Advances in the assessment and treatment of ADHD in adults with ID Dr Dimitrios Paschos MRCPSych Consultant Psychiatrist & Hon. Research Fellow •Islington Learning Disabilities Partnership •Adult ADHD Service, Camden & Islington NHS FT •Institute of Psychiatry, King’s College London These slides are the intellectual property of Dr Paschos and must not be reproduced
Transcript
Advances in the assessment and treatment of ADHD in adults with ID
Dr Dimitrios Paschos MRCPSych Consultant Psychiatrist & Hon. Research Fellow •Islington Learning Disabilities Partnership •Adult ADHD Service, Camden & Islington NHS FT •Institute of Psychiatry, King’s College London
These slides are the intellectual property of Dr Paschos and must not be reproduced
Aims
• Increase confidence in recognising ADHD across the range of ID
• Increase confidence in prescribing & monitoring stimulant medication
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
• Does ADHD co-exist with ID?
These slides are the intellectual property of Dr Paschos and must not be reproduced
Still controversial?
From medical colleagues:
• ‘ADHD does not exist’ or ‘Everyone has ADHD’
• ‘No one had ADHD when I was growing up’
• ‘He doesn’t have ADHD – he was able to concentrate well during the consultation (7 mins)’
These slides are the intellectual property of Dr Paschos and must not be reproduced
WHY DIAGNOSE ADHD?
• Common (3-4% of children & 1% of adults)
• Disabling (academic, occupational & social impairment)
• High risk of psychiatric co-morbidity
• Treatable
• USA: over 90% of adults with ADHD never diagnosed
These slides are the intellectual property of Dr Paschos and must not be reproduced
DSM-IV Diagnostic Criteria
A: 1) 6 out of 9 inattention items
2) 6 out of 9 hyperactivity / impulsivity items
B: symptoms were present before age 7 years
C: impairment present in two or more settings (e.g. at school [or work] and at home)
These slides are the intellectual property of Dr Paschos and must not be reproduced
DSM-IV Diagnostic Criteria
D: clear evidence of clinically significant impairment in social, academic, or occupational functioning
E: symptoms do not occur exclusively during the course of:
• Autism
• Schizophrenia or other Psychotic Disorder
• Symptoms not better accounted for by Mood, Anxiety or Personality Disorder
These slides are the intellectual property of Dr Paschos and must not be reproduced
Inattention symptoms
Often.. 1. fails to give close attention to details or makes careless mistakes in schoolwork,
work, or other activities 2. has difficulty sustaining attention in tasks or play activities 3. does not seem to listen when spoken to directly 4. does not follow through on instructions and fails to finish schoolwork, chores, or
duties in the workplace (not due to oppositional behavior or failure to understand instructions)
5. has difficulty organizing tasks and activities 6. avoids, dislikes, or is reluctant to engage in tasks that require sustained mental
effort (such as schoolwork or homework) 7. loses things necessary for tasks or activities (e.g., toys, school assignments, pencils,
books, or tools) 8. easily distracted by extraneous stimuli 9. forgetful in daily activities
These slides are the intellectual property of Dr Paschos and must not be reproduced
Hyperactivity symptoms
Often… 1. fidgets with hands or feet or squirms in seat 2. leaves seat in classroom or in other situations in which
remaining seated is expected 3. runs about or climbs excessively in situations in which it is
inappropriate (in adolescents or adults, may be limited to subjective feelings of restlessness)
4. has difficulty playing or engaging in leisure activities quietly 5. is “on the go” or acts as if “driven by a motor” 6. talks excessively
These slides are the intellectual property of Dr Paschos and must not be reproduced
Impulsivity symptoms
Often…
1. blurts out answers before questions have been completed
2. has difficulty awaiting turn
3. interrupts or intrudes on others (e.g., butts into conversations or games)
These slides are the intellectual property of Dr Paschos and must not be reproduced
DSM-5 changes
• 5 instead of 6 symptoms in adults
• Age of onset changed to 11 years old ( from 7)
These slides are the intellectual property of Dr Paschos and must not be reproduced
Validity of diagnostic construct
• Reliability for operationally defined ADHD well established
• Validity questioned because of : - Symptom overlap with other common mental
disorders -Symptoms lie in a continuum in the general
population -No natural boundary between affected and
unaffected individuals
These slides are the intellectual property of Dr Paschos and must not be reproduced
Validating criteria I
• Symptom clustering
-consistent research finding for both subtypes
• Distinguishing symptoms
-ADHD often precedes the development of conduct disorder- the reverse does not occur
These slides are the intellectual property of Dr Paschos and must not be reproduced
Validating criteria I – COMT gene
• Catechol-O-Methy Transferance gene
(causing increased breakdown of dopamine)
• associated with antisocial behaviour in adolescents with ADHD (finding reported in 4 separate samples)
These slides are the intellectual property of Dr Paschos and must not be reproduced
catechol-O-methyltransferase (COMT) polymorphism
(Eisenberg, 1999)
• n=164
• DSM IV criteria, Conners Teaching Rating Hyperactivity scale, Continuous Performance Test False Alarm scale
• impulsive-hyperactive type of ADHD associated with the high enzyme activity COMT val allele.
