60
ADVANCES IN ULTRASOUND THI,CEUS and TRUS PRESENTOR-DR.SANGEETA JHA MODERATOR-DR GAURAV SHRIVASTAVA
| Date post: | 26-Jan-2017 |
| Category: |
Health & Medicine |
| Upload: | sangeeta-jha |
| View: | 233 times |
| Download: | 0 times |

ADVANCES IN ULTRASOUND
THI,CEUS and TRUS
PRESENTOR-DR.SANGEETA JHA MODERATOR-DR GAURAV SHRIVASTAVA

TISSUE HARMONIC IMAGING• Is a grayscale ultrasound mode that provides images of higher quality than
conventional sonography Based on the phenomenon of nonlinear distortion of acoustic signal as it
travels through the body.Imaging begins with insonation of tissue with ultrasound waves of a specific
transmitted frequency. Harmonics are produced by tissue vibration and are usually integral
multiples of the transmitted frequency In comparison ,conventional ultrasound waves are generated at the surface
of the transducer and progressively decrease in intensity as they traverse the body
Harmonic wave frequencies are higher integer multiples of the transmitted frequency, Current technology uses only the second harmonic(twice the transmitted frequency) for imaging.
The processed image is formed with use of the harmonic-frequency bandwidth in the received signal after the transmitted frequency spectrum is filtered out

Time sequence illustrates the generation of harmonic frequencies. Time step 1 contains a wave of single frequency. As the wave travels into the tissue (time step 2), it becomes distorted. Additional frequency components are created that are integer multiples of the initial frequency. These components are called “harmonic frequencies.” As the wave continues to travel, it becomes highly distorted (time step 3) and very rich in harmonic frequencies. Harmonic frequencies are created and accumulate as the wave travels through the tissue. Amplitudes of the higher harmonics are extremely small. Therefore, current technology uses only the second harmonic (2f), which is twice the nominal transmitted frequency.

Frequency spectrum of the transmitted and received waves. The fundamental wave (f) is generated at the transducer surface and attenuates linearly as it is transmitted through the body. The harmonic wave (2f) is generated as the fundamental wave travels through the body. The harmonic wave increases exponentially in intensity before attenuating within the deeper tissues.
Harmonic imaging uses only the second harmonic frequency in the echo signal received by filtering out the transmitted frequency spectrum in the signal

Schematic depicts the relative intensities and frequency changes of harmonic ultrasound beamsand fundamental transmitted waves with increasing depth in tissues.

ADVANTAGE OF THI1) Improved axial resolution -due to shorter wavelength 2) better lateral resolution -due to improved focusing
with higher frequencies, 3) less artifact than with conventional US- Reduced
artifact in harmonic imaging is due to the relatively small amplitude of the harmonic waves, which reduces detection of echoes from multiple scattering events.
4) less side lobes artifacts.5) Better imaging option for obese patients- harmonic
beams are produced beyond the body wall, thereby reducing the defocusing effect of the body wall.
Harmonic imaging increases diagnostic confidence in differentiating cystic from solid hepatic lesions, Improves detection of gallbladder and biliary calculi,
Improves pancreatic definition
Allows distinction of simple from complex renal cysts.
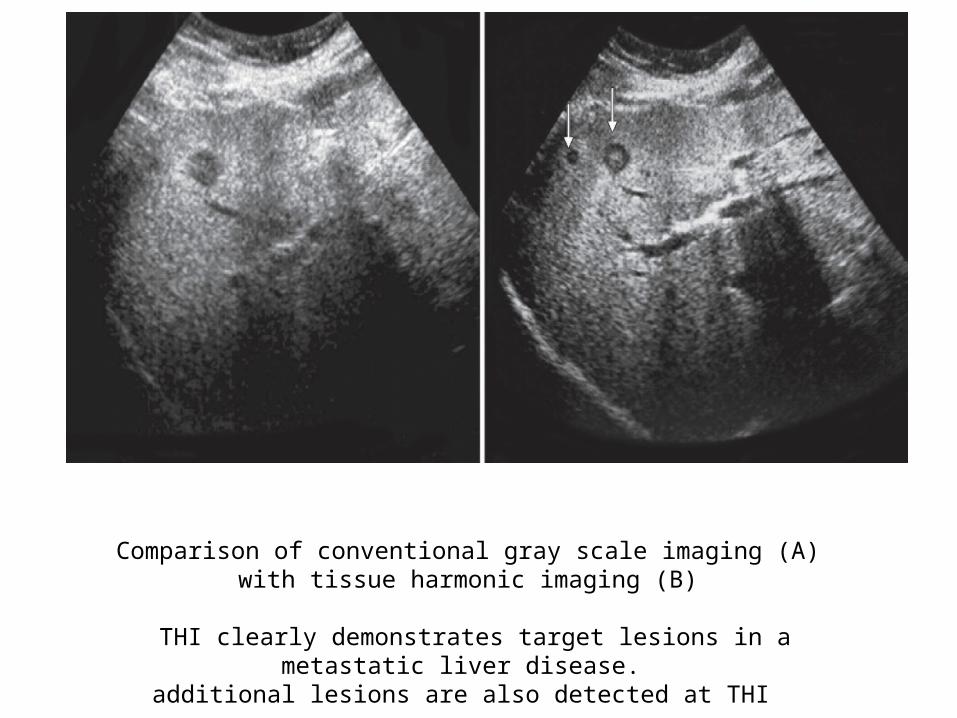
Comparison of conventional gray scale imaging (A) with tissue harmonic imaging (B)
THI clearly demonstrates target lesions in a metastatic liver disease.
additional lesions are also detected at THI

