Page 1
KANE COUNTY CASTRO, Davoust, Kenyon, Molina, Smith, Taylor, Vazquez
HUMAN SERVICES COMMITTEE
WEDNESDAY, NOVEMBER 19, 2014
County Board Room Agenda 9:00 AM
Kane County Government Center, 719 S. Batavia Ave., Bldg. A, Geneva, IL 60134
Kane County Page 1
1. Call to Order
2. Approval of Minutes: October 22, 2014
3. Monthly Financial Reports
A. October Human Services Committee Financial Reports (attached)
4. Veteran's Assistance Commission
A. VAC Report (attached)
B. Veteran Events (attached)
5. Department of Human Resource Management
A. Monthly EEO graphs and reports (attached)
B. Health Insurance Changes and Collections (attached)
6. Old Business
7. New Business
A. Resolution: Approving Contract for Employee Assistance Provider (Metropolitan Family Services)
B. Resolution: Amending Personnel Policy Handbook (Insurance Benefits)
C. Resolution: Amending and Restating County of Kane Flexible Benefits Plan
8. Reports Placed On File
9. Executive Session
10. Resolution: Establishing Annual Salary for Executive Director of Human Resource Management (Sheila D. McCraven) (not included) 11. Adjournment
Page 2
Current Month Transactions
Total Amended Budget
YTD Actual Transactions
Total % Received
660 Veterans' Commission 10,854 340,976 301,663 88.47%380 Veterans' Commission 10,854 340,976 301,663 88.47%
Grand Total 10,854 340,976 301,663 88.47%
Human Services Committee Revenue Report - SummaryThrough October 31, 2014 (91.7% YTD)
Packet Pg. 2
Page 3
Current Month Transactions
Total Amended Budget
YTD Actual Transactions
YTD Encumbrances
Total % Used
120 Human Resource Management 130,975 2,431,141 2,642,144 1,178 108.73%001 General Fund 9,832 414,210 321,106 256 77.58%010 Insurance Liability 121,142 2,016,931 2,321,038 922 115.12%
660 Veterans' Commission 14,064 340,976 247,917 55 72.72%380 Veterans' Commission 14,064 340,976 247,917 55 72.72%
Grand Total 145,039 2,772,117 2,890,062 1,233 104.30%
Human Services Committee Expenditure Report - SummaryThrough October 31, 2014 (91.7% YTD, 92.31% Payroll)
Packet Pg. 3
Page 4
Current Month Transactions
Total Amended Budget
YTD Actual Transactions
YTD Encumbrances
Total % Used
120 Human Resource Management 130,975 2,431,141 2,642,144 1,178 108.73%001 General Fund 9,832 414,210 321,106 256 77.58%
Personnel Services- Salaries & Wages 8,158 295,731 247,230 0 83.60%Personnel Services- Employee Benefits 1,674 77,118 44,147 0 57.25%Commodities 0 4,662 4,705 256 106.41%Contractual Services 0 36,699 25,024 0 68.19%
010 Insurance Liability 121,142 2,016,931 2,321,038 922 115.12%Personnel Services- Salaries & Wages 5,274 138,183 110,145 0 79.71%Personnel Services- Employee Benefits 1,566 45,215 31,384 0 69.41%Commodities 0 600 282 0 47.03%Contractual Services 114,303 1,827,270 2,179,227 922 119.31%Contingency and Other 0 5,663 0 0 0.00%
660 Veterans' Commission 14,064 340,976 247,917 55 72.72%380 Veterans' Commission 14,064 340,976 247,917 55 72.72%
Personnel Services- Salaries & Wages 6,558 176,606 150,175 0 85.03%Personnel Services- Employee Benefits 2,882 78,703 62,961 0 80.00%Commodities 54 11,890 2,279 55 19.63%Contractual Services 4,570 72,703 32,502 0 44.70%Capital 0 1,074 0 0 0.00%
Grand Total 145,039 2,772,117 2,890,062 1,233 104.30%
Human Services Committee Expenditure Report - DetailThrough October 31, 2014 (91.7% YTD, 92.31% Payroll)
Packet Pg. 4
Page 5
Vendor Invoice No. Invoice Description Status Held Reason Invoice Date Due Date G/L Date Received Date Payment Date Invoice AmountFund 001 - General Fund
Department 120 - Human Resource ManagementSub-Department 120 - Human Resource Management
Account 52130 - Repairs and Maint- Computers3854 - Identisys 227786 ID equipment supplied Paid by Check
# 34100809/24/2014 09/29/2014 09/29/2014 10/06/2014 101.70
Account 52130 - Repairs and Maint- Computers Totals Invoice Transactions 1 $101.70Account 55000 - Miscellaneous Contractual Exp
1299 - Kane County Regional Office of Education
0000008636 fingerprinting August 2014
Paid by Check # 341127
09/09/2014 09/29/2014 09/29/2014 10/06/2014 280.00
Account 55000 - Miscellaneous Contractual Exp Totals Invoice Transactions 1 $280.00Account 60010 - Operating Supplies
2291 - Chicago Office Technology Group (COTG)
347155 Quarterly Maintenance 6/19-9/19/14
Paid by EFT # 24674
09/19/2014 09/18/2014 09/18/2014 10/06/2014 128.92
Account 60010 - Operating Supplies Totals Invoice Transactions 1 $128.92Account 60020 - Computer Related Supplies
8771 - Smartgroup Systems 26328 HP inkjet cartridge Paid by EFT # 24809
09/10/2014 09/29/2014 09/29/2014 10/06/2014 48.00
Account 60020 - Computer Related Supplies Totals Invoice Transactions 1 $48.00Account 60050 - Books and Subscriptions
6441 - Emergency Closing Center 3097-09/2014 emergency closing Paid by Check # 340979
09/29/2014 09/29/2014 09/29/2014 10/06/2014 25.00
Account 60050 - Books and Subscriptions Totals Invoice Transactions 1 $25.00Sub-Department 120 - Human Resource Management Totals Invoice Transactions 5 $583.62
Department 120 - Human Resource Management Totals Invoice Transactions 5 $583.62Fund 001 - General Fund Totals Invoice Transactions 5 $583.62
Fund 010 - Insurance LiabilityDepartment 120 - Human Resource Management
Sub-Department 130 - Insurance Liability- HRMAccount 50000 - Project Administration Services
8258 - CCMSI 0083703-IN claims and admin fee - September 2014
Paid by Check # 340920
09/23/2014 09/29/2014 09/29/2014 10/06/2014 6,291.67
Account 50000 - Project Administration Services Totals Invoice Transactions 1 $6,291.67Account 50150 - Contractual/Consulting Services
1248 - Kinnally Flaherty Krentz & Loran PC 5301-00/16 (PMK) Special Asst State's Attny
Paid by Check # 341285
09/30/2014 10/07/2014 10/07/2014 10/20/2014 2,327.50
Account 50150 - Contractual/Consulting Services Totals Invoice Transactions 1 $2,327.50Account 53000 - Liability Insurance
8258 - CCMSI 2014-00001228 Workers Comp Claims Paid by EFT # 25286
10/07/2014 10/07/2014 10/07/2014 10/07/2014 72,797.03
3171 - Strypes Plus More, Inc. 12602 Vehicle and Auto Repair-Squad 61
Paid by EFT # 25028
09/12/2014 10/08/2014 10/08/2014 10/20/2014 140.00
3171 - Strypes Plus More, Inc. 12601 Auto Repair-squad 95 Paid by EFT # 25028
09/12/2014 10/08/2014 10/08/2014 10/20/2014 100.00
Run by Finance Reports on 11/04/2014 10:04:08 AM Page 1 of 3
Human Services Accounts Payable by GL Distribution
Payment Date Range 10/01/14 - 10/31/14
Packet Pg. 5
Page 6
Vendor Invoice No. Invoice Description Status Held Reason Invoice Date Due Date G/L Date Received Date Payment Date Invoice AmountFund 010 - Insurance Liability
Department 120 - Human Resource ManagementSub-Department 130 - Insurance Liability- HRM
Account 53000 - Liability Insurance1016 - Wine Sergi & Co LLC 68329 Notary Bond -Katie
HellerPaid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
1016 - Wine Sergi & Co LLC 68330 Notary Bond-Elena Fuentes
Paid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
1016 - Wine Sergi & Co LLC 68331 Notary Bond-Jennifer Vazquez
Paid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
1016 - Wine Sergi & Co LLC 68332 Notary Bond-Janet Halsey
Paid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
1016 - Wine Sergi & Co LLC 68333 Notary Bond-Angela Knorr
Paid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
1016 - Wine Sergi & Co LLC 68334 Notary Bond-Janice Gabreleski
Paid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
1016 - Wine Sergi & Co LLC 68335 Notary Bond-Btittany Hankes
Paid by EFT # 25049
10/01/2014 10/08/2014 10/08/2014 10/20/2014 25.00
Account 53000 - Liability Insurance Totals Invoice Transactions 10 $73,212.03Account 53010 - Workers Compensation
8258 - CCMSI 2014-00001229 Workers Comp Payment
Paid by EFT # 25287
10/15/2014 10/15/2014 10/15/2014 10/15/2014 17,394.50
Account 53010 - Workers Compensation Totals Invoice Transactions 1 $17,394.50Account 53020 - Unemployment Claims
3594 - Illinois Department of Employment Security
91914 Illinois Unemployment Underpayment
Paid by Check # 341011
09/19/2014 09/25/2014 09/25/2014 10/06/2014 1,811.16
Account 53020 - Unemployment Claims Totals Invoice Transactions 1 $1,811.16Sub-Department 130 - Insurance Liability- HRM Totals Invoice Transactions 14 $101,036.86
Department 120 - Human Resource Management Totals Invoice Transactions 14 $101,036.86Fund 010 - Insurance Liability Totals Invoice Transactions 14 $101,036.86
Fund 380 - Veterans' CommissionDepartment 660 - Veterans' Commission
Sub-Department 660 - Veterans' CommissionAccount 52140 - Repairs and Maint- Copiers
8930 - Impact Networking, LLC 412806 Copy Overage 09/2014 Paid by EFT # 24731
09/19/2014 09/19/2014 09/19/2014 10/09/2014 10/06/2014 8.76
Account 52140 - Repairs and Maint- Copiers Totals Invoice Transactions 1 $8.76Account 53100 - Conferences and Meetings
9019 - Jacob Zimmerman 91214 Conference Paid by Check # 341119
09/12/2014 09/19/2014 09/19/2014 10/06/2014 15.00
Account 53100 - Conferences and Meetings Totals Invoice Transactions 1 $15.00
Run by Finance Reports on 11/04/2014 10:04:08 AM Page 2 of 3
Human Services Accounts Payable by GL Distribution
Payment Date Range 10/01/14 - 10/31/14
Packet Pg. 6
Page 7
Vendor Invoice No. Invoice Description Status Held Reason Invoice Date Due Date G/L Date Received Date Payment Date Invoice AmountFund 380 - Veterans' Commission
Department 660 - Veterans' CommissionSub-Department 660 - Veterans' Commission
Account 53110 - Employee Training4526 - Fifth Third Bank 8705 JZ - 09/14 Credit Card Payment Paid by EFT #
2469409/04/2014 09/25/2014 09/25/2014 09/26/2014 10/06/2014 35.00
Account 53110 - Employee Training Totals Invoice Transactions 1 $35.00Account 53120 - Employee Mileage Expense
9019 - Jacob Zimmerman 91214 Conference Paid by Check # 341119
09/12/2014 09/19/2014 09/19/2014 10/06/2014 198.24
Account 53120 - Employee Mileage Expense Totals Invoice Transactions 1 $198.24Account 55000 - Miscellaneous Contractual Exp
9346 - 212 Healy St Properties, LLC M3742-0914 Rent Assistance (T.M.) Paid by EFT # 24645
09/18/2014 10/02/2014 09/19/2014 09/22/2014 10/06/2014 400.00
1054 - ComEd 6423230046 09/14
Electric Assistance (T.B.)
Paid by Check # 340955
09/19/2014 10/13/2014 09/29/2014 09/25/2014 10/06/2014 19.13
9502 - Alejondra Hurtado H3212-0914 Rent Assistance (J.H.) Paid by EFT # 24722
09/11/2014 09/25/2014 09/19/2014 09/19/2014 10/06/2014 580.00
9408 - KP Ventures LLC M3751-0914 Rent Assistance (R.M.) Paid by EFT # 24743
09/11/2014 09/26/2014 09/19/2014 09/19/2014 10/06/2014 400.00
1054 - ComEd 5586551078-0914
Electric Bill (M.C.) Paid by Check # 341184
09/19/2014 10/13/2014 10/02/2014 10/02/2014 10/20/2014 32.64
5228 - Harbor Village Apartments C4052-1014 Rent Assistance (M.C.) Paid by Check # 341249
10/02/2014 10/23/2014 10/02/2014 10/09/2014 10/20/2014 137.00
9408 - KP Ventures LLC M3751-1014 Rent Assistance (R.M.) Paid by EFT # 24958
10/09/2014 10/23/2014 10/14/2014 10/14/2014 10/20/2014 400.00
Account 55000 - Miscellaneous Contractual Exp Totals Invoice Transactions 7 $1,968.77Account 60000 - Office Supplies
4526 - Fifth Third Bank 8705 JZ - 09/14 Credit Card Payment Paid by EFT # 24694
09/04/2014 09/25/2014 09/25/2014 09/26/2014 10/06/2014 28.13
1024 - Ice Mountain Direct 14I8106647400 September Water Service
Paid by EFT # 24937
10/02/2014 10/22/2014 10/02/2014 10/06/2014 10/20/2014 10.55
3578 - Warehouse Direct Office Products 2460003-0 Office Supplies Paid by EFT # 25046
10/02/2014 11/02/2014 10/02/2014 10/03/2014 10/20/2014 43.31
Account 60000 - Office Supplies Totals Invoice Transactions 3 $81.99Sub-Department 660 - Veterans' Commission Totals Invoice Transactions 14 $2,307.76
Department 660 - Veterans' Commission Totals Invoice Transactions 14 $2,307.76Fund 380 - Veterans' Commission Totals Invoice Transactions 14 $2,307.76
Grand Totals Invoice Transactions 33 $103,928.24
Run by Finance Reports on 11/04/2014 10:04:08 AM Page 3 of 3
Human Services Accounts Payable by GL Distribution
Payment Date Range 10/01/14 - 10/31/14
Packet Pg. 7
Page 8
Vendor Invoice No. Invoice Description Status Held Reason Invoice Date Due Date G/L Date Received Date Payment Date Invoice AmountFund 120 - Grand Victoria Casino Elgin
Department 010 - County BoardSub-Department 020 - Riverboat
Account 45420 - Tuition Reimbursement4326 - Keith Berkhout 11142013 tuition reimbursement
Self-study for Realtor License-4 courses
Paid by Check # 334728
11/14/2013 11/19/2013 11/19/2013 12/02/2013 80.00
4648 - Daniel Eder 11142013 tuition reimbursement: Marketing of healthcare svcs.
Paid by Check # 334795
11/14/2013 11/19/2013 11/19/2013 12/02/2013 2,360.00
5321 - Michelle Halbesma 11142013 tuition reimbursement: Criminal Justice Administration
Paid by Check # 334820
11/14/2013 11/19/2013 11/19/2013 12/02/2013 2,560.00
9018 - Suzanna Lindsey 11192013 tuition reimbursement: Statistical Literacy
Paid by Check # 334887
11/19/2013 11/19/2013 11/19/2013 12/02/2013 1,735.00
1863 - Matthew Nelson 11142013 tuition reimbursement: Learn More Spanish
Paid by Check # 334910
11/14/2013 11/19/2013 11/19/2013 12/02/2013 129.00
8081 - AMANDA K PATRICOSKI 11142013 tuition reimbursement: Research Methods/Theories of Human Develo
Paid by Check # 334930
11/14/2013 11/19/2013 11/19/2013 12/02/2013 3,450.00
8828 - Ayesha Tague 11142013 tuition reimbursement: Learn More Spanish
Paid by Check # 334981
11/14/2013 11/19/2013 11/19/2013 12/02/2013 129.00
8040 - Kelly R. Wiggins 11142013 tuition reimbursement: Learn More Spanish
Paid by EFT # 20564
11/14/2013 11/19/2013 11/19/2013 12/02/2013 129.00
9261 - Vanessa Aguirre 01022014 reimburse tuition Paid by Check # 335636
01/02/2014 01/02/2014 11/30/2013 01/13/2014 1,960.00
5321 - Michelle Halbesma 01022014 reimburse tuition Paid by Check # 335739
01/02/2014 01/02/2014 11/30/2013 01/13/2014 1,920.00
8795 - Marisa Hanczar 01022014 reimburse tuition Paid by Check # 335740
01/02/2014 01/02/2014 11/30/2013 01/13/2014 3,840.00
4290 - LaTanya Hill 01022014 reimburse tuition Paid by EFT # 21008
01/02/2014 01/02/2014 11/30/2013 01/13/2014 1,725.00
9020 - Christopher Janovsky 01022014 reimburse tuition Paid by Check # 335774
01/02/2014 01/02/2014 11/30/2013 01/13/2014 1,026.99
4856 - Tim Mescher 01022014 reimburse tuition Paid by Check # 335801
01/02/2014 01/02/2014 11/30/2013 01/13/2014 360.00
9007 - Michael Roehr 01022014 reimburse tuition Paid by Check # 335837
01/02/2014 01/02/2014 11/30/2013 01/13/2014 3,486.00
5395 - Arlene Ryndak 01022014 reimburse tuition Paid by EFT # 21055
01/02/2014 01/02/2014 11/30/2013 01/13/2014 849.00
4463 - Julie Wiegel 01022014 reimburse tuition Paid by Check # 335883
01/02/2014 01/02/2014 11/30/2013 01/13/2014 2,360.00
4789 - Rosio Mendez 01212014 tuition reimbursement - Ethics & Integrity
Paid by Check # 336110
01/21/2014 01/13/2014 11/30/2013 01/27/2014 2,220.00
Run by Finance Reports on 11/04/2014 10:05:32 AM Page 1 of 3
Tuition Reimbursement YTDPayment Date Range 12/01/13 - 10/31/14
Packet Pg. 8
Page 9
Vendor Invoice No. Invoice Description Status Held Reason Invoice Date Due Date G/L Date Received Date Payment Date Invoice AmountFund 120 - Grand Victoria Casino Elgin
Department 010 - County BoardSub-Department 020 - Riverboat
Account 45420 - Tuition Reimbursement8315 - Isabel Ocon 01212014 tuition reimbursement -
Policy PaperPaid by Check # 336133
01/21/2014 01/13/2014 11/30/2013 01/27/2014 1,920.00
8081 - AMANDA K PATRICOSKI 01162014 reimburse tuition 2 classes Practice I & Practice II
Paid by Check # 336143
01/16/2014 01/13/2014 11/30/2013 01/27/2014 3,450.00
7091 - LISA TARQUINIO 01162014 tuition reimbursement - Criminology
Paid by EFT # 21229
01/16/2014 01/13/2014 11/30/2013 01/27/2014 2,220.00
9021 - KRYSTA M KAUS 01272014 tuition reimbursement - 2 classes
Paid by Check # 336405
01/27/2014 01/30/2014 11/30/2013 02/10/2014 1,900.00
5053 - Salvador Rodriguez 01272014 tuition reimbursement/Criminal Justice in America
Paid by Check # 336463
01/27/2014 01/30/2014 11/30/2013 02/10/2014 2,160.00
8634 - CRAIG K CAMPBELL 02142014 tuition reimbursement Paid by EFT # 21447
02/14/2014 02/10/2014 02/10/2014 02/24/2014 2,360.00
9018 - Suzanna Lindsey 1407-01 LAS-105 Intro to Sociology
Paid by Check # 337286
03/05/2014 03/06/2014 03/06/2014 03/24/2014 1,735.00
8081 - AMANDA K PATRICOSKI 1401-01 SWK-6382 Practice II: Community
Paid by Check # 337325
03/12/2014 03/06/2014 03/06/2014 03/24/2014 1,458.34
8634 - CRAIG K CAMPBELL 1303-01 MBA500-Financial Accounting
Paid by EFT # 22017
03/28/2014 03/31/2014 03/31/2014 04/07/2014 2,360.00
4648 - Daniel Eder 1406-01 MPH 657 Disater Management in Public Health
Paid by Check # 337498
03/24/2014 03/31/2014 03/31/2014 04/07/2014 2,360.00
7194 - THOMAS F ROSEBUSH 1302-01 PSF5600-Public Safety Leadership
Paid by Check # 337638
03/18/2014 03/31/2014 03/31/2014 04/07/2014 1,892.00
9020 - Christopher Janovsky 1405-01 CAHC 500 Professional Identity and Ethics in Counseling
Paid by Check # 338898
05/12/2014 06/10/2014 06/10/2014 06/16/2014 1,026.99
4463 - Julie Wiegel 1404-01 MPH 611 Public Health Biology
Paid by Check # 339029
05/12/2014 06/10/2014 06/10/2014 06/16/2014 2,360.00
4565 - Anthony Franklin Sr. 1304-01 SEC-592 IT Governance
Paid by EFT # 23247
06/18/2014 06/24/2014 06/24/2014 06/30/2014 2,298.00
8315 - Isabel Ocon 1409-01 CRJ 5070-Criminal Justice Administration
Paid by Check # 339229
05/24/2014 06/24/2014 06/24/2014 06/30/2014 2,400.00
9007 - Michael Roehr 1403-01 PP8060-Group Psychotherapy
Paid by Check # 339250
06/09/2014 06/24/2014 06/24/2014 06/30/2014 2,400.00
8634 - CRAIG K CAMPBELL 1303-4 MGMT 612 -Methods of Org Research
Paid by EFT # 23431
05/23/2014 07/07/2014 07/07/2014 07/14/2014 2,360.00
5321 - Michelle Halbesma 1412-01 CRJ-6950 CBSA;Thesis Prep
Paid by Check # 339409
06/23/2014 07/07/2014 07/07/2014 07/14/2014 1,920.00
Run by Finance Reports on 11/04/2014 10:05:32 AM Page 2 of 3
Tuition Reimbursement YTDPayment Date Range 12/01/13 - 10/31/14
Packet Pg. 9
Page 10
Vendor Invoice No. Invoice Description Status Held Reason Invoice Date Due Date G/L Date Received Date Payment Date Invoice AmountFund 120 - Grand Victoria Casino Elgin
Department 010 - County BoardSub-Department 020 - Riverboat
Account 45420 - Tuition Reimbursement5053 - Salvador Rodriguez 1305-01 CRJ-5030
Design/Analysis CJ Research
Paid by Check # 339515
06/24/2014 07/07/2014 07/07/2014 07/14/2014 2,160.00
5053 - Salvador Rodriguez 1411-01 CRJ-5050 Crime Causation Theory
Paid by Check # 339515
06/24/2014 07/07/2014 07/07/2014 07/14/2014 2,160.00
4835 - Ryne McGill 1410-01 CRIMJ-2240-025 Juvenile Delinquency
Paid by Check # 339742
06/22/2014 07/22/2014 07/22/2014 07/28/2014 420.00
8634 - CRAIG K CAMPBELL 1303-05 MBA671-Strategic Management
Paid by EFT # 23838
08/01/2014 08/05/2014 08/05/2014 08/11/2014 2,360.00
4565 - Anthony Franklin Sr. 1408-01 SEC-591 Disaster Recovery/Forensics & Security
Paid by EFT # 23877
08/01/2014 08/05/2014 08/05/2014 08/11/2014 2,298.00
7194 - THOMAS F ROSEBUSH 1413-02 PSF5602 Leadership & Human Resource Management
Paid by Check # 340028
07/28/2014 08/05/2014 08/05/2014 08/11/2014 1,892.00
6021 - Richard A. Grenda 1418-01 EDU6505 The Teacher Leader's Role in Pro. Dev.
