512
Alberta Health and Wellness Drug Benefit List Effective April 1, 2012

Alberta Health and Wellness
Drug Benefit List
Effective April 1, 2012

78BInquiries should be directed to: Pharmacy Services Alberta Blue Cross 10009 108 Street NW Edmonton AB T5J 3C5 Telephone Number: (780) 498-8370 (Edmonton) (403) 294-4041 (Calgary) 1-800-361-9632 (Toll Free) FAX Number: (780) 498-8384 1-877-828-4106 (Toll Free) 109BWebsite: HUhttp://www.health.alberta.ca/AHCIP/drug-benefit-list.html U Administered by Alberta Blue Cross on behalf of Alberta Health and Wellness. The Drug Benefit List (DBL) is a list of drugs for which coverage may be provided to program participants. The DBL is not intended to be, and must not be used as a diagnostic or prescribing tool. Inclusion of a drug on the DBL does not mean or imply that the drug is fit or effective for any specific purpose. Prescribing professionals must always use their professional judgment and should refer to product monographs and any applicable practice guidelines when prescribing drugs. The product monograph contains information that may be required for the safe and effective use of the product. Binder and contents: $42.00 ($40.00 + $2.00 G.S.T.) Contents only: $36.75 ($35.00 + $1.75 G.S.T.) A cheque or money order must accompany the request for copies.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. i EFFECTIVE APRIL 1, 2012
1BTable of Contents
79BPART 1 80BSECTION 1—POLICIES AND GUIDELINES
Introduction Acknowledgments ..................................................................................................................................1.1 Eligibility .................................................................................................................................................1.1 Additional Notes Regarding Application of the List ................................................................................1.1 Legend ...................................................................................................................................................1.3 Example of Drug Product Listings .........................................................................................................1.4 Drug Review Procedure .........................................................................................................................1.5 Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics ......................1.7 Submissions for Drug Reviews Interpretation Notices ...........................................................................................................................1.10 Submission Requirements ...................................................................................................................1.12 Criteria for Listing Drug Products .........................................................................................................1.23 Interchangeable Drug Products – Additional Criteria ..........................................................................1.25 Interchangeable Drug Products – Additional Criteria Appendices ......................................................1.29 Review of Benefit Status (ROBS) Criteria ...........................................................................................1.36 Supply Shortage Policy for Drug Products ..........................................................................................1.37 Units of Issue for Pricing ......................................................................................................................1.38 Policy for Administering Interchangeability Challenges .......................................................................1.40 Your Comments are Important to Us ...................................................................................................1.42 Price Policy Definitions ............................................................................................................................................1.43 Alberta Price Confirmation (APC) ........................................................................................................1.46 Interim APC ..........................................................................................................................................1.48 Fixed Pricing Rules (For Interchangeable Drugs) ...............................................................................1.49 Non-Fixed Pricing Rules (For Brand and Other Drugs) .......................................................................1.50 Exceptions ...........................................................................................................................................1.50 Price Reductions ..................................................................................................................................1.51 Minister’s Authority ...............................................................................................................................1.52 Least Cost Alternative (LCA) Price Policy ...........................................................................................1.55 Maximum Allowable (MAC) Price Policy ..............................................................................................1.56 Restricted Benefits Restricted Benefits ...............................................................................................................................1.57 Limited Restricted Benefits ..................................................................................................................1.58 Products Designated as Limited Restricted Benefits ...........................................................................1.58 Special Authorization Guidelines Special Authorization Policy ................................................................................................................1.59 Special Authorization Procedures ....................................................................................................... 1A.1 Special Authorization Forms ............................................................................................................... 1A.2 Drug Special Authorization Request Form ......................................................................................... 1A.4 Donepezil/Galantamine/Rivastigmine Special Authorization Request Form ...................................... 1A.6 Clopidogrel Special Authorization Request Form ............................................................................... 1A.8

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 ii
83B84B3BTable of Contents, continued
Darbepoetin/Epoetin Special Authorization Request Form ..................................................................... 1A.10 Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form ....................................................................................................... 1A.13 Ezetimibe Special Authorization Request Form ...................................................................................... 1A.15 Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form .......................................................................................................................................... 1A.17 Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form .............................. 1A.19 Etanercept for Juvenile Idiopathic Arthritis Special Authorization Request Form ................................... 1A.21 Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form .......................................................................................................................................... 1A.23 Select Quinolones Special Authorization Request Form ........................................................................ 1A.25 Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Nasal Spray Salmon for Osteoporosis Special Authorization Request Form ....................................................................................................... 1A.28 Celecoxib Special Authorization Request Form ...................................................................................... 1A.31 Filgrastim/Pegfilgrastim Special Authorization Request Form ................................................................ 1A.33 Fentanyl Special Authorization Request Form ........................................................................................ 1A.35 Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form .......................................................................................................................................... 1A.37 Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form .......................................................................................................................................... 1A.39 Adalimumab for Crohn’s/ Infliximab for Crohn’s/Fistulizing Crohn’s Disease Special Authorization Request Form .................................................................................................................... 1A.41 Rituximab for Rheumatoid Arthritis Special Authorization Request Form .............................................. 1A.43 Imiquimod Special Authorization Request Form ..................................................................................... 1A.45 Dutasteride/Finasteride Special Authorization Request Form ................................................................ 1A.47 Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form ............... 1A.49 Abatacept for Juvenile Idiopathic Arthritis Special Authorization Request Form .................................... 1A.51 Montelukast/Zafirlukast Special Authorization Request Form ................................................................ 1A.53 Febuxostat Special Authorization Request Form .................................................................................... 1A.55 Denosumab Special Authorization Request Form .................................................................................. 1A.57 Omalizumab Special Authorization Request Form ................................................................................. 1A.59 Eculizumab Special Authorization Request Form.................................................................................. 1A.61 Eculizumab Consent Form.....................................................................................................................1A.66
81BSECTION 2—MULTIPLE SCLEROSIS (MS) DRUG COVERAGE Clinical Criteria for Coverage .......................................................................................................................2.1 Contraindications to Coverage .....................................................................................................................2.1 Alberta Multiple Sclerosis (MS) Drug Review Panel ....................................................................................2.2 Process for Multiple Sclerosis (MS) Drug Coverage ....................................................................................2.2 Avonex/Betaseron/Copaxone/Extavia/Rebif/Tysabri MS Drug Coverage Application .................................2.4 Drug Products Under Multiple Sclerosis (MS) Drug Coverage Program ...................................................2.10

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. iii EFFECTIVE APRIL 1, 2012
SECTION 3—CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
Special Authorization Policy ..................................................................................................................3.1 Criteria for Coverage ..............................................................................................................................3.3
83B84B3BTable of Contents, continued
SECTION 3A—CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
Criteria for Coverage ..................................................................................................................... ……..3A Role of the Prescribers .......................................................................................................................... 3A Criteria for Optional Special Authorization of Select Drug Products ................................................... 3A.1
SECTION 4—RARE DISEASES DRUG COVERAGE PROGRAM Rare Diseases Drug Coverage ........................................................................................................ …..4.1 Contraindications ...................................................................................................................................4.1 Rare Diseases Drugs Eligible for Coverage ..........................................................................................4.2 Alberta Rare Diseases Clinical Review Panel .......................................................................................4.2 Process for Rare Diseases Drug Coverage...........................................................................................4.2
85BPART 2
86BPHARMACOLOGIC–THERAPEUTIC CLASSIFICATION OF DRUGS 04:00 Antihistamine Drugs ....................................................................................................... 1 08:00 Anti-Infective Agents ...................................................................................................... 3 10:00 Antineoplastic Agents ................................................................................................... 19 12:00 Autonomic Drugs .......................................................................................................... 21 20:00 Blood Formulation, Coagulation and Thrombosis ........................................................ 27 24:00 Cardiovascular Drugs ................................................................................................... 33 28:00 Central Nervous System Agents .................................................................................. 69 34:00 Dental Agents ............................................................................................................. 121 36:00 Diagnostic Agents ...................................................................................................... 123 40:00 Electrolytic, Caloric, and Water Balance .................................................................... 125 48:00 Respiratory Tract Agents............................................................................................ 129 52:00 Eye, Ear, Nose and Throat (EENT) Preparations ...................................................... 131 56:00 Gastrointestinal Drugs ................................................................................................ 141 60:00 Gold Compounds ....................................................................................................... 151 64:00 Heavy Metal Antagonists............................................................................................ 153 68:00 Hormones and Synthetic Substitutes ......................................................................... 155 80:00 Serums, Toxoids and Vaccines .................................................................................. 169 84:00 Skin and Mucous Membrane Agents ......................................................................... 171 86:00 Smooth Muscle Relaxants.......................................................................................... 181 88:00 Vitamins ...................................................................................................................... 183 92:00 Miscellaneous Therapeutic Agents ............................................................................ 185 94:00 Devices ....................................................................................................................... 189

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 iv
88B83B84B3BTable of Contents, continued
87BAPPENDICES Appendix 1 Abbreviations ............................................................................................................. 190 Appendix 2 Pharmaceutical Manufacturers ................................................................................. 191
INDICES Index 1 Alphabetical List of Pharmaceutical Products .................................................................. 193 Index 2 Numerical List by Drug Identification Number .................................................................. 226

Section 1 Policies and Guidelines
PART 1
SECTION 1
Policies and
Guidelines

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 1 EFFECTIVE APRIL 1, 2012
INTRODUCTION Acknowledgments
Alberta Health and Wellness acknowledges the important role Alberta Blue Cross continues to play in the production of the List and in the development of an overall strategy and initiatives to better manage Alberta Health and Wellness sponsored drug programs.
Eligibility The Alberta Health and Wellness Drug Benefit List defines the drugs and drug products that are covered by Alberta government-sponsored drug programs. These programs are for Albertans and their dependents who are covered by: 1. the Alberta Blue Cross Non-Group Coverage (Group 1) offered by the Alberta Health Care
Insurance Plan, 2. the Alberta Blue Cross Coverage for Seniors (Group 66) provided to all Alberta senior
citizens and those on the Alberta Widows’ Pension Plan (Group 66A), or 3. the drug coverage provided to individuals approved by Alberta Health and Wellness for
Palliative Care Drug Coverage. (For these individuals the Palliative Care Drug Benefit Supplement must also be considered), or
4. the drug coverage provided to Alberta Human Services and Alberta Seniors (AISH) clients. (For these clients the Alberta Human Services Drug Benefit Supplement must also be considered.)
Additional Notes Regarding Application of the List
1. The List is not intended to be used as a scientific reference or prescribing guide.
2. Formularies used by hospitals and continuing care facilities are developed independently of the List.
3. Drugs are classified according to the Pharmacologic–Therapeutic classifications (PTC) developed by the American Society of Health-System Pharmacists for the purpose of the American Hospital Formulary Service.
Permission to use this system has been granted by the American Society of Health-System Pharmacists. The Society is not responsible for the accuracy of transpositions or excerpts from the original content.
Where necessary, additional PTCs may have been assigned by Alberta Health and Wellness to facilitate product location in the List.
4. Where appropriate, the Compendium of Pharmaceuticals and Specialties, published by the Canadian Pharmacist’s Association, was used as a reference source for the trade name, generic name, manufacturer, strength and dosage form.
The Canadian Pharmacist’s Association is not responsible for the accuracy of transpositions or excerpts from the original content.
5. Other reference sources used for the trade name, generic name, manufacturer, strength and dosage form are: completed Drug Identification Number (DIN) notification form Notice of Compliance (NOC) Product Monograph

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 2
6. DINs listed reflect current manufacturer information available as of March 31, 2012.
7. Alberta Health and Wellness reserves the right to make changes, without notice, to the List through the on-line interactive List, and any such changes to the on-line interactive List are effective the date of the change (unless otherwise stated) and regardless of the date of publication in the paper version or updates.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 3 EFFECTIVE APRIL 1, 2012
Legend
Pharmacologic–Therapeutic classification.
Pharmacologic–Therapeutic sub-classification.
Nonproprietary or generic ingredient name of the drug.
Drug strength and dosage form.
The Drug Identification Number (DIN), assigned by the Therapeutic Products Directorate (TPD), Health Protection Branch, Health Canada.
A box containing an X to the left of the DIN indicates that the product is not interchangeable with other products or interchangeability has not been assessed within the category.
All active ingredients of combination products are listed.
Strengths of active ingredients are listed in the same order as the ingredients. This example indicates that the topical cream contains 1% hydrocortisone acetate and 10% urea.
Brand name of the drug.
Three letter identification code assigned to each manufacturer. The codes are listed in Appendix 2 at the end of the List.
For products which are marked as non-interchangeable, the price is indicated in regular type (not bold type). These prices are supplied by the manufacturer and are expressed in decimal dollars.
For those products which are single source, the price is indicated in regular type (not bold type). These prices are supplied by the manufacturer and are expressed in decimal dollars.
Interchangeable grouping where the Least Cost Alternative (LCA) Price Policy has not been applied. This example indicates these two products are deemed interchangeable. These prices are supplied by the manufacturer and are expressed in decimal dollars.
The LCA Price for the selected interchangeable category appears in bold type. The LCA price is the maximum price which will be paid. The prices listed are expressed as decimal dollars. An authorized health care provider may request special authorization if a particular brand is essential in the care of a patient where the LCA Price would otherwise apply. For further information refer to the Special Authorization Guidelines section of the AHWDBL or List.
Products or devices designated as restricted benefits and limited restricted benefits are identified by a comment after the generic name. The comment indicates “RESTRICTED BENEFIT” or “LIMITED RESTRICTED BENEFIT” along with an explanation of the limits and/or restrictions. In this example, coverage of Accolate is restricted to the treatment of asthma in patients 12 to 18 years of age inclusive. For more information about products or devices designated as restricted benefits, refer to the restricted benefits section of the List.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1 • 4
7BExample of Drug Product Listings
08:00 ANTI-INFECTIVE AGENTS 08:30.92 ANTIPROTOZOALS (MISCELLANEOUS ANTIPROTOZOALS)
METRONIDAZOLE 250 MG ORAL TABLET
00000545066 METRONIDAZOLE AAP $ 0.0640 5 MG / ML INJECTION
00000870420 FLAGYL BAX $ 0.0240 00000649074 METRONIDAZOLE HSP $ 0.0266
28:00 CENTRAL NERVOUS SYSTEM AGENTS 28:08:04.92 ANALGESICS AND ANTIPYRETICS NONSTEROIDAL ANTI-INFLAMMATORY AGENTS (OTHER NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
NAPROXEN 250 MG ORAL ENTERIC-COATED TABLET
00002246699 APO-NAPROXEN EC APX $ 0.1068 $ 0.2467 00002365847 AVA-NAPROXEN EC AVA $ 0.1068 $ 0.2467 00002350785 NAPROXEN EC SNS $ 0.1068 $ 0.2467 00002243312 NOVO-NAPROX EC TEV $ 0.1068 $ 0.2467 00002162792 NAPROSYN E HLR $ 0.1068 $ 0.4487
MAC pricing has been applied based on the LCA price for 1 x 250 mg oral tablet.
68:00 HORMONES AND SYNTHETIC SUBSTITUTES 68:16.04 ESTROGENS AND ANTIESTROGENS (ESTROGENS)
CONJUGATED ESTROGENS 0.3 MG ORAL TABLET
00002043394 PREMARIN WAY $ 0.3117 0.625 MG ORAL TABLET
00000265470 C.E.S VCL $ 0.1090 00002043408 PREMARIN WAY $ 0.3117
84:00 SKIN AND MUCOUS MEMBRANE AGENTS 84:06 ANTI-INFLAMMATORY AGENTS
HYDROCORTISONE ACETATE/ UREA 1 % * 10 % TOPICAL CREAM
00000503134 UREMOL-HC GSK $ 0.1877 1 % * 10 % TOPICAL LOTION
00000560022 UREMOL-HC GSK $ 0.1044 HYDROCORTISONE
1 % TOPICAL LOTION 00000578541 SARNA HC GSK $ 0.1008 00000192600 EMO-CORT GSK $ 0.1706
48:00 RESPIRATORY TRACT AGENTS 48:10.24 ANTI-INFLAMMATORY AGENTS (LEUKOTRIENE MODIFIERS)
ZAFIRLUKAST RESTRICTED BENEFIT - This product is a benefit for patients 12 to 18 years of age inclusive for the prophylaxis and treatment of asthma. (For eligibility in patients over 18 years of age refer to the Criteria for Special Authorization of Select Drug Products of the List, and Criteria for Special Authorization of Select Drug Products in the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
20 MG ORAL TABLET 00002236606 ACCOLATE AZC $ 0.8054
10 12
14
12
34
5
131313
13131313
9
7
8
77777
116
15
7777777
1313
7
5

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 5 EFFECTIVE APRIL 1, 2012
DRUG REVIEWS
The Minister of Health and Wellness makes the final decisions on changes to the Alberta Health and Wellness Drug Benefit List (List) after considering the recommendations of the Expert Committee on Drug Evaluation and Therapeutics (Expert Committee), and/or the Canadian Expert Drug Advisory Committee (CEDAC), and/or Alberta Health and Wellness. Drug manufacturers wishing to have their drug product(s) listed on the List are required to make submissions in accordance with the procedures and criteria published in the List. Common Drug Review Alberta is a participant in the national Common Drug Review procedure (CDR Procedure*) and considers recommendations from CEDAC. Submissions relating to the New Chemical Entities and New Combination Products that have received a Health Canada Notice of Compliance (NOC) should be directed to the CDR Directorate for consideration, and must comply with the CDR Procedure requirements.
• New Chemical Entity is an active moiety that has not been previously approved for sale in Canada by Health Canada and marketed in Canada. • New Combination Product consists of two or more active moieties that have not previously been approved for sale in Canada and marketed in Canada in that combination. It may consist of either two or more new active moieties or two or more old active moieties or a combination of new and old active moieties.
Expert Committee on Drug Evaluation and Therapeutics Drug Reviews The Minister of Health and Wellness has established an Expert Committee on Drug Evaluation and Therapeutics to refine and maintain the List on an ongoing basis. All drug products not eligible for review under the CDR Procedure or the Interchangeable Expedited Review procedure must be reviewed by the Expert Committee prior to their determination as benefits on the List. The Expert Committee considers the scientific, therapeutic, clinical and socio-economic merits of drug products. The Committee receives advice and assistance from external consultants and agencies when needed. The Expert Committee makes recommendations on the List to Alberta Health and Wellness through the Executive Director, Pharmaceutical Funding and Guidance, Health Policy and Service Standards Division. Interchangeable Reviews Drug products may be considered for listing as interchangeable through Expedited Review or Full Review. Expedited Review drug products are not required to undergo a full review by the Expert Committee. Interchangeable drug product submissions will be screened by Alberta Blue Cross to determine eligibility for an Expedited Review and the results provided to Alberta Health and Wellness. Interchangeable drug submissions requiring Full Review will be reviewed by the Expert Committee under its usual drug review procedure.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 6
Referrals Alberta Health and Wellness at all times and in all circumstances reserves the right to refer any submission to the CDR Procedure and/or the Expert Committee for further advice or for a full review. Deferrals The Expert Committee and/or Alberta Health and Wellness reserve the right to defer any submission it deems appropriate in order to ensure that it may complete a review in a manner that protects patient safety and maintains the integrity of the AHWDBL and the government-sponsored drug programs. Examples of reasons for deferrals include, but are not limited to:
1. To request additional information in order to conduct a review and prepare recommendations;
2. Where additional time, research and/or consultation is required before a review can be completed or a recommendation can be made;
3. Where new or novel issues are raised; 4. Where issues, questions or concerns relating to any of the listing criteria or factors
arise, including but not limited to: (a) interchangeable safety issues, (b) whether the criteria requires expansion or clarification, (c) the drug product, (d) the listing, (e) the price, (f) any other relevant criteria or factor.
*Information regarding the CDR Procedure may be obtained through the Canadian Agency for Drugs and Technologies in Health.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 7 EFFECTIVE APRIL 1, 2012
Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics
Committee Members
James L. SILVIUS, BA, MD, FRCPC Chair Clinical Associate Professor Geriatric Medicine University of Calgary 10301 Southport Lane SW Calgary, Alberta T2W 1S7 Robert J. HERMAN, MD, FRCPC Vice-Chair Professor Division of General Internal Medicine Faculty of Medicine University of Calgary Health Science Centre 3330 Hospital Drive NW Calgary, Alberta T2N 4N1 Margaret BARR, BSc(Pharm) Pharmacist 5238-42 Street Ponoka, Alberta T4J 1C9 Jeffrey A. JOHNSON, BSP, MSc, PhD Professor School of Public Health University of Alberta 2-040 Li Ka Shing Centre Edmonton, Alberta T6G 2N3 Saibal NANDY, MBBS, MRCPsych, FRCPC Psychiatrist 101-1424 Southview Drive SE Medicine Hat, Alberta T1B 4E7 Glen J. PEARSON, BScPhm, PharmD, FCSHP Associate Professor of Medicine Co-Director, Cardiac Transplant Clinic Director of Research, Cardiovascular Risk Reduction Clinic Division of Cardiology 2C2 Walter Mackenzie Health Sciences Centre Edmonton, Alberta T6G 2B7 Cheryl A. SADOWSKI, BSc(Pharm), PharmD, FCSHP Associate Professor 3-171 Edmonton Clinic Health Academy 11405-87 Avenue Edmonton, Alberta T6G 1C9
Committee Members (cont’d) Kelly B. ZARNKE, MD, MSc, FRCPC Associate Professor and Head, Division of General Internal Medicine Chief, Division of General Internal Medicine, Alberta Health Services Health Sciences Centre, Room 1470 University of Calgary 3330 Hospital Drive NW Calgary, Alberta T2N 4N1 Alberta Health and Wellness Liaison Steve LONG, BSc(Pharm), MBA Executive Director Pharmaceutical Funding and Guidance Branch Health Workforce Division Alberta Health and Wellness 11th Floor, 10025 Jasper Avenue NW Edmonton, Alberta T5J 1S6 Mark HARASYMUK, BSc(Pharm) Senior Manager, Operations Pharmaceutical Funding and Guidance Branch Health Workforce Division Alberta Health and Wellness 11th Floor, 10025 Jasper Avenue NW Edmonton, Alberta T5J 1S6 Administrative/Scientific Support Carlyn VOLUME-SMITH, BSc(Pharm), MSc, PhD Senior Manager Scientific and Research Services Alberta Blue Cross 10009 - 108 Street NW Edmonton, Alberta T5J 3C5 Sherry DIELEMAN, BSc(Pharm), MSc Senior Pharmacist Associate Scientific and Research Services Alberta Blue Cross Micheal S. GUIRGUIS, BSc(Pharm), PhD Senior Scientific Associate Scientific and Research Services Alberta Blue Cross Rhonda C. SHKROBOT, BSc(Pharm) Senior Pharmacist Associate Scientific and Research Services Alberta Blue Cross

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 8
SUBMISSIONS for DRUG REVIEWS 1) Only submissions satisfying all of the submission requirements of the applicable category of
drug product that are deemed complete by the applicable submission deadline date will be put forward for review.
2) In addition to the submission requirements, the Expert Committee and/or Alberta Health and Wellness, at their sole discretion, reserve the right to request the drug product file from Health Canada’s Therapeutic Products Directorate (TPD), or any additional information from the manufacturer, CEDAC, or any other entity that the Expert Committee and/or Alberta Health and Wellness consider necessary, which may result in a delay in the listing recommendation for the drug product.
3) There is no obligation or guarantee that every completed submission will be reviewed, and/or a recommendation made, by a specific date or at the next scheduled meeting of the Expert Committee.
4) Pre-NOC submissions may be made; however, the submission will only be reviewed once it is complete.
5) Any request by a manufacturer to hold a submission will result in a submission being deemed incomplete as of the date of the request. A submission on hold will only be considered complete once correspondence is received from a manufacturer to proceed with the submission.
6) Only one (1) copy of a submission for a drug product is required. A determination by Alberta Blue Cross that a submission is complete is preliminary and made only for the purposes of forwarding the submission for review.
7) Drug manufacturers are permitted to provide other information they feel may be important to the review of a submission e.g. selected references or additional studies completed after a drug product had been submitted to the Therapeutic Products Directorate, Health Canada. Comparative studies with other listed drug products are most relevant.
8) Information on submission deadlines are posted on the Alberta Health and Wellness Drug Benefit List website which can be accessed at http://www.ab.bluecross.ca/dbl/manufacturers.html. Notice of Significant Changes - By making a submission, and if a drug product is listed on the List, manufacturers acknowledge and agree that they are required to notify the Senior Manager, Scientific and Research Services of any significant change to listed drug products. Significant changes are considered to be changes in NOC, DIN, product name, manufacturer or distributor, indication, product monograph, packaging, formulation, manufacturing specifications or any change that could potentially affect the bioavailability or bioequivalence of a drug product. All submissions should be sent to the attention of: Senior Manager Scientific and Research Services Alberta Blue Cross 10009 108 Street NW Edmonton, Alberta T5J 3C5
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 9 EFFECTIVE APRIL 1, 2012
All inquiries should be directed to: Coordinator Scientific and Research Services Alberta Blue Cross 10009 108 Street NW Edmonton, Alberta T5J 3C5 Phone: (780) 498-8098
Fax: (780) 498-3534

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 10
Interpretation Notices
From time to time, or as circumstances warrant, certain practices or procedures may be adopted by the Committee pertaining to the interpretation of the procedures and criteria published in the AHWDBL Policies and Guidelines. In order to assist manufacturers in preparing and submitting effective drug review submissions, the Expert Committee has determined that, where it deems appropriate, notice of these practices will be provided to manufacturers through “Interpretation Notices”. The Notices are intended to be a guide to assist manufacturers, but in situations where the Notices lead to inconsistencies or conflicts, the criteria in the Drug Review Procedure and Submission Requirements and Criteria, will apply. Notices will be published electronically and it continues to be the responsibility of manufacturers to monitor amendments to the AHWDBL. For convenience only, hard copies of Notices may be provided with the AHWDBL Interim Updates where deemed appropriate by Alberta Blue Cross.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 11 EFFECTIVE APRIL 1, 2012
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
INTERPRETATION NOTICE #1
INTERCHANGEABILITY and NON-CANADIAN REFERENCE PRODUCTS
The Submission Requirements and Criteria of the AHWDBL require manufacturers to provide the Expert Committee on Drug Evaluation and Therapeutics (“Expert Committee”) with data comparing the submitted drug product to the reference drug product. Under the Interchangeable Drug Products Criteria, manufacturers are also required to demonstrate bioequivalence with the reference drug product in accordance with the Criteria. At various times, some manufacturers have submitted interchangeability submissions using a Non-Canadian Reference Product (NCRP). After reviewing several submissions, the Expert Committee has adopted the practice of permitting manufacturers to demonstrate bioequivalency by providing data comparing the submitted drug product to a NCRP that meets the Criteria for use of a Non-Canadian Reference Product as set out in Health Canada’s Drugs Directorate Policy regarding the use of a Non-Canadian Reference Product under the provisions of Section C.08.002.1(c) of the Food and Drug Regulations (the “NCRP Criteria”). Important Note: Health Canada does not determine interchangeability and therefore, a determination by Health Canada that a product meets the NCRP Criteria is not sufficient proof for the Expert Committee’s purposes. The Expert Committee will continue to consider and assess all of the submission materials, and make its own determination whether the NCRP Criteria, the Submission Requirements and the Criteria are met, and whether the product may be designated as interchangeable. The practice in these situations is that, after receipt of the submission, Alberta Blue Cross makes a request to Health Canada for a copy of the Therapeutic Products Directorate’s review (TPD File) for the submitted product(s). Manufacturers are advised that, in order to avoid a possible deferral, they may include a full copy of the TPD File in their submission. If necessary, submissions may be deferred until the TPD File is received. Product submissions may, at the discretion of Alberta Blue Cross, be scheduled for review if the TPD File is received 7 days prior to the meeting date. As with all submissions, the Expert Committee retains the right to request additional materials from the manufacturer, Health Canada or any other entity it determines appropriate in order to conduct its review. Issue Date: November 9, 2006

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 12
SUBMISSION REQUIREMENTS
The following Submission Requirements pertain to submissions not eligible for review under the CDR Procedure. A) New Chemical Entities/Single Source Drug Products The following submission requirements pertain to New Chemical Entities, New Combination Products where one or more of the active moieties have never been listed on the List, and other single source drug products that have never been listed on the List; and are not eligible for review under the CDR Procedure. Submissions for drug products in this category should first be directed to the CDR Directorate. 1. Consent Letter
• an unrestricted letter authorizing Alberta Health and Wellness and its agent/designate to access, discuss, use, collect from, and disclose to its agents, consultants, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH) and all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services and the government of any province or territory in Canada, all submission information and information in the possession of Health Canada, CADTH, PMPRB, Alberta Health Services and the government of any province or territory in Canada
2. Letter Confirming Ability to Supply • a letter signed by a senior official providing assurance that the manufacturer is able to
supply the specific drug product and strength from the time of listing in a quantity sufficient to meet the anticipated demand in Alberta for a minimum of 6 months.
3. A hard copy and electronic (CD) copy of the following from the Common Technical Document:
a. Clinical Overview (Module 2.5), and b. Clinical Summary (modules 2.7.1, 2.7.3, 2.7.4 and 2.7.6).
Note: If a Common Technical Document was not prepared for Health Canada, a Comprehensive Summary may be acceptable in lieu.
4. Copy of completed Drug Identification Number (DIN) notification form 5. Copy of Notice of Compliance (NOC) 6. Current Patent Status
• a signed statement from the manufacturer stating that the submitted product does not infringe any patents
• expiry date(s) of all Canadian patent(s) 7. Price Information
• The proposed price for Alberta (which must be in compliance with the Price Policy) 8. Product Monograph
• in addition to a hard copy, an electronic (CD) copy of the TPD-approved Product Monograph compatible with Microsoft Word is required
9. Economic Information • a comprehensive pharmacoeconomic analysis in accordance with: the “Guidelines for
the economic evaluation of health technologies: Canada [3rd Edition]”. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.; cost-effectiveness and cost-utility data and the impact on “direct” healthcare costs are most useful

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 13 EFFECTIVE APRIL 1, 2012
• a completed Budget Impact Assessment for the Alberta Health and Wellness Drug Benefit List form. Note: copies of the most recent version of this form can be obtained by accessing the Alberta Health and Wellness Drug Benefit List website at www.ab.bluecross.ca/dbl/manufacturers.html, or by contacting the Coordinator, Scientific and Research Services, Alberta Blue Cross at Phone: (780) 498-8098 or Fax: (780) 498-3534.
10. If requested, the manufacturer must provide written confirmation from the CDR Directorate that the drug product is not eligible for review under the CDR Procedure.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 14
B) Changes to Special Authorization or Restricted Benefit Status of Listed Single Source Drug Products Due to a New Indication The following submission requirements pertain to single source drug products currently listed via special authorization or as restricted benefits that have received a new indication from Health Canada, where the manufacturer wishes to request expansion of the coverage criteria or change in benefit status due to the new indication and where the drug products are not eligible for review under the CDR Procedure. Submissions for drug products in this category that have been previously reviewed under the CDR Procedure should first be directed to the CDR Directorate. 1. Consent Letter
• an unrestricted letter authorizing Alberta Health and Wellness and its agent/designate to access, discuss, use, collect from, and disclose to its agents, consultants, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH) and all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services and the government of any province or territory in Canada, all submission information and information in the possession of Health Canada, CADTH, PMPRB, Alberta Health Services and the government of any province or territory in Canada
2. Letter Confirming Ability to Supply • a letter signed by a senior official providing assurance that the manufacturer is able to
supply the specific drug product and strength from the time of listing in a quantity sufficient to meet the anticipated demand in Alberta for a minimum of 6 months.
3. Justification for the Expanded Coverage Criteria or Change in Benefit Status • a separate document indicating the reason for and evidence to justify the need for the
expanded coverage criteria or change in benefit status due to the new indication 4. A hard copy and electronic (CD) copy of the following from the Common Technical Document:
o Clinical Overview (Module 2.5), and o Clinical Summary (modules 2.7.1, 2.7.3, 2.7.4 and 2.7.6)
5. Note: If a Common Technical Document was not prepared for Health Canada, a Comprehensive Summary may be acceptable in lieu. Copy of Notice of Compliance (NOC) for the new indication.
6. Current Patent Status • a signed statement from the manufacturer stating that the submitted product does not
infringe any patents • expiry date(s) of all Canadian patent(s)
7. Price Information • The proposed price for Alberta (which must be in compliance with the Price
Policy) 8. Product Monograph (revised to include the new indication)
• in addition to a hard copy, an electronic (CD) copy of the TPD-approved Product Monograph compatible with Microsoft Word is required

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 15 EFFECTIVE APRIL 1, 2012
9. Economic Information • a comprehensive pharmacoeconomic analysis prepared with respect to the new
indication only in accordance with: the “Guidelines for the economic evaluation of health technologies: Canada [3rd Edition]”. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.; cost-effectiveness and cost-utility data and the impact on “direct” healthcare costs are most useful
• a completed Budget Impact Assessment for the Alberta Health and Wellness Drug
Benefit List form prepared with respect to the new indication only. Note: copies of the most recent version of this form can be obtained by accessing the Alberta Health and Wellness Drug Benefit List website at www.ab.bluecross.ca/dbl/manufacturers.html, or by contacting the Coordinator, Scientific and Research Services, Alberta Blue Cross at Phone: (780) 498-8098 or
Fax: (780) 498-3534. 10. If requested, the manufacturer must provide written confirmation from the CDR
Directorate that the drug product is not eligible for review under the CDR Procedure.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 16
C) Line Extension Drug Products
The following submission requirements pertain to new strengths and formulations or reformulations of drug products that are currently listed or are under consideration for listing on the List and where products are not eligible for review under the CDR Procedure. Submissions for drug products in this category that have previously been reviewed under the CDR Procedure should first be directed to the CDR Directorate.
1. Consent Letter • an unrestricted letter authorizing Alberta Health and Wellness and its agent/designate
to access, discuss, use, collect from, and disclose to its agents, consultants, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH) and all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services and the government of any province or territory in Canada, all submission information and information in the possession of Health Canada, CADTH, PMPRB, Alberta Health Services and the government of any province or territory in Canada
2. Letter Confirming Ability to Supply • a letter signed by a senior official providing assurance that the manufacturer is able to
supply the specific drug product and strength from the time of listing in a quantity sufficient to meet the anticipated demand in Alberta for a minimum of 6 months.
3. Justification for the Line Extension • a separate document indicating the reason for and evidence to justify the need for the
new strength, formulation or reformulation of the drug product 4. A hard copy and electronic (CD) copy of the following from the Common Technical Document:
Clinical Overview (Module 2.5), and Clinical Summary (modules 2.7.1, 2.7.3, 2.7.4 and 2.7.6).
Note: If a Common Technical Document was not prepared for Health Canada, a Comprehensive Summary may be acceptable in lieu. In the event a Comprehensive Summary was not prepared for Health Canada (i.e. clinical studies have not been conducted on the new strength, formulation or reformulation) then the manufacturer must provide evidence establishing a clear linkage between the submitted product(s) and a currently listed product(s). This can be in the form of:
i. bioequivalence data; or ii. evidence of formulation proportionality (i.e. a comparison of master
formulae for all submitted strengths) and evidence of a similar dissolution profile.
5. Copy of completed Drug Identification Number (DIN) notification form 6. Copy of Notice of Compliance (NOC) 7. Current Patent Status
• a signed statement from the manufacturer stating that the submitted product does not infringe any patents
• expiry date(s) of all Canadian patent(s) 8. Copy of completed and approved Certified Product Information Document (CPID)
• in lieu of the CPID, a Master Formula and Final Product Specifications must be provided
9. Price Information • The proposed price for Alberta (which must be in compliance with the Price Policy)

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 17 EFFECTIVE APRIL 1, 2012
10. Product Monograph (revised to include the line extension) • in addition to a hard copy, an electronic (CD) copy of the TPD-approved Product
Monograph compatible with Microsoft Word 11. Economic Information
• a completed Budget Impact Assessment for the Alberta Health and Wellness Drug Benefit List form. Note: copies of this form can be obtained by accessing the Alberta Health and Wellness Drug Benefit List website at www.ab.bluecross.ca/dbl/manufacturers.html, or by contacting the Coordinator, Scientific and Research Services, Alberta Blue Cross at Phone: (780) 498-8098 or Fax: (780) 498-3534.
12. If requested, the manufacturer must provide written confirmation from the CDR Directorate that the drug product is not eligible for review under the CDR Procedure.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 18
D) Interchangeable Drug Products The following submission requirements pertain to multisource drug products submitted for listing in an interchangeable grouping in the Alberta Health and Wellness Drug Benefit List.
For Expedited and Full Reviews:
1. Consent Letter • an unrestricted letter authorizing Alberta Health and Wellness and its agent/designate
to access, discuss, use, collect from, and disclose to its agents, consultants, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH) and all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services and the government of any province or territory in Canada, all submission information and information in the possession of Health Canada, CADTH, PMPRB, Alberta Health Services and the government of any province or territory in Canada
2. Letter Confirming Ability to Supply • a letter signed by a senior official providing assurance that the manufacturer is able to
supply the specific drug product and strength from the time of listing in a quantity sufficient to meet the anticipated demand in Alberta for a minimum of 6 months.
3. Copy of completed Drug Identification Number (DIN) notification form 4. Copy of Notice of Compliance (NOC)
• Note: For Old Drug Products (a drug product where the active ingredient is designated as an “old drug” by Health Canada and the drug product was approved on the basis of a DIN application), a Notice of Compliance is not required.
5. Current Patent Status • a signed statement from the manufacturer stating that the submitted product does not
infringe any patents 6. For Pseudo-Generic Drug Products: Letters from both the manufacturer of the
submission drug product and the manufacturer of the innovator brand or a currently listed drug product within the submission product’s interchangeable grouping, stating that the submission drug product is manufactured under the identical master formula and manufacturing and quality control specifications, as the innovator brand or the currently listed drug product.
7. Price Information • The proposed pricing in Alberta must be in compliance with the Price Policy.
Exceptions to the Fixed Pricing Rules may be considered at the sole discretion of the Minister. Accordingly, a request for an exception (as per sections 18-21 of the Price Policy) must accompany a submission that does not meet the Price Policy in order for it to be deemed complete.
8. Copy of completed and approved Certified Product Information Document (CPID) Note: In lieu of the CPID, a Master Formula and Final Product Specifications must be provided
9. Product Monograph • in addition to a hard copy, an electronic (CD) copy of the TPD-approved Product
Monograph compatible with Microsoft Word is required Note: For Old Drug Products, the Prescribing Information may be provided in lieu of the Product Monograph.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 19 EFFECTIVE APRIL 1, 2012
For FULL REVIEWS ONLY, the following ADDITIONAL information must be provided: 10. Evidence that the listing criteria for interchangeable drug products has been met. See
Criteria for Listing Drug Products and Interchangeable Drug Products sections for specific applicable criteria.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 20
E) Resubmissions Resubmission Requests – General 1. A resubmission request may be made for a Drug Product that is not currently listed on
the AHWDBL or List (collectively referred to as the “AHWDBL”) in a case where the Drug Product:
a. was previously listed on the AHWDBL; b. was the subject of a previous submission for listing on the AHWDBL; or c. is listed on the AHWDBL but is subject to restrictions.
2. A resubmission request: a. must comply with the requirements set out below; and b. may be made by a Manufacturer for a Drug Product only once in a 12 month
period, running from April 1st through to March 31st, unless the Minister of Alberta Health and Wellness (Minister), in the Minister’s sole discretion, invites a Manufacturer to make a resubmission request.
3. The Minister, the Expert Committee on Drug Evaluation and Therapeutics (Expert
Committee), and Alberta Health and Wellness (AHW): a. may request information in addition to the requirements set out below; and b. may from time to time set deadlines by which a resubmission request may be
made, or a request for additional information must be provided.
4. In the case where: a. additional information has been requested by the Minister, the Expert
Committee or AHW, the resubmission request is not considered to be complete unless and until the requested additional information is provided to the Minister, the Expert Committee or AHW; and
b. a deadline has been set as referred to above, failure to provide a complete resubmission request within such deadline means that a resubmission request will not be reviewed by the Expert Committee or AHW or considered by the Minister.
5. The Minister may, in the Minister’s sole discretion, refer a Drug Product, that was the
subject of a resubmission request which meets the requirements set out in this policy, to an Alberta Price Confirmation (APC) or Interim APC process.
6. In the event that a Drug Product is referred to an APC or Interim APC process, the
Manufacturer must comply with the Price Policy and the Terms and Conditions of the APC or Interim APC. A referral to an APC or Interim APC or the submission of a Price Confirmation or Confirmed Price for the Drug Product by the Manufacturer does not obligate the Minister to list a Drug Product on the AHWDBL.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 21 EFFECTIVE APRIL 1, 2012
7. In the event that the Minister, in the Minister’s sole discretion, requires additional advice or input on a resubmission request, the Minister may refer the resubmission request to the CDR Procedure, the Expert Committee or any other entity for further advice or a full review.
8. For additional clarity, the provisions outlined under the “Submissions for Drug Reviews” are also deemed to apply to resubmission requests except as specifically modified by the provisions in this subsection “E) Resubmissions”, in which case this subsection applies.
Resubmission Requests Requiring Expert Committee Review
9. In addition to the requirements in “Resubmission Requests – General” above, this section applies to a resubmission request for a Drug Product that was reviewed by the Expert Committee and a decision was made by the Minister to:
a. not add the Drug Product to the AHWDBL for reasons other than those specified
in section 12 below; b. add the Drug Product to the AHWDBL with restrictions; or c. maintain current listing status of the Drug Product on the AHWDBL despite the
Manufacturer’s request for change. 10. A general resubmission request may be made for a previously submitted Drug Product
on the Resubmission for the Alberta Health and Wellness Drug Benefit List form. The form can be obtained at www.ab.bluecross.ca/dbl/manfacturers.html or by contacting the Coordinator, Scientific and Research Services, Alberta Blue Cross by phone at (780) 498-8098 or by fax at (780) 498-3534.
11. A resubmission request must be complete and must include:
a. a completed Resubmission for the Alberta Health and Wellness Drug Benefit List form. A resubmission request requires review by the Expert Committee and a recommendation made by the Expert Committee for the Minister’s consideration for listing or not listing the Drug Product on the AHWDBL. The form must contain new information not previously submitted for a review of the Drug Product by the Expert Committee, unless otherwise indicated;
b. an unconditional consent letter authorizing AHW and its employees, contractors, consultants and agents to collect and use information respecting a Drug Product and to disclose the subject information to AHW, its employees, contractors, consultants and agents, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH), all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services (AHS) and the government of a province or territory in Canada. Information that may be collected, used and disclosed includes, but is not limited to, all Drug Product submission and resubmission information and information about the Drug Product in the possession of Health Canada, CADTH, all persons, parties or entities involved in the CDR Procedure, PMPRB, AHS, AHW, the Expert Committee, and the government of a province or territory;

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 22
c. a confirmation letter signed by a senior official of the Manufacturer stating that the Manufacturer is able and willing to supply the Alberta market with the subject Drug Product in a quantity consistent with applicable APC or Interim APC requirements; and
d. a revised Budget Impact Assessment (BIA) form in the case where new economic information about the Drug Product is available, that has not been previously submitted, to support the resubmission request.
Resubmission Requests based on the AHWDBL Price Policy
12. In addition to the requirements in “Resubmission Requests – General” above, this section applies to resubmission requests for a Drug Product that:
a. has not been listed on the AHWDBL, or that has been removed from the
AHWDBL, by the Minister where the requirements of an Alberta Price Confirmation (APC), Interim APC or the Price Policy were not satisfied; or
b. has been removed from the AHWDBL at the request of the Manufacturer.
13. A price policy resubmission request may be made on the Alberta Price Policy Resubmission Form for the Alberta Health and Wellness Drug Benefit List. The form can be obtained at www.ab.bluecross.ca/dbl/manfacturers.html or by contacting the Coordinator, Scientific and Research Services, Alberta Blue Cross by phone at (780) 498-8098 or by fax at (780) 498-3534.
14. A resubmission request must be complete and must include:
a. a completed Alberta Price Policy Resubmission Form for the Alberta Health and Wellness Drug Benefit List ;
b. an unconditional consent letter authorizing AHW and its employees, contractors , consultants and agents to collect and use information respecting a Drug Product and to disclose the subject information to AHW, its employees, contractors, consultants and agents, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH), all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services (AHS) and the government of a province or territory in Canada. Information that may be collected, used and disclosed includes, but is not limited to, all Drug Product submission and resubmission information and information about the Drug Product in the possession of Health Canada, CADTH, all persons, parties or entities involved in the CDR Procedure, PMPRB, AHS, AHW, the Expert Committee, and the government of a province or territory; and
c. a confirmation letter signed by a senior official of the Manufacturer stating that the Manufacturer is able and willing to supply the Alberta market with the subject Drug Product in a quantity consistent with applicable APC or Interim APC requirements.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 23 EFFECTIVE APRIL 1, 2012
Criteria for Listing Drug Products
• The Criteria for Listing Drug Products apply to all drug product submissions.
• If more than one criterion apply, at the sole discretion of the Expert Committee on Drug Evaluation and Therapeutics (Expert Committee), Alberta Health and Wellness or the Minister, the most stringent and/or appropriate combination of criteria will apply.
• For multisource drug products seeking a designation of interchangeability, the drug product must also meet the additional criteria outlined under “Interchangeable Drug Products”.
1. Clinical studies must have demonstrated the safety and efficacy of the product in appropriate populations. 2. The product must:
a. possess therapeutic advantage over other presently accepted therapies or treatments of the disease entity for which the product is indicated, or b. be more cost-effective than presently accepted therapy.
3. Assessment of therapeutic advantage may include consideration of: i. clinical efficacy; ii. risk/benefit ratio; iii. toxicity; iv. compliance; v. clinical outcomes; vi. Health Canada warnings and advisories; vii. population health issues; or viii. any other factor which affects the therapeutic value of the product.
4. The Expert Committee, Alberta Health and Wellness and/or the Minister may, in addition to all of the factors listed above, also consider any factors that they consider appropriate, including but not limited to any or all of the following:
i. the recommendations from the CDR review, ii. failure by a manufacturer to supply a sufficient quantity of drug product to
meet the demand in Alberta (as determined by Alberta Health and Wellness at its sole discretion, and based on any information it deems appropriate),
iii. failure by a manufacturer to provide (A) a Price Confirmation, or (B) a Price Confirmation or Confirmed Price in accordance with the Price
Policy and/or the Alberta Price Confirmation (APC) Terms and Conditions;
iv. failure by a manufacturer to comply with any APC Terms and Conditions;

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 24
v. type of drug, drug product, class or category and indications for use, vi. other available alternative products, treatments or therapies, vii. whether the product is interchangeable, viii. cost of the product and/or potential cost savings or impact on drug
expenditures under the List, ix. volume of use and amounts paid out for similar products, classes or
categories, x. utilization patterns xi. expenditure management and resources, xii. patent issues, xiii. coverage provided by other programs, xiv. for interchangeable products, concerns that are related to or affect the
interchangeability of the drug product, xv. issues, concerns, objectives, goals and/or mandates related to any
government policies, plans or programs, and xvi. patient care concerns related to factors external to the drug product.
5. New Chemical Entities, New Combination Products and other single source products not eligible for review under the CDR Procedure may, at the sole discretion of Alberta Health and Wellness and/or the Minister, be considered for priority review and possible addition to the List if the product submission is otherwise complete, and the product has been granted “Priority Review” status by the Therapeutic Products Directorate, Health Canada. A copy of documentation from the Therapeutic Products Directorate granting ‘Priority Review’ status is required.
6. The onus is on the manufacturer to formally request, in writing, consideration on a priority review basis if, in the opinion of the manufacturer, the product meets any of the above priority review criteria. Request for priority review does not automatically mean that the submission will be considered on that basis. The decision whether to conduct a priority review will be made by Alberta Health and Wellness and/or the Minister at their sole option and discretion.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 25 EFFECTIVE APRIL 1, 2012
Interchangeable Drug Products - Additional Criteria
Principle: Decisions respecting interchangeability and drug lists remain in the domain of the institution responsible for the costs of the product which includes hospitals, provincial governments and other third party payers (6/9/95 Canada Gazette Part ll, Vol. 129, No. 18) Preface: The Alberta Health and Wellness Drug Benefit List (AHWDBL) contains designations of interchangeability for approved multisource drug products. The Expert Committee on Drug Evaluation and Therapeutics makes recommendations on interchangeability to Alberta Health and Wellness through the Executive Director, Pharmaceutical Funding and Guidance Branch, Health Policy and Service Standards Division. The Minister of Health and Wellness makes the final decisions on interchangeability after reviewing the recommendations of the Expert Committee and/or Alberta Health and Wellness. Definitions: (Note: additional definitions in the applicable Appendices may apply) Interchangeable Drug Product: An interchangeable drug product is a drug product that has been designated as interchangeable by the Minister of Health and Wellness after reviewing the recommendations of the Expert Committee or Alberta Health and Wellness. Recommendations regarding interchangeability are made taking into consideration the scientific, therapeutic, clinical and socio-economic merits of drug products in accordance with the published criteria. Drug products designated as interchangeable are expected to be safe when interchanged with other drug products in the interchangeable grouping, and to have the same therapeutic effectiveness when administered to patients under the conditions specified in the labeling. The designation of interchangeability is made only for the purpose of funding of drug benefits covered under the Alberta government-sponsored drug benefit programs and is not to be used as a scientific reference or prescribing guide. Multisource Drug Product: Drug products are considered to be multisource drug products when they are manufactured and/or distributed by more than one manufacturer. Pharmaceutical Alternative: Drug products may be considered to be pharmaceutical alternatives if they use the same route of administration and contain the same active therapeutic ingredient(s) but are different salts, esters or complexes of that moiety, or are different dosage forms or strengths. Pharmaceutical Equivalent: Drug products are considered to be pharmaceutical equivalents if they contain the same active therapeutic ingredient(s), are of comparable dosage form(s), route of administration and are identical in strength or concentration. Pseudo-Generic Drug Product: A pseudo-generic drug product is a drug product that is manufactured under the identical master formulae and manufacturing and quality control specifications as a) the innovator brand of the drug; or b) any drug product that is currently listed on the AHWDBL within the submission product’s interchangeable grouping.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 26
TPD Reports - refers collectively to the following Health Canada Therapeutic Products Directorate (TPD) guidance publications as of December 31, 2009: o Conduct and Analysis of Bioavailability and Bioequivalence Studies - Part A: Oral
Dosage Formulations Used for Systemic Effects, and Part B: Oral Modified Release Formulations; (which may be referred to in the List as “TPD Part A”, and “TPD Part B”); and
o Report C: Report on Bioavailability of Oral Dosage Formations, Not in Modified Release Form, of Drugs used for System Effects, Having Complicated or Variable Pharmacokinetics (which may be referred to in the List as “TPD Report C”); and
o Bioequivalence Requirements: Comparative Bioavailability Studies Conducted in the Fed State. Interchangeable Reviews:
A. The Expert Committee and/or Alberta Health and Wellness and/or the Minister may, in addition to considering the Interchangeable Drug Products criteria, also consider any other criteria in the AHWDBL, including but not limited to the Criteria for Listing Drug Products.
B. Recommendations regarding interchangeability are made taking into consideration the scientific, therapeutic, clinical and socio-economic merits of drug products in accordance with the published criteria. Drug products designated as interchangeable are expected to be safe when interchanged with other drug products in the interchangeable grouping, and to have the same therapeutic effect when administered to patients under the conditions specified in the labeling.
C. Issuance of a Notice of Compliance by the TPD which includes a Declaration of Equivalence does not mean the drug product will automatically be designated as interchangeable.
Expedited Reviews 1. Multisource drug products seeking a listing designation as interchangeable may be eligible for an expedited review if:
a. The drug product submission complies with the submission requirements.
b. The drug product does NOT fall into any of the categories of drug products that require a Full Review (below), unless the drug product is a Pseudo-Generic Drug Product.
c. The drug product is not a subsequent entry biologic (subsequent entry biologics are not eligible for review as interchangeable products).
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 27 EFFECTIVE APRIL 1, 2012
d. The drug product has been granted a Notice of Compliance by Health Canada that includes a declaration of bioequivalence with a Canadian brand/innovator reference product that is listed (or at the sole discretion of Alberta Health and Wellness and/or the Minister, has been previously listed) on the Alberta Health and Wellness Drug Benefit List.
e. The drug product must be a pharmaceutical equivalent to the Canadian innovator reference product.
f. The proposed price in Alberta provided in the manufacturer’s submission complies with the Price Policy.
g. Even if the drug submission review is expedited, Alberta Health and Wellness and/or the Minister may refuse to list a drug product, or the listing of the drug product may be delayed, if the manufacturer has failed
(A) to provide a Price Confirmation, (B) to provide a Price Confirmation or Confirmed Price in accordance with the Price
Policy and/or the applicable APC Terms and Conditions; or (C) to comply with the terms and conditions of an applicable APC.
Full Reviews Multisource drug products seeking a listing designation as interchangeable that fall within the categories listed below are required to undergo a Full Review by the Expert Committee. The following additional interchangeability criteria will apply to Full Reviews: 1. The drug product must be a
a. pharmaceutical equivalent; or b. pharmaceutical alternative,
as determined at the sole discretion of the Expert Committee. 2. The drug product is not a subsequent entry biologic (subsequent entry biologics are not
eligible for review as interchangeable products).
3. The proposed price in Alberta contained in the manufacturer’s submission complies with the Price Policy.
4. The drug product has been demonstrated to be bioequivalent, or has provided evidence of comparative therapeutic efficacy, with the reference drug product as outlined below;
a. For drug products in the following categories, for which bioequivalence studies
CAN be conducted:
i. For Critical Dose Drug Products, the drug product must meet the criteria in the Critical Dose Drug Product Appendix.
ii. For Non-Linear Drug Products, the drug product must meet the criteria in the Non-Linear Drug Product Appendix.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 28
iii. For Rapid Onset Drug Products, the drug product must meet the criteria in the Rapid Onset Drug Product Appendix.
iv. For Drug Products for which Bioequivalence is Supported by Metabolite Data, the drug product must meet the criteria in the Drug Products with Metabolite Data Appendix.
v. For Drug Products for which Bioequivalence is Supported by Measurement of the Drug in a Matrix other than Plasma or Serum (e.g., Whole Blood, Urine, Tissue), the drug product must meet the criteria in the Drug Product with Alternate Matrix Measurement Appendix.
vi. For Old Drug Products, the product must meet the criteria in the Old Drug Product Appendix.
vii. For Drug products which possess complex delivery systems, the product must meet the criteria in the Complex Delivery System Drug Product Appendix.
b. For drug products in the above categories for which bioequivalence studies
CANNOT be conducted:
i) Evidence of comparative therapeutic efficacy of the submitted product with the reference product via:
(A) a therapeutic equivalence study; or (B) Studies that meet the requirements and standards for pharmacodynamic studies outlined in TPD Report C;
and
ii) Sufficient rationale for why a bioequivalence study cannot be conducted.
c. For drug product submissions using a Non-Canadian Reference Product (NCRP):
i) An NCRP may only be used when it meets the Criteria for use of a Non-
Canadian Reference Product as set out in Health Canada’s Drugs Directorate Policy regarding the use of a Non- Canadian Reference Product under the provisions of Section C.08.002.1(c) of the Food and Drug Regulations (the “NCRP Criteria”). See also Interpretation Notice #1.
ii) If the NCRP Criteria is met, the drug product must demonstrate bioequivalence to the NCRP through studies that meet the requirements and standards of the applicable TPD Reports.
5. The drug product must meet all other criteria outlined in the applicable Appendix.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 29 EFFECTIVE APRIL 1, 2012
6. In addition, the Expert Committee may also consider any other factor that may affect the interchangeability of a drug product, including but not limited to:
• characteristics of the drug product (e.g. shape, scoring, configuration, packaging, labelling);
• excipients and non-medicinal ingredient(s) (e.g. sugar, sodium); • expiration times; • storage conditions.
Interchangeable Drug Products - Additional Criteria APPENDICES
Critical Dose Drug Product Appendix Critical Dose Drug: Is a drug where comparatively small differences in dose or concentration lead to dose- and concentration-dependent, serious therapeutic failures and/or serious adverse drug reactions which may be persistent, irreversible, slowly reversible or life threatening, which could result in inpatient hospitalization or prolongation of existing hospitalization, persistent disability or incapacity, or death. Critical dose drugs include:
a) Any drug listed in Appendix I - List of Critical Dose Drugs of Health Canada’s Guidance for Industry entitled Bioequivalence Requirements: Critical Dose Drugs; and
b) Any other drug that the Expert Committee determines meets the above definition, which determination may include consideration of any other matter that may affect the interchangeability of a product containing a critical dose drug.
Criteria: Bioequivalence studies must meet the requirements and standards in the TPD Reports, with the exception that the following standards will be used: 1. The 90% confidence interval of the relative mean AUC of the test to reference formulation
should be within 90.0 to 112.0%; the relevant AUC or AUCs as described in TPD Reports A and B are to be determined.
2. The 90% confidence interval of the relative mean measured Cmax of the test to reference formulation should be between 80.0 and 125.0%.
3. These requirements are to be met in both the fasted and fed states. 4. These standards should be met on log transformed parameters calculated from the
measured data and from data corrected for measured drug content (percent potency of label claim).
5. If a steady-state study is required, the 90% confidence interval of the relative mean measured Cmin of the test to reference formulation should also be between 80.0 and 125.0%.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 30
Non-Linear Drug Product Appendix Non-Linear Drug: A drug is considered to be a Non-Linear Drug if the Health Canada approved product monograph for the Canadian innovator drug product states that it is a non-linear drug. Criteria: 1. Bioequivalence studies must meet the requirements and standards in the TPD Reports, and these requirements and standards should be met in single dose studies in both the fasted and fed states, with the following exceptions:
a) if non-linearity occurs after the drug enters the systemic circulation, a fed study may be waived unless there is sufficient evidence, at the Expert Committee’s sole discretion, that a product exhibits a food effect; or b) if a condition (fasted or fed) for product ingestion is contraindicated, that condition may be waived in a bioequivalence trial. For bioequivalence testing the fasting and fed doses should be the same.
2. At the sole discretion of the Expert Committee, it may be acceptable to conduct bioequivalence studies at either the highest or lowest strength of a range of proportionally formulated strengths as outlined below:
a) For drugs with non-linear pharmacokinetics in the single unit dose range of approved strengths resulting in greater than proportional increases in AUC with increasing dose, the bioequivalence studies should be conducted on at least the highest strength. That is, where non-linearity arises from capacity-limited clearance, the highest strength for the proposed indications should be tested. For drugs where the non-linear concentration range is reached only after multiple doses within the approved dosing regimen, studies utilizing multiple units of the highest formulation strength or steady-state studies in the non-linear range may be required. Where steady-state studies are conducted, single dose studies will not be required. In all situations, safety in dosing should be considered.
b) For drugs with non-linear pharmacokinetics in the single unit dose range of approved strengths resulting in less than proportional increases in AUC with increasing dose, the bioequivalence studies should be conducted on at least the lowest strength (single dose unit). That is, where non-linearity arises from capacity-limited absorption, the test dose should be a single unit of the lowest strength.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 31 EFFECTIVE APRIL 1, 2012
Rapid Onset Drug Product Appendix
Rapid Onset Drugs: Are as defined in TPD Report C. Criteria: Bioequivalence studies must meet the requirements and standards in the TPD Reports, except that the relative mean AUCReftmax of the test to reference formulation should be within 80 to 125%, where AUCReftmax for a test product is defined as the area under the curve to the time of the maximum concentration of the reference product, calculated for each study subject.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 32
Drug Product with Metabolite Data Appendix For drug product submissions for which evidence of bioequivalence is supported by metabolite, rather than the parent drug, data. Criteria:
1. Bioequivalence studies must meet the requirements and standards in the TPD Reports.
2. If the parent drug is not detectable due to rapid biotransformation or limitations in available assay methodology, the use of metabolite data may be acceptable.
3. The measured metabolite must be a primary (first step) measureable by a validated assay, and there must be sufficient scientific justification for a waiver of the measurement of the parent drug and the use of metabolite data.
4. The choice of using the metabolite instead of the parent drug is to be clearly stated, a priori, in the objective of the study in the study protocol.
5. The use of metabolite concentrations in urine is not acceptable.
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 33 EFFECTIVE APRIL 1, 2012
Drug Product with Alternate Matrix Measurement Appendix
For drug product submissions for which bioequivalence data is supported by measurement of the drug in a matrix other than plasma or serum (e.g., whole blood, urine, extravascular tissue). Criteria:
• Bioequivalence studies must meet the requirements and standards in the TPD Reports.
• The assay used for measurement of the drug (or metabolite) must be validated for the alternate matrix of measurement.
• Sufficient rationale for why the use of an alternate matrix measurement study is appropriate.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 34
Old Drug Product Appendix Old Drugs: Are drug products where the active therapeutic ingredient(s) is designated as an “old drug” by Health Canada and the drug product is approved on the basis of a DIN application (i.e. an NOC is not issued by Health Canada). Criteria:
1. Bioequivalence studies must meet the requirements and standards in the TPD Reports.
2. For old drug products for which bioequivalence studies CANNOT be conducted, the submission must include:
i) Evidence of comparative therapeutic efficacy of the submitted product with the reference product via:
(A) a therapeutic equivalence study; or (B) studies that meet the requirements and standards for pharmacodynamic studies outlined in TPD Report C; or (C) surrogate comparisons using in vivo or in vitro test methods.
and
ii) Sufficient rationale for why a bioequivalence study cannot be conducted.
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 35 EFFECTIVE APRIL 1, 2012
Complex Delivery System Drug Product Appendix Complex Delivery System Drugs: Are drug products that possess complex drug release characteristics in the pharmaceutical dosage form that are intended to:
(1) deliver the drug at a rate that is independent of time and the concentration of the drug (i.e. zero order process), or (2) deliver the drug to a specific physiological site (i.e. site-specific release).
Criteria: 1. Bioequivalence studies must meet the requirements and standards in the TPD Reports. 2. A detailed description of the pharmaceutical dosage forms and specific drug release characteristics of the submitted drug product and reference drug product must be provided to permit evaluation of the similarity of drug release of the respective formulations.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 36
Review of Benefit Status (ROBS) Criteria
The Expert Committee and/or Alberta Health and Wellness may at any time review the benefit status of a drug product, a group of drug products, a class or classes of drug products, or a category or categories of drug products listed or being considered for listing on the AHWDBL (collectively “Products”). The Expert Committee and/or Alberta Health and Wellness may, at their sole option and discretion, recommend altering or discontinuing the benefit status for Products if one or more of the following criteria are met. These are general criteria only, which are intended to be applied flexibly, having regard to each individual case. The criteria may be modified or adapted as the situation may require, and not all criteria will apply to each case:
1. There has been a significant change to the Product(s). Significant changes may include changes in NOC, DIN, product name, manufacturer or distributor, indication, product monograph, packaging, formulation, or any change that could potentially affect the bioavailability or bioequivalence of a product.
2. The Product(s), no longer possesses demonstrated therapeutic advantage compared to other presently accepted therapies or treatments of the disease entity for which the Product(s) is/are indicated. Assessment of therapeutic advantage may include consideration of clinical efficacy, risk/benefit ratio, toxicity, compliance, clinical outcomes, Health Canada advisories, population health issues, and any factor which affects the therapeutic value of the product, class or category.
3. The Product(s) is/are no longer cost-effective compared to other presently accepted therapies or treatments of the disease entity for which the Product(s) is/are indicated.
4. To enable broader coverage of higher priority Product(s). 5. When a product has been discontinued by the manufacturer. 6. When Product(s) is/are changed from prescription to non-prescription status, the Expert
Committee may recommend continuing, altering or discontinuing benefit status of the Product(s) based upon scientific, therapeutic, clinical and socio-economic merits of the Product(s).
7. For all ROBS reviews, the Expert Committee, Alberta Health and Wellness and/or the Minister may, in addition to all of the factors listed above, also consider any factors that they consider appropriate, including but not limited to any of the criteria for listing drug products and interchangeable drug products.
Unsolicited information from manufacturers relating to ROBS Reviews will not be put before the
Expert Committee. However, if the Expert Committee determines that a change in benefit status
may be warranted, manufacturers of the affected Product(s) will be notified and provided with an
opportunity to make submissions to the Expert Committee prior to the final recommendation
being made. Notification will include advice regarding the form of submission that will be
accepted, the deadline for filing the submission and any other relevant advice. Any submissions
that do not comply with the notification advice will not be put before the Expert Committee.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 37 EFFECTIVE APRIL 1, 2012
Supply Shortages
Where a manufacturer has not supplied, or is not supplying, a sufficient quantity of drug product to meet the demand in Alberta (as determined by Alberta Health and Wellness at its sole option and discretion, and based on any information it deems appropriate):
1. If the unavailable product is a single-source product on the List, products not otherwise allowed as benefits may be added temporarily or temporarily reimbursed for the Alberta government-sponsored drug programs.
3. Products added or reimbursed under this policy may remain as temporary benefits until the supply shortage is rectified.
4. In order to remain as benefits after the shortage is rectified, manufacturers of these products must follow the usual submission and review process for listing.
5. Alberta Health and Wellness may recover any cost difference from the manufacturer unable to supply a drug product.
6. Alberta Health and Wellness may at its sole discretion, take any other steps or require any information from a manufacturer or other person, that is reasonably required to manage a supply shortage.
7. Alberta Health and Wellness may:
• refuse to list any product of the manufacturer, • refuse to consider any product submission of the manufacturer for expedited or
priority review; or • cancel or modify the listing of the product that is not meeting the supply demand.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 38
Units of Issue for Pricing
These units of issue are used for presenting prices in the List. Dosage Form Unit of Issue Priced in AHWDBL
Ampoules ............................................................. Millilitre Bladder Irrigation Solutions .................................. Millilitre Dental Pastes ....................................................... Gram Devices................................................................. Device Inhalation Capsules .............................................. Capsule Inhalation Cartridges ............................................ Cartridge Inhalation Disks .................................................... Disk Inhalation Solutions or Suspensions .................... Millilitre – all preparations including nebules Inhalation Unit Dose Solution ............................... Millilitre Injections .............................................................. Vial – where reconstitution is required (or ………………………………………………………..Millilitre or Unit where indicated) Injections .............................................................. Millilitre – where no reconstitution is required ……………………………………………………….(or Vial where indicated) Injections – Cartridges ......................................... Millilitre Injections – Emulsion ........................................... Millilitre Injections – Syringes ............................................ Syringe (or Millilitre where indicated) Injection – Implant ................................................ System Injection Syringe/Oral Capsule ............................ Kit Injection Vial/Oral Capsule ................................... Kit Injection Vial/Oral Tablet ...................................... Kit Injection Syringe/Oral Tablet ................................ Kit Intrauterine Insert ................................................. System Irrigating Solutions ............................................... Millilitre Lock Flush ............................................................ Millilitre Metered Dose Aerosols........................................ Dose Metered Inhalation Powder .................................. Dose Nasal Metered Dose Aerosols ............................. Dose Nasal Metered or Unit Dose Sprays .................... Dose Nasal Solutions .................................................... Millilitre Nasal Sprays ........................................................ Millilitre Ophthalmic Solutions or Suspensions or Drops..................................... Millilitre Ophthalmic Gels or Ointment ............................... Gram Ophthalmic Long Acting Gellan Solutions............ Millilitre Oral Caplets ......................................................... Caplet Oral Capsules – all formulations .......................... Capsule Oral Drops ........................................................... Millilitre Oral Granules ....................................................... Bulk size – Gram ............................................................................. Individual Packet – Packet

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 39 EFFECTIVE APRIL 1, 2012
Units of Issue for Pricing, continued
Dosage Form Unit of Issue Priced in AHWDBL Oral Liquids – all formulations .................................... …...Millilitre Oral Powders .............................................................. …...Gram (or Dose where indicated) Oral Powder Packets…………………………………….. Individual Packet Oral Rinses ................................................................. …...Millilitre Oral Tablets – all formulations .......................................... Tablet Oral Tablets – oral contraceptives .................................... Tablet Oral Tablet/Capsule .......................................................... Kit Oral Wafer ........................................................................ Wafer Otic Ointments or Gels ..................................................... Gram Otic Solutions or Suspensions or Drops .................................................. Millilitre (or Vial where indicated)
Rectal Enemas ................................................................. Enema Rectal Foams .................................................................... Gram Rectal Ointments .............................................................. Gram Rectal Retention Enemas ................................................. Enema Rectal Suppositories - all formulations ............................. Suppository Scalp Lotions .................................................................... Millilitre Scalp Solutions ................................................................. Millilitre Sublingual Metered Dose Spray.........................................Dose Sublingual Tablet .............................................................. Tablet Topical Bars ...................................................................... Gram Topical Cleansers ............................................................. Millilitre Topical Creams/Ointments - all formulations ................... Gram Topical Gauzes ................................................................. Dressing Topical Gels - all formulations .......................................... Gram Topical Jellies ................................................................... Millilitre Topical Lotions.................................................................. Millilitre or Gram Topical Powders ............................................................... Gram Topical Solutions ............................................................. Millilitre Topical Washes ................................................................ Millilitre or Gram Transdermal Gel ............................................................... Gram Transdermal Patches ....................................................... Patch Vaginal Capsules or Ovules or Tablets ............................ Capsule or Ovule or Tablet Vaginal Creams or Ointments or Gels .............................. Gram Vaginal Douches............................................................... Millilitre Vaginal Ovule/Topical Cream ........................................... Kit Vaginal Slow Release Rings ........................................... Ring Vaginal Suppositories ....................................................... Suppository

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 40
Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics: Policy for Administering Interchangeability Challenges
Note: This Policy is not applicable for drug products that are eligible for, and are reviewed under, the Expedited Review Process for interchangeable drug products. From time-to-time, the Expert Committee on Drug Evaluation and Therapeutics receives unsolicited information (“Challenge Information”) from a manufacturer (the “Challenger”) suggesting that additional information should be taken into account when a submission for interchangeability for a multisource product is being considered by the Expert Committee. Alberta Health and Wellness is not prepared to have any Challenge Information considered by the Expert Committee unless the manufacturer whose product is being challenged (the “Applicant”) is provided with a full copy of the Challenge Information and is given an opportunity to respond to it.
As a result, Alberta Health & Wellness has developed and approved the following process for the handling of Challenge Information.
1. Challenge Information must comply with the following conditions. 2. Challenge information must be received by Alberta Blue Cross:
• For first-entry interchangeable product submissions – Within 15 days of the date of issuance of the NOC for the Applicant’s product.
• For all other submissions, by the submission deadline date. 3. All Challenge Information must include an unconditional Written Consent
4. If the above unconditional Written Consent is not submitted as required, the Challenge Information will not be considered by the Expert Committee.
, signed by the Challenger, authorizing Alberta Health and Wellness and its agent/designate to (a) disclose to the Applicant all Challenge Information; and (b) to access, discuss, use, collect from, and disclose to its agents, consultants, Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH) and all persons, parties or entities involved in the CDR Procedure, the Patented Medicine Price Review Board (PMPRB), Alberta Health Services and the government of any province or territory in Canada, all submission information and Challenge Information and any information in the possession of Health Canada, the Canadian Agency for Drugs and Technologies in Health (CADTH), the Patented Medicine Price Review Board (PMPRB), Alberta Health Services and the government of any province or territory in Canada.
5. If Written Consent is submitted as required, the Challenge Information will be duplicated in its entirety and forwarded by Alberta Blue Cross to the Applicant, inviting a response (“Applicant Response”). The Applicant Response must be received by Alberta Blue Cross no later than 15 days after the date of the letter from Alberta Blue Cross.
6. If an Applicant Response is not received by Alberta Blue Cross within the time provided, only the Challenge Information will be provided to the Expert Committee for consideration. If an Applicant Response is received within the time provided, both the Applicant Response and the Challenge Information will be provided to the Expert Committee for consideration.
7. No further information may be submitted to the Expert Committee for consideration.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 41 EFFECTIVE APRIL 1, 2012
8. The Applicant Response should only address information contained in the Challenge Information. Anything in the Applicant Response that does not relate to information contained in the Challenge Information may, at the sole discretion of the Expert Committee, be disregarded.
9. It is a condition of each and every Submission and Challenge that the terms, conditions,
criteria and time limitations contained in this policy will apply and that: a) Applicants, by filing a Submission and Applicant Response; and, b) Challengers, by submitting Challenge Information agree to and are bound by this policy.
10. In the event the anticipated Applicant submission is not received, Challenge Information will be destroyed 6 months after receipt.
Inquiries may be made to: Senior Manager
Scientific and Research Services Alberta Blue Cross 10009 - 108 Street NW Edmonton AB T5J 3C5 Phone: (780) 498-5978 Fax: (780) 498-3534

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 42
Your Comments are Important to Us
To improve the high standards established for this publication, the Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics would like to offer you an opportunity for input. Should you have any concerns and/or suggestions concerning product listings or criteria for coverage of products available via special authorization, etc. please let us know.
Please note: this is not a mechanism for an appeal for a specific patient.
If you are writing in support of a product listing change or a revision to the special authorization criteria for coverage, you must provide evidence in support of your comments from the peer-reviewed scientific literature. In order to meet the expectations of stakeholders relative to objectivity and transparency, all individuals providing comments are required to advise the Expert Committee of any potential conflicts of interest below (please check appropriate box):
Conflict of Interest: Yes No If Yes, please indicate the nature of the potential conflict of interest below:
____________________________________________________________________________________ ____________________________________________________________________________________ Please provide your comments in the space provided below:
____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ Contact Information: Name and Address: __________________________________________________________________ Phone/Fax: __________________________________________________________________________ Please print form and mail/fax to: Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics c/o Senior Manager
Scientific and Research Services Alberta Blue Cross 10009 108 Street NW Edmonton, Alberta T5J 3C5 FAX to: (780) 498-3534

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 43 EFFECTIVE APRIL 1, 2012
AHWDBL - Updated Price Policy
Effective February 9, 2012 PRICE POLICY ____________________________________________________ DEFINITIONS In this Price Policy,
Alberta Blue Cross or ABC or Blue Cross means the ABC Benefits Corporation, Alberta Health and Wellness Drug Benefit List, List or AHWDBL means, unless otherwise indicated, the most recent drug benefit list (including drug benefit listing policies and processes and benefit supplements) published by the Minister from time to time, Alberta Price Confirmation or APC means an Alberta Price Confirmation that may be issued by the Minister from time to time, APC Terms and Conditions means the terms and conditions outlined in an APC, Base Cost means the price per unit of issue, less any permitted Distribution Allowance, submitted in respect of a Drug Product in a Drug Product submission or in a prior APC (whichever is most recent), Brand Drug means an originator/brand Drug Product listed or under consideration for listing in the AHWDBL, Brand Price means the price of the Brand Drug published in the February AHWDBL in an Established IC Grouping or, if there is more than one originator/brand product in the Established IC Grouping, the Brand Price is the lowest published price of a Brand Drug in the Established IC Grouping,
Confirmed Price means a Confirmed Price as set out in clause 3, Distribution Allowance means the amount that may be included in a Price Confirmation where permitted by this Price Policy, Device means a product approved by Health Canada as a device and listed or under consideration for listing by the Minister on the AHWDBL, Drug Product means anything that is listed or under consideration for listing by the Minister on the AHWDBL,
Drug Program Act or DPA means the Drug Program Act of Alberta,

