Top Poole Hospital NHS Foundation Trust Council of Governors Council of Governors January 2014 16 January 2014 - 16:30 Board Rooms, BH15 2JB AGENDA 1 Apologies for Absence 2 Declaration of Interests 3 Draft Minutes of Meeting held on 26 September 2013 CoG Jan 14 A CoG Minutes Sep 13 Part 1 Draft 6 4 Matters Arising/Action List CoG Jan 14 B Actions 13 5 Chairman’s Comments 6 FOR APPROVAL 7 Draft Council’s 2014/15 Governance Cycle Owner: Co Sec CoG Jan 14 C2 Draft Governance Cycle 15 CoG Jan 14 C Gov Cycle cover sheet Apr 14 14 8 Chairman’s and Non-Executive Directors Appraisal Process - 2013/14 and Onwards Owner: Co Sec CoG Jan 14 D 1 Chairman and Non-Executive Director 18 CoG Jan 14 D 2 Chairman and Non Executive Appraisa 19 9 Revised NREC Terms of Reference Owner: Chairman CoG Jan 14 E1 NREC ToR Cover Sheet 33 CoG Jan 14 E2 NREC ToR 34 10 NREC Transitional Arrangements for Tenure of Membership Owner: Chairman CoG Jan 14 F1 NREC Membership Transitional Arrange 37 CoG Jan 14 F2 NREC Membership Transitional Arrange 38
The minutes of the meeting of the Council of Governors of Poole Hospital NHS Foundation Trust held on 26 September 2013 at 5.30 pm in the Board Room, Poole Hospital.
Present: Mrs A Schofield Chairman Cllr. J Adams Bournemouth Borough Council AVM G Carleton Purbeck, East Dorset & Christchurch Mrs L Cherrett Clinical Staff Ms C Cherry Bournemouth University Mr A Creamer Poole Mr B Faith Poole Mrs R Gould Purbeck, East Dorset and Christchurch Mr G Hermsen Poole
Mrs B Hooper Purbeck, East Dorset and Christchurch Cllr. D Jones Dorset County Council
Miss K Knudsen Clinical Staff Canon J LLoyd Non-Clinical Staff Mrs S Lowrey Clinical Staff.
Mr J Pride Poole Mr T Purnell Bournemouth
Cllr. A Stribley Borough of Poole Mrs S Yeoman Poole
In attendance: Mr M Beswick Company Secretary
Mr C Bown Chief Executive Mr Mathew Hepenstal Deloittes LLP Dame Yvonne Moores Trust Vice Chairman Miss J Retigan Minute Taker Mr M Smits Director of Nursing & Patient Services
Mr G Spencer Senior Independent Director Mr R Talbot Medical Director Mr P Turner Director of Finance
CoG 094/13 Apologies for Absence
Apologies for absence were received from Mrs V Duckenfield; Poole, Mr R King; Poole, Dr C McCall; Dorset Clinical Commissioning Group, Mrs I McLellan; North Dorset, West Dorset, Weymouth and Portland, Mr B Newman; Bournemouth and Mrs E Purcell; Poole.
CoG 095/13 Declarations of Interest
It was noted that the Council of Governors could potentially have an interest in any item related to merger.
The Chairman noted her interest in Section A of the Part 2 meeting. CoG 099/13 Minutes of the Meeting held of the 25 July 2013 (Paper A)
The minutes were agreed as an accurate record of the meeting.
CoG 100/13 Matters Arising (Paper B)
046/13 – The Chairman reported that hard copies of the Director, Governor Interaction Best Practice Guide were awaited, and it was expected this would be the subject of further discussion in January. ACTION: AS
050/13 – The Chairman noted that a presentation from the Ambulance
Service and also the Dorset Clinical Commission Group remained as items for a future meeting but had been deferred due to other demands.
075/13 – The erroneous figures in Appendix 4 of the Annual Audit &
Governance Report had been corrected. 076/13 – The Chairman reported that Mr Smits had completed the draft action
plan for the Trust response to the Francis Report and, alongside a review of the Trust’s governance arrangements, would be submitted to the October Board of Directors meeting.
It was noted that all actions, unless subject to this agenda, had been executed.
CoG 101/13 Chairman’s Comments
The Chairman reported that Mrs Sherry would be leaving the Trust on 3 October. The Council recorded their appreciation of her work and it was agreed a formal letter of thanks would be sent to Mrs Sherry from the Council of Governors. ACTION: AS The Annual Members Meeting would take place on 30 September and all were encouraged to attend this important event. The Chairman and Chief Executive had held a positive meeting with the
Chairman and Chief Officer of the Clinical Commissioning Group (CCG) in
early July.
The Hospital Church Service would take place at 3 o’clock on 20 October at
St Mary’s Church, Longfleet Road, Poole.
Governor elections had commenced and all constituencies had multiple
candidates except Bournemouth, for which Terry Purnell had been returned
uncontested.
Two Board Seminars had taken place in August. At the first the Board had considered a review of the Board and its committees and the governance arrangements which were under review following recent publications, e.g. Francis Report, Keogh Report, etc. Also considered had been the position with merger. At the second Seminar they had considered future strategies for Poole Hospital and discussed the recent meeting with Monitor.
Upcoming Fundraising events were noted, including the Bournemouth Festival of Running on 5-6 October, The Great Poole Hospital Bake Off taking place between 9 October and 6 November and the China Trek in early October. Further details on these and other events would be available from the Fundraising Office.
The report was NOTED.
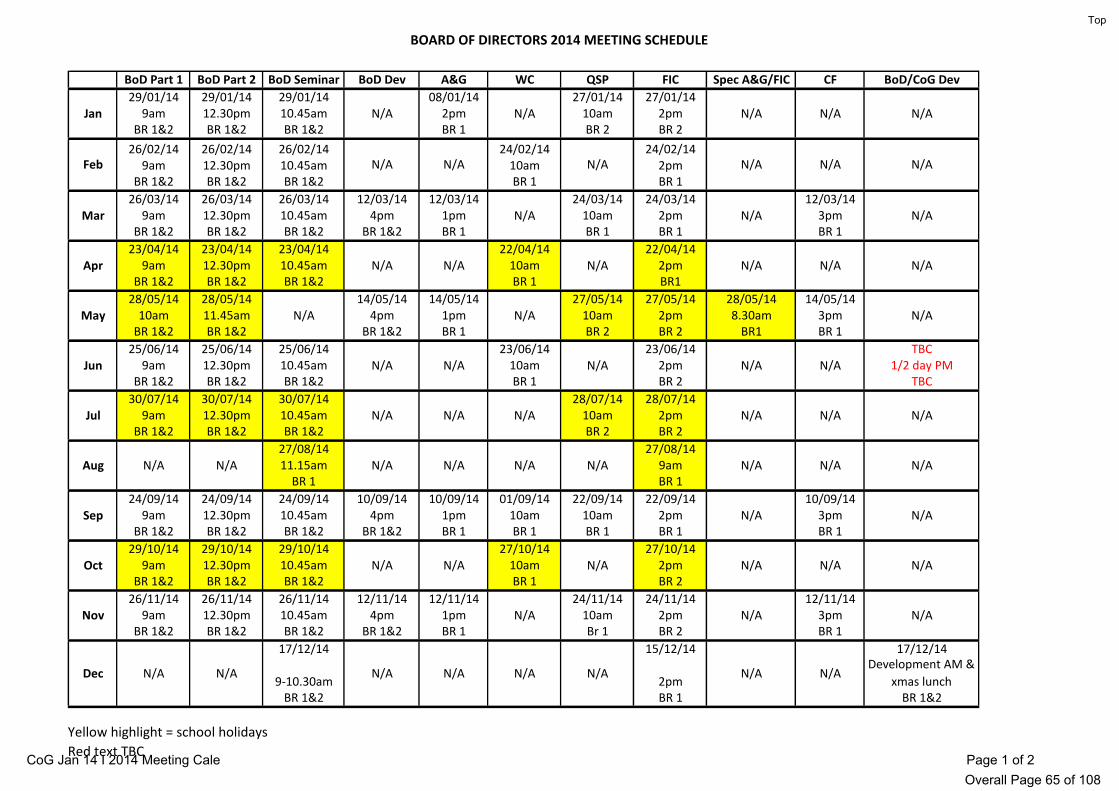
CoG 102/13 Proposed 2014 Meeting Dates (Paper C) The Chairman presented the programme of meetings for 2014 which followed
the usual pattern. Discussion regarding start times for meetings of the Council of Governors
took place and it was agreed that these would commence earlier, subject to the opinion of the next cohort of Governors to be elected. ACTION: MB
The report was APPROVED. 2012/13 Annual Report & Accounts CoG 103/13 Annual Report & Accounts (Including Audit Opinion) (Paper D)
The Chief Executive reported that the 2012/13 Annual Report and Accounts had been laid before Parliament in June. He noted that the report recognised the current financial challenges in the NHS. The Finance Director presented the accounts and noted the distortion caused by the revaluation of estates. Cllr. Adams noted the costs for clinical negligence claims and the Finance Director reported that as the Trust had a maternity unit they were subject to high value claims. The Chairman noted that claims were kept under regular review by the Board of Directors. Mr Hepenstal reported that the external audit had resulted in a clean audit report and everything had been completed to the timetable set by Monitor. The report was RECEIVED.
CoG 104/13 Supporting Information
Letter & Report: The Quality Accounts (Paper E)
Mr Hepenstal presented the report and noted the requirements of the audit, set out in the Executive Summary on page 4 of his report, which followed Monitor’s Audit Code. Mr Hepenstal reported that the content of the Quality Report had been reviewed for consistency and no issues had been identified. The data for three indicators had been tested and for one of these two errors had been found. The sample size had been extended and no further errors had been found and it had been concluded that these were isolated errors and the recommendation put forward to prevent future occurrences had been adopted by the Trust.
The report was discussed and the challenging Clostridium Difficile target was noted. The report was NOTED
Letter on the Financial Audit (Paper F)
Mr Hepenstal presented the report and noted the work of staff to provide information and meet set time scales. He was pleased to report the Trust had achieved an unqualified audit report. The Director of Finance reported that the Trust had been content with the audit and noted a good working relationship with Deloitte LLP. The report was NOTED.
CoG 105/13 Annual Complaints Report (Paper G)
The Medical Director presented the report. He noted that the Trust encouraged patients and carers to complain as this allowed the organisation to learn. It was noted that complaints continued to increase steadily across the NHS.
The nature of complaints was discussed. The increase in complaints relating
to discharge arrangements was noted as was the management of expectations in a changing health service. The Medical Director again emphasised the value of actions taken and lessons learnt as a result of complaints.
