103
Advisor Live ® Antimicrobial stewardship – Why now and how? November 19, 2015 Download today’s slides at www.premierinc.com/events @PremierHA #AdvisorLive #GetSmartWeek
| Date post: | 13-Jan-2017 |
| Category: |
Healthcare |
| Upload: | premier-inc |
| View: | 73 times |
| Download: | 3 times |
Advisor Live®
Antimicrobial stewardship – Why now and how?
November 19, 2015
Download today’s slides at www.premierinc.com/events
@PremierHA
#AdvisorLive
#GetSmartWeek
2© 2015 PREMIER, INC.
Logistics

3© 2015 PREMIER, INC.
Faculty
MODERATOR
Gina Pugliese, RN, MS, FSHEAVice President
Premier Safety Institute®
CAPT Arjun Srinivasan, MDAssociate Director,
Healthcare associated infection
prevention programs, CDC
Michael Postelnick, RPh BCPS
AQ Infectious DiseasesSenior Infectious Diseases Pharmacist
Northwestern Memorial Hospital, Chicago
Craig Barrett PharmD,BCPSDirector, Safety Solutions, Premier Inc.
@PremierHA
#AdvisorLive
#GetSmartWeek

4© 2015 PREMIER, INC.
CAPT Arjun Srinivasan, MD,
Associate Director
Healthcare Associated Infection Prevention Programs
Division of Healthcare Quality Promotion, CDC
@PremierHA
#AdvisorLive
#GetSmartWeek

CAPT Arjun Srinivasan, MD
Associate Director for Healthcare Associated
Infection Prevention Programs
Division of Healthcare Quality Promotion
Improving Antibiotic Stewardship in Hospitals-Why Now?
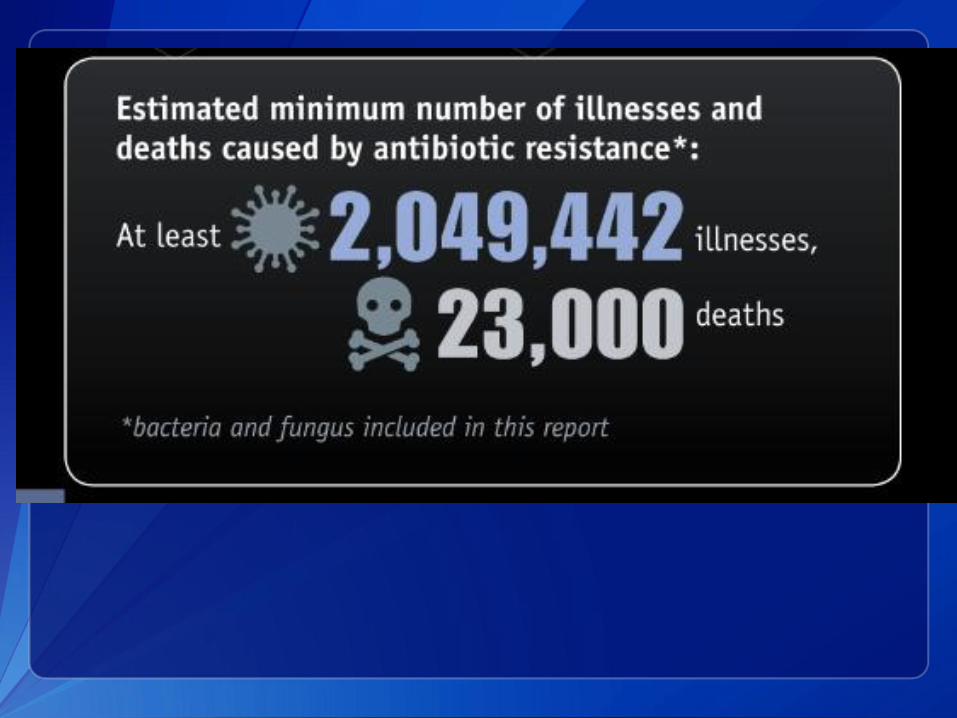
Why Antibiotic Stewardship?
• In hospitals, antibiotic stewardship programs
have been proven to:
– Improve antibiotic use
– Reduce antibiotic resistance
– Reduce complications of antibiotic use- especially
Clostridium difficile
– Improve patient outcomes
– Save money
•IDSA/SHEA Guidelines for Antimicrobial Stewardship Programs
http://www.journals.uchicago.edu/doi/pdf/10.1086/510393
77HAI Regional Training HAI Training Requirements is sponsored by SHEA and the CDC
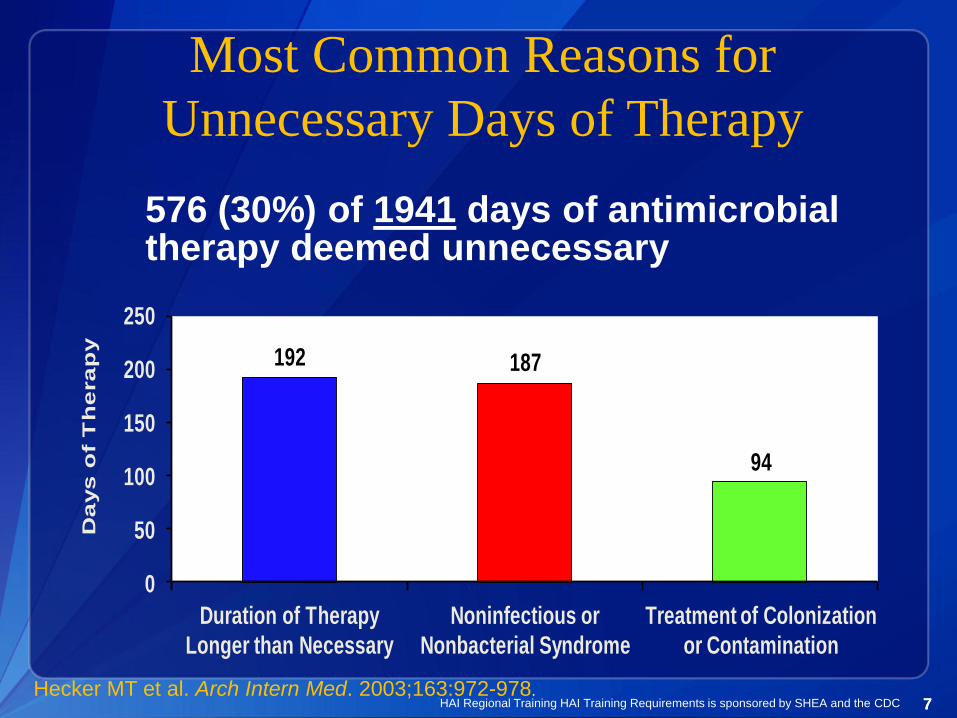
Most Common Reasons for
Unnecessary Days of Therapy
192 187
94
0
50
100
150
200
250
Duration of Therapy
Longer than Necessary
Noninfectious or
Nonbacterial Syndrome
Treatment of Colonization
or Contamination
Da
ys
of
Th
era
py
576 (30%) of 1941 days of antimicrobial therapy deemed unnecessary
Hecker MT et al. Arch Intern Med. 2003;163:972-978.