Tissue harmonic imaging (A) demonstrates much better delineation of both cystic and solid lesions in this patient
of Renal angiomyolipomas, when compared to conventional grayscale imaging (B)
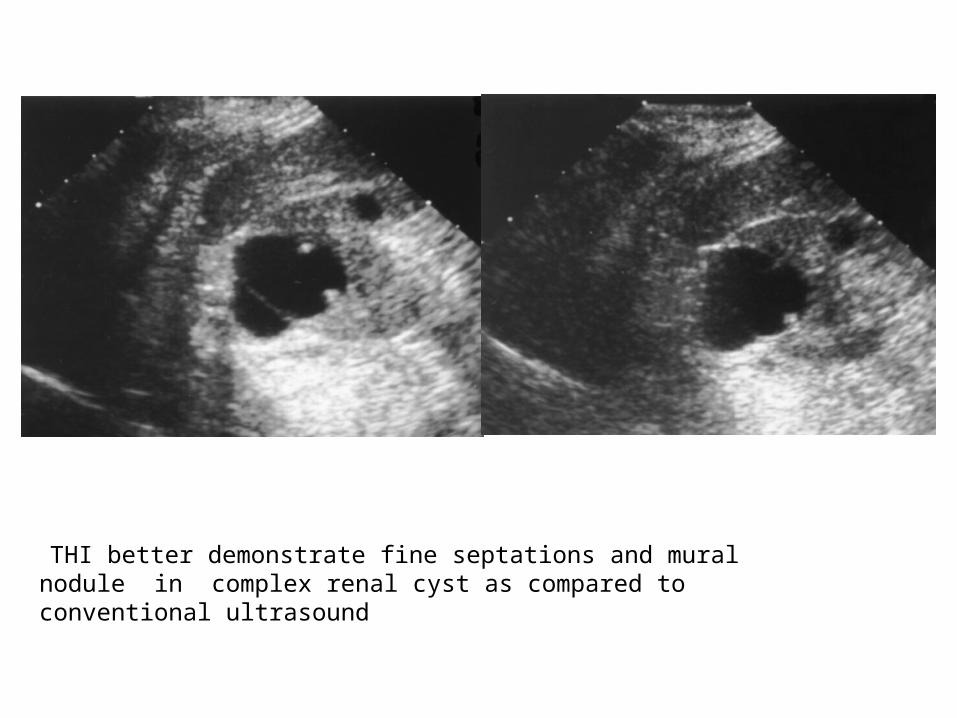
THI better demonstrate fine septations and mural nodule in complex renal cyst as compared to conventional ultrasound

Choledocholithiasis with liver metastases. Both the harmonic (a) and conventional (b) US images show a dilated common duct and multiple liver metastases. The obstructing stone in the common duct was detected on only a,

Gallbladder polyp. Small polyp on the anterior surface of the gallbladder is seen on the harmonic image (a) with marked reduction of noise in the gallbladder lumen compared with that on the conventional US image (b).
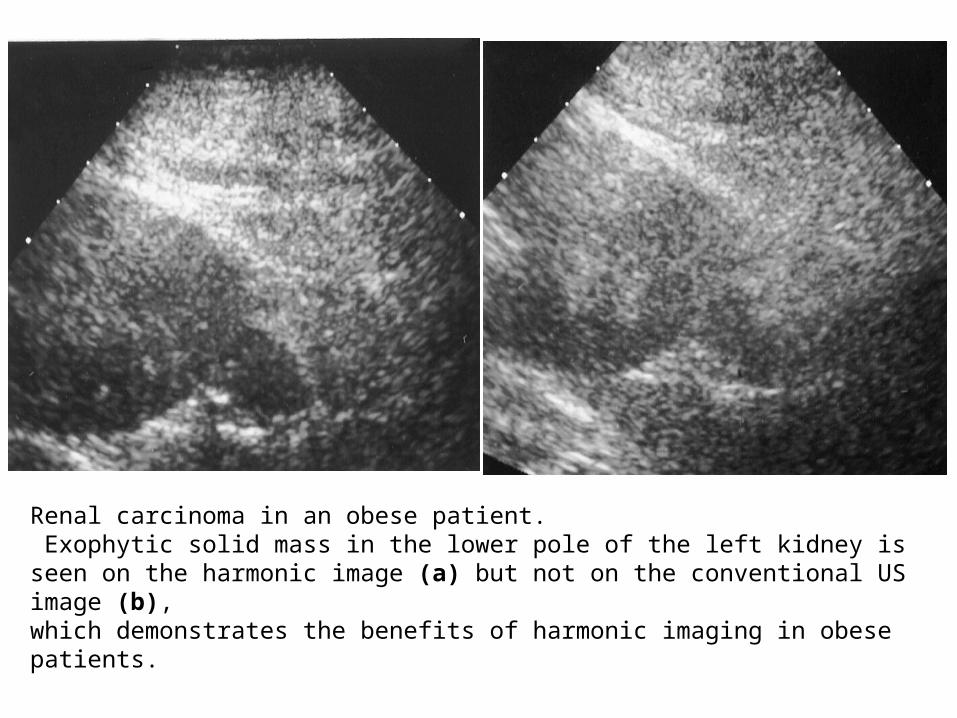
Renal carcinoma in an obese patient. Exophytic solid mass in the lower pole of the left kidney is seen on the harmonic image (a) but not on the conventional US image (b),which demonstrates the benefits of harmonic imaging in obese patients.

