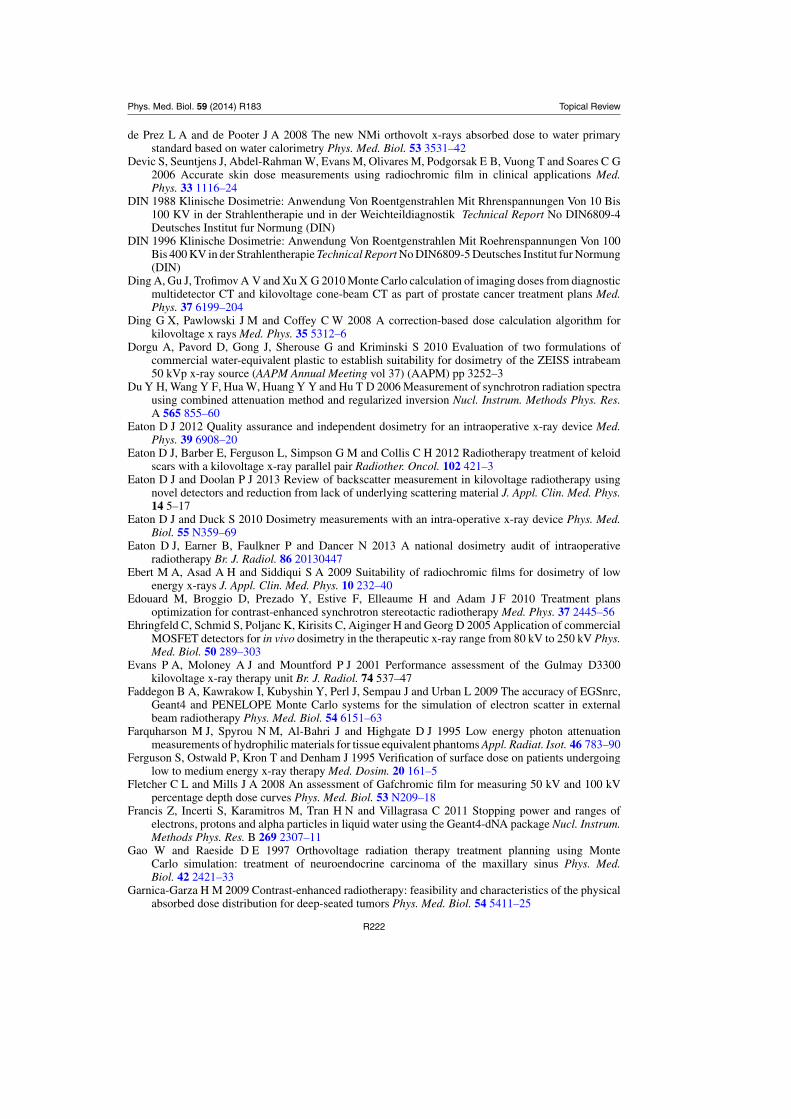
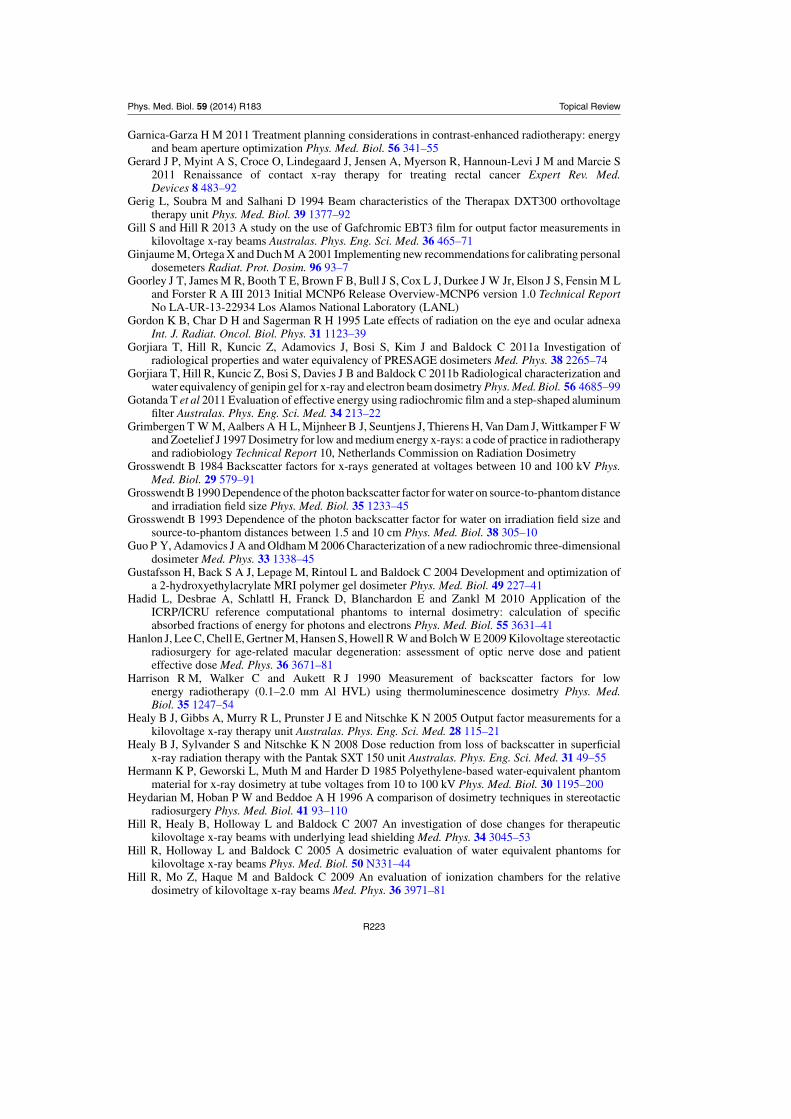
Hill et al (2009) examined ten different ionization chambers for the relative dosimetryof kilovoltage x-ray beams with energies ranging from 50 to 280 kVp. The various chambersstudied were Farmer type chambers, scanning thimble chambers, parallel plate chambers anda PTW PinPoint chamber. The measured data were compared to BEAMnrc Monte Carlocalculations for depth doses for all x-ray beams. The results indicate that the AdvancedMarkus, Markus, NACP and Roos parallel plate ionization chambers were suitable for themeasurement of depth doses for all x-ray beam energies with a total uncertainty of less than3%. These parallel plate chambers were also suitable for measuring in the regions close tothe water surface. The Farmer and scanning chambers had an excellent energy response butwere not suitable for measurements at depths close to the surface due to perturbation effectswhich caused a flattening in the depth doses of up to several per cent right at the surface. Theresults of this comparison for 50 and 280 kVp x-ray beams and in the region close to the waterphantom surface are shown in figures 2 and 3, respectively. Therefore using a larger detector,such as a Farmer chamber, for dose measurements near the water phantom surface will resultin incorrect dose values.
Based on the results listed above, a number of parallel plate ionization chambers aresuitable for the relative dosimetry of kilovoltage x-ray beams and have superior spatialresolution in the depth direction. In particular, the NACP, Markus, Advanced Markus, Roosand PTW N23342 parallel plate chambers were found to be acceptable for most depth dosemeasurements in the energy range from 40–300 kVp (Gerig et al 1994, Hill et al 2009, Knooset al 2007, Li et al 1997a, 1998, Munck Af Rosenschold et al 2008). In general, these parallelplate chambers give doses that are within a few percentage of either Monte Carlo calculations,published depth doses using BJR Report 25 or with doses measured at depth using Farmertype ionization chambers.
Therefore, these parallel plate chambers can be used to directly measure depth doseswithout needing to apply any depth correction factors with uncertainties of less than 3%.While Farmer type and scanning ionization chambers are generally suitable for both depthdose and profile measurements, they are limited in the minimum depth for which they canaccurately measure. New ionization chambers or ones that have not been previously studiedshould only be used after dosimetric comparisons with a well characterized ionization chamber.
4.4.3. Relative output factors. Relative output factors are required to specify the dose outputfor a particular applicator and/or lead cutout as compared to the dose output for the referenceapplicator (Mayles et al 2007, Williams and Thwaites 2000). Generally, the output factor isdefined at the surface of a water phantom but can also be defined at depth (Hill et al 2005,Williams and Thwaites 2000).
There are a number of methodologies described in the literature for the determination ofrelative dose output factors (Evans et al 2001, Healy et al 2005, Hill et al 2005, Jurado et al2005, Newton et al 2011, Pidikiti et al 2011).
(i) Direct measurement at the surface of a water or a Solid Water equivalent phantom (Healyet al 2005, Hill et al 2005, Jurado et al 2005, Newton et al 2011).
(ii) Measurements at depth in a water or a Solid Water equivalent phantom and application ofPDD data (Evans et al 2001, Jurado et al 2005).
(iii) Measurements in air and use of BSF to determine dose at the water surface (Evans et al2001, Newton et al 2011).
R200
Phys. Med. Biol. 59 (2014) R183 Topical Review
Figure 2. Measured percentage depth dose curves for a variety of ionization chambersand BEAMnrc calculations for a 50 kVp x-ray beam (Hill et al 2009).
The use of published BSF and depth dose data for the calculation of output factorsleads to an increase in dose uncertainties (Chica et al 2008, Ma et al 2001, Munck AfRosenschold et al 2008). There are significant differences between measured output factorsand factors calculated using the ratio of published BSFs. Healy et al (2005) found differencesof more than 10% in measured and calculated output factors for x-ray beams with HVLof 1 and 2 mm of Al and for field sizes of 2 mm diameter. It has also been shown thatoutput factors should be measured in water or a solid phantom which is radiologicallywater equivalent particularly for lower energy photon beams (Healy et al 2005, Hill et al2005). Output factors measured in Plastic Water and perspex have given differences of morethan 5% as compared to those in water, which can potentially lead to a patient overdose orunderdose.
For these reasons, it is recommended that output factors are measured in water (or a waterequivalent solid phantom) for all the combinations of beam energy, applicators and/or field
R201
Phys. Med. Biol. 59 (2014) R183 Topical Review
Figure 3. Measured percentage depth dose curves for a variety of ionization chambersand BEAMnrc calculations for a 280 kVp x-ray beam (Hill et al 2009).
sizes. The use of published BSF or output factors can be used as a verification of measureddata and one should be aware of the uncertainties in the published data (BJR Report 25 1996,Chica et al 2008).
4.4.4. Relative dosimetry of very small field sizes. Several studies have determined therelative dosimetry data for kilovoltage x-rays used for intraoperatative radiation therapy (IORT)and animal irradiators often with very small field sizes (Eaton and Duck 2010, Eaton 2012,Ebert et al 2009, Newton et al 2011, Pidikiti et al 2011). The IORT x-ray units typically deliverx-rays with peak potentials of 50 kVp. By comparison, animal irradiators use kilovoltage x-raytubes generally at higher voltages of around 225 kVp but deliver x-ray beams with small fieldsizes ranging from 40 mm diameter down to 1 mm diameter. Depth dose and profile data havebeen determined in some of these studies using Gafchromic EBT2 film, PinPoint ionization
R202
Phys. Med. Biol. 59 (2014) R183 Topical Review
chambers, PRESAGE radiochromic dosimeters and stereotactic diodes. Newton et al (2011)found there was consistency in the agreement in depth doses and profiles measured using theionization chambers, Gafchromic EBT2 film and the PRESAGE dosimeter.
5. Backscatter factors
The BSF is defined as the ratio between a dose quantity measured on the central axis at thesurface of a phantom facing the radiation source and the same dose quantity at the sameposition free in air (Benmakhlouf et al 2011, Carlsson 1993, Mayles 2007, Petoussi-Hensset al 1998). The reference phantom material for radiation therapy is water and there has beena lot of investigation into the BSF for water Bw.
The most commonly used definition of Bw is the ratio of the water collision kerma at apoint on the beam axis at the surface of a full scatter water phantom to the water collisionkerma at the same point in the primary beam with no phantom present (Grosswendt 1984,Ma and Seuntjens 1999). This definition of Bw has been used by the various kilovoltage x-raybeam reference dosimetry protocols (Andreo et al 2000, Grimbergen et al 1997, IPSM 1991,Klevenhagen et al 1996, Ma et al 2001). An alternative definition for Bw is the ratio of theair-kerma at the surface of a phantom such as water to the air-kerma at the same point in spacein the absence of the phantom or free-in-air; this definition is used more in diagnostic radiology(Benmakhlouf et al 2011, Grosswendt 1984, Ma and Seuntjens 1999, Petoussi-Henss et al1998).
Grosswendt (1984) determined that Bw could be calculated from the primary and scatteredphoton spectra at the surface of a water phantom by the following relationship:
Bw =) E
0
!" dφdE
#0 +" dφ
dE
#w$E
!µen(E )
ρ
$w
dE) E
0
" dφdE
#0E!
µen(E )ρ
$w
dE(5)
where" dφ
dE
#0 is the spectrum of primary photons," dφ
dE
#w is the spectrum of photons scatteredwithin the water phantom at the point of interest on the surface,
!µen(E )
ρ
$w
is the mass–energyabsorption coefficient of the photons of energy E in the water and the energy spectrum of thephoton beam is from 0 to energy E.
It has been shown that the BSF varies as a complex function of the x-ray beam energy, fieldsize, SSD and also with different materials in the phantom (Butson et al 2008b, Grosswendt1984, 1990, 1993, Johns and Cunningham 1983, Kim et al 2006, 2010, Klevenhagen et al2000). The BSF has a maximum value for x-ray beams with a HVL of about 1.0 mm Cu or apeak potential of about 150 kVp (Johns and Cunningham 1983).
5.1. Monte Carlo calculations
The main approach in determining BSFs for water and other phantom materials for kilovoltagex-ray beams has been using Monte Carlo calculations (Carlsson 1993, Chica et al 2008,Grosswendt 1984, 1990, 1993, IPSM 1991, Klevenhagen et al 1996, Knight 1992, Maand Seuntjens 1999, Patrocinio et al 1996, Petoussi-Henss et al 1998). However, using themethodology of Grosswendt as listed above, one requires knowledge of the photon spectra forthe calculations. The photon spectra used in various BSF calculations have been determinedfrom the measured spectral data, analytical calculations of the spectra, published spectral dataor by Monte Carlo models of the whole x-ray unit (Aoki and Koyama 2002, Birch and Marshall1979, Chica et al 2008, Grosswendt 1984, 1990, Kim et al 2010, Munck Af Rosenschold et al2008, Nelson and Hill 2011, Seuntjens et al 1987a, 1987b).
R203
Phys. Med. Biol. 59 (2014) R183 Topical Review
5.2. Published BSFs and uncertainties
The AAPM and IPEMB reference dosimetry protocols for kilovoltage x-ray beams make use ofBw based on Monte Carlo calculations (Grosswendt 1984, 1990, 1993, Klevenhagen et al 1996,Ma et al 2001). As stated in the AAPM protocol, these calculations have been independentlyverified by the measurements and independent Monte Carlo calculations (Klevenhagen 1989,Klevenhagen et al 1991a, Knight 1992, Ma et al 2001). The AAPM protocol presents Bw forx-ray beams with a HVL ranging from 0.04 mm Al up to 5 mm Cu and for a wide range offield diameters and SSDs.
A number of investigations have shown that the use of published BSFs can lead to largeuncertainties in dose calculations such as those used in the reference dosimetry. The study byChica et al (2008) examined the uncertainty in absorbed dose calculations due to uncertaintiesin both BSFs and mass–energy absorption coefficients as calculated using the HVL of theradiation beam. They found that the uncertainty can be larger than 5% for some of the x-raybeams and recommended that Bw be calculated using additional parameters such as kVp, inaddition to HVL, so as to reduce the uncertainty to be less than 3%. This approach has beenadopted in at least one kilovoltage dosimetry protocol (Grimbergen et al 1997).
Munck Af Rosenschold et al (2008) designed a full Monte Carlo model of an x-ray unitin order to determine Bw for their 120 and 200 kV x-ray beams. This was in the context ofcomparing different reference dosimetry protocols and comparisons with the published beamdata. They found the differences between published and calculated Bw were within 3% but theuse of calculated Bw reduced the uncertainty in the absorbed dose calculation. However, theystated that using just the HVL as the x-ray beam quality specifier may be the main cause ofsuch differences.
5.3. Measured BSFs
Measurement of the BSF requires the measurement of dose at the surface of a phantom andin-air at the same point. For low-energy x-ray beams, there may be problems with the accuracyof absorbed dose measurements with ionization chambers or other dosimeters (Klevenhagenet al 1991a). The size and shape of the dosimeter may cause perturbations of the photon fluenceand the energy response of the detector may change if the x-ray spectrum changes betweenthe reference and measuring points (Patrocinio et al 1996).
Thin window parallel plate ionization chambers have been used to measured BSFs forx-ray beams in the energy range from 16–40 kVp (Klevenhagen 1989, Kim et al 2006). Theyfound measured BSFs agreed with previously published BSFs generally to within 3–5%.However, the larger differences occurred for x-ray beams with an HVL less than 1 mm andwere attributed to differences in beam filtration.
TLDs have been used in several studies for comparison with BSF factors determined usingionization chamber measurements and Monte Carlo calculations. In two studies, lithium borate(TLD800) was used to measure BSFs for comparison with ionization chamber measurementsand Monte Carlo calculations (Coudin and Marinello 1998, Harrison et al 1990). The studyby Harrison et al (1990) was instrumental in identifying inaccuracies in published BSFs.The results from both studies found a good agreement between BSFs that were measured withTLDs and Monte Carlo calculations. However, there were differences of up to 9% as comparedto ionization chamber measurements.