These slides are the intellectual property of Dr Paschos and must not be reproduced
Validating criteria II
• Distinguishing ADHD from normal range of inattention, hyperactivity, impulsivity
-Severity in comparison to norms
-Non-fluctuating course
-Risk for co-occuring disorders
-Association with functional impairment
These slides are the intellectual property of Dr Paschos and must not be reproduced
Cognitive models of ADHD
• Problems with state regulation (related to arousal and activation levels)
• Delay aversion
• Inhibitory deficits: poor executive functioning
• Mood / motivation dysregulation
These slides are the intellectual property of Dr Paschos and must not be reproduced
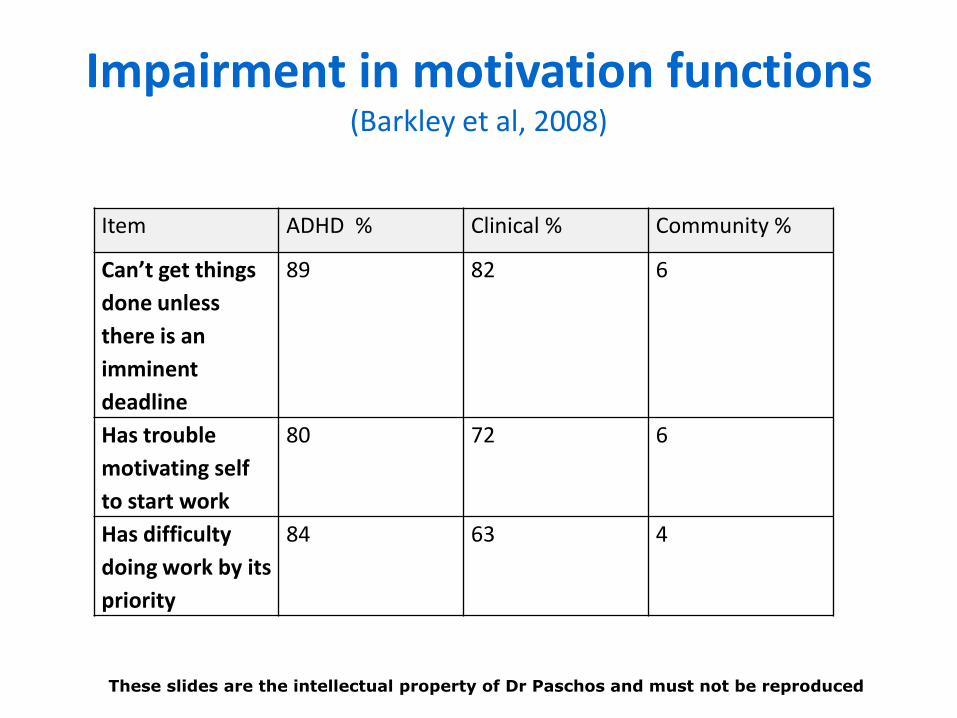
Impairment in motivation functions (Barkley et al, 2008)
Item ADHD % Clinical % Community %
Can’t get things
done unless
there is an
imminent
deadline
89 82 6
Has trouble
motivating self
to start work
80 72 6
Has difficulty
doing work by its
priority
84 63 4
These slides are the intellectual property of Dr Paschos and must not be reproduced
Cognitive models of ADHD II
• Multivariate family and twin analyses found 2 cognitive factors accounting for most ADHD:
-Reaction time and reaction time variability
-Omission and commission errors in continued performance tasks
These slides are the intellectual property of Dr Paschos and must not be reproduced
Intra-individual variability of ADHD impairments
• Transient but frequent lapses of attention
• Moment to moment variability in performance
Most studies focused on differences in performance between individuals with ADHD and those without
These slides are the intellectual property of Dr Paschos and must not be reproduced
Aetiology: genetic, environmental and neurobiological factors
• Association with wide range of measures
• Both environmental and genetic factors likely to play important role
These slides are the intellectual property of Dr Paschos and must not be reproduced
Structural and functional neuroanatomy of ADHD
• reductions in volume in cerebrum and cerebellum
• activation of more diffuse areas than controls during the performance of cognitive tasks