Paid by Check # 340182
08/11/2014 08/19/2014 08/19/2014 08/25/2014 1,410.00
8795 - Marisa Hanczar 1414-01 CRJ3610WI-01 Research Methods
Paid by Check # 340188
08/08/2014 08/19/2014 08/19/2014 08/25/2014 1,960.00
4504 - Karen Ann Miller 1415-01 2014 Planning Law Review
Paid by EFT # 24114
08/11/2014 08/19/2014 08/19/2014 08/25/2014 175.00
6258 - Steven Jones 1422-01 CRJ6300 Proactive Police Administration
Paid by Check # 340465
08/25/2014 08/29/2014 08/29/2014 09/08/2014 1,695.00
9021 - KRYSTA M KAUS 1423-01 EDUC5140 Comparative & International Education
Paid by Check # 340469
08/15/2014 08/29/2014 08/29/2014 09/08/2014 2,850.00
4835 - Ryne McGill 1410-02 CRIMJ-1152-060 Criminal Law
Paid by Check # 340487
08/11/2014 08/29/2014 08/29/2014 09/08/2014 840.00
8081 - AMANDA K PATRICOSKI 1401-02 SWK 6801-01 Professional Writing
Paid by Check # 340516
08/22/2014 08/29/2014 08/29/2014 09/08/2014 941.66
4364 - Judith Bland 1417-01 40th NOVA Conference Paid by EFT # 24427
09/10/2014 09/11/2014 09/11/2014 09/22/2014 245.00
8634 - CRAIG K CAMPBELL 1421-02 MGMT581 & MGMT582 Paid by EFT # 24873
10/10/2014 10/14/2014 10/14/2014 10/20/2014 2,360.00
Account 45420 - Tuition Reimbursement Totals Invoice Transactions 51 $92,665.98Sub-Department 020 - Riverboat Totals Invoice Transactions 51 $92,665.98Department 010 - County Board Totals Invoice Transactions 51 $92,665.98
Fund 120 - Grand Victoria Casino Elgin Totals Invoice Transactions 51 $92,665.98Grand Totals Invoice Transactions 51 $92,665.98
Run by Finance Reports on 11/04/2014 10:05:32 AM Page 3 of 3
Tuition Reimbursement YTDPayment Date Range 12/01/13 - 10/31/14
Packet Pg. 10
Page 11
Kane County Purchasing Card Information
Human Services Committee
October 2014 Statement
Transaction Date Merchant Name Additional Information Transaction Amount
Department Total
Committee Total
Page 1 of 111/5/2014 Packet Pg. 11
Page 12
Veterans Assistance Commission Claims Synopsis
Table 1: Disability Claims Processing Times
Table 2: Number of Disability Claims Pending at Chicago VA Regional Office
370
304.9 302.2 261 241.7 276.2
298.4 293.5
289.7
289.3 290.2
273.5 261.2 247.5 239.2 226 220.9
216.1 209.3
182
165.6
158.3
0
50
100
150
200
250
300
350
400
VA Processing Time
VAC Processing Time
VA's Goal
12,613
12,822
9,601
8,884
8,924 8,845
10,239 10,465 11,346
12,469 12,090
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
Claims Pending
Packet Pg. 12
Page 13
VETERANS ASSISTANCE COMMISSION CLAIM REPORT
Category December January February March April May June July August September October November FY 2014 Total
Service Connected Disability Claims 16 17 19 17 28 18 17 20 21 13 17 203
Non-Service Connected Disability Claims 5 6 12 9 4 16 13 10 6 5 7 93
Dependent's Compensation Claims 1 0 1 6 0 1 0 0 1 0 1 11
Widow's Pension Claims 0 4 2 6 4 5 5 4 2 3 2 37
VA Monetary Awards 92,730.39$ 102,257.04$ 97,204.74$ 95,955.07$ 174,766.52$ 207,109.19$ $1,853,064.88
VCAA Response / Follow up 9 6 7 8 13 8 17 7 10 2 6 93
Total Forms Completed 109 160 148 158 207 154 140 132 145 89 146 1,588
Claims Decision Reviews 11 19 10 19 22 11 12 15 17 19 22 177
Total Claims Pending 196 217 236 240 210 228 206 219 226 213 227
Appeals Filed 1 1 1 0 1 0 1 3 0 0 2 10
Dependent Ancilliary Benefit Claims 0 4 0 5 1 0 0 0 1 0 11
Burial Benefits Applications 0 3 3 0 3 3 3 0 5 0 3 23
VA Home Loan / Insurance Applications 0 0 0 0 3 0 0 0 3 0 2 8
DD-214 / Military Records Request 5 18 9 20 22 8 9 7 25 15 11 149
Discharges Entered into VAC Database 8 17 18 2 22 15 1 1 11 33 5 133
Correction / Upgrade of Military Records 0 1 0 2 0 1 0 1 0 1 1 7
Federal Veterans Education Applications 0 1 1 0 0 1 0 0 0 0 1 4
State Veterans Education Applications 0 1 3 0 1 1 0 0 0 0 0 6
Veterans Health Care Applications 3 9 2 9 8 4 1 3 3 1 0 43
State War Bonus Applications 3 6 5 0 4 3 0 0 1 0 1 23
VAC Outreach Events 9 7 4 10 6 12 5 11 6 14 7 91
THROUGH APRIL $1,083,041.93
Packet Pg. 13
Page 14
VETERANS ASSISTANCE COMMISSION FAP REPORT
Category Dec 13 Jan 14 Feb 14 Mar 14 Apr 14 May 14 Jun 14 Jul 14 Aug 14 Sep 14 Oct 14 Nov 14 Year Totals
Shelter $980 $1,864 $1,048 $1,725 $1,600 $1,200 $1,780 $1,200 $1,805 $1,405 $1,142 $15,748
Gas Utility $36 $0 $64 $0 $193 $0 $46 $0 $0 $0 $17 $356
Electrical Utility $17 $41 $106 $0 $116 $117 $54 $0 $51 $19 $109 $630
Water/Waste Water/Garbage $0 $0 $32 $0 $0 $0 $78 $47 $0 $0 $0 $157
Heat $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
Food $50 $75 $200 $0 $0 $50 $0 $125 $175 $125 $275 $1,075
Personal Needs $25 $50 $125 $0 $50 $25 $25 $125 $150 $25 $200 $800
Telephone $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
Medical $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
Emergency Aid $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
Transportation $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
Burial $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $900 $900
FAP Applications Issued 10 9 16 11 4 5 9 7 6 6 4 87
FAP Applications Received 5 3 7 9 5 0 3 3 1 2 7 45
FAP Approved 0 3 1 3 1 2 2 2 3 0 1 18
FAP Renewed (Assessments) 3 2 3 1 4 3 3 3 5 5 5 37
FAP Denied 3 2 1 7 5 7 2 2 1 3 8 41
Dependents Assisted 2 4 3 0 0 0 2 3 5 3 7 29
Referrals to Other Agencies 35 17 16 19 22 35 27 26 6 19 39 261
VAC Correspondence 17 16 13 37 104 175 54 40 92 37 84 669
Veterans Transported 6 12 16 21 19 19 21 1 0 1 7 123
Monthly Mileage 379 439 626 886 742 888 633 74 0 51 146 4,864
Packet Pg. 14
Page 15
Join us for monthly programs to provide information on a varying range of topics dealing with Veterans and to meet and discuss with other Veterans. Co�ee and hot tea will be served.No registration.
MedicareThursday, November 20South Elgin Room7 - 8:30 pm
veterans information networking session
www.gailborden.info
Dependent BenefitsThursday, December 18South Elgin Room7 - 8:30 pm
Packet Pg. 15
Page 17
Edward Hines, Jr. VA HospitalVeterans Food Pantry
The Greater Chicago Food Depository in partnership with Hines VA Hospital and AmeriCorps, is providing food for those who served.
What:
Who:
When:
Where:
On-site food pantry that provides nutritious and healthy food for Veterans.
Veterans Veterans will be asked to provide identification (examples include: VA ID card, DD214 & photo ID, VA appointment slip & photo ID).
Every Thursday from 11 a.m. to 1 p.m. (Starting November 6)Veterans can access the food pantry once per month.
Hines VA HospitalAuditorium LobbyBuilding 9
For more information, please contact the Food Pantry Coordinator Mark Eaglebarger at [email protected] or Hines VA Social Worker Kerry Thomas at 708-202-4487.
Greater Chicago Food Depository chicagosfoodbank.org 773-247-FOOD
Packet Pg. 17
Page 18
November 2014 - Number of Job Applicants by Position
Department Position
Date Position
Posted
No. of
Applicants
During Report
Month
Total No. of
Applicants to
Date**
Position
Filled Date FilledBuilding Management Maintenance Worker 10/20/14 8 8 Open Open
Court Services Aurora Adult Probation Officer 8/4/14 0 44 Closed 10/19/14
Court Services Elgin Adult Probation Officer 9/9/14 0 37 Closed Interviewing
Court Services Support Staff Tri Cities 9/9/14 0 24 Closed 12/1/14
Court Services Supervisor 4/10/14 0 17 Closed 8/31/14
Employment & Education KCDEE Employment Training Represenative 10/20/14 2 2 Open Open
Health Department Assistant Director Communicable Disease 7/25/14 0 10 Closed Interviewing
Health Department Division Director of Disease Prevention 10/7/14 12 12 Open Intervewing
Health Department CHSII Community Health Practitioner 8/14/14 0 5 Closed Interviewing
Health Department CHSII Environmental Health Practitioner 9/16/14 4 14 Open OpenHealth Department Clinical Nursing Supervisor 7/21/14 0 2 Closed Interviewing
Information Technologies Desktop Specialist 9/8/14 4 8 Open Open
Judiciary/Court Services Juvenile Drug Court Coordinator 9/2/14 0 5 Closed Interviewing
KDOT Civil Engineer Co-Op Intern 2-Openings Jan-Aug 2015 6/16/14 0 0 Open Open
KDOT Project Manager Civil Engineer 4/9/14 0 6 Open Open
KDOT Seasonal Maintainer/Snowbird 10/1/14 6 6 Closed 12/1/14
KDOT Traffic Safety Engineer (hiring 2 one filled) 10/6/14 4 4 Closed 10/14/14
State's Attorney Office Juvenile Justice Council Coordinator 10/1/14 1 1 Open Open
NA * General Application NA* NA* 2 2 NA NA
* NA - No Position posted
Packet Pg. 18
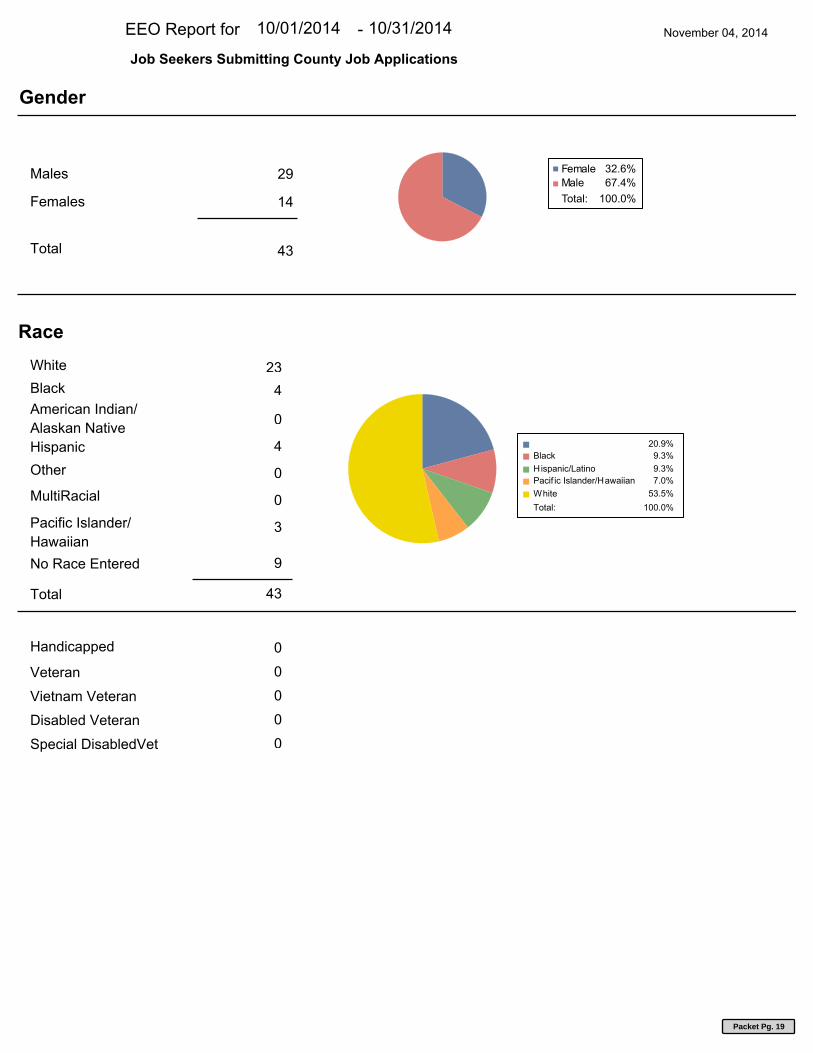
Page 19
EEO Report for November 04, 201410/01/2014 10/31/2014-
Job Seekers Submitting County Job Applications
Males 29
14 Females
Female 32.6%
Male 67.4%
Total: 100.0%
Gender
43 Total
4
23
Black
White
Race
American Indian/
Alaskan Native 0
Hispanic 4
Other 0
MultiRacial 0
Pacific Islander/
Hawaiian 3
43 Total
No Race Entered 9
20.9%
Black 9.3%
Hispanic/Latino 9.3%
Pacif ic Islander/Hawaiian 7.0%
White 53.5%
Total: 100.0%
Handicapped
0
0
Veteran
Vietnam Veteran
Disabled Veteran
Special DisabledVet
0
0
0
Packet Pg. 19
Page 20
Kane County New Hires EEO Report10/1/2014 - 10/31/2014
2Administrative Support
6Professionals
1Technicians
Administrative Support 22.2%2
Professionals 66.7%6Technicians 11.1%1
Total: 100.0%9
EEOC Category
8Female
1Male
Female 88.9%8
Male 11.1%1
Total: 100.0%9
Gender
1Hispanic or Latino
8White
Hispanic or Latino 11.1%1
White 88.9%8
Total: 100.0%9
Race
Page 1 of 2
Packet Pg. 20
Page 21
Kane County New Hires EEO Report10/1/2014 - 10/31/2014
1Circuit Clerk
1
CourtServices/Court
ServicesAdministration
1
CourtServices/Juvenile
Justice Center
1Finance
2Health
1
Regional Office ofEducation
1State's Attorney
1Transportation
Circuit Clerk 11.1%1Court Services/Court Services Administration 11.1%1Court Services/Juvenile Justice Center 11.1%1Finance 11.1%1Health 22.2%2Regional Office of Education 11.1%1State's Attorney 11.1%1Transportation 11.1%1
Total: 100.0%9
Department
Page 2 of 2
Packet Pg. 21
Page 22
Kane County New Hire Report
10/1/2014 - 10/31/2014
Department Employee Name HireDateStatusJobTitle
BOENZI, AMANDA MCircuit Clerk 10/20/2014ACTIVEDeputy Clerk
VEGA, ZULAY CCourt Services/Court Services Administration 10/20/2014ACTIVEHybrid Juvenile Probation Ofcr
JACOBS, SARAH ACourt Services/Juvenile Justice Center 10/14/2014ACTIVEYouth Counselor JJC
DOBERSZTYN, THERESA FFinance 10/01/2014ACTIVEAsst Director of Purchasing
COOK, EMMA EHealth 10/07/2014ACTIVECHS II Comm Health Practitioner
SLIVKA, ALEXIS MHealth 10/14/2014ACTIVECHS III Comm Health Practitioner
WEIL, STEFFANIE ARegional Office of Education 10/27/2014ACTIVEParaprofessional
GERDING, JULIANNE MState's Attorney 10/20/2014ACTIVELaw Intern
ZULKOWSKI, STEPHEN DTransportation 10/14/2014ACTIVETraffic Permit Engineer
9 New Hire Employees
Page 1 of 111/12/2014
Packet Pg. 22
Page 23
Kane County Terminations EEO Report10/1/2014 - 10/31/2014
5Full Time
Full Time 100.0%5
Total: 100.0%5
EEOC Category
4Female
1Male
Female 80.0%4
Male 20.0%1
Total: 100.0%5
Gender
5White
White 100.0%5
Total: 100.0%5
Race
Page 1 of 2
Packet Pg. 23
Page 24
Kane County Terminations EEO Report10/1/2014 - 10/31/2014
1
BuildingManagement
1Circuit Clerk
1
CourtServices/Court
ServicesAdministration
1KCDEE
1State's Attorney
Building Management 20.0%1Circuit Clerk 20.0%1
Court Services/Court Services Administration 20.0%1KCDEE 20.0%1State's Attorney 20.0%1
Total: 100.0%5
Department
Page 2 of 2
Packet Pg. 24
Page 25
Kane County Termination Report
10/1/2014 - 10/31/2014
Department Employee Name Termination Date
ANDERSON, KENNETH GBuilding Management 10/17/2014
PEARSON, JESSICACircuit Clerk 10/21/2014
MCCADAM, KATHLEEN SCourt Services/Court Services Administration 10/24/2014
RITCHEY, CRYSTAL MKCDEE 10/16/2014
KOWALCZYK, KARINAState's Attorney 10/17/2014
5 Terminated Employees
Page 1 of 111/12/2014
Packet Pg. 25
Page 26
PPO 4
HMOIL 1
HMOBA 2
Dependents 3
TOTAL 10
PPO 2
HMOIL 1
HMOBA 1
TOTAL 4
Add Cancel
PPO 1 0
HMOIL 1 1
HMOBA 0 1
TOTAL 2 2
PPO 0
HMOIL 0
HMOBA 1
TOTAL 1
IMRF DeductionsAmount Checks Amount TOTALS
PPO 36 25,017.47$ 6 5,681.61$
HMOIL 3 1,802.89$ 0 -$ HMOBA 14 6,953.41$ 4 3,102.57$
Dental Only 6 321.34$ 0
TOTAL 59 34,095.11$ 10 8,784.18$ 42,879.29$
IMRF DeductionsAmount Checks Amount
PPO 2 1,947.14$ 3 2,325.39$
HMOIL 0 -$ 0 -$
HMOBA 1 454.72$ 2 938.03$
Dental 0 -$ 2 105.59$
TOTAL 3 2,401.86$ 7 3,369.01$ 5,770.87$
Checks Amount
PPO 1 314.68$
HMOIL 0 -$
HMOBA 1 110.20$
TOTAL 2 424.88$ 424.88$
COBRA ENROLLED: 10
ON UNPAID LOA: 2
October 2014 Monthly SummaryNEW HIRE
EMPLOYEE TERMINATIONS
EMPLOYEES ADDING/CANCEL SELF/ DEPENDENTS (Q.E.)
