diabetes, thyroid disorders, disorders of the lung, and advanced age are known risk factors for the development
of acute AF. [1] [3] [4] [8] [9] However, AF may occur in the absence of any underlying cardiac or non-cardiac
diseases, for example, as a result of heavy alcohol intake. [4] [14]
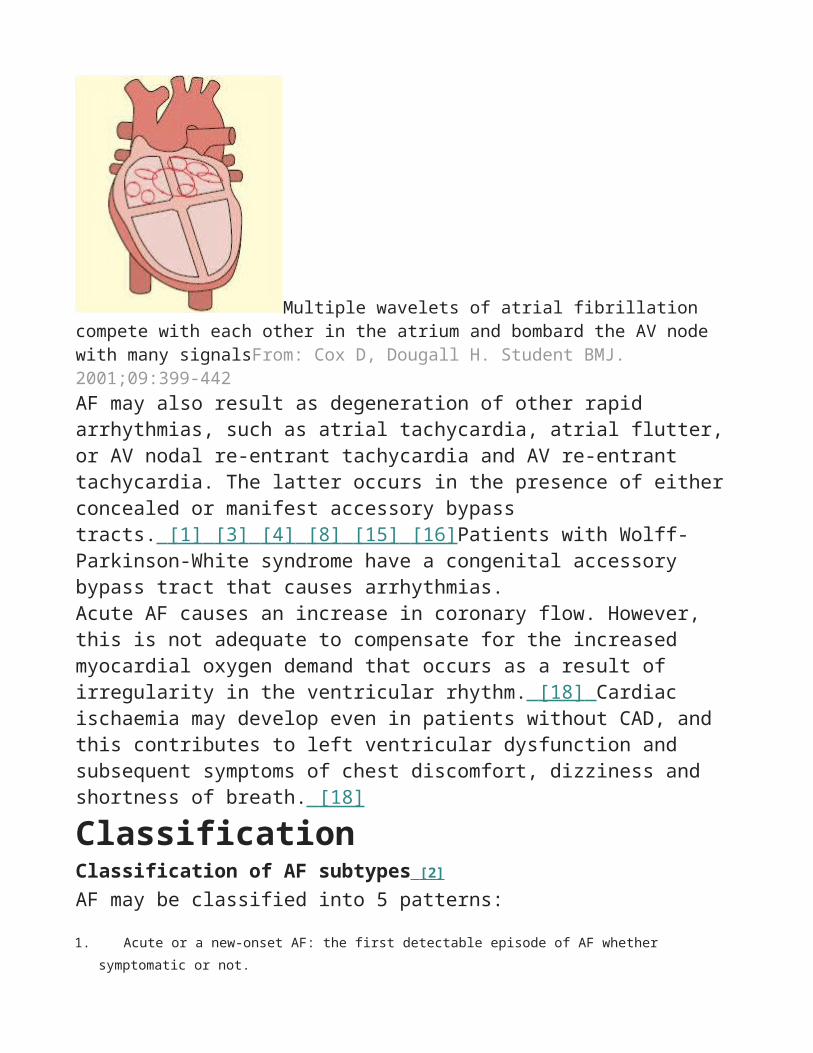
PathophysiologyPathophysiology of AF involves multiple aetiologies and complex electrophysiological changes.[1] [3] [4] [8] [15] [16] [17] AF is usually associated with anatomically and histologically abnormal atria as a result of underlying heart disease. Dilation of the atria with fibrosis and inflammation causes a difference in refractory periods within the atrial tissue and promotes electrical re-entry that results in AF. The fractionation of a mother wave into multiple wavelets in the presence of enlarged atria in conjunction with the short refractory periods and slow conduction properties of the atria lead to sustained AF. The presence of rapidly firing foci, typically in the pulmonary veins, may trigger AF that is sustained by the first mechanism. [17]
Multiple wavelets of atrial fibrillation compete with each other in the atrium and bombard the AV node with many signalsFrom: Cox D, Dougall H. Student BMJ. 2001;09:399-442AF may also result as degeneration of other rapid arrhythmias, such as atrial tachycardia, atrial flutter, or AV nodal re-entrant tachycardia and AV re-entrant tachycardia. The latter occurs in the presence of either concealed or manifest accessory bypass tracts. [1] [3] [4] [8] [15] [16] Patients with Wolff-Parkinson-White syndrome have a congenital accessory bypass tract that causes arrhythmias.Acute AF causes an increase in coronary flow. However, this is not adequate to compensate for the increased myocardial oxygen demand that occurs as a result of irregularity in the ventricular rhythm. [18] Cardiac ischaemia may develop even in patients without CAD, and this contributes to left ventricular
patients with ECG changes suggestive of Wolff-Parkinson-White syndrome who present with
AF and rapid ventricular rate.
