Capture the Fracture: a Best Practice Frameworkand global campaign to break the fragility fracture cycle
K. Åkesson & D. Marsh & P. J. Mitchell & A. R. McLellan &
J. Stenmark & D. D. Pierroz & C. Kyer & C. Cooper &
IOF Fracture Working Group
Received: 21 January 2013 /Accepted: 11 March 2013 /Published online: 16 April 2013# The Author(s) 2013. This article is published with open access at Springerlink.com
AbstractSummary The International Osteoporosis Foundation(IOF) Capture the Fracture Campaign aims to supportimplementation of Fracture Liaison Services (FLS)throughout the world.Introduction FLS have been shown to close the ubiquitoussecondary fracture prevention care gap, ensuring that fragil-ity fracture sufferers receive appropriate assessment andintervention to reduce future fracture risk.Methods Capture the Fracture has developed internationallyendorsed standards for best practice, will facilitate change atthe national level to drive adoption of FLS and increaseawareness of the challenges and opportunities presented bysecondary fracture prevention to key stakeholders. The Best
Practice Framework (BPF) sets an international benchmarkfor FLS, which defines essential and aspirational elementsof service delivery.Results The BPF has been reviewed by leading experts frommany countries and subject to beta-testing to ensure that it isinternationally relevant and fit-for-purpose. The BPF willalso serve as a measurement tool for IOF to award ‘Capturethe Fracture Best Practice Recognition’ to celebrate success-ful FLS worldwide and drive service development in areasof unmet need. The Capture the Fracture website will pro-vide a suite of resources related to FLS and secondaryfracture prevention, which will be updated as new materialsbecome available. A mentoring programme will enablethose in the early stages of development of FLS to learn
IOF Fracture Working Group members include: Åkesson K (chair),Boonen S (Leuven, Belgium), Brandi ML (Florence, Italy), Cooper C(Oxford, UK), Dell R (Downey, USA) co-opted, Goemaere S (Gent,Belgium), Goldhahn J (Basel, Switzerland), Harvey N (Southampton,UK), Hough S (Cape Town, South Africa), Javaid MK (Oxford, UK),Lewiecki M (Albuquerque, USA), Lyritis G (Athens, Greece), MarshD (London, UK), Napoli N (Rome, Italy), Obrant K (Malmo, Sweden),Silverman S (Beverly Hills, USA), Siris E (New York, USA) and SosaM (Las Palmas de Gran Canaria, Spain)
This position paper was endorsed by the Committee of ScientificAdvisors of IOF.
K. ÅkessonDepartment of Orthopaedics Malmo, Skåne University Hospital,Malmo, Sweden
D. MarshUniversity College London, London, UK
P. J. MitchellSynthesis Medical Limited, Auckland, New Zealand
A. R. McLellanGardiner Institute, Western Infirmary, Glasgow, UK
J. Stenmark :D. D. Pierroz :C. KyerInternational Osteoporosis Foundation,Nyon, Switzerland
C. Cooper (*)MRC Lifecourse Epidemiology Unit, University of Southampton,Southampton, UKe-mail: [email protected]
C. CooperNIHR Musculoskeletal Biomedical Research Unit,University of Oxford, Oxford, UK
Osteoporos Int (2013) 24:2135–2152DOI 10.1007/s00198-013-2348-z
from colleagues elsewhere that have achieved Best PracticeRecognition. A grant programme is in development to aidclinical systems which require financial assistance toestablish FLS in their localities.Conclusion Nearly half a billion people will reach retire-ment age during the next 20 years. IOF has developedCapture the Fracture because this is the single most impor-tant thing that can be done to directly improve patient care,of both women and men, and reduce the spiralling fracture-related care costs worldwide.
Keywords Capture the Fracture . Coordinator-based . FLS .
Fracture Liaison Service . Fracture prevention . Fragilityfracture
The International Osteoporosis Foundation Capturethe Fracture Campaign
In 2012, the International Osteoporosis Foundation (IOF)launched the Capture the Fracture Campaign [1, 2]. Capturethe Fracture is intended to substantially reduce the incidence ofsecondary fractures throughout the world. This will be deliv-ered by establishment of a new standard of care for fragilityfracture sufferers, whereby health care providers always re-spond to the first fracture to prevent the second and subsequentfractures. The most effective way to achieve this goal isthrough implementation of coordinator-based, post-fracturemodels of care. Exemplar models have been referred to as‘Fracture Liaison Services’ (United Kingdom [3–7], Europe[8, 9] and Australia [10–12]), ‘Osteoporosis Coordinator Pro-grams’ (Canada [13, 14]) or ‘Care Manager Programs’ (USA[15, 16]). For the purposes of this position paper, they will bereferred to as Fracture Liaison Services (FLS).
During the first 10 years of the twenty-first century—thefirst Bone and Joint Decade [17]—considerable progress wasmade in terms of establishment of exemplar FLS in manycountries [1] and the beginning of inclusion of secondaryfracture prevention into national health policies [18–26].However, FLS are currently established in a very small pro-portion of facilities that receive fracture patients worldwide,and many governments are yet to create the political frame-work to support funding of new services. The goal of Capturethe Fracture is to facilitate adoption of FLS globally. This willbe achieved by recognising and sharing best practice withhealth care professionals and their organisations, nationalosteoporosis societies and the patients they represent, andpolicymakers and their governments. This position paperdescribes why Capture the Fracture is needed and preciselyhow the campaign will operate over the coming years. IOFbelieves this is the single most important thing that can bedone to directly improve patient care, for women andmen, andreduce spiralling fracture-related health care costs worldwide.
The need for a global campaign
Half of women and a fifth of men will suffer a fragilityfracture in their lifetime [23, 27–29]. In year 2000,there were an estimated 9 million new fragility fracturesincluding 1.6 million at the hip, 1.7 million at the wrist,0.7 million at the humerus and 1.4 million symptomaticvertebral fractures [30]. More recent studies suggest that5.2 million fragility fractures occurred during 2010 in12 industrialised countries in North America, Europeand the Pacific region [31] alone, and an additional590,000 major osteoporotic fractures occurred in theRussian Federation [32]. Hip fracture rates are increas-ing rapidly in Beijing in China; between 2002 and 2006rates in women rose by 58 % and by 49 % in men [33].The costs associated with fragility fractures are currentlyenormous for Western populations and expected todramatically increase in Asia, Latin America and theMiddle East as these populations age:
& In 2005, the total direct cost of osteoporotic fractures inEurope was 32 billion EUR per year [34], which isprojected to rise to 37 billion EUR by 2025 [35]
& In 2002, the combined cost of all osteoporotic fracturesin the USA was 20 billion USD [36]
& In 2006, China spent 1.6 billion USD on hip fracturecare, which is projected to rise to 12.5 billion USD by2020 and 265 billion USD by 2050 [37]
A challenge on this scale can be both daunting andbewildering for those charged with developing a response,whether at the level of an individual institution or a nationalhealth care system. Fortuitously, nature has provided us withan opportunity to systematically identify almost half ofindividuals who will break their hip in the future. Patientspresenting with a fragility fracture today are twice as likelyto suffer future fractures compared to peers that haven’tsuffered a fracture [38, 39]. Crucially, from the obverseview, amongst individuals presenting with a hip fracture,almost half have previously broken another bone [40–43]. Abroad spectrum of effective agents are available to preventfuture fractures amongst those presenting with new frac-tures, and can be administered as daily [44–46], weekly[47, 48] or monthly tablets [49, 50], or as daily [51, 52],quarterly [53], six-monthly [54] or annual injections [55].Thus, a clear opportunity presents to disrupt the fragilityfracture cycle illustrated in Fig. 1, by consistently targetingfracture risk assessment, and treatment where appropriate, tofragility fracture sufferers [56].
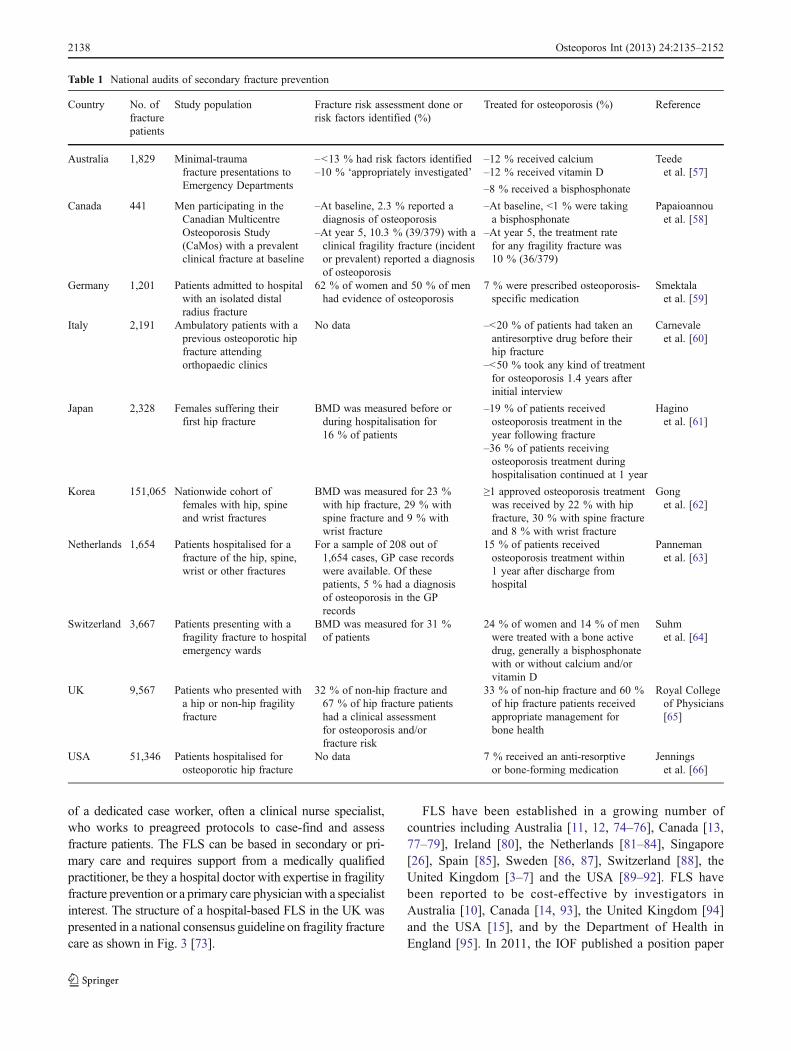
Regrettably, the majority of health care systems aroundthe world are currently failing to respond to the first fractureto prevent the second. The ubiquitous nature of the second-ary fracture prevention care gap is evident from the national
2136 Osteoporos Int (2013) 24:2135–2152
audits summarised in Table 1, for both women and men[57–66]. Additionally, a substantial number of regional andlocal audits have been summarised in the 2012 IOF WorldOsteoporosis Day Report, which mirror the findings of thenational audits [1]. The secondary fracture prevention caregap is persistent. A recent prospective observational studyof >60,000 women aged ≥55 years, recruited from 723primary physician practices in 10 countries, reported thatless than 20 % of women with new fractures receivedosteoporosis treatment [67]. A province-wide study in Man-itoba, Canada has revealed that post-fracture diagnosis andtreatment rates have not substantially changed between1996/1997 and 2007/2008, despite increased awareness ofosteoporosis care gaps during the intervening decade [68].
The reason that the care gap exists, and persists, is multi-factorial in nature. A systematic review from Elliot-Gibsonand colleagues in 2004 identified the following issues [69]:
& Cost concerns relating to diagnosis and treatment& Time required for diagnosis and case finding& Concerns relating to polypharmacy& Lack of clarity regarding where clinical responsibility
resides
The issue regarding where clinical responsibility residesresonates with health care professionals throughout theworld. Harrington’s metaphorical depiction captures theessence of the problem [70]:
‘Osteoporosis care of fracture patients has beencharacterised as the Bermuda Triangle made up oforthopaedists, primary care physicians and osteo-porosis experts into which the fracture patientdisappears’
Surveys have shown that in the absence of a robust carepathway for fragility fracture patients, a ‘Catch-22’ scenarioprevails [71]. Orthopaedic surgeons rely on primary caredoctors to manage osteoporosis; primary care doctors routine-ly only do so if so advised by the orthopaedic surgeon; andosteoporosis experts—usually endocrinologists or rheumatol-ogists—have no cause to interact with the patient during thefracture episode. The proven solution to close the secondaryfracture prevention care gap is to eliminate this confusion byestablishing a Fracture Liaison Service (FLS).
Systematic literature review of programs designed todeliver secondary preventive care reported that two thirdsof services employ a dedicated coordinator to act as the linkbetween the patient, the orthopaedic team, the osteoporosisand falls prevention services, and the primary care physician[72]. Successful and sustainable FLS report that clearlydefining the scope of the service from the outset is essential.Some FLS began by focusing initially on hip fracturepatients, and subsequently expanded the scope of the serviceuntil all fracture patients presenting to their institution wereassessed as illustrated in Fig. 2.