Susceptibility Profile of KPC-Producing K.
pneumoniaeAntimicrobial Interpretation Antimicrobial Interpretation
Amikacin I Chloramphenicol R
Amox/clav R Ciprofloxacin R
Ampicillin R Ertapenem R
Aztreonam R Gentamicin R
Cefazolin R Imipenem R
Cefpodoxime R Meropenem R
Cefotaxime R Pipercillin/Tazo R
Cetotetan R Tobramycin R
Cefoxitin R Trimeth/Sulfa R
Ceftazidime R Polymyxin B MIC >4mg/ml
Ceftriaxone R Colistin MIC >4mg/ml
Cefepime R Tigecycline R
C. difficile• Data from population-based surveillance in
2011.
• ~453,000 total annual C. difficile infections.
• ~15,000 attributable deaths
– 80% of deaths in patients >65 years old
– 66% of cases were healthcare associated.
– About $1 billion in excess healthcare costs and re-
admissions
• C difficile infections are now part of the
inpatient quality reporting program• N Engl J Med 2015; 372:825-834
Antibiotic Stewardship to Combat
C. difficile
• 2014 meta-analysis on the impact of stewardship
on C. difficile included 16 studies.
• Stewardship programs were significantly
protective against C. difficile
– Pooled risk ratio 0.48; 95% CI: 0.38, 0.62
• Restrictive interventions were most effective.
• Protection especially strong in geriatric settings.
Feazel LM et al. J Antimicrob Chemother, March 2014
1212
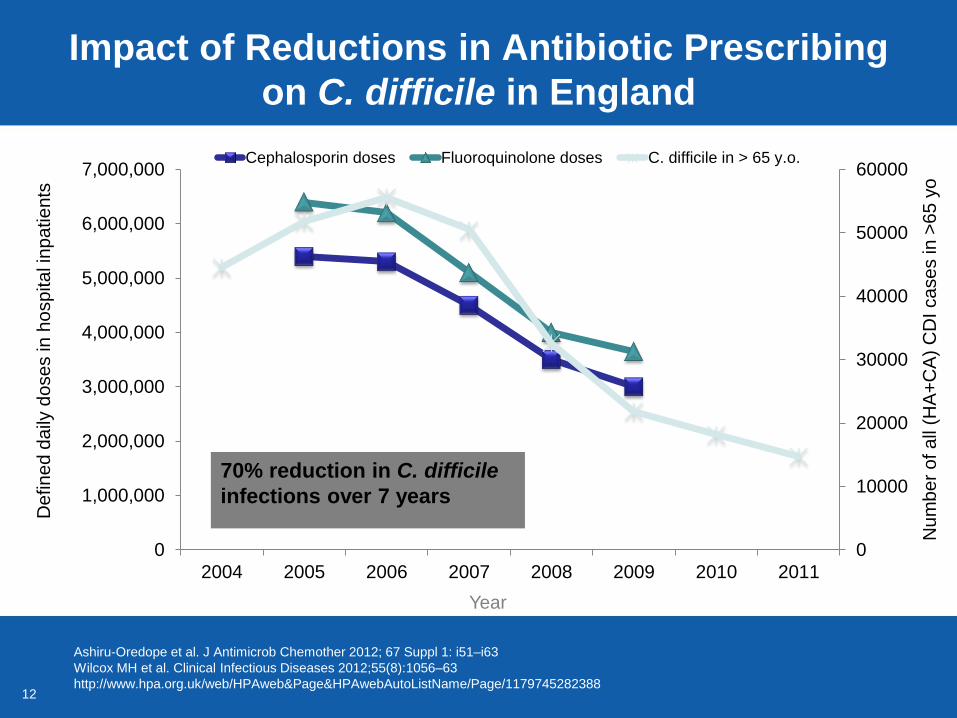
Impact of Reductions in Antibiotic Prescribing
on C. difficile in England
0
10000
20000
30000
40000
50000
60000
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
2004 2005 2006 2007 2008 2009 2010 2011
Cephalosporin doses Fluoroquinolone doses C. difficile in > 65 y.o.
70% reduction in C. difficile
infections over 7 years
Year
De
fin
ed
da
ily d
ose
s in
ho
sp
ita
l in
pa
tie
nts
Num
ber
of all
(HA
+C
A)
CD
I cases in >
65 y
o
Ashiru-Oredope et al. J Antimicrob Chemother 2012; 67 Suppl 1: i51–i63
Wilcox MH et al. Clinical Infectious Diseases 2012;55(8):1056–63
http://www.hpa.org.uk/web/HPAweb&Page&HPAwebAutoListName/Page/1179745282388
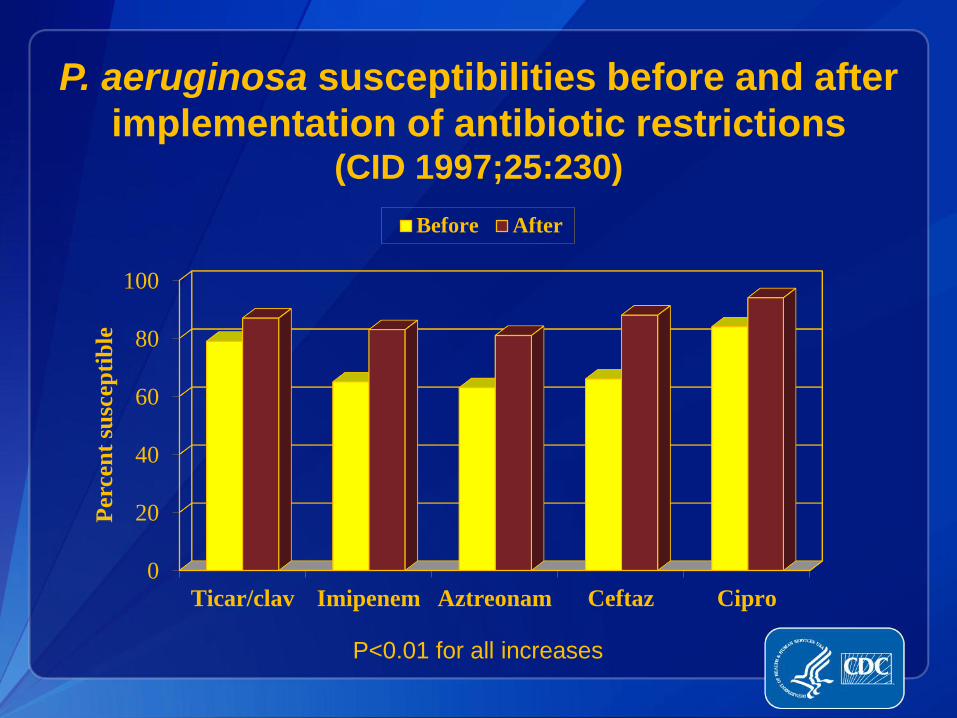
P. aeruginosa susceptibilities before and after
implementation of antibiotic restrictions (CID 1997;25:230)
0
20
40
60
80
100
Ticar/clav Imipenem Aztreonam Ceftaz Cipro
Perc
en
t su
scep
tib
le
Before After
P<0.01 for all increases

Clinical outcomes better with
antimicrobial stewardship program
0102030405060708090
100
Appropriate Cure Failure
AMP
UP
RR 2.8 (2.1-3.8) RR 1.7 (1.3-2.1) RR 0.2 (0.1-0.4)
Perc
en
t
AMP = Antibiotic Management Program
UP = Usual PracticeFishman N. Am J Med. 2006;119:S53.
15© 2015 PREMIER, INC.
Michael Postelnick, RPh BCPS AQ Infectious Diseases
Senior Infectious Diseases Pharmacist
Northwestern Memorial Hospital
Chicago, IL
@PremierHA
#AdvisorLive
#GetSmartWeek

Michael Postelnick, RPh BCPS AQ Infectious DiseasesSenior Infectious Diseases PharmacistNorthwestern Memorial HospitalChicago, IL
Measuring the Impact of Antimicrobial Stewardship Interventions on Antimicrobial Resistance

Source: Penicillin finder assays its future. New York Times. 26 June 1945: 21
Call to Antimicrobial Stewardship
“….the microbes are educated to resist penicillin and a host of penicillin-fast organisms is bred out…… In such cases the thoughtless person playing with penicillin is morally responsible for the death of the man who finally succumbs to infection with the penicillin-resistant organism.”
- Sir Alexander Fleming, June 26, 1945
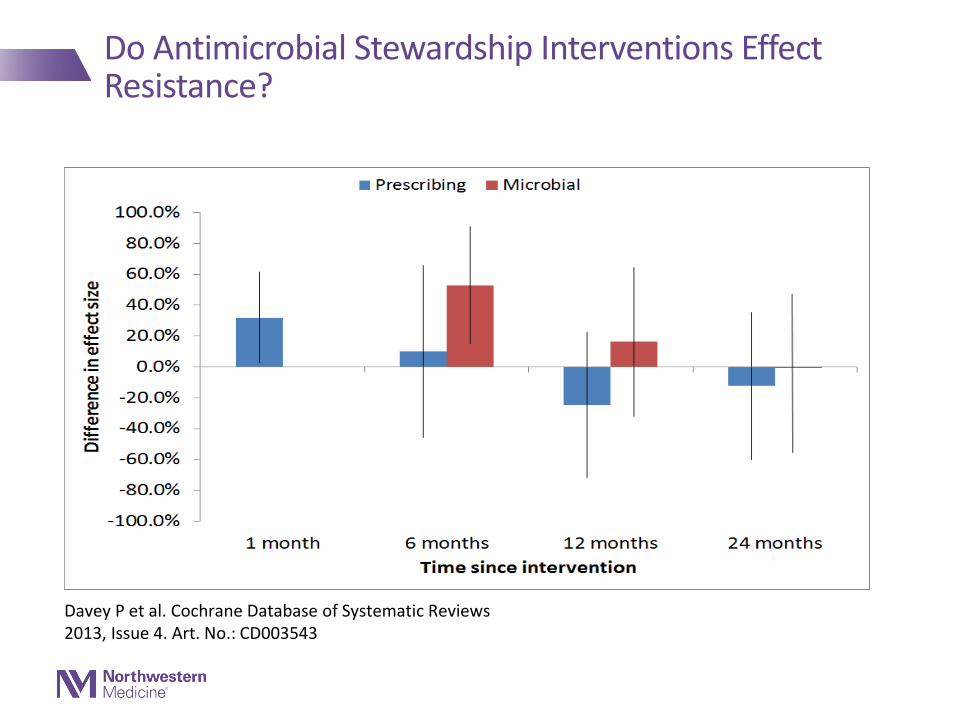
Davey P et al. Cochrane Database of Systematic Reviews 2013, Issue 4. Art. No.: CD003543
Do Antimicrobial Stewardship Interventions Effect Resistance?
Presentation Overview
•Measuring Antimicrobial Use
•Measuring Antimicrobial Resistance
•Overview of Antimicrobial Stewardship at Northwestern Memorial Hospital
•Representative Stewardship Initiatives
•Current Stewardship Focus at NMH
•Future Directions
Measuring Antimicrobial UseIt is widely believed that you cannot manage what you cannot measure. It is also true that you cannot measure what you cannot define 1
1. Ibrahim OM and Polk RE. Infect Dis Clin N Am 28; 2014: 195-214