EMPLOYEES ADDED DUE TO QUALIFYING EVENT (Q.E.)
RETIREES ENROLLED: 69
Packet Pg. 26
Page 27
RESOLUTION/ORDINANCE EXECUTIVE SUMMARY
Resolution No.
Approving Contract for Employee Assistance Provider (Metropolitan Family Services)
Committee Flow: Human Services Committee, Executive Committee, County Board Contact: Sheila McCraven, 630.232.5932
Budget Information:
Was this item budgeted? Yes Appropriation Amount: $15,741
If not budgeted, explain funding source:
Summary:
This resolution approves the continuation of employee assistance services for Kane County employees. The contract is being awarded to the incumbent, Metropolitan Family Services.
Packet Pg. 27
Page 28
STATE OF ILLINOIS
COUNTY OF KANE
RESOLUTION NO.
APPROVING CONTRACT FOR EMPLOYEE ASSISTANCE PROVIDER (METROPOLITAN FAMILY SERVICES)
WHEREAS, the Kane County Board wishes to continue its Employee Assistance Program
for employees; and
WHEREAS, Global Group received quotes from seven (7) providers, including the
incumbent Metropolitan Family Services; and
WHEREAS, Metropolitan Family Services continues to offer competitive pricing for this
service which includes 65 hours of wellness training and on-site crisis response service;
WHEREAS, the Human Services Committee has recommended that Metropolitan Family
Services continue as the County’s provider, at a cost of $15,741 based upon its ability to provide a
full range of services, 24/7 access and professional staff.
NOW, THEREFORE, BE IT RESOLVED NOW by the Kane County Board that the Chairman
is authorized to enter into a contract with Metropolitan Family Services, for the provision of
professional employee assistance services, at a cost not to exceed fifteen thousand seven hundred
and forty-one dollars (15,741).
Line Item Line Item Description Was Personnel/Item/Service approved
in original budget or a subsequent
budget revision?
Are funds currently available for this
Personnel/Item/Service in the specific
line item?
If funds are not currently available
in the specified line item, where
are the funds available?
001.120.120.50000 Project Administration Yes Yes
Passed by the Kane County Board on December 9, 2014.
________________________________ _____________________________ John A. Cunningham Christopher J. Lauzen Clerk, County Board Chairman, County Board Kane County, Illinois Kane County, Illinois
Vote:
14-12 EAP
Packet Pg. 28
Page 29
County of Kane 2015 Employee Benefits Renewal September 11, 2014
Comprehensive strateg ies. Individual attention.
County of Kane Marketing Summary Employee Assistance
Carrier:Plan:Flexible Spending Account Fees:Toll‐free Access 24 hours Person to Person VisitOn‐Site Crisis Response ServiceWellness Training/ManagerLegalFinancialElder CareCommunication MaterialsProvide Quarterly Reports
Additional Fees (optional):
additional services Estimated Eligible
Current RenewalMonthly Cost per Employee $1.10 $0.99Estimated Annual Cost $17,490 $15,741Change from Current Costs ($1,749)Percentage Change from Current ‐10%
5 year rate guarantee 3 year rate guarantee 5 Year Rate Guarantee 2 year Rate Guarantee‐10% ‐3% 51% 35%
5 year rate guarantee264%
(1,749.00) (477.00) $8,904.00 6,042.00 $46,110.00$15,741 $17,013 $26,394 $23,532 $63,600$0.99 $1.07 $1.66 $1.48 $4.00
1325 1325 1325 1325 1325 1325$225 per staff hour $300 per staff hour $300 per staff hour $225 per staff hour $500 per staff hour $250 ‐$275 per staff hour
Health Advocacy included/not available on a stand alone
Included Quarterly Quarterly Included Annual Annual Included Included Included Included Included Includedincluded Included/telephonic Included/telephonic Included/telephonic Included/telephonic Included/telephonicincluded Included/telephonic Included/telephonic Included/telephonic Included/telephonic Included/telephonicincluded Included/telephonic Included/telephonic Included/telephonic Included/telephonic Included/telephonic
65 hours combined 10 hours 20 hours combined 65 hours combined 24 hours/combined 65 hours combined65 hours combined 20 hours 20 hours combined 65 hours combined 24 hours/combined 65 hours combined
3 per year per problem area 3 per year per problem area 3 per year per problem area 3 per year per problem area 5 per year per problem area 3 per year per problem areaIncluded Included Included Included Included IncludedCurrent Option Option Option Option Option
Metropolitan Family Services Ceridian Perspectives ComPsych Workplace Solutions Health AdvocateEmployee Assistance Program Employee Assistance Program Employee Assistance Program Employee Assistance Program Employee Assistance Program Employee Assistance Program
Packet P
g. 29
Page 30
RESOLUTION/ORDINANCE EXECUTIVE SUMMARY
Resolution No.
Amending Personnel Policy Handbook (Insurance Benefits)
Committee Flow: Human Services Committee, Executive Committee, County Board Contact: Sheila McCraven, 630.232.5932
Budget Information:
Was this item budgeted? Appropriation Amount:
If not budgeted, explain funding source:
Summary:
The Insurance Benefits Policy is being amended to bring the policy in compliance with the Patient Protection and Affordable Care Act which requires a large employer to make health insurance available to all employees working an average of 30 hours per week based upon the applicable measurement period. The policy is also amended to specify eligibility requirements for vision insurance.
Packet Pg. 30
Page 31
STATE OF ILLINOIS
COUNTY OF KANE
RESOLUTION NO.
AMENDING PERSONNEL POLICY HANDBOOK (INSURANCE BENEFITS)
WHEREAS, from time to time, the Human Services Committee recommends that certain amendments are made to the policies contained in the Kane County Personnel Policy Handbook and
WHEREAS, the Human Services Committee recommends that the Insurance Benefits Policy
contained in the Personnel Policy Handbook be amended to comply with the provisions of the Patient Protection and Affordable Care Act; and to make other eligibility clarifications; and
NOW, THEREFORE, BE IT RESOLVED by the Kane County Board that the Insurance
Benefits policy contained in the Kane County Personnel Policy Handbook is amended as set forth
below.
INSURANCE BENEFITS
All regular full-time and regular part-time employees who work a minimum of 21 hours per
week are eligible to enroll in the County's comprehensive group medical, dental, vision, life and
supplemental insurance plans.
Eligibility for coverage will go into effect after 60 days of continuous employment are
completed. Thereafter, employees have 30 days to enroll; otherwise, the employee will be
considered a late enrollee.
Employee participation in each plan is voluntary and optional.
A. Premiums - Premium costs for health and dental insurance are shared by the
employee and the County through payroll deduction. Vision insurance is provided
without cost to active employees and to retired subsidy employees who are enrolled
in any of the County’s health plans.
B. Part-time employees who regularly work less than 30 hours per week as determined
by a measurement period analysis will pay the full premium for all plans for
coverage. Employees who regularly work 30 or more hours per week as
determined by a measurement period analysis, will pay the same employee
Packet Pg. 31
Page 32
contribution rate as full-time employees. The applicable measurement period is
defined by the Patient Protection and Affordable Care Act and its implementing
regulations.
C. A pre-tax deduction Section 125 plan is available at the time of enrollment which
that allows employees to pay their share of the insurance premiums with before tax
dollars. The amount of each employee’s contribution is linked to participation in the
County’s Employee Wellness Plan.
D. Dependent Eligibility - From time to time, Kane County may require employees
enrolled the County’s health plans to participate in a dependent audit to verify the
eligibility of their enrolled dependents. Employees who refuse to cooperate and
dependents who fail to meet eligibility requirements shall be removed from Kane
County’s health plans. If it is discovered that an employee has provided false
information about their enrolled dependents or fails to timely notify Human
Resources about a change of status that could affect the eligibility of their enrolled
dependents, the Human Services Committee has discretion to take additional action
that may result in the both the employee and the ineligible dependents losing the
County’s health coverage and reimbursing the County for paid claims.
E. Continuation Coverage - There are certain situations where coverage under a
medical plan would otherwise end, such as termination, retirement or divorce. A
continuation option is available where eligible employees may elect to purchase
continued health coverage at the group rate under the plans for a restricted period.
applicable retiree or COBRA rate for an allowable period as set by statute. Neither
vision nor dental insurance is available for retired or Medicare-eligible employees
who reach age 65. Human Resources has information on this continued coverage.
F. Patient Protection and Affordable Care Act - Beginning in 2013 2015, there will be a
$2,500 $2,550 limit on the amount participants can contribute to their healthcare
FSA. This limit is subject to change in subsequent years by the Internal Revenue
Service. See the Kane County Flexible Benefits Plan Summary Document for the
currently allowable limit that has been adopted by Kane County.
G. Optional Death Benefit - Employees who have health insurance elsewhere or do not
Packet Pg. 32
Page 33
wish to participate under the health plan offered by Kane County, may waive their
health insurance with Kane County and gain a supplemental death benefit. This
option provides that should the employee die while employed by Kane County, six
(6) months salary would be paid to the beneficiary. This is in addition to the IMRF
death benefits. The option of re-enrolling in the medical insurance plan is only
available during the annual open enrollment period or in certain extraordinary non-
medical situations. Health insurance coverage may be waived for the death benefit
anytime throughout the year.
The employee is responsible for notifying the Human Resources Department of any status
change which that could affect insurance coverage such as marriage, civil union, divorce, birth of a
baby. Specific information about health, dental, vision, life or supplemental insurance benefits, pre-
tax plan or the optional death benefit can be obtained from the Human Resources Department.
Passed by the Kane County Board on December 9, 2014.
________________________________ _____________________________ John A. Cunningham Christopher J. Lauzen Clerk, County Board Chairman, County Board Kane County, Illinois Kane County, Illinois
Vote:
14-12 Insurance Benefits
Packet Pg. 33
Page 34
RESOLUTION/ORDINANCE EXECUTIVE SUMMARY
Resolution No.
Amending and Restating County of Kane Flexible Benefits Plan
Committee Flow: Human Services Committee, Executive Committee, County Board Contact: Sheila McCraven, 630.232.5932
Budget Information:
Was this item budgeted? NA Appropriation Amount:
If not budgeted, explain funding source:
Summary:
The Flexible Spending Plan document and summary are being amended as follows: 1) a shortened run-out period for terminating employees (reduced from 90 to 30 days); 2)new election change events as permitted under the Affordable Care Act (ACA); 3)revised FSA maximum amount to $2,550 as permitted pursuant to the ACA; 4)revised to reflect use of debit cards; 5)revised to indicate new TPA (Flexible Benefits); 6)revised claims procedures to shorten FSA appeal period from 180 days to 60 days; 7)added some additional legal protections and clarifications, including protection in the event of fraud and/or improper reimbursements.
Packet Pg. 34
Page 35
STATE OF ILLINOIS
COUNTY OF KANE
RESOLUTION NO.
AMENDING AND RESTATING COUNTY OF KANE FLEXIBLE BENEFITS PLAN
WHEREAS, by Resolution 91-22 dated February 12, 1991 the County heretofore established the County of Kane Pre-Tax Deduction Plan (the “Plan”) to provide for the payment of the portion of the group medical insurance premium payable by the employees of the County on a pre-tax basis; and
WHEREAS, by Resolution 05-446 dated December 13, 2005, the County amended and
restated the Plan to allow participation in flexible spending accounts for health and dependent care; and
WHEREAS, by Resolution 12-357 dated October 25, 2012, the County amended and
restated the Plan to permit participation by qualified Kane County employees who are enrolled in the Teamsters Health and Welfare plan; and
WHEREAS, by Resolution 13-382, dated December 13, 2013, the County amended and
restated the Plan to permit the rollover up to $500 of unused funds at the end of the 2013 plan year and for each year thereafter; and
WHEREAS, County desires to amend and restate the Plan for the benefit of its eligible employees as follows: 1)to shorten the run-out period for terminating employees (reduced from 90 to 30 days); 2)to add new election change events as permitted under the Affordable Care Act (ACA); 3)to revise the FSA maximum amount to $2,550 as permitted pursuant to the ACA; 4)to reflect the use of debit cards; 5)to indicate new TPA (Flexible Benefits); 6) to revise claims procedures to shorten FSA appeal period from 180 days to 60 days; 7) to add some additional legal protections and clarifications, including protection in the event of fraud and/or improper reimbursements.
NOW, THEREFORE, BE IT RESOLVED that the County does hereby adopt the County of
Kane Flexible Benefits Plan as amended, and authorizes the Chairman to execute any necessary documents for the implementation of the plan that is attached.
Line Item Line Item Description Was Personnel/Item/Service approved
in original budget or a subsequent
budget revision?
Are funds currently available for this
Personnel/Item/Service in the specific
line item?
If funds are not currently available
in the specified line item, where
are the funds available?
Passed by the Kane County Board on December 9, 2014.
________________________________ _____________________________ John A. Cunningham Christopher J. Lauzen Clerk, County Board Chairman, County Board Kane County, Illinois Kane County, Illinois
Vote:
14-12 Amending FSA Plan
Packet Pg. 35
Page 36
COUNTY OF KANE
FLEXIBLE BENEFITS PLAN
(Effective as of January December 31, 20153)
Packet Pg. 36
Page 37
i
TABLE OF CONTENTS
Page
ARTICLE 1 - INTRODUCTION .................................................................................................. 1
1.1 Purpose .................................................................................................................... 1
1.2 Effective Date and Plan Year .................................................................................. 1
1.3 Administration ........................................................................................................ 1
ARTICLE 2 - ELIGIBILITY AND PARTICIPATION................................................................ 2
2.1 Eligibility ................................................................................................................ 2
2.2 Cessation of Participation ....................................................................................... 2
2.3 Reinstatement of Former Participant ...................................................................... 3
2.4 Death ....................................................................................................................... 3
ARTICLE 3 - CONTRIBUTIONS ................................................................................................ 5
3.1 Contributions by Participants .................................................................................. 5
3.2 Irrevocability of Election by the Participant During the Plan Year ........................ 6
3.3 Continuation of Coverage ..................................................................................... 10
ARTICLE 4 - PAYMENT OF BENEFITS ................................................................................. 12
4.1 Covered Benefits ................................................................................................... 12
4.2 Insurance Benefits ................................................................................................. 12
ARTICLE 5 - GENERAL PROVISIONS ................................................................................... 13
5.1 Information to be Furnished by Participants ......................................................... 13
5.2 Uniform Rules ....................................................................................................... 13
5.3 Changes by County ............................................................................................... 13
5.4 Plan Administrator/County Decision Final ........................................................... 13
5.5 Gender and Number .............................................................................................. 14
5.6 Severability of Provisions ..................................................................................... 14
5.7 Binding Effect ....................................................................................................... 14
5.8 Headings of Articles and Sections ........................................................................ 14
5.9 Controlling Law .................................................................................................... 14
5.10 Employment Rights .............................................................................................. 14
5.11 Indemnification of Plan Administrator ................................................................. 15
5.12 Cost of Plan Administration.................................................................................. 15
Packet Pg. 37
Page 38
ii
5.13 Evidence ................................................................................................................ 15
5.14 Interests Not Transferable ..................................................................................... 15
5.15 Facility of Payment ............................................................................................... 15
5.16 No Guarantee of Tax Consequences ..................................................................... 15
5.17 Indemnification of Employer ................................................................................ 16
5.18 Delegation of Authority ........................................................................................ 16
ARTICLE 6 - AMENDMENT AND TERMINATION .............................................................. 17
6.1 Amendment ........................................................................................................... 17
6.2 Termination ........................................................................................................... 17
6.3 Benefits on Termination ....................................................................................... 17
ARTICLE 7 - COMPLIANCE WITH THE HIPAA PRIVACY AND SECURITY RULE....... 18
7.1 Purpose .................................................................................................................. 18
7.2 Disclosure of PHI to County ................................................................................. 19
7.3 Plan Sponsor Certification .................................................................................... 20
ARTICLE 8 - EXECUTION OF PLAN ...................................................................................... 23
SUPPLEMENT A PRE-TAX PREMIUM ACCOUNT ............................................................ A-1
SUPPLEMENT B FLEXIBLE SPENDING ACCOUNT ........................................................ B-1
SUPPLEMENT C DEPENDENT CARE REIMBURSEMENT ACCOUNT ......................... C-1
Packet Pg. 38
Page 39
1
ARTICLE 1 - INTRODUCTION
1.1 Purpose. The County of Kane Flexible Benefits Plan (the "Plan") has been
established by the County of Kane (the "County") to provide its eligible employees a choice
between certain non taxable and taxable benefits. The Plan is maintained for the exclusive
benefit of eligible employees of the County and is intended to meet the requirements of, and to
constitute, a cafeteria plan under Section 125 of the Internal Revenue Code of 1986, as amended
(the "Code"), and any comparable section or sections of any future legislation that amends,
supplements or supersedes said section of the Code.
1.2 Effective Date and Plan Year. The "Effective Date" of the Plan as set forth herein
is January 1, 2011, or as otherwise provided in the Plan with respect to individual provisions, and
this restatement of the Plan is effective January 1, 20153. A "Plan Year" is the 12-consecutive
month period beginning on each January 1 and ending on the next following December 31.
1.3 Administration. The Plan will be administered by the County or any person,
persons or entity so designated by the County to serve as Plan Administrator. If no Plan
Administrator is designated by the County, the County, itself, is deemed to be the Plan
Administrator. Any notice or document required to be given to or filed with the County will be
properly given or filed if delivered or mailed by registered mail, postage prepaid, to the County
Board Chairman at Kane County Government Center, 719 Batavia, Geneva, Illinois 60134.
Packet Pg. 39
Page 40
2
ARTICLE 2 - ELIGIBILITY AND PARTICIPATION
2.1 Eligibility. Each employee of the County who is eligible to participate and enrolls
in either the County's group medical or group dental plan shall be eligible to become a
Participant in the Plan as of the later of (i) the Effective Date, or (ii) the first day that the
employee becomes eligible to participate in the County's group health plan (medical or dental),
with actual enrollment to occur as soon as practicable following the employee’s submission of a
completed election form. Also, an employee of the County’s Department of Transportation who
is eligible to participate in the Suburban Teamsters of Northern Illinois Welfare Fund (the
“Teamsters Plan”) shall be eligible to become a participant in the Plan on the first day that the
employee becomes eligible to participate in the Teamsters Plan, with actual enrollment to occur
as soon as practicable following the employee’s submission of a completed election form. If an
employee of the County also provides services to the County as an independent contractor or
director, the employee is eligible to participate in the Plan solely in his capacity as an employee.