In conventional US, optimal resolution was achieved by using a higher frequency. This, at times, compromised adequate penetration, which necessitated use of a lower frequency.
Harmonic imaging provides better resolution by using a higher frequency for imaging without compromising depth penetration.

CONTRAST ENHANCED ULTRASOUNDIt has twin components--ultrasound contrast agent (UCA)- contrast specific imaging modes.
It can detect the hemodynamics of the targeted organ and provide detailed information of the microvascularity and microperfusion observed by real time scanning .

Although Doppler imaging may provide valuable directional blood flow information but is is most effective for evaluating large blood vessels with fast flowing blood such as the carotid arteries,leg veins,and major visceral vessels of the abdomen, including the portal veins and hepatic arteries.
The ability of Doppler imaging to detect blood flow at the tissue perfusion level is limited.

The remedy for this problem is to add microbubble contrast agents and specialized ultrasound imaging techniques.
The former enhances the Doppler signal from blood, whereas the latter serves to suppress the signals from the background tissue while enhancing the sensitivity to the Doppler signals from the microbubbles within the blood pool. These additions allow ultrasound imaging of blood flow at the tissue perfusion level, thus enabling ultrasound to play a competitive role relative to CT and MRI in the evaluation of the solid and hollow organs of the abdomen and pelvis.

CONTRAST AGENTSmicrobubbles composed of tiny bubbles of an injectable
gas in a supporting shell.They are blood pool agents and remain confined to the
intravascular space after intravenous injection. Small microbubbles (1-10 um) can pass through the
lung capillaries and remain in circulation for a short time and eventually get dissolved.
The gas gets exhaled while the shell gets metabolized in the liver.
The UCAs, while in circulation, strongly increase the ultrasound backscatter and produce enhancement of echogenicity for the assessment of blood flow


FIRST GENERATION US CONTRAST AGENTSTendency to dissolve into the solution very quickly, resulting in short imaging window. ECHOVIST was the first commercially available UCA introduced in 1991,
Made of air bubbles coated with galactose
Had a very short life in the blood with minimal transpulmonary circulation limiting its clinical utility.
It was predominantly used for the evaluation of the cardiac shunt and the female genital tract.

ALBUNEX was the first FDA approved contrast agent in 1994.
Composed of air filled albumin microspheres suspended in 5 percent w/v human albumin solution.
In vivo half life < 5 minutes.
It was used predominantly for the evaluation of cardiac shunts and valvular regurgitation with limited extra-cardiac applications
It is no longer manufactured.

LEVOVIST Came up In 1996, it was a relatively longer lasting UCA
It contained air bubbles with a galactose/ palmitic acid surfactant coating .
Main indications for use were cardiac, intracranial and abdominal.
However, the Levovist bubbles easily collapsed under ultrasound emission owing to its fragile properties, therefore real time images could not be obtained for a longer period

SECOND GENERATION US CONTRAST AGENTS The second generation UCAs are pure blood pool agents as they are
unable to destroy the vascular endothelium and thus remain exclusively intravascular resulting in prolonged enhancement of the vascular system. No extravasation into the interstitial fluid occurs.
Contain insoluble gases like sulphur hexafluoride (SF6) or perfluorocarbons and have a surface shell made of different substances like phospholipids, albumin or polymers providing better stabilization.
Their smaller size enables a successful transpulmonary passage to reach the various target organs.
After intravenous injection, due to their low solubility in water, better stabilization and strong harmonic response-- prolonged visualization of dynamic enhancement of the organ can be observed on real-time ultrasound scanning


OPTISON AND LUMINITY Made of octafluoropropane coated with albumin and lipid shell
respectively.
The octafluoropropane gas has low water solubility and is more stable providing longer imaging period.
However, their sole indication for use has been cardiac.
SONOVUE contains sulphur hexafluoride stabilized by phospholipid shell.
It is an ideal ultrasound contrast agent for vascular phase imaging of different target organs and is being used widely with promising results.
It is the only contrast agent available in India.

SONAZOID Most recent second generation UCA
Contains perflubutane and has a hard shell.
exhibits the longest window period for imaging, the extended late phase.
It has been successfully used in the evaluation of liver tumors.
This UCA can depict the hemodynamics of the liver in the vascular and the post vascular phase also called the ‘Kupffer phase’. This is because, the Kupffer cells of the liver phagocytose Sonazoid microbubbles and thus persist in the liver for long.
it is available only in Japan.