Measuring Antimicrobial Use
Measure Calculation Advantages Disadvantages Use?
DOT/1000 PD DOT/(PD/1000) More accurate than DDD
Requires pt. level data
Becoming standardmetric
DOT/1000 admissions
DOT/(admissions/1000)
Not a function of LOS
Requires riskadjustment (RA)
Secondary measure
DDD/1000 PD http://www.whocc.no/ddd/definition_and_general_considera/
Easily calculated, does not require pt level data
Less accurate and consistent
Comparison across countries
LOT/discharge Total LOT/discharge Provides average duration of tx
Not normalized forLOS, needs RA
Identify excessive tx durations
DOT/LOT ratio DOT/LOT Measures agg-regate combo tx
Pt level data needed
Identify un-necessary combo
Proportion receiving abx
Treatedpts/admissions
Needs risk adjustment
Identify unnecessary tx

Interpreting Antimicrobial Use Data
•Benchmarking•Use data must be risk adjusted
•Internal – ICU vs general care floor
•External – Academic medical center vs small rural hospital
•Identify Outliers
•Perform DUE to determine intervention strategies (if needed)
• Unnecessary therapy
• Prolonged durations
• Unusual resistance patterns
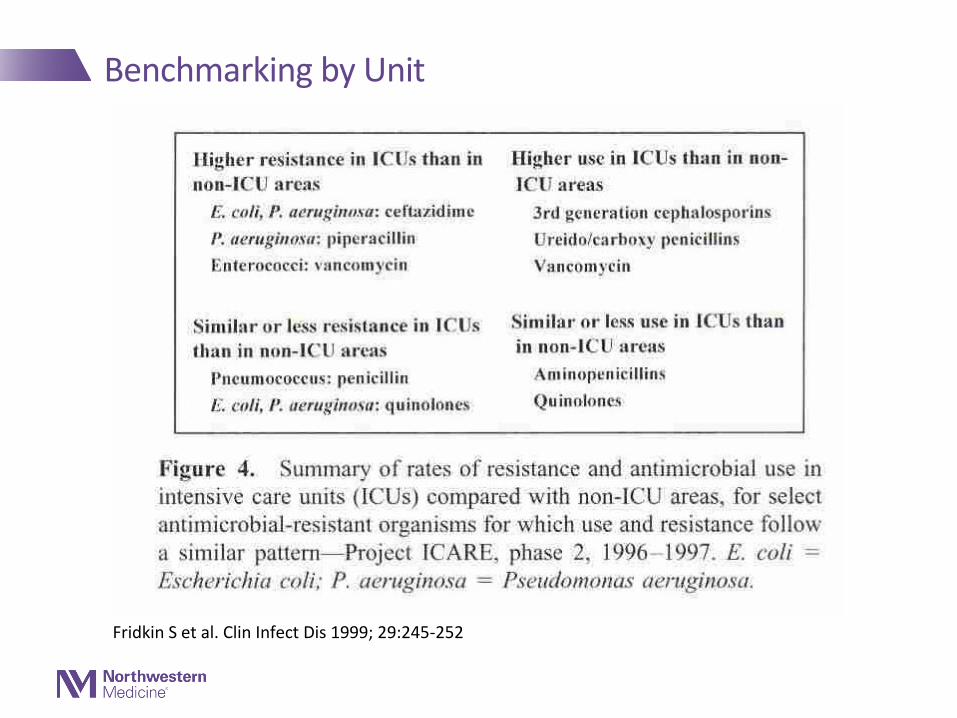
Benchmarking by Unit
Fridkin S et al. Clin Infect Dis 1999; 29:245-252
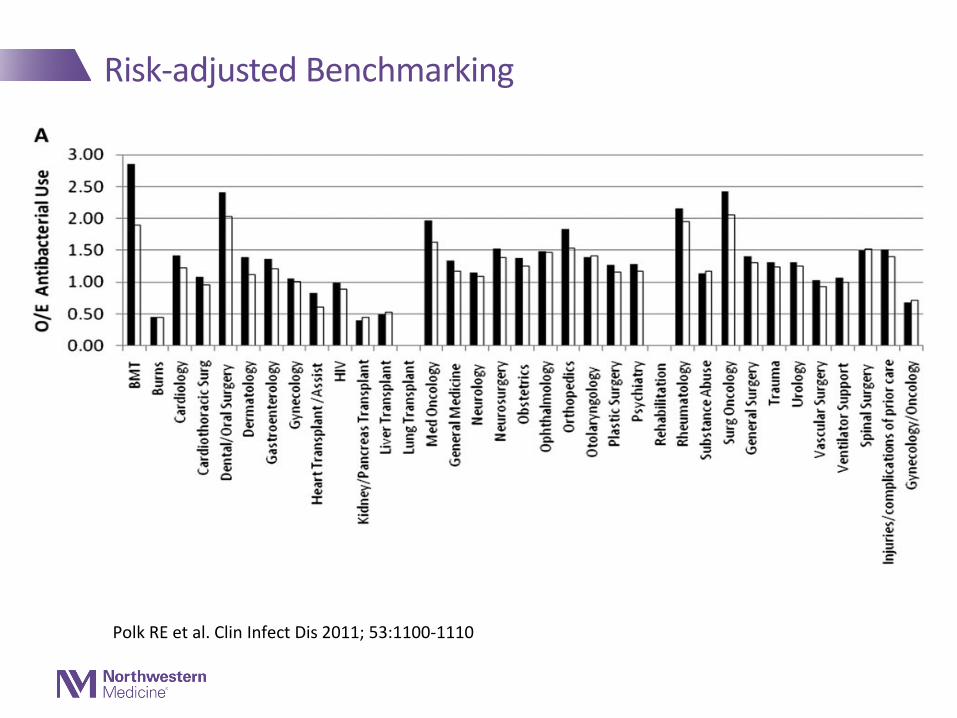
Risk-adjusted Benchmarking
Polk RE et al. Clin Infect Dis 2011; 53:1100-1110
Measuring Antimicrobial Resistance
The Hospital Antibiogram
•Most widely available measure of resistant organisms
•Measures proportion of susceptible organisms over time
•Designed for:•Assisting empiric antimicrobial selection
•Guidance on formulary choices
•CLSI sets guidance for construction
Schulz LT et al. Pharmacotherapy 2012;32(8):668–676

Antibiograms to Assess Stewardship Interventions
Schulz LT et al. Pharmacotherapy 2012;32(8):668–676
What Factors Effect the Ability to Demonstrate Interventional Impact on Resistance?
•Magnitude of Change•Time-series analysis to forecast resistance changes related to antibiotic use
•Ceftazidime/gram negative bacilli and imipenem/Pseudomonas examined
•Complex mathematical model designed for analysis
• Lag-time accounted for
•Impact of changes in antimicrobial use significant but small
• 6% of variation in Pseudomonas susceptibility predicted by imipenem use variation
Lopez-Lozano JM et al. International Journal of Antimicrobial Agents 14 (2000) 21–31

What Factors Effect the Ability to Demonstrate Interventional Impact on Resistance?
•Dynamics of Resistance are Complex•Bacterial resistance mechanisms effect multiple antibiotics
•Stewardship interventions local-resistance is global
•Unintended consequences (“squeezing the balloon”)
•Multiple simultaneous interventions
• Stewardship
• Infection Control
•Regression to the mean
Antimicrobial Stewardship at Northwestern Memorial Hospital
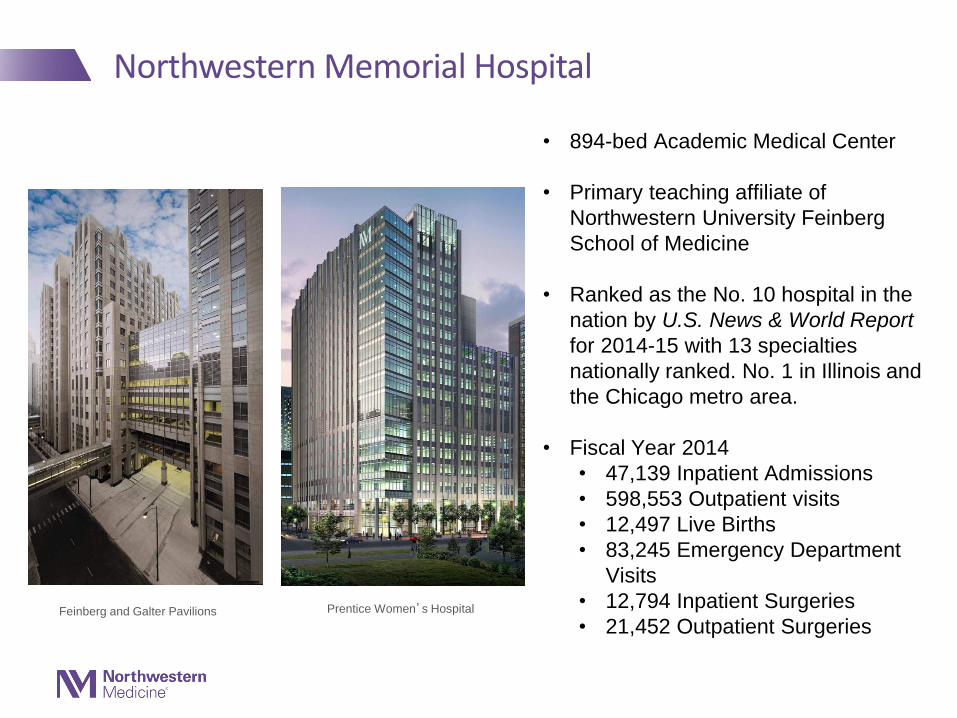
• 894-bed Academic Medical Center
• Primary teaching affiliate of
Northwestern University Feinberg
School of Medicine
• Ranked as the No. 10 hospital in the
nation by U.S. News & World Report
for 2014-15 with 13 specialties
nationally ranked. No. 1 in Illinois and
the Chicago metro area.
• Fiscal Year 2014
• 47,139 Inpatient Admissions
• 598,553 Outpatient visits
• 12,497 Live Births
• 83,245 Emergency Department
Visits
• 12,794 Inpatient Surgeries
• 21,452 Outpatient Surgeries
Northwestern Memorial Hospital
Feinberg and Galter Pavilions Prentice Women’s Hospital