The core objectives of an FLS are:
1. Inclusive case finding2. Evidence-based assessment—stratify risk, identify
secondary causes of osteoporosis, tailor therapy3. Initiate treatment in accordance with relevant guidelines4. Improve long-term adherence with therapy
The operational characteristics of a comprehensive FLShave been described as follows [1]. The FLS will ensurefracture risk assessment, and treatment where appropriate, isdelivered to all patients presenting with fragility fractures in theparticular locality or institution. The service will be comprised
Fig. 1 The fragility fracturecycle (reproduced withpermission of the Departmentof Health in England [56])
Osteoporos Int (2013) 24:2135–2152 2137
of a dedicated case worker, often a clinical nurse specialist,who works to preagreed protocols to case-find and assessfracture patients. The FLS can be based in secondary or pri-mary care and requires support from a medically qualifiedpractitioner, be they a hospital doctor with expertise in fragilityfracture prevention or a primary care physician with a specialistinterest. The structure of a hospital-based FLS in the UK waspresented in a national consensus guideline on fragility fracturecare as shown in Fig. 3 [73].
FLS have been established in a growing number ofcountries including Australia [11, 12, 74–76], Canada [13,77–79], Ireland [80], the Netherlands [81–84], Singapore[26], Spain [85], Sweden [86, 87], Switzerland [88], theUnited Kingdom [3–7] and the USA [89–92]. FLS havebeen reported to be cost-effective by investigators inAustralia [10], Canada [14, 93], the United Kingdom [94]and the USA [15], and by the Department of Health inEngland [95]. In 2011, the IOF published a position paper
Table 1 National audits of secondary fracture prevention
Country No. offracturepatients
Study population Fracture risk assessment done orrisk factors identified (%)
Treated for osteoporosis (%) Reference
Australia 1,829 Minimal-traumafracture presentations toEmergency Departments
–<13 % had risk factors identified –12 % received calcium Teedeet al. [57]–10 % ‘appropriately investigated’ –12 % received vitamin D
–8 % received a bisphosphonate
Canada 441 Men participating in theCanadian MulticentreOsteoporosis Study(CaMos) with a prevalentclinical fracture at baseline
–At baseline, 2.3 % reported adiagnosis of osteoporosis
–At baseline, <1 % were takinga bisphosphonate
Papaioannouet al. [58]
–At year 5, 10.3 % (39/379) with aclinical fragility fracture (incidentor prevalent) reported a diagnosisof osteoporosis
–At year 5, the treatment ratefor any fragility fracture was10 % (36/379)
Germany 1,201 Patients admitted to hospitalwith an isolated distalradius fracture
62 % of women and 50 % of menhad evidence of osteoporosis
7 % were prescribed osteoporosis-specific medication
Smektalaet al. [59]
Italy 2,191 Ambulatory patients with aprevious osteoporotic hipfracture attendingorthopaedic clinics
No data –<20 % of patients had taken anantiresorptive drug before theirhip fracture
Carnevaleet al. [60]
–<50 % took any kind of treatmentfor osteoporosis 1.4 years afterinitial interview
Japan 2,328 Females suffering theirfirst hip fracture
BMD was measured before orduring hospitalisation for16 % of patients
–19 % of patients receivedosteoporosis treatment in theyear following fracture
Haginoet al. [61]
–36 % of patients receivingosteoporosis treatment duringhospitalisation continued at 1 year
Korea 151,065 Nationwide cohort offemales with hip, spineand wrist fractures
BMD was measured for 23 %with hip fracture, 29 % withspine fracture and 9 % withwrist fracture
≥1 approved osteoporosis treatmentwas received by 22 % with hipfracture, 30 % with spine fractureand 8 % with wrist fracture
Gonget al. [62]
Netherlands 1,654 Patients hospitalised for afracture of the hip, spine,wrist or other fractures
For a sample of 208 out of1,654 cases, GP case recordswere available. Of thesepatients, 5 % had a diagnosisof osteoporosis in the GPrecords
15 % of patients receivedosteoporosis treatment within1 year after discharge fromhospital
Pannemanet al. [63]
Switzerland 3,667 Patients presenting with afragility fracture to hospitalemergency wards
BMD was measured for 31 %of patients
24 % of women and 14 % of menwere treated with a bone activedrug, generally a bisphosphonatewith or without calcium and/orvitamin D
Suhmet al. [64]
UK 9,567 Patients who presented witha hip or non-hip fragilityfracture
32 % of non-hip fracture and67 % of hip fracture patientshad a clinical assessmentfor osteoporosis and/orfracture risk
33 % of non-hip fracture and 60 %of hip fracture patients receivedappropriate management forbone health
Royal Collegeof Physicians[65]
USA 51,346 Patients hospitalised forosteoporotic hip fracture
No data 7 % received an anti-resorptiveor bone-forming medication
Jenningset al. [66]
2138 Osteoporos Int (2013) 24:2135–2152
on coordinator-based systems for secondary fracture preven-tion [96] which was followed in 2012 by the AmericanSociety for Bone and Mineral Research Secondary Preven-tion Task Force Report [97]. These major internationalinitiatives underscore the degree of consensus shared byprofessionals throughout the world on the need for FLS tobe adopted and adapted for implementation in all countries.FLS serves as an exemplar in relation to the Health CareQuality Initiative of the Institute of Medicine (IOM) [98].The IOM defines quality as:
‘The degree to which health services for individualsand populations increase the likelihood of desiredhealth outcomes and are consistent with current pro-fessional knowledge’
We know that secondary fracture prevention is clinicallyand cost-effective, but does not routinely happen. FLScloses the disparity between current knowledge and currentpractice.
An important component of the Capture the Fracture Cam-paign will be to establish global reference standards for FLS.Several systematic reviews have highlighted that a range ofservice models have been designed to close the secondaryfracture prevention care gap, with varying degrees of success[72, 99, 100]. Having clarity on precisely what constitutes bestpractice will provide a mechanism for FLS in different localitiesand countries to learn from one another. The Capture theFracture ‘Best Practice Framework’ described later in this po-sition paper aims to provide a mechanism to facilitate this goal.
How Capture the Fracture works
Background
The Capture the Fracture Campaign was launched at theIOF European Congress on Osteoporosis and Osteoarthritisin Bordeaux, France in March 2012. Healthcare professio-nals that have played a leading role in establishing FLS andrepresentatives from national patient societies shared theirefforts to embed FLS in national policy in their countries. InOctober 2012, the IOF World Osteoporosis Day report wasdevoted to Capture the Fracture [1] and disseminated atevents organised by national societies throughout the world[101]. This position paper presents the aims and structure ofthe Capture the Fracture Campaign. A Steering Committeecomprised of the authorship group of this position paper hasled development of the campaign and will provide ongoingsupport to the implementation of the next steps.
Aims
The aims of Capture the Fracture are:
& Standards: To provide internationally endorsed stand-ards for best practice in secondary fracture prevention.Specific components are:
– Best Practice Framework
Fig. 2 Defining the scope of an FLS and expansion of fracture pop-ulation assessed [1] n.b. The ultimate goal of an FLS is to capture100 % of fragility fracture sufferers. This figure recognises that devel-opment of FLS may be incremental
* Older patients, where appropriate, are identified and referred for falls assessment
Comprehensive communication of management plan to GPsupported by fully integrated FLS database system
Fig. 3 The operationalstructure of a hospital-basedFracture Liaison Service [73]Asterisk (*) older patients,where appropriate, areidentified and referred for fallsassessment
Osteoporos Int (2013) 24:2135–2152 2139
– Best Practice Recognition– Showcase of best practices
& Change: Facilitation of change at the local and nationallevel will be achieved by:
– Mentoring programmes– Implementation guides and toolkits– Grant programme for developing systems
& Awareness: Knowledge of the challenges and opportu-nities presented by secondary fracture prevention will beraised globally by:
– An ongoing communications plan– Anthology of literature, worldwide surveys and
audits– International coalition of partners and endorsers
Internationally endorsed standards
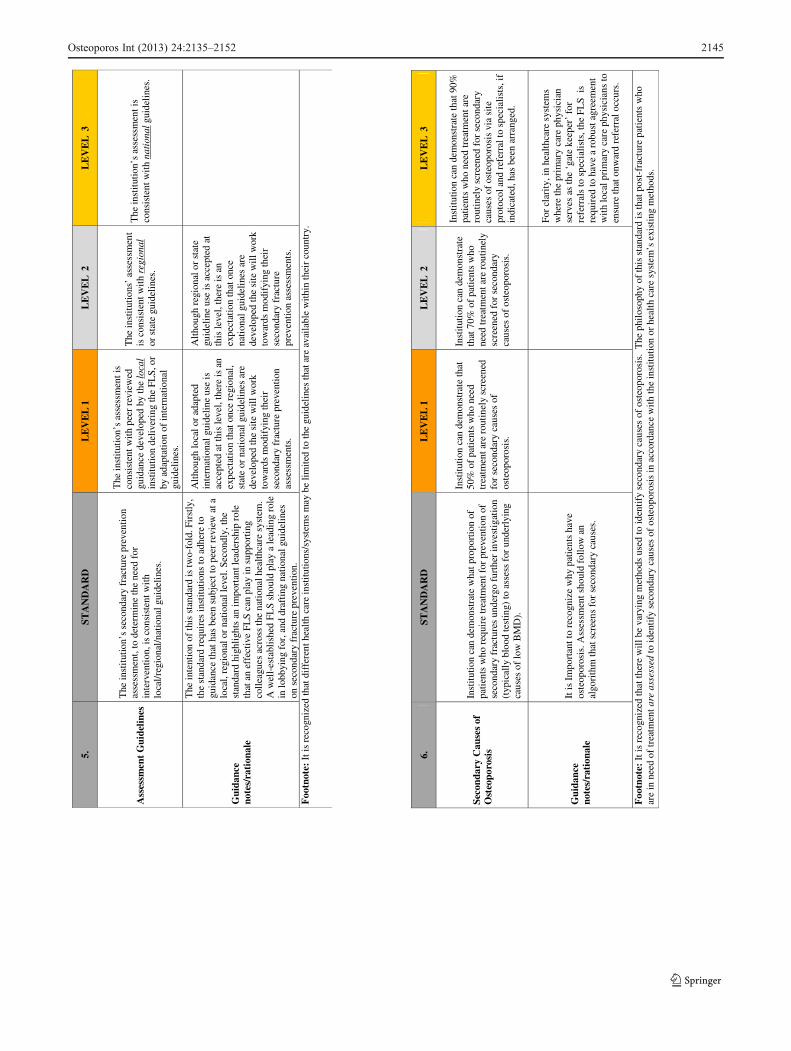
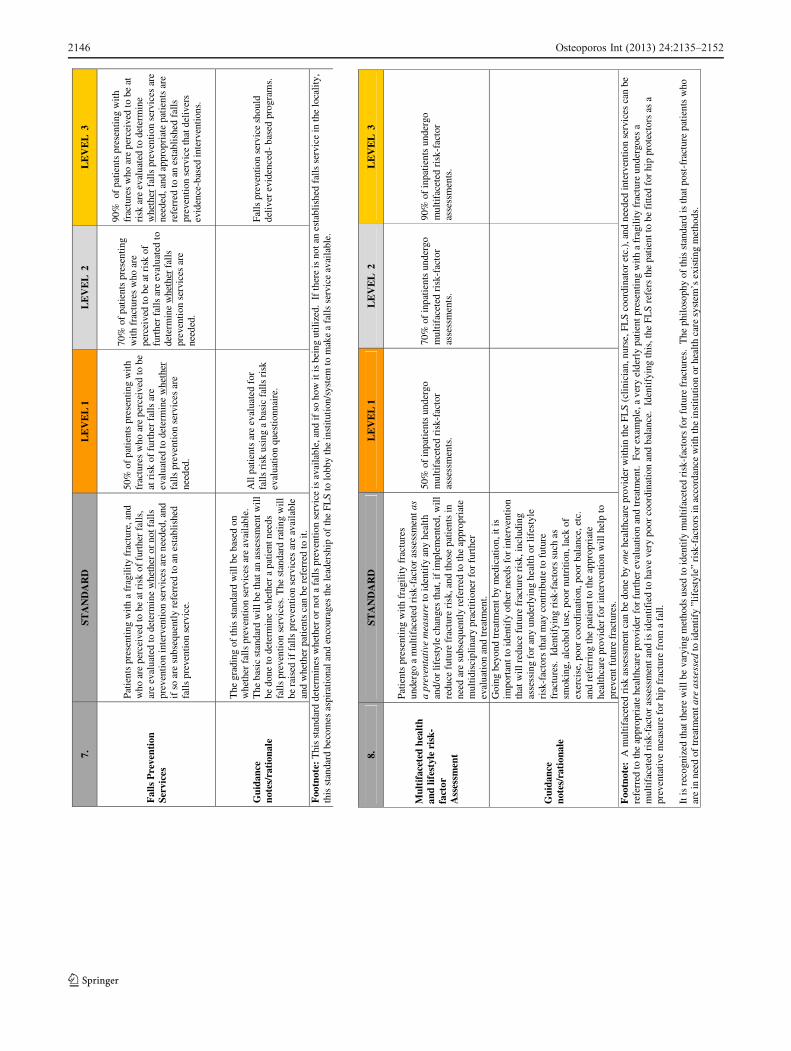
The centrepiece of the Capture the Fracture Campaign is theBest Practice Framework (BPF), provided as Appendix. TheBPF is comprised of 13 standards which set an internationalbenchmark for Fracture Liaison Services. Each standard hasthree levels of achievement: Level 1, Level 2 or Level 3.The BPF:
1. Defines the essential and aspirational buildingblocks that are necessary to implement a successfulFLS, and
2. Serves as the measurement tool for IOF to award‘Capture the Fracture Best Practice Recognition’ incelebration of successful FLS worldwide
Establishing standards for health care delivery systems thathave global relevance is very difficult. However, the ‘parallelevolution’ of FLS with broadly similar structure and functionin many countries of the world, as described previously,suggested that a meaningful platform for benchmarking couldbe created. The structure of healthcare systems varies consid-erably throughout the world, so the context within which FLShave, and will be established in different countries may bemarkedly different. Accordingly, the BPF has been developedwith cognisance that the scope of an FLS—and the limits of itsfunction and effectiveness—may be constrained by the natureof health care infrastructure in the country of origin. To thisend, clinical innovators who choose to submit their FLS forbenchmarking by the BPF are encouraged to:
& Use existing procedures as they correspond to theirhealth care system: Existing, individual systems and
procedures that are currently in place can be used tomeasure performance against the standards.