2.2 Cessation of Participation. A Participant will cease to be a Participant as of the
earlier of (i) the date on which the Plan terminates, (ii) the date on which the Participant ceases
to be an employee eligible to participate under Section 2.1, (iii) the date of the Participant's
death, subject to Section 2.4, or (iv) the date the Participant ceases to make any contributions to
the Plan. Notwithstanding the preceding sentence, a Participant, his spouse and dependents may
be entitled to continue participation under the Plan with respect to the Flexible Spending
Account as described in Supplement B pursuant to Section 3.3 of this Plan and the requirements
of Code Section 4980B and regulations issued thereunder (“COBRA”). Additionally, a
Participant who becomes eligible for COBRA continuation coverage under the County’s group
health plan or the Teamsters Plan and who continues to receive income from employment by the
County (for example, if the Participant experiences a reduction in hours but continues to be an
employee or if the Participant receives severance pay), may pay for any group health coverage
provided pursuant to COBRA with pre-tax dollars through payroll withholding pursuant to
Supplement A.
If a Participant terminates employment, the Participant’s pre-tax group welfare insurance
(such as group medical or dental) contributions under the Plan (if any) will cease (unless, as
described above, the Participant receives some form of salary continuation, such as severance
pay, and is entitled and elects to continue group health insurance (e.g., group medical or dental)).
Packet Pg. 40
Page 41
3
Additionally, the Participant’s contributions (if any) to the Dependent Care Reimbursement
Account, and the Flexible Spending Account will cease (unless he is entitled to and elects
COBRA continuation coverage with respect to the Flexible Spending Account).
2.3 Reinstatement of Former Participant. If the Participant terminates employment
and then is rehired during the same Plan Year, the Participant’s pre-tax welfare insurance
elections (if any) in the Plan and his elections with respect to contributions to the Dependent
Care Reimbursement Account and the Flexible Spending Account (if any) will be reinstated
automatically for the remainder of the Plan Year. However, if the Participant is rehired more
than thirty days after his termination, he shall be eligible to make new elections for the remainder
of such Plan Year. If such reinstatement occurs after the end of the Plan Year in which the
Participant’s termination occurred, the Participant shall be eligible to participate in the Plan after
he has satisfied the eligibility requirements of Section 2.1 of the Plan subsequent to his date of
rehire.
2.4 Death. If a Participant dies, his participation in the Plan shall cease. However, a
representative of the Participant's estate may submit claims for expenses or benefits incurred
during the portion of the Plan Year preceding the Participant's date of death. Additionally, the
Participant’s spouse and dependents may be entitled to continue coverage under the Flexible
Spending Account pursuant to Section 3.3.
Packet Pg. 41
Page 42
4
ARTICLE 3 - CONTRIBUTIONS
3.1 Contributions by Participants. Each Participant may elect in writing to reduce his
future annual compensation from the County in such amount as the Participant designates (not to
exceed the maximum amounts specified in the Supplements attached hereto) for any or all of the
benefits available under the Plan. Any compensation reduction election shall be made in
accordance with the policies and procedures established from time to time by the County. A
compensation reduction election must be in writing and filed with the County prior to the later of
(i) the first day of the Plan Year for which it is to be effective (or such earlier date established by
the County in order to allow adequate time for processing), or (ii) for the first year of eligibility,
the thirtieth (30th) day after a Participant's date of eligibility (with the election to be retroactively
applicable, but the compensation reductions to apply only to compensation not yet currently
available on the date of the election). If the cost of participation in one of the County’s
contributory welfare plans (e.g., medical or dental insurance) or the Teamsters Plan increases or
decreases during any Plan Year, and, under the terms of the respective plan, the Participant is
required to make a corresponding change in payments, the County may, on a reasonable and
consistent basis, automatically make a prospective increase or decrease in the contributions to the
Plan of affected Participants. In addition, if the cost of participation in one of the County’s
contributory welfare plans (e.g., medical or dental insurance) or the Teamsters Plan increased
during the Plan Year, or any prior Plan Year, and, under the terms of the respective plan, the
Participant was required to make a corresponding change in payments, but the County
inadvertently failed to implement such change, the County may, on a reasonable and consistent
basis, require the Participant to pay the difference. One (but not the only) means for doing so
would be to enter into a payment plan whereby any past-due payments that were required to be
paid by the Participant are withheld from the Participant's pay over a reasonable period of time.
3.2 Irrevocability of Election by the Participant During the Plan Year. An election of
benefits made under the Plan, shall be irrevocable by the Participant during the Plan Year for
which made, except as provided herein. A Participant may revoke a benefit election for the
balance of a Plan Year and file a new election only in the following circumstances:
(a) HIPAA Special Enrollment: A Participant may revoke an existing election
and make a new election that corresponds with special enrollment rights
Packet Pg. 42
Page 43
5
under the Health Insurance Portability and Accountability Act of 1996
(“HIPAA”) as amended.
(b) Changes in Status: A Participant may revoke a benefit election for the
balance of a Plan Year and file a new election if both the revocation and
the new election are on account of and consistent with a change in status
that affects eligibility of the Participant, his spouse or dependent for
coverage under an employer’s cafeteria plan or other employee welfare
benefit plan in which the individual is a participant. A change in status for
this purpose includes:
(1) a change in legal marital status, including the Participant’s
marriage, death of the Participant’s spouse, divorce, legal
separation or annulment;
(2) an event that changes an employee’s number of dependents,
including birth, death, adoption and placement for adoption, or an
event that otherwise results in an increase or decrease in the
number of a Participant’s family members or dependents who may
benefit from coverage under the Plan;
(3) a change in employment status of the Participant or the
Participant’s spouse or dependent including the termination or
commencement of employment, a strike or lockout, a
commencement of or return from an unpaid leave of absence, a
change in worksite, a reduction or increase in hours of
employment, including a switch from part-time to full-time
employment status or vice versa, or a switch from hourly to
salaried employment or vice versa;
(4) an event causing the Participant’s dependent to satisfy or cease to
satisfy the requirements for coverage due to attainment of age,
student status, or any similar circumstance as provided in the
welfare plan under which the Participant receives coverage for that
dependent;
Packet Pg. 43
Page 44
6
(5) a change in the place of residence of the Participant, the
Participant’s spouse or dependent that affects eligibility; and
(6) such other events as the Plan Administrator determines qualify as a
change in status, consistent with regulations and rulings of the
Internal Revenue Service.
(c) Reduction of weekly hours of employment below 30: A Participant may
revoke an existing election and make a new election if he experiences a
reduction in hours of employment such that (1) the Participant reasonably
is expected to work an average of less than 30 hours per week after
reasonably having been expected to average at least 30 hours per week
(even if the reduction in hours of employment does not result in the
Participant’s ceasing to be eligible under the County’s group health plan);
and (2) the revocation of a benefit election under the Plan corresponds to
the intended enrollment of the Participant and the Participant’s spouse or
dependent, who cease coverage due to the revocation in another plan that
provides minimum essential coverage, where such new coverage is
effective no later than the first day of the second month following the
month that includes the date the benefit election is revoked;
(d) Enrollment in a Qualified Health Plan: A Participant may revoke an
existing election and make a new election that corresponds with his
enrollment in a “Qualified Health Plan” (as purchased through a
marketplace established pursuant to Section 1131 of the Patient Protection
and Affordable Care Act of 2010 (a “Marketplace”)), if (1) the Participant
is eligible for a “special enrolment period” to enroll in a Qualified Health
Plan pursuant to guidance issued by the Department of Health and Human
Services and any other applicable guidance, or the Participant seeks to
enroll in a Marketplace during the Marketplace’s annual open enrollment
period; and (2) the revocation of a benefit election under the Plan
corresponds to the intended enrollment of the Participant and the
Participant’s spouse or dependent, who cease coverage due to the
revocation, in a Qualified Health Plan through a Marketplace for new
coverage that is effective beginning no later than the day immediately
following the last day of the revoked coverage.
(c)(e) COBRA Eligibility: In the event a Participant, a Participant’s spouse or
dependent becomes eligible for continuation coverage under the County’s
group health plan or the Teamsters Plan, the Participant may elect to
modify payments under the Plan as appropriate in order to pay for the
continuation coverage elected.
Packet Pg. 44
Page 45
7
(d)(f) Court Order: Upon the entry of a judgment, decree or court order
(including a qualified medical child support order under Section 609 of the
Employee Retirement Income Security Act of 1974) resulting from a
divorce, legal separation, annulment or change in legal custody requiring
the Participant or the Participant’s former spouse to provide, or cancel,
health coverage for a Participant’s child or for a foster child who is a
dependent of the Participant, a Participant may make a corresponding
change in election (cancellation to be permitted only if the order also
requires another person to provide coverage for the child and such
coverage actually is provided).
(e)(g) Entitlement to Medicare/Medicaid: In the event the Participant or the
Participant’s spouse or dependent who is enrolled in the County’s group
health plan or the Teamsters Plan becomes entitled to or loses eligibility
for coverage under Medicare or Medicaid, then the Participant may cancel,
reduce, commence or increase coverage for himself, his spouse or his
dependent accordingly.
(f)(h) Significant Change in Cost or Coverage: Other than with respect to the
Flexible Spending Account provided for in Supplement B,
(1) if the cost to the Participant (if any) for a benefit package option
(e.g., a welfare benefit offered through this Plan, or an option for
coverage under an underlying health plan, such as an indemnity
option, an HMO option, or a PPO option) significantly increases or
decreases (whether that increase or decrease results from an action
taken by the employee or from an action taken by the County), or,
with respect to the Dependent Care Reimbursement Account
election, a significant cost change is imposed by a dependent care
provider who is not a relative of the Participant, a Participant may
make a corresponding election change for the balance of the Plan
Year;
(2) if coverage under one of the County’s welfare plans (e.g., medical
or dental coverage), the Teamsters Plan, or a welfare plan of an
Packet Pg. 45
Page 46
8
employee’s spouse or dependent, is significantly curtailed or
ceases (for example, there is a significant increase in the
deductible, copay or out-of-pocket cost sharing limit under a health
plan) during such Plan Year, but there is not a loss of coverage as
defined in (3) below, an affected Participant may revoke his
election for that coverage and, in lieu thereof, elect to receive on a
prospective basis coverage under another benefit package option
providing similar coverage, provided such changes are permitted
under the terms of the applicable welfare benefit plan;
(3) if a Participant or his spouse or dependent has a significant
curtailment of coverage that is a loss of coverage (that is, a
complete loss of coverage under the benefit package option or
other coverage option (including the elimination of a benefits
package option, an HMO ceasing to be available in the area where
the individual resides, or the individual losing all coverage under
the option by reason of an overall lifetime or annual limitation)),
the affected Participant may revoke his election under the Plan
and, in lieu thereof, elect either to receive on a prospective basis
coverage under another benefit package option providing similar
coverage or to drop coverage if no similar benefit package option
is available, provided such changes are permitted under the terms
of the applicable welfare benefit plan;
(4) if a new benefit package option or other coverage option is added
or if coverage under an existing benefit package option or other
coverage option is significantly improved, a Participant may
revoke his election, and, in lieu thereof, make an election on a
prospective basis for coverage under the new or improved benefit
package option, provided such changes are permitted under the
terms of the applicable welfare benefit plan; or
(5) a Participant may make an election change on account of and
corresponding with a change made under the plan of the spouse’s,
Packet Pg. 46
Page 47
9
former spouse’s or dependent’s employer provided the election
under the spouse’s or dependent’s plan satisfies both that plan’s
election change rules and IRS regulations regarding election
changes, or the spouse’s or dependent’s plan has a different period
of coverage.
(g)(i) FMLA: Family Medical Leave Act.
With respect to a Participant on a paid leave of absence under the Family
Medical Leave Act (“FMLA”), the Participant’s existing election will
remain in effect and the Participant’s share of premiums to the Pre-Tax
Premium Account and/or contributions to a Flexible Spending Account
will be paid in the same manner as prior to the leave. Additionally, the
Participant may make an election change with respect to a Dependent Care
Reimbursement Account, provided the change is on account of and
consistent with the leave. The Participant will not be entitled to
reimbursement of Dependent Care claims incurred during an FMLA leave.
With respect to a Participant on an unpaid FMLA leave of absence, the
Participant may revoke an existing election or continue coverage during
the leave with respect to health benefits (such as medical or dental) under
the County’s health plans or the Teamsters Plan, or with respect to the
Flexible Spending Account.
If the Participant elects to continue coverage, the Participant has two
payment options: (i) pre-pay or (ii) pay-as-you-go. Under the pre-pay
option, the Participant may pay the premiums and contributions due
during the FMLA leave period (but only with respect to benefits through
the end of the current plan year) on a pre-tax salary reduction basis from
any taxable compensation or on an after-tax basis prior to commencement
of the leave. If the Participant’s FMLA leave period spans two Plan
Years, the amount due for the FMLA leave period that extends into the
new Plan Year must be paid on or after the first day of the new Plan Year,
for example, upon the Participant's return to work. Alternatively, the
amount due for that period may be pre-paid on an after-tax basis. Under
Packet Pg. 47
Page 48
10
the pay-as-you-go option, the Participant may pay his share of premium
payments and contributions on a monthly basis on the first of every month
(the same schedule as COBRA payments). These payments typically
would be made on an after-tax basis, unless the Participant receives
taxable compensation during the leave period (e.g., as a result of unused
sick days or vacation days). The County may cancel the Participant’s
coverage retroactive to the beginning of the period for which a payment
was due if a Participant fails to make any payment before the end of the
grace period for payment, provided that with respect to Participants on an
FMLA leave, the County notifies such Participants of the overdue
payment at least 15 days before the end of such grace period.
Alternatively, the County, at its option, may continue his coverage during
the leave and then recoup the Participant’s share of premiums and
contributions from available taxable compensation upon the Participant’s
return from leave.
If the Participant does not elect to continue coverage while on FMLA
leave, the Participant will be entitled to reinstatement upon return to
employment on the same terms as prior to taking FMLA leave, subject to
any changes in benefit levels that may have taken place during the leave.
Upon reinstatement in the Flexible Spending Account, the Participant may
resume coverage at the level in effect before the FMLA leave and make up
the unpaid premium payments, or the Participant may resume coverage at
a level that is reduced and resume premium payments at the level in effect
before the FMLA leave. If the Participant does not elect to continue
coverage during the FMLA leave under the Flexible Spending Account
while on FMLA leave, the Participant will not be entitled to
reimbursement for claims incurred during the FMLA leave.
Any election change (other than those made in connection with a court order or as an
exercise of rights pursuant to a statute that provides for a specific election period such as HIPAA
or COBRA) must be requested within thirty (30) days from the date of the change event (or
within such other reasonable period as established by the Plan). Any new election shall be
Packet Pg. 48
Page 49
11
effective not earlier than the first pay period covered by the new salary reduction election, unless
an earlier effective date is required by HIPAA or other applicable law. Additionally, a
Participant may not make any change that would reduce the Participant's level of Flexible
Spending Account coverage under Supplement B to an amount that would be less than the
amount of benefits claimed under such coverage as of the date the change would become
effective.
3.3 Continuation of Coverage. A Participant shall be entitled to continue
participation for such benefits under the Plan as required pursuant to and consistent with the
continuation coverage requirements of Code Section 4980B (“COBRA”) and regulations issued
thereunder. In particular, COBRA requires that Participants with positive Flexible Spending
Account balances be permitted to continue participation with respect to the Flexible Spending
Account component of the Plan described in Supplement B through the remainder of the Plan
Year in which a qualifying event that otherwise would result in a loss of coverage has occurred.
(a) A “qualifying event” in the case of a Participant is a reduction in hours of
employment or the termination of employment (for reasons other than
gross misconduct).
(b) A “qualifying event” in the case of a spouse of a Participant is the death of
the Participant, divorce or legal separation from the Participant, or the
reduction in the Participant’s hours of employment or the termination of
the Participant’s employment (for reasons other than gross misconduct).
(c) A “qualifying event” in the case of the Participant’s dependent child is the
death of the Participant, the divorce of the dependent’s parents, the
reduction in the Participant’s hours of employment, the termination of the
Participant’s employment (for reasons other than gross misconduct), or the
dependent ceasing to be eligible as a “dependent” under the County’s
group health plan or the Teamsters Plan.
(d) Under COBRA, the Participant, his spouse or dependent has 60 days from
the later of the date the person would lose coverage as a result of the
qualifying event and the date that the Plan provides notice to the family of
their COBRA rights in which to elect to continue coverage. COBRA
coverage under the Flexible Spending Account may be continued until the
Packet Pg. 49
Page 50
12
end of the Plan Year in which the qualifying event occurred. Continuation
coverage may end if the cost of the continuation coverage is not paid in a
timely fashion or if the Flexible Spending Account component of the Plan
is discontinued with respect to all employees. Additional information
about COBRA will be provided to Participants and their families in the
notices that are distributed when the Participant first becomes eligible to
participate in the Plan and again upon the occurrence of a qualifying
event.
(e) A Participant who elects to continue coverage under the Flexible Spending
Account or who elects to continue coverage under the County’s group
health (e.g., medical or dental) plan or the Teamsters Plan pursuant to
COBRA voluntarily may elect to have any payments due for such benefits
withheld on a pre-tax basis from any remaining compensation payable to
the Participant by the County. Alternatively, a Participant may make
after-tax contributions for such benefits. All such payments shall be made
in accordance with the written policies and procedures as may be
established by the County from time to time.
Packet Pg. 50
Page 51
13
ARTICLE 4 - PAYMENT OF BENEFITS
4.1 Covered Benefits. An account will be established for each Participant (with
separate sub-accounts established for each benefit elected by the Participant) to which is credited
the Participant's contributions for such benefit and from which is charged disbursements for the
benefit. To the extent of the credited balance in the applicable sub-account, the County shall pay
the covered expenses of each benefit selected by a Participant as such expenses are incurred
during such Plan Year. The covered expenses, when paid, shall be charged against such
Participant's sub-account and shall reduce the balance thereof. Notwithstanding the preceding, a
Participant shall be entitled to receive reimbursement up to the entire amount the Participant has
elected under the Flexible Spending Account for the Plan Year, plus any amounts carried over from
the preceding Plan Year (in accordance with Section B-8). This amount shall be available as of the
first day of the Plan Year. Only substantiated covered expenses incurred on or after the later of
the (i) Plan’s Effective Date and (ii) the date the Participant is enrolled in the Plan, shall be paid
or reimbursed.
4.2 Insurance Benefits. The rights and conditions with respect to any benefits
payable from group welfare insurance contracts selected by the County, or by the Teamsters
Plan, shall be determined solely with respect to such insurance contracts. The County shall not
be responsible for the validity of any insurance contract issued hereunder or for the failure on the
part of any insurer issuing such insurance contract to make any payments thereunder or for the
action of any person which may delay or render null and void or unenforceable, in whole or in
part, any insurance contract. The rights and conditions with respect to any benefits payable from
any self-insured group welfare plan shall be determined solely pursuant to the provisions of thate
plan’s documents.
ARTICLE 5 - GENERAL PROVISIONS
5.1 Information to be Furnished by Participants. Participants shall furnish to the
County such documents, receipts, expense reports, evidence, data or information as the County
considers necessary or desirable for the purpose of administering the Plan. In order to receive
benefits under the Plan, a Participant must furnish full, true and complete evidence satisfactory to
the County and must promptly sign any document related to the Plan requested by the County.
5.2 Uniform Rules. The County shall administer the Plan on a reasonable and
nondiscriminatory basis and shall apply uniform rules to all Participants similarly situated.
Packet Pg. 51
Page 52
14
5.3 Changes by County. If the County determines, before or during any Plan Year,
that the Plan may fail to satisfy for such Plan Year any nondiscrimination requirement imposed
by the Code or any limitation on benefits provided to "highly compensated” employees or "key
employees" as defined under the Code, the County shall take such action as it deems appropriate,
under rules uniformly applicable to similarly situated Participants, to assure compliance with
such requirements or limitations. Such action may include, without limitation, a modification of
elections by highly compensated employees or key employees to reduce the amount of their
salary reductions with or without the consent of such Participants.
5.4 Plan Administrator/County Decision Final. The County or its designated Plan
Administrator has discretionary authority to determine eligibility for benefits, to decide claims,
and to determine all other matters under the Plan. Benefits under this Plan will be paid only if
the County or the designated Plan Administrator decides in its discretion that the applicant is
entitled to them. Any interpretation of the provisions of the Plan by the County or the Plan
Administrator and any decision made by the County or Plan Administrator on any matter within
its respective discretion shall be binding on all persons. A misstatement or other mistake of fact
shall be corrected when it becomes known and the County or Plan Administrator shall make such
adjustment or account thereof as it considers equitable and practicable. Neither the County nor
the Plan Administrator shall be liable in any manner for any determination of fact made in good
faith.
5.5 Gender and Number. Where the context permits, words in the masculine gender
shall include the feminine and neuter genders, the singular shall include the plural, and the plural
shall include the singular.