Evolution of Antimicrobial Stewardship NMH 1987-2015
• 1987-1990: Implement Antimicrobial Formulary and Pharmacokinetic Dosing Service
• 1990-1993: Implement Empiric Antimicrobial Guidelines
• 1993-2002: Prospective audit and feedback
• 2002-2003: Initiate “Formal” Stewardship Program
• 2003: Implement Clinical Decision Support
• 2013: CDC-AUR participation

Current Stewardship Structure at NMH• Stewardship physician (0.5 FTE)
Daily TAM review and intervention
Design and support educational initiatives
Provide MD support for all stewardship activities
• Stewardship pharmacists (5 co-funded faculty, approximately 1.4 FTE)
Daily restricted antimicrobial review
72 hour review
MALDI-TOF intervention
Support clinical pharmacist stewardship activities
• Unit-based Clinical Pharmacist
Antimicrobial dosing
IV to PO recommendations
Guideline-based recommendations
72 hour review
Antimicrobial de-escalation

What Have We Accomplished
•Continued control of antimicrobial costs•2014 cost savings = $120,000
•Empiric Antimicrobial Use Guidelines and Incorporation into Order Sets•Optimized Dosing of Antimicrobials
•Comprehensive dosing protocols
•Prolonged infusion protocols for beta-lactams•Leveraging Clinical Decision Support for Bug-drug Mismatches and Restricted Antimicrobials•Expansion of Training Programs for Infectious Diseases Pharmacists

Where Have We Struggled
•Measurement of Impact on Utilization and Resistance•Systematic metrics
•Benchmarking
•Antimicrobial Stewardship Outcomes Research

Representative Stewardship Interventions

Order Sets

Antimicrobial Indications

TAM Alerts
• Identify patients with susceptibility results without active antimicrobial therapy
• Evaluated daily by stewardship physician
• Small minority require clinical intervention
• An average of 4 “critical interventions” identified monthly
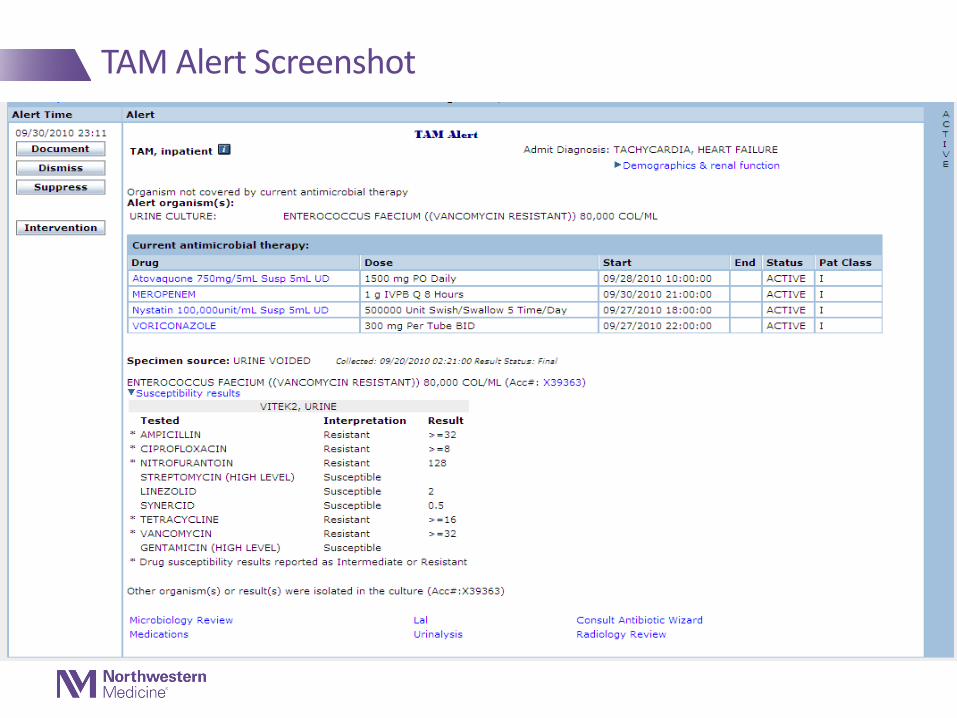
TAM Alert Screenshot
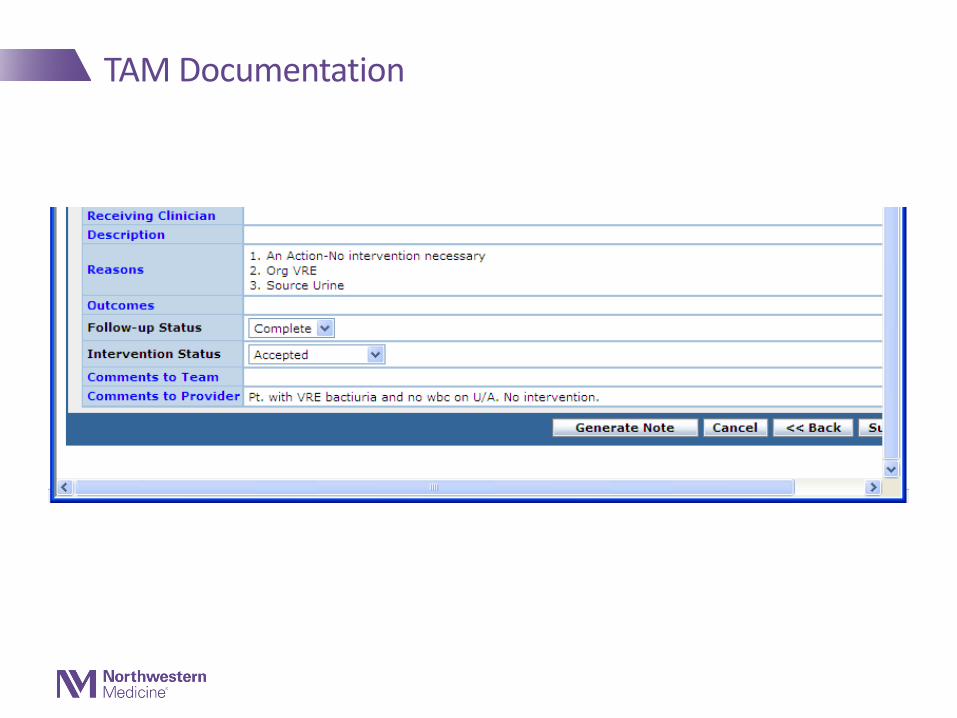
TAM Documentation

TAM Alerts by Disposition
142
251
165154
122
32
56 56
2819
9 1121
13 8
0
50
100
150
200
250
300
MAR-MAY 09 JUN-AUG 09 SEPT-NOV 09 DEC 09-FEB 10 MAR-MAY 10
Total
No Intervention
Overtreatment
Undertreatment
Critical Alerts

Examples of Critical Alert Interventions
• Patient with methicillin-resistant S. aureus (MRSA) frombursa fluid On clindamycin (isolate R)
ASP notified hospitalist
Patient was discharged with seven days of PO linezolid
• Patient with growth of P. aeruginosa from cerebrospinal fluid in a patient with lumbar drain History of spine surgery with pseudomeningocele formation + CSF
leak
ASP notified neurosurgery
Infectious disease consulted, ceftazidime initiated

Restricted Antimicrobial Alerts
• Reviewed daily by stewardship pharmacist
• Evaluated against P&T approved criteria
• Interventions coordinated with unit-based clinical pharmacist
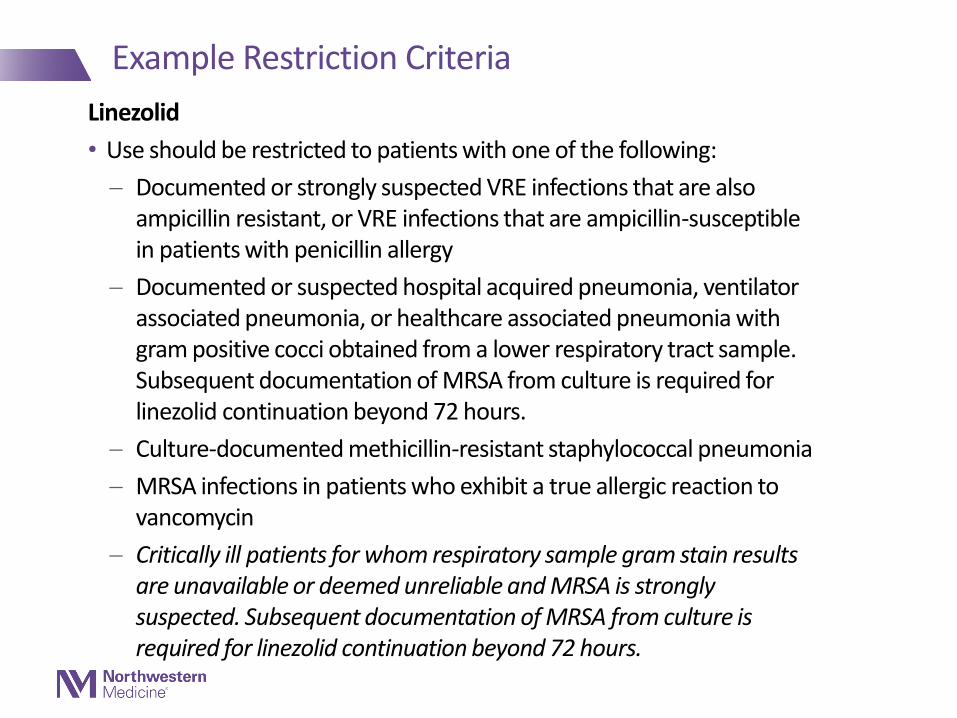
Example Restriction Criteria
Linezolid
• Use should be restricted to patients with one of the following:
Documented or strongly suspected VRE infections that are also ampicillin resistant, or VRE infections that are ampicillin-susceptible in patients with penicillin allergy
Documented or suspected hospital acquired pneumonia, ventilator associated pneumonia, or healthcare associated pneumonia with gram positive cocci obtained from a lower respiratory tract sample. Subsequent documentation of MRSA from culture is required for linezolid continuation beyond 72 hours.
Culture-documented methicillin-resistant staphylococcal pneumonia
MRSA infections in patients who exhibit a true allergic reaction to vancomycin
Critically ill patients for whom respiratory sample gram stain results are unavailable or deemed unreliable and MRSA is strongly suspected. Subsequent documentation of MRSA from culture is required for linezolid continuation beyond 72 hours.

