49
AHI PPS Year 1 Progress Report Collaboration • Catalyst • Community May 2016

AHI PPS Year 1 Progress Report
Collaboration • Catalyst • Community
May 2016

2
DSRIP
“[DSRIP is] not about launching 10 or 11 projects, not about ticking boxes to hit particular requirements, not about moving the needle on performance measures. It’s about a fundamental restructuring towards a system that really rewards value. It’s beginning to sink in with folks that that’s really the endgame here, and what they should be working towards.”
State government officialReport of the Commonwealth Fund, April 2016, “Implementing New York’s DSRIP Program; Implications for Medicaid Payment and Delivery System Reform”.

By incentivizing care collaboration and paying for performance, DSRIP is the catalyst for NYS Healthcare to transition to Value Based Payment (VBP)
3
DSRIP – the catalyst for VBP
Current State
• Providers are paid on a FFS basis; volume incentive
• Avoidable visits are rewarded • Prevention, coordination,
integration: lack strong incentives
Future State
• MCOs reward value over volume; 80-90% of payments are value-based
• Care patterns add value not excess volume
• Transformations in the delivery system are sustainable
DSRIP
2015 2020
Adapted from: Value Based Payment Roadmap. Mar 2016. NYS DOH DSRIP Website.

CMS NYS PPS
4
DSRIP Funding
Risk: if the VBP Roadmap goals are not met, overall DSRIP dollars from CMS to NYS will be significantly reduced

5
Population Health Management
PHM Competencies
Information and Communication Infrastructure
Clinical & Quality Management
Financial and Risk Management
Network Development & Physician Alignment

6
What’s in our Plan?
– Governance– Financial Sustainability and
Budget– Cultural Competency and
Health Literacy– IT Systems and Processes– Performance Reporting– Population Health
Management– Clinical Integration– Physician Engagement– Workforce Strategy
AHI PPS Organizational Components

7
AHI PPS EARNS 100% of all possible ACHIEVEMENT VALUES

1. Governance
2. Finance
3. PHM / IT Systems & Processes
4. Workforce
5. Cultural Competency / Health Literacy
• Community Based Organizations
ORGANIZATIONAL COMPONENTS DY1 STATUS
8

A best practice is that before any rule is created or any decision is made, a prior decision must be addressed: who gets to make the decision, and when, and using what information & processes?
GOVERNANCE: Decisions, decisions, decisions…..
9

10
DSRIP Principles

M1: Finalize governance structure and sub- committee structure 09/30/15
M2: Establish clinical governance structure 12/31/15
M3: Finalize bylaws and/or policies and/or Committee Guidelines 09/30/15
M4: Establish governance structure reporting and monitoring processes 12/31/15
M5: Finalize community engagement plan 09/30/15
M6: Finalize partnership agreements or contracts with CBOs In progress
M7: Finalize agency coordination plan In progress
M9: Inclusion of CBOs in PPS Implementation Plan 09/30/15
11
GOVERNANCE MILESTONES
NOTE: M8 Reported under Workforce

AHI Reconfigured
Board of Directors
Adirondack Health Institute
Executive Committee
Finance Committee
Audit & Compliance Committee
Governance Committee
AHI PPS Steering
Ad HocCommittees
Population Health Improvement
Program
Health Home
Adirondack Rural Health Network
Standing Committees
• New By-laws• New Board Composition• New Committee Structure
Next Slide

AHI Board of Directors
AHI PPS Steering Committee
Finance Committee
Clinical Governance and
Quality Committee
IT & Data Sharing Committee
Community Beneficiary & Engagement Committee
Network Committee
Workforce Committee
Compensation & Benefits
Workgroup
Employee Engagement Workgroup
Recruitment & Retention
Workgroup
Training and Resources
Workgroup
Data Security & Confidentiality
Workgroup
PHM & Performance Reporting &
Analytics Workgroup
Interoperability & Data Exchange
Workgroup
Budget and Funds Flow Workgroup
Financial Sustainability Workgroup
Valued Based Payment
Workgroup
Adirondacks ACO
Provides certain support services to the PPS
pursuant to a contract with AHI
Compliance Workgroup
Reviews all actions/decisions of the other Committees
Approves all recommendations of the
Steering Committee