Atrial tachycardia Clinical
history and
physical
examinatio
n may not
be useful
to
differentiat
e from AF.
However,
atrial
tachycardi
a (in
particular,
multifocal
atrial
tachycardi
a) is more
common in
patients
with
severe
COPD.
ECG shows abnormal P waves. In multifocal atrial tachycardia, there are at least 3 different
morphologies of P waves. View image
Step-by-step diagnostic approachMost patients with acute AF present with rapid palpitations, fluttering in the chest, dizziness, or shortness of breath. Some patients may also present with stroke and embolic events. The onset of the first episode, its duration, and precipitating factors should be established.
History and examinationMost patients present with symptoms related to the arrhythmia, most of which occur as a result of a rapid ventricular rate. Typical symptoms include palpitations, a sense of the heart racing, dizziness and shortness of breath. Some patients may present with focal neurological deficits such as hemiplegia or dysphasia due to a stroke.
The pulse should be assessed. An irregularly irregular pulse, both in the rhythm and volume, is characteristic. Signs of the underlying cause of AF, such as elevated jugular venous pressure and bibasilar crepitations in heart failure or tremor, sweating, and goitre in hyperthyroidism, should be looked for.
ECGAn ECG should be the first test requested. Absent P waves that have been replaced by irregular fibrillatory waves, and irregularly irregular QRS complexes will confirm the diagnosis of AF.
Atrial fibrillationFrom the collections of Arti N. Shah and Bharat K. KanthariaIn contrast, P waves that have been replaced by a saw tooth appearance in the inferior limb leads, and QRS complexes that are regularly (typically 2:1, 3:1, 4:1) irregular are characteristic of atrial flutter. View image Abnormal and variable morphology P waves can occur in atrial tachycardia. View imageThe ECG may also show evidence of possible underlying causes, such as LVH or previous MI.
Investigation for causal factorsBlood biochemistry should be checked for abnormal potassium or magnesium levels. Cardiac biomarkers should be checked if chest pain is a
feature. Thyroid function testing should be part of the initial assessment, particularly in older people, as classic signs of thyrotoxicosis may not be obvious. [20] Liver function tests (LFTs) are useful to determine presence of a multisystem disorder affecting the liver. Furthermore, LFTs are useful to choose appropriate anti-arrhythmic agents and to monitor anti-arrhythmic drug therapy. For example, amiodarone is contraindicated in the presence of liver dysfunction; and amiodarone treatment should be discontinued when LFTs show abnormalities.
A chest x-ray (CXR) should be performed to look for underlying structural heart disease, such as enlargement of the cardiac chambers or valvular calcification, and signs of heart failure. The CXR may also suggest a precipitating cause of AF, such as pneumonia.
Following the initial assessment, patients should undergo echocardiography to evaluate cardiac chamber size and left ventricular function. This may also reveal an underlying cause such as valvular disease. A transesophageal echocardiogram (TEE) is essential in patients before cardioversion (unless they are already anticoagulated) to rule out left atrial clots.
Electrophysiological studies may be required to identify arrhythmias such as Wolff-Parkinson-White syndrome, atrial flutter, or paroxysmal supraventricular tachycardia. [1] Exercise echocardiography and the exercise nuclear imaging stress test are both useful to identify structural abnormalities of the heart and assess for CAD. A stress test is also useful to assess adequate rate control when a rate control strategy is used. The exercise stress test also helps to determine whether there is a “use dependence” proarrhythmic effect of class Ic anti-arrhythmic agents such as flecainide and propefanone.
A treadmill exercise stress test may be useful for risk stratification for risk of sudden cardiac death in patients with Wolff-Parkinson-White syndrome. The sudden loss of preexcitation delta waves at a faster heart rate during exercise stress testing indicates that the antegrade conduction property of the accessory bypass tract is weaker, and the risk of sudden cardiac death from AF is therefore lower.
Click to view diagnostic guideline references. Diagnostic criteriaRisk factors for thromboembolism in patients with AF [1]
Less validated or weaker risk factors
Female gender
Age 65 to 74 years
CAD
Thyrotoxicosis.
Moderate risk factors
Age ≥75 years
Hypertension
Heart failure
LV ejection fraction ≤35%
Diabetes mellitus.
High risk factors
Previous stroke, transient ischaemic attack, or embolism
Mitral stenosis
Prosthetic heart valve.
CHADS2 scoring system for risk of thromboembolism [22] [2]
In patients with AF and non-valvular (particularly rheumatic) heart disease, the risk of thromboembolic stroke may be estimated by calculating the CHADS2 score. The variables are congestive heart failure (C), hypertension (H), age (A), diabetes mellitus (D), and a history of stroke (S). Each variable is given 1 point except the presence of a history of stroke or prior transient ischaemic attack, which is given 2 points. The validation of this scheme indicates low risk for a CHADS2 score of 0, moderate risk for a CHADS2
score of 1 to 2, and high risk for a CHADS2 score of >2 for future risk of thromboembolic stroke.