IMAGING TECHCHNIQUE• A good US machine equipped with low MI contrast imaging
mode is required.
• For intravenous use-recommended dose of SonoVue is 2.4 ml.
• A higher dose is used for endoscopic contrast enhanced ultrasound (CE-EUS) and when using high frequency transducers.
• For renal and pancreatic evaluation a low dose of 1.0 ml is used.
• For extravascular use, a few drops of SonoVue in 10 to 100 ml of saline may be sufficient.
For intravenous use of UCAs-• Antecubital access using 20 gauge venflon with a three way
connector is obtained.
• The contrast material in the vial, e.g. (SonoVue) is prepared in the soluble form 5 minutes prior and shaken well to be properly dissolved for use.
• The target organ is visualized on the B mode US and then keeping the lesion in focus the contrast-specific imaging mode is turned on.
• A simultaneous display of the tissue and contrast signals can be seen on the monitor as a dual window which ensures the target lesion remains in the field of view throughout the study.

• The freshly prepared Sonovue is administered as an intravenous bolus followed by flushing with 10 ml of 0.9 percent normal saline.
• The enhancement characteristics of the target organ is observed on real time by continuously scanning till the three vascular phases post injection.
• The observation is recorded on the cine mode.
• Post procedure, the patient is observed for about an hour for any adverse reaction if any due to the UCA
SAFETY OF UCAs UCAs are well tolerated and safe with few non-specific side effects. Clearance of UCA is very fast and 80 to 90 percent of it gets eliminated through the lungs in 11 minutes.Life threatening anaphylactoid complications are very rare (0.001%).
Unlike other contrast agents used for CT or MRI, the UCAs are not nephrotoxic as they have no renal excretion. Hence, CEUS can be safely done in patients with compromised renal function.

CONTRAINDICATIONS TO THE USE OF UCAS • cardio-pulmonary disease • pregnancy and breast-feeding • severe coronary artery disease. • Cautious use is recommended in neonates• use prior to extra-corporeal shock wave therapy
ADVANTAGES OF CEUScost-effective can provide accurate diagnostic information
comparable to CT and MRIcan be performed at the bedside no ionizing radiationhas no nephrotoxicity-do not require lab evaluation
and can be used repeatedly in renal failure patients.
DIAGNOSTIC APPLICATIONS OF UCAsApplications in Hepatic Imagingliver has a dual blood supply -hepatic artery and the
portal vein which allows evaluation of the liver by real time scanning in three vascular phases
Enhancement pattern of the liver nodule is observed -arterial phase (AP) upto 30 secs-portal venous phase (PP) from 31 to 120 secs and -delayed phase (DP) from 120 to 180 secs.Intermittent scanning is done where contrast is seen
persisting in the late phase upto 5 minutes or so. If another mass needs to be studied in the same patient,
then the same procedure is repeated with a fresh bolus of UCA after 10 minutes.

Enhancement patterns of benign focal liver lesions Focal liver lesion Arterial phase Portal venous phase Late phase
Hemangioma Peripheral nodular enhancement
Partial/complete centripetal fill in
Complete enhancement
Focal nodular hyperplasia
Hyperenhancing from the center, early Spoke wheel arteries, feeding artery
Hyperenhancing Iso/hyperenhancing Unenhanced central scar
Hepatocellular adenoma
Hyperenhancing, complete
Isoenhancing Isoenhancing
Focal fatty infiltration/sparing
Isoenhancing Isoenhancing Isoenhancing
Simple cyst Nonenhancing Nonenhancing Nonenhancing

Hemangioma – Typical pattern. showing peripheral nodular enhancement (arrow heads) in the AP at 23 secs post-contrast injection (A) with progressive centripetal enhancement (B) becoming isoenhancing (arrow) in the LP at 240 secs (C)
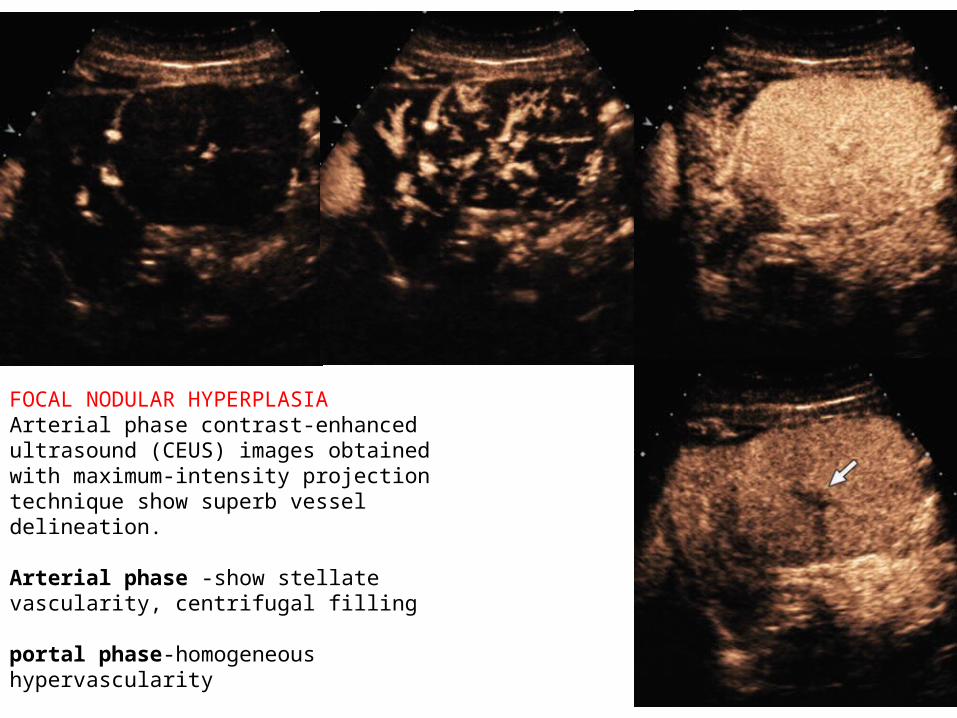
FOCAL NODULAR HYPERPLASIAArterial phase contrast-enhanced ultrasound (CEUS) images obtained with maximum-intensity projection technique show superb vessel delineation.
Arterial phase -show stellate vascularity, centrifugal filling
portal phase-homogeneous hypervascularity
late phase at 3 minutes -shows sustained contrast enhancement and central nonenhancing scar