14
DSRIP Year 1 Development: GOVERNANCE
• Compliance
• Network Committee

15
DSRIP Year 1 Development: FINANCE
• All Milestones Met: Financial Structures & Reporting Processes; assessment of network financial health.
• Workgroups Established
• Year 1 Disbursement of Engagement Funds completed
• CFO recruited
• Funds Flow: to be completed DY2Q1 (June 2016)
• DY2 partner disbursements in development

• AHI PPS Finance & Steering Committees have endorsed another round of “partner funds”, $5 million in total, to be disbursed during DY2Q1.
– Funds Flow Workgroup to develop methodology for the disbursement.
• AHI PPS Finance & Steering Committees have endorsed Innovation Fund RFP Concept: anticipate awarding $5 million total over the DSRIP period to support innovative projects.
An overview of the Innovation Fund RFP proposal and timeline is presented on next slides; all items are proposed, pending finalization and review by Committees.
16
UPDATE: Funds Flow & Innovation Fund
Proposal

• Innovation
– Service design, delivery, payment models
– Healthcare & “related services”; social, community-based, prevention, wellness
• Triple AIM
• Sustainability
17
INNOVATION FUND: Purpose

18
INNOVATION FUND: Proposed Timeline
Funding Period Begins
January 2017
August 2016 ~ RFP Release

APPLICATION COMPONENTS (character limit – no spaces; 3000 characters is equivalent to one single spaced page of text). The total page limit is 8 pages (does not include cover page, workplan, budget, letters of support)
– Cover Page - Project Title, Applicant Organization & Contact Information– Executive Summary (3000) – Purpose - Goals & Objectives (3000)– Statement of Need (3000)– Organizational Capacity (3000)– Project Narrative (6000)– Plan for Evaluation (3000)– Sustainability Plan (3000)– Workplan (template to be provided)– Budget (template to be provided)– Letters of Support (required)
19
INNOVATION FUND: Application

• LOIs & Applications
• Members - at least 1 member from each of the AHI PPS Governing Committees, at least 1 member of the AHI Board of Directors, at least 2 individuals who do not represent an AHI PPS partner organization.
• Incorporate LGU and/or mechanism to identify items projects LGU purview
20
INNOVATION FUND: Review Panel

– purpose and goals are clearly articulated– the proposal strengthens, extends, or otherwise supports the success of, one of
the 11 AHI PPS projects– strength of the narrative; it explains how the goals and objectives will be met–major budget items have been identified– project represents an innovative approach to the design, delivery, and/or
payment models for health care and related services.
21
INNOVATION FUND: Letter of Intent
• AHI to provide template
• Solicited twice annually
• Proposed Review Criteria

• Population Health Management
• Data Sharing
• Performance Measurement
22
Population Health Management / HIT Focus
Create an information architecture which helps transform health care delivery from a process which generates data, to a process which utilizes information to achieve improved clinical performance outcomes and reduced cost.
AHI PPS is developing processes to:
• Ensure timely, easy, and secure access to information;• Provide information that enables outcomes improvement;• Increase collaboration and information sharing.
23
PPS IT Goals

It is the goal of AHI PPS Information Technology (IT) to help further DSRIP Program goals by:
• Providing support to transform care delivery for the PPS’s Medicaid population by increasing quality and efficiency and improving the patient experience;
• Offering an interoperable system that uses clinical, utilization and administrative data to measure performance and identify actionable opportunities for improvement;
• Providing services that both support the delivery of quality health care and improve the decision-making process.
24
DSRIP IT Goals