& Meaning of the term ‘institution’: Throughout the BPF,the word ‘institution’ is used which is intended to be ageneric term for: the inpatient and/or outpatient facili-ties, and/or health care systems for which the FLS wasestablished to serve.
& Limit applications to ‘systems’ of care: The BPF is intendedfor larger ‘systems’ of care, within the larger healthcare setting, which consist of multidisciplinary pro-viders and deal with a significant volume of fracturepatients.
& Recognise that the BPF is both achievable and ambi-tious: Some of the BPF standards address essentialaspects of an FLS, while others are aspirational. Aweight has been assigned to each standard based onhow important the standard is in relation to an FLSdelivering best practice care. This:
1. Enables recognition of systems who have achievedthe most essential elements, while leavingroom for improvement towards implementingthe aspirational elements
2. Allows systems to achieve a standard of care,Silver for example, with a range of levels ofachievement across the 13 standards
Applications will be received through a web-based ques-tionnaire, at www.capturethefracture.org, which gathers infor-mation about the FLS and its achievements as they correspondto the Best Practice Framework. IOF staff will process sub-missions which will be reviewed and validated by members ofthe Steering Committee to generate a summary profile. Thiswill determine the level of recognition to be assigned to theFLS as Unclassified, Bronze, Silver or Gold across four keyfragility fracture patient groups—hip fracture, other in-patient fractures, outpatient fracture, vertebral fracture—and organizational characteristics. Applicants achieving Cap-ture the Fracture Recognition will be recognised by IOFin the following ways:
& Placement of the applicant’s FLS on the Capture theFracture website’s interactive map, including the systemname, location, link and programme showcase
& Awarded use of the IOF-approved, Capture the FractureBest Practice Recognition logo for use on the applicant’swebsites and materials
Facilitating change at the local and national level
The Capture the Fracture website—www.capturethefracture.org—provides links to resources related to FLSand secondary fracture prevention. These include FLS
implementation guides and national toolkits which havebeen developed for some countries. As new resourcesbecome available, the website will serve as a portal forsharing of materials to support healthcare professionalsand national patient societies to establish FLS in theirinstitutions and countries.
Further supporting the establishment of FLS, Cap-ture the Fracture will organise a locality specific men-toring programme between sites that have achievedBest Practice Recognition and those systems that arein early stage development. An opportunity exists tocreate a global network to support sharing of the suc-cesses and challenges that will be faced in the processof implementing best practice. This network has thepotential to contribute significantly to adoption ofFLS throughout the world. During 2013, IOF intendsto develop a grant programme to aid clinical systemsaround the world which require financial assistance toestablish FLS.
Raising awareness
A substantial body of literature on secondary fracture pre-vention and FLS has developed over the last decade. Afeature of the Capture the Fracture website is a ResearchLibrary which organises the world’s literature into an acces-sible format. This includes sections on care gaps and casefinding; assessment, treatment and adherence; and healtheconomic analysis.
IOF has undertaken to establish an international coa-lition of partners and endorsers to progress implementa-tion of FLS. At the national level, establishment ofmulti-sector coalitions has played an important role inachieving prioritisation of secondary fracture preventionand FLS in national policy and reimbursement systems[1]. The Capture the Fracture website provides a mecha-nism to share such experience between organisationsand national societies in different countries. Increasingawareness that the secondary fracture prevention caregap has been closed by implementation of FLS, andthat policy and reimbursement systems have been crea-ted to support establishment of new FLS, will catalysebroader adoption of the model.
A global call to action
During the next 20 years, 450 million people worldwidewill celebrate their 65th birthday [102]. As a result, inthe absence of systematic preventive intervention, thehuman and financial costs of fragility fractures will risedramatically. Policymakers, professional organisations,patient societies, payers and the private sector mustwork together to ensure that every fracture that could
be prevented is prevented. Almost half of hip fracturepatients suffer a previous fragility fracture before break-ing their hip, creating an obvious opportunity for inter-vention. However, currently, a secondary fractureprevention care gap exists throughout the world. Thiscare gap can and must be eliminated by implementationof Fracture Liaison Services. The Capture the FractureCampaign provides all necessary evidence, internationalstandards of care, practical resources and a network ofinnovators to support colleagues globally to close thesecondary prevention care gap. We call upon those re-sponsible for fracture patient care throughout the world toimplement Fracture Liaison Services as a matter ofurgency.
Acknowledgments The authors would like to thank GilbertoLontro (Senior Graphic Designer, IOF), Chris Aucoin (MultimediaIntern) and Shannon MacDonald, RN (Science Coordinator, IOF)for their excellent and many contributions to development of theCapture the Fracture Campaign. We are also very grateful to thefollowing colleagues throughout the world who have provideinvaluable support in the development of the Best Practice Frame-work: Dr. Andrew Bunta (Own the Bone, American OrthopaedicAssociation, USA), Dr. Pedro Carpintero (University HospitalReina Sofia, Cordoba, Spain), Dr. Manju Chandran (SingaporeGeneral Hospital, Singapore), Dr. Gavin Clunie (AddenbrookesHospital, Cambridge, UK), Professor Elaine Dennison (Universityof Southampton, UK), Ravi Jain (Osteoporosis Canada), ProfessorStephen Kates (University of Rochester Medical Center, USA),Dr. Ambrish Mithal (Medanta Medicity, Gurgaon, India), Dr. EricNewman (Geisinger Health System, USA), Dr. Marcelo Pinheiro(Universidade Federal de São Paulo, Brazil), Professor MarkusSeibel (The University of Sydney at Concord, Australia), Dr.Bernardo Stolnicki (Federal Hospital Ipanema, Brazil), ProfessorThierry Thomas (Groupe de Recherche et d’Information surL' Ostéoporose [GRIO], France), Dr. Jan Vaile (Royal PrinceAlfred Hospital, Sydney, Australia), Dr. John Van Der Kallen(John Hunter Hospital, Newcastle, Australia).
Conflicts of interest None.
Open Access This article is distributed under the terms of the Crea-tive Commons Attribution License which permits any use, distribution,and reproduction in any medium, provided the original author(s) andthe source are credited.
Appendix. Capture the Fracture Best Practice Framework
The 13 Capture the Fracture Best Practice Standards are:
8. Multifaceted health and lifestyle risk-factorAssessment Standard
9. Medication Initiation Standard10. Medication Review Standard11. Communication Strategy Standard12. Long-term Management Standard13. Database Standard
The BPF contains standards that are both essential andaspirational; therefore, a weight is assigned to each standardbased on how essential the standard is to a successful FLS.Three levels of achievement against each standard attract
scores of 1, 2 or 3 (n.b. standard 12 is dichotomous). Theweighting and scoring system is as follows:
The standards are weighted: The scores within each standard are:
Essential=weight of 1 Level 1=1
Medium=weight of 2 Level 2=2
Aspirational=weight of 3 Level 3=3
The calculator is as follows (for each standard, multiplythe weight by the Level 1, Level 2 or Level 3 achieved, andadd the total):
It is important that the output of the framework tool isclear for health care professionals, patients and the public asit well permit meaningful comparisons both across sitesnationally and globally as well as through the coming yearsas services evolve.
To this end, a level of recognition will be assigned to eachcentre as a summary profile from Unclassified throughBronze, Silver and/or Gold in up to four key fragility fracturepatient groups—hip fractures, other in-patient fractures, out-patient fractures and vertebral fractures—and organizationalcharacteristics. This will be achieved in a two-stage process.
Sites will independently complete a fracture service ques-tionnaire and submit this to the IOF Capture the FractureCommittee of Scientific Advisors (IOF CTF CSA). The IOFCTF CSA would acknowledge receipt of the form andperform a draft grading from both administrative and clini-cal perspectives depending on the achievement of the IOFBPF standards within each domain. A summary profile for
each domain will be made as a series of star ratings(Unclassified, Bronze, Silver and Gold).
The draft summary profile will then be fed back to thesite with a request for further information if there are areasof uncertainty. On receipt of the site’s response, a suggestedfinal summary profile will be presented to the IOF CTFCSA for approval. Importantly, should this process of rec-ognition highlight areas for improving the fracture site ques-tionnaire, additional recommendations will be presented tothe IOF CFA CSA and, if approved, an updated version ofthe questionnaire will be hosted on the website for futuresites to complete. Through this iterative clinically led pro-cess, the IOF BPF will remain responsive to changes inclinical practice globally as well as retain key attributes thatpermit meaningful comparisons in service excellenceglobally.
The details of the 13 standards are provided below withexplanatory guidance:
Standard Weight Level 1 Level 2 Level 3 Achievement Level ENTERLevel1/Level2/Level3SCORE HERE
Standard Total(weight×level)
1 Patient Identification 1 x 1 2 3 0
2 Patient Evaluation 1 x 1 2 3 0
3 Post-fracture Assessment Timing 2 x 1 2 3 0
4 Vertebral Fracture 3 x 1 2 3 0
5 Assessment Guidelines 3 x 1 2 3 0
6 Secondary Causes of Osteoporosis 3 x 1 2 3 0
7 Falls Prevention Services 1 x 1 2 3 0
8 Multifaceted health and lifestylerisk-factor Assessment
3 x 1 2 3 0
9 Medication Initiation 1 x 1 2 3 0
10 Medication Review 2 x 1 2 3 0
11 Communication Strategy 2 x 1 2 3 0
12 Long-term Management 2 x 1 3 0
13 Database 1 x 1 2 3 0
TOTAL Achievement Level 0
2142 Osteoporos Int (2013) 24:2135–2152
Foo
tnot
e:
1.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Pat
ient
Ide
ntif
icat
ion
Frac
ture
pat
ient
s w
ithi
n th
e sc
ope
of th
e in
stitu
tion
(inp
atie
nt a
nd/o
r ou
tpat
ient
fac
ility
or
heal
th c
are
syst
em)
are
iden
tifie
d to
ena
ble
deli
very
of
seco
ndar
y fr
actu
re p
reve
ntio
n.
Cli
nica
l fra
ctur
e pa
tien
ts a
re
bein
g id
enti
fied
but
no
patie
nt
trac
king
sys
tem
exi
sts
to e
valu
ate
perc
enta
ge o
f pa
tient
s th
at a
re
iden
tifie
d ve
rsus
thos
e th
at a
re
not.
Cli
nica
l fra
ctur
e pa
tien
ts a
re
bein
g id
enti
fied
and
a
pati
ent t
rack
ing
syst
em
exis
ts to
eva
luat
e pe
rcen
tage
of
pat
ient
s th
at a
re id
entif
ied
vers
us th
ose
that
are
not
.
Cli
nica
l fra
ctur
e pa
tien
ts a
re b
eing
id
entif
ied
and
a pa
tien
t tra
ckin
g sy
stem
exi
sts
to e
valu
ate
perc
enta
ge o
f pa
tien
ts th
at a
re id
enti
fied
ver
sus
thos
e th
at a
re n
ot.
The
qua
lity
of
data
ca
ptur
e ha
s be
en s
ubje
ct to
in
depe
nden
t rev
iew
.
Gui
danc
e no
tes/
rati
onal
e
Thi
s in
tent
ion
of th
is s
tand
ard
is to
asc
erta
in th
eR
OU
TE
by
whi
ch f
ract
ure
pati
ents
are
id
entif
ied.