The Medical Director reported that following a request from the Board of
Directors, quarterly complaints reports now included an appendix on the work of the Patient Advice and Liaison Service (PALS). The PALS service receives many enquiries of which less than ten percent were recommended to be taken forward as formal complaints; approximately fifty percent of these were pursued. The Medical Director reported that all complaints were RAG rated and all amber and red complaints were investigated to ensure learning was identified, regardless of the complaint being formally pursued.
The report was discussed in detail and NOTED. CoG 106/13 Report from NREC Meeting 26 September 2013 The Chairman reported that a meeting of the Nominations, Remuneration and
Evaluation Committee took place and would be discussed further in the Part 2 meeting.
The report was NOTED. CoG 107/13 2013/14 Quality Accounts Content The Director of Nursing & Patient Services reported that in previous years the
Council of Governors had contributed to the setting of quality targets. It was noted he would contact those Governors who had previously been involved in
this work and details for others who wished to contribute would be issued in the Governor Newsletter. ACTION: MSm
The report was NOTED. CoG 108/13 Integrated Trust Performance Report Month 5 (Paper H) The Finance Director reported that the Trust continued to maintain the
planned financial position with the achievement of a small surplus and the cash position at £12 million. He noted that the surplus was supported by some non recurring income and benefits and that the results confirmed the financial challenges which would continue to increase.
The Chief Executive detailed the position with key performance targets and
noted the strong performance in the Emergency Department with the challenging four hour target, which remained fragile. The Chairman noted that this demonstrated the strong leadership and hard work of staff at Poole Hospital.
The report was considered in detail with a particular focus on theatre
utilisation, the stroke unit, patients with dementia and shortages in certain areas for medical staff. It was noted that some information was missing for day cases and it was agreed that this would be subsequently issued to Governors. ACTION: CB
The report was NOTED. CoG 109/13 Merger Update (Paper I) The Chief Executive reported that the provisional findings of the Competition
Commission (CC) had been received since the last meeting. Representatives from both Royal Bournemouth & Christchurch Hospitals (RBCH) and Poole Hospital had attended formal hearings and responded to questions and information requests from the CC. The CC had held a public drop in event. The Chief Executive reported that no decision had yet been made and the final report would be issued by the CC no later than 21 October.
The Chief Executive noted that responses for each potential scenario had
been prepared as there would be little warning prior to publication by the CC. Discussion on possible outcomes took place and it was agreed that this would
be considered at the next Informal Governor meeting in October when the decision would have been received. ACTION: AS
The report was NOTED. CoG 110/13 Monitor’s Risk Assessment Framework (FTN Briefing) (Paper J) The Company Secretary presented the report which was submitted to inform
the Council of Governors of the Revised Monitor Risk Assurance Framework (RAF).
It was noted that the new RAF would become operational for the third quarter
The report was NOTED. CoG 111/13 Register of Interests (Paper K) The Chairman presented the report and noted that any changes should be
notified to the Company Secretary’s office. The report was NOTED. CoG 112/13 Reports from Reference Groups Membership Engagement and Recruitment Mrs Yeoman thanked those Governors who continued to support the
recruitment of members. Mrs Yeoman noted that Governors were working with Karen Hollocks, Head
of Communication, and the Children’s Unit, to attract young people as members.
The report was NOTED.
Future Plans & Priorities
Mr Purnell reported he had met with the Director of Finance and Company Secretary and two meetings had been scheduled for Future Plans & Priorities Group, to consider the impact of the CC decision and key planning assumptions for 2014/15. Mr Purnell noted that the first meeting would take place at six o’clock on 31 October and all Governors were invited to attend. The second would be in April 2013 and would consider the 2014/15 draft annual plan. The report was NOTED.
CoG 113/13 Future Agenda Items
The Chairman reported that the CCG and SWAST presentations would be arranged as appropriate.
A development session would be arranged for 18 December and further detail
would be provided in the weekly Governor Newsletter. ACTION: AS CoG 114/13 Notices of Motion
No notices of motion were received.
CoG 115/13 Urgent Notices of Motion
No urgent notices of motion were received. CoG 116/13 Date of Next Meeting
16 January 2014 (time to be confirmed) in the Board Room, Poole Hospital.
POOLE HOSPITAL NHS FOUNDATION TRUST COUNCIL OF GOVERNORS
GOVERNANCE CYCLE (Apr 14)
Code of Governance Reference
REPORTS Q4 May 14
Q1 July 14
Q2 Oct 14
Q3 Jan 15
LEAD
Committee/Reference Groups
Constitution Receive report/minutes from Nominations, Remuneration and Evaluations Committee
AD HOC
AD HOC
AD HOC
AD HOC
Chair
Reference Groups
Receive updates from any of the three Reference Groups:
Membership Engagement
Future Plans and Priorities
Quality Report (Ad Hoc)
X
X X X
MERG Chair
FPP Chair
DoNPS
Regular Reports
Monthly Report Cycle
Receive Chairman's Comments X X X X Chair
A.5.9. Receive Trust Performance Report (assurance of according with terms of authorisation)
X X X X CEO
Good Practice
Receive Strategic Risk Report (Part 2)
X X X X DoNPS
Good Practice
Receive Quarterly Submissions to Monitor (Part 2)
X X X X DoF
Good Practice
Receive Feedback from Monitor on Quarterly Submissions (Part 2)
X X X X DoF
Annual Report Cycle
B.6. Receive outcome of the Chairman’s and non-executive directors’ annual performance evaluation (Part 2)
X Chair/ SID
D.2.4. Approve recommendations from Nominations, Remuneration and Evaluation Committee on Chairman’s and non-executives’ remuneration/ allowances/terms & conditions
X Chair/ CEO
B.6.5. Receive Council of Governors Assessment of collective Performance
C.3. Agree with Audit & Governance Committee the criteria for the appointment/reappointment and removal of the Trust’s auditors (appointment Oct 12 for 3 years) Receive the Letter of Engagement from the Auditor Appoint Auditors
Chair A&GC/ DoF Chair/ DoF Chair A&G
Constitution Review policy for Composition of CoG and non- executive directors (CoG (Constitution Review) April 15 & NEDs April 14)
Chair
Constitution Review Membership Strategy (June 14)
Co Sec
NREC ToR Review the Terms of Reference of the Nominations, Remuneration and Evaluation Committee (postponed)
Meeting Date: January 2014 Agenda Item: 8 Paper No: D
Title:
Chairman’s and Non-Executive Directors Appraisal Processes for 2013/14 and onwards
Purpose:
To approve the update the Chairman’s and Non-Executive Directors Appraisal Processes
Summary:
In light of the 2012/13 round the Chairman’s and Non-Executive Directors appraisal processes for future years has been updated to;
Amend Chairman’s appraisal Appendix B from a “scoring” pro –forma to a performance narrative
Increase the recipients of the Chairman’s questionnaire from 5 to the whole of Council.
Corrects the inaccuracy (Page 1 Chairman’s Appraisal Processes Step 3) from Lead Governor to Deputy Chairman of Governors.
The attached paper asks that the Nominations Remuneration and Evaluation Committee (NREC) makes an oral recommendation to the Council of Governors that it approves the update of the Chairman’s and Non-Executive Directors Appraisal Processes
Recommendation:
To approve the oral recommendation from NREC on the update to the Chairman’s and Non-Executive Directors Appraisal Processes
Report to the Council of Governors 16 January 2014.
CHAIRMAN AND NON EXECUTIVE APPRAISALS 2013/14 and Onwards
In April 2012 the Council of Governors agreed the processes for undertaking the 2011/12 and the 2012/13 performance appraisals of the Chairman and Non-Executive Directors.
Non-Executive Directors’Appraisal Process
In summary the non-executives’ appraisal process has the following key steps;
Step 1 Each Non-Executive Director will prepare a self-assessment using parts 1 to 3 of the appraisal proforma (See Appendix A below).
Step 2 Chairman and each Non-Executive Director discuss performance and professional/personal development on a one to one basis, following which parts 4 and 5 of the appraisal proforma are completed
Step 3 An agreed set of objectives and a personal development plan are produced for the coming year.
Step 4 The appraisal form is summarised and shared with the NREC, by the Chairman, A report of the outcome of the NEDs’ appraisals (including any development areas identified) shall be presented to the NREC by the Chairman. A summary of this report shall be presented by the Chairman to the next available meeting of the Council of Governors.
This paper confirms the appraisal processes for 2013/14 and onwards for tthe non-executive directors and seeks the approval of the Council of Governors to these processes.
Chairman’s Appraisal Process
In summary the Chairman’s appraisal process has the following key steps;
Step 1 The Chair will prepare a self-assessment of performance using the proforma (see Appendix B below)
Step 2 The Senior Independent Director (SID) requests all Board Directors to complete a confidential assessment of the Chair, using the Chair peer assessment proforma (see Appendix C below). Through the Company Secretary’s Office, the SID requests all Governors to complete the proforma (see Appendix D below)
Step 3 The SID contacts the Deputy Chairman of Governors to establish if there are any additional views or comments the Deputy Chairman is aware of, arising from Governors, which are relevant to include in the appraisal. The SID contacts the Chief Executive, to establish any additional views or comments arising from Executive Directors. The SID also canvasses the views and comments of Non-Executive Directors.
Recommendation
The Council of Governors approve the processes for the Chairman’s’ appraisal in 2013/14 and onwards.
The Council of Governors approve the processes the non-executive directors’ appraisals in 2013/14 and onwards.
Respondents may wish to add comment in support of their responses. If so, please do so in the box provided on the next page
No Statement 1 2 3 4 5
1
The Chairman is an effective leader of the Board, ensuring its effectiveness on all aspects of its role and setting its agenda.
2
The Chairman ensures that the Directors receive accurate, timely and clear information.
3
The Chairman ensures that opportunities are given to Directors to continually update their skills and knowledge to fulfil their role both on the Board and on Board Committees.
4
The Chairman ensures effective communication with stakeholders.
5
The Chairman facilitates the effective contribution of Non- Executive Directors.
6
The Chairman ensures constructive relations between Executive and Non-Executive Directors.
Respondents may wish to add comment in support of their responses. If so, please do so in the box provided on the next page
No Statement 1 2 3 4 5
1
The Chairman is an effective leader of the Council of Governors, ensuring its effectiveness on all aspects of its role and setting its agenda.
2
The Chairman ensures that the Governors receive accurate, timely and clear information.
3
The Chairman ensures that opportunities are given to Governors to continually update their skills and knowledge to fulfil their role on the Council of Governors, for example through Council of Governors Development Sessions.
4
The Chairman ensures effective communication with stakeholders.
5
The Chairman facilitates the effective contribution of Governors.
6
The Chairman ensures constructive relations between Executive and Non-Executive Directors and Governors.