Restricted Alert Screenshot
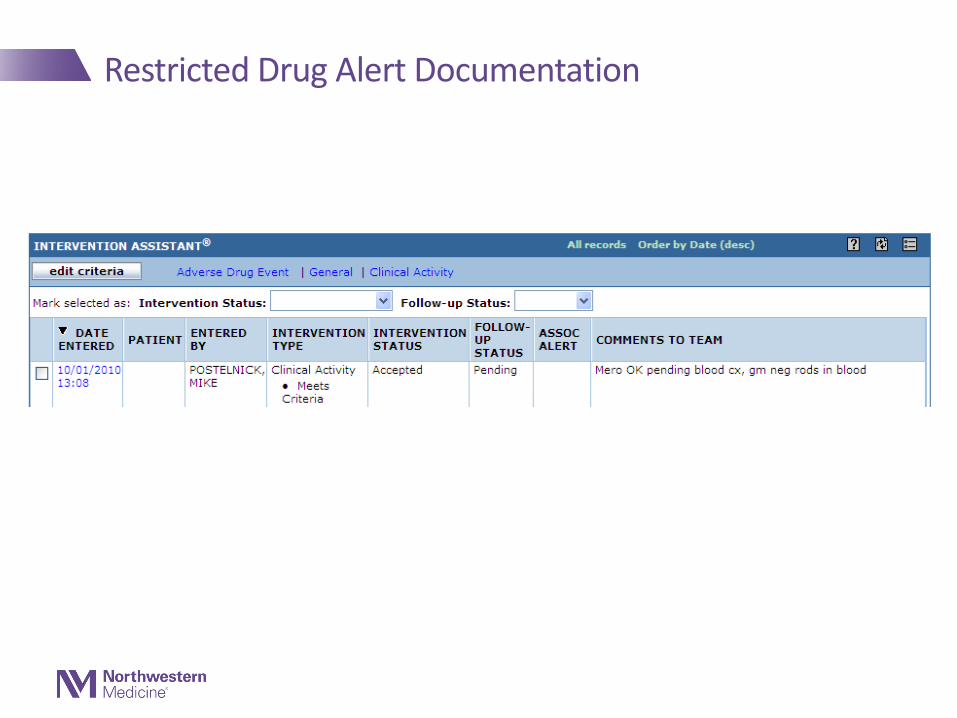
Restricted Drug Alert Documentation
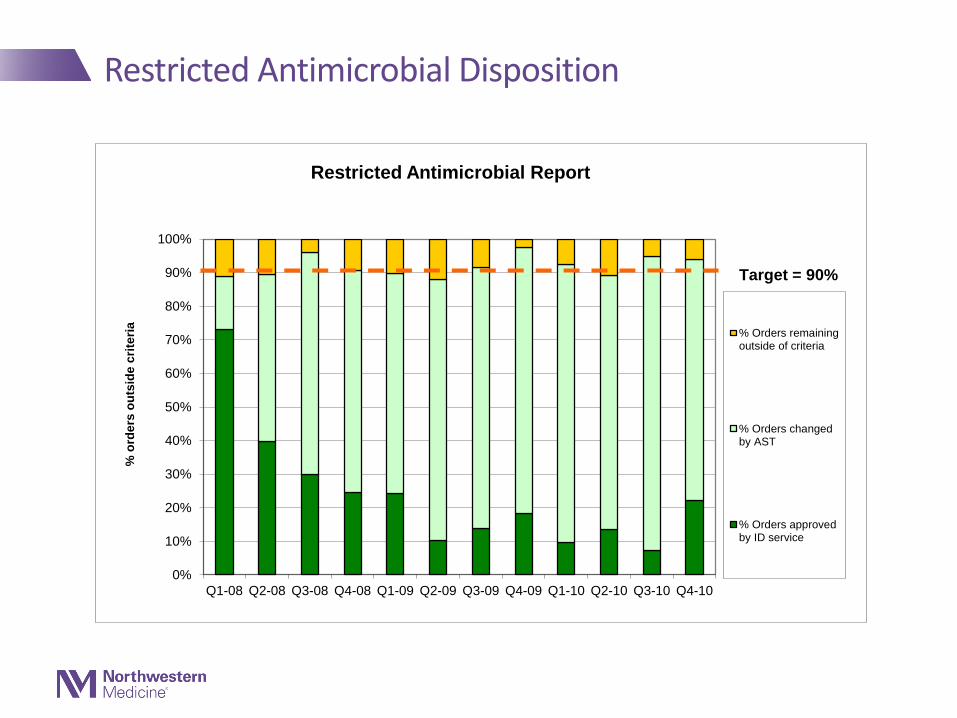
Restricted Antimicrobial Disposition
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Q1-08 Q2-08 Q3-08 Q4-08 Q1-09 Q2-09 Q3-09 Q4-09 Q1-10 Q2-10 Q3-10 Q4-10
% o
rde
rs o
uts
ide
cri
teri
a
Restricted Antimicrobial Report
% Orders remainingoutside of criteria
% Orders changedby AST
% Orders approvedby ID service
Target = 90%
Custom Alert Capability
•User generated
•Flexible
•Focused
•Simple for end user to design
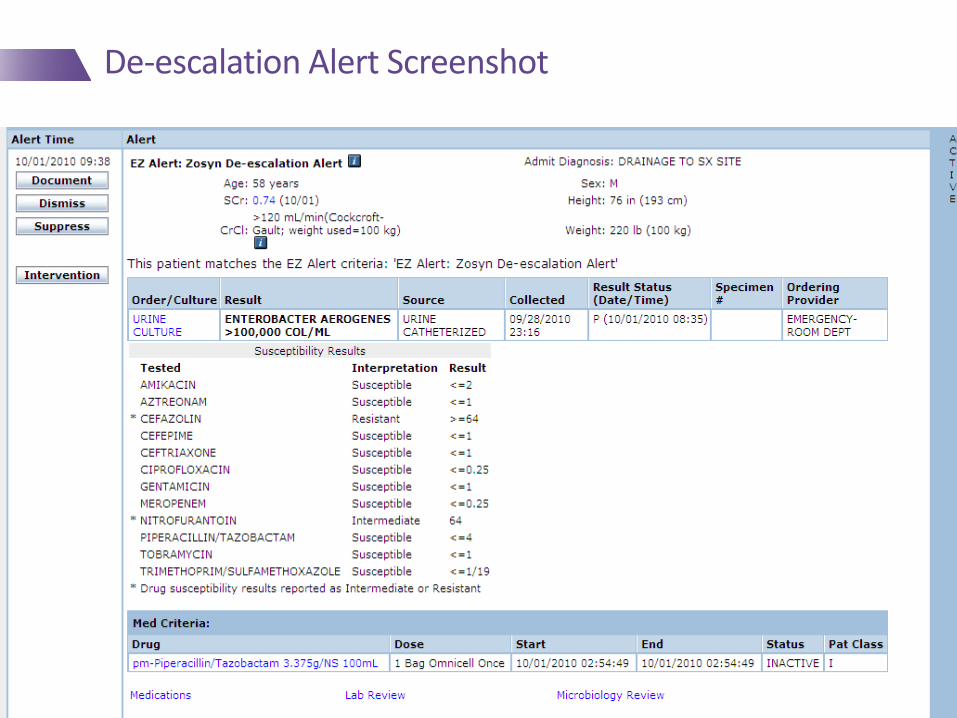
De-escalation Alert Screenshot