• Governed by the Information Technology & Data Sharing (IT&DS) Committee, which reports to the DSRIP Steering Committee.
• Responsibilities: Develop and implement an IT strategy for the AHI PPS:– PPS information and data management goals, standards, practices and processes;– Data governance;– Aligning the PPS’s information technology;– Monitoring and evaluating information technology expenditures;– Processes and protocols.
• IT&DS’s Three Workgroups:– Population Health Management, Performance Management, Analytics;– Interoperability/Data Exchange;– Data Security/Confidentiality.
25
DSRIP IT Governance

• John Dudla Hudson Headwaters Health Network• Bob Cawley AHI - Adirondack Health Institute• George DeAngelis Adirondack Health• Wouter J Rietsema MD University of Vermont Health Network - CVPH• Valerie Ainsworth, LCSW-R Mental Health Association in Essex County• Ken Dales Mountain Lake Services• Jan M. Dahlen Behavioral Health Services North, Inc.• Martin (Marty) Brown Nathan Littauer Hospital• John Kelleher Glens Falls Hospital• Pete Gilhooly Glens Falls Hospital• Dennis Hadley St. Joseph’s ATRC in Saranac Lake, NY• Beth Foley Center for Disability Services• Andrew Bascom HCR Home Care• Andy Cruikshank Fort Hudson Home Care• Jorge Grillo St. Lawrence Health System
26
HIT WG
24 meetings (10/23/14 – 10/15/15
PMH preview event – 6/25/15

Five meetings to date from 12/16/15 to 4/21/16
• Kim Atkins Planned Parenthood Mohawk Hudson, Inc.• Martin (Marty) Brown Nathan Littauer Hospital• Bob Cawley AHI – Adirondack Health Institute• Andrew Cruikshank Fort Hudson Home Care• Ken Dales NYSARC North Country Management Services• John Dudla Hudson Headwaters Health Network• Jessica Fraser Hudson Headwaters Health Network• Jorge Grillo St. Lawrence Health System• Dennis Hadley St. Joseph's ATRC in Saranac Lake, NY• John Kelleher Glens Falls Hospital• Aaron Kramer Adirondack Health• Mark Lukens Behavioral Health Services North, Inc. • David Murray Center for Disability Services• Wouter Rietsema, MD University of Vermont Health Network - CVPH
Ad Hoc Meetings, PPS CIO Meetings, Auditing participants
27
IT & DS Committee

Needs Assessment
• Assess Infrastructure Needs, Plan, Design
• Acquire, Implement Hardware/Software Solutions
• Operate DSRIP Infrastructure, Upgrade as Needed
Interfaces, Data Collection
• Identify Interfaces
• Develop Data Collection Interfaces
• Collect Source Data Via Interfaces
28
Infrastructure

Population Health Management
• Data Analytics, Registry
• Care Management and Coordination
EHRs
• Identify EHR, Other Data Needs
• Implement Partner Upgrades to Existing EHRs
• Implement EHR/EHR Lite for Paper-Based Providers
• Document and Report Full EHR Data
Tracking Actively Engaged Patients (Due DY2Q4—3/31/17)
• Implement Electronic Tracking of Patients—Quarterly
• Track Actively Engaged Patients Electronically
29
Infrastructure

Alerts, Secure Messaging• Assess Alerts, Secure Messaging Readiness
• Initial Implementation of Alerts, Secure Messaging
• Remaining Implementation of Alerts, Secure Messaging
• Alerts, Secure Messaging Across the PPS
Performance Reporting and Management• DSRIP Project Metrics
• Reporting to DOH
• Reporting to PPS Partners
30
Infrastructure

Patient-Centered Medical Home:• Assess PCMH Readiness
• Implement EHR Upgrades Needed for PCMH Recognition, Apply for Recognition
• Providers Operate as Patient-Centered Medical Homes
Stage 2 Meaningful Use (Due DY3Q4—3/31/18)
• Assess MU Readiness
• Implement EHR Upgrades Needed for MU
• Providers Attest to MU Stage 2
• Providers Continue to Be Eligible for MU Incentives
31
PCMH and MU