• hypoactivation of the dorsal anterior cingulate cortex, the frontal cortex and the basal ganglia
These slides are the intellectual property of Dr Paschos and must not be reproduced
Dorsal anterior midcingulate cortex
Critical role in attention, novelty detection, response inhibition and motivation
Most evidence of dysfunction in ADHD across all studies
Embedded in both reward processing and attention network
These slides are the intellectual property of Dr Paschos and must not be reproduced
Role of dopamine
• Role in attention, cognition and reward / learning
• SSRIs did not show the same symptom relief
These slides are the intellectual property of Dr Paschos and must not be reproduced
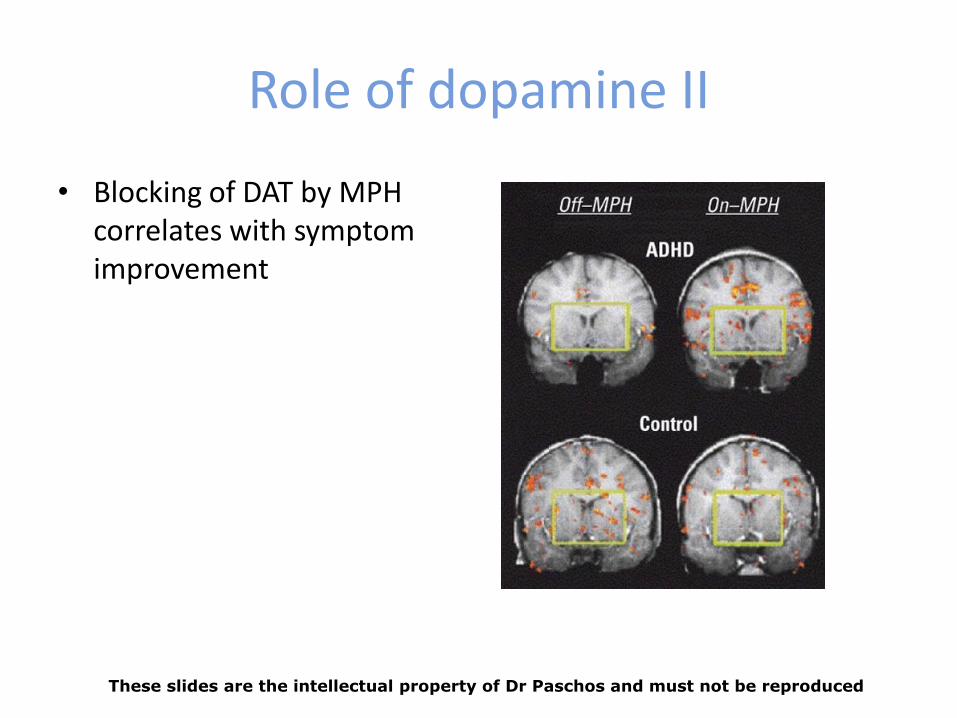
Role of dopamine II
• Blocking of DAT by MPH correlates with symptom improvement
These slides are the intellectual property of Dr Paschos and must not be reproduced
Environmental risks
• Diet
• Toxins: Lead, Mercury
• Pregnancy and delivery complications
• Fetal alcohol exposure
• Psychosocial adversity
These slides are the intellectual property of Dr Paschos and must not be reproduced
EPIDEMIOLOGY
Prevalence of ADHD in Adults
• 2.5 to 4.3% (Kessler et al, 2006)
• Male to female ratio 2:1 - 3:1
• Prescription data (UK): discontinuation rates in young adults far in excess of what would be expected by remission rates (McCarty et al, 2009)
These slides are the intellectual property of Dr Paschos and must not be reproduced
EPIDEMIOLOGY
• Kooij et al (2005) validity of adult ADHD in a population based sample (n=1815) of adults18-75 yrs
• Prevalence in adults: 1% (cut-off 6 Sx; and 2.5% cut-off 4 Sx)
These slides are the intellectual property of Dr Paschos and must not be reproduced
Intelligence and ADHD
• IQ tests not comprehensive assessment of higher executive functions (Delis et al, 2007)
• Sample of 49 high IQ (>120) children with ADHD showed pattern of cognitive, psychiatric and behavioural features typical of children with average IQ and ADHD
• High IQ young adults with ADHD & impairments in working memory
These slides are the intellectual property of Dr Paschos and must not be reproduced