De-escalation Documentation
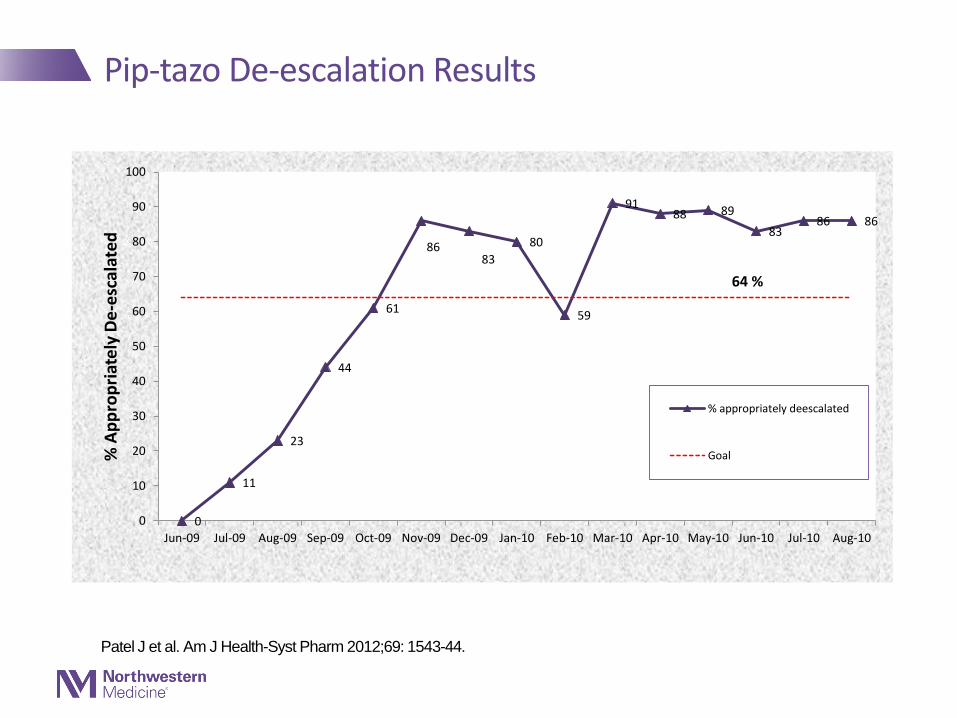
Pip-tazo De-escalation Results
0
11
23
44
61
8683
80
59
9188 89
8386 86
64 %
0
10
20
30
40
50
60
70
80
90
100
Jun-09 Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10 Aug-10
% A
pp
rop
riat
ely
De
-esc
alat
ed
% appropriately deescalated
Goal
Patel J et al. Am J Health-Syst Pharm 2012;69: 1543-44.


Ciprofloxacin MIC Alert
System Generated Antibiograms
• Simple, rapid generation
• Allows for unit and site specific evaluations
• Enhances ability to customize local guidelines
• Increases probability of active initial empiric therapy
• Can help minimize overly broad empiric treatment

Hospital-wide Antibiogram

Unit-specific AntibiogramMICU 2014 Gram negative rods
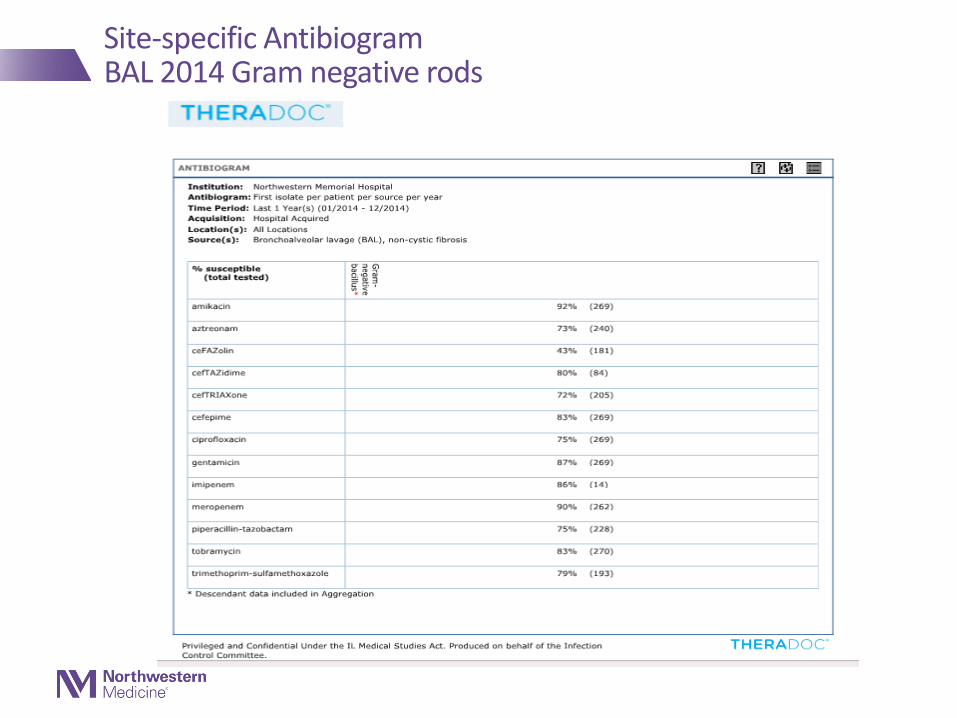
Site-specific AntibiogramBAL 2014 Gram negative rods
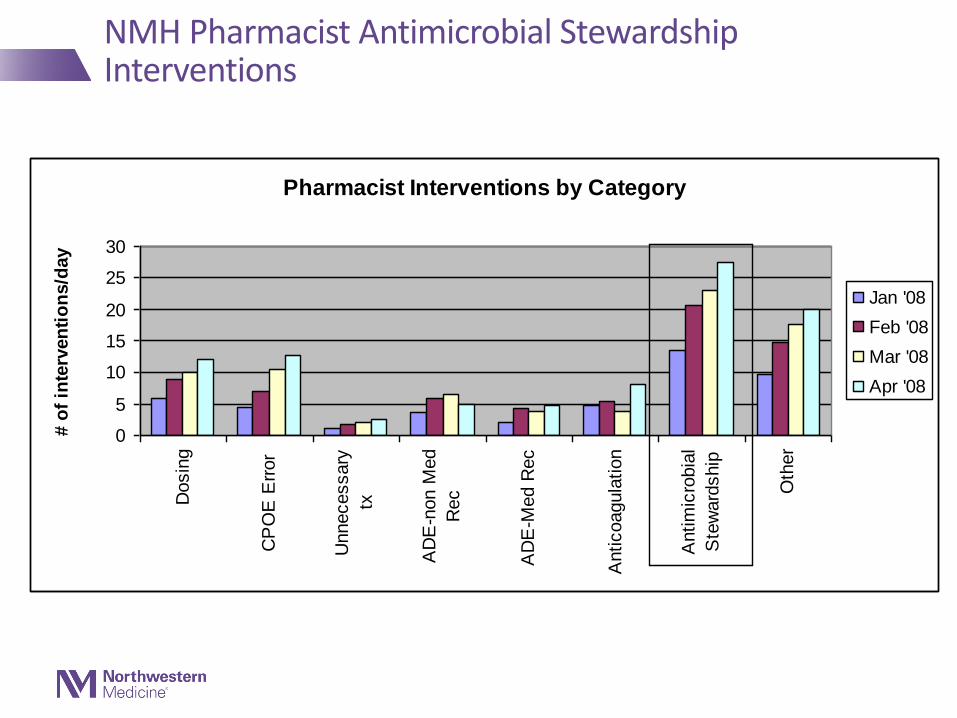
Pharmacist Interventions by Category
0
5
10
15
20
25
30
Dosin
g
CP
OE
Err
or
Unnecessary
tx
AD
E-n
on M
ed
Rec
AD
E-M
ed R
ec
Anticoagula
tion
Antim
icro
bia
l
Ste
ward
ship
Oth
er
# o
f in
terv
en
tio
ns/d
ay
Jan '08
Feb '08
Mar '08
Apr '08
NMH Pharmacist Antimicrobial Stewardship Interventions
Current Stewardship Focus

Clostridium difficile Reduction Initiative
• Hospital C. diff rates are a publicly reported metric
• Partnership with Infection Prevention
• Initiative components:
Education to ensure appropriate testing
Continued strong infection prevention efforts
10% reduction in overall antibiotic use
Patient and family outreach
10% Reduction Interventions and Metric
• Interventions
72 hour structured antibiotic timeout• EMR-triggered review of antibiotics at 72 hours
Mandated end to prolonged post-operative surgical drain prophylaxis
End treatment of asymptomatic bacteriuria
Rapid Diagnostics• Stewardship-driven implementation of MALDI-TOF on blood and respiratory
samples
• Metric
CDC AU DOT data for identified antibiotics

Future Directions

Leveraging the EMR
• Switching from Cerner to Epic offers opportunities
Better use of clinical pathways and order sets
Better use of Point of Ordering Clinical Decision Support• Structured Antibiotic Timeout
New EMR System provides opportunities to change practice habits
• Switching from Cerner to Epic offers risks
Adequate resources
Time and energy devoted to switch can sap momentum from initiatives
Benchmarking
• CDC AUR program provides opportunities for risk adjusted benchmarking
Potential to identify areas to focus improvements
AUR may better define association of use and development of resistance
• Improved TheraDoc Reporting Tools
May provide for closer monitoring and local benchmarking
May provide the ability to focus interventions

Conclusions
• Identifying and reporting relevant metrics to demonstrate the impact of a stewardship program are often challenging
• The EMR and Clinical Decision Support Software such as TheraDoc can be leveraged to facilitate meaningful stewardship interventions
• Progress is being made in developing useful and potentially meaningful stewardship benchmarking methods
• The expanded threats posed by antimicrobial resistance has made antimicrobial stewardship more recognized and important than ever