The Nominations, Remuneration and Evaluation Committee Terms of Reference
Purpose:
To Update the Committees Terms of Reference
Summary:
The Terms of Reference have been updated for tenure of membership on the Committee. The changes are shown in the document in bold italic text at para 2.2. The attached paper asks that the Nominations Remuneration and Evaluation Committee (NREC) makes an oral recommendation to the Council of Governors that it approves the update NREC’s to the Terms of Reference
Recommendation:
To approve the oral recommendation from NREC on the update to NREC’s to the Terms of Reference.
NOMINATIONS, REMUNERATION AND EVALUATIONS COMMITTEE
TERMS OF REFERENCE
1. CONSTITUTION 1.1 The Nominations, Remuneration and Evaluations Committee is a sub-committee of
the Council of Governors. 1.2 The Committee is responsible for advising and/or making recommendations to the
Council of Governors relating to:
i) evaluation of the performance of the Chairman and Non-Executives;
ii) the remuneration, allowances and other terms and conditions of office for the Chairman and Non-Executives;
iii) the composition of the Council of Governors and the non executive directors;
iv) the recruitment process for the selection of candidates for the office of Chairman or other Non-Executive Directors;
v) the selection of candidates selected for interview for the office of Chief Executive or Executive Directors;
vi) to consider the continuing tenure of absentee Council Governors.
1.3 The Nominations, Remuneration and Evaluations Committee will produce an Annual
Report on its own work.
2. MEMBERSHIP 2.1 The Chairman of the Trust, or in his absence, the Vice Chairman is to preside at
meetings of the Nominations, Remuneration and Evaluation Committee. If the Chairman is absent from a meeting or temporarily absent on grounds of a declared interest the Vice-Chairman shall preside. If the Chairman and Vice-Chairman are absent, such Non-Executive Director as the Governors present shall choose shall preside. The Committee will comprise of two public governors, one appointed governor and one staff governor.
2.2 Governors comprising the Committee will be nominated by constituency.
Where there is more than one nomination a ballot of that constituency will take place. The term of office will be for a 3 year term with a permitted maximum of 2 x 3 year terms.
2.3 In discharging its responsibilities the Chief Executive of the Trust will be entitled to
attend the meeting of the Committee unless the Committee decides otherwise, and the Committee will be required to take account of the Chief Executive’s views.
2.4 For the appointment of Chairman to the Trust the Committee will seek the services of
2.5 For all appointments and matters relating to remuneration the Committee will seek advice from the professional human resources services of the Trust who may in turn look for professional external support.
3. FREQUENCY 3.1 The Committee will meet a minimum of once a year. Additionally if required for
Chairman/Non Executive Director appointment. 3.2 Following consultation by the Chairman, additional meetings may take place in electronic format (email, telecommunication). 4. QUORUM 4.1 The quorum is at least three members present (or contributing to an electronic
forum), one of whom must be a publicly elected Governor. 5. AUTHORITY 5.1 The Committee is authorised by the Council of Governors to carry out any activity
within its Terms of Reference. 6. REPORTING MECHANISM 6.1 Minutes of each Committee will be formally recorded and submitted to the Council of
Governors. 6.2 The Chairman should draw to the attention of the Council of Governors any matters
relevant to the Committees duties. 7. PROCESS 7.1 The Committee will:
i) on a regular and systematic basis monitor the performance of the Chairman and other Non-Executive Directors and make reports thereon to the Council of Governors when requested to do so or when in the opinion of the Nominations, Remuneration and Evaluation Committee the results of such monitoring ought properly to be brought to the attention of the Council of Governors;
ii) consider and make recommendations to the Council of Governors as to the remuneration and allowances and other terms and conditions of office of the Chairman and Non-Executive Directors;
iii) review the composition of the Council of Governors and the non executive directors from time to time.
iv) to determine the processes for the selection of candidates for office as Chairman or other Non-Executive Director of the Trust having first consulted with the Board of Directors as to these matters and having regard to such views as may be expressed by the Board of Directors;
v) using the Trust’s HR Services to seek candidates for office and to assess, shortlist and select for interview such candidates as are considered
appropriate and in doing so the Nominations, Remuneration and Evaluation Committee shall be at liberty to seek advice and assistance from persons other than members of the Committee or of the Council of Governors such as external organisations recognised as experts in recruitment;
vi) to make recommendations to the Council of Governors of the candidate for appointment as Chairman or other Non-Executive Director, as the case may be.
7.2 A schematic of the Committees working is attached as Appendix 1.
8. REVIEW 8.1 The Terms of Reference will be reviewed in January 2017 or at the request of the
Council of Governors by the Committee making recommendations to the Council of Governors as appropriate.
MICHAEL BESWICK Company Secretary November 2009 Updated: November 2010 to reflect new Chairman arrangements agreed by the Council on 23 November 2010. Further update January 2014 for tenure of membership
S:\CORPORATE DIRECTORATES\Strategic-Development\FT Governance\Register\E CoG Requirements\E13 CoG Nominations Committee and guidelines\E13 - NREC ToR Nov 2010.doc
The Nominations, Remuneration and Evaluation Committee Tenure of Membership
Purpose:
To approve the proposed changes for the transition of the tenure of NREC membership (See paper E )
Summary:
With the proposed changes to membership tenure to a 3 year term with a maximum of 6 years (See paper E) steps need to be put in place for transition to allow normal business to proceed. The transitional arrangements are proposed on the attached report
Recommendation:
To approve the recommended the changes for the transition of the tenure of NREC membership (See paper E )
Allow greater levels of assurance, scrutiny and support Learn about the clinical business
For greater assurance and scrutiny;
Consider the reporting of the Monitor quarterly governance certification to the Council
Development of the Informal Reference Groups
Getting best out of governors and their time
The reference groups of the Council of Governors, supported by the relevant Trust staff, are to continue. Other reference groups will be initiated in response to the needs of governors and a new reference group is proposed for governors training and development
Will be set up as and when required.
Developing the Role of Governors
Governors to deploy “effective” challenge in all circumstance Allow greater levels of assurance, scrutiny and support
The role of governor will be developed through the attendance and material provided through the Trust and by Monitor the Foundation Trust Network, Foundation Trust Governor Association and the South West Governor Exchange Network.
Governor access available through normal channels. Please refer to the Main report containing this annex
Development Resources
Assist Governors to carry out their statutory duties
Access to Foundation Trust Network (FTN) development events and the South West Governors Exchange Network (SWGEN)
Details provided as they arise.
Access to “Your Statutory Duties: A Reference Guide for NHS Foundation Trust Governors” and “Guide to Monitor for NHS Foundation Trust Governors”.
Provided as a hard copies and available on Monitor’s website or paper copy on request.
Access to in-house training as appropriate available to Governors to help to carry out their statutory duties. Establish a governor led process for managing the Governors Development Plan
Ask the Company Secretary Function for details. Please refer to the Main report containing this annex
To receive the Trust’s revised Membership Development Strategy
Summary:
The Membership Development Strategy was considered by the Council’s Membership Engagement and Recruitment Reference Group and Council are asked to receive the strategy which will be a matter for Board approval at its February 2014 meeting
Recommendation:
The Council of Governors receive the Trust’s revised Membership Development Strategy
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 7 of 17
1 RELEVANT TO
1.1 All Governors of the Trust serving on the Council of Governors, Board of Directors, membership staff and foundation trust members.
2 PURPOSE
2.1 The Membership Development Strategy sets out the way in which Poole Hospital NHS Foundation Trust will maintain membership numbers, grow a representative membership and develop and engage with its members. The Strategy will ensure that the Trust adopts a planned and co-ordinated approach to membership ensuring that it is representative and that members have the opportunity to participate in the future development of the Trust.
3 DEFINITIONS
3.1 This is a Board level strategy produced with the guidance and input of the Council of Governors.
4 DOCUMENT DEVELOPMENT
4.1 As a foundation trust we are accountable to our local community through our members and the Council of Governors. This strategy sets out a planned and co-ordinated approach to membership ensuring that engagement is structured within the Trust.
4.2 The strategy builds on a long tradition of putting patients and public at the centre of everything we do at the Trust, which is enshrined in our unique philosophy of care, “The Poole Approach”. “The Poole Approach” sets values and principles by which we pledge to deliver “friendly, professional, patient-centred care with dignity and respect for all”.
5 ASSOCIATED DOCUMENTS
5.1 There are no documents associated with this strategy.
6 REFERENCES
Poole Hospital NHS Foundation Trust’s provider licence: Poole Hospital NHS Foundation Trust | NHS foundation trust directory and register of licence holders | Monitor
7 CONSULTATION
7.1 Consultation and review of the strategy is undertaken with the Membership Engagement and Recruitment Group of the Council of Governors.
8 AIMS AND OBJECTIVES
8.1 The Trust aims to:
have a meaningful membership that is interested in the future of the Trust and is representative of the community we serve;
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 8 of 17
ensure that members have a say in helping us develop the future quality and type of services provided;
use our membership base to strengthen our links with the community and all stakeholders.
8.2 We will achieve this by:
Gaining new members in line with targets agreed by our Council of Governors;
ensuring that members are drawn from across our catchment area, which reflects age, gender, diversity and socio-economic groupings;
involving our members in the improvement of services and their delivery, through the Council of Governors.
9 DEFINING THE TRUST’S MEMBERSHIP
9.1 The Trust provides a wide range of acute services to people in Poole, East Dorset and Purbeck. We serve as the major trauma centre for East Dorset and provide a number of core services – ear, nose and throat, child health and maternity for a wider catchment area, including Bournemouth and Christchurch. The Trust also provides specialist services, such as oral surgery and neurological care for the whole of Dorset and is the Cancer Centre for Dorset.
9.2 The Trust employs around 4,100 staff and has over 300 volunteers.
9.3 It is important that our membership truly represents all of our stakeholders: the communities we serve, our staff and our partner organisations. Therefore our governors are drawn from our public, our staff and partnership organisations making the Trust more accountable to the people it serves.
Public Membership
9.4 Public membership is open to anyone aged 12 and over who lives in Dorset and is not employed by the Trust.
9.5 The public membership constituency is divided into four geographical areas that reflect our general, emergency and specialist catchment areas based on local authority boundaries, population numbers and patient flows. To ensure equitable representation, the number of seats on the Council of Governors allocated to each of these areas takes account of these factors.
Public Constituencies Council of Governors (no. of seats)
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 9 of 17
TOTAL 14
9.6 The 14 public seats on the Council of Governors are elected by the public members of the foundation trust.
Staff Membership
9.7 Our staff and volunteers automatically become members of the Foundation Trust unless they choose to opt out. The Council of Governor seats are split between the staff ratio of clinical and non-clinical staff.