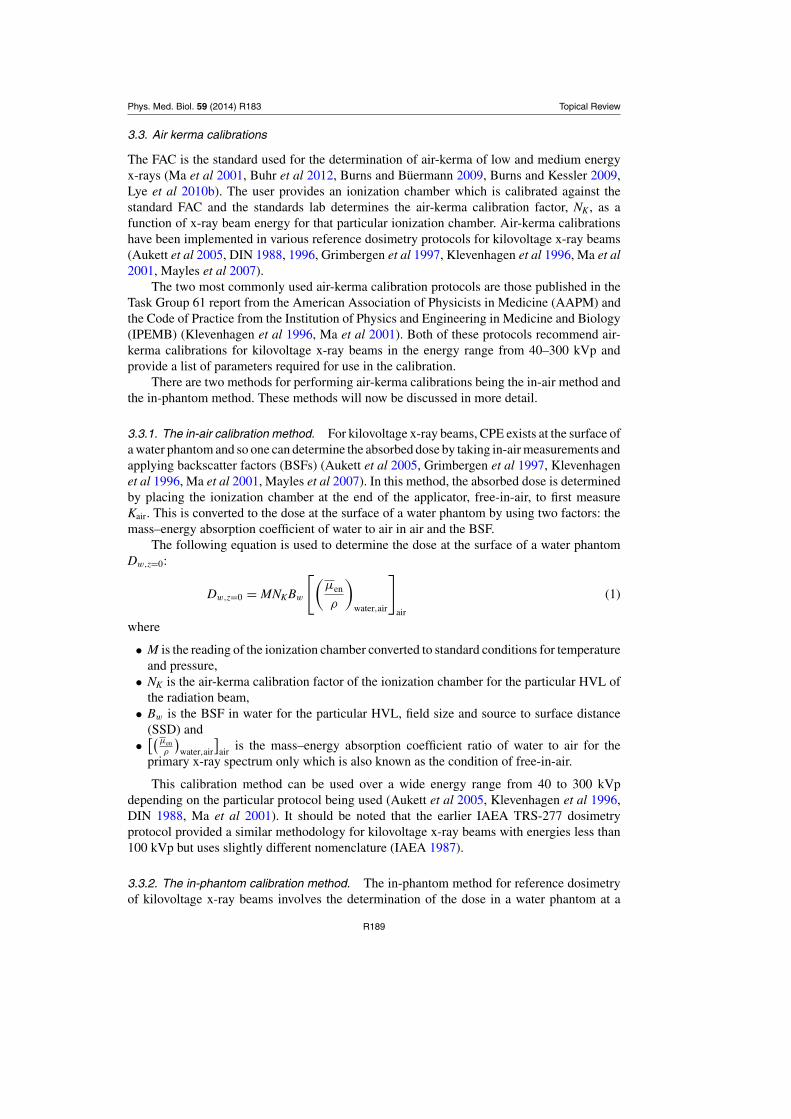
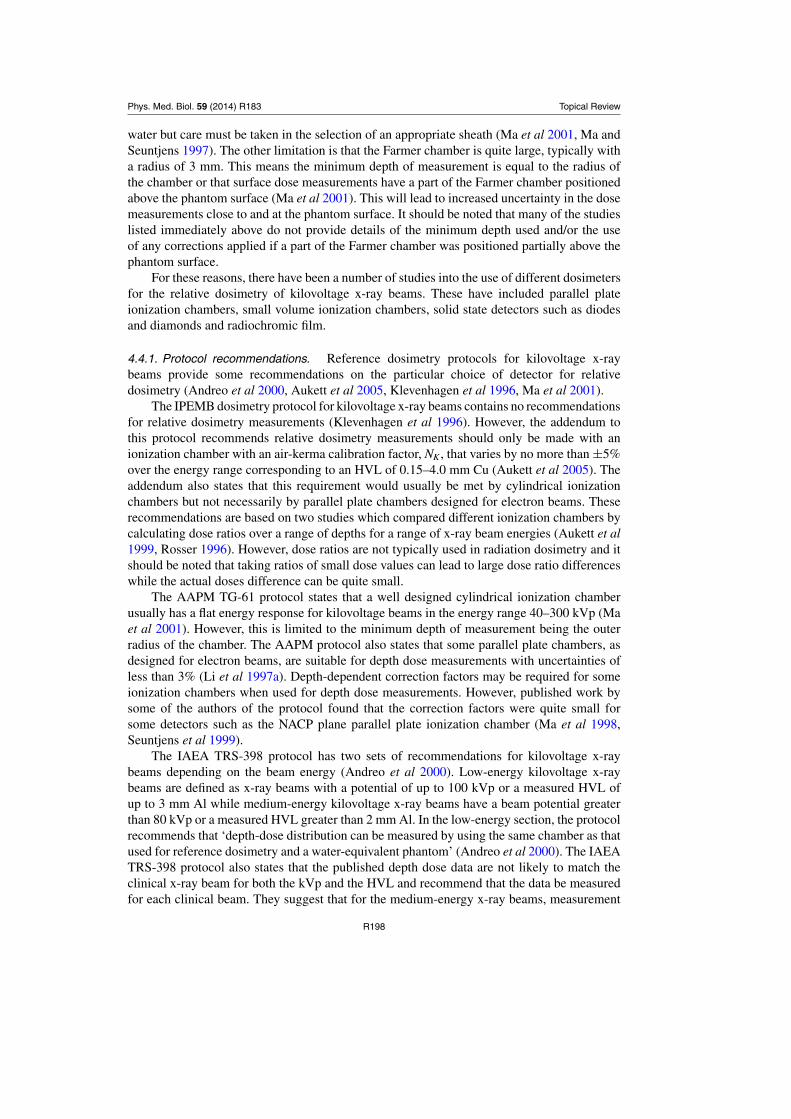
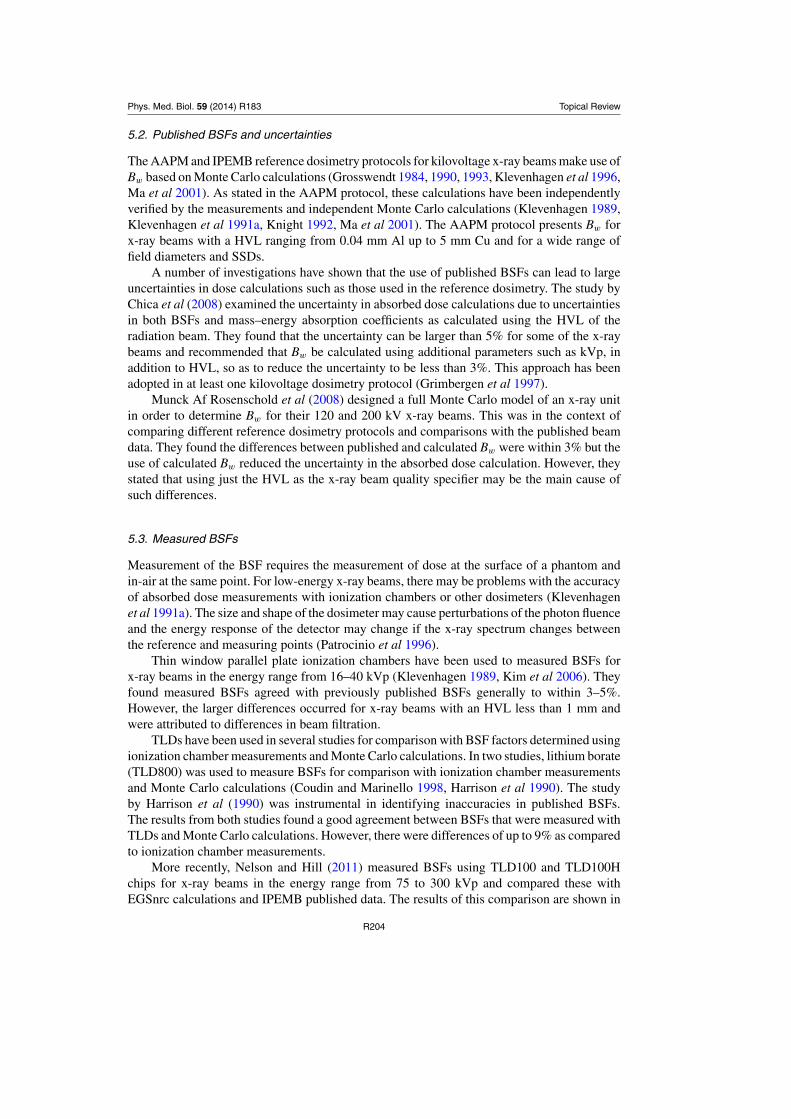
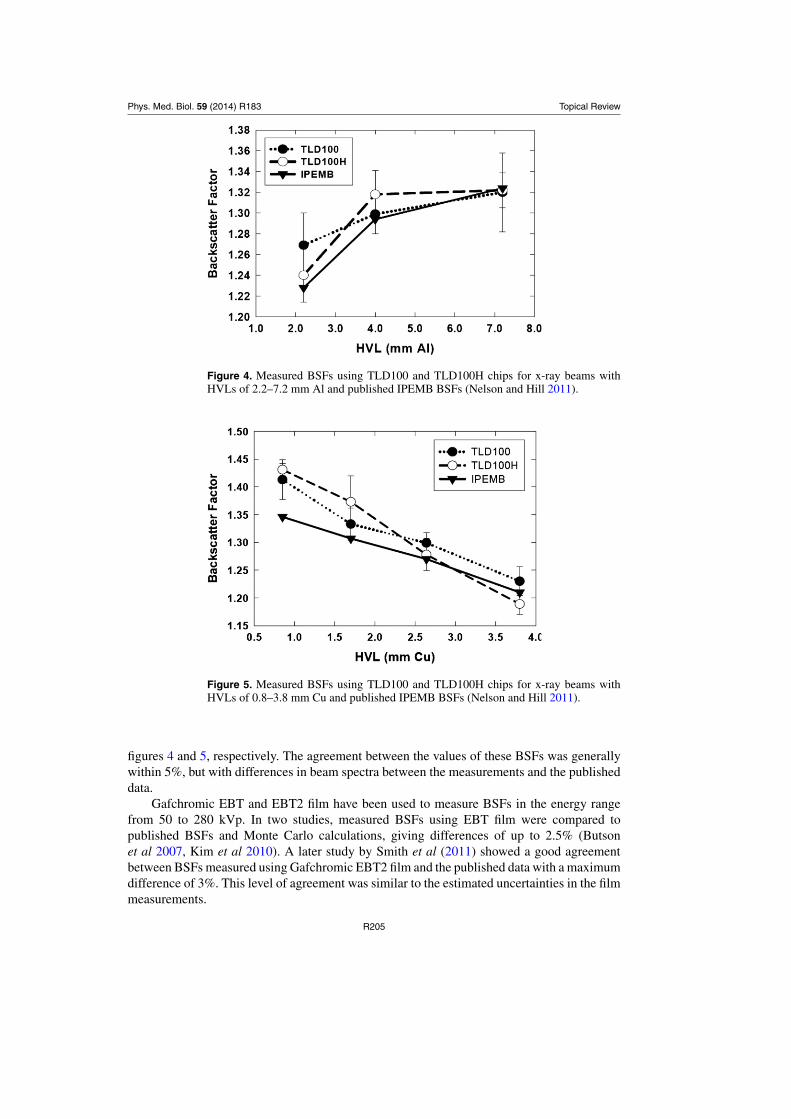
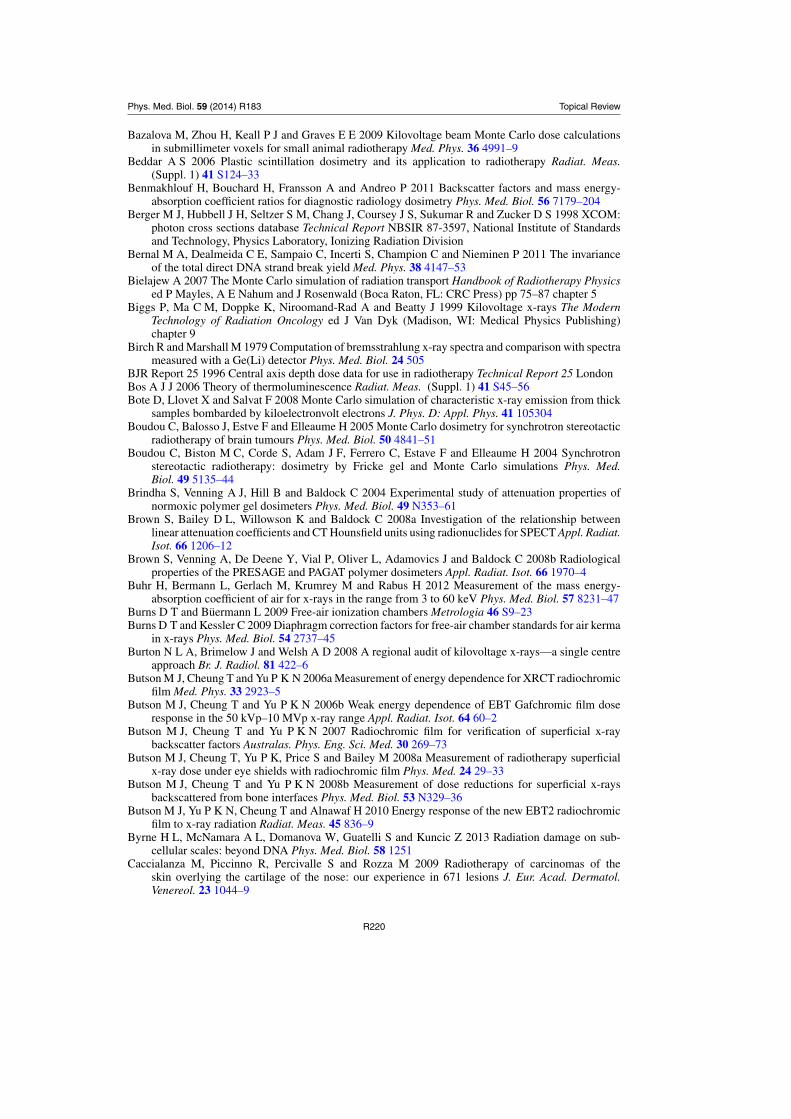
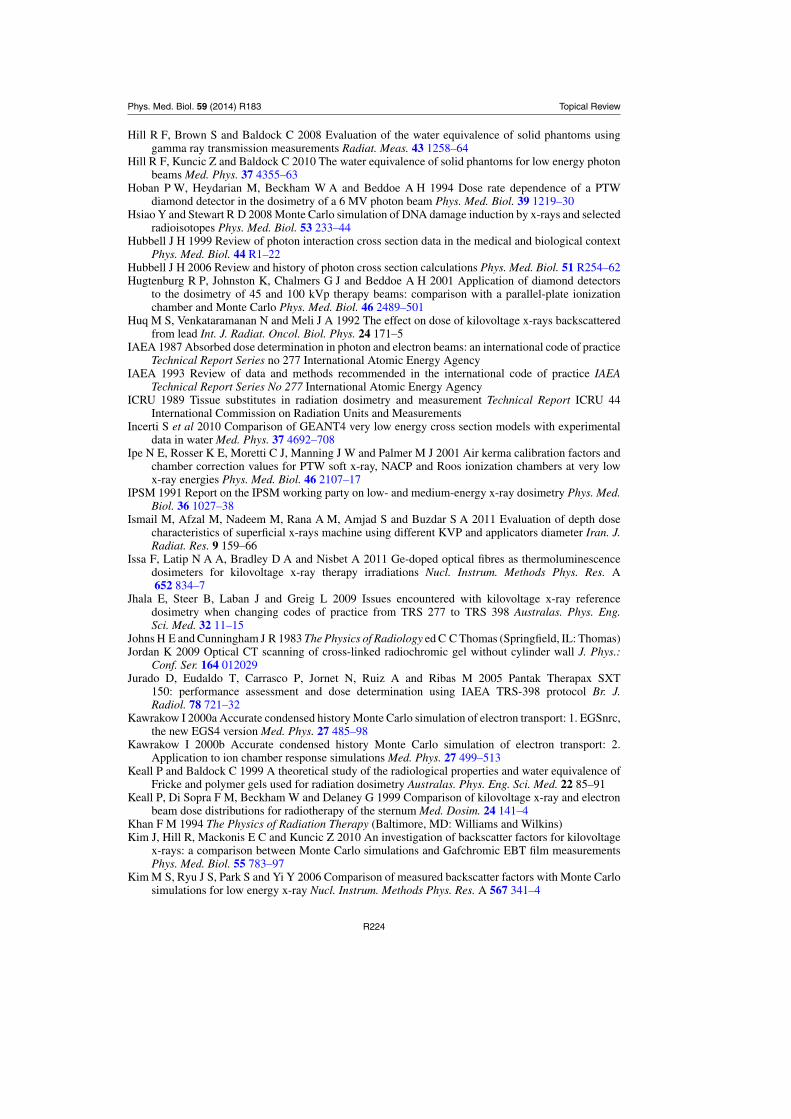
More recently, Nelson and Hill (2011) measured BSFs using TLD100 and TLD100Hchips for x-ray beams in the energy range from 75 to 300 kVp and compared these withEGSnrc calculations and IPEMB published data. The results of this comparison are shown in
R204
Phys. Med. Biol. 59 (2014) R183 Topical Review
Figure 4. Measured BSFs using TLD100 and TLD100H chips for x-ray beams withHVLs of 2.2–7.2 mm Al and published IPEMB BSFs (Nelson and Hill 2011).
Figure 5. Measured BSFs using TLD100 and TLD100H chips for x-ray beams withHVLs of 0.8–3.8 mm Cu and published IPEMB BSFs (Nelson and Hill 2011).
figures 4 and 5, respectively. The agreement between the values of these BSFs was generallywithin 5%, but with differences in beam spectra between the measurements and the publisheddata.