The stroke rate per 100 patients-years without antithrombotic therapy according to CHADS2 score is as follows:
Score 0: stroke risk 1.9% (95% CI 1.2-3.0)
Score 1: stroke risk 2.8% (95% CI 2.0-3.8)
Score 2: stroke risk 4.0% (95% CI 3.1-5.1)
Score 3: stroke risk 5.9% (95% CI 4.6-7.3)
Score 4: stroke risk 8.5% (95% CI 6.3-11.1)
Score 5: stroke risk 12.5% (95% CI 8.2-17.5)
Score 6: stroke risk 18.2% (95% CI 10.5-27.4).
The CHADS2 score system is useful and easy to remember. However, because the risk of thromboembolic events is a continuum, categorisation of the risks into low, moderate, and high is artificial, especially taking only a few risk factors into account. The recent 2010 European Society of Cardiology guidelines emphasise a risk factor-based approach using the CHA2DS2-VASc score system. [2] In this system, 2 points are assigned for a history of stroke or transient ischaemic attack; 2 points for age ≥75 years; and 1 point each for age 65 to 74 years, a history of hypertension, diabetes, recent cardiac failure, vascular disease (MI, complex aortic plaque, and peripheral arterial disease [PAD], including prior revascularisation, amputation due to PAD, or angiographic evidence of PAD), and female sex. Based on the CHA2DS2-VASc score system, the adjusted stroke rate (% per year) is as follows:Score 0: stroke rate 0%
In addition to consideration of the risk of stroke and benefit of anticoagulation therapy, the risk of haemorrhage (particularly intracranial) has to be considered. For patients taking warfarin, several scoring systems aim to stratify this risk of bleeding. In the HEMORR2HAGES score, points are assigned for each risk factor: hepatic or renal disease (H), ethanol abuse (E), malignancy (M), older age (>75 years) (O), reduced platelet count or function (R), rebleeding risk (R), uncontrolled hypertension (H), anaemia (A), genetic factor (G), excessive fall risk (E), and stroke (S). One point is awarded for each risk factor, except for a prior bleed (rebleeding risk), which is given 2 points.
Using this system, the risk of major bleeding in National Registry of Atrial Fibrillation participants prescribed warfarin, stratified by HEMORR2HAGES score, was as follows:
HAS-BLED is a scoring system in which the clinical characteristics of hypertension (H), abnormal renal or hepatic function (A), stroke (S), bleeding or its risks (B), labile INRs (L), elderly age group (>65 years) (E), and
drugs/alcohol (drugs such as antiplatelets) (D) are given 1 point each. Based on this scoring system, the risk of bleeding is significantly higher for scores of ≥3.
Case history #1A 65-year-old man with a history of hypertension, diabetes mellitus, and hyperlipidaemia presents to the emergency department with the first episode of rapid palpitations, shortness of breath, and discomfort in his chest. These symptoms started acutely and have been present for 4 hours. Physical examination shows an irregularly irregular radial pulse at rate between 90 and 110 bpm, BP 110/70 mmHg, and respiratory rate of 20 breaths per minute. Heart sounds are irregular, but no S3 or S4 gallop or murmurs are audible. There are no other abnormalities on examination.
Case history #2A 56-year-old woman with a 6- week history of weight loss, anxiety, and insomnia presents with palpitation and dyspnoea. Her pulse rate is irregular at 140 to 150 bpm. Her BP is 95/55 mmHg. She looks thin, frail, and rather anxious and jittery. Her palms are sweaty and have fine tremors. She has a palpable smooth goitre. Examination of the eyes shows bilateral exophthalmoses.
Treatment Options
Patient group
Treatment
line Treatmenthide all
haemodynamically unstable 1st direct current (DC) cardioversion
Used immediately if the patient is haemodynamically
unstable with chest pain, shortness of breath,
dizziness or syncope, hypotension, and rapid heart
rate.
DC cardioversion is performed under adequate
short-acting general anaesthesia and involves
delivery of an electrical shock synchronised with the
intrinsic activity of the heart by sensing the R wave
of the ECG (i.e., synchronised). The energy output
for successful termination of acute AF varies from
200 J to a maximum of 400 J depending on the
Patient group
Treatment
line Treatmenthide all
body size and the presence of other co-morbid
conditions. Lower energy of 100 J may be used as
the starting level when biphasic energy is used.