9.8 Staff members can only be a member of a staff constituency.
Staff Constituencies Council of Governors (no. of seats)
Clinical 3
Non-Clinical 1
TOTAL 4
9.9 The four staff seats on the Council of Governors are elected by the staff members of the foundation trust.
Partnership Organisations
9.10 In addition to our elected Governors, we have invited six of our partner organisations to nominate one Governor each to sit on the Council of Governors. This reflects our close working relationships with our main commissioners of care; the Primary Care Trusts (PCTs), local authorities and Bournemouth University.
Partnership Organisations Council of Governors (no. of seats)
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 10 of 17
10 COUNCIL OF GOVERNORS
10.1 The Council of Governors is made up of a total of 23 members as detailed above. The Council forms the major link between the Trust’s Board of Directors and the foundation trust members and partner organisations.
10.2 The Council of Governors are not responsible for managing the day to day running or operational business of the Trust.
10.3 Governors are expected to promote and champion the work of the Trust within the constituencies they represent and actively seek to become engaged with issues supporting the Trust’s vision and goals. Governors are also expected to recruit new members and to publicise any Trust meetings or events.
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 11 of 17
11.1 Interested parties can join the Trust as a member by filling in the membership form held on the Trust’s website or through obtaining a printed membership leaflet.
11.2 Becoming a member is easy, free of charge and need not involve any additional time.
11.3 Members can get involved as little or as much as they want, in accordance with our governance and constitutional arrangements.
12 WHAT ARE THE BENEFITS TO BECOMING A MEMBER
12.1 Joining the Trust gives our members a voice so that they can help shape the future of Poole Hospital.
12.2 Staff members can:
access to the Trust’s newsletter via the website
access their governor through surgeries or a dedicated e-mail address
be asked for their views on future developments of the Hospital through consultation as and when available;
receive invitations via Trust communication routes to the Annual Members’ meeting
If eligible, have the opportunity to stand for election for the Council of Governors.
12.3 All public members will receive a welcome letter, the Trust’s newsletter and election papers. Public members will where they have indicated they wish to take part:
receive invitations to events and seminars including the Annual Members’ Meeting (AMM);
be asked for their views on future developments of the Hospital through consultation as and when available;
if eligible, have the opportunity to stand for election for the Council of Governors.
12.4 Members will be supporting their local hospital and will have access to their local Governor, through the Membership Office.
13 RECRUITMENT AND RETENTION OF MEMBERS
13.1 Although accountable to local communities, NHS Foundation Trusts are regulated independently by Monitor. Monitor expects foundation trusts to demonstrate that they are working to increase a representative membership and improving interaction and engagement with members.
13.2 This means that we will not simply increase numbers, but encourage a meaningful membership, which reflects the diversity, gender, age and socio economic groupings of the populations we serve.
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 12 of 17
13.3 The membership targets for recruiting public members is agreed annually by the Membership Engagement and Recruitment Group on behalf of the Council of Governors, these targets are published in the Trust’s Annual Plan which is agreed by the Board of Directors. ,
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 13 of 17
13.4 The Trust will look to maintain membership totals focussing recruitment attention on areas where representation could be improved.
13.5 By developing an engaged and representative membership, we hope that people will choose to stay with us. Most of the leavers of the Trust are members that have either moved away or who have died.
13.6 Our staff constituency is relatively stable, reflecting the comparatively low staff turnover rate for the Foundation Trust. To date no staff member has chosen to opt out of membership. We have put in place arrangements to encourage staff that are retiring to become public members by providing a leaflet within their pension packs.
14 HOW WE WILL MANAGE THE MEMBERSHIP
14.1 The Company Secretary Business Manager is responsible for leading the governors with the Membership Engagement and Recruitment Group Chairman in areas of membership recruitment, engagement and development. A bespoke database will provide efficient annual reporting to Monitor and the Trust can improve its services to members.
14.2 The Membership Engagement and Recruitment Group of the Council of Governors will meet three or four times a year to review progress annually against the Membership Strategy. This ensures that Governors are fully involved in membership development and engagement.
14.3 All members are sent copies of Foundation Talkback, our newsletter. One copy is sent per household for members living at the same address. Most members have asked to have communications by mail, although e-mail requests are proving more popular. Staff members have access to Foundation Talkback via the website. Copies are distributed widely around the Hospital for patient areas and are available electronically on our website www.poole.nhs.uk.
14.4 Communications between members and the Council are facilitated by the Membership Office. Staff Governors have a dedicated e-mail address, which is publicised in Grapevine and the intranet and they hold regular surgeries for staff.
15 HOW WE WILL DEVELOP OUR MEMBERSHIP
15.1 Our membership broadly reflects the populations we serve in terms of gender and diversity. However, as may be expected given the demographics of our local area, we have proportionally slightly more members in the female and older age groups.
15.2 Recruitment and engagement activities are recorded at the Membership Engagement and Recruitment Group through a quarterly report detailing past, current and future activity.
15.3 In order to support the recruitment and engagement plans, we will:
involve Governors more actively in membership recruitment and engagement in their constituencies through a programme of event speaking and visits to local groups and organisations. We will provide presentation materials in different formats and, if necessary, training to support Governors in this role;
place greater focus on recruiting members from the younger age groups. We will do this by working with schools, colleges and youth groups;
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 14 of 17
work with industry and commerce to try to attract more members from among the working ‘well’ adult population;
hold at least annually a Health Talk with the assistance of the Communications Department;
develop a members’ section on the new Trust website when available with an area specifically aimed at attracting younger members;
explore new and alternative ways of communicating with our members, that may be targeted at specific groups.
16 APPROVAL PROCESS
16.1 The strategy will be approved by the Board of Directors.
17 DISSEMINATION
17.1 The strategy will be disseminated to:
Governors through their meeting of the Council of Governors;
Members through the Trust’s website;
Trust Staff through the Trust’s Intranet.
18 EQUALITY IMPACT ASSESSMENT
18.1 The equality impact assessment for the Membership Development Strategy is attached as Appendix One.
19 REVIEW AND REVISION ARRANGEMENTS INCLUDING VERSION CONTROL
19.1 The Membership Development Strategy will be reviewed every three years, or earlier if required by the Membership Engagement and Recruitment Group of the Council of Governors.
19.2 Version control will be managed by the Trust’s Intranet “Web Asset Management System” (WAM), including numbering of documents to add tracking and retrieval.
20 MONITORING COMPLIANCE AND EFFECTIVENESS
20.1 Monitoring and compliance of membership will be through the Annual Plan and Annual Report to the Board of Directors and review of progress against the action plan annually by the Membership Engagement and Recruitment Group of the Council of Governors.
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 15 of 17
APPENDIX ONE - EQUALITY IMPACT ASSESSMENT
To be completed by following the Trust Equality Impact Assessment Guidance
Date of assessment
13 July 2010
Care Group or Directorate:
Communications & Marketing
Author:
Anita Bonham
Position:
Business Manager
Assessment area
Membership Service and Function
Purpose
Strategy
Objectives
To set out the Trust's plans to manage, recruit, engage and develop members of the Trust.
Intended outcomes An efficient, representative and engaged membership for the Trust in line with its Terms of Authorisation
What is the overall impact on those affected?
Ethnic Groups Gender groups
Religious Groups Disabled Persons Other
Low Low Low Low Low
Available information:
The membership database and workforce data holds information regarding gender, ethnicity and disability
Assessment of overall impact:
The inpact of the Strategy is low and is written to support a representative membership dependent on the local population. The Strategy will be available to all members and public through the Trust's website
Consultation:
Governors have been involved in the production of this document.
Actions:
The document will be reviewed by the Council of Governors and Board of Directors
Cog Jan 14 H 2 Revised Membership Development Strategy Strategy
CS01 Version 4.0
Date: September 2013 Author: Co Sec Business Manager Page 18 of 17
Title of document being reviewed:
Y/N/ Unsure
Comments
20. Process to Monitor Compliance and Effectiveness
Are there measurable standards or KPI's to support the monitoring of compliance with and effectiveness of the document?
Y
Is there a plan to review or audit compliance within the document?
Y
21. Format and Style
Does the document follow the correct style and format of the Document Control Procedure?
Y
22. Overall Responsibility for the Document
Is it clear who will be responsible for co-ordinating the dissemination, implementation and review of the documentation?
Y
Individual Approval
If you are happy to approve this document, please sign and date it and forward to the chair of the committee/group where it will receive final approval.
Job Title Company Secretary Date May 2011
Print Name Michael Beswick Signature
Committee Approval
If the committee is happy to approve this document, please sign and date it and forward copies for inclusion on the Intranet.
Council agreed to bring forward its public meetings from 5.30pm to 4.30pm. The revised meeting calendar reflects this change and the impact on other meeting start times.
Recommendation:
The Council of Governors receive the revised 2014 Meeting Calendar
Purpose: To report on performance against key indicators for the Trust in November 2013.
Summary:
Financial Performance The Trust has incurred a deficit of £81k in November despite increased levels of donated income. This reduces the surplus for the 8 months to £160k compared to plan of £142k. The Trust is continuing to forecast a surplus of £0.2m for year but the Trust is now operating with a recurring deficit which is currently being off-set by non-recurring and non-cash generating benefits. The Trust will require additional transitional funding in 2014/15 to off-set this under-lying deficit and the impact of another year of real reductions in NHS funding. The local commissioners have confirmed that some additional, transitional funding will be available and discussions will continue during the coming months. However at this stage, on current projections, it is likely that the Trust will have a monthly deficit from April of up to £0.5m per month. The underlying deficit is already having an impact on the Trust’s cash reserves which have fallen from £15m at the start of the year to £9.4m in November and are projected to fall further to £8m by the end of the year. Clinical Performance & Quality The Monitor A&E metric (95% within 4 hours) was achieved in November (95.6%). RTT standards for admitted and non-admitted clock stops were met for November at aggregate level. Stroke performance was achieved in November. The Breast Screening service achieved 3 of the 4 targets. There were no Mixed Sex Accommodation (MSA) breaches in November.
There was one C-Diff case identified in November, the year to date total is five which is within the planned level for the year of 19. The MRSA year to date total for 2013-14 is remains one, following the identification of a case in October. The DM01 based diagnostic target was achieved, as 1% or less of patients were waiting more than six weeks at month end. All the cancer standards have been confirmed as achieved in October, the most recent period available. The 48 hour operating target (95%) was achieved in November for fractured Neck of Femur (NoF) and Trauma patients. The remaining NoF targets were not met in November. The monthly delayed discharges snapshot for November was 4.18%.
Recommendation:
For discussion and noting.