Differences in the development of cortical thickness of children with ADHD and below median IQ ADHD versus
matched controls
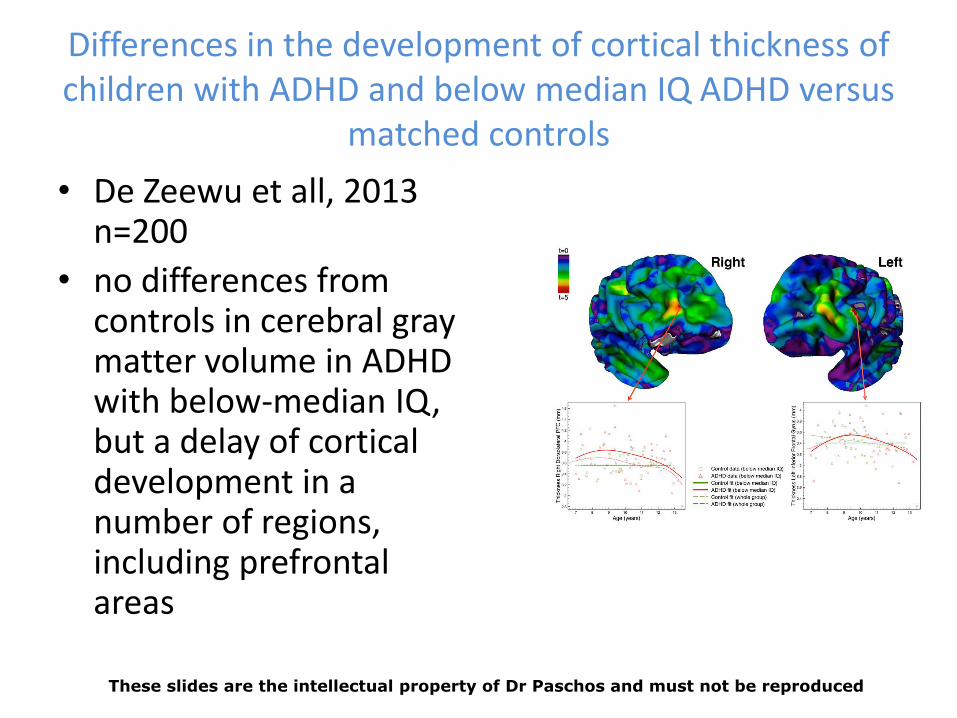
• De Zeewu et all, 2013 n=200
• no differences from controls in cerebral gray matter volume in ADHD with below-median IQ, but a delay of cortical development in a number of regions, including prefrontal areas
These slides are the intellectual property of Dr Paschos and must not be reproduced
ADHD in adults with Mild / Borderline ID
Maltezos, 2008 • N= 48 LD-ADHD (IQ< 80) vs 221 ADHD non -LD
(IQ>=80) • LD group higher number of the current
inattentive symptoms' ratings and higher scores for all items during childhood
• Non-LD group: most symptoms improved from childhood to adulthood
• LD Group: five components accounted 73.98% of the variance for informants' ratings
These slides are the intellectual property of Dr Paschos and must not be reproduced
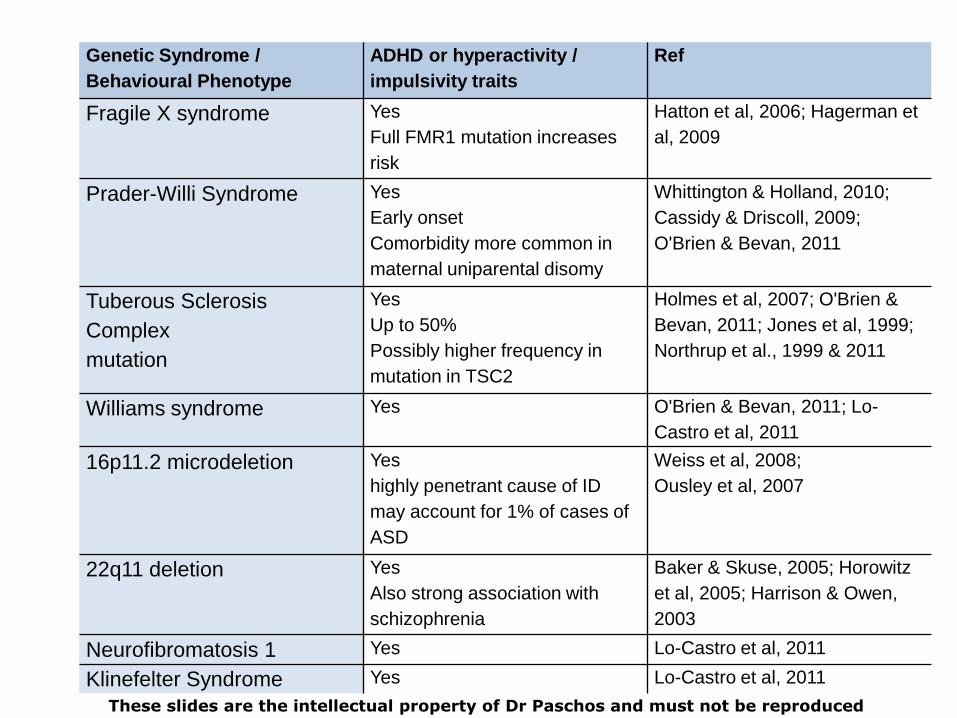
Genetic Syndrome /
Behavioural Phenotype
ADHD or hyperactivity /
impulsivity traits
Ref
Fragile X syndrome Yes
Full FMR1 mutation increases
risk
Hatton et al, 2006; Hagerman et
al, 2009
Prader-Willi Syndrome Yes
Early onset
Comorbidity more common in
maternal uniparental disomy
Whittington & Holland, 2010;
Cassidy & Driscoll, 2009;
O'Brien & Bevan, 2011
Tuberous Sclerosis
Complex
mutation
Yes
Up to 50%
Possibly higher frequency in
mutation in TSC2
Holmes et al, 2007; O'Brien &
Bevan, 2011; Jones et al, 1999;
Northrup et al., 1999 & 2011
Williams syndrome Yes O'Brien & Bevan, 2011; Lo-
Castro et al, 2011
16p11.2 microdeletion Yes
highly penetrant cause of ID
may account for 1% of cases of
ASD
Weiss et al, 2008;
Ousley et al, 2007
22q11 deletion Yes
Also strong association with
schizophrenia
Baker & Skuse, 2005; Horowitz
et al, 2005; Harrison & Owen,
2003
Neurofibromatosis 1 Yes Lo-Castro et al, 2011
Klinefelter Syndrome Yes Lo-Castro et al, 2011
These slides are the intellectual property of Dr Paschos and must not be reproduced
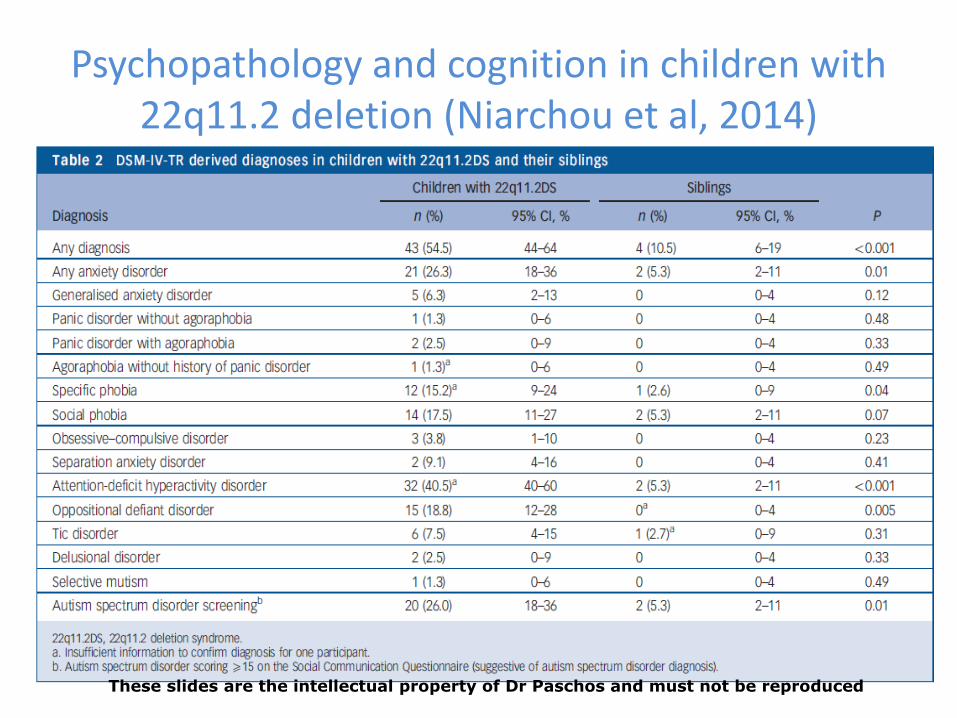
Psychopathology and cognition in children with 22q11.2 deletion (Niarchou et al, 2014)
These slides are the intellectual property of Dr Paschos and must not be reproduced