Presumptive
Patient group
Treatment
line Treatmenthide all
haemodynamically stable with
left atrial thrombus
without heart failure 1st rate control with beta-blockers and/or calcium-channel blockers (CCBs)
Rate-control therapy is required until cardioversion is
successful.
Beta-blockers and CCBs slow AV nodal conduction
of cardiac impulses and subsequently reduce
ventricular rate.
Beta-blockers are particularly useful when acute AF
is associated with an acute MI or angina, and when
acute AF is precipitated after exercise.
Esmolol is useful in patients at risk of complications
from beta-blockade, particularly those with reactive
airway disease, left ventricular dysfunction, and/or
peripheral vascular disease.
CCBs are preferred in patients with chronic lung
disease where bronchospasm may occur with beta-
blockers.
Both groups of medications may cause severe
bradycardia, heart block, asystole, heart failure, or
hypotension.
If rate control is inadequate with monotherapy, a
combination of a beta-blocker and CCB may be
used.
Primary Options
Patient group
Treatment
line Treatmenthide all
metoprolol : 2.5 to 5 mg intravenous bolus initially,
may repeat every 5 minutes to a total of 3 doses;
200 mg orally twice daily
OR
esmolol : 500 micrograms/kg intravenously as a
loading dose, followed by 50 micrograms/kg/min
infusion for 4 minutes, if no response after 5 minutes,
repeat loading dose and increase infusion, consult
specialist for further guidance on dose
OR
diltiazem : 0.25 mg/kg/dose intravenous bolus, may
give second bolus of 0.35 mg/kg if necessary,
followed by 5-15 mg/hour infusion
OR
verapamil : 2.5 to 10 mg intravenous bolus, may give
second bolus of 5-10 mg after 30 minutes if
necessary
Secondary Options
metoprolol : 2.5 to 5 mg intravenous bolus initially,
may repeat every 5 minutes to a total of 3 doses;
200 mg orally twice daily
or
esmolol : 500 micrograms/kg intravenously as a
loading dose, followed by 50 micrograms/kg/min
infusion for 4 minutes, if no response after 5 minutes,
repeat loading dose and increase infusion, consult
specialist for further guidance on dose
-- AND --
diltiazem : 0.25 mg/kg/dose intravenous bolus, may
give second bolus of 0.35 mg/kg if necessary,
followed by 5-15 mg/hour infusion
or
verapamil : 2.5 to 10 mg intravenous bolus, may give
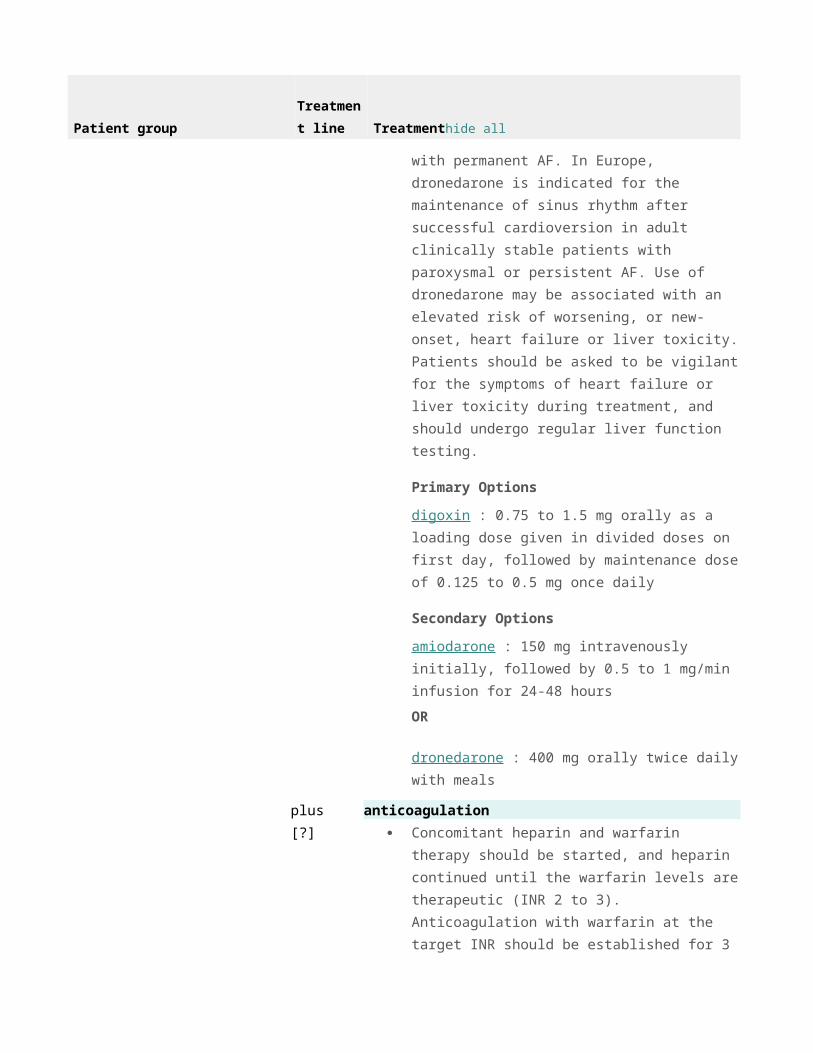
amiodarone : 150 mg intravenously initially, followed
by 0.5 to 1 mg/min infusion for 24-48 hours
OR
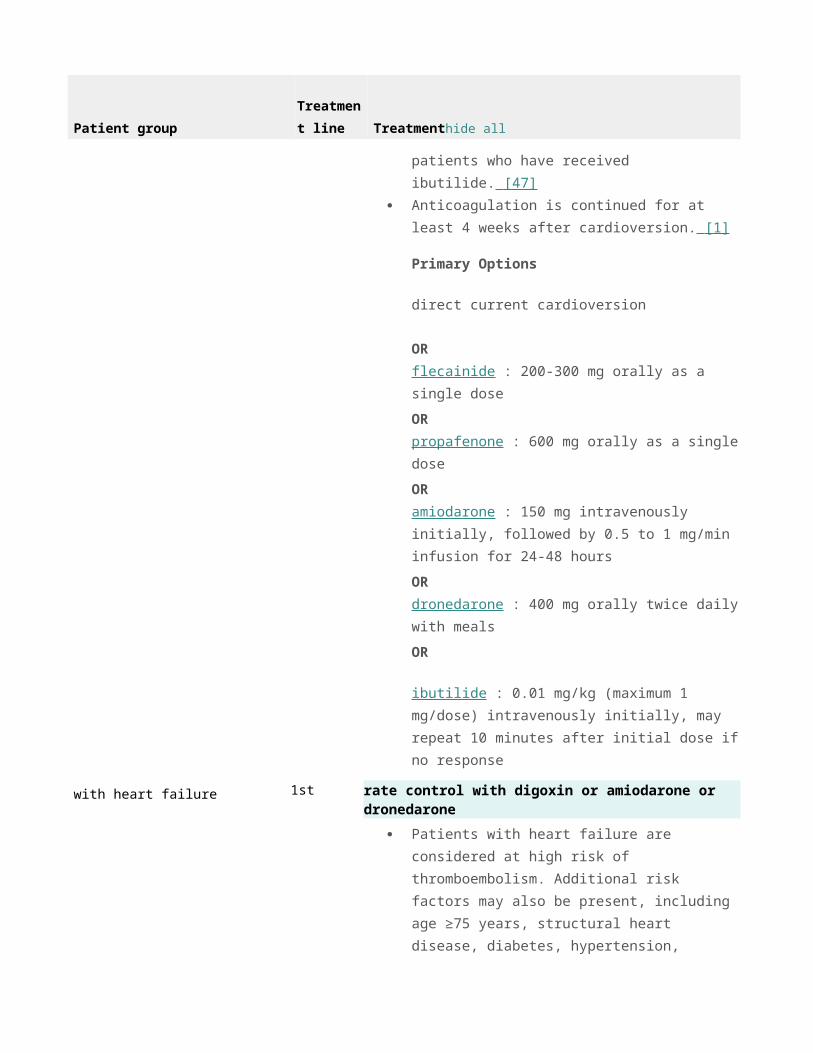
dronedarone : 400 mg orally twice daily with meals
OR
ibutilide : 0.01 mg/kg (maximum 1 mg/dose)
intravenously initially, may repeat 10 minutes after
initial dose if no response
Acute