The
sta
ndar
d re
cogn
ises
that
som
e in
stitu
tions
will
man
age
just
inpa
tient
s, s
ome
wil
l man
age
just
out
patie
nts
and
othe
rs w
ill
man
age
both
in-
and
outp
atie
nts.
The
Nom
inat
ion
Plat
form
Que
stio
nnai
re (
NPQ
) w
ill i
dent
ify
whi
ch ty
pe o
f fr
actu
re p
atie
nts
are
incl
uded
wit
hin
the
scop
e of
the
inst
itut
ion.
The
inst
itut
ion
does
not
hav
e a
syst
em to
trac
k ev
ery
pati
ent
pres
entin
g to
the
inst
itutio
n w
ith
a fr
actu
re, s
o ca
nnot
acc
urat
ely
dete
rmin
e th
e pr
opor
tion
of
all
pati
ents
that
are
rea
ched
by
the
serv
ice.
The
inst
itut
ion
does
hav
e a
syst
em to
trac
k ev
ery
pati
ent
pres
entin
g to
the
inst
itutio
n w
ith
a fr
actu
re, s
o ca
nac
cura
tely
det
erm
ine
the
prop
ortio
n of
all
pat
ient
s th
at a
re r
each
ed b
y th
e se
rvic
e.
The
inst
itut
ion
does
hav
e a
syst
em to
tr
ack
ever
ypa
tien
t pre
sent
ing
to th
e in
stitu
tion
wit
h a
frac
ture
, and
has
da
ta q
uali
ty c
ontr
ol a
sses
smen
t m
easu
res
inde
pend
ent o
f th
e te
am th
at
deli
ver
post
-fra
ctur
e ca
re e
.g. a
n ex
isti
ng h
ospi
tal-
wid
e da
ta q
uali
ty
assu
ranc
e te
am o
r cl
inic
al c
odin
g qu
alit
y te
am th
at is
eit
her
inte
rnal
or
exte
rnal
to th
e ho
spita
l/sy
stem
. I
t is
reco
gniz
ed th
at h
ealt
h ca
re in
stit
utio
ns/s
yste
ms
wil
l hav
e va
ryin
g m
etho
ds to
def
ine
thei
r ’f
ract
ure
pati
ent’
gro
up, w
heth
er it
be
by d
iagn
osti
c co
des
(IC
D, C
IM10
),
pati
ent a
ge, f
ract
ure
type
etc
., fr
om w
hich
to e
nabl
e se
cond
ary
frac
ture
pre
vent
ion.
2.
STA
ND
AR
D
LE
VE
L1
LE
VE
LL
EV
EL
3
Pat
ient
Eva
luat
ion
Id
enti
fied
fra
ctur
e pa
tient
s w
ithi
n th
e sc
ope
of th
e in
stitu
tion
are
asse
ssed
for
fut
ure
frac
ture
ris
k.
Of
thos
e pa
tien
ts id
entif
ied,
in
who
m p
rogr
essi
on to
imm
edia
te
trea
tmen
t is
not w
arra
nted
, 50%
ar
e as
sess
ed f
or s
ubse
quen
t fr
actu
re r
isk.
Of
thos
e pa
tien
ts id
entif
ied,
in
who
m p
rogr
essi
on to
im
med
iate
trea
tmen
t is
not
war
rant
ed, 7
0% a
re a
sses
sed
for
subs
eque
nt f
ract
ure
risk
.
Of
thos
e pa
tien
ts id
entif
ied,
in w
hom
pr
ogre
ssio
n to
imm
edia
te tr
eatm
ent
is n
ot w
arra
nted
, 90%
or
mor
e ar
e as
sess
ed f
or s
ubse
quen
t fra
ctur
e ri
sk.
Gui
danc
e no
tes/
rati
onal
e
Thi
s st
anda
rd is
con
cern
ed w
ith
the
num
ber
of
pati
ents
bei
ng a
sses
sed
for
subs
eque
nt f
ract
ure
risk
. The
inte
ntio
n of
this
sta
ndar
d is
to a
scer
tain
w
hat p
ropo
rtio
n of
all
pat
ient
s pr
esen
ting
to th
e in
stitu
tion
or s
yste
m w
ith
a fr
actu
re a
re e
valu
ated
for
futu
re f
ract
ure
risk
. The
sta
ndar
d re
cogn
ises
th
at s
ome
inst
itut
ions
will
man
age
just
inpa
tien
ts,
som
e w
ill m
anag
e ju
st o
utpa
tien
ts a
nd o
ther
s w
ill
man
age
both
in-
and
outp
atie
nts.
Add
ition
ally
, the
st
anda
rd r
ecog
nise
s ci
rcum
stan
ces
whe
n th
e be
st
prac
tice
is to
byp
ass
frac
ture
eva
luat
ion
and
go
stra
ight
to tr
eatm
ent p
roto
cols
(e.
g. f
or p
atie
nts
who
are
80+
).
F
ootn
ote:
Eva
luat
ion
on th
is s
tand
ard
wil
l tak
e in
to a
ccou
nt th
e di
ffic
ulti
es a
ssoc
iate
d w
ith
asse
ssin
g pa
tien
ts w
ith
dem
entia
or
impa
ired
cog
nitiv
e fu
ncti
on.
Osteoporos Int (2013) 24:2135–2152 2143
3.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Pos
t F
ract
ure
Ass
essm
ent
Tim
ing
Post
-fra
ctur
e as
sess
men
t for
sec
onda
ry f
ract
ure
prev
enti
on is
con
duct
ed in
a ti
mel
y fa
shio
n af
ter
frac
ture
pre
sent
atio
n.
Post
-fra
ctur
e as
sess
men
t for
se
cond
ary
frac
ture
pre
vent
ion
occu
rs w
ithi
n 12
-16
wee
ks o
f cl
inic
al f
ract
ure
pres
enta
tion
.
Post
-fra
ctur
e as
sess
men
t for
se
cond
ary
frac
ture
pr
even
tion
occ
urs
wit
hin
8-12
wee
ks o
f cl
inic
al f
ract
ure
pres
enta
tion
.
Post
-fra
ctur
e as
sess
men
t for
se
cond
ary
frac
ture
pre
vent
ion
occu
rs
wit
hin
8 w
eeks
of
clin
ical
fra
ctur
e pr
esen
tati
on.
Gui
danc
e no
tes/
rati
onal
e
Thi
s st
anda
rd is
con
cern
ed w
ith
the
tim
ing
of
whe
n su
bseq
uent
fra
ctur
e ri
sk a
sses
smen
t is
done
. T
his
asse
ssm
ent c
an p
erfo
rmed
by
any
qual
ifie
d pr
ovid
er b
ut m
ust b
e tr
acke
d by
the
FLS
coor
dina
tor
and
mus
t con
tain
app
ropr
iate
pos
t-fr
actu
re a
sses
smen
t ele
men
ts s
uch
as b
one
dens
ity
test
ing,
ris
k as
sess
men
t or
othe
r as
sess
men
t pro
cedu
res
rele
vant
to th
e pa
tien
t.
Thi
s is
to e
nsur
e a
form
al f
ract
ure
risk
ass
essm
ent
has
been
don
e.
The
pro
port
ion
of p
atie
nts
whi
ch
this
sta
ndar
d ap
plie
s to
is d
efin
ed
by th
e 50
%, 7
0% a
nd 9
0% r
ange
s re
quir
ed to
ach
ieve
Lev
el 1
, L
evel
2 o
r L
evel
3, r
espe
ctiv
ely,
in
Sta
ndar
d 2.
The
pro
port
ion
of p
atie
nts
whi
ch th
is s
tand
ard
appl
ies
to is
def
ined
by
the
50%
, 70
% a
nd 9
0% r
ange
s re
quir
ed to
ach
ieve
Lev
el 1
, L
evel
2 o
r L
evel
3,
resp
ecti
vely
, in
Stan
dard
2.
The
pro
port
ion
of p
atie
nts
whi
ch
this
sta
ndar
d ap
plie
s to
is d
efin
ed b
y th
e 50
%, 7
0% a
nd 9
0% r
ange
s re
quir
ed to
ach
ieve
Lev
el 1
, Lev
el 2
or
Lev
el 3
, res
pect
ivel
y, in
Sta
ndar
d 2.
Foo
tnot
e: U
tiliz
ing
the
heal
th c
are
inst
itutio
n/sy
stem
’s a
vera
ge ti
min
g pr
otoc
ols,
app
lica
nts
are
enco
urag
ed to
giv
e as
acc
urat
e a
tim
e-fr
ame
as p
ossi
ble
for
whe
n th
e po
st-f
ract
ure
asse
ssm
ent f
or s
econ
dary
fra
ctur
e pr
even
tion
is c
ondu
cted
. It
is n
oted
, how
ever
, tha
t con
duct
ing
post
-fra
ctur
e as
sess
men
t at a
tim
e gr
eate
r th
an f
our
mon
ths
post
-fra
ctur
e is
too
late
.
Foo
tnot
e:
4.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Ver
tebr
al F
ract
ure
Inst
itut
ion
has
a sy
stem
whe
reby
pat
ient
s w
ith
prev
ious
ly u
nrec
ogni
sed
vert
ebra
l fra
ctur
es a
re
iden
tifie
d an
d un
derg
o se
cond
ary
frac
ture
pr
even
tion
eva
luat
ion.
Pati
ents
wit
h cl
inic
al v
erte
bral
fr
actu
res
unde
rgo
asse
ssm
ent
and/
or r
ecei
ve tr
eatm
ent f
or
prev
enti
on o
f se
cond
ary
frac
ture
s.
Pati
ents
wit
h no
n-ve
rteb
ral
frac
ture
s ro
utin
ely
unde
rgo
asse
ssm
ent w
ith
late
ral
vert
ebra
l mor
phom
etry
by
DX
A (
or p
ossi
bly
by p
lain
sp
ine
radi
olog
y) to
ass
ess
for
vert
ebra
l fra
ctur
es.
Pati
ents
who
are
rep
orte
d by
the
Inst
itut
ion’
s R
adio
logi
sts
to h
ave
vert
ebra
l fra
ctur
es o
n pl
ain
Xra
ys,
CT
& M
RI
scan
s (w
heth
er th
ese
are
sere
ndip
itous
or
not)
are
iden
tifi
ed
by th
e FL
S in
ord
er th
at th
ey
unde
rgo
asse
ssm
ent f
or tr
eatm
ent
for
prev
entio
n of
sec
onda
ry
frac
ture
s.
Gui
danc
e no
tes/
rati
onal
e
The
maj
orit
y of
ver
tebr
al f
ract
ures
are
un
reco
gnis
ed o
r un
dete
cted
. The
inte
ntio
n of
this
st
anda
rd is
to e
stab
lish
wha
t sys
tem
s th
e in
stitu
tion
has
put i
n pl
ace
to id
entif
y ve
rteb
ral
frac
ture
s am
ongs
t pat
ient
s pr
esen
ting
and/
or
adm
itted
to th
e in
stitu
tion
for
any
cond
itio
n.
Kno
wle
dge
of v
erte
bral
fra
ctur
e st
atus
in a
ddit
ion
to B
MD
has
bee
n sh
own
to s
igni
fica
ntly
impr
ove
frac
ture
ris
k pr
edic
tion
for
seco
ndar
y fr
actu
res.
Up
to a
qua
rter
of
pati
ents
pr
esen
ting
to a
n FL
S w
ith
non-
vert
ebra
l fra
ctur
es w
ere
show
n to
ha
ve v
erte
bral
def
orm
itie
s by
V
erte
bral
Fra
ctur
e A
sses
smen
t te
chno
logy
. The
sta
ndar
d is
co
gnis
ant t
hat f
or s
ome
frac
ture
pa
tien
ts c
ondu
ctin
g ve
rteb
ral
frac
ture
ass
essm
ent m
ay n
ot b
e pr
acti
cal f
or c
hang
e m
anag
emen
t e.
g. a
mon
gst h
ip f
ract
ure
pati
ents
.
For
thos
e pa
tien
ts r
efer
red
into
a lo
cal b
one
dens
itom
etry
uni
t for
a D
XA
sc
an o
n ac
coun
t of
reas
ons
othe
r th
an a
pri
or f
ract
ure
hist
ory,
asc
erta
inin
g ve
rteb
ral f
ract
ure
stat
us m
ay
infl
uenc
e tr
eatm
ent
deci
sion
s si
gnif
ican
tly
for
a pr
opor
tion
of p
atie
nts.
A s
ubst
antia
l vol
ume
of im
agin
g is
un
dert
aken
am
ongs
t ove
r 50
yea
r ol
ds w
hich
pre
sent
s an
opp
ortu
nity
to
sig
nifi
cant
ly in
crea
se
iden
tific
atio
n ra
tes
of p
atie
nts
wit
h pr
evio
usly
unr
ecog
nise
d ve
rteb
ral
frac
ture
s in
the
cour
se o
f ca
re f
or
othe
r co
nditi
ons.