Prepared
by:
PAUL TURNER Director of Finance / KATE THOMAS Performance Manager /SOPHIE JORDAN Operations & Performance Manager
Presented
by:
PAUL TURNER Director of Finance JACKIE NICKLIN/BARBARA PEDDIE Joint Acting Chief Operating Officer MARTIN SMITS Director of Nursing SARAH-JANE TAYLOR HR Director
Assurance
Framework:
YES Risk
Register I/D
No:
Healthcare Standards:
Please specify which standard/
standards that apply;
CQC Standard (Please provide details:
Other; i.e /NHSLA/HSE etc Monitor compliance: YES
Human Resources implications NO Financial implications YES
Legal implications NO
Please ensure all boxes are completed in order to comply with national requirements
FINANCE 1.1 The Trust has incurred a deficit of £81k in November despite increased levels of donated income. This
reduces the surplus for the 8 months to £160k compared to plan of £142k.
1.2 The Trust is continuing to forecast a surplus of £0.2m for year but the Trust is now operating with a recurring deficit which is currently being off-set by non-recurring and non-cash generating benefits.
1.3 The Trust will require additional transitional funding in 2014/15 to off-set this under-lying deficit and the impact of another year of real reductions in NHS funding. The local commissioners have confirmed that some additional, transitional funding will be available and discussions will continue during the coming months. However at this stage, on current projections, it is likely that the Trust will have a monthly deficit from April of up to £0.5m per month.
1.4 The underlying deficit is already having an impact on the Trust’s cash reserves which have fallen from £15m at the start of the year to £9.4m in November and are projected to fall further to £8m by the end of the year.
WORKFORCE
1.5 The Trust workforce metrics are rated green except for staff turnover (Auxilliaries and HCA) ;
Staff Turnover (overall) at 0.85%, (7.24% year to date) rated green
Staff Turnover (Auxiliaries and HCA) at 1.35%, (year to date 12.62%) red rated
Staff sickness at 3.81%, (3.45% year to date) rated green 1.6 Appraisal recorded on ESR shows an improved picture at 71%. 1.7 Temporary staffing levels remain high primarily due to bed pressures and the need to have planned additional
capacity to support winter pressures. HIGHLIGHTS
1.8 The Monitor A&E metric (95% within 4 hours) was achieved in November (95.6%). RTT standards for
admitted and non-admitted clock stops were met for November at aggregate level.
1.9 The DM01 based diagnostic target was achieved, as less than 1% of patients were waiting more than six weeks at month end.
3 Endoscopy patient waiting > 6 weeks;
30 Radiology patients waiting > 6 weeks;
1 Urodynamic patient waiting > 6 weeks. 1.10 There was one C-Diff case identified in November, the year to date total is five which is within the planned
level for the year of 19. 1.11 There were no Mixed Sex Accommodation (MSA) breaches in November. 1.12 Stroke performance was achieved in November. 1.13 The overall hospital standardised mortality rate (HSMR) for the Trust was 91.7, within the target of 100, and
1.14 RTT targets were met. However at speciality level for non-admitted, Urology, Ophthalmology, Trauma & Orthopaedics and Neurology failed to meet the 90% target due to back log clearance. Looking forward, further breaches are expected in the surgical specialties where capacity has been insufficient to meet demand and backlogs have developed.
1.15 All cancer standards were met in October. However, there remain challenges in achieving the 62 day wait for first treatment and also the two week wait breast symptomatic target.
1.16 ASIs continued to exceed the 10% local target during November (17%). This has been due to both demand and capacity.
1.17 The 48 hour operating target (95%) was achieved in November for fractured Neck of Femur (NoF) and Trauma patients. The following NoF targets were not met in November:
87% operated on within 36 hours of being deemed clinically appropriate (95% target)
77% operated on within 36 hours of admission (90% target)
1.18 The MRSA year to date total for 2013-14 remains one, following the identification of a case in October. 1.19 The monthly delayed discharges snapshot for November was 4.18% (target <3.5%), this was mainly due to
inability to place self funding patients.
1.20 The Breast Screening target was achieved for 3 of the 4 targets; the metric for screening to actual attendence was not met due to temporary reduced capacity.
The Patient Experience scorecard is comprised of six key indicators; three of these are part of the Monitor scorecard. For the most recent year to date position (November 2013)
C-Diff
See Monitor section
MRSA
The MRSA year to date total for 2013-14 remains one. This metric is no longer part of the monitor framework (RAF), but would still be subject to Monitor scrutiny in the event of an outbreak or sudden increase in cases.
Action: Infection Control issues remain under continued scrutiny by DoN/Infection Control.
Mixed Sex Accommodation (MSA)
There have been no occurrences of mixed sex accommodation (MSA) breaches in November.
Venous Thromboembolism (VTE)
VTE performance for November was 96.85%, continuing to achieve the 2013/14 target of 95%.
Patie
nt E
xp
erie
nc
e S
co
recard
Key Issue
Overview RAG Sch
Clinical Quality
The Clinical Quality scorecard is comprised of five key indicators, none of which are part of the Monitor scorecard. For the most recent year to date position (September/ November 2013) there are red rated indicators relating to SUIs only.
Mortality
During the three month period ended September 2013, (the latest information available from the Dr Foster information service) the overall hospital standardised mortality rate (HSMR) for the Trust was 91.7, within the target of 100, and an improvement on the previous month.
Mortality performance for September 2013 has been green rated as both the overall and HSMR number of deaths was less than the expected level calculated by Dr Foster.
An audit has now been undertaken. The Mortality group will continue to ensure that;
o cases with a zero or very low co-morbidity rating are reviewed ; o deaths are reviewed by clinicians; o pneumonia remains under scrutiny.
Serious Untoward Incidents
There was 1 SUI identified in November; this was reported within the prescribed timescale. (Figures reported prior to August are not comparable with those reported in subsequent months. )
Efficiency The Efficiency scorecard is comprised of four key indicators; none of these are part of the Monitor scorecard. For the most recent year to date position (September/ November 2013) there are two red rated indicators:
Theatre Utilisation (Performance Report Appended)
Main theatre utilisation (86%) achieved the 85% target in November.
Day theatre utilisation did not achieve 80% target (77%). Bed Occupancy
Average bed occupancy in November was 98%, and did not meet the internal target of 95%. Daycase Rate
The day case rate for September was 78.4%, achieving the 75% target.
Effic
ien
cy S
co
reca
rd
Workforce Indicators
The Workforce Indicator Scorecard (Appended) comprises of eight key measures of HR performance
Staff Turnover (overall) at 0.85%, (7.24% year to date) rated green
Staff Turnover (Auxiliaries and HCA) at 1.35%, (year to date 12.62%) red rated
Staff sickness at 3.81%, (3.45% year to date) rated green
Finance & Activity
The Trust has incurred a deficit of £81k in November despite increased levels
of donated income. This reduces the surplus for the 8 months to £160k
compared to plan of £142k.
The Trust is continuing to forecast a surplus of £0.2m for year but the Trust is
now operating with a recurring deficit which is currently being off-set by non-
recurring and non-cash generating benefits.
The Trust will require additional transitional funding in 2014/15 to off-set this
under-lying deficit and the impact of another year of real reductions in NHS
funding. The local commissioners have confirmed that some additional,
transitional funding will be available and discussions will continue during the
coming months. However at this stage, on current projections, it is likely that
the Trust will have a monthly deficit from April of up to £0.5m per month.
The underlying deficit is already having an impact on the Trust’s cash reserves
which have fallen from £15m at the start of the year to £9.4m in November and
are projected to fall further to £8m by the end of the year.
4. OPERATIONS SUMMARY ~ NOVEMBER 2013 (For the period of 1st to 30th November 2013)
ACTIVITY
4.1 This report summarises various operational aspects year to date. The performance information relates to actual activity rather than a comparison against contract.
4.2 There is no significant in month variance to the non-elective admissions year to date.
4.3 Attendances in the Emergency Department have marginally decreased by 0.8% YTD compared to the same period last year. There was a 5% decrease in attendances in November 2013 compared to previous year.
4.4 Elective activity continues to steadily increase, with 3.7% more elective admissions and the day case rate increasing by 3.6%.
4.5 The number of Maternity admissions have reduced YTD by 9.6%. This is due to a
reclassification of admitted activity to outpatient within the Antenatal Day Assessment Unit. 4.6 Paediatric non-elective admissions have decreased in month by 4.4% YTD, 12-13 activity
was excessively high over the summer period in 2012-13 and is now settling down to normal activity levels for the spring/summer period.
4.7 The variance in Trust activity (YTD) is summarised below
4.10 The graph below shows the average length of stay for children (elective and non-elective).
4.11 The graph below shows the average LOS for Maternity, the increase from July 2013 reflects the reclassification of short stay ANDA inpatients as outpatient attendances.
4.12 The percentage of time the Trust is in a red bed state is a clear indication of how pressurised the whole system is. The Hospital was in a red bed state for 53% of the time during November 2013.
4.13 The percentage of patients formally delayed on the last Thursday of November 2013 (DH reporting methodology) was 4.18%, 0.68% over Trust target. This is an improvement on October performance of 4.7%. The Trust has experienced a high number of delays in month with a number of complex discharges requiring escalation to partner agencies.
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
Apr May June July Aug Sept Oct Nov Dec Jan Feb Mar
% Delayed Transfers of Care From Acute Beds including Paediatrics
Yr13/14
Yr12/13
Yr11/12
4.14 Delays during November were due to: Self-Funding patients (36%), Social Services (20%),
Community Hospitals (19%), Angiography/Angioplasty at RBCHFT (14%), CHC assessment process (6%) and Intermediate Care (5%). Actions continue to be progressed on a continuous basis to improve delays overall and tackle the main causes of delays.
4.15 The total number of bed days lost during November (503) due to patients waiting for transfer to an alternative provider has improved compared to October 2013 (737).
CANCELLATIONS All Waiting List Cancellations
4.16 The number of Elective admissions cancelled as a percentage of all elective admissions decreased to 15.4% in month compared to 17.2% recorded in October 2013. This mirrors the trend in 12/13.
4.21 The readmission rate is calculated by dividing the number of discharges that were followed by an emergency readmission within 30 days by total number of discharges (excluding deaths).
4.22 The table below shows the readmission rates by specialty from August 2012 to date.
Discharging spec ialty of
or iginal admiss ion Oc t-12 Nov -12 Dec -12 Jan-13 Feb-13 Mar-13 Apr -13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oc t-13
Grand Total 4.2% 4.1% 4.5% 4.3% 4.1% 4.4% 4.3% 4.4% 4.1% 4.1% 4.0% 4.5% 4.5%
Month of Discharge of Or iginal Admiss ion
4.23 There are significant readmission rates in October (>10%) within Accident and Emergency
(10.4%), Cardiology (10.8%), General Medicine (10.4%) and Geriatric Medicine (10.7%). This is being monitored closely by the Directorate teams to ensure safe discharging is in place.