Treatment approachThe 3 elements in the management of acute AF are:
1. Ventricular rate control
2. Restoration and maintenance of sinus rhythm
3. Prevention of thromboembolic events. [1] [25] [26] [27]
Management of acute AF depends on the nature of its presentation, so the urgency of the treatment required should be assessed. Most cases of acute AF revert to sinus rhythm spontaneously, but do require adequate ventricular rate control with drugs such as beta-blockers, calcium-channel blockers, and occasionally digoxin. Cases that revert spontaneously usually do so in the first 24 hours. [3] Those patients who do not revert may require either direct current (DC) cardioversion or pharmacological cardioversion. Depending on further risks for AF, patients may require treatment with various anti-arrhythmic agents to prevent AF. Among the newly available anti-arrhythmic agents, dronedarone, a multichannel blocker that inhibits the sodium, potassium, and calcium channels and has non-competitive anti-adrenergic activity similar to sotalol, propafenone, and flecainide, has lower efficacy than amiodarone to maintain sinus rhythm. [28] [29] [30] [31] Acute AF may be the first symptomatic presentation of paroxysmal AF, and it is necessary to
perform transoesophageal echocardiography (TOE) to rule out left atrial (LA) clots before cardioversion.Many patients require anticoagulation before, during, and after cardioversion to prevent thromboembolic events. Because commonly used oral anticoagulants (vitamin K antagonists) take several days to have therapeutic effect, patients presenting with acute AF are treated with IV heparin (activated partial thromboplastin time [aPTT] of 45-60 seconds) or subcutaneous low molecular weight heparin while they are awaiting cardioversion and being evaluated for long-term anticoagulation. Dabigatran, a direct thrombin inhibitor, has been released after its comparison with warfarin in a large randomised trial, the RE-LY trial. As compared with warfarin, dabigatran was associated with lower rates of stroke and systemic embolism but similar rates of major haemorrhage. At a lower dose of dabigatran, the rates of stroke and systemic embolism were similar to those for warfarin. The rate of MI was higher with both doses of dabigatran than with warfarin. [27] [32] [33] Dabigatran may be associated with an increased risk of stroke, heart attack, and blood clot in patients with mechanical prosthetic valves and, therefore, should not be used in these patients. [FDA: dabigatran safety alert] (external link) Based on the current evidence, it is reasonable to use dabigatran as a first-line agent or subsequent replacement for warfarin in suitable