5.6 Severability of Provisions. In the event that any provision of the Plan shall be
held to be illegal or invalid for any reason, said illegality or invalidity shall not affect the
remaining provisions but shall be fully severable, and the Plan shall be construed and enforced as
if said illegal invalid provision had never been inserted therein.
5.7 Binding Effect. The Plan and all actions and decisions hereunder, shall be
binding upon the heirs, executors, administrators, successors and assigns from any and all parties
hereto and Participants, present and future.
Packet Pg. 52
Page 53
15
5.8 Headings of Articles and Sections. The headings of Articles and Sections are
included solely for the convenience of reference, and if there is any conflict between such
headings and the text of the Plan, the text shall control.
5.9 Controlling Law. Except to the extent preempted by the laws of the United
States, the laws of the State of Illinois shall be controlling in all matters relating to the Plan.
5.10 Employment Rights. The Plan does not constitute a contract of employment, and
participation in the Plan will not give any employee the right to be retained in the employ of the
County, nor any right or claim to any benefit under the Plan, unless such right or claim has
specifically accrued under the terms of the Plan.
5.11 Indemnification of Plan Administrator. The County agrees to indemnify and to
defend to the fullest extent permitted by law any employee serving as the Administrator or as a
member of a committee designated as Plan Administrator (including any employee or former
employee who formerly served as Plan Administrator or as a member of such committee) against
all liabilities, damages, costs and expenses (including attorney’s fees and amounts paid in
settlement of any claims approved by the County) occasioned by any act or omission to act in
connection with the Plan, if such act or omission is in good faith.
5.12 Cost of Plan Administration. The cost and expenses incurred by the County in
administering the Plan shall be paid by the County.
5.13 Evidence. Any evidence required of anyone under the Plan may be by certificate,
affidavit, document or other information that the person acting on it considers pertinent and
reliable, and signed, made or presented by the proper party or parties, or in such other form as
the County may prescribe or deem satisfactory.
5.14 Interests Not Transferable. The interests of Participants under the Plan are not
subject to the claims of their creditors and may not be transferred or encumbered.
5.15 Facility of Payment. When, in the County's opinion, a Participant is under a legal
disability or is incapacitated in any way so as to be unable to manage his financial affairs, the
County may (but need not) make payments reimbursing such Participant's expenses to the
Participant's legal representative, or to his spouse, or the County may apply the payment for the
benefit of the Participant in any way the County considers advisable.
5.16 No Guarantee of Tax Consequences. Neither the Plan Administrator nor the
County makes any commitment or guarantee that any amounts paid to or for the benefit of a
Packet Pg. 53
Page 54
16
Participant under this Plan will be excludable from the Participant’s gross income for federal,
state, or local income tax purposes. It shall be the obligation of each Participant to determine
whether each payment under this Plan is excludable from the Participant’s gross income for
federal, state, and local income tax purposes and to notify the Plan Administrator if the
Participant has any reason to believe that such payment is not so excludable.
5.17 Indemnification of Employer. If any Participant receives one or more payments
or reimbursements under this Plan on a tax-free basis and if such payments do not qualify for
such treatment under the Code, then such Participant shall indemnify and reimburse the County
for any liability that it may incur for failure to withhold federal income taxes, Social Security
taxes, or other taxes from such payments or reimbursements.
5.18 Delegation of Authority. Whenever the County under the terms of this document
is permitted or required to perform any action or service, such action or service shall be done and
performed by any officer or individual representative of the County who is duly authorized by
the County or another individual to whom the County has properly assigned or delegated such
duties.
5.19 Misrepresentations or Fraud. If a Participant deliberately defrauds or misleads the
Plan Administrator about the eligibility or entitlement to benefits of himself or another person,
the Plan Administrator has the right to terminate Plan coverage for that Participant and/or any
family members immediately and retroactively. The Plan shall be entitled to recover (including
by means of offset against future benefits or by withholding from future compensation, to the
extent permitted by law) from the Participant and/or his family members any claims mistakenly
paid due to mistake, fraud or a wrongful attempt to procure coverage, and to recover any costs
and expenses arising from such fraud or misrepresentation, including, but not limited to, costs
and expenses recoverable in actions at law and in equity. Additionally, fraud on the part of the
Participant shall be grounds for disciplinary action up to and including termination of
employment.
Packet Pg. 54
Page 55
17
ARTICLE 6 - AMENDMENT AND TERMINATION
6.1 Amendment. While the County expects and intends to continue the Plan, the
County expressly reserves the right, in its sole and unrestricted discretion, to amend the Plan at
any time, except that any amount which had become payable under the Plan prior to the date an
amendment is effective shall be paid or payable in accordance with the terms of the Plan as in
effect immediately prior to the date of the amendment. Unless otherwise provided under the
Plan, all amendments to the Plan must be in writing and shall be prospective in nature.
6.2 Termination. The Plan may be terminated at any time by the County.
6.3 Benefits on Termination. On termination of the Plan, any amounts that became
payable under the terms of the Plan prior to the date of termination shall be paid in accordance
with the terms of the Plan as in effect prior to the date of such termination.
Packet Pg. 55
Page 56
18
ARTICLE 7 - COMPLIANCE WITH THE HIPAA PRIVACY AND SECURITY RULE
7.1 Purpose. This Section, in compliance with the Privacy Rule and the Security Rule
contained in the Administrative Simplification requirements of the Health Insurance Portability
and Accountability Act of 1996 and the regulations thereunder found at 45 C.F.R. Parts 160, 162
and 164 ("HIPAA"), is intended to allow disclosure of Protected Health Information ("PHI")
including electronic PHI as defined under HIPAA, to County (the "Plan Sponsor") for the
purposes specified below.
Generally, PHI, as defined under HIPAA, includes all individually identifiable
information related to an individual’s past, present or future physical or mental health condition
or to payment for health care. PHI includes information maintained by the Plan in oral, written,
or electronic form. PHI does not include information that has been de-identified. De-identified
information is information that does not identify the individual and with respect to which there is
no reasonable basis to believe that the information can be used to identify the individual.
Electronic PHI (“ePHI”) refers to PHI that is transmitted by or maintained in electronic
media including electronic storage media (such as hard drives, magnetic tapes or disks, optical
disks, and digital memory cards) and electronic transmission media (such as the Internet,
extranets, leased lines, dial-up lines, private networks, telephone voice response systems and
faxback systems, but not paper-to-paper faxes or voicemail messages).
This Section applies only to the “health care components” of the Plan as that term is
defined in 164 CFR §504 of the Privacy Rule contained in the Administrative Simplification
Provisions of HIPAA. In other words, only the Flexible Spending Account benefits provided
pursuant to Supplement B are designated as health care components of the Plan.
To the extent that there is any conflict between this Section and any other Plan
provisions, the terms of this Section as set forth below control. The Plan Administrator and its
duly authorized representatives retain full discretion in interpreting and applying these rules.
7.2 Disclosure of PHI to County. Plan may disclose PHI to the County in the
following circumstances:
Plan receives an authorization from the individual to disclose PHI to the
County.
Plan discloses information to the County on whether an individual is
participating in the Plan.
Packet Pg. 56
Page 57
19
Plan also may provide summary health information to the County so that
the County may modify, amend or terminate the Plan. Summary health
information is information that summarizes the claims history, claims
expenses, or type of claims experienced by the individuals for whom the
County has provided health benefits under the Plan, from which individual
identifiers (other than certain limited geographical information), such as
names and social security numbers, have been removed.
Otherwise, Plan shall disclose PHI to the County only to the extent necessary for the
County to perform administrative functions on behalf of the Plan. (If the County does not
perform such functions, Plan will not disclose PHI to the County other than as indicated above.)
Administrative functions include activities that would meet the definition under the HIPAA
Privacy Rule of treatment, payment, and health care operations activities. Such activities
include, but are not limited to, the following:
Review and resolution of claims for benefits and appeals
Determinations with respect to eligibility and coverage
Determining employee contribution rates
Quality assessment
Auditing, monitoring, and fraud detection and investigation programs
Cost management
Solicitation of proposals for services to be provided to or on behalf of the
Plan
Related computer and systems programming and development.
Notwithstanding anything to the contrary, in no event shall the County be permitted to
use or disclose PHI in a manner that is inconsistent with HIPAA.
7.3 Plan Sponsor Certification. The Plan agrees that it will disclose PHI to the
County only upon receipt of a certification that this Plan document incorporates the following
provisions and that the County agrees to abide by such provisions:
(a) Prohibition on Unauthorized Use or Disclosure of PHI. The County will
not use or disclose any PHI received from the Plan, except as permitted in
the Plan documents or as required by law.
Packet Pg. 57
Page 58
20
(b) Agents (Including Subcontractors). The County will require each of its
agents, including subcontractors, to whom the County provides PHI that it
received from the Plan, to agree to the same restrictions and conditions
that apply to the County with respect to such information.
(c) Impermissible Purposes. The County will not use or disclose PHI for
employment-related actions and decisions or in connection with any other
of the County's benefits or employee benefit plans.
(d) Reporting. The County will report to the Plan any use or disclosure of
PHI, of which it becomes aware, that is inconsistent with the uses and
disclosures permitted by the Plan. Specifically, the Plan Sponsor will
report to the Plan any Breach occurring on or after September 23, 2009, as
defined by 45 CFR § 164.402.
(e) Access to PHI by Participants. The County will make PHI available to the
Plan to permit Participants upon request to inspect and copy their PHI to
the extent provided by 45 CFR § 164.524.
(f) Amendment of PHI. The County will make PHI available to Participants
who request to amend or correct PHI that is inaccurate or incomplete and
will incorporate any amendments to PHI to the extent required and/or
permitted by 45 CFR § 164.526.
(g) Accounting of PHI. The County will make available the information
required to provide an accounting of disclosures in accordance with 45
CFR § 164.528.
(h) Disclosure to the Secretary. The County will make its internal practices,
books and records relating to the use and disclosure of PHI received from
the Plan available to the Secretary of the Department of Health and
Human Services or its designee for the purpose of determining the Plan's
compliance with HIPAA.
(i) Breach Notification. The Plan Sponsor will cooperate with the Plan’s
efforts to comply with the Breach notification regulations set forth in 45
CFR §§ 164.404, 164.406 and 164.408.
Packet Pg. 58
Page 59
21
(j) Return or Destruction of PHI. When the PHI is no longer needed for the
purpose for which disclosure was made, the County must, if feasible,
return to the Plan or destroy all PHI that the County received from the
Plan, and retain no copies in any form. If return or destruction is not
feasible, the County agrees to limit further uses and disclosures to the
purposes that make the return or destruction infeasible.
(k) Adequate Separation. The County must ensure that adequate separation
exists between the Plan and the County so that PHI will be used only for
plan administration. The following employees, classes of employees or
persons under the control of the County may have access to and may use
PHI, but only to the extent necessary to perform the administration
functions that (i) are to be performed by the County as set forth under (b)
above and (ii) are assigned to such employees as a part of their job duties:
An officer or employee or committee thereof that serves as Plan
Administrator;
An officer or employee who serves as a Plan fiduciary;
An officer or employee who serves as the Privacy or Security
Officer under HIPAA;
An employee of the Human Resources, Payroll, Accounting,
Finance, Information Technology, or Legal Departments.
In the event that any such persons do not comply with the requirements set
forth herein, such persons shall be subject to disciplinary action by the
County for noncompliance, pursuant to the County’s discipline and
termination or removal procedures. The County shall take whatever
actions necessary to resolve such noncompliance. Regardless of whether a
person is disciplined, terminated or removed pursuant to this paragraph,
the Plan reserves the right to direct that the County modify or revoke any
person’s access to or use of PHI, and the County shall take such action as
warranted. Anyone who suspects an improper use or disclosure of PHI
may report the occurrence to the Plan's Privacy Officer at the telephone
number and address provided in the Plan’s notice of privacy practices.
Packet Pg. 59
Page 60
22
(l) Protection of Electronic PHI. If electronic PHI is created, received,
maintained, or transmitted to or by the Plan Sponsor on behalf of the Plan,
the Plan Sponsor will do the following:
Ensure that the “adequate separation” described in subparagraph
(10) above is supported by reasonable and appropriate security
measures;
Implement administrative, physical, and technical safeguards that
reasonably and appropriately protect the confidentiality, integrity,
and availability of such electronic PHI;
Ensure that any agent (including a subcontractor) to whom it
provides such electronic PHI agrees to implement reasonable and
appropriate security measures to protect the information; and
Report to the Plan any security incident of which it becomes
aware. For purposes of this provision, “security incident” is
defined as the attempted or successful unauthorized access, use,
disclosure, modification, or destruction of information or
interference with system operations in an information system.
Notwithstanding the above, if the only ePHI that is disclosed to the Plan
Sponsor is disclosed pursuant to a HIPAA-compliant authorization or is
limited to Summary Health Information (as defined in the Privacy Rule)
disclosed for the purpose either of obtaining premium bids for providing
health insurance coverage under the Plan, or modifying, amending or
terminating the plan, and information regarding an individual’s
participation, enrollment or disenrollment, the requirements of this
subparagraph do not apply.
Packet Pg. 60
Page 61
23
ARTICLE 8 - EXECUTION OF PLAN
IN WITNESS WHEREOF, the Plan and Supplements A, B and C are hereby executed
effective as of the _______________ day of _______________, 20143.
1. ATTEST: 2. COUNTY OF KANE
3. By:
4. By:
5. Its:
6. Its:
Packet Pg. 61
Page 62
A-1
SUPPLEMENT A
PRE-TAX PREMIUM ACCOUNT
A-1 Purpose. Each Plan Year, each Participant will be entitled to pay his share (if
any) of the premium cost for the elected group welfare insurance coverage (such as group
medical or dental) for that year with pre-tax dollars through payroll withholding. Salary
reduction amounts from the last month of one Plan Year may be applied to pay group health
insurance premiums for insurance during the first month of the immediately following Plan Year.
A-2 Election of Coverage. In order to elect coverage under the Pre-Tax Premium
Account, a Participant must file the necessary election form provided by the County within the
applicable period pursuant to Section 3.1 of the Plan. The form must specify the type of
coverage elected and whether pre-tax dollars are to be applied for premium payments. If pre-tax
dollars are to be used for either medical or dental insurance, then both types of insurance must be
paid for pre-tax. If, for succeeding Plan Years, a Participant does not submit a new election
form, he will be deemed to have elected the type and level of coverage under the Pre-Tax
Premium Account in effect on the last day of the preceding Plan Year.
A-3 Incorporated Plans. The County's group welfare insurance plans, as adopted by
the County, and the Teamsters Plan, to which employees may make pre-tax contributions are
hereby incorporated by reference into the Plan.
A-4 Irrevocable Elections. Any coverage elected under Section A-2 shall be
irrevocable for the duration of the Plan Year except in the event of a change in status, or as
otherwise provided pursuant to Section 3.2 of the Plan.
Packet Pg. 62
Page 63
B-1
SUPPLEMENT B
FLEXIBLE SPENDING ACCOUNT
B-1 Purpose. Each Participant will be entitled to choose between (a) reimbursement
for "Medical Care Expenses" (as defined below) not reimbursed by any other plan or taken as an
income tax deduction, and (b) cash compensation. It is intended that this Flexible Spending
Account (the "Health Care Account") qualify as a nondiscriminatory cafeteria plan benefit under
Code Section 125 and as an accident and health care plan within the meaning of Code Section
105(e) and that reimbursements paid hereunder be eligible for exclusion from the Participant's
income under Code Section 105(b).
B-2 Election of Coverage. In order to elect coverage under the Health Care Account,
Participants must file the appropriate election form provided by the County within the applicable
period pursuant to Section 3.1 of the Plan. Each Participant may designate no less than $120 and
no more than $2,5500 (as indexed for inflation) of coverage under the Health Care Account (the
"elected coverage"), and his compensation from the County shall be reduced, by the amount of
the elected coverage, and shall be credited to the Participant's Health Care Account.
B-3 Allowable Benefits Under Health Care Account. Reimbursements to a Participant
shall be permitted hereunder only with respect to “Medical Care Expenses,” that is, amounts
expended (and not reimbursed by any other plan or taken as an income tax deduction) for
"medical care" (within the meaning of Code Section 213(d)) of the Participant or the
Participant’s tax qualified dependents under Code Section 105(b).
(a) For purposes of a Health Care Account, examples of Medical Care Expenses are
set forth below:
1. Deductibles and co-payments under the County's health plans or the
Teamsters Plan (including dental and vision plans) or under personal
accident and health insurance carried by the Participant, his spouse, or
covered dependents;
2. Prescription drugs;
3. Over-the-counter drugs and products such as antacids, allergy medicines,
pain relievers and cold medicines will not be reimbursed unless the
individual has a prescription for such over-the-counter drugs and
medicines, except that a prescription is not needed for insulin;
Packet Pg. 63
Page 64
B-2
4. Eye care, including vision checkups, eyeglasses and contact lenses;
5. Hearing care, including hearing examinations and hearing aids;
6. Routine physical examinations;
7. Any other medical care item that constitutes medical care within the
meaning of Code Section 213(d).
B-4 Substantiation/Correcting Improper Reimbursements. A Participant must provide
third-party substantiation of any Medical Care Expenses incurred for which reimbursement is
sought by the Participant.
In the event that a Medical Care Expense is improperly reimbursed due to insufficient or
improper substantiation, overpayment, fraud or otherwise, the Plan Administrator shall, to the
extent that it deems administratively possible and otherwise permissible under applicable law,
seek repayment of such improper reimbursement by (1) requesting the Participant direct payment
to the Plan, (2) withholding the corresponding amount from the Participant’s compensation on an
after-tax basis (where such withholding is permissible under applicable law), or (3) offsetting the
improper reimbursement against other valid Medical Care Expense claims.
B-5 Limitations. For each Plan Year, the Participant may be reimbursed for Medical
Care Expenses up to the full amount of elected coverage the Participant has elected for the Plan Year
plus any amounts carried over from a prior Pplan Yyear (in accordance with Section B-8), less any
prior reimbursements for this period. The amount of elected coverage by a Participant for a Plan Year
is only available to reimburse expenses that are incurred during the Plan Year during which an
election is in effect hereunder, unless such amount is carried over to a subsequent Plan Year (in
accordance with Section B-8). Participants shall have ninety daysthree months following the end
of the Plan Year to submit claims for such expenses, except that terminated employees will have
thirty days from the date of their termination to submit claims. An expense is incurred during the
Plan Year if the services giving rise to the expenses are performed during the Plan Year. An
expense shall not be deemed to be incurred during the Plan Year merely because a Participant
receives a bill for the expense during the Plan Year or pays for the expense during the Plan Year.
B-6 Nondiscrimination Requirements. It is intended that contributions and benefits
under the Flexible Spending Account not be discriminatory under the provisions of the Code. In
that regard, notwithstanding anything contained herein to the contrary, the Plan Administrator
may limit the amounts reimbursed or paid to any Participant who is considered a highly
Packet Pg. 64
Page 65
B-3
compensated individual under Code Sections 105(h)(5) or 125(e) or to any Participant who is
considered a key employee under Code Section 125(b)(2) to the extent the Plan Administrator
deems such limitation advisable to comply with any restrictions contained in the Code.
B-7 Forfeiture. Unless as otherwise provided in Section B-11, if a Participant incurs
during the Plan Year a Participant incurs aggregate expenses qualifying for reimbursement less than
the dollar amount of coverage the Participant elects for such Plan Year, any remaining amount in
excess of $500 in the Participant’s Health Care Account as of the end of that Plan Year (and after
application of Section B-10) shall be forfeited. Any amount of coverage in excess of $500 for a Plan
Year that is unused due to the Participant’s failure to submit proper claims for reimbursements in
conformity with the procedure prescribed by the Plan also shall be forfeited. Subject to the
requirements of applicable law, forfeitures will be paid to the County to defray Plan administrative
expenses, reduce required salary reduction amounts for the next Plan Year on a reasonable and
uniform basis, or be allocated to participating employees on a reasonable and uniform basis.
B-8 Carry-over. Up to $500 of the amount remaining in the Participant’s Health Care
Account as of the end of the Plan Year (and after application of Section B-10) shall be carried
over for use by the Participant during the next following Plan Year.
B-9 Irrevocable Elections. Any coverage elected under Section B-2 shall be
irrevocable for the duration of the Plan Year except in the event of a change in status, or as
otherwise provided pursuant to Section 3.2 of the Plan.