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 44
Effective Brand Price means the price of the Brand Drug published in the AHWDBL in the New IC Grouping effective the date Alberta Blue Cross received the IC Drug submission or submissions (that trigger the creation of the New IC Grouping) in accordance with the AHWDBL submission requirements or, if there is more than one Brand Drug, the Effective Brand Price is the published price of the lowest priced Brand Drug in the New IC Grouping, Effective Period means the Effective Period stated in an APC, Entry IC Drug means a Drug Product that is listed or under consideration for listing in a New IC Grouping, Established IC Grouping means an IC Grouping that was established on or before February 9, 2012 and listed in the February AHWDBL, February AHWDBL means the last AHWDBL published by the Minister on or before February 9, 2012, Fixed Price means the applicable Fixed Price as set out in the Fixed Pricing Rules, IC Drug means a Drug Product that is listed, or is under consideration for listing, as interchangeable with one or more Drug Products as determined by the Minister in accordance with the requirements relating to interchangeability in the AHWDBL, IC Grouping means a category on the AHWDBL where there are two or more IC Drugs listed or under consideration for listing as part of one grouping on the AHWDBL as determined by the Minister, Interim APC means an APC issued by the Minister for one or more Drug Products, or one or more categories or groupings of Drug Products during an Effective Period, Interim APC Terms and Conditions means the terms and conditions outlined in an Interim APC, Least Cost Alternative Price or LCA Price means the maximum amount established by the Minister which will be paid by the Government of Alberta for a Drug Product in an Established IC Grouping or New IC Grouping for members of a Plan, Licensed Pharmacy means a pharmacy that is licensed or required to be licensed under the Pharmacy and Drug Act of Alberta, List has the same meaning as “Alberta Health and Wellness Drug Benefit List”, MAC Grouping means a grouping of Drug Products that have been listed in the AHWDBL and are subject to a MAC Price; a MAC Grouping may include a grouping of IC Drugs, in which case the grouping shall be treated as an Established IC Grouping, Manufacturer means an entity that manufactures, sells or distributes a Drug Product,
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 45 EFFECTIVE APRIL 1, 2012
Maximum Allowable Cost Price or MAC Price means the maximum amount established by the Minister that will be paid by the Government of Alberta for a Drug Product in a MAC Grouping for members of a Plan, Maximum Term means the Maximum Term stated in an APC. Minister means Her Majesty the Queen in Right of Alberta, as represented by the Minister of Health and Wellness, New IC Grouping means an IC Grouping that was established or may be established after February 9, 2012, Other Drug means a Drug Product that is not an IC Drug, an Entry IC Drug, or a Brand Drug listed or under consideration for listing on the AHWDBL. For further clarity, the status of an Other Drug Product changes to that of an IC Drug when another IC Drug is listed or under consideration for listing in the same grouping as the Other Drug, which grouping becomes an IC Grouping, Plan means a plan or program for which the Government of Alberta provides benefits in respect of Drug Products listed on the AHWDBL, Price Confirmation means the package of documents identified in an APC which must be completed and submitted in accordance with this Price Policy and the APC Terms and Conditions, Product Listing Agreement or PLA means a product listing agreement that is entered into or may be entered into by the Minister in respect of any Drug Product in accordance with the Minister’s Product Listing Agreement Policy, including any Drug Product that is listed or under consideration for listing on the AHWDBL, Product Listing Agreement Policy means any product listing agreement policy (including any processes related thereto) that may be published by the Minister from time to time.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 46
ALBERTA PRICE CONFIRMATION (APC) 1. The Minister may from time to time issue an Alberta Price Confirmation (APC), where a
Manufacturer will be invited to submit a Price Confirmation, with one or more Confirmed Prices, in accordance with the APC Terms and Conditions.
2. The Manufacturer must ensure that a Price Confirmation and a Confirmed Price submitted by a Manufacturer comply with this Price Policy and the APC Terms and Conditions.
3. For purposes of an APC and submitting a Price Confirmation, and subject to exceptions permitted by and approved under the Price Policy, the Confirmed Price for a Drug Product is:
a. For a Drug Product subject to the Fixed Pricing Rules, a price that is less than or equal to the Fixed Price (per unit of issue) as defined in the Price Policy (and shown in the Base Cost column of the electronic APC that may be accessed through the Alberta Blue Cross Manufacturer/vendor Online Services web site).
A Distribution Allowance is not permitted.
b. For a Drug Product subject to the Non-Fixed Pricing Rules:
i. either
(a) the Base Cost, or
(b) a revised Base Cost, as set out in section 22,
both of which must not exceed the highest price permitted in the Non-Fixed Pricing Rules;
and
ii. where permitted, a Distribution Allowance which must not exceed the amount permitted by this Price Policy.
4. In addition, a Confirmed Price:
a. is applicable to a Drug Product regardless of the package size for each Drug Product;
and b. must not include the Goods and Services Tax (GST) or any other tax.
5. Exceptions to the Fixed Pricing and Non-Fixed Pricing Rules may be requested. 6. If an exception is requested for a Drug Product in a Price Confirmation, but is not approved
by the Minister, the Manufacturer will not be given another opportunity to submit a new Price Confirmation or a new Confirmed Price in respect of such Drug Product, unless:
a. the Minister, at the Minister’s sole discretion, determines it is advisable to do so; or b. the Manufacturer follows the applicable resubmission process referred to in the
AHWDBL.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 47 EFFECTIVE APRIL 1, 2012
7. The Minister may, in his sole discretion, extend the duration of the Effective Period for a period, or periods, of time up to and including the last day of the Maximum Term.
8. (a) The Manufacturer is responsible for ensuring that sufficient supply of a Drug Product, for which a Confirmed Price has been submitted, is available for the Alberta market for the duration of the Maximum Term.
(b) If the Manufacturer anticipates that it may be unable to comply with the provisions of section 8(a), the Manufacturer must advise Alberta Blue Cross immediately in writing.
9. The Manufacturer agrees and warrants that the Confirmed Price is the maximum price at which the Drug Product will be available for sale to a Licensed Pharmacy for the duration of the Maximum Term.
10. Further, the Manufacturer agrees that it will take all necessary steps to ensure that any distributor, wholesaler or other person with whom it enters into a contract or any other arrangement, including (without limitation) the transfer or assignment of any or all rights and/or obligations in connection with a Drug Product that is listed on the AHWDBL:
i. makes the Drug Product available for sale to a Licensed Pharmacy, for the duration of the Maximum Term, at a price that does not exceed the Confirmed Price, and
ii. complies with the Price Policy and all the APC Terms and Conditions relating to such Drug Product.
11. The Minister may consider a Price Confirmation or Confirmed Price and may, at the
Minister’s sole discretion:
a. accept none, one or more Price Confirmations (with or without any request for an exception to the Fixed Pricing or Non-Fixed Pricing Rules (as applicable)); and
b. accept none, one or more Confirmed Prices (with or without any request for an exception to the Fixed Pricing or Non-Fixed Pricing Rules (as applicable)) submitted in one or more Price Confirmations.
12. Notwithstanding the acceptance of a Confirmed Price, the Minister is not obligated to pay
that price for members of a Plan, but may establish special or exceptional prices, including but not limited to establishing:
a. an LCA Price, b. a MAC Price, or c. a special or exceptional price.
13. When considering a Price Confirmation or Confirmed Price for acceptance, and in determining whether to establish an LCA Price, a MAC Price, or a special or exceptional price, the Minister may consider any factor or criteria outlined in the AHWDBL, any matter permitted by the Drug Program Act, or any matter that the Minister determines is in the public interest.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 48
INTERIM APC 14. Notwithstanding the acceptance of a Price Confirmation, or all or part of a Price Confirmation,
or one or more Confirmed Prices, in the event that:
a. a new Drug Product is being considered for listing in an Established IC Grouping, New IC Grouping or MAC Grouping,
b. a Manufacturer submits a price reduction in accordance with this Price Policy for a Drug Product listed in an Established IC Grouping, New IC Grouping or MAC Grouping, or
c. for any reason that the Minister determines that it is advisable to do so,
the Minister may, at the Minister’s sole discretion, issue an Interim APC for one or more Drug Products, or one or more groupings of Drug Products, and extend the Effective Period pursuant to section 7.
15. If a Manufacturer submits a new Drug Product submission for review and listing on the AHWDBL, and an Interim APC is issued, the Manufacturer must submit a Confirmed Price for that Drug Product that:
a. is equal to or less than the price as outlined in the Drug Product submission, and b. does not exceed the prices permitted under this Price Policy,
or the Drug Product may not be listed or the listing of the Drug Product may be delayed.
16. When an Interim APC is issued, all Manufacturers who have a Drug Product listed in the affected Established IC Grouping, New IC Grouping or MAC Grouping will be invited, but are not required, to submit a new Price Confirmation and Confirmed Price for the affected Drug Product, and in the event that a new Price Confirmation for an affected Drug Product is not submitted, or if a Price Confirmation with the same Confirmed Price for the affected Drug Product is submitted, then the Confirmed Price shown in the most recent AHWDBL (prior to the issuance of the Interim APC) shall continue to apply to the affected Drug Product.
17. In the event the Minister issues an Interim APC, and a Price Confirmation or all or part of a Price Confirmation, or one or more Confirmed Prices are accepted as a result of the Interim APC, the Interim APC Terms and Conditions supercede any previous APC or Interim APC Terms and Conditions for the affected Drug Products for the remainder of the Effective Period, with the exception of an affected Drug Product that continues to subsist on the AWHDBL in accordance with the provisions of section 16. For further clarity, this provision does not affect the Minister’s unfettered discretion at any time to make any decisions or take any steps including (without limitation) to amend a published price, an LCA Price, a MAC Price, the Price Policy, the Product Listing Agreement Policy, the AHWDBL or make any other adjustments the Minister considers advisable.
18. Publication of amended Confirmed Prices is at the discretion of the Minister.
19. Unless permitted in this Price Policy or by the Minister, at the Minister’s sole discretion, a Price Confirmation and a Confirmed Price may not exceed a Price Confirmation and a Confirmed Price for a Drug Product that has been submitted and approved by the Minister through a prior APC relating to such Drug Product.
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 49 EFFECTIVE APRIL 1, 2012
20. The provisions in this Price Policy that apply to an APC also apply to an Interim APC, and where the term APC is used in such sections, it shall be deemed to read Interim APC in the case of an Interim APC. This section does not apply to section 17.
FIXED PRICING RULES
21. The Fixed Pricing Rules apply to any Drug Product, other than any Brand Drug or Other Drug, that is listed or under consideration for listing on the AHWDBL. Effective April 1, 2012, a Confirmed Price:
a. must not exceed the Fixed Price as follows:
i. For an IC Drug listed or under consideration for listing in an Established IC Grouping , the Fixed Price will be less than or equal to:
A. the published price of such Drug Product on February 9,
2012, where the Drug Product was listed in an Established IC Grouping in the February AHWDBL;
B. the LCA Price of the applicable Established IC Grouping
on February 9, 2012, where the Drug Product was not (or will not be) listed in the Established IC Grouping prior to March 31, 2012;
C. in the case of a Drug Product:
a. for which a Price Confirmation and a Confirmed Price was submitted in response to the Interim APC issued on February 1, 2012; and
b. that is listed on the AHWDBL, pursuant to that
Interim APC, prior to March 31, 2012, the price of the such Drug Product that is published on the AHWDBL as of March 31, 2012; or
ii. For an Entry IC Drug, the Fixed Price will be less than or equal to:
A. 45% of the Effective Brand Price, where the Drug Product is under consideration for listing in a New IC Grouping which includes or will include a Brand Drug; or
B. 45% of the Effective Other Drug Price, where the Drug Product is under consideration for listing in a New IC Grouping which includes or will include an Other Drug; and
b. must not include a Distribution Allowance.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 50
NON-FIXED PRICING RULES (FOR BRAND DRUGS AND OTHER DRUGS)
22. Effective April 1, 2012, the Confirmed Price for a Brand Drug and an Other Drug must comply with the following:
a. The Confirmed Price must be less than or equal to:
i. the Base Cost; or
ii. a revised Base Cost may be submitted that is equal to (i) the Base Cost plus (ii) a percentage (%) of the Base Cost that is equal to the annual average percentage change from the previous year of the Consumer Price Index for Canada, all items, not seasonally adjusted, published by Statistics Canada.
b. The Confirmed Price may include a Distribution Allowance if:
i. the Manufacturer confirms through the Price Confirmation that it
distributes or sells the Drug Product only through a licensed wholesaler; and
ii. the Distribution Allowance does not exceed 7.5% of either the Base Cost
or revised Base Cost (as applicable) permitted under clause 22.a.
c. The Confirmed Price in respect of a Drug Product may only increase once per 12 month period commencing on April 1st in one year and continuing through March 31st
in the next year, and must be submitted through a Price Confirmation. EXCEPTIONS
23. Notwithstanding the Fixed Pricing Rules and the Non-Fixed Pricing Rules, exceptions to the Fixed Pricing Rules and Non-Fixed Pricing Rules may be considered at the sole discretion of the Minister. Where an exception is requested, the Minister reserves the right to request such additional evidence and information in support of such request as he deems appropriate.
24. The Minister may, but is not required to, consider exceptions where:
a. For an Entry IC Drug, there was a decrease of greater than 20% in the price of the Brand Drug or the Other Drug (as applicable) published in the AHWDBL within the 12 months preceding the date that the Drug Product submission in respect of the Entry IC Drug was received by Alberta Blue Cross;
b. For an IC Drug, all Drug Products in the Established IC Grouping or New IC Grouping have
i. less than 250 claims1
ii. an annual net cost; and
2
1 “claims” means the total number of prescriptions submitted for reimbursement to the Plans for all Drug Products in the grouping.
of less than $50,000;

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 51 EFFECTIVE APRIL 1, 2012
for Plans, as calculated by the Minister and based on claims experience information provided by Alberta Blue Cross relating to Plans, for the period of time that the Drug Product was listed on the AHWDBL in the previous 12 months;
c. The manufacturing and distribution costs for a Drug Product exceed the maximum price for such Drug Product permitted by the Fixed Pricing Rules or Non-Fixed Pricing Rules (as applicable3
d. Where exceptional circumstances exist
);
4
, and the Minister determines that an exception is appropriate.
25. Exceptions will not be considered for an IC Drug if the Confirmed Price for another Drug Product in the Established IC Grouping or New IC Grouping is at or below the Fixed Price.
26. Requests for an exception may delay the listing or price publication of the Drug Product. PRICE REDUCTIONS
27. During an Effective Period (whether extended pursuant to section 7 or otherwise), further price reductions for Drug Products listed on the AHWDBL will be considered as follows:
a. For IC Drugs and Drug Products listed in a MAC Grouping if the proposed price is
i. 5% less than, or ii. would represent an annual net cost5
savings of more than $100,000 for the Plans, as calculated by the Minister, for the period of time that the Drug Product was listed on the AHWDBL in the previous 12 months, in comparison to
the LCA Price or MAC Price published at the time Alberta Blue Cross receives the proposed price reduction.
b. For all other Drug Products, by notifying the Minister by sending a written notice to Alberta Blue Cross.
28. Establishment of a new LCA Price or MAC Price and publication of a reduced price is subject to:
2 “cost” means the drug material cost for claims 3 Please provide a breakdown of the costs attributed to (a) the costs for each raw material separately, including that of the active pharmaceutical ingredient, (b) the cost of manufacturing (excluding costs of raw materials), (c) cost of distribution (including direct distribution fees paid to distributors but excluding all rebates/professional allowances), and (d) other (if applicable, please specify what “other” costs represent). Rebates/professional allowances must be excluded from all costs provided herein. Costs must be stated in one unit of measure consistent for all costs requested herein (for example, cost per tablet). 4 Exceptional circumstances include, but are not limited to, circumstances where, in the opinion of the Minister, significant patient safety or access concerns, or significant increased costs to the Plans could result if the Drug Product was not available on the AHWDBL. 5 “cost” means the drug material cost for claims

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 52
a. the Manufacturer submitting a Price Confirmation and a reduced Confirmed Price for the new price in accordance with the APC Terms and Conditions;
b. acceptance of the new Confirmed Price by the Minister; and c. the Minister’s sole discretion regarding the establishment of a new LCA Price or MAC
Price, and the time, place and method of publication.
MINISTER’S AUTHORITY
29. Notwithstanding anything to the contrary, where
a. no Price Confirmation and Confirmed Price is submitted in respect of a Drug Product;
b. there is a failure to submit a Price Confirmation or Confirmed Price in respect of a Drug Product in accordance with the APC Terms and Conditions,
c. there is a rejection or non-acceptance of a Price Confirmation, or of all or part of a Price Confirmation, or of one or more Confirmed Prices, or of a request for an exception to either the Fixed Pricing Rules or Non-Fixed Pricing Rules,
d. there is a failure by the Manufacturer to comply with the APC Terms and Conditions in respect of a Drug Product listed or under consideration for listing on the AHWDBL;
e. the Minister considers that a PLA that is satisfactory to the Minister must be entered into prior to and/or as a condition of the listing, or continued listing, of a Drug Product on the AHWDBL,
the Minister may, at the Minister’s sole discretion, do any one or more of the following:
i. cancel the listing of,
ii. modify the listing of,
iii. refuse to add to the AHWDBL,
iv. refuse to expedite the submission of,
v. cancel or modify the benefit payable for,
vi. modify or impose rules, terms, restrictions or conditions (including the execution of a PLA satisfactory to the Minister) relating to, or
vii. take any other action in relation to
the Drug Product for any period of time deemed appropriate by the Minister.
30. Notwithstanding any other provision in this Price Policy, and for the avoidance of doubt, the Minister, in his sole discretion, has and retains the sole right to determine all matters relating to the listing or continued listing of a Drug Product on the AHWDBL, including (without limitation) the sole right to determine:

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 53 EFFECTIVE APRIL 1, 2012
a. whether or not the Fixed Pricing Rules or the Non-Fixed Pricing Rules apply to a
Drug Product, b. whether or not a Drug Product is to be considered as an IC Drug, a Brand Drug,
or an Other Drug for purposes of this Price Policy and an APC, c. whether or not to extend the Effective Period of an APC pursuant to section 7,
and
d. whether or not a PLA must be executed as a condition of the listing or continued listing of a Drug Product on the AHWDBL.
31. For further clarity, in all cases where the execution of a PLA in respect of a Drug Product is required as a condition of the listing or continued listing of a Drug Product on the AHWDBL, the provisions of the Product Listing Agreement Policy must be satisfied. Nothing in this Price Policy is intended to limit or override the application or any provisions of the Product Listing Agreement Policy. The requirements for listing or continued listing of a Drug Product outlined in the AHWDBL, including (without limitation) this Price Policy, as well as the Product Listing Agreement Policy must be satisfied.
32. Notwithstanding anything to the contrary, and notwithstanding the acceptance of a Price Confirmation, or all or part of a Price Confirmation, or one or more Confirmed Prices, the Minister shall have the unfettered discretion to
a. make any decisions or take any steps to amend a published price, an LCA Price, a MAC Price, a special or exceptional price, the Price Policy, the Product Listing Agreement Policy, the AHWDBL or make any other adjustments the Minister considers advisable;
b. make any decisions, take any actions or steps, or do anything that is authorized by the Drug Program Act;
c. pursue, negotiate and enter into agreements with one or more Manufacturers, distributors or vendors, including (without limitation) a PLA Agreement,
d. make arrangements with other persons to provide access to Drug Products for members of the Plans,
e. make any decisions, or take any actions or steps, or do anything that the Minister considers appropriate (including, without limitation, issuing an APC), and
f. terminate an APC, a Price Confirmation, or all or part of a Price Confirmation, or one or more Confirmed Prices, or the listing of any or all Drug Products on the AHWDBL, upon 10 days written notice to any affected Manufacturer, which notice is deemed to be given by the Minister and received by the Manufacturer upon (a) publication of the written notice on the AHWDBL website operated by Alberta Blue Cross, or (b) by sending the notice via telefax to the last known telefax number of the Manufacturer, and the method of notice is at the Minister’s discretion,
in order to maintain the integrity of the AHWDBL, to ensure reasonable access to treatment for members of the Plans, or to serve the public interest.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 54
33. Subject to section 32, where the Minister amends the Price Policy during an Effective Period, the Minister shall provide Manufacturers of Drug Products listed on the AHWDBL as at that date with 30 days notice of such amendment, and the Minister may also issue an APC in relation to any Drug Product affected by such amendment.
34. The Minister reserves the right to pursue any remedies available to the Minister in the event of any non-compliance with, or any breach of, the Price Policy or APC Terms and Conditions.
35. a. The Minister, Alberta Blue Cross, and their respective officers, employees, and
agents, are not liable for any actions, damages, claims, liabilities, costs, expenses, or losses in any way, including consequential, special, indirect, incidental, punitive or special damages, costs, expenses, or losses (including, without limitation, lost profits and opportunity costs) arising out of or relating to an APC, an Interim APC, any Price Confirmation, a Confirmed Price, or the AHWDBL, even if the Minister or Alberta Blue Cross have been advised of the possibility of such damages beforehand. The provisions of this clause shall apply regardless of the form of action, damage, claim, liability, cost, expense, or loss, whether in contract, statute, tort (including, without limitation, negligence), or otherwise, and
b. in no event shall the maximum aggregate liability of the Minister, Alberta Blue Cross, and their respective officers, employees, and agents, for damages related to an APC, an Interim APC, a Price Confirmation, a Confirmed Price, or the AHWDBL be greater than $25,000, or the Manufacturer’s actual costs of preparing and submitting a Price Confirmation in response to an APC, whichever is less.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 55 EFFECTIVE APRIL 1, 2012
Least Cost Alternative (LCA) Price Policy
1. The Least Cost Alternative Price or LCA Price means the maximum amount established by
the Minister which will be paid by the Government of Alberta for a Drug Product in an Established or New IC Grouping for members of a Plan.
2. Where the Minister establishes an LCA Price in Established and New IC Groupings the LCA
Price: a. is the lowest unit cost for a Drug Product in an IC Grouping that was submitted by the
Manufacturer and accepted by the Minister in the most recent Alberta Price Confirmation.
b. appears in bold type in the far right column of the AHWDBL. c. applies to all Drug Products in the applicable IC Grouping, unless the Minister
determines that an exception should be made.
3. Where the Minister establishes an LCA Price in Established and New IC Groupings, the Government of Alberta will pay the Actual Acquisition Cost for the Drug Product to a maximum of the LCA Price.
4. Notwithstanding section 2 above, the LCA Price Policy does not apply to: • conjugated estrogens; • devices; and • injectable Drug Products with different package sizes in an IC Grouping.
5. Subject to a Special Authorization being granted pursuant to section 6, where a physician prescribes or a patient chooses an IC Drug that is priced higher than the LCA Price established by the Minister in the applicable IC Grouping, the patient will be responsible for any additional costs (being the difference in price between the higher-priced IC Drug and the LCA Price).
6. A physician may request Special Authorization if an IC Drug that is priced higher than the applicable LCA Price is essential in the care of a patient. For further information refer to the Special Authorization Guidelines section of the AHWDBL.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 56
Maximum Allowable (MAC) Price Policy
1. The MAC Price means the maximum amount established by the Minister which will be paid by the Government of Alberta for a Drug Product in a MAC Grouping for members of a Plan.
2. A MAC Grouping means a grouping of Drug Products that have been listed in the AHWDBL
or the List as being subject to a MAC Price; a MAC Grouping may include a grouping of IC Drugs, in which case the grouping shall be treated as an Established IC Grouping.
3. Where the Minister has established a MAC Price for a MAC Grouping:
a. The MAC Price appears in bold italic type and is displayed in the AHWDBL in the second column from the right where two price columns are listed. A comment in bold italic type appears following a MAC Grouping to explain the basis for establishing the MAC Price.
b. The Government of Alberta will pay the Actual Acquisition Cost for the Drug Product to a maximum of the MAC Price.
4. The MAC Price Policy applies to the following MAC Groupings:
PTC 28:08.04.92 Selected Oral Modified-Release Dosage Forms of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
• PTC 40:12 Potassium Chloride (K+) 8 mEq Oral Sustained-Release Tablets
5. Subject to a Special Authorization being granted, where a physician prescribes or a patient
chooses a Drug Product in a MAC Grouping that is priced higher- than a MAC Price established by the Minister for the applicable MAC Grouping, the patient will be responsible for any additional costs (being the difference in price between the higher-priced Drug Product and the MAC Price).
6. A physician may request Special Authorization if the Drug Product that is priced higher than
the applicable MAC Price is essential in the care of a patient. For further information refer to the Special Authorization Guidelines section of the AHWDBL.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 57 EFFECTIVE APRIL 1, 2012
RESTRICTED BENEFITS
Restricted Benefits
Selected devices or drug products are eligible benefits with restrictions in the Alberta Health and Wellness Drug Benefit List. For these products a comment is displayed in the List after the ingredient name. The comment initially states “RESTRICTED BENEFIT” and is followed by an explanation of the restriction. For an example, refer to the Legend in the Introduction section of the List.
Products Designated as Restricted Benefits
The products listed below are restricted benefits in the List.
PTC 08:18.08.20 Lamivudine 100 mg oral tablet Tenofovir Disoproxil Fumarate 300 mg oral tablet
PTC 08:18.20 Peginterferon Alfa-2A 180 mcg/0.5 ml injection syringe and 180 mg/ml injection
PTC 08:18.32 Adefovir Dipivoxil 10 mg oral tablet Entecavir 0.5 mg oral tablet PTC 12:24.04 Cyclobenzaprine HCL 10 mg oral tablet
PTC 12:92 Varenicline Tartrate 0.5 mg oral tablet Varenicline Tartrate 1 mg oral tablet
PTC 20:12.04.92 Rivaroxaban 10 mg oral tablet
PTC 28:16.08.04 Risperidone 1 mg/ml oral solution Aripiprazole 2 mg oral tablet Aripiprazole 5 mg oral tablet
PTC 28:32.28 Naratriptan HCL 1 mg and 2.5 mg oral tablet Rizatriptan Benzoate 5 mg oral tablet, 10 mg oral tablet, 5 mg oral wafer and 10 mg oral
wafer Sumatriptan Hemisulfate 5 mg/dose and 20 mg/dose unit dose nasal spray

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 58
Sumatriptan Succinate 50 mg oral tablet, 100 mg oral tablet and 6 mg/syr injection syringe Zolmitriptan 2.5 mg oral tablet, 2.5 mg oral dispersible tablet and 5 mg/dose unit dose nasal
spray PTC 48:10.24 Montelukast Sodium 4 mg oral chewable tablet, 5 mg oral chewable tablet, 10 mg oral tablet,
and 4 mg oral granule Zafirlukast 20 mg oral tablet PTC 52:08.08 Mometasone Furoate 50 mcg/dose aqueous nasal spray
PTC 52:92 Ranibizumab 2.3 mg/vial injection
PTC 56:22.92 Aprepitant/Aprepitant 80 mg/125 mg capsule
PTC 92:00 Leflunomide 10 mg oral tablet and 20 mg oral tablet
PTC 94:00 Aerosol Holding Chamber Aerosol Holding Chamber/Mask - Infant Aerosol Holding Chamber/Mask - Pediatric Aerosol Holding Chamber Mask - Adult
Limited Restricted Benefits
Selected drug products are eligible benefits with limits and restrictions in the Alberta Health and Wellness Drug Benefit List. For these products a comment is displayed in the List after the ingredient name. The comment initially states “LIMITED RESTRICTED BENEFIT” and is followed by an explanation of the limits and restrictions. For an example, refer to the Legend in the Introduction of the List.
Product(s) Designated as Limited Restricted Benefits
The product(s) listed below are limited restricted benefits in the List.
PTC 20:12.18
Clopidogrel Bisulfate 75 mg oral tablet

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1 • 59 EFFECTIVE APRIL 1, 2012
SPECIAL AUTHORIZATION GUIDELINES Special Authorization Policy
Drug Products Eligible for Consideration by Special Authorization Drug products may be considered for coverage by special authorization under one or more of the following circumstances, unless a specific product falls under the criteria for drug products not
1. The drug is covered by Alberta Health and Wellness under specified criteria (listed in the following sections). Drug Products and indications other than those specified are not eligible for consideration by special authorization.
eligible for consideration by special authorization. Please see the end of this section for information regarding drug products not eligible for consideration by special authorization.
2. The drug is normally covered by another government program or agency for a specific approved clinical condition, but is needed for the treatment of a clinical condition that is not covered by that government program or agency.
3. The drug is required because other drug products listed in the Alberta Health and Wellness Drug Benefit List are contraindicated or inappropriate because of the clinical condition of the patient.
4. The particular brand of drug is considered essential in the care of a patient, where the LCA price policy would otherwise apply. Coverage of a specific brand may be considered where a patient has experienced significant allergic reactions or documented untoward therapeutic effects with alternate brands in an interchangeable grouping. Coverage of a brand name product will not
5. A particular drug product or dosage form of a drug is essential in the care of a patient where the MAC price policy would otherwise apply. Exceptions may occur at the product level. Coverage may be considered only where a patient has experienced significant allergic reactions or documented untoward therapeutic effects with the drug product which establishes the MAC pricing.
be considered in situations where the interchangeable grouping includes a pseudo-generic to the brand name drug.
Prior approval must be granted by Alberta Blue Cross to ensure coverage by special authorization. For those special authorization requests that are approved, the effective date for authorization is the beginning of the month in which the physician’s request is received by Alberta Blue Cross.
Special authorization is granted for a defined period as indicated in each applicable special authorization drug product criteria (the “Approval Period”). If continued treatment is necessary beyond the Approval Period, it is the responsibility of the patient and physician to re-apply for coverage prior to the expiration date of the Approved Period, unless
Auto-Renewal Process
the Auto-Renewal Process or Step Therapy Approval Process apply (see below).
Selected drug products are eligible for the following auto-renewal process (for eligibility, see the Special Authorization criteria for each drug product).
1. For initial approval, a special authorization request must be submitted. If approval is granted, it will be effective for the Approval Period outlined in the drug product’s Special Authorization criteria.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1 • 60
2. As long as the patient has submitted a claim for the drug product within the preceding Approval Period (example: within the preceding 6 months), approval will be automatically renewed for a further Approval Period (example: a further 6 months). There is no need for the prescriber to submit a new request as the automated real-time claims adjudication system will read the patient’s claims history to determine if a claim has been made within the preceding Approval Period.
3. If the patient does not
make a claim for the drug product during the Approval Period, the approval will lapse and a new special authorization request must be submitted.
Step Therapy Approval Process Select drug products are eligible for coverage via the step therapy process, outlined below.
1. If the patient has made a claim for the First-Line* drug product(s) within the preceding 12 months, the claim for the step therapy drug will be approved.
2. The automated real-time claims adjudication system will read the patient’s claims history to determine if the required First-Line* drug product(s) have been claimed within the preceding 12 months.
3. Subsequent claims for drug product(s) permitted by step therapy will continue to be approved as long as the drug product has been claimed within the preceding 12 months.
4. The regular special authorization approval process will continue to be available for step therapy approvals for those patients whose First-Line* drug claims cannot be adjudicated through the automated real-time claims adjudication system.
* A First-Line drug product includes any drug(s) or drug product(s) that, under the drug product’s Special Authorization criteria, are required to be utilized before reimbursement for the drug product is permitted.
Drug Products Not Eligible for Consideration by Special Authorization The following categories of drug products are not eligible for special authorization: 1. Drug products deleted from the List. 2. Drug products not yet reviewed by the Alberta Health and Wellness Expert Committee on
Drug Evaluation and Therapeutics. This applies to: products where a complete submission has been received from the manufacturer and
the product is under review, products where an incomplete submission has been received from the manufacturer,
and products where the manufacturer has not made a submission for review.
Drug products not yet reviewed may encompass new pharmaceutical products, new strengths of products already listed, reformulated products and new interchangeable (generic) products.
3. Drug products that have completed the review process and are not included on the List. 4. Most drugs available through Health Canada’s Special Access Program. 5. Drug products when prescribed for cosmetic indications. 6. Nonprescription or over-the-counter drug products are generally not eligible.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 1
38BSpecial Authorization Procedures
A prescriber’s request for special authorization should be directed by mail or FAX to: Clinical Drug Services Alberta Blue Cross 10009 108 Street NW Edmonton, Alberta T5J 3C5
FAX: (780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free fax for all other areas
1. For most drug products, written requests from a prescriber may be submitted on the general Drug
Special Authorization Request (form number ABC 20061).
Select drug products such as Donepezil/Galantamine/Rivastigmine (form number ABC 30776), Clopidogrel (form number ABC 30786), Darbepoetin/Epoetin (form number ABC 30888), Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis (form number ABC 30902), Ezetimibe (form number ABC 30925), Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin (form number ABC 30932), Peginterferon Alfa-2a for Chronic Hepatitis C (form number ABC 30944), Etanercept for Juvenile Idiopathic Rheumatoid Arthritis (form number ABC 30948), Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis (form number ABC 30964), Select Quinolones (form number 30966), Alendronate/Raloxifene/ Risedronate/Synthetic Calcitonin Salmon Nasal Spray for Osteoporosis (form number ABC 31086), Celecoxib (form number ABC 31140), Filgrastim/Pegfilgrastim (form number ABC 31150) Fentanyl (form number ABC 31169), Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis (Form number ABC 31192), Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis (form number ABC 31195), Adalimumab for Crohn’s/ Infliximab for Crohn’s/Fistulizing Crohn’s Disease (form number ABC 31200), Rituximab for Rheumatoid Arthritis (form number ABC 31205), Imiquimod (form number ABC 31222), Dutasteride/Finasteride (form number ABC 31257), Paliperidone/Risperidone Prolonged Release Injection (form number ABC 31258), Abatacept for Juvenile Idiopathic Arthritis (form number ABC 31291), Montelukast/Zafirlukast (form number ABC 31313), Febuxostat (form number 31376), Denosumab (form number 31377), Omalizumab (form number 31406) and Eculizumab (form number ABC 31386 and ABC 31408) have a unique special authorization request form. All requests for these drug products must be submitted using the applicable form.
Special authorization request forms can be found on the following pages.
2. A separate request is required for each patient.
3. For a request for special authorization to be considered, the prescriber (an individual authorized by law to prescribe) must contact Alberta Blue Cross and provide the following information:
Patient Identification patient’s name, address and card holder’s name (if different than the patient’s), Alberta Blue Cross identification number or coverage number/client number of any other applicable
coverage (e.g. Alberta Human Services and Alberta Seniors (AISH) or Alberta Personal Health number, and
date of birth.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 1A • 2 EFFECTIVE APRIL 1, 2012
Prescriber Identification name of prescriber (e.g. physician, dentist, or optometrist), address, telephone number and FAX number (if applicable), and professional association registration number (e.g. College of Physicians and Surgeons, Alberta Dental
Association, or Alberta College of Optometrists registration number).
Drug Requested name, strength and dosage form, dosage schedule, and proposed duration of therapy.
Reason for the Request diagnosis and/or indication for which the drug is being used, information regarding previous medications which have been used
and the patient’s response to therapy where appropriate, proposed results of therapy, and any additional information that may assist in making a decision on the
request for special authorization.
39BSpecial Authorization Forms
Special Authorization forms can be found on the following pages:
Drug Special Authorization Request Form (ABC 20061) Donepezil/Galantamine/Rivastigmine Special Authorization Request Form (ABC 30776) - All
requests for donepezil HCl, galantamine hydrobromide or rivastigmine hydrogen tartrate and must be submitted using this form only.
Clopidogrel Special Authorization Request Form (ABC 30786) - All requests for clopidogrel bisulfate must be submitted using this form only.
Darbepoetin/Epoetin Special Authorization Request Form (ABC 30888) - All requests for darbepoetin or epoetin alfa must be submitted using this form only.
Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902) - All requests for abatacept, adalimumab, anakinra, etanercept, golimumab, infliximab or tocilizumab for Rheumatoid Arthritis must be submitted using this form only.
Ezetimibe Special Authorization Request Form (ABC 30925) - All requests for ezetimibe must be submitted using this form only.
Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form (ABC 30932) - All requests for peginterferon alfa-2a/ribavirin or peginterferon alfa-2b/ribavirin must be submitted using this form only.
Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form (ABC 30944) - All requests for peginterferon alfa-2a for Chronic Hepatitis C must be submitted using this form only.
Etanercept for Juvenile Idiopathic Arthritis Special Authorization Request Form (ABC 30948) - All requests for etanercept for Juvenile Idiopathic Arthritis must be submitted using this form only.
Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form (ABC 30964) - All requests for adalimumab, etanercept, golimumab or infliximab for Psoriatic Arthritis must be submitted using this form only.
Select Quinolones Special Authorization Request Form (ABC 30966) - All requests for ciprofloxacin, levofloxacin, moxifloxacin or ofloxacin must be submitted using this form only.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 3
Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon Nasal Spray for Osteoporosis Special Authorization Request Form (ABC 31086) - All requests for alendronate, raloxifene, risedronate or synthetic calcitonin salmon for Osteoporosis must be submitted using this form only.
Celecoxib Special Authorization Request Form (ABC 31140) – All requests for celecoxib must be submitted using this form only.
Filgrastim/Pegfilgrastim Special Authorization Request Form (form number ABC 31150) – All request for filgrastim or pegfilgrastim must be submitted using this form only.
Fentanyl Special Authorization Request Form (form number ABC 31169) - All requests for fentanyl or fentanyl citrate must be submitted using this form only.
Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form (ABC 31192) - All requests for adalimumab, etanercept, infliximab or ustekinumab for Plaque Psoriasis must be submitted using this form only.
Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form (ABC 31195) - All requests for adalimumab, etanercept, golimumab or infliximab for Ankylosing Spondylitis must be submitted using this form only.
Adalimumab for Crohn’s/Infliximab for Crohn’s/Fistulizing Crohn’s Disease Special Authorization Request Form (ABC 31200) - All requests for adalimumab for Moderately to Severely Active Crohn's Disease or infliximab for Moderately to Severely Active Crohn’s/Fistulizing Crohn’s Disease must be submitted using this form only.
Rituximab for Rheumatoid Arthritis Special Authorization Request Form (ABC 31205) - All requests for abatacept or rituximab for Rheumatoid Arthritis must be submitted using this form only.
Imiquimod Special Authorization Request Form (ABC 31222) – All requests for imiquimod must be submitted using this form only.
Dutasteride/Finasteride Special Authorization Request Form (ABC 31257) – All requests for dutasteride or finasteride must be submitted using this form only.
Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form (ABC 31258) – All requests for paliperidone/risperidone prolonged release injection must be submitted using this form only.
Abatacept for Juvenile Idiopathic Arthritis Special Authorization Request Form (ABC 31291) - All requests for abatacept for Juvenile Idiopathic Arthritis must be submitted using this form only.
Montelukast/Zafirlukast Special Authorization Request Form (ABC 31313) – All requests for montelukast or zafirlukast must be submitted using this form only.
Febuxostat Special Authorization Request Form (ABC 31376) – All requests for febuxostat must be submitted using this form only.
Denosumab Special Authorization Request Form (ABC 31377) – All requests for denosumab must be submitted using this form only.
Omalizumab Special Authorization Request Form (ABC 31406)- All requests for omalizumab must be submitted using this form only.
Eculizumab Special Authorization Request Form (ABC 31386) – All requests for eculizumab must be submitted using this form only.
Eculizumab Consent Form (ABC 31408) -– All requests for eculizumab must be accompanied by this form.
The following official forms are provided for your convenience to photocopy and use as required. Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please DO NOT mail or re-fax your request

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 1A • 4 EFFECTIVE APRIL 1, 2012
40BDrug Special Authorization Request Form
On the reverse is the official Drug Special Authorization Request Form (ABC 20061).
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

DRUG SPECIAL AUTHORIZATION REQUEST
Please complete all required sections to allow your request to be processed. PATIENT INFORMATION COVERAGE TYPE:
PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
NEW RENEWAL DRUG REQUEST Note: Request may or may not be approved by Alberta Blue Cross Drug(s), Dosage(s) and Duration Requested:
Diagnosis and / or Indication which drug is being used to treat: (Include applicable information regarding previous medications, patient response to therapy and proposed results of therapy.)
Additional information relating to request:
PRESCRIBER’S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 20061 (R11/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 1A • 6 EFFECTIVE APRIL 1, 2012
Donepezil/Galantamine/Rivastigmine Special Authorization Request Form
On the reverse is the official Donepezil/Galantamine/Rivastigmine Special Authorization Request Form (ABC 30776).
• All requests for donepezil HCl, galantamine hydrobromide or rivastigmine hydrogen tartrate must be submitted using the Donepezil/Galantamine/Rivastigmine Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

DONEPEZIL/GALANTAMINE/RIVASTIGMINE SPECIAL AUTHORIZATION REQUEST FORM
Please complete ALL sections to allow your request to be processed. Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross
Alberta Human Services
Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION
PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA
CARNA
ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
CITY , PROVINCE PHONE:
FAX:
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Coverage of DONEPEZIL, GALANTAMINE, RIVASTIGMINE For the treatment of Alzheimer's disease in patients with an MMSE (Mini Mental State Exam) score between 10-26 and/or an InterRAI-Cognitive Performance Scale score between 1-4. Coverage cannot be provided for two or more medications used in the treatment of Alzheimer's disease (donepezil, galantamine, rivastigmine) when these medications are intended for use in combination. Special authorization coverage may be granted for a maximum of 24 months per request. For each request, an updated MMSE score or InterRAI-Cognitive Performance Scale score and the date on which the exam was administered must be provided. Renewal requests may be considered for patients where the updated MMSE score is 10 or higher or the InterRAI-Cognitive Performance Scale is 4 or lower while on this drug.
Note: • an MMSE score below 10 or an InterRAI-Cognitive Performance Scale score greater than 4 at any time will result in discontinuation
of coverage.
PLEASE COMPLETE ALL SECTIONS TO ALLOW YOUR REQUEST TO BE PROCESSED
Indicate which drug is requested:
Donepezil Galantamine Rivastigmine
Please confirm the diagnosis for which this drug is requested: For the treatment of: Dementia of the Alzheimer’s Type other, please specify: __________________________________________________
Please provide a current MMSE or InterRAI-Cognitive Performance Scale score* and the date the exam was administered: MMSE Score: _____________________ InterRAI-Cognitive Performance Scale Score: _____________ Date of exam: _____________________ Date of exam: ______________________________________
PRESCRIBER'S SIGNATURE DATE Please forward this request to: • Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 • FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5 ABC 30776 (R12/2011) The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of Independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 1A • 8 EFFECTIVE APRIL 1, 2012
Clopidogrel Special Authorization Request Form
On the reverse is the official Clopidogrel Special Authorization Request Form (ABC 30786). • All requests for clopidogrel bisulfate must be submitted using the Clopidogrel Special
Authorization Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
CLOPIDOGREL SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE:
PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE
IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Post-Stent Coverage Section I (Must complete for requests for post-stent coverage)
For the prevention of thrombosis, for one month, when prescribed following intravascular bare metal stent placement. Patients who have received one month of coverage via the Limited Restricted Benefit will not be eligible for additional coverage under this criterion. * For the prevention of thrombosis, for up to 12 months, when prescribed following intravascular drug eluting stent (DES) placement. Patients who have received one month of coverage via the Limited Restricted Benefit may be eligible for an additional 11 months of coverage (i.e., up to 12 months of coverage) following the submission of a special authorization request. * * Special Authorization for post-stent coverage is required when the prescriber prescribing the medication is not a Specialist in Cardiology, Cardiac Surgery, Cardiovascular & Thoracic Surgery, or General Surgery; for treatment after repeat stents; or for continued coverage of up to 12 months following intravascular drug eluting stent (DES) placement.
Please indicate the type and date of the stent: Date of stenting procedure: ________________________________________
bare metal stent (1 month of coverage)
drug eluting stent (12 months of coverage)
For additional coverage, please proceed to Section II below
Other Criteria for Coverage For the prevention of cerebrovascular (e.g. stroke, TIA) and non-cerebrovascular ischemic events in patients who have a contraindication to ASA. Special Authorization for this criterion may be granted for 24 months. For use in patients who have experienced a non-cerebrovascular ischemic event while on ASA. Special Authorization for this criterion may be granted for 24 months. For use in patients who have experienced a cerebrovascular ischemic event (e.g. stroke, TIA) while on dipyridamole/ASA (Aggrenox) or for whom dipyridamole/ASA (Aggrenox) is contraindicated. Special Authorization for this criterion may be granted for 24 months. Coverage will not be considered when clopidogrel and ASA/dipyridamole are intended for use in combination. Section II (Complete ALL that apply) Does this patient have a contraindication/intolerance to ASA? YES NO
Please indicate the cerebrovascular ischemic event experienced: Please specify the non-cerebrovascular ischemic event experienced:
stroke TIA
Did the cerebrovascular event occur while this patient was on dipyridamole/ASA (Aggrenox)?
Please indicate which anti-platelet therapy this patient was on when the non-cerebrovascular event occurred:
YES NO ASA other (specify):_____________________________
If applicable, please indicate which product this patient has a contraindication/intolerance to: Patient was not on anti-platelet therapy
dipyridamole/ASA (Aggrenox) dipyridamole
PRESCRIBER 'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30786 (R11/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 1A • 10 EFFECTIVE APRIL 1, 2012
Darbepoetin/Epoetin Special Authorization Request Form
On the reverse is the official Darbepoetin/Epoetin Special Authorization Request Form (ABC 30888). • All requests for darbepoetin or epoetin alfa must be submitted using the Darbepoetin/Epoetin
Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.
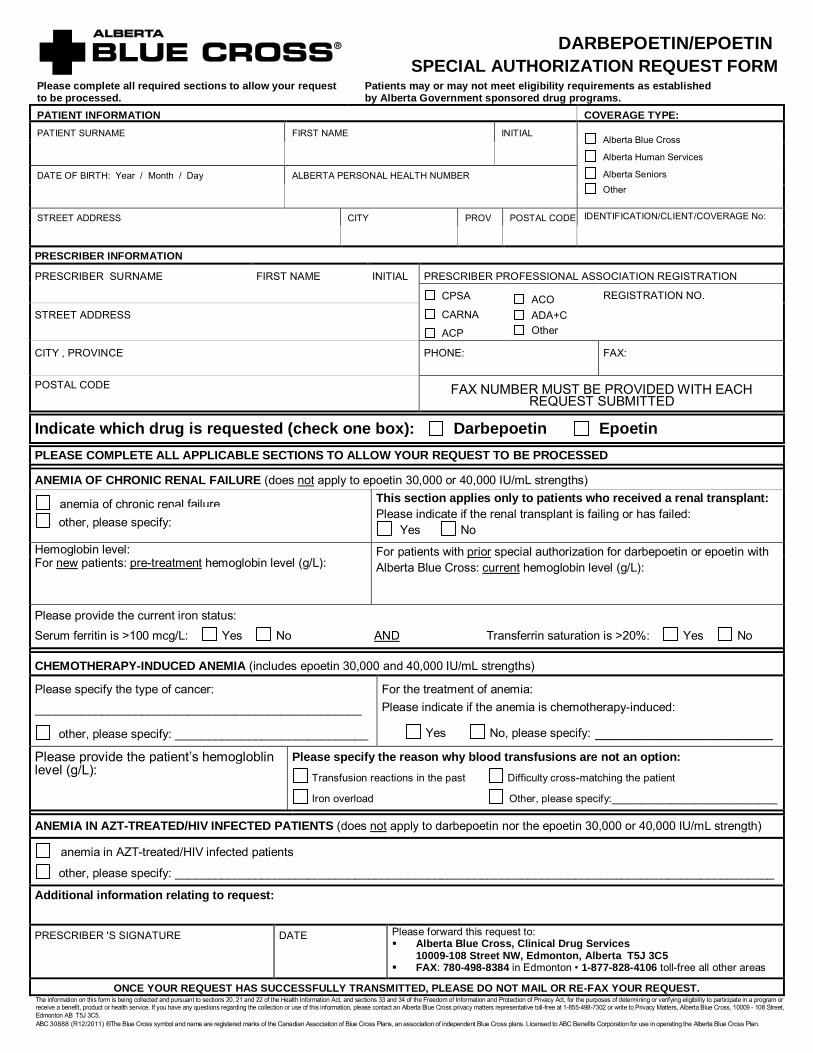
DARBEPOETIN/EPOETIN SPECIAL AUTHORIZATION REQUEST FORM
Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross
Alberta Human Services
Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION
PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA
CARNA
ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
CITY , PROVINCE PHONE: FAX:
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Indicate which drug is requested (check one box): Darbepoetin Epoetin
PLEASE COMPLETE ALL APPLICABLE SECTIONS TO ALLOW YOUR REQUEST TO BE PROCESSED
ANEMIA OF CHRONIC RENAL FAILURE (does not
anemia of chronic renal failure
apply to epoetin 30,000 or 40,000 IU/mL strengths)
other, please specify: ____________________________
This section applies only to patients who received a renal transplant: Please indicate if the renal transplant is failing or has failed:
Yes No Hemoglobin level: For patients with prior special authorization for darbepoetin or epoetin with
Alberta Blue Cross: currentFor hemoglobin level (g/L): new patients: pre-treatment
Please provide the current iron status:
hemoglobin level (g/L):
Serum ferritin is >100 mcg/L: Yes No AND
CHEMOTHERAPY-INDUCED ANEMIA (includes epoetin 30,000 and 40,000 IU/mL strengths)
Transferrin saturation is >20%: Yes No
Please specify the type of cancer: _________________________________________________
other, please specify: _____________________________
For the treatment of anemia: Please indicate if the anemia is chemotherapy-induced:
Yes No, please specify: ____________________
Please provide the patient’s hemogloblin level (g/L):
Please specify the reason why blood transfusions are not an option: Transfusion reactions in the past Difficulty cross-matching the patient
Iron overload Other, please specify:____________________________
ANEMIA IN AZT-TREATED/HIV INFECTED PATIENTS (does not
anemia in AZT-treated/HIV infected patients apply to darbepoetin nor the epoetin 30,000 or 40,000 IU/mL strength)
other, please specify: __________________________________________________________________________________________
Additional information relating to request: PRESCRIBER 'S SIGNATURE DATE Please forward this request to:
Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30888 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

Criteria for Coverage:
DARBEPOETIN
“For the treatment of anemia of chronic renal failure in patients with low hemoglobin (<100 g/L). Hemoglobin levels should be maintained within 100 – 110 g/L. According to current practice guidelines patients’ iron status should be monitored regularly, and wherever possible patients should be iron replete as demonstrated by serum ferritin >100 mcg/L and transferrin saturation >20%.” “For the treatment of chemotherapy-induced anemia in patients with non-myeloid malignancies with low hemoglobin (<100 g/L) in whom blood transfusions are not possible due to transfusion reactions, cross-matching difficulties or iron overload. If hemoglobin is rising by more than 20 g/L per month, the dose of Aranesp should be reduced by about 25%.” In order to comply with the second criterion: if the patient has iron overload the prescriber must state this in the request or alternatively, information is required regarding the patient’s transferrin saturation, along with results of liver function tests if applicable. For the first criterion, renewal requests may be considered if the patient’s hemoglobin is < 120 g/L while on Aranesp. For the second criterion, renewal requests may be considered if the patient's hemoglobin is < 110 g/L while on Aranesp.
EPOETIN (ALL strengths except 30,000 and 40,000 IU/mL)
“For the treatment of anemia of chronic renal failure in patients with low hemoglobin (< 100 g/L). Hemoglobin levels should be maintained within 100 - 110 g/L. According to current practice guidelines patients’ iron status should be monitored regularly, and wherever possible patients should be iron replete as demonstrated by serum ferritin >100 mcg/L and transferrin saturation >20%.” "For the treatment of anemia in AZT-treated/HIV infected patients." "For the treatment of chemotherapy-induced anemia in patients with non-myeloid malignancies with low hemoglobin (<100 g/L) in whom blood transfusions are not possible due to transfusion reactions, cross-matching difficulties or iron overload. If hemoglobin is rising by more than 20 g/L per month, the dose of Eprex should be reduced by about 25%.” In order to comply with the third criterion: if the patient has iron overload the prescriber must state this in the request or alternatively, information is required regarding the patient's transferrin saturation, along with the results of liver function tests if applicable. For the first criterion, renewal requests may be considered if the patient’s hemoglobin is < 120 g/L while on Eprex. For the third criterion, renewal requests may be considered if the patient's hemoglobin is < 110 g/L while on Eprex.
EPOETIN 30,000 and 40,000 IU/mL strengths
"For the treatment of chemotherapy-induced anemia in patients with non-myeloid malignancies with low hemoglobin (<100 g/L) in whom blood transfusions are not possible due to transfusion reactions, cross-matching difficulties or iron overload. If hemoglobin is rising by more than 20 g/L per month, the dose of Eprex should be reduced by about 25%. Patients may be granted a maximum allowable dose of 40,000 IU per week.” In order to comply with this criterion, if the patient has iron overload the prescriber must state this in the request, or alternatively, information is required regarding the patient's transferrin saturation, along with the results of liver function tests, if applicable. Renewal requests may be considered if the patient's hemoglobin is <110 g/L while on Eprex. ABC 30888 (R12/2011)
DARBEPOETIN/EPOETIN SPECIAL AUTHORIZATION CRITERIA
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 13
Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/ Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form
On the reverse is the official Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximabb/ Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
• All requests for abatacept, adalimumab, anakinra, etanercept, golimumab, infliximab or tocilizumab for Rheumatoid Arthritis must be submitted using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

ABATACEPT/ADALIMUMAB/ANAKINRA/ETANERCEPT/GOLIMUMAB/ INFLIXIMAB/TOCILIZUMAB for Rheumatoid Arthritis
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No: NOTIFICATION: PATIENT CONSENT: You may be eligible to receive Enbrel, Humira, Kineret or Remicade drug benefits. Personal and health information is required in order to determine eligibility and, in the event you are approved to receive drug benefits, to maintain eligibility, process payments and conduct the Alberta Post-Marketing Study Addressing ENBREL/HUMIRA/KINERET/REMICADE (“Study”). The Study will assist Alberta Health and Wellness to monitor, plan, evaluate and manage the cost-effectiveness of providing Enbrel, Humira, Kineret or Remicade as a benefit under the AHWDBL. Therefore, your consent is required as set out herein. Important: In order to be eligible for, and to maintain eligibility for, Enbrel, Humira, Kineret or Remicade drug benefit both you and your physician(s) must agree to and continue to actively and consistently participate in the Study as required by Alberta Blue Cross, Alberta Health and Wellness, its affiliates and agents throughout the special authorization period. Refusal to provide the requested consent will result in benefits being denied, and withdrawal of consent will result in benefits being revoked.
I hereby authorize: (A)The below physician(s) to disclose to Alberta Blue Cross, Alberta Human Services, and Alberta Seniors (the "Designated Recipients") any of my personal or health information contained on this Request Form or requested by the Designated Recipients (collectively “My Information”); and (B) The Designated Recipients to use and collect My Information for the purposes stated on this form; and (C) The Designated Recipients to disclose My Information to any affiliates or agents of the Designated Recipients for the purposes stated on this form. I acknowledge that: I have been made aware of the reasons why my health information is needed, and the risks and benefits of consenting or refusing to consent to disclosure of my health information; and (2) I am aware that I may revoke this consent (in writing) at anytime. Signature/Effective Date Patient’s Signature
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO. STREET ADDRESS
CITY , PROVINCE PHONE:
FAX:
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis: Current weight (kg): Indicate requested drug: Tocilizumab Dosage:
Dosing Frequency: Rheumatoid Arthritis Other (specify)
Abatacept Etanercept
Adalimumab Infliximab
Anakinra Golimumab
Scores: * DAS28 Score ___.____ OR ACR20 (renewals only) Date: _____________
AND HAQ Score ___.___ ___ Date: _____________ * New requests for patients currently maintained on the requested biologics require pre-treatment scores. Scores must be provided to the correct number of decimal places. DAS28 should be reported to one decimal place and HAQ should be reported to two decimal places.
Please provide reason if a switch to a different biologic agent is requested:
Note: Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
For all biologics EXCEPT Abatacept: Will the patient be maintained on methotrexate in combination with the requested biologic? YES NO
For Abatacept ONLY: Will the patient be maintained on methotrexate or another DMARD in combination with Abatacept? YES NO
If NO to any of the above, please specify reason:
Please provide the following information for all NEW requests: Previous medications utilized: Dose, duration and response is required for ALL FOUR of the following:
Methotrexate PO: Methotrexate SC or IM: Methotrexate with another DMARD other than leflunomide (specify agent) : Leflunomide:
Please provide the following information for all NEW anakinra/tocilizumab requests: Previous medications utilized: Indicate the contraindication or adverse effects related to the following:
Abatacept: Adalimumab: Etanercept: Infliximab: Golimumab: Rituximab: Tocilizumab:
PRESCRIBER'S SIGNATURE DATE
Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
I am currently an active participant in the Alberta Post-Marketing Study addressing Enbrel / Humira / Kineret / Remicade
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30902 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 15
Ezetimibe Special Authorization Request Form
On the reverse is the official Ezetimibe Special Authorization Request Form (ABC 30925).
• All requests for ezetimibe must be submitted using the Ezetimibe Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

EZETIMIBE SPECIAL AUTHORIZATION REQUEST FORM
Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Coverage of EZETIMIBE For the treatment of hypercholesterolemia in patients who are intolerant to statins or in whom a statin is contraindicated and who are at high cardiovascular risk*, or; For the treatment of hypercholesterolemia when used in combination with a statin in patients failing to achieve target LDL with a statin at maximum tolerable dose or maximum recommended dose as per respective product monograph and who are at high cardiovascular risk* Special authorization may be granted for 6 months. This product is eligible for auto-renewal.
*High cardiovascular risk is defined as possessing one of the following: 1) pre-existing cardiovascular disease and/or cerebrovascular disease, or 2) diabetes, or 3) familial hypercholesterolemia, or 4) greater than or equal to 20% risk as defined by the Framingham Risk Assessment Tool,
OR 5) three or more of the following risk factors:
• family history of premature cardiovascular disease
• smoking • hypertension
• obesity • glucose intolerance • renal disease.
NEW Please provide the following information for all NEW requests: A. Diagnosis: hypercholesterolemia other, please specify
B. Information regarding previous STATIN use: Statin(s) HAS been utilized. Please specify which statin has been utilized (including dose and duration):
Nature of response to STATIN: Intolerance Failure to achieve target LDL Other
Statin(s) has NOT been utilized. Contraindication? Yes No Please elaborate: C. Presence of CARDIOVASCULAR risk factors (CHECK ALL THAT APPLY):
In order to comply with the above criteria check at least three of the following: family history of premature cardiovascular disease smoking hypertension obesity glucose intolerance renal disease AND/OR In order to comply with the above criteria check at least one of the following:
pre-existing cardiovascular disease and/or cerebrovascular disease diabetes familial hypercholesterolemia greater than or equal to 20% risk as defined by the Framingham Risk Assessment Tool
D. Additional information relating to request:
RENEWAL This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER’S SIGNATURE DATE Please forward this request to: • Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 • FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30925 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 17
Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form
On the reverse is the official Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form (ABC 30932).
• All requests for peginterferon alfa-2a/ribavirin or peginterferon alfa-2b/ribavirin must be submitted using the Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

PEGINTERFERON ALFA-2A+RIBAVIRIN/PEGINTERFERON ALFA-2B+RIBAVIRIN
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
NOTIFICATION: PATIENT CONSENT: You may be eligible to receive Pegetron or Pegasys RBV drug benefits. Information from your prescriber is required to determine eligibility. Your consent is required: (A) for your prescriber to release necessary and relevant information to Alberta Blue Cross, Alberta Health and Wellness and, if requested, to Alberta Human Services and Alberta Seniors; and (B) for Alberta Blue Cross to release that and related usage information to Alberta Health and Wellness.
I hereby authorize: (A) my prescriber to release to Alberta Blue Cross, Alberta Health and Wellness, and (if they request it) to Alberta Human Services and Alberta Seniors (the aforesaid being the "designated recipients"); and (B) Alberta Blue Cross to release to Alberta Health and Wellness the information on this form and information relating to my usage of and experience with the drug and treatment results, and I consent to the designated recipients collecting such information. Date: Patient’s Signature:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Drug Requested: Diagnosis of chronic hepatitis C: Evidence of active liver disease:
Peginterferon Alfa-2a+Ribavirin (E.g. Pegasys RBV)
Peginterferon Alfa-2b+Ribavirin (E.g. Pegetron)
Both: a) is the patient anti-HCV positive,
pre-treatment................................ AND; b) is the patient serum HCV RNA
positive (by PCR), pre-treatment......................................
YES NO Not Tested
Either: a) does the patient have elevated liver enzymes
(ALT and/or AST), pre-treatment ……………. OR; b) does the patient have an abnormal liver
biopsy (inflammation and/or fibrosis)
YES NO Not Tested
If the patient is anti-HCV negative but serum HCV RNA positive, please explain:
If patient is currently on Peginterferon Alfa-2a + Ribavirin or Peginterferon Alfa-2b + Ribavirin indicate start date:
Year / Month / Day
INITIAL REQUEST: EXTENSION REQUEST: Initial length of approval:
Advanced fibrosis or cirrhosis (regardless of genotype)……………………………………………... 48 weeks
Genotype 1..…………………………………………14 weeks Is a baseline serum sample stored for future testing? YES NO
Genotype 2 or 3 with HIV co-infection……….14 weeks Is a baseline serum sample stored for future testing? YES NO
Genotype 1, 2 or 3 post-liver transplant……..26 weeks
Initial and maximum length of approval: Genotype 2 or 3 (not co-infected with HIV)....….24 weeks Genotype 4, 5 or 6…..…………………………….. 48 weeks
Request for treatment extension at 14 weeks: For Genotype 1 (non-liver transplant) patients and Genotype 2 or 3 patients with HIV co-infection: Is the patient serum HCV RNA negative at 12 weeks?
YES
NO
Patient may be eligible for additional 34 weeks of coverage (total 48 wks) Has the patient achieved a reduction of viral load by at least 2 logs (100 fold)?
YES
NO
The patient may be eligible for an additional 14 weeks of therapy to confirm response. Additional serum HCV RNA test results are required at 24 weeks
Request for treatment extension at 26 weeks: For Genotype 1, 2 or 3 post-liver transplant patients and for patients from the above section that achieved a 2-log drop but were not serum HCV negative at 12 weeks: Is the patient serum HCV RNA negative at 24 weeks?
YES NO The patient may be eligible for a total of 48 weeks of therapy. PREVIOUS THERAPY: Consideration may be given in patients who have previously received therapy who meet at least one of the following criteria: Advanced fibrosis or cirrhosis. Patient relapsed following non-pegylated interferon/ribavirin combination therapy. Patient failed to respond to or relapsed following interferon monotherapy Additional information relating to request:
PRESCRIBER 'S SIGNATURE DATE Please forward this request to: • Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 • FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30932 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 19
Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form
On the reverse is the official Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form (ABC 30944).
• All requests for peginterferon alfa-2a for Chronic Hepatitis C must be submitted using the Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

PEGINTERFERON ALFA-2A for Chronic Hepatitis C SPECIAL AUTHORIZATION REQUEST FORM
Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE:
PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
NOTIFICATION: PATIENT CONSENT: You may be eligible to receive Pegasys drug benefits. Information from your prescriber is required to determine eligibility. Your consent is required: (A) for your prescriber to release necessary and relevant information to Alberta Blue Cross, Alberta Health and Wellness and, if requested, to Alberta Human Services and Alberta Seniors; and (B) for Alberta Blue Cross to release that and related usage information to Alberta Health and Wellness.
I hereby authorize: (A) my prescriber to release to Alberta Blue Cross, Alberta Health and Wellness, and (if they request it) to Alberta Human Services and Alberta Seniors (the aforesaid being the “designated recipients”); and (B) Alberta Blue Cross to release to Alberta Health and Wellness the information on this form and information relating to my usage of and experience with the drug and treatment results, and I consent to the designated recipients collecting such information.
Date Patient’s Signature
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
DIAGNOSIS OF CHRONIC HEPATITIS C: EVIDENCE OF ACTIVE LIVER DISEASE: Both: a) is the patient anti-HCV positive,
pre-treatment…......................…………… AND; b) is the patient serum HCV RNA positive (by PCR),
pre-treatment…........................
YES NO Not Tested
Either: a) does the patient have elevated liver enzymes
(ALT and/or AST), pre-treatment…….……………
OR; b) does the patient have an abnormal liver biopsy
(inflammation and/or fibrosis)...……………………
YES NO Not Tested
If the patient is anti-HCV negative but serum HCV RNA positive, please explain:
If patient is currently on peginterferon alfa-2a, indicate start date:
Year / Month / Day
INITIAL REQUEST: EXTENSION REQUEST:
Is the patient intolerant to ribavirin? YES NO Request for treatment extension at 14 weeks (excluding patients with advanced fibrosis and cirrhosis):
Is the patient serum HCV RNA negative at 12 weeks?
YES → Patient may be eligible for additional 34 weeks of coverage (total 48 wks)
NO → Has the patient achieved a reduction of viral load by at least 2 logs (100 fold)?
YES → Patient may be eligible for additional 34 weeks of coverage (total 48 wks)
NO
Is a baseline serum sample stored for future testing? YES NO
Initial length of approval: Advanced fibrosis or cirrhosis (regardless of genotype)…… 48 weeks
Genotype 1…………..…………………………………….………. 14 weeks
Genotype 2 or 3 …………………………..…………………….… 14 weeks
Genotype 4, 5 or 6 .………………………………………………. 14 weeks
PREVIOUS THERAPY: Consideration may be given to patients who have previously received therapy and who meet at least one of the following:
Advanced fibrosis or cirrhosis. Patient relapsed following non-pegylated interferon/ribavirin combination therapy. Additional information relating to request:
PRESCRIBER’S SIGNATURE DATE Please forward this request to: • Alberta Blue Cross, Clinical Drug Services
10009-108 Street NW, Edmonton, Alberta T5J 3C5 • FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30944 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 21
Etanercept for Juvenile Idiopathic Arthritis Special Authorization Request Form
On the reverse is the official Etanercept for Juvenile Idiopathic Arthritis Special Authorization Request Form (ABC 30948).
• All requests for etanercept for Juvenile Idiopathic Arthritis must be submitted using the Etanercept for Juvenile Rheumatoid Arthritis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

ETANERCEPT for Juvenile Idiopathic Arthritis SPECIAL AUTHORIZATION REQUEST FORM
Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
NOTIFICATION: PATIENT CONSENT: You may be eligible to receive Enbrel drug benefits. Personal and health information is required in order to determine eligibility and, in the event you are approved to receive drug benefits, to maintain eligibility, process payments and conduct the Alberta Post-Marketing Study Addressing ENBREL (“Study”). The Study will assist Alberta Health and Wellness to monitor, plan, evaluate and manage the cost-effectiveness of providing Enbrel as a benefit under the AHWDBL. Therefore, your consent is required as set out herein. Important: In order to be eligible for, and to maintain eligibility for Enbrel drug benefit both you and your physician(s) must agree to and continue to actively and consistently participate in the Study as required by Alberta Blue Cross, Alberta Health and Wellness, its affiliates and agents throughout the special authorization period. Refusal to provide the requested consent will result in benefits being denied, and withdrawal of consent will result in benefits being revoked.
I hereby authorize: (A)The below physician(s) to disclose to Alberta Blue Cross, Alberta Health and Wellness, Alberta Human Services, and Alberta Seniors (the "Designated Recipients") any of my personal or health information contained on this Request Form or requested by the Designated Recipients (collectively “My Information”); and (B) The Designated Recipients to use and collect My Information for the purposes stated on this form; and (C) The Designated Recipients to disclose My Information to any affiliates or agents of the Designated Recipients for the purposes stated on this form. I acknowledge that: I have been made aware of the reasons why my health information is needed, and the risks and benefits of consenting or refusing to consent to disclosure of my health information; and (2) I am aware that I may revoke this consent (in writing) at anytime. ___________________________________ ___________________________________ Signature Effective Date Patient or Guardian Signature: ___________________________________ Print Name of Guardian
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis:
Polyarticular Juvenile Idiopathic Arthritis
Other (specify)
Patient’s current weight (kg): _________ Requested dose (mg/kg): ___________
JRA30 Date of assessment:___________________________
1. Rheumatologist global 4. No. of joints assessment (0-10) ______________________ with LROM ______________
2. Patient global assessment (0-10) __________ 5. CHAQ (0-3) ______________
3. Number of active joints* __________________ 6. ESR (mm/hr) ________ or CRP ________
*joints with swelling not due to deformity or joints with limitation of motion with pain, tenderness or both
Please provide the following information for ALL new requests: Previous DMARDs utilized (specify agent): Dose, duration and response is required: Additional information relating to request PRESCRIBER'S SIGNATURE DATE Please forward this request to:
Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: (780) 498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
I am currently an active participant in the Alberta Post-Marketing Study addressing Enbrel ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30948 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 1A • 23
Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form
On the reverse is the official Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form (ABC 30964).
• All requests for adalimumab, etanercept, golimumab or infliximab for Psoriatic Arthritis must be submitted using the Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

ADALIMUMAB/ETANERCEPT/GOLIMUMAB/INFLIXIMAB for Psoriatic Arthritis
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION
PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests:
Diagnosis: Polyarticular Psoriatic Arthritis Pauciarticular Psoriatic ArthritisJoints affected:
Knee joint(s) Hip joint(s) Other (specify): Other (specify):
Current weight (kg):
Indicate requested drug:
Dosage: Dosing Frequency: Adalimumab
Etanercept Golimumab Infliximab
Scores:*
DAS28 Score ___._____ OR ACR20 (renewals only) Date:______________
AND
HAQ Score ___.___ ___ Date: ______________
Please provide reason if a switch to a different biologic agent is requested:
Note: Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
* New requests for patients currently maintained on the requested biologic require pre-treatment scores. Scores must be provided to the correct number of decimal places. DAS28 should be reported to one decimal place and HAQ should be reported to two decimal places.
Will the patient be maintained on methotrexate in combination with the requested biologic?
YES NO (If not, please specify reason):
Please provide the following information for all NEW requests: Previous medications utilized: Dose, duration and response is required for ALL THREE of the following:
Methotrexate PO:
Methotrexate SC or IM:
DMARD other than MTX (specify agent):
Additional information relating to request (e.g. reasons why any of the above therapies were not tried):
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30964 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 25
Select Quinolones Special Authorization Request Form
On the reverse is the official Select Quinolones Special Authorization Request Form (ABC 30966). • All requests for ciprofloxacin, levofloxacin, moxifloxacin or ofloxacin must be submitted using
the Select Quinolones Special Authorization Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

SELECT QUINOLONES* *ciprofloxacin/levofloxacin/moxifloxacin/ofloxacin
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed. Incomplete requests CANNOT BE EXPEDITED.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Only the following conditions may be authorized for coverage. Drug Requested and Condition requiring quinolone treatment: Please check the boxes that apply to your patient.
CIPROFLOXACIN Respiratory Tract Infection: End stage COPD with or without bronchiectasis, where there has been
documentation of previous Pseudomonas aeruginosa colonization/infection Pneumonic illness in cystic fibrosis Genitourinary Tract Infection: Urinary Tract Infection Prostatitis Prophylaxis of urinary tract surgical procedures Gonococcal infection Skin & Soft Tissue / Bone & Joint Infection: Malignant / invasive otitis externa Bone / joint infection due to gram-negative organism(s) Therapy / step-down therapy of polymicrobial infection in combination with
clindamycin or metronidazole, e.g. diabetic foot infection, decubitus ulcers Gastrointestinal Tract Infection: Bacterial gastroenteritis where antimicrobial therapy is indicated Typhoid fever (enteric fever) Therapy / step-down therapy of polymicrobial infection in combination with
clindamycin or metronidazole, e.g. intra-abdominal infections Other: Prophylaxis of adult contacts of cases of invasive meningococcal disease Therapy / step-down therapy of hospital acquired gram-negative infections Empiric therapy of febrile neutropenia in combination with other appropriate
agents Exception case of allergy or intolerance to all other appropriate therapies
as defined by relevant guidelines/references, i.e. AMA CPGs or Bugs & Drugs
LEVOFLOXACIN MOXIFLOXACIN Community acquired pneumonia after failure of first line therapy,
as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy
Community acquired pneumonia in patients with co morbidities (asthma, lung cancer, COPD, diabetes, alcoholism, chronic renal or liver failure, CHF, chronic corticosteroid use, malnutrition or acute weight loss, hospitalization within previous 3 months, HIV/AIDS, smoking)
Acute exacerbation of chronic bronchitis after failure of first and
Acute sinusitis after failure of first line therapy, as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy, in patients with β–lactam (penicillin & cephalosporin) allergy
second line therapy, as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy
For use in other current Health Canada approved indications when prescribed by a specialist in Infectious Diseases.
OFLOXACIN Pelvic inflammatory disease Epididymo-orchitis/epididymitis most likely due to enteric
organisms For the treatment of Chlamydial infection For the treatment of Gonococcal infection For use in other current Health Canada approved indications
when prescribed by a specialist in Infectious Diseases
Please specify details: For use in other current Health Canada approved indications when
prescribed by a specialist in Infectious Diseases
PHYSICIAN'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5
FAX: 780-498-8384 in Edmonton 1-877-828-4106 toll-free all other areas
ONCE YOU HAVE CONFIRMED YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30966 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

BACKGROUND INFORMATION REGARDING SELECT QUINOLONE SPECIAL AUTHORIZATION PROCESS
Optional Special Authorization introduced for quinolones At the request of Alberta Health and Wellness, Alberta Employment and Immigration, Alberta Seniors and Community Supports and Alberta Children and Youth Services, Alberta Blue Cross applied criteria effective September 15, 2005 for coverage of select quinolone antibiotics covered through their drug benefit programs:
• ciprofloxacin, levofloxacin, moxifloxacin, and ofloxacin. Norfloxacin continues to be eligible for coverage as an unrestricted benefit. Rationale These criteria are the result of a comprehensive evidence-based review undertaken as an initiative of the Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics through the Review of Benefit Status (ROBS) process. This review examined systemic antimicrobial agents currently covered via the Alberta Health and Wellness Drug Benefit List. The mandate of the review was to encourage optimal utilization and to help prevent antimicrobial resistance. The review was conducted according to the established ROBS process, and included systematic reviews of the medical literature and analysis of current utilization patterns. External Alberta physicians and pharmacists with expertise in the treatment of infectious diseases provided advice and assistance for this review process. Information and experience from other provincial jurisdictions that have undertaken similar antimicrobial reviews were also taken into consideration in this review. The review was completed in accordance with pre-determined guiding principles that sought to allow optimal practice to proceed, ensuring optimal use and helping prevent resistance, while at the same time being unencumbered by undue paperwork and unnecessary restrictions.
Role of Physicians In conjunction with these new criteria, physicians have two options by which patients may be eligible for coverage of these specific antimicrobial products. This offers a streamlined alternative to traditional Special Authorization. 1) Physicians can register to be a designated prescriber. Registration allows for patients to receive coverage of quinolones
without Special Authorization as long as the prescription is written for one of the criteria for coverage set out in the Alberta Health and Wellness Drug Benefit List. These criteria are attached for your reference. Should a designated physician wish to prescribe one of the select quinolones outside the coverage criteria, they may do so but must indicate this on the prescription; however, patients will not be eligible for payment under the government-sponsored program for such prescriptions and the patient may choose to receive the product at their expense.
2) Physicians who choose not to register will be considered ‘non-designated prescribers’.
• Such physicians will be required to apply for Special Authorization on the patient’s behalf. • A patient’s claims for prescriptions written by non-designated physicians will be subject to a first fill forgiveness
rule. This means the first claim will be paid but subsequent claims for the same active ingredient (irrespective of strength, route and form) within a 90 day period will require Special Authorization.
• Special authorization requests must be submitted using the Select Quinolones Special Authorization Request Form. If the appropriate sections of this request form are completed and coverage criteria are met, the request will be processed within approximately 6 to 18 hours of receiving the request. Subsequent claims will be rejected unless Special Authorization is granted.
To register to become a designated prescriber
please return your completed registration by FAX to 1-877-305-9911. For more information, please contact
Clinical Drug Services, Alberta Blue Cross, at 780-498-8368.
® The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan. ABC 30966 SA form and comm (R12/2011)

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 1A • 28 EFFECTIVE APRIL 1, 2012
Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon Nasal Spray for Osteoporosis Special Authorization Request Form
On the reverse is the official Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon Nasal Spray for Osteoporosis Special Authorization Request Form (ABC 31086).
• All requests for alendronate, raloxifene, risedronate or synthetic calcitonin salmon for Osteoporosis must be submitted using the Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon for Osteoporosis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

ALENDRONATE / RALOXIFENE / RISEDRONATE / SYNTHETIC CALCITONIN SALMON NASAL SPRAY FOR OSTEOPOROSIS
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests:
Indicate which drug is requested (check ONE box)*: Alendronate (10mg, 70mg, 70mg + 5600U vitamin D3) Raloxifene Risedronate Synthetic Calcitonin Salmon Nasal Spray *Coverage cannot be provided for two or more osteoporosis medications (alendronate, calcitonin, denosumab, etidronate, raloxifene, risedronate) when intended for use as combination therapy. Requests for other osteoporosis medications covered via special authorization will not be considered until 6 months after the last dose of denosumab. Please provide the following information for all NEW requests:
Diagnosis: For the treatment of Osteoporosis Osteopenia Bone pain secondary to: ______________________________ Other, please specify: __________________________
Has the patient experienced FRACTURES related to the diagnosis? NO YES
Information regarding previous etidronate use: Etidronate HAS been utilized.
Nature of response to etidronate: Lack of response (i.e. demonstrated as a > 2% loss in bone mineral density in one year) Intolerance Other (please specify):________________________________________________________
Etidronate has NOT been utilized: Contraindication. Please elaborate:____________________________________________________________________________ Other reason(s) etidronate was NOT tried (please specify):_________________________________________________________
Additional information relating to request:
RENEWAL This product is eligible for auto-renewal for the treatment of osteoporosis. A Special Authorization renewal request is required only if the Special Authorization approval for the treatment of osteoporosis has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy: PRESCRIBER'S SIGNATURE DATE Please forward this request to:
• Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 • FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31086 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALENDRONATE / RALOXIFENE / RISEDRONATE / SYNTHETIC CALCITONIN SALMON NASAL SPRAY FOR OSTEOPOROSIS
SPECIAL AUTHORIZATION CRITERIA Patients may or may not meet eligibility requirements as established by
Alberta Government sponsored drug programs.
Criteria for Coverage:
ALENDRONATE** (10mg, 70mg, 70mg + 5600U vitamin D3 oral tablets) RALOXIFENE RISEDRONATE** Special Authorization Criteria for OSTEOPOROSIS “For the treatment of osteoporosis in patients who have documented hip, vertebral or other fractures. Special authorization for may be granted for 6 months.” “For the treatment of osteoporosis in patients with documented evidence of intolerance or lack of response to etidronate (i.e. demonstrated as a > 2 % loss in bone mineral density in one year). Special authorization may be granted for 6 months.” “Coverage cannot be provided for two or more osteoporosis medications (alendronate, calcitonin, etidronate, raloxifene, risedronate) when these medications are intended for use as combination therapy.” These products are eligible for auto-renewal for the treatment of osteoporosis.
**Please note: alendronate and risedronate also have Special Authorization criteria for Paget’s disease. Please refer to the Alberta Health and Wellness Drug Benefit List for alendronate and risedronate’s other criteria for the indication of Paget’s disease.
http://www.health.alberta.ca/AHCIP/drug-benefit-list.html
SYNTHETIC CALCITONIN SALMON Nasal Spray Special Authorization Criteria: "For the treatment of osteoporosis in patients with documented evidence of intolerance or lack of response to etidronate (i.e. demonstrated as a >2% loss in bone mineral density in one year). Special authorization may be granted for 6 months." "Coverage cannot be provided for two or more osteoporosis medications (alendronate, calcitonin, etidronate, raloxifene, risedronate) when these medications are intended for use as combination therapy." This product is eligible for auto-renewal.
ABC 31086 (R12/2011)

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 31
Celecoxib Special Authorization Request Form
On the reverse is the official Celebrex Special Authorization Request Form (ABC 31140).
• All requests for celecoxib must be submitted using the Celecoxib Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 401-1150 in Edmonton and area 1-888-401-1150 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
CELECOXIB SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY, PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Coverage of CELECOXIB
For patients who are at high risk of upper gastrointestinal (GI) complications due to a proven history of prior complicated GI events (e.g. GI perforation, obstruction or major bleeding), OR
For patients who have a documented history of ulcers proven radiographically and/or endoscopically.
Special authorization may be granted for 6 months.
This product is eligible for auto-renewal.
NEW Please provide the following information for NEW requests (check ALL that apply):
1) Is this patient at high risk of upper GI complications? Yes No
2) Does this patient have a documented history of ulcers? Yes No
Additional information relating to request:
RENEWAL This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER’S SIGNATURE DATE Please forward this request to: • Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FOR CELECOXIB REQUESTS ONLY: • FAX: 780-401-1150 in Edmonton •1-888-401-1150 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
THIS SECTION IS FOR ALBERTA BLUE CROSS USE ONLY
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31140 (R11/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 33
Filgrastim/Pegfilgrastim Special Authorization Request Form
On the reverse is the official Filgrastim/Pegfilgrastim Special Authorization Request Form (ABC 31150)
• All requests for filgrastim or pegfilgrastim must be submitted using the Filgrastim/Pegfilgrastim Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
FILGRASTIM/PEGFILGRASTIM SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Indicate which drug is requested (check ONE box): FILGRASTIM (complete Section I or II) PEGFILGRASTIM (complete Section I only) Criteria for Coverage of FILGRASTIM Criteria for Coverage of PEGFILGRASTIM To decrease the incidence of infection, as manifested by febrile neutropenia, in patients with non-myeloid malignancies receiving myelosuppressive anti-neoplastic drugs with curative intent. This drug must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates). For the reduction in the duration of neutropenia, fever, antibiotic use and hospitalization, following induction and consolidation treatment for acute myeloid leukemia. This drug must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates). To increase neutrophil counts and to reduce the incidence and duration of infection in patients with a diagnosis of congenital, cyclic or idiopathic neutropenia. This drug must be prescribed by the Directors of Divisions of Hematology in tertiary care centres (or their designates). For the treatment of patients undergoing Peripheral Blood Progenitor Cell (PBPC) collection and therapy when prescribed by a designated prescriber. Please note for the first criterion: Coverage cannot be considered for palliative patients.
To decrease the incidence of infection, as manifested by febrile neutropenia, in patients 18 years of age and older with non-myeloid malignancies receiving myelosuppressive anti-neoplastic drugs with curative intent. This drug product must be prescribed by Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates). Please note: Coverage cannot be considered for palliative patients.
Section I (Filgrastim requests for the first criterion and all pegfilgrastim requests, check ALL that apply)
Please SPECIFY the type of cancer being treated with chemotherapy for curative intent: _______________________________________ AND Please provide the indication for which the drug is requested:
patient has febrile neutropenia patient had febrile neutropenia from a previous cycle of the same chemotherapy patient will be undergoing a high dose or aggressive chemotherapy where febrile neutropenia is very likely to occur other, please SPECIFY: _______________________________________________________________________________________
Section II (Filgrastim requests for other criteria, check ALL that apply)
Please provide the indication for which filgrastim is requested: patient has neutropenia AND a diagnosis of congenital, cyclic or idiopathic neutropenia OR acute myeloid leukemia
other, please SPECIFY: _____________________________________________
patient is undergoing Peripheral Blood Progenitor Cell (PBPC) collection and therapy
Additional information relating to request: PRESCRIBER'S SIGNATURE DATE Please forward this request to:
Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: (780) 498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31150 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 35
Fentanyl Special Authorization Request Form
On the reverse is the official Fentanyl Special Authorization Request Form (ABC 31169). • All requests for fentanyl or fentanyl citrate must be submitted using the Fentanyl Special
Authorization Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
FENTANYL SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO. STREET ADDRESS
CITY , PROVINCE PHONE:
FAX:
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
CRITERIA FOR COVERAGE OF FENTANYL Fentanyl Injection For the treatment of persistent, severe chronic pain in those patients who cannot swallow, or who are intolerant of, morphine and/or hydromorphone, if not contraindicated. Special authorization may be granted for 6 months. This product is eligible for auto-renewal.
Fentanyl Patch For the treatment of persistent, severe chronic pain in those patients who require continuous around-the-clock analgesia for an extended period of time in those patients who cannot swallow. Special authorization may be granted for 6 months. For the treatment of persistent, severe chronic pain in those patients who require continuous around-the-clock analgesia for an extended period of time in those patients who require opioid therapy at a total daily dose of at least 60 mg/day oral morphine equivalents. Patients must have tried and not been able to tolerate at least two discrete courses of therapy with two of the following agents: morphine, hydromorphone and oxycodone, if not contraindicated. Special authorization may be granted for 6 months. This product is eligible for auto-renewal.
NEW Please provide the following for all new patients:
Product(s) requested: FENTANYL INJECTION FENTANYL PATCH
Nature of the patient’s pain: Persistent, severe chronic pain Other:
For FENTANYL PATCH requests: Patients must have tried at least two discrete courses* of therapy with two of the required agents: morphine, hydromorphone and oxycodone.
* A discrete course is defined as a separate treatment course, which may involve more than one agent, used at one time to manage the patient’s condition.
Treatment course 1: MEDICATION used & RESPONSE to each drug (or CONTRAINDICATIONS to drug): morphine
hydromorphone
oxycodone
other (specify)
Treatment course 2: MEDICATION used & RESPONSE to each drug (or CONTRAINDICATIONS to drug): morphine
hydromorphone
oxycodone
other (specify)
For FENTANYL INJECTION requests:
Previous MEDICATION used & RESPONSE to each drug (or CONTRAINDICATIONS to drug):
morphine
hydromorphone
If patient is unable to swallow, please provide information regarding specific reasons patient is unable take oral medications:
RENEWAL This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER 'S SIGNATURE DATE Please forward this request to: • Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 • FAX: 780 498-8384 Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31169 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 37
Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form
On the reverse is the official Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form (ABC 31192).
• All requests for adalimumab, etanercept, infliximab or ustekinumab for Plaque Psoriasis must be submitted using the Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
57BOnce your request has successfully transmitted, please do not mail or re-fax your request

ADALIMUMAB/ETANERCEPT/INFLIXIMAB/USTEKINUMAB for
Plaque Psoriasis SPECIAL AUTHORIZATION REQUEST FORM
Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE:
PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests:
Diagnosis:
Plaque Psoriasis
Other (specify): _______________________
Indicate requested drug: Adalimumab Etanercept Infliximab Ustekinumab
Current Weight (Kg):
Dosage:
Dosing Frequency:
Location: Significant involvement of face, palms of the hands, soles of the feet or genital region: YES NO
Scores:
PASI__________ Date__________________
DLQI__________ Date__________________
Please provide reason if a switch to a different biologic agent is requested: Note: Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
Please provide the following information for all NEW requests:
Previous medications/therapies utilized: Dose, duration and response is required for the following:
Methotrexate PO:
Methotrexate SC or IM:
Cyclosporine:
Phototherapy:
Additional information relating to request (e.g. reasons why any of the above therapies were not tried): PRESCRIBER’S SIGNATURE DATE Please forward this request to:
Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5
FAX: 780- 498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31192 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 39
Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form
On the reverse is the official Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form (ABC 31195).
• All requests for adalimumab, etanercept, golimumab or infliximab for Ankylosing Spondylitis must be submitted using the Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
59BOnce your request has successfully transmitted, please do not mail or re-fax your request.