Thi
s st
anda
rd r
ecog
nize
s th
at v
erte
bral
fra
ctur
e pa
tien
ts a
re d
iffi
cult
to id
entif
y. T
his
stan
dard
is a
spir
atio
nal b
ut s
ince
ver
tebr
al f
ract
ures
are
the
mos
t com
mon
fra
gili
ty
frac
ture
it w
ould
be
rem
iss
to n
ot in
clud
e th
e at
tem
pt to
iden
tify
them
in th
is f
ram
ewor
k.
2144 Osteoporos Int (2013) 24:2135–2152
on s
econ
dary
fra
ctur
e pr
even
tion
.F
ootn
ote:
5.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Ass
essm
ent
Gui
delin
es
The
inst
itut
ion’
s se
cond
ary
frac
ture
pre
vent
ion
asse
ssm
ent,
to d
eter
min
e th
e ne
ed f
or
inte
rven
tion
, is
cons
iste
nt w
ith
loca
l/re
gion
al/n
atio
nal g
uide
line
s.
The
inst
itut
ion’
s as
sess
men
t is
cons
iste
nt w
ith
peer
rev
iew
ed
guid
ance
dev
elop
ed b
y th
e lo
cal
inst
itutio
n de
liver
ing
the
FLS,
or
by a
dapt
atio
n of
inte
rnat
iona
l gu
idel
ines
.
The
inst
itut
ions
’ as
sess
men
t is
con
sist
ent w
ith
regi
onal
or
sta
te g
uide
line
s.
The
inst
itut
ion’
s as
sess
men
t is
cons
iste
nt w
ith
nati
onal
gui
deli
nes.
Gui
danc
e no
tes/
rati
onal
e
The
inte
ntio
n of
this
sta
ndar
d is
two-
fold
. Fir
stly
, th
e st
anda
rd r
equi
res
inst
itut
ions
to a
dher
e to
gu
idan
ce th
at h
as b
een
subj
ect t
o pe
er r
evie
w a
t a
loca
l, re
gion
al o
r na
tion
al le
vel.
Seco
ndly
, the
st
anda
rd h
ighl
ight
s an
impo
rtan
t lea
ders
hip
role
th
at a
n ef
fect
ive
FLS
can
play
in s
uppo
rtin
g co
llea
gues
acr
oss
the
nati
onal
hea
lthca
re s
yste
m.
A w
ell-
esta
blis
hed
FLS
shou
ld p
lay
a le
adin
g ro
le
in lo
bbyi
ng f
or, a
nd d
raft
ing
nati
onal
gui
deli
nes
Alt
houg
h lo
cal o
r ad
apte
d in
tern
atio
nal g
uide
line
use
is
acce
pted
at t
his
leve
l, th
ere
is a
n ex
pect
atio
n th
at o
nce
regi
onal
, st
ate
or n
atio
nal g
uide
line
s ar
e de
velo
ped
the
site
wil
l wor
k to
war
ds m
odif
ying
thei
r se
cond
ary
frac
ture
pre
vent
ion
asse
ssm
ents
.
Alt
houg
h re
gion
al o
r st
ate
guid
elin
e us
e is
acc
epte
d at
th
is le
vel,
ther
e is
an
expe
ctat
ion
that
onc
e na
tion
al g
uide
line
s ar
e de
velo
ped
the
site
wil
l wor
k to
war
ds m
odif
ying
thei
r se
cond
ary
frac
ture
pr
even
tion
ass
essm
ents
.
It i
s re
cogn
ized
that
dif
fere
nt h
ealt
h ca
re in
stitu
tions
/sys
tem
s m
ay b
e lim
ited
to th
e gu
idel
ines
that
are
ava
ilab
le w
ithin
thei
r co
untr
y.
6.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Seco
ndar
y C
ause
s of
O
steo
poro
sis
Inst
itut
ion
can
dem
onst
rate
wha
t pro
port
ion
of
pati
ents
who
req
uire
trea
tmen
t for
pre
vent
ion
of
seco
ndar
y fr
actu
res
unde
rgo
furt
her
inve
stig
atio
n (t
ypic
ally
blo
od te
stin
g) to
ass
ess
for
unde
rlyi
ng
caus
es o
f lo
w B
MD
).
Inst
itut
ion
can
dem
onst
rate
that
50
% o
f pa
tien
ts w
ho n
eed
trea
tmen
t are
rou
tine
ly s
cree
ned
for
seco
ndar
y ca
uses
of
oste
opor
osis
.
Inst
itut
ion
can
dem
onst
rate
th
at 7
0% o
f pa
tien
ts w
ho
need
trea
tmen
t are
rou
tine
ly
scre
ened
for
sec
onda
ry
caus
es o
f os
teop
oros
is.
Inst
itut
ion
can
dem
onst
rate
that
90%
pa
tient
s w
ho n
eed
trea
tmen
t are
ro
utin
ely
scre
ened
for
sec
onda
ry
caus
es o
f os
teop
oros
is v
ia s
ite
prot
ocol
and
ref
erra
l to
spec
iali
sts,
if
indi
cate
d, h
as b
een
arra
nged
.
Gui
danc
e no
tes/
rati
onal
e
It is
Im
port
ant t
o re
cogn
ize
why
pat
ient
s ha
ve
oste
opor
osis
. Ass
essm
ent s
houl
d fo
llow
an
algo
rith
m th
at s
cree
ns f
or s
econ
dary
cau
ses.
For
clar
ity,
in h
ealt
hcar
e sy
stem
s w
here
the
prim
ary
care
phy
sici
an
serv
es a
s th
e ‘g
ate
keep
er’
for
refe
rral
s to
spe
cial
ists
, the
FL
S is
re
quir
ed to
hav
e a
robu
st a
gree
men
t w
ith
loca
l pri
mar
y ca
re p
hysi
cian
s to
en
sure
that
onw
ard
refe
rral
occ
urs.
Foo
tnot
e: I
t is
reco
gniz
ed th
at th
ere
wil
l be
vary
ing
met
hods
use
d to
iden
tify
sec
onda
ry c
ause
s of
ost
eopo
rosi
s. T
he p
hilo
soph
y of
this
sta
ndar
d is
that
pos
t-fr
actu
re p
atie
nts
who
ar
e in
nee
d of
trea
tmen
t are
ass
esse
d to
iden
tify
seco
ndar
y ca
uses
of
oste
opor
osis
in a
ccor
danc
e w
ith
the
inst
ituti
on o
r he
alth
car
e sy
stem
’s e
xist
ing
met
hods
.
Osteoporos Int (2013) 24:2135–2152 2145
and
whe
ther
pat
ient
s ca
n be
ref
erre
d to
it.
Foo
tnot
e:
7.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Fal
ls P
reve
ntio
n Se
rvic
es
Pati
ents
pre
sent
ing
wit
h a
frag
ility
fra
ctur
e, a
nd
who
are
per
ceiv
ed to
be
at r
isk
of f
urth
er f
alls
, ar
e ev
alua
ted
to d
eter
min
e w
heth
er o
r no
t fal
ls
prev
enti
on in
terv
enti
on s
ervi
ces
are
need
ed, a
nd
if s
o ar
e su
bseq
uent
ly r
efer
red
to a
n es
tabl
ishe
d fa
lls
prev
entio
n se
rvic
e.
50%
of
pati
ents
pre
sent
ing
wit
h fr
actu
res
who
are
per
ceiv
ed to
be
at r
isk
of f
urth
er f
alls
are
ev
alua
ted
to d
eter
min
e w
heth
erfa
lls
prev
enti
on s
ervi
ces
are
need
ed.
70%
of
pati
ents
pre
sent
ing
wit
h fr
actu
res
who
are
pe
rcei
ved
to b
e at
ris
k of
fu
rthe
r fa
lls a
re e
valu
ated
to
dete
rmin
e w
heth
er f
alls
pr
even
tion
ser
vice
s ar
e ne
eded
.
90%
of
patie
nts
pres
enti
ng w
ith
frac
ture
s w
ho a
re p
erce
ived
to b
e at
ri
sk a
re e
valu
ated
to d
eter
min
e w
heth
er f
alls
pre
vent
ion
serv
ices
are
ne
eded
, and
app
ropr
iate
pat
ient
s ar
e re
ferr
ed to
an
esta
blis
hed
falls
pr
even
tion
ser
vice
that
del
iver
s ev
iden
ce-b
ased
inte
rven
tion
s.
Gui
danc
e no
tes/
rati
onal
e
The
gra
ding
of
this
sta
ndar
d w
ill b
e ba
sed
on
whe
ther
fal
ls p
reve
ntio
n se
rvic
es a
re a
vail
able
. T
he b
asic
sta
ndar
d w
ill b
e th
at a
n as
sess
men
t wil
l be
don
e to
det
erm
ine
whe
ther
a p
atie
nt n
eeds
fa
lls
prev
entio
n se
rvic
es. T
he s
tand
ard
rati
ng w
illbe
rai
sed
if f
alls
pre
vent
ion
serv
ices
are
ava
ilab
le
All
pat
ient
s ar
e ev
alua
ted
for
fall
s ri
sk u
sing
a b
asic
fal
ls r
isk
eval
uati
on q
uest
ionn
aire
.
Fall
s pr
even
tion
serv
ice
shou
ld
deli
ver
evid
ence
d- b
ased
pro
gram
s.
Thi
s st
anda
rd d
eter
min
es w
heth
er o
r no
t a f
alls
pre
vent
ion
serv
ice
is a
vail
able
, and
if s
o ho
w it
is b
eing
uti
lized
. If
ther
e is
not
an
esta
blis
hed
falls
ser
vice
in th
e lo
cali
ty,
this
sta
ndar
d be
com
es a
spir
atio
nal a
nd e
ncou
rage
s th
e le
ader
ship
of
the
FLS
to lo
bby
the
inst
itut
ion/
syst
em to
mak
e a
fall
s se
rvic
e av
aila
ble.
8.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Mul
tifa
cete
d he
alth
an
d lif
esty
le r
isk-
fact
or
Ass
essm
ent
Pati
ents
pre
sent
ing
wit
h fr
agil
ity
frac
ture
s un
derg
o a
mul
tifa
cete
d ri
sk-f
acto
r as
sess
men
t as
a pr
even
tati
ve m
easu
re to
iden
tify
any
heal
th
and/
or li
fest
yle
chan
ges
that
, if
impl
emen
ted,
wil
lre
duce
fut
ure
frac
ture
ris
k, a
nd th
ose
pati
ents
in
need
are
sub
sequ
entl
y re
ferr
ed to
the
appr
opri
ate
mul
tidis
cipl
inar
y pr
acti
tion
er f
or f
urth
er
eval
uati
on a
nd tr
eatm
ent.
50%
of
inpa
tien
ts u
nder
go
mul
tifac
eted
ris
k-fa
ctor
as
sess
men
ts.
70%
of
inpa
tien
ts u
nder
go
mul
tifac
eted
ris
k-fa
ctor
as
sess
men
ts.
90%
of
inpa
tien
ts u
nder
go
mul
tifac
eted
ris
k-fa
ctor
as
sess
men
ts.
Gui
danc
e no
tes/
rati
onal
e
Goi
ng b
eyon
d tr
eatm
ent b
y m
edic
atio
n, it
is
impo
rtan
t to
iden
tify
othe
r ne
eds
for
inte
rven
tion
th
at w
ill r
educ
e fu
ture
fra
ctur
e ri
sk, i
nclu
ding
as
sess
ing
for
any
unde
rlyi
ng h
ealt
h or
life
styl
e ri
sk-f
acto
rs th
at m
ay c
ontr
ibut
e to
fut
ure
frac
ture
s. I
dent
ifyi
ng r
isk-
fact
ors
such
as
smok
ing,
alc
ohol
use
, poo
r nu
triti
on, l
ack
of
exer
cise
, poo
r co
ordi
nati
on, p
oor
bala
nce,
etc
. an
d re
ferr
ing
the
pati
ent t
o th
e ap
prop
riat
e he
alth
care
pro
vide
r fo
r in
terv
enti
on w
ill h
elp
to
prev
ent f
utur
e fr
actu
res.
F
ootn
ote:
A m
ultif
acet
ed r
isk
asse
ssm
ent c
an b
e do
ne b
y on
e he
alth
care
pro
vide
r w
ithi
n th
e FL
S (c
lini
cian
, nur
se, F
LS
coor
dina
tor
etc.
), a
nd n
eede
d in
terv
entio
n se
rvic
es c
an b
e re
ferr
ed to
the
appr
opri
ate
heal
thca
re p
rovi
der
for
furt
her
eval
uati
on a
nd tr
eatm
ent.
For
exa
mpl
e, a
ver
y el
derl
y pa
tien
t pre
sent
ing
wit
h a
frag
ilit
y fr
actu
re u
nder
goes
a
mul
tifac
eted
ris
k-fa
ctor
ass
essm
ent a
nd is
iden
tifi
ed to
hav
e ve
ry p
oor
coor
dina
tion
and
bala
nce.