• Enhancement patterns of malignant focal liver lesions
FLL Arterial phase Portal venous phase Late Phase
Metastasis Rim-enhancement Hypoenhancing Hypo/non enhancing
HCC(non-cirrhotic )
HCC(cirrhotic)
Hyperenhancing
Inhomogenous hyperenhancing
Isoenhancing
Isoenhancing
Hypo/non enhancing
Iso/hypoenhancing
Cholangiocarcinoma Rim-like hyperenhancement, central hypoenhancement /Inhomogenous hyperenhancement
Hypoenhancing Non enhancing

HCC-Typical pattern. AP image -at 26 secs showing hyperenhancement (arrow) (A)hypoenhancement (arrow) in the VP at 45 secs

HCC- Atypical pattern. AP image showing inhomogeneous hyperenhancement (arrow) at 30 secs (A) with retained contrast appearing isoenhancing (arrows) in the VP and LP at 110 and 240 secs respectively (B and C). Histopathology suggested well differentiated HCC

Hepatic metastasis from colon cancer- arterial phase showing marked rimenhancement . in late phases shows hypoenhancecement.

Applications in Pancreatic Imaging Detection of Focal Pancreatic Lesions If the lesion is less than 2 cms-CEUS is superior to US alone, comparable efficacy with that of EUS,more diagnostic accuracy than CT Four patterns of enhancement of focal pancreatic lesions are seen- no enhancement-type Ivascularity less than adjacent pancreatic parenchyma-type IIvascularity equal to adjacent pancreatic parenchyma-type III more than the adjacent pancreatic parenchyma-type IV.
Pancreatic adenocarcinoma usually demonstrate type I and II patterns.Pancreatic neuroendocrine tumors can depict significant enhancement in the arterial phase of CEUS(type IV) even when it may not show significant increased vascularity on Doppler imaging
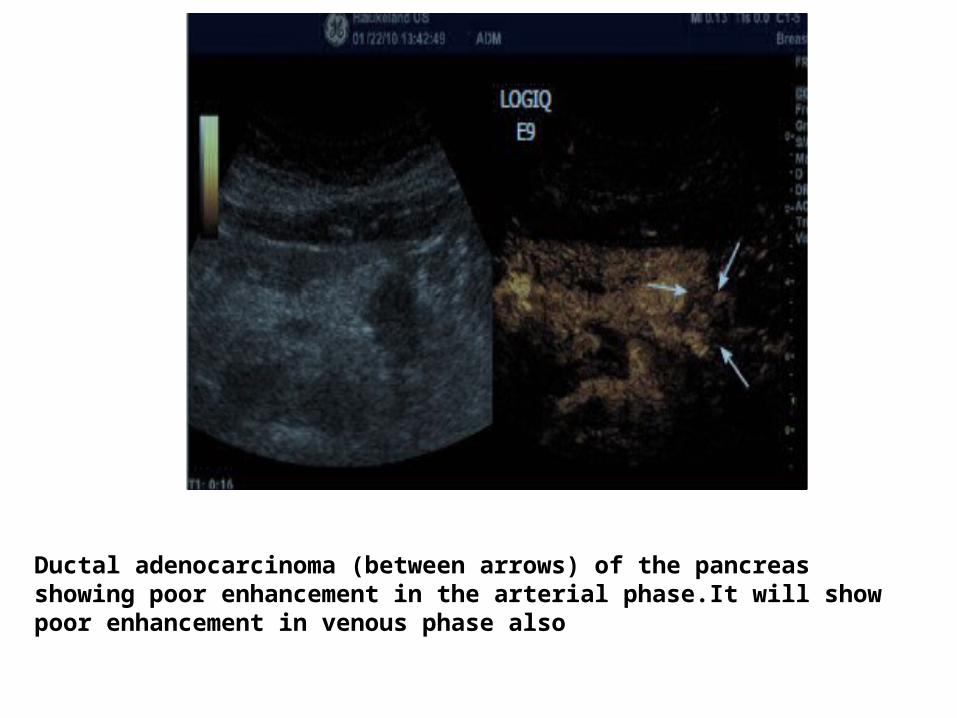
Ductal adenocarcinoma (between arrows) of the pancreasshowing poor enhancement in the arterial phase.It will show poor enhancement in venous phase also