Gafchromic EBT and EBT2 film have been used to measure BSFs in the energy rangefrom 50 to 280 kVp. In two studies, measured BSFs using EBT film were compared topublished BSFs and Monte Carlo calculations, giving differences of up to 2.5% (Butsonet al 2007, Kim et al 2010). A later study by Smith et al (2011) showed a good agreementbetween BSFs measured using Gafchromic EBT2 film and the published data with a maximumdifference of 3%. This level of agreement was similar to the estimated uncertainties in the filmmeasurements.
R205
Phys. Med. Biol. 59 (2014) R183 Topical Review
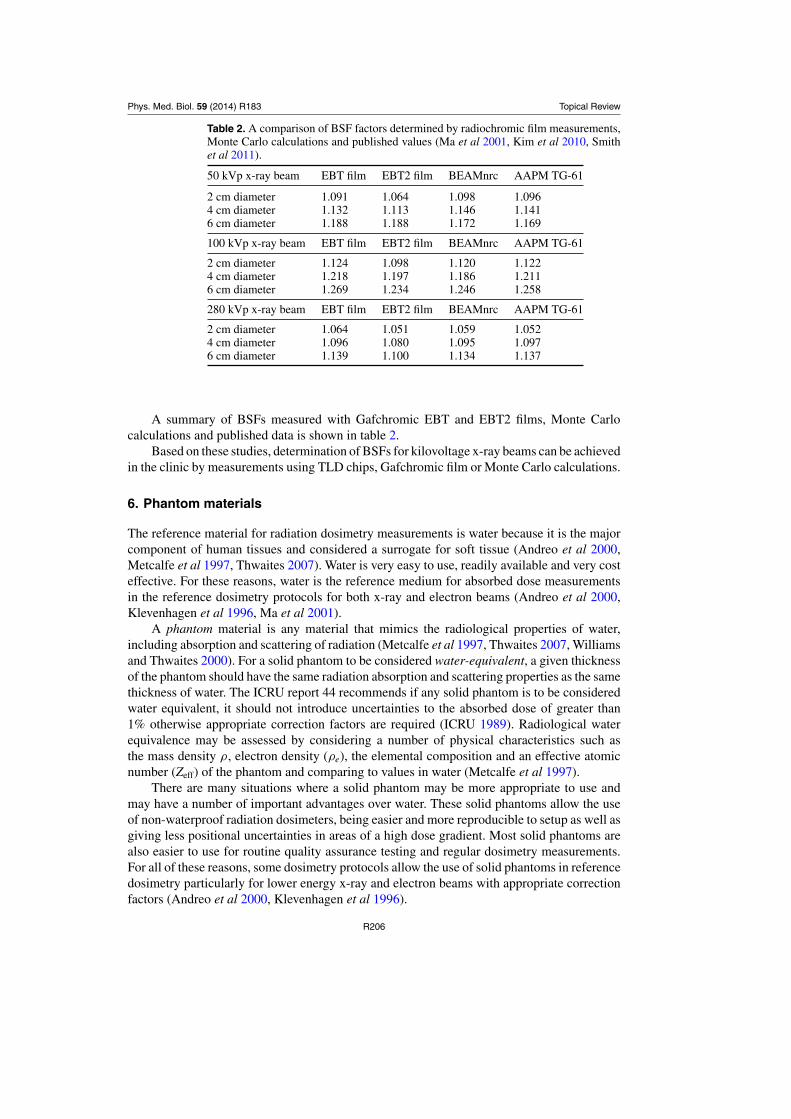
Table 2. A comparison of BSF factors determined by radiochromic film measurements,Monte Carlo calculations and published values (Ma et al 2001, Kim et al 2010, Smithet al 2011).
50 kVp x-ray beam EBT film EBT2 film BEAMnrc AAPM TG-61
2 cm diameter 1.091 1.064 1.098 1.0964 cm diameter 1.132 1.113 1.146 1.1416 cm diameter 1.188 1.188 1.172 1.169
100 kVp x-ray beam EBT film EBT2 film BEAMnrc AAPM TG-61
2 cm diameter 1.124 1.098 1.120 1.1224 cm diameter 1.218 1.197 1.186 1.2116 cm diameter 1.269 1.234 1.246 1.258
280 kVp x-ray beam EBT film EBT2 film BEAMnrc AAPM TG-61
2 cm diameter 1.064 1.051 1.059 1.0524 cm diameter 1.096 1.080 1.095 1.0976 cm diameter 1.139 1.100 1.134 1.137
A summary of BSFs measured with Gafchromic EBT and EBT2 films, Monte Carlocalculations and published data is shown in table 2.
Based on these studies, determination of BSFs for kilovoltage x-ray beams can be achievedin the clinic by measurements using TLD chips, Gafchromic film or Monte Carlo calculations.
6. Phantom materials
The reference material for radiation dosimetry measurements is water because it is the majorcomponent of human tissues and considered a surrogate for soft tissue (Andreo et al 2000,Metcalfe et al 1997, Thwaites 2007). Water is very easy to use, readily available and very costeffective. For these reasons, water is the reference medium for absorbed dose measurementsin the reference dosimetry protocols for both x-ray and electron beams (Andreo et al 2000,Klevenhagen et al 1996, Ma et al 2001).
A phantom material is any material that mimics the radiological properties of water,including absorption and scattering of radiation (Metcalfe et al 1997, Thwaites 2007, Williamsand Thwaites 2000). For a solid phantom to be considered water-equivalent, a given thicknessof the phantom should have the same radiation absorption and scattering properties as the samethickness of water. The ICRU report 44 recommends if any solid phantom is to be consideredwater equivalent, it should not introduce uncertainties to the absorbed dose of greater than1% otherwise appropriate correction factors are required (ICRU 1989). Radiological waterequivalence may be assessed by considering a number of physical characteristics such asthe mass density ρ, electron density (ρe), the elemental composition and an effective atomicnumber (Zeff) of the phantom and comparing to values in water (Metcalfe et al 1997).
There are many situations where a solid phantom may be more appropriate to use andmay have a number of important advantages over water. These solid phantoms allow the useof non-waterproof radiation dosimeters, being easier and more reproducible to setup as well asgiving less positional uncertainties in areas of a high dose gradient. Most solid phantoms arealso easier to use for routine quality assurance testing and regular dosimetry measurements.For all of these reasons, some dosimetry protocols allow the use of solid phantoms in referencedosimetry particularly for lower energy x-ray and electron beams with appropriate correctionfactors (Andreo et al 2000, Klevenhagen et al 1996).
R206
Phys. Med. Biol. 59 (2014) R183 Topical Review
Table 3. Composition of phantom materials A150, PAGAT, perspex (PMMA),polystyrene, Plastic Water (PW), Plastic Water DT (PWDT), RMI-457 Solid Water(RMI-457), white polystyrene (RW3), Virtual Water (VW) and water.
DensityPhantom (gm cm-1) Fractional weights of the elements
There are many solid phantom materials available for radiation dosimetry measurementsincluding perspex, polystyrene and a range of epoxy resin based analogue materials. Thefractional weight of many common phantom materials are listed in table 3 (Andreo et al(2000), Brown et al (2008b), Hill et al (2008), Ramaseshan et al (2008), Seco and Evans(2006)).
6.1. Testing for water equivalence
Testing for the radiological water equivalence of a solid phantom material has been performedusing a number of experimental and analytical methodologies as follows:
(i) Comparison of relative dosimetry measurements such as depth doses, output factors andBSFs (Allahverdi et al 1999, Christ 1995, Dorgu et al 2010, Healy et al 2005, Hermannet al 1985, Hill et al 2005, Li et al 1999, Liu et al 2003, Ramaseshan et al 2008, Shrimptonet al 1981, Tello et al 1995, Thomadsen et al 1995).
(ii) Transmission measurements using either gamma rays or x-ray beams (Brown et al 2008a,Constantinou et al 1982, Hermann et al 1985, Hill et al 2008).
(iii) Determination of CT numbers or electron densities of different materials (Bazalova et al2008, Brown et al 2008a, Gorjiara et al 2011a, 2011b, Seco and Evans 2006).
(iv) Relative dosimetry calculations from brachytherapy sources (Luxton 1994, Meigooni et al1988, 1994, Meli et al 1988, Pantelis et al 2004, Reniers et al 2004).
(v) Determination of the mass–energy absorption coefficients (Baldock et al 2010, Brownet al 2008b, Farquharson et al 1995, Hill et al 2005, Keall and Baldock 1999, Midgley2005, Reft 1989, Stern and Kubo 1995, Venning et al 2005b, White 1977, 1978).
(vi) Monte Carlo calculations of relative doses or phantom material correction factors (Gorjiaraet al 2011a, 2011b, Hill et al 2010, Seuntjens et al 2005).
A number of studies have evaluated the use of various epoxy resin solid phantoms for bothreference dose calibrations and relative dosimetry of megavoltage x-ray and electron beams(Allahverdi et al 1999, Tello et al 1995, Thomadsen et al 1995). It was found that radiationdoses measured in these particular solid phantoms can differ by more than 1%, as comparedto water, leading to the need for correction factors.
R207
Phys. Med. Biol. 59 (2014) R183 Topical Review
However, as emphasized by White (1978), radiological water equivalence is often assumedover a large energy range when in fact testing is often performed for a limited energy range. Themethod recommended by White for comparing the radiation properties of the solid phantomis to calculate the total mass-attenuation coefficient (µ/ρ), total mass–energy absorptioncoefficient (µ/ρen), electron mass stopping powers (S/ρ) and electron angular scatteringpowers (θ2/ρl) over the energy range of interest.
6.2. Solid phantom dosimetry for kilovoltage x-ray beams
For therapeutic kilovoltage x-ray beams, a number of studies have investigated the relativedosimetry of solid phantoms in comparison to water. In early studies, the investigationsinvolved varying comparisons including calculating mass attenuation coefficients, mass–energy absorption coefficients, BSFs, attenuation curves and/or depth doses in solid phantomssuch as RW1, an older version of RMI Solid Water, polystyrene and in water (Hermann et al1985, Shrimpton et al 1981, Stern and Kubo 1995). Both the RMI Solid Water and RW1materials were found to be water equivalent even for low energies, while polystyrene gavedepth dose differences of up to 10%.
Li et al (1999) compared the MS11 epoxy resin solid phantom, polystyrene and polymethylmethacrylate (PMMA) by measuring relative detector readings as a function of depth for 100and 300 kVp x-ray beams. Their results indicated that doses measured in the MS11 phantommaterial were within 1% of those in water for both x-ray beam energies. In comparison, therelative doses measured in both the polystyrene and PMMA phantoms were higher than thosein water.
Hill et al (2005) studied the radiological water equivalence of RMI-457 Solid Water(Gammex Inc., Wisconsin, USA) and Plastic Water (PW) (Computerized Imaging ReferenceSystems, Virginia, USA) by comparing relative and reference dosimetry measurements forx-ray beams in the energy range 75–300 kVp. They found that RMI-457 Solid Water wassuitable for depth doses and output factors for all beam energies with a maximum deviationof 2.4% for the 75 kVp x-ray beam depth dose. In comparison, PW gave large differences inthe depth doses of more than 20% and also in the relative output factors of up to 6%.
One study evaluated measured depth doses in PW, Solid Water, perspex (PMMA) andwater for x-ray beam qualities with HVLs of 1–13 mm Al (Healy et al 2005). They found thatPerspex over-predicts the dose as compared to water while doses measured in a Solid Waterphantom gave a good agreement to the doses in water for all energies. However, the dosesmeasured with PW were all consistently lower than the doses measured in water.
Gamma ray transmission measurements from a technetium-99m source were used toevaluate radiological water equivalence of RMI-457 Solid Water, PW and RW3 whitepolystyrene (PTW-Freiburg, Freiburg, Germany) (Hill et al 2008). Linear attenuationcoefficients were determined from the transmission values and compared with calculatedvalues determined from Monte Carlo calculated transmission curves using the EGSnrc MonteCarlo code and NIST values. The results showed that RMI-457 Solid Water, PW and solidphantoms had transmission values that agreed to those in water to within 1.5% for this gammaray energy.
One study evaluated the radiological water equivalence of the Plastic Water diagnostictherapy (PWDT) solid phantom (Computerized Imaging Reference Systems, Virginia, USA)(Ramaseshan et al 2008). Depth doses were measured for a wide range of x-ray energiesincluding 80, 100 and 250 kVp beams. It was found that doses measured with PWDT agreedto within 1.5% of those determined in water and Solid Water, confirming that the PWDT solidphantom is suitable for dosimetry of low energy x-rays.
R208
Phys. Med. Biol. 59 (2014) R183 Topical Review
Figure 6. Calculated depth doses in a number of commonly used solid phantoms for a50 kVp x-ray beam and with a 2 cm diameter field size (Hill et al 2010).
Figure 7. Calculated depth doses in a number of commonly used solid phantoms for a180 kVp x-ray beam and with a 8 cm diameter field size (Hill et al 2010).
Hill et al (2010) performed a study of the radiological water equivalence of ten commonlyused solid phantoms and water for low energy photon beams using the PENELOPE MonteCarlo code. The calculations performed in all phantoms were depth doses, lateral beam profilesas well as dose to a small water volume at the surface of the solid phantom for x-ray beamswith energies from 50–300 kVp. The results showed that the A150, PAGAT gel, PWDT, RMI-457 Solid Water and Virtual Water (VW) (CMNC, Tennessee, USA) could be consideredradiologically water equivalent at all photon energies with dose differences of less than 2%. Incomparison, the following phantoms gave significant dose differences as compared to water:PW, PMMA, polystyrene, PRESAGE and RW3. The results of the comparison of depth dosesin the different solid phantoms for a 50 kVp x-ray beam (2 cm diameter field) and for a 180kVp x-ray beam (8 cm diameter field) are shown in figures 6 and 7, respectively.
R209
Phys. Med. Biol. 59 (2014) R183 Topical Review
Table 4. A summary of suitable and unsuitable solid phantom materials for kilovoltagex-ray beam dosimetry based on radiological water equivalence.
X-ray Suitable Unsuitableenergy phantom phantom
Reference range material material
Hermann et al (1985) 10–100 kVp MS11Meigooni et al (1994) 50–300 kVp RMI Solid Water Plastic WaterStern and Kubo (1995) 40–150 kVp RMI Solid Water PolystyreneLi et al (1999) 40–150 kVp MS11 PMMA
PolystyreneReniers et al (2004) I125 WT1 Solid Water PMMA
PTW RW1Hill et al (2005) 75–300 kVp RMI-457 Solid Water Virtual WaterHealy et al (2005) 80–150 kVp Solid Water PMMA
Plastic WaterRamaseshan et al (2008) 75–300 kVp Plastic Water DTHill et al (2010) 50–280 kVp A150 Plastic Water
PAGAT PMMAPlastic Water DT PolystyreneRMI-457 PRESAGEVirtual Water RW3
Based on these studies, it is recommended to use one of the solid phantoms which has beenshown to have a good agreement in doses with water such as A150, MS11, RMI-457 SolidWater, PWDT and VW. A summary of the suitable and unsuitable solid phantom materials,along with the particular x-ray energy range, is presented in table 4. Any solid phantom shouldbe tested in the clinic to ensure that it is suitably water equivalent and this should include themeasured data for the x-ray beam energies used.
6.3. Effective atomic numbers of solid phantoms
It has been suggested that solid phantoms may be characterized for radiological waterequivalence by calculation of their effective atomic number Zeff (Manohara et al 2008, Raoet al 1985, Taylor et al 2008, Yang et al 1987). The original definition of Zeff for a mixturewas proposed by Mayneord and given by the following equation:
Zeff =*
+
i
αiZni
,1/n
(6)
where αi is the fractional electronic composition, Zi is the atomic number of the ith elementand n = 2.94 (White 1977). The fractional electronic composition is given by the followingequation:
αi = wi (Zi/Ai)-i wi (Zi/Ai)
(7)
where Ai is the mass number and wi is the fractional chemical composition of the ith element.This method has been used extensively in the literature with other authors using varying
values of n ≃ 2.94–3.5 (see e.g. Bazalova et al 2008, Johns and Cunningham 1983, White1977). However, this methodology may only be valid in the region where the photoelectriceffect is the dominant interaction process (Johns and Cunningham 1983). Several authors haveextended this definition of Zeff to use different values of n according to changes in the dominant
R210
Phys. Med. Biol. 59 (2014) R183 Topical Review
photon interaction process with photon energy (Naydenov et al 2004, White 1977, Yang et al1987).
A number of studies have shown that Zeff varies as a function of photon energy if onecompares the radiological properties of the phantom material over the energy range of interest(Manohara et al 2008, Naydenov et al 2004, Rao et al 1985, Taylor et al 2008, Yang et al1987). The other limitation of many calculations of Zeff is that they are often limited to singlephoton energies and do not consider the spectrum of photons in an x-ray beam (Rao et al1985).
An alternative definition is that of mean atomic number Z which is defined in the followingequation (Andreo et al 2000):
Z =-
i wiZ2
iAi-
i wiZiAi
. (8)
This methodology is used by the IAEA TRS-381 and TRS-398 reference dosimetry protocolsto characterize different solid phantom materials for radiation dosimetry measurements.However, this is a single parameter and is not necessarily valid over all photon energies.In addition, it has been shown that Z is not a good indicator of radiological water equivalenceof a phantom for low energy x-rays (Hill et al 2010).
Based on these results, it is not recommended to use calculations of Zeff or Z fordetermining the radiological water equivalence of a solid phantom for low energy x-raybeams.