patients who do not have marked renal insufficiency, and who do not have mechanical prosthetic valves. [32] [33] [34] Another reasonable alternative to warfarin is the direct factor Xa inhibitor rivaroxaban. [32] [33] [35] The ROCKET AF trial compared rivaroxaban with warfarin in patients with non-valvular AF who were at increased risk for stroke. Rivaroxaban was found to be non-inferior to warfarin for the prevention of stroke or systemic embolism. The risk of major bleeding with rivaroxaban was similar to that of warfarin. [32] [33] [36] Apixaban is another direct factor Xa inhibitor that has been shown to be at least as efficacious as warfarin. [32] [33] Following favourable results from the ARISTOTLE trial, apixaban has now been approved to prevent stroke in patients with non-valvular AF in some countries. [37] The choice of anticoagulation strategy depends on the presentation. Factors in the patient's presentation and diagnostic assessment which guide appropriate treatment include the following:
Whether the patient is haemodynamically stable or unstable
If haemodynamically stable, whether the patient is symptomatic or asymptomatic
history of prior thromboembolism, or left ventricular ejection fraction ≤35%.
Need for hospital admissionPatients who present with new-onset AF who are at low risk for major clinical consequences (young patients with no structural heart diseases, no major cardiac symptoms, or haemodynamic compromise) may be discharged directly from the emergency department after stable sinus rhythm is restored.
Admission to hospital is indicated for the following patient groups:
Patients with underlying heart disease who have haemodynamic consequences or symptoms of angina,
heart failure, or syncope or who are at risk for a complication resulting from therapy of the arrhythmia
Older patients
Associated or precipitant medical conditions that require further treatment, such as heart failure,
pulmonary problems (e.g., pneumonia, pulmonary embolism), hypertension, or hyperthyroidism.
Haemodynamically unstable AFAF with a rapid ventricular rate causing ongoing chest pain, hypotension, shortness of breath, dizziness, or syncope requires immediate DC cardioversion. This is performed under adequate short-acting general anaesthesia and involves delivery of an electrical shock synchronised with the intrinsic activity of the heart by sensing the R wave of the ECG (i.e., synchronised). The energy output for successful termination of acute AF varies from 200 J to a maximum of 400 J depending on the body size and the presence of other co-morbid conditions. Lower energy of 100 J may be used as the starting level when biphasic energy is used.