Neuroendocrine tumour (arrow) shows a rapid intense enhancementin the early arterial phase of contrast-enhanced ultrasound examination
Differentiation of Cystic Pancreatic Tumors from Pancreatic Pseudocyst CEUS can differentiate a cystic pancreatic neoplasm from a pseudocyst by demonstrating the enhancement of septae, nodules and solid components in a tumor.On the contrary; pancreatic pseudocysts are devoid of any contrast enhancement, even though the internal contents may appear echogenic on US
Detection of Pancreatic Necrosis in Acute Pancreatitis
Applications in Renal Imaging Characterization of Renal Masses -Since CEUS is more sensitive to detection of blood flow than CECT, it can differentiate a solid mass lesion from a cystic one with greater accuracy. It also scores over CECT in characterization of complex cystic renal masses as it can detect the septa and solid components in Bosniak grade 2 to 4 cysts with better sensitivity than CECT.Differentiation of Renal Tumors from Pseudotumors- Enhancement of pseudotumors is similar to the normal renal parenchyma on all phases of enhancement.Enhancement pattern of solid renal tumors differs from that of the normal renal parenchyma in at least one phase of enhancement.

Renal Vascular Lesions-Differentiate renal infarcts from ischemic areas- The infarcted area shows no enhancement whereas hypoperfused area retains its blood flow, although reducedDifferentiate renal infarct from cortical necrosis- shows preserved hilar vascularity in contrast to infarct.
Application in Abdominal Trauma CEUS can detect intra-abdominal solid organ injuries (including liver, splenic, renal lesions) with higher sensitivity and specificity than US
A contusion is seen as a hypoechoic area within the enhancing parenchyma with ill defined borders
A laceration is a more well defined linear non-enhancing area
In hypovolemic shock all the abdominal solid organs show reduced enhancement

US-B-mode (b) and CEUS (c) in a 40 year- male patient with blunt abdominaltrauma.parenchymal lacerative area not recognizable by US B-Mode examinationCEUS demonstrate splenic hypoechoic lesion

US-B-mode (b) and CEUS (c) in a patient with blunt abdominaltrauma. intra-parenchymal traumatic area in liver (a) not recocognizable by US B-Mode examination (b)CEUS demonstrate hepatic hypoechoic lesion.