APPENDIX 1 ~ REFERRAL TO TREATMENT (RTT) EXCEPTION REPORT
Prepared by: Kate Thomas, Trust Performance Manager November 2013
PERFORMANCE REPORT – NOVEMBER 2013
Summary of Risk: The NHS Operating Framework 2012-13 RTT operational standards are:
- Non-admitted target: 95% of RTT periods where patients received their first definitive treatment in an outpatient (non-admitted) setting must be completed within 18 weeks of referral.
- Admitted target: 90% of RTT periods where the patient needs to be admitted (as an inpatient or day case) for their first definitive treatment must be completed within 18 weeks of referral.
- Incomplete target: 92% of patients who have not yet started treatment should have been waiting no more than 18 weeks (patients who have had a clock start but have not had a clock stop).
Within the PHFT contract with the CCG, it is expected that each of the main specialties achieves all three targets at specialty level. All remaining ‘sub-specialties’ are grouped together into a category ‘X01’; this category must be achieved at aggregated level.
Current position: The Trust RTT position at the end of November 2013:
At aggregate and Unify specialty level, all specialties passed the admitted target for November 2013. The non -admitted target was not achieved in Urology (92.5%), Trauma & Orthopaedics (92.9%), Ophthalmology (90.5%) or Neurology (89.9%).
At the Trust Weekly Performance meeting, monitoring at patient level continues of all patients waiting over 26 weeks for treatment, and the reasons for the pathway delays.
Actions
The Performance Team has reviewed the position on the four specialties that did not achieve the non-admitted target in November. Urology and neurology have now cleared the recent backlog, but T&O and Ophthalmology have been identified as having challenges in December and beyond. Urology (92.5% non-admitted): The backlog has now been cleared, and urology should achieve RTT in December. Trauma & Orthopaedics (92.9% non-admitted): There are still a number of long waiters booked to be seen and as this looks likely to exceed 5% of average months clock stops it is anticipated that T&O may not achieve the 95% target in January/February. Ophthalmology (90.5% non-admitted): The Directorate Manager has been working closely with RBCH to put in place a plan to alleviate the pressures. Despite this work, it is anticipated that the specialty will breach the non-admitted target in December and January due to the number of patients waiting over 18 weeks in the weeks preceding the additional activity. Neurology (89.9% non-admitted): The backlog has now been cleared, and neurology should achieve RTT in December.
Pressures regarding waiting times for CT/MRI scans and the time taken to receive the CT scan report continue to be challenging; this is being managed in conjunction with the radiology department.
APPENDIX 2 ~ CANCER WAITING TIMES EXCEPTION REPORT
Prepared by: Anne Foulkes, Business & Performance Manager November 2013
October All targets were achieved in October The main challenges for the Trust for performance in the quarter, Q3 2013/14 are
Achievement of the 62-day (2WW Referral To Treatment) Wait For First Treatment: All in Quarter 3 13/14 (Oct – Dec) remains challenging. It is anticipated that October and November will be narrowly achieved but there are a high number of potential breaches in December which could put the quarter at risk due to a number of multifactorial factors – complex pathway, patient compliance, cross trust referrals. Close monitoring of individual patients along the pathway continues.
Provisional results to date indicate that the 14 day target from Receipt of Referral to 1st appointment for patients with Non-cancer Breast Symptoms target was not met in November. The best estimate of the number of breaches in the month is 6 - All breaches have been due to patient choice. The average number of breaches that can be carried in a quarter is 10, with 9 already reported for the quarter to date, no more than 1 breach can be carried in December and the target still achieved. Other Trusts are being contacted to establish what processes are in place elsewhere to identify any shared learning
APPENDIX 3 ~ EMERGENCY DEPARTMENT PROFESSIONAL STANDARDS EXCEPTION REPORT
Prepared by: Martin Smith/Matt Welch, Matron/Directorate Manager/ Assistant Manager November 2013
The Risk: The 4-hour target for November was met at 95.64% (which gave a Quarter Three performance at that stage, of 95.77%.) The remaining professional standards are monitored on a weekly basis and reported to the Trust’s performance meeting. Whilst the standards do not carry Monitor weighting, they are a key gauge for quality within the department. The performance for November and Quarter 3 (current position) is outlined below:
Performance has been mixed across the range of performance standards. ‘Clinician seen time’ and ‘Total time in department’ have unfavourably increased; overall performance has also decreased. There was a pattern of concentrated high attendances in late evening, which caused significant pressures on all measures.
Current Position and Actions:
Medical staffing has been improved and will continue to improve in the short-term as new registrars and junior
doctors arrive. Work is still on-going to ensure that staff are working at the most appropriate times to ensure
resilience in the event of unusually high attendances.
Action:
Two Consultants were interviewed and appointed in December, they will take up post in Q4.
Changes made to the registrar rota to ensure better coverage and sustainability.
Extra Nurse Practitioner shifts, paid for by the Urgent Care Board funding, began in late November.
In progress:
Review of consultant job plans and rotas to provide maximum cover across the 24-hour period.
Identification of future days with likely high attendance in order to provide better staffing cover.
Mandy Tanner, General Manager Radiology Ian Sprigmore, General Manager Obstetrics and Gynaecology
November 2013
The Risk: 34 patients in total were not seen within six weeks from the date of referral for their diagnostic test.
Current Position: Urodynamics There was 1 patient waiting over six weeks at the end of November. This was due to patient having a UTI therefore test postponed. Gynaecology General Manager has made visits to peripheral hospitals to ensure all patients are tested for UTI’s prior to referral for urodynamic investigation. Wimborne Hospital is compliant however Swanage and Blandford currently non-compliant. Radiology There were 30 patients waiting over six weeks at the end of November. This is comprised of 10 Ultrasounds and 20 MRI patients. This has been largely due to the long-term sickness absence of a Consultant Radiologist which resulted in a reduction of lists in ultrasound. Consultant absence also resulted in reduced capacity to report MRI scans. Endoscopy There were 3 patients (2 active surveillance and 1 patient choice) waiting six weeks and over at the end of November (one end of month breach in October). There were 431 patients on the waiting list as at 30th November (327 at the end of October) and over 97% of patients referred to the department are being seen within six weeks - with very few exceptions. There have been continuing pressures on the waiting lists during November due to on-going issues with the endoscopy washers; as a result, a number of patients have been cancelled in November, and rebooked within the 6 week target. This has mainly affected OGD and flexible-sigmoidoscopies as the department was reluctant to cancel any colonoscopies. In addition we have seen a rise in flexi-sigmoidoscopies from an average of around 66-70 per week in September / October to an average of 95 a week in November.
Total loss of washer capacity on site has resulted in all scopes being washed in the Harbour, RBCH or Wimborne. The Department have managed extremely well in the short term –the Business case for the purchase of three new washers was signed off and the new washers were delivered on 9
th December. It is
planned that these washers will be up and running by the end of January 2014.
Building work in the Endoscopy department has commenced and should be completed by the beginning of February 2014. Due to this and the on-going issues with the scopes, activity will be reduced during this time resulting in our waiting list numbers continuing to rise.
Action: Continue to closely monitor the waiting list and in particular review USS/MRI demand and review
compliance with Urodynamics pathway referrals from peripheral sites.
APPENDIX 5 ~ STROKE TARGET EXCEPTION REPORT: ≥80% OF PATIENTS SHOULD SPEND >90% OF THEIR LOS ON THE STROKE UNIT
Prepared by: Barry Duell, Deputy General Manager – Medicine, DMfE & Specialist Services
November 2013
The Risk: The Trust has achieved this target month by month in year.
Current Position:
In November there were 46 Stroke patients discharged during the month, with 89% (41) of patients spending > 90% of their LOS on the Stroke Unit (target ≥ 80%).
The following table indicates the number of live Stroke discharges and the % that achieved the target in the previous months.
November
The Trust has maintained this target for the last year.
Direct access dropped slightly in November to 86% (37 patients). There were 5 cases of non-direct access via Ansty & A3 and 1 patient that also required Trauma care, all of which we believe were appropriate at the time. There will be no follow up on these patients.
CT scan access <24 hours for November was 93% (40 patients), target 100%.
In November the TIA service saw 52 referrals, with 32 (61%) being classed as high risk.
We saw, treated and investigated 18 (56%) of these within the required 24 hours. A large number of patients were received as late referrals by SPOA and would have been managed within the required time if we had received timely referrals. This will be brought up with the CCG at the next commissioning meeting in February.
Actions:
1. Consolidation and review of ward reconfiguration.
2. Substantive Stroke and Geriatric Consultant posts are currently out to advert.
Prepared by: Barry Duell/Yvonne Hunter/David Clark/Hannah Elton
Directorate Managers – Medical, Surgical & Child Health Directorates
November 2013
Appointment Slot Issue (ASI): Trust performance for November was 17%
Summary: Provider to ensure that ‘sufficient appointment slots’ are made available on the Choose and Book system. Standard: <4% slot availability issues. The Trust risks fines for every week >10%. Current Position: At end of November 2013, the Trust position was 17%. Rheumatology: Polling at 12 weeks. 120 ASI. Orthopaedic All: Polling at 6 weeks. 74 ASI. Ophthalmology Adult: Polling at 8 weeks. 30 ASI. Orthopaedic Paeds: Polling at 9 weeks. 16 ASI. Colorectal: Polling at 7 weeks. 11 ASI. Gastroenterology: Polling at 12 weeks. 34 ASI. Respiratory: Polling at 9 weeks. 35 ASI. Breast: Polling at 2 weeks. 19 ASI. General Surgery: Polling at 6 weeks. 24 ASI. Urology: Polling at 12 weeks. 29 ASI.
Actions for November/December 2013:
Rheumatology:
ASI concerns reported to Deputy COO & COO for discussion at CCG performance meetings. CCG remain appraised of continuing impact of increased referral rates on departmental capacity. PHT and CCG aware of over performance against 2012/13 totals.
Locum Consultant Dr Asim Kurshid commenced in post on October 7th. Clinics have been opened
since October 14th. Discussions will now commence regarding substantive post in department and a
business case will be developed to support this.
New OP clinic being set up to take place on Friday am. This will be advertised on C&B. Template for Thursday pm also reviewed and new slots made available.
SpR in post working 3 days per week (full time between RBCH and PHT).
ESP cover continues to cover unmet SpR clinics, sessions remain on choose and book.
Agreement to return routine pain referrals to their GP to be managed in the community. Rheumatology pathways and capacity may continue to be adversely affected by Pain Clinic referrals until the community service has commenced.