Haemodynamically stable AF: symptomaticPatients require rate-control therapy until cardioversion is successful. If there is no evidence of heart failure, beta-blockers or calcium-channel blockers are
the preferred choice. If rate control is inadequate with monotherapy, a combination of a beta-blocker and calcium-channel blocker may be used. Patient should be carefully monitored to prevent excess AV nodal blockade. [1] If there is evidence of heart failure, digoxin[B Evidence] or amiodarone[C Evidence] should be used.Patients presenting with acute AF of <48 hours' duration and no evidence of LA thrombus on TOE should have DC[C Evidence] or pharmacological cardioversion. DC cardioversion is fast, safe, and efficient. Pharmacological cardioversion is accomplished with the use of anti-arrhythmic agents. However, these must be used with caution as they may cause bradycardia or tachyarrhythmias. Anti-arrhythmic agents with variable, but demonstrated, efficacy for cardioversion of acute AF include flecainide,[B Evidence] propafenone,[A Evidence] ibutilide, vernakalant, [38] [39] [40] dronedarone, [28] [29] [30] [31] and amiodarone.[C Evidence] [B Evidence] Class III agents (including amiodarone and ibutilide) are less efficacious than class IC agents (flecainide and propafenone) in conversion to sinus rhythm. [1] [41] [42] [43] Intravenous vernakalant has demonstrated superior efficacy to amiodarone for acute conversion of recent-onset AF. [40] Oral vernakalant appears to be effective in preventing AF recurrence post-cardioversion. [44] Dronedarone is a multiclass anti-arrhythmic agent. It is approved in Europe for the maintenance of sinus rhythm after successful cardioversion in adult clinically stable patients with paroxysmal or persistent AF and associated cardiovascular risk factors (i.e., age >70 years, hypertension, diabetes, prior cerebrovascular accident, left atrial diameter ≥50 mm, or left ventricular ejection fraction <40%). Dronedarone is contraindicated in patients with NYHA class IV heart failure, or NYHA class II-III heart failure with a recent decompensation requiring admission to hospital or referral to a specialised heart failure clinic. Dronedarone is also contraindicated in patients with AF who cannot, or will not, be converted into normal sinus rhythm (i.e., permanent AF) as a safety review showed that dronedarone doubles the risk of serious cardiovascular events including stroke, heart failure, and death in patients with permanent AF. In Europe, it is indicated for the maintenance of sinus rhythm after successful cardioversion in adult clinically stable patients with paroxysmal or persistent AF. Although dronedarone is less effective than amiodarone for the maintenance of sinus rhythm, dronedarone has fewer adverse effects. [28] [45] However, use of dronedarone may be associated with an elevated risk of worsening, or new-onset, heart failure or liver toxicity. Patients should be asked to be vigilant for the symptoms of heart failure or
liver toxicity during treatment, and should undergo regular liver function testing.The strategy for managing anticoagulation in these patients is as follows:
If the thromboembolic risk is low, no anticoagulation is required.
If the thromboembolic risk is high, IV heparin (aPTT of 45-60 seconds) or subcutaneous low molecular
weight heparin should be started before cardioversion. Once sinus rhythm is restored, the patients should be
started on warfarin and heparin continued until the the warfarin levels are therapeutic (INR 2-3). Anticoagulation
is continued for at least 4 weeks after cardioversion. [1] [46]
If the onset of symptoms is >48 hours or unknown and there is no evidence of LA thrombus on TOE, patients should have DC[C Evidence] or pharmacological cardioversion, but the cardioversion should not be attempted until the patient is established on anticoagulation. The strategy for managing anticoagulation in these patients is as follows:
If the thromboembolic risk is low, heparin should be started, and cardioversion should be delayed until
the patient is established on heparin with a target activated partial thromboplastin time of 45 to 60 seconds.
Following successful cardioversion, heparin can be discontinued and the patient started on long-term aspirin
therapy.
If the thromboembolic risk is high, concomitant heparin and warfarin therapy should be started, and
heparin continued until the warfarin levels are therapeutic (INR 2-3). [1] [15] Anticoagulation with warfarin at the
target INR should be established for 3 to 4 weeks before cardioversion is attempted. [15] Anticoagulation is
continued for at least 4 weeks after cardioversion. [1] [46]
If there is evidence of LA thrombus on TOE, concomitant heparin and warfarin therapy should be started, and heparin continued until the warfarin levels are therapeutic (INR 2-3). Anticoagulation with warfarin at the target INR should be established for 3 to 4 weeks before cardioversion is attempted. Anticoagulation is continued for at least 4 weeks after cardioversion, and may be required for longer in some patients. [1] [46]
Haemodynamically stable AF: asymptomaticPatients with low thromboembolic risk can be observed. Most cases of acute AF revert to sinus rhythm spontaneously, usually in the first 24 hours. If AF does not resolve spontaneously, rate-control therapy is required until cardioversion is successful. Cardioversion can be attempted without the need for anticoagulation.
Patients with high thromboembolic risk require immediate anticoagulation. Concomitant heparin and warfarin therapy should be started, and heparin
continued until the warfarin levels are therapeutic (INR 2-3). Patients should be observed to see whether AF resolves spontaneously. If the AF does not resolve, anticoagulation with warfarin at the target INR should be established for 3 to 4 weeks before cardioversion is attempted. Rate-control therapy is required until cardioversion is performed. Anticoagulation is continued for at least 4 weeks after cardioversion.