Psychopathology and cognition in children with 22q11.2 deletion (Niarchou et al, 2014)
These slides are the intellectual property of Dr Paschos and must not be reproduced
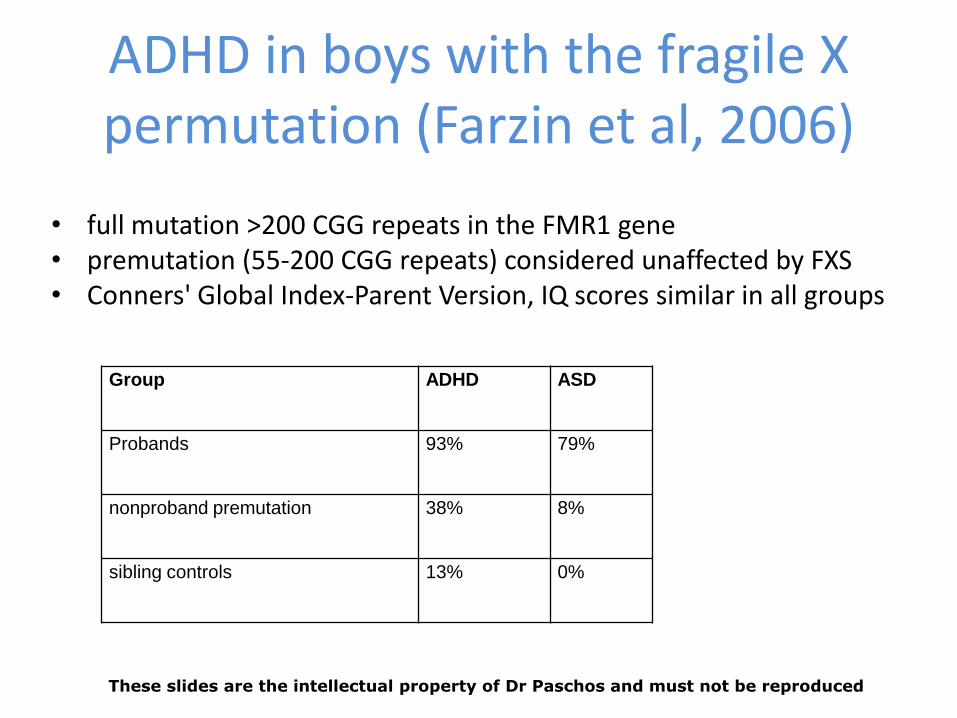
ADHD in boys with the fragile X permutation (Farzin et al, 2006)
• full mutation >200 CGG repeats in the FMR1 gene • premutation (55-200 CGG repeats) considered unaffected by FXS • Conners' Global Index-Parent Version, IQ scores similar in all groups
Group ADHD ASD
Probands 93% 79%
nonproband premutation 38% 8%
sibling controls 13% 0%
These slides are the intellectual property of Dr Paschos and must not be reproduced
ASSESSMENT: Principles
• History of childhood ADHD is essential
• Collateral history always necessary
• Continuous rather than episodic features (developmental disorder)
These slides are the intellectual property of Dr Paschos and must not be reproduced
ASSESSMENT
1. Structured full psychiatric interview with focus on – Family history – Personal, developmental, educational, occupational, and social
history – Current ADHD symptoms – Co morbid conditions / substance misuse
2. Neuropsychological evaluation
These slides are the intellectual property of Dr Paschos and must not be reproduced
MSE during assessment for ADHD
• Restlessness and distractibility may not be seen
• Sensitivity of symptoms to stimulating or novel situations
• Patients can normalise behaviour for short periods of time
These slides are the intellectual property of Dr Paschos and must not be reproduced
ASSESSMENT – rating scales
• Variety of validated questionnaires (Connors, Barkley) to assess current symptoms, monitor response to treatment
• Scales for retrospective childhood diagnosis, side effects
• Semi-structured interview schedules
These slides are the intellectual property of Dr Paschos and must not be reproduced
Adult ADHD Self-Report Scale (ASRS-v1.1) Symptom Checklist (WHO, available free on the web)
These slides are the intellectual property of Dr Paschos and must not be reproduced
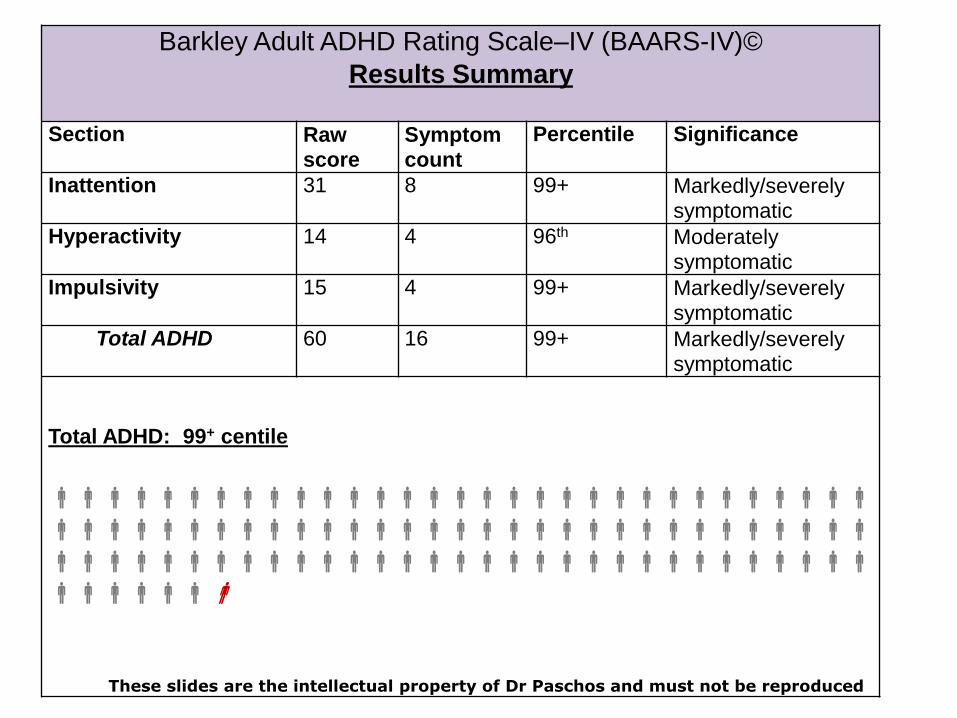
symptomatic Total ADHD 60 16 99+ Markedly/severely
symptomatic
Total ADHD: 99+ centile
These slides are the intellectual property of Dr Paschos and must not be reproduced