Resignation of Lead Practitioner (Nursing) and planned sickness for Dr Paul Thompson will add difficulty to the management of patients within their 18/52 pathway. Some nursing sessions will be covered in-house to try and reduce impact.
Orthopaedic (all):
Slightly reduced number of ASI’s in November, in part due to temporary increase in polling range. However, this will need to be reduced again because of the negative impact it will have on patient pathways post first appointment.
RBH are still willing to receive referrals of patients who cannot be seen here without a delay for their first appointment but in spite of putting on additional clinics the capacity there is also currently full.
Overall Trauma Orthopaedics is running at 21.8% OPD attendance above the contracted level (24.2% for new patients, 119.5% for follow ups and this is causing considerable pressure on both fracture and elective services.
The CCG are aware of the increase in Trauma Orthopaedics and are due to visit the Trust on 24 December when this is one of the specialties due to be discussed.
Currently working with RBH to reinstate unplanned lost adult capacity and to rectify the issue of new patient slots being used for follow ups.
Orthopaedic (Paeds):
A reduction in ASI’s to 16 in the month of November, in part due to increasing the polling range back to ten weeks, which is only a temporary measure.
This service is led by one consultant only with middle grade support and consultant leave has an adverse effect on the ability to see new patients and new patient activity in this sub-specialty has been slightly reduced because of recent leave.
Two theatre lists in the new Year are going to be converted to OPD clinics with the expectation of reducing waiting times slightly and bringing the polling range back to nine weeks.
Gastroenterology:
34 ASI in November caused by some adjacent annual leave taken by Medical staff. No visible increase in referral numbers. Capacity and demand work being undertaken will highlight any opportunity to review service provision.
Respiratory:
Dr Mallawathantri leaves her post in December. Clinical slots are now closed causing an approximate 30% reduction in capacity across the service until new staff are in post.
Breast:
ASI’s in the breast service are mainly due to the 2 week polling range, the days that patients access choose and book and the capacity at that precise time. When the ASI’s are booked manually if capacity is running as planned, which it was in November, and there are not excessive referrals there is usually no issue with booking these patients within 2 weeks.
General Surgery:
Total of 24 ASI’s in November, only one of which came in during the last week. General Surgery does not routinely feature with high numbers of ASI’s and in November was due in the main to the effect of the Christmas Bank Holidays on capacity during the polling range for the period concerned.
Urology:
Slight increase in number of ASI’s this month.
Small reduction in capacity in November due to last minute notification of study leave by RBH led to rebooking of some new patients and reduction in slots then available on choose and book. Due to current screening programme in Urology RBH unable to replace clinic until January.
Specialty currently 16.7% above contract for new patients and 6.4% above contract for follow ups.
Prepared by: Yvonne Hunter, General Manager – Trauma & Orthopaedics
November 2013
Trauma Targets- Waiting Times for Surgery: Fractured Neck of Femur within 36 hours of being clinically appropriate for surgery (CCG target 95%) Fractured Neck of Femur within 36 hours of admission (Best Practice Tariff Criteria – internal target 90%) Trauma Patients within 48 hours of being deemed fit for surgery (CCG target 95%) Compliance with the theatre quality and access targets remains vulnerable and can be affected by prolonged periods of high activity, daily fluctuations in the demand, the mix of patients, the pattern of admissions or any combination of these.
November Position: *87% of Fractured Neck of Femur operated on within 36 hours of being deemed clinically appropriate (96% were operated on within 48 hours of being deemed clinically appropriate and 70% within 24 hours.) *77% of Fractured Neck of Femur operated on within 36 hours of admission *95% of all Trauma and NOF patients operated within 48 hours of being fit for surgery The graph below shows the performance over the past year against the number of acute Trauma admissions.
The Service went into escalation for at least 7 days in November due to an increase in admissions, additional theatre lists were created, including an extra all day Sunday list to clear the backlog of patients and prevent a more prolonged period of escalation. In total 17 fractured necks of femur patients breached the target for surgery within 36 hours of admission The reasons for not achieving the targets are in the table below,
Patients not fit pre-op & needed optimising
Other trauma/NOF cases taking priority
Insufficient theatre capacity – 7 NOF’s admitted in 24hr period
Awaited specialist surgeon for THR/complex surgery
Actions: To continue with all the current practices around prioritising fractured neck of femur patients, breach avoidance/breach management for individual patients and highlighting crucial patients and their breach times to surgeons and to theatres. To continue to undertake a review of each breach in detail and highlight any changes required as a result. Ortho-geriatricians working with the TAC Team to review in detail the patients who are not fit on admission and require optimising prior to surgery, in particular looking at protocols around patients admitted with high INR’s (see medical breaches above). Maintain the on-going review of trauma demand vs. theatre capacity following the busy summer months and moving into what is usually a quieter winter period to inform future decisions re provision of theatre capacity.
The Risk: Day Theatres is not reaching the 80% target.
Current Position:
Previous calculations have shown that best achievement for Day Theatres ranges between 80 and 82%. This is based on the number of patients that is reasonable to put on each session which range from 2 patients to 6 patients. Based on these levels of activity it is impossible for every list to achieve 85% as any list with three patients or more is already unable to achieve the target. Working on the potential operating time available for each list based on the number of cases utilisation would be expected: 2 patients excluding team brief and turnaround time – 92% 3 patients - 89% 4 patients – 85% 5 patients – 82% 6 patients – 79% Based on the above matrix utilisation available for November 2013 was 84% Day Theatre reached 78% utilisation for November 2013 which is 1% increase in utilisation compared to October 2013.
Day Theatre utilisation This quarter (Q3)
Previous quarter
(Q2)
Sept 13 Oct 13 Nov 13
% % % %
OVERALL 77 77 76 OVERALL 77
ENT 73 74 72 ENT 73
General surgery 85 88 78 General surgery
85
Gynae 80 80 77 Gynae 80
OMF 73 74 76 OMF 73
Trauma 76 72 76 Trauma 76
80% and above 79% - 76% 75% and below
Graph 1 shows the total utilisation in Day Theatres. There is now a break down by speciality. Comparisions are made quarter on quarter with movement in efficiency shown. All specialities with the exception of Trauma.
Graph 2 shows the number of patients that were booked for total sessions and the number of completed patient episodes. The patient cancellations on the day for this month were 0.8% which is within the agreed acceptable level of 2%.
Graph 3 shows the percentage of time lost across total sessions in Day Theatres as indicated by the reasons on the chart and the movements, month on month and quarter on quarter. Again as with last month there were a number of short notice absences due to sickness of Anaesthetists. Both the Anaesthetic Department, Surgeons and Theatres worked hard to minimise any cancellations.
Actions:
- Review the management of emergency gynae cases added to elective lists
- Provide ENT Consultant with all day surgery list in main theatre once every four weeks
- review the principles of the Enhanced Recovery Programme for General Surgery and consider
APPENDIX 9 ~ DELAYED TRANSFER OF CARE - EXCEPTION REPORT
Prepared by: Sophie Jordan Head of Operations
December 2013
Target: The National Target is to achieve under 3.5% of formal Delayed Transfers of Care (DToC)
Current Position: The monthly snapshot showed 4.18% Delayed Transfers of Care. This was an improvement on last months performance of 4.70%, however there remain a number of actions to ensure the Trust achieve this target with support from partner agencies. The table below shows a breakdown of the delays:
Description of delay Bed days lost in month Percentage of all in month delays
Self Funding 181 36%
Social Services 103 20%
Community Hospitals 95 19%
Angiography/Angioplasty 68 14%
Continuing Health Care 29 6%
Intermediate Care 27 5%
The graph below shows the performance of the Trust against the target since April 2011
Actions:
1. Daily reporting of formal and informal delays to partner agencies, which are discussed in detail after the 1000 bed meeting. Issues escalated on the day by senior staff.
2. Self Funding Social Worker in place for Poole Borough Council. 3. Review of the Interim Orthopaedic pathway in collaboration with CCG lead and Social Service leads. 4. Link Discharge Co-ordinator Group established to share good practice across the wards. 5. Urgent Care Board agreement in principle to support a 3 month pilot of a Band 7 CHC lead nurse to
support wards and the pathway from January 2014 6. Winter planning initiatives in place since October/November include, additional access to step up/step
down beds, Social Worker presence on wards in evenings (1700-1900), access to night service. 7. Agreement to keep packages of care open up to 5 days on assessment units
APPENDIX 10 ~ DORSET BREAST SCREENING UNIT (DBSU) EXCEPTION REPORT
Prepared by: Shirley Langdon,
November 2013
Current Position
The DBSU failed to meet one target in November 2013. This was the date of attended appointment.
Background The 3 year screening round is planned for all women to be invited for screening within 34-36 months. Changes to the round would impact on achieving round length targets across the round. Additional support was requested and supported from the COO however there was no capacity within Radiology for additional hours to be given to BS and Radiologists were unable to cover sufficient additional sessions to impact on achieving the target.
Actions for November/December 2013:
Screening to attended appointment: The unit achieved 80% screening to date of first attended appointment (National Minimum Standard is 90% within 3 weeks). 91% of women were offered an assessment appointment within 3 weeks of attending their screening appointment
Explanation:
Extended unplanned sick leave of a Consultant Radiologist and a Consultant Radiographer affected film reporting and assessment clinic capacity. Additional support was requested and approved but there was no capacity within Radiology for additional hours to be given to BS and Breast Radiologists were unable to cover sufficient additional sessions.
Continuing staff shortages in the A+C staff affected the efficiency of A+C processes (1wte long term sick, 1wte vacancy and 1wte managing performance /investigation). Requesting previous films for reporting and making assessment appointments take priority over other tasks which affect achieving the target however reporting normal results (for screen to RR target) and processes to maintain the functioning of the BS service (round length target) still have to be done in a timely way. The A+C work associated with postponing clinics would be counterproductive in terms of work required to cancel and rebook the numbers of women involved and would also affect the round length target .
The Consultant Radiographer returned to work on a phased return, work was assigned to her with support from HR however she had further unplanned sick leave resulting in an assessment clinic being cancelled. The four women in this clinic were rebooked within the same week but were then more than 3 weeks from their date of screening
Of the 20 women assessed at four weeks nine women changed their appointment due to patient choice, four were rebooked because of cancellation of a clinic due to unplanned sick leave and six were due to slower processing of tasks due to A+C staff shortages. One woman received her invitation letter after her appointment.
Next Steps:
- Interim support staff have been appointed to A&C staff and new appointments to A&C start in January 2014.
- Consultant Radiographer has now resumed normal workload.
- Additional Radiologist sessions agreed until March 2014.
To present the updated Register of Interests for the Council of Governors.