Post-cardioversion managementPatients with a newly detected first episode of acute AF converted to sinus rhythm are not continued on rhythm maintenance therapy as the risks outweigh the benefits. Low thromboembolic-risk patients presenting within 48 hours of the onset of symptoms do not require long-term aspirin or anticoagulation. Low thromboembolic-risk patients presenting after this time should be continued on long-term aspirin therapy. Long-term anticoagulation is required for patients with identified high risk for thromboembolism even after sinus rhythm has been restored. [1] [46]
Emerging treatmentsAzimilideBlocks both the rapid (Ikr) and slow (Iks) components of the delayed rectifier potassium current and possesses anti-arrhythmic activity at faster heart rates. Several clinical studies have demonstrated the safety and efficacy of azimilide in the management of ventricular as well as supraventricular arrhythmias. [50]
TedisamilA class III anti-arrhythmic agent that has been reported to block several potassium currents. At higher concentrations, tedisamil inhibits the rapid inward sodium current as well as the chloride channel. Tedisamil is being investigated for acute termination of AF and atrial flutter.[51] [52]
TrecetilideTrecetilide, a congener of ibutilide, is being evaluated in both IV and oral preparations for the termination and prevention of AF. [53]
ACE inhibitors and angiotensin receptor blockersThe renin-angiotensin-aldosterone system has emerged as an important hormonal system in the initiation and pathogenesis of AF. Therefore, ACE inhibitors and angiotensin receptor blockers are emerging as upstream
therapy for the prevention of AF. However, they may not be used as primary or sole anti-arrhythmic therapy in patients with AF. [54] [55]
StatinsStatins have demonstrated some diverse pleiotropic properties, which include their influence on endothelial function, inflammation, plaque stability, thrombosis, angiogenesis, apoptosis, and gene expression. It is by modulating these factors that lipid-lowering drugs are considered to exhibit their anti-arrhythmic properties. Many clinical trials and their meta-analyses indicate that the use of statins significantly decreases the risk of incidence or recurrence of AF in patients in sinus rhythm with a history of previous AF or undergoing cardiac surgery or after acute coronary syndrome. [56] [57]
MagnesiumMany clinical trials and their meta-analyses indicate that intravenous magnesium is not very effective in converting acute-onset AF to sinus rhythm when compared with placebo or an alternative anti-arrhythmic drug. However, as a rate-control regimen, adding intravenous magnesium to digoxin reduces fast ventricular response in acute-onset AF. [58] [59]
MonitoringPatients presenting with acute AF who have paroxysmal, persistent, or permanent AF need long-term follow-up. Depending on the nature of the underlying cause of AF (i.e., CAD, valvular heart disease, or heart failure), patients should have regular (minimum 6 to 12 months) echocardiograms and consideration of exercise stress testing.
Patients who are taking anti-arrhythmic agents need follow-up for ECG monitoring. Exercise stress testing is recommended to assess for use-dependence pro-arrhythmia of ventricular tachycardia in patients taking flecainide and propafenone.
A regular follow-up to check and monitor INR is mandatory for those patients who are taking warfarin for anticoagulation. Routine monitoring of digoxin levels is not required but levels can be checked if toxicity or inadequate dosing is suspected.
Patients who have identifiable and known triggers to AF, such as alcohol, stimulants, caffeine, or nicotine, should be advised to avoid such triggers to help prevent recurrence.
ComplicationsComplicationhide all
acute stroke
see our comprehensive coverage of Overview of stroke
Patients usually have paroxysmal to persistent AF with risk factors to thromboembolic events, such as left atrial
dilation, CHF, hypertension, diabetes, hyperlipidaemia, and advanced age.
Controversy exists as regards treatment of established embolic acute stroke in the presence of acute AF.
Anticoagulation in this setting may cause haemorrhagic stroke. Consultation with a consultant (neurologist) is
highly recommended. Novel approaches to interrupt thrombus propagation by intravascular devices are being
studied.
MI
see our comprehensive coverage of Overview of acute coronary syndrome
Rapid ventricular rate and increased myocardial demand may lead to acute MI in people with CAD.
CHF
see our comprehensive coverage of Acute exacerbation of congestive heart failure
Rapid ventricular rate, increased myocardial demand, and unfavourable haemodynamics may lead to acute
heart failure in people with CAD, left ventricular dysfunction, and valvular pathology.
Last updated: Jan 28, 2
PrognosisThe prognosis of acute AF depends on several factors, such as the precipitating event, underlying cardiac status, risk of thromboembolism, and whether the nature of the AF is paroxysmal, persistent, or permanent. In young patients with no structural cardiac abnormalities who have an episode of acute AF as a result of alcohol bingeing, prognosis is excellent with avoidance of alcohol. In contrast, short- and long-term prognosis for patients presenting with new onset of AF with heart failure following MI is poor. Furthermore, a meta-analysis has shown that there is an increased risk of mortality with the presence of AF in the setting of MI, which persists regardless of the timing of AF. [60] Patients with prior AF or new-onset AF following MI need close clinical follow-up.