B-10 Run-Out Period. A Run-Out Period is a period after the end of the Plan Year
during which a Participant can submit a claim for reimbursement for a qualified benefit incurred
during the Plan Year. Notwithstanding any provision in the Plan to the contrary, the Plan shall
reimburse the expenses of any Participant submitted during the applicable Run-Out Period, to the
extent they are otherwise eligible for reimbursement under the terms of the Plan. For this
purpose, the term “Run-Out Period” shall mean the 3-month period immediately following the
close of each Plan Year.
B-11 Qualified Reservist Distributions. This Section contains special provisions that
are intended to incorporate qualified reservist distributions permitted by the Heroes Earnings
Assistance and Relief Tax Act of 2008, P.L. 110-245 (the “HEART Act”). The provisions of
this Section shall operate in conjunction with other Plan provisions. In case of conflict or
ambiguity between this section and other provisions of the Plan, the Plan shall be administered in
Packet Pg. 65
Page 66
B-4
accordance with the intention of this Section, as stated above, to the extent permitted under
applicable law, regulatory requirement, or published tax guidance.
Notwithstanding any provision in the Plan to the contrary, the Plan shall distribute to a
Participant all or a portion of the balance in the Participant’s Health Care Account if:
(a) such Participant is a member of a reserve component ordered or called to active duty
for a period of 180 days or more or for an indefinite period, and
(b) such distribution is made during the period beginning on the date of such order or call
and ending on the last date that reimbursements could otherwise be made for the Plan Year
which includes the date of such order or call.
No qualified reservist distributions shall be paid on behalf of anyone other than a
Participant who is ordered or called to active duty. The Participant ordered or called to active
duty must provide the County with a copy of the order or call to active duty before an amount
may be distributed. The request for a qualified reservist distribution must be made on or after the
date of the order or call to active duty, and before the last day of the Plan Year during which the
order or call to active duty occurred. Qualified reservist distributions shall be paid no later than
sixty days after the date of the request for a qualified reservist distribution.
For purposes of making a qualified reservist distribution, the Participant’s Health Care
Account balance available for such a distribution will be the amount contributed to the Health
Care Account as of the date of the qualified reservist distribution request minus Health Care
Account reimbursements received as of the date of the qualified reservist distribution request.
A qualified reservist distribution will not be made with respect to amounts (1) attributable
to a prior plan year (including a plan year ending on or before June 18, 2008), or (2) attributable
to non-Health Care Accounts.
With respect to medical expenses incurred after the date a qualified reservist distribution
is requested, the Plan will terminate the Participant’s right to submit claims.
Packet Pg. 66
Page 67
C-1
SUPPLEMENT C
DEPENDENT CARE REIMBURSEMENT ACCOUNT
C-1 Purpose. Each eligible Participant will be entitled to choose between (a)
reimbursement for "Dependent Care Expenses" (as defined below) for which a dependent care
tax credit is not taken, and (b) cash compensation. It is intended that the Dependent Care
Reimbursement Account (the "Dependent Care Account") qualify as a nondiscriminatory
cafeteria plan benefit under Code Section 125 and as a dependent care reimbursement plan
within the meaning of Code Section 129 and that reimbursements paid hereunder be eligible for
exclusion from Participants' income under Code Section 129(a).
C-2 Election of Coverage. In order to elect coverage under the Dependent Care
Account, Participants must file the appropriate election form provided by the County within the
applicable period pursuant to Section 3.1 of the Plan. Each Participant may designate no less
than $120 and no more than up to $5,000 ($2,500 where the Participant is married and files a
separate return) of coverage (the "elected coverage"), provided however, that each Participant's
elected coverage under the Dependent Care Account shall be limited to the lesser of (a) the
Participant's Earned Income for the Plan Year, or (b) the Participant's spouse's Earned Income for
the Plan Year. For purposes of this Supplement C, Earned Income means the individual's
compensation from the individual’s employer plus the amount of the individual's net earnings
from self-employment during the Plan Year, computed without regard to any community
property laws, without taking into account any amount received as a pension or annuity, and
without taking into account any amounts paid under the Plan or under a dependent care
reimbursement plan of any other employer. If the Participant's spouse is a Qualifying Individual
or is a full-time student (as defined in Code Section 21(d)(2)), such spouse will be deemed to
have Earned Income for purposes of this Supplement for each month during the Plan Year in
which the spouse has such status, equal to either (1) $200, if there is one Qualifying Individual
with respect to the Participant; or (2) $400, if there is more than one Qualifying Individual with
respect to the Participant. The $5,000 limit shall be reduced by the amount of dependent care
assistance received under a plan of the employer of the Participant's spouse. The Participant's
compensation from the County shall be reduced, by the amount of the elected coverage, in equal
amounts each payroll period and shall be credited each payroll period to the Participant's
Dependent Care Account.
Packet Pg. 67
Page 68
C-2
C-3 Allowable Benefits Under The Dependent Care Account. Reimbursements to a
Participant shall be permitted hereunder only with respect to Dependent Care Expenses which
are incurred while an election is in effect either during the Plan Year, or, if shorter, during the
Participant's period of employment within the Plan Year, for which a dependent care tax credit is
not taken on the Participant's income tax return, up to the amount of coverage elected by the
Participant for the Plan Year. Dependent Care Expenses shall include only amounts paid which
constitute "employment related expenses" within the meaning of Code Section 21. Dependent
Care Expenses must be incurred for the care of a Qualifying Individual ((i) a child of a
Participant who is under the age of thirteen (13) and with respect to whom the Participant is
entitled to the deduction under Code Section 151(c), or, (ii) a “Dependent” (as defined in Code
Section 152, except if the Participant is divorced then as defined in Code Section 21(e)(5)) or the
Participant's spouse who is physically or mentally incapable of caring for himself) and to enable
the Participant to be gainfully employed. Dependent Care Expenses shall be limited to: (a)
amounts paid for services rendered in the Participant's home; or (b) amounts paid for services
rendered outside of the Participant's home only if such services are provided for the care of a
Qualified Individual who is under age thirteen (13), or who is age thirteen (13) or older and who
regularly spends at least eight (8) hours a day in the Participant's home provided that services
rendered in a dependent care center (as defined in Code Section 21) must satisfy the
requirements of Code Section 21 and the regulations promulgated thereunder.
C-4 Limitations. For each Plan Year, the Participant may be reimbursed for
Dependent Care Expenses up to the dollar amount of elected coverage the Participant has
accumulated in his Dependent Care Account through contributions to that date less any prior
reimbursements for this period. If the Participant's expenses exceed the accumulated amount to
date, the Participant will receive additional reimbursements hereunder as the Participant
accumulates additional funds in his Dependent Care Account. The amount of elected coverage
by a Participant for a Plan Year is only available to reimburse expenses that are incurred during
the Plan Year during which an election is in effect hereunder. Participants shall have ninety
daysthree months following the end of the Plan Year to submit claims for these expenses, except
that terminated employees will have thirty days from the date of their termination to submit
claims. An expense is incurred during the Plan Year if the services giving rise to the expense are
performed during the Plan Year. An expense shall not be deemed to be incurred during the Plan
Packet Pg. 68
Page 69
C-3
Year merely because a Participant receives a bill for the expense during the Plan Year or pays for
the expense during the Plan Year.
C-5 Nondiscrimination Requirements. It is intended that contributions and benefits
under the Dependent Care Reimbursement Account not be discriminatory as prohibited by Code
Section 129(d). FurtherAccordingly, the average benefits provided to non-highly compensated
employees (excluding, in the Plan Administrator’s discretion, employees earning less than
$25,000) must be at least 55% of the average benefits provided to highly compensated
employees (as defined in Code Section 414(q)). If the Plan Administrator believes that this limit
may be exceeded, it may, in its own discretion and notwithstanding anything herein to the
contrary, limit the amount of benefits paid with respect to such individuals to the extent the Plan
Administrator deems such limitation advisable in order to comply with the restrictions contained
herein or any other nondiscrimination provision contained in the Code.
C-6 Forfeiture. If a Participant incurs during the Plan Year aggregate expenses
qualifying for reimbursement less than the amount of elected coverage for a Plan Year, any
remaining amount in his Dependent Care Account as of the end of the Plan Year shall be
forfeited. Any amount of elected coverage for a Plan Year unused due to the Participant's failure
to submit proper claims for reimbursements in conformity with the procedures prescribed by the
Plan shall also be forfeited. Subject to requirements of applicable law, forfeitures will be paid to
the County.
C-7 Irrevocable Elections. Any coverage elected under Section C-2 shall be
irrevocable for the duration of the Plan Year except in the event of a change in status, or as
otherwise provided pursuant to Section 3.2 of the Plan.
C-8 Spend Down for Terminated Employees. Expenses incurred within ninety (90)
days after the date an employee ceases participation in the Plan (for example, after termination)
may be reimbursed from unused benefits.
C-9 Run-Out Period. A Run-Out Period is a period after the end of the Plan Year
during which a Participant can submit a claim for reimbursement for a qualified benefit incurred
during the Plan Year. Notwithstanding any provision in the Plan to the contrary, the Plan shall
reimburse the expenses of any Participant submitted during the applicable Run-Out Period, to the
extent they are otherwise eligible for reimbursement under the terms of the Plan. For this
Packet Pg. 69
Page 70
C-4
purpose, the term “Run-Out Period” shall mean the 3-month period immediately following the
close of each Plan Year.
Packet Pg. 70
Page 71
SUMMARY OF THE
COUNTY OF KANE
FLEXIBLE BENEFITS PLAN
EFFECTIVE JANUARY 1, 2015DECEMBER 31, 2013
This booklet describes the Plan provisions that currently affect your benefits under the
Plan. If, in the future, the provisions described herein should change for any reason, you will be
provided with a summary of the changes.
IF FOR ANY REASON THERE IS AN OMISSION OR MISSTATEMENT IN
THIS BOOKLET, OR ANY DIFFERENCE BETWEEN THIS BOOKLET AND THE
LEGAL PLAN DOCUMENTS, THE LEGAL PLAN DOCUMENTS WILL IN ALL
RESPECTS CONTROL AND GOVERN.
Packet Pg. 71
Page 72
-i-
TABLE OF CONTENTS
Page
SUMMARY OF THE ..................................................................................................................... 1
COUNTY OF KANE ...................................................................................................................... 1
FLEXIBLE BENEFITS PLAN....................................................................................................... 1
PREAMBLE ................................................................................................................................... 1
GENERAL INFORMATION ......................................................................................................... 2
WHICH TWELVE (12) MONTH PERIOD DOES THE PLAN USE FOR
RECORDKEEPING PURPOSES? ......................................................................................... 3
WHO PAYS FOR THE BENEFITS UNDER THE PLAN? .......................................................... 3
WHEN WILL I BE ELIGIBLE TO PARTICIPATE IN THE PLAN? .......................................... 3
HOW DO I ELECT TO PARTICIPATE IN THE BENEFITS AVAILABLE THROUGH
THE PLAN? ............................................................................................................................ 4
WHEN AND UNDER WHAT CIRCUMSTANCES MAY I CHANGE MY
ELECTION? ............................................................................................................................ 4
ELECTION CHANGES IMPOSED BY THE PLAN .................................................................. 10
WHAT BENEFITS ARE AVAILABLE UNDER THE PLAN? ................................................. 10
WHAT HAPPENS IF I DON’T USE UP ALL OF THE ELECTED BENEFITS PRIOR
TO THE END OF THE PLAN YEAR? ................................................................................ 14
WHAT HAPPENS IF I RECEIVE REIMBURSEMENTS TO WHICH I AM NOT
ENTITLED UNDER THE PLAN? ....................................................................................... 14
WHAT HAPPENS IF I TERMINATE EMPLOYMENT? .......................................................... 15
AM I ENTITLED TO CONTINUE COVERAGE UNDER THE PLAN? .................................. 15
WHAT HAPPENS IF THIS PLAN IS DISCONTINUED OR AMENDED? ............................. 21
ADMINISTRATION .................................................................................................................... 21
PROCEDURES FOR MAKING A CLAIM AND AN APPEAL FOR BENEFITS ................... 22
FULL DETAILS IN LEGAL PLAN DOCUMENTS .................................................................. 26
GENERAL PLAN INFORMATION ........................................................................................... 27
PREAMBLE ................................................................................................................................... 1
GENERAL INFORMATION ......................................................................................................... 2
Packet Pg. 72
Page 73
WHICH TWELVE (12) MONTH PERIOD DOES THE PLAN USE FOR
RECORDKEEPING PURPOSES? ......................................................................................... 3
WHO PAYS FOR THE BENEFITS UNDER THE PLAN? .......................................................... 3
WHEN WILL I BE ELIGIBLE TO PARTICIPATE IN THE PLAN? .......................................... 3
HOW DO I ELECT TO PARTICIPATE IN THE BENEFITS AVAILABLE THROUGH
THE PLAN? ............................................................................................................................ 3
WHEN AND UNDER WHAT CIRCUMSTANCES MAY I CHANGE MY
ELECTION? ............................................................................................................................ 3
ELECTION CHANGES IMPOSED BY THE PLAN .................................................................... 7
WHAT BENEFITS ARE AVAILABLE UNDER THE PLAN? ................................................... 8
WHAT HAPPENS IF I DON’T USE UP ALL OF THE ELECTED BENEFITS PRIOR
TO THE END OF THE PLAN YEAR? ................................................................................ 10
WHAT HAPPENS IF I TERMINATE EMPLOYMENT? .......................................................... 10
AM I ENTITLED TO CONTINUE COVERAGE UNDER THE PLAN? .................................. 10
WHAT HAPPENS IF THIS PLAN IS DISCONTINUED OR AMENDED? ............................. 16
ADMINISTRATION .................................................................................................................... 16
PROCEDURES FOR MAKING A CLAIM AND AN APPEAL FOR BENEFITS ................... 16
FULL DETAILS IN LEGAL PLAN DOCUMENTS .................................................................. 19
GENERAL PLAN INFORMATION ........................................................................................... 21
Packet Pg. 73
Page 74
PREAMBLE
The County of Kane (the “County”) is pleased to sponsor a cafeteria plan for the eligible
employees of the County effective as of January 1, 2006. The Plan is named the County of Kane
Flexible Benefits Plan (hereinafter sometimes referred to as the “Plan”).
This Summary of the Plan is effective January 1, 2015December 31, 2013, and is
intended to provide you with a general description of its highlights. If you have any questions
after reading the Summary, please contact the Plan Administrator, at the Department of Human
Resources Management.
IF FOR ANY REASON THERE IS AN OMISSION OR MISSTATEMENT IN
THIS BOOKLET, OR ANY DIFFERENCE BETWEEN THIS BOOKLET AND THE
LEGAL PLAN DOCUMENTS, THE LEGAL PLAN DOCUMENTS WILL IN ALL
RESPECTS CONTROL AND GOVERN.
Packet Pg. 74
Page 75
-2-
GENERAL INFORMATION
Through the Plan you can elect to participate in the following benefits:
(a) Pre-Tax Premium Account.
(b) Flexible Spending Account.
(c) Dependent Care Reimbursement Account.
These are separate benefits. Your election to be covered under one benefit will not
obligate you to participate in the other benefits.
Participation in the Plan allows you to make contributions (that are withheld from your
paychecks) to a Pre-Tax Premium Account to pay for your share of the cost of your participation
in the County’s group welfare plans (such as group medical or dental) or the Teamsters Plan on a
pre-tax basis. Participation also allows you to make contributions (also via paycheck
withholding) that go into the reimbursement accounts for reimbursement of eligible health care
and dependent care expenses on a pre-tax basis. The contributions withheld from your
paychecks are excluded from your taxable income and, as a result, your taxable income is
reduced.
This can be illustrated by the following example:
With Without
Your Plan Your Plan
-------- --------
Gross Taxable Wages $25,000. $25,000.
Pre-tax Contribution $1,800. N/A
-------- --------
Taxable Wages $23,200. $25,000.
Estimated Taxes* $3,480. $3,750.
After-tax Expenditure N/A $1,800.
-------- --------
Take-home Pay $19,720. $19,450.
* Joint Return, 15% marginal tax rate
By paying for benefits before taxes are calculated, estimated taxes are reduced by $270, which is
$22.50 per month more in take-home pay for the example person. In other words, paying for
Packet Pg. 75
Page 76
-3-
benefits without participating in the Plan costs this person $22.50 more per month.
Because participation in the Plan reduces your gross taxable income, it may affect your
entitlement to Social Security benefits. In most instances, the benefit of the current tax savings
(as illustrated above) will outweigh the slight impact on future Social Security benefits.
Please consult your tax advisor for a more accurate estimate for your situation.
WHICH TWELVE (12) MONTH PERIOD DOES THE PLAN USE FOR
RECORDKEEPING PURPOSES?
Records for the Plan are maintained on a twelve-consecutive month period beginning on
January 1 and ending on December 31. This is called the Plan Year.
WHO PAYS FOR THE BENEFITS UNDER THE PLAN?
All contributions to the Plan will be made by you from income withheld from your
paychecks that you elect to have diverted to the Plan.
WHEN WILL I BE ELIGIBLE TO PARTICIPATE IN THE PLAN?
All employees of the County who are eligible to participate in the County’s group
medical plan and group dental plan are eligible to contribute to the Pre-Tax Premium Account,
Flexible Spending Account and the Dependent Care Reimbursement Account on the later of
January 1, 2006, or on the date that the employee becomes eligible for and enrolls in the
County’s group medical or dental plan. Also, an employee of the County’s Department of
Transportation who is eligible to participate in the Suburban Teamsters of Northern Illinois
Welfare Fund (the “Teamsters Plan”) shall be eligible to become a participant in the Plan on the
first day that the employee becomes eligible to participate in the Teamsters Plan, with actual
enrollment to occur as soon as practicable following the employee’s submission of a completed
election form. If an employee of the County also provides services to the County as an
independent contractor or director, the employee is eligible to participate in the Plan solely in his
capacity as an employee.
Packet Pg. 76
Page 77
-4-
HOW DO I ELECT TO PARTICIPATE IN THE BENEFITS AVAILABLE THROUGH
THE PLAN?
Prior to meeting the eligibility requirements, you will be given a Section 125 Plan
Enrollment form and a Health/Dependent Care Flexible Spending Accounts-FSA Enrollment
form. The forms must be completed and returned to the Department of Human Resource
Management within thirty (30) days from your date of eligibility. Your election will be effective
beginning with the first day of the payroll period coincident with or next following the date you
submit a completed Compensation Reduction Agreement form, provided that the form is
received by the Department of Human Resource Management within thirty (30) days from your
date of eligibility. In order to continue coverage with respect to the Flexible Spending Account,
however, you must submit a new Health/Dependent Care Flexible Spending Accounts-FSA
Enrollment form each year.
WHEN AND UNDER WHAT CIRCUMSTANCES MAY I CHANGE MY ELECTION?
You will be notified once each year, during the 45-day period prior to each January 1, of
your right to change your election and provided with a new Health/Dependent Care Flexible
Spending Accounts-FSA Enrollment form. The form must be returned to the Department of
Human Resource Management at least 30 days prior to January 1 of each Plan Year or such other
time as determined by the County and set forth in a written policy to be communicated to all
eligible employees.
Additionally, if the cost of participation in one of the County’s welfare plans (e.g.,
medical or dental coverage) or the Teamsters Plan increases or decreases during a period of
coverage, and, under the terms of the respective plan, you are required to make a corresponding
change in payments, the Plan may, on a reasonable and consistent basis, automatically make a
prospective increase or decrease in your elective contributions to the Plan. In addition, if the cost
of participation in one of the County’s contributory welfare plans (e.g., medical or dental
insurance) increased during the Plan Year, or any prior Plan Year, and, under the terms of the
respective plan, you were required to make a corresponding change in payments, but the County
inadvertently failed to implement such change, the County may, on a reasonable and consistent
basis, require you to pay the difference. One (but not the only) means for doing so would be to
enter into a payment plan whereby any past-due payments that were required to be paid by you
are withheld from your pay over a reasonable period of time.
Packet Pg. 77
Page 78
-5-
Once an election is made, it cannot be changed by you during the Plan Year except under
the following circumstances:
1. HIPAA Special Enrollment: You may revoke an existing election and make a new
election that corresponds with special enrollment rights under the Health
Insurance Portability and Accountability Act of 1996 (“HIPAA”).