Ide
ntif
ying
this
, the
FL
S re
fers
the
pati
ent t
o be
fitt
ed f
or h
ip p
rote
ctor
s as
a
prev
enta
tive
mea
sure
for
hip
fra
ctur
e fr
om a
fal
l.
It is
rec
ogni
zed
that
ther
e w
ill b
e va
ryin
g m
etho
ds u
sed
to id
entif
y m
ultif
acet
ed r
isk-
fact
ors
for
futu
re f
ract
ures
. T
he p
hilo
soph
y of
this
sta
ndar
d is
that
pos
t-fr
actu
re p
atie
nts
who
ar
e in
nee
d of
trea
tmen
t are
ass
esse
d to
iden
tify
”lif
esty
le”
risk
-fac
tors
in a
ccor
danc
e w
ith
the
inst
itutio
n or
hea
lth
care
sys
tem
’s e
xist
ing
met
hods
.
2146 Osteoporos Int (2013) 24:2135–2152
Foo
tnot
e:
9.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Med
icat
ion
Init
iati
on
All
fra
ctur
e pa
tien
ts o
ver
50yr
, not
on
trea
tmen
t at
the
tim
e of
fra
ctur
e pr
esen
tati
on, a
re in
itiat
edor
are
ref
erre
d to
thei
r pr
imar
y ca
re
phys
icia
n/pr
ovid
er f
or in
itiat
ion,
whe
re r
equi
red,
on
ost
eopo
rosi
s tr
eatm
ent i
n ac
cord
ance
wit
h ev
iden
ce-b
ased
loca
l/re
gion
al/n
atio
nal
guid
elin
es.
50%
of
frac
ture
pat
ient
s, w
ho a
re
elig
ible
for
trea
tmen
t acc
ordi
ng
to th
e ev
iden
ce-b
ased
lo
cal/
natio
nal/r
egio
nal g
uide
line
, ar
e in
itiat
ed o
n os
teop
oros
is
med
icin
es.
70%
of
frac
ture
pat
ient
s,
who
are
eli
gibl
e fo
r tr
eatm
ent a
ccor
ding
to th
e ev
iden
ce-b
ased
lo
cal/
nati
onal
/reg
iona
l gu
idel
ine,
are
init
iate
d on
os
teop
oros
is m
edic
ines
.
90%
of
frac
ture
pat
ient
s, w
ho th
at
are
elig
ible
for
trea
tmen
t acc
ordi
ng
to th
e ev
iden
ce-b
ased
lo
cal/n
atio
nal/r
egio
nal g
uide
line
, ar
e in
itia
ted
on o
steo
poro
sis
med
icin
es.
Gui
danc
e no
tes/
rati
onal
e
The
sta
ndar
d is
not
a g
ener
al m
easu
rem
ent o
f pe
r ce
nt o
f pa
tien
ts tr
eate
d, b
ut r
athe
r a
mea
sure
men
t of
the
per
cent
of
pati
ents
wit
hin
the
appl
icab
le
guid
elin
e w
ho a
re tr
eate
d.
The
sta
ndar
d is
co
gnis
ant t
hat n
ot a
ll fr
actu
re p
atie
nts
over
50
year
s of
age
will
req
uire
trea
tmen
t.
Thi
s fr
amew
ork
reco
gniz
es v
aria
tion
s in
the
unde
rlyi
ng h
ealt
h ca
re s
yste
m.
Dep
ende
nt o
n th
e na
ture
of
the
heal
th c
are
syst
em, t
he s
peci
alis
t may
be
able
initi
ate
trea
tmen
t or,
whe
n th
e pr
imar
y ca
re p
hysi
cian
/pro
vide
r is
the
’gat
ekee
per’
, the
spe
cial
ist c
an r
efer
the
pati
ent t
o th
e pr
imar
y ca
re p
hysi
cian
/pro
vide
r fo
r in
itiat
ion
of tr
eatm
ent.
In
eith
er c
ase,
evi
denc
e is
sou
ght t
hat t
his
proc
ess
is a
s ro
bust
as
poss
ible
.
10.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Med
icat
ion
Rev
iew
For
pati
ents
alr
eady
rec
eivi
ng o
steo
poro
sis
med
icat
ions
whe
n th
ey p
rese
nt w
ith
a fr
actu
re,
reas
sess
men
t is
offe
red
whi
ch in
clud
es r
evie
w o
f m
edic
atio
n co
mpl
ianc
e, c
onsi
dera
tion
of
alte
rnat
ive
oste
opor
osis
med
icat
ions
and
op
tim
isat
ion
of n
on-p
harm
acol
ogic
al
inte
rven
tion
s.
Inst
itut
ion
dem
onst
rate
s th
at it
re
view
s th
e m
edic
atio
ns o
f 50
% o
f pa
tien
ts c
aptu
red
abov
e (b
y th
e FL
S), w
ho a
re o
n tr
eatm
ent a
t tim
e of
fra
ctur
e an
d pe
rfor
ms
a re
view
of
med
icat
ion
com
plia
nce
and/
or c
onsi
dera
tion
of
alte
rnat
ive
inte
rven
tion
s.
Inst
itut
ion
dem
onst
rate
s th
at
it r
evie
ws
the
med
icat
ions
of
70%
of
pati
ents
cap
ture
d ab
ove
(by
the
FLS)
, who
are
on
trea
tmen
t at t
ime
of
frac
ture
and
per
form
s a
revi
ew o
f m
edic
atio
n co
mpl
ianc
e an
d/or
co
nsid
erat
ion
of a
ltern
ativ
e in
terv
enti
ons.
Inst
itut
ion
dem
onst
rate
s th
at it
re
view
s th
e m
edic
atio
ns o
f 9
0% o
f pa
tient
s ca
ptur
ed a
bove
(by
the
FLS)
, who
are
on
trea
tmen
t at t
ime
of f
ract
ure
and
perf
orm
s a
revi
ew o
f m
edic
atio
n co
mpl
ianc
e an
d/or
co
nsid
erat
ion
of a
lter
nativ
e in
terv
enti
ons.
Gui
danc
e no
tes/
rati
onal
e
The
inte
ntio
n of
this
sta
ndar
d is
to a
sses
s w
heth
erth
e FL
S re
view
s pa
tien
ts th
at h
ave
frac
ture
d w
hils
t, se
emin
gly,
rec
eivi
ng tr
eatm
ent f
or
oste
opor
osis
, and
wha
t pro
port
ion
of th
is s
ub-
grou
p of
pat
ient
s un
derg
o th
orou
gh r
evie
w.
Osteoporos Int (2013) 24:2135–2152 2147
Foo
tnot
e:
11.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Com
mun
icat
ion
Stra
tegy
Inst
itut
ion’
s FL
S m
anag
emen
t pla
n is
co
mm
unic
ated
to p
rim
ary
and
seco
ndar
y ca
re
clin
icia
ns a
nd c
onta
ins
info
rmat
ion
requ
ired
by
and
appr
oved
by
loca
l sta
keho
lder
s.
Inst
itut
ion’
s FL
S m
anag
emen
t pl
an is
com
mun
icat
ed to
pri
mar
y an
d se
cond
ary
care
phy
sici
ans.
Inst
itut
ion
dem
onst
rate
s th
at
the
FLS
man
agem
ent p
lan
is
com
mun
icat
ed to
pri
mar
y an
d se
cond
ary
care
cl
inic
ians
and
con
tain
s at
le
ast 5
0% o
f cr
iteri
a lis
ted.
*
Inst
itut
ion
dem
onst
rate
s th
at th
e FL
S m
anag
emen
t pla
n is
co
mm
unic
ated
to p
rim
ary
and
seco
ndar
y ca
re c
lini
cian
s an
d co
ntai
ns a
t lea
st 9
0% o
f cr
iteri
a li
sted
.*
Gui
danc
e no
tes/
rati
onal
e
The
inte
ntio
n of
this
sta
ndar
d is
to u
nder
stan
d to
w
hat e
xten
t the
FL
S m
anag
emen
t pla
n -
and
com
mun
icat
ion
of it
to r
elev
ant c
lini
cal
coll
eagu
es in
pri
mar
y an
d se
cond
ary
care
– h
as
soug
ht th
ose
coll
eagu
es’
opin
ions
on
how
bes
t to
suit
thei
r ne
eds
to e
nsur
e op
tim
um a
dher
ence
w
ith
reco
mm
enda
tion
s fr
om th
e FL
S.
Thi
s st
anda
rd p
erta
ins
mai
nly
to s
itua
tions
whe
n pa
tien
ts p
rese
nt to
an
inpa
tien
t or
outp
atie
nt f
acili
ty f
or a
non
-ort
hopa
edic
rel
ated
rea
son,
and
whi
lst t
here
, it i
s op
port
unis
tica
lly
disc
over
ed th
at a
fra
ctur
e ex
ists
(i.e
. che
st x
-ray
for
pne
umon
ia d
isco
vers
a v
erte
bral
fra
ctur
e).
In th
is c
ase
a po
st-f
ract
ure
man
agem
ent p
lan
is p
ut in
to p
lace
and
co
mm
unic
ated
to th
e pa
tien
t as
wel
l as
to a
ll h
ealt h
car
e pr
ovid
ers
and
paye
rs (
if r
efer
ral r
equi
red)
invo
lved
wit
h th
e pa
tien
t’s
care
. *T
he c
rite
ria
men
tone
d in
Lev
el 2
and
Lev
el 3
incl
udes
:
•Fr
actu
re r
isk
scor
e •
DX
A –
BM
D
•D
XA
– v
erte
bral
fra
ctur
e as
sess
men
t or
spin
e X
ray
resu
lt if
don
e in
stea
d •
Prim
ary
oste
opor
osis
ris
k fa
ctor
s
•Se
cond
ary
caus
es o
f os
teop
oros
is (
if a
ppli
cabl
e)
•Fr
actu
re/f
all r
isk
fact
ors
•C
urre
nt d
rug
trea
tmen
t (if
app
lica
ble)
•
Med
icat
ion
com
plia
nce
revi
ew
•Fo
llow
-up
plan
•
Lif
esty
le r
isk-
fact
or a
sses
smen
t •
Tim
e si
nce
last
fra
ctur
e
2148 Osteoporos Int (2013) 24:2135–2152
Foo
tnot
e:
12.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Lon
g-te
rm
Man
agem
ent
Inst
itut
ion
has
a pr
otoc
ol in
pla
ce f
or lo
ng-t
erm
fo
llow
up
of e
vide
nce-
base
d in
itial
inte
rven
tion
s an
d a
long
term
adh
eren
ce p
lan.
Tre
atm
ent r
ecom
men
datio
ns, f
or
pati
ents
req
uiri
ng d
rug
trea
tmen
ts, i
nclu
de a
long
-ter
m
follo
w-u
p pl
an th
at o
ccur
s >1
2 m
onth
s af
ter
frac
ture
adv
isin
g w
hen
the
pati
ent s
houl
d un
derg
o fu
ture
rea
sses
smen
t of
frac
ture
ri
sk a
nd o
f ne
ed f
or tr
eatm
ent.
Tre
atm
ent r
ecom
men
dati
ons,
for
pa
tien
ts r
equi
ring
dru
g tr
eatm
ents
, in
clud
e bo
th a
sho
rt-t
erm
fol
low
-up
plan
<12
mon
ths
aft
er f
ract
ure,
A
ND
a lo
ng-t
erm
fol
low
-up
plan
>
12 a
fter
fra
ctur
e, a
dvis
ing
whe
n th
e pa
tien
t sho
uld
unde
rgo
futu
re
reas
sess
men
t of
frac
ture
ris
k, th
e ne
ed f
or tr
eatm
ent a
nd c
lear
gu
idan
ce o
n w
hen
and
wit
h w
hom
lie
s re
spon
sibi
lity
for
mon
itori
ng
adhe
renc
e to
trea
tmen
t.
Gui
danc
e no
tes/
rati
onal
e
The
inte
ntio
n of
this
sta
ndar
d is
to a
scer
tain
wha
tpr
oces
ses
are
in p
lace
to e
nsur
e th
at lo
ng-t
erm
m
anag
emen
t of
frac
ture
ris
k is
rel
iabl
y pr
ovid
ed.
In h
ealt
hcar
e sy
stem
s w
ith
esta
blis
hed
prim
ary
care
infr
astr
uctu
re, l
ocal
pri
mar
y ca
re m
ust b
e in
volv
ed in
dev
elop
ing
the
proc
esse
s th
at th
ey
wil
l im
plem
ent f
or th
is a
spec
t of
post
-fra
ctur
e ca
re. I
n he
alth
care
sys
tem
s th
at la
ck p
rim
ary
care
in
fras
truc
ture
, the
FL
S m
ust e
stab
lish
eff
ecti
ve
feed
back
pro
cess
es d
irec
tly
from
the
pati
ent o
r ca
rer
and
devi
se s
trat
egie
s to
ens
ure
foll
ow-u
p by
th
e FL
S.