32
IT Strategic Roadmap

33
Population Health Roadmap

Support providers, staff and the PPS to become a data-driven, evidence-based system in order to measure quality, identify high risk patients, and provide care management for patients to improve outcomes, the PHM supports providers, staff and the PPS to become a data-driven, evidence-based system.
• Analyze PPS PHM Needs, Develop RFP, Contract w/ Vendors;
• Design, Build, Test, Implement PHM Solution(s) across PPS;
• Analyze, Report, Adjust Care to Patient Needs.
34
Population Health

35
PHM Requirements Executive Summary
36
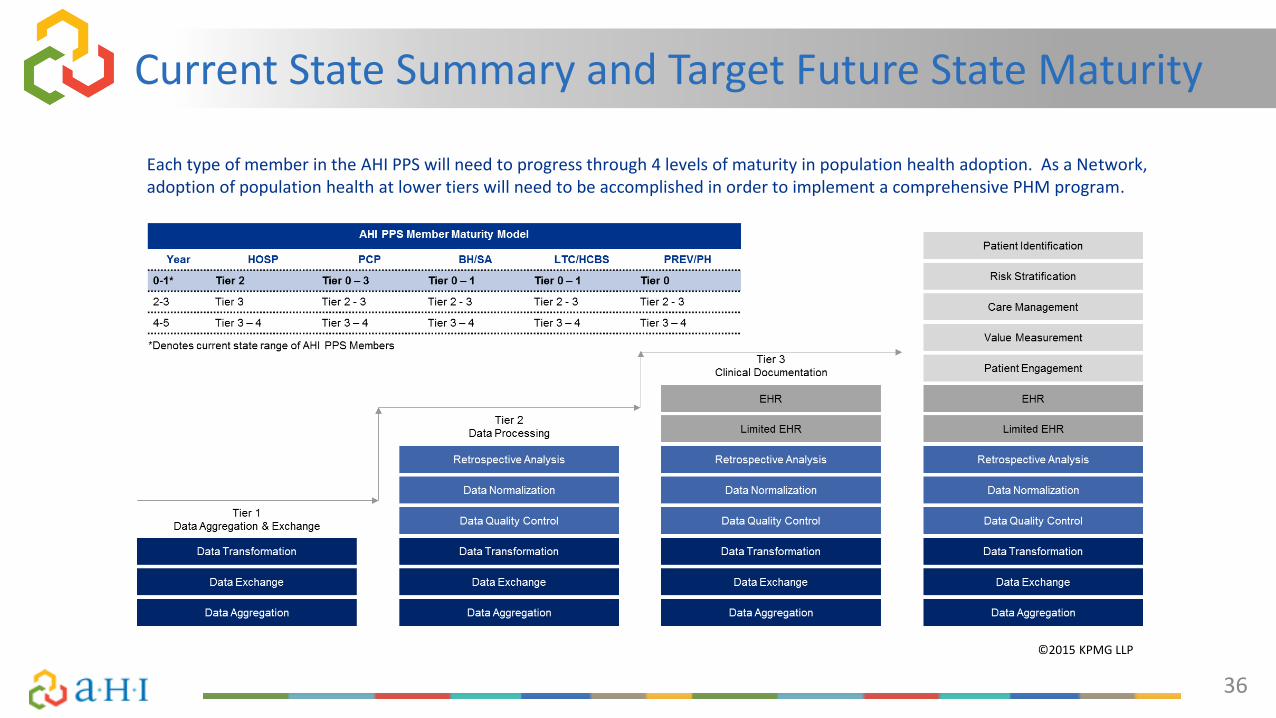
Current State Summary and Target Future State Maturity
Each type of member in the AHI PPS will need to progress through 4 levels of maturity in population health adoption. As a Network, adoption of population health at lower tiers will need to be accomplished in order to implement a comprehensive PHM program.
©2015 KPMG LLP