ADALIMUMAB/ETANERCEPT/GOLIMUMAB/INFLIXIMAB for Ankylosing Spondylitis
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis: Current
weight (kg): Indicate requested drug:
Adalimumab
Etanercept
Golimumab
Infliximab
Dosage: Dosing frequency:
Ankylosing Spondylitis (meeting modified NY criteria)
Other (please SPECIFY): ____________________________
Please provide the following information for all NEW requests: Previous medications utilized: Have two or more NSAIDs been tried for a minimum of 4 weeks each at maximum tolerated or recommended doses?
YES (please SPECIFY below) NO
Please SPECIFY the NSAID Please SPECIFY the dose, duration, and response
NSAID #1:
NSAID #2:
Other, please SPECIFY: Please provide the following information for all NEW* requests:
BASDAI #1 Date:
BASDAI #2: Date:
Spinal Pain VAS #1 (cm): Date:
Spinal Pain VAS #2 (cm): Date:
* New requests for patients currently maintained on the requested biologic require pre-treatment scores. Scores 1 and 2 for each parameter must be at least 8 weeks apart.
Please provide the following information for all RENEWAL requests:
BASDAI Date:
Spinal pain VAS (cm) Date:
Please provide reason if a switch to a different biologic agent is requested:
Note: Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
Additional information relating to request:
PRESCRIBER'S SIGNATURE DATE
Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31195 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 41
Adalimumab for Crohn’s/Infliximab for Crohn’s/Fistulizing Crohn’s Disease Special Authorization Request Form
On the reverse is the official Adalimumab for Crohn’s/Infliximab for Crohn’s/Fistulizing Crohn’s Disease Special Authorization Request Form (ABC 31200).
• All requests for adalimumab for Moderately to Severely Active Crohn's Disease or infliximab for Moderately to Severely Active Crohn’s/Fistulizing Crohn’s Disease must be submitted using the Adalimumab for Crohn’s/Infliximab for Crohn’s/Fistulizing Crohn’s Disease Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

-
ADALIMUMAB for Crohn’s / INFLIXIMAB for Crohn’s / Fistulizing Crohn’s Disease SPECIAL AUTHORIZATION REQUEST FORM
Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE ID/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis:
Moderately to Severely Active Crohn’s Fistulizing Crohn’s
Indicate requested drug:
Adalimumab Dose:____________ Frequency:___________ Date of last dose:__________________
Infliximab Dose:____________ Frequency:___________ Date of last dose:__________________
Current weight (kg):___________ Other (specify) __________
For INITIAL request, please indicate if the drug is requested for NEW patient who has never been treated with the requested drug by any health care provider
EXISTING patient who is being treated, or have previously been treated with the requested drug
Please provide reason if a switch to a different biologic agent or change in dose is requested:
Note: Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
Infliximab For Fistulizing Crohn’s Disease: Adalimumab or Infliximab For Moderately to Severely Active Crohn’s Disease:
INITIAL request: Dose, duration and response is required for all medications previously utilized:
INITIAL request: Dose, duration and response is required for all medications previously utilized:
Azathioprine: Azathioprine:
6-mercaptopurine: 6-mercaptopurine: Antibiotics (specify the drug name): Methotrexate: NEW patient: Does the patient have actively draining perianal or enterocutaneous fistula(s) that have recurred or persisted despite previous therapy:
Yes No
Mesalamine: Glucocorticoid(s) (specify drug name): For ALL requests for Moderately to Severely Active Crohn’s Disease, please provide
Modified Harvey-Bradshaw Index score: _______________
Date of score: _______________
EXISTING patient: Please indicate response to treatment with infliximab:
Closure of individual fistulas as evidenced by no or minimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline.
Incomplete response (specify): Additional information relating to request (e.g. reasons why any of the above therapies were not tried): PRESCRIBER'S SIGNATURE DATE Please forward this request to:
Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31200 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 43
Rituximab for Rheumatoid Arthritis Special Authorization Request Form
On the reverse is the official Rituximab for Rheumatoid Arthritis Special Authorization Request Form (ABC 31205).
• All requests for rituximab for Rheumatoid Arthritis must be submitted using the Rituximab for Rheumatoid Arthritis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

RITUXIMAB for Rheumatoid Arthritis
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE:
PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY, PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis:
Rheumatoid Arthritis Other (specify)
Dosage: Dosing Frequency:
Please provide reason if a switch from a different biologic agent to rituximab is requested: Date of last dose:
_________________________________
Note: Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
Scores:*
DAS28 Score __________
Date: __________________ AND HAQ Score ____________
Date: __________________
Requests for Re-treatment after 2 dose course
Date of initial dose of the previous course of therapy:
_____________________ Response Scores 16-24 weeks after initial dose of previous course of therapy: DAS28 Score _______ Date: _____________ AND HAQ Score _________ Date: _____________ Current scores: DAS28 Score ________ Date: _____________ AND HAQ Score _________ Date: _____________
* New requests for patients currently maintained on the requested biologic also require pre-treatment scores. Scores must be provided to the correct number of decimal places. DAS28 should be reported to one decimal place and HAQ should be reported to two decimal places.
Will the patient be maintained on methotrexate in combination with rituximab? YES NO (If not, please specify reason):
Please provide the following information for all NEW requests: Previous medications/therapies utilized: Dose, duration and response is required for ALL FIVE of the following:
Methotrexate PO: Methotrexate SC or IM: Methotrexate with another DMARD other than leflunomide (specify agent) Leflunomide: Anti-TNF therapy:
Additional information relating to request (e.g. reasons why any of the above therapies were not tried):
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780 498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31205 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 45
Imiquimod Special Authorization Request Form
On the reverse is the official Imiquimod Special Authorization Request Form (ABC 31222). • All requests for imiquimod must be submitted using the Imiquimod Special Authorization
Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
IMIQUIMOD SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Coverage of IMIQUIMOD For the treatment of Actinic Keratosis located on the head and neck in patients who have failed treatment with cryotherapy (where appropriate) and 5-fluorouracil (5-FU). Special authorization may be granted for 6 months. This product is eligible for auto-renewal.
NEW Please provide the following information for NEW requests (check ALL that apply):
Diagnosis: Actinic Keratosis → Area affected:
Head or neck Other (specify): ______________________________________________________ Other (specify):
Previous medications/therapies utilized: Please indicate if the following medication/therapy have been tried and the response:
1) cryotherapy: Yes → Response:
Lack of response Intolerance Other (specify):__________________
No → Not appropriate Other (specify):___________________________________ AND
2) 5-fluorouracil (5-FU): Yes→ Response:
Lack of response Intolerance Other (specify):____________________ No (specify reason, if applicable): __________________________________________________
Additional information relating to request
RENEWAL This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31222 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 47
Dutasteride/Finasteride Special Authorization Request Form
On the reverse is the official Dutasteride/Finasteride Special Authorization Request Form (ABC 31257). • All requests for dutasteride or finasteride must be submitted using the Dutasteride/Finasteride
Special Authorization Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
DUTASTERIDE/FINASTERIDE SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Indicate which drug is requested (check one box): Dutasteride Finasteride
Criteria for Coverage of DUTASTERIDE / FINASTERIDE For the treatment of benign prostatic hyperplasia in patients who are poor surgical risks or who have enlarged prostates and have moderate to severe symptoms suggestive of obstruction. Special authorization may be granted for 6 months. This product is eligible for auto-renewal.
NEW Please provide the following information for NEW requests (Section 1, AND Section 2 or 3 must be completed):
Section 1: Diagnosis:
Benign Prostatic Hyperplasia Other (specify): ________________________________________
Section 2: Surgical Risk: Is the patient a poor surgical risk? → no yes If yes, please specify any underlying medical condition(s) or other circumstances by which this patient would be deemed a poor surgical risk:
Has this patient had surgical intervention (TURP) for this condition in the past? yes no
Section 3: Enlarged Prostate: Does this patient have enlarged prostate with moderate to severe symptoms suggestive of obstruction?
yes
no
Additional information relating to request
RENEWAL This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5.
ABC 31257 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 49
Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form
On the reverse is the official Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form (ABC 31258).
• All requests for paliperidone or risperidone prolonged release injection must be submitted using the Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
PALIPERIDONE/RISPERIDONE PROLONGED RELEASE INJECTION SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY, PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Indicate which drug is requested: Risperidone Prolonged Release Injection Paliperidone Prolonged Release Injection
NEW Please provide the following information for NEW requests:
Diagnosis: schizophrenia or related psychotic disorder other, please specify
Compliance Issues: Has this patient demonstrated a pattern of significant non-compliance with other dosage forms that is compromising or has compromised this patient’s therapeutic success?
Yes No If no, please elaborate:
Previous drug therapy (CHECK ALL THAT APPLY): In order to comply with criteria, check at least two of the following:
Experiences extra-pyramidal symptoms with either an oral or depot first generation antipsychotic agent that precludes the use of a first generation antipsychotic depot product
Is refractory to trials of at least two other antipsychotic therapies (Note: one trial must include a first generation antipsychotic agent)
Possesses clinical evidence of previous successful treatment with risperidone or paliperidone therapy
Additional information relating to request
RENEWAL This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31258 (R02/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 51
Abatacept for Juvenile Idiopathic Arthritis Special Authorization Request Form
On the reverse is the official Abatacept for Juvenile Idiopathic Arthritis Special Authorization Request Form (ABC 31291).
• All requests for abatacept for Juvenile Idiopathic Arthritis must be submitted using the Abatacept for Juvenile Idiopathic Arthritis Special Authorization Request Form only.
• Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

ABATACEPT for Juvenile Idiopathic Arthritis
SPECIAL AUTHORIZATION REQUEST FORM Please complete all required sections to allow your request to be processed.
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE:
PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis:
Polyarticular Juvenile Idiopathic Arthritis Other (specify)
Current weight (kg): Dosage: Dosing Frequency:
Current JRA30 FLARE score (provide for ALL requests) JRA30 RESPONSE score at 16 to 20 weeks after first dose of previous abatacept treatment (provide for RETREATMENT requests)
Date of assessment:___________________________ 1. Rheumatologist global 4. No. of joints
assessment (0-10) ___________ with LROM ___________
2. Patient global 5. CHAQ (0-3) ___________
assessment (0-10) ___________
3. No. of active joints* ___________ 6. ESR (mm/hr) __________
or CRP ______________ *joints with swelling not due to deformity or joints with limitation of motion with pain, tenderness or both.
Date of assessment:___________________________ 1. Rheumatologist global 4. No. of joints
assessment (0-10) ___________ with LROM ___________
2. Patient global 5. CHAQ (0-3) ___________
assessment (0-10) ___________
3. No. of active joints* ___________ 6. ESR (mm/hr) __________
or CRP ______________ *joints with swelling not due to deformity or joints with limitation of motion with pain, tenderness or both.
Please provide the following information for all NEW requests: Previous medications utilized: Dose, duration and response is required:
DMARD(s) (specify agents):
Etanercept:
Other (specify agent) :
Additional information relating to request (e.g. reasons why any of the above therapies were not tried):
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780 498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST. The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31291 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 53
63BMontelukast/Zafirlukast Special Authorization Request Form
On the reverse is the official Montelukast/Zafirlukast Special Authorization Request Form (ABC 31313). • All requests for montelukast or zafirlukast must be submitted using the
Montelukast/Zafirlukast Special Authorization Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
MONTELUKAST/ZAFIRLUKAST SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Indicate which drug is requested (check one box): Montelukast (5mg + 10mg) Zafirlukast (20mg)
Criteria for Coverage of MONTELUKAST / ZAFIRLUKAST For the prophylaxis and chronic treatment of asthma in patients over the age of 18 who meet one of the following criteria: a) when used as adjunctive therapy in patients who do not respond adequately to high doses of inhaled glucocorticosteroids and long-acting beta 2 agonists. Patients must be unable to use long-acting beta 2 agonists or have demonstrated persistent symptoms while on long-acting beta 2 agonists, OR b) cannot operate inhaler devices.
For the prophylaxis of exercise-induced bronchoconstriction in patients over the age of 18 where tachyphylaxis exists for long-acting beta 2 agonists.
Special authorization for both criteria may be granted for 6 months. This product is eligible for auto-renewal. Note: Refer to the Alberta Health and Wellness Drug Benefit List for Restricted Benefit coverage of patients 2 to 18 years of age inclusive for Montelukast and 12 to 18 years of age inclusive for Zafirlukast.
NEW Please provide the following information for NEW requests (Section 1, AND Section 2 or 3 must be completed): Section 1: Indication:
Prophylaxis and chronic treatment of asthma (If yes, proceed to Section 2A or 2B only). Prophylaxis of exercise-induced bronchoconstriction (If yes, proceed to Section 3 only). Other (specify): ______________________________________________________________________________________________
Section 2: Prophylaxis and chronic treatment of asthma: A. Previous Medication Use: Is the patient maintained on inhaled glucocorticosteroids?
Yes No (If no, specify reason):_________________________________________________
Is the patient on a long-acting beta 2 agonist (e.g. salmeterol or formoterol)? Yes → Response: Persistent symptoms
Other (specify)_______________________________________________ No (If no, specify reason):________________________________________________________
B. Use of Inhaler Device Please indicate if the patient has difficulty using an inhaler device:
Yes (Please elaborate on the nature of the difficulty)____________ ______________________________
No
Section 3: Prophylaxis of exercise induced bronchoconstriction: Does this patient have tachyphylaxis with long-acting beta 2 agonists? Yes No Other (specify): ___________________________ Additional information relating to request:
RENEWAL: This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy:
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31313 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 55
63BFebuxostat Special Authorization Request Form
On the reverse is the official Febuxostat Special Authorization Request Form (ABC 31376). • All requests for febuxostat must be submitted using the Febuxostat Special Authorization
Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.
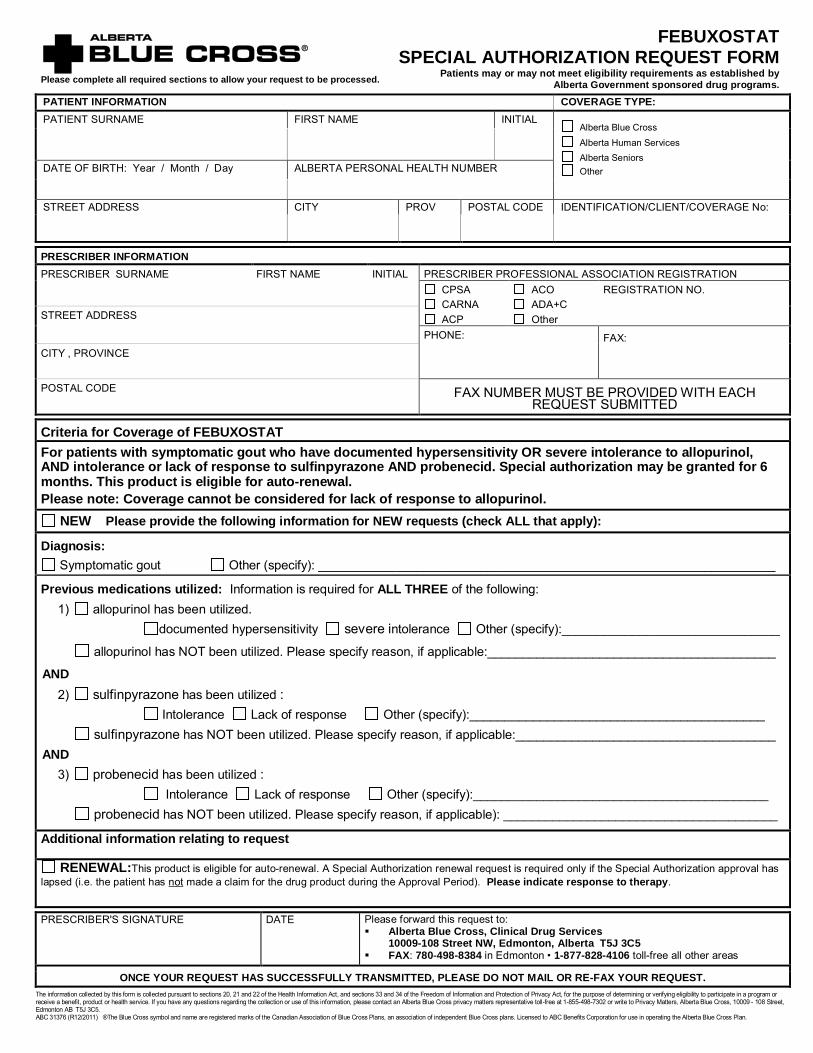
Please complete all required sections to allow your request to be processed.
FEBUXOSTAT SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Coverage of FEBUXOSTAT For patients with symptomatic gout who have documented hypersensitivity OR severe intolerance to allopurinol, AND intolerance or lack of response to sulfinpyrazone AND probenecid. Special authorization may be granted for 6 months. This product is eligible for auto-renewal. Please note: Coverage cannot be considered for lack of response to allopurinol.
NEW Please provide the following information for NEW requests (check ALL that apply):
Diagnosis: Symptomatic gout Other (specify): _________________________________________________________________
Previous medications utilized: Information is required for ALL THREE of the following: 1) allopurinol has been utilized.
documented hypersensitivity severe intolerance Other (specify):_______________________________
allopurinol has NOT been utilized. Please specify reason, if applicable:_________________________________________
AND 2) sulfinpyrazone has been utilized :
Intolerance Lack of response Other (specify):__________________________________________ sulfinpyrazone has NOT been utilized. Please specify reason, if applicable:_____________________________________
AND 3) probenecid has been utilized :
Intolerance Lack of response Other (specify):__________________________________________ probenecid has NOT been utilized. Please specify reason, if applicable): _______________________________________
Additional information relating to request
RENEWAL:This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy.
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31376 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 57
63BDenosumab Special Authorization Request Form
On the reverse is the official Denosumab Special Authorization Request Form (ABC 31377). • All requests for denosumab must be submitted using the Denosumab Special Authorization
Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

Please complete all required sections to allow your request to be processed.
DENOSUMAB SPECIAL AUTHORIZATION REQUEST FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION COVERAGE TYPE: PATIENT SURNAME FIRST NAME INITIAL
Alberta Blue Cross Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
PRESCRIBER INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION
CPSA CARNA ACP
ACO ADA+C Other
REGISTRATION NO.
STREET ADDRESS
PHONE:
FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Criteria for Coverage of DENOSUMAB For the treatment of postmenopausal osteoporosis in women for whom oral bisphosphonates are contraindicated due to hypersensitivity OR an endoscopically or radiographically confirmed untreatable abnormality of the esophagus which delays esophageal emptying (e.g., stricture or achalasia), AND Who have at least two of the following:
- Age of greater than or equal to 75 years - A prior fragility fracture - A bone mineral density (BMD) T-score of of less than or equal to -2.5
Special authorization may be granted for 12 months. Patients will be limited to receiving one dose of denosumab per prescription at their pharmacy. Coverage cannot be provided for two or more osteoporosis medications (alendronate, calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intended for use as combination therapy.
NEW Please provide the following information for NEW requests:
Diagnosis: Postmenopausal osteoporosis Other (specify): ________________________________________
Please indicate which of the following pertain to this patient (check ALL that apply): contraindication to oral bisphosphonates
If so, must specify nature of contraindication _____________________________________________________ endoscopically or radiographically confirmed untreatable abnormality of the esophagus which delays esophageal emptying (e.g., stricture or achalasia)
prior fragility fracture bone mineral density (BMD) T-Score of less than or equal to -2.5
Additional information relating to request
RENEWAL: This product is eligible for auto-renewal. A Special Authorization renewal request is required only if the Special Authorization approval has lapsed (i.e. the patient has not made a claim for the drug product during the Approval Period). Please indicate response to therapy.
PRESCRIBER'S SIGNATURE DATE Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5 FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5.
ABC 31377 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 59
63B63BOmalizumab Special Authorization Request Form
On the reverse is the official Omalizumab Special Authorization Request Form (ABC 31406). • All requests for omalizumab must be submitted using the Omalizumab Special Authorization
Request Form only. • Photocopy this form and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

OMALIZUMAB SPECIAL AUTHORIZATION REQUEST FORM
PATIENT INFORMATION Patients may or may not meet eligibility requirements as established
by Alberta Government sponsored drug programs. PATIENT SURNAME FIRST NAME INITIAL Alberta Blue Cross
Alberta Human Services Alberta Seniors Other
DATE OF BIRTH: Year / Month / Day ALBERTA PERSONAL HEALTH NUMBER
STREET ADDRESS CITY PROV POSTAL CODE IDENTIFICATION/CLIENT/COVERAGE No:
SPECIALIST IN RESPIROLOGY OR CLINICAL IMMUNOLOGIST INFORMATION PRESCRIBER SURNAME FIRST NAME INITIAL PRESCRIBER PROFESSIONAL ASSOCIATION REGISTRATION CPSA
CARNA ACP
ACO ADA+C Other
REGISTRATION NO. STREET ADDRESS
PHONE: FAX: CITY , PROVINCE
POSTAL CODE FAX NUMBER MUST BE PROVIDED WITH EACH REQUEST SUBMITTED
Please provide the following information for ALL requests: Diagnosis:
Confirmation of Severe Asthma Other (specify)
Date of Confirmation of Diagnosis : Current weight (kg):
Smoker Non-Smoker
Laboratory Data (For renewals only FEV1 is required) Scores (For renewals only AQLQ and one ACQ-5 are required) Total serum human immunoglobulin (IgE) Value (IU/ml)
Date Asthma Quality of Life Questionnaire (AQLQ – Juniper) Score
Date
Confirmation of IgE mediated allergy to a perennial allergen by clinical history and allergy skin testing
Date
ACQ-5
Score #1 Date
FEV1 Date Score #2 Date
Please provide the following information for NEW requests: Number of exacerbations of asthma within the previous 12 month period that resulted in: An Emergency Room visit / Hospitalization: Unscheduled physician visits resulting in oral corticosteroids: Please check one of the following :
One or more severe exacerbations of asthma requiring a hospital admission or Emergency Room visit within the previous year while on systemic corticosteroids: OR One or more severe exacerbations of asthma requiring a hospital admission or Emergency Room visit requiring documented use of systemic corticosteroids (oral corticosteroids initiated or increased for at least 3 days, or parenteral corticosteroids); OR Three or more severe exacerbations of asthma within the previous year, which required an unscheduled physician visit and resulted in courses (or chronic use >50% of the year) of systemic corticosteroids.
Previous medications utilized: Name of Medication, dose, duration and response is required for ALL of the following: High-dose inhaled corticosteroids :
Long-acting beta-2 agonists :
Oral corticosteroids :
Chronic use (>50% of the year) of oral corticosteroids? YES NO
Please provide the following information for all RENEWAL requests: Number of exacerbations of asthma within the previous 12 month period that resulted in: An Emergency Room visit / Hospitalization: Unscheduled physician visits resulting in oral corticosteroids: Please check ALL of the following that apply :
Patient demonstrated at least a 25% reduction in the number of exacerbations, which required oral corticosteroids from the 12 months prior to initiation of omalizumab that required systemic corticosteroids. For patients that were on chronic (>50% of the year) courses of oral corticosteroids use in the prior 12 months to initiation of omalizumab, tapering of oral corticosteroid use by at least 25% from baseline. A reduction in the number of exacerbations that have led to a hospital admission or emergency room visits, compared to the 12 months prior to the commencement of omalizumab.
PRESCRIBER'S SIGNATURE DATE
Please forward this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5
FAX: 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas ONCE YOUR REQUEST HAS SUCCESSFULLY TRANSMITTED, PLEASE DO NOT MAIL OR RE-FAX YOUR REQUEST.
The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31406 (2011/12) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 1A • 61
Eculizumab Special Authorization Request Form and Consent Form
On the reverse is the official Eculizumab Special Authorization Request Form (ABC 31386) and the official Eculizumab Consent Form (ABC 31408)
• All requests for eculizumab must be submitted using the Eculizumab Special Authorization Request Form and Eculizumab Consent Form.
• Photocopy these forms and use as required. • Submit completed forms by FAX to Alberta Blue Cross:
(780) 401-1150 in Edmonton and area 1-888-401-1150 toll-free for all other areas
Once your request has successfully transmitted, please do not mail or re-fax your request.

ECULIZUMAB SPECIAL AUTHORIZATION REQUEST FORM Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION Page 1 of 4 Patient Surname First Name Middle Initial Sex Date of Birth Alberta Personal Health Number M / F Year Month Day
Street Address City Province Postal Code
Identification/Client/Coverage No: Coverage
Type: Alberta Blue Cross Alberta Human Services
Alberta Seniors Other
SPECIALIST IN HEMATOLOGY INFORMATION Surname First Name Middle Initial
Street Address City Province Postal Code
Telephone Number Fax Number College of Physicians and Surgeons Registration No.
Date Form Completed Last Consult Date Specialist in Hematology Signature
INFORMATION REQUIRED
For INITIAL REQUESTS please complete the first 2 pages, and submit laboratory data and consent form as attachments. For SIX-MONTH RENEWALS please complete applicable sections of the first 3 pages, and submit laboratory data as an attachment. For ANNUAL RENEWALS please complete applicable sections of all 4 pages, and submit laboratory data as an attachment. Note: Additional pages may be attached as required. Please submit all required pages and attachments together. TREATMENT REQUESTED
Eculizumab (Soliris) Dosage and Frequency Requested
Check which situation applies and provide date requested.
New to Drug: Planned treatment start date (YY/MM/DD) New to Coverage (on drug already): Date treatment began (YY/MM/DD) Renewal
CONFIRMATION OF DIAGNOSIS (Complete on initial request) Yes No Date (YY/MM/DD) Lab result Does the patient have a PNH granulocyte clone size (by flow cytometry and/or FLAER test) equal to or greater than 10%?
Does the patient have a Lactate Dehydrogenase (LDH) level at least 1.5 times the upper limit of normal?
Please mail this request to: Alberta Blue Cross, Clinical Drug Services
10009-108 Street NW, Edmonton, Alberta T5J 3C5
Or fax to 780-401-1150 in Edmonton 1-888-401-1150 toll-free all other areas
Case Number
The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31386 (2011/12) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ECULIZUMAB SPECIAL AUTHORIZATION REQUEST FORM
Patient’s Alberta Personal
Health Number (only) Page 2 of 4
ADDITIONAL CLINICAL CRITERIA (Complete on initial request) Does the patient have any of the following? Yes No Comment
a) Thrombosis: Evidence that the patient has had a thrombotic or embolic event which required the institution of therapeutic anticoagulant therapy
b) Transfusions: Evidence that the patient has been transfused with at least four units of red blood cells in the last twelve months
c) Anemia: Evidence that the patient has chronic or recurrent anemia where causes other than hemolysis have been excluded and demonstrated by more than one measure of less than or equal to 70g/L or by more than one measure of less than or equal to 100 g/L with concurrent symptoms of anemia
d) Pulmonary insufficiency: Evidence that the patient has debilitating shortness of breath and/or chest pain resulting in limitation of normal activity (New York Heart Association Class III) and/or established diagnosis of pulmonary arterial hypertension, where causes other than PNH have been excluded
e) Renal insufficiency: Evidence that the patient has a history of renal insufficiency, demonstrated by an eGFR less than or equal to 60mL/min/1.73m2, where causes other than PNH have been excluded
f) Smooth muscle spasm: Evidence that the patient has recurrent episodes of severe pain requiring hospitalisation and/or narcotic analgesia, where causes other than PNH have been excluded
CONTRAINDICATIONS TO COVERAGE Does the patient have any of the following? Yes No Small granulocyte clone size - a granulocyte clone size below 10% Aplastic anaemia with two or more of the following: neutrophil count below 0.5 x 109/L, platelet count below 20 x 109/L, reticulocytes below 25 x 109/L, or severe bone marrow hypocellularity
Presence of another life threatening or severe disease where the long term prognosis is unlikely to be influenced by therapy (for example acute myeloid leukaemia or high-risk myelodysplastic syndrome)
Presence of another medical condition that might reasonably be expected to compromise a response to therapy
MENINGOCOCCAL VACCINATION
Yes No Vaccination date (YY/MM/DD) Initial Requests: Has the patient received a meningococcal vaccination with a quadravalent vaccine (A,C,Y and W135) at least two weeks prior to receiving the first dose of eculizumab?
Renewal Requests: Has the patient been monitored and revaccinated according to current medical guidelines for vaccine use?
TRANSFUSION HISTORY (please provide data for the last 12 months on initial requests, and for the last 6 months on renewals)
Transfusion Date (YY/MM/DD) RBC Units Platelet Units Comment
ABC 31386 (2011/12) ® The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.
Case Number

ECULIZUMAB SPECIAL AUTHORIZATION REQUEST FORM
Patient’s Alberta Personal
Health Number (only) Page 3 of 4
MONITORING REQUIREMENTS (Please attach the following laboratory results with each renewal request) - Lactate dehydrogenase (LDH) - Full blood count and reticulocytes - Iron studies - Urea, electrolytes and eGFR Recent clinical history (Update for each renewal request, attach additional pages as required)
ABC 31386 (2011/12) ® The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.
Case Number

ECULIZUMAB SPECIAL AUTHORIZATION REQUEST FORM
Patient’s Alberta Personal
Health Number (only) Page 4 of 4
MONITORING REQUIREMENTS (Please attach the following laboratory results with annual renewal requests or more frequently if required)
- PNH Granulocyte clone size (by flow cytometry)
Progress report on the clinical symptoms that formed the basis of initial eligibility (Update annually, attach additional pages as required) Thrombosis Transfusions Anemia Pulmonary insufficiency Renal insufficiency Smooth Muscle Spasm
Quality of life, through clinical narrative (Update annually, attach additional pages as required)
ABC 31386 (2011/12) ® The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.
Case
Number

ECULIZUMAB CONSENT FORM
Patients may or may not meet eligibility requirements as established by Alberta Government sponsored drug programs.
PATIENT INFORMATION Page 1 of 2 Patient Surname First Name Middle Initial Sex Date of Birth Alberta Personal Health Number M / F Year Month Day
Street Address City Province Postal Code
Identification/Client/Coverage No: Coverage
Type: Alberta Blue Cross Alberta Human Services
Alberta Seniors Other
SPECIALIST IN HEMATOLOGY INFORMATION Surname First Name Middle Initial
Street Address City Province Postal Code
Telephone Number Fax Number College of Physicians and Surgeons Registration No.
PATIENT CONSENT FOR SERVICE I have received a copy of the policy relating to Eculizumab in the current version of the Alberta Health and Wellness Drug Benefit List (AHWDBL), as updated from time to time (the Policy) and have read and understand the requirements of a patient receiving Alberta government sponsored funded treatment.
I agree to comply with the requirements for coverage as set out in the Policy, including (without limitation) the requirements for monitoring, review and data collection.
I understand and agree that I must continue to qualify for, and continue to be a member of, an Alberta government sponsored drug program to continue to be eligible for eculizumab coverage in accordance with the Policy.
I understand and agree that approval for initial and continued coverage is conditional upon meeting and continuing to meet the requirements of the Policy.
I understand that my consent must be and is ongoing and my failure to comply with the requirements as set out in the Policy may preclude me from continuing to be eligible for eculizumab coverage.
I understand that prior to potential discontinuance of eculizumab coverage, as outlined in the Policy, my Specialist in Hematology will receive notice of this in writing. I understand that my Specialist in Hematology has a responsibility to notify me, and to work with me to address the reason for potential withdrawal of eculizumab coverage.
I understand that therapy may be withdrawn at the request of the patient or the patient’s parent/guardian at any time. Notification of withdrawal from therapy must be made by the Specialist in Hematology or patient in writing. I understand there may be side effects from medication and I have discussed the risks and benefits of this treatment with my Specialist in Hematology.
I, either as the patient or as the patient’s parent/guardian (as appropriate), and on behalf of the patient’s heirs and my estate and any other person claiming through the patient, hereby release the Minister, the Minister’s delegate, the Minister’s agents and employees from any and all liability and all claims for any and all damages, injuries, loss and costs which may arise directly or indirectly in relation to or in connection with the Application and coverage, funding and use of eculizumbab for the patient pursuant to the Policy, including (without limitation) all claims relating to coverage, any changes in coverage, any restrictions or conditions of coverage, discontinuance of coverage, and the patient’s use of eculizumab. I agree and acknowledge that this release is binding on the patient, the patient’s heirs and estate, and any other person claiming through the patient against the Minister, the Minister’s agents and employees.
Name of Patient: ___________________________________________________
Signature of Patient (for patients > or equal to 18 years old): _________________________________ Date: ____________________
Name of Parent/Guardian (for patients <18 years old): _______________________________________________________________
Signature of Parent/Guardian (for patients <18 years old): ___________________________________ Date: ____________________
The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 31408 (12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

Section 2 Multiple Sclerosis (M
S) Drug C
overage
SECTION 2
Multiple Sclerosis (MS) Drug Coverage

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST REFRESHED MULTIPLE SCLEROSIS (MS) DRUG COVERAGE
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 2 • 1 EFFECTIVE APRIL 1, 2012
MULTIPLE SCLEROSIS (MS) DRUG COVERAGE
Selected drug products used in the treatment of relapsing multiple sclerosis (MS) may be considered for coverage for patients covered under Alberta government-sponsored drug programs. For further information regarding eligibility for Alberta government-sponsored drug programs, refer to the Introduction section of the List.
In order to be eligible for Multiple Sclerosis (MS) Drug Coverage, an individual must:
have valid Alberta government-sponsored drug coverage; meet specific clinical criteria according to Multiple Sclerosis (MS) Drug Coverage program
requirements; have a Multiple Sclerosis (MS) Drug Coverage Application form(s) submitted on their behalf to Alberta
Blue Cross by any “MS Neurologist” identified by the Alberta Multiple Sclerosis (MS) Drug Review Panel, and
have their Application approved by the Review Panel.
64BClinical Criteria to be considered for Coverage
To be considered for coverage of Avonex, Betaseron/Extavia, Copaxone, and Rebif, patients must be assessed by an “MS Neurologist” and meet the following clinical criteria: have a diagnosis of clinically definite relapsing-remitting multiple sclerosis:
• have had at least two attacks/exacerbations of MS during the previous two years. (An attack is defined as the appearance of new symptoms or worsening of old symptoms, lasting at least 48 hours in the absence of fever, not associated with withdrawal from steroids. Attacks must be separated by a period of at least one month.)
• are ambulatory with or without aid (i.e. a cane or walker). OR to be considered for coverage of Betaseron/Extavia: have a diagnosis of secondary progressive multiple sclerosis with relapses:
• have had at least two attacks/exacerbations of MS during the previous two years. (An attack is defined as the appearance of new symptoms or worsening of old symptoms, lasting at least 72 hours in the absence of fever, not associated with withdrawal from steroids, and preceded by stability for at least one month. Attacks must be separated by a period of at least one month.)
• have an EDSS score of less than or equal to 5.5. To be considered for coverage of Tysabri, see the clinical criteria as listed in the Drug Products Under Multiple Sclerosis (MS) Drug Coverage Program.
65BContraindications to Coverage
In addition to meeting the above clinical criteria, the patient must have none of the following contraindications:
Significant illness likely to alter compliance or substantially reduce life expectancy. Active, severe depression: in the absence of a depression waiver from a psychologist or psychiatrist.
The depression waiver must accompany the Multiple Sclerosis (MS) Drug Coverage Application form(s) for patients with active, severe depression.
Planned or current pregnancy, nursing women. Contraindications for Tysabri, refer to the clinical criteria as listed in the Drug Products Under Multiple
Sclerosis (MS) Drug Coverage Program.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST REFRESHED MULTIPLE SCLEROSIS (MS) DRUG COVERAGE
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 2 • 2
66BAlberta Multiple Sclerosis (MS) Drug Review Panel
The Alberta Multiple Sclerosis (MS) Drug Review Panel is an external review panel composed of neurologists and other health professionals with expertise in MS, appointed by the Minister of Health and Wellness.
The Review Panel’s functions include:
making recommendations to Alberta Health and Wellness on Multiple Sclerosis (MS) Drug Coverage program requirements, including maintenance of the eligibility criteria;
identifying “MS Neurologists” for the purposes of this program, and; reviewing applications for Multiple Sclerosis (MS) Drug Coverage.
67BProcess for Multiple Sclerosis (MS) Drug Coverage
Participating “MS Neurologists” must complete a separate Multiple Sclerosis (MS) Drug Coverage Application form(s) for each patient. The completed application may be forwarded to Alberta Blue Cross by mail or by facsimile.
Alberta Blue Cross, in providing administrative support to the Review Panel, receives and screens each application for completeness, then forwards it to the Review Panel for assessment. Alberta Blue Cross responds to applicants on the Review Panel’s behalf. After an application is assessed by the Review Panel, Alberta Blue Cross notifies the “MS Neurologist” and the patient by letter of the Review Panel’s decision. If the patient is approved for Multiple Sclerosis (MS) Drug Coverage an MS Nurse (a nurse with extensive knowledge of MS and MS therapies) will provide the patient with education regarding: (i) potential benefits and limitations of therapy, (ii) side-effects, (iii) how drug administration will be taught, (iv) how the patient will be followed, (v) how the patient can access help or information, (vi) how the treatment will be reimbursed and the requirements for reimbursement, (vii) indications for treatment to possibly be discontinued, and (viii) what should be reported and to whom. The MS Nurse will also ensure that the prescribing neurologist is aware of the timelines for the necessary ongoing follow-up to ensure safe and appropriate ongoing use of therapies. A new Multiple Sclerosis (MS) Drug Coverage Application form(s) must be completed by an “MS Neurologist” to review coverage if the patient requires a different Multiple Sclerosis (MS) Drug and for renewal requests.
To be eligible for Multiple Sclerosis (MS) Drug Coverage, prescriptions must be written by an “MS Neurologist” identified by the Review Panel. Regular monitoring of patients during the first year of therapy is needed in order to ensure the appropriate treatment option and dose, and to minimize the potential for wastage. Therefore, prescription quantities are limited to a one-month supply for the first year of therapy. This also applies to drug changes and to patients new or transferring to this program. Once the patient has been stabilized on a MS drug (excluding Tysabri) and dosage for one year and received program renewal authorization, up to 100 days’ supply may be dispensed at a time.
Government will not be responsible for reimbursement of costs associated with wastage or improper storage of the drug.
Prior approval must be granted to ensure coverage. Approval is granted for a specific period, to a maximum of 12 months unless otherwise indicated. If continued treatment is necessary, it is the responsibility of the patient and “MS Neurologist” to re-apply for drug coverage prior to the expiry date of the authorization period.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST REFRESHED MULTIPLE SCLEROSIS (MS) DRUG COVERAGE
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 2 • 3 EFFECTIVE APRIL 1, 2012
Completed Multiple Sclerosis (MS) Drug Coverage Application forms should be directed by mail or FAX to: Clinical Drug Services Alberta Blue Cross 10009 108 Street NW Edmonton, Alberta T5J 3C5
(780) 498-8384 in Edmonton and area 1-877-828-4106 toll-free for all other areas
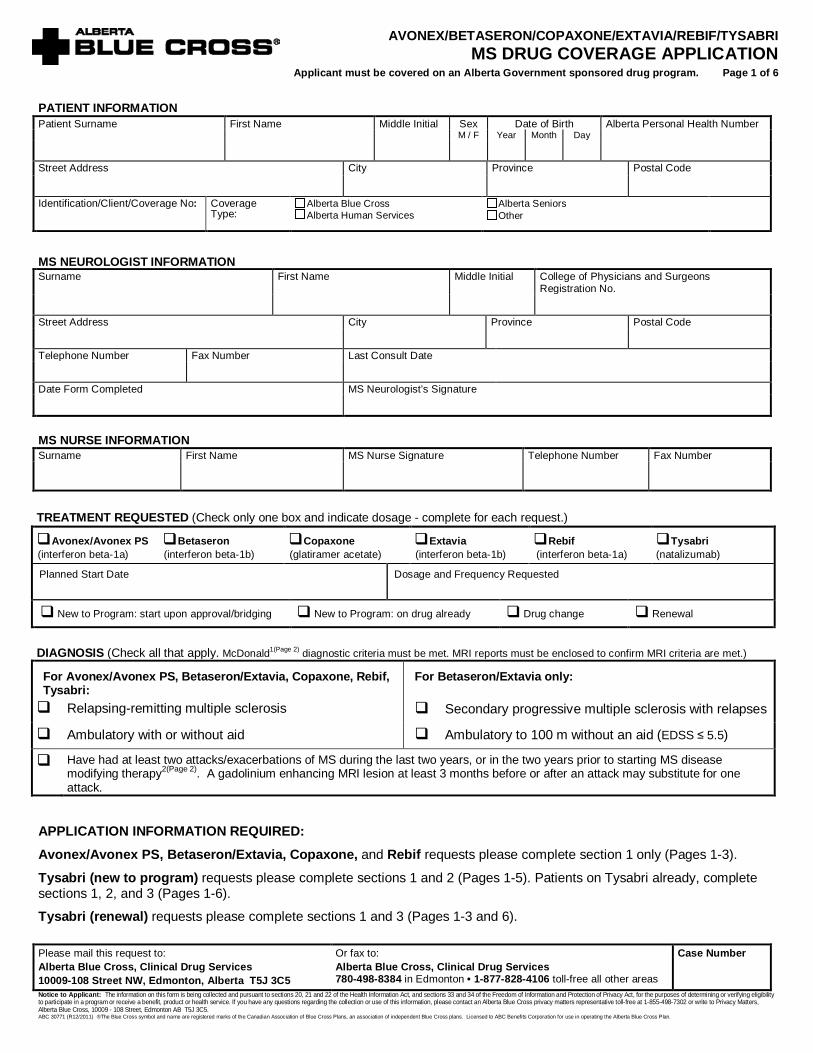
AVONEX/BETASERON/COPAXONE/EXTAVIA/REBIF/TYSABRI MS DRUG COVERAGE APPLICATION
Applicant must be covered on an Alberta Government sponsored drug program. Page 1 of 6
PATIENT INFORMATION Patient Surname First Name Middle Initial Sex Date of Birth Alberta Personal Health Number M / F Year Month Day
Street Address City Province Postal Code
Identification/Client/Coverage No: Coverage
Type:
Alberta Blue Cross Alberta Human Services
Alberta Seniors Other
MS NEUROLOGIST INFORMATION Surname First Name Middle Initial College of Physicians and Surgeons
Registration No.
Street Address City Province Postal Code
Telephone Number Fax Number Last Consult Date
Date Form Completed MS Neurologist’s Signature
MS NURSE INFORMATION Surname First Name MS Nurse Signature Telephone Number Fax Number
TREATMENT REQUESTED (Check only one box and indicate dosage - complete for each request.)
Avonex/Avonex PS (interferon beta-1a)
Betaseron (interferon beta-1b)
Copaxone (glatiramer acetate)
Extavia (interferon beta-1b)
Rebif (interferon beta-1a)
Tysabri (natalizumab)
Planned Start Date Dosage and Frequency Requested
New to Program: start upon approval/bridging New to Program: on drug already Drug change Renewal
DIAGNOSIS (Check all that apply. McDonald1(Page 2) diagnostic criteria must be met. MRI reports must be enclosed to confirm MRI criteria are met.)
For Avonex/Avonex PS, Betaseron/Extavia, Copaxone, Rebif, Tysabri: Relapsing-remitting multiple sclerosis
For Betaseron/Extavia only:
Secondary progressive multiple sclerosis with relapses
Ambulatory with or without aid Ambulatory to 100 m without an aid (EDSS ≤ 5.5)
Have had at least two attacks/exacerbations of MS during the last two years, or in the two years prior to starting MS disease modifying therapy2(Page 2). A gadolinium enhancing MRI lesion at least 3 months before or after an attack may substitute for one attack.
APPLICATION INFORMATION REQUIRED: Avonex/Avonex PS, Betaseron/Extavia, Copaxone, and Rebif requests please complete section 1 only (Pages 1-3).
Tysabri (new to program) requests please complete sections 1 and 2 (Pages 1-5). Patients on Tysabri already, complete sections 1, 2, and 3 (Pages 1-6).
Tysabri (renewal) requests please complete sections 1 and 3 (Pages 1-3 and 6). Please mail this request to: Alberta Blue Cross, Clinical Drug Services 10009-108 Street NW, Edmonton, Alberta T5J 3C5
Or fax to: Alberta Blue Cross, Clinical Drug Services 780-498-8384 in Edmonton • 1-877-828-4106 toll-free all other areas
Case Number
Notice to Applicant: The information on this form is being collected and pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purposes of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection or use of this information, please contact an Alberta Blue Cross privacy matters representative toll-free at 1-855-498-7302 or write to Privacy Matters, Alberta Blue Cross, 10009 - 108 Street, Edmonton AB T5J 3C5. ABC 30771 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

AVONEX/BETASERON/COPAXONE/EXTAVIA/REBIF/TYSABRI MS DRUG COVERAGE APPLICATION
Section 1: Complete for ALL MS Drug applications Patient’s Alberta Personal
Health Number (only) Page 2 of 6
PREVIOUS MS DISEASE MODIFYING TREATMENT (Complete for each request.)
DRUG DATE STARTED DATE STOPPED REASON FOR DRUG STOPPAGE*
* Examples of reasons drug may be stopped: lack of efficacy, intolerability, non-compliance, pregnancy, financial reasons, interferon antibody positive
CONTRAINDICATIONS (Complete for each request.)
Yes No
1. Significant illness likely to alter compliance or substantially reduce life expectancy........................................................................... 2. Planned or current pregnancy, or nursing............................................................................................................................................ 3. a. Active, severe depression; or ……………………………………………………………………………………………………………..
b. Active, severe depression; waiver from a psychologist or psychiatrist attached3......................................................................... 4. Progression without relapse4...........................................................................................................................................................….
OTHER CLINICAL DATA (Complete for each request.)
Age: Gender: Male Female Date of onset: ___________/___________(Year/Month)5
Current Prescribed Medications:
Allergies:
Page 1 and 2: 1. McDonald Criteria (Ann Neurol 2001; 50:121-127) Summary: patients must meet one of the following conditions:
a) 2 attacks confirmed by objective findings and evidence of 2 clinically objective lesions. b) 2 attacks confirmed by objective findings, and 1 clinically objective lesion, and either dissemination in space by MRI as below or at least 2 MRI lesions
and CSF oligoclonal bands or increased IgG index. c) 1 attack confirmed by objective findings, and 2 clinically objective lesion sites, and dissemination in time by MRI. d) 1 attack confirmed by objective findings, and 1 clinically objective lesion, and dissemination in space by MRI [or 2 MRI lesions and + CSF] and
dissemination in time by MRI. Dissemination in space by MRI: (3 of 4 of the following): 1) 1 gd+ lesion or 9 T2 hyperintense lesions (cord or brain); 2) 1 infratentorial lesion; 3) 1 juxtacortical lesion; 4) 3 periventricular lesions Dissemination in time by MRI: Either 1) a gd+ lesion on an MRI at least 3 (or more) months after an attack, at a different site; or, 2) a new T2 lesion at least 3 months after scan that was completed at least 3 months after the initial documented attack, at a different site.
2. In RRMS an attack is defined as the appearance of new symptoms or worsening of old symptoms, lasting at least 48 hours in the absence of fever, and not associated with withdrawal from steroids. In SPMS it is more difficult to differentiate attacks from disease fluctuation; therefore, attacks must meet these criteria, must have lasted at least 72 hours, and new neurologic deficits must have been documented by a physician. Attacks must be separated by a period of at least one month.
3. Required prior to approval for all patients who have not been on treatment for at least 6 months. 4. Progression is worsening neurologic impairment not due to residual deficits from attacks. 5. Consider onset as the time of first convincing MS symptoms. This would include episodes such as transverse myelitis or optic neuritis, but not (in most
cases) non-specific symptoms such as dizziness, visual blurring or fatigue.
Case Number
ABC 30771 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

AVONEX/BETASERON/COPAXONE/EXTAVIA/REBIF/TYSABRI MS DRUG COVERAGE APPLICATION
Section 1: Complete for ALL MS Drug applications Patient’s Alberta Personal
Health Number (only) Page 3 of 6
QUALIFYING ATTACKS (Not required for renewals.)
TWO MOST RECENT ATTACKS:
Date of attack onset (or MRI):
MRI ATTACK EQUIVALENT
(Y/N)
SEVERITY6 RECOVERY FUNCTIONAL SYSTEMS INVOLVED OBJECTIVE CHANGES
(SPMS ONLY)
Year Month Day Yes No
Mild Moderate Severe Very Severe
None Incomplete Complete
Pyramidal Sensory Cerebellar Brain Stem Bowel/bladder Visual Cognitive/cerebral
Yes No
Year Month Day Yes No
Mild Moderate Severe Very Severe
None Incomplete Complete
Pyramidal Sensory Cerebellar Brain Stem Bowel/bladder Visual Cognitive/cerebral
Yes No
BASELINE AND FOLLOW-UP DATA (Complete for each request.)
PRE DRUG
YY/MM/DD
CURRENT if on drug
YY/MM/DD
YEAR 1
YY/MM/DD
YEAR 2
YY/MM/DD
YEAR 3
YY/MM/DD
YEAR 4
YY/MM/DD
Date7 (Year / Month / Day)
EDSS
Pyramidal
Cerebellar
Brain Stem
Visual Score
Sensory
Bowel/Bladder
Cognitive
# of attacks during 2 yrs prior to baseline assessment
# of attacks during the last 12 months
Relapse at time of assessment (Yes or No)
Progressive course (Yes or No)
Interferon antibodies (Yes, No, Not applicable, or Unknown)
6. Severity: Mild - symptoms present but no change in function; Moderate - requires modification or more time to carry out activity; Severe - unable to carry
out usual activity; Very Severe - requires others to provide personal care for them. 7. Date of examination must be 0-6 months preceding this request, or if already on drug, from the most recent annual assessment.
Case Number
ABC 30771 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

AVONEX/BETASERON/COPAXONE/EXTAVIA/REBIF/TYSABRI MS DRUG COVERAGE APPLICATION
Section 2: Complete for NEW Tysabri requests Patient’s Alberta Personal Health Number (only)
Page 4 of 6
ELIGIBILITY Yes No
Patient has previously been demonstrated to have at least nine T2 hyperintense lesions on brain MRI NEUTRALIZING ANTIBODIES, INTOLERANCE, OR REFRACTORY TO INTERFERON BETA (Avonex, Betaseron/Extavia, or Rebif) Patient has demonstrated one of the following: I. NEUTRALIZING ANTIBODIES to INTERFERON Yes No Clinically significant titres, report must be provided
OR II. INTOLERANCE TO INTERFERON BETA (Avonex, Betaseron/Extavia, or Rebif) Yes No 'Intolerance' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs, or a persisting adverse event that is unresponsive to recommended management techniques and which is incompatible with further use of that class of DMT. Describe the intolerance and response to management techniques tried in detail below (or attach letter):
OR
III. REFRACTORY TO INTERFERON BETA (Avonex, Betaseron/Extavia, or Rebif) Within a 12 month period on drug: Yes No
a. The patient reported adherence to the interferon beta at the standard dose defined as receiving 80% of prescribed dosing
EITHER b or c:
b. The patient experienced two relapses (neurologic deficits must have persisted for at least 3 months for one of the relapses; an exception may be considered where the second relapse is severe6(page 3) and the application is submitted within 3 months of the relapse onset):
Date of Onset YYYY/MM/DD Neurologic Deficits (describe) Persistence of Deficits:
Clinical Relapse 1 (>30 days from initiation of DMT)
Residual Deficits: Yes No If Yes, how long after onset were deficits detected (e.g., 3 months):
Clinical Relapse 2 (>30 days from relapse 1)
If applying within 3 months of onset, also describe severity of deficits: Residual Deficits: Yes No
If Yes, how long after onset were deficits detected (e.g., 3 months):
OR c. The patient experienced one relapse and one inflammatory event on MRI report (neurologic deficits must have persisted for at least 1 month for the relapse):
Date of Onset YYYY/MM/DD Neurologic Deficits (describe) Persistence of Deficits:
Clinical Relapse (>30 days from initiation of DMT)
Neurologic deficits on examination at least one month after relapse onset: Yes No
MRI (>90 days from clinical relapse; attach reports) A definite gadolinium enhancing T1 lesion (not questionable faint enhancement) that was present on an MRI obtained at least 3 months after initiation of DMT and not within 3 months of a relapse; OR The appearance of 2 or more new, or newly enlarging, T2 hyperintense lesions, greater than 3 mm in size. - To confirm that these new T2 lesions occurred on treatment, the baseline MRI must have been completed at least one month after starting DMT. - To confirm that the MRI lesions were not associated with the relapse, the relapse can not have occurred between the 2 MRI scans. - To confirm that the T2 lesions occurred during the 12 month qualifying period, both MRI scans and the relapse must occur within a 12 month period.
Yes No
Case Number
ABC 30771 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

AVONEX/BETASERON/COPAXONE/EXTAVIA/REBIF/TYSABRI MS DRUG COVERAGE APPLICATION
Section 2: Complete for NEW Tysabri requests Patient’s Alberta Personal Health Number (only)
Page 5 of 6
INTOLERANCE OR REFRACTORY TO GLATIRAMER ACETATE (Copaxone) Patient has demonstrated one of the following:
I. INTOLERANCE TO GLATIRAMER ACETATE (Copaxone) Yes No 'Intolerance' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs, or a persisting adverse event that is unresponsive to recommended management techniques and which is incompatible with further use of that class of DMT. Describe the intolerance and response to management techniques tried in detail below (or attach letter):
OR
II. REFRACTORY TO GLATIRAMER ACETATE (Copaxone) Within a 12 month period on drug:
Yes No
a. The patient reported adherence to the glatiramer acetate at the standard dose defined as receiving 80% of prescribed dosing EITHER b or c:
b. The patient experienced two relapses (neurologic deficits must have persisted for at least 3 months for one of the relapses; an exception may be considered where the second relapse is severe6(page 3) and the application is submitted within 3 months of the relapse onset):
Date of Onset YYYY/MM/DD Neurologic Deficits (describe) Persistence of Deficits:
Clinical Relapse 1 (>30 days from initiation of DMT)
Residual Deficits: Yes No If Yes, how long after onset were deficits detected (e.g., 3 months):
Clinical Relapse 2 (>30 days from relapse 1)
If applying within 3 months of onset, also describe severity of deficits: Residual Deficits: Yes No
If Yes, how long after onset were deficits detected (e.g., 3 months):
OR c. The patient experienced one relapse and one inflammatory event on MRI report (neurologic deficits must have persisted for at least 1 month for the relapse):
Date of Onset YYYY/MM/DD Neurologic Deficits (describe) Persistence of Deficits:
Clinical Relapse (>30 days from initiation of DMT)
Neurologic deficits on examination at least one month after relapse onset: Yes No
MRI (>90 days from clinical relapse; attach reports) A definite gadolinium enhancing T1 lesion (not questionable faint enhancement) that was present on an MRI obtained at least 3 months after initiation of DMT and not within 3 months of a relapse; OR The appearance of 2 or more new, or newly enlarging, T2 hyperintense lesions, greater than 3 mm in size. - To confirm that these new T2 lesions occurred on treatment, the baseline MRI must have been completed at least one month after starting DMT. - To confirm that the MRI lesions were not associated with the relapse, the relapse can not have occurred between the 2 MRI scans. - To confirm that the T2 lesions occurred during the 12 month qualifying period, both MRI scans and the relapse must occur within a 12 month period.
Yes No
CONTRAINDICATIONS (Does the patient have any of the following?): Yes No
1. Any evidence of disease progression independent of relapses (i.e., has developed secondary progressive MS)………………………………..
2. Immune compromised due to immunosuppressant or antineoplastic therapy or due to immunodeficiency (HIV, leukemia, lymphoma, etc.)…
3. History of progressive multifocal leukoencephalopathy (PML)…………………………………………………………………………………………..
4. Concurrent malignancy, or significant illness likely to alter compliance or substantially reduce life expectancy ………………………………….
5. Planned or current pregnancy, or nursing …………………………………………………………………………………………………………………
Case Number ABC 30771 (R12/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan

AVONEX/BETASERON/COPAXONE/EXTAVIA/REBIF/TYSABRI MS DRUG COVERAGE APPLICATION
Section 3: Complete for Tysabri Renewals and patients Patient’s Alberta Personal
Health Number (only) Page 6 of 6
currently on Tysabri
Tysabri treatment start date (YYYY/MM/DD): ________________ Yes No
The patient has not missed any doses, or delayed any doses by more than 1 week with the exception of medically authorized delays (Rationale for such delays must be justified in a narrative; only serious medical conditions are acceptable)
The patient must be assessed by an MS Neurologist and have an MRI with gadolinium at least every 12 months (attach reports)
NEUTRALIZING ANTIBODIES TO TYSABRI (Complete for patients currently on Tysabri.)
There must be evidence that neutralizing antibodies to Tysabri are absent (attach report):
Are neutralizing antibodies absent at 6 to 8 months after initiation of therapy?
Yes If Yes: no further testing is required No If No: Are neutralizing antibodies absent on repeat testing? Yes No
RESPONSE TO TYSABRI (Complete for ALL patients on Tysabri, update for each request.)
On assessment, the MS Neurologist must confirm in writing that the patient is a 'responder': Yes No There has been no more than one inflammatory event in the last year (defined as either a clinical relapse or gadolinium enhancing lesion): If no, the patient had four or more relapses in the year prior to starting treatment, and there is at least a 50% reduction in relapse rate over the entire Tysabri treatment period.
PRIOR to Tysabri treatment: Indicate confirmed inflammatory events over the 2 years prior to initiation of treatment with Tysabri (include all independent clinical relapses and MRI events):
WHILE ON Tysabri treatment: Indicate all confirmed inflammatory events after initiation of treatment with Tysabri (include all independent clinical relapses and MRI events):
MRI Clinical relapse
Date of onset/MRI (YYYY/MM/DD)
No inflammatory events
MRI Clinical relapse
Date of onset/MRI (YYYY/MM/DD)
CONTRAINDICATIONS (Complete at every renewal. Does the patient have any of the following?): Yes No 1. Any evidence of disease progression independent of relapses (i.e., has developed secondary progressive MS)………………………………….
2. Immune compromised due to immunosuppressant or antineoplastic therapy or due to immunodeficiency (HIV, leukemia, lymphoma, etc.)…..
3. History of progressive multifocal leukoencephalopathy (PML)…………………………………………………………………………………………….
4. Concurrent malignancy, or significant illness likely to alter compliance or substantially reduce life expectancy ……………………………………
5. Planned or current pregnancy, or nursing …………………………………………………………………………………………………………………..
Case Number ABC 30771 (R02/2011) ®The Blue Cross symbol and name are registered marks of the Canadian Association of Blue Cross Plans, an association of independent Blue Cross plans. Licensed to ABC Benefits Corporation for use in operating the Alberta Blue Cross Plan.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTMULTIPLE SCLEROSIS (MS) DRUG COVERAGE
GLATIRAMER ACETATE
INTERFERON BETA-1A
INTERFERON BETA-1A/ INTERFERON BETA-1A
INTERFERON BETA-1B
20 MG / SYR INJECTION SYRINGE
6 MIU / VIAL INJECTION
44 MCG / ML INJECTION CARTRIDGE
88 MCG / ML INJECTION CARTRIDGE
6 MIU / SYR INJECTION SYRINGE
22 MCG / SYR INJECTION SYRINGE
44 MCG / SYR INJECTION SYRINGE
8.8 MCG / SYR * 22 MCG / SYR INJECTION SYRINGE
9.6 MIU / VIAL INJECTION
00002245619
00002237770
00002318253
00002318261
00002269201
00002237319
00002237320
00002281708
0000216964900002337819
COPAXONE
AVONEX (30 MCG)
REBIF (1.5 ML CARTRIDGE)
REBIF (1.5 ML CARTRIDGE)
AVONEX PS/PEN (30 MCG/0.5 ML)
REBIF (0.5 ML SYRINGE)
REBIF (0.5 ML SYRINGE)
REBIF (INITIATION PACK)
BETASERON (0.3 MG)EXTAVIA (0.3 MG)
TMP
BIO
SRO
SRO
BIO
SRO
SRO
SRO
BHPNOV
46.4400
393.2961
258.9998
315.3041
409.5831
129.4999
157.6520
129.4999
99.3593 99.3593
EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$$
The following drug products may be considered for coverage under the Multiple Sclerosis (MS) Drug Coverage program for patients who have a diagnosis of relapsing-remitting multiple sclerosis, and who participate in Alberta government-sponsored drug programs.
The following drug products may be considered for coverage under the Multiple Sclerosis (MS) Drug Coverage program for patients who have a diagnosis of relapsing-remitting multiple sclerosis, and who participate in Alberta government-sponsored drug programs.
The following drug products may be considered for coverage under the Multiple Sclerosis (MS) Drug Coverage program for patients who have a diagnosis of relapsing-remitting multiple sclerosis, and who participate in Alberta government-sponsored drug programs.
The following drug products may be considered for coverage under the Multiple Sclerosis (MS) Drug Coverage program for patients who have a diagnosis of relapsing-remitting multiple sclerosis OR secondary progressive multiple sclerosis with relapses, and who participate in Alberta government-sponsored drug programs.
10Section 2 .
Drug Products Under Multiple Sclerosis (MS) Drug Coverage Program
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTMULTIPLE SCLEROSIS (MS) DRUG COVERAGE
PRODUCT IS NOT INTERCHANGEABLE
NATALIZUMAB
EFFECTIVE APRIL 1, 2012
"Natalizumab coverage may be provided for the treatment of relapsing remitting multiple sclerosis (RRMS) to reduce the frequency of clinical exacerbations, to decrease the number andvolume of active brain lesions identified on magnetic resonance imaging (MRI) scans and to delay the progression of physical disability, in adult patients (18 years of age or older) who have active RRMS that is causing CNS injury, who have previously been demonstrated to have at least nine T2 hyperintense lesions on brain MRI, and who are refractory or intolerant to both interferon beta (Avonex, Betaseron/Extavia or Rebif) and glatiramer acetate (Copaxone). Patients who develop neutralizing antibodies to interferon will be considered to have failed interferon.
Neutralizing Antibodies to interferon
If neutralizing antibodies are present, a report indicating clinically significant titres must be provided.
Refractory
When the above agents are taken at the recommended doses 'Refractory' is defined as:Within a 12-month period the patient has:
1) Been adherent to the disease modifying therapy (DMT) (i.e., greater than 80% of approved doses have been administered);
AND
2a) Experienced at least two relapses confirmed by the presence of neurologic deficits on examination.- The first qualifying relapse must have begun at least one month after treatment initiation- There must be at least one month between the onset of relapses- Neurologic deficits must have persisted for at least 3 months for one of the relapses. Alternatively, information on a second qualifying relapse with severe deficits (defined as unable to carry out usual activities of daily living), submitted within 3 months of the date of onset, will beconsidered.
OR
2b) Experienced one relapse confirmed by the presence of neurologic deficits on examination.- This relapse must have begun at least one month after treatment initiation.- Neurologic deficits must have persisted for at least 1 month
AND
Have evidence of active inflammatory MS disease activity on brain or spine MRI that:- started/occurred during treatment with DMT, and- was not associated with a clinical relapse
MRI evidence may be:- a definite gadolinium enhancing T1 lesion (not questionable faint enhancement) that was present on an MRI obtained at least 3 months after initiation of DMT and not within 3 months of a relapse;OR- The appearance of 2 or more new, or newly enlarging, T2 hyperintense lesions, greater than 3 mm in size.- To confirm that these new T2 lesions occurred on treatment, the baseline MRI must have beencompleted at least one month after starting DMT.- To confirm that the MRI lesions were not associated with the relapse, the relapse cannot have occurred between the 2 MRI scans.- To confirm that the T2 lesions occurred during the 12 month qualifying period, both MRI scans and the relapse must occur within a 12 month period.
11Section 2 .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTMULTIPLE SCLEROSIS (MS) DRUG COVERAGE
NATALIZUMAB
EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
Documentation supporting this criterion requires a radiologist's report that directly compares 2 brain MRI scans and that indicates the MRI scan dates, and that clearly states that 2 or more new, or newly enlarging, T2 lesions at least 3 mm in size are present on the second scan.
Intolerant
'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in the product monograph, or a persisting adverse event that is unresponsive to recommended management techniques and which is incompatible with further use of that class of DMT.
Contraindications
Coverage will not be approved if any of the following contraindications exist:- Any evidence of disease progression independent of relapses (i.e., has developed secondary progressive MS)- Immune compromised due to immunosuppressant or antineoplastic therapy or due to immunodeficiency (HIV, leukemia, lymphoma, etc.)- History of progressive multifocal leukoencephalopathy (PML)- Concurrent malignancy or significant illness likely to alter compliance or substantially reduce life expectancy- Planned or current pregnancy, or nursing
Coverage
For coverage, this drug must be prescribed by a Specialist in Neurology ("MS Neurologist") who has been identified by the Alberta MS Drug Review Panel.
Initial Coverage
- Within the 2 years prior to the Tysabri application, the patient must meet the same relapse criteria that are required for other MS therapies considered for MS Drug Coverage (2 relapses during the last 2 years, one of which may be an MRI enhancing lesion). In most cases this will be satisfied by the treatment failure demonstrated but, if a patient failed interferon and glatirameracetate more than one year earlier, ongoing active disease must be confirmed. Exceptions may be made for patients switching due to recent development of intolerance or neutralizing antibodies.- Coverage will not be approved when any DMT or other immunosuppressive therapy is to be used in combination with Tysabri (except corticosteroids which can be used for up to 12 weeks during Tysabri initiation in patients with coexisting Crohn's Disease or similar situations).- Patients who have failed Tysabri will not be eligible for a subsequent trial of Tysabri (except in exceptional circumstances).
Following this assessment, coverage may be approved for 13 doses of 300 mg (i.e., one dose administered every 4 weeks for a period of 12 months). Patients will be limited to receiving 1 dose (4 weeks supply) of Tysabri per prescription at their pharmacy.
Continued Coverage
For continued coverage beyond 13 doses, the patient must meet the following criteria:
1) At the first renewal there must be evidence that neutralizing antibodies to Tysabri are absent. This requires an initial test between 6 to 8 months of treatment. If neutralizing antibodies are absent, no further testing is required. If neutralizing antibodies are present, testing must be repeated prior to the renewal request.
2) The patient must be assessed by an MS Neurologist and have an MRI with gadolinium at least every 12 months;
12Section 2 .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTMULTIPLE SCLEROSIS (MS) DRUG COVERAGE
PRODUCT IS NOT INTERCHANGEABLE
NATALIZUMAB
20 MG / ML INJECTION00002286386 TYSABRI BIO 178.7463
EFFECTIVE APRIL 1, 2012
$
AND
3) On assessment, the MS Neurologist must confirm in writing that the patient is a 'responder' that meets all of the following criteria:- There has been no more than one inflammatory event in the last year (defined as either a clinical relapse or gadolinium enhancing lesion). The rare exception is a patient who has had four or more relapses in the year prior to starting treatment; in this case there must be at least a 50% reduction in relapse rate over the entire Tysabri treatment period.- The patient has not missed any doses, or delayed any doses by more than 1 week with the exception of medically authorized delays (rationale for such delays must be justified in a narrative; only serious medical conditions are acceptable).- None of the contraindications identified above exist.
Following this assessment, continued coverage may be approved for maintenance therapy of 300 mg every 4 weeks for a period of 12 months. Patients will be limited to receiving 1 dose of Tysabri per prescription at their pharmacy."
13Section 2 .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

Section 3 Criteria for Special A
uthorization of Select Drug Products
SECTION 3
Criteria for Special Authorization
of Select Drug Products

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 3 • 1 EFFECTIVE APRIL 1, 2012
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
The drug products listed in this section may be considered for coverage by special authorization for patients covered under Alberta Health and Wellness-sponsored drug programs. (For Alberta Human Services and Alberta Seniors (AISH) clients, the special authorization criteria for coverage can be found in the Criteria for Special Authorization of Select Drug Products section of the Alberta Human Services Drug Benefit Supplement.)
68BSpecial Authorization Policy
99BDRUG PRODUCTS ELIGIBLE FOR CONSIDERATION BY SPECIAL AUTHORIZATION Drug products may be considered for coverage by special authorization under one or more of the following circumstances, unless a specific product falls under the criteria for drug products Unot U eligible for consideration by special authorization. Please see the end of this section for information regarding drug products not eligible for consideration by special authorization. 1. The drug is covered by Alberta Health and Wellness under specified criteria (listed in the following
sections). Drug Products and indications other than those specified are not eligible for consideration by special authorization.
2. The drug is normally covered by another government program or agency for a specific approved clinical condition, but is needed for the treatment of a clinical condition that is not covered by that government program or agency.
3. The drug is required because other drug products listed in the Alberta Health and Wellness Drug Benefit List are contraindicated or inappropriate because of the clinical condition of the patient.
4. The particular brand of drug is considered essential in the care of a patient, where the LCA price policy would otherwise apply. Coverage of a specific brand may be considered where a patient has experienced significant allergic reactions or documented untoward therapeutic effects with alternate brands in an interchangeable grouping. Coverage of a brand name product will UnotU be considered in situations where the interchangeable grouping includes a pseudo-generic to the brand name drug.
5. A particular drug product or dosage form of a drug is essential in the care of a patient where the MAC price policy would otherwise apply. Exceptions may occur at the product level. Coverage may be considered only where a patient has experienced significant allergic reactions or documented untoward therapeutic effects with the drug product which establishes the MAC pricing.
Prior approval must be granted by Alberta Blue Cross to ensure coverage by special authorization. For those special authorization requests that are approved, the effective date for authorization is the beginning of the month in which the physician’s request is received by Alberta Blue Cross.
Special authorization is granted for a defined period as indicated in each applicable special authorization drug product criteria (the “Approval Period”). If continued treatment is necessary beyond the Approval Period, it is the responsibility of the patient and physician to re-apply for coverage UpriorU to the expiration date of the Approved Period, UunlessU the Auto-Renewal Process or Step Therapy Approval Process apply (see below).