Applications in Breast Imaging Benign masses (like fibroadenoma) show smooth vessels at the periphery and less avid enhancement
whereas the malignant masses appear spiculated have more tortuous vessels with irregular course, and have inter-vascular shunts
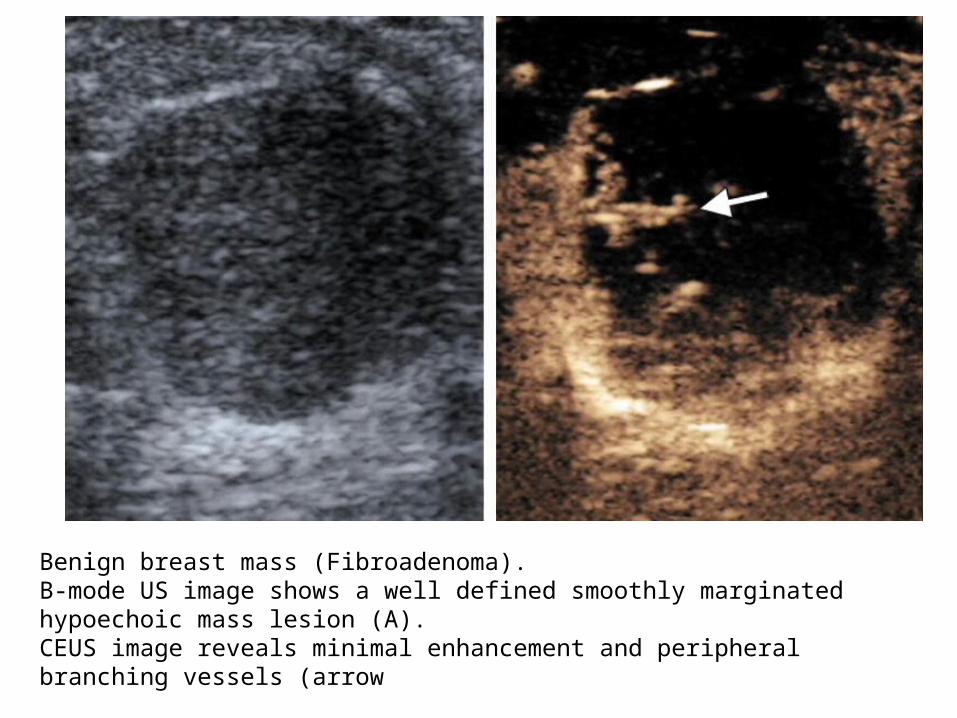
Benign breast mass (Fibroadenoma). B-mode US image shows a well defined smoothly marginated hypoechoic mass lesion (A). CEUS image reveals minimal enhancement and peripheral branching vessels (arrow
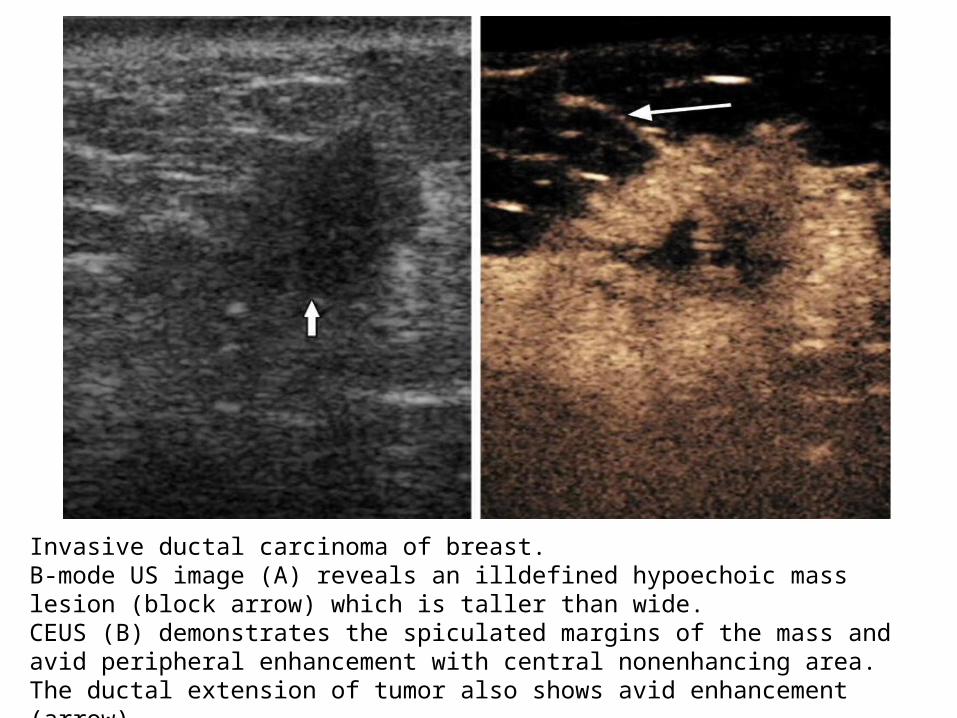
Invasive ductal carcinoma of breast.B-mode US image (A) reveals an illdefined hypoechoic mass lesion (block arrow) which is taller than wide.CEUS (B) demonstrates the spiculated margins of the mass and avid peripheral enhancement with central nonenhancing area. The ductal extension of tumor also shows avid enhancement (arrow)
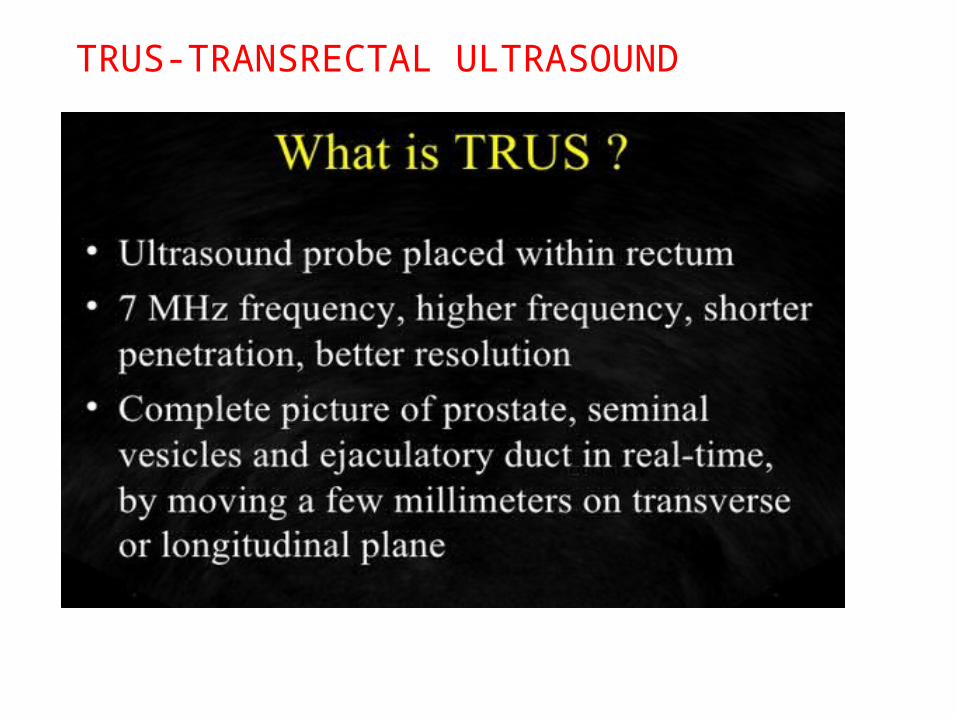
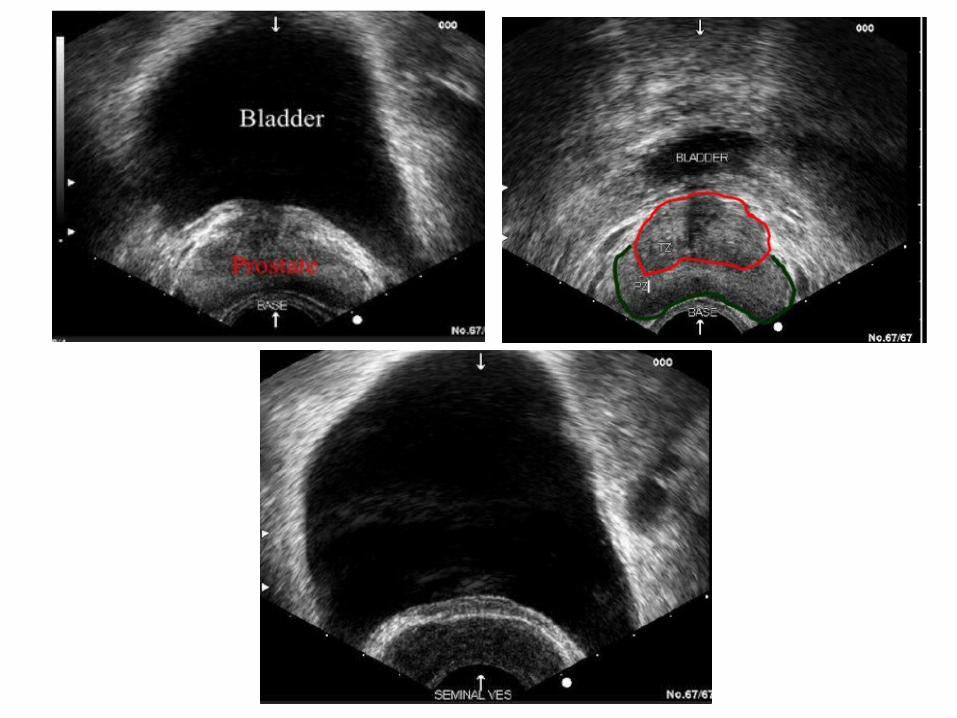
TRUS-TRANSRECTAL ULTRASOUND