67© 2015 PREMIER, INC.
CAPT Arjun Srinivasan, MD,
Associate Director
Healthcare Associated Infection Prevention Programs
Division of Healthcare Quality Promotion, CDC
@PremierHA
#AdvisorLive
#GetSmartWeek
CAPT Arjun Srinivasan, MD
The National Perspective on Antibiotic Stewardship
Implementing Antibiotic Stewardship
Hospitals don’t all look the same, and neither
do stewardship programs.
There must be flexibility in how programs are
implemented.
But, there are certain key elements that have
been strongly associated with success.
Core Elements for Antibiotic Stewardship Programs
Leadership commitment from administration
Single leader responsible for outcomes
Single pharmacy leader
Antibiotic use tracking
Regular reporting on antibiotic use and
resistance
Educating providers on use and resistance
Specific improvement interventionshttp://www.cdc.gov/getsmart/healthcare/implementation/core-
elements.html
Where We Are Now: NHSN Annual Facility
Survey of ~4000 US Hospitals
In 2014, 39.2% of US hospitals reported having
a stewardship program that meets all 7 CDC
core elements for hospital stewardship programs.
Factors associated with meeting all Core
Elements
Larger bed size
Teaching status
Leadership support (written > salary)
Preliminary findings from NHSN 2015 Annual Facility Survey - Not for distribution
Key Next Steps on Implementing
Stewardship Programs• CDC is working with many organizations
through the National Quality Partnership to
develop a “playbook” to provide more specific
suggestions on implementing stewardship
programs.
• Working to connect with smaller hospitals that
have implemented all of the core elements to
get key lessons learned.

National Healthcare Safety Network Antibiotic Use Option
Captures electronic data on antibiotics
administered, along with
admission/discharge/transfer data.
Calculates rates of administration for use:
By facilities to monitor interventions on single
units or facility wide
To collect aggregate information on antibiotic use
at a regional and national level
Eventually, to create antibiotic use benchmarks.
Standardized Antibiotic Administration Ratio (SAAR)
CDC’s 1st attempt at developing a
benchmarking measure for antibiotic use.
Similar in principle to the Standardized
Infection Ration (SIR).
SAAR expresses observed antibiotic use
compared to predicted use.
CDC worked with many partners to develop
the SAAR measure to try and make it most
useful for stewardship.
Standardized Antibiotic Administration Ratio (SAAR)
Experts in stewardship suggested that a variety
of different SAARs would be useful.
SAARs for a variety of different patient
populations.
SAARs for a variety of different groups of
antibiotics.
An Update on the Antibiotic Use Option of NHSN
The Standardized Antibiotic Administration
Ratio was approved for endorsement by the
Patient Safety Committee of the National
Quality Forum in June.
Requested approval was for public health
surveillance and quality improvement only.
A final vote is expected later 2015 or early
2016.
Key Points About the SAAR
The SAAR is risk adjusted based only on
facility characteristics (e.g. presence of ICUs,
hospital size).
The SAAR only helps directs stewardship
efforts to locations and antibiotics where use
appears to deviate from expected.
High use might be perfectly justified, low use
might be harming patients.
Measuring Appropriate Use
We all agree that the ultimate goal of
stewardship is to improve appropriate use of
antibiotics.
It will be hard to measure progress towards
that goal if we don’t have measures of
appropriate use.
CDC is collaborating with partners to try and
help with ways to assess this.

Assessing Appropriate Use
CDC collaborated with partners to create
assessment tools for appropriate use that
hospitals can use for quality improvement.
Available on Get Smart for Healthcare website.
The 2015-15 national antibiotic use point
prevalence survey will include an assessment
of appropriate use for 2 agents (vancomycin
and quinolones) and 2 conditions (community
acquired pneumonia and urinary tract
infections)

Antibiotic Use in US Hospitals-
Key Areas for Attention• In a 2011 survey in ~180 hospitals, CDC and
state collaborators reviewed charts of patients
who got antibiotics to determine the reason for
use, the top three were:
– Lower respiratory tract infections: 34.6%
– Urinary tract infections: 22.3%
– Skin and soft tissue infections: 15.4%
• These 3 infections accounted for more than
half of all in-patient antibiotic use.
JAMA. 2014;312(14):1438-1446

Stewardship in CAP
• Prospective intervention for patients being
treated for CAP.
• Treatment duration reduced from 10 d to 7 d
(p<0.001) with 148 fewer antibiotic days.
• Antibiotics more frequently narrowed based on
culture results (67% v. 19%).
• Fewer patients got duplicate therapy (10% vs
45%).
CID 2012;54:1581-7
“Kicking CAUTI”
• Quality improvement effort in two VA
hospitals in Texas.
• Developed a simple algorithm to improve
sending of urine cultures.
– Defined specific criteria when urine cultures were
indicated.
• Monitored impact on urine cultures and
treatment of UTI in intervention and control
hospitals.
JAMA Intern Med. 2015 Jul;175(7):1120-7.

“Kicking CAUTI”
• Rate of urine culture ordering in interventions
hospitals decreased during the intervention
period:
– From 41.2 to 23.3 per 1000 bed-days; (incidence
rate ratio [IRR], 0.57; 95% CI, 0.53-0.61)
– To 12.0 per 1000 bed-days; (IRR, 0.29; 95% CI,
0.26-0.32) during the maintenance period
– P < .001 for both.
• No change in control hospitals
Skin and Soft Tissue Infections
• Have become common reasons for admission
for antibiotics.
• Are overwhelmingly caused by gram positive
pathogens.
• Despite this, patients are often treated with
agents active against gram negatives and
anaerobes.
Improving Treatment of Skin and
Soft Tissue Infections (SSTI)• Facility implemented a SSTI diagnosis and
treatment guideline.
• Intervention resulted in:
– 3 day reduction in antibiotic treatment (13 v 10d)
– Less use of agents with gram negative and
anaerobic activity
– Better use of diagnostic studies and consults
Jenkins TC Arch Intern Med 2011;171(12):1072-
1079.

Regulatory Requirements?
• Presidential advisors have called for CMS to
make antibiotic stewardship a requirement in
acute and long term care facilities through the
Conditions of Participation.
• CMS has already proposed such a requirement
in long term care.
• They have indicated that they are considering
this for acute care as well.
Accreditation Standards
• The Joint Commission has developed a draft
standard on antimicrobial stewardship that has
been reviewed by several stakeholders and was
recently approved by the Standards and Survey
Procedures Committee.
– It will now go for broader review before being
finalized.
• The standard aligns with and draws from the
CDC core elements.
Conclusion
• This is a critical time for our efforts to
implement antibiotic stewardship programs to
improve antibiotic use.
• We need to continue to build on this
momentum.
• Please tell me what we can do (or do more of)
to support your important work.

89© 2015 PREMIER, INC.
Craig Barrett PharmD, BCPS
Director, Safety Solutions, Premier Inc.
Former roles: Pharmacy clinical specialist for surgery and director of
pharmacy residency program at Carolinas HealthCare in Charlotte
@PremierHA
#AdvisorLive
#GetSmartWeek
90© 2015 PREMIER, INC.
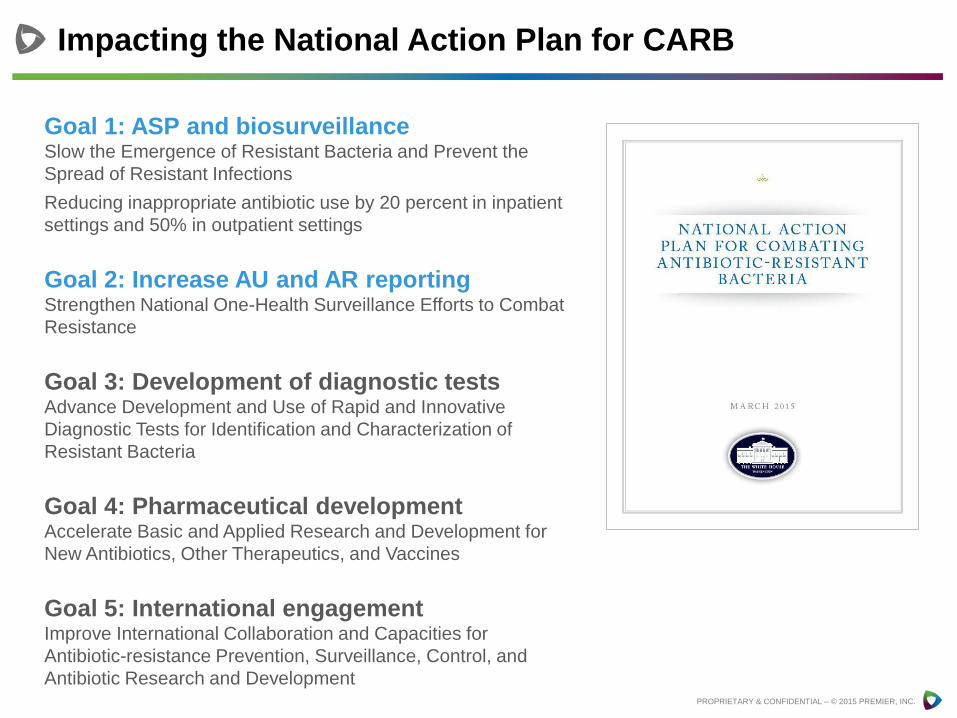
Impacting the National Action Plan for CARB
PROPRIETARY & CONFIDENTIAL – © 2015 PREMIER, INC.
Goal 1: ASP and biosurveillanceSlow the Emergence of Resistant Bacteria and Prevent the
Spread of Resistant Infections
Reducing inappropriate antibiotic use by 20 percent in inpatient
settings and 50% in outpatient settings
Goal 2: Increase AU and AR reportingStrengthen National One-Health Surveillance Efforts to Combat
Resistance
Goal 3: Development of diagnostic testsAdvance Development and Use of Rapid and Innovative
Diagnostic Tests for Identification and Characterization of
Resistant Bacteria
Goal 4: Pharmaceutical developmentAccelerate Basic and Applied Research and Development for
New Antibiotics, Other Therapeutics, and Vaccines
Goal 5: International engagementImprove International Collaboration and Capacities for
Antibiotic-resistance Prevention, Surveillance, Control, and
Antibiotic Research and Development
91© 2015 PREMIER, INC.
Economic impact of redundant antimicrobial therapy in US hospitals. Schultz L, Lower TJ, Srinivasan A, Nielson D, Pugliese G. Infect Control Hosp Epidemiol 2014;35(10):1229-1235
Premier, in collaboration with the CDC,
conducted a study of potentially
redundant antimicrobials.
Objective: This study explored the
incidence and economic impact of
potentially redundant antimicrobial
therapy.
Methods:
• Design: Retrospective analysis
• Study Population: All inpatient
discharges in 505 non-federal facilities
in Premier’s hospital database
• Study Period: January 1, 2008 to
December 31, 2011
• Evaluation: Potentially redundant
antimicrobial therapy defined as
overlapping antibiotic spectra for 2 or
more consecutive days. The study
evaluated 23 IV antimicrobial
combinations.