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. EFFECTIVE APRIL 1, 2012 Section 3 • 2
100BAUTO-RENEWAL PROCESS Selected drug products are eligible for the following auto-renewal process (for eligibility, see the Special Authorization criteria for each drug product).
1. For initial approval, a special authorization request must be submitted. If approval is granted, it will be effective for the Approval Period outlined in the drug product’s Special Authorization criteria
2. As long as the patient has submitted a claim for the drug product within the preceding Approval Period (example: within the preceding 6 months), approval will be automatically renewed for a further Approval Period (example: a further 6 months). There is no need for the prescriber to submit a new request as the automated real-time claims adjudication system will read the patient’s claims history to determine if a claim has been made within the preceding Approval Period.
3. If the patient does UnotU make a claim for the drug product during the Approval Period, the approval will lapse and a new special authorization request must be submitted.
101BSTEP THERAPY APPROVAL PROCESS
102BSelect drug products are eligible for coverage via the step therapy process, outlined below.
1. 103BIf the patient has made a claim for the First-Line* drug product(s) within the preceding 12 months, the claim for the step therapy drug will be approved.
2. 104BThe automated real-time claims adjudication system will read the patient’s claims history to determine if the required First-Line* drug product(s) have been claimed within the preceding 12 months.
3. 105BSubsequent claims for drug product(s) permitted by step therapy will continue to be approved as long as the drug product has been claimed within the preceding 12 months.
4. 106BThe regular special authorization approval process will continue to be available for step therapy approvals for those patients whose First-Line* drug claims cannot be adjudicated through the automated real-time claims adjudication system.
* A First-Line drug product includes any drug(s) or drug product(s) that, under the drug product’s Special Authorization criteria, are required to be utilized before reimbursement for the drug product is permitted.
107BDRUG PRODUCTS NOT ELIGIBLE FOR CONSIDERATION BY SPECIAL AUTHORIZATION
The following categories of drug products are not eligible for special authorization: 1. Drug products deleted from the List. 2. Drug products not yet reviewed by the Alberta Health and Wellness Expert Committee on Drug
Evaluation and Therapeutics. This applies to: * products where a complete submission has been received from the manufacturer and the product is
under review, * products where an incomplete submission has been received from the manufacturer, and * products where the manufacturer has not made a submission for review.
Drug products not yet reviewed may encompass new pharmaceutical products, new strengths of products already listed, reformulated products and new interchangeable (generic) products.
3. Drug products that have completed the review process and are not included on the List. 4. Most drugs available through Health Canada’s Special Access Program. 5. Drug products when prescribed for cosmetic indications. 6. Nonprescription or over-the-counter drug products are generally not eligible.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. Section 3 • 3 EFFECTIVE APRIL 1, 2012
69BCriteria for Coverage
Wording that appears within quotation marks (“ ”) in this section is the official special authorization criteria, as recommended by the Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics, and approved by the Minister of Health and Wellness. Wording that is not enclosed in quotation marks outlines specific information required to interpret criteria, guidelines for submitting requests and/or information regarding conditions under which coverage cannot be provided.
Products Available Through Health Canada’s Special Access Program
PEMOLINE “For the treatment of attention deficit hyperactivity disorder where approval has been provided by Health Canada’s Special Access Program.”
37.5 MG ORAL TABLET DIN N/A* CYLERT ABB
75 MG ORAL TABLET DIN N/A* CYLERT ABB
*As Cylert has been withdrawn from market, the DINs are no longer valid. Where authorizations for Cylert have been granted, coverage for this product will be provided under PIN 00000999917.
Other Products
The remaining drug products in this section are listed alphabetically according to the generic ingredient name of the drug. These products can be found on the following pages.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ABATACEPT
4 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Rheumatoid Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate or other DMARDS, for the reduction in signs and symptoms of severely active Rheumatoid Arthritis(RA) in adult patients (18 years of age or older) who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4 month trial). [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily).
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for five doses of up to 1000 mg/dose administered at 0, 2, 4, 8 and 12 weeks.-Patients will be limited to receiving one dose of abatacept per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond five doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after the initial five doses to determine response between 12 and 16 weeks of receiving the initial dose.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for one dose of up to 1000 mgevery 4 weeks for a period of 12 months. Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- confirmation of maintenance of ACR20, OR- maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ABATACEPT
5 EFFECTIVE APRIL 1, 2012 Section 3 .
All requests (including renewal requests) for abatacept for Rheumatoid Arthritis must be completed using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
Juvenile Idiopathic Arthritis:
"Special authorization coverage may be provided for the reduction in signs and symptoms of moderately to severely active polyarticular juvenile idiopathic arthritis (JIA) in patients 6 years of age and older who:- Have 5 or more active joints (defined by either swelling or limitation of motion plus pain and/or tenderness), AND- Are refractory to one or more disease modifying anti-rheumatic agents (DMARDS) conventionally used in children (minimum three month trial), AND- Are refractory to or intolerant to etanercept (minimum 12 week trial).
'Refractory' is defined as lack of effect at the recommended doses and duration of treatments aslisted above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in the product monographs.
For coverage, this drug must be prescribed by a prescriber affiliated with a Pediatric Rheumatology Clinic in Edmonton or Calgary ("Pediatric Rheumatology Specialist").
- Coverage may be approved for one dose of 10 mg/kg (maximum dose 1000 mg) at 0, 2, 4, 8, 12 and 16 weeks (total of six doses).- Patients will be limited to receiving one dose of abatacept per prescription at their pharmacy.
For potential coverage for retreatment with abatacept following a subsequent disease flare, the patient must meet the following criteria:1) The patient must be assessed by a Pediatric Rheumatology Specialist after the initial 16 weeks, but no longer than 20 weeks after, treatment with this biologic agent to determine and document initial treatment response.2) The Pediatric Rheumatology Specialist must confirm in writing that the patient is a responder that meets the following criteria (JRA30):- 30% improvement from baseline in at least three of the following six response variables, with worsening of 30% or more in no more than one of the six variables. The variables include: i. global assessment of the severity of the disease by the Pediatric Rheumatology Specialist, ii. global assessment of overall well-being by the patient or parent, iii. number of active joints (joints with swelling not due to deformity or joints with limitation of motion with pain tenderness or both), iv. number of joints with limitation of motion, v. functional ability based on CHAQ scores, vi. ESR or CRP3) Data from all of the six variables comprising the JRA30 and the CHAQ scores must be reported.
Following assessment and confirmation of initial treatment response, coverage for retreatment with abatacept may be approved for one dose of 10 mg/kg (maximum dose 1000 mg) at 0, 2*, 4,8, 12 and 16 weeks (total of up to six doses; *the week 2 dose on retreatment is optional, to be administered at the discretion of the Pediatric Rheumatology Specialist). In order to be considered for coverage for retreatment, the patient must meet the following criteria:1) The patient has been assessed by a Pediatric Rheumatology Specialist and the presence of disease flare confirmed. Disease flare is defined as worsening of at least 30% or greater in at least 3 of 6 JRA30 variables for JIA and 30% or greater improvement in no more than one variable.2) The Pediatric Rheumatology Specialist must confirm in writing that the patient has had an initial treatment response (as assessed above) and that the patient has experienced a disease flare (as defined above)."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ABATACEPT
250 MG / VIAL (BASE) INJECTION00002282097 ORENCIA BMS 495.4779
6 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
Section 3 .
Please note: Coverage is provided for treatment of disease flares only. However, if a patient experiences a subsequent flare within 12 months of initiation of treatment with abatacept, they may be eligible for continuous coverage (i.e., one dose of 10 mg/kg (maximum dose 1000 mg) every 4 weeks) for a maximum period of two years, provided the patient has demonstrated a response to initial treatment."
All requests (including renewal requests) for abatacept for Juvenile Idiopathic Arthritis must be completed using the Abatacept for Juvenile Idiopathic Arthritis Special Authorization Request Form (ABC 31291).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ADALIMUMAB
7 EFFECTIVE APRIL 1, 2012 Section 3 .
Rheumatoid Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4 month trial) [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily)
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology who agrees to and continues to actively and consistently participate in the Alberta Post-Marketing Study ("Study") as required by Alberta Health and Wellness or its agent, throughout the special authorization approval period ("RA Specialist"). The patient must also provide all consents and authorizations required to permit the RA Specialist to actively and consistently participate in the Study. Special authorization approval for the patient may be revoked if the RA Specialist does not continually, actively and consistently participate in the Study.
- Initial coverage may be approved for five doses as follows: An initial 40 mg dose, followed by additional 40 mg doses at 2, 4, 6 and 8 weeks after the first dose.- Patients will be limited to receiving a one-month supply of adalimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond five doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after the initial five doses to determine response. 2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for 40 mg every other week for a period of 12 months. Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ADALIMUMAB
8 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- confirmation of maintenance of ACR20, or - maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for adalimumab for Rheumatoid Arthritis must be completed using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
Psoriatic Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for reducing signs and symptoms and inhibiting the progression of structural damage of active arthritis in adult patients (18 years of age or older) with moderate to severe polyarticular psoriaticarthritis (PsA) or pauciarticular PsA with involvement of knee or hip joint who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- An adequate trial of another disease modifying anti-rheumatic agent(s) (minimum 4 month trial).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 40 mg administered every other week for 8 weeks.- Patients will be limited to receiving a one-month supply of adalimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond 8 weeks, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after 8 weeks, but no longer than 12 weeks after, to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ADALIMUMAB
9 EFFECTIVE APRIL 1, 2012 Section 3 .
- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for doses of 40 mg every other week, for a period of 12 months. Ongoing coverage may be considered if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or- Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests. It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for adalimumab for Psoriatic Arthritis must be completed using the Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis SpecialAuthorization Request Form (ABC 30964).
Ankylosing Spondylitis:
"Special authorization coverage may be provided for the reduction in the signs and symptoms ofseverely active Ankylosing Spondylitis, as defined by the Modified New York criteria for Ankylosing Spondylitis, in adult patients (18 years of age or older) who have active disease as demonstrated by:
- a BASDAI greater than or equal to 4 units, demonstrated on 2 occasions at least 8 weeks apartAND- a Spinal Pain VAS of greater than or equal to 4 cm (on a 0-10 cm scale), demonstrated on 2 occasions at least 8 weeks apart AND- who are refractory or intolerant to treatment with 2 or more NSAIDS each taken for a minimum of 4 weeks at maximum tolerated or recommended doses.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 12 weeks as follows: An initial 40 mg dose, followed by additional 40 mg doses administered every two weeks for up to 12 weeks after the first dose.- Patients will be limited to receiving a one-month supply of adalimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ADALIMUMAB
10 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
For continued coverage beyond 12 weeks, the patient must meet the following criteria:1) The patient must be assessed at 12 weeks by an RA Specialist after the initial 12 weeks of therapy to determine response.2) The RA Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Reduction of the BASDAI score by at least 50% of the pre-treatment value or by 2 or more units, AND - Reduction of the Spinal Pain VAS by 2 cm or more.
Following this assessment, continued coverage may be approved for one 40 mg dose every other week for a period of 12 months. Ongoing coverage may be considered if the patient is re-assessed by an RA Specialist every 12 months and is confirmed to be continuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for adalimumab for Ankylosing Spondylitis must be completed using the Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form (ABC 31195).
Moderately to Severely Active Crohn's Disease:
"Special authorization coverage may be approved for coverage of adalimumab for the reduction in signs and symptoms and induction and maintenance of clinical remission of Moderately to Severely Active Crohn's Disease in patients who meet the following criteria:
- Adalimumab must be prescribed by a Specialist in Gastroenterology or a physician appropriately trained by the University of Alberta or the University of Calgary and recognized as a prescriber by Alberta Blue Cross for adalimumab for coverage for the treatment of Moderately to Severely Active Crohn's Disease patients ('Specialist').- Patients must be 18 years of age or older to be considered for coverage of adalimumab.- Patients will be limited to receiving a one-month supply of adalimumab per prescription at their pharmacy.- Patients may be allowed to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy (both primary loss of response and secondary loss of response) or due to serious adverse effects or contraindications. An adequatetrial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
Prior to initiation of adalimumab therapy for New Patients:
'New Patients' are patients who have never been treated with adalimumab by any health care provider.
Moderately to Severely Active Crohn's Disease:
Prior to initiation of adalimumab therapy, New Patients must have a current Modified (without the physical exam) Harvey Bradshaw Index score of greater than or equal to 7 (New Patient's Baseline Score), AND be Refractory.
Refractory is defined as one or more of the following:1) Serious adverse effects or reactions to the treatments specified below; OR 2) Contraindications (as defined in product monographs) to the treatments specified below; OR3) Previous documented lack of effect at doses and for duration of all treatments specified below: a) mesalamine: minimum of 3 grams/day for a minimum of 6 weeks; AND refractory to, or dependent on, glucocorticoids: following at least one tapering dosing schedule of 40 mg/day,
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ADALIMUMAB
11 EFFECTIVE APRIL 1, 2012 Section 3 .
tapering by 5 mg each week to 20 mg, then tapering by 2.5 mg each week to zero, or similar.
[Note: Patients who have used the above treatments in combination will not be required to be challenged with individual treatments as monotherapy]
ANDb) Immunosuppressive therapy as follows: - Azathioprine: minimum of 2 mg/kg/day for a minimum of 3 months; OR - 6-mercaptopurine: minimum of 1 mg/kg/day for a minimum of 3 months; OR- Methotrexate: minimum or 15 mg/week for a minimum of 3 months.OR - Immunosuppressive therapy discontinued at less than 3 months due to serious adverse effectsor reactions.
Applications for coverage must include information regarding the dosages and duration of trial ofeach treatment the patient received, a description of any adverse effects, reactions, contraindications and/or lack of effect, as well as any other information requested by Alberta Blue Cross.
Coverage Criteria for Moderately to Severely Active Crohn's Disease
- New Patients must meet the criteria above prior to being considered for approval. - All approvals are also subject to the following applicable criteria.
Induction Dosing for New Patients:
- Coverage for Induction Dosing may only be approved for New Patients (those who have never been treated with adalimumab by any health care provider).- 'Induction Dosing' means a maximum of one 160 mg dose of adalimumab per New Patient at week 0 followed by an 80 mg dose at week 2.- New Patients are eligible to receive Induction Dosing only once, after which time the Maintenance Dosing for New Patients and Continued Coverage for Maintenance Dosing criteria will apply.- As an interim measure, 40 mg doses of adalimumab will be provided at weeks 4, 6, 8 and 10 toallow time to determine whether the New Patient meets coverage criteria for Maintenance Dosing below.
Maintenance Dosing:
'Maintenance Dosing' means one 40 mg dose of adalimumab per patient provided no more often than every other week starting at week 4 for a period of 12 months to:- New Patients following the completion of Induction Dosing; OR - Existing Patients, who are patients that are being treated, or have previously been treated, withadalimumab.
Maintenance Dosing for New Patients after Completion of Induction Dosing:
- The New Patient must be assessed by a Specialist within 12 weeks after the initiation of Induction Dosing to determine response by obtaining a Modified Harvey Bradshaw Index score for patients with Moderately to Severely Active Crohn's Disease; AND- The Specialist must confirm the Modified Harvey Bradshaw Index score shows a decrease from the New Patient's Baseline Score of greater than or equal to 3 points for patients with Moderately to Severely Active Crohn's.
Maintenance Dosing for Existing Patients:
- The patient must be assessed by a Specialist annually (within 2 months of the expiry of a patient's special authorization) at least 2 weeks after the day a dose of adalimumab was administered to the patient and prior to administration of the next dose to obtain: a Modified
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ADALIMUMAB
12 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Harvey Bradshaw Index Score (Existing Patient's Baseline Score) for Moderately to Severely Active Crohn's Disease; AND - these measures must be provided to Alberta Blue Cross for assessment for continued coverage for maintenance dosing.
Continued Coverage for Maintenance Dosing:
Continued coverage may be considered for one 40 mg dose of adalimumab per patient providedno more often than every other week for a period of 12 months, if the following criteria are met atthe end of each 12 month period:
- The New Patient or the Existing Patient must be assessed by a Specialist annually (within 2 months of the expiry of a patient's special authorization) at least 2 weeks after the day a dose of adalimumab was administered to the patient and prior to administration of the next dose to obtain: a Modified Harvey Bradshaw Index Score for Moderately to Severely Active Crohn's Disease; AND- For New Patients: The Specialist must confirm that the patient has maintained a greater than or equal to 3 point decrease from the New Patient's Baseline Score for Moderately to Severely Active Crohn's; OR- For Existing Patients: The Specialist must confirm that the patient has maintained the Existing Patient's Baseline Score."
All requests (including renewal requests) for adalimumab for Moderately to Severely Active Crohn's Disease must be completed using the Adalimumab for Crohn's/Infliximab for Crohn's/Fistulizing Crohn's Special Authorization Request Form (ABC 31200).
Plaque Psoriasis:
"Special authorization coverage may be provided for the reduction in signs and symptoms of severe, debilitating psoriasis in patients who:- Have a total PASI of 10 or more and a DLQI of more than 10, OR- Who have significant involvement of the face, palms of the hands, soles of the feet or genital region; AND- Who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory, OR- Cyclosporine (6 weeks treatment); AND- Phototherapy (unless restricted by geographic location)
Patients who have a contraindication to either cyclosporine or methotrexate will be required to complete an adequate trial of the other pre-requisite medication prior to potential coverage beingconsidered.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be prescribed by a Specialist in Dermatology ("Dermatology Specialist").
- Initial coverage may be approved for an initial dose of 80 mg, followed by one 40 mg dose every other week beginning one week after the first dose, for a total of nine doses.- Patients will be limited to receiving a one-month supply of adalimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ADALIMUMAB
40 MG / SYR INJECTION SYRINGE00002258595 HUMIRA ABB 784.1265
13 EFFECTIVE APRIL 1, 2012
$
Section 3 .
trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond nine doses, the patient must meet all of the following criteria:1) The patient must be assessed by a Dermatology Specialist after the initial nine doses to determine response.2) The Dermatology Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Greater than or equal to 75% reduction in PASI score, OR- Greater than or equal to 50% reduction in PASI score AND improvement of greater than or equal to 5 points in the DLQI.
Following this assessment, continued coverage may be considered for one 40 mg dose of adalimumab every other week for a period of 12 months. Ongoing coverage may be considered if the patient is re-assessed by a Dermatology Specialist every 12 months and is confirmed to becontinuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for adalimumab for Plaque Psoriasis must be completed using the Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form (ABC 31192).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ALENDRONATE SODIUM
10 MG ORAL TABLET
40 MG ORAL TABLET
70 MG ORAL TABLET
00002248728000022701290000224737300002288087
0000225810200002201038
00002352966000022997120000224873000002258110000022863350000226171500002284006000022752790000228810900002245329
APO-ALENDRONATEMYLAN-ALENDRONATENOVO-ALENDRONATESANDOZ ALENDRONATE
CO ALENDRONATEFOSAMAX
ALENDRONATEALENDRONATE-FCAPO-ALENDRONATECO ALENDRONATEMYLAN-ALENDRONATENOVO-ALENDRONATEPMS-ALENDRONATE-FCRATIO-ALENDRONATESANDOZ ALENDRONATEFOSAMAX
APXMYPTEVSDZ
COBMFC
SNSMELAPXCOBMYPTEVPMSRPHSDZMFC
1.1057 1.1057 1.1057 1.1057
2.6097 4.0743
5.5750 5.5750 5.5750 5.5750 5.5750 5.5750 5.5750 5.5750 5.5750
10.2385
14 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$
$$$$$$$$$$
Section 3 .
"For the treatment of osteoporosis in patients who have documented hip, vertebral or otherfractures. Special authorization may be granted for 6 months."
"For the treatment of osteoporosis in patients with documented evidence of intolerance or lack ofresponse to etidronate (i.e. demonstrated as a > 2% loss in bone mineral density in one year).Special authorization for this criteria may be granted for 6 months."
"Coverage cannot be provided for two or more osteoporosis medications (alendronate,calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intendedfor use as combination therapy."
"Requests for other osteoporosis medications covered via special authorization will not be considered until 6 months after the last dose of denosumab."
"For the treatment of Paget's disease. Special Authorization for this criteria may be granted to a maximum of 6 months."
All requests for alendronate sodium for Osteoporosis must be completed using the Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon for Osteoporosis Special Authorization Request Form (ABC 31086).
The following product(s) are eligible for auto-renewal for the treatment of osteoporosis.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ALENDRONATE SODIUM/ VITAMIN D3
ALFUZOSIN HCL
AMPICILLIN
70 MG * 5,600 UNIT ORAL TABLET
10 MG ORAL SUSTAINED-RELEASE TABLET
250 MG ORAL CAPSULE
500 MG ORAL CAPSULE
00002314940
00002315866000023142820000230467800002245565
00000020877
00000020885
FOSAVANCE
APO-ALFUZOSINNOVO-ALFUZOSIN PRSANDOZ ALFUZOSINXATRAL
NOVO-AMPICILLIN
NOVO-AMPICILLIN
MFC
APXTEVSDZSAV
TEV
TEV
4.5533
0.5980 0.5980 0.5980 1.1020
0.3331
0.6459
15 EFFECTIVE APRIL 1, 2012
$
$$$$
$
$
Section 3 .
"For the treatment of osteoporosis in patients who have documented hip, vertebral or otherfractures."
"For the treatment of osteoporosis in patients with documented evidence of intolerance or lack ofresponse to etidronate (i.e. demonstrated as a > 2% loss in bone mineral density in one year)."
"Coverage cannot be provided for two or more osteoporosis medications (alendronate,calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intendedfor use as combination therapy.""Requests for other osteoporosis medications covered via special authorization will not be considered until 6 months after the last dose of denosumab."
"Special authorization for these criteria may be granted for 6 months."
All requests for alendronate sodium/vitamin D3 must be completed using the Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon for Osteoporosis Special Authorization Request Form (ABC 31086).
The following product(s) are eligible for auto-renewal.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): DOXAZOSIN OR TERAZOSIN
"For the treatment of the symptoms of benign prostatic hyperplasia (BPH) in patients who are unresponsive to a six-week trial with a non-selective alpha-blocker (e.g., terazosin ) or in whom non-selective alpha-blockers are not tolerated or are contraindicated."
"Special authorization may be granted for 24 months"
"For the treatment of infections caused by susceptible Shigella and Salmonella."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ANAKINRA
16 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) in whom other biologics are contraindicated or in patients whohave experienced serious adverse events while on other biologics and who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4-month trial). [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND - Leflunomide (minimum 10 week trial at 20 mg daily).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology who agrees to and continues to actively and consistently participate in the Alberta Post-Marketing Study ("Study") as required by Alberta Health and Wellness or its agent, throughout the special authorization approval period ("RA Specialist"). The patient must also provide all consents and authorizations required to permit the RA Specialist to actively and consistently participate in the Study. Special authorization approval for the patient may be revoked if the RA Specialist does not continually, actively and consistently participate in the Study.
- Initial coverage may be approved for one 100 mg dose administered daily for 8 weeks.- Patients will be limited to receiving a one-month supply of anakinra per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond 8 weeks, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after 8 weeks but no longer than 12 weeksafter treatment to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for one 100 mg dose administered once daily for a period of 12 months. Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ANAKINRA
AZITHROMYCIN
AZTREONAM
100 MG / SYR INJECTION SYRINGE
600 MG ORAL TABLET
75 MG / VIAL INHALATION POWDER FOR SOLUTION
00002245913
00002330911000022560880000226164200002231143
00002329840
KINERET
AZITHROMYCINCO AZITHROMYCINPMS-AZITHROMYCINZITHROMAX
CAYSTON
BVM
SNSCOBPMSPFI
GIL
51.4936
7.1161 7.1161 7.1161
12.9745
51.7681
17 EFFECTIVE APRIL 1, 2012
$
$$$$
$
Section 3 .
2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or- Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for anakinra must be completed using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/ Tocilizumab for RheumatoidArthritis Special Authorization Request Form (ABC 30902).
"For the prevention of disseminated Mycobacterium avium complex disease in patients with advanced HIV infection or other immunocompromised conditions.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): TOBRAMYCIN INHALATION SOLUTION
"For the treatment of chronic pulmonary Pseudomonas aeruginosa infections when used as cyclic treatment (28-day cycles) in patients 6 years of age and older with moderate to severe cystic fibrosis (CF) and deteriorating clinical condition despite treatment with inhaled tobramycin."
"Coverage will not be considered when inhaled tobramycin and inhaled aztreonam are intended for use in combination."
"Special authorization may be granted for 6 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
BENZOYL PEROXIDE
BUDESONIDE
BUSERELIN ACETATE
CABERGOLINE
10 % TOPICAL (ALCOHOL) GEL
20 % TOPICAL (ALCOHOL) GEL
3 MG ORAL CONTROLLED-RELEASE CAPSULE
1 MG / ML (BASE) NASAL SOLUTION
1 MG / ML (BASE) INJECTION
6.3 MG (BASE) INJECTION IMPLANT
0.5 MG ORAL TABLET
00000263699
00000373036
00002229293
00002225158
00002225166
00002228955
0000230140700002242471
PANOXYL 10
PANOXYL 20
ENTOCORT
SUPREFACT INTRANASAL
SUPREFACT
SUPREFACT DEPOT
CO CABERGOLINEDOSTINEX
GSK
GSK
AZC
SAV
SAV
SAV
COBPAL
0.1572
0.2048
1.7050
8.4065
11.9794
813.5707
8.8550 13.6901
18 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$$
Section 3 .
"For the treatment of severe acne as defined by scarring acne.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"For the treatment of inflammatory bowel disease (e.g. Crohn's, ulcerative colitis, ulcerative ileitis, etc.). This drug product must be prescribed by a specialist in Gastroenterology, Internal Medicine or Pediatrics (or by a specialist in General Surgery on a case-by-case basis, in geographic areas where access to these specialties is not available).
Special authorization may be granted for 12 months."
The following product(s) are eligible for auto-renewal.
"When prescribed for non-cancer, non-cosmetic or non-fertility indications.
Special authorization may be granted for 6 months."
Information is required regarding the patient's diagnosis/indication for use of this medication.
The following product(s) are eligible for auto-renewal.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): BROMOCRIPTINE
"For the treatment of hyperprolactinemia in patients who are intolerant to or who have failed bromocriptine. Special authorization may be granted for 24 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CASPOFUNGIN
CEFADROXIL
CELECOXIB
CLINDAMYCIN PHOSPHATE/ BENZOYL PEROXIDE
50 MG / VIAL INJECTION
70 MG / VIAL INJECTION
500 MG ORAL CAPSULE
100 MG ORAL CAPSULE
200 MG ORAL CAPSULE
1 % (BASE) * 5 % TOPICAL GEL
00002244265
00002244266
0000224077400002235134
00002239941
00002239942
0000224847200002243158
CANCIDAS
CANCIDAS
APO-CEFADROXILNOVO-CEFADROXIL
CELEBREX
CELEBREX
BENZACLINCLINDOXYL
MFC
MFC
APXTEV
PFI
PFI
SAVGSK
222.0000
222.0000
0.8421 0.8421
0.7340
1.4683
0.9587 0.9744
19 EFFECTIVE APRIL 1, 2012
$
$
$$
$
$
$$
Section 3 .
"For esophageal candidiasis in patients who are intolerant to fluconazole and itraconazole, or who have failed both agents as evidenced by significant clinical deterioration due to the fungal infection during a course of therapy or no resolution after a full course of therapy."
"For the treatment of skin and skin structure infections."
"1) For patients who are at high risk of upper gastrointestinal (GI) complications due to a proven history of prior complicated GI events (e.g. GI perforation, obstruction or major bleeding) or
2) For patients who have a documented history of ulcers proven radiographically and/or endoscopically.
Special authorization for both criteria may be granted for 6 months."
All requests for celecoxib must be completed using the Celecoxib Special Authorization RequestForm (ABC 31140).
The following product(s) are eligible for auto-renewal.
"For the treatment of severe acne as defined by scarring acne.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CLOPIDOGREL BISULFATE
75 MG (BASE) ORAL TABLET00002252767000023030270000235153600002348004000023593160000229316100002238682
APO-CLOPIDOGRELCO CLOPIDOGRELMYLAN-CLOPIDOGRELPMS-CLOPIDOGRELSANDOZ CLOPIDOGRELTEVA-CLOPIDOGRELPLAVIX
APXCOBMYPPMSSDZTEVSAV
1.1804 1.1804 1.1804 1.1804 1.1804 1.1804 2.6512
20 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$
Section 3 .
(Refer to 20:12.18 of the Alberta Health and Wellness Drug Benefit List for one month of coverage, following the first intravascular stent placement, when prescribed by a Specialist in Cardiology, Cardiac Surgery, Cardiovascular & Thoracic Surgery, or General Surgery.)
"For the prevention of thrombosis, for one month, when prescribed following intravascular bare metal stent placement. Patients who have received one month of coverage via the Limited Restricted Benefit will not be eligible for additional coverage under this criterion." **
"For the prevention of thrombosis, for up to 12 months, when prescribed following intravascular drug eluting stent (DES) placement. Patients who have received one month of coverage via the Limited Restricted Benefit may be eligible for an additional 11 months of coverage (i.e., up to 12 months of coverage) following the submission of a special authorization request." **
"For the prevention of cerebrovascular (e.g. stroke, TIA) and non-cerebrovascular ischemic events in patients who have a contraindication to ASA. Special authorization for this criterion may be granted for 24 months."
"For use in patients who have experienced a non-cerebrovascular ischemic event while on ASA.Special authorization for this criterion may be granted for 24 months."
"For use in patients who have experienced a cerebrovascular ischemic event (e.g. stroke, TIA) while on dipyridamole/ASA (Aggrenox) or for whom dipyridamole/ASA (Aggrenox) is contraindicated. Special authorization for this criterion may be granted for 24 months."
"Coverage will not be considered when clopidogrel and dipyridamole/ASA are intended for use in combination."
** Special Authorization for post-stent coverage is required when the prescriber prescribing the medication is not a designated prescriber, for treatment after repeat stents, or for continued coverage of up to 12 months following intravascular drug eluting stent (DES) placement.
In order to comply with the first and second criteria, information is required regarding the date, type of stent, and stenting procedure. In order to comply with the third criterion, information is required as to why ASA cannot be used. In order to comply with the fourth criterion, information is required regarding the type of ischemic event experienced while on ASA. In order to comply with the fifth criterion, information is required regarding the type of ischemic event experienced while on dipyridamole/ASA (Aggrenox) and/or why dipyridamole/ASA (Aggrenox) cannot be used.
All requests for clopidogrel bisulfate must be completed using the Clopidogrel Special Authorization Request Form (ABC 30786).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CYCLOSPORINE
CYPROTERONE ACETATE
DANAPAROID SODIUM
10 MG ORAL CAPSULE
25 MG ORAL CAPSULE
50 MG ORAL CAPSULE
100 MG ORAL CAPSULE
100 MG / ML ORAL SOLUTION
50 MG ORAL TABLET
100 MG / ML INJECTION
1,250 UNIT / ML INJECTION
00002237671
0000224707300002150689
0000224707400002150662
0000224282100002150670
0000224432400002150697
0000224589800000704431
00000704423
00002129043
NEORAL
SANDOZ CYCLOSPORINENEORAL
SANDOZ CYCLOSPORINENEORAL
SANDOZ CYCLOSPORINENEORAL
APO-CYCLOSPORINENEORAL
CYPROTERONEANDROCUR
ANDROCUR DEPOT
ORGARAN
NOV
SDZNOV
SDZNOV
SDZNOV
APXNOV
AAPPMS
PMS
MFC
0.6706
1.3050 1.5588
2.5450 3.0390
5.0900 6.0802
3.7708 5.4047
1.4085 1.4339
26.8130
33.7083
21 EFFECTIVE APRIL 1, 2012
$
$$
$$
$$
$$
$$
$
$
Section 3 .
"For the treatment of severe psoriasis in those patients where other standard therapy has failed. This drug product must be prescribed by a specialist in Dermatology."
"For the treatment of severe rheumatoid arthritis in patients who are unable to tolerate or have failed an adequate trial of methotrexate. This drug product must be prescribed by a specialist in Rheumatology (or by a Specialist in Internal Medicine with an interest in Rheumatology on a case-by-case basis, in geographic areas where access to this specialty is not available)."
"For the treatment of steroid dependent and steroid resistant nephrotic syndrome. Consideration will be given where cyclosporine is used for the induction and maintenance of remissions or for the maintenance of steroid induced remissions. This drug product must be prescribed by a specialist in Pediatrics or Nephrology."
"Special authorization for all criteria may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"When prescribed for non-cancer, non-cosmetic indications.
Special authorization may be granted for 6 months."
Information is required regarding the patient's diagnosis/indication for use of this medication.
The following product(s) are eligible for auto-renewal.
"For the treatment of patients with heparin-induced thrombocytopenia."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DARBEPOETIN
DARIFENACIN HYDROBROMIDE
10 MCG / SYR INJECTION SYRINGE
20 MCG / SYR INJECTION SYRINGE
100 MCG / ML INJECTION SYRINGE
200 MCG / ML INJECTION SYRINGE
500 MCG / ML INJECTION SYRINGE
7.5 MG (BASE) ORAL EXTENDED-RELEASE TABLET
15 MG (BASE) ORAL EXTENDED-RELEASE TABLET
00002246354
00002246355
00002246357
00002246358
00002246360
00002273217
00002273225
ARANESP (0.4 ML SYRINGE)
ARANESP (0.5 ML SYRINGE)
ARANESP (0.3/ 0.4/ 0.5 ML SYR)
ARANESP (0.3/ 0.4/ 0.5/ 0.65 ML SYR)
ARANESP (0.3/0.4/0.6/1.0 ML SYR)
ENABLEX
ENABLEX
AMG
AMG
AMG
AMG
AMG
NOV
NOV
28.8100
57.6200
288.1000
536.0000
1444.1900
1.6150
1.6150
22 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
For this product - pricing has been established on a per millilitre basis.
For this product - pricing has been established on a per millilitre basis.
For this product - pricing has been established on a per millilitre basis.
$
$
$
$
$
$
$
Section 3 .
"For the treatment of anemia of chronic renal failure in patients with low hemoglobin (<100 g/L). Hemoglobin levels should be maintained within 100 - 110 g/L. According to current practice guidelines patients' iron status should be monitored regularly, and wherever possible patients should be iron replete as demonstrated by serum ferritin > 100 mcg/L and transferrin saturation > 20%."
"For the treatment of chemotherapy-induced anemia in patients with non-myeloid malignancies with low hemoglobin (<100 g/L) in whom blood transfusions are not possible due to transfusion reactions, cross-matching difficulties or iron overload. If hemoglobin is rising by more than 20 g/Lper month, the dose of Aranesp should be reduced by about 25%."
In order to comply with the second criterion: if the patient has iron overload the prescriber must state this in the request or alternatively, information is required regarding the patient's transferrinsaturation, along with the results of liver function tests if applicable.
For the first criterion, renewal requests may be considered if the patient's hemoglobin is < 120 g/L while on Aranesp.
For the second criterion, renewal requests may be considered if the patient's hemoglobin is < 110 g/L while on Aranesp.
All requests for darbepoetin must be completed using the Darbepoetin/Epoetin Special Authorization Request Form (ABC 30888).
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): OXYBUTYNIN
"For patients who are intolerant to oxybutynin.
Special authorization may be granted for 24 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DEFERASIROX
DENOSUMAB
125 MG ORAL DISPERSIBLE TABLET FOR SUSPENSION
250 MG ORAL DISPERSIBLE TABLET FOR SUSPENSION
500 MG ORAL DISPERSIBLE TABLET FOR SUSPENSION
60 MG / SYR INJECTION SYRINGE
00002287420
00002287439
00002287447
00002343541
EXJADE
EXJADE
EXJADE
PROLIA
NOV
NOV
NOV
AMG
10.8949
21.7898
43.5805
339.5700
23 EFFECTIVE APRIL 1, 2012
$
$
$
$
Section 3 .
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): DEFEROXAMINE
"For patients who require iron chelation therapy but who have an inadequate response to a sufficient trial (i.e. a minimum of 6 months) of deferoxamine, or for whom deferoxamine is contraindicated.
Contraindications may include one or more of the following: known or suspected sensitivity to deferoxamine, recurrent injection or infusion-site reactions associated with deferoxamine administration (e.g., cellulitis), inability to obtain or maintain vascular access, severe needle phobia, concomitant bleeding disorders, immunocompromised patients with a risk of infection with parenteral administration, or risk of bleeding due to anticoagulation.
According to the product monograph, Exjade (deferasirox) is contraindicated in high risk myelodysplastic syndrome (MDS) patients, any other MDS patient with a life expectancy less than one year and patients with other hematological and nonhematological malignancies who are not expected to benefit from chelation therapy due to the rapid progression of their disease.
Special authorization may be granted for 24 months."
"For the treatment of postmenopausal osteoporosis in women for whom oral bisphosphonates arecontraindicated due to hypersensitivity OR an endoscopically or radiographically confirmed untreatable abnormality of the esophagus which delays esophageal emptying (e.g., stricture or achalasia), AND who have at least two of the following:- Age greater than or equal to 75 years- A prior fragility fracture- A bone mineral density (BMD) T-score of less than or equal to -2.5
Special authorization may be granted for 12 months.
Patients will be limited to receiving one dose of denosumab per prescription at their pharmacy.
Coverage cannot be provided for two or more osteoporosis medications (alendronate,calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intendedfor use as combination therapy.
All requests for denosumab must be completed using the Denosumab Special Authorization Request Form (ABC 31377).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DONEPEZIL HCL
DUTASTERIDE
5 MG ORAL TABLET
10 MG ORAL TABLET
0.5 MG ORAL CAPSULE
00002232043
00002232044
00002247813
ARICEPT
ARICEPT
AVODART
PFI
PFI
GSK
5.1801
5.1801
1.7813
24 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
Section 3 .
"For the treatment of Alzheimer's disease in patients with an MMSE (Mini Mental State Exam) score between 10-26 and/or an InterRAI-Cognitive Performance Scale score between 1-4.
Coverage cannot be provided for two or more medications used in the treatment of Alzheimer's disease (donepezil, galantamine, rivastigmine) when these medications are intended for use in combination.
Special authorization coverage may be granted for a maximum of 24 months per request.
For each request, an updated MMSE score or InterRAI-Cognitive Performance Scale score and the date on which the exam was administered must be provided.
Renewal requests may be considered for patients where the updated MMSE score is 10 or higher or the InterRAI-Cognitive Performance Scale is 4 or lower while on this drug."
All requests (including renewal requests) for donepezil HCI must be completed using the Donepezil/Galantamine/Rivastigmine Special Authorization Request Form (ABC 30776).
"For the treatment of benign prostatic hyperplasia in patients who are poor surgical risks or who have enlarged prostates and have moderate to severe symptoms suggestive of obstruction.
Special authorization may be granted for 6 months"
Information is required regarding the medical condition(s) or circumstances by which this patient would be deemed a poor surgical risk.
All requests (including renewal requests) for dutasteride must be completed using the Dutasteride/Finasteride Special Authorization Request Form (ABC 31257).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ECULIZUMAB
25 EFFECTIVE APRIL 1, 2012 Section 3 .
ECULIZUMAB
1. ELIGIBILITY CRITERIA FOR ECULIZUMAB COVERAGE
In order to maintain the integrity of the AHWDBL, and having regard to the financial and social implications of covering eculizumab for the treatment of paroxysmal nocturnal hemoglobinuria (PNH), the following special authorization criteria must be satisfied. In order to be eligible for eculizumab coverage for the treatment of PNH, a patient must have submitted a completed Application and have satisfied all of the following requirements:
The patient must:1) Be diagnosed with PNH in accordance with the requirements specified in the Clinical Criteria for eculizumab;2) Have Alberta government-sponsored drug coverage;3) Meet the Registration Requirements; 4) Satisfy the Clinical Criteria for eculizumab (initial or continued coverage, as appropriate); AND5) Meet the criteria specified in Contraindications to Coverage and Discontinuance of Coverage.
There is no guarantee that any application, whether for initial or continued coverage, will be approved. Depending on the circumstances of each case, the Minister or the Minister's delegate may:- approve an Application;- approve an Application with conditions;- deny an Application;- discontinue an approved Application; OR- defer an Application pending the provision of further supporting information.
The process for review and approval is explained in further detail below.
2. REGISTRATION REQUIREMENTS
If the patient is a citizen or permanent resident of Canada, the patient must be continuously registered in the Alberta Health Care Insurance Plan for a minimum of one (1) year prior to an application for coverage unless: - the patient is less than one (1) year of age at the date of the application, then the patient's parent/guardian/legal representative must be registered continuously in the Alberta Health Care Insurance Plan for a minimum of one (1) year; OR- the patient has moved to Alberta from another province or territory in Canada (the" province of origin"), and immediately prior to moving to Alberta, was covered for eculizumab in the province of origin by a provincial or territorial government sponsored drug plan, (or the province of origin provided equivalent coverage for eculizumab as does Alberta) and the patient has been registered in the Alberta Health Care Insurance Plan (the patient must provide supporting documentation from the province of origin to prove prior coverage). If the patient is not a citizen or permanent resident of Canada, the patient must be continuously registered in the Alberta Health Care Insurance Plan for a minimum of five (5) years prior to an application for coverage unless:- the patient is less than five years of age at the date of the application, then the patients parent/guardian/legal representative must be registered continuously in the Alberta Health Care Insurance Plan for a minimum of five years; OR- the patient has moved to Alberta from another province or territory in Canada (the "province of origin"), and immediately prior to moving to Alberta, was covered for eculizumab in the province of origin by a provincial or territorial government sponsored drug plan, (or the province of origin provided equivalent coverage for eculizumab as does Alberta) and the patient has been registered in the Alberta Health Care Insurance Plan (the patient must provide supporting documentation from the province of origin to prove prior coverage).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ECULIZUMAB
26 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
The Minister reserves the right to modify or waive the Registration Requirements applicable to a given patient if the patient or the patient's parent/guardian/legal representative can establish to the satisfaction of the Minister that the patient has not moved to Alberta for the sole/primary purpose of obtaining coverage of eculizumab.
3. CLINICAL CRITERIA
In addition to meeting Sections 1 and Sections 2 herein, to be considered for coverage of eculizumab, a patient must be assessed by a Specialist in Hematology (i.e. a physician who holds specialty certification in Hematology from the Royal College of Physicians and Surgeons of Canada) and meet all of the following clinical criteria (initial or continued coverage, as appropriate).
a. CLINICAL CRITERIA - INITIAL COVERAGEAll of the following Clinical Criteria must be established on the basis of evidence to the satisfaction of the Minister or the Minister's delegate for initial coverage:
1) The diagnosis of PNH must have been established by flow cytometry and/or a FLAER test. The proportion of circulating cells of each type which are GPI-deficient and hence of the PNH clone is quantitated by flow cytometry. Patients must have a: - PNH granulocyte clone size equal to or greater than 10%, AND - Raised LDH (value at least 1.5 times the upper limit of normal for the reporting laboratory).
2) Patients with a clone size equal to or greater than 10% also require AT LEAST ONE of the following:- Thrombosis: Evidence that the patient has had a thrombotic or embolic event which required the institution of therapeutic anticoagulant therapy;- Transfusions: Evidence that the patient has been transfused with at least four (4) units of red blood cells in the last twelve (12) months;- Anemia: Evidence that the patient has chronic or recurrent anemia where causes other than hemolysis have been excluded and demonstrated by more than one measure of less than or equal to 70g/L or by more than one measure of less than or equal to 100 g/L with concurrent symptoms of anemia;- Pulmonary insufficiency: Evidence that the patient has debilitating shortness of breath and/or chest pain resulting in limitation of normal activity (New York Heart Association Class III) and/or established diagnosis of pulmonary arterial hypertension, where causes other than PNH have been excluded;- Renal insufficiency: Evidence that the patient has a history of renal insufficiency, demonstratedby an eGFR less than or equal to 60mL/min/1.73m2, where causes other than PNH have been excluded; OR- Smooth muscle spasm: Evidence that the patient has recurrent episodes of severe pain requiring hospitalisation and/or narcotic analgesia, where causes other than PNH have been excluded.
AND
3) All patients must receive meningococcal vaccination with a quadravalent vaccine (A, C, Y andW135) at least two (2) weeks prior to receiving the first dose of eculizumab. All patients must bemonitored and revaccinated according to current medical guidelines for vaccine use. Treating physicians will be required to submit confirmation of meningococcal vaccination in order for their patients to continue to be eligible for treatment with eculizumab.
b. CLINICAL CRITERIA - CONTINUED COVERAGEAll of the following Clinical Criteria must be established on the basis of evidence to the satisfaction of the Minister or the Minister's delegate for continued coverage:1) Patient eligibility must be reviewed six (6) months after commencing therapy and every six (6)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ECULIZUMAB
27 EFFECTIVE APRIL 1, 2012 Section 3 .
months thereafter;
AND
2) Continued eligibility will be subject to the assessment of evidence, in accordance with the following monitoring requirements, which demonstrates:- Clinical improvement in the patient, OR- Stabilization of the patient's condition;
Monitoring requirements;
The patient's Specialist in Hematology must provide the following monitoring information every six (6) months:- Lactate dehydrogenase (LDH);- Full blood count and reticulocytes;- Transfusion history for previous six months;- Iron studies;- Urea, electrolytes and eGFR; - Recent clinical history; AND- Any other information requested by the Minister, the Minister's delegate, or an Expert Advisor.
The patient's Specialist in Hematology must provide the following monitoring information every twelve (12) months:- Confirmation that the patient has been vaccinated or revaccinated (meningococcal) according to current medical guidelines for vaccine use;- Progress reports on the clinical symptoms that formed the basis of initial eligibility;- Quality of life, through clinical narrative; - Granulocyte clone size (by flow cytometry): AND- Any other information requested by the Minister, the Minister's delegate, or an Expert Advisor.
c. CONTRAINDICATIONS TO COVERAGE
In addition to meeting all of the Initial Coverage Clinical Criteria or the Continued Coverage Clinical Criteria referred to above (as appropriate), the patient must not have any of the followingcontraindications:- Small granulocyte clone size - a granulocyte clone size below 10%; - Aplastic anaemia with two or more of the following: neutrophil count below 0.5 x 109/L, platelet count below 20 x 109/L, reticulocytes below 25 x 109/L, or severe bone marrow hypocellularity; - Patients with a presence of another life threatening or severe disease where the long term prognosis is unlikely to be influenced by therapy (for example acute myeloid leukaemia or high-risk myelodysplastic syndrome); OR- The presence of another medical condition that in the opinion of the Minister or Minister's delegate might reasonably be expected to compromise a response to therapy.
d. DISCONTINUANCE OF COVERAGE
Coverage may be discontinued where one or more of the following situations apply:- The patient or the patient's Specialist in Hematology fails to comply adequately with treatment or measures, including monitoring requirements, taken to evaluate the effectiveness of the therapy;- There is a failure to provide the Minister, the Minister's delegate, or an Expert Advisor with information as required or as requested;- If in the opinion of the Minister or the Minister's delegate, therapy fails to relieve the symptoms of disease that originally resulted in the patient being approved by the Minister or the Minister's delegate; - The patient has (or develops) a condition referred to in Contraindications to Coverage.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ECULIZUMAB
28 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
The patient's Specialist in Hematology will be advised if their patient is at risk of being withdrawnfrom treatment for failure to comply with the above requirements or other perceived "non-compliance" and given a reasonable period of time to respond prior to coverage being discontinued.
4. PROCESS FOR ECULIZUMAB COVERAGE
For both initial and continued coverage the following documents (the Application) must be completed and submitted:
- An Eculizumab Special Authorization Request Form completed by the patient's Specialist in Hematology;- An Eculizumab Consent Form completed by the patient, or a patient's parent/guardian/legal representative, and the patients Specialist in Hematology (for any initial coverage application); AND- Any other documentation that may be required by the Minister or the Minister's delegate.
a. EXPERT REVIEW
Once the Minister or the Minister's delegate has confirmed that the patient meets the Registration Requirement or granted a waiver of the Registration Requirement, the Application will be given to one or more Expert Advisors for review.
The Application, together with the recommendation or recommendations of the Expert Advisor(s), is then forwarded to the Minister or the Minister's delegate for a decision regarding coverage.
After the Minister or Minister's delegate has rendered a decision, the patient's Specialist in Hematology and the patient or patient's parent/guardian/legal representative will be notified by letter of the Minister's decision.
5. APPROVAL OF COVERAGEThe Minister or the Minister's delegate's decision in respect of an Application will specify the effective date of eculizumab coverage, if coverage is approved.
Initial coverage may be approved for a period of up to six (6) months as follows: One dose of 600mg of eculizumab administered weekly for the first four (4) weeks of treatment (total of four 600mg doses), followed by one dose of 900mg of eculizumab administered every two (2) weeks from week five (5) of treatment (total of eleven 900mg doses).
Continued coverage may be approved for up to one dose of 900mg of eculizumab administered every two (2) weeks, for a period of six (6) months (total of thirteen 900mg doses).
If a patient is approved for coverage, prescriptions for eculizumab must be written by a Specialist in Hematology. To avoid wastage, prescription quantities are limited to a one-month supply. Extended quantity and vacation supplies are not permitted. The Government is not responsible and will not pay for costs associated with wastage or improper storage of eculizumab.
Approval of coverage is granted for a specific period, to a maximum of six (6) months. If continued treatment is necessary, it is the responsibility of the patient or patient's parent/guardian/legal representative and the Specialist in Hematology to submit a new Application to re-apply for eculizumab coverage, and receive a decision thereon, prior to the expiry date of the authorization period.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ECULIZUMAB
EPOETIN ALFA
300 MG / VIAL INJECTION
30,000 UNIT / SYR INJECTION SYRINGE
40,000 UNIT / SYR INJECTION SYRINGE
00002322285
00002288680
00002240722
SOLIRIS
EPREX
EPREX
API
JAI
JAI
7248.1875
452.5105
452.5105
29 EFFECTIVE APRIL 1, 2012
$
$
$
Section 3 .
"For the treatment of chemotherapy-induced anemia in patients with non-myeloid malignancies with low hemoglobin (<100 g/L) in whom blood transfusions are not possible due to transfusion reactions, cross-matching difficulties or iron overload. If hemoglobin is rising by more than 20 g/L per month, the dose of Eprex should be reduced by about 25%. Patients may be granted a maximum allowable dose of 40,000 IU per week."
In order to comply with this criterion, if the patient has iron overload the prescriber must state this in the request, or alternatively, information is required regarding the patient's transferrin saturation, along with the results of liver function tests, if applicable.
Renewal requests may be considered if the patient's hemoglobin is <110 g/L while on Eprex."
All requests for epoetin alfa must be completed using the Darbepoetin/Epoetin Special Authorization Request Form (ABC 30888).
6. WITHDRAWAL
Therapy may be withdrawn at the request of the patient or the patient's parent/guardian/legal representative at any time. Notification of withdrawal from therapy must be made by the Specialist in Hematology or patient in writing.
Applications, withdrawal requests, and any other information to be provided must be sent to Clinical Drug Services, Alberta Blue Cross.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
EPOETIN ALFA
1,000 UNIT / SYR INJECTION SYRINGE
2,000 UNIT / SYR INJECTION SYRINGE
3,000 UNIT / SYR INJECTION SYRINGE
4,000 UNIT / SYR INJECTION SYRINGE
5,000 UNIT / SYR INJECTION SYRINGE
6,000 UNIT / SYR INJECTION SYRINGE
8,000 UNIT / SYR INJECTION SYRINGE
10,000 UNIT / SYR INJECTION SYRINGE
20,000 UNIT / SYR INJECTION SYRINGE
00002231583
00002231584
00002231585
00002231586
00002243400
00002243401
00002243403
00002231587
00002243239
EPREX (0.5 ML SYRINGE)
EPREX (0.5 ML SYRINGE)
EPREX (0.3 ML SYRINGE)
EPREX (0.4 ML SYRINGE)
EPREX (0.5 ML SYRINGE)
EPREX (0.6 ML SYRINGE)
EPREX (0.8 ML SYRINGE)
EPREX (1 ML SYRINGE)
EPREX (0.5 ML SYRINGE)
JAI
JAI
JAI
JAI
JAI
JAI
JAI
JAI
JAI
15.3188
30.6375
45.9563
61.2750
76.5938
91.9125
122.5500
153.1875
301.6665
30 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
Section 3 .
"For the treatment of anemia of chronic renal failure in patients with low hemoglobin (< 100 g/L). Hemoglobin levels should be maintained within 100 - 110 g/L. According to current practice guidelines patients' iron status should be monitored regularly, and wherever possible patients should be iron replete as demonstrated by serum ferritin > 100 mcg/L and transferrin saturation > 20%."
"For the treatment of anemia in AZT-treated/HIV infected patients."
"For the treatment of chemotherapy-induced anemia in patients with non-myeloid malignancies with low hemoglobin (<100 g/L) in whom blood transfusions are not possible due to transfusion reactions, cross-matching difficulties or iron overload. If hemoglobin is rising by more than 20 g/Lper month, the dose of Eprex should be reduced by about 25%."
In order to comply with the third criterion: if the patient has iron overload the prescriber must state this in the request or alternatively, information is required regarding the patient's transferrinsaturation, along with the results of liver function tests if applicable.
For the first criterion, renewal requests may be considered if the patient's hemoglobin is < 120 g/L while on Eprex.
For the third criterion, renewal requests may be considered if the patient's hemoglobin is < 110 g/L while on Eprex.
All requests for epoetin alfa must be completed using the Darbepoetin/Epoetin Special Authorization Request Form (ABC 30888).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ERTAPENEM
ERYTHROMYCIN/ TRETINOIN
1 G / VIAL INJECTION
4 % * 0.01 % TOPICAL GEL
4 % * 0.025 % TOPICAL GEL
4 % * 0.05 % TOPICAL GEL
00002247437
00002015994
00001905112
00001945262
INVANZ
STIEVAMYCIN MILD
STIEVAMYCIN REGULAR
STIEVAMYCIN FORTE
MFC
GSK
GSK
GSK
49.9500
0.8925
0.8925
0.8925
31 EFFECTIVE APRIL 1, 2012
$
$
$
$
Section 3 .
"For therapy of complicated polymicrobial skin and skin structure infections."
"For the therapy of community-acquired intra-abdominal infections."
"For culture & susceptibility directed therapy against infections with Enterobacteriaceae producing AmpC or extended-spectrum beta-lactamases (ESBLs) where there is resistance to first line agents."
"For use in other Health Canada approved indications, in consultation with a specialist in Infectious Diseases."
In order to comply with all of the above criteria, information is required regarding the type of infection and organisms involved. Also, where the criteria restrict coverage of the requested drug to non-first line therapy, information is required regarding previous first-line antibiotic therapy that has been utilized, the patient's response to therapy, and the first line agents the organism is resistant to or why other first-line therapies cannot be used in this patient. Also, where applicable, the specialist in Infectious Diseases that recommended this drug is required.
"For the treatment of severe acne as defined by scarring acne.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ETANERCEPT
32 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Rheumatoid Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) who are refractory or intolerant to:
- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4-month trial). [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology who agrees to and continues to actively and consistently participate in the Alberta Post-Marketing Study ("Study") as required by Alberta Health and Wellness or its agent, throughout the special authorization approval period ("RA Specialist"). The patient must also provide all consents and authorizations required to permit the RA Specialist to actively and consistently participate in the Study. Special authorization approval for the patient may be revoked if the RA Specialist does not continually, actively and consistently participate in the Study.
- Initial coverage may be approved for 50 mg per week for 8 weeks.- Patients will be limited to receiving a one-month supply of etanercept per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond 8 weeks, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after 8 weeks, but no longer than 12 weeks after treatment to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for 50 mg per week, for a period of 12 months. Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ETANERCEPT
33 EFFECTIVE APRIL 1, 2012 Section 3 .
1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or - Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for etanercept for Rheumatoid Arthritis must be completed using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
Juvenile Idiopathic Arthritis:
"Special authorization coverage may be provided for the reduction in signs and symptoms of severely active polyarticular juvenile idiopathic arthritis (JIA) in patients 4 years of age and older who:- Have 5 or more active joints (defined by either swelling or limitation of motion plus pain and/or tenderness), AND- Are refractory to one or more disease modifying anti-rheumatic agents (DMARDS) conventionally used in children (minimum three month trial).
"Refractory" is defined as one or more of the following: lack of effect, serious adverse effects (e.g., leukopenia, hepatitis) or contraindications to treatments as defined in the product monographs.
For coverage, this drug must be prescribed by a prescriber affiliated with a Pediatric Rheumatology Clinic in Edmonton or Calgary who agrees to and continues to actively and consistently participate in the Alberta Post-Marketing Study ("Study") as required by Alberta Health and Wellness and its agent, throughout the special authorization approval period (Pediatric RA Specialist). The patient or patient's guardian must also provide all consents and authorizations required to permit the Pediatric RA Specialist to actively and consistently participate in the Study. Special authorization approval for the patient may be revoked if the Pediatric RA Specialist does not continually, actively and consistently participate in the Study.
- Coverage may be approved for 0.8 mg/kg/dose (maximum dose 50 mg) weekly for 12 weeks.- Patients will be limited to receiving a one-month supply of Enbrel per prescription at their pharmacy.
For continued coverage of this agent beyond 12 weeks, the patient must meet the following criteria:1) The patient must be assessed by a Pediatric RA Specialist after 12 weeks, but no longer than16 weeks after, treatment with this biologic agent to determine response.2) The Pediatric RA Specialist must confirm in writing that the patient is a responder that meets the following criteria (JRA30):- 30% improvement from baseline in at least three of the following six response variables, with worsening of 30% or more in no more than one of the six variables. The variables include: i. global assessment of the severity of the disease by the Pediatric RA Specialist, ii. global assessment of overall well-being by the patient or parent, iii. number of active joints (joints with swelling not due to deformity or joints with limitation of motion with pain tenderness or both), iv. number of joints with limitation of motion, v. functional ability based on CHAQ scores, vi. ESR or CRP
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ETANERCEPT
34 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
3) Data from all of the six variables comprising the JRA30 and the CHAQ scores must be reported in each request
Following this assessment, continued coverage may be approved for 0.8 mg/kg/dose (maximumdose 50 mg) weekly, for a maximum of twelve months. After twelve months, in order to be considered for continued coverage, the patient must be re-assessed every twelve months by a Pediatric RA Specialist and must meet the following criteria:1) The patient has been assessed by a Pediatric RA Specialist to determine response, and2) The Pediatric RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by maintenance of the JRA30,3) Data from all of the six variables comprising the JRA30 and the CHAQ scores must be reported in each request.
Once a child with JIA has had two disease-free years, it is common clinical practice for drug treatment to be stopped."
All requests (including renewal requests) for etanercept for Juvenile Idiopathic Arthritis must be completed using the Etanercept for Juvenile Idiopathic Arthritis Special Authorization Request Form (ABC 30948).
Psoriatic Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for reducing signs and symptoms and inhibiting the progression of structural damage of active arthritis in adult patients (18 years of age or older) with moderate to severe polyarticular psoriaticarthritis (PsA) or pauciarticular PsA with involvement of knee or hip joint who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- An adequate trial of another disease modifying anti-rheumatic agent(s) (minimum 4 month trial).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 50 mg per week for 8 weeks.- Patients will be limited to receiving a one-month supply of etanercept per prescription at their pharmacy. - Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond 8 weeks, the patient must meet the following criteria: The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ETANERCEPT
35 EFFECTIVE APRIL 1, 2012 Section 3 .
1) The patient must be assessed by an RA Specialist after 8 weeks, but no longer than 12 weeks after treatment to determine response. 2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria: - ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for 50 mg per week, for a period of 12 months. Ongoing coverage may be considered if the following criteria are met at theend of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or- Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for etanercept for Psoriatic Arthritis must be completed using the Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form (ABC 30964).
Ankylosing Spondylitis:
"Special authorization coverage may be provided for the reduction in the signs and symptoms ofseverely active Ankylosing Spondylitis, as defined by the Modified New York criteria for Ankylosing Spondylitis, in adult patients (18 years of age or older) who have active disease as demonstrated by:
- a BASDAI greater than or equal to 4 units, demonstrated on 2 occasions at least 8 weeks apartAND- a Spinal Pain VAS of greater than or equal to 4 cm (on a 0-10 cm scale), demonstrated on 2 occasions at least 8 weeks apart AND- who are refractory or intolerant to treatment with 2 or more NSAIDS each taken for a minimum of 4 weeks at maximum tolerated or recommended doses.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 50 mg per week for 12 weeks.- Patients will be limited to receiving a one-month supply of etanercept per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ETANERCEPT
36 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond 12 weeks, the patient must meet the following criteria:1) The patient must be assessed at week 12 by an RA Specialist after the initial twelve weeks oftherapy to determine response.2) The RA Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Reduction of the BASDAI score by at least 50% of the pre-treatment value or by 2 or more units, AND - Reduction of the Spinal Pain VAS by 2 cm or more.
Following this assessment, continued coverage may be approved for 50 mg per week for a period of 12 months. Ongoing coverage may be considered if the patient is re-assessed by an RA Specialist every 12 months and is confirmed to be continuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for etanercept for Ankylosing Spondylitis must be completed using the Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form (ABC 31195).
Plaque Psoriasis:
"Special authorization coverage may be provided for the reduction in signs and symptoms of severe, debilitating plaque psoriasis in patients who:- Have a total PASI of 10 or more and a DLQI of more than 10, OR- Who have significant involvement of the face, palms of the hands, soles of the feet or genital region; AND- Who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory, OR- Cyclosporine (6 weeks treatment); AND- Phototherapy (unless restricted by geographic location)
Patients who have a contraindication to either cyclosporine or methotrexate will be required to complete an adequate trial of the other pre-requisite medication prior to potential coverage beingconsidered.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be prescribed by a Specialist in Dermatology ("Dermatology Specialist").
-Initial coverage may be approved for up to 100 mg per week for 12 weeks.-Patients will be limited to receiving a one-month supply of etanercept per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ETANERCEPT
EZETIMIBE
25 MG / VIAL INJECTION
50 MG / SYR INJECTION SYRINGE
10 MG ORAL TABLET
00002242903
00002274728
00002247521
ENBREL
ENBREL
EZETROL
AMG
AMG
MFC
189.4150
378.9425
1.7927
37 EFFECTIVE APRIL 1, 2012
Note: 1 x 50 mg syringe is interchangeable with 2 x 25 mg vials
$
$
$
Section 3 .
which it is being prescribed.
For continued coverage beyond 12 weeks, the patient must meet all of the following criteria:1) The patient must be assessed by a Dermatology Specialist after the initial 12 weeks of therapy to determine response.2) The Dermatology Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Greater than or equal to 75% reduction in PASI score, OR- Greater than or equal to 50% reduction in PASI score AND improvement of greater than or equal to 5 points in the DLQI
Following this assessment, continued coverage may be considered for 50 mg per week for a period of 12 months. Ongoing coverage may be considered if the patient is re-assessed by a Dermatology Specialist every 12 months and is confirmed to be continuing to respond to therapyby meeting criteria as outlined in (2) above."
All requests (including renewal requests) for etanercept for Plaque Psoriasis must be completed using the Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form (ABC 31192).
"For the treatment of hypercholesterolemia in patients who are intolerant to statins or in whom a statin is contraindicated and who are at high cardiovascular risk*; or
For the treatment of hypercholesterolemia when used in combination with a statin in patients failing to achieve target LDL with a statin at maximum tolerable dose or maximum recommendeddose as per respective product monograph and who are at high cardiovascular risk*:
* High cardiovascular risk is defined as possessing one of the following:1) Pre-existing cardiovascular disease and/or cerebrovascular disease, or2) Diabetes, or3) Familial hypercholesterolemia, or4) Greater than or equal to 20% risk as defined by the Framingham Risk Assessment Tool, or5) Three or more of the following risk factors:- Family history of premature cardiovascular disease- Smoking- Hypertension- Obesity- Glucose intolerance- Renal disease.
Special authorization for these criteria may be granted for 6 months."
All requests for ezetimibe must be completed using the Ezetimibe Special Authorization RequestForm (ABC 30925).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FEBUXOSTAT
FENTANYL
80 MG ORAL TABLET
12 MCG/HR TRANSDERMAL PATCH
25 MCG/HR TRANSDERMAL PATCH
00002357380
00002311925000023413790000233010500002327112
0000231463000002341387000023301130000228294100002327120
ULORIC
RATIO-FENTANYLPMS-FENTANYL MTXRAN-FENTANYL MATRIXSANDOZ FENTANYL PATCH
NOVO-FENTANYL 25PMS-FENTANYL MTXRAN-FENTANYL MATRIXRATIO-FENTANYLSANDOZ FENTANYL PATCH
TAK
RPHPMSRANSDZ
TEVPMSRANRPHSDZ
1.7092
2.6860 2.6861 2.6861 2.6861
5.9500 5.9500 5.9500 5.9500 5.9500
38 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$$
$$$$$
Section 3 .
"For patients with symptomatic gout who have documented hypersensitivity OR severe intolerance to allopurinol, AND intolerance or lack of response to sulfinpyrazone AND probenecid.
Special authorization may be granted for 6 months."
Please note: Coverage cannot be considered for lack of response to allopurinol.
All requests for febuxostat must be completed using the Febuxostat Special Authorization Request Form (ABC 31376).
The following product(s) are eligible for auto-renewal.
"For the treatment of persistent, severe chronic pain in those patients who require continuous around-the-clock analgesia for an extended period of time in those patients who cannot swallow.Special authorization may be granted for 6 months."
"For the treatment of persistent, severe chronic pain in those patients who require continuous around-the-clock analgesia for an extended period of time in those patients who require opioid therapy at a total daily dose of at least 60 mg/day oral morphine equivalents. Patients must havetried and not been able to tolerate at least two discrete courses of therapy with two of the following agents: morphine, hydromorphone and oxycodone, if not contraindicated. Special authorization may be granted for 6 months."
Information is required regarding previous medications utilized and the patient's response to therapy. Also, information regarding the number of discrete (separate) courses of these medications is required. A discrete course is defined as a separate treatment course, which mayinvolve more than 1 agent, used at one time to manage the patient's condition.
All requests for fentanyl must be completed using the Fentanyl Special Authorization Request Form (ABC 31169).
(Please note: The following fentanyl products are benefits not requiring special authorization for individuals approved by Alberta Health and Wellness for Palliative Care Drug Coverage. Refer tothe Palliative Care Drug Benefit Supplement for additional information on this coverage.)
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
FENTANYL
FENTANYL CITRATE
50 MCG/HR TRANSDERMAL PATCH
75 MCG/HR TRANSDERMAL PATCH
100 MCG/HR TRANSDERMAL PATCH
0.05 MG / ML (BASE) INJECTION
0000231464900002341395000023301210000228296800002327147
0000231465700002341409000023301480000228297600002327155
0000231466500002341417000023301560000228298400002327163
00000888346
NOVO-FENTANYL 50PMS-FENTANYL MTXRAN-FENTANYL MATRIXRATIO-FENTANYLSANDOZ FENTANYL PATCH
NOVO-FENTANYL 75PMS-FENTANYL MTXRAN-FENTANYL MATRIXRATIO-FENTANYLSANDOZ FENTANYL PATCH
NOVO-FENTANYL 100PMS-FENTANYL MTXRAN-FENTANYL MATRIXRATIO-FENTANYLSANDOZ FENTANYL PATCH
FENTANYL CITRATE
TEVPMSRANRPHSDZ
TEVPMSRANRPHSDZ
TEVPMSRANRPHSDZ
HSP
11.2000 11.2000 11.2000 11.2000 11.2000
15.7500 15.7500 15.7500 15.7500 15.7500
19.6000 19.6000 19.6000 19.6000 19.6000
1.8859
39 EFFECTIVE APRIL 1, 2012
$$$$$
$$$$$
$$$$$
$
Section 3 .
"For the treatment of persistent, severe chronic pain in those patients who cannot swallow, or who are intolerant of, morphine and/or hydromorphone, if not contraindicated. Special authorization may be granted for 6 months."
Information is required regarding previous medications utilized and the patient's response to therapy. Information should include the use of agents such as morphine and/or hydromorphone, if not contraindicated for the patient.
All requests for fentanyl citrate must be completed using the Fentanyl Special Authorization Request Form (ABC 31169).
(Please note: The following fentanyl citrate product is a benefit not requiring special authorization for individuals approved by Alberta Health and Wellness for Palliative Care Drug Coverage. Refer to the Palliative Care Drug Benefit Supplement for additional information on this coverage.)
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FILGRASTIM
FINASTERIDE
0.3 MG / ML INJECTION
5 MG ORAL TABLET
00001968017
0000236538300002354462000023550430000235722400002356058000023485000000231011200002371820000023069050000232257900002010909
NEUPOGEN
APO-FINASTERIDECO FINASTERIDEFINASTERIDEJAMP-FINASTERIDEMYLAN-FINASTERIDENOVO-FINASTERIDEPMS-FINASTERIDERAN-FINASTERIDERATIO-FINASTERIDESANDOZ FINASTERIDEPROSCAR
AMG
APXCOBAHIJPCMYPTEVPMSRANRPHSDZMFC
200.8295
0.8338 0.8338 0.8338 0.8338 0.8338 0.8338 0.8338 0.8338 0.8338 0.8338 1.9182
40 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$$$$$$$$$
Section 3 .
"To decrease the incidence of infection, as manifested by febrile neutropenia, in patients with non-myeloid malignancies receiving myelosuppresive anti-neoplastic drugs with curative intent. This drug product must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates)."
"For the reduction in the duration of neutropenia, fever, antibiotic use and hospitalization following induction and consolidation treatment for acute myeloid leukemia. This drug product must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates)."
"To increase neutrophil counts and to reduce the incidence and duration of infection in patients with a diagnosis of congenital, cyclic or idiopathic neutropenia. This drug product must be prescribed by the Directors of Divisions of Hematology in tertiary care centres (or their designates)."
"For the treatment of patients undergoing Peripheral Blood Progenitor Cell (PBPC) collection and therapy when prescribed by a designated prescriber."
All requests for filgrastim must be completed using the Filgrastim/Pegfilgrastim Special Authorization Request Form (ABC 31150).
Please note for the first criterion: Coverage cannot be considered for palliative patients.
"For the treatment of benign prostatic hyperplasia in patients who are poor surgical risks or who have enlarged prostates and have moderate to severe symptoms suggestive of obstruction.
Special authorization may be granted for 6 months."
Information is required regarding the medical condition(s) or circumstances by which this patient would be deemed a poor surgical risk.
All requests (including renewal requests) for finasteride must be completed using the Dutasteride/Finasteride Special Authorization Request Form (ABC 31257).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
FLUCONAZOLE
FLUTAMIDE
GALANTAMINE HYDROBROMIDE
10 MG / ML ORAL SUSPENSION
250 MG ORAL TABLET
8 MG (BASE) ORAL EXTENDED-RELEASE CAPSULE
16 MG (BASE) ORAL EXTENDED-RELEASE CAPSULE
24 MG (BASE) ORAL EXTENDED-RELEASE CAPSULE
00002024152
00002238560000022300890000223010400000637726
000023394390000231694300002266717
000023394470000231695100002266725
000023394550000231697800002266733
DIFLUCAN
APO-FLUTAMIDENOVO-FLUTAMIDEPMS-FLUTAMIDEEUFLEX
MYLAN-GALANTAMINE ERPAT-GALANTAMINE ERREMINYL ER
MYLAN-GALANTAMINE ERPAT-GALANTAMINE ERREMINYL ER
MYLAN-GALANTAMINE ERPAT-GALANTAMINE ERREMINYL ER
PFI
APXTEVPMSMFC
MYPPATJAI
MYPPATJAI
MYPPATJAI
1.0652
1.3530 1.3530 1.3530 1.3922
2.1970 2.1970 5.4018
2.1970 2.1970 5.4018
2.1970 2.1970 5.4018
41 EFFECTIVE APRIL 1, 2012
$
$$$$
$$$
$$$
$$$
Section 3 .
"For susceptible infections in immunocompromised patients (e.g. patients with AIDS, cancer, or transplant patients)."
"When prescribed for non-cancer, non-cosmetic indications.
Special authorization may be granted for 6 months."
Information is required regarding the patient's diagnosis/indication for use of this medication.
The following product(s) are eligible for auto-renewal.
"For the treatment of Alzheimer's disease in patients with an MMSE (Mini Mental State Exam) score between 10-26 and/or an InterRAI-Cognitive Performance Scale score between 1-4.
Coverage cannot be provided for two or more medications used in the treatment of Alzheimer's disease (donepezil, galantamine, rivastigmine) when these medications are intended for use in combination.
Special authorization coverage may be granted for a maximum of 24 months per request.
For each request, an updated MMSE score or InterRAI-Cognitive Performance Scale score and the date on which the exam was administered must be provided.
Renewal requests may be considered for patients where the updated MMSE score is 10 or higher or the InterRAI-Cognitive Performance Scale is 4 or lower while on this drug."
All requests (including renewal requests) for galantamine hydrobromide must be completed using the Donepezil/Galantamine/Rivastigmine Special Authorization Request Form (ABC 30776).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
GOLIMUMAB
42 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Ankylosing Spondylitis:
"Special authorization coverage may be provided for the reduction in the signs and symptoms ofseverely active Ankylosing Spondylitis, as defined by the Modified New York criteria for Ankylosing Spondylitis, in adult patients (18 years of age or older) who have active disease as demonstrated by:- a BASDAI greater than or equal to 4 units, demonstrated on 2 occasions at least 8 weeks apartAND- a Spinal Pain VAS of greater than or equal to 4 cm (on a 0-10 cm scale), demonstrated on 2 occasions at least 8 weeks apart AND- who are refractory or intolerant to treatment with 2 or more NSAIDS each taken for a minimum of 4 weeks at maximum tolerated or recommended doses.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 50 mg once per month for four doses.- Patients will be limited to receiving one dose (50 mg) of golimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond four doses the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after the initial four doses to determine response.2) The RA Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Reduction of the BASDAI score by at least 50% of the pre-treatment value or by 2 or more units, AND- Reduction of the Spinal Pain VAS by 2 cm or more.
Following this assessment, continued coverage may be approved for 50 mg once per month for a further 12 month period. Should continued coverage criteria be met, coverage will only be granted for 12 doses per 12 month period. Ongoing coverage may be considered if the patient isre-assessed by an RA Specialist every 12 months and is confirmed to be continuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for golimumab for Ankylosing Spondylitis must be completed using the Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form (ABC 31195).
Psoriatic Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for reducing signs and symptoms of active arthritis in adult patients (18 years of age or older) with moderate to severe polyarticular psoriatic arthritis (PsA) or pauciarticular PsA with involvement of knee or hip joint who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
GOLIMUMAB
43 EFFECTIVE APRIL 1, 2012 Section 3 .
patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- An adequate trial of another disease modifying anti-rheumatic agent(s) (minimum 4 month trial).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 50 mg per month for four doses.- Patients will be limited to receiving one dose (50 mg) of golimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond four doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after four doses to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for 50 mg per month, for a further 12 month period. Should coverage criteria be met, coverage will only be granted for 12 doses per 12-month period. Ongoing coverage may be considered if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or- Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for golimumab for Psoriatic Arthritis must be completedusing the Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form (ABC 30964).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
GOLIMUMAB
44 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Rheumatoid Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4-month trial). [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for 50 mg per month for a total of four doses.- Patients will be limited to receiving one dose (50 mg) of golimumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond four doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after four doses to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for 50 mg per month, for a further 12 month period. Should continued coverage criteria be met, coverage will only be granted for 12 doses per 12 month period. Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or - Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
GOLIMUMAB
GOSERELIN ACETATE
50 MG / SYR INJECTION SYRINGE
3.6 MG / SYR (BASE) INJECTION SYRINGE
10.8 MG / SYR (BASE) INJECTION SYRINGE
0000232477600002324784
00002049325
00002225905
SIMPONISIMPONI
ZOLADEX
ZOLADEX LA
JAIJAI
AZC
AZC
1555.5250 1555.5250
419.7875
1196.4750
45 EFFECTIVE APRIL 1, 2012
$$
$
$
Section 3 .
requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for golimumab for Rheumatoid Arthritis must be completed using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
"When prescribed for non-cancer, non-cosmetic or non-fertility indications.
Special authorization may be granted for 6 months."
Information is required regarding the patient's diagnosis/indication for use of this medication.
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
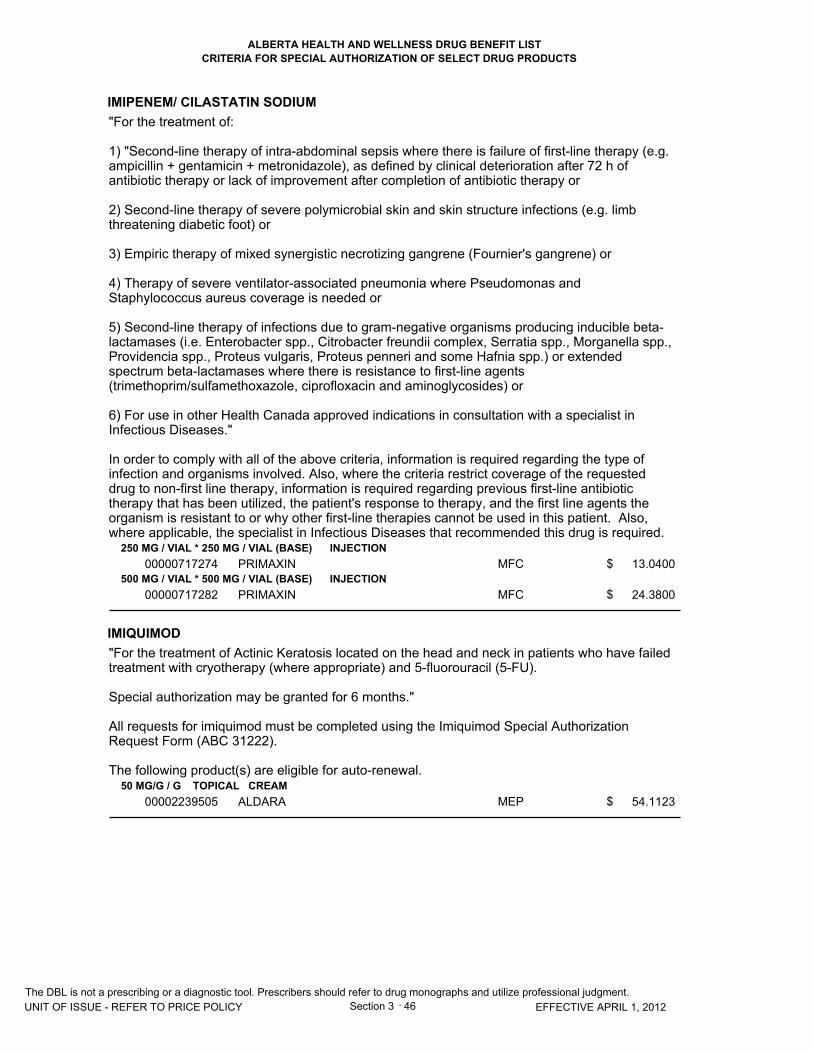
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
IMIPENEM/ CILASTATIN SODIUM
IMIQUIMOD
250 MG / VIAL * 250 MG / VIAL (BASE) INJECTION
500 MG / VIAL * 500 MG / VIAL (BASE) INJECTION
50 MG/G / G TOPICAL CREAM
00000717274
00000717282
00002239505
PRIMAXIN
PRIMAXIN
ALDARA
MFC
MFC
MEP
13.0400
24.3800
54.1123
46 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
Section 3 .
"For the treatment of:
1) "Second-line therapy of intra-abdominal sepsis where there is failure of first-line therapy (e.g. ampicillin + gentamicin + metronidazole), as defined by clinical deterioration after 72 h of antibiotic therapy or lack of improvement after completion of antibiotic therapy or
2) Second-line therapy of severe polymicrobial skin and skin structure infections (e.g. limb threatening diabetic foot) or
3) Empiric therapy of mixed synergistic necrotizing gangrene (Fournier's gangrene) or
4) Therapy of severe ventilator-associated pneumonia where Pseudomonas and Staphylococcus aureus coverage is needed or
5) Second-line therapy of infections due to gram-negative organisms producing inducible beta-lactamases (i.e. Enterobacter spp., Citrobacter freundii complex, Serratia spp., Morganella spp., Providencia spp., Proteus vulgaris, Proteus penneri and some Hafnia spp.) or extended spectrum beta-lactamases where there is resistance to first-line agents (trimethoprim/sulfamethoxazole, ciprofloxacin and aminoglycosides) or
6) For use in other Health Canada approved indications in consultation with a specialist in Infectious Diseases."
In order to comply with all of the above criteria, information is required regarding the type of infection and organisms involved. Also, where the criteria restrict coverage of the requested drug to non-first line therapy, information is required regarding previous first-line antibiotic therapy that has been utilized, the patient's response to therapy, and the first line agents the organism is resistant to or why other first-line therapies cannot be used in this patient. Also, where applicable, the specialist in Infectious Diseases that recommended this drug is required.
"For the treatment of Actinic Keratosis located on the head and neck in patients who have failed treatment with cryotherapy (where appropriate) and 5-fluorouracil (5-FU).
Special authorization may be granted for 6 months."
All requests for imiquimod must be completed using the Imiquimod Special Authorization Request Form (ABC 31222).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
INFLIXIMAB
47 EFFECTIVE APRIL 1, 2012 Section 3 .
Rheumatoid Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) who are refractory or intolerant to:
- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4 month trial) [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily)
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology who agrees to and continues to actively and consistently participate in the Alberta Post-Marketing Study ("Study") as required by Alberta Health and Wellness or its agent, throughout the special authorization approval period ("RA Specialist"). The patient must also provide all consents and authorizations required to permit the RA Specialist to actively and consistently participate in the Study. Special authorization approval for the patient may be revoked if the RA Specialist does not continually, actively and consistently participate in the Study.
- Initial coverage may be approved for three doses as follows: An initial dose of 3 mg/kg, followed by additional 3 mg/kg doses at 2 and 6 weeks after the first infusion.- Patients will be limited to receiving one dose of infliximab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond three doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after the initial three doses to determine response. 2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for one 3 mg/kg dose every 8 weeks for a period of 12 months [Note: For patients who have an incomplete response, consideration may be given to adjusting the dose up to 10 mg/kg and/or treating as often as every 4 weeks]. Ongoing coverage may be considered only if the following criteria are met at theend of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
INFLIXIMAB
48 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
therapy as indicated by:- confirmation of maintenance of ACR20, OR - maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for infliximab for Rheumatoid Arthritis must be completed using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
Moderately to Severely Active Crohn's Disease and Fistulizing Crohn's Disease:
"Special authorization coverage may be approved for coverage of infliximab for the reduction in signs and symptoms and induction and maintenance of clinical remission of Moderately to Severely Active Crohn's Disease and/or treatment of Fistulizing Crohn's Disease in patients whomeet the following criteria:
- Infliximab must be prescribed by a Specialist in Gastroenterology or a physician appropriately trained by the University of Alberta or the University of Calgary and recognized as a prescriber by Alberta Blue Cross for infliximab for coverage for the treatment of Moderately to Severely Active Crohn's Disease and/or Fistulizing Crohn's Disease patients (`Specialist').- Patients must be 18 years of age or older to be considered for coverage of infliximab.- Patients will be limited to receiving one dose of infliximab per prescription at their pharmacy.- Patients may be allowed to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy (both primary loss of response and secondary loss of response) or due to serious adverse effects or contraindications. An adequatetrial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
Prior to initiation of infliximab therapy for New Patients:
'New Patients' are patients who have never been treated with infliximab by any health care provider.
Moderately to Severely Active Crohn's Disease:
Prior to initiation of infliximab therapy, New Patients must have a current Modified (without the physical exam) Harvey Bradshaw Index score of greater than or equal to 7 (New Patient's Baseline Score), AND be Refractory.
Refractory is defined as one or more of the following:1) Serious adverse effects or reactions to the treatments specified below; OR 2) Contraindications (as defined in product monographs) to the treatments specified below; OR3) Previous documented lack of effect at doses and for duration of all treatments specified below: a) mesalamine: minimum of 3 grams/day for a minimum of 6 weeks; AND refractory to, or dependent on, glucocorticoids: following at least one tapering dosing schedule of 40 mg/day, tapering by 5 mg each week to 20 mg, then tapering by 2.5 mg each week to zero, or similar;
[Note: Patients who have used the above treatments in combination will not be required to be challenged with individual treatments as monotherapy]
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
INFLIXIMAB
49 EFFECTIVE APRIL 1, 2012 Section 3 .
ANDb) Immunosuppressive therapy as follows: - Azathioprine: minimum of 2 mg/kg/day for a minimum of 3 months; OR - 6-mercaptopurine: minimum of 1 mg/kg/day for a minimum of 3 months; OR- Methotrexate: minimum or 15 mg/week for a minimum of 3 months.OR - Immunosuppressive therapy discontinued at less than 3 months due to serious adverse effectsor reactions.
Applications for coverage must include information regarding the dosages and duration of trial ofeach treatment the patient received, a description of any adverse effects, reactions, contraindications and/or lack of effect, as well as any other information requested by Alberta Blue Cross.
Fistulizing Crohn's Disease:
Prior to initiation of infliximab therapy, New Patients must have actively draining perianal or enterocutaneous fistula(s) that have recurred or persisted despite:
a) A course of an appropriate dose of antibiotic therapy (e.g. ciprofloxacin or metronidazole) for a minimum of 3 weeks; ANDb) Immunosuppressive therapy: - Azathioprine: minimum of 2 mg/kg/day for a minimum of 6 weeks; OR - 6-mercaptopurine: minimum of 1 mg/kg/day for a minimum of 6 weeks; OR - Immunosuppressive therapy discontinued at less than 6 weeks due to serious adverse effects or reactions.
[Note: Patients who have used the above treatments in combination for the treatment of Fistulizing Crohn's will not be required to be challenged with individual treatments as monotherapy]
Applications for coverage must include information regarding the dosages and duration of trial ofeach treatment the patient received, a description of any adverse effects, reactions, contraindications and/or lack of effect, as well as any other information requested by Alberta Blue Cross.
Coverage Criteria for Moderately to Severely Active Crohn's Disease AND/OR Fistulizing Crohn's Disease
- New Patients must meet the criteria above prior to being considered for approval. - All approvals are also subject to the following applicable criteria.
Induction Dosing for New Patients:
- Coverage for Induction Dosing may only be approved for New Patients (those who have never been treated with infliximab by any health care provider).- 'Induction Dosing' means a maximum of one 5 mg/kg dose of infliximab per New Patient at each 0, 2 and 6 weeks (for a maximum total of three doses).- New Patients are eligible to receive Induction Dosing only once, after which time the Maintenance Dosing for New Patients and Continued Coverage for Maintenance Dosing criteria will apply.
Maintenance Dosing:
'Maintenance Dosing' means one 5 mg/kg dose of infliximab per patient provided no more often than every 8 weeks for a period of 12 months to:- New Patients following the completion of Induction Dosing; OR - Existing Patients, who are patients that are being treated, or have previously been treated, withinfliximab.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
INFLIXIMAB
50 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Maintenance Dosing for New Patients after Completion of Induction Dosing:
- The New Patient must be assessed by a Specialist between weeks 10 and 14 after the initiation of Induction Dosing to determine response by obtaining a Modified Harvey Bradshaw Index score for patients with Moderately to Severely Active Crohn's Disease and/or closure of individual fistulas as evidenced by no or minimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline for Fistulizing Crohn's; AND- The Specialist must confirm the Modified Harvey Bradshaw Index score shows a decrease from the New Patient's Baseline Score of greater than or equal to 3 points for patients with Moderately to Severely Active Crohn's and/or confirm closure of individual fistulas as evidenced by no or minimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline for Fistulizing Crohn's.
Maintenance Dosing for Existing Patients:
- The patient must be assessed by a Specialist at least 4 to 8 weeks after the day the last dose of infliximab was administered to the patient and prior to administration of the next dose to obtain: a Modified Harvey Bradshaw Index Score (Existing Patient's Baseline Score) for Moderately to Severely Active Crohn's and/or closure of individual fistulas as evidenced by no orminimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline for Fistulizing Crohn's; AND
- these measures must be provided to Alberta Blue Cross for assessment for continued coverage for maintenance dosing.
(For existing patients with Moderately to Severely Active Crohn's Disease with an incomplete response or for existing patients with Fistulizing Crohn's who respond then lose their response, the dose may be adjusted to 10 mg/kg by making an additional special authorization request to Alberta Blue Cross for the increased dose.)
Continued Coverage for Maintenance Dosing:
Continued coverage may be considered for one 5 mg/kg dose of infliximab per patient provided no more often than every 8 weeks for a period of 12 months, if the following criteria are met at the end of each 12 month period:
- The New Patient or the Existing Patient must be assessed by a Specialist at least 4 to 6 weeksafter the day the last dose of infliximab was administered to the patient and prior to the administration of the next dose to obtain a Modified Harvey Bradshaw Index Score for Moderately to Severely Active Crohn's and/or closure of individual fistulas as evidenced by no orminimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline for Fistulizing Crohn's; AND- For New Patients: The Specialist must confirm that the patient has maintained a greater than or equal to 3 point decrease from the New Patient's Baseline Score for Moderately to Severely Active Crohn's and/or closure of individual fistulas as evidenced by no or minimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline for Fistulizing Crohn's; OR- For Existing Patients: The Specialist must confirm that the patient has maintained the Existing Patient's Baseline Score and/or closure of individual fistulas as evidenced by no or minimal fistula drainage despite gentle finger compression of fistulas that were draining at baseline for Fistulizing Crohn's.
(For new and existing patients with Moderately to Severely Active Crohn's Disease with an incomplete response or for new and existing patients with Fistulizing Crohn's who respond then lose their response, the maintenance dose may be adjusted to 10 mg/kg by making an additional special authorization request to Alberta Blue Cross for the increased dose.)"
All requests (including renewal requests) for infliximab for Moderately to Severely Active Crohn'sThe DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
INFLIXIMAB
51 EFFECTIVE APRIL 1, 2012 Section 3 .
Disease and Fistulizing Crohn's Disease must be completed using the Adalimumab for Crohn's/Infliximab for Crohn's/Fistulizing Crohn's Disease Special Authorization Request Form (ABC 31200).
Ankylosing Spondylitis:
"Special authorization coverage may be provided for the reduction in the signs and symptoms and improvement in physical function of severely active Ankylosing Spondylitis, as defined by the Modified New York criteria for Ankylosing Spondylitis, in adult patients (18 years of age or older) who have active disease as demonstrated by:
- a BASDAI greater than or equal to 4 units, demonstrated on 2 occasions at least 8 weeks apartAND- a Spinal Pain VAS of greater than or equal to 4 cm (on a 0-10 cm scale), demonstrated on 2 occasions at least 8 weeks apart AND- who are refractory or intolerant to treatment with 2 or more NSAIDS each taken for a minimum of 4 weeks at maximum tolerated or recommended doses.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for three doses as follows: An initial dose of 5 mg/kg, followed by additional 5 mg/kg doses at 2 and 6 weeks after the first infusion.- Patients will be limited to receiving one dose of infliximab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond three doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after the initial three doses to determine response.2) The RA Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Reduction of the BASDAI score by at least 50% of the pre-treatment value or by 2 or more units, AND - Reduction of the Spinal Pain VAS by 2 cm or more.
Following this assessment, continued coverage may be approved for one 5 mg/kg dose of infliximab every 6 to 8 weeks for a period of 12 months. Ongoing coverage may be considered ifthe patient is re-assessed by an RA Specialist every 12 months and is confirmed to be continuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for infliximab for Ankylosing Spondylitis must be completed using the Adalimumab/Etanercept/Golimumab/Infliximab for Ankylosing Spondylitis Special Authorization Request Form (ABC 31195).
Psoriatic Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for reducing signs and symptoms and inhibiting the progression of structural damage of active
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
INFLIXIMAB
52 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
arthritis in adult patients (18 years of age or older) with moderate to severe polyarticular psoriaticarthritis (PsA) or pauciarticular PsA with involvement of knee or hip joint who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- An adequate trial of another disease modifying anti-rheumatic agent(s) (minimum 4 month trial).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for three doses as follows: An initial dose of 5 mg/kg, followed by additional 5 mg/kg doses at 2 and 6 weeks after the first infusion.- Patients will be limited to receiving one dose of infliximab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond three doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after the initial three doses to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for one 5 mg/kg dose every 8 weeks, for a period of 12 months. Ongoing coverage may be considered if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to therapy as indicated by:- Confirmation of maintenance of ACR20, or- Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewal requests. It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for infliximab for Psoriatic Arthritis must be completed The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
INFLIXIMAB
53 EFFECTIVE APRIL 1, 2012 Section 3 .
using the Adalimumab/Etanercept/Golimumab/Infliximab for Psoriatic Arthritis Special Authorization Request Form (ABC 30964).
Plaque Psoriasis:
"Special authorization coverage may be provided for the reduction in signs and symptoms of severe, debilitating plaque psoriasis in patients who:- Have a total PASI of 10 or more and a DLQI of more than 10, OR- Who have significant involvement of the face, palms of the hands, soles of the feet or genital region; AND- Who are refractory or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory, OR- Cyclosporine (6 weeks treatment); AND- Phototherapy (unless restricted by geographic location)
Patients who have a contraindication to either cyclosporine or methotrexate will be required to complete an adequate trial of the other pre-requisite medication prior to potential coverage beingconsidered.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be prescribed by a Specialist in Dermatology ("Dermatology Specialist").
- Initial coverage may be approved as follows: An initial dose of 5 mg/kg, followed by additional 5 mg/kg doses at 2 and 6 weeks after the first infusion.- Patients will be limited to receiving one dose of infliximab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond three doses, the patient must meet all of the following criteria:1) The patient must be assessed by a Dermatology Specialist after the initial three doses to determine response.2) The Dermatology Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Greater than or equal to 75% reduction in PASI score, or- Greater than or equal to 50% reduction in PASI score AND improvement of greater than or equal to 5 points in the DLQI.
Following this assessment, continued coverage may be considered for one 5 mg/kg dose of infliximab every 8 weeks for a period of 12 months. Ongoing coverage may be considered if the patient is re-assessed by a Dermatology Specialist every 12 months and is confirmed to be continuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for infliximab for Plaque Psoriasis must be completed using the Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
INFLIXIMAB
IPRATROPIUM BROMIDE
ITRACONAZOLE
LACOSAMIDE
100 MG / VIAL INJECTION
125 MCG / ML INHALATION UNIT DOSE SOLUTION
250 MCG / ML INHALATION UNIT DOSE SOLUTION
10 MG / ML ORAL SOLUTION
50 MG ORAL TABLET
100 MG ORAL TABLET
00002244016
0000223113500002097176
00002216221000022312440000223124500002097168
00002231347
00002357615
00002357623
REMICADE
PMS-IPRATROPIUMRATIO-IPRATROPIUM UDV
MYLAN-IPRATROPIUM STERINEBSPMS-IPRATROPIUM (1ML)PMS-IPRATROPIUM (2ML)RATIO-IPRATROPIUM UDV
SPORANOX
VIMPAT
VIMPAT
JAI
PMSRPH
MYPPMSPMSRPH
JAI
UCB
UCB
1010.5000
0.3775 0.3775
0.7550 0.7550 0.7550 0.7550
0.8417
2.4940
3.5690
54 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$
$$$$
$
$
$
Section 3 .
Authorization Request Form (ABC 31192).
"For use in patients with manual dexterity problems or visual limitations who are unable to prepare a dose of the drug using the multi-dose solution."
"For use in patients who are hypersensitive to preservatives contained in multi-dose solutions."
"Special authorization for both criteria may be granted for 24 months."
Information is required regarding the nature of the difficulties experienced by the patient in preparing a dose using the multi-dose preparation; or the nature of the patient's hypersensitivity to the preservatives contained in the multi-dose solution.
The following product(s) are eligible for auto-renewal.
"For the treatment of oral and/or esophageal candidiasis in immunocompromised patients who are intolerant to fluconazole, or who have failed fluconazole as evidenced by significant clinical deterioration due to the fungal infection during a course of therapy or no resolution after a full course of therapy."
"For adjunctive therapy in adult patients with refractory partial-onset seizures who meet all of thefollowing criteria:- Are currently receiving two or more antiepileptic medications, AND- Have failed or demonstrated intolerance to three other antiepileptic medications, AND- Therapy must be initiated by a Neurologist.
For the purpose of administering these criteria failure is defined as inability to achieve satisfactory seizure control.
Coverage may be granted for a maximum dose of 400 mg daily.
Special authorization may be granted for six months."
Each of these products is eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
LACOSAMIDE
LANREOTIDE ACETATE
LEUPROLIDE ACETATE
150 MG ORAL TABLET
200 MG ORAL TABLET
60 MG / SYR INJECTION SYRINGE
90 MG / SYR INJECTION SYRINGE
120 MG / SYR INJECTION SYRINGE
3.75 MG / VIAL INJECTION
5 MG / ML INJECTION
7.5 MG / VIAL INJECTION
11.25 MG / VIAL INJECTION
22.5 MG / VIAL INJECTION
00002357631
00002357658
00002283395
00002283409
00002283417
00000884502
00000727695
00000836273
00002239834
00002230248
VIMPAT
VIMPAT
SOMATULINE AUTOGEL (0.3 ML SYRINGE)
SOMATULINE AUTOGEL (0.3 ML SYRINGE)
SOMATULINE AUTOGEL (0.5 ML SYRINGE)
LUPRON DEPOT
LUPRON
LUPRON DEPOT
LUPRON DEPOT
LUPRON DEPOT
UCB
UCB
TCI
TCI
TCI
ABB
ABB
ABB
ABB
ABB
4.6440
5.7190
1184.6500
1580.2500
1978.0000
347.1800
67.6464
387.9700
1034.4100
1071.0000
55 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$
$
$
$
Section 3 .
"For the treatment of acromegaly when prescribed by or in consultation with a Specialist in Internal Medicine.
Special authorization may be granted for 12 months."
The following product(s) are eligible for auto-renewal.
"When prescribed for non-cancer, non-cosmetic or non-fertility indications.
Special authorization may be granted for 6 months."
Information is required regarding the patient's diagnosis/indication for use of this medication.
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
LEVOCARNITINE
LINEZOLID
330 MG ORAL TABLET
100 MG / ML ORAL SOLUTION
200 MG / ML INJECTION
600 MG ORAL TABLET
00002144328
00002144336
00002144344
00002243684
CARNITOR
CARNITOR
CARNITOR
ZYVOXAM
PPC
PPC
PPC
PFI
1.3078
0.3961
12.5220
77.5358
56 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
Section 3 .
"For the treatment of primary carnitine deficiency. Information is required regarding the ratio of acyl:free carnitine and total plasma carnitine levels."
"For the treatment of patients with an inborn error of metabolism that results in secondary carnitine deficiency. Information is required regarding the patient's diagnosis."
"Special authorization may be granted for 6 months."
In order to comply with the first criteria: Information is required regarding pre-treatment acyl:freecarnitine and total plasma carnitine levels.
The following product(s) are eligible for auto-renewal.
"For the treatment of:
1) Vancomycin-resistant enterococcus infections or
2) Methicillin-resistant Staphylococcus aureus (MRSA)/methicillin-resistant coagulase-negative Staphylococcus infections in patients who are unresponsive to or intolerant of vancomycin or
3) Susceptible organisms in patients severely intolerant or allergic to all other appropriate alternatives (e.g. beta-lactam antibiotics, clindamycin, trimethoprim/sulfamethoxazole and vancomycin) or to facilitate patient discharge from hospital where it otherwise would not be possible.
This product must be prescribed in consultation with a specialist in Infectious Diseases in all instances."
In order to comply with the above criteria, information is required regarding the type of infection and organisms involved. Information is also required regarding previous antibiotic therapy that has been utilized and the patient's response to therapy and the first line agents the organism is resistant to or why other first-line therapies cannot be used in this patient. The specialist in Infectious Diseases that recommended this drug is also required.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
MEGESTROL ACETATE
MEGESTROL ACETATE
40 MG / ML ORAL SUSPENSION
40 MG ORAL TABLET
160 MG ORAL TABLET
00002168979
00002195917
00002195925
MEGACE OS
MEGESTROL
MEGESTROL
BMS
AAP
AAP
1.6404
1.0828
4.5827
57 EFFECTIVE APRIL 1, 2012
$
$
$
Section 3 .
"For the treatment of non-cancer indications (e.g. cachexia in HIV/AIDS patients and cancer patients) in patients who cannot swallow tablets.
Special authorization may be granted for 6 months."
(Please note: The above megestrol acetate product is a benefit not requiring special authorization for individuals approved by Alberta Health and Wellness for Palliative CareDrug Coverage. Refer to the Palliative Care Drug Benefit Supplement for additional information on this coverage.)
The following product(s) are eligible for auto-renewal.
"For the treatment of non-cancer indications (e.g. cachexia in HIV/AIDS patients and cancer patients).
Special authorization may be granted for 6 months."
(Please note: The above megestrol acetate products are benefits not requiring special authorization for individuals approved by Alberta Health and Wellness for Palliative CareDrug Coverage. Refer to the Palliative Care Drug Benefit Supplement for additional information on this coverage.)
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
MEROPENEM
METHYLPREDNISOLONE ACETATE/ NEOMYCIN SULFATE/ ALUMINUM CHLORHYDROXIDE COMPLEX/ SULFUR
MODAFINIL
500 MG / VIAL INJECTION
1 G / VIAL INJECTION
2.5 MG / ML * 2.5 MG / ML * 100 MG / ML * 50 MG / ML TOPICAL LOTION
100 MG ORAL TABLET
00002218488
00002218496
00000195057
0000228539800002239665
MERREM
MERREM
NEO-MEDROL ACNE
MODAFINILALERTEC
AZC
AZC
PFI
AAPSHB
27.1545
54.3090
0.2797
0.9293 1.3174
58 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$$
Section 3 .
1) "As an alternative to imipenem for severe polymicrobial infections involving gram-negative organisms resistant to first-line agents in patients with documented seizure disorder/CNS abnormality or
2) As an alternative agent for severe polymicrobial infections involving gram-negative organismsresistant to first-line agents and to imipenem but susceptible to meropenem or
3) Therapy of meningitis due to gram-negative organisms producing inducible beta-lactamases (i.e. Enterobacter spp., Citrobacter freundii complex, Serratia spp., Morganella spp., Providenciaspp., Proteus vulgaris, Proteus penneri and some Hafnia spp.) or
4) For treatment of CNS infections due to gram-negative organisms that are resistant to third-generation cephalosporins but are susceptible to meropenem or
5) Therapy for infections involving multi-resistant Pseudomonas aeruginosa, where there is documented susceptibility to meropenem or
6) For use in other Health Canada approved indications, in consultation with a specialist in Infectious Diseases."
In order to comply with all of the above criteria, information is required regarding the type of infection and organisms involved. Also, where the criteria restrict coverage of the requested drug to non-first line therapy, information is required regarding previous first-line antibiotic therapy that has been utilized, the patient's response to therapy, and the first line agents the organism is resistant to or why other first-line therapies cannot be used in this patient. Also, where applicable, the specialist in Infectious Diseases that recommended this drug is required.
"For the treatment of severe acne as defined by scarring acne."
"For the treatment of acne rosacea and seborrheic dermatitis."
"Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"For the treatment of documented narcolepsy. This drug product must be prescribed by a specialist in Neurology or Psychiatry, or a sleep specialist affiliated with a recognized level 1 lab.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
MONTELUKAST SODIUM
10 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL CHEWABLE TABLET
000023746090000236822600002373947000023285930000235552300002238217
0000237761600002354985000023303930000235551500002238216
APO-MONTELUKASTMYLAN-MONTELUKASTPMS-MONTELUKAST FCSANDOZ MONTELUKASTTEVA-MONTELUKASTSINGULAIR
APO-MONTELUKASTPMS-MONTELUKASTSANDOZ MONTELUKASTTEVA-MONTELUKASTSINGULAIR
APXMYPPMSSDZTEVMFC
APXPMSSDZTEVMFC
1.0641 1.0641 1.0641 1.0641 1.0641 2.4238
0.7245 0.7245 0.7245 0.7245 1.6503
59 EFFECTIVE APRIL 1, 2012
$$$$$$
$$$$$
Section 3 .
(Refer to 48:10.24 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 6 to 18 years of age inclusive).
"For the prophylaxis and chronic treatment of asthma in patients over the age of 18 who meet one of the following criteria:a) when used as adjunctive therapy in patients who do not respond adequately to high doses of inhaled glucocorticosteroids and long-acting beta 2 agonists. Patients must be unable to use long-acting beta 2 agonists or have demonstrated persistent symptoms while on long-acting beta 2 agonists, orb) cannot operate inhaler devices."
"For the prophylaxis of exercise-induced bronchoconstriction in patients over the age of 18 where tachyphylaxis exists for long-acting beta 2 agonists."
"Special authorization for both criteria may be granted for 6 months."
In order to comply with the first criteria, information should indicate either a) current use of inhaled steroids and contraindications or poor response to long-acting beta 2 agonists (e.g. salmeterol or formoterol) or,b) the nature of the patient's difficulties with using inhaler devices.
In order to comply with the second criteria, information should include the nature of the patient's response to long-acting beta 2 agonists (e.g. salmeterol or formoterol).
All requests (including renewal requests) for montelukast must be completed using the Montelukast/Zafirlukast Special Authorization Request Form (ABC 31313).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
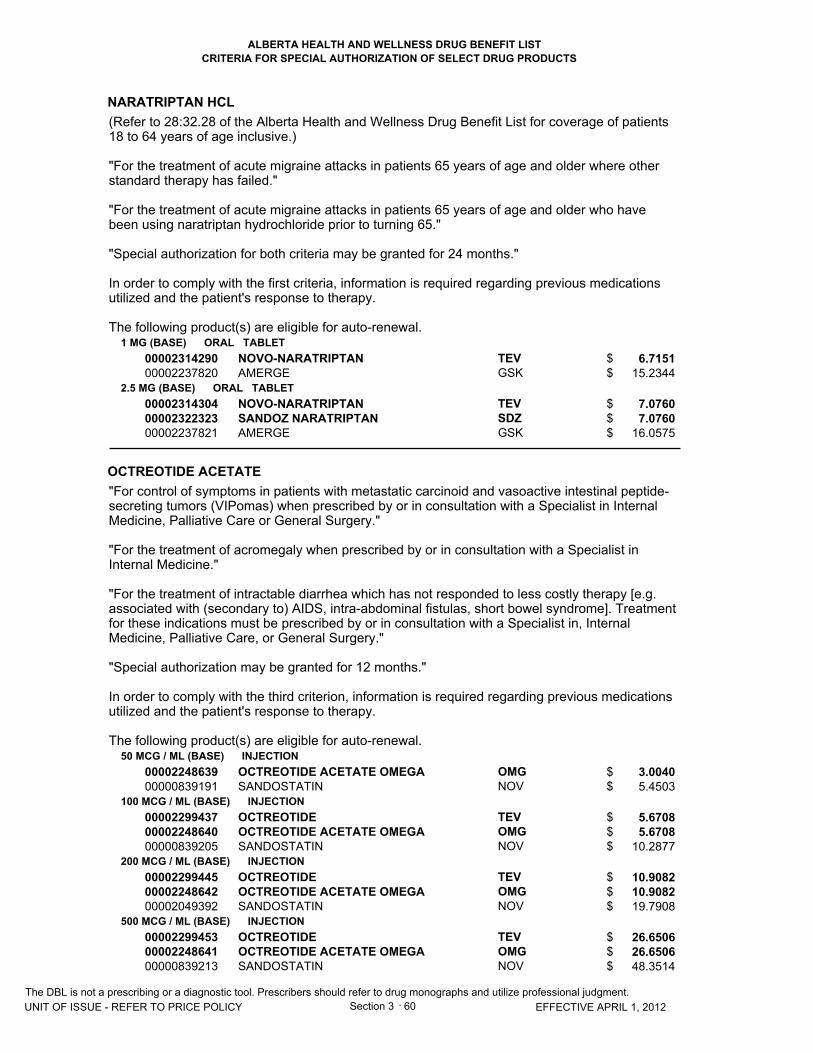
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
NARATRIPTAN HCL
OCTREOTIDE ACETATE
1 MG (BASE) ORAL TABLET
2.5 MG (BASE) ORAL TABLET
50 MCG / ML (BASE) INJECTION
100 MCG / ML (BASE) INJECTION
200 MCG / ML (BASE) INJECTION
500 MCG / ML (BASE) INJECTION
0000231429000002237820
000023143040000232232300002237821
0000224863900000839191
000022994370000224864000000839205
000022994450000224864200002049392
000022994530000224864100000839213
NOVO-NARATRIPTANAMERGE
NOVO-NARATRIPTANSANDOZ NARATRIPTANAMERGE
OCTREOTIDE ACETATE OMEGASANDOSTATIN
OCTREOTIDEOCTREOTIDE ACETATE OMEGASANDOSTATIN
OCTREOTIDEOCTREOTIDE ACETATE OMEGASANDOSTATIN
OCTREOTIDEOCTREOTIDE ACETATE OMEGASANDOSTATIN
TEVGSK
TEVSDZGSK
OMGNOV
TEVOMGNOV
TEVOMGNOV
TEVOMGNOV
6.7151 15.2344
7.0760 7.0760
16.0575
3.0040 5.4503
5.6708 5.6708
10.2877
10.9082 10.9082 19.7908
26.6506 26.6506 48.3514
60 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$$
$$
$$$
$$$
$$$
Section 3 .
(Refer to 28:32.28 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 18 to 64 years of age inclusive.)
"For the treatment of acute migraine attacks in patients 65 years of age and older where other standard therapy has failed."
"For the treatment of acute migraine attacks in patients 65 years of age and older who have been using naratriptan hydrochloride prior to turning 65."
"Special authorization for both criteria may be granted for 24 months."
In order to comply with the first criteria, information is required regarding previous medications utilized and the patient's response to therapy.
The following product(s) are eligible for auto-renewal.
"For control of symptoms in patients with metastatic carcinoid and vasoactive intestinal peptide-secreting tumors (VIPomas) when prescribed by or in consultation with a Specialist in Internal Medicine, Palliative Care or General Surgery."
"For the treatment of acromegaly when prescribed by or in consultation with a Specialist in Internal Medicine."
"For the treatment of intractable diarrhea which has not responded to less costly therapy [e.g. associated with (secondary to) AIDS, intra-abdominal fistulas, short bowel syndrome]. Treatmentfor these indications must be prescribed by or in consultation with a Specialist in, Internal Medicine, Palliative Care, or General Surgery."
"Special authorization may be granted for 12 months."
In order to comply with the third criterion, information is required regarding previous medications utilized and the patient's response to therapy.
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
OCTREOTIDE ACETATE10 MG / VIAL (BASE) INJECTION
20 MG / VIAL (BASE) INJECTION
30 MG / VIAL (BASE) INJECTION
00002239323
00002239324
00002239325
SANDOSTATIN LAR
SANDOSTATIN LAR
SANDOSTATIN LAR
NOV
NOV
NOV
1414.4205
1827.3818
2344.5105
61 EFFECTIVE APRIL 1, 2012
$
$
$
Section 3 .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
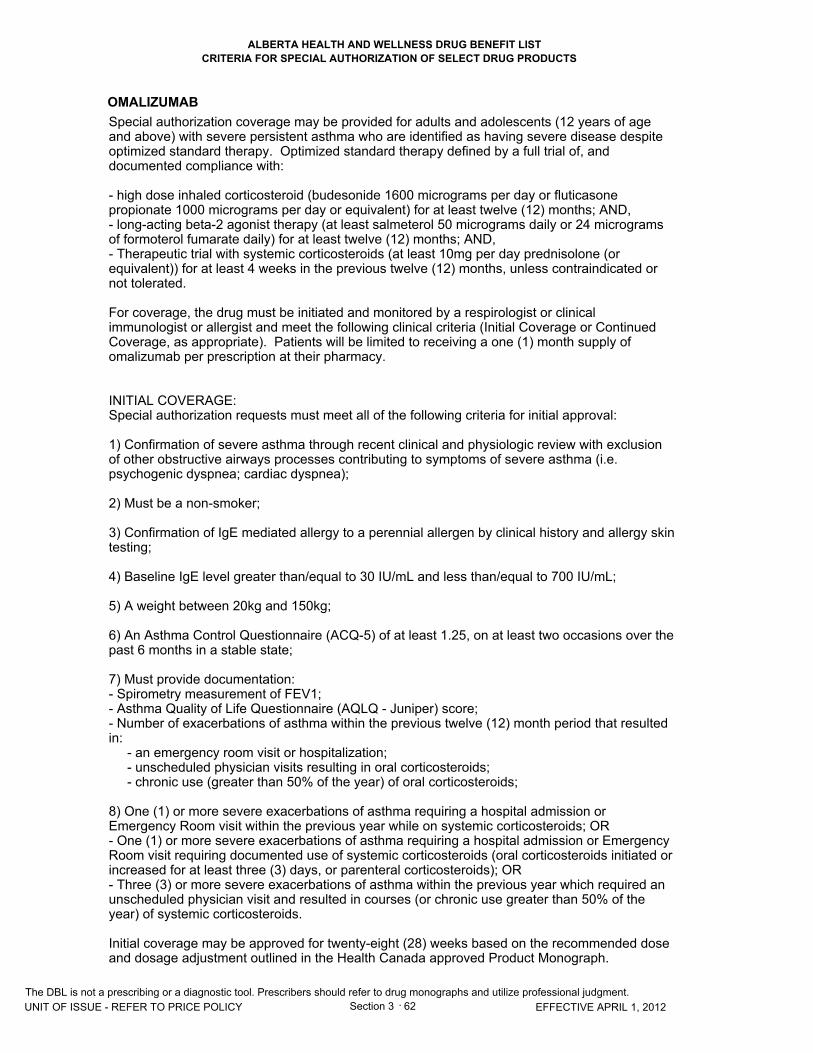
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
OMALIZUMAB
62 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Special authorization coverage may be provided for adults and adolescents (12 years of age and above) with severe persistent asthma who are identified as having severe disease despite optimized standard therapy. Optimized standard therapy defined by a full trial of, and documented compliance with:
- high dose inhaled corticosteroid (budesonide 1600 micrograms per day or fluticasone propionate 1000 micrograms per day or equivalent) for at least twelve (12) months; AND,- long-acting beta-2 agonist therapy (at least salmeterol 50 micrograms daily or 24 micrograms of formoterol fumarate daily) for at least twelve (12) months; AND,- Therapeutic trial with systemic corticosteroids (at least 10mg per day prednisolone (or equivalent)) for at least 4 weeks in the previous twelve (12) months, unless contraindicated or not tolerated. For coverage, the drug must be initiated and monitored by a respirologist or clinical immunologist or allergist and meet the following clinical criteria (Initial Coverage or Continued Coverage, as appropriate). Patients will be limited to receiving a one (1) month supply of omalizumab per prescription at their pharmacy.
INITIAL COVERAGE:Special authorization requests must meet all of the following criteria for initial approval:
1) Confirmation of severe asthma through recent clinical and physiologic review with exclusion of other obstructive airways processes contributing to symptoms of severe asthma (i.e. psychogenic dyspnea; cardiac dyspnea);
2) Must be a non-smoker;
3) Confirmation of IgE mediated allergy to a perennial allergen by clinical history and allergy skintesting;
4) Baseline IgE level greater than/equal to 30 IU/mL and less than/equal to 700 IU/mL;
5) A weight between 20kg and 150kg;
6) An Asthma Control Questionnaire (ACQ-5) of at least 1.25, on at least two occasions over thepast 6 months in a stable state;
7) Must provide documentation:- Spirometry measurement of FEV1;- Asthma Quality of Life Questionnaire (AQLQ - Juniper) score;- Number of exacerbations of asthma within the previous twelve (12) month period that resulted in: - an emergency room visit or hospitalization; - unscheduled physician visits resulting in oral corticosteroids; - chronic use (greater than 50% of the year) of oral corticosteroids;
8) One (1) or more severe exacerbations of asthma requiring a hospital admission or Emergency Room visit within the previous year while on systemic corticosteroids; OR - One (1) or more severe exacerbations of asthma requiring a hospital admission or Emergency Room visit requiring documented use of systemic corticosteroids (oral corticosteroids initiated or increased for at least three (3) days, or parenteral corticosteroids); OR- Three (3) or more severe exacerbations of asthma within the previous year which required an unscheduled physician visit and resulted in courses (or chronic use greater than 50% of the year) of systemic corticosteroids.
Initial coverage may be approved for twenty-eight (28) weeks based on the recommended dose and dosage adjustment outlined in the Health Canada approved Product Monograph.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
OMALIZUMAB
OXYBUTYNIN CHLORIDE
150 MG / VIAL INJECTION
10 MG ORAL EXTENDED-RELEASE TABLET
15 MG ORAL EXTENDED-RELEASE TABLET
00002260565
00002273578
00002273586
XOLAIR
UROMAX
UROMAX
NOV
PUR
PUR
645.0000
1.4679
1.5813
63 EFFECTIVE APRIL 1, 2012
$
$
$
Section 3 .
CONTINUED MAINTENANCE TREATMENT:A patient must be assessed for response to initial coverage of omalizumab with a minimum of twenty-four (24) weeks of therapy with omalizumab, and this assessment must be submitted to Alberta Blue Cross no later than four (4) weeks from the date of assessment.
The assessment must be done by the respirologist or clinical immunologist or allergist or such other clinicians as the Minister may designate who initiated therapy. If the following criteria are met, special authorization may be granted for a further twelve (12) month period. Continued coverage may be considered if the following criteria are met at the end of each additional twelve (12) month period:
1) Demonstrated that the patient has an Improvement in FEV1 greater than 12% (and for adults a minimum greater than 200 mL) from initiation of therapy; ORUnchanged FEV1 with a clinically meaningful Improvement in Asthma Quality of Life Questionnaire score from baseline (greater than/equal to 0.5 mean from baseline); AND - a decrease in the ACQ-5 of at least 0.5; OR - a ACQ-5 score of less than/equal to 1.
2) Patients must demonstrate at least a 25% reduction in the number of exacerbations, which required oral corticosteroids from the twelve (12) months prior to initiation of omalizumab that required systemic corticosteroids; ORFor patients that were on chronic (greater than 50% of the year) courses of oral corticosteroids use in the prior twelve (12) months to initiation of omalizumab, tapering of oral corticosteroid useby at least 25% from baseline.
3) A reduction in the number of exacerbations that have led to a hospital admission or emergency room visits, compared to the twelve (12) months prior to the commencement of omalizumab.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): IMMEDIATE RELEASE OXYBUTYNIN
"For patients who are intolerant of immediate release oxybutynin."
"Special authorization may be granted for 24 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PALIPERIDONE PALMITATE
PAPAVERINE HCL
PEGFILGRASTIM
50 MG / SYR (BASE) INJECTION SYRINGE
75 MG / SYR (BASE) INJECTION SYRINGE
100 MG / SYR (BASE) INJECTION SYRINGE
150 MG / SYR (BASE) INJECTION SYRINGE
32.5 MG / ML INJECTION
6 MG / SYR INJECTION SYRINGE
00002354217
00002354225
00002354233
00002354241
00000009881
00002249790
INVEGA SUSTENNA (0.5 ML SYR)
INVEGA SUSTENNA (0.75 ML SYR)
INVEGA SUSTENNA (1 ML SYR)
INVEGA SUSTENNA (1.5 ML SYR)
PAPAVERINE HCL
NEULASTA (0.6 ML SYRINGE)
JAI
JAI
JAI
JAI
SDZ
AMG
326.9075
490.3935
490.3935
653.8365
1.8450
2686.4250
64 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
Section 3 .
"For the management of the manifestations of schizophrenia in patients who demonstrate a pattern of significant non-compliance that compromises therapeutic success AND who meet at least two of three of the following criteria:- Experiences extra-pyramidal symptoms with either an oral or depot first generation antipsychotic agent that precludes the use of a first generation antipsychotic depot product; OR- Is refractory to trials of at least two other antipsychotic therapies (Note: one trial must include afirst generation antipsychotic agent); OR- Possesses clinical evidence of previous successful treatment with risperidone or paliperidone therapy.
Special Authorization may be granted for six months."
All requests (including renewal requests) for paliperidone prolonged release injection must becompleted using the Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form (ABC 31258).
The following product(s) are eligible for auto-renewal.
"For the relief of cerebral or peripheral ischemia with arterial spasm.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"To decrease the incidence of infection, as manifested by febrile neutropenia, in patients 18 years of age and older with non-myeloid malignancies receiving myelosuppressive antineoplastic drugs with curative intent. This drug product must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates)."
All requests for pegfilgrastim must be completed using the Filgrastim/Pegfilgrastim Special Authorization Request Form (ABC 31150).
Please note: Coverage cannot be considered for palliative patients.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PEGINTERFERON ALFA-2A
65 EFFECTIVE APRIL 1, 2012 Section 3 .
(Refer to 08:18.20 of the Alberta Health and Wellness Drug Benefit List for coverage of peginterferon alfa-2a for the treatment of Chronic Hepatitis B.)
Chronic Hepatitis C
"For the treatment of chronic hepatitis C in patients with evidence of active liver disease, who qualify for treatment with Pegasys RBV (peginterferon alfa-2a/ribavirin) but who are intolerant to ribavirin.
All Chronic Hepatitis C Patients Prior to Initiation of Therapy:
- To determine treatment duration and prognosis, HCV genotype testing is required for all patients.- At least three weeks before anticipated start date of therapy, please submit to Alberta Blue Cross a Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form (ABC30944), along with appropriate lab results. In order to meet the requirements of provincial privacy legislation, the patient's signature must be affixed to each completed form.
All Chronic Hepatitis C Patients (with the Exception of Advanced Fibrosis or Cirrhosis Patients):
Prior to initiation of therapy:
- Patients must have a baseline serum sample stored for future viral load testing in the event that the week 12 HCV RNA test is positive.
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Patients may receive an initial approval for 14 weeks of coverage.
At 12 weeks of treatment:
- HCV RNA testing is required for all patients at the 12th week of treatment.- If the HCV RNA test is positive, viral load testing is required on the previously stored baseline serum sample, and the 12 week serum sample, for evaluation of continued coverage.
Renewal approval period (for patients meeting criteria):
- Patients who respond to therapy, as measured by a reduction of viral load by at least 2 logs (100 fold) or HCV RNA not detected at 12 weeks, may be approved for an additional 34 weeks of coverage (total 48 weeks).
All Chronic Hepatitis C Patients with Advanced Fibrosis or Cirrhosis:
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Patients with advanced fibrosis or cirrhosis may receive approval for 48 weeks of coverage.
Consideration for therapy in chronic hepatitis C patients who have previously received therapy:
- Consideration for therapy in patients who have previously received therapy may be given for patients who meet at least one of the following criteria:
- Advanced fibrosis or cirrhosis.- Patients who have relapsed following non-pegylated interferon/ribavarin combination therapy."
In order to comply with this criterion: Confirmation of the diagnosis of chronic hepatitis C and The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PEGINTERFERON ALFA-2A
180 MCG / SYR INJECTION SYRINGE00002248077 PEGASYS (0.5 ML SYRINGE) HLR 425.5280
66 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
Section 3 .
presence of active liver disease is required. Information must include the patient's pre-treatment anti-HCV and serum HCV RNA (by PCR) status. Information is also required regarding whether liver enzymes (ALT/AST) are elevated, or the results of a liver biopsy. All requests for peginterferon alfa-2a for Chronic Hepatitis C must be completed using the Peginterferon Alfa-2a for Chronic Hepatitis C Special Authorization Request Form (ABC 30944). In order to meet the requirements of provincial privacy legislation, the patient's signature must be affixed to each completed form.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PEGINTERFERON ALFA-2A/ RIBAVIRIN
67 EFFECTIVE APRIL 1, 2012 Section 3 .
"For the treatment of chronic hepatitis C in patients with evidence of active liver disease.
Prior to initiation of Pegasys RBV therapy:
- To determine treatment duration and prognosis, HCV genotype testing is required for all patients.- At least three (3) weeks before anticipated start date of therapy, please submit a Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form (ABC 30932) along with appropriate lab results to Alberta Blue Cross.
All Patients (with the Exception of Post-Liver Transplant Patients and Advanced Fibrosis or Cirrhosis Patients):
Prior to initiation of Pegasys RBV therapy:
- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection must have a baseline serum sample stored for future viral load testing in the event that the week 12 HCV RNA test is positive.
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection, may receive an initial approval for 14 weeks of coverage.- Genotype 2 or 3 patients may receive initial and maximal approval for 24 weeks of coverage.These patients will not be eligible for continued approval.- Genotype 4, 5 and 6 patients may receive initial and maximal approval for 48 weeks of coverage. These patients will not be eligible for continued approval.
At 12 weeks of treatment:
- HCV RNA testing is required for all Genotype 1 patients and Genotype 2 or 3 patients with HIVco-infection at the 12th week of treatment.- If the HCV RNA test is positive, viral load testing is required on the previously stored baseline serum sample and the 12th week serum sample for evaluation of continued coverage.
Renewal approval period (for patients meeting criteria):
- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection who respond to therapy as measured by a negative HCV RNA status at 12 weeks, may be approved for an additional 34 weeks of coverage (i.e. total 48 weeks).- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection who achieve areduction in viral load by at least 2 logs (100 fold) but do not possess negative HCV RNA status at week 12 may be approved for an additional 14 weeks of coverage. Patients should be retested for HCV RNA status at 24 weeks:- Patients who respond to therapy, as measured by a negative HCV RNA status at 24 weeks, may be approved for an additional 20 weeks of coverage (i.e. total 48 weeks).- Those who fail to demonstrate negative HCV RNA status at 24 weeks will not be eligible for continued approval.
Post-Liver Transplant Patients:
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Genotype 1 and Genotype 2 or 3 patients may receive an initial approval for 26 weeks of coverage.- Genotype 4, 5 and 6 patients may receive initial and maximal approval for 48 weeks of coverage. These patients will not be eligible for continued approval.
At 24 weeks of treatment:The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PEGINTERFERON ALFA-2A/ RIBAVIRIN
180 MCG * 200 MG INJECTION SYRINGE/TABLET00002253429 PEGASYS RBV (KIT) HLR 425.5280
68 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
Section 3 .
- HCV RNA testing is required for all Genotype 1 and Genotype 2 or 3 patients at the 24th week of treatment.
Renewal approval period (for patients meeting criteria):
- Genotype 1 and Genotype 2 or 3 patients who respond to therapy as measured by a negative HCV RNA status at 24 weeks, may be approved for an additional 22 weeks of coverage (i.e. total 48 weeks).- Those who fail to demonstrate negative HCV RNA status at 24 weeks will not be eligible for continued approval.
Advanced Fibrosis or Cirrhosis Patients:
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Patients with advanced fibrosis or cirrhosis may receive approval for 48 weeks of coverage.
Consideration for therapy in ALL patients (including post-liver transplant patients) who have previously received therapy:
- Consideration for therapy in patients who have previously received therapy may be given for patients who meet at least one of the following criteria:- Advanced fibrosis or cirrhosis. - Patients who have relapsed following non-pegylated interferon/ribavarin combination therapy.- Patients who have failed to respond to or relapsed following interferon monotherapy."
Confirmation of the diagnosis of chronic hepatitis C and presence of active liver disease is required. Information must include the patient's pre-treatment anti-HCV and serum HCV RNA (by PCR) status. Information is also required regarding whether liver enzymes (ALT/AST) are elevated, or the results of liver biopsy. All requests for peginterferon alfa-2a/ribavirin must be completed using the Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form (ABC 30932). In order to meet the requirements of provincial privacy legislation, the patient's signature must be affixed to each completed form.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PEGINTERFERON ALFA-2B/ RIBAVIRIN
69 EFFECTIVE APRIL 1, 2012 Section 3 .
"For the treatment of chronic hepatitis C in patients with evidence of active liver disease.
Prior to initiation of Pegetron therapy:
- To determine treatment duration and prognosis, HCV genotype testing is required for all patients.- At least three (3) weeks before anticipated start date of therapy, please submit a Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form (ABC 30932) along with appropriate lab results to Alberta Blue Cross.
All Patients (with the Exception of Post-Liver Transplant Patients and Advanced Fibrosis or Cirrhosis Patients):
Prior to initiation of Pegetron therapy:
- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection must have a baseline serum sample stored for future viral load testing in the event that the week 12 HCV RNA test is positive.
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection, may receive an initial approval for 14 weeks of coverage.- Genotype 2 or 3 patients may receive initial and maximal approval for 24 weeks of coverage.These patients will not be eligible for continued approval.- Genotype 4, 5 and 6 patients may receive initial and maximal approval for 48 weeks of coverage. These patients will not be eligible for continued approval.
At 12 weeks of treatment:
- HCV RNA testing is required for all Genotype 1 patients and Genotype 2 or 3 patients with HIVco-infection at the 12th week of treatment.- If the HCV RNA test is positive, viral load testing is required on the previously stored baseline serum sample and the 12th week serum sample for evaluation of continued coverage.
Renewal approval period (for patients meeting criteria):
- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection who respond to therapy as measured by a negative HCV RNA status at 12 weeks, may be approved for an additional 34 weeks of coverage (i.e. total 48 weeks).- Genotype 1 patients and Genotype 2 or 3 patients with HIV co-infection who achieve a reduction in viral load by at least 2 logs (100 fold) but do not possess negative HCV RNA status at week 12 may be approved for an additional 14 weeks of coverage. Patients should be retested for HCV RNA status at 24 weeks:- Patients who respond to therapy, as measured by a negative HCV RNA status at 24 weeks, may be approved for an additional 20 weeks of coverage (i.e. total 48 weeks).- Those who fail to demonstrate negative HCV RNA status at 24 weeks will not be eligible for continued approval.
Post-Liver Transplant Patients:
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Genotype 1 and Genotype 2 or 3 patients may receive an initial approval for 26 weeks of coverage.- Genotype 4, 5 and 6 patients may receive initial and maximal approval for 48 weeks of coverage. These patients will not be eligible for continued approval.
At 24 weeks of treatment:The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PEGINTERFERON ALFA-2B/ RIBAVIRIN
50 MCG * 200 MG INJECTION VIAL/CAPSULE
150 MCG * 200 MG INJECTION VIAL/CAPSULE
80 MCG * 200 MG INJECTION SYRINGE/CAPSULE
100 MCG * 200 MG INJECTION SYRINGE/CAPSULE
120 MCG * 200 MG INJECTION SYRINGE/CAPSULE
150 MCG * 200 MG INJECTION SYRINGE/CAPSULE
00002246026
00002246030
00002254581
00002254603
00002254638
00002254646
PEGETRON (KIT)
PEGETRON (KIT)
PEGETRON REDIPEN (KIT)
PEGETRON REDIPEN (KIT)
PEGETRON REDIPEN (KIT)
PEGETRON REDIPEN (KIT)
MFC
MFC
MFC
MFC
MFC
MFC
752.2000
831.1800
752.2000
752.2000
831.1800
831.1800
70 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
Section 3 .
- HCV RNA testing is required for all Genotype 1 and Genotype 2 or 3 patients at the 24th week of treatment.
Renewal approval period (for patients meeting criteria):
- Genotype 1 and Genotype 2 or 3 patients who respond to therapy as measured by a negative HCV RNA status at 24 weeks, may be approved for an additional 22 weeks of coverage (i.e. total 48 weeks).- Those who fail to demonstrate negative HCV RNA status at 24 weeks will not be eligible for continued approval.
Advanced Fibrosis or Cirrhosis Patients:
Initial Alberta Blue Cross approval periods (for patients meeting criteria):
- Patients with advanced fibrosis or cirrhosis may receive approval for 48 weeks of coverage. Consideration for therapy in ALL patients (including post-liver transplant patients) who have previously received therapy:
- Consideration for therapy in patients who have previously received therapy may be given for patients who meet at least one of the following criteria:- Advanced fibrosis or cirrhosis. - Patients who have relapsed following non-pegylated interferon/ribavarin combination therapy.- Patients who have failed to respond to or relapsed following interferon monotherapy."
Confirmation of the diagnosis of chronic hepatitis C and presence of active liver disease is required. Information must include the patient's pre-treatment anti-HCV and serum HCV RNA (by PCR) status. Information is also required regarding whether liver enzymes (ALT/AST) are elevated, or the results of liver biopsy. All requests for peginterferon alfa-2b/ribavirin must be completed using the Peginterferon Alfa-2a+Ribavirin/Peginterferon Alfa-2b+Ribavirin Special Authorization Request Form (ABC 30932). In order to meet the requirements of provincial privacy legislation, the patient's signature must be affixed to each completed form.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PIOGLITAZONE HCL
15 MG (BASE) ORAL TABLET
30 MG (BASE) ORAL TABLET
45 MG (BASE) ORAL TABLET
000023034420000230294200002363232000023028610000232647700002298279000022749140000230766900002303124000023014230000229790600002242572
0000230345000002302950000023632400000230288800002365529000023264850000229828700002274922000023076770000233958700002303132000023014310000229791400002242573
0000230346900002302977000023632590000230289600002365537000023264930000229829500002274930000023077230000233959500002303140000023014580000229792200002242574
ACCEL PIOGLITAZONEAPO-PIOGLITAZONEAVA-PIOGLITAZONECO PIOGLITAZONEMINT-PIOGLITAZONEMYLAN-PIOGLITAZONENOVO-PIOGLITAZONEPHL-PIOGLITAZONEPMS-PIOGLITAZONERATIO-PIOGLITAZONESANDOZ PIOGLITAZONEACTOS
ACCEL PIOGLITAZONEAPO-PIOGLITAZONEAVA-PIOGLITAZONECO PIOGLITAZONEJAMP-PIOGLITAZONEMINT-PIOGLITAZONEMYLAN-PIOGLITAZONENOVO-PIOGLITAZONEPHL-PIOGLITAZONEPIOGLITAZONE HYDROCHLORIDEPMS-PIOGLITAZONERATIO-PIOGLITAZONESANDOZ PIOGLITAZONEACTOS
ACCEL PIOGLITAZONEAPO-PIOGLITAZONEAVA-PIOGLITAZONECO PIOGLITAZONEJAMP-PIOGLITAZONEMINT-PIOGLITAZONEMYLAN-PIOGLITAZONENOVO-PIOGLITAZONEPHL-PIOGLITAZONEPIOGLITAZONE HYDROCHLORIDEPMS-PIOGLITAZONERATIO-PIOGLITAZONESANDOZ PIOGLITAZONEACTOS
ACPAPXAVACOBMPIMYPTEVPHHPMSRPHSDZTAK
ACPAPXAVACOBJPCMPIMYPTEVPHHAHIPMSRPHSDZTAK
ACPAPXAVACOBJPCMPIMYPTEVPHHAHIPMSRPHSDZTAK
1.3201 1.3201 1.3201 1.3201 1.3201 1.3201 1.3201 1.3201 1.3201 1.3201 1.3201 2.4909
1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 1.8495 3.4897
2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 2.7808 5.2472
71 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$
$$$$$$$$$$$$$$
$$$$$$$$$$$$$$
Section 3 .
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): METFORMIN
"For the treatment of Type 2 diabetes in patients who have an inadequate response to a sufficient trial (i.e. a minimum of 6 months) of metformin or who are intolerant to metformin (e.g. dermatologic reactions) or for whom the product is contraindicated."
Special authorization may be granted for 24 months.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PIPERACILLIN SODIUM/ TAZOBACTAM SODIUM
QUINAGOLIDE
2 G / VIAL (BASE) * 250 MG / VIAL (BASE) INJECTION
3 G / VIAL (BASE) * 375 MG / VIAL (BASE) INJECTION
4 G / VIAL (BASE) * 500 MG / VIAL (BASE) INJECTION
0.075 MG ORAL TABLET
0.15 MG ORAL TABLET
0000230844400002299623
00002170817
0000230845200002299631
00002170795
0000230846000002299658
00002170809
00002223767
00002223775
PIPERACILLIN AND TAZOBACTAMPIPERACILLIN SODIUM/TAZOBACTAM SODIUMTAZOCIN
PIPERACILLIN AND TAZOBACTAMPIPERACILLIN SODIUM/TAZOBACTAM SODIUMTAZOCIN
PIPERACILLIN AND TAZOBACTAMPIPERACILLIN SODIUM/TAZOBACTAM SODIUMTAZOCIN
NORPROLAC
NORPROLAC
APXSDZ
WAY
APXSDZ
WAY
APXSDZ
WAY
FEI
FEI
9.6120 9.6120
12.8162
14.4180 14.4180
19.2242
19.2250 19.2250
25.6334
1.1718
1.7523
72 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$$
$
$$
$
$
$
Section 3 .
For the treatment of:
1) "Second-line therapy of intra-abdominal sepsis where there are serious adverse events due to first-line therapy or documented failure of first-line therapy (e.g. ampicillin + gentamicin + metronidazole), as defined by clinical deterioration after 72 h of antibiotic therapy or lack of improvement after completion of antibiotic therapy or 2) Second-line therapy of severe polymicrobial skin and skin structure infections (e.g. limb threatening diabetic foot) or
3) Therapy of severe ventilator-associated pneumonia where Pseudomonas and Staphylococcus aureus coverage is needed, or
4) Therapy for infections involving multi-resistant Pseudomonas aeruginosa from pulmonary secretions in cystic fibrosis patients, lung transplant patients or patients with bronchiectasis , where there is documented susceptibility to piperacillin/tazobactam sodium, or
5) For use in other Health Canada approved indications, in consultation with a specialist in Infectious Diseases."
In order to comply with all of the above criteria, information is required regarding the type of infection and organisms involved. Also, where the criteria restrict coverage of the requested drug to non-first line therapy, information is required regarding previous first-line antibiotic therapy that has been utilized, the patient's response to therapy, and the first line agents the organism is resistant to or why other first-line therapies cannot be used in this patient. Also, where applicable, the specialist in Infectious Diseases that recommended this drug is required.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): BROMOCRIPTINE
"For the treatment of hyperprolactinemia in patients who are intolerant to or who have failed bromocriptine. Special authorization may be granted for 24 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
RALOXIFENE HCL
RIFABUTIN
RILUZOLE
60 MG ORAL TABLET
150 MG ORAL CAPSULE
50 MG ORAL TABLET
00002279215000023122980000235892100002239028
00002063786
00002242763
APO-RALOXIFENENOVO-RALOXIFENEPMS-RALOXIFENEEVISTA
MYCOBUTIN
RILUTEK
APXTEVPMSLIL
PFI
SAV
1.1038 1.1038 1.1038 2.0215
4.2808
10.5536
73 EFFECTIVE APRIL 1, 2012
$$$$
$
$
Section 3 .
"For the treatment of osteoporosis in patients who have documented hip, vertebral or otherfractures. Special authorization for this criteria may be granted for 6 months."
"For the treatment of osteoporosis in patients with documented evidence of intolerance or lack ofresponse to etidronate (i.e. demonstrated as a > 2% loss in bone mineral density in one year).Special authorization for this criteria may be granted for 6 months."
"Coverage cannot be provided for two or more osteoporosis medications (alendronate,calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intendedfor use as combination therapy."
"Requests for other osteoporosis medications covered via special authorization will not be considered until 6 months after the last dose of denosumab."
All requests for raloxifene HCl must be completed using the Alendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon for Osteoporosis Special Authorization Request Form (ABC 31086).
The following product(s) are eligible for auto-renewal.
"For the prevention of disseminated Mycobacterium avium complex disease in patients with advanced HIV infection or other immunocompromised conditions.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"For use in patients who have probable or definite diagnosis of amyotrophic lateral sclerosis (ALS) as defined by World Federation of Neurology (WFN) criteria who have a vital capacity of >60% predicted and do not have a tracheostomy for invasive ventilation. This drug must be prescribed by a Specialist in Neurology."
"Patients who previously received Rilutek and were not eligible for the Phase IV study can also be considered for coverage if they meet the special authorization criteria."
"Coverage cannot be renewed once the patient has a tracheostomy for the purpose of invasive ventilation."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RISEDRONATE SODIUM
5 MG ORAL TABLET
30 MG ORAL TABLET
35 MG ORAL TABLET
0000229837600002242518
0000229838400002239146
000023536870000236481600002357984000022983920000230220900002319861000023702550000232729500002246896
NOVO-RISEDRONATEACTONEL
NOVO-RISEDRONATEACTONEL
APO-RISEDRONATEAVA-RISEDRONATEMYLAN-RISEDRONATENOVO-RISEDRONATEPMS-RISEDRONATERATIO-RISEDRONATERISEDRONATESANDOZ RISEDRONATEACTONEL
TEVWCC
TEVWCC
APXAVAMYPTEVPMSRPHSNSSDZWCC
0.8998 2.0559
5.8340 13.3397
4.8169 4.8169 4.8169 4.8169 4.8169 4.8169 4.8169 4.8169
11.2069
74 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$
$$$$$$$$$
Section 3 .
"For the treatment of osteoporosis in patients who have documented hip, vertebral or otherfractures. Special authorization may be granted for 6 months."
"For the treatment of osteoporosis in patients with documented evidence of intolerance or lack ofresponse to etidronate (i.e. demonstrated as a > 2% loss in bone mineral density in one year).Special authorization for this criteria may be granted for 6 months."
"Coverage cannot be provided for two or more osteoporosis medications (alendronate,calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intendedfor use as combination therapy."
"Requests for other osteoporosis medications covered via special authorization will not be considered until 6 months after the last dose of denosumab."
"For the treatment of Paget's disease. Special Authorization for this criteria may be granted to amaximum of 2 months. Renewal requests may be considered following an observation period ofat least 2 months."
"Coverage cannot be provided for two or more medications used in the treatment of Paget'sdisease when these medications are intended for use in combination or when therapy with twoor more medications overlap."
All requests for risedronate sodium for Osteoporosis must be completed using theAlendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon for Osteoporosis SpecialAuthorization Request Form (ABC 31086).
The following product(s) are eligible for auto-renewal for the treatment of osteoporosis.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
RISPERIDONE
25 MG / VIAL INJECTION
37.5 MG / VIAL INJECTION
50 MG / VIAL INJECTION
00002255707
00002255723
00002255758
RISPERDAL CONSTA
RISPERDAL CONSTA
RISPERDAL CONSTA
JAI
JAI
JAI
173.1718
259.7415
346.3220
75 EFFECTIVE APRIL 1, 2012
$
$
$
Section 3 .
"For the management of the manifestations of schizophrenia and related psychotic disorders in patients who demonstrate a pattern of significant non-compliance that compromises therapeutic success AND who meet at least two of three of the following criteria:- Experiences extra-pyramidal symptoms with either an oral or depot first generation antipsychotic agent that precludes the use of a first generation antipsychotic depot product; OR- Is refractory to trials of at least two other antipsychotic therapies (Note: one trial must include a first generation antipsychotic agent); OR- Possesses clinical evidence of previous successful treatment with risperidone or paliperidone therapy.
Special Authorization may be granted for six months."
All requests (including renewal requests) for risperidone prolonged release injection must be completed using the Paliperidone/Risperidone Prolonged Release Injection Special Authorization Request Form (ABC 31258).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RITUXIMAB
10 MG / ML INJECTION00002241927 RITUXAN HLR 48.7083
76 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
Section 3 .
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) who are refractory or intolerant to: - Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4 month trial). [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily); AND- One anti-tumor necrosis factor (anti-TNF) therapy (e.g., etanercept, infliximab or adalimumab) (minimum 12 week trial).
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications totreatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for a dose of 1000 mg of rituximab administered at 0 and 2 weeks (total of 2 - 1000 mg doses).- Patients will be limited to receiving one dose of rituximab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception of anakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except under exceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For coverage for an additional two-dose course of therapy, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after each course of therapy, between 16 and 24 weeks after receiving the initial dose of each course of therapy, to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- An improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place] following the initial course of rituximab; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places] following the initial course of rituximab.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above, AND3) The patient must have experienced a subsequent loss of effect as defined by a worsening greater than or equal to 0.6 in the DAS28 score AND possess a DAS28 score of greater than or equal to 3.2.
Subsequent courses of therapy cannot be considered prior to 24 weeks elapsing from the initial dose of the previous course of therapy."
All requests (including renewal requests) for rituximab for Rheumatoid Arthritis must be completed using the Rituximab for Rheumatoid Arthritis Special Authorization Request Form (ABC 31205).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
RIVASTIGMINE HYDROGEN TARTRATE
1.5 MG (BASE) ORAL CAPSULE
3 MG (BASE) ORAL CAPSULE
4.5 MG (BASE) ORAL CAPSULE
6 MG (BASE) ORAL CAPSULE
2 MG / ML (BASE) ORAL SOLUTION
00002336715000023328090000230598400002306034000023112830000232456300002242115
00002336723000023328170000230599200002306042000023112910000232457100002242116
00002336731000023328250000230601800002306050000023113050000232459800002242117
00002336758000023328330000230602600002306069000023113130000232460100002242118
00002245240
APO-RIVASTIGMINEMYLAN-RIVASTIGMINENOVO-RIVASTIGMINEPMS-RIVASTIGMINERATIO-RIVASTIGMINESANDOZ RIVASTIGMINEEXELON
APO-RIVASTIGMINEMYLAN-RIVASTIGMINENOVO-RIVASTIGMINEPMS-RIVASTIGMINERATIO-RIVASTIGMINESANDOZ RIVASTIGMINEEXELON
APO-RIVASTIGMINEMYLAN-RIVASTIGMINENOVO-RIVASTIGMINEPMS-RIVASTIGMINERATIO-RIVASTIGMINESANDOZ RIVASTIGMINEEXELON
APO-RIVASTIGMINEMYLAN-RIVASTIGMINENOVO-RIVASTIGMINEPMS-RIVASTIGMINERATIO-RIVASTIGMINESANDOZ RIVASTIGMINEEXELON
EXELON
APXMYPTEVPMSRPHSDZNOV
APXMYPTEVPMSRPHSDZNOV
APXMYPTEVPMSRPHSDZNOV
APXMYPTEVPMSRPHSDZNOV
NOV
1.2605 1.2605 1.2605 1.2605 1.2605 1.2605 2.8013
1.2605 1.2605 1.2605 1.2605 1.2605 1.2605 2.8013
1.2605 1.2605 1.2605 1.2605 1.2605 1.2605 2.8013
1.2605 1.2605 1.2605 1.2605 1.2605 1.2605 2.8013
1.4728
77 EFFECTIVE APRIL 1, 2012
$$$$$$$
$$$$$$$
$$$$$$$
$$$$$$$
$
Section 3 .
"For the treatment of Alzheimer's disease in patients with an MMSE (Mini Mental State Exam) score between 10-26 and/or an InterRAI-Cognitive Performance Scale score between 1-4.
Coverage cannot be provided for two or more medications used in the treatment of Alzheimer's disease (donepezil, galantamine, rivastigmine) when these medications are intended for use in combination.
Special authorization coverage may be granted for a maximum of 24 months per request.
For each request, an updated MMSE score or InterRAI-Cognitive Performance Scale score and the date on which the exam was administered must be provided.
Renewal requests may be considered for patients where the updated MMSE score is 10 or higher or the InterRAI-Cognitive Performance Scale is 4 or lower while on this drug."
All requests (including renewal requests) for rivastigmine hydrogen tartrate must be completed using the Donepezil/Galantamine/Rivastigmine Special Authorization Request Form (ABC 30776).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RIZATRIPTAN BENZOATE
ROSIGLITAZONE MALEATE
10 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL DISINTEGRATING TABLET
10 MG (BASE) ORAL DISINTEGRATING TABLET
2 MG (BASE) ORAL TABLET
4 MG (BASE) ORAL TABLET
8 MG (BASE) ORAL TABLET
00002240521
00002240518
00002240519
00002241112
00002241113
00002241114
MAXALT
MAXALT RPD
MAXALT RPD
AVANDIA
AVANDIA
AVANDIA
MFC
MFC
MFC
GSK
GSK
GSK
15.2201
15.2201
15.2201
1.4787
2.3203
3.3180
78 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
Section 3 .
(Refer to 28:32.28 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 18 to 64 years of age inclusive.)
"For the treatment of acute migraine attacks in patients 65 years of age and older where other standard therapy has failed."
"For the treatment of acute migraine attacks in patients 65 years of age and older who have been using rizatriptan benzoate prior to turning 65."
"Special authorization for both criteria may be granted for 24 months."
In order to comply with the first criteria, information is required regarding previous medications utilized and the patient's response to therapy.
The following product(s) are eligible for auto-renewal.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): METFORMIN
"For the treatment of Type 2 diabetes in patients who have an inadequate response to a sufficient trial (i.e. a minimum of 6 months) of metformin or who are intolerant to metformin (e.g. dermatologic reactions) or for whom the product is contraindicated."
Special authorization may be granted for 24 months.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ROSIGLITAZONE MALEATE/ METFORMIN HCL
SAXAGLIPTIN HCL
1 MG (BASE) * 500 MG ORAL TABLET
2 MG (BASE) * 500 MG ORAL TABLET
2 MG (BASE) * 1,000 MG ORAL TABLET
4 MG (BASE) * 500 MG ORAL TABLET
4 MG (BASE) * 1,000 MG ORAL TABLET
5 MG (BASE) ORAL TABLET
00002247085
00002247086
00002248440
00002247087
00002248441
00002333554
AVANDAMET
AVANDAMET
AVANDAMET
AVANDAMET
AVANDAMET
ONGLYZA
GSK
GSK
GSK
GSK
GSK
BMS
0.6903
1.2482
1.3633
1.7142
1.8637
2.7560
79 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
Section 3 .
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): METFORMIN
"For the treatment of Type 2 diabetes in patients who have an inadequate response to a sufficient trial (i.e. a minimum of 6 months) of metformin."
Special authorization may be granted for 24 months.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): METFORMINSECOND-LINE DRUG PRODUCT(S): SULFONYLUREASAND WHERE INSULIN IS NOT AN OPTION
As add-on therapy for the treatment of Type 2 diabetes in patients with intolerance to and/or inadequate glycemic control on:- a sufficient trial (i.e. a minimum of 6 months) of metformin, AND- a sulfonylurea, AND- for whom insulin is not an option.
Or, for whom these products are contraindicated.
Special authorization may be granted for 24 months.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SOLIFENACIN SUCCINATE
SOMATROPIN
SOMATROPIN R-DNA ORIGIN
5 MG ORAL TABLET
10 MG ORAL TABLET
6 MG / VIAL INJECTION
12 MG / VIAL INJECTION
3.3 MG / VIAL INJECTION
5 MG / VIAL INJECTION
5.83 MG / ML INJECTION
6.7 MG / ML INJECTION
8 MG / ML INJECTION
8.8 MG / VIAL INJECTION
00002277263
00002277271
00002243077
00002243078
0000232506300002215136
00002237971
00002350122
00002325071
0000235013000002350149
00002272083
VESICARE
VESICARE
HUMATROPE
HUMATROPE
OMNITROPESAIZEN
SAIZEN
SAIZEN
OMNITROPE
SAIZEN (1.5 ML)SAIZEN (2.5 ML)
SAIZEN
ASP
ASP
LIL
LIL
SDZSRO
SRO
SRO
SDZ
SROSRO
SRO
1.6125
1.6125
301.0215
602.0430
111.6567 155.7675
233.8340
280.5750
223.3133
374.1000 374.1000
374.1322
80 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$$
$
$
$
$$
$
Section 3 .
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): OXYBUTYNIN
"For patients who are intolerant to oxybutynin.
Special authorization may be granted for 24 months."
"For replacement of endogenous growth hormone in adults with severe growth hormone deficiency. Information is required regarding the results of a diagnostic insulin tolerance test. Growth hormone values less than 3 mcg/litre during hypoglycemia are indicative of severe growth hormone deficiency.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"For replacement of endogenous growth hormone in adults with severe growth hormone deficiency. Information is required regarding the results of a diagnostic insulin tolerance test. Growth hormone values less than 3 mcg/litre during hypoglycemia are indicative of severe growth hormone deficiency.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SULFUR/ SULFACETAMIDE SODIUM
SUMATRIPTAN HEMISULFATE
5 % * 10 % TOPICAL LOTION
5 MG / DOSE (BASE) NASAL UNIT DOSE SPRAY
20 MG / DOSE (BASE) NASAL UNIT DOSE SPRAY
00002220407
00002230418
00002230420
SULFACET-R
IMITREX
IMITREX
SAV
GSK
GSK
1.0350
15.4648
15.9148
81 EFFECTIVE APRIL 1, 2012
$
$
$
Section 3 .
"For the treatment seborrheic dermatitis and bacterial folliculitis.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
(Refer to 28:32.28 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 18 to 64 years of age inclusive.)
"For the treatment of acute migraine attacks in patients 65 years of age and older where other standard therapy has failed."
"For the treatment of acute migraine attacks in patients 65 years of age and older who have been using sumatriptan prior to turning 65."
"Special authorization for both criteria may be granted for 24 months."
In order to comply with the first criteria, information is required regarding previous medications utilized and the patient's response to therapy.
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SUMATRIPTAN SUCCINATE
50 MG (BASE) ORAL TABLET
100 MG (BASE) ORAL TABLET
6 MG / SYR (BASE) INJECTION SYRINGE
000023662580000226891400002286823000022865210000226838800002257890000022564360000226302500002212153
00002366266000022689220000223936700002286831000022865480000226839600002257904000022564440000226303300002212161
0000236169800002212188
AVA-SUMATRIPTANMYLAN-SUMATRIPTANNOVO-SUMATRIPTAN DFSUMATRIPTANAPO-SUMATRIPTANCO SUMATRIPTANPMS-SUMATRIPTANSANDOZ SUMATRIPTANIMITREX DF
AVA-SUMATRIPTANMYLAN-SUMATRIPTANNOVO-SUMATRIPTANNOVO-SUMATRIPTAN DFSUMATRIPTANAPO-SUMATRIPTANCO SUMATRIPTANPMS-SUMATRIPTANSANDOZ SUMATRIPTANIMITREX DF
SUMATRIPTAN SUN (0.5 ML)IMITREX (0.5 ML)
AVAMYPTEVSNSAPXCOBPMSSDZGSK
AVAMYPTEVTEVSNSAPXCOBPMSSDZGSK
SPGGSK
8.9350 8.9350 8.9350 8.9350 8.9364 8.9364 8.9364 8.9364
16.2935
9.8433 9.8433 9.8433 9.8433 9.8433 9.8442 9.8442 9.8442 9.8442
17.9491
30.8600 47.3968
82 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$
$$$$$$$$$$
$$
Section 3 .
(Refer to 28:32.28 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 18 to 64 years of age inclusive.)
"For the treatment of acute migraine attacks in patients 65 years of age and older where other standard therapy has failed."
"For the treatment of acute migraine attacks in patients 65 years of age and older who have been using sumatriptan prior to turning 65."
"Special authorization for both criteria may be granted for 24 months."
In order to comply with the first criteria, information is required regarding previous medications utilized and the patient's response to therapy.
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
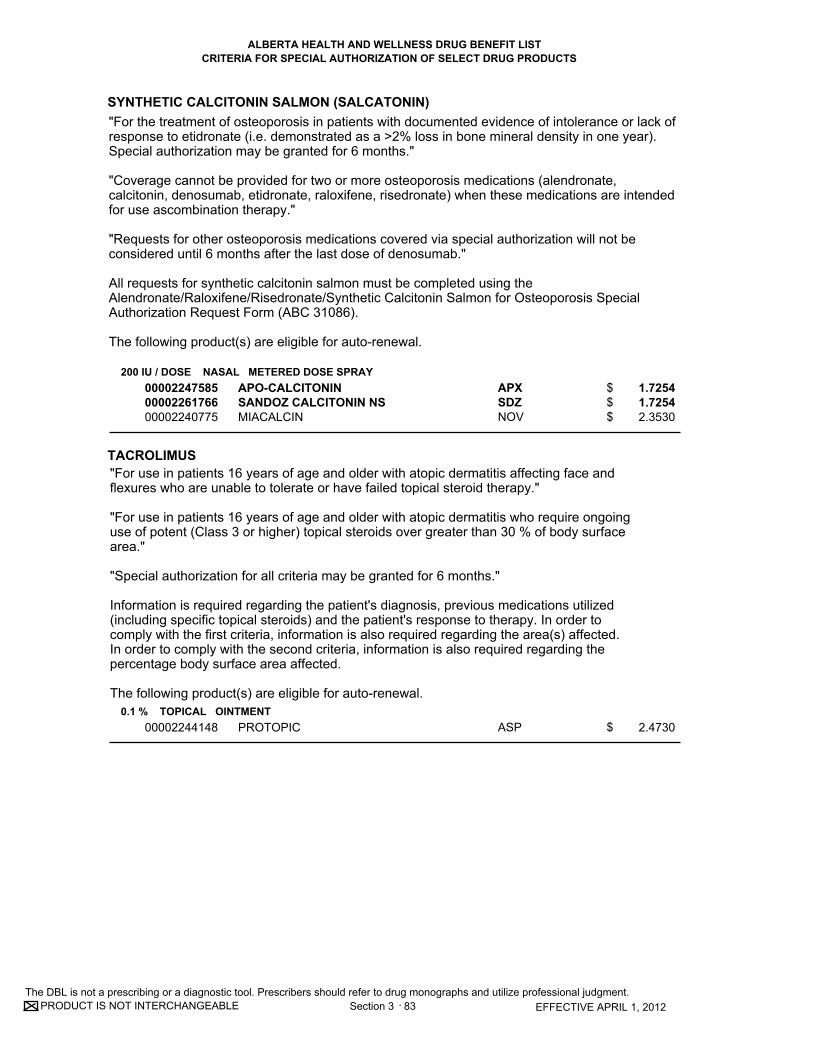
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SYNTHETIC CALCITONIN SALMON (SALCATONIN)
TACROLIMUS
200 IU / DOSE NASAL METERED DOSE SPRAY
0.1 % TOPICAL OINTMENT
000022475850000226176600002240775
00002244148
APO-CALCITONINSANDOZ CALCITONIN NSMIACALCIN
PROTOPIC
APXSDZNOV
ASP
1.7254 1.7254 2.3530
2.4730
83 EFFECTIVE APRIL 1, 2012
$$$
$
Section 3 .
"For use in patients 16 years of age and older with atopic dermatitis affecting face and flexures who are unable to tolerate or have failed topical steroid therapy."
"For use in patients 16 years of age and older with atopic dermatitis who require ongoinguse of potent (Class 3 or higher) topical steroids over greater than 30 % of body surface area."
"Special authorization for all criteria may be granted for 6 months."
Information is required regarding the patient's diagnosis, previous medications utilized (including specific topical steroids) and the patient's response to therapy. In order to comply with the first criteria, information is also required regarding the area(s) affected. In order to comply with the second criteria, information is also required regarding the percentage body surface area affected.
The following product(s) are eligible for auto-renewal.
"For the treatment of osteoporosis in patients with documented evidence of intolerance or lack ofresponse to etidronate (i.e. demonstrated as a >2% loss in bone mineral density in one year).Special authorization may be granted for 6 months."
"Coverage cannot be provided for two or more osteoporosis medications (alendronate,calcitonin, denosumab, etidronate, raloxifene, risedronate) when these medications are intendedfor use ascombination therapy."
"Requests for other osteoporosis medications covered via special authorization will not be considered until 6 months after the last dose of denosumab."
All requests for synthetic calcitonin salmon must be completed using theAlendronate/Raloxifene/Risedronate/Synthetic Calcitonin Salmon for Osteoporosis Special Authorization Request Form (ABC 31086).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
TACROLIMUS
TESTOSTERONE
TESTOSTERONE UNDECANOATE
0.03 % TOPICAL OINTMENT
12.2 MG TRANSDERMAL PATCH
24.3 MG TRANSDERMAL PATCH
40 MG ORAL CAPSULE
00002244149
00002239653
00002245972
00000782327
PROTOPIC
ANDRODERM (2.5 MG/DAY)
ANDRODERM (5 MG/DAY)
ANDRIOL
ASP
PAL
PAL
MFC
2.3110
1.9959
3.9919
0.9400
84 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
Section 3 .
"For use in patients 2 to 15 years of age inclusive with atopic dermatitis who are unable to tolerate or have failed topical steroid therapy."
"For use in patients 2 to 15 years of age inclusive with atopic dermatitis who require ongoing use of potent (Class 3 or higher) topical steroids."
"For use in patients 16 years of age and older with atopic dermatitis affecting face and flexures who are unable to tolerate or have failed topical steroid therapy."
"For use in patients 16 years of age and older with atopic dermatitis who require ongoinguse of potent (Class 3 or higher) topical steroids over greater than 30 % of body surface area."
"Special authorization for all criteria may be granted for 6 months."
Information is required regarding the patient's diagnosis, previous medications utilized (including specific topical steroids) and the patient's response to therapy. In order to comply with the third criteria, information is also required regarding the area(s) affected. In order to comply with the fourth criteria, information is also required regarding the percentage body surface area affected.
The following product(s) are eligible for auto-renewal.
"For use in males for the treatment of congenital and acquired primary and secondary hypogonadism."
"Coverage cannot be considered when used for the treatment of androgen decline in the aging male (ADAM)."
"Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
"For use in males for the treatment of congenital and acquired primary and secondary hypogonadism."
"Coverage cannot be considered when used for the treatment of androgen decline in the aging male (ADAM)." "Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TETRABENAZINE
TIZANIDINE HCL
25 MG ORAL TABLET
4 MG (BASE) ORAL TABLET
00002199270
000022598930000227205900002239170
NITOMAN
APO-TIZANIDINEMYLAN-TIZANIDINEZANAFLEX
VCL
APXMYPPAL
6.9360
0.4129 0.4129 0.7746
85 EFFECTIVE APRIL 1, 2012
$
$$$
Section 3 .
"For the treatment of hyperkinetic movement disorders when prescribed by specialists in Neurology, Psychiatry, or Geriatric Medicine.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): DIAZEPAM OR BACLOFEN
"For the treatment of spasticity in patients with documented evidence of intolerance or lack of response to diazepam or baclofen. Special authorization is granted for 24 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
TOCILIZUMAB
86 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY Section 3 .
Rheumatoid Arthritis:
"Special authorization coverage may be provided for use in combination with methotrexate for the reduction in signs and symptoms of severely active Rheumatoid Arthritis (RA) in adult patients (18 years of age or older) who are refractory or intolerant to:
- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who do not exhibit a clinicalresponse to PO methotrexate or experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory; AND- Methotrexate with other disease modifying anti-rheumatic agent(s) (minimum 4-month trial). [e.g., methotrexate with hydroxychloroquine or methotrexate with sulfasalazine]; AND- Leflunomide (minimum 10 week trial at 20 mg daily); AND- At least one anti-tumor necrosis factor (anti-TNF) therapy (e.g., etanercept, infliximab oradalimumab) (minimum 12 week trial); AND- Abatacept or rituximab (minimum 12 - 16 week trial).
Special authorization coverage of this agent may be provided for use as monotherapy in adult patients for whom methotrexate is contraindicated and/or for those patients who have experienced serious adverse effects.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be initiated by a Specialist in Rheumatology ("RA Specialist").
- Initial coverage may be approved for one dose of 4 mg/kg or 8 mg/kg (up to a maximum of 800mg per dose) of tocilizumab administered at 0, 4, 8, 12 and 16 weeks (total of 5 doses).- Patients will be limited to receiving one dose of tocilizumab per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another (with the exception ofanakinra) following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum thecompletion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they weredeemed unresponsive to therapy.- Patients will not be permitted to switch from anakinra to other biologic agents except underexceptional circumstances.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage beyond the initial 5 doses, the patient must meet the following criteria:1) The patient must be assessed by an RA Specialist after 16 weeks, but no longer than 20 weeks after treatment to determine response.2) The RA Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:- ACR20 OR an improvement of 1.2 units in the DAS28 score [reported to one (1) decimal place]; AND- An improvement of 0.22 in HAQ score [reported to two (2) decimal places].It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above.
Following this assessment, continued coverage may be approved for one dose of 4 mg/kg to 8 mg/kg (up to a maximum of 800 mg per dose) every 4 weeks, for a period of 12 months. Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:1) The patient has been assessed by an RA Specialist to determine response;2) The RA Specialist must confirm in writing that the patient has maintained a response to
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TOCILIZUMAB
TOLTERODINE L-TARTRATE
TRETINOIN
80 MG / VIAL INJECTION
200 MG / VIAL INJECTION
400 MG / VIAL INJECTION
2 MG ORAL EXTENDED-RELEASE CAPSULE
4 MG ORAL EXTENDED-RELEASE CAPSULE
0.01 % TOPICAL CREAM
0.025 % TOPICAL CREAM
0.05 % TOPICAL CREAM
0.1 % TOPICAL CREAM
0.01 % TOPICAL GEL
0.025 % TOPICAL GEL
00002350092
00002350106
00002350114
00002244612
00002244613
00000657204
00000578576
00000518182
00000662348
00001926462
0000192647000000587966
ACTEMRA (4 ML)
ACTEMRA (10 ML)
ACTEMRA (20 ML)
DETROL LA
DETROL LA
STIEVA-A
STIEVA-A
STIEVA-A
STIEVA-A FORTE
VITAMIN A ACID
VITAMIN A ACIDSTIEVA-A
HLR
HLR
HLR
PFI
PFI
GSK
GSK
GSK
GSK
SAV
SAVGSK
192.6400
481.6000
963.2000
2.0556
2.0556
0.3221
0.3221
0.3221
0.3221
0.3186
0.3186 0.3221
87 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$
$
$
$
$$
Section 3 .
therapy as indicated by:- Confirmation of maintenance of ACR20, OR - Maintenance of a minimum improvement of 1.2 units in DAS28 score [reported to one (1) decimal place] from baseline.3) A current HAQ score [reported to two (2) decimal places] must be included with all renewalrequests.It should be noted that the initial score for the DAS28 or HAQ score on record will be rounded to the correct number of decimal places as indicated above."
All requests (including renewal requests) for tocilizumab for Rheumatoid Arthritis must becompleted using the Abatacept/Adalimumab/Anakinra/Etanercept/Golimumab/Infliximab/ Tocilizumab for Rheumatoid Arthritis Special Authorization Request Form (ABC 30902).
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): OXYBUTYNIN
"For patients who are intolerant to oxybutynin."
"Special authorization may be granted for 24 months."
"For the treatment of severe acne as defined by scarring acne.
Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
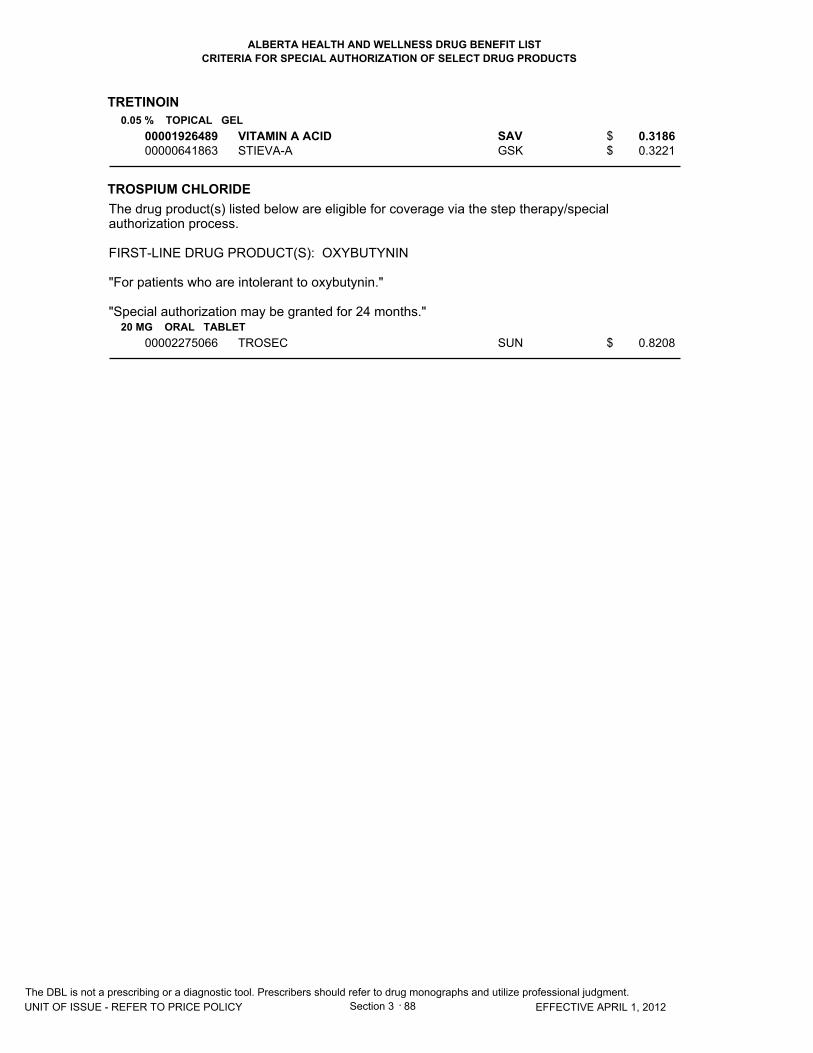
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
TRETINOIN
TROSPIUM CHLORIDE
0.05 % TOPICAL GEL
20 MG ORAL TABLET
0000192648900000641863
00002275066
VITAMIN A ACIDSTIEVA-A
TROSEC
SAVGSK
SUN
0.3186 0.3221
0.8208
88 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
Section 3 .
The drug product(s) listed below are eligible for coverage via the step therapy/special authorization process.
FIRST-LINE DRUG PRODUCT(S): OXYBUTYNIN
"For patients who are intolerant to oxybutynin."
"Special authorization may be granted for 24 months."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
USTEKINUMAB
45 MG INJECTION VIAL OR SYRINGE00002320673 STELARA (0.5 ML VIAL OR SYRINGE) JAI 4729.5592
89 EFFECTIVE APRIL 1, 2012
For this product - pricing has been established on a per vial or syringe basis.$
Section 3 .
"Special authorization coverage may be provided for the reduction in signs and symptoms of severe, debilitating plaque psoriasis in patients who:- Have a total PASI of 10 or more and a DLQI of more than 10, OR- Who have significant involvement of the face, palms of the hands, soles of the feet or genital region; AND- Who are refractory to or intolerant to:- Methotrexate at 20 mg (PO, SC or IM) or greater total weekly dosage (15 mg or greater if patient is 65 years of age or older) for more than 12 weeks. Patients who experience gastrointestinal intolerance to PO methotrexate must have a trial of parenteral methotrexate before being accepted as refractory, OR- Cyclosporine (6 weeks treatment); AND- Phototherapy (unless restricted by geographic location)
Patients who have a contraindication to either cyclosporine or methotrexate will be required to complete an adequate trial of the other pre-requisite medication prior to potential coverage beingconsidered.
'Refractory' is defined as lack of effect at the recommended doses and for duration of treatmentsspecified above.'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs.
For coverage, this drug must be prescribed by a Specialist in Dermatology ("Dermatology Specialist").
- Initial coverage may be approved for three doses of 45 mg at weeks 0, 4 and 16.- Patients will be limited to receiving one dose per prescription at their pharmacy.- Patients will be permitted to switch from one biologic agent to another following an adequate trial of the first biologic agent if unresponsive to therapy, or due to serious adverse effects or contraindications. An adequate trial is defined as at a minimum the completion of induction dosing (e.g. initial coverage period).- Patients will not be permitted to switch back to a previously trialed biologic agent if they were deemed unresponsive to therapy.- Patients are limited to receiving one biologic agent at a time regardless of the condition for which it is being prescribed.
For continued coverage, the patient must meet all of the following criteria:1) The patient must be assessed by a Dermatology Specialist after the initial16 weeks of therapyto determine response.2) The Dermatology Specialist must confirm, in writing, that the patient is a 'responder' that meets the following criteria:- Greater than or equal to 75% reduction in PASI score, OR- Greater than or equal to 50% reduction in PASI score AND improvement of greater than or equal to 5 points in the DLQI.
Following this assessment, continued coverage may be considered for 45 mg every 12 weeks for a period of 12 months. Ongoing coverage may be considered if the patient is re-assessed by a Dermatology Specialist every 12 months and is confirmed to be continuing to respond to therapy by meeting criteria as outlined in (2) above."
All requests (including renewal requests) for ustekinumab for Plaque Psoriasis must be completed using the Adalimumab/Etanercept/Infliximab/Ustekinumab for Plaque Psoriasis Special Authorization Request Form (ABC 31192).
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
VALGANCICLOVIR HCL
VANCOMYCIN HCL
VARENICLINE TARTRATE
450 MG (BASE) ORAL TABLET
125 MG (BASE) ORAL CAPSULE
250 MG (BASE) ORAL CAPSULE
0.5 MG (BASE) ORAL TABLET
1 MG (BASE) ORAL TABLET
00002245777
00000800430
00000788716
00002291177
00002291185
VALCYTE
VANCOCIN
VANCOCIN
CHAMPIX
CHAMPIX
HLR
MLI
MLI
PFI
PFI
24.5726
8.1241
16.2477
1.8496
1.8495
90 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
Section 3 .
"For the treatment of CMV retinitis in patients with acquired immunodeficiency syndrome (AIDS).""Special authorization may be granted for 12 months."
"For the prevention of CMV disease in solid organ transplant patients at risk (i.e. risk is defined as donor +ve/recipient -ve for CMV, or recipient +ve post-active treatment of CMV disease with IV ganciclovir, or recipient +ve in patients receiving antilymphocyte antibody [ALA]). For the purpose of administering this criterion, islet transplant recipients are at similar risk of CMV disease to patients undergoing a solid organ transplant and qualify for drug coverage.""Special authorization may be granted for 100 days."
"For the prevention of CMV disease in kidney transplant patients at risk (i.e. risk is defined as donor +ve/recipient -ve for CMV, or recipient +ve post-active treatment of CMV disease with IV ganciclovir, or recipient +ve in patients receiving antilymphocyte antibody [ALA]).""Special authorization may be granted for 200 days."
"For the treatment of:
1) Clostridium difficile enteritis if there is clinical deterioration or documented failure on metronidazole therapy. Documented failure is defined as no clinical improvement after 5 days oftherapy or
2) Laboratory confirmed relapse of Clostridium difficile enteritis with symptoms after 2 courses ofmetronidazole therapy or
3) Clostridium difficile enteritis if there is documented or impending toxic megacolon or
4) Clostridium difficile enteritis if there is intolerance or side effects to metronidazole therapy."
For subsequent prescriptions, patients may obtain this product via special authorization with the following criteria for coverage:
"For use in patients 18 years of age and older for smoking cessation treatment in conjunction with smoking cessation counseling.
Special authorization coverage may be granted for a maximum of 24 weeks of therapy per year."
This product is not eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
VARENICLINE TARTRATE/ VARENICLINE TARTRATE
VORICONAZOLE
0.5 MG * 1 MG ORAL TABLET
50 MG ORAL TABLET
200 MG ORAL TABLET
200 MG / VIAL INJECTION
00002298309
00002256460
00002256479
00002256487
CHAMPIX (STARTER PACK)
VFEND
VFEND
VFEND
PFI
PFI
PFI
PFI
1.8499
13.4179
53.6494
153.6622
91 EFFECTIVE APRIL 1, 2012
$
$
$
$
Section 3 .
For subsequent prescriptions, patients may obtain this product via special authorization with the following criteria for coverage:
"For use in patients 18 years of age and older for smoking cessation treatment in conjunction with smoking cessation counseling.
Special authorization coverage may be granted for a maximum of 24 weeks of therapy per year."
This product is not eligible for auto-renewal.
"For the treatment of invasive aspergillosis for post-hospital discharge only."
"For treatment of culture proven invasive candidiasis with documented resistance to fluconazole."
"This medication must be prescribed in consultation with a specialist in Infectious Diseases."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ZAFIRLUKAST
ZOLEDRONIC ACID
ZOLEDRONIC ACID
20 MG ORAL TABLET
0.05 MG / ML INJECTION
0.8 MG / ML INJECTION
00002236606
00002269198
00002248296
ACCOLATE
ACLASTA
ZOMETA CONCENTRATE
AZC
NOV
NOV
0.8054
7.2111
119.1272
92 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
Section 3 .
"For the treatment of Paget's disease. Special Authorization for this criterion may be granted for one dose per 12 month period."
"Coverage cannot be provided for two or more medications used in the treatment of Paget's disease when these medications are intended for use in combination or when therapy with two or more medications overlap."
"For the treatment of tumor-induced hypercalcemia in patients with documented evidence of intolerance or lack of response to clodronate or pamidronate. Special authorization may be granted for 6 months."
The following product(s) are eligible for auto-renewal.
(Refer to 48:10.24 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 12 to 18 years of age inclusive).
"For the prophylaxis and chronic treatment of asthma in patients over the age of 18 who meet one of the following criteria:
a) when used as adjunctive therapy in patients who do not respond adequately to high doses of inhaled glucocorticosteroids and long-acting beta 2 agonists. Patients must be unable to use long-acting beta 2 agonists or have demonstrated persistent symptoms while on long-acting beta 2 agonists, or
b) cannot operate inhaler devices."
"For the prophylaxis of exercise-induced bronchoconstriction in patients over the age of 18 where tachyphylaxis exists for long-acting beta 2 agonists."
"Special authorization for both criteria may be granted for 6 months."
In order to comply with the first criteria, information should indicate either a) current use of inhaled steroids and contraindications or poor response to long-acting beta 2 agonists (e.g. salmeterol or formoterol) or, b) the nature of the patient's difficulties with using inhaler devices. In order to comply with the second criteria, information should include the nature of the patient's response to long-acting beta 2 agonists (e.g. salmeterol or formoterol).
All requests (including renewal requests) for zafirlukast must be completed using the Montelukast/Zafirlukast Special Authorization Request Form (ABC 31313).
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
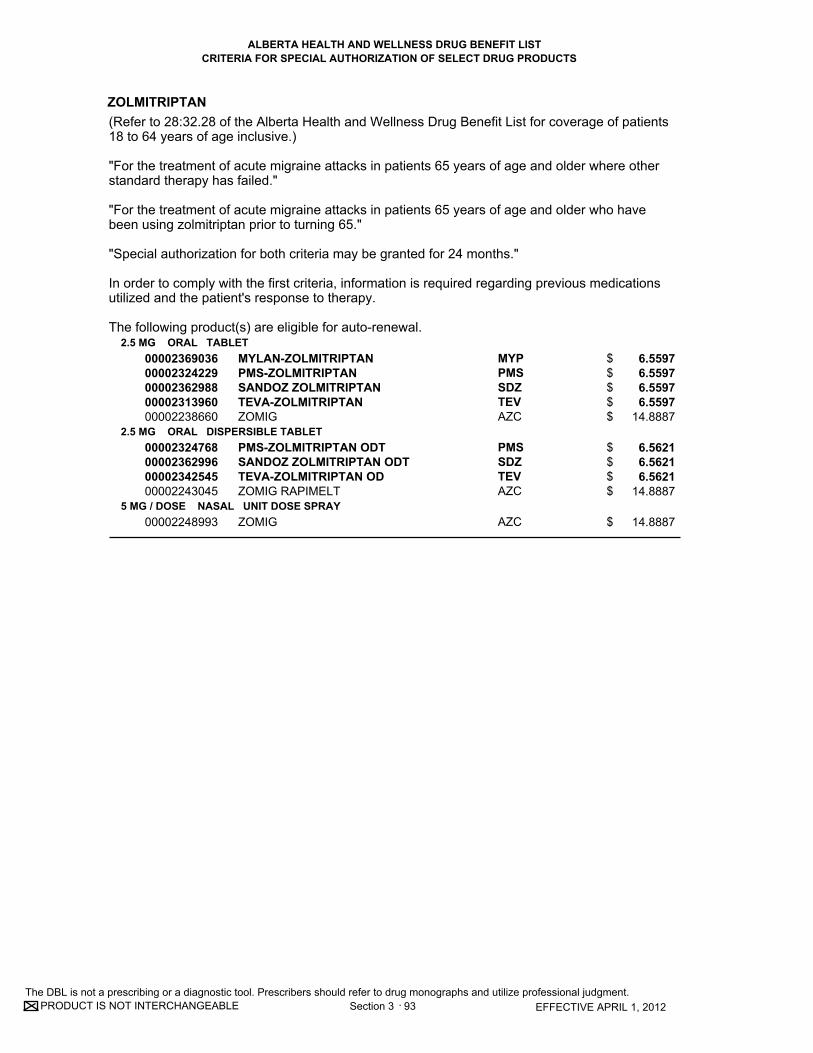
CRITERIA FOR SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ZOLMITRIPTAN
2.5 MG ORAL TABLET
2.5 MG ORAL DISPERSIBLE TABLET
5 MG / DOSE NASAL UNIT DOSE SPRAY
0000236903600002324229000023629880000231396000002238660
00002324768000023629960000234254500002243045
00002248993
MYLAN-ZOLMITRIPTANPMS-ZOLMITRIPTANSANDOZ ZOLMITRIPTANTEVA-ZOLMITRIPTANZOMIG
PMS-ZOLMITRIPTAN ODTSANDOZ ZOLMITRIPTAN ODTTEVA-ZOLMITRIPTAN ODZOMIG RAPIMELT
ZOMIG
MYPPMSSDZTEVAZC
PMSSDZTEVAZC
AZC
6.5597 6.5597 6.5597 6.5597
14.8887
6.5621 6.5621 6.5621
14.8887
14.8887
93 EFFECTIVE APRIL 1, 2012
$$$$$
$$$$
$
Section 3 .
(Refer to 28:32.28 of the Alberta Health and Wellness Drug Benefit List for coverage of patients 18 to 64 years of age inclusive.)
"For the treatment of acute migraine attacks in patients 65 years of age and older where other standard therapy has failed."
"For the treatment of acute migraine attacks in patients 65 years of age and older who have been using zolmitriptan prior to turning 65."
"Special authorization for both criteria may be granted for 24 months."
In order to comply with the first criteria, information is required regarding previous medications utilized and the patient's response to therapy.
The following product(s) are eligible for auto-renewal.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