2. Change in Status: If you have a change in status you may revoke or change a
benefit election provided the election change is on account of and consistent with
the change in status, and the change in status affects the eligibility of yourself,
your spouse or dependeant under an employer’s cafeteria plan or other employee
welfare benefit plan in which any of you are a participant. A change in status
includes:
(a) your marriage, the death of your spouse, your divorce, legal separation or
annulment;
(b) the death of your dependent, or the birth, adoption or placement for
adoption of your child, or an event that otherwise results in an increase or
decrease in the number of your family members or dependents who may
benefit from coverage under the Plan;
(c) a change in employment status of your spouse or dependent or yourself
including the termination or commencement of employment, a strike or
lockout, a commencement of or return from an unpaid leave of absence, a
change in worksite, a reduction or increase in hours of employment,
including a switch from part-time to full-time employment status or vice
versa, or a switch from hourly to salaried employment or vice versa;
(d) an event causing your dependent to satisfy or cease to satisfy the
requirements for coverage due to attainment of age, student status, or any
similar circumstance as provided in the health plan under which you
receive coverage;
(e) a change in the place of residence of yourself or your spouse or dependent;
and
Packet Pg. 78
Page 79
-6-
(f) such other events as the Plan Administrator determines qualify as a change
in status, consistent with regulations and rulings of the Internal Revenue
Service.
3. Reduction of weekly hours of employment below 30: You may revoke an existing
election and make a new election if you experience a reduction in hours of
employment such that (1) you reasonably are expected to work an average of less
than 30 hours per week after reasonably having been expected to average at least
30 hours per week (even if the reduction in hours of employment does not result
in you ceasing to be eligible under the County’s group health plan); and (2) the
revocation of a benefit election under the Plan corresponds to the intended
enrollment of yourself and, as applicable, your spouse or dependent, who cease
coverage due to the revocation in another plan that provides minimum essential
coverage, where such new coverage is effective no later than the first day of the
second month following the month that includes the date the benefit election is
revoked;
4. Enrollment in a Qualified Health Plan: You may revoke an existing election and
make a new election that corresponds with your enrollment in a “Qualified Health
Plan” (as purchased through a marketplace established pursuant to Section 1131
of the Patient Protection and Affordable Care Act of 2010 (a “Marketplace”)), if
(1) you are eligible for a “special enrolment period” to enroll in such Qualified
Health Plan pursuant to guidance issued by the Department of Health and Human
Services and any other applicable guidance, or you seek to enroll in a Marketplace
during the Marketplace’s annual open enrollment period; and (2) the revocation of
your benefit election under the Plan corresponds to the intended enrollment of
yourself and, if applicable, your spouse or dependent, who cease coverage due to
the revocation, in a Qualified Health Plan through a Marketplace for new
coverage that is effective beginning no later than the day immediately following
the last day of the revoked coverage;[LMDBLT1]
3.5. COBRA Eligibility: In the event you, your spouse or your dependent becomes
eligible for continuation coverage under your County’s group medical or dental
plan or the Teamsters Plan pursuant to federal law known as “COBRA,” you may
Packet Pg. 79
Page 80
-7-
elect to modify payments under the Plan as appropriate in order to pay for the
continuation coverage;
4.6. Court Order: Upon the entry of a judgment, decree or court order (including a
qualified medical child support order under Section 609 of the Employee
Retirement Income Security Act of 1974) resulting from a divorce, legal
separation, annulment or change in legal custody requiring you or your former
spouse to provide or cancel health coverage with respect to a child (cancellation
to be permitted only if the order also requires another person to provide coverage
for the child and such coverage actually is provided);
5.7. Entitlement to Medicare/Medicaid: In the event you, your spouse or your
dependent who isare enrolled in the County’s group health plan or the Teamsters
Plan becomes entitled to or loses eligibility for coverage under Medicare or
Medicaid, then you may cancel, reduce, add, or increase coverage for yourself,
your spouse or your dependent accordingly.
6.8. Significant change in Cost or Coverage (not applicable to the Flexible Spending
Account election): You may revoke an election and file a new election for the
balance of the Plan Year under the following circumstances:
(a) if the cost to you (if any) for a benefit package option (e.g., a welfare
benefit offered through this Plan, or an option for coverage under an
underlying health plan, such as an indemnity option, an HMO option, or a
PPO option) significantly increases or decreases (whether that increase or
decrease results from an action taken by you or from an action taken by
the County), or, with respect to the Dependent Care Reimbursement
Account election, a significant cost change is imposed by a dependent care
provider who is not your relative, you may make a corresponding election
change for the balance of the Plan Year;
(b) if coverage under one of the County’s welfare plans (e.g., medical or
dental coverage) or the Teamsters Plan or a welfare plan of your spouse or
dependent, is significantly curtailed or ceases (for example, there is a
significant increase in the deductible, copay or out-of-pocket cost sharing
limit under a health plan) during such Plan Year, but there is not a loss of
Packet Pg. 80
Page 81
-8-
coverage as defined in (c) below, you may revoke your election for that
coverage and, in lieu thereof, elect to receive on a prospective basis
coverage under another benefit package option providing similar
coverage, provided such changes are permitted under the terms of the
applicable welfare benefit plan;
(c) if you or your spouse or dependent has a significant curtailment of
coverage that is a loss of coverage (that is, a complete loss of coverage
under the benefit package option or other coverage option (including the
elimination of a benefits package option, an HMO ceasing to be available
in the area where you reside, or your losing all coverage under the option
by reason of an overall lifetime or annual limitation)), you may revoke
your election under the Plan and, in lieu thereof, elect either to receive on
a prospective basis coverage under another benefit package option
providing similar coverage or to drop coverage if no similar benefit
package option is available, provided such changes are permitted under
the terms of the applicable welfare benefit plan;
(d) if a new benefit package option or other coverage option is added or if
coverage under an existing benefit package option or other coverage
option is significantly improved, you may revoke your election, and, in
lieu thereof, make an election on a prospective basis for coverage under
the new or improved benefit package option, provided such changes are
permitted under the terms of the applicable welfare benefit plan; or
(e) you may make an election change on account of and corresponding with a
change made under the plan of your spouse’s, former spouse’s or
dependent’s employer provided the election under your spouse’s or
dependent’s plan satisfies both that plan’s election change rules and IRS
regulations regarding election changes, or your spouse’s or dependent’s
plan has a different period of coverage.
7.9. FMLA: In the event that you take a paid leave of absence under the Family
Medical Leave Act (“FMLA”), your elections under the Plan with respect to the
Pre-Tax Premium Account and the Flexible Spending Account will remain the
Packet Pg. 81
Page 82
-9-
same, and you will continue to make contributions in the same way that you made
them prior to taking the leave of absence. You may make an election change with
respect to a Dependent Care Reimbursement Account, provided the change is on
account of and consistent with the leave. You will not be entitled to
reimbursement of Dependent Care claims incurred during an FMLA leave.
If you take an unpaid leave of absence under the FMLA, you may revoke an
existing election or continue health coverage (such as medical or dental coverage)
under the County’s health plans or the Teamsters Plan (to the extent permitted by
that plan), or coverage under the Flexible Spending Account.
If you elect to continue coverage, you have two payment options: (i) pre-pay or
(ii) pay-as-you-go. Under the pre-pay option, you may pay the premiums and
contributions due during the FMLA leave period on a pre-tax salary reduction
basis from any taxable compensation or on an after-tax basis prior to
commencement of the leave. (Certain restrictions apply, however, if your FMLA
leave spans two Plan Years.) Under the pay-as-you-go option, you may pay your
share of premium payments and contributions on a monthly basis on the first of
every month (the same schedule as COBRA payments). These payments
typically would be made on an after-tax basis, unless you receive taxable
compensation during the leave period (e.g., as a result of unused sick days or
vacation days). If you fail to make payments when due, the County may
discontinue your coverage during the leave. The County, at its option, may
continue your coverage during the leave and then recoup your share of premiums
and contributions from available taxable compensation upon your return from
leave.
If you do not elect to continue coverage while on FMLA leave, you are entitled to
reinstatement upon your return to employment on the same terms as prior to
taking FMLA leave, subject to any changes in benefit levels that may have taken
place during the leave.
Upon reinstatement in the Flexible Spending Account, you may resume coverage
at the level in effect before the FMLA leave and make up the unpaid premium
payments, or you may resume coverage at a level that is reduced and resume
Packet Pg. 82
Page 83
-10-
premium payments at the level in effect before the FMLA leave. If you do not
elect to continue coverage during the FMLA leave under the Flexible Spending
Account while on FMLA leave, you will not be entitled to reimbursement for
claims incurred during the FMLA leave.
Any election change (other than those made in connection with a court order or as an
exercise of rights pursuant to a statute that provides for a specific election period such as HIPAA
or COBRA) must be requested in writing within thirty (30) days from the date of the change
event. Any new election shall be effective not earlier than the first day of the next pay period
covered by the new Health/Dependent Care Flexible Spending Accounts-FSA Enrollment form.
You may not make an election change that would reduce your Flexible Spending Account
coverage to an amount that would be less than the amount of benefits claimed under such
coverage as of the date the change would become effective.
ELECTION CHANGES IMPOSED BY THE PLAN
Although it is unlikely that your elections and benefits under the Plan will be affected by
the numerous discrimination tests that apply to them under the Internal Revenue Code, you
should know that there are a number of legal limitations that apply to the Plan. The Plan
Administrator reserves the right to modify any benefit elections by the amount necessary to
allow the Plan to satisfy any applicable nondiscrimination requirements. If these discrimination
tests ever apply to you, the Plan Administrator will inform you of the effect on your Plan
elections and benefits.
Additionally, if the cost of participation in one of the County’s welfare insurance plans
(e.g., medical or dental coverage) or the Teamsters Plan increases or decreases during a period of
coverage, and, under the terms of the respective plan, you are required to make a corresponding
change in payments, the Plan may, on a reasonable and consistent basis, automatically make a
prospective increase or decrease in your elective contributions to the Plan.
WHAT BENEFITS ARE AVAILABLE UNDER THE PLAN?
(a) PRE-TAX PREMIUM ACCOUNT
You may elect to pay your share for coverage under the County’s group welfare plans
(e.g. group medical or dental insurance) or the Teamsters Plan with pre-tax dollars. If you do not
complete and return a new election form each plan year, you will be treated as having elected to
continue your coverage option as in effect on the last day of the preceding plan year. If pre-tax
Packet Pg. 83
Page 84
-11-
dollars are to be used for either medical or dental insurance, then both types of insurance must be
paid for pre-tax.
(b) FLEXIBLE SPENDING ACCOUNT
You may elect to put a minimum of $120 and a maximum of up to $2,5500 (as indexed
for inflation) of your compensation per year into a Flexible Spending Account to pay your
unreimbursed medical expenses with pre-tax dollars. If you do not use the entire amount you
have elected to put into the account during the Plan Year for unreimbursed health care expenses
incurred during the Plan Year, you may carry over up to $500 of the unused balance to the next
Plan Year. Subject to the active military duty exception described below, you will lose any
unused balance above the $500 that may be carried over to the next Plan Year. It is therefore
important to estimate conservatively the amount of your prospective unreimbursed medical
expenses for the Plan Year before electing the amount to contribute since your election cannot be
changed except under certain narrow circumstances.
The eligible expenses are those permitted by Section 213 of the Internal Revenue Code
and include out-of-pocket medical, dental and vision expenses incurred by you, your spouse and
your dependents. There is no reimbursement for the cost (e.g. premiums) of other health care
coverage maintained outside of the Plan. Examples of eligible expenses are set forth below:
Deductibles and co-payments under the County's health plans (including
dental and vision plans) or the Teamsters Plan or under personal accident
and health insurance carried by you, your spouse, or covered dependents;
Prescription drugs;
Over-the-counter drugs and products such as antacids, allergy medicines,
pain relievers and cold medicines if you have a prescription, except that no
prescription is needed for over-the-counter insulin;
Eye care, including vision checkups, eyeglasses and contact lenses;
Hearing care, including hearing examinations and hearing aids;
Routine physical examinations;
Any other medical care item that constitutes medical care within the
meaning of Code Section 213(d).
The County has delegated responsibility for claims administration to a third party
administrator as set forth in the section entitled “General Plan Information” (hereinafter referred
Packet Pg. 84
Page 85
-12-
to as the “Claims Administrator”). In order to be reimbursed for an eligible health care expense,
you must submit to the Claim Administrator a completed claim form and itemized bill from the
service provider. You have ninety90 days following the end of the Plan Year to submit claims
for reimbursement with respect to eligible expenses incurred during the immediately preceding
Plan Year, except that terminated employees will have thirty days from the date of their
termination to submit claims.
If there is not enough money in your Flexible Spending Account at any time during the
year to cover the claim you have submitted, the Claims Administrator will pay your claim, up to
the total amount you have elected to contribute to this account for the Plan Year plus any
amounts up to $500 carried over from the previous Plan Year. For example, assume that you
have elected to establish a Flexible Spending Account of $600 for the Plan Year by contributing
$50 each month. Further, assume that during the first month when there is only $50 in your
account, you have qualified medical expenses of $300. The Plan must reimburse you the full
$300 and take the risk that you might terminate employment before you have contributed $300.
That said, if you are a reservist called to active duty for a period of at least 180 days or for an
indefinite period, the Plan may distribute to you all or a portion of the balance in your Flexible
Spending Account. The balance available for such a distribution will be the entire amount
elected for the Flexible Spending Account for the Plan Year plus any carryover from the
previous Plan Year, minus Flexible Spending Account reimbursements received as of the date of
the qualified reservist distribution request. In order to receive this money, you must request it on
or after the date of the order or call to active duty, and before the last day of the Plan Year during
which the order or call to active duty occurred. Before the Plan issues such a distribution, you
must provide the County with a copy of the order or call to active duty. Distributions will be
made no later than 60 days after the date of the request.
(c) DEPENDENT CARE REIMBURSEMENT ACCOUNT
You may elect to put a minimum of $120 and a maximum of $5,000 of your
compensation per year, if you are single, into the Dependent Care Reimbursement Account in
order to pay with pre-tax dollars for child care expenses and other dependent care costs to enable
you to work. If you are married, filing a joint federal income tax return with your spouse, you
and your spouse may together put up to $5,000 per year (but no more than the lower of your two
incomes except that if your spouse is a full-time student or is disabled she is considered to have a
Packet Pg. 85
Page 86
-13-
monthly income of $200 for one dependent or $400 for two dependents) into the Dependent Care
Reimbursement Account. If you are married, filing separately, your limit is $2,500. If you are
married and your spouse does not work (and she is not a full-time student or disabled), then you
may not participate. The limits above apply to the total amount of dependent care assistance you
may receive during the Plan Year. Therefore, if you receive any such benefits under a plan of
your spouse’s company, these amounts must be offset against the amount you may contribute to
this Plan. If you do not use the entire amount you have elected to put into the account for the
Plan Year for dependent care expenses incurred during either the Plan Year, you will lose the
unused balance.
The eligible expenses that may be reimbursed are those incurred for eligible dependents
in certain qualifying dependent care arrangements. Eligible dependents include your children up
to age 13 and your other dependents (for federal tax purposes) who are physically or mentally
unable to care for themselves and reside in your home at least eight hours per day. Qualifying
dependent care arrangements include a day care center, provided that if care is provided by the
facility for more than six individuals, it must comply with applicable state and local laws; an
educational institution for pre-school children (for older children, only expenses for non-school
care are eligible for reimbursement); and care provided inside or outside your home by an
individual who is not your child under age 19 or your dependent (for federal tax purposes).
In order to be reimbursed for an eligible dependent care expense, you must submit to the
Plan Administrator a completed claim form and evidence of the qualifying expense (including
the service provider’s federal company identification number or social security number). If there
is not enough money in your Dependent Care Reimbursement Account at any time during the
year to cover the claim you have submitted, the Claims Administrator will pay your claim up to
the balance in your account and will hold your claim until additional money is deposited into
your account. You have ninety days following the end of the Plan Year to submit claims for
reimbursement with respect to eligible expenses incurred during the immediately preceding Plan
Year, except that terminated employees will have thirty days from the date of their termination to
submit claims.
Packet Pg. 86
Page 87
-14-
WHAT HAPPENS IF I DON’T USE UP ALL OF THE ELECTED BENEFITS PRIOR TO
THE END OF THE PLAN YEAR?
As indicated above, except with respect to up to $500 that may be carried over to a
subsequent Plan Year under the Flexible Spending Account, you must use the entire amount that
you have put into the account during a particular Plan Year for health care and dependent care
expenses incurred during that Plan Year; otherwise, you will lose the unused balance. Following
the end of the Plan Year, you have three months in which to submit claims for reimbursement for
expenses incurred during the Plan Year. This is called the “Run-Out Period.”
For example, assume that $600 remains in your Flexible Spending Account at the end of
the 2015 Plan Year and that you have elected $2,400 of Flexible Spending Account coverage for
2016. Because the carryover is limited to $500, you will lose $100 from your account at the end
of the 2015 Plan Year, and the remaining $500 will carry over for use during the 2016 Plan Year.
This means that you will have a total of $2,900 (i.e., $2,400 election + $500 carryover) available
in your Flexible Spending Account for 2016.
WHAT HAPPENS IF I RECEIVE REIMBURSEMENTS TO WHICH I AM NOT
ENTITLED UNDER THE PLAN?
If any over-payments are made to you under the Plan, you will be responsible for
reimbursing the Plan for such amounts. Reimbursement may be made by any reasonable means
available, including, but not limited to, offset against future benefits at the Plan’s discretion,
direct payment by you to the County or withholding from your future paychecks at the County’s
discretion. By participating in the Plan, you specifically authorize such withholding if needed to
correct overpayments.
Moreover, if you deliberately defraud or mislead the Plan Administrator about the
eligibility or entitlement to benefits of yourself or another person, the Plan Administrator has the
right to terminate Plan coverage for you and/or any family members immediately and
retroactively. The Plan shall be entitled to recover (as described above) from the you and/or
your family members any claims mistakenly paid due to mistake, fraud or a wrongful attempt to
procure coverage, and to recover any costs and expenses arising from such fraud or
misrepresentation, including, but not limited to, costs and expenses recoverable in actions at law
and in equity. Additionally, fraud on your part shall be grounds for disciplinary action up to and
including termination of employment.
Packet Pg. 87
Page 88
-15-
WHAT HAPPENS IF I TERMINATE EMPLOYMENT?
If you terminate employment, your pre-tax contributions to the Pre-Tax Premium
Account and the Dependent Care Reimbursement Account will cease. You may be entitled to
continue your Flexible Spending Account pursuant to the COBRA coverage continuation rules as
described in the next section. If you terminate employment and are rehired during the same Plan
Year, your election in the Plan automatically will be reinstated for the remainder of the Plan
Year. If you incur dependent care expenses after you terminate employment or otherwise cease
participation in the Plan, you may be reimbursed from the unused balance of your Dependent
Care Reimbursement Account for expenses incurred during the Plan Year. However, you may
not be reimbursed for amounts beyond your unused account balance, and you may not contribute
additional amounts to the account.
If you terminate employment and are rehired during the same Plan Year, your election in
the Plan automatically will be reinstated for the remainder of the Plan Year. However, if you are
rehired more than 30 days after your termination, you will be eligible to make new elections for
the remainder of the Plan Year.
AM I ENTITLED TO CONTINUE COVERAGE UNDER THE PLAN?
Continuation of coverage under the County’s group medical and dental plans or the
Teamsters Plan will be governed by the terms of those plans in compliance with the federal
COBRA law. COBRA does not apply to Dependent Care Account benefits.
Dependent care expenses incurred after you cease participation in the Plan (for example,
after termination) and on or prior to the last day of that Plan Year may be reimbursed from
unused benefits remaining in your Dependent Care Account. However, you may not be
reimbursed for amounts beyond your unused account balance, and you may not contribute
additional amounts to the account.
Under certain circumstances (described as “qualifying events”) that otherwise would
cause you to lose coverage under the Plan (such as a termination or reduction in hours of
employment), you may be entitled under federal law (known as “COBRA”) to continue
participation in your Flexible Spending Account for the remainder of the Plan Year if you have a
positive account balance. This section generally explains COBRA continuation coverage, when
it may become available to you and your family, and what you need to do to protect the right to
receive it. COBRA (and the description of COBRA continuation coverage contained here)
Packet Pg. 88
Page 89
-16-
applies only to the group health benefits offered under the Flexible Spending Account and not to
the Dependent Care Reimbursement Account.
For additional information about your rights and obligations under the Plan and under
federal law, you should contact the Department of Human Resource Management. The Plan
provides no greater COBRA rights than what COBRA itself requires, and nothing in this section
is intended to expand your rights beyond COBRA’s requirements.
(a) What Is COBRA Continuation Coverage?
COBRA continuation coverage is a continuation of Plan coverage when coverage would
otherwise end because of a life event known as a “qualifying event.” Specific qualifying events
are listed later in this section. After a qualifying event occurs and any required notice of that
event properly is provided to the Plan Administrator, COBRA continuation coverage must be
offered to each person losing coverage who is a “qualified beneficiary.” You and your
dependents could become qualified beneficiaries and be entitled to elect COBRA if coverage
under the Plan is lost because of the qualifying event.