Summary:
The Council of Governor register of interest is to be reviewed annually in line with the anniversary of becoming a foundation trust. Should governors have any changes to the register at anytime they are to inform the Company Secretary function for noting at the next Council of Governor meeting.
Recommendation:
The Council of Governors are asked to note the register of interests.
18-week target Delivery of a maximum 18-week wait from GP referral to start of treatment (RTT)
A & E Accident and Emergency
A&GC Audit & Governance Committee
AfC Agenda for Change is the pay system for NHS staff implemented in 2004. A summary of the system is available on the Department of Health website
AHPs Allied Health Professionals – physiotherapists, occupational therapists, speech therapists and orthotists. Previously PAMs (Professions Allied to Medicine)
AIRS Adverse Incident Recording System – the Trust’s no-blame system for reporting all clinical and non-clinical adverse incidents and near misses
AQP Any Qualified Provider – this scheme means that, for some conditions, patients will be able to choose from a range of approved providers, such as hospitals or high street service providers.
ASI Appointment Slot Issue
ASU Acute Stroke Unit
c.difficile Clostridium difficile - the major cause of antibiotic-associated diarrhoea and colitis, an intestinal infection that mostly affects elderly patients with other underlying diseases.
CEA Clinical Excellence Awards - given to recognise and reward the exceptional contribution of NHS consultants, over and above that normally expected in a job, to the values and goals of the NHS and to patient care
CHKS CHKS is a national independent provider of comparative performance and benchmarking healthcare data
CEPOD CEPOD (Confidential Enquiry into Perioperative Death) lists are theatre lists specifically dedicated for the provision of emergency surgery
CHC Continuing Healthcare
CIP Cost Improvement Plan
CMT Clinical Management Team
CoG The Council of Governors comprises:
14 public governors who are elected by members of their own constituency – Poole (8); Purbeck, East Dorset & Christchurch (3); Bournemouth (2); North Dorset, West Dorset , Weymouth & Portland (1);
4 staff governors who are elected by members of Trust staff – clinical (3); non-clinical (1);
6 appointed governors nominated by the Trust’s partner organisations – Bournemouth & Poole PCT (1); Dorset PCT (1); Dorset County Council (1); Poole Borough Council (1) Bournemouth Borough Council (1); Bournemouth University (1).
CQC The Care Quality Commission is the independent regulator of health and social care in England. The CQC regulates health and adult social care services, whether provided by the NHS, local authorities, private companies or voluntary organisations, and protects the rights of people detained under the Mental Health Act
CQUIN Commissioning for Quality and Innovation - the CQUIN payment framework makes a proportion of providers' income conditional on quality and innovation. Its aim is to support the vision set out in High Quality Care for All of an NHS where quality is the organising principle. The framework was launched in April 2009 and helps ensure quality is part of the commissioner-provider discussion everywhere.
CRES Cost Releasing Efficiency Saving
CRT Clinical Record Tracking – a bar-code based system for recording the location of patients’ medical records.
DATIX National software programme for Risk Management
DME Department of Medicine for the Elderly
Dr Foster Dr Foster Intelligence, a joint venture between the Department of Health’s Information Centre and a private sector company Dr Foster LLP. Dr Foster provides a range of health information to the public (online and via supplements in the national media) and makes NHS performance data available under licence to health sector organisations
DToC Delayed Transfer of Care
EBITDA Earnings Before Interest, Taxation, Depreciation and Amortisation
EBME Electrical, Biomedical Equipment
ENT Ear, Nose and Throat
ESR Electronic Staff Record - the national, integrated Human Resources (HR) and Payroll system used by all NHS organisations throughout England and Wales. The ESR has a bi-directional interface with NHS Pensions. Personal data for all staff will be transferred to a data warehouse. This will include contact details, salary information, HR records, trainings, qualification, occupational health and other records. It will also include sensitive information such as sickness record absence, disabilities, ethnic origin
EWTD European Working Time Directive - lays down minimum requirements in relation to working hours/rest periods/annual leave for all workers and working arrangements for night workers. The current limit is an average of 48 hours work per week.
FCE Finished Consultant Episode is a measurement which assigns a patient’s episode of care to a consultant
FFCE First Finished Consultant Episode identifies the first consultant episode of care during a patients hospital stay
FIC Finance & Investment Committee
Foundation Trust/FT
NHS foundation trusts are autonomous organisations, free from central Government control. They decide how to improve their services and can retain any surpluses they generate, or borrow money, to support these investments. They establish strong connections with their local communities; local people can become members and governors. These freedoms mean NHS foundation trusts can better shape their healthcare services around local needs and priorities. NHS foundation trusts remain providers of healthcare according to core NHS principles: free care, based on need and not ability to pay. Poole Hospital NHS Foundation Trust was authorised on 1 November 2007
FRP Financial Recovery Plan.
H@N Hospital at Night - the provision of multi disciplinary teams working in hospital Out of Hours who between them have the full range of skills and competencies to meet patients’ immediate needs
HDU High Dependency Unit, for patients requiring close monitoring and high levels of care but not life support
HR Human Resources
HRG Healthcare Resource Group – groupings of treatment episodes which are similar in resource use and in clinical response
HSE Health & Safety Executive
ICU or ITU Intensive Care Unit or Intensive Therapy Unit
I&E Income and Expenditure
IT or IM&T Information Technology or Information Management & Technology
KSF Knowledge & Skills Framework - identifies the knowledge and skills that individuals need to apply in their post. Used to provide a fair and objective framework on which to base review and development for all staff
LNC Local Negotiating Committee – the main management/medical staff forum
Monitor The independent regulator of NHS Foundation Trusts. Monitor rigorously assesses applicants for NHS foundation trust status and subsequently monitors their activities to ensure that they comply with the requirements of their terms of authorisation. Monitor has powers to intervene in the running of a foundation trust in the event of failings in its healthcare standards or other aspects of its activities, which amount to a significant breach in the terms of its authorisation
Mortality rate The ratio of total deaths to total population in a specified community or area over a specified period of time. The death rate is often expressed as the number of deaths per 1,000 of the population per year.
MRSA Methicillin Resistant Staphylococcus Aureus – an antibiotic resistant infection commonly found on the skin and/or in the noses of healthy people. Although usually harmless at these sites, it may occasionally get into the body (eg through breaks in the skin such as abrasions, cuts, wounds, surgical incisions or indwelling catheters) and cause infections. These infections may be mild (eg pimples or boils) or serious (eg infection of the bloodstream, bones or joints). An infection of the bloodstream is called a bacteraemia
MSC Medical Staff Committee
NCEPOD NCEPOD (National Confidential Enquiry into Perioperative Death) lists are theatre lists specifically dedicated for the provision of emergency surgery
NHSLA National Health Service Litigation Authority – the NHS clinical “insurance” scheme
NICE National Institute for Health & Clinical Excellence
NICU Neonatal Intensive Care Unit
NPfIT National Programme for Information Technology
NPSA National Patient Safety Agency
NSF National Service Framework - sets national standards and identifies key interventions for a defined service or care group. Also sets measurable goals within specified time frames.
NREC Nominations, Remuneration & Evaluations Committee - a sub-committee of the CoG responsible for the making recommendations to the CoG regarding the appointment, remuneration and performance review of the Chairman and non-executive directors
NVQ
National Vocational Qualification
OMF Oral Maxillo Facial
OFT Office of Fair Trading
PA/SPA Programmed Activities and Supporting Professional Activities. PAs identify medical staff clinical sessional commitments. SPAs are defined as “activities that underpin direct clinical care. This may include participation in training, medical education, continuing professional development, formal teaching, audit, job planning, appraisal, research, clinical management and local clinical governance activities.”
PACS Picture Archiving and Communications System – the digital storage of x-rays
PALS Patient Advice and Liaison Service - provide information, advice and support to help patients, families and their carers
PBC Practice Based Commissioning – an initiative which enables clinicians and other front line staff to redesign services that better meet the needs of their patients
PbR Payment by Results - the funding system for the NHS in England. This pays a standard tariff for the treatment of different conditions. Not all hospital activity is funded by PbR and hospitals still have to negotiate “block funding” to cover these areas – eg. diagnostic and screening tests.
PCT Primary Care Trust. The two local PCTs are now known as NHS Bournemouth & Poole and NHS Dorset.
PEAT Patient Environment Action Team - PEAT team Inspections are a national initiative coordinated by the Department of Health
PFI Private Finance Initiative
PEWS Poole Early Warning System – a system to identify and alert staff of the deteriorating patient based on scoring patient observations against a number of criteria. Patients causing ‘alarm’ are reviewed by the nurse in charge of the ward and an emergency call made to switchboard requesting attendance of a member of the patients medical team or on call team
PHFT Poole Hospital NHS Foundation Trust
PMETB Postgraduate Medical Education and Training Board
PMO Programme Management Office
PROM Patient Recorded Outcomes Measures
PTIP Post Transaction Implementation Plan
PYLL Potential Years of Life Lost
QIPP The Quality, Innovation, Productivity and Prevention Programme. This is about ensuring that each pound spent is used to bring maximum benefit and quality of care to patients.
QSP Quality, Safety and Performance Committee
RBH Royal Bournemouth & Christchurch Hospitals NHS Foundation Trust
RCI/Reference costs
Reference Cost Index – reference costs are the average cost to the NHS of providing a defined service within a given financial year. The RCI compares the actual cost of activity with the same activity at national average costs - organisations with costs equal to the national average score 100 whilst an organisations with a score of 80 or 115 has costs 20% below/ or 15% above the national average. The RCI is used for benchmarking and as the basis of PbR
RTT Referral to Treatment. The current RTT Target is 18 weeks.
Self-funding patients
This relates to patients who are not eligible for funding of future long-term care due to personal assets over the agreed threshold of £23,250, therefore they are deemed to be responsible for funding their care themselves.
SHA Strategic Health Authority – NHS South West is one of the ten Strategic Health Authorities in England formed on 1 July 2006
SLA Service Level Agreement - a SLA is an agreement that sets out formally the relationship between service providers and customers for the supply of a service by one or another.
SLM Service Line Management
SLR Service Line Report
SMR Standardised Mortality rate – see Mortality Rate
SpR Specialist Registrar – medical staff grade below consultant
SPF Staff partnership Forum – the main management/ staff forum, previously known as the JCNC (Joint Negotiating & Consultation Committee)
SUI Serious Untoward Incident
TAL
NHS Direct provides The Appointments Line service as part of the Choose & Book system. Choose and Book is the electronic hospital appointments booking system. It allows people to make their first outpatient appointment online, at their GP practice, or by calling the Appointments Line (TAL). Patients can choose the place, date and time of the appointment to suit them.