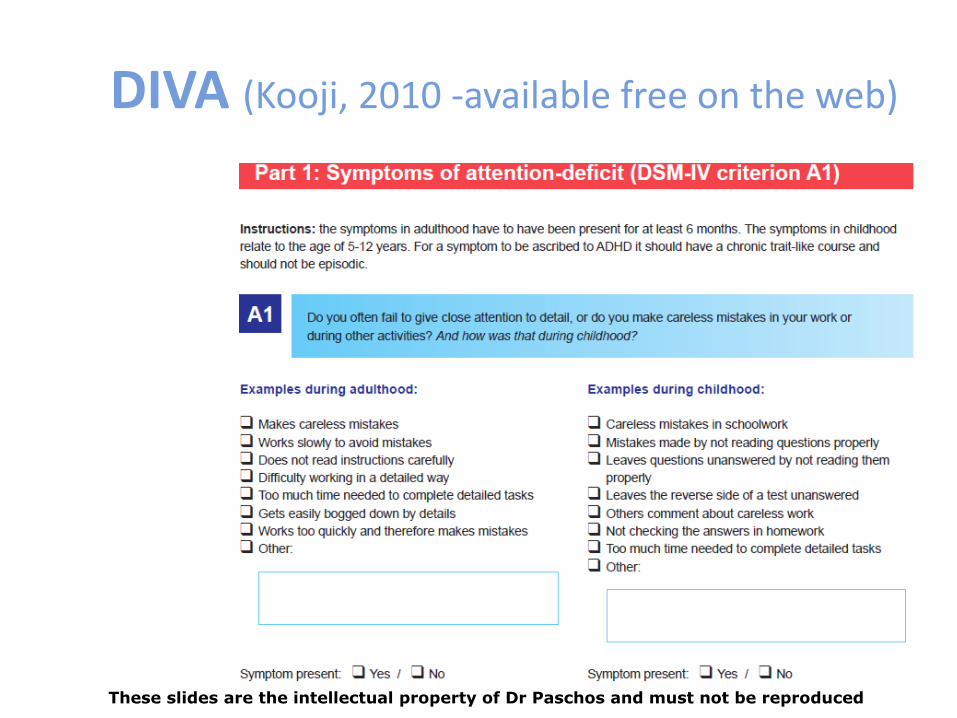
DIVA (Kooji, 2010 -available free on the web)
These slides are the intellectual property of Dr Paschos and must not be reproduced
Children with ID and ADHD – use of rating scales
(Deb et al, 2008) • Aim to find cut-off scores for the Conners’ Parent Rating
Scales-Revised (CPRS-R) and the • Conners’ Teacher Rating Scale-Revised (CTRS-R) • CPRS-R total score of 42: sensitivity of 0.9 and specificity of
0.67 • CTRS-R total score of 40: sensitivity of 0.69 and specificity
of 0.67 • CPRS-R scores may distinguish between children with ID
with and without ADHD but not the CTRS-R scores • Need to develop an ADHD screening instrument specifically
for ID
These slides are the intellectual property of Dr Paschos and must not be reproduced
Neuropsychology Assessment
1. General Intellectual Functioning
– WAIS
2. Attention
a. Selective
b. Divided
c. Switching
d. Sustained
3. Impulsivity
4. Executive Function
These slides are the intellectual property of Dr Paschos and must not be reproduced
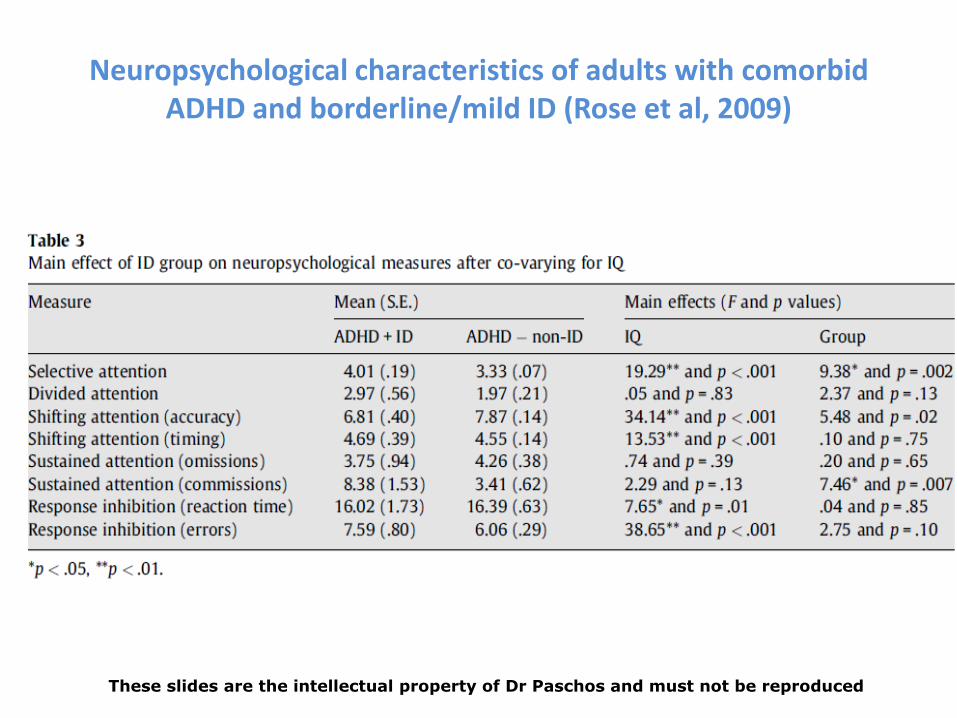
Neuropsychological characteristics of adults with comorbid ADHD and borderline/mild ID (Rose et al, 2009)
• ADHD and mild-borderline ID (N = 59), ADHD and normal intellectual functioning (N = 95)
• co morbid group had significantly lower scores
• Differences remained significant after co-varying for level of intellectual functioning
• ADHD and ID group vulnerable to ‘double deficit’
These slides are the intellectual property of Dr Paschos and must not be reproduced
Neuropsychological characteristics of adults with comorbid ADHD and borderline/mild ID (Rose et al, 2009)
These slides are the intellectual property of Dr Paschos and must not be reproduced
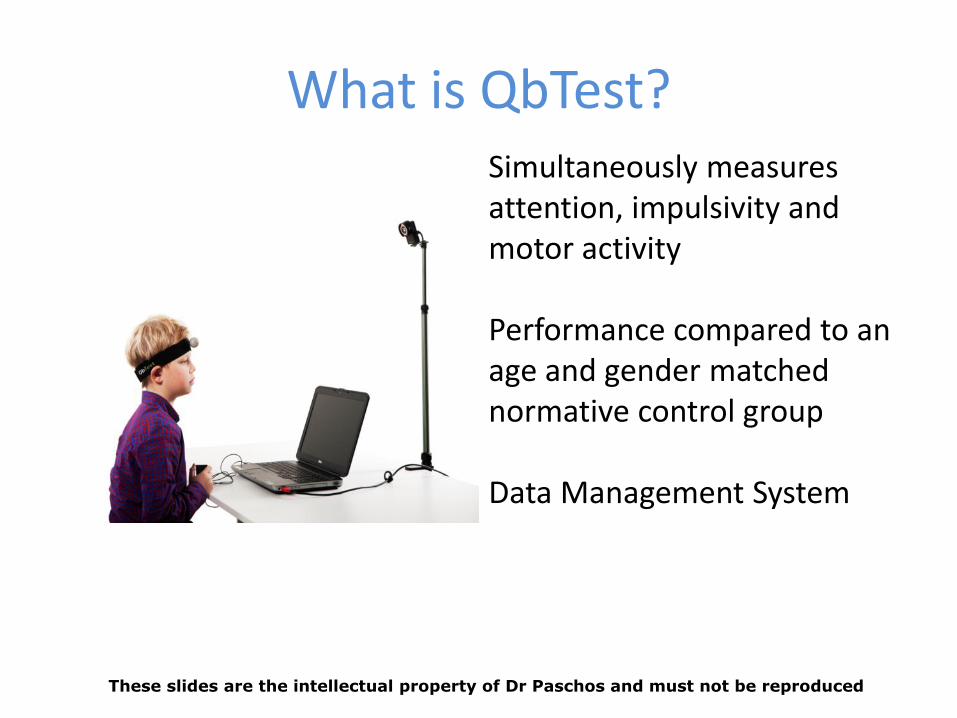
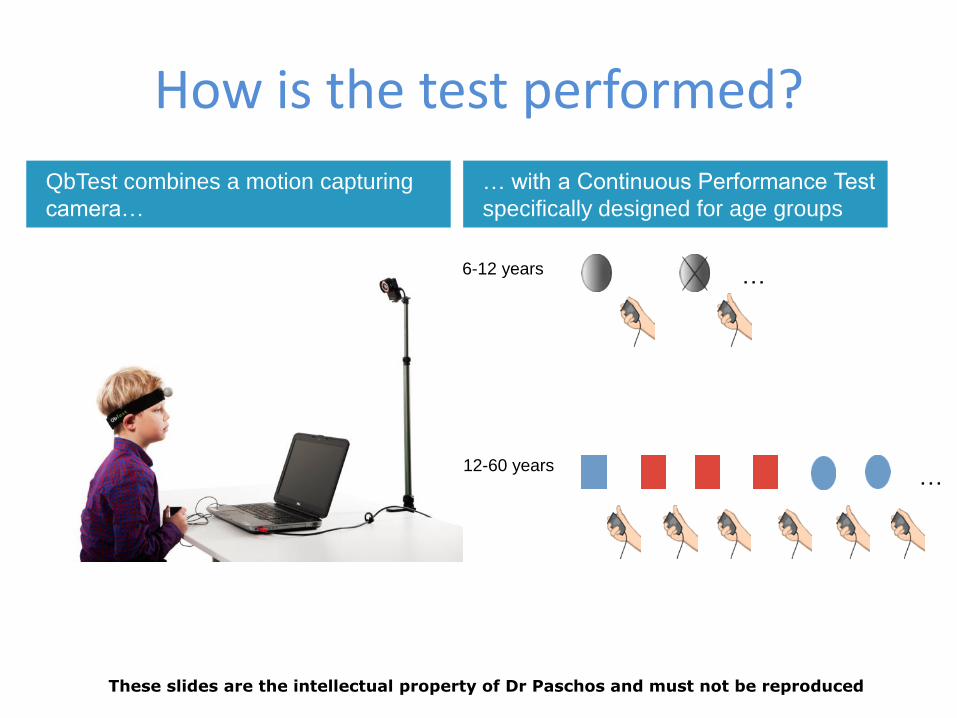
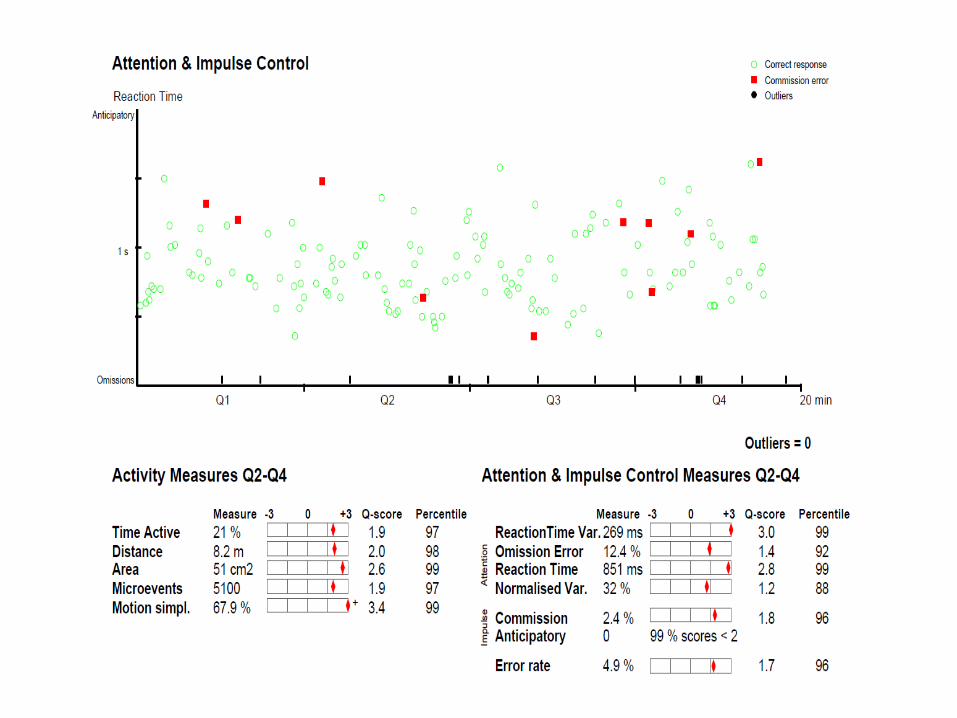
What is QbTest? Simultaneously measures attention, impulsivity and motor activity Performance compared to an age and gender matched normative control group Data Management System
These slides are the intellectual property of Dr Paschos and must not be reproduced
How is the test performed?