6.4. Effects of different phantom materials on BSF
It has been shown that the BSF varies according to the thickness of underlying phantommaterial and varies slightly for different SSDs (Klevenhagen 1982). In addition, there arechanges in backscatter dose due to underlying high atomic number materials such as bone orlead as compared to a water phantom only (Butson et al 2008b, Healy et al 2005, Hill et al2007, Huq et al 1992, Lanzon and Sorell 1993). This is due to the increased dose absorptionin the high atomic number material leading to a reduction in the backscatter radiation at thephantom surface.
It has also been shown that the scattering properties of different solid phantoms can varysignificantly as compared to water particularly for lower energy x-ray beams. Any differencesin backscatter can have implications for radiation dosimetry measurements as these largewater equivalent phantoms are used to provide full backscatter conditions (Klevenhagen et al1996). Some materials such as PMMA and the ICRU soft tissue material are used routinelyfor radiation dosimetry measurements (Schauer et al 2000, Schwahn and Gesell 2008, Traubet al 1997). One study used Monte Carlo methods to calculate BSF ratios of various ICRUtissues as compared to water (Ma and Seuntjens 1999). They found negligible differences ofless than 1% for the ICRU soft tissue but differences of up to 15% for the ICRU bone.
In the study by Hill et al (2010), it was found that different solid phantoms had significantvariations in backscatter contribution to the dose to a small volume of water located at thesurface of the solid phantom. They found that there were differences of up to 9.1% forpolystyrene as compared to water only for a 50 kVp x-ray beam. There were significantdifferences in surface dose when the PW, PMMA and RW3 solid phantoms were used forbackscatter. However, the differences in dose decreased as the x-ray beam energy becamehigher. Another study compared BSFs determined from measurements in ISO water phantomsand Perspex phantoms along with calculated BSFs in ICRU tissues and in PMMA (Schauer
R211
Phys. Med. Biol. 59 (2014) R183 Topical Review
et al 2000). They found that the BSFs measured in PMMA were up to 6.9% greater than thosemeasured in the ISO water phantom.
Based on these results, it is recommended that one uses a radiologically equivalentphantom for any dosimetry measurements including an appropriate choice for backscattermaterial.
7. Treatment planning
7.1. Manual calculations
Treatment planning for kilovoltage x-ray beams is generally performed by manual calculationsof either monitor units or treatment times. The dose is usually prescribed at the surface wherethe relative depth dose value is 100%. However in some cases, the radiation oncologist maywish to prescribe a dose at depth for which a depth dose correction is required. The energyof the particular beam selected is usually based on the depth dose characteristics with thesurface dose of 100% and the required doses at depth to ensure sufficient dose coverage e.g.depth of the 95% or 90% dose value. Isodose curves can be used by the radiation oncologistfor planning purposes in order to view a 2D map of the radiation dose. However, it should benoted that there will be a slight asymmetry in the isodoses due to the heel effect (Johns andCunningham 1983, Mayles et al 2007).
The dose delivered to a patient for a particular x-ray beam energy will depend on a numberof factors (Mayles et al 2007, Williams and Thwaites 2000).
(i) Depth dose value at the dose prescription point.(ii) Treatment applicator.
(iii) Area of the radiation beam including any shielding.(iv) Any offset between the end of the applicator and skin surface.
The x-ray unit is usually calibrated using a reference applicator and so the relative doseoutput for any other applicator needs to be considered by use of an applicator factor. Thereference applicator is either a large diameter circular applicator or a 10 × 10 cm2 squareapplicator.
Cutout factors are required if a lead cutout is used to define the beam shape. These cutoutfactors are usually measured in water or a water equivalent solid phantom. The cutout factorcan be estimated by taking the ratio of the BSF for the cutout and the BSF for the openapplicator but this method does not consider differences of scatter in the applicators used. Inaddition, the BSFs are most likely interpolated from a dataset of generic BSFs (BJR Report25 1996, Klevenhagen et al 1996). For a very irregular cutout shape, a Clarkson integrationmethod can be used to improve accuracy of the predicted cutout factor (Mayles et al 2007).
An inverse square law correction factor should be applied if there is a gap between the endof the applicator and the skin surface. However, additional correction factors may be requiredfor very large gap distances of greater than 15 cm (Li et al 1997b).
Most current kilovoltage x-ray units provide dose delivery based on the selection ofmonitor units (Van Dyk 1999). However, many units can also provide dose delivery based ona timer mode and this will be the only option available for older x-ray units that do not have amonitoring ionization chamber.
7.2. Computer calculations
Modern radiotherapy treatment planning systems have been designed for dose calculationsof megavoltage x-ray and electron beams (Mayles et al 2007, Van Dyk 1999). These dose
R212
Phys. Med. Biol. 59 (2014) R183 Topical Review
calculation algorithms such as pencil beam and convolution/superposition rely on electrondensity information from the CT data and dose kernels. However, these are applicable primarilyfor megavoltage x-ray beams where the Compton effect is the dominant interaction processand is dependent on the electron density of the particular medium.
There have been a limited number of investigation of using treatment planningsystems for kilovoltage x-ray beams. Alaei et al (2000) investigated the accuracy of aconvolution/superposition treatment planning system for predicting kilovoltage x-ray beamdosimetry. Customized dose calculation kernels for beam energies down to 20 keV were usedin the planning system. They found that the agreement between TLD measured and computeddoses was within 2% for materials similar to water. However, in the region around boneinhomogeneities, there were dose differences of up to 145%.
More recently, calculation algorithms for kilovoltage x-ray beams have been developedprimarily for on-board imaging systems on linear accelerators (Ding et al 2008, Pawlowskiand Ding 2011). These algorithms include corrections for different tissues types such as softtissue and bone and have been shown to give dose errors of less than 3% (Pawlowski and Ding2011). While these algorithms were designed for cone-beam CT dose calculations, there is thepotential for them to be also used for therapeutic kilovoltage x-ray beams.
Several groups have investigated the use of Monte Carlo methods to calculate isodosesfor patient CT data (Gao and Raeside 1997, Knoos et al 2007). The latter work presentspatient dose calculations that were performed for both head/neck and thoracic treatments andproposed that such calculations would be of benefit to the radiation oncologist (Knoos et al2007).
7.3. Dose to other tissues
The dose at the surface of a different medium, Dmed,z=0 can be determined from the dose atthe water phantom surface, Dw,z=0 by a correction factor, Cmed
w , which is defined as follows(Ma et al 2001):
Cmedw = Bmed
Bw
%&µen
ρ
'
med,w
(
air
(9)
where!"µen
ρ
#med,w
$air is the ratio of the mass–energy-absorption coefficients of the medium
and water averaged over the primary photon spectrum free in air and Bmed and Bw are theBSFs for the medium and the water respectively (Ma et al 2001). The AAPM TG-61 reportcontains published correction factors for a number of different tissue types and are based onthe previously calculated data (Ma and Seuntjens 1999, Seuntjens et al 1987b).
7.4. Shielding and interface effects
High density materials such as lead are often used for shielding of healthy tissues duringkilovoltage x-ray beam treatments. Lead is an excellent shielding material due to its highatomic number and density as well as being malleable and so can be modified to the shapeof the patient. However, it is important to note that the lead will also reduce backscatter andlead to a dose reduction in the dose at the surface (Das and Chopra 1995, Eaton and Doolan2013, Healy et al 2008, Hill et al 2007, Huq et al 1992, Lanzon and Sorell 1993). This dosereduction is a function of field size, lead shielding thickness, beam energy and the depth ofthe lead shielding with a maximum reduction occurring for beam energies at approximately100 kVp (Das and Chopra 1995, Healy et al 2008, Hill et al 2007). Figure 8 shows the surfacedose ratio, which is defined as the ratio of measured surface doses with an underlying lead
R213
Phys. Med. Biol. 59 (2014) R183 Topical Review
Figure 8. Measured surface dose ratios for lead shielding at a range of depths with a100 kVp x-ray beam and for field sizes of 2, 5 and 8 cm diameter (Hill et al 2007).
sheet and in a full water phantom, for a 100 kVp x-ray beam and three field sizes with the leadsheet positioned at a range of depths.
It has also been shown that underlying bone or air cavities also lead to a reduction inbackscatter and therefore a reduction in the surface dose (Butson et al 2008b, Hill et al 2007).Therefore, it is recommended that an assessment be made of any possible reduction in dose.
Related to this are conditions where there is a lack of full backscatter. For example, ifyou are treating the hand, the dose at the surface will not receive full backscatter thus leadingto a reduction in the surface dose (Healy et al 2008, Klevenhagen 1982). It is recommendedto treat such patients with additional backscatter material under the hand. Alternatively, onecould increase the treatment time to counter the loss of backscatter with a factor calculatedfrom the published data (Klevenhagen 1982).
There are also significant dose perturbations close to the interface between water/soft-tissue and a high density material (Das and Chopra 1995, Das 1997, Mitchell et al 1998,Regulla et al 2000). The comprehensive study by Das and Chopra (1995) investigated thevariations in the backscatter dose perturbation factor (BSDF) as a function of the atomicnumber of the shielding material, beam energy, field size and distance from the interface. Theyshowed that the BSDF can be more than a factor of 15 for a soft-tissue/lead interface. It isrecommended that when lead is used behind the treatment volume, such as the lip or the ear,the lead is covered with a layer of low atomic number materials such as wax (Mayles et al2007).
Lead shielding is commonly used for treatments using kilovoltage x-ray beams to definethe shape of the radiation beam. However, lead can generate contaminant electrons which cansignificantly increase the dose right at the surface (Lee and Chan 2000, Lye et al 2010a). Inthe study by Lye et al (2010a), Monte Carlo calculations and Gafchromic film measurementswere used to determine the amount of electron contamination. They found that the doseenhancement, due to electron contamination, was double the dose at the edge of the lead ascompared to the central axis for the 150 kVp beam and three times for the 300 kVp beam. Itwas recommended that these contaminant electrons could be removed by wrapping the lead
R214
Phys. Med. Biol. 59 (2014) R183 Topical Review
cutout with thin plastic wrap. It should be noted that increased electron contamination can alsobe generated from treatment cones made of high atomic number materials (Klevenhagen et al1991b).
For kilovoltage treatments close to the eye, the use of internal eye shields can be usedto reduce dose to critical structures such as the lens which have much lower dose tolerances(Amdur et al 1992, Baker et al 2002, Butson et al 2008a, Gordon et al 1995, Wang et al 2012).While the eye shield may provide a large reduction in the primary dose, scattered radiationcan contribute up to 25% of the prescribed dose (Baker et al 2002). These studies showed thatthe actual dose to the lens, even with shielding, varied significantly according to the field size,shielded area and beam energy.
8. Monte Carlo methods for radiation transport
Monte Carlo calculation methods are widely used for solving radiation transport problemsand a number of excellent review articles are recommended for more details (Bielajew 2007,Rogers 2006, Salvat and Fernandez-Varea 2009, Verhaegen and Seuntjens 2003). The MonteCarlo codes applicable for medical radiation physics are EGSnrc (Kawrakow 2000a, 2000b),FLUKA (Kling et al 2001), GEANT4 (Agostinelli et al 2003, Allison et al 2006), MCNPX(Kling et al 2001, Verhaegen and Seuntjens 2003, Waters et al 2007) and PENELOPE (Salvatet al 2006a, Sempau et al 2003). These codes are capable of simulating photon–electrontransport through matter in the relevant energy range in medical physics applications coveringfrom keV up to many MeV.
However, it should be noted that the different codes can give significant differences intheir results, such as dose calculations, particularly in the low energy photon range (Almansaet al 2007, Reniers et al 2004, Rivard et al 2010, Verhaegen and Seuntjens 2003, Ye et al2004). One component of these differences is the use of different photon cross section data(Hubbell 2006, Zaidi 2000). Photon cross section databases have developed with time usingboth theoretical calculations and the experimental data (Hubbell 1999, 2006). The most up-to-date databases are the Evaluated Photon Data Library (EPDL97) which is managed by theLawrence Livermore National Laboratory and the XCOM database which is managed by theNational Institute of Standards and Technology (Berger et al 1998, Cullen et al 1997). Anumber of studies have evaluated the differences between EPDL97 and XCOM along witholder databases that are still available (Almansa et al 2007, Ye et al 2004, Zaidi 2000). Thesestudies have shown that there are significant differences in cross section values particularlyfor the lower photon energies and for high atomic number materials.
Monte Carlo methods have been widely used to solve radiation transport problems forthe characterization and dosimetry of low energy x-ray beams. These will now be discussedin relation to the most commonly used Monte Carlo codes for radiation transport calculations:EGSnrc, GEANT4, MCNP and PENELOPE.
8.1. EGSnrc
The EGSnrc Monte Carlo code has been verified by comparison with the experimental datain a number of studies involving low energy photon beams (Ali and Rogers 2008a, 2008b,Chibani and Li 2002, Kawrakow 2000a, Mainegra-Hing et al 2008, Reniers et al 2004, Rogers2006, Verhaegen 2002). In one study, Mainegra-Hing et al (2008) compared correction factorsfor FACs and found a good agreement between Monte Carlo calculations and measuredcorrection factors. Ali and Rogers (2008a) performed a range of benchmark calculations ofthe EGSnrc code in the kilovoltage energy range for charged particle backscatter coefficients
R215
Phys. Med. Biol. 59 (2014) R183 Topical Review
with comparison against experimental measurements. They found the agreement between bothsets of data generally within 4%.
Numerous studies have used ESGnrc/BEAMnrc to model therapeutic clinical kilovoltagex-ray units with beams in the energy range from 50 to 300 kVp (Fletcher and Mills 2008, Hillet al 2009, Keall et al 1999, Kim et al 2010, Knight and Nahum 1994, Knoos et al 2007,Lye et al 2010a, Ma et al 1998, Munck Af Rosenschold et al 2008, Natto 2002, Ubrich et al2008, Verhaegen et al 1999). These studies used Monte Carlo simulations to generate therelative dosimetry data such as depth doses, relative profiles and BSFs for comparison withthe measured data. In two recent studies, Knoos et al (2007), Munck Af Rosenschold et al(2008) used BEAMnrc to model a Gulmay kilovoltage x-ray unit. They used BEAMnrc tocalculate depth doses and profiles in a water phantom as well as isodoses in patient CT data.Other studies have used BEAMnrc to model CT scanners or kilovoltage treatment units asused for animal studies (Bazalova et al 2009, Chow 2010, Omrane et al 2003).
EGSnrc/EGS4 has been used to determine the energy response of different radiationdetectors (Agyingi et al 2006, Ma and Nahum 1995a, 1995b, Mobit et al 1998, 2000, Ubrichet al 2008). One study investigated the response of ionization chambers in medium-energykilovoltage x-ray beams for the energy range 70–280 kVp (Ubrich et al 2008). They studiedthe influence of the central electrode dimensions on the beam quality correction factor kQ. Theagreement between calculated and measured kQ was better than 0.6% if the correct geometrywas used for the central electrode. A number of these studies have used BEAMnrc to modelFACs as used in primary dosimetry standards laboratories as well as the temperature–pressurecorrection factor PTP for ionization chambers (La Russa and Rogers 2006, La Russa et al 2007,Lye et al 2010b).
Several studies have calculated doses using EGSnrc/EGS4 in water and solid phantommaterials for kilovoltage x-ray beams (Gorjiara et al 2011a, 2011b, Hill et al 2008, 2009, Maand Seuntjens 1999, Reniers et al 2004, Ye et al 2004). Reniers et al (2004) calculated theradial dose distribution in several phantom materials from low energy brachytherapy sourcesand compared with measured doses using TLDs. They found a good agreement betweencalculated and measured doses when the new cross section data were used, particularly forphoton energies less than 100 keV.
8.2. Geant4
The software toolkit Geant46 was originally developed by CERN for high-energy particlephysics applications. Its radiation transport simulation capability has been substantiallyextended to the relatively low energies applicable to medical physics applications. For energiesin the kilovoltage range in particular, Geant4 provides user-specified low energy and very low-energy (now called Geant4-DNA) electromagnetic radiation physics models that continue tobe comprehensively tested for dosimetry calculations (Allison et al 2006, Amako et al 2005,Faddegon et al 2009, Francis et al 2011, Incerti et al 2010, Poon and Verhaegen 2005).
To date, Geant4 has been used in a number of Monte Carlo studies for low energyx-ray beams such as transmission values, dose calculations for different tissues, modellingof kilovoltage x-ray units and dosimetry of low energy brachytherapy sources (Clausen et al2012, Landry et al 2010, Li et al 2012, Lian et al 2011, Rivard et al 2010).
The low-energy models in Geant4 use the Livermore and PENELOPE cross-sections forphoton and electron transport, which have been validated down to energies of 250 eV. Thesemodels have been applied to brachytherapy (Afsharpour et al 2012) as well as radiobiology
6 geant4.web.cern.ch
R216
Phys. Med. Biol. 59 (2014) R183 Topical Review
and microdosimetry simulations (Byrne et al 2013, Chauvie et al 2007, Kuncic et al 2012).Geant4-DNA provides cross-section models for electrons in liquid water down to energies ofjust a few eV and is thus contributing to emerging radiobiology and nanodosimetry simulationstudies (Bernal et al 2011, McNamara et al 2012).
8.3. MCNP
The most recently released version of the MCNP Monte Carlo code is MCNP6 (Goorleyet al 2013). MCNP has been used to model low energy x-ray beams in a number of studies(Boudou et al 2004, 2005, Ding et al 2010, Edouard et al 2010, Hadid et al 2010, Hanlon et al2009, Nuttens et al 2008). Some of these studies used MCNP to calculate doses in water andvarious solid phantom materials as well as interface dosimetry including comparisons withother Monte Carlo codes (Chibani and Li 2002, Hadid et al 2010, Reniers et al 2004, Ye et al2004). In one study, Traub et al (1997) calculated BSF for different solid calibration phantomsand found differences of up to 8% between the different phantom materials.