• Assess metrics and data needed, define reporting needs, establish data governance, plan interim & long-term performance management solutions;
• Obtain data to/from HIE/RHIO/payers;
• Develop reports and dashboards;
• Report on PPS and partner performance, identify improvements needed, develop/execute action plans.
37
Performance Management

38
DSRIP Performance Management Structure

39
Current State Summary – PPS Technological Capability

Data Security & Confidentiality: Ensure that our system is secure at all levels and patients can trust that their privacy is preserved, while being able to share the information they authorize. (Due DY2Q1—6/30/16)
RHIO/HIE Connectivity, Clinical Interoperability: Connecting care settings and supporting organizations to one another via the Health Information Exchange (HIE) or Regional Health Information Organization (RHIO), to create a regional, patient-centered record for all patients. (Due DY3Q4—3/31/18)
40
Data Security & Confidentiality/Interconnectivity

Telehealth/Telemedicine
Utilizing telemedicine to address gaps in care for a largely rural region, telemedicine can support access to specialty care as well as integrating primary care and behavioral health.
Home Monitoring
Patient home monitoring can extend care management resources to better care for patients with multiple chronic conditions.
41
Telehealth/Telemedicine/Home Monitoring

• Analyze HIT survey results;
• Establish infrastructure;
• Population Health Management solution search and selection
42
Next Steps

DSRIP Year 1 Development : WORKFORCE
M1: Define Workforce Target State 6/30/16
M2: Create a Workforce Transition Roadmap 9/30/16
M3: Gap Analysis 9/30/16
M4: Complete Compensation & Benefits Analysis 6/30/16
M5: Training Strategy 9/30/16
• All Workgroups Established & Functioning• Process for accessing Training funds established.• Mandated DY1 Workforce Spend MET • Milestones due June 2016 ~ on track

M1: Finalize a Cultural Competency / Health Literacy (CCHL) Strategy. 9/30/15
M2: Develop a training strategy addressing the drivers of health disparities. 6/30/16
Milestones: CULTURAL COMPETENCY ~ HEALTH LITERACY
45
CBOs in the AHI PPS: A Snapshot
• 68 CBOs have signed Terms of Participation
• Represented in each of the 11 PPS projects, on Steering Committee, and governance sub-committees
• Cover 9 county service area
• Sectors include housing/homeless services, community action, public health, behavioral health and substance abuse, family services, EMS, home care

46
Road to Value Based Payment (VBP)
“Many CBOs have years of experiencing improving SDH (Social Determinants of Health). This expert understanding of community needs, coupled with support and clinical expertise of a provider network, could make a significant impact on population health and generate savings for the entities involved.”
NYS DOH Path toward Value Based Payment: Annual Update, June 2016: Year 2 , p. 42
47
Collaborating for the future
What’s next?
•Provider organizations and CBOs should begin to build collaborative relationships within DSRIP’s framework.
• Identify potential partnership opportunities by assessing:
- Local social determinants to health- Needs identified by community- Gaps identified by data and hotspotting, partners, projects and workstreams- alignment with PPS project goals

Collaborate on Shared Goals
• Population Health
• Triple Aim
• PPS Quality Measures
• Prevention Agenda Indicators
• PPS Project Requirements
• Actively Engaged
48
Building a Collaboration
Define Your Value• How can your organization help
achieve the goal(s)? • What services or functions can you
perform that will enable success?• Why are you the organization best
able to fill this role?• How much does it cost you to
provide the service or function? • How is the service currently
reimbursed or funded? • What would be a better way?

49
PPS Funds Flow – Supporting CBOs
Three Avenues:
• AHI PPS Innovation Fund• CBO, or group of CBOs, responds to the RFP
• Vendor Agreement with AHI PPS• CBO contracts directly with AHI
• Subcontractor to an AHI PPS Participating Organization• CBO contracts with a PPS Partner to provide a service

