Section 3A C
riteria for Optional Special A
uthorization of Select Drug Products
SECTION 3A
Criteria for Optional Special Authorization
of Select Drug Products
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize Professional judgment.
Section 3A EFFECTIVE APRIL 1, 2012
CRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
The drug products listed in this section may be considered for coverage by optional special authorization for patients covered under Alberta Health and Wellness-sponsored drug programs. (For Alberta Human Services and Alberta Seniors (AISH) clients, the optional special authorization criteria for coverage can be found in the Criteria for Optional Special Authorization of Select Drug Products section of the Alberta Human Services Drug Benefit Supplement.)
70BCriteria for Coverage
Wording that appears within quotation marks (“ “) in this section is the official optional special authorization criteria, as recommended by the Alberta Health and Wellness Expert Committee on Drug Evaluation and Therapeutics, and approved by the Minister of Health and Wellness. Wording that is not enclosed in quotation marks outlines specific information required to interpret criteria, guidelines for submitting requests and/or information regarding conditions under which coverage cannot be provided.
71BRole of the Prescribers
In conjunction with the criteria, prescribers have two options by which patients may be eligible for coverage of these select optional special authorization drug products.
1) Prescribers can register to be a designated prescriber. Registration allows for patients to receive coverage of select drug products without special authorization as long as the prescription is written for one of the criteria for coverage set out in this section. Should a designated prescriber wish to prescribe one of the select drug products outside the coverage criteria, they may do so but must indicate this on the prescription; however, patients will not be eligible for payment under the Alberta government-sponsored program for such prescription and the patient may choose to receive the product at their expense. The registration form may be found on the previous page.
2) Prescribers who choose not to register will be considered non-designated prescribers. Such prescribers will be required to apply for special authorization on the patient’s behalf.