…
… 6-12 years
12-60 years
… with a Continuous Performance Test
specifically designed for age groups
QbTest combines a motion capturing
camera…
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
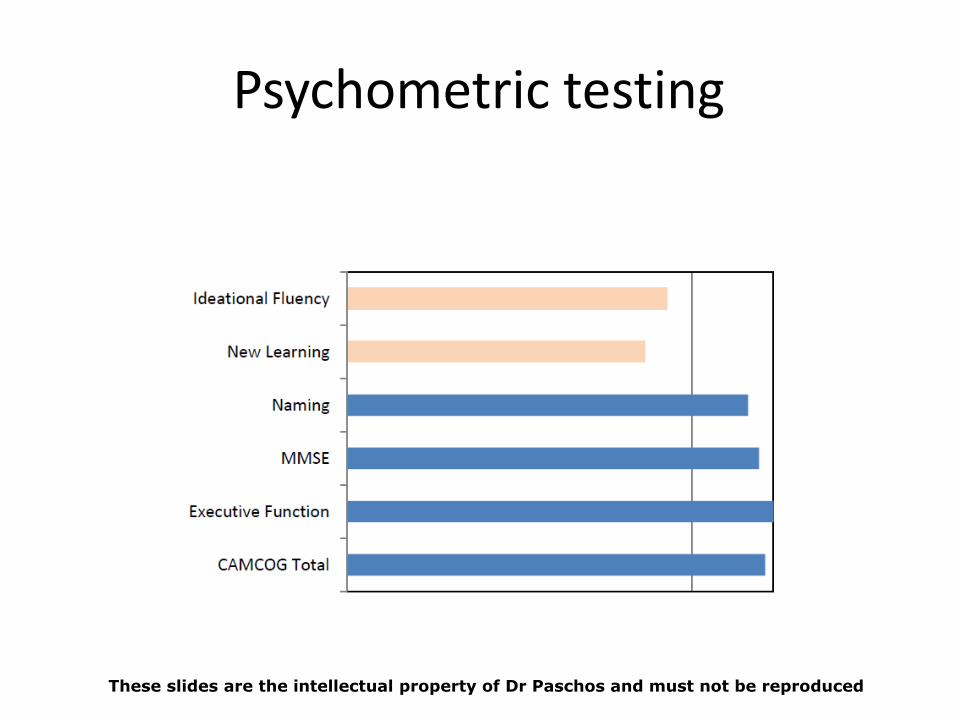
Psychometric testing
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
CO-MORBIDITIES: Adults
• Anxiety disorders 50%
• Mood disorders, antisocial disorders, and alcohol/drug: substantial prevalence rates
ADHD and Epilepsy (children)
• Kaufmann et al, 2009 • 20% of children with epilepsy have ADHD vs 3% to 7% • Possible causes: common genetic propensity,
noradrenergic system dysregulation, subclinical epileptiform discharges, seizures, antiepileptic drug effects
• Children with ADHD: higher than normal rate of electroencephalography abnormalities (5.6-30.1% vs. 3.5%)
• MPT equally efficient in children with isolated ADHD and in children with ADHD and epilepsy (70%-77%)
• Caution: reports of seizure aggravation in MPT-treated children with uncontrolled epilepsy have raised concern.
ADHD and criminality
• N= 25,656
• Significant reduction of 32% in the criminality rate for men and 41% for women as compared with non-medication periods
Lichtenstein et al, 2012
ADHD, BAD, BPD: similarities and differences (Handbook for ADHD in adults, UKAAN 2013)
Borderline Bipolar
Similarities with
ADHD
Childhood or adolescent onset Chronic trait like course Impulsivity – anger Impaired social relationships Mood instability Pervasive across situations
Identity disturbance Recurrent suicidal behaviour Chronic feelings of emptiness Frantic efforts to avoid
abandonment
Episodic course Elated mood Psychosis Often lacks insight
TREATMENT
• Psychosocial interventions
• Pharmacotherapy
These slides are the intellectual property of Dr Paschos and must not be reproduced
PSYCHOSOCIAL INTERVENTIONS
• CBT
• Family /couple interventions
• ADHD coaching
• Self-help groups
• Anger management, skills development
These slides are the intellectual property of Dr Paschos and must not be reproduced
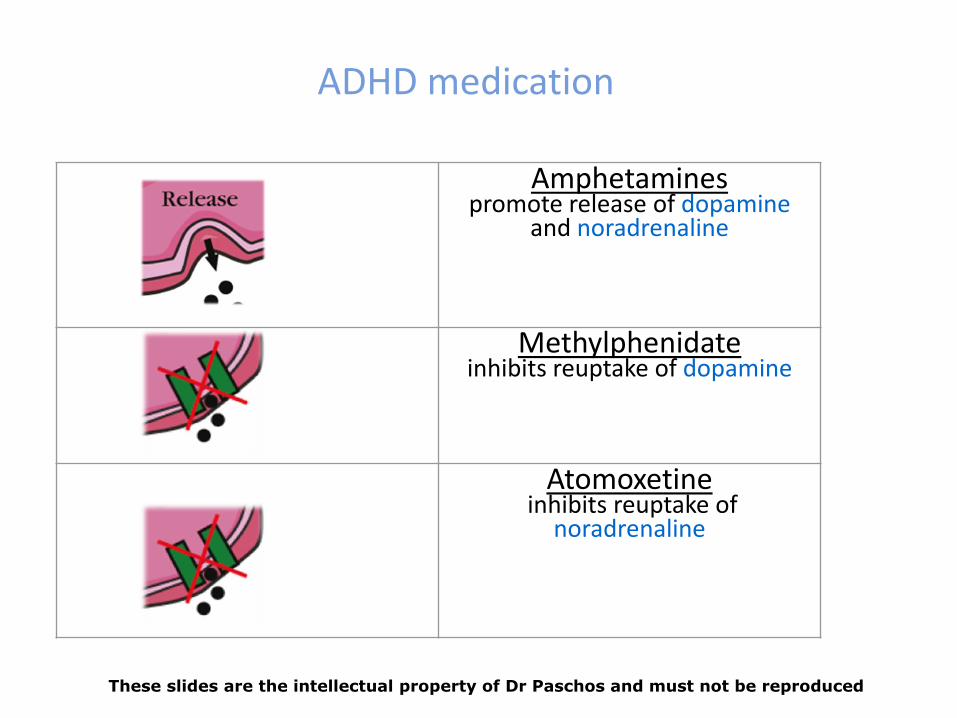
Amphetamines promote release of dopamine
and noradrenaline
Methylphenidate inhibits reuptake of dopamine
Atomoxetine inhibits reuptake of
noradrenaline
ADHD medication
These slides are the intellectual property of Dr Paschos and must not be reproduced
Drug treatment of ADHD
• Part of a holistic treatment programme
• Before starting and every 6 months: pulse, blood pressure, weight
• Bloods and ECG
• Review need to continue treatment annually