The MCNP code has also been used for calculating the dosimetry data from kilovoltagex-ray beams including depth doses and profiles by a full geometric model of the therapeutickilovoltage x-ray unit (Natto 2002, Verhaegen et al 1999). In the study by Kim et al (2006),the MCNP code was used to calculate BSFs for kilovoltage x-ray beams and compared tomeasurements using a solid state detector. More recently, Rivard et al (2010) compared thedosimetry of different low energy brachytherapy sources from MCNPX and other Monte Carlocodes. They found that there was no statistically significant difference in calculated dose orkerma value between the Monte Carlo codes for the same beam spectrum.
8.4. PENELOPE
The PENELOPE code has been successfully benchmarked against the experimental data andother Monte Carlo codes including for kilovoltage x-rays (Almansa et al 2007, Chica et al2009, Loehr et al 2009, Salvat et al 2006a, Sempau et al 2003, Ye et al 2004). For this reason,the PENELOPE code has been used in studies of radiation dosimetry or radiobiology for lowenergy x-ray beams (Burns and Kessler 2009, Chica et al 2008, Garnica-Garza 2009, 2011,Ginjaume et al 2001, Hsiao and Stewart 2008, Prezado et al 2009).
Several studies have evaluated the accuracy of the PENELOPE code for predicting x-rayspectra, by comparison with both the experimental data and theoretical calculations (Bote et al2008, Llovet et al 2003, Salvat et al 2006b, Tian et al 2009). In one study, Llovet et al (2003)found that the PENELOPE code was suitable for calculating x-ray spectra emitted from targetsbombarded with kilovoltage electron beams and gave a good agreement with the experimentalspectral data. Subsequently, the PENELOPE code has been used for calculating x-ray spectrafrom tungsten and other targets (Garnica-Garza 2011).
A number of studies have used PENELOPE to evaluate the radiological water equivalenceof different solid phantoms for low energy photons (Hill et al 2010, Marques et al 2010). ThePENELOPE code has also been used for calculating the dosimetry data from kilovoltage x-raybeams including depth doses, profiles and BSFs as well as radial dose distributions from lowenergy brachytherapy sources (Assiamah et al 2007, Chica et al 2008, 2009, 2010, Croce et al2012, Hill et al 2010, Ye et al 2004).
9. Conclusions and future perspectives
Kilovoltage x-ray beams will continue to provide a useful treatment modality in manyradiotherapy departments. While being used predominantly for skin cancers, a number of
R217
Phys. Med. Biol. 59 (2014) R183 Topical Review
recent developments have seen their application in both intraoperative x-ray units and animalirradiators. Reported issues in the past relate to achieving accurate relative dosimetry and alsowith the recommendations for the use of generic published data. However, it has been shownthat it is now possible to measure relative doses accurately using a wide range of dosimetrytools. In addition, in silico Monte Carlo techniques are being used to solve many problems forboth relative dosimetry and for determining required factors for reference dosimetry.
There are still significant areas requiring investigation and development, in order to furtherimprove the accuracy of the dosimetry and clinical application of kilovoltage therapy x-raybeams. Clear current examples are: the development and validation of kilovoltage treatmentplanning systems; the investigation of new dosimeters including 3D dosimetry systems;increasing use of Monte Carlo approaches and the increased accuracy and availability ofdose-to-water based calibrations for kilovoltage x-ray beams. In addition, developments inkilovoltage x-ray beam use in related areas are likely to inform and strengthen the physicsand dosimetry knowledge base for therapy beam use. For example, there is increased useof kilovoltage x-ray imaging on linear accelerators and other treatment units. There is alsosignificant work in microbeam and irradiation systems for radiobiology work which requireimproved dosimetry and delivery methods. Thus it is expected that this area of clinical radiationphysics will continue to provide significant research challenges.
Acknowledgments
The following people are thanked for their assistance, collaborations and discussions relatedto kilovoltage x-ray beams: Dr Mamoon Haque, Elizabeth Claridge Mackonis, Simran Gill,Johnny Morales, May Whitaker, David Odgers, Anna Ralston, Matthew Sobolewski, Gwi Choand Associate Professor Chris Milross from the Chris O’Brien Lifehouse, Sydney, Australia;Zhao Mo, Joanne Kim, Dr Tina Gorjiara, Leon Smith, Sam Blake, David Wang and SaxbyBrown who were all students in the Institute of Medical Physics, School of Physics, Universityof Sydney, Australia; Dr Phil Vial from the Liverpool Cancer Therapy Centre, Sydney,Australia; Vinod Nelson from the Macarthur Cancer Therapy Centre, Sydney, Australia;Mario Perez from Royal North Shore Hospital, Sydney, Australia; Professor Paul Tofts fromthe Institute of Neurology, University College London, London, UK.
References
Adamovics J and Maryanski M J 2006 Characterisation of PRESAGE: a new 3-D radiochromic solidpolymer dosemeter for ionising radiation Radiat. Prot. Dosim. 120 107–12
Afsharpour H, Landry G, Damours M, Enger S, Reniers B, Poon E, Carrier J F, Verhaegen Fand Beaulieu L 2012 ALGEBRA: algorithm for the heterogeneous dosimetry based on GEANT4for BRAchytherapy Phys. Med. Biol. 57 3273–80
Agostinelli S et al 2003 G4–a simulation toolkit Nucl. Instrum. Methods Phys. Res. A 506 250–303Agyingi E O, Mobit P N and Sandison G A 2006 Energy response of an aluminium oxide detector in
kilovoltage and megavoltage photon beams: an EGSnrc Monte Carlo simulation study Radiat. Prot.Dosim. 118 28–31
Akselrod M S, Btter-Jensen L and McKeever S W S 2006 Optically stimulated luminescence and its usein medical dosimetry Radiat. Meas. 41 (Suppl. 1) S78–99
Alaei P, Gerbi B J and Geise R A 2000 Evaluation of a model-based treatment planning system for dosecomputations in the kilovoltage energy range Med. Phys. 27 2821–6
Ali E S and Rogers D W 2008a Benchmarking EGSnrc in the kilovoltage energy rangeagainst experimental measurements of charged particle backscatter coefficients Phys. Med.Biol. 53 1527–43
Ali E S M and Rogers D W O 2008b Energy spectra and angular distributions of charged particlesbackscattered from solid targets J. Phys. D: Appl. Phys. 41 055505
Ali E S M and Rogers D W O 2008c Quantifying the effect of off-focal radiation on the output ofkilovoltage x-ray systems Med. Phys. 35 4149–60
Allahverdi M, Nisbet A and Thwaites D I 1999 An evaluation of epoxy resin phantom materials formegavoltage photon dosimetry Phys. Med. Biol. 44 1125–32
Allison J et al 2006 Geant4 developments and applications IEEE Trans. Nucl. Sci. 53 270–8Almansa J F, Guerrero R, Al-Dweri F M O, Anguiano M and Lallena A M 2007 Dose distribution in
water for monoenergetic photon point sources in the energy range of interest in brachytherapy:Monte Carlo simulations with PENELOPE and GEANT4 Radiat. Phys. Chem. 76 766–73
Amako K et al 2005 Comparison of Geant4 electromagnetic physics models against the NIST referenceIEEE Trans. Nucl. Sci. 52 910–8
Amdur R J, Kalbaugh K J, Ewald L M, Parsons J T, Mendenhall W M, Bova F J and Million R R 1992Radiation therapy for skin cancer near the eye: kilovoltage x-rays versus electrons Int. J. Radiat.Oncol. Biol. Phys. 23 769–79
Andreo P, Burns D T, Hohlfield K, Huq M S, Kanai T, Laitano F, Smyth V and Vynckier S 2000Absorbed dose determination in external beam radiotherapy, an international code of practice fordosimetry based on standards of absorbed dose to water Technical Report Series No 398 (Vienna:IAEA)
Aoki K and Koyama M 2002 Measurement of backscattered x-ray spectra at the water surface in theenergy range 60 kV to 120 kV Phys. Med. Biol. 47 1205–17
Archer B R and Wagner L K 1988a Determination of diagnostic x-ray spectra with characteristic radiationusing attenuation analysis Med. Phys. 15 637–41
Archer B R and Wagner L K 1988b A modified x-ray spectra reconstruction technique Phys. Med.Biol. 33 1399–406
Arjomandy B, Tailor R, Anand A, Sahoo N, Gillin M, Prado K and Vicic M 2010 Energy dependenceand dose response of Gafchromic EBT2 film over a wide range of photon, electron, and protonbeam energies Med. Phys. 37 1942–7
Arndt C D, Wang I Z, Saito N G and Podgorsak M B 2011 Dosimetric calibration and characterizationfor experimental mouse thoracic irradiation using orthovoltage x rays Radiat. Res. 175 784–9
Assiamah M, Nam T L and Keddy R J 2007 Radiation doses from low energy x-ray beams measuredwith synthetic diamond compared with calculated values obtained from the PENELOPE MonteCarlo code Appl. Radiat. Isot. 65 952–8
Attix F H 2004 Introduction to Radiological Physics and Radiation Dosimetry (New York: Wiley)Aukett R J, Burns J E, Greener A G, Harrison R M, Moretti C, Nahum A E and Rosser K E 2005
Addendum to the IPEMB code of practice for the determination of absorbed dose for x-rays below300 kV generating potential (0.035 mm Al-4 mm Cu HVL) Phys. Med. Biol. 50 2739–48
Aukett R J, Harrison R M and Rosser K E 1999 The characteristics of ionization chambers formeasurements with x-rays in the kilovoltage range Kilovoltage X-ray Beam Dosimetry forRadiotherapy and Radiobiology ed C M Ma and J P Seuntjens (Madison, WI: Medical PhysicsPublishing) pp 195–211
Aukett R J, Thomas D W, Seaby A W and Gittins J T 1996 Performance characteristics of the PantakDXT-300 kilovoltage x-ray treatment machine Br. J. Radiol. 69 726–34
Austerlitz C, Mota H, Gay H, Campos D, Allison R and Sibata C 2008 On the need for quality assurancein superficial kilovoltage radiotherapy Radiat. Prot. Dosim. 130 476–81
Avanzo M, Rink A, Dassie A, Massarut S, Roncadin M, Borsatti E and Capra E 2012 In vivodosimetry with radiochromic films in low-voltage intraoperative radiotherapy of the breast Med.Phys. 39 2359–68
Babic S and Schreiner L J 2006 An NMR relaxometry and gravimetric study of gelatin-free aqueouspolyacrylamide dosimeters Phys. Med. Biol. 51 4171–87
Baker C R, Luhana F and Thomas S J 2002 Absorbed dose behind eye shields during kilovoltage photonradiotherapy Br. J. Radiol. 75 685–8
Baldock C, De Deene Y, Doran S, Ibbott G, Jirasek A, Lepage M, McAuley K B, Oldham Mand Schreiner L J 2010 Polymer gel dosimetry Phys. Med. Biol. 55 R1–63
Baldock C, Murry P and Kron T 1999 Uncertainty analysis in polymer gel dosimetry Phys. Med.Biol. 44 N243–6
Bazalova M, Carrier J F, Beaulieu L and Verhaegen F 2008 Dual-energy CT-based material extractionfor tissue segmentation in Monte Carlo dose calculations Phys. Med. Biol. 53 2439–56
Bazalova M, Zhou H, Keall P J and Graves E E 2009 Kilovoltage beam Monte Carlo dose calculationsin submillimeter voxels for small animal radiotherapy Med. Phys. 36 4991–9
Beddar A S 2006 Plastic scintillation dosimetry and its application to radiotherapy Radiat. Meas.(Suppl. 1) 41 S124–33
Benmakhlouf H, Bouchard H, Fransson A and Andreo P 2011 Backscatter factors and mass energy-absorption coefficient ratios for diagnostic radiology dosimetry Phys. Med. Biol. 56 7179–204
Berger M J, Hubbell J H, Seltzer S M, Chang J, Coursey J S, Sukumar R and Zucker D S 1998 XCOM:photon cross sections database Technical Report NBSIR 87-3597, National Institute of Standardsand Technology, Physics Laboratory, Ionizing Radiation Division
Bernal M A, Dealmeida C E, Sampaio C, Incerti S, Champion C and Nieminen P 2011 The invarianceof the total direct DNA strand break yield Med. Phys. 38 4147–53
Bielajew A 2007 The Monte Carlo simulation of radiation transport Handbook of Radiotherapy Physicsed P Mayles, A E Nahum and J Rosenwald (Boca Raton, FL: CRC Press) pp 75–87 chapter 5
Biggs P, Ma C M, Doppke K, Niroomand-Rad A and Beatty J 1999 Kilovoltage x-rays The ModernTechnology of Radiation Oncology ed J Van Dyk (Madison, WI: Medical Physics Publishing)chapter 9
Birch R and Marshall M 1979 Computation of bremsstrahlung x-ray spectra and comparison with spectrameasured with a Ge(Li) detector Phys. Med. Biol. 24 505
BJR Report 25 1996 Central axis depth dose data for use in radiotherapy Technical Report 25 LondonBos A J J 2006 Theory of thermoluminescence Radiat. Meas. (Suppl. 1) 41 S45–56Bote D, Llovet X and Salvat F 2008 Monte Carlo simulation of characteristic x-ray emission from thick
samples bombarded by kiloelectronvolt electrons J. Phys. D: Appl. Phys. 41 105304Boudou C, Balosso J, Estve F and Elleaume H 2005 Monte Carlo dosimetry for synchrotron stereotactic
radiotherapy of brain tumours Phys. Med. Biol. 50 4841–51Boudou C, Biston M C, Corde S, Adam J F, Ferrero C, Estave F and Elleaume H 2004 Synchrotron
stereotactic radiotherapy: dosimetry by Fricke gel and Monte Carlo simulations Phys. Med.Biol. 49 5135–44
Brindha S, Venning A J, Hill B and Baldock C 2004 Experimental study of attenuation properties ofnormoxic polymer gel dosimeters Phys. Med. Biol. 49 N353–61
Brown S, Bailey D L, Willowson K and Baldock C 2008a Investigation of the relationship betweenlinear attenuation coefficients and CT Hounsfield units using radionuclides for SPECT Appl. Radiat.Isot. 66 1206–12
Brown S, Venning A, De Deene Y, Vial P, Oliver L, Adamovics J and Baldock C 2008b Radiologicalproperties of the PRESAGE and PAGAT polymer dosimeters Appl. Radiat. Isot. 66 1970–4
Buhr H, Bermann L, Gerlach M, Krumrey M and Rabus H 2012 Measurement of the mass energy-absorption coefficient of air for x-rays in the range from 3 to 60 keV Phys. Med. Biol. 57 8231–47
Burns D T and Buermann L 2009 Free-air ionization chambers Metrologia 46 S9–23Burns D T and Kessler C 2009 Diaphragm correction factors for free-air chamber standards for air kerma
in x-rays Phys. Med. Biol. 54 2737–45Burton N L A, Brimelow J and Welsh A D 2008 A regional audit of kilovoltage x-rays—a single centre
approach Br. J. Radiol. 81 422–6Butson M J, Cheung T and Yu P K N 2006a Measurement of energy dependence for XRCT radiochromic
film Med. Phys. 33 2923–5Butson M J, Cheung T and Yu P K N 2006b Weak energy dependence of EBT Gafchromic film dose
response in the 50 kVp–10 MVp x-ray range Appl. Radiat. Isot. 64 60–2Butson M J, Cheung T and Yu P K N 2007 Radiochromic film for verification of superficial x-ray
backscatter factors Australas. Phys. Eng. Sci. Med. 30 269–73Butson M J, Cheung T, Yu P K, Price S and Bailey M 2008a Measurement of radiotherapy superficial
x-ray dose under eye shields with radiochromic film Phys. Med. 24 29–33Butson M J, Cheung T and Yu P K N 2008b Measurement of dose reductions for superficial x-rays
backscattered from bone interfaces Phys. Med. Biol. 53 N329–36Butson M J, Yu P K N, Cheung T and Alnawaf H 2010 Energy response of the new EBT2 radiochromic
film to x-ray radiation Radiat. Meas. 45 836–9Byrne H L, McNamara A L, Domanova W, Guatelli S and Kuncic Z 2013 Radiation damage on sub-
cellular scales: beyond DNA Phys. Med. Biol. 58 1251Caccialanza M, Piccinno R, Percivalle S and Rozza M 2009 Radiotherapy of carcinomas of the
skin overlying the cartilage of the nose: our experience in 671 lesions J. Eur. Acad. Dermatol.Venereol. 23 1044–9
Carlsson C A 1993 Differences in reported backscatter factors for low-energy x-rays: a literature studyPhys. Med. Biol. 38 521–31
Chain J N M, Jirasek A, Schreiner L J and McAuley K B 2011 Cosolvent-free polymer geldosimeters with improved dose sensitivity and resolution for x-ray CT dose response Phys. Med.Biol. 56 2091–102