ALBERTA GOVERNMENT SPONSORED DRUG BENEFIT PROGRAMS OPTIONAL SPECIAL AUTHORIZATION
REGISTRATION FOR DESIGNATED PRESCRIBER STATUS for Alberta Health and Wellness Drug Benefit List Claim Coverage
Select Quinolone Antibiotics
ciprofloxacin, levofloxacin, moxifloxacin, ofloxacin
Please complete all sections of this form and return it by fax to Alberta Blue Cross
Registrations will be accepted on an ongoing basis
PRESCRIBER SURNAME FIRST NAME INITIAL OFFICE PHONE: FAX:
OFFICE ADDRESS CITY PROVINCE POSTAL CODE
COLLEGE OF PHYSICIANS AND SURGEONS REGISTRATION NO. OR PROFESSIONAL REGISTRATION NO.
I have reviewed the criteria for coverage of select quinolone products, and I agree to abide with these criteria as updated from time to time in the Optional Special Authorization section of the Alberta Health and Wellness Drug Benefit List for coverage under the program.
SIGNATURE OF PRESCRIBER (required): DATE: The information collected by this form is collected pursuant to sections 20, 21 and 22 of the Health Information Act, and sections 33 and 34 of the Freedom of Information and Protection of Privacy Act, for the purpose of determining or verifying eligibility to participate in a program or receive a benefit, product or health service. If you have any questions regarding the collection of this information, please contact the Co-chairs of the Alberta Blue Cross Privacy Steering Committee at 780-498-8108 or 780-498-8597, 10009 - 108 Street, Edmonton AB, T5J 3C5.
PLEASE RETURN YOUR COMPLETED REGISTRATION BY FAX TO 1-877-305-9911 ABC 81897 Reg Form (R06/2009)

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTCRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
CIPROFLOXACIN
100 MG / ML ORAL SUSPENSION00002237514 CIPRO BAI 0.6126
1 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
"For the treatment of:
1) Respiratory Tract Infections: -end stage COPD with or without bronchiectasis, where there has been documentation of previous Pseudomonas aeruginosa colonization/infection or - pneumonic illness in cystic fibrosis; or
2) Genitourinary Tract Infections: - urinary tract infections, - prostatitis, - prophylaxis of urinary tract surgical procedures or - gonococcal infections; or
3) Skin and Soft Tissue/Bone and Joint Infections: - malignant/invasive otitis externa, - bone/joint infections due to gram negative organisms or - therapy/step-down therapy of polymicrobial infections in combination with clindamycin or metronidazole e.g. diabetic foot infection, decubitus ulcers; or
4) Gastrointestinal Tract Infections: - bacterial gastroenteritis where antimicrobial therapy is indicated, - typhoid fever (enteric fever), or- therapy/step-down therapy of polymicrobial infections in combination with clindamycin or metronidazole e.g. intra-abdominal infections; or
5) Other: - prophylaxis of adult contacts of cases of invasive meningococcal disease, - therapy/step-down therapy of hospital acquired gram negative infections, - empiric therapy of febrile neutropenia in combination with other appropriate agents or - exceptional case of allergy or intolerance to all other appropriate therapies as defined by relevant guidelines/references i.e. AMA CPGs or Bugs and Drugs.- for use in other current Health Canada approved indications when prescribed by a specialist in Infectious Diseases."
All requests for ciprofloxacin must be completed using the Select Quinolones Special Authorization Request Form (ABC 30966).
Section 3A
Patient claims for select quinolone prescriptions written by a non-designated prescriber will be subject to a first forgiveness rule, meaning the first claim will be paid. Subsequent claims for the same product (irrespective of strength, route and form) within a 90-day period would require the prescriber to apply for special authorization for coverage on the patient�s behalf.
.
Criteria For Optional Special Authorization Of Select Drug Products
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTCRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
PRODUCT IS NOT INTERCHANGEABLE
CIPROFLOXACIN HCL
250 MG (BASE) ORAL TABLET000022295210000233213200002353318000022473390000231742700002245647000021617370000224843700002303728000022468250000224875600002155958
APO-CIPROFLOXCIPROFLOXACINCIPROFLOXACINCO CIPROFLOXACINMINT-CIPROFLOXACINMYLAN-CIPROFLOXACINNOVO-CIPROFLOXACINPMS-CIPROFLOXACINRAN-CIPROFLOXRATIO-CIPROFLOXACINSANDOZ CIPROFLOXACINCIPRO
APXRANSNSCOBMPIMYPTEVPMSRANRPHSDZBAI
1.3992 1.3992 1.3992 1.3992 1.3992 1.3992 1.3992 1.3992 1.3992 1.3992 1.3992 2.6598
2 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$
"For the treatment of
1) Respiratory Tract Infections: - end stage COPD with or without bronchiectasis, where there has been documentation of previous Pseudomonas aeruginosa colonization/infection; or - pneumonic illness in cystic fibrosis; or
2) Genitourinary Tract Infections: - urinary tract infections; or - prostatitis; or - prophylaxis of urinary tract surgical procedures; or - gonococcal infections; or
3) Skin and Soft Tissue/Bone and Joint Infections: - malignant/invasive otitis externa; or - bone/joint infections due to gram negative organisms; or - therapy/step-down therapy of polymicrobial infections in combination with clindamycin or metronidazole e.g. diabetic foot infection, decubitus ulcers; or
4) Gastrointestinal Tract Infections: - bacterial gastroenteritis where antimicrobial therapy is indicated; or - typhoid fever (enteric fever); or - therapy/step-down therapy of polymicrobial infections in combination with clindamycin or metronidazole e.g. intra-abdominal infections; or
5) Other: - prophylaxis of adult contacts of cases of invasive meningococcal disease; or- therapy/step-down therapy of hospital acquired gram negative infections; or- empiric therapy of febrile neutropenia in combination with other appropriate agents; or - exceptional case of allergy or intolerance to all other appropriate therapies as defined by relevant guidelines/references i.e. AMA CPGs or Bugs and Drugs; or- for use in other current Health Canada approved indications when prescribed by a specialist in Infectious Diseases."
All requests for Ciprofloxacin must be completed using the Select Quinolones Special Authorization Request Form (ABC 30966).
Section 3A .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTCRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
CIPROFLOXACIN HCL500 MG (BASE) ORAL TABLET
750 MG (BASE) ORAL TABLET
000022295220000233214000002353326000022473400000231743500002245648000021617450000224843800002303736000022468260000224875700002155966
000022295230000233215900002353334000022473410000231744300002245649000021617530000224843900002303744000022468270000224875800002155974
APO-CIPROFLOXCIPROFLOXACINCIPROFLOXACINCO CIPROFLOXACINMINT-CIPROFLOXACINMYLAN-CIPROFLOXACINNOVO-CIPROFLOXACINPMS-CIPROFLOXACINRAN-CIPROFLOXRATIO-CIPROFLOXACINSANDOZ CIPROFLOXACINCIPRO
APO-CIPROFLOXCIPROFLOXACINCIPROFLOXACINCO CIPROFLOXACINMINT-CIPROFLOXACINMYLAN-CIPROFLOXACINNOVO-CIPROFLOXACINPMS-CIPROFLOXACINRAN-CIPROFLOXRATIO-CIPROFLOXACINSANDOZ CIPROFLOXACINCIPRO
APXRANSNSCOBMPIMYPTEVPMSRANRPHSDZBAI
APXRANSNSCOBMPIMYPTEVPMSRANRPHSDZBAI
1.5786 1.5786 1.5786 1.5786 1.5786 1.5786 1.5786 1.5786 1.5786 1.5786 1.5786 3.0009
2.9774 2.9774 2.9774 2.9774 2.9774 2.9774 2.9774 2.9774 2.9774 2.9774 2.9774 5.4952
3 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$
$$$$$$$$$$$$
Section 3A .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTCRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
PRODUCT IS NOT INTERCHANGEABLE
LEVOFLOXACIN
250 MG ORAL TABLET
500 MG ORAL TABLET
750 MG ORAL TABLET
0000228470700002361027000023154240000231397900002248262000022846770000229863500002236841
0000228471500002361035000023154320000231398700002248263000022846850000229864300002236842
000023259420000231544000002285649000023055850000229865100002246804
APO-LEVOFLOXACINAVA-LEVOFLOXACINCO LEVOFLOXACINMYLAN-LEVOFLOXACINNOVO-LEVOFLOXACINPMS-LEVOFLOXACINSANDOZ LEVOFLOXACINLEVAQUIN
APO-LEVOFLOXACINAVA-LEVOFLOXACINCO LEVOFLOXACINMYLAN-LEVOFLOXACINNOVO-LEVOFLOXACINPMS-LEVOFLOXACINSANDOZ LEVOFLOXACINLEVAQUIN
APO-LEVOFLOXACINCO LEVOFLOXACINNOVO-LEVOFLOXACINPMS-LEVOFLOXACINSANDOZ LEVOFLOXACINLEVAQUIN
APXAVACOBMYPTEVPMSSDZJAI
APXAVACOBMYPTEVPMSSDZJAI
APXCOBTEVPMSSDZJAI
2.8494 2.8494 2.8494 2.8494 2.8494 2.8494 2.8494 5.3300
3.2153 3.2153 3.2153 3.2153 3.2153 3.2153 3.2153 6.0142
5.6889 5.6889 5.6889 5.6889 5.6889
10.6414
4 EFFECTIVE APRIL 1, 2012
$$$$$$$$
$$$$$$$$
$$$$$$
"To be prescribed according to ONE of the following criteria:
For the treatment of
1) Community acquired pneumonia after failure of first line therapy, as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy; or
2) Community acquired pneumonia in patients with co-morbidities (asthma, lung cancer, COPD, diabetes, alcoholism, chronic renal or liver failure, CHF, chronic corticosteroid use, malnutrition or acute weight loss, hospitalization within previous 3 months, HIV/AIDS, smoking); or
3) Acute exacerbation of chronic bronchitis after failure of first and second line therapy, as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy; or
4) Acute sinusitis after failure of first line therapy, as defined by clinical deterioration after 72 h ofantibiotic therapy or lack of improvement after completion of antibiotic therapy, in patients with beta-lactam (penicillin and cephalosporin) allergy; or
5) For use in other current Health Canada approved indications when prescribed by a specialist in Infectious Diseases."
All requests for Levofloxacin must be completed using the Select Quinolones Special Authorization Request Form (ABC 30966).
Section 3A .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LISTCRITERIA FOR OPTIONAL SPECIAL AUTHORIZATION OF SELECT DRUG PRODUCTS
MOXIFLOXACIN HCL
OFLOXACIN
400 MG (BASE) ORAL TABLET
200 MG ORAL TABLET
300 MG ORAL TABLET
400 MG ORAL TABLET
00002242965
00002231529
00002231531
00002231532
AVELOX
OFLOXACIN
OFLOXACIN
OFLOXACIN
BAI
AAP
AAP
AAP
6.3885
1.4019
1.6472
1.6472
5 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
"To be prescribed according to ONE of the following criteria:
For the treatment of
1) Community acquired pneumonia after failure of first line therapy, as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy; or
2) Community acquired pneumonia in patients with co-morbidities (asthma, lung cancer, COPD, diabetes, alcoholism, chronic renal or liver failure, CHF, chronic corticosteroid use, malnutrition or acute weight loss, hospitalization within previous 3 months, HIV/AIDS, smoking); or
3) Acute exacerbation of chronic bronchitis after failure of first and second line therapy, as defined by clinical deterioration after 72 hours of antibiotic therapy or lack of improvement after completion of antibiotic therapy; or
4) Acute sinusitis after failure of first line therapy, as defined by clinical deterioration after 72 h ofantibiotic therapy or lack of improvement after completion of antibiotic therapy, in patients with beta-lactam (penicillin and cephalosporin) allergy; or
5) For use in other current Health Canada approved indications when prescribed by a specialist in Infectious Diseases."
All requests for Moxifloxacin HCl must be completed using the Select Quinolones Special Authorization Request Form (ABC 30966).
"To be prescribed according to ONE of the following criteria:
For the treatment of
1) Pelvic inflammatory disease; or
2) Epididymo-orchitis/epididymitis most likely due to enteric organisms; or
3) Chlamydia infection; or
4) Gonococcal infection; or
5) For use in other current Health Canada approved indications when prescribed by a specialist in Infectious Diseases."
All requests for Ofloxacin must be completed using the Select Quinolones Special Authorization Request Form (ABC 30966).
Section 3A .The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

Section 4 Rare D
iseases Drug C
overage Program
SECTION 4
Rare Diseases Drug Coverage Program
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST RARE DISEASES DRUG COVERAGE PROGRAM
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 4 • 1 EFFECTIVE APRIL 1, 2012
RARE DISEASES DRUG COVERAGE PROGRAM
Selected drug products used in the treatment of rare diseases may be considered for coverage for individuals covered under Alberta government-sponsored drug programs. The Minister of Health and Wellness makes the final decisions regarding coverage under this Program, and may list a drug product under this section when the Minister considers it in the public interest to do so.1
.
RARE DISEASES DRUG COVERAGE
In order to be eligible for the Rare Diseases Drug Coverage Program, an individual must: • have Alberta government-sponsored drug coverage; • be continuously registered in the Alberta Health Care Insurance Plan for a minimum of five
years unless: the individual is less than five years of age at the date of the application, then the
individual’s parent/guardian/legal representative must be registered continuously in the Alberta Health Care Insurance Plan for a minimum of five years;
OR the individual has moved to Alberta from another province or territory in Canada (the
“province of origin”), and immediately prior to moving to Alberta, was covered for a drug product listed in this section in the province of origin by a provincial or territorial government sponsored drug plan, and
• meet the clinical criteria for a rare disease drug product published on the List;
the individual has been registered in the Alberta Health Care Insurance Plan (the individual must provide supporting documentation from the province of origin to prove prior coverage).
• have a Rare Diseases Drug Coverage Application form (“Application”) submitted on their behalf to Alberta Blue Cross by the individual’s “Rare Disease Specialist”;
• have the Application reviewed and approved for coverage by the Alberta Rare Diseases Clinical Review Panel (“Review Panel”)
• complete the required forms, and consent to and acknowledge that approval for initial and continued coverage is conditional upon clinical outcomes; regular monitoring of the individual’s clinical outcomes will be required, and that coverage will be discontinued if there is inadequate response or the individual’s
condition deteriorates as outlined in the withdrawal criteria established in relation to a specific rare diseases drug product and/or as assessed by the Review Panel.
Contraindications
In addition to meeting the above criteria, the individual must not have the following contraindications: • Significant illness, not including one of the rare diseases, likely to substantially alter or reduce
life expectancy.
1 Section 1 of the AHWDBL does not apply to the Rare Diseases Drug Coverage Program

The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 Section 4 • 2
Rare Diseases Drugs Eligible for Coverage
Drug products approved by Health Canada for the treatment of Rare Diseases may be considered for coverage in accordance with this section. Rare Diseases are genetic, lysosmal storage disorders occurring at a rate of less than one per 50,000 for the Canadian population for a specific disease (as determined by Alberta Health and Wellness). As of April 1, 2009, drug products for the treatment of the following rare diseases are currently under consideration for coverage: • Gaucher’s disease • Fabry disease • MPS-I (Hurler/Hurler Scheie) • Hunter disease • Pompe disease
Alberta Rare Diseases Clinical Review Panel
The Alberta Rare Diseases Clinical Review Panel (“Review Panel”) is a review panel composed of specialists treating rare diseases and other health professionals with clinical expertise, appointed by the Minister of Health and Wellness. The Review Panel’s functions include: • Providing advice to Alberta Health and Wellness regarding the Rare Diseases Drug Coverage
Program; • Reviewing and applying clinical knowledge and skills to individual applications for Rare
Diseases Drug Coverage; and • Providing advice to the Expert Committee on Drug Evaluation and Therapeutics regarding
drug products under consideration for coverage under this section, clinical criteria for rare diseases drug products and identifying appropriate “Rare Disease Specialists”.
Process for Rare Diseases Drug Coverage
Participating “Rare Disease Specialists” must complete a Rare Diseases Drug Coverage Application form for each individual. The form must be the one specific to the rare diseases drug product being requested. The completed application may be forwarded to Alberta Blue Cross by mail or by facsimile. To be considered for Rare Diseases Drug Coverage, the “Rare Disease Specialist” must confirm the individual (or individual’s parent/guardian/legal representative) has been provided with information regarding the Rare Diseases Drug Coverage Program and have completed the required forms.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST RARE DISEASES DRUG COVERAGE PROGRAM
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
Section 4 • 3 EFFECTIVE APRIL 1, 2012
Alberta Blue Cross, in providing administrative support to the Review Panel, receives and screens each application for completeness, then forwards to Alberta Health and Wellness to confirm that the individual has met the Alberta Health Care Insurance Plan registration requirement (please see above). Once it has been confirmed that the individual meets the Alberta Health Care Insurance Plan registration requirement, Alberta Blue Cross forwards the application to the Review Panel for assessment. Alberta Blue Cross responds to applicants on the Review Panel’s behalf. After an application has been assessed by the Review Panel, Alberta Blue Cross notifies the individual’s “Rare Disease Specialist” and the individual or individual’s parent/guardian/legal representative by letter of the Review Panel’s decision. Eligibility will be effective the date coverage is approved by the Review Panel. Renewals require a new drug product specific Rare Diseases Drug Coverage Application form that is completed by a “Rare Disease Specialist”. To be eligible for Rare Diseases Drug Coverage, prescriptions must be written by a “Rare Disease Specialist” as identified by the eligibility criteria for the drug product. To avoid wastage, prescription quantities are limited to a one-month supply. Extended quantity and vacation supplies are not permitted. Out-of-country claims will only be reimbursed in accordance with standard rules and regulations; individuals should verify with Alberta Blue Cross these rules and regulations prior
to obtaining drug products out of the country.
Government will not be responsible for reimbursement of costs associated with wastage or improper storage of rare diseases drug products. Prior approval must be granted to ensure coverage. Approval is granted for a specific period, to a maximum of 12 months. If continued treatment is necessary, it is the responsibility of the individual or individual’s parent/guardian/legal representative and the “Rare Disease Specialist” to re-apply for drug product coverage prior to the expiry date of the authorization period.

Pharmacologic -Therapeutic C
lassification of Drugs
PART 2
Pharmacologic – Therapeutic Classification of Drugs
04:00 Antihistam
ine Drugs
04:00
Antihistamine Drugs

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DIPHENHYDRAMINE HCL
PROMETHAZINE HCL
TRIMEPRAZINE TARTRATE
KETOTIFEN FUMARATE
50 MG / ML INJECTION
25 MG / ML (BASE) INJECTION
2.5 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
1 MG (BASE) ORAL TABLET
0.2 MG / ML (BASE) ORAL SYRUP
00000596612
00000567434
00001926306
00001926292
0000223073000000577308
00002176084
DIPHENHYDRAMINE
PROMETHAZINE
PANECTYL
PANECTYL
NOVO-KETOTIFENZADITEN
NOVO-KETOTIFEN
SDZ
SDZ
ERF
ERF
TEVTEV
TEV
ANTIHISTAMINE DRUGS
ANTIHISTAMINE DRUGS
ANTIHISTAMINE DRUGS
FIRST GENERATION ANTIHISTAMINES
FIRST GENERATION ANTIHISTAMINES
OTHER ANTIHISTAMINES
04
04
04
:00
:00
:00
04:04.04
04:04.12
04:92
4.0452
1.1500
0.2913
0.3574
0.6335 0.8086
0.1397
1 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$$
$
(ETHANOLAMINE DERIVATIVES)
(PHENOTHIAZINE DERIVATIVES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

08:00 Anti-Infective A
gents
08:00
Anti-Infective Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
MEBENDAZOLE
GENTAMICIN SULFATE
TOBRAMYCIN
TOBRAMYCIN SULFATE
CEFAZOLIN SODIUM
CEPHALEXIN
100 MG ORAL CHEWABLE TABLET
40 MG / ML (BASE) INJECTION
28 MG INHALATION CAPSULE
60 MG / ML (BASE) INHALATION SOLUTION
10 MG / ML (BASE) INJECTION
40 MG / ML (BASE) INJECTION
500 MG / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
10 G / VIAL (BASE) INJECTION
250 MG ORAL TABLET
500 MG ORAL TABLET
00000556734
00002242652
00002365154
00002239630
00002241209
00002241210
0000230893200002108119
000022972050000230895900002108127
000022972130000230896700002108135
000007687230000058341300000865877
000007687150000058342100000865885
VERMOX
GENTAMICIN
TOBI PODHALER
TOBI
TOBRAMYCIN
TOBRAMYCIN
CEFAZOLINSTERILE CEFAZOLIN SODIUM
CEFAZOLINCEFAZOLINSTERILE CEFAZOLIN SODIUM
CEFAZOLINCEFAZOLINSTERILE CEFAZOLIN SODIUM
APO-CEPHALEXNOVO-LEXINNU-CEPHALEX
APO-CEPHALEXNOVO-LEXINNU-CEPHALEX
JAI
SDZ
NOV
NOV
SDZ
SDZ
SDZTEV
APXSDZTEV
APXSDZTEV
APXTEVNXP
APXTEVNXP
(FIRST GENERATION CEPHALOSPORINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTHELMINTICS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
08
:00
:00
:00
08:08
08:12.02
08:12.06.04
4.1426
2.9650
13.8232
11.0585
2.3150
3.2100
4.0000 4.0000
6.0000 6.0000 6.0000
56.0000 56.0000 56.0000
0.2250 0.2250 0.2250
0.4500 0.4500 0.4500
3 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$$
$$$
$$$
$$$
$$$
(AMINOGLYCOSIDES)
CEPHALOSPORINS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CEPHALEXIN
CEFPROZIL
250 MG ORAL CAPSULE
500 MG ORAL CAPSULE
25 MG / ML ORAL SUSPENSION
50 MG / ML ORAL SUSPENSION
250 MG ORAL TABLET
500 MG ORAL TABLET
25 MG / ML ORAL SUSPENSION
50 MG / ML ORAL SUSPENSION
00000342084
00000342114
00000342106
00000342092
00002292998000023472450000236284800002332035000022935280000230217900002163659
00002293005000023472530000236285600002332043000022935360000230218700002163667
000022939430000234726100002362864000023292040000230342600002163675
00002293951000023472880000236287200002332027000022935790000230343400002163683
NOVO-LEXIN
NOVO-LEXIN
NOVO-LEXIN
NOVO-LEXIN
APO-CEFPROZILAURO-CEFPROZILAVA-CEFPROZILCEFPROZILRAN-CEFPROZILSANDOZ CEFPROZILCEFZIL
APO-CEFPROZILAURO-CEFPROZILAVA-CEFPROZILCEFPROZILRAN-CEFPROZILSANDOZ CEFPROZILCEFZIL
APO-CEFPROZILAURO-CEFPROZILAVA-CEFPROZILRAN-CEFPROZILSANDOZ CEFPROZILCEFZIL
APO-CEFPROZILAURO-CEFPROZILAVA-CEFPROZILCEFPROZILRAN-CEFPROZILSANDOZ CEFPROZILCEFZIL
TEV
TEV
TEV
TEV
APXAURAVARANRANSDZBMS
APXAURAVARANRANSDZBMS
APXAURAVARANSDZBMS
APXAURAVARANRANSDZBMS
(FIRST GENERATION CEPHALOSPORINS)
(SECOND GENERATION CEPHALOSPORINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.06.04
08:12.06.08
0.3515
0.6646
0.0885
0.1390
0.9703 0.9703 0.9703 0.9703 0.9703 0.9703 1.8054
1.9025 1.9025 1.9025 1.9025 1.9025 1.9025 3.5398
0.0948 0.0948 0.0948 0.0948 0.0948 0.1765
0.1896 0.1896 0.1896 0.1896 0.1896 0.1896 0.3526
4 EFFECTIVE APRIL 1, 2012
$
$
$
$
$$$$$$$
$$$$$$$
$$$$$$
$$$$$$$
CEPHALOSPORINS
CEPHALOSPORINS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CEFUROXIME AXETIL
CEFIXIME
CEFOTAXIME SODIUM
CEFTAZIDIME
CEFTRIAXONE SODIUM
250 MG (BASE) ORAL TABLET
500 MG (BASE) ORAL TABLET
400 MG ORAL TABLET
20 MG / ML ORAL SUSPENSION
500 MG / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
2 G / VIAL (BASE) INJECTION
1 G / VIAL INJECTION
2 G / VIAL INJECTION
6 G / VIAL INJECTION
0.25 G / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
2 G / VIAL (BASE) INJECTION
00002244393000023448230000224265600002212277
00002244394000023448310000224265700002212285
00000868981
00000868965
00002225085
00002225093
00002225107
00002212218
00002212226
00002212234
00002292866
0000229227000002292874
0000229228900002292882
APO-CEFUROXIMEAURO-CEFUROXIMERATIO-CEFUROXIMECEFTIN
APO-CEFUROXIMEAURO-CEFUROXIMERATIO-CEFUROXIMECEFTIN
SUPRAX
SUPRAX
CLAFORAN
CLAFORAN
CLAFORAN
FORTAZ
FORTAZ
FORTAZ
CEFTRIAXONE FOR INJECTION USP
CEFTRIAXONE FOR INJECTION USPCEFTRIAXONE FOR INJECTION USP
CEFTRIAXONE FOR INJECTION USPCEFTRIAXONE FOR INJECTION USP
APXAURRPHGSK
APXAURRPHGSK
SAV
SAV
SAV
SAV
SAV
GSK
GSK
GSK
APX
SDZAPX
SDZAPX
(SECOND GENERATION CEPHALOSPORINS)
(THIRD GENERATION CEPHALOSPORINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.06.08
08:12.06.12
0.9745 0.9745 0.9745 1.7767
1.9304 1.9304 1.9304 3.5195
3.8055
0.4478
6.5467
10.2985
20.6185
24.2821
47.7418
143.2940
7.5250
23.8000 23.8000
46.9000 46.9000
5 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$$$
$
$
$
$
$
$
$
$
$
$$
$$
CEPHALOSPORINS
CEPHALOSPORINS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CHLORAMPHENICOL SODIUM SUCCINATE
ERYTHROMYCIN
ERYTHROMYCIN ESTOLATE
ERYTHROMYCIN ETHYLSUCCINATE
ERYTHROMYCIN STEARATE
1 G / VIAL (BASE) INJECTION
250 MG ORAL TABLET
250 MG ORAL CAPSULE (ENTERIC-COATED PELLET)
333 MG ORAL CAPSULE (ENTERIC-COATED PELLET)
50 MG / ML (BASE) ORAL SUSPENSION
600 MG (BASE) ORAL TABLET
40 MG / ML (BASE) ORAL SUSPENSION
80 MG / ML (BASE) ORAL SUSPENSION
250 MG ORAL TABLET
500 MG ORAL TABLET
00000312363
00000682020
0000072667200000607142
0000192593800000873454
00000262595
00000637416
00000605859
00000652318
00000545678
00000688568
CHLOROMYCETIN
ERYTHRO-BASE
ERYTHRO-ECERYC
ERYTHRO-ECERYC
NOVO-RYTHRO ESTOLATE
ERYTHRO-ES
NOVO-RYTHRO EES
NOVO-RYTHRO EES
ERYTHRO-S
ERYTHRO-S
ERF
AAP
AAPPFI
AAPPFI
TEV
AAP
TEV
TEV
AAP
AAP
(ERYTHROMYCINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.08
08:12.12.04
19.7932
0.1965
0.3900 0.5285
0.4332 0.5872
0.1270
0.3615
0.0967
0.1464
0.2277
0.5832
6 EFFECTIVE APRIL 1, 2012
$
$
$$
$$
$
$
$
$
$
$
(CHLORAMPHENICOL)
MACROLIDES
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
AZITHROMYCIN
CLARITHROMYCIN
250 MG ORAL TABLET
20 MG / ML ORAL SUSPENSION
40 MG / ML ORAL SUSPENSION
250 MG ORAL TABLET
500 MG ORAL TABLET
500 MG ORAL EXTENDED-RELEASE TABLET
25 MG / ML ORAL SUSPENSION
50 MG / ML ORAL SUSPENSION
000022474230000236336400002330881000022553400000227453100002278359000022678450000227858800002261634000022752870000226582600002212021
0000236337200002315157000022743880000233238800002223716
0000236338000002315165000022743960000233239600002223724
0000224885600002247573000022478180000226653900001984853
000023663980000224885700002247574000022478190000226654700002126710
00002244756
00002146908
00002244641
APO-AZITHROMYCINAVA-AZITHROMYCINAZITHROMYCINCO AZITHROMYCINGD-AZITHROMYCINMYLAN-AZITHROMYCINNOVO-AZITHROMYCINPHL-AZITHROMYCINPMS-AZITHROMYCINRATIO-AZITHROMYCINSANDOZ AZITHROMYCINZITHROMAX
AVA-AZITHROMYCINNOVO-AZITHROMYCINPMS-AZITHROMYCINSANDOZ AZITHROMYCINZITHROMAX
AVA-AZITHROMYCINNOVO-AZITHROMYCINPMS-AZITHROMYCINSANDOZ AZITHROMYCINZITHROMAX
MYLAN-CLARITHROMYCINPMS-CLARITHROMYCINRATIO-CLARITHROMYCINSANDOZ CLARITHROMYCINBIAXIN BID
AVA-CLARITHROMYCINMYLAN-CLARITHROMYCINPMS-CLARITHROMYCINRATIO-CLARITHROMYCINSANDOZ CLARITHROMYCINBIAXIN BID
BIAXIN XL
BIAXIN
BIAXIN
APXAVASNSCOBGMDMYPTEVPHHPMSRPHSDZPFI
AVATEVPMSSDZPFI
AVATEVPMSSDZPFI
MYPPMSRPHSDZABB
AVAMYPPMSRPHSDZABB
ABB
ABB
ABB
(OTHER MACROLIDES)
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
08:00
08:12.12.92
2.9650 2.9650 2.9650 2.9650 2.9650 2.9650 2.9650 2.9650 2.9650 2.9650 2.9650 5.4062
0.6407 0.6407 0.6410 0.6410 1.1686
0.9080 0.9080 0.9083 0.9083 1.6559
0.7419 0.7419 0.7419 0.7419 1.6833
1.8249 1.8249 1.8249 1.8249 1.8249 3.3271
2.5144
0.2924
0.5674
7 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$
$$$$$
$$$$$
$$$$$
$$$$$$
$
$
$
MACROLIDES
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PENICILLIN G SODIUM
PENICILLIN V POTASSIUM
AMOXICILLIN TRIHYDRATE
1,000,000 IU / VIAL INJECTION
5,000,000 IU / VIAL INJECTION
10,000,000 IU / VIAL INJECTION
300 MG ORAL TABLET
25 MG / ML ORAL LIQUID
60 MG / ML ORAL LIQUID
125 MG (BASE) ORAL CHEWABLE TABLET
250 MG (BASE) ORAL CHEWABLE TABLET
250 MG (BASE) ORAL CAPSULE
500 MG (BASE) ORAL CAPSULE
00001930672
00000883751
00001930680
000006422150000002120200000717568
00000642223
0000064223100000391603
00002036347
00002036355
000023527100000062811500002238171000004067240000086556700002230243
000023527290000062812300002238172000004067160000086557500002230244
PENICILLIN G SODIUM
PENICILLIN G SODIUM
PENICILLIN G SODIUM
APO-PEN-VKNOVO-PEN-VKNU-PEN-VK
APO-PEN-VK
APO-PEN-VKNOVO-PEN-VK
NOVAMOXIN
NOVAMOXIN
AMOXICILLINAPO-AMOXIMYLAN-AMOXICILLINNOVAMOXINNU-AMOXIPMS-AMOXICILLIN
AMOXICILLINAPO-AMOXIMYLAN-AMOXICILLINNOVAMOXINNU-AMOXIPMS-AMOXICILLIN
TEV
TEV
TEV
APXTEVNXP
APX
APXTEV
TEV
TEV
SNSAPXMYPTEVNXPPMS
SNSAPXMYPTEVNXPPMS
(NATURAL PENICILLINS)
(AMINOPENICILLINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.16.04
08:12.16.08
2.5216
5.3584
9.3509
0.0710 0.0710 0.0710
0.0535
0.0618 0.0618
0.4378
0.6335
0.1750 0.1750 0.1750 0.1750 0.1750 0.1750
0.3417 0.3417 0.3417 0.3417 0.3417 0.3417
8 EFFECTIVE APRIL 1, 2012
$
$
$
$$$
$
$$
$
$
$$$$$$
$$$$$$
PENICILLINS
PENICILLINS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
AMOXICILLIN TRIHYDRATE
AMOXICILLIN TRIHYDRATE/ CLAVULANATE POTASSIUM
AMPICILLIN SODIUM
25 MG / ML (BASE) ORAL SUSPENSION
50 MG / ML (BASE) ORAL SUSPENSION
250 MG (BASE) * 125 MG (BASE) ORAL TABLET
500 MG (BASE) * 125 MG (BASE) ORAL TABLET
875 MG (BASE) * 125 MG (BASE) ORAL TABLET
25 MG / ML (BASE) * 6.25 MG / ML (BASE) ORAL SUSPENSION
40 MG / ML (BASE) * 5.7 MG / ML (BASE) ORAL SUSPENSION
50 MG / ML (BASE) * 12.5 MG / ML (BASE) ORAL SUSPENSION
80 MG / ML (BASE) * 11.4 MG / ML (BASE) ORAL SUSPENSION
250 MG / VIAL (BASE) INJECTION
500 MG / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
00002352745000023527610000045214900001934171000006281310000086554000002230245
00002352753000023527880000062815800000452130000019341630000086555900002230246
00002243350
000022433510000224377100001916858
00002245623000022481380000224702100002238829
000022439860000224464600001916882
00002238831
000022439870000224464700001916874
00002238830
00000872644
00000872652
00001933345
AMOXICILLINAMOXICILLIN SUGAR-REDUCEDNOVAMOXINNOVAMOXIN SUGAR-REDUCEDAPO-AMOXINU-AMOXIPMS-AMOXICILLIN
AMOXICILLINAMOXICILLIN SUGAR-REDUCEDAPO-AMOXINOVAMOXINNOVAMOXIN SUGAR-REDUCEDNU-AMOXIPMS-AMOXICILLIN
APO-AMOXI CLAV
APO-AMOXI CLAVRATIO-ACLAVULANATECLAVULIN-500F
APO-AMOXI CLAVNOVO-CLAVAMOXINRATIO-ACLAVULANATECLAVULIN-875
APO-AMOXI CLAVRATIO-ACLAVULANATE 125FCLAVULIN-125F
CLAVULIN-200
APO-AMOXI CLAVRATIO-ACLAVULANATE 250FCLAVULIN-250F
CLAVULIN-400
AMPICILLIN SODIUM
AMPICILLIN SODIUM
AMPICILLIN SODIUM
SNSSNSTEVTEVAPXNXPPMS
SNSSNSAPXTEVTEVNXPPMS
APX
APXRPHGSK
APXTEVRPHGSK
APXRPHGSK
GSK
APXRPHGSK
GSK
TEV
TEV
TEV
(AMINOPENICILLINS)
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
08:00
08:12.16.08
0.0352 0.0352 0.0352 0.0352 0.0353 0.0353 0.0353
0.0540 0.0540 0.0540 0.0540 0.0540 0.0540 0.0540
0.9375
0.8911 0.8911 1.5910
1.2610 1.2610 1.2610 2.3870
0.0704 0.0704 0.1258
0.1548
0.1211 0.1211 0.2162
0.2959
2.1538
2.2589
3.7824
9 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$
$$$$$$$
$
$$$
$$$$
$$$
$
$$$
$
$
$
$
PENICILLINS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
AMPICILLIN SODIUM
CLOXACILLIN SODIUM
NORFLOXACIN
2 G / VIAL (BASE) INJECTION
250 MG (BASE) ORAL CAPSULE
500 MG (BASE) ORAL CAPSULE
25 MG / ML (BASE) ORAL LIQUID
500 MG / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
2 G / VIAL (BASE) INJECTION
400 MG ORAL TABLET
00001933353
00000337765
00000337773
00000337757
00001912429
00001975447
00001912410
0000222952400002366304000022696270000223768200002246596
AMPICILLIN SODIUM
NOVO-CLOXIN
NOVO-CLOXIN
NOVO-CLOXIN
CLOXACILLIN SODIUM
CLOXACILLIN SODIUM
CLOXACILLIN SODIUM
APO-NORFLOXAVA-NORFLOXACINCO NORFLOXACINNOVO-NORFLOXACINPMS-NORFLOXACIN
TEV
TEV
TEV
TEV
TEV
TEV
TEV
APXAVACOBTEVPMS
(AMINOPENICILLINS)
(PENICILLINASE-RESISTANT PENICILLINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
08
:00
:00
:00
08:12.16.08
08:12.16.12
08:12.18
7.5648
0.3515
0.6646
0.0855
4.7910
5.8890
7.6856
1.2204 1.2204 1.2204 1.2204 1.2204
10 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$
$$$$$
PENICILLINS
PENICILLINS
(QUINOLONES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SULFAMETHOXAZOLE/ TRIMETHOPRIM
SULFASALAZINE
DOXYCYCLINE HYCLATE
100 MG * 20 MG ORAL TABLET
400 MG * 80 MG ORAL TABLET
800 MG * 160 MG ORAL TABLET
40 MG / ML * 8 MG / ML ORAL SUSPENSION
80 MG / ML * 16 MG / ML INJECTION
500 MG ORAL TABLET
500 MG ORAL ENTERIC-COATED TABLET
100 MG (BASE) ORAL TABLET
100 MG (BASE) ORAL CAPSULE
00000445266
000004452740000051063700000865710
000004452820000051064500000865729
00000726540
00000550086
0000059846100002064480
0000059848800002064472
000008742560000235124200002158574
0000074071300002351234000007252500000204466800000024368
APO-SULFATRIM
APO-SULFATRIMNOVO-TRIMELNU-COTRIMOX
APO-SULFATRIM DSNOVO-TRIMEL DSNU-COTRIMOX DS
NOVO-TRIMEL
SEPTRA
PMS-SULFASALAZINESALAZOPYRIN
PMS-SULFASALAZINESALAZOPYRIN EN-TABS
APO-DOXYDOXYCYCLINENOVO-DOXYLIN
APO-DOXYDOXYCYCLINENOVO-DOXYLINNU-DOXYCYCLINEVIBRAMYCIN
APX
APXTEVNXP
APXTEVNXP
TEV
TPI
PMSPFI
PMSPFI
APXSNSTEV
APXSNSTEVNXPPFI
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.20
08:12.24
0.0911
0.0482 0.0482 0.0482
0.1221 0.1221 0.1221
0.0954
1.4232
0.2221 0.2749
0.3382 0.4329
0.5860 0.5860 0.5860
0.5860 0.5860 0.5860 0.5860 1.8602
11 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$
$$$
$
$
$$
$$
$$$
$$$$$
(SULFONAMIDES)
(TETRACYCLINES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
MINOCYCLINE HCL
TETRACYCLINE HCL
VANCOMYCIN HCL
50 MG (BASE) ORAL CAPSULE
100 MG (BASE) ORAL CAPSULE
250 MG ORAL CAPSULE
500 MG / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
000020840900000228722600002230735000021081430000229441900002237313
000020841040000228723400002230736000021081510000229442700002237314
00000580929
0000224182000002342855
0000224182100002342863
APO-MINOCYCLINEMINOCYCLINEMYLAN-MINOCYCLINENOVO-MINOCYCLINEPMS-MINOCYCLINESANDOZ MINOCYCLINE
APO-MINOCYCLINEMINOCYCLINEMYLAN-MINOCYCLINENOVO-MINOCYCLINEPMS-MINOCYCLINESANDOZ MINOCYCLINE
TETRACYCLINE
PMS-VANCOMYCINVAL-VANCO
PMS-VANCOMYCINVAL-VANCO
APXSNSMYPTEVPMSSDZ
APXSNSMYPTEVPMSSDZ
AAP
PMSVLP
PMSVLP
(GLYCOPEPTIDES)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.24
08:12.28.16
0.5350 0.5350 0.5350 0.5350 0.5350 0.5350
1.0332 1.0332 1.0332 1.0332 1.0332 1.0332
0.0706
31.0500 31.0500
58.9900 58.9900
12 EFFECTIVE APRIL 1, 2012
$$$$$$
$$$$$$
$
$$
$$
(TETRACYCLINES)
MISCELLANEOUS ANTIBACTERIALS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CLINDAMYCIN HCL
CLINDAMYCIN PALMITATE HCL
CLINDAMYCIN PHOSPHATE
COLISTIMETHATE SODIUM
150 MG (BASE) ORAL CAPSULE
300 MG (BASE) ORAL CAPSULE
15 MG / ML (BASE) ORAL SOLUTION
150 MG / ML (BASE) INJECTION
150 MG / VIAL INJECTION
0000224523200002364719000022583310000224170900000030570
0000224523300002364727000022583580000224171000002182866
00000225851
000022305400000223053500000260436
00002244849
APO-CLINDAMYCINAVA-CLINDAMYCINMYLAN-CLINDAMYCINNOVO-CLINDAMYCINDALACIN C
APO-CLINDAMYCINAVA-CLINDAMYCINMYLAN-CLINDAMYCINNOVO-CLINDAMYCINDALACIN C
DALACIN C PALMITATE
CLINDAMYCINCLINDAMYCIN (60 & 120 ML)DALACIN C PHOSPHATE
COLISTIMETHATE FOR INJECTION
APXAVAMYPTEVPFI
APXAVAMYPTEVPFI
PFI
SDZSDZPFI
STM
(LINCOMYCINS)
(POLYMYXINS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIBACTERIALS
ANTIBACTERIALS
08
08
:00
:00
08:12.28.20
08:12.28.28
0.4890 0.4890 0.4890 0.4890 1.0118
0.9780 0.9780 0.9780 0.9780 2.0235
0.1336
3.3250 3.3250 4.4069
35.4154
13 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$
$$$$$
$
$$$
$
MISCELLANEOUS ANTIBACTERIALS
MISCELLANEOUS ANTIBACTERIALS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TERBINAFINE HCL
FLUCONAZOLE
ITRACONAZOLE
KETOCONAZOLE
250 MG (BASE) ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
2 MG / ML INJECTION
100 MG ORAL CAPSULE
200 MG ORAL TABLET
0000223989300002320134000022547270000235707000002242503000022403460000224080700002294273000022621770000235312100002031116
0000223737000002281260000022452920000223697800002245643
0000224529300002236979000022456440000223737100002281279
000022479220000224774900000891835
00002047454
000022372350000223106100002122197
APO-TERBINAFINEAURO-TERBINAFINECO TERBINAFINEJAMP-TERBINAFINEMYLAN-TERBINAFINENOVO-TERBINAFINEPMS-TERBINAFINEPMS-TERBINAFINESANDOZ TERBINAFINETERBINAFINELAMISIL
APO-FLUCONAZOLECO FLUCONAZOLEMYLAN-FLUCONAZOLENOVO-FLUCONAZOLEPMS-FLUCONAZOLE
MYLAN-FLUCONAZOLENOVO-FLUCONAZOLEPMS-FLUCONAZOLEAPO-FLUCONAZOLECO FLUCONAZOLE
FLUCONAZOLEFLUCONAZOLE OMEGADIFLUCAN
SPORANOX
APO-KETOCONAZOLENOVO-KETOCONAZOLENU-KETOCON
APXAURCOBJPCMYPTEVPMSPMSSDZSNSNOV
APXCOBMYPTEVPMS
MYPTEVPMSAPXCOB
TEVOMGPFI
JAI
APXTEVNXP
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIFUNGALS
ANTIFUNGALS
08
08
:00
:00
08:14.04
08:14.08
2.5243 2.5243 2.5243 2.5243 2.5243 2.5243 2.5243 2.5243 2.5243 2.5243 4.4398
2.9186 2.9186 2.9186 2.9186 2.9186
5.1766 5.1766 5.1766 5.1776 5.1776
0.3187 0.3187 0.5390
4.4192
1.1835 1.1835 1.1835
14 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$
$$$$$
$$$$$
$$$
$
$$$
(ALLYLAMINES)
(AZOLES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
AMPHOTERICIN B
NYSTATIN
DAPSONE
LAMIVUDINE
TENOFOVIR DISOPROXIL FUMARATE
50 MG / VIAL INJECTION
500,000 UNIT ORAL TABLET
100,000 UNIT / ML ORAL SUSPENSION
100 MG ORAL TABLET
100 MG ORAL TABLET
300 MG (BASE) ORAL TABLET
00000029149
00002194198
0000079266700002194201
00002041510
00002239193
00002247128
FUNGIZONE IV
RATIO-NYSTATIN
PMS-NYSTATINRATIO-NYSTATIN
DAPSONE
HEPTOVIR
VIREAD
BMS
RPH
PMSRPH
NTI
GSK
GIL
(NUCLEOSIDE AND NUCLEOTIDE REVERSE TRANSCRIPTASE INHIBITORS)
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIFUNGALS
ANTIMYCOBACTERIALS
ANTIVIRALS
08
08
08
:00
:00
:00
08:14.28
08:16.92
08:18.08.20
72.4931
0.2521
0.0520 0.0520
1.4405
5.0620
19.1382
15 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$$
$
$
$
RESTRICTED BENEFIT - This product is a benefit when initiated by a Specialist in Internal Medicine or a designated prescriber.
RESTRICTED BENEFIT - This product is a benefit for the treatment of chronic hepatitis B when prescribed by a Specialist in Internal Medicine or a designated prescriber.
(POLYENES)
(MISCELLANEOUS ANTIMYCOBACTERIALS)
ANTIRETROVIRALS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PEGINTERFERON ALFA-2A
ACYCLOVIR
ADEFOVIR DIPIVOXIL
ENTECAVIR
180 MCG / SYR INJECTION SYRINGE
200 MG ORAL TABLET
400 MG ORAL TABLET
800 MG ORAL TABLET
40 MG / ML ORAL SUSPENSION
10 MG ORAL TABLET
0.5 MG ORAL TABLET
00002248077
000022865560000220762100002242784000022859590000207862700000634506
00002286564000022076480000224246300002285967000021974130000207863500001911627
000022865720000220765600002242464000022859750000219742100002078651
00000886157
00002247823
00002282224
PEGASYS (0.5 ML SYRINGE)
ACYCLOVIRAPO-ACYCLOVIRMYLAN-ACYCLOVIRNOVO-ACYCLOVIRRATIO-ACYCLOVIRZOVIRAX
ACYCLOVIRAPO-ACYCLOVIRMYLAN-ACYCLOVIRNOVO-ACYCLOVIRNU-ACYCLOVIRRATIO-ACYCLOVIRZOVIRAX
ACYCLOVIRAPO-ACYCLOVIRMYLAN-ACYCLOVIRNOVO-ACYCLOVIRNU-ACYCLOVIRRATIO-ACYCLOVIR
ZOVIRAX
HEPSERA
BARACLUDE
HLR
SNSAPXMYPTEVRPHGSK
SNSAPXMYPTEVNXPRPHGSK
SNSAPXMYPTEVNXPRPH
GSK
GIL
BMS
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIVIRALS
ANTIVIRALS
08
08
:00
:00
08:18.20
08:18.32
425.5280
0.7702 0.7702 0.7702 0.7702 0.7702 1.4043
1.5519 1.5519 1.5519 1.5519 1.5519 1.5519 2.8294
2.8557 2.8557 2.8557 2.8557 2.8557 2.8557
0.2749
25.0245
22.0000
16 EFFECTIVE APRIL 1, 2012
$
$$$$$$
$$$$$$$
$$$$$$
$
$
$
RESTRICTED BENEFIT - This product is a benefit for the treatment of chronic hepatitis B when prescribed by a Specialist in Internal Medicine or a designated prescriber. (For eligibility for the treatment of chronic hepatitis C refer to Criteria for Special Authorization of Select Drug Products of the List and Criteria for Special Authorization of Select Drug Products of the Alberta Human Services Drug Benefit Supplement for Alberta Human Services and Alberta Seniors (AISH) clients.)
RESTRICTED BENEFIT - This product is a benefit for the treatment of chronic hepatitis B when prescribed by a Specialist in Internal Medicine or a designated prescriber.
RESTRICTED BENEFIT - This product is a benefit for the treatment of chronic hepatitis B when prescribed by a Specialist in Internal Medicine or a designated prescriber.
(INTERFERONS)
(NUCLEOSIDES AND NUCLEOTIDES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
GANCICLOVIR SODIUM
VALACYCLOVIR
IODOQUINOL
CHLOROQUINE PHOSPHATE
HYDROXYCHLOROQUINE SULFATE
PRIMAQUINE PHOSPHATE
PYRIMETHAMINE
500 MG / VIAL (BASE) INJECTION
500 MG ORAL TABLET
1,000 MG ORAL TABLET
210 MG ORAL TABLET
650 MG ORAL TABLET
250 MG ORAL TABLET
200 MG ORAL TABLET
15 MG (BASE) ORAL TABLET
25 MG ORAL TABLET
00002162695
0000229582200002331748000023515790000229845700002219492
00002354705
00001997769
00001997750
00000021261
000022466910000225260000002017709
00002017776
00000004774
CYTOVENE
APO-VALACYCLOVIR (CAPLET)CO VALACYCLOVIRMYLAN-VALACYCLOVIR (CAPLET)PMS-VALACYCLOVIR (CAPLET)VALTREX (CAPLET)
APO-VALACYCLOVIR (CAPLET)
DIODOQUIN
DIODOQUIN
NOVO-CHLOROQUINE
APO-HYDROXYQUINEMYLAN-HYDROXYCHLOROQUINEPLAQUENIL SULFATE
PRIMAQUINE PHOSPHATE
DARAPRIM
HLR
APXCOBMYPPMSGSK
APX
GLE
GLE
TEV
APXMYPSAV
SAV
COR
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIVIRALS
ANTIPROTOZOALS
ANTIPROTOZOALS
08
08
08
:00
:00
:00
08:18.32
08:30.04
08:30.08
45.1908
2.0422 2.0422 2.0422 2.0422 3.6472
3.0531
0.6975
0.8655
0.4010
0.3301 0.3301 0.6616
0.4287
1.4803
17 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$$$
$
$
$
$
$$$
$
$
(NUCLEOSIDES AND NUCLEOTIDES)
(AMEBICIDES)
(ANTIMALARIALS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
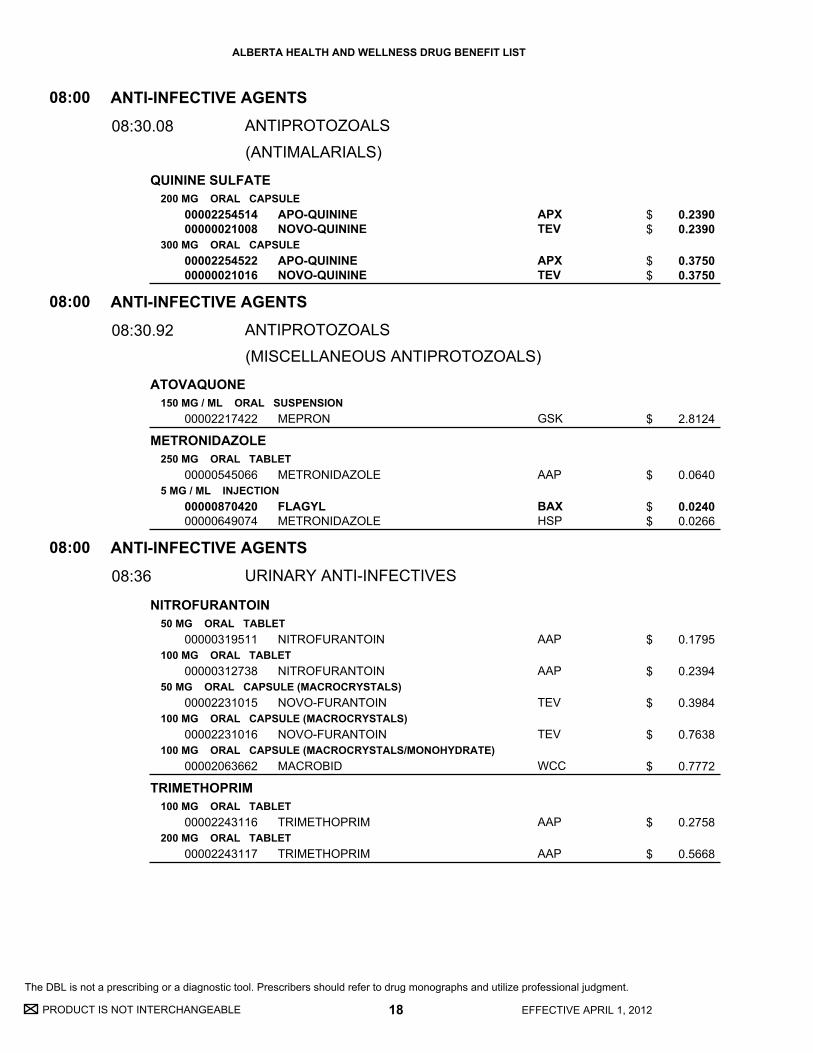
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
QUININE SULFATE
ATOVAQUONE
METRONIDAZOLE
NITROFURANTOIN
TRIMETHOPRIM
200 MG ORAL CAPSULE
300 MG ORAL CAPSULE
150 MG / ML ORAL SUSPENSION
250 MG ORAL TABLET
5 MG / ML INJECTION
50 MG ORAL TABLET
100 MG ORAL TABLET
50 MG ORAL CAPSULE (MACROCRYSTALS)
100 MG ORAL CAPSULE (MACROCRYSTALS)
100 MG ORAL CAPSULE (MACROCRYSTALS/MONOHYDRATE)
100 MG ORAL TABLET
200 MG ORAL TABLET
0000225451400000021008
0000225452200000021016
00002217422
00000545066
0000087042000000649074
00000319511
00000312738
00002231015
00002231016
00002063662
00002243116
00002243117
APO-QUININENOVO-QUININE
APO-QUININENOVO-QUININE
MEPRON
METRONIDAZOLE
FLAGYLMETRONIDAZOLE
NITROFURANTOIN
NITROFURANTOIN
NOVO-FURANTOIN
NOVO-FURANTOIN
MACROBID
TRIMETHOPRIM
TRIMETHOPRIM
APXTEV
APXTEV
GSK
AAP
BAXHSP
AAP
AAP
TEV
TEV
WCC
AAP
AAP
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTI-INFECTIVE AGENTS
ANTIPROTOZOALS
ANTIPROTOZOALS
URINARY ANTI-INFECTIVES
08
08
08
:00
:00
:00
08:30.08
08:30.92
08:36
0.2390 0.2390
0.3750 0.3750
2.8124
0.0640
0.0240 0.0266
0.1795
0.2394
0.3984
0.7638
0.7772
0.2758
0.5668
18 EFFECTIVE APRIL 1, 2012
$$
$$
$
$
$$
$
$
$
$
$
$
$
(ANTIMALARIALS)
(MISCELLANEOUS ANTIPROTOZOALS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