Inst
itut
ion
can
dem
onst
rate
the
prop
ortio
n of
pat
ient
s or
igin
ally
as
sess
ed b
y th
e FL
S ha
ve a
long
-te
rm f
ollo
w-u
p pl
an in
pla
ce th
at
has
been
sub
ject
at y
ears
1 &
2
and
beyo
nd.
Inst
itut
ion
can
dem
onst
rate
the
prop
ortio
n of
pat
ient
s or
igin
ally
as
sess
ed b
y th
e FL
S ha
ve a
sho
rt-
term
fol
low
-up
plan
with
in 6
-12
mon
ths,
as
wel
l as
a lo
ng te
rm
man
agem
ent p
lan
in p
lace
that
has
be
en s
ubje
ct a
t yea
rs 1
& 2
and
be
yond
.
A k
ey r
espo
nsib
ility
of
an F
LS
of c
are
is to
hav
e a
prot
ocol
in p
lace
to e
nsur
e lo
ng-t
erm
fol
low
-up
will
take
pla
ce, a
nd c
lear
gui
danc
e on
whe
n an
d w
ith
who
m li
es th
e re
spon
sibi
lity
for
mon
itor
ing
adhe
renc
e to
trea
tmen
t whe
ther
it b
e by
the
FLS,
ref
erre
d to
the
prim
ary
care
phy
sici
an/p
rovi
der,
or
by a
noth
er m
eans
that
sui
ts th
e un
derl
ying
hea
lth
care
sys
tem
.
Foo
tnot
e:13.
STA
ND
AR
D
LE
VE
L1
LE
VE
L2
LE
VE
L3
Dat
abas
e
All
iden
tifie
d fr
agil
ity
frac
ture
pat
ient
s ar
e re
cord
ed in
a d
atab
ase
whi
ch f
eeds
into
cen
tral
na
tiona
l dat
abas
e.
Frag
ility
fra
ctur
e pa
tient
rec
ords
(f
or p
atie
nts
capt
ured
abo
ve)
are
reco
rded
in a
loca
l dat
abas
e.
Site
dem
onst
rate
s th
at a
ll
frag
ility
fra
ctur
e pa
tien
t re
cord
s id
enti
fied
abo
ve a
re
reco
rded
in a
dat
abas
e th
at
can
be s
hare
d re
gion
ally
for
da
ta c
ompa
riso
n.
Site
dem
onst
rate
s th
at a
ll f
ragi
lity
frac
ture
pat
ient
rec
ords
iden
tifie
d ab
ove
are
stor
ed in
a c
entr
al,
natio
nal d
atab
ase.
The
dat
abas
e ca
n pr
ovid
e be
nchm
arki
ng a
gain
st a
ll
prov
ider
uni
ts.
Gui
danc
e no
tes/
rati
onal
e
The
inte
ntio
n of
this
sta
ndar
d is
to h
ighl
ight
the
impo
rtan
ce o
f ha
ving
an
effe
ctiv
e da
taba
se to
un
derp
in th
e se
rvic
e. T
he s
tand
ard
also
em
phas
is
the
aspi
ratio
nal o
bjec
tive
of
deve
lopi
ng lo
cal,
regi
onal
and
nat
iona
l dat
abas
es th
at w
ould
ena
ble
benc
hmar
king
of
care
aga
inst
the
othe
r FL
S pr
ovid
er u
nits
thro
ugho
ut th
e co
untr
y.
A lo
cal d
atab
ase
for
reco
rdin
g fr
agil
ity f
ract
ure
pati
ent r
ecor
ds, L
evel
1, i
s es
sent
ial t
o an
FL
S. A
nat
iona
l dat
abas
e is
asp
irat
iona
l and
is im
port
ant t
o st
rive
tow
ard,
an
d th
eref
ore
is s
et a
t Lev
el 3
.
Osteoporos Int (2013) 24:2135–2152 2149
References
1. International Osteoporosis Foundation (2012) Capture theFracture: a global campaign to break the fragility fracturecycle. http://www.worldosteoporosisday.org/ Accessed 17Dec 2012
2. International Osteoporosis Foundation (2012) Capture theFracture: break the worldwide fragility fracture cycle.http://www.osteofound.org/capture-fracture Accessed 1 Nov2012
3. McLellan AR, Gallacher SJ, Fraser M, McQuillian C (2003) Thefracture liaison service: success of a program for the evaluationand management of patients with osteoporotic fracture.Osteoporos Int 14:1028–1034
4. Wright SA, McNally C, Beringer T, Marsh D, Finch MB (2005)Osteoporosis fracture liaison experience: the Belfast experience.Rheumatol Int 25:489–490
5. Clunie G, Stephenson S (2008) Implementing and running afracture liaison service: an integrated clinical service providinga comprehensive bone health assessment at the point of fracturemanagement. J Orthop Nurs 12:156–162
6. Premaor MO, Pilbrow L, Tonkin C, Adams M, Parker RA,Compston J (2010) Low rates of treatment in postmenopausalwomen with a history of low trauma fractures: results of audit in aFracture Liaison Service. QJM 103:33–40
7. Wallace I, Callachand F, Elliott J, Gardiner P (2011) An evalua-tion of an enhanced fracture liaison service as the optimal modelfor secondary prevention of osteoporosis. JRSM Short Rep 2:8
8. Boudou L, Gerbay B, Chopin F, Ollagnier E, Collet P, Thomas T(2011) Management of osteoporosis in fracture liaison serviceassociated with long-term adherence to treatment. Osteoporos Int22:2099–2106
9. Huntjens KM, van Geel TA, Blonk MC, Hegeman JH, van derElst M, Willems P et al (2011) Implementation of osteoporosisguidelines: a survey of five large fracture liaison services in theNetherlands. Osteoporos Int 22:2129–2135
11. Inderjeeth CA, Glennon DA, Poland KE, Ingram KV, Prince RL,Van VR et al (2010) A multimodal intervention to improvefragility fracture management in patients presenting to emergencydepartments. Med J Aust 193:149–153
12. Lih A, Nandapalan H, Kim M, Yap C, Lee P, Ganda K et al(2011) Targeted intervention reduces refracture rates in patientswith incident non-vertebral osteoporotic fractures: a 4-year pro-spective controlled study. Osteoporos Int 22:849–858
13. Bogoch ER, Elliot-Gibson V, Beaton DE, Jamal SA, Josse RG,Murray TM (2006) Effective initiation of osteoporosis diagnosisand treatment for patients with a fragility fracture in an orthopae-dic environment. J Bone Joint Surg Am 88:25–34
14. Sander B, Elliot-Gibson V, Beaton DE, Bogoch ER, Maetzel A(2008) A coordinator program in post-fracture osteoporosis man-agement improves outcomes and saves costs. J Bone Joint SurgAm 90:1197–1205
15. Dell R, Greene D, Schelkun SR, Williams K (2008) Osteoporosisdisease management: the role of the orthopaedic surgeon. J BoneJoint Surg Am 90(Suppl 4):188–194
16. Greene D, Dell RM (2010) Outcomes of an osteoporosis disease-management program managed by nurse practitioners. J AmAcad Nurse Pract 22:326–329
17. The Bone and Joint Decade (2012) Global Alliance forMusculoskeletal Health. http://bjdonline.org/ Accessed 14 Nov 2012
18. National Institute for Health and Clinical Excellence (2008)Alendronate (review), etidronate (review), risedronate (review),raloxifene (review) strontium ranelate and teriparatide (review)for the secondary prevention of osteoporotic fragility fractures inpostmenopausal women. Technology Appraisal 161. NICE,London
19. National Institute for Health and Clinical Excellence (2010)Denosumab for the prevention of osteoporotic fractures inpostmenopausal women. NICE Technology AppraisalGuidance 204. NICE, London
20. National Institute for Health and Clinical Excellence (2012)Osteoporosis: assessing the risk of fragility fracture. NICEClinical Guideline 146. NICE, London
21. British Geriatrics Society (2010) Best practice tariff for hip frac-ture—making ends meet http://www.bgs.org.uk/index.php?option=com_content&view=article&id=700:tariffhipfracture&catid=47:fallsandbones&Itemid=307 Accessed 14 Nov 2012
22. Brown P, Carr W, Mitchell P (2012) Osteoporosis is a new domainin the GMS contract for 2012/13. http://www.eguidelines.co.uk/eguidelinesmain/gip/vol_15/apr_12/brown_osteoporosis_apr12.php Accessed 14 Nov 2012
23. Strom O, Borgstrom F, Kanis JA, Compston J, Cooper C,McCloskey EV et al (2011) Osteoporosis: burden, health careprovision and opportunities in the EU: a report prepared incollaboration with the International Osteoporosis Foundation(IOF) and the European Federation of Pharmaceutical IndustryAssociations (EFPIA). Arch Osteoporos 6:59–155
24. Australian Government (2006) PBS extended listing of alendro-nate for treating osteoporosis and Medicare extended listing forbone mineral density testing. In Department of Health andAgeing (ed). Canberra
25. PHARMAC (2012) In: Wilson K, Bloor R, Jennings D (eds)Pharmaceutical schedule. Pharmaceutical Management Agency,Wellington
26. National Healthcare Group (2012) OPTIMAL (OsteoporosisPatient Targeted and Integrated Management for Active Living)Programme. https://www.cdm.nhg.com.sg/Programmes/OsteoporosisOPTIMAL/tabid/108/language/en-GB/Default.aspxAccessed 11 May 2012
27. van Staa TP, Dennison EM, Leufkens HG, Cooper C (2001)Epidemiology of fractures in England andWales. Bone 29:517–522
28. U.S. Department of Health and Human Services (2004) Bonehealth and osteoporosis: a report of the Surgeon General. U.S.Department of Health and Human Services, Office of the SurgeonGeneral, Rockville, MD
29. Kanis JA, McCloskey EV, Johansson H, Cooper C, Rizzoli R,Reginster JY, on behalf of the Scientific Advisory Board of theEuropean Society for Clinical and Economic Aspects ofOsteoporosis and Osteoarthritis (ESCEO) and the Committee ofScientific Advisors of the International Osteoporosis Foundation(IOF) (2013) European guidance for the diagnosis and manage-ment of osteoporosis in postmenopausal women. Osteoporos Int24:23–57
30. Johnell O, Kanis JA (2006) An estimate of the worldwide prev-alence and disability associated with osteoporotic fractures.Osteoporos Int 17:1726–1733
31. Wade SW, Strader C, Fitzpatrick LA, Anthony MS (2012) Sex-and age-specific incidence of non-traumatic fractures in selectedindustrialized countries. Arch Osteoporos 1–2:219–227
32. Lesnyak O, Ershova O, Belova K, et al. (2012) Epidemiology offracture in the Russian Federation and the development of aFRAX model. Arch Osteoporos 1–2:67–73
33. Xia WB, He SL, Xu L, Liu AM, Jiang Y, Li M et al (2012)Rapidly increasing rates of hip fracture in Beijing, China. J BoneMiner Res 27:125–129
34. Kanis JA, Johnell O (2005) Requirements for DXA for the man-agement of osteoporosis in Europe. Osteoporos Int 16:229–238
35. Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C,Stenmark J, McCloskey EV, Jönsson B, Kanis JA (2013)Osteoporosis in the European Union: medical management, epi-demiology and economic burden. A report prepared in collabo-ration with the International Osteoporosis Foundation (IOF) andthe European Federation of Pharmaceutical Industry Associations(EFPIA). Arch Osteoporos. doi:10.1007/s11657-013-0136-1
37. International Osteoporosis Foundation (2009) The Asian Audit: epi-demiology, costs and burden of osteoporosis in Asia 2009. IOF, Nyon
38. Klotzbuecher CM, Ross PD, Landsman PB, Abbott TA 3rd,Berger M (2000) Patients with prior fractures have an increasedrisk of future fractures: a summary of the literature and statisticalsynthesis. J Bone Miner Res 15:721–739
39. Kanis JA, Johnell O, De Laet C et al (2004) A meta-analysis ofprevious fracture and subsequent fracture risk. Bone 35:375–382
40. Gallagher JC, Melton LJ, Riggs BL, Bergstrath E (1980)Epidemiology of fractures of the proximal femur in Rochester,Minnesota. Clin Orthop Relat Res 163–171
41. Port L, Center J, Briffa NK, Nguyen T, Cumming R, Eisman J(2003) Osteoporotic fracture: missed opportunity for interven-tion. Osteoporos Int 14:780–784
42. McLellan A, Reid D, Forbes K, Reid R, Campbell C, Gregori A,Raby N, Simpson A (2004) Effectiveness of strategies for thesecondary prevention of osteoporotic fractures in Scotland (CEPS99/03). NHS Quality Improvement Scotland, Glasgow
43. Edwards BJ, Bunta AD, Simonelli C, Bolander M, Fitzpatrick LA(2007) Prior fractures are common in patients with subsequenthip fractures. Clin Orthop Relat Res 461:226–230
44. Black DM, Cummings SR, Karpf DB et al (1996) Randomisedtrial of effect of alendronate on risk of fracture in women withexisting vertebral fractures. Fracture Intervention Trial ResearchGroup. Lancet 348:1535–1541
45. McClung MR, Geusens P, Miller PD et al (2001) Effect ofrisedronate on the risk of hip fracture in elderly women. HipIntervention Program Study Group. N Engl J Med 344:333–340
46. Reginster JY, Seeman E, De Vernejoul MC et al (2005) Strontiumranelate reduces the risk of nonvertebral fractures in postmenopaus-al women with osteoporosis: treatment of Peripheral Osteoporosis(TROPOS) study. J Clin Endocrinol Metab 90:2816–2822