Chauvie S, Francis Z, Guatelli S, Incerti S, Mascialino B, Moretto P, Nieminen P and Pia M G 2007Geant4 physics processes for microdosimetry simulation: design foundation and implementation ofthe first set of models IEEE Trans. Nucl. Sci. 54 2619–28
Cheung T, Butson M J and Yu P K 2003 MOSFET dosimetry in vivo at superficial and orthovoltagex-ray energies Australas. Phys. Eng. Sci. Med. 26 82–4
Cheung T, Butson M J and Yu P K N 2004 Experimental energy response verification of XR type Tradiochromic film Phys. Med. Biol. 49 N371–6
Chibani O and Li X A 2002 Monte Carlo dose calculations in homogeneous media and at interfaces: acomparison between GEPTS, EGSnrc, MCNP and measurements Med. Phys. 29 835–47
Chica U, Anguiano M and Lallena A M 2008 Study of the formalism used to determine the absorbeddose for low-energy x-ray beams Phys. Med. Biol. 53 6963–77
Chica U, Anguiano M and Lallena A M 2009 Benchmark of PENELOPE for low and medium energyx-rays Phys. Med. 25 51–7
Chica U, Florez G, Anguiano M and Lallena A M 2010 A simple analytical expression to calculate thebackscatter factor for low energy x-ray beams Phys. Med. 25 51–7
Chica U, Anguiano M, Vilches M and Lallena A M 2014 Quality indexes based on water measurementsfor low and medium energy x-ray beams: a theoretical study with PENELOPE Med. Phys.41 012101
Chiu-Tsao S T, Ho Y, Shankar R, Wang L and Harrison L B 2005 Energy dependence of response ofnew high sensitivity radiochromic films for megavoltage and kilovoltage radiation energies Med.Phys. 32 3350–4
Chow J C L 2010 Depth dose dependence of the mouse bone using kilovoltage photon beams: a MonteCarlo study for small-animal irradiation Radiat. Phys. Chem. 79 567–74
Christ G 1995 White polystyrene as a substitute for water in high energy photon dosimetry Med.Phys. 22 2097–100
Clausen S, Schneider F, Jahnke L, Fleckenstein J, Hesser J, Glatting G and Wenz F 2012 A Monte Carlobased source model for dose calculation of endovaginal TARGIT brachytherapy with INTRABEAMand a cylindrical applicator Z. Med. Phys. 22 197–204
Constantinou C, Attix F H and Paliwal B R 1982 A solid water phantom material for radiotherapy x-rayand gamma-ray beam calibrations Med. Phys. 9 436–41
Coudin D and Marinello G 1998 Lithium borate TLD for determining the backscatter factors forlow-energy x rays: comparison with chamber-based and Monte Carlo derived values Med.Phys. 25 347–53
Croce O, Hachem S, Franchisseur E, Marcie S, Gerard J P and Bordy J M 2012 Contact radiotherapyusing a 50 kV x-ray system: evaluation of relative dose distribution with the Monte Carlo codePENELOPE and comparison with measurements Radiat. Phys. Chem. 81 609–17
Cullen D E, Chen M H, Hubbell J H, Perkins S T, Plechaty E F, Rathkopf J A and Schfield J H 1997Tables and graphs of photon-interaction cross sections from 10 eV to 100 GeV, derived from theLLNL Technical Report UCRL-50400, Lawrence Livermore National Laboratory
D’Alimonte L, Sinclair E and Seed S 2011 Orthovoltage energies for palliative care in the 21st century:is there a need? Radiography 17 84–7
Das I J 1997 Forward dose perturbation at high atomic number interfaces in kilovoltage x-ray beamsMed. Phys. 24 1781–7
Das I J 1998 Broad beam attenuation of kilovoltage photon beams: effect of ion chambers Br. J. Radiol.71 68–73
Das I J and Chopra K L 1995 Backscatter dose perturbation in kilovoltage photon beams at high atomicnumber interfaces Med. Phys. 22 767–73
De Deene Y, Hurley C, Venning A, Vergote K, Mather M, Healy B J and Baldock C 2002 A basic studyof some normoxic polymer gel dosimeters Phys. Med. Biol. 47 3441–63
Delgado V 1999 Comparison between measured and predicted attenuation curves of x-ray beams Med.Phys. 26 2183–9
Delgado V 2007 Determination of x-ray spectra from attenuation data by imposing a priori positivenessand bounded support: theory and experimental validation Med. Phys. 34 994–1006
de Prez L A and de Pooter J A 2008 The new NMi orthovolt x-rays absorbed dose to water primarystandard based on water calorimetry Phys. Med. Biol. 53 3531–42
Devic S, Seuntjens J, Abdel-Rahman W, Evans M, Olivares M, Podgorsak E B, Vuong T and Soares C G2006 Accurate skin dose measurements using radiochromic film in clinical applications Med.Phys. 33 1116–24
DIN 1988 Klinische Dosimetrie: Anwendung Von Roentgenstrahlen Mit Rhrenspannungen Von 10 Bis100 KV in der Strahlentherapie und in der Weichteildiagnostik Technical Report No DIN6809-4Deutsches Institut fur Normung (DIN)
DIN 1996 Klinische Dosimetrie: Anwendung Von Roentgenstrahlen Mit Roehrenspannungen Von 100Bis 400 KV in der Strahlentherapie Technical Report No DIN6809-5 Deutsches Institut fur Normung(DIN)
Ding A, Gu J, Trofimov A V and Xu X G 2010 Monte Carlo calculation of imaging doses from diagnosticmultidetector CT and kilovoltage cone-beam CT as part of prostate cancer treatment plans Med.Phys. 37 6199–204
Ding G X, Pawlowski J M and Coffey C W 2008 A correction-based dose calculation algorithm forkilovoltage x rays Med. Phys. 35 5312–6
Dorgu A, Pavord D, Gong J, Sherouse G and Kriminski S 2010 Evaluation of two formulations ofcommercial water-equivalent plastic to establish suitability for dosimetry of the ZEISS intrabeam50 kVp x-ray source (AAPM Annual Meeting vol 37) (AAPM) pp 3252–3
Du Y H, Wang Y F, Hua W, Huang Y Y and Hu T D 2006 Measurement of synchrotron radiation spectrausing combined attenuation method and regularized inversion Nucl. Instrum. Methods Phys. Res.A 565 855–60
Eaton D J 2012 Quality assurance and independent dosimetry for an intraoperative x-ray device Med.Phys. 39 6908–20
Eaton D J, Barber E, Ferguson L, Simpson G M and Collis C H 2012 Radiotherapy treatment of keloidscars with a kilovoltage x-ray parallel pair Radiother. Oncol. 102 421–3
Eaton D J and Doolan P J 2013 Review of backscatter measurement in kilovoltage radiotherapy usingnovel detectors and reduction from lack of underlying scattering material J. Appl. Clin. Med. Phys.14 5–17
Eaton D J and Duck S 2010 Dosimetry measurements with an intra-operative x-ray device Phys. Med.Biol. 55 N359–69
Eaton D J, Earner B, Faulkner P and Dancer N 2013 A national dosimetry audit of intraoperativeradiotherapy Br. J. Radiol. 86 20130447
Ebert M A, Asad A H and Siddiqui S A 2009 Suitability of radiochromic films for dosimetry of lowenergy x-rays J. Appl. Clin. Med. Phys. 10 232–40
Edouard M, Broggio D, Prezado Y, Estive F, Elleaume H and Adam J F 2010 Treatment plansoptimization for contrast-enhanced synchrotron stereotactic radiotherapy Med. Phys. 37 2445–56
Ehringfeld C, Schmid S, Poljanc K, Kirisits C, Aiginger H and Georg D 2005 Application of commercialMOSFET detectors for in vivo dosimetry in the therapeutic x-ray range from 80 kV to 250 kV Phys.Med. Biol. 50 289–303
Evans P A, Moloney A J and Mountford P J 2001 Performance assessment of the Gulmay D3300kilovoltage x-ray therapy unit Br. J. Radiol. 74 537–47
Faddegon B A, Kawrakow I, Kubyshin Y, Perl J, Sempau J and Urban L 2009 The accuracy of EGSnrc,Geant4 and PENELOPE Monte Carlo systems for the simulation of electron scatter in externalbeam radiotherapy Phys. Med. Biol. 54 6151–63
Farquharson M J, Spyrou N M, Al-Bahri J and Highgate D J 1995 Low energy photon attenuationmeasurements of hydrophilic materials for tissue equivalent phantoms Appl. Radiat. Isot. 46 783–90
Ferguson S, Ostwald P, Kron T and Denham J 1995 Verification of surface dose on patients undergoinglow to medium energy x-ray therapy Med. Dosim. 20 161–5
Fletcher C L and Mills J A 2008 An assessment of Gafchromic film for measuring 50 kV and 100 kVpercentage depth dose curves Phys. Med. Biol. 53 N209–18
Francis Z, Incerti S, Karamitros M, Tran H N and Villagrasa C 2011 Stopping power and ranges ofelectrons, protons and alpha particles in liquid water using the Geant4-dNA package Nucl. Instrum.Methods Phys. Res. B 269 2307–11
Gao W and Raeside D E 1997 Orthovoltage radiation therapy treatment planning using MonteCarlo simulation: treatment of neuroendocrine carcinoma of the maxillary sinus Phys. Med.Biol. 42 2421–33
Garnica-Garza H M 2009 Contrast-enhanced radiotherapy: feasibility and characteristics of the physicalabsorbed dose distribution for deep-seated tumors Phys. Med. Biol. 54 5411–25
Garnica-Garza H M 2011 Treatment planning considerations in contrast-enhanced radiotherapy: energyand beam aperture optimization Phys. Med. Biol. 56 341–55
Gerard J P, Myint A S, Croce O, Lindegaard J, Jensen A, Myerson R, Hannoun-Levi J M and Marcie S2011 Renaissance of contact x-ray therapy for treating rectal cancer Expert Rev. Med.Devices 8 483–92
Gerig L, Soubra M and Salhani D 1994 Beam characteristics of the Therapax DXT300 orthovoltagetherapy unit Phys. Med. Biol. 39 1377–92
Gill S and Hill R 2013 A study on the use of Gafchromic EBT3 film for output factor measurements inkilovoltage x-ray beams Australas. Phys. Eng. Sci. Med. 36 465–71
Ginjaume M, Ortega X and Duch M A 2001 Implementing new recommendations for calibrating personaldosemeters Radiat. Prot. Dosim. 96 93–7
Goorley J T, James M R, Booth T E, Brown F B, Bull J S, Cox L J, Durkee J W Jr, Elson J S, Fensin M Land Forster R A III 2013 Initial MCNP6 Release Overview-MCNP6 version 1.0 Technical ReportNo LA-UR-13-22934 Los Alamos National Laboratory (LANL)
Gordon K B, Char D H and Sagerman R H 1995 Late effects of radiation on the eye and ocular adnexaInt. J. Radiat. Oncol. Biol. Phys. 31 1123–39
Gorjiara T, Hill R, Kuncic Z, Adamovics J, Bosi S, Kim J and Baldock C 2011a Investigation ofradiological properties and water equivalency of PRESAGE dosimeters Med. Phys. 38 2265–74
Gorjiara T, Hill R, Kuncic Z, Bosi S, Davies J B and Baldock C 2011b Radiological characterization andwater equivalency of genipin gel for x-ray and electron beam dosimetry Phys. Med. Biol. 56 4685–99
Gotanda T et al 2011 Evaluation of effective energy using radiochromic film and a step-shaped aluminumfilter Australas. Phys. Eng. Sci. Med. 34 213–22
Grimbergen T W M, Aalbers A H L, Mijnheer B J, Seuntjens J, Thierens H, Van Dam J, Wittkamper F Wand Zoetelief J 1997 Dosimetry for low and medium energy x-rays: a code of practice in radiotherapyand radiobiology Technical Report 10, Netherlands Commission on Radiation Dosimetry
Grosswendt B 1984 Backscatter factors for x-rays generated at voltages between 10 and 100 kV Phys.Med. Biol. 29 579–91
Grosswendt B 1990 Dependence of the photon backscatter factor for water on source-to-phantom distanceand irradiation field size Phys. Med. Biol. 35 1233–45
Grosswendt B 1993 Dependence of the photon backscatter factor for water on irradiation field size andsource-to-phantom distances between 1.5 and 10 cm Phys. Med. Biol. 38 305–10
Guo P Y, Adamovics J A and Oldham M 2006 Characterization of a new radiochromic three-dimensionaldosimeter Med. Phys. 33 1338–45
Gustafsson H, Back S A J, Lepage M, Rintoul L and Baldock C 2004 Development and optimization ofa 2-hydroxyethylacrylate MRI polymer gel dosimeter Phys. Med. Biol. 49 227–41
Hadid L, Desbrae A, Schlattl H, Franck D, Blanchardon E and Zankl M 2010 Application of theICRP/ICRU reference computational phantoms to internal dosimetry: calculation of specificabsorbed fractions of energy for photons and electrons Phys. Med. Biol. 55 3631–41
Hanlon J, Lee C, Chell E, Gertner M, Hansen S, Howell R W and Bolch W E 2009 Kilovoltage stereotacticradiosurgery for age-related macular degeneration: assessment of optic nerve dose and patienteffective dose Med. Phys. 36 3671–81
Harrison R M, Walker C and Aukett R J 1990 Measurement of backscatter factors for lowenergy radiotherapy (0.1–2.0 mm Al HVL) using thermoluminescence dosimetry Phys. Med.Biol. 35 1247–54
Healy B J, Gibbs A, Murry R L, Prunster J E and Nitschke K N 2005 Output factor measurements for akilovoltage x-ray therapy unit Australas. Phys. Eng. Sci. Med. 28 115–21
Healy B J, Sylvander S and Nitschke K N 2008 Dose reduction from loss of backscatter in superficialx-ray radiation therapy with the Pantak SXT 150 unit Australas. Phys. Eng. Sci. Med. 31 49–55
Hermann K P, Geworski L, Muth M and Harder D 1985 Polyethylene-based water-equivalent phantommaterial for x-ray dosimetry at tube voltages from 10 to 100 kV Phys. Med. Biol. 30 1195–200
Heydarian M, Hoban P W and Beddoe A H 1996 A comparison of dosimetry techniques in stereotacticradiosurgery Phys. Med. Biol. 41 93–110
Hill R, Healy B, Holloway L and Baldock C 2007 An investigation of dose changes for therapeutickilovoltage x-ray beams with underlying lead shielding Med. Phys. 34 3045–53
Hill R, Holloway L and Baldock C 2005 A dosimetric evaluation of water equivalent phantoms forkilovoltage x-ray beams Phys. Med. Biol. 50 N331–44
Hill R, Mo Z, Haque M and Baldock C 2009 An evaluation of ionization chambers for the relativedosimetry of kilovoltage x-ray beams Med. Phys. 36 3971–81
Hill R F, Brown S and Baldock C 2008 Evaluation of the water equivalence of solid phantoms usinggamma ray transmission measurements Radiat. Meas. 43 1258–64
Hill R F, Kuncic Z and Baldock C 2010 The water equivalence of solid phantoms for low energy photonbeams Med. Phys. 37 4355–63
Hoban P W, Heydarian M, Beckham W A and Beddoe A H 1994 Dose rate dependence of a PTWdiamond detector in the dosimetry of a 6 MV photon beam Phys. Med. Biol. 39 1219–30
Hsiao Y and Stewart R D 2008 Monte Carlo simulation of DNA damage induction by x-rays and selectedradioisotopes Phys. Med. Biol. 53 233–44
Hubbell J H 1999 Review of photon interaction cross section data in the medical and biological contextPhys. Med. Biol. 44 R1–22
Hubbell J H 2006 Review and history of photon cross section calculations Phys. Med. Biol. 51 R254–62Hugtenburg R P, Johnston K, Chalmers G J and Beddoe A H 2001 Application of diamond detectors
to the dosimetry of 45 and 100 kVp therapy beams: comparison with a parallel-plate ionizationchamber and Monte Carlo Phys. Med. Biol. 46 2489–501
Huq M S, Venkataramanan N and Meli J A 1992 The effect on dose of kilovoltage x-rays backscatteredfrom lead Int. J. Radiat. Oncol. Biol. Phys. 24 171–5
IAEA 1987 Absorbed dose determination in photon and electron beams: an international code of practiceTechnical Report Series no 277 International Atomic Energy Agency
IAEA 1993 Review of data and methods recommended in the international code of practice IAEATechnical Report Series No 277 International Atomic Energy Agency
ICRU 1989 Tissue substitutes in radiation dosimetry and measurement Technical Report ICRU 44International Commission on Radiation Units and Measurements
Incerti S et al 2010 Comparison of GEANT4 very low energy cross section models with experimentaldata in water Med. Phys. 37 4692–708
Ipe N E, Rosser K E, Moretti C J, Manning J W and Palmer M J 2001 Air kerma calibration factors andchamber correction values for PTW soft x-ray, NACP and Roos ionization chambers at very lowx-ray energies Phys. Med. Biol. 46 2107–17
IPSM 1991 Report on the IPSM working party on low- and medium-energy x-ray dosimetry Phys. Med.Biol. 36 1027–38
Ismail M, Afzal M, Nadeem M, Rana A M, Amjad S and Buzdar S A 2011 Evaluation of depth dosecharacteristics of superficial x-rays machine using different KVP and applicators diameter Iran. J.Radiat. Res. 9 159–66
Issa F, Latip N A A, Bradley D A and Nisbet A 2011 Ge-doped optical fibres as thermoluminescencedosimeters for kilovoltage x-ray therapy irradiations Nucl. Instrum. Methods Phys. Res. A652 834–7