10:00 Antineoplastic A
gents
10:00
Antineoplastic Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
METHOTREXATE
METHOTREXATE SODIUM
2.5 MG ORAL TABLET
10 MG ORAL TABLET
25 MG / ML (BASE) INJECTION
25 MG / ML (BASE) INJECTION
000021829630000224479800002170698
00002182750
0000209970500002182955
00002182777
APO-METHOTREXATERATIO-METHOTREXATE SODIUMMETHOTREXATE
METHOTREXATE
METHOTREXATE SOD.(UNPRESERVED)METHOTREXATE SOD.(UNPRESERVED)
METHOTREXATE SOD. (PRESERVED)
APXRPHWAY
HSP
TEVHSP
HSP
ANTINEOPLASTIC AGENTS10:00
10:00
0.6325 0.6325 0.6799
2.6894
4.3574 4.3574
8.9998
19 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$
$$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

12:00 Autonom
ic Drugs
12:00
Autonomic Drugs

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
NEOSTIGMINE BROMIDE
PILOCARPINE HCL
PYRIDOSTIGMINE BROMIDE
ATROPINE SULFATE
BELLADONNA/ ERGOTAMINE TARTRATE/ PHENOBARBITAL
DICYCLOMINE HCL
GLYCOPYRROLATE
HYOSCINE BUTYLBROMIDE
15 MG ORAL TABLET
5 MG ORAL TABLET
60 MG ORAL TABLET
180 MG ORAL SUSTAINED-RELEASE TABLET
0.4 MG / ML INJECTION
0.6 MG / ML INJECTION
0.2 MG * 0.6 MG * 40 MG ORAL SUSTAINED-RELEASE TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
2 MG / ML ORAL SYRUP
10 MG / ML INJECTION
0.2 MG / ML INJECTION
10 MG ORAL TABLET
20 MG / ML INJECTION
00000869945
00002216345
00000869961
00000869953
00000392782
00000392693
00000176141
00002103087
00002103095
00002102978
00000392812
00002039508
00000363812
00000363839
PROSTIGMIN
SALAGEN
MESTINON
MESTINON-SR
ATROPINE SULFATE
ATROPINE SULFATE
BELLERGAL SPACETABS
BENTYLOL
BENTYLOL
BENTYLOL
DICYCLOMINE HYDROCHLORIDE
GLYCOPYRROLATE
BUSCOPAN
BUSCOPAN
VCL
PFI
VCL
VCL
SDZ
SDZ
TPI
AXC
AXC
AXC
SDZ
SDZ
BOE
BOE
AUTONOMIC DRUGS
AUTONOMIC DRUGS
PARASYMPATHOMIMETIC (CHOLINERGIC) AGENTS
ANTICHOLINERGIC AGENTS
12
12
:00
:00
12:04
12:08.08
0.4904
1.1986
0.4820
1.0543
1.8300
1.9900
1.3812
0.1257
0.2373
0.0673
3.5900
3.7000
0.3222
4.3860
21 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$
$
$
$
(ANTIMUSCARINICS / ANTISPASMODICS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
IPRATROPIUM BROMIDE
IPRATROPIUM BROMIDE/ SALBUTAMOL SULFATE
TIOTROPIUM BROMIDE MONOHYDRATE
MIDODRINE HCL
BUDESONIDE/ FORMOTEROL FUMARATE DIHYDRATE
FORMOTEROL FUMARATE
20 MCG / DOSE METERED DOSE AEROSOL
250 MCG / ML INHALATION SOLUTION
0.03 % NASAL SPRAY
0.2 MG / ML * 1 MG / ML (BASE) INHALATION SOLUTION
18 MCG INHALATION CAPSULE
2.5 MG ORAL TABLET
5 MG ORAL TABLET
100 MCG / DOSE * 6 MCG / DOSE METERED INHALATION POWDER
200 MCG / DOSE * 6 MCG / DOSE METERED INHALATION POWDER
12 MCG INHALATION CAPSULE
00002247686
00002126222000022391310000221047900002231136
0000223962700002163705
000022726950000224378900002231675
00002246793
00002278677
00002278685
00002245385
00002245386
00002230898
ATROVENT HFA
APO-IPRAVENTMYLAN-IPRATROPIUMNOVO-IPRAMIDEPMS-IPRATROPIUM
PMS-IPRATROPIUMATROVENT
MYLAN-COMBO STERINEBSRATIO-IPRA SAL UDVCOMBIVENT UDV
SPIRIVA
MIDODRINE
MIDODRINE
SYMBICORT 100 TURBUHALER
SYMBICORT 200 TURBUHALER
FORADIL
BOE
APXMYPTEVPMS
PMSBOE
MYPRPHBOE
BOE
AAP
AAP
AZC
AZC
NOV
(SELECTIVE BETA 2-ADRENERGIC AGONISTS)
AUTONOMIC DRUGS
AUTONOMIC DRUGS
AUTONOMIC DRUGS
ANTICHOLINERGIC AGENTS
SYMPATHOMIMETIC (ADRENERGIC) AGENTS
SYMPATHOMIMETIC (ADRENERGIC) AGENTS
12
12
12
:00
:00
:00
12:08.08
12:12.04
12:12.08.12
0.0946
0.5530 0.5530 0.5530 0.5530
0.5561 0.9930
0.3377 0.3377 0.6030
2.1667
0.3631
0.6052
0.5599
0.7279
0.8795
22 EFFECTIVE APRIL 1, 2012
$
$$$$
$$
$$$
$
$
$
$
$
$
(ANTIMUSCARINICS / ANTISPASMODICS)
(ALPHA-ADRENERGIC AGONISTS)
BETA-ADRENERGIC AGONISTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FORMOTEROL FUMARATE DIHYDRATE
ORCIPRENALINE SULFATE
SALBUTAMOL
SALBUTAMOL SULFATE
SALMETEROL XINAFOATE
SALMETEROL XINAFOATE/ FLUTICASONE PROPIONATE
6 MCG / DOSE METERED INHALATION POWDER
12 MCG / DOSE METERED INHALATION POWDER
2 MG / ML ORAL SYRUP
100 MCG / DOSE METERED DOSE AEROSOL
2 MG (BASE) ORAL TABLET
4 MG (BASE) ORAL TABLET
0.5 MG / ML (BASE) INHALATION SOLUTION
1 MG / ML (BASE) INHALATION SOLUTION
5 MG / ML (BASE) INHALATION SOLUTION
2 MG / ML (BASE) INHALATION UNIT DOSE SOLUTION
50 MCG / DOSE (BASE) METERED INHALATION POWDER
50 MCG / DOSE (BASE) INHALATION DISK
25 MCG / DOSE (BASE) * 125 MCG / DOSE METERED DOSE AEROSOL
25 MCG / DOSE (BASE) * 250 MCG / DOSE METERED DOSE AEROSOL
00002237225
00002237224
00002236783
000022325700000224566900002241497
00002146843
00002146851
0000220824500002239365
00001926934000022082290000198686400002213419
00002069571000008608080000215441200002213486
00002173360000022082370000223936600002213427
00002231129
00002214261
00002245126
00002245127
OXEZE TURBUHALER
OXEZE TURBUHALER
APO-ORCIPRENALINE
AIROMIR CFC-FREEAPO-SALVENT CFC FREEVENTOLIN HFA
APO-SALVENT
APO-SALVENT
PMS-SALBUTAMOLRATIO-SALBUTAMOL UNIT DOSE P.F
MYLAN-SALBUTAMOL STERINEBS P.F.PMS-SALBUTAMOLRATIO-SALBUTAMOL SULF U.D.P.F.VENTOLIN NEBULES P.F.
PMS-SALBUTAMOLRATIO-SALBUTAMOLSANDOZ SALBUTAMOLVENTOLIN
MYLAN-SALBUTAMOL STERINEBS P.F.PMS-SALBUTAMOL POLYNEBRATIO-SALBUTAMOL UNI DOSE P.F.VENTOLIN NEBULES P.F.
SEREVENT DISKUS
SEREVENT
ADVAIR 125
ADVAIR 250
AZC
AZC
APX
MEPAPXGSK
APX
APX
PMSRPH
MYPPMSRPHGSK
PMSRPHSDZGSK
MYPPMSRPHGSK
GSK
GSK
GSK
GSK
(SELECTIVE BETA 2-ADRENERGIC AGONISTS)
AUTONOMIC DRUGS
SYMPATHOMIMETIC (ADRENERGIC) AGENTS
12:00
12:12.08.12
0.5956
0.7934
0.0574
0.0269 0.0325 0.0325
0.1274
0.2134
0.1492 0.1492
0.2434 0.2434 0.2434 0.4444
0.5900 0.5900 0.5900 1.0782
0.4622 0.4622 0.4622 0.8441
1.0051
4.0205
0.8599
1.2208
23 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$$$
$
$
$$
$$$$
$$$$
$$$$
$
$
$
$
BETA-ADRENERGIC AGONISTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SALMETEROL XINAFOATE/ FLUTICASONE PROPIONATE
TERBUTALINE SULFATE
EPINEPHRINE
EPINEPHRINE HCL
DIHYDROERGOTAMINE MESYLATE
ERGOLOID MESYLATES
ERGOTAMINE TARTRATE/ CAFFEINE
50 MCG / DOSE (BASE) * 100 MCG / DOSE METERED INHALATION POWDER
50 MCG / DOSE (BASE) * 250 MCG / DOSE METERED INHALATION POWDER
50 MCG / DOSE (BASE) * 500 MCG / DOSE METERED INHALATION POWDER
0.5 MG / DOSE METERED INHALATION POWDER
0.15 MG / SYR INJECTION SYRINGE
0.3 MG / SYR INJECTION SYRINGE
1 MG / ML INJECTION
4 MG / ML NASAL SPRAY
1 MG / ML INJECTION
1 MG ORAL TABLET
1 MG * 100 MG ORAL TABLET
00002240835
00002240836
00002240837
00000786616
0000226820500000578657
0000224731000000509558
00000155357
00002228947
0000224116300000027243
00000176176
00000176095
ADVAIR 100 DISKUS
ADVAIR 250 DISKUS
ADVAIR 500 DISKUS
BRICANYL TURBUHALER
TWINJECT AUTO INJECTOREPIPEN JR
TWINJECT AUTO INJECTOREPIPEN
ADRENALIN
MIGRANAL
DIHYDROERGOTAMINE MESYLATEDIHYDROERGOTAMINE (DHE)
HYDERGINE
CAFERGOT
GSK
GSK
GSK
AZC
PALKNG
PALKNG
ERF
STM
SDZSTM
STM
NOV
(SELECTIVE BETA 2-ADRENERGIC AGONISTS)
AUTONOMIC DRUGS
AUTONOMIC DRUGS
AUTONOMIC DRUGS
SYMPATHOMIMETIC (ADRENERGIC) AGENTS
SYMPATHOMIMETIC (ADRENERGIC) AGENTS
SYMPATHOLYTIC (ADRENERGIC BLOCKING) AGENTS
12
12
12
:00
:00
:00
12:12.08.12
12:12.12
12:16
1.4367
1.7198
2.4415
0.0821
82.4580 88.8165
82.4580 88.8165
0.6048
10.9696
3.7933 4.1076
1.0781
0.8907
24 EFFECTIVE APRIL 1, 2012
$
$
$
$
$$
$$
$
$
$$
$
$
BETA-ADRENERGIC AGONISTS
(ALPHA- AND BETA-ADRENERGIC AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CYCLOBENZAPRINE HCL
DANTROLENE SODIUM
BACLOFEN
10 MG ORAL TABLET
25 MG ORAL CAPSULE
100 MG ORAL CAPSULE
10 MG ORAL TABLET
20 MG ORAL TABLET
0.05 MG / ML INJECTION
0.5 MG / ML INJECTION
000021771450000228706400002231353000020800520000217184800002212048
00001997602
00001997653
000021393320000237141300002287021000020883980000213609000002236963000020637350000223650700000455881
000021393910000237142100002287048000020884010000213610400002236964000020637430000223650800000636576
00002131048
00002131056
APO-CYCLOBENZAPRINECYCLOBENZAPRINEMYLAN-CYCLOBENZAPRINENOVO-CYCLOPRINENU-CYCLOBENZAPRINEPMS-CYCLOBENZAPRINE
DANTRIUM
DANTRIUM
APO-BACLOFENAVA-BACLOFENBACLOFENMYLAN-BACLOFENNU-BACLOPHL-BACLOFENPMS-BACLOFENRATIO-BACLOFENLIORESAL
APO-BACLOFENAVA-BACLOFENBACLOFENMYLAN-BACLOFENNU-BACLOPHL-BACLOFENPMS-BACLOFENRATIO-BACLOFENLIORESAL D.S.
LIORESAL INTRATHECAL
LIORESAL INTRATHECAL
APXSNSMYPTEVNXPPMS
JHP
JHP
APXAVASNSMYPNXPPHHPMSRPHNOV
APXAVASNSMYPNXPPHHPMSRPHNOV
NOV
NOV
AUTONOMIC DRUGS
AUTONOMIC DRUGS
AUTONOMIC DRUGS
SKELETAL MUSCLE RELAXANTS
SKELETAL MUSCLE RELAXANTS
SKELETAL MUSCLE RELAXANTS
12
12
12
:00
:00
:00
12:20.04
12:20.08
12:20.12
0.3731 0.3731 0.3731 0.3731 0.3731 0.3731
0.3780
0.7684
0.2911 0.2911 0.2911 0.2911 0.2911 0.2911 0.2911 0.2911 0.7190
0.5667 0.5667 0.5667 0.5667 0.5667 0.5667 0.5667 0.5667 1.3994
14.8648
11.1381
25 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$
$
$
$$$$$$$$$
$$$$$$$$$
$
$
RESTRICTED BENEFIT - Coverage is limited to 126 tablets per plan participant per year as anadjunct to rest and physical therapy for the treatment of acute muscle spasm.
(CENTRALLY ACTING SKELETAL MUSCLE RELAXANTS)
(DIRECT-ACTING SKELETAL MUSCLE RELAXANTS)
(GABA-DERIVATIVE SKELETAL MUSCLE RELAXANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
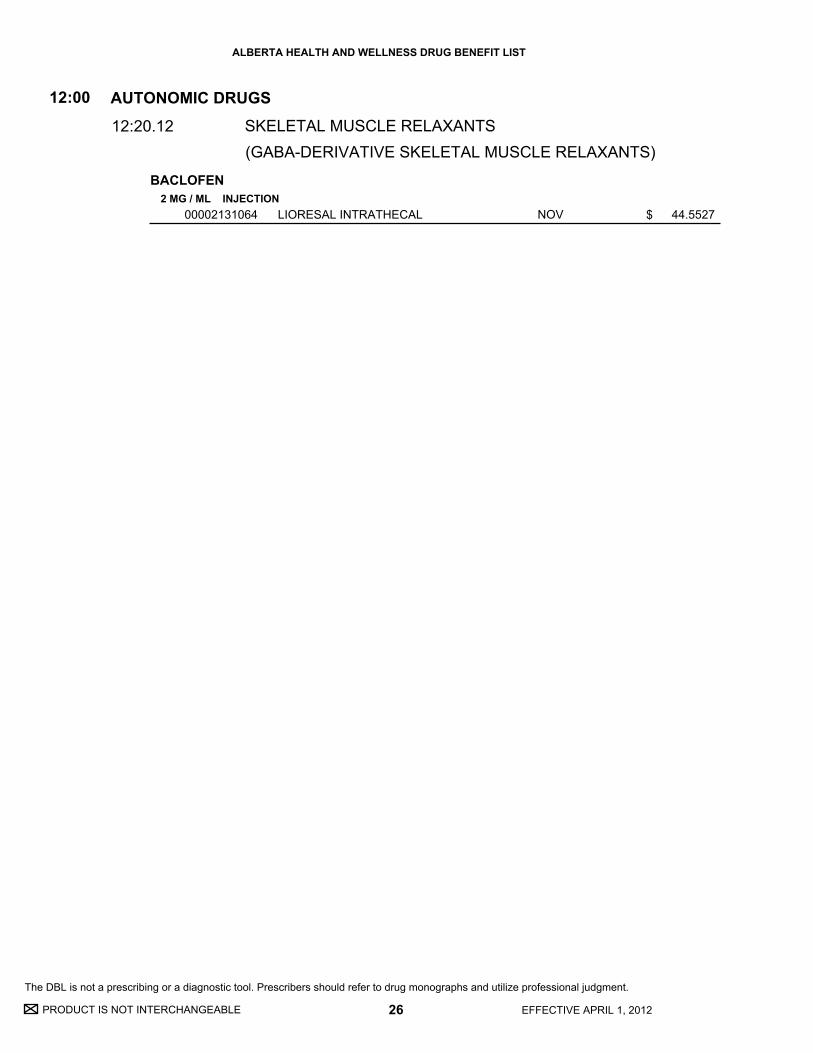
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
BACLOFEN2 MG / ML INJECTION
00002131064 LIORESAL INTRATHECAL NOV
AUTONOMIC DRUGS
SKELETAL MUSCLE RELAXANTS
12:00
12:20.12
44.5527
26 EFFECTIVE APRIL 1, 2012
$
(GABA-DERIVATIVE SKELETAL MUSCLE RELAXANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

20:00 Blood Form
ation, Coagulation and Throm
bosis
20:00
Blood Formation, Coagulation and Thrombosis

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
IRON DEXTRAN COMPLEX
ACENOCOUMAROL
WARFARIN SODIUM
50 MG / ML INJECTION
1 MG ORAL TABLET
4 MG ORAL TABLET
1 MG ORAL TABLET
2 MG ORAL TABLET
2.5 MG ORAL TABLET
3 MG ORAL TABLET
0000220596300002221780
00000010383
00000010391
000022429240000224446200002265273000022426800000234402500001918311
000022429250000224446300002265281000022426810000234403300001918338
000022429260000224446400002265303000022426820000234404100001918346
000022456180000228749800002265311000022426830000234406800002240205
DEXIRONINFUFER
SINTROM
SINTROM
APO-WARFARINMYLAN-WARFARINNOVO-WARFARINTARO-WARFARINWARFARINCOUMADIN
APO-WARFARINMYLAN-WARFARINNOVO-WARFARINTARO-WARFARINWARFARINCOUMADIN
APO-WARFARINMYLAN-WARFARINNOVO-WARFARINTARO-WARFARINWARFARINCOUMADIN
APO-WARFARINMYLAN-WARFARINNOVO-WARFARINTARO-WARFARINWARFARINCOUMADIN
MYPSDZ
PAL
PAL
APXMYPTEVTARSNSBMS
APXMYPTEVTARSNSBMS
APXMYPTEVTARSNSBMS
APXMYPTEVTARSNSBMS
(COUMARIN DERIVATIVES)
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
ANTIANEMIA DRUGS
ANTITHROMBOTIC AGENTS
20
20
:00
:00
20:04.04
20:12.04.08
14.7812 14.8253
0.5087
1.5997
0.1747 0.1747 0.1747 0.1747 0.1747 0.3277
0.1847 0.1847 0.1847 0.1847 0.1847 0.3467
0.1479 0.1479 0.1479 0.1479 0.1479 0.2775
0.2290 0.2290 0.2290 0.2290 0.2290 0.4297
27 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$
$$$$$$
$$$$$$
$$$$$$
$$$$$$
(IRON PREPARATIONS)
ANTICOAGULANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
WARFARIN SODIUM
DALTEPARIN SODIUM
4 MG ORAL TABLET
5 MG ORAL TABLET
6 MG ORAL TABLET
7.5 MG ORAL TABLET
10 MG ORAL TABLET
10,000 IU / ML INJECTION
25,000 IU / ML INJECTION
2,500 IU / SYR INJECTION SYRINGE
5,000 IU / SYR INJECTION SYRINGE
7,500 IU / SYR INJECTION SYRINGE
10,000 IU / SYR INJECTION SYRINGE
12,500 IU / SYR INJECTION SYRINGE
15,000 IU / SYR INJECTION SYRINGE
000022429270000224446500002265338000022426840000234407600002007959
000022429280000224446600002265346000022426850000234408400001918354
00002242686
00002242697
0000224292900002244467000022426870000234411400001918362
00002132664
00002231171
00002132621
00002132648
00002352648
00002352656
00002352664
00002352672
APO-WARFARINMYLAN-WARFARINNOVO-WARFARINTARO-WARFARINWARFARINCOUMADIN
APO-WARFARINMYLAN-WARFARINNOVO-WARFARINTARO-WARFARINWARFARINCOUMADIN
TARO-WARFARIN
TARO-WARFARIN
APO-WARFARINMYLAN-WARFARINTARO-WARFARINWARFARINCOUMADIN
FRAGMIN
FRAGMIN
FRAGMIN (0.2 ML SYRINGE)
FRAGMIN (0.2 ML SYRINGE)
FRAGMIN (0.3 ML SYRINGE)
FRAGMIN (0.4 ML SYRINGE)
FRAGMIN (0.5 ML SYRINGE)
FRAGMIN (0.6 ML SYRINGE)
APXMYPTEVTARSNSBMS
APXMYPTEVTARSNSBMS
TAR
TAR
APXMYPTARSNSBMS
PFI
PFI
PFI
PFI
PFI
PFI
PFI
PFI
(COUMARIN DERIVATIVES)
(HEPARINS)
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
ANTITHROMBOTIC AGENTS
ANTITHROMBOTIC AGENTS
20
20
:00
:00
20:12.04.08
20:12.04.16
0.2290 0.2290 0.2290 0.2290 0.2290 0.4297
0.1482 0.1482 0.1482 0.1482 0.1482 0.2780
0.3040
0.3267
0.2659 0.2659 0.2659 0.2659 0.4989
17.1238
42.8064
5.4223
10.8446
16.2669
21.6892
27.1115
32.5338
28 EFFECTIVE APRIL 1, 2012
$$$$$$
$$$$$$
$
$
$$$$$
$
$
$
$
$
$
$
$
ANTICOAGULANTS
ANTICOAGULANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DALTEPARIN SODIUM
ENOXAPARIN SODIUM
HEPARIN SODIUM
NADROPARIN CALCIUM
TINZAPARIN SODIUM
18,000 IU / SYR INJECTION SYRINGE
100 MG / ML INJECTION
30 MG / SYR INJECTION SYRINGE
100 MG / ML INJECTION SYRINGE
150 MG / ML INJECTION SYRINGE
1,000 UNIT / ML INJECTION
10,000 UNIT / ML INJECTION
25,000 UNIT / ML INJECTION
10 UNIT / ML INJECTION LOCK FLUSH
100 UNIT / ML INJECTION LOCK FLUSH
9,500 IU / ML INJECTION SYRINGE
19,000 IU / ML INJECTION SYRINGE
10,000 IU / ML INJECTION
20,000 IU / ML INJECTION
2,500 IU / SYR INJECTION SYRINGE
3,500 IU / SYR INJECTION SYRINGE
4,500 IU / SYR INJECTION SYRINGE
10,000 IU / SYR INJECTION SYRINGE
00002352680
00002236564
00002012472
00002236883
00002242692
00000453811
00000579718
00000453781
00000725323
0000072531500000727520
00002236913
00002240114
00002167840
00002229515
00002229755
00002358158
00002358166
00002231478
FRAGMIN (0.72 ML SYRINGE)
LOVENOX
LOVENOX (0.3 ML SYRINGE)
LOVENOX (0.4 - 1 ML SYRINGE)
LOVENOX HP (0.8ML/1ML SYRINGE)
HEPARIN LEO
HEPARIN LEO
HEPARIN LEO
HEPARIN LOCK FLUSH
HEPARIN LOCK FLUSHHEPARIN LEO
FRAXIPARINE (.3-1ML SYR)
FRAXIPARINE FORTE (.6-1ML SYR)
INNOHEP
INNOHEP
INNOHEP (0.25 ML SYRINGE)
INNOHEP (0.35 ML SYRINGE)
INNOHEP (0.45 ML SYRINGE)
INNOHEP (0.5 ML SYRINGE)
PFI
SAV
SAV
SAV
SAV
LEO
LEO
LEO
HSP
HSPLEO
GSK
GSK
LEO
LEO
LEO
LEO
LEO
LEO
(HEPARINS)
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
ANTITHROMBOTIC AGENTS
20:00
20:12.04.16
39.0397
22.4998
6.7940
22.5008
33.7507
0.5545
2.7596
8.8317
0.3094
0.3120 0.4716
9.8137
19.6274
18.0174
36.5978
18.1750
18.1621
18.1675
37.0937
29 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
For this product - pricing has been established on a per millilitre basis.
For this product - pricing has been established on a per millilitre basis.
For this product - pricing has been established on a per millilitre basis.
For this product - pricing has been established on a per millilitre basis.
For this product - pricing has been established on a per millilitre basis.
$
$
$
$
$
$
$
$
$
$$
$
$
$
$
$
$
$
$
ANTICOAGULANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TINZAPARIN SODIUM
FONDAPARINUX SODIUM
RIVAROXABAN
DIPYRIDAMOLE/ ASA
TICLOPIDINE HCL
14,000 IU / SYR INJECTION SYRINGE
18,000 IU / SYR INJECTION SYRINGE
2.5 MG / SYR INJECTION SYRINGE
7.5 MG / SYR INJECTION SYRINGE
10 MG ORAL TABLET
200 MG * 25 MG ORAL CAPSULE
250 MG ORAL TABLET
00002358174
00002358182
00002245531
00002258056
00002316986
00002242119
000022377010000223974400002236848000022375600000224358700002343045
INNOHEP (0.7 ML SYRINGE)
INNOHEP (0.9 ML SYRINGE)
ARIXTRA (0.5 ML SYRINGE)
ARIXTRA (0.6 ML SYRINGE)
XARELTO
AGGRENOX
APO-TICLOPIDINEMYLAN-TICLOPIDINENOVO-TICLOPIDINENU-TICLOPIDINESANDOZ TICLOPIDINETICLOPIDINE
LEO
LEO
GSK
GSK
BAI
BOE
APXMYPTEVNXPSDZSNS
(HEPARINS)
(MISCELLANEOUS ANTICOAGULANTS)
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
ANTITHROMBOTIC AGENTS
ANTITHROMBOTIC AGENTS
ANTITHROMBOTIC AGENTS
20
20
20
:00
:00
:00
20:12.04.16
20:12.04.92
20:12.18
37.1158
37.1108
16.9378
27.4394
9.5243
0.8492
0.6885 0.6885 0.6885 0.6885 0.6885 0.6885
30 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$$$$$$
RESTRICTED BENEFIT - This product is a benefit for the prophylaxis of venous thromboembolic events in patients who have undergone elective total hip replacement or total knee replacement surgery. Coverage is restricted to two 14-day courses of therapy per patientper year.
ANTICOAGULANTS
ANTICOAGULANTS
(PLATELET AGGREGATION INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PENTOXIFYLLINE
TRANEXAMIC ACID
400 MG ORAL SUSTAINED-RELEASE TABLET
500 MG ORAL TABLET
0000223009000002221977
00002064405
APO-PENTOXIFYLLINE SRTRENTAL
CYKLOKAPRON
APXSAV
PFI
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
BLOOD FORMULATION, COAGULATION AND THROMBOSIS
HEMORRHEOLOGIC AGENTS
ANTIHEMORRHAGIC AGENTS
20
20
:00
:00
20:24
20:28.16
0.5846 0.8704
1.2395
31 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
(HEMOSTATICS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