47. Rizzoli R, Greenspan SL, Bone G 3rd et al (2002) Two-yearresults of once-weekly administration of alendronate 70 mg forthe treatment of postmenopausal osteoporosis. J Bone Miner Res17:1988–1996
48. Harris ST, Watts NB, Li Z, Chines AA, Hanley DA, Brown JP(2004) Two-year efficacy and tolerability of risedronate once aweek for the treatment of women with postmenopausal osteopo-rosis. Curr Med Res Opin 20:757–764
49. Reginster JY, Adami S, Lakatos P et al (2006) Efficacy andtolerability of once-monthly oral ibandronate in postmenopausalosteoporosis: 2 year results from the MOBILE study. Ann RheumDis 65:654–661
50. McClung MR, Zanchetta JR, Racewicz A, et al. (2012) Efficacyand safety of risedronate 150-mg once a month in the treatment ofpostmenopausal osteoporosis: 2-year data. Osteoporos Int24:293–299
51. Neer RM, Arnaud CD, Zanchetta JR et al (2001) Effect ofparathyroid hormone (1–34) on fractures and bone mineral den-sity in postmenopausal women with osteoporosis. N Engl J Med344:1434–1441
52. Greenspan SL, Bone HG, Ettinger MP et al (2007) Effect ofrecombinant human parathyroid hormone (1–84) on vertebral
fracture and bone mineral density in postmenopausal women withosteoporosis: a randomized trial. Ann Intern Med 146:326–339
53. Eisman JA, Civitelli R, Adami S et al (2008) Efficacy andtolerability of intravenous ibandronate injections in postmeno-pausal osteoporosis: 2-year results from the DIVA study. JRheumatol 35:488–497
54. Cummings SR, San Martin J, McClung MR et al (2009)Denosumab for prevention of fractures in postmenopausal wom-en with osteoporosis. N Engl J Med 361:756–765
55. Black DM, Delmas PD, Eastell R et al (2007) Once-yearlyzoledronic acid for treatment of postmenopausal osteoporosis.N Engl J Med 356:1809–1822
56. Department of Health (2010) Herald Fractures: clinical burden ofdisease and financial impact. Department of Health, London
57. Teede HJ, Jayasuriya IA, Gilfillan CP (2007) Fracture preventionstrategies in patients presenting to Australian hospitals withminimal-trauma fractures: a major treatment gap. Intern Med J37:674–679
58. Papaioannou A, Kennedy CC, Ioannidis G et al (2008) Theosteoporosis care gap in men with fragility fractures: theCanadian Multicentre Osteoporosis Study. Osteoporos Int19:581–587
59. Smektala R, Endres HG, Dasch B, Bonnaire F, Trampisch HJ,Pientka L (2009) Quality of care after distal radius fracture inGermany. Results of a fracture register of 1,201 elderly patients.Der Unfallchirurg 112:46–54
60. Carnevale V, Nieddu L, Romagnoli E, Bona E, Piemonte S,Scillitani A et al (2006) Osteoporosis intervention in ambulatorypatients with previous hip fracture: a multicentric, nationwideItalian survey. Osteoporos Int 17:478–483
61. Hagino H, Sawaguchi T, Endo N, Ito Y, Nakano T, Watanabe Y(2012) The risk of a second hip fracture in patients after their firsthip fracture. Calcif Tissue Int 90:14–21
62. Gong HS, Oh WS, Chung MS, Oh JH, Lee YH, Baek GH (2009)Patients with wrist fractures are less likely to be evaluated andmanaged for osteoporosis. J Bone Joint Surg Am 91:2376–2380
63. Panneman MJ, Lips P, Sen SS, Herings RM (2004)Undertreatment with anti-osteoporotic drugs after hospitalizationfor fracture. Osteoporos Int 15:120–124
64. Suhm N, Lamy O, Lippuner K, OsteoCare study group (2008)Management of fragility fractures in Switzerland: results of anationwide survey. Swiss Med Wkly 138:674–683
65. Royal College of Physicians’ Clinical Effectiveness andEvaluation Unit (2011) Falling standards, broken promises: re-port of the national audit of falls and bone health in older people2010. Royal College of Physicians, London
66. Jennings LA, Auerbach AD, Maselli J, Pekow PS, LindenauerPK, Lee SJ (2010) Missed opportunities for osteoporosis treat-ment in patients hospitalized for hip fracture. J Am Geriatr Soc58:650–657
67. Greenspan SL, Wyman A, Hooven FH et al (2012) Predictors oftreatment with osteoporosis medications after recent fragilityfractures in a multinational cohort of postmenopausal women. JAm Geriatr Soc 60:455–461
68. Leslie WD, Giangregorio LM, Yogendran M, Azimaee M, MorinS, Metge C et al (2012) A population-based analysis of the post-fracture care gap 1996–2008: the situation is not improving.Osteoporos Int 23:1623–1629
69. Elliot-Gibson V, Bogoch ER, Jamal SA, Beaton DE (2004)Practice patterns in the diagnosis and treatment of osteoporosisafter a fragility fracture: a systematic review. Osteoporos Int15:767–778
70. Harrington J (2006) Dilemmas in providing osteoporosis care forfragility fracture patients. US Musculoskelet Rev Touch BriefII:64–65
71. Chami G, Jeys L, Freudmann M, Connor L, Siddiqi M (2006)Are osteoporotic fractures being adequately investigated?: a ques-tionnaire of GP & orthopaedic surgeons. BMC Fam Pract 7:7
72. Sale JE, Beaton D, Posen J, Elliot-Gibson V, Bogoch E (2011)Systematic review on interventions to improve osteoporosis in-vestigation and treatment in fragility fracture patients. OsteoporosInt 22:2067–2082
73. British Orthopaedic Association, British Geriatrics Society(2007) The care of patients with fragility fracture, 2nd edn.British Orthopaedic Association, London
74. Vaile J, Sullivan L, Bennett C, Bleasel J (2007) First FractureProject: addressing the osteoporosis care gap. Intern Med J37:717–720
75. Giles M, Van Der Kallen J, Parker V, Cooper K, Gill K, Ross L et al(2011) A team approach: implementing a model of care for prevent-ing osteoporosis related fractures. Osteoporos Int 22:2321–2328
76. Kuo I, Ong C, Simmons L, Bliuc D, Eisman J, Center J (2007)Successful direct intervention for osteoporosis in patients withminimal trauma fractures. Osteoporos Int 18:1633–1639
77. Ward SE, Laughren JJ, Escott BG, Elliot-Gibson V, Bogoch ER,Beaton DE (2007) A program with a dedicated coordinator im-proved chart documentation of osteoporosis after fragility frac-ture. Osteoporos Int 18:1127–1136
78. Majumdar SR, Beaupre LA, Harley CH, Hanley DA, Lier DA,Juby AG et al (2007) Use of a case manager to improve osteo-porosis treatment after hip fracture: results of a randomizedcontrolled trial. Arch Intern Med 167:2110–2115
79. Majumdar SR, Johnson JA, Bellerose D et al (2011) Nurse case-manager vs multifaceted intervention to improve quality of oste-oporosis care after wrist fracture: randomized controlled pilotstudy. Osteoporos Int 22:223–230
80. Ahmed M, Durcan L, O’Beirne J, Quinlan J, Pillay I (2012)Fracture liaison service in a non-regional orthopaedic clinic—acost-effective service. Irish Med J 105(24):26–27
81. Blonk MC, Erdtsieck RJ, Wernekinck MG, Schoon EJ (2007)The fracture and osteoporosis clinic: 1-year results and 3-monthcompliance. Bone 40:1643–1649
82. Huntjens KM, van Geel TC, Geusens PP, Winkens B, Willems P,van den Bergh J et al (2011) Impact of guideline implementationby a fracture nurse on subsequent fractures and mortality inpatients presenting with non-vertebral fractures. Injury 42(Suppl4):S39–S43
83. van Helden S, Cauberg E, Geusens P, Winkes B, van der WeijdenT, Brink P (2007) The fracture and osteoporosis outpatient clinic:an effective strategy for improving implementation of an osteo-porosis guideline. J Eval Clin Pract 13:801–805
84. Schurink M, Hegeman JH, Kreeftenberg HG, Ten Duis HJ (2007)Follow-up for osteoporosis in older patients three years after afracture. Neth J Med 65:71–74
85. Carpintero P, Gil-Garay E, Hernandez-Vaquero D, Ferrer H,Munuera L (2009) Interventions to improve inpatient osteoporo-sis management following first osteoporotic fracture: thePREVENT project. Arch Orthop Trauma Surg 129:245–250
86. Astrand J, Thorngren KG, Tagil M, Akesson K (2008) 3-yearfollow-up of 215 fracture patients from a prospective and con-secutive osteoporosis screening program. Fracture patients care!Acta orthopaedica 79:404–409
87. Astrand J, Nilsson J, Thorngren KG (2012) Screening for osteo-porosis reduced new fracture incidence by almost half: a 6-year
follow-up of 592 fracture patients from an osteoporosis screeningprogram. Acta Orthop 83(6):661–665
88. Chevalley T, Hoffmeyer P, Bonjour JP, Rizzoli R (2002) Anosteoporosis clinical pathway for the medical management ofpatients with low-trauma fracture. Osteoporos Int 13:450–455
89. Newman ED, Ayoub WT, Starkey RH, Diehl JM, Wood GC(2003) Osteoporosis disease management in a rural health carepopulation: hip fracture reduction and reduced costs in postmen-opausal women after 5 years. Osteoporos Int 14:146–151
90. Dell RM, Greene D, Anderson D, Williams K (2009)Osteoporosis disease management: what every orthopaedic sur-geon should know. J Bone Joint Surg Am 91(Suppl 6):79–86
91. Harrington JT, Barash HL, Day S, Lease J (2005) Redesigningthe care of fragility fracture patients to improve osteoporosismanagement: a health care improvement project. ArthritisRheum 53:198–204
92. Edwards BJ, Bunta AD, Madison LD, DeSantis A, Ramsey-Goldman R, Taft L et al (2005) An osteoporosis and fractureintervention program increases the diagnosis and treatment forosteoporosis for patients with minimal trauma fractures. Jt CommJ Qual Patient Saf 31:267–274
93. Majumdar SR, Lier DA, Beaupre LA, Hanley DA,Maksymowych WP, Juby AG et al (2009) Osteoporosis casemanager for patients with hip fractures: results of a cost-effectiveness analysis conducted alongside a randomized trial.Arch Intern Med 169:25–31
94. McLellan AR, Wolowacz SE, Zimovetz EA, Beard SM,Lock S, McCrink L et al (2011) Fracture liaison servicesfor the evaluation and management of patients with osteo-porotic fracture: a cost-effectiveness evaluation based on datacollected over 8 years of service provision. Osteoporos Int22:2083–2098
95. Department of Health (2009) Fracture prevention services: aneconomic evaluation. Department of Health, London
96. Marsh D, Akesson K, Beaton DE, Bogoch ER, Boonen S, BrandiML et al (2011) Coordinator-based systems for secondary pre-vention in fragility fracture patients. Osteoporos Int 22:2051–2065
97. Eisman JA, Bogoch ER, Dell R et al (2012) Making the firstfracture the last fracture: ASBMR task force report on secondaryfracture prevention. J Bone Miner Res 27:2039–2046
98. Institute of Medicine of the National Academies (2012) Crossingthe quality chasm: the IOM Health Care Quality Initiative. http://www.iom.edu/Global/News%20Announcements/Crossing-the-Quality-Chasm-The-IOM-Health-Care-Quality-Initiative.aspxAccessed 17 Dec 2012
99. Ganda K, Puech M, Chen JS, Speerin R, Bleasel J, Center JR,Eisman JA, March L, Seibel MJ (2013) Models of care for thesecondary prevention of osteoporotic fractures: a systematic re-view and meta-analysis. Osteoporos Int 24:393–406
100. Little EA, EcclesMP (2010) A systematic review of the effectivenessof interventions to improve post-fracture investigation and manage-ment of patients at risk of osteoporosis. Implement Sci: IS 5:80
101. International Osteoporosis Foundation (2012) Stop at One:Make your first break your last-events. http://www.worldosteoporosisday.org/events-eng Accessed 16 Nov 2012
102. Global Coalition on Aging (2012) Welcome to the GlobalCoalition on Aging. http://www.globalcoalitiononaging.com/Accessed 16 Nov 2012