These slides are the intellectual property of Dr Paschos and must not be reproduced
Stimulants Non-stimulants
Methylphenidate
Short acting: Medikinet,
Ritalin
Long Acting: Concerta XL,
Equasym XL, Medikinet XL
Atomoxetine
Strattera
Dexamphetamine
Dexedrine
Elvanse
Licensed medication for treatment of ADHD in children in the UK
These slides are the intellectual property of Dr Paschos and must not be reproduced
Stimulants for adults with ADHD and ID
Jou et al, 2004
• Small open label study
• Aberrant Behaviour Checklist-Community Version (ABC-C)
• Clinical Global Impression scale
• Significant improvements in the hyperactivity and irritability subscales of the ABC-C
• Adverse events minimal
These slides are the intellectual property of Dr Paschos and must not be reproduced
Methylphenidate in Children with ADHD With or Without LD
(Williamson et al, 2014)
• 6-week, double-blind,randomized, placebo-controlled, crossover studies evaluating individually determined doses of OROS methylphenidate versus placebo (n=135)
• In children with ADHD with or without comorbid LD, behaviour and performance improved during treatment
These slides are the intellectual property of Dr Paschos and must not be reproduced
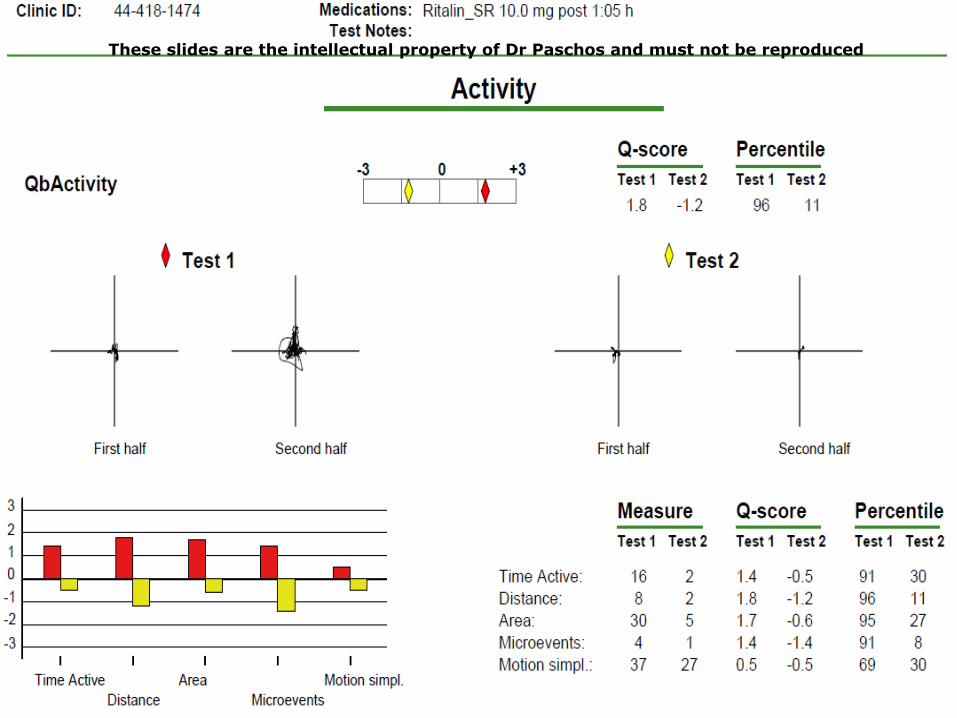
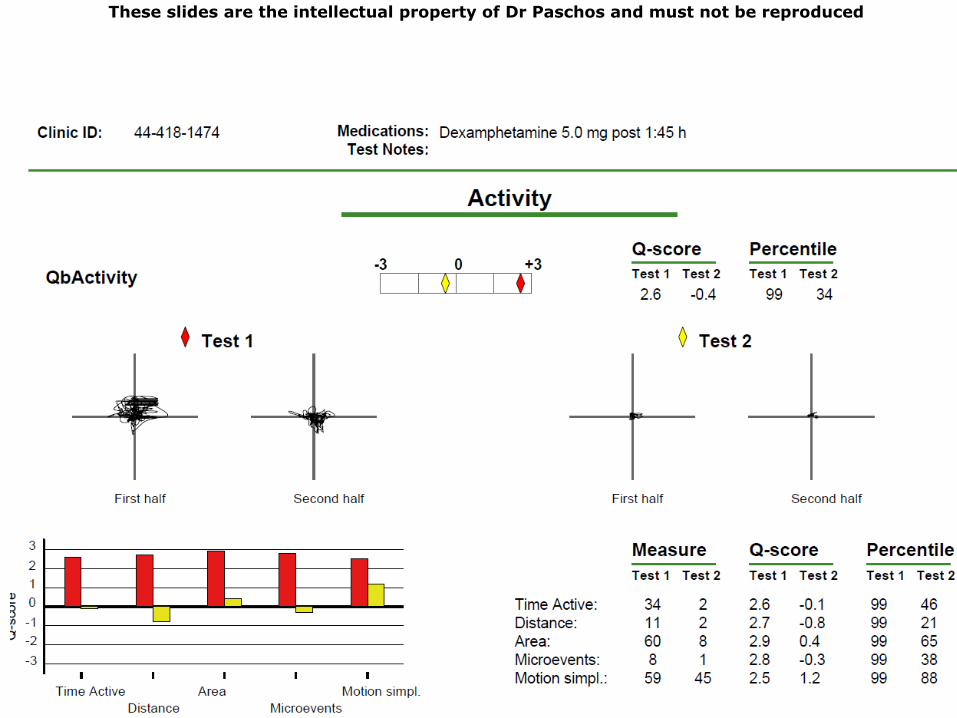
Case A- treatment
• Bloods, ECG, BP, Pulse normal
• No other psychiatric problems
• No substance misuse
• Started on Methylphenidate 5mg bd, titrated up to 10mg tds
• Highly significant improvements in all core ADHD deficits, academic performance and self management
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
These slides are the intellectual property of Dr Paschos and must not be reproduced
Stimulants: Efficacy
Children response rates 25-73%
Reduced efficacy in adults
1) Lack of consistent diagnostic criteria
2) Inadequate dosage
3) Presence of comorbidity
4) Poorly developed outcome measures
These slides are the intellectual property of Dr Paschos and must not be reproduced
Stimulants side effects
• Well tolerated in adults • Common side effects: insomnia, edginess, diminished
appetite, dysphoria, headache • Usually remit spontaneously over time • Effect on BP/HR usually minimal • US 1999 to 2003: 25 deaths, 26 serious adverse events such
as heart attack or stroke
These slides are the intellectual property of Dr Paschos and must not be reproduced
ELVANSE® (lisdexamfetamine dimesylate)
• Inactive pro-drug
• Slow release, long lasting effect
• Less potential for abuse
These slides are the intellectual property of Dr Paschos and must not be reproduced