TECHNIQUELeft lateral position
DRE
Introduce rectal ultrasound probe
No anaesthesia is required
Mild sedation is required if we have to do some drainage,aspiration or biopsy



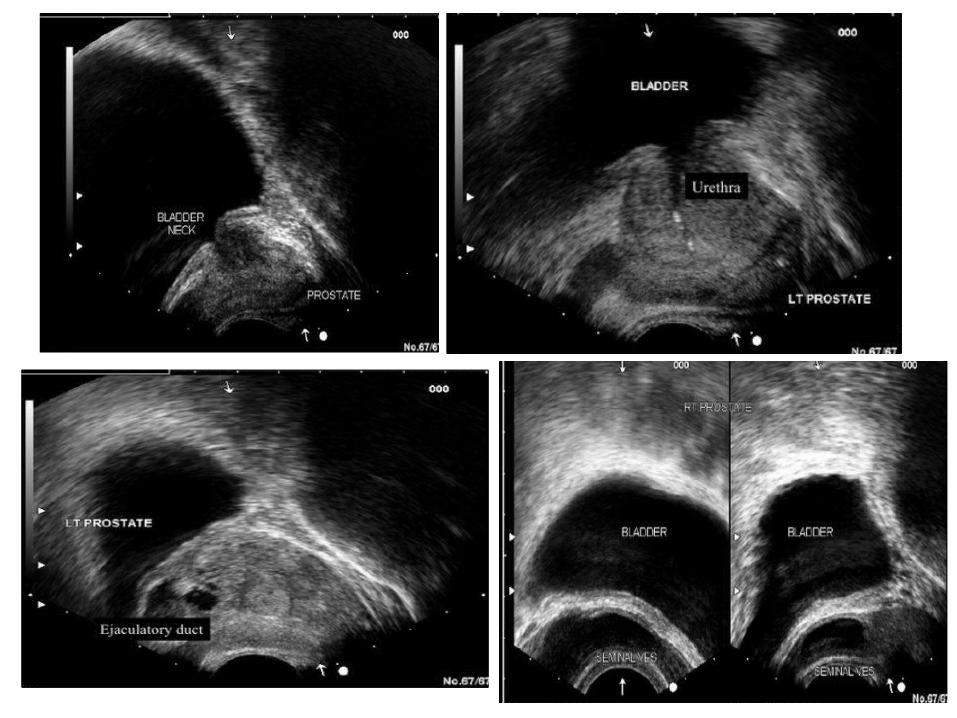
INDICATIONS OF TRUS1. Prostatic cancer- diagnosis, staging and TRUS
guided biopsy
2. Benign prostatic hyperplasia
3. Evaluation of male infertility-vas diference obstruction-dilated seminal vesicle>1.6cm in transverse plane
Dilated ejaculatory duct>2.5mm in transverse plane.

