Jhala E, Steer B, Laban J and Greig L 2009 Issues encountered with kilovoltage x-ray referencedosimetry when changing codes of practice from TRS 277 to TRS 398 Australas. Phys. Eng.Sci. Med. 32 11–15
Johns H E and Cunningham J R 1983 The Physics of Radiology ed C C Thomas (Springfield, IL: Thomas)Jordan K 2009 Optical CT scanning of cross-linked radiochromic gel without cylinder wall J. Phys.:
Conf. Ser. 164 012029Jurado D, Eudaldo T, Carrasco P, Jornet N, Ruiz A and Ribas M 2005 Pantak Therapax SXT
150: performance assessment and dose determination using IAEA TRS-398 protocol Br. J.Radiol. 78 721–32
Kawrakow I 2000a Accurate condensed history Monte Carlo simulation of electron transport: 1. EGSnrc,the new EGS4 version Med. Phys. 27 485–98
Kawrakow I 2000b Accurate condensed history Monte Carlo simulation of electron transport: 2.Application to ion chamber response simulations Med. Phys. 27 499–513
Keall P and Baldock C 1999 A theoretical study of the radiological properties and water equivalence ofFricke and polymer gels used for radiation dosimetry Australas. Phys. Eng. Sci. Med. 22 85–91
Keall P, Di Sopra F M, Beckham W and Delaney G 1999 Comparison of kilovoltage x-ray and electronbeam dose distributions for radiotherapy of the sternum Med. Dosim. 24 141–4
Khan F M 1994 The Physics of Radiation Therapy (Baltimore, MD: Williams and Wilkins)Kim J, Hill R, Mackonis E C and Kuncic Z 2010 An investigation of backscatter factors for kilovoltage
x-rays: a comparison between Monte Carlo simulations and Gafchromic EBT film measurementsPhys. Med. Biol. 55 783–97
Kim M S, Ryu J S, Park S and Yi Y 2006 Comparison of measured backscatter factors with Monte Carlosimulations for low energy x-ray Nucl. Instrum. Methods Phys. Res. A 567 341–4
Klevenhagen S C 1982 The build-up of backscatter in the energy range 1 mm Al to 8 mm Al HVT(radiotherapy beams) Phys. Med. Biol. 27 1035–43
Klevenhagen S C 1989 Experimentally determined backscatter factors for x-rays generated at voltagesbetween 16 and 140 kV Phys. Med. Biol. 34 1871–82
Klevenhagen S C, Aukett R J, Burns J E, Harrison R M, Knight R T, Nahum A E and Rosser K E 1991aMemorandum from the Institute of Physical Sciences in Medicine. Back-scatter and F-factors forlow- and medium-energy x-ray beams in radiotherapy Br. J. Radiol. 64 836–41
Klevenhagen S C, Aukett R J, Harrison R M, Moretti C, Nahum A E and Rosser K E 1996 The IPEMBcode of practice for the determination of absorbed dose for x-rays below 300 kV generatingpotential (0.035 mm Al–4 mm Cu HVL; 10–300 kV generating potential) Phys. Med.Biol. 41 2605–25
Klevenhagen S C, D’Souza D and Bonnefoux I 1991b Complications in low energy x-ray dosimetrycaused by electron contamination Phys. Med. Biol. 36 1111–6
Klevenhagen S C, Thwaites D I and Aukett R J 2000 Kilovoltage x-rays Radiotherapy Physics in Practiceed J R Williams and D I Thwaites (Oxford, UK: Oxford University Press) pp 99–117 chapter 6
Kling A, Barao F J C, Nakagawa M, Tavora L and Vaz P 2001 Advanced Monte Carlo for RadiationPhysics, Particle Transport Simulation and Applications (Monte Carlo 2000 Conf.) (Berlin:Springer)
Knight R T 1992 Backscatter factors for low and medium energy x-rays calculated by the Monte Carlomethod Internal Report ICR-PHYS-1/93 Royal Marsden NHS Trust
Knight R T and Nahum A E 1994 Depth and field-size dependence of ratios of mass-energy absorptioncoefficient, water-to-air, for kV x-ray dosimetry Proc. Int. Symp. on Measurement Assurance inDosimetry (Vienna, 1993) IAEA-SM-330/17 (Vienna: IAEA) pp 361–79
Knoos T, Munck Af Rosenschold P and Wieslander E 2007 Modelling of an orthovoltage x-ray therapyunit with the EGSnrc Monte Carlo package J. Phys.: Conf. Ser. 74 021009
Krauss A, Bauermann L, Kramer H M and Selbach H J 2012 Calorimetric determination of the absorbeddose to water for medium-energy x-rays with generating voltages from 70 to 280 kV Phys. Med.Biol. 57 6245
Kron T 1994 Thermoluminescence dosimetry and its applications in medicine: part 1. Physics, materialsand equipment Australas. Phys. Eng. Sci. Med. 17 175–99
Kron T 1995 Thermoluminescence dosimetry and its applications in medicine: part 2. History andapplications Australas. Phys. Eng. Sci. Med. 18 1–25
Kron T, Duggan L, Smith T, Rosenfeld A, Butson M, Kaplan G, Howlett S and Hyodo K1998 Dose response of various radiation detectors to synchrotron radiation Phys. Med. Biol.43 3235–59
Kron T, Metcalfe P and Pope J 1993 Investigation of the tissue equivalence of gels used for NMRdosimetry Phys. Med. Biol. 38 139–50
Kuncic Z, Byrne H L, McNamara A L, Guatelli S, Domanova W and Incerti S 2012 In siliconanodosimetry: new insights into nontargeted biological responses to radiation Comput. Math.Methods Med. 2012 147252
Kurup R G and Glasgow G P 1993 Dosimetry of a kilovoltage radiotherapy x-ray machine Med. Dosim.18 179–86
La Russa D J, McEwen M and Rogers D W O 2007 An experimental and computational investigationof the standard temperature–pressure correction factor for ion chambers in kilovoltage x rays Med.Phys. 34 4690–9
La Russa D J and Rogers D W O 2006 An EGSnrc investigation of the PTP correction factor for ionchambers in kilovoltage x rays Med. Phys. 33 4590–9
Landry G, Reniers B, Murrer L, Lutgens L, Bloemen-Van Gurp E, Pignol J P, Keller B, Beaulieu Land Verhaegen F 2010 Sensitivity of low energy brachytherapy Monte Carlo dose calculations touncertainties in human tissue composition Med. Phys. 37 5188–98
Lanzon P J and Sorell G C 1993 The effect of lead underlying water on the backscatter of x-rays of beamqualities 0.5 mm to 8 mm Al HVT Phys. Med. Biol. 38 1137–44
Lee C and Chan D 2000 Electron contamination from the lead cutout used in kilovoltage radiotherapyPhys. Med. Biol. 45 1–8
Lessard F, Archambault L, Plamondon M, Despres P, Therriault-Proulx F, Beddar S and Beaulieu L2012 Validating plastic scintillation detectors for photon dosimetry in the radiologic energy rangeMed. Phys. 39 5308–16
Li X, Zhang D and Liu B 2012 Transmission of broad W/Rh and W/Al (target/filter) x-ray beams operatedat 25–49 kVp through common shielding materials Med. Phys. 39 4132–8
Li X A, Ma C M and Salhani D 1997a Measurement of percentage depth dose and lateral beam profilefor kilovoltage x-ray therapy beams Phys. Med. Biol. 42 2561–8
Li X A, Salhani D and Ma C M 1997b Characteristics of orthovoltage x-ray therapy beams at extendedSSD for applicators with end plates Phys. Med. Biol. 42 357–70
Li X A, Ma C M and Salhani D 1999 Relative dosimetry measurement for kilovoltage x-rayunits Kilovoltage X-ray Beam Dosimetry for Radiotherapy and Radiobiology ed C M Ma andJ P Seuntjens (Madison, WI: Medical Physics Publishing) pp 213–26
Li X A, Ma C M, Salhani D and Agboola O 1998 Dosimetric evaluation of a widely used kilovoltagex-ray unit for endocavitary radiotherapy Med. Phys. 25 1464–71
Lian C P L, Othman M A R, Cutajar D, Butson M, Guatelli S and Rosenfeld A B 2011 Monte Carlostudy of the energy response and depth dose water equivalence of the MOSkin radiation dosimeterat clinical kilovoltage photon energies Australas. Phys. Eng. Sci. Med. 34 273–9
Lindsay P, Rink A, Ruschin M and Jaffray D 2010 Investigation of energy dependence of EBT andEBT-2 Gafchromic film Med. Phys. 37 571–6
Liu L, Prasad S C and Bassano D A 2003 Evaluation of two water-equivalent phantom materials foroutput calibration of photon and electron beams Med. Dosim. 28 267–9
Llovet X, Sorbier L, Campos C S, Acosta E and Salvat F 2003 Monte Carlo simulation of x-ray spectragenerated by kilo-electron-volt electrons J. Appl. Phys. 93 3844–51
Locke J, Karimpour S, Young G, Lockett M A and Perez C A 2001 Radiotherapy for epithelial skincancer Int. J. Radiat. Oncol. Biol. Phys. 51 748–55
Loehr A, Durst J, Michel T, Anton G and Geithner P 2009 Comparison of recent experimental data withMonte Carlo tools such as RoSi, Geant4 and Penelope IEEE Nuclear Science Symp. Conf. Record,NSS/MIC 2009 pp 3904–8
Luxton G 1994 Comparison of radiation dosimetry in water and in solid phantom materials for I-125and Pd-103 brachytherapy sources: EGS4 Monte Carlo study Med. Phys. 21 631–41
Lye J E, Butler D J and Webb D V 2010a Enhanced epidermal dose caused by localized electroncontamination from lead cutouts used in kilovoltage radiotherapy Med. Phys. 37 3935–9
Lye J E, Butler D J and Webb D V 2010b Monte Carlo correction factors for the ARPANSA kilovoltagefree-air chambers and the effect of moving the limiting aperture Metrologia 47 11–20
Ma C M, Coffey C W, DeWerd L A, Liu C, Nath R, Seltzer S M and Seuntjens J P 2001 AAPMprotocol for 40–300 kV x-ray beam dosimetry in radiotherapy and radiobiology Med.Phys. 28 868–93
Ma C M, Li X A and Seuntjens J P 1998 Study of dosimetry consistency for kilovoltage x-ray beamsMed. Phys. 25 2376–84
Ma C M and Nahum A E 1991 Bragg–Gray theory and ion chamber dosimetry for photon beams Phys.Med. Biol. 36 413–28
Ma C M and Nahum A E 1995a Calculations of ion chamber displacement effect corrections for medium-energy x-ray dosimetry Phys. Med. Biol. 40 45–62
Ma C M and Nahum A E 1995b Monte Carlo calculated stem effect corrections for NE2561 and NE2571chambers in medium-energy x-ray beams Phys. Med. Biol. 40 63–72
Ma C M and Seuntjens J P 1997 Correction factors for water-proofing sleeves in kilovoltage x-ray beamsMed. Phys. 24 1507–13
Ma C M and Seuntjens J P 1999 Mass-energy absorption coefficient and backscatter factor ratios forkilovoltage x-ray beams Phys. Med. Biol. 44 131–43
Mainardi R T and Bonzi E V 2008 An indirect method of x-ray spectra measurement by simultaneousattenuations of the scattered beam Radiat. Phys. Chem. 77 537–44
Mainegra-Hing E and Kawrakow I 2006 Efficient x-ray tube simulations Med. Phys. 33 2683–90Mainegra-Hing E, Reynaert N and Kawrakow I 2008 Novel approach for the Monte Carlo calculation of
free-air chamber correction factors Med. Phys. 35 3650–60Manohara S R, Hanagodimath S M and Gerward L 2008 Energy dependence of effective atomic numbers
for photon energy absorption and photon interaction: studies of some biological molecules in theenergy range 1 keV–20 MeV Med. Phys. 35 388–402
Marques T, Schwarcke M, Garrido C E, Baffa O and Nicolucci P 2010 Dosimetric properties of MAGIC-fpolymer gel assessed to radiotherapy clinical beams J. Phys.: Conf. Ser. 250 54–8
Mayles P 2007 Kilovoltage x-rays Handbook of Radiotherapy Physics ed P Mayles, A E Nahumand J Rosenwald (Boca Raton, FL: CRC Press) pp 439–49 chapter 24
Mayles P, Nahum A E and Rosenwald J 2007 Handbook of Radiotherapy Physics (Boca Raton, FL:CRC Press)
McKerracher C and Thwaites D I 2006 Calibration of an x-ray cabinet unit for radiobiology use Phys.Med. Biol. 51 3315
McNamara A L, Guatelli S, Prokopovich D A, Reinhard M I and Rosenfeld A B 2012 A comparison ofx-ray and proton beam low energy secondary electron track structures using the low energy modelsof Geant4 Int. J. Radiat. Biol. 88 164–70
Meigooni A S, Li Z, Mishra V and Williamson J F 1994 A comparative study of dosimetric propertiesof plastic water and solid water in brachytherapy applications Med. Phys. 21 1983–7
Meigooni A S, Meli J A and Nath R 1988 A comparison of solid phantoms with water for dosimetry of125I brachytherapy sources Med. Phys. 15 695–701
Meli J A, Meigooni A S and Nath R 1988 On the choice of phantom material for the dosimetry of 192Irsources Int. J. Radiat. Oncol. Biol. Phys. 14 587–94
Mesbahi A and Zakariaee S 2013 Effect of anode angle on photon beam spectra and depth dosecharacteristics for x-rad320 orthovoltage unit Rep. Pract. Oncol. Radiother. 18 148–52
Metcalfe P, Kron T and Hoban P 1997 The Physics of Radiotherapy X-rays from Linear Accelerators(Madison, WI: Medical Physics Publishing)
Midgley S M 2005 Measurements of the x-ray linear attenuation coefficient for low atomic numbermaterials at energies 32–66 and 140 keV Radiat. Phys. Chem. 72 525–35
Mitchell G, Kron T and Back M 1998 High dose behind inhomogeneities during medium-energy x-rayirradiation Phys. Med. Biol. 43 1343–50
Mobit P, Agyingi E and Sandison G 2006 Comparison of the energy-response factor of LiF and Al2O3in radiotherapy beams Radiat. Prot. Dosim. 119 497–9
Mobit P N, Nahum A E and Lest P M 1998 A Monte Carlo study of the quality dependence factors ofcommon TLD materials in photon and electron beams Phys. Med. Biol. 43 2015–32
Mobit P N, Sandison G A and Nahum A E 2000 Photon fluence perturbation correction factors for solidstate detectors irradiated in kilovoltage photon beams Phys. Med. Biol. 45 267–77
Moscovitch M and Horowitz Y S 2006 Thermoluminescent materials for medical applications: LiF:Mg,Tiand LiF:Mg, Cu, P Radiat. Meas. 41 (Suppl. 1) S71–7
Munck Af Rosenschold P, Nilsson P and Knoos T 2008 Kilovoltage x-ray dosimetry—an experimentalcomparison between different dosimetry protocols Phys. Med. Biol. 53 4431–42
Nahum A E 1996 Perturbation effects in dosimetry: part 1. Kilovoltage x-rays and electrons Phys. Med.Biol. 41 1531–80
Natto S S 2002 Performance characteristics of the Pantak Therapax-150 superficial x-ray treatmentmachine: measurements and calculations Australas. Phys. Eng. Sci. Med. 25 162–7
Naydenov S V, Ryzhikov V D and Smith C F 2004 Direct reconstruction of the effective atomicnumber of materials by the method of multi-energy radiography Nucl. Instrum. Methods Phys.Res. A 215 552–60
Nelson V K and Hill R F 2011 Backscatter factor measurements for kilovoltage x-ray beams usingthermoluminescent dosimeters TLDs Radiat. Meas. 46 2097–9
Nelson V K, McLean I D and Holloway L 2008 Use of thermoluminescent dosimetry (TLD) for qualityassurance of orthovoltage x-ray therapy machines Radiat. Meas. 43 908–11
Newton J, Oldham M, Thomas A, Li Y, Adamovics J, Kirsch D G and Das S 2011 Commissioning asmall-field biological irradiator using point, 2D and 3D dosimetry techniques Med.Phys. 38 6754–62
Niroomand-Rad A, Blackwell C R, Coursey B M, Gall K P, Galvin J M, McLaughlin W L,Meigooni A S, Nath R, Rodgers J E and Soares C G 1998 Radiochromic film dosimetry:Recommendations of AAPM Radiation Therapy Committee Task Group 55 Med. Phys.25 2093–115
Niroomand-Rad A, Gillin M T, Lopez F and Grimm D F 1987 Performance characteristics of anorthovoltage x-ray therapy machine Med. Phys. 14 874–8
Nisbet A, Aukett R J, Davison A, Glendinning A G, Thwaites D I and Bonnett D E 1999 An experimentalcomparison of kilovoltage x-ray dosimetry protocols Kilovoltage X-ray Beam Dosimetry forRadiotherapy and Radiobiology ed C M Ma and J P Seuntjens (Madison, WI: Medical PhysicsPublishing) pp 43–54
Nisbet A, Thwaites D I and Sheridan M E 1998 A dosimetric intercomparison of kilovoltage x-rays,megavoltage photons and electrons in the Republic of Ireland Radiother. Oncol. 48 95–101
Nunn A A, Davis S D, Micka J A and DeWerd L A 2008 LiF:Mg, Ti TLD response as a function ofphoton energy for moderately filtered x-ray spectra in the range of 20–250 kVp relative to Co60Med. Phys. 35 1859–69
Nuttens V E, Wra A C, Bouchat V and Lucas S 2008 Determination of biological vector characteristicsand nanoparticle dimensions for radioimmunotherapy with radioactive nanoparticles Appl. Radiat.Isot. 66 168–72
Omrane L B, Verhaegen F, Chahed N and Mtimet S 2003 An investigation of entrance surface dosecalculations for diagnostic radiology using Monte Carlo simulations and radiotherapy dosimetryformalisms Phys. Med. Biol. 48 1809–24
Palmer A, Mzenda B, Kearton J and Wills R 2011 Analysis of regional radiotherapy dosimetry auditdata and recommendations for future audits Br. J. Radiol. 84 733–42