COBRA continuation coverage is the same coverage that the Plan gives to other similarly
situated persons under the Plan who are not receiving continuation coverage. Each qualified
beneficiary who elects COBRA continuation coverage will have the same rights under the Plan
as other persons covered under the Plan.
(b) Who Is Entitled to Elect COBRA?
If you are an employee, you will be entitled to elect COBRA if you lose your group
health coverage under the Plan because either one of the following qualifying events happens:
Your hours of employment are reduced, or
Your employment ends for any reason other than your gross misconduct.
If you are the spouse of an employee, you will be entitled to elect COBRA if you lose
your group health coverage under the Plan because any of the following qualifying events
happens:
Your spouse’s hours of employment are reduced;
Your spouse’s employment ends for any reason other than his or her gross
misconduct;
Your spouse dies; or
You become divorced or legally separated from your spouse.
Packet Pg. 89
Page 90
-17-
Your children who are dependents will be entitled to elect COBRA if they lose group
health coverage under the Plan because any of the following qualifying events happens:
The parent-employee’s hours of employment are reduced;
The parent-employee’s employment ends for any reason other than his or her
gross misconduct;
The parent-employee dies;
The parents become divorced or legally separated; or
The child stops being eligible for coverage under the Plan as a “dependent” as
defined by the Plan.
However, COBRA coverage is provided subject to your eligibility for such coverage. In
particular, you must have been both eligible for coverage and actually covered by the Plan on the
day prior to the date of the qualifying event. The Plan Administrator reserves the right to
terminate your COBRA coverage retroactively if you are determined to have been ineligible.
(c) When is COBRA Coverage Available?
COBRA continuation coverage is available under the Flexible Spending Account only if
there is a positive account balance at the time of the qualifying event that otherwise would cause
a loss of coverage. The Plan will offer COBRA continuation coverage to qualified beneficiaries
only after the Plan Administrator has been notified that a qualifying event has occurred. When
the qualifying event is the end of employment or reduction of hours of employment, or the death
of the employee, the employer must notify the Plan Administrator of the qualifying event.
(d) You Must Give Notice of Some Qualifying Events
For the other qualifying events (divorce or legal separation of the employee and spouse or
a dependent child’s losing eligibility for coverage as a dependent child), you will not be entitled
to COBRA unless you notify the Plan Administrator in writing within 60 days after the later of
(i) the date of the qualifying event, and (ii) the date on which the qualified beneficiary would
lose coverage under the terms of the Plan as result of the qualifying event. You must provide
this notice to the Plan Administrator.
The notice must be mailed or hand-delivered. Oral notice, including notice by telephone,
is not acceptable. If mailed, the notice must be postmarked no later than the deadline. If hand-
delivered, the notice must be received no later than the deadline. Electronic notice, including
notice that is sent via e-mail or facsimile, is not acceptable. The notice may be provided by the
Packet Pg. 90
Page 91
-18-
covered employee (i.e., the employee or former employee who is or was covered under the Plan),
another qualified beneficiary who lost coverage to the covered employee’s termination or
reduction in hours and is still receiving COBRA coverage, or a representative acting on behalf of
either one.
The notice must contain the Plan name, the employee’s name, address, birth date, and
social security (or other identification) number, the name and address of any impacted spouse or
dependent, a description of the qualifying event, the date of the event, and adequate
documentation of the event (such as a divorce decree or decree of legal separation, or a copy of
the dependent’s birth certificate, as applicable). A form for providing this notice may be
available from the Plan Administrator, but need not be used so long as all the relevant
information is included in the written notice.
If you provide a written notice that does not contain all of the information and
documentation required, such a notice will nevertheless be considered timely if all of the
following conditions are met:
the notice is mailed or hand-delivered to the individual and address specified;
the notice is provided by the deadline;
from the written notice provided, the Plan Administrator is able to determine that
the notice relates to the Plan;
from the written notice provided, the Plan Administrator is able to identify the
covered employee and qualified beneficiary(ies), the qualifying event (the
divorce, legal separation, or child’s loss of dependent status), and the date on
which the qualifying event occurred; and
the notice is supplemented in writing with the additional information and
documentation necessary to meet the Plan’s requirements within 15 business days
after a written or oral request from the Plan Administrator for more information
(or, if later, by the deadline for this notice).
If any of these conditions is not met, the incomplete notice will be rejected and COBRA
will not be offered. If all of these conditions are met, the Plan Administrator will treat the notice
as having been provided on the date that the Plan Administrator receives all of the required
information and documentation but will accept the notice as timely.
(e) Electing COBRA Continuation Coverage
Packet Pg. 91
Page 92
-19-
Once the Plan Administrator receives notice that a qualifying event has occurred,
COBRA continuation coverage will be offered to each of the qualified beneficiaries. Each
qualified beneficiary will have an independent right to elect COBRA continuation coverage.
Covered employees (and Spouses if the Spouse is a qualified beneficiary) may elect COBRA
continuation coverage on behalf of all of the qualified beneficiaries, and parents may elect
COBRA continuation coverage on behalf of their children.
Any qualified beneficiary for whom COBRA is not elected within the 60-day election
period described in the Plan’s COBRA Election Notice will lose his or her right to elect COBRA
continuation coverage.
Your election must be provided to the Plan Administrator via hand-delivery, U.S. Mail,
or some form of express mail delivery.
(f) Special Second Election Period under the Trade Act
Under the Trade Act of 2002, special COBRA rights apply to certain employees and
former employees who are eligible for federal trade adjustment assistance (TAA) or alternative
trade adjustment assistance (ATAA). The process for determining individual eligibility for trade
adjustment assistance begins when employees (or their representatives) petition the Department
of Labor to recognize their employer as being adversely affected by trade.
Eligible individuals are entitled to a second opportunity to elect COBRA for themselves
and certain family members (if they did not already elect COBRA) during a special second
election period. This special second election period lasts for 60 days or less. It is the 60-day
period beginning on the first day of the month in which an eligible employee or former employee
becomes eligible for TAA or ATAA, but only if the election is made within the six months
immediately after the individual’s group health plan coverage ended. If you are an employee or
former employee and you qualify or may qualify for TAA or ATAA, please contact the Plan
Administrator. Contact the Plan Administrator promptly after qualifying for TAA or ATAA or
you will lose the right to elect COBRA during a special second election period.
(g)(f) How Much Does COBRA Continuation Coverage Cost?
Generally, each qualified beneficiary is required to pay the entire cost of COBRA
continuation coverage, plus a two percent administrative fee. All COBRA premiums must be
paid by personal check or money order (unless arrangements are made to deduct premiums from
remaining paychecks).
Packet Pg. 92
Page 93
-20-
(h)(g) When must payment for COBRA continuation coverage be made?
First payment for COBRA continuation coverage
If you elect COBRA continuation coverage, you do not have to send any payment with
your election. However, you must make your first payment for continuation coverage not later
than 45 days after the date of your election. (This is the date your election is post-marked, if
mailed, or the date your election is received by the Plan Administrator, if hand-delivered.) If you
do not make your first payment for COBRA continuation coverage in full within 45 days of the
date of your election, you will lose all continuation coverage rights under the Plan.
Your first premium payment must include payment for the period from the date that you
lost (or otherwise would have lost) coverage until the date of your election, and each regularly
scheduled monthly premium that became due during the period between your election and the
first payment. You are responsible for making sure that the amount of your first payment is
correct. You may contact the Plan Administrator to confirm the correct amount of your first
payment.
Claims for reimbursement may not be processed and paid until you have elected COBRA
and made the first payment.
Monthly payments for COBRA continuation coverage
After you make your first payment for COBRA continuation coverage, you will be
required to make monthly payments for each subsequent month of coverage. Under the Plan,
each of these monthly payments for continuation coverage is due on the first of the month for
that month’s COBRA continuation coverage. If you make a monthly payment on or before the
first day of the month to which it applies, your coverage under the Plan will continue for that
coverage period without any break. If you do not make a monthly payment on or before the first
day of the month, your coverage may be suspended pending payment. The Plan is not required
to send monthly notices of payments due for these coverage periods. It is your responsibility to
pay your COBRA premiums on time, regardless of whether you receive a monthly bill.
Grace periods for monthly payments
Although monthly payments are due on the first day of each month of COBRA
continuation coverage, you will be given a grace period of 30 days to make each monthly
payment. Your COBRA continuation coverage will be provided for each month as long as
payment for that month is made before the end of the grace period for that payment. If you fail
Packet Pg. 93
Page 94
-21-
to make a monthly payment before the end of the grace period for that coverage period, you will
lose all rights to COBRA continuation coverage under the Plan.
(i)(h) How Long Does COBRA Continuation Coverage Last?
COBRA continuation coverage with respect to your Flexible Spending Account is a
temporary continuation of coverage that generally lasts until the end of the Plan Year in which
the qualifying event occurs.
(j)(i) If You Have Questions
Questions concerning your Plan or your COBRA continuation coverage rights should be
addressed to the Department of Human Resource Management.
For more information about your rights under COBRA, the Health Insurance Portability
and Accountability Act (“HIPAA”), and other laws affecting group health plans, contact the
nearest Regional or District Office of the U.S. Department of Labor’s employee Benefits
Security Administration (“EBSA”) in your area or visit the EBSA website at www.dol.gov/ebsa.
(Addresses and phone numbers of Regional and District EBSA Offices are available through
EBSA’s website.)
For more information regarding your COBRA continuation coverage rights, please
consult the General Notice of COBRA Continuation Coverage Rights that is provided to you at
the time that you become eligible to enroll in this Plan. You also will receive a full explanation
of your COBRA rights when you become entitled to continuation coverage.
WHAT HAPPENS IF THIS PLAN IS DISCONTINUED OR AMENDED?
While this Plan is intended to be a permanent and continuing program, the County
reserves the right to terminate the Plan at any time. On termination of the Plan, any amounts that
become payable under the terms of the Plan prior to the date of termination shall be paid in
accordance with the terms of the Plan as in effect prior to the date of such termination.
The County also reserves the right to amend or modify the Plan at any time. Any amount
that had become payable under the Plan prior to the effective date of any such amendment shall
be paid or payable in accordance with the terms of the Plan as in effect immediately prior to the
date of the amendment.
ADMINISTRATION
The Plan Administrator has discretionary authority to determine eligibility for benefits, to
decide claims, to interpret and construe plan provisions and to determine all other matters under
Packet Pg. 94
Page 95
-22-
the Plan. Benefits under this Plan will be paid only if the Plan Administrator decides in its
discretion that the applicant is entitled to them. Any interpretation of the provisions of the Plan
by the Plan Administrator and any decision made by it on any matter within its discretion shall
be binding on all persons. A misstatement or other mistake of fact shall be corrected when it
becomes known and the Plan Administrator shall make such adjustment or account thereof as it
considers equitable and practicable. The Plan Administrator shall not be liable in any manner for
any determination of fact made in good faith.
PROCEDURES FOR MAKING A CLAIM AND AN APPEAL FOR BENEFITS
Any claim for benefits under the underlying group welfare plans of the County (such as
group medical or dental insurance benefits) or the Teamsters Plan shall be reviewed in
accordance with the claims procedures contained in the applicable insurance policies and plan
documents. You should refer to the plan description of the group welfare plan (if any) for a
description of the claims procedures. Otherwise, please follow the claims procedures outlined
below for claims with respect to benefits under this Plan.
You must follow the procedures below for filing a claim and requesting review of a
denied claim before bringing any legal action. If you fail to raise an issue during the initial claim
or as part of your request for review, you will be precluded from raising such issue in any further
proceedings. If a claim is denied upon appeal, any legal action with respect to that claim must be
brought within one year of the date of the decision upon appeal.
Claims for Benefits with respect to your Pre-Tax Premium Account
Any claim for benefits under the Plan with respect to benefits from your Pre-Tax
Premium Account should be made in writing by you or your authorized representative by filing it
with the Claims Administrator along with such evidence as reasonably may be required to
support your claim. If your claim is denied in whole or in part, you will be informed in writing.
Claims for Benefits with respect to your Dependent Care Account
Any claim for benefits under the Plan with respect to your Dependent Care Account
should be made in writing by you or your authorized representative by filing it with the Claims
Administrator along with such evidence as reasonably may be required. Claims must be filed no
later than the end of the Run-out Period (in other words, within three (3) months following the
end of the Plan Year with respect to eligible expenses incurred during the immediately preceding
Plan Year). Any amounts remaining in your account will be forfeited.
Packet Pg. 95
Page 96
-23-
In order to be reimbursed for an eligible dependent care expense, you must submit to the
Plan Administrator a completed claim form and evidence of the qualifying expense (including
the service provider’s federal company identification number or social security number and the
date, description and cost of the service). Dependent care expenses may not be reimbursed before
the care is provided. If there is not enough money in your Dependent Care Reimbursement
Account at any time during the year to cover the claim you have submitted, the Plan
Administrator will pay your claim up to the balance in your account and will hold your claim
until additional money is deposited into your account.
If your claim is denied in whole or in part, you will be informed in writing within a
reasonable timeframe and given the following information:
1. The specific reason or reasons why the claim is denied;
2. Reference to the specific Plan provisions on which the denial is based;
3. A description of any additional material or information necessary to enable you to
perfect your claim and an explanation of why such material or information is
necessary;
4. An explanation of the Plan’s review procedure, including a statement that any
appeal of the denial must be made in writing to the Claims Administrator within
60 days after receipt of the notice of denial and must include a full description of
the pertinent issues and the basis of the appeal; and
5. A statement describing any other rights you might have after you have exhausted
these administrative claims procedures.
The procedure for obtaining a review of a denied claim is as follows:
1. Your request for a review of the decision denying your claim or part of it must be
made in writing by you or your authorized representative not later than 60 days
after you receive notice of the denial.
2. Your request should be sent to the Claims Administrator.
3. Your request for review may include any issues, comments, documents, records,
or additional information or material relating to the claim, and the Claims
Administrator’s review will take into account all such information provided that it
is submitted in writing.
Packet Pg. 96
Page 97
-24-
4. On review, you will be afforded reasonable access to all documents relevant to
your claim.
5. The Claims Administrator may hold a hearing or otherwise ascertain such facts as
it deems necessary.
6. The Claims Administrator will give you a decision in writing within a reasonable
timeframe after receiving your request for review. You will be given the reasons
for the Claims Administrator’s decision and will be referred to the Plan provisions
on which the decision is based.
Claim for Benefits with respect to your Flexible Spending Account
Any claim for benefits under the Plan with respect to benefits from your Flexible
Spending Account should be made by you or your authorized representative in writing by filing
it with the Claims Administrator along with such evidence as reasonably may be required by the
end of the Run-out Period (in other words, within three (3) months following the end of the Plan
Year).
In order to be reimbursed for an eligible health care expense, you must submit to the Plan
Administrator a completed claim form and itemized bill from the service provider. You must
provide adequate substantiationdocumentation (i.e., an Explanation of Benefits statement, paid
receipt, or as otherwise determined by the Plan) of the expenses you incur in order to be
reimbursed. Further instructions will be provided on the claim form. Only expenses incurred on
or after you are enrolled in the Plan will be reimbursed.
Alternatively, you may pay for eligible health care expenses with your Plan debit card
provided that you comply with applicable substantiation procedures. Some expenses may be
validated automatically at the time the expense is incurred (like co-pays for medical care). For
other expenses, the card payment is only conditional and you will still have to submit supporting
documents. You will receive more information from the Claims Administrator about what you
must do to obtain reimbursement.
To the extent that the Claims Administrator, in its discretion, determines that you have
failed to properly substantiate your claim for reimbursement or there has otherwise been an
overpayment, the Claims Administrator shall, to the extent that it deems administratively
possible and otherwise permissible under applicable law, seek repayment of any such excess
reimbursement by (1) requesting you directly reimburse the Plan, (2) withholding the
Packet Pg. 97
Page 98
-25-
corresponding amount from your compensation on an after-tax basis (where such withholding is
permissible under applicable law), or (3) offsetting the improper reimbursement against other
eligible Flexible Spending Account claims.
You have until the end of the Run-out Period to submit claims for reimbursement with
respect to eligible expenses incurred during the immediately preceding Plan Year. If there is not
enough money in your Flexible Spending Account at any time during the year to cover the claim
you have submitted, the Claims Plan Administrator will pay your claim, up to the total amount
you have elected to contribute to this account for the Plan Year plus any carryover amounts. For
example, assume that you have elected to establish a Flexible Spending Account of $600 for the
Plan Year by contributing $50 each month. Further, assume that during the first month when
there is only $50 in your account, you have qualified medical expenses of $300. The Plan must
reimburse you the full $300 and take the risk that you might terminate employment before you
have contributed $300.
If your claim is denied in whole or in part, you will be informed in writing within a
reasonable timeframe and given the following information:
(a) The specific reason or reasons why the claim is denied;
(b) Reference to the specific Plan provisions on which the denial is based;
(c) A description of any additional material or information necessary to enable you to
perfect your claim and an explanation of why such material or information is
necessary; and
(d) An explanation of the Plan’s review procedure, including a statement that any
appeal of the denial must be made in writing to the Kane County Human Services
Committee within 60 days after receipt of the notice of denial and must include a
full description of the pertinent issues and the basis of the appeal.
The procedure for obtaining a review of a denied claim is as follows:
(a) Your request for a review of the decision denying your claim or part of it must be
made in writing by you or your authorized representative not later 60180 days
after you receive notice of the denial.
(b) Your request should be sent to the Kane County Human Services Committee (the
“Committee”).
Packet Pg. 98
Page 99
-26-
(c) Your request for review may include any issues, comments, documents, records,
or additional information or material relating to the claim, and the review will
take into account all such information provided that it is submitted in writing.
(d) On review, you will be afforded reasonable access to all documents relevant to
your claim.
(e) The Committeelaims Administrator may hold a hearing or otherwise ascertain
such facts as it deems necessary.
(f) The Committeelaims Administrator will give you a decision in writing within a
reasonable timeframe after receiving your request for review. You will be given
the reasons for the Committeelaims Administrator’s decision and will be referred
to the Plan provisions on which the decision is based. [LMDBLT2]
FULL DETAILS IN LEGAL PLAN DOCUMENTS
THE COUNTY RESERVES THE RIGHT TO CONSTRUE AND INTERPRET THE
TERMS OF THE PLAN.
THIS SUMMARY ATTEMPTS TO DESCRIBE THE PLAN IN EASY TO
UNDERSTAND LANGUAGE AND TO DO SO AS ACCURATELY AS POSSIBLE.
HOWEVER, THE COMPLETE PROVISIONS OF THE PLAN ARE CONTAINED IN THE
LEGAL PLAN DOCUMENTS. IF FOR ANY REASON THERE IS AN OMISSION OR
MISSTATEMENT IN THIS SUMMARY, OR ANY DIFFERENCE BETWEEN THIS
SUMMARY AND THE LEGAL PLAN DOCUMENTS, THE LEGAL PLAN DOCUMENTS
WILL IN ALL RESPECTS CONTROL AND GOVERN. THESE LEGAL PLAN
DOCUMENTS ARE AVAILABLE FOR YOUR EXAMINATION DURING NORMAL
BUSINESS HOURS AT THE ADDRESS LISTED ON THE LAST PAGE OF THIS
SUMMARY.
Packet Pg. 99
Page 100
-27-
GENERAL PLAN INFORMATION
The following describes information, which is of prime importance to you as a Plan
Participant.
Plan Name: County of Kane Flexible Benefits Plan
Type of Plan: Section 125 Cafeteria Plan
Plan Sponsor: County of Kane
Plan Administrator: County of Kane, Department of Human Resource Management
Business Address: Kane County Government Center
719 Batavia
Geneva, IL 60134
Business Telephone No.: (630) 232-3560
Federal Employer
Identification No.:
36-6006585
Plan Number: 502
Effective Date of Plan: January 1, 2006
Plan Year: January 1 to December 31
Agent for Service of
Legal Process:
County Board Chairman
Kane County Government Center
719 Batavia
Geneva, IL 60134
Packet Pg. 100
Page 101
-28-
Claims Administrator: Flexible Benefit Service Corporation
10275 West Higgins Road
Suite 500
Rosemont, Illinois 60018
866-472-5351
www.myflexlogin.com
PayFlex Systems USA, Inc.
1802 Farnam Drive, Suite 100
Omaha, Nebraska 68154
(402) 884-7030
Packet Pg. 101