92© 2015 PREMIER, INC.
78% (394) hospitals had at least 1 of the 23 unnecessary drug combinations prescribed for 2 or
more days across 32,507 cases.
70% of cases represented 3 specific drug combinations for anaerobic infections. Metronidazole and piperacillin-tazobactam made up 53% of cases.
Nearly 150,000 days of potentially inappropriate antibiotic therapy, resulting in nearly $13 million in
potentially avoidable healthcare costs.
If these cases were representative of all U.S. hospitals over that same period of time, more than
$163 million could have been saved.
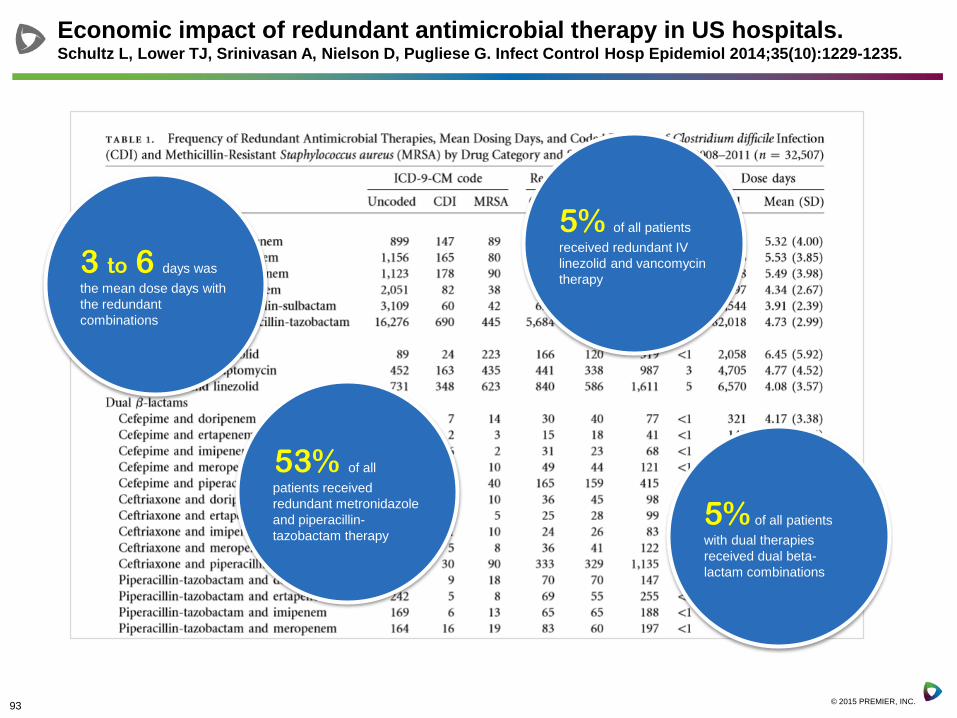
Economic impact of redundant antimicrobial therapy in US hospitals. Schultz L, Lower TJ, Srinivasan A, Nielson D, Pugliese G. Infect Control Hosp Epidemiol 2014;35(10):1229-1235.
78%
70%
150,000
$163M
93© 2015 PREMIER, INC.
Economic impact of redundant antimicrobial therapy in US hospitals. Schultz L, Lower TJ, Srinivasan A, Nielson D, Pugliese G. Infect Control Hosp Epidemiol 2014;35(10):1229-1235.
53% of all
patients received
redundant metronidazole
and piperacillin-
tazobactam therapy
5% of all patients
received redundant IV
linezolid and vancomycin
therapy
5% of all patients
with dual therapies
received dual beta-
lactam combinations
3 to 6 days was
the mean dose days with
the redundant
combinations

94© 2015 PREMIER, INC.
Antimicrobial stewardship is an effective strategy in
reducing overutilization and redundant therapy,
antimicrobial resistance, patient harm, and wasteful
spending.
Based on the study findings of metronidazole used with
piperacillin-tazobactam as the most common
inappropriate or redundant combination, this single
combination should be considered a possible initial target
for antimicrobial stewardship programs.
One successful approach that has been recommended is
for healthcare organizations to develop a list of “never”
combinations of antibiotics or redundant combinations
and provide alerts to providers when these combinations
are ordered.
Applying Lessons Learned
95© 2015 PREMIER, INC.
Launch of QUEST mini collaborative of 50 healthcare
organizations as part of White House commitment
September 2015 to June 2016.
Goals:
• Implement CDC Core Elements for hospital antibiotic stewardship
programs
• Reduce potentially inappropriate use of redundant combinations
of intravenous anti-anaerobic antibiotics
Results and learnings will be shared widely
More info at premierinc.com/antibiotics
Premier Collaborative on Antimicrobial Stewardship
96© 2015 PREMIER, INC.
Premier Research Institute
• Publication with the CDC in September 2014
• 78% of hospital patients treated received unnecessary or
duplicative IV antibiotics
• 70% of the inappropriate use was related to three specific
combinations of IV antibiotics used to treat anaerobic infections
Premier QUEST and PFP Hospitals
• QUEST sprint webinar series on AMS w/CDC
• Participate in performance improvement initiatives to drive AMS
techniques into patient safety practices
PremierConnect Quality
• Developed redundant/duplicative antibiotic usage reports
• Shared reports with member hospitals in October 2014
Premier Activities to Improve Antimicrobial Stewardship

97© 2015 PREMIER, INC.
PremierConnect Safety
• 1000 facilities use Premier’s CDSS to support ASP initiatives
• 27 facilities (~25% of all facilities) have submitted data to NHSN
Antimicrobial Use (AU) module
Premier Advocacy
• Participant in White House Forum on Antibiotic Stewardship
• Participant in Stakeholder Forum on Antimicrobial Resistance (S-
FAR)
• CDC White House Partner for “Get Smart Week 2015”
• Participant in National Quality Partners Antibiotic Stewardship
Action Team
• Participant in NQF initiative to develop a practical playbook to
advance effective antibiotic stewardship
Premier Activities to Improve Antimicrobial Stewardship

98© 2015 PREMIER, INC.
Premier’s Impact on the National Action Plan for CARB
PROPRIETARY & CONFIDENTIAL – © 2015 PREMIER, INC.
Goal 1: ASP and biosurveillance• Premier Research Institute
• PremierConnect Quality
• Premier QUEST and PFP Hospitals
• PremierConnect Safety
• Premier Advocacy
Goal 2: Increase AU and AR reporting• PremierConnect Safety
99© 2015 PREMIER, INC.
Premier resources on antimicrobial stewardship on
Premier Safety Institute® website
Tools, resources, solutions,
blogs on measurement, and
e-surveillance for antimicrobial
stewardship from Premier at
premierinc.com/antibiotics
Thank [email protected]

101© 2015 PREMIER, INC.
Your questions
Enter your questions in this
window on your webinar
screen
or Tweet@PremierHA
#AdvisorLive

102© 2015 PREMIER, INC.
Faculty
MODERATOR
Gina Pugliese, RN, MS, FSHEAVice President
Premier Safety Institute®
CAPT Arjun Srinivasan, MDAssociate Director,
Healthcare associated infection
prevention programs, CDC
Michael Postelnick, RPh BCPS
AQ Infectious DiseasesSenior Infectious Diseases Pharmacist
Northwestern Memorial Hospital, Chicago
Craig Barrett PharmD,BCPSDirector, Safety Solutions, Premier Inc.
@PremierHA
#AdvisorLive
#GetSmartWeek

103© 2015 PREMIER, INC.
Visit the Premier Safety Institute for tools,
resources, and e-surveillance solutions
www.premierinc.com/antibiotics
Want to find out more about today’s topic?
Answer the poll question here now.
Thank you for joining us
Connect with Premier

