Pantelis E, Karlis A K, Kozicki M, Papagiannis P, Sakelliou L and Rosiak J M 2004 Polymer gelwater equivalence and relative energy response with emphasis on low photon energy dosimetry inbrachytherapy Phys. Med. Biol. 49 3495–514
Patrocinio H J, Bissonnette J P, Bussiere M R and Schreiner L J 1996 Limiting values of backscatterfactors for low-energy x-ray beams Phys. Med. Biol. 41 239
Pawlowski J M and Ding G X 2011 A new approach to account for the medium-dependent effect inmodel-based dose calculations for kilovoltage x-rays Phys. Med. Biol. 56 3919–34
Peixoto J G and Andreo P 2000 Determination of absorbed dose to water in reference conditions forradiotherapy kilovoltage x-rays between 10 and 300 kV: a comparison of the data in the IAEA,IPEMB, DIN and NCS dosimetry protocols Phys. Med. Biol. 45 563–75
Perez C A, Brady L W, Halperin E C and Schmidt-Ullrich R K 2004 Principles and Practice of RadiationOncology 4th edn (Philadelphia, PA: Williams & Wilkins)
Perrin B A, Whitehurst P, Cooper P and Hounsell A R 2001 The measurement of kappach factorsfor application with the IPEMB very low energy dosimetry protocol Phys. Med. Biol.46 1985–95
Petoussi-Henss N, Zankl M, Drexler G, Panzer W and Regulla D 1998 Calculation of backscatter factorsfor diagnostic radiology using Monte Carlo methods Phys. Med. Biol. 43 2237
Pidikiti R, Stojadinovic S, Speiser M, Song K H, Hager F, Saha D and Solberg T D 2011Dosimetric characterization of an image-guided stereotactic small animal irradiator Phys. Med.Biol. 56 2585–99
Planskoy B 1980 Evaluation of diamond radiation dosemeters Phys. Med. Biol. 25 519–32Podgorsak E B, Gosselin M and Evans M D 1998 Superficial and orthovoltage x-ray beam dosimetry
Med. Phys. 25 1206–11Podgorsak M B, Schreiner L J and Podgorsak E B 1990 Surface dose in intracavitary orthovoltage
radiotherapy Med. Phys. 17 635–40Poen J C 1999 Clinical applications of orthovoltage radiotherapy: tumours of the skin, endorectal therapy
and intraoperative radiation therapy Kilovoltage X-ray Beam Dosimetry for Radiotherapy andRadiobiology ed C M Ma and J P Seuntjens (Madison, WI: Medical Physics Publishing) pp 1–5
Poludniowski G G 2007 Calculation of x-ray spectra emerging from an x-ray tube: part II. X-rayproduction and filtration in x-ray targets Med. Phys. 34 2175–86
Poludniowski G G and Evans P M 2007 Calculation of x-ray spectra emerging from an x-ray tube. partI. Electron penetration characteristics in x-ray targets Med. Phys. 34 2164–74
Poludniowski G, Evans P M and Webb S 2009 Rayleigh scatter in kilovoltage x-ray imaging: is theindependent atom approximation good enough? Phys. Med. Biol. 54 6931–42
Poon E and Verhaegen F 2005 Accuracy of the photon and electron physics in GEANT4 for radiotherapyapplications Med. Phys. 32 1696–711
Prezado Y, Fois G, Le Duc G and Bravin A 2009 Gadolinium dose enhancement studies in microbeamradiation therapy Med. Phys. 36 3568–74
Ramaseshan R, Kohli K, Cao F and Heaton R 2008 Dosimetric evaluation of plastic water diagnostictherapy J. Appl. Clin. Med. Phys. 9 98–111
Rampado O, Garelli E, Deagostini S and Ropolo R 2006 Dose and energy dependence of response ofGafchromic XR-QA film for kilovoltage x-ray beams Phys. Med. Biol. 51 2871–81
Rao B V, Raju M L, Narasimham K L, Parthasaradhi K and Rao B M 1985 Interaction of low-energyphotons with biological materials and the effective atomic number Med. Phys. 12 745–8
Rapp B, Perichon N, Denoziere M, Daures J, Ostrowsky A and Bordy J M 2013 The LNE-lNHBwater calorimeter for primary measurement of absorbed dose at low depth in water: application tomedium-energy x-rays Phys. Med. Biol. 58 2769
Reft C S 1989 Output calibration in solid water for high energy photon beams Med. Phys.16 299–301
Reft C S 2009 The energy dependence and dose response of a commercial optically stimulatedluminescent detector for kilovoltage photon, megavoltage photon and electron, proton and carbonbeams Med. Phys. 36 1690–9
Regulla D, Friedland W, Hieber L, Panzer W, Seidenbusch M and Schmid E 2000 Spatially limitedeffects of dose and let enhancement near tissue/gold interfaces at diagnostic x ray qualities Radiat.Prot. Dosim. 90 159–63
Reinhardt S, Hillbrand M, Wilkens J J and Assmann W 2012 Comparison of Gafchromic EBT2 andEBT3 films for clinical photon and proton beams Med. Phys. 39 5257–62
Reniers B, Verhaegen F and Vynckier S 2004 The radial dose function of low-energy brachytherapyseeds in different solid phantoms: comparison between calculations with the EGSnrc and MCNP4CMonte Carlo codes and measurements Phys. Med. Biol. 49 1569–82
Rink A, Vitkin I A and Jaffray D A 2007 Energy dependence (75 kVp to 18 MV) of radiochromic filmsassessed using a real-time optical dosimeter Med. Phys. 34 458–63
Rivard M J, Granero D, Perez-Calatayud J and Ballester F 2010 Influence of photon energy spectra frombrachytherapy sources on Monte Carlo simulations of kerma and dose rates in water and air Med.Phys. 37 869–76
Roentgen W C 1895 Uber eine neue Art von Strahlen (On a new kind of rays) Technical Report WurzburgPhysical and Medical Society
Rogers D W O 2006 Fifty years of Monte Carlo simulations for medical physics Phys. Med.Biol. 51 R287–301
Rong Y and Welsh J S 2010 Surface applicator calibration and commissioning of an electronicbrachytherapy system for nonmelanoma skin cancer treatment Med. Phys. 37 5509–17
Rosenfeld A B 2006 Electronic dosimetry in radiation therapy Radiat. Meas. 41 S134–53Rosser K E 1996 Measurement of absorbed dose to water for medium energy x-rays Technical Report
CIRA(EXT)006 National Physical LaboratoryRosser K E 1998 An alternative beam quality index for medium-energy x-ray dosimetry Phys. Med.
Biol. 43 587–98Salvat F and Fernandez-Varea J M 2009 Overview of physical interaction models for photon and electron
transport used in Monte Carlo codes Metrologia 46 S112–38Salvat F, Fernandez-Varea J M and Sempau J 2006a PENELOPE-2006, A code system for Monte Carlo
simulation of electron and photon transport Technical Report NEA No 6222\Salvat F, Fernndez-Varea J M, Sempau J and Llovet X 2006b Monte Carlo simulation of bremsstrahlung
emission by electrons Radiat. Phys. Chem. 75 1201–19Schauer D A, Cassata J R and King J J 2000 A comparison of measured and calculated photon backscatter
from dosemeter calibration phantoms Radiat. Prot. Dosim. 88 319–21Schneider F, Fuchs H, Lorenz F, Steil V, Ziglio F, Kraus-Tiefenbacher U, Lohr F and Wenz F
2009 A novel device for intravaginal electronic brachytherapy Int. J. Radiat. Oncol. Biol. Phys.74 1298–305
Schwahn S O and Gesell T F 2008 Variations in backscatter observed in PMMA whole-body dosimetryslab phantoms Radiat. Prot. Dosim. 128 375–81
Seco J and Evans P M 2006 Assessing the effect of electron density in photon dose calculations Med.Phys. 33 540–52
Sellakumar P, Kumar A S, Supe S S, Anand M R, Nithya K and Sajitha S 2009 Evaluation ofdosimetric functions for Ir-192 source using radiochromic film Nucl. Instrum. Methods Phys. Res.B 267 1862–6
Sempau J, Fernandez-Varea J M, Acosta E and Salvat F 2003 Experimental benchmarks of the MonteCarlo code PENELOPE Nucl. Instrum. Methods Phys. Res. B 207 107–23
Senden R J, De Jean P, McAuley K B and Schreiner L J 2006 Polymer gel dosimeters with reducedtoxicity: a preliminary investigation of the NMR and optical dose-response using different monomersPhys. Med. Biol. 51 3301–14
Seuntjens J, Aalbers A H L, Grimbergen T W M, Mijnheer B J, Thierens H, Van Dam J, Wittkamper F W,Zoetelief J, Piessens M and Piret P 1999 Suitability of diamond detectors to measure central axisdepth kerma curves for low- and medium-energy x-rays Kilovoltage X-ray Beam Dosimetry forRadiotherapy and Radiobiology ed C M Ma and J P Seuntjens (Madison, WI: Medical PhysicsPublishing) pp 227–38
Seuntjens J P and Duane S 2009 Photon absorbed dose standards Metrologia 46 S39Seuntjens J, Olivares M, Evans M and Podgorsak E 2005 Absorbed dose to water reference dosimetry
using solid phantoms in the context of absorbed-dose protocols Med. Phys. 32 2945–53
Seuntjens J, Thierens H and Segaert O 1987a Response of coaxial Ge(Li) detectors to narrow beams ofphotons for stripping of x-ray bremsstrahlung spectra Nucl. Inst. Methods Phys. Res. A 258 127–31
Seuntjens J, Thierens H, Van Der Plaetsen A and Segaert O 1987b Conversion factor f for x-ray beamqualities, specified by peak tube potential and HVL value Phys. Med. Biol. 32 595–603
Seuntjens J, Thierens H and Schneider U 1993 Correction factors for a cylindrical ionization chamberused in medium-energy x-ray beams Phys. Med. Biol. 38 805
Seuntjens J, Thierens H, Van der Plaetsen A and Segaert O 1988 Determination of absorbed dose towater with ionization chambers calibrated in free air for medium-energy x-rays Phys. Med. Biol.33 1171
Seuntjens J and Verhaegen F 1996 Dependence of overall correction factor of a cylindrical ionizationchamber on field size and depth in medium-energy x-ray beams Med. Phys. 23 1789–96
Shrimpton P C, Wall B F and Fisher E S 1981 The tissue-equivalence of the Alderson Randoanthropomorphic phantom for x-rays of diagnostic qualities Phys. Med. Biol. 26 133
Sidky E Y, Yu L, Pan X, Zou Y and Vannier M 2005 A robust method of x-ray source spectrum estimationfrom transmission measurements: Demonstrated on computer simulated, scatter-free transmissiondata J. Appl. Phys. 97 11
Smith L, Hill R, Nakano M, Kim J and Kuncic Z 2011 The measurement of backscatter factors ofkilovoltage x-ray beams using Gafchromic EBT2 film Australas. Phys. Eng. Sci. Med. 34 261–6
Snow J R, Micka J A and DeWerd L A 2013 Microionization chamber air-kerma calibration coefficientsas a function of photon energy for x-ray spectra in the range of 20–250 kVp relative to Co60 Med.Phys. 40 041711
Soares C G 2006 Radiochromic film dosimetry Radiat. Meas. 41 S100–16Stern R L and Kubo H D 1995 Considerations for superficial photon dosimetry Med. Phys.
22 1469–70Sutherland J G H and Rogers D W O 2010 Monte Carlo calculated absorbed-dose energy dependence
of EBT and EBT2 film Med. Phys. 37 1110–6Taylor M L, Franich R D, Trapp J V and Johnston P N 2008 The effective atomic number of dosimetric
gels Australas. Phys. Eng. Sci. Med. 31 131–8Tello V M, Tailor R C and Hanson W F 1995 How water equivalent are water-equivalent solid materials
for output calibration of photon and electron beams? Med. Phys. 22 1177–89Thomadsen B, Constantinou C and Ho A 1995 Evaluation of water-equivalent plastics as phantom
material for electron-beam dosimetry Med. Phys. 22 291–6Thomas A, Newton J, Adamovics J and Oldham M 2011 Commissioning and benchmarking a 3D
dosimetry system for clinical use Med. Phys. 38 4846–57Thwaites D 2007 Phantoms for dose determination in reference conditions Handbook of Radiotherapy
Physics ed P Mayles, A E Nahum and J Rosenwald (Boca Raton, FL: CRC Press) chapter 18.8pp 361–5
Thwaites D, Scalliet P, Leer J W and Overgaard J 1995 Quality assurance in radiotherapy: Europeansociety for therapeutic radiology and oncology advisory report to the commission of the Europeanunion for the Europe against cancer programme Radiother. Oncol. 35 61–73
Thwaites D I 1996 Optimising the use of external dosimetric intercomparisons and audits, based onexperience of different approaches Radiother. Oncol. 40 S44
Tian L, Zhu J, Liu M and An Z 2009 Bremsstrahlung spectra produced by kilovolt electron impact onthick targets Nucl. Instrum. Methods Phys. Res. B 267 3495–9
Tomic N, Devic S, DeBlois F and Seuntjens J 2010 Reference radiochromic film dosimetry in kilovoltagephoton beams during CBCT image acquisition Med. Phys. 37 1083–92
Trapp J V, Michael G, de Deene Y and Baldock C 2002 Attenuation of diagnostic energy photons bypolymer gel dosimeters Phys. Med. Biol. 47 4247–58
Traub R J, McDonald J C and Murphy M K 1997 Determination of photon backscatter from severalcalibration phantoms Radiat. Prot. Dosim. 74 13–20
Tucker D M, Barnes G T and Chakraborty D P 1991a Semiempirical model for generating tungstentarget x-ray spectra Med. Phys. 18 211–8
Tucker D M, Barnes G T and Wu X 1991b Molybdenum target x-ray spectra: a semiempirical modelMed. Phys. 18 402–7
Ubrich F, Wulff J, Kranzer R and Zink K 2008 Thimble ionization chambers in medium-energy x-raybeams and the role of constructive details of the central electrode: Monte Carlo simulations andmeasurements Phys. Med. Biol. 53 4893–906
Van Dyk J 1999 The Modern Technology of Radiation Oncology (Madison, WI: Medical PhysicsPublishing)
Venning A J, Hill B, Brindha S, Healy B and Baldock C 2005a Investigation of the PAGAT polymer geldosimeter using magnetic resonance imaging Phys. Med. Biol. 50 3875
Venning A J, Nitschke K N, Keall P J and Baldock C 2005b Radiological properties of normoxic polymergel dosimeters Med. Phys. 32 1047–53
Verhaegen F 2002 Evaluation of the EGSnrc Monte Carlo code for interface dosimetry near high-Zmedia exposed to kilovolt and 60Co photons Phys. Med. Biol. 47 1691–705
Verhaegen F, Granton P and Tryggestad E 2011 Small animal radiotherapy research platforms Phys.Med. Biol. 56 R55–83
Verhaegen F, Nahum A E, Van de Putte S and Namito Y 1999 Monte Carlo modelling of radiotherapykV x-ray units Phys. Med. Biol. 44 1767–89
Verhaegen F and Seuntjens J 2003 Monte Carlo modelling of external radiotherapy photon beams Phys.Med. Biol. 48 R107–64
Villarreal-Barajas J E and Khan R F H 2014 Energy response of EBT3 radiochromic films: implicationsfor dosimetry in kilovoltage range J. Appl. Clin. Med. Phys. 15 331–8
Waggener R G, Blough M M, Terry J A, Chen D, Lee N E, Zhang S and McDavid W D 1999 X-rayspectra estimation using attenuation measurements from 25 kVp to 18 MV Med. Phys. 26 1269–78
Wang D, Sobolewski M and Hill R 2012 The dosimetry of eye shields for kilovoltage x-ray beamsAustralas. Phys. Eng. Sci. Med. 35 491–5
Waters L S, McKinney G W, Durkee J W, Fensin M L, Hendricks J S, James M R, Johns R Cand Pelowitz D B 2007 The MCNPX Monte Carlo Radiation Transport Code vol 896 (Los Alamos,NM: Los Alamos National Laboratory) pp 81–90
White D R 1977 An analysis of the Z-dependence of photon and electron interactions Phys. Med.Biol. 22 219–28
White D R 1978 Tissue substitutes in experimental radiation physics Med. Phys. 5 467–79Williams J R and Thwaites D I 2000 Radiotherapy Physics in Practice 2nd edn (Oxford: Oxford
University Press)Yang N C, Leichner P K and Hawkins W G 1987 Effective atomic numbers for low-energy total photon
interactions in human tissues Med. Phys. 14 759–66Yao C H, Liu B S, Chang C J, Hsu S H and Chen Y S 2004 Preparation of networks of gelatin and
genipin as degradable biomaterials Mater. Chem. Phys. 83 204–8Ye S J, Brezovich I A, Pareek P and Naqvi S A 2004 Benchmark of PENELOPE code for low-energy
photon transport: Dose comparison with MCNP4 and EGS4 Phys. Med. Biol. 49 387–97Yin Z, Hugtenburg R P, Green S and Beddoe A H 2004 Dose responses of diamond detectors to
monoenergetic x-rays Nucl. Instrum. Methods Phys. Res. B 213 646–9Yoo S, Grimm D, Zhu R, Jursinic P, Lopez F, Rownd J and Gillin M 2002 Clinical implementation of
AAPM TG61 protocol for kilovoltage x-ray beam dosimetry Med. Phys. 29 2269–73Yukihara E G and McKeever S W S 2008 Optically stimulated luminescence OSL dosimetry in medicine
Phys. Med. Biol. 53 R351–79Zaidi H 2000 Comparative evaluation of photon cross-section libraries for materials of interest in PET
Monte Carlo simulations IEEE Trans. Nucl. Sci. 47 2722–35