24:00 Cardiovascular D
rugs
24:00
Cardiovascular Drugs

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DISOPYRAMIDE
PROCAINAMIDE HCL
MEXILETINE HCL
FLECAINIDE ACETATE
PROPAFENONE HCL
100 MG ORAL CAPSULE
150 MG ORAL CAPSULE
250 MG ORAL SUSTAINED-RELEASE TABLET
500 MG ORAL SUSTAINED-RELEASE TABLET
750 MG ORAL SUSTAINED-RELEASE TABLET
100 MG ORAL CAPSULE
200 MG ORAL CAPSULE
50 MG ORAL TABLET
100 MG ORAL TABLET
150 MG ORAL TABLET
300 MG ORAL TABLET
00002224801
00002224828
00000638692
00000638676
00000638684
00002230359
00002230360
0000227553800001966197
0000227554600001966200
0000224332400000603708
0000224332500000603716
RYTHMODAN
RYTHMODAN
PROCAN SR
PROCAN SR
PROCAN SR
NOVO-MEXILETINE
NOVO-MEXILETINE
FLECAINIDETAMBOCOR
FLECAINIDETAMBOCOR
APO-PROPAFENONERYTHMOL
APO-PROPAFENONERYTHMOL
SAV
SAV
ERF
ERF
ERF
TEV
TEV
AAPMEP
AAPMEP
APXABB
APXABB
(CLASS IA ANTIARRYTHMICS)
(CLASS IB ANTIARRYTHMICS)
(CLASS IC ANTIARRYTHMICS)
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
CARDIAC DRUGS
CARDIAC DRUGS
CARDIAC DRUGS
24
24
24
:00
:00
:00
24:04.04.04
24:04.04.08
24:04.04.12
0.2918
0.4218
0.3951
0.5445
0.8767
1.0203
1.3663
0.3956 0.5788
0.7912 1.1578
0.4275 1.1834
0.7537 2.0859
33 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$$
$$
$$
$$
ANTIARRHYTHMIC AGENTS
ANTIARRHYTHMIC AGENTS
ANTIARRHYTHMIC AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
AMIODARONE HCL
DIGOXIN
CHOLESTYRAMINE RESIN
COLESTIPOL HCL
100 MG ORAL TABLET
200 MG ORAL TABLET
0.0625 MG ORAL TABLET
0.125 MG ORAL TABLET
0.25 MG ORAL TABLET
0.05 MG / ML ORAL ELIXIR
0.05 MG / ML INJECTION
0.25 MG / ML INJECTION
4 G ORAL POWDER PACKET
1 G ORAL TABLET
5 G ORAL POWDER PACKET
00002292173
000023643360000224619400002364263000022406040000223983500002242472000022400710000224383600002036282
00002335700
00002335719
00002335727
00002242320
00002048272
00002048264
0000089096000002210320
00002132680
0000064297500002132699
PMS-AMIODARONE
AMIODARONEAPO-AMIODARONEAVA-AMIODARONEMYLAN-AMIODARONENOVO-AMIODARONEPMS-AMIODARONERATIO-AMIODARONESANDOZ AMIODARONECORDARONE
TOLOXIN
TOLOXIN
TOLOXIN
TOLOXIN PEDIATRIC
DIGOXIN PEDIATRIC
DIGOXIN
OLESTYR LIGHTOLESTYR REGULAR
COLESTID
COLESTIDCOLESTID ORANGE
PMS
SNSAPXAVAMYPTEVPMSRPHSDZWAY
MMT
MMT
MMT
MMT
SDZ
SDZ
MMTMMT
PFI
PFIPFI
(CLASS III ANTIARRYTHMICS)
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
CARDIAC DRUGS
CARDIAC DRUGS
ANTILIPEMIC AGENTS
24
24
24
:00
:00
:00
24:04.04.20
24:04.08
24:06.04
0.7269
1.2394 1.2394 1.2394 1.2394 1.2394 1.2394 1.2394 1.2394 2.2133
0.2705
0.2705
0.2705
1.1192
7.7700
3.1300
1.4900 1.4900
0.2769
0.9902 0.9902
34 EFFECTIVE APRIL 1, 2012
$
$$$$$$$$$
$
$
$
$
$
$
$$
$
$$
ANTIARRHYTHMIC AGENTS
(CARDIOTONIC AGENTS)
(BILE ACID SEQUESTRANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
BEZAFIBRATE
FENOFIBRATE
GEMFIBROZIL
400 MG ORAL SUSTAINED-RELEASE TABLET
100 MG ORAL TABLET
67 MG ORAL CAPSULE
100 MG ORAL CAPSULE
200 MG ORAL CAPSULE
160 MG ORAL CAPSULE/TABLET
600 MG ORAL TABLET
300 MG ORAL CAPSULE
00002083523
0000224685900002356570000022890830000228804400002241601
0000224318000002243551
00002225980
0000223986400002364409000022860920000214695900002240210000022435520000227355100002250039
0000224686000002356589000022890910000228805200002241602
0000197958200002230476000021420740000205846400002230183
0000197957400002185407000022417040000205845600002239951
BEZALIP
APO-FENO-SUPERFENOFIBRATE-SNOVO-FENOFIBRATE-SSANDOZ FENOFIBRATE SLIPIDIL SUPRA
APO-FENO-MICRONOVO-FENOFIBRATE MICRONIZED
APO-FENOFIBRATE
APO-FENO-MICROAVA-FENOFIBRATE MICROFENOFIBRATE MICROLIPIDIL MICROMYLAN-FENOFIBRATE MICRONOVO-FENOFIBRATE MICRONIZEDPMS-FENOFIBRATE MICRORATIO-FENOFIBRATE MC
APO-FENO-SUPER (TABLET)FENOFIBRATE-S (TABLET)NOVO-FENOFIBRATE-S (TABLET)SANDOZ FENOFIBRATE S (TABLET)LIPIDIL SUPRA (TABLET)
APO-GEMFIBROZILMYLAN-GEMFIBROZILNOVO-GEMFIBROZILNU-GEMFIBROZILPMS-GEMFIBROZIL
APO-GEMFIBROZILMYLAN-GEMFIBROZILNOVO-GEMFIBROZILNU-GEMFIBROZILPMS-GEMFIBROZIL
ACV
APXSNSTEVSDZFAB
APXTEV
APX
APXAVASNSFABMYPTEVPMSRPH
APXSNSTEVSDZFAB
APXMYPTEVNXPPMS
APXMYPTEVNXPPMS
CARDIOVASCULAR DRUGS
ANTILIPEMIC AGENTS
24:00
24:06.06
1.9639
0.6511 0.6511 0.6511 0.6511 1.1130
0.4325 0.4325
0.6105
1.0890 1.0890 1.0890 1.0890 1.0890 1.0890 1.0890 1.0890
0.7502 0.7502 0.7502 0.7502 1.2823
0.6208 0.6208 0.6208 0.6208 0.6208
0.2964 0.2964 0.2964 0.2964 0.2964
35 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$$$
$$
$
$$$$$$$$
$$$$$
$$$$$
$$$$$
(FIBRIC ACID DERIVATIVES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ATORVASTATIN CALCIUM10 MG (BASE) ORAL TABLET
20 MG (BASE) ORAL TABLET
40 MG (BASE) ORAL TABLET
80 MG (BASE) ORAL TABLET
0000234870500002310899000022883460000237320300002302675000023137070000235029700002295261000023134480000232494600002230711
0000229528800002348713000023109020000228835400002373211000023026830000231345600002313715000023503190000232495400002230713
0000234872100002310910000022883620000237323800002302691000023137230000235032700002295296000023134640000232496200002230714
0000234874800002310929000022883700000237324600002302713000023137580000235033500002295318000023134720000232497000002243097
ATORVASTATINCO ATORVASTATINGD-ATORVASTATINMYLAN-ATORVASTATINNOVO-ATORVASTATINRAN-ATORVASTATINRATIO-ATORVASTATINAPO-ATORVASTATINPMS-ATORVASTATINSANDOZ ATORVASTATINLIPITOR
APO-ATORVASTATINATORVASTATINCO ATORVASTATINGD-ATORVASTATINMYLAN-ATORVASTATINNOVO-ATORVASTATINPMS-ATORVASTATINRAN-ATORVASTATINRATIO-ATORVASTATINSANDOZ ATORVASTATINLIPITOR
ATORVASTATINCO ATORVASTATINGD-ATORVASTATINMYLAN-ATORVASTATINNOVO-ATORVASTATINRAN-ATORVASTATINRATIO-ATORVASTATINAPO-ATORVASTATINPMS-ATORVASTATINSANDOZ ATORVASTATINLIPITOR
ATORVASTATINCO ATORVASTATINGD-ATORVASTATINMYLAN-ATORVASTATINNOVO-ATORVASTATINRAN-ATORVASTATINRATIO-ATORVASTATINAPO-ATORVASTATINPMS-ATORVASTATINSANDOZ ATORVASTATINLIPITOR
SNSCOBGMDMYPTEVRANRPHAPXPMSSDZPFI
APXSNSCOBGMDMYPTEVPMSRANRPHSDZPFI
SNSCOBGMDMYPTEVRANRPHAPXPMSSDZPFI
SNSCOBGMDMYPTEVRANRPHAPXPMSSDZPFI
CARDIOVASCULAR DRUGS
ANTILIPEMIC AGENTS
24:00
24:06.08
0.8049 0.8049 0.8049 0.8049 0.8049 0.8049 0.8049 0.8050 0.8050 0.8050 1.8738
1.0062 1.0062 1.0062 1.0062 1.0062 1.0062 1.0062 1.0062 1.0062 1.0062 2.3422
1.0816 1.0816 1.0816 1.0816 1.0816 1.0816 1.0816 1.0817 1.0817 1.0817 2.5176
1.0816 1.0816 1.0816 1.0816 1.0816 1.0816 1.0816 1.0817 1.0817 1.0817 2.5178
36 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$
$$$$$$$$$$$
$$$$$$$$$$$
$$$$$$$$$$$
(HMG-COA REDUCTASE INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FLUVASTATIN SODIUM
LOVASTATIN
80 MG (BASE) ORAL EXTENDED-RELEASE TABLET
20 MG (BASE) ORAL CAPSULE
40 MG (BASE) ORAL CAPSULE
20 MG ORAL TABLET
40 MG ORAL TABLET
00002250527
00002061562
00002061570
00002220172000023642390000224857200002353229000022431270000224654200002246013000022458220000224705600000795860
00002220180000023642470000224857300002353237000022431290000224654300002246014000022458230000224705700000795852
LESCOL XL
LESCOL
LESCOL
APO-LOVASTATINAVA-LOVASTATINCO LOVASTATINLOVASTATINMYLAN-LOVASTATINNOVO-LOVASTATINPMS-LOVASTATINRATIO-LOVASTATINSANDOZ LOVASTATINMEVACOR
APO-LOVASTATINAVA-LOVASTATINCO LOVASTATINLOVASTATINMYLAN-LOVASTATINNOVO-LOVASTATINPMS-LOVASTATINRATIO-LOVASTATINSANDOZ LOVASTATINMEVACOR
NOV
NOV
NOV
APXAVACOBSNSMYPTEVPMSRPHSDZMFC
APXAVACOBSNSMYPTEVPMSRPHSDZMFC
CARDIOVASCULAR DRUGS
ANTILIPEMIC AGENTS
24:00
24:06.08
1.5863
0.9387
1.3181
1.0907 1.0907 1.0907 1.0907 1.0907 1.0907 1.0907 1.0907 1.0907 2.0609
2.0117 2.0117 2.0117 2.0117 2.0117 2.0117 2.0117 2.0117 2.0117 3.7647
37 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$$$$$$$$$$
$$$$$$$$$$
(HMG-COA REDUCTASE INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PRAVASTATIN SODIUM
ROSUVASTATIN CALCIUM
10 MG ORAL TABLET
20 MG ORAL TABLET
40 MG ORAL TABLET
5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
20 MG (BASE) ORAL TABLET
40 MG (BASE) ORAL TABLET
000022435060000224818200002330954000023174510000225709200002247008000022476550000089374900002332191000023565460000228442100002247856
000022435070000224818300002330962000023174780000225710600002247009000022476560000089375700002332205000023565540000228444800002247857
000022435080000224818400002330970000023174860000225711400002247010000022476570000222205100002332213000023565620000228445600002247858
00002265540
00002247162
00002247163
00002247164
APO-PRAVASTATINCO PRAVASTATINJAMP-PRAVASTATINMINT-PRAVASTATINMYLAN-PRAVASTATINNOVO-PRAVASTATINPMS-PRAVASTATINPRAVACHOLPRAVASTATINPRAVASTATINRAN-PRAVASTATINSANDOZ PRAVASTATIN
APO-PRAVASTATINCO PRAVASTATINJAMP-PRAVASTATINMINT-PRAVASTATINMYLAN-PRAVASTATINNOVO-PRAVASTATINPMS-PRAVASTATINPRAVACHOLPRAVASTATINPRAVASTATINRAN-PRAVASTATINSANDOZ PRAVASTATIN
APO-PRAVASTATINCO PRAVASTATINJAMP-PRAVASTATINMINT-PRAVASTATINMYLAN-PRAVASTATINNOVO-PRAVASTATINPMS-PRAVASTATINPRAVACHOLPRAVASTATINPRAVASTATINRAN-PRAVASTATINSANDOZ PRAVASTATIN
CRESTOR
CRESTOR
CRESTOR
CRESTOR
APXCOBJPCMPIMYPTEVPMSBMSRANSNSRANSDZ
APXCOBJPCMPIMYPTEVPMSBMSRANSNSRANSDZ
APXCOBJPCMPIMYPTEVPMSBMSRANSNSRANSDZ
AZC
AZC
AZC
AZC
CARDIOVASCULAR DRUGS
ANTILIPEMIC AGENTS
24:00
24:06.08
0.9530 0.9530 0.9530 0.9530 0.9530 0.9530 0.9530 0.9530 0.9530 0.9530 0.9530 0.9530
1.1243 1.1243 1.1243 1.1243 1.1243 1.1243 1.1243 1.1243 1.1243 1.1243 1.1243 1.1243
1.3543 1.3543 1.3543 1.3543 1.3543 1.3543 1.3543 1.3543 1.3543 1.3543 1.3543 1.3543
1.3868
1.4620
1.8275
2.1392
38 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$
$$$$$$$$$$$$
$$$$$$$$$$$$
$
$
$
$
(HMG-COA REDUCTASE INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
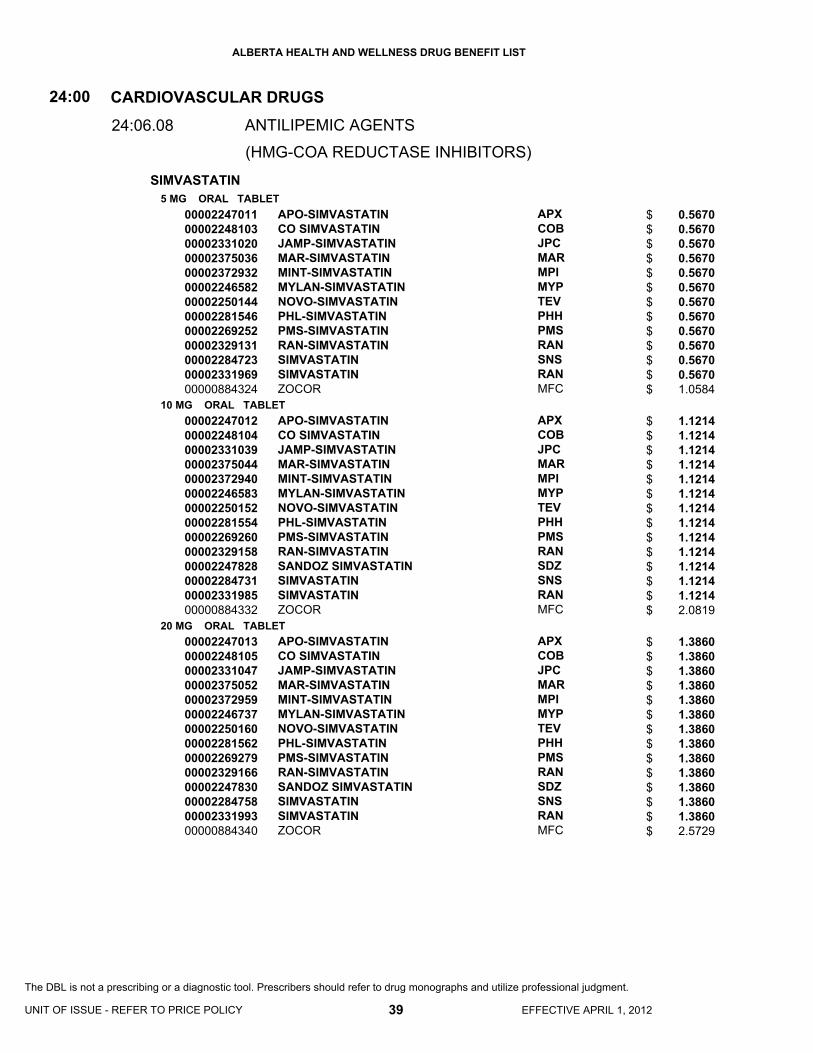
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SIMVASTATIN5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
00002247011000022481030000233102000002375036000023729320000224658200002250144000022815460000226925200002329131000022847230000233196900000884324
0000224701200002248104000023310390000237504400002372940000022465830000225015200002281554000022692600000232915800002247828000022847310000233198500000884332
0000224701300002248105000023310470000237505200002372959000022467370000225016000002281562000022692790000232916600002247830000022847580000233199300000884340
APO-SIMVASTATINCO SIMVASTATINJAMP-SIMVASTATINMAR-SIMVASTATINMINT-SIMVASTATINMYLAN-SIMVASTATINNOVO-SIMVASTATINPHL-SIMVASTATINPMS-SIMVASTATINRAN-SIMVASTATINSIMVASTATINSIMVASTATINZOCOR
APO-SIMVASTATINCO SIMVASTATINJAMP-SIMVASTATINMAR-SIMVASTATINMINT-SIMVASTATINMYLAN-SIMVASTATINNOVO-SIMVASTATINPHL-SIMVASTATINPMS-SIMVASTATINRAN-SIMVASTATINSANDOZ SIMVASTATINSIMVASTATINSIMVASTATINZOCOR
APO-SIMVASTATINCO SIMVASTATINJAMP-SIMVASTATINMAR-SIMVASTATINMINT-SIMVASTATINMYLAN-SIMVASTATINNOVO-SIMVASTATINPHL-SIMVASTATINPMS-SIMVASTATINRAN-SIMVASTATINSANDOZ SIMVASTATINSIMVASTATINSIMVASTATINZOCOR
APXCOBJPCMARMPIMYPTEVPHHPMSRANSNSRANMFC
APXCOBJPCMARMPIMYPTEVPHHPMSRANSDZSNSRANMFC
APXCOBJPCMARMPIMYPTEVPHHPMSRANSDZSNSRANMFC
CARDIOVASCULAR DRUGS
ANTILIPEMIC AGENTS
24:00
24:06.08
0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 0.5670 1.0584
1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 1.1214 2.0819
1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 2.5729
39 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$$
$$$$$$$$$$$$$$
$$$$$$$$$$$$$$
(HMG-COA REDUCTASE INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
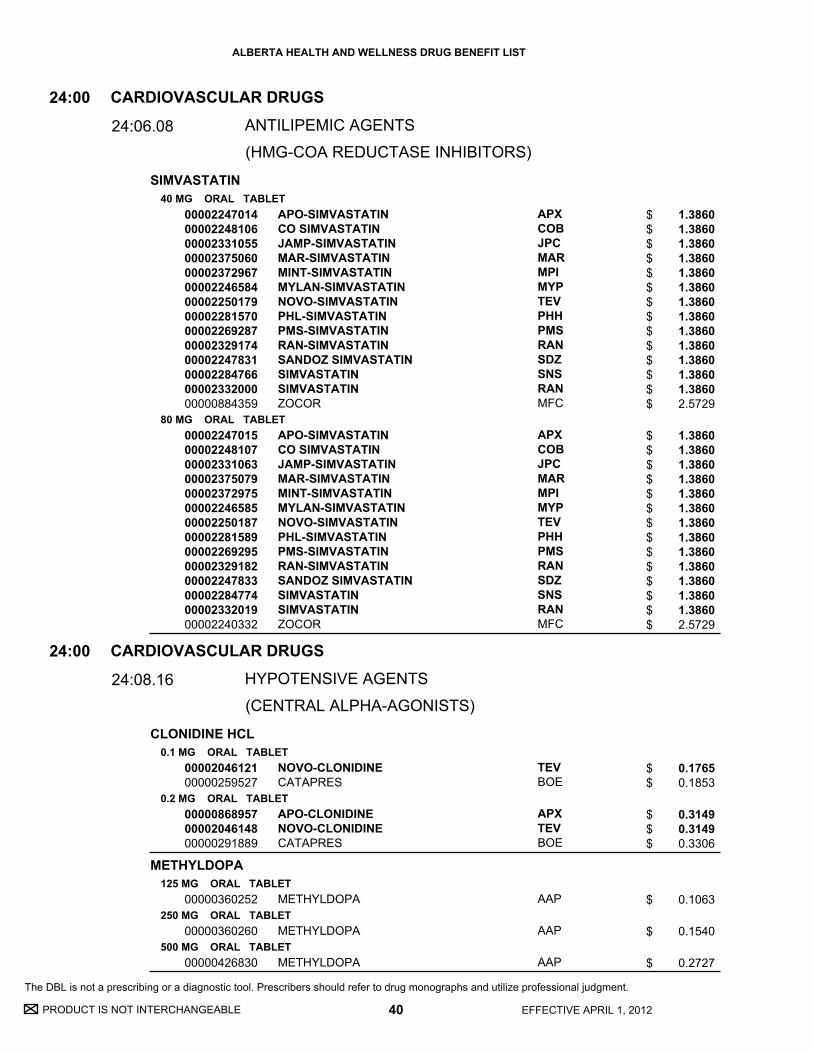
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SIMVASTATIN
CLONIDINE HCL
METHYLDOPA
40 MG ORAL TABLET
80 MG ORAL TABLET
0.1 MG ORAL TABLET
0.2 MG ORAL TABLET
125 MG ORAL TABLET
250 MG ORAL TABLET
500 MG ORAL TABLET
0000224701400002248106000023310550000237506000002372967000022465840000225017900002281570000022692870000232917400002247831000022847660000233200000000884359
0000224701500002248107000023310630000237507900002372975000022465850000225018700002281589000022692950000232918200002247833000022847740000233201900002240332
0000204612100000259527
000008689570000204614800000291889
00000360252
00000360260
00000426830
APO-SIMVASTATINCO SIMVASTATINJAMP-SIMVASTATINMAR-SIMVASTATINMINT-SIMVASTATINMYLAN-SIMVASTATINNOVO-SIMVASTATINPHL-SIMVASTATINPMS-SIMVASTATINRAN-SIMVASTATINSANDOZ SIMVASTATINSIMVASTATINSIMVASTATINZOCOR
APO-SIMVASTATINCO SIMVASTATINJAMP-SIMVASTATINMAR-SIMVASTATINMINT-SIMVASTATINMYLAN-SIMVASTATINNOVO-SIMVASTATINPHL-SIMVASTATINPMS-SIMVASTATINRAN-SIMVASTATINSANDOZ SIMVASTATINSIMVASTATINSIMVASTATINZOCOR
NOVO-CLONIDINECATAPRES
APO-CLONIDINENOVO-CLONIDINECATAPRES
METHYLDOPA
METHYLDOPA
METHYLDOPA
APXCOBJPCMARMPIMYPTEVPHHPMSRANSDZSNSRANMFC
APXCOBJPCMARMPIMYPTEVPHHPMSRANSDZSNSRANMFC
TEVBOE
APXTEVBOE
AAP
AAP
AAP
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
ANTILIPEMIC AGENTS
HYPOTENSIVE AGENTS
24
24
:00
:00
24:06.08
24:08.16
1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 2.5729
1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 1.3860 2.5729
0.1765 0.1853
0.3149 0.3149 0.3306
0.1063
0.1540
0.2727
40 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$$$
$$$$$$$$$$$$$$
$$
$$$
$
$
$
(HMG-COA REDUCTASE INHIBITORS)
(CENTRAL ALPHA-AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DIAZOXIDE
HYDRALAZINE HCL
MINOXIDIL
ETHACRYNIC ACID
FUROSEMIDE
100 MG ORAL CAPSULE
10 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
2.5 MG ORAL TABLET
10 MG ORAL TABLET
25 MG ORAL TABLET
20 MG ORAL TABLET
40 MG ORAL TABLET
80 MG ORAL TABLET
500 MG ORAL TABLET
10 MG / ML ORAL SOLUTION
10 MG / ML INJECTION
00000503347
00000441619
00000441627
00000441635
00000514497
00000514500
00002258528
0000039678800002364573000023514200000033773000002224690
0000036216600002364581000023514390000033774900002224704
00000707570000023646030000235144700000765953
00002224755
00002224720
00000527033
PROGLYCEM
APO-HYDRALAZINE
APO-HYDRALAZINE
APO-HYDRALAZINE
LONITEN
LONITEN
EDECRIN
APO-FUROSEMIDEAVA-FUROSEMIDEFUROSEMIDENOVO-SEMIDELASIX
APO-FUROSEMIDEAVA-FUROSEMIDEFUROSEMIDENOVO-SEMIDELASIX
APO-FUROSEMIDEAVA-FUROSEMIDEFUROSEMIDENOVO-SEMIDE
LASIX SPECIAL
LASIX
FUROSEMIDE
MFC
APX
APX
APX
PFI
PFI
ATP
APXAVASNSTEVSAV
APXAVASNSTEVSAV
APXAVASNSTEV
SAV
SAV
SDZ
(LOOP DIURETICS)
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
HYPOTENSIVE AGENTS
HYPOTENSIVE AGENTS
24
24
:00
:00
24:08.20
24:08.24.08
1.6179
0.1347
0.2314
0.3633
0.3689
0.8132
3.5475
0.0445 0.0445 0.0445 0.0445 0.0938
0.0670 0.0670 0.0670 0.0670 0.1405
0.1220 0.1220 0.1220 0.1220
3.2411
0.2963
0.8651
41 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$$$$$
$$$$$
$$$$
$
$
$
(DIRECT VASODILATORS)
DIURETICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
OLMESARTAN MEDOXOMIL
OLMESARTAN MEDOXOMIL/ HYDROCHLOROTHIAZIDE
ISOSORBIDE DINITRATE
ISOSORBIDE-5-MONONITRATE
NITROGLYCERIN
20 MG ORAL TABLET
40 MG ORAL TABLET
20 MG * 12.5 MG ORAL TABLET
40 MG * 12.5 MG ORAL TABLET
40 MG * 25 MG ORAL TABLET
10 MG ORAL TABLET
30 MG ORAL TABLET
5 MG ORAL SUBLINGUAL TABLET
20 MG ORAL SUSTAINED-RELEASE TABLET
60 MG ORAL EXTENDED-RELEASE TABLET
0.3 MG ORAL SUBLINGUAL TABLET
0.6 MG ORAL SUBLINGUAL TABLET
0.4 MG / DOSE SUBLINGUAL METERED DOSE SPRAY
2 % TOPICAL OINTMENT
00002318660
00002318679
00002319616
00002319624
00002319632
00000441686
00000441694
00000670944
00000740721
000022728300000230128800002126559
00000037613
00000037621
000022435880000223899800002231441
00001926454
OLMETEC
OLMETEC
OLMETEC PLUS
OLMETEC PLUS
OLMETEC PLUS
ISDN
ISDN
ISDN
CEDOCARD-SR
APO-ISMNPMS-ISMNIMDUR
NITROSTAT
NITROSTAT
MYLAN-NITRORHO-NITRO PUMPSPRAYNITROLINGUAL PUMPSPRAY
NITROL
MFC
MFC
MFC
MFC
MFC
AAP
AAP
AAP
PAL
APXPMSAZC
PFI
PFI
MYPSDZSAV
PAL
(ANGIOTENSIN II RECEPTOR ANTAGONISTS)
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
HYPOTENSIVE AGENTS
VASODILATING AGENTS
24
24
:00
:00
24:08.44.08
24:12.08
1.0187
1.0187
1.0187
1.0187
1.0187
0.0392
0.0921
0.0668
0.4195
0.3973 0.3973 0.7364
0.1257
0.1257
0.0421 0.0421 0.0785
0.6390
42 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$
$
$
$$$
$
$
$$$
$
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
(NITRATES AND NITRITES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
NITROGLYCERIN
ALPROSTADIL
DIPYRIDAMOLE
NYLIDRIN HCL
SODIUM TETRADECYL SULFATE
0.2 MG/HR TRANSDERMAL PATCH
0.4 MG/HR TRANSDERMAL PATCH
0.6 MG/HR TRANSDERMAL PATCH
0.8 MG/HR TRANSDERMAL PATCH
500 MCG / ML INJECTION
25 MG ORAL TABLET
50 MG ORAL TABLET
75 MG ORAL TABLET
6 MG ORAL TABLET
1 % INJECTION
00001911910000022307320000216280600000584223
00001911902000022307330000216352700000852384
00001911929000022307340000216353500002046156
00002011271
00000559253
00000895644
00000895652
00000895660
00001926713
00000511234
NITRO-DUR 0.2TRINIPATCH 0.2MINITRAN 0.2TRANSDERM-NITRO 0.2
NITRO-DUR 0.4TRINIPATCH 0.4MINITRAN 0.4TRANSDERM-NITRO 0.4
NITRO-DUR 0.6TRINIPATCH 0.6MINITRAN 0.6TRANSDERM-NITRO 0.6
NITRO-DUR 0.8
PROSTIN VR
APO-DIPYRIDAMOLE (FC)
APO-DIPYRIDAMOLE (FC)
APO-DIPYRIDAMOLE (FC)
ARLIDIN
TROMBOJECT
MFCPALMEPNOV
MFCPALMEPNOV
MFCPALMEPNOV
MFC
PFI
APX
APX
APX
ERF
OMG
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
VASODILATING AGENTS
VASODILATING AGENTS
SCLEROSING AGENTS
24
24
24
:00
:00
:00
24:12.08
24:12.92
24:16
0.5667 0.5780 0.6387 0.7112
0.6400 0.6528 0.7215 0.8035
0.6400 0.6528 0.7218 0.8035
1.1100
259.1986
0.2633
0.2932
0.4397
0.5113
3.7500
43 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$$$
$$$$
$
$
$
$
$
$
$
(NITRATES AND NITRITES)
(MISCELLANEOUS VASODILATING AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DOXAZOSIN MESYLATE
PRAZOSIN HCL
TAMSULOSIN HCL
1 MG (BASE) ORAL TABLET
2 MG (BASE) ORAL TABLET
4 MG (BASE) ORAL TABLET
1 MG (BASE) ORAL TABLET
2 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
0.4 MG ORAL EXTENDED-RELEASE TABLET
0.4 MG ORAL SUSTAINED-RELEASE CAPSULE
0000224058800002240498000022427280000224452700001958100
0000224058900002240499000022427290000224452800001958097
0000224059000002240500000022427300000224452900001958119
000008828010000193419800001913794
000008828280000193420100001913808
000008828360000193422800001913816
00002362406000023662310000234020800002368242
000022985700000228139200002294885000022942650000229512100002331780
APO-DOXAZOSINMYLAN-DOXAZOSINNOVO-DOXAZOSINPMS-DOXAZOSINCARDURA
APO-DOXAZOSINMYLAN-DOXAZOSINNOVO-DOXAZOSINPMS-DOXAZOSINCARDURA
APO-DOXAZOSINMYLAN-DOXAZOSINNOVO-DOXAZOSINPMS-DOXAZOSINCARDURA
APO-PRAZONOVO-PRAZINNU-PRAZO
APO-PRAZONOVO-PRAZINNU-PRAZO
APO-PRAZONOVO-PRAZINNU-PRAZO
APO-TAMSULOSIN CRAVA-TAMSULOSIN CRSANDOZ TAMSULOSIN CRTEVA-TAMSULOSIN CR
MYLAN-TAMSULOSINNOVO-TAMSULOSINRAN-TAMSULOSINRATIO-TAMSULOSINSANDOZ TAMSULOSINTAMSULOSIN
APXMYPTEVPMSPFI
APXMYPTEVPMSPFI
APXMYPTEVPMSPFI
APXTEVNXP
APXTEVNXP
APXTEVNXP
APXAVASDZTEV
MYPTEVRANRPHSDZRAN
CARDIOVASCULAR DRUGS
ALPHA-ADRENERGIC BLOCKING AGENTS
24:00
24:20
0.3410 0.3410 0.3410 0.3410 0.6218
0.4091 0.4091 0.4091 0.4091 0.7458
0.5319 0.5319 0.5319 0.5319 0.9699
0.2055 0.2055 0.2055
0.2791 0.2791 0.2791
0.3806 0.3806 0.3806
0.2700 0.2700 0.2700 0.2700
0.5464 0.5464 0.5464 0.5464 0.5464 0.5464
44 EFFECTIVE APRIL 1, 2012
$$$$$
$$$$$
$$$$$
$$$
$$$
$$$
$$$$
$$$$$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
TERAZOSIN HCL1 MG (BASE) ORAL TABLET
2 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
00002234502000022330470000224351800002218941000023504750000223080500000818658
00002234503000022330480000224351900002218968000023504830000223080600000818682
00002234504000022330490000224352000002218976000023504910000223080700000818666
00002234505000022308080000223305000002243521000022189840000235050500000818674
APO-TERAZOSINNU-TERAZOSINPMS-TERAZOSINRATIO-TERAZOSINTERAZOSINTEVA-TERAZOSINHYTRIN
APO-TERAZOSINNU-TERAZOSINPMS-TERAZOSINRATIO-TERAZOSINTERAZOSINTEVA-TERAZOSINHYTRIN
APO-TERAZOSINNU-TERAZOSINPMS-TERAZOSINRATIO-TERAZOSINTERAZOSINTEVA-TERAZOSINHYTRIN
APO-TERAZOSINNOVO-TERAZOSINNU-TERAZOSINPMS-TERAZOSINRATIO-TERAZOSINTERAZOSINHYTRIN
APXNXPPMSRPHSNSTEVABB
APXNXPPMSRPHSNSTEVABB
APXNXPPMSRPHSNSTEVABB
APXTEVNXPPMSRPHSNSABB
CARDIOVASCULAR DRUGS
ALPHA-ADRENERGIC BLOCKING AGENTS
24:00
24:20
0.3490 0.3490 0.3490 0.3490 0.3490 0.3490 0.7323
0.4436 0.4436 0.4436 0.4436 0.4436 0.4436 0.9309
0.6025 0.6025 0.6025 0.6025 0.6025 0.6025 1.2642
0.8820 0.8820 0.8820 0.8820 0.8820 0.8820 1.8506
45 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$
$$$$$$$
$$$$$$$
$$$$$$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ACEBUTOLOL HCL
ATENOLOL
100 MG (BASE) ORAL TABLET
200 MG (BASE) ORAL TABLET
400 MG (BASE) ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
000022862460000214760200002363798000022377210000223788500002204517000021655460000191014000001926543
000022862540000214761000002363801000022377220000223788600002204525000021655540000191015900001926551
000022862620000214762900002363828000022377230000223788700002204533000021655620000191016700001926578
0000236096900002368013000023036470000224658100002266660
00000773689000022555450000236756400002371987000023680210000214689400001912062000022383160000223760000002267985000021717910000223173100002039532
ACEBUTOLOLAPO-ACEBUTOLOLAVA-ACEBUTOLOLMYLAN-ACEBUTOLOLMYLAN-ACEBUTOLOL (TYPE S)NOVO-ACEBUTOLOLNU-ACEBUTOLOLRHOTRALSECTRAL
ACEBUTOLOLAPO-ACEBUTOLOLAVA-ACEBUTOLOLMYLAN-ACEBUTOLOLMYLAN-ACEBUTOLOL (TYPE S)NOVO-ACEBUTOLOLNU-ACEBUTOLOLRHOTRALSECTRAL
ACEBUTOLOLAPO-ACEBUTOLOLAVA-ACEBUTOLOLMYLAN-ACEBUTOLOLMYLAN-ACEBUTOLOL (TYPE S)NOVO-ACEBUTOLOLNU-ACEBUTOLOLRHOTRALSECTRAL
AVA-ATENOLOLMINT-ATENOLMYLAN-ATENOLOLPMS-ATENOLOLTEVA-ATENOLOL
APO-ATENOLCO ATENOLOLJAMP-ATENOLOLMAR-ATENOLOLMINT-ATENOLMYLAN-ATENOLOLNOVO-ATENOLPHL-ATENOLOLPMS-ATENOLOLRAN-ATENOLOLRATIO-ATENOLOLSANDOZ ATENOLOLTENORMIN
SNSAPXAVAMYPMYPTEVNXPSDZSAV
SNSAPXAVAMYPMYPTEVNXPSDZSAV
SNSAPXAVAMYPMYPTEVNXPSDZSAV
AVAMPIMYPPMSTEV
APXCOBJPCMARMPIMYPTEVPHHPMSRANRPHSDZAZC
CARDIOVASCULAR DRUGS
BETA-ADRENERGIC BLOCKING AGENTS
24:00
24:24
0.1630 0.1630 0.1630 0.1630 0.1630 0.1630 0.1630 0.1630 0.3709
0.2440 0.2440 0.2440 0.2440 0.2440 0.2440 0.2440 0.2440 0.5564
0.4848 0.4848 0.4848 0.4848 0.4848 0.4848 0.4848 0.4848 1.1072
0.1730 0.1730 0.1730 0.1730 0.1730
0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.3460 0.6418
46 EFFECTIVE APRIL 1, 2012
$$$$$$$$$
$$$$$$$$$
$$$$$$$$$
$$$$$
$$$$$$$$$$$$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ATENOLOL
ATENOLOL/ CHLORTHALIDONE
BISOPROLOL FUMARATE
100 MG ORAL TABLET
50 MG * 25 MG ORAL TABLET
100 MG * 25 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
00000773697000022555530000236757200002371995000023680480000214743200001912054000022383180000223760100002267993000021718050000223173300002039540
000022487630000230291800002049961
000022487640000230292600002049988
0000225613400002363887000022674700000230263200002247439
0000225617700002363895000022674890000230264000002247440
APO-ATENOLCO ATENOLOLJAMP-ATENOLOLMAR-ATENOLOLMINT-ATENOLMYLAN-ATENOLOLNOVO-ATENOLPHL-ATENOLOLPMS-ATENOLOLRAN-ATENOLOLRATIO-ATENOLOLSANDOZ ATENOLOLTENORMIN
APO-ATENIDONENOVO-ATENOLTHALIDONETENORETIC 50/25
APO-ATENIDONENOVO-ATENOLTHALIDONETENORETIC 100/25
APO-BISOPROLOLAVA-BISOPROLOLNOVO-BISOPROLOLPMS-BISOPROLOLSANDOZ BISOPROLOL
APO-BISOPROLOLAVA-BISOPROLOLNOVO-BISOPROLOLPMS-BISOPROLOLSANDOZ BISOPROLOL
APXCOBJPCMARMPIMYPTEVPHHPMSRANRPHSDZAZC
APXTEVAZC
APXTEVAZC
APXAVATEVPMSSDZ
APXAVATEVPMSSDZ
CARDIOVASCULAR DRUGS
BETA-ADRENERGIC BLOCKING AGENTS
24:00
24:24
0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 0.5687 1.0549
0.3847 0.3847 0.7138
0.6303 0.6303 1.1696
0.2205 0.2205 0.2205 0.2205 0.2205
0.3654 0.3654 0.3654 0.3654 0.3654
47 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$$
$$$
$$$
$$$$$
$$$$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CARVEDILOL
LABETALOL HCL
3.125 MG ORAL TABLET
6.25 MG ORAL TABLET
12.5 MG ORAL TABLET
25 MG ORAL TABLET
100 MG ORAL TABLET
200 MG ORAL TABLET
5 MG / ML INJECTION
0000224793300002370735000023649130000234751200002248752000022459140000226802700002252309
0000224793400002370743000023649210000234752000002248753000022459150000226803500002252317
0000224793500002370751000023649480000234755500002248754000022459160000226804300002252325
00002247936000023707860000236495600002347571000022459170000226805100002252333
00002106272
00002106280
00002231689
APO-CARVEDILOLAVA-CARVEDILOLCARVEDILOLMYLAN-CARVEDILOLPHL-CARVEDILOLPMS-CARVEDILOLRAN-CARVEDILOLRATIO-CARVEDILOL
APO-CARVEDILOLAVA-CARVEDILOLCARVEDILOLMYLAN-CARVEDILOLPHL-CARVEDILOLPMS-CARVEDILOLRAN-CARVEDILOLRATIO-CARVEDILOL
APO-CARVEDILOLAVA-CARVEDILOLCARVEDILOLMYLAN-CARVEDILOLPHL-CARVEDILOLPMS-CARVEDILOLRAN-CARVEDILOLRATIO-CARVEDILOL
APO-CARVEDILOLAVA-CARVEDILOLCARVEDILOLMYLAN-CARVEDILOLPMS-CARVEDILOLRAN-CARVEDILOLRATIO-CARVEDILOL
TRANDATE
TRANDATE
LABETALOL HYDROCHLORIDE
APXAVASNSMYPPHHPMSRANRPH
APXAVASNSMYPPHHPMSRANRPH
APXAVASNSMYPPHHPMSRANRPH
APXAVASNSMYPPMSRANRPH
PAL
PAL
SDZ
CARDIOVASCULAR DRUGS
BETA-ADRENERGIC BLOCKING AGENTS
24:00
24:24
0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564
0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564
0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564
0.7564 0.7564 0.7564 0.7564 0.7564 0.7564 0.7564
0.2677
0.4733
1.3900
48 EFFECTIVE APRIL 1, 2012
$$$$$$$$
$$$$$$$$
$$$$$$$$
$$$$$$$
$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
METOPROLOL TARTRATE
NADOLOL
25 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
100 MG ORAL SUSTAINED-RELEASE TABLET
200 MG (BASE) ORAL SUSTAINED-RELEASE TABLET
1 MG / ML (BASE) INJECTION
40 MG ORAL TABLET
80 MG ORAL TABLET
160 MG ORAL TABLET
00002246010000023568130000230205500002248855
00000618632000007493540000236482400002364840000023568210000235039400002174545000008426480000064803500000865605000022308030000235418700000397423
0000061864000000751170000023648320000236485900002356848000023504080000217455300000842656000006480430000086561300002230804000022478760000235419500000397431
000022851690000230339600000658855
000022851770000230341800000534560
00000590819
0000078250500002126753
0000078246700002126761
00000782475
APO-METOPROLOLJAMP-METOPROLOL-LMYLAN-METOPROLOLPMS-METOPROLOL-L
APO-METOPROLOLAPO-METOPROLOL (TYPE L)AVA-METOPROLOLAVA-METOPROLOL (TYPE L)JAMP-METOPROLOL-LMETOPROLOLMYLAN-METOPROLOL (TYPE L)NOVO-METOPROLNOVO-METOPROL (FC)NU-METOPPMS-METOPROLOL-LSANDOZ METOPROLOL (TYPE L)LOPRESOR
APO-METOPROLOLAPO-METOPROLOL (TYPE L)AVA-METOPROLOLAVA-METOPROLOL (TYPE L)JAMP-METOPROLOL-LMETOPROLOLMYLAN-METOPROLOL (TYPE L)NOVO-METOPROLNOVO-METOPROL (FC)NU-METOPPMS-METOPROLOL-LSANDOZ METOPROLOL (TYPE L)SANDOZ METOPROLOL (TYPE L)LOPRESOR
APO-METOPROLOL SRSANDOZ METOPROLOL SRLOPRESOR SR
APO-METOPROLOL SRSANDOZ METOPROLOL SRLOPRESOR SR
LOPRESOR
APO-NADOLNOVO-NADOLOL
APO-NADOLNOVO-NADOLOL
APO-NADOL
APXJPCMYPPMS
APXAPXAVAAVAJPCSNSMYPTEVTEVNXPPMSSDZNOV
APXAPXAVAAVAJPCSNSMYPTEVTEVNXPPMSSDZSDZNOV
APXSDZNOV
APXSDZNOV
NOV
APXTEV
APXTEV
APX
CARDIOVASCULAR DRUGS
BETA-ADRENERGIC BLOCKING AGENTS
24:00
24:24
0.0643 0.0643 0.0643 0.0643
0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.1225 0.2990
0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.2223 0.6134
0.1789 0.1789 0.3350
0.3246 0.3246 0.6079
1.2849
0.2465 0.2465
0.3515 0.3515
1.2046
49 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$$$$$$$$$$$$
$$$$$$$$$$$$$$
$$$
$$$
$
$$
$$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PINDOLOL
PINDOLOL/ HYDROCHLOROTHIAZIDE
PROPRANOLOL HCL
5 MG ORAL TABLET
10 MG ORAL TABLET
15 MG ORAL TABLET
10 MG * 25 MG ORAL TABLET
10 MG * 50 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
40 MG ORAL TABLET
80 MG ORAL TABLET
120 MG ORAL TABLET
60 MG ORAL SUSTAINED-RELEASE CAPSULE
80 MG ORAL SUSTAINED-RELEASE CAPSULE
120 MG ORAL SUSTAINED-RELEASE CAPSULE
160 MG ORAL SUSTAINED-RELEASE CAPSULE
000007558770000086900700000886149000022315360000226178200000417270
000007558850000086901500000886009000022315370000226179000000443174
000007558930000086902300000886130000022315390000226180400000417289
00000568627
00000568635
0000040278800000496480
0000066371900000740675
0000040275300000496499
0000040276100000496502
00000504335
00002042231
00002042258
00002042266
00002042274
APO-PINDOLNOVO-PINDOLNU-PINDOLPMS-PINDOLOLSANDOZ PINDOLOLVISKEN
APO-PINDOLNOVO-PINDOLNU-PINDOLPMS-PINDOLOLSANDOZ PINDOLOLVISKEN
APO-PINDOLNOVO-PINDOLNU-PINDOLPMS-PINDOLOLSANDOZ PINDOLOLVISKEN
VISKAZIDE 10/25
VISKAZIDE 10/50
APO-PROPRANOLOLNOVO-PRANOL
APO-PROPRANOLOLNOVO-PRANOL
APO-PROPRANOLOLNOVO-PRANOL
APO-PROPRANOLOLNOVO-PRANOL
APO-PROPRANOLOL
INDERAL-LA
INDERAL-LA
INDERAL-LA
INDERAL-LA
APXTEVNXPPMSSDZNOV
APXTEVNXPPMSSDZNOV
APXTEVNXPPMSSDZNOV
NOV
NOV
APXTEV
APXTEV
APXTEV
APXTEV
APX
WAY
WAY
WAY
WAY
CARDIOVASCULAR DRUGS
BETA-ADRENERGIC BLOCKING AGENTS
24:00
24:24
0.2283 0.2283 0.2283 0.2283 0.2283 0.6134
0.3965 0.3965 0.3965 0.3965 0.3965 1.0475
0.5825 0.5825 0.5825 0.5825 0.5825 1.5195
0.9402
0.9402
0.0192 0.0192
0.0346 0.0346
0.0348 0.0348
0.0585 0.0585
0.3091
0.5979
0.6742
1.0380
1.2276
50 EFFECTIVE APRIL 1, 2012
$$$$$$
$$$$$$
$$$$$$
$
$
$$
$$
$$
$$
$
$
$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SOTALOL HCL
TIMOLOL MALEATE
80 MG ORAL TABLET
160 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
000022104280000236367400002270625000022297780000223118100002200996000022383260000208422800002257831
000021677940000236368200002270633000022297790000223118200002163772000022383270000208423600002257858
000007558420000194779600002044609
000007558500000194781800002044617
0000075586900001947826
APO-SOTALOLAVA-SOTALOLCO SOTALOLMYLAN-SOTALOLNOVO-SOTALOLNU-SOTALOLPMS-SOTALOLRATIO-SOTALOLSANDOZ SOTALOL
APO-SOTALOLAVA-SOTALOLCO SOTALOLMYLAN-SOTALOLNOVO-SOTALOLNU-SOTALOLPMS-SOTALOLRATIO-SOTALOLSANDOZ SOTALOL
APO-TIMOLNOVO-TIMOLNU-TIMOLOL
APO-TIMOLNOVO-TIMOLNU-TIMOLOL
APO-TIMOLNOVO-TIMOL
APXAVACOBMYPTEVNXPPMSRPHSDZ
APXAVACOBMYPTEVNXPPMSRPHSDZ
APXTEVNXP
APXTEVNXP
APXTEV
CARDIOVASCULAR DRUGS
BETA-ADRENERGIC BLOCKING AGENTS
24:00
24:24
0.5932 0.5932 0.5932 0.5932 0.5932 0.5932 0.5932 0.5932 0.5932
0.6492 0.6492 0.6492 0.6492 0.6492 0.6492 0.6492 0.6492 0.6492
0.1817 0.1817 0.1817
0.2835 0.2835 0.2835
0.5670 0.5670
51 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$
$$$$$$$$$
$$$
$$$
$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
AMLODIPINE BESYLATE
FELODIPINE
2.5 MG ORAL TABLET
5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
2.5 MG ORAL EXTENDED-RELEASE TABLET
5 MG ORAL EXTENDED-RELEASE TABLET
0000232676000002295148
000023312840000233193400002273373000022974850000228013200002331071000023571940000237171500002362651000022721130000225049700002326779000022840650000232185800002259605000022843830000235771200000878928
000023312920000233194200002273381000022974930000228014000002331098000023572080000237172300002362678000022721210000225050000002326787000022840730000232186600002259613000022843910000235772000000878936
0000222198500002057778
000022219930000228026400000851779
PHL-AMLODIPINEPMS-AMLODIPINE
AMLODIPINEAMLODIPINEAPO-AMLODIPINECO AMLODIPINEGD-AMLODIPINEJAMP-AMLODIPINEJAMP-AMLODIPINEMAR-AMLODIPINEMINT-AMLODIPINEMYLAN-AMLODIPINENOVO-AMLODIPINEPHL-AMLODIPINEPMS-AMLODIPINERAN-AMLODIPINERATIO-AMLODIPINESANDOZ AMLODIPINESEPTA-AMLODIPINENORVASC
AMLODIPINEAMLODIPINEAPO-AMLODIPINECO AMLODIPINEGD-AMLODIPINEJAMP-AMLODIPINEJAMP-AMLODIPINEMAR-AMLODIPINEMINT-AMLODIPINEMYLAN-AMLODIPINENOVO-AMLODIPINEPHL-AMLODIPINEPMS-AMLODIPINERAN-AMLODIPINERATIO-AMLODIPINESANDOZ AMLODIPINESEPTA-AMLODIPINENORVASC
RENEDILPLENDIL
RENEDILSANDOZ FELODIPINEPLENDIL
PHHPMS
SNSRANAPXCOBGMDJPCJPCMARMPIMYPTEVPHHPMSRANRPHSDZSEPPFI
SNSRANAPXCOBGMDJPCJPCMARMPIMYPTEVPHHPMSRANRPHSDZSEPPFI
SAVAZC
SAVSDZAZC
CARDIOVASCULAR DRUGS
CALCIUM-CHANNEL BLOCKING AGENTS
24:00
24:28.08
0.3328 0.3328
0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 0.6656 1.4433
0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 0.9880 2.1425
0.3408 0.5472
0.4980 0.5097 0.7310
52 EFFECTIVE APRIL 1, 2012
$$
$$$$$$$$$$$$$$$$$$
$$$$$$$$$$$$$$$$$$
$$
$$$
(DIHYDROPYRIDINES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FELODIPINE
NIFEDIPINE
DILTIAZEM HCL
10 MG ORAL EXTENDED-RELEASE TABLET
20 MG ORAL EXTENDED-RELEASE TABLET
30 MG ORAL EXTENDED-RELEASE TABLET
60 MG ORAL EXTENDED-RELEASE TABLET
5 MG ORAL CAPSULE
10 MG ORAL CAPSULE
30 MG ORAL TABLET
60 MG ORAL TABLET
120 MG ORAL EXTENDED-RELEASE TABLET
180 MG ORAL EXTENDED-RELEASE TABLET
240 MG ORAL EXTENDED-RELEASE TABLET
300 MG ORAL EXTENDED-RELEASE TABLET
360 MG ORAL EXTENDED-RELEASE TABLET
000022220000000228027200000851787
00002237618
0000215590700002349167
0000215599000002321149
00000725110
00000755907
000007713760000086292400000886068
000007713840000086293200000886076
00002256738
00002256746
00002256754
00002256762
00002256770
RENEDILSANDOZ FELODIPINEPLENDIL
ADALAT XL
ADALAT XLMYLAN-NIFEDIPINE EXTENDED RELEASE
ADALAT XLMYLAN-NIFEDIPINE EXTENDED RELEASE
NIFEDIPINE
NIFEDIPINE
APO-DILTIAZNOVO-DILTAZEMNU-DILTIAZ
APO-DILTIAZNOVO-DILTAZEMNU-DILTIAZ
TIAZAC XC
TIAZAC XC
TIAZAC XC
TIAZAC XC
TIAZAC XC
SAVSDZAZC
BAI
BAIMYP
BAIMYP
AAP
AAP
APXTEVNXP
APXTEVNXP
VCL
VCL
VCL
VCL
VCL
CARDIOVASCULAR DRUGS
CARDIOVASCULAR DRUGS
CALCIUM-CHANNEL BLOCKING AGENTS
CALCIUM-CHANNEL BLOCKING AGENTS
24
24
:00
:00
24:28.08
24:28.92
0.7238 0.7647 1.0973
1.3424
0.7177 0.7177
1.1285 1.1285
0.3955
0.5243
0.2075 0.2075 0.2075
0.3637 0.3637 0.3637
0.8194
1.0887
1.4470
1.4441
1.4447
53 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$
$$
$$
$
$
$$$
$$$
$
$
$
$
$
(DIHYDROPYRIDINES)
(MISCELLANEOUS CALCIUM-CHANNEL BLOCKING AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DILTIAZEM HCL120 MG ORAL CONTROLLED-DELIVERY CAPSULE
180 MG ORAL CONTROLLED-DELIVERY CAPSULE
240 MG ORAL CONTROLLED-DELIVERY CAPSULE
300 MG ORAL CONTROLLED-DELIVERY CAPSULE
120 MG ORAL EXTENDED-RELEASE CAPSULE
180 MG ORAL EXTENDED-RELEASE CAPSULE
0000223099700002370611000022425380000223105200002355752000022297810000224333800002097249
0000223099800002370638000022425390000223105300002355760000022297820000224333900002097257
0000223099900002370646000022425400000223105400002355779000022297830000224334000002097265
00002229526000023706540000224254100002355787000022297840000224334100002097273
0000229103700002370441000022716050000224591800002231150
0000229104500002370492000022716130000224591900002231151
APO-DILTIAZ CDCO DILTIAZEM CDNOVO-DILTAZEM CDNU-DILTIAZ-CDPMS-DILTIAZEM CDRATIO-DILTIAZEM CDSANDOZ DILTIAZEM CDCARDIZEM CD
APO-DILTIAZ CDCO DILTIAZEM CDNOVO-DILTAZEM CDNU-DILTIAZ-CDPMS-DILTIAZEM CDRATIO-DILTIAZEM CDSANDOZ DILTIAZEM CDCARDIZEM CD
APO-DILTIAZ CDCO DILTIAZEM CDNOVO-DILTAZEM CDNU-DILTIAZ-CDPMS-DILTIAZEM CDRATIO-DILTIAZEM CDSANDOZ DILTIAZEM CDCARDIZEM CD
APO-DILTIAZ CDCO DILTIAZEM CDNOVO-DILTAZEM CDPMS-DILTIAZEM CDRATIO-DILTIAZEM CDSANDOZ DILTIAZEM CDCARDIZEM CD
APO-DILTIAZ TZCO DILTIAZEM TNOVO-DILTIAZEM HCL ERSANDOZ DILTIAZEM TTIAZAC
APO-DILTIAZ TZCO DILTIAZEM TNOVO-DILTIAZEM HCL ERSANDOZ DILTIAZEM TTIAZAC
APXCOBTEVNXPPMSRPHSDZVCL
APXCOBTEVNXPPMSRPHSDZVCL
APXCOBTEVNXPPMSRPHSDZVCL
APXCOBTEVPMSRPHSDZVCL
APXCOBTEVSDZVCL
APXCOBTEVSDZVCL
CARDIOVASCULAR DRUGS
CALCIUM-CHANNEL BLOCKING AGENTS
24:00
24:28.92
0.7904 0.7904 0.7904 0.7904 0.7904 0.7904 0.7904 1.4734
1.0492 1.0492 1.0492 1.0492 1.0492 1.0492 1.0492 1.9559
1.3916 1.3916 1.3916 1.3916 1.3916 1.3916 1.3916 2.5944
1.7395 1.7395 1.7395 1.7395 1.7395 1.7395 3.2431
0.4778 0.4778 0.4778 0.4778 0.8533
0.6471 0.6471 0.6471 0.6471 1.1556
54 EFFECTIVE APRIL 1, 2012
$$$$$$$$
$$$$$$$$
$$$$$$$$
$$$$$$$
$$$$$
$$$$$
(MISCELLANEOUS CALCIUM-CHANNEL BLOCKING AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DILTIAZEM HCL
VERAPAMIL HCL
240 MG ORAL EXTENDED-RELEASE CAPSULE
300 MG ORAL EXTENDED-RELEASE CAPSULE
360 MG ORAL EXTENDED-RELEASE CAPSULE
80 MG ORAL TABLET
120 MG ORAL TABLET
120 MG ORAL SUSTAINED-RELEASE TABLET
180 MG ORAL SUSTAINED-RELEASE TABLET
240 MG ORAL SUSTAINED-RELEASE TABLET
0000229105300002370506000022716210000224592000002231152
0000229106100002370514000022716480000224592100002231154
0000229108800002370522000022716560000224592200002231155
000007824830000223792100000886033
000007824910000223792200000886041
000022468930000221034700001907123
000022468940000221035500001934317
0000224689500002210363000022119200000223779100000742554
APO-DILTIAZ TZCO DILTIAZEM TNOVO-DILTIAZEM HCL ERSANDOZ DILTIAZEM TTIAZAC
APO-DILTIAZ TZCO DILTIAZEM TNOVO-DILTIAZEM HCL ERSANDOZ DILTIAZEM TTIAZAC
APO-DILTIAZ TZCO DILTIAZEM TNOVO-DILTIAZEM HCL ERSANDOZ DILTIAZEM TTIAZAC
APO-VERAPMYLAN-VERAPAMILNU-VERAP
APO-VERAPMYLAN-VERAPAMILNU-VERAP
APO-VERAP SRMYLAN-VERAPAMIL SRISOPTIN SR
APO-VERAP SRMYLAN-VERAPAMIL SRISOPTIN SR
APO-VERAP SRMYLAN-VERAPAMIL SRNOVO-VERAMIL SRPMS-VERAPAMIL SRISOPTIN SR
APXCOBTEVSDZVCL
APXCOBTEVSDZVCL
APXCOBTEVSDZVCL
APXMYPNXP
APXMYPNXP
APXMYPABB
APXMYPABB
APXMYPTEVPMSABB
CARDIOVASCULAR DRUGS
CALCIUM-CHANNEL BLOCKING AGENTS
24:00
24:28.92
0.8584 0.8584 0.8584 0.8584 1.5328
1.0572 1.0572 1.0572 1.0572 1.8878
1.2943 1.2943 1.2943 1.2943 2.3112
0.2735 0.2735 0.2735
0.4250 0.4250 0.4250
0.6900 0.6900 1.3448
0.6558 0.6558 1.5186
0.8720 0.8720 0.8720 0.8720 2.0252
55 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$
$$$$$
$$$$$
$$$
$$$
$$$
$$$
$$$$$
(MISCELLANEOUS CALCIUM-CHANNEL BLOCKING AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
BENAZEPRIL HCL
CAPTOPRIL
CILAZAPRIL
5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
12.5 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
1 MG ORAL TABLET
2.5 MG ORAL TABLET
0000229033200000885835
00002290340
0000227391800000885851
00000893595000021635510000194296400001913824
00000893609000021635780000194297200001913832
00000893617000021635860000194298000001913840
00000893625000021635940000194299900001913859
0000229113400002350963000022837780000226635000002280442
00002291142000023509710000228521500002283786000022663690000228045000001911473
BENAZEPRILLOTENSIN
BENAZEPRIL
BENAZEPRILLOTENSIN
APO-CAPTOMYLAN-CAPTOPRILNOVO-CAPTORILNU-CAPTO
APO-CAPTOMYLAN-CAPTOPRILNOVO-CAPTORILNU-CAPTO
APO-CAPTOMYLAN-CAPTOPRILNOVO-CAPTORILNU-CAPTO
APO-CAPTOMYLAN-CAPTOPRILNOVO-CAPTORILNU-CAPTO
APO-CILAZAPRILCILAZAPRILMYLAN-CILAZAPRILNOVO-CILAZAPRILPMS-CILAZAPRIL
APO-CILAZAPRILCILAZAPRILCO CILAZAPRILMYLAN-CILAZAPRILNOVO-CILAZAPRILPMS-CILAZAPRILINHIBACE
AAPNOV
AAP
AAPNOV
APXMYPTEVNXP
APXMYPTEVNXP
APXMYPTEVNXP
APXMYPTEVNXP
APXSNSMYPTEVPMS
APXSNSCOBMYPTEVPMSHLR
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.5577 0.8380
0.6595
0.7567 1.1370
0.2120 0.2120 0.2120 0.2120
0.3000 0.3000 0.3000 0.3000
0.5590 0.5590 0.5590 0.5590
1.0395 1.0395 1.0395 1.0395
0.3717 0.3717 0.3717 0.3717 0.3717
0.4284 0.4284 0.4284 0.4284 0.4284 0.4284 0.7872
56 EFFECTIVE APRIL 1, 2012
$$
$
$$
$$$$
$$$$
$$$$
$$$$
$$$$$
$$$$$$$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CILAZAPRIL
CILAZAPRIL/ HYDROCHLOROTHIAZIDE
ENALAPRIL MALEATE
5 MG ORAL TABLET
5 MG * 12.5 MG ORAL TABLET
2.5 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
00002291150000023509980000228522300002283794000022663770000228046900001911481
000022849870000231373100002181479
000020200250000236345300002291878000023000360000230068000002300079000023522300000229993300000851795
000020198840000236346100002291886000023000440000223300500002300087000023522490000229994100000708879
000020198920000236348800002291894000023000520000223300600002300095000023522570000229996800000670901
APO-CILAZAPRILCILAZAPRILCO CILAZAPRILMYLAN-CILAZAPRILNOVO-CILAZAPRILPMS-CILAZAPRILINHIBACE
APO-CILAZAPRIL/HCTZNOVO-CILAZAPRIL/HCTZINHIBACE PLUS
APO-ENALAPRILAVA-ENALAPRILCO ENALAPRILMYLAN-ENALAPRILNOVO-ENALAPRILPMS-ENALAPRILRAN-ENALAPRILSANDOZ ENALAPRILVASOTEC
APO-ENALAPRILAVA-ENALAPRILCO ENALAPRILMYLAN-ENALAPRILNOVO-ENALAPRILPMS-ENALAPRILRAN-ENALAPRILSANDOZ ENALAPRILVASOTEC
APO-ENALAPRILAVA-ENALAPRILCO ENALAPRILMYLAN-ENALAPRILNOVO-ENALAPRILPMS-ENALAPRILRAN-ENALAPRILSANDOZ ENALAPRILVASOTEC
APXSNSCOBMYPTEVPMSHLR
APXTEVHLR
APXAVACOBMYPTEVPMSRANSDZMFC
APXAVACOBMYPTEVPMSRANSDZMFC
APXAVACOBMYPTEVPMSRANSDZMFC
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.4977 0.4977 0.4977 0.4977 0.4977 0.4977 0.9146
0.5020 0.5020 0.9145
0.4172 0.4172 0.4172 0.4172 0.4172 0.4172 0.4172 0.4172 0.7803
0.4935 0.4935 0.4935 0.4935 0.4935 0.4935 0.4935 0.4935 0.9231
0.5932 0.5932 0.5932 0.5932 0.5932 0.5932 0.5932 0.5932 1.1092
57 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$
$$$
$$$$$$$$$
$$$$$$$$$
$$$$$$$$$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
ENALAPRIL MALEATE
ENALAPRIL MALEATE/ HYDROCHLOROTHIAZIDE
FOSINOPRIL SODIUM
20 MG ORAL TABLET
5 MG * 12.5 MG ORAL TABLET
10 MG * 25 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
000020199060000236349600002291908000023000600000223300700002300109000023522650000229997600000670928
0000235292300002300222
000023529310000230023000000657298
00002266008000023325660000233100400002262401000022478020000229452400001907107
00002266016000023325740000233101200002262428000022478030000229453200001907115
APO-ENALAPRILAVA-ENALAPRILCO ENALAPRILMYLAN-ENALAPRILNOVO-ENALAPRILPMS-ENALAPRILRAN-ENALAPRILSANDOZ ENALAPRILVASOTEC
APO-ENALAPRIL MALEATE/HCTZNOVO-ENALAPRIL/HCTZ
APO-ENALAPRIL MALEATE/HCTZNOVO-ENALAPRIL/HCTZVASERETIC
APO-FOSINOPRILFOSINOPRILJAMP-FOSINOPRILMYLAN-FOSINOPRILNOVO-FOSINOPRILRAN-FOSINOPRILMONOPRIL
APO-FOSINOPRILFOSINOPRILJAMP-FOSINOPRILMYLAN-FOSINOPRILNOVO-FOSINOPRILRAN-FOSINOPRILMONOPRIL
APXAVACOBMYPTEVPMSRANSDZMFC
APXTEV
APXTEVMFC
APXRANJPCMYPTEVRANBMS
APXRANJPCMYPTEVRANBMS
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.7156 0.7156 0.7156 0.7156 0.7156 0.7156 0.7156 0.7156 1.3385
0.6436 0.6436
0.6108 0.6108 1.1425
0.4878 0.4878 0.4878 0.4878 0.4878 0.4878 0.9125
0.5866 0.5866 0.5866 0.5866 0.5866 0.5866 1.0973
58 EFFECTIVE APRIL 1, 2012
$$$$$$$$$
$$
$$$
$$$$$$$
$$$$$$$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
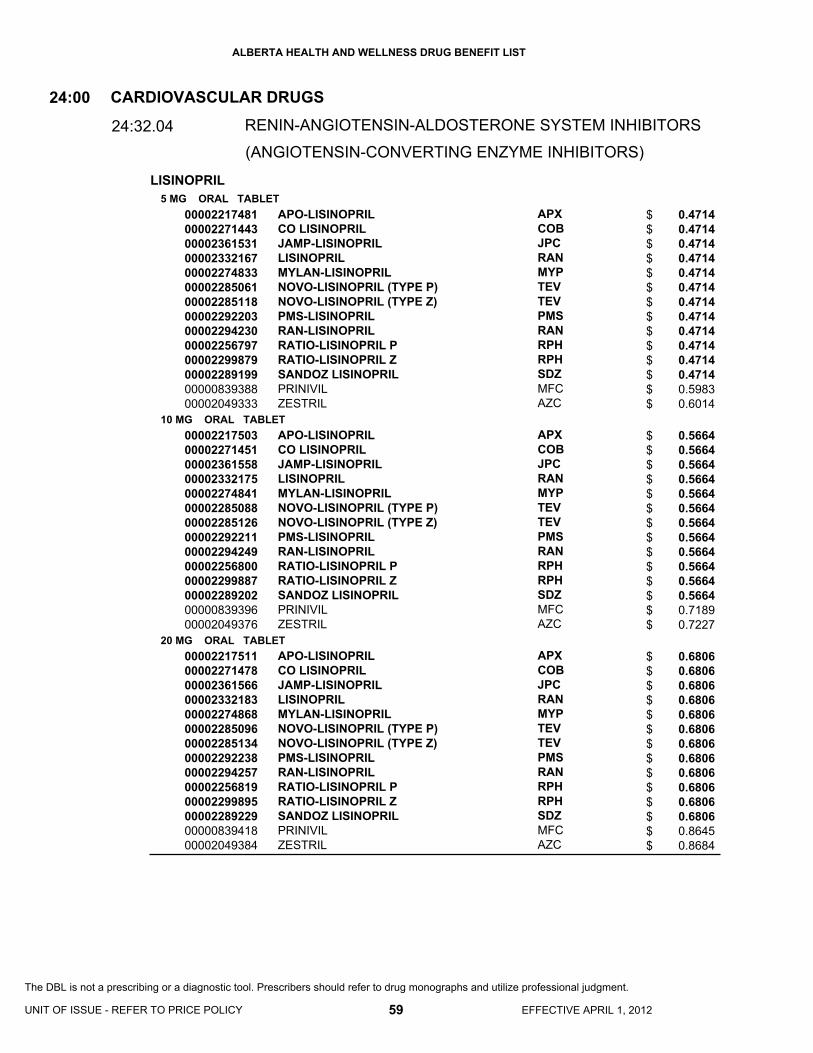
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
LISINOPRIL5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
0000221748100002271443000023615310000233216700002274833000022850610000228511800002292203000022942300000225679700002299879000022891990000083938800002049333
0000221750300002271451000023615580000233217500002274841000022850880000228512600002292211000022942490000225680000002299887000022892020000083939600002049376
0000221751100002271478000023615660000233218300002274868000022850960000228513400002292238000022942570000225681900002299895000022892290000083941800002049384
APO-LISINOPRILCO LISINOPRILJAMP-LISINOPRILLISINOPRILMYLAN-LISINOPRILNOVO-LISINOPRIL (TYPE P)NOVO-LISINOPRIL (TYPE Z)PMS-LISINOPRILRAN-LISINOPRILRATIO-LISINOPRIL PRATIO-LISINOPRIL ZSANDOZ LISINOPRILPRINIVILZESTRIL
APO-LISINOPRILCO LISINOPRILJAMP-LISINOPRILLISINOPRILMYLAN-LISINOPRILNOVO-LISINOPRIL (TYPE P)NOVO-LISINOPRIL (TYPE Z)PMS-LISINOPRILRAN-LISINOPRILRATIO-LISINOPRIL PRATIO-LISINOPRIL ZSANDOZ LISINOPRILPRINIVILZESTRIL
APO-LISINOPRILCO LISINOPRILJAMP-LISINOPRILLISINOPRILMYLAN-LISINOPRILNOVO-LISINOPRIL (TYPE P)NOVO-LISINOPRIL (TYPE Z)PMS-LISINOPRILRAN-LISINOPRILRATIO-LISINOPRIL PRATIO-LISINOPRIL ZSANDOZ LISINOPRILPRINIVILZESTRIL
APXCOBJPCRANMYPTEVTEVPMSRANRPHRPHSDZMFCAZC
APXCOBJPCRANMYPTEVTEVPMSRANRPHRPHSDZMFCAZC
APXCOBJPCRANMYPTEVTEVPMSRANRPHRPHSDZMFCAZC
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.4714 0.5983 0.6014
0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.5664 0.7189 0.7227
0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.6806 0.8645 0.8684
59 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$$$
$$$$$$$$$$$$$$
$$$$$$$$$$$$$$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
LISINOPRIL/ HYDROCHLOROTHIAZIDE
PERINDOPRIL ERBUMINE
PERINDOPRIL ERBUMINE/ INDAPAMIDE HEMIHYDRATE
QUINAPRIL HCL
10 MG * 12.5 MG ORAL TABLET
20 MG * 12.5 MG ORAL TABLET
20 MG * 25 MG ORAL TABLET
10 MG * 12.5 MG ORAL TABLET
20 MG * 12.5 MG ORAL TABLET
20 MG * 25 MG ORAL TABLET
2 MG ORAL TABLET
4 MG ORAL TABLET
8 MG ORAL TABLET
4 MG * 1.25 MG ORAL TABLET
8 MG * 2.5 MG ORAL TABLET
5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
00002261979000023628800000236294500002297736000023017680000230236500002103729
00002261987000023628990000236295300002297744000023017760000230237300002045737
00002261995000023629020000236296100002297752000023017840000230238100002045729
00002302136
0000230214400000884413
00002302152
00002123274
00002123282
00002246624
00002246569
00002321653
00001947664
00001947672
APO-LISINOPRIL/HCTZAVA-LISINOPRIL HCTLISINOPRIL/HCTZ (TYPE Z)MYLAN-LISINOPRIL HCTZNOVO-LISINOPRIL/HCTZ (TYPE Z)SANDOZ LISINOPRIL HCTZESTORETIC
APO-LISINOPRIL/HCTZAVA-LISINOPRIL HCTLISINOPRIL/HCTZ (TYPE Z)MYLAN-LISINOPRIL HCTZNOVO-LISINOPRIL/HCTZ (TYPE Z)SANDOZ LISINOPRIL HCTZESTORETIC
APO-LISINOPRIL/HCTZAVA-LISINOPRIL HCTLISINOPRIL/HCTZ (TYPE Z)MYLAN-LISINOPRIL HCTZNOVO-LISINOPRIL/HCTZ (TYPE Z)SANDOZ LISINOPRIL HCTZESTORETIC
NOVO-LISINOPRIL/HCTZ (TYPE P)
NOVO-LISINOPRIL/HCTZ (TYPE P)PRINZIDE
NOVO-LISINOPRIL/HCTZ (TYPE P)
COVERSYL
COVERSYL
COVERSYL
COVERSYL PLUS
COVERSYL PLUS HD
ACCUPRIL
ACCUPRIL
APXAVASNSMYPTEVSDZAZC
APXAVASNSMYPTEVSDZAZC
APXAVASNSMYPTEVSDZAZC
TEV
TEVMFC
TEV
SEV
SEV
SEV
SEV
SEV
PFI
PFI
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.5019 0.5019 0.5019 0.5019 0.5019 0.5019 0.9303
0.6030 0.6030 0.6030 0.6030 0.6030 0.6030 1.1180
0.6030 0.6030 0.6030 0.6030 0.6030 0.6030 1.1180
0.4076
0.4898 0.8904
0.6068
0.7015
0.8783
1.2294
1.0581
1.2294
0.9649
0.9649
60 EFFECTIVE APRIL 1, 2012
$$$$$$$
$$$$$$$
$$$$$$$
$
$$
$
$
$
$
$
$
$
$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
QUINAPRIL HCL
QUINAPRIL HCL/ HYDROCHLOROTHIAZIDE
RAMIPRIL
20 MG (BASE) ORAL TABLET
40 MG (BASE) ORAL TABLET
10 MG (BASE) * 12.5 MG ORAL TABLET
20 MG (BASE) * 12.5 MG ORAL TABLET
20 MG * 25 MG ORAL TABLET
1.25 MG ORAL CAPSULE/TABLET
2.5 MG ORAL CAPSULE/TABLET
5 MG ORAL CAPSULE/TABLET
00001947680
00001947699
00002237367
00002237368
00002237369
00002251515000023632670000229548200002331101000023011480000229536900002332299000023105030000229139800002221829
000022515310000236327500002295490000023311280000230115600002247945000022479170000233230200002374846000023105110000229140100002221837
000022515740000236328300002295504000023311360000230116400002247946000022479180000233231000002374854000023105380000229142800002221845
ACCUPRIL
ACCUPRIL
ACCURETIC 10/12.5
ACCURETIC 20/12.5
ACCURETIC 20/25
APO-RAMIPRIL (CAPSULE)AVA-RAMIPRIL (TABLET)CO RAMIPRIL (CAPSULE)JAMP-RAMIPRIL (CAPSULE)MYLAN-RAMIPRIL (CAPSULE)PMS-RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAN-RAMIPRIL (CAPSULE)SANDOZ RAMIPRIL (TABLET)ALTACE (CAPSULE)
APO-RAMIPRIL (CAPSULE)AVA-RAMIPRIL (TABLET)CO RAMIPRIL (CAPSULE)JAMP-RAMIPRIL (CAPSULE)MYLAN-RAMIPRIL (CAPSULE)NOVO-RAMIPRIL (CAPSULE)PMS-RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAN-RAMIPRIL (CAPSULE)SANDOZ RAMIPRIL (TABLET)ALTACE (CAPSULE)
APO-RAMIPRIL (CAPSULE)AVA-RAMIPRIL (TABLET)CO RAMIPRIL (CAPSULE)JAMP-RAMIPRIL (CAPSULE)MYLAN-RAMIPRIL (CAPSULE)NOVO-RAMIPRIL (CAPSULE)PMS-RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAN-RAMIPRIL (CAPSULE)SANDOZ RAMIPRIL (TABLET)ALTACE (CAPSULE)
PFI
PFI
PFI
PFI
PFI
APXAVACOBJPCMYPPMSRANRANSDZSAV
APXAVACOBJPCMYPTEVPMSRANSNSRANSDZSAV
APXAVACOBJPCMYPTEVPMSRANSNSRANSDZSAV
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.9649
0.9649
0.9647
0.9647
0.9333
0.4174 0.4174 0.4174 0.4174 0.4174 0.4174 0.4174 0.4174 0.4174 0.7608
0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.8780
0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.4815 0.8780
61 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$$$$$$$$$$
$$$$$$$$$$$$
$$$$$$$$$$$$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
RAMIPRIL
RAMIPRIL/ HYDROCHLOROTHIAZIDE
TRANDOLAPRIL
10 MG ORAL CAPSULE/TABLET
2.5 MG * 12.5 MG ORAL TABLET
5 MG * 12.5 MG ORAL TABLET
5 MG * 25 MG ORAL TABLET
10 MG * 12.5 MG ORAL TABLET
10 MG * 25 MG ORAL TABLET
0.5 MG ORAL CAPSULE
1 MG ORAL CAPSULE
2 MG ORAL CAPSULE
4 MG ORAL CAPSULE
000022515820000236329100002295512000023311440000230117200002247947000022479190000233232900002374862000023105460000229143600002221853
0000234213800002283131
0000234214600002283158
0000234216200002283174
0000234215400002283166
0000234217000002283182
00002231457
00002231459
00002231460
00002239267
APO-RAMIPRIL (CAPSULE)AVA-RAMIPRIL (TABLET)CO RAMIPRIL (CAPSULE)JAMP-RAMIPRIL (CAPSULE)MYLAN-RAMIPRIL (CAPSULE)NOVO-RAMIPRIL (CAPSULE)PMS-RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAMIPRIL (CAPSULE)RAN-RAMIPRIL (CAPSULE)SANDOZ RAMIPRIL (TABLET)ALTACE (CAPSULE)
PMS-RAMIPRIL-HCTZALTACE HCT
PMS-RAMIPRIL-HCTZALTACE HCT
PMS-RAMIPRIL-HCTZALTACE HCT
PMS-RAMIPRIL-HCTZALTACE HCT
PMS-RAMIPRIL-HCTZALTACE HCT
MAVIK
MAVIK
MAVIK
MAVIK
APXAVACOBJPCMYPTEVPMSRANSNSRANSDZSAV
PMSSAV
PMSSAV
PMSSAV
PMSSAV
PMSSAV
ABB
ABB
ABB
ABB
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.04
0.6100 0.6100 0.6100 0.6100 0.6100 0.6100 0.6100 0.6100 0.6100 0.6100 0.6100 1.1119
0.2250 0.3213
0.2263 0.4116
0.2263 0.4116
0.2865 0.5241
0.2865 0.5241
0.4030
0.6901
0.7931
0.9785
62 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$
$$
$$
$$
$$
$$
$
$
$
$
(ANGIOTENSIN-CONVERTING ENZYME INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CANDESARTAN CILEXETIL
CANDESARTAN CILEXETIL/ HYDROCHLOROTHIAZIDE
EPROSARTAN MESYLATE
EPROSARTAN MESYLATE/ HYDROCHLOROTHIAZIDE
IRBESARTAN
8 MG ORAL TABLET
16 MG ORAL TABLET
32 MG ORAL TABLET
16 MG * 12.5 MG ORAL TABLET
32 MG * 12.5 MG ORAL TABLET
32 MG * 25 MG ORAL TABLET
400 MG (BASE) ORAL TABLET
600 MG (BASE) ORAL TABLET
600 MG * 12.5 MG ORAL TABLET
75 MG ORAL TABLET
150 MG ORAL TABLET
00002365359000023765390000232696500002239091
00002365367000023765470000232697300002239092
0000237655500002311658
00002244021
00002332922
00002332957
00002240432
00002243942
00002253631
000023733190000232807000002372347000023472960000231706000002316390000023284610000231597100002237923
000023733270000232808900002372371000023473180000231707900002316404000023284880000231599800002237924
APO-CANDESARTANCO CANDESARTANSANDOZ CANDESARTANATACAND
APO-CANDESARTANCO CANDESARTANSANDOZ CANDESARTANATACAND
CO CANDESARTANATACAND
ATACAND PLUS
ATACAND PLUS
ATACAND PLUS
TEVETEN
TEVETEN
TEVETEN PLUS
AVA-IRBESARTANCO IRBESARTANIRBESARTANMYLAN-IRBESARTANPMS-IRBESARTANRATIO-IRBESARTANSANDOZ IRBESARTANTEVA-IRBESARTANAVAPRO
AVA-IRBESARTANCO IRBESARTANIRBESARTANMYLAN-IRBESARTANPMS-IRBESARTANRATIO-IRBESARTANSANDOZ IRBESARTANTEVA-IRBESARTANAVAPRO
APXCOBSDZAZC
APXCOBSDZAZC
COBAZC
AZC
AZC
AZC
ABB
ABB
ABB
AVACOBSNSMYPPMSRPHSDZTEVSAV
AVACOBSNSMYPPMSRPHSDZTEVSAV
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.08
0.5608 0.5608 0.5608 1.2728
0.5608 0.5608 0.5608 1.2728
0.5608 1.2728
1.2578
1.2578
1.2578
0.7075
1.0836
1.0836
0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 1.2633
0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 1.2633
63 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$$$
$$
$
$
$
$
$
$
$$$$$$$$$
$$$$$$$$$
(ANGIOTENSIN II RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
IRBESARTAN
IRBESARTAN/ HYDROCHLOROTHIAZIDE
LOSARTAN POTASSIUM
300 MG ORAL TABLET
150 MG * 12.5 MG ORAL TABLET
300 MG * 12.5 MG ORAL TABLET
300 MG * 25 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
000023733350000232810000002372398000023473260000231708700002316412000023284960000231600500002237925
000023733430000235739900002372886000023285180000236320800002330512000023374280000231601300002241818
000023733510000235740200002372894000023285260000236321600002330520000023374360000231602100002241819
0000237337800002357410000023729080000232853400002363224000023305390000233744400002316048
00002182815
00002182874
00002182882
AVA-IRBESARTANCO IRBESARTANIRBESARTANMYLAN-IRBESARTANPMS-IRBESARTANRATIO-IRBESARTANSANDOZ IRBESARTANTEVA-IRBESARTANAVAPRO
AVA-IRBESARTAN/HCTZCO IRBESARTAN/HCTIRBESARTAN/HCTZPMS-IRBESARTAN-HCTZRAN-IRBESARTAN HCTZRATIO-IRBESARTAN HCTZSANDOZ IRBESARTAN HCTTEVA-IRBESARTAN/HCTZAVALIDE 150/12.5
AVA-IRBESARTAN/HCTZCO IRBESARTAN/HCTIRBESARTAN/HCTZPMS-IRBESARTAN-HCTZRAN-IRBESARTAN HCTZRATIO-IRBESARTAN HCTZSANDOZ IRBESARTAN HCTTEVA-IRBESARTAN/HCTZAVALIDE 300/12.5
AVA-IRBESARTAN/HCTZCO IRBESARTAN/HCTIRBESARTAN/HCTZPMS-IRBESARTAN-HCTZRAN-IRBESARTAN HCTZRATIO-IRBESARTAN HCTZSANDOZ IRBESARTAN HCTTEVA-IRBESARTAN/HCTZ
COZAAR
COZAAR
COZAAR
AVACOBSNSMYPPMSRPHSDZTEVSAV
AVACOBSNSPMSRANRPHSDZTEVSAV
AVACOBSNSPMSRANRPHSDZTEVSAV
AVACOBSNSPMSRANRPHSDZTEV
MFC
MFC
MFC
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.08
0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 1.2633
0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 1.2633
0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 0.5444 1.2633
0.5407 0.5407 0.5407 0.5407 0.5407 0.5407 0.5407 0.5407
1.2590
1.2590
1.2590
64 EFFECTIVE APRIL 1, 2012
$$$$$$$$$
$$$$$$$$$
$$$$$$$$$
$$$$$$$$
$
$
$
(ANGIOTENSIN II RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
LOSARTAN POTASSIUM/ HYDROCHLOROTHIAZIDE
TELMISARTAN
TELMISARTAN/ AMLODIPINE BESYLATE
TELMISARTAN/ HYDROCHLOROTHIAZIDE
VALSARTAN
50 MG * 12.5 MG ORAL TABLET
100 MG * 12.5 MG ORAL TABLET
100 MG * 25 MG ORAL TABLET
40 MG ORAL TABLET
80 MG ORAL TABLET
40 MG * 5 MG ORAL TABLET
40 MG * 10 MG ORAL TABLET
80 MG * 5 MG ORAL TABLET
80 MG * 10 MG ORAL TABLET
80 MG * 12.5 MG ORAL TABLET
80 MG * 25 MG ORAL TABLET
80 MG ORAL TABLET
160 MG ORAL TABLET
00002230047
00002297841
00002241007
00002240769
00002240770
00002371022
00002371030
00002371049
00002371057
00002244344
00002318709
00002371529000023671220000233749500002363100000023567590000235665100002244781
00002371537000023671300000233750900002363119000023567670000235667800002244782
HYZAAR
HYZAAR
HYZAAR DS
MICARDIS
MICARDIS
TWYNSTA
TWYNSTA
TWYNSTA
TWYNSTA
MICARDIS PLUS
MICARDIS PLUS
APO-VALSARTANAVA-VALSARTANCO VALSARTANRAN-VALSARTANSANDOZ VALSARTANTEVA-VALSARTANDIOVAN
APO-VALSARTANAVA-VALSARTANCO VALSARTANRAN-VALSARTANSANDOZ VALSARTANTEVA-VALSARTANDIOVAN
MFC
MFC
MFC
BOE
BOE
BOE
BOE
BOE
BOE
BOE
BOE
APXAVACOBRANSDZTEVNOV
APXAVACOBRANSDZTEVNOV
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.08
1.2590
1.2327
1.2590
1.1657
1.1657
0.6818
0.6818
0.6818
0.6818
1.1657
1.1657
0.5724 0.5724 0.5724 0.5724 0.5724 0.5724 1.2896
0.5724 0.5724 0.5724 0.5724 0.5724 0.5724 1.2892
65 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$
$$$$$$$
$$$$$$$
(ANGIOTENSIN II RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
VALSARTAN
VALSARTAN/ HYDROCHLOROTHIAZIDE
320 MG ORAL TABLET
80 MG * 12.5 MG ORAL TABLET
160 MG * 12.5 MG ORAL TABLET
160 MG * 25 MG ORAL TABLET
320 MG * 12.5 MG ORAL TABLET
320 MG * 25 MG ORAL TABLET
000023715450000236714900002356775000023566860000233751700002289504
0000236706800002373734000023566940000235699600002241900
0000236707600002373742000023567080000235700300002241901
0000236708400002373750000023567160000235701100002246955
0000236709200002373769000023570380000235672400002308908
0000236710600002373777000023570460000235673200002308916
APO-VALSARTANAVA-VALSARTANSANDOZ VALSARTANTEVA-VALSARTANCO VALSARTANDIOVAN
AVA-VALSARTAN HCTMYLAN-VALSARTAN HCTZSANDOZ VALSARTAN HCTTEVA-VALSARTAN/HCTZDIOVAN-HCT
AVA-VALSARTAN HCTMYLAN-VALSARTAN HCTZSANDOZ VALSARTAN HCTTEVA-VALSARTAN/HCTZDIOVAN-HCT
AVA-VALSARTAN HCTMYLAN-VALSARTAN HCTZSANDOZ VALSARTAN HCTTEVA-VALSARTAN/HCTZDIOVAN-HCT
AVA-VALSARTAN HCTMYLAN-VALSARTAN HCTZTEVA-VALSARTAN/HCTZSANDOZ VALSARTAN HCTDIOVAN-HCT
AVA-VALSARTAN HCTMYLAN-VALSARTAN HCTZTEVA-VALSARTAN/HCTZSANDOZ VALSARTAN HCTDIOVAN-HCT
APXAVASDZTEVCOBNOV
AVAMYPSDZTEVNOV
AVAMYPSDZTEVNOV
AVAMYPSDZTEVNOV
AVAMYPTEVSDZNOV
AVAMYPTEVSDZNOV
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.08
0.5500 0.5500 0.5500 0.5500 0.5501 1.2421
0.5724 0.5724 0.5724 0.5724 1.2834
0.5724 0.5724 0.5724 0.5724 1.2869
0.5724 0.5724 0.5724 0.5724 1.2912
0.5633 0.5633 0.5633 0.5634 1.2719
0.5633 0.5633 0.5633 0.5634 1.2719
66 EFFECTIVE APRIL 1, 2012
$$$$$$
$$$$$
$$$$$
$$$$$
$$$$$
$$$$$
(ANGIOTENSIN II RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
HYDROCHLOROTHIAZIDE/ SPIRONOLACTONE
SPIRONOLACTONE
25 MG * 25 MG ORAL TABLET
50 MG * 50 MG ORAL TABLET
25 MG ORAL TABLET
100 MG ORAL TABLET
0000061323100000180408
0000065718200000594377
0000061321500000028606
0000061322300000285455
NOVO-SPIROZINEALDACTAZIDE 25
NOVO-SPIROZINEALDACTAZIDE 50
NOVO-SPIROTONALDACTONE
NOVO-SPIROTONALDACTONE
TEVPFI
TEVPFI
TEVPFI
TEVPFI
CARDIOVASCULAR DRUGS
RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITORS
24:00
24:32.20
0.1088 0.1405
0.2301 0.2979
0.1068 0.1405
0.2487 0.3311
67 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$
$$
$$
(MINERALOCORTICOID (ALDOSTERONE) RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

28:00 Central N
ervous System A
gents
28:00
Central Nervous System Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
COMPOUND PRESCRIPTION
COMPOUND PRESCRIPTION
ASA
BUTALBITAL/ CAFFEINE/ ASA
TOPICAL
TOPICAL
TOPICAL
TOPICAL
650 MG ORAL ENTERIC-COATED TABLET
50 MG * 40 MG * 330 MG ORAL TABLET
50 MG * 40 MG * 330 MG ORAL CAPSULE
00000999105
00000999205
00000999102
00000999202
00000010340
00000608211
0000060823800000226327
COMPD- NSAID/ ANALG/MUSCLE RELAX (NOT DICLOFENAC)-TOPICAL
COMPD-NSAID/ ANALG/MUSCLE RELAX (NOT DICLOFENAC)-TOPICAL
COMPOUND-DICLOFENAC (TOPICAL)
COMPOUND- DICLOFENAC (TOPICAL)
ENTROPHEN 10
RATIO-TECNAL
RATIO-TECNALFIORINAL
XXX
XXX
XXX
XXX
PPH
RPH
RPHNOV
(SALICYLATES)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
ANALGESICS AND ANTIPYRETICS
ANALGESICS AND ANTIPYRETICS
28
28
28
:00
:00
:00
28:08
28:08.04
28:08.04.24
0.0000
0.0000
0.0000
0.0000
0.0879
0.6088
1.0304 1.6313
69 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
(NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
NONSTEROIDAL ANTI-INFLAMMATORY AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DICLOFENAC SODIUM
DICLOFENAC SODIUM/ MISOPROSTOL
75 MG ORAL SUSTAINED-RELEASE TABLET
100 MG ORAL SUSTAINED-RELEASE TABLET
25 MG ORAL ENTERIC-COATED TABLET
50 MG ORAL ENTERIC-COATED TABLET
50 MG RECTAL SUPPOSITORY
100 MG RECTAL SUPPOSITORY
50 MG * 200 MCG ORAL TABLET
75 MG * 200 MCG ORAL TABLET
00002162814000023666810000235240000002158582000022315040000226190100000782459
000020911940000236670300002048698000022315050000226194400000590827
000008391750000236666500000808539000008860170000230261600002261952
00000839183000023666730000235239700000808547000023026240000226196000000514012
00002231506000022412240000226192800000632724
000022315080000226193600000632732
00001917056
00002229837
APO-DICLO SRAVA-DICLOFENAC SRDICLOFENAC SODIUM SRNOVO-DIFENAC SRPMS-DICLOFENAC-SRSANDOZ DICLOFENAC SRVOLTAREN SR
APO-DICLO SRAVA-DICLOFENAC SRNOVO-DIFENAC SRPMS-DICLOFENAC-SRSANDOZ DICLOFENAC SRVOLTAREN SR
APO-DICLOAVA-DICLOFENACNOVO-DIFENACNU-DICLOPMS-DICLOFENACSANDOZ DICLOFENAC
APO-DICLOAVA-DICLOFENACDICLOFENAC SODIUMNOVO-DIFENACPMS-DICLOFENACSANDOZ DICLOFENACVOLTAREN
PMS-DICLOFENACSANDOZ DICLOFENACSANDOZ DICLOFENACVOLTAREN
PMS-DICLOFENACSANDOZ DICLOFENACVOLTAREN
ARTHROTEC-50
ARTHROTEC-75
APXAVASNSTEVPMSSDZNOV
APXAVATEVPMSSDZNOV
APXAVATEVNXPPMSSDZ
APXAVASNSTEVPMSSDZNOV
PMSSDZSDZNOV
PMSSDZNOV
PFI
PFI
(OTHER NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.04.92
0.5706 0.5706 0.5706 0.5706 0.5706 0.5706 1.2832
0.7608 0.7608 0.7608 0.7608 0.7608 1.8292
0.1902 0.1902 0.1902 0.1902 0.1902 0.1902
0.3804 0.3804 0.3804 0.3804 0.3804 0.3804 0.9305
0.6237 0.6237 0.6237 1.3974
0.8397 0.8397 1.8808
0.6507
0.8857
70 EFFECTIVE APRIL 1, 2012
$ 0.5706 $ 0.5706 $ 0.5706 $ 0.5706 $ 0.5706 $ 0.5706 $ 0.5706
$ 0.7608 $ 0.7608 $ 0.7608 $ 0.7608 $ 0.7608 $ 0.7608
$ 0.3804 $ 0.3804 $ 0.3804 $ 0.3804 $ 0.3804 $ 0.3804 $ 0.3804
MAC pricing has been applied based on the LCA Price for 3 x 25 mg oral enteric-coated tablets.
MAC pricing has been applied based on the LCA Price for 4 X 25 mg oral enteric-coated tablets.
MAC pricing has been applied based on the LCA Price for 2 x 25 mg oral enteric-coated tablets.
$$$$$$$
$$$$$$
$$$$$$
$$$$$$$
$$$$
$$$
$
$
NONSTEROIDAL ANTI-INFLAMMATORY AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DIFLUNISAL
ETODOLAC
FLOCTAFENINE
FLURBIPROFEN
IBUPROFEN
INDOMETHACIN
250 MG ORAL TABLET
500 MG ORAL TABLET
200 MG ORAL CAPSULE
300 MG ORAL CAPSULE
200 MG ORAL TABLET
400 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
300 MG ORAL TABLET
400 MG ORAL TABLET
600 MG ORAL TABLET
25 MG ORAL CAPSULE
50 MG ORAL CAPSULE
50 MG RECTAL SUPPOSITORY
0000203948600002048493
00002039494
00002232317
00002232318
00002244680
00002244681
000019120460000210050900002020661
000019120380000210051700002020688
00000441651
0000050605200000629340
000006293590000058511400002020726
000006111580000033742000000865850
000006111660000033743900000865869
00002231799
APO-DIFLUNISALNOVO-DIFLUNISAL FC
APO-DIFLUNISAL
ETODOLAC
ETODOLAC
FLOCTAFENINE
FLOCTAFENINE
APO-FLURBIPROFENNOVO-FLURPROFENNU-FLURBIPROFEN
APO-FLURBIPROFENNOVO-FLURPROFENNU-FLURBIPROFEN
APO-IBUPROFEN
APO-IBUPROFENNOVO-PROFEN
NOVO-PROFENAPO-IBUPROFENNU-IBUPROFEN
APO-INDOMETHACINNOVO-METHACINNU-INDO
APO-INDOMETHACINNOVO-METHACINNU-INDO
SANDOZ INDOMETHACIN
APXTEV
APX
AAP
AAP
AAP
AAP
APXTEVNXP
APXTEVNXP
APX
APXTEV
TEVAPXNXP
APXTEVNXP
APXTEVNXP
SDZ
(OTHER NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.04.92
0.5646 0.5646
0.7150
0.8170
0.8170
0.4488
0.8732
0.2564 0.2564 0.2564
0.3508 0.3508 0.3508
0.1087
0.0758 0.0758
0.0465 0.1313 0.1313
0.0871 0.0871 0.0871
0.1511 0.1511 0.1511
0.8842
71 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$
$
$
$
$$$
$$$
$
$$
$$$
$$$
$$$
$
NONSTEROIDAL ANTI-INFLAMMATORY AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
INDOMETHACIN
KETOPROFEN
KETOROLAC TROMETHAMINE
MEFENAMIC ACID
NABUMETONE
NAPROXEN
100 MG RECTAL SUPPOSITORY
200 MG ORAL SUSTAINED-RELEASE TABLET
50 MG ORAL ENTERIC-COATED TABLET
100 MG ORAL ENTERIC-COATED TABLET
50 MG ORAL CAPSULE
100 MG RECTAL SUPPOSITORY
10 MG ORAL TABLET
10 MG / ML INJECTION
30 MG / ML INJECTION
250 MG ORAL CAPSULE
500 MG ORAL TABLET
125 MG ORAL TABLET
250 MG ORAL TABLET
0000193413900002231800
00002172577
00000790435
00000842664
00000790427
00002015951
00002229080000022302010000223791000002162660
00002162644
00002239944
00002229452
00002238639000022445630000234328200002240867
00000522678
00000522651000023507500000056535000000865648
RATIO-INDOMETHACINSANDOZ INDOMETHACIN
KETOPROFEN SR
KETOPROFEN-E
KETOPROFEN-E
KETOPROFEN
PMS-KETOPROFEN
APO-KETOROLACNOVO-KETOROLACNU-KETOROLACTORADOL
TORADOL
KETOROLAC TROMETHAMINE
MEFENAMIC
APO-NABUMETONEMYLAN-NABUMETONENABUMETONENOVO-NABUMETONE
APO-NAPROXEN
APO-NAPROXENNAPROXENNOVO-NAPROXNU-NAPROX
RPHSDZ
AAP
AAP
AAP
AAP
PMS
APXTEVNXPHLR
HLR
SDZ
AAP
APXMYPSNSTEV
APX
APXSNSTEVNXP
(OTHER NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.04.92
0.8920 0.8920
1.4932
0.3626
0.7335
0.3626
1.1453
0.4085 0.4085 0.4085 0.7441
2.4058
4.3000
0.5362
0.3769 0.3769 0.3769 0.3769
0.0781
0.1068 0.1068 0.1068 0.1068
72 EFFECTIVE APRIL 1, 2012
$ 1.4670
MAC pricing has been applied based on the price for 2 x 100 mg oral enteric-coated tablets.
$$
$
$
$
$
$
$$$$
$
$
$
$$$$
$
$$$$
NONSTEROIDAL ANTI-INFLAMMATORY AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
NAPROXEN375 MG ORAL TABLET
500 MG ORAL TABLET
750 MG ORAL SUSTAINED-RELEASE TABLET
250 MG ORAL ENTERIC-COATED TABLET
375 MG ORAL ENTERIC-COATED TABLET
500 MG ORAL ENTERIC-COATED TABLET
25 MG / ML ORAL SUSPENSION
500 MG RECTAL SUPPOSITORY
0000060080600002365820000023507690000062709700000865656
0000059227700002365839000023507770000058986100000865664
00002162466
0000224669900002365847000023507850000224331200002162792
00002246700000023658550000224343200002350793000022433130000229470200002162415
00002246701000023658630000224102400002350807000022433140000229471000002162423
00002162431
00002017237
APO-NAPROXENAVA-NAPROXENNAPROXENNOVO-NAPROXNU-NAPROX
APO-NAPROXENAVA-NAPROXENNAPROXENNOVO-NAPROXNU-NAPROX
NAPROSYN SR
APO-NAPROXEN ECAVA-NAPROXEN ECNAPROXEN ECNOVO-NAPROX ECNAPROSYN E
APO-NAPROXEN ECAVA-NAPROXEN ECMYLAN-NAPROXEN ECNAPROXEN ECNOVO-NAPROX ECPMS-NAPROXEN ECNAPROSYN E
APO-NAPROXEN ECAVA-NAPROXEN ECMYLAN-NAPROXEN ECNAPROXEN ECNOVO-NAPROX ECPMS-NAPROXEN ECNAPROSYN E
NAPROSYN
PMS-NAPROXEN
APXAVASNSTEVNXP
APXAVASNSTEVNXP
HLR
APXAVASNSTEVHLR
APXAVAMYPSNSTEVPMSHLR
APXAVAMYPSNSTEVPMSHLR
HLR
PMS
(OTHER NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.04.92
0.1458 0.1458 0.1458 0.1458 0.1458
0.2110 0.2110 0.2110 0.2110 0.2110
1.4202
0.2467 0.2467 0.2467 0.2467 0.4487
0.3234 0.3234 0.3234 0.3234 0.3234 0.3234 0.5890
0.5842 0.5842 0.5842 0.5842 0.5842 0.5842 1.0623
0.0673
0.8883
73 EFFECTIVE APRIL 1, 2012
$ 0.2916
$ 0.1068 $ 0.1068 $ 0.1068 $ 0.1068 $ 0.1068
$ 0.1458 $ 0.1458 $ 0.1458 $ 0.1458 $ 0.1458 $ 0.1458 $ 0.1458
$ 0.2110 $ 0.2110 $ 0.2110 $ 0.2110 $ 0.2110 $ 0.2110 $ 0.2110
UNIT OF ISSUE - REFER TO PRICE POLICY
MAC pricing has been applied based on the LCA price for 2 x 375 mg oral tablets.
MAC pricing has been applied based on the LCA price for 1 x 250 mg oral tablet.
MAC pricing has been applied based on the LCA price for 1 x 375 mg oral tablet.
MAC pricing has been applied based on the LCA price for 1 x 500 mg oral tablet.
$$$$$
$$$$$
$
$$$$$
$$$$$$$
$$$$$$$
$
$
NONSTEROIDAL ANTI-INFLAMMATORY AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
NAPROXEN SODIUM
PIROXICAM
SULINDAC
TENOXICAM
TIAPROFENIC ACID
275 MG ORAL TABLET
550 MG ORAL TABLET
10 MG ORAL CAPSULE
20 MG ORAL CAPSULE
20 MG RECTAL SUPPOSITORY
150 MG ORAL TABLET
200 MG ORAL TABLET
20 MG ORAL TABLET
200 MG ORAL TABLET
300 MG ORAL TABLET
00000784354000023510130000077838900002162725
00001940309000023510210000202660000002162717
000006428860000069571800000865761
000006428940000069569600000865788
00002154463
000007783540000074558800002042576
000007783620000074559600002042584
00002230661
0000213611200002179679
000021361200000217968700002146886
APO-NAPRO-NANAPROXEN SODIUMNOVO-NAPROX SODIUMANAPROX
APO-NAPRO-NA DSNAPROXEN SODIUM DSNOVO-NAPROX SODIUM DSANAPROX DS
APO-PIROXICAMNOVO-PIROCAMNU-PIROX
APO-PIROXICAMNOVO-PIROCAMNU-PIROX
PMS-PIROXICAM
APO-SULINNOVO-SUNDACNU-SULINDAC
APO-SULINNOVO-SUNDACNU-SULINDAC
TENOXICAM
APO-TIAPROFENICNOVO-TIAPROFENIC
APO-TIAPROFENICNOVO-TIAPROFENICNU-TIAPROFENIC
APXSNSTEVHLR
APXSNSTEVHLR
APXTEVNXP
APXTEVNXP
PMS
APXTEVNXP
APXTEVNXP
AAP
APXTEV
APXTEVNXP
(OTHER NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.04.92
0.3422 0.3422 0.3422 0.6707
0.6667 0.6667 0.6667 1.2913
0.4147 0.4147 0.4147
0.7158 0.7158 0.7158
2.0580
0.3824 0.3824 0.3824
0.4840 0.4840 0.4840
1.2418
0.3437 0.3437
0.4104 0.4104 0.4104
74 EFFECTIVE APRIL 1, 2012
$$$$
$$$$
$$$
$$$
$
$$$
$$$
$
$$
$$$
NONSTEROIDAL ANTI-INFLAMMATORY AGENTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ASA/ CODEINE PHOSPHATE/ CAFFEINE CITRATE
BUTALBITAL/ CODEINE PHOSPHATE/ ASA/ CAFFEINE
CODEINE PHOSPHATE
CODEINE PHOSPHATE/ ACETAMINOPHEN
CODEINE PHOSPHATE/ ACETAMINOPHEN/ CAFFEINE
CODEINE PHOSPHATE/ ASA/ CAFFEINE CITRATE
CODEINE PHOSPHATE/ ASA/ MEPROBAMATE/ CAFFEINE CITRATE
375 MG * 15 MG * 30 MG ORAL TABLET
50 MG * 15 MG * 330 MG * 40 MG ORAL CAPSULE
50 MG * 30 MG * 330 MG * 40 MG ORAL CAPSULE
15 MG ORAL TABLET
30 MG ORAL TABLET
5 MG / ML ORAL SYRUP
30 MG / ML INJECTION
30 MG * 300 MG ORAL TABLET
60 MG * 300 MG ORAL TABLET
1.6 MG / ML * 32 MG / ML ORAL ELIXIR
15 MG * 300 MG * 15 MG ORAL TABLET
30 MG * 300 MG * 15 MG ORAL TABLET
30 MG * 375 MG * 30 MG ORAL TABLET
15 MG * 350 MG * 200 MG * 30 MG ORAL TABLET
00002234510
0000060820300000176192
0000060818100000176206
00000593435
00000593451
00000779474
00000544884
00000608882
0000062146300002163918
00002163942
0000065324100002163934
0000065327600002163926
00002238645
00002238646
282
RATIO-TECNAL-C 1/4FIORINAL-C 1/4
RATIO-TECNAL-C 1/2FIORINAL-C 1/2
RATIO-CODEINE
RATIO-CODEINE
RATIO-CODEINE
CODEINE PHOSPHATE
RATIO-EMTEC-30
RATIO-LENOLTEC NO.4TYLENOL NO. 4
TYLENOL WITH CODEINE
RATIO-LENOLTEC NO.2TYLENOL NO. 2
RATIO-LENOLTEC NO.3TYLENOL NO. 3
292
282 MEP
PPH
RPHNOV
RPHNOV
RPH
RPH
RPH
SDZ
RPH
RPHJAI
JAI
RPHJAI
RPHJAI
PPH
PPH
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.08
0.0734
1.1051 1.7495
1.3532 2.1423
0.0723
0.0966
0.0304
1.4100
0.1570
0.1652 0.2018
0.1121
0.0710 0.0868
0.0782 0.0955
0.1898
0.2370
75 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$
$$
$
$
$
$
$
$$
$
$$
$$
$
$
(OPIATE AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
COMPOUND PRESCRIPTION
HYDROMORPHONE HCL1 MG ORAL TABLET
2 MG ORAL TABLET
4 MG ORAL TABLET
8 MG ORAL TABLET
3 MG ORAL CONTROLLED-RELEASE CAPSULE
4.5 MG ORAL CONTROLLED-RELEASE CAPSULE
6 MG ORAL CONTROLLED-RELEASE CAPSULE
9 MG ORAL CONTROLLED-RELEASE CAPSULE
12 MG ORAL CONTROLLED-RELEASE CAPSULE
18 MG ORAL CONTROLLED-RELEASE CAPSULE
24 MG ORAL CONTROLLED-RELEASE CAPSULE
30 MG ORAL CONTROLLED-RELEASE CAPSULE
1 MG / ML ORAL LIQUID
2 MG / ML INJECTION
00000999108
00000999208
000008854440000231940300000705438
000008854360000231941100000125083
000008854010000231943800000125121
000008854280000231944600000786543
00002125323
00002359502
00002125331
00002359510
00002125366
00002243562
00002125382
00002125390
0000191638600000786535
0000214590100000627100
COMPOUND NARCOTIC MIXTURES - ORAL AND INJECTION
COMPOUND NARCOTIC MIXTURES - ORAL AND INJECTION
PMS-HYDROMORPHONETEVA-HYDROMORPHONEDILAUDID
PMS-HYDROMORPHONETEVA-HYDROMORPHONEDILAUDID
PMS-HYDROMORPHONETEVA-HYDROMORPHONEDILAUDID
PMS-HYDROMORPHONETEVA-HYDROMORPHONEDILAUDID
HYDROMORPH CONTIN
HYDROMORPH CONTIN
HYDROMORPH CONTIN
HYDROMORPH CONTIN
HYDROMORPH CONTIN
HYDROMORPH CONTIN
HYDROMORPH CONTIN
HYDROMORPH CONTIN
PMS-HYDROMORPHONEDILAUDID
HYDROMORPHONEDILAUDID
XXX
XXX
PMSTEVPUR
PMSTEVPUR
PMSTEVPUR
PMSTEVPUR
PUR
PUR
PUR
PUR
PUR
PUR
PUR
PUR
PMSPUR
SDZPUR
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.08
0.0000
0.0000
0.0959 0.0959 0.1031
0.1417 0.1417 0.1523
0.2240 0.2240 0.2408
0.3528 0.3528 0.3793
0.7251
0.8750
1.0874
1.4340
1.8845
2.7187
3.4792
4.1683
0.0665 0.0851
1.1380 1.2255
76 EFFECTIVE APRIL 1, 2012
$
$
$$$
$$$
$$$
$$$
$
$
$
$
$
$
$
$
$$
$$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
(OPIATE AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
HYDROMORPHONE HCL
MEPERIDINE HCL
METHADONE COMPOUND
METHADONE HCL
MORPHINE HCL
10 MG / ML INJECTION
20 MG / ML INJECTION
50 MG / ML INJECTION
250 MG / VIAL INJECTION
3 MG RECTAL SUPPOSITORY
50 MG ORAL TABLET
50 MG / ML INJECTION
75 MG / ML INJECTION
100 MG / ML INJECTION
ORAL LIQUID
1 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
25 MG ORAL TABLET
1 MG / ML ORAL SOLUTION
10 MG / ML ORAL LIQUID
30 MG ORAL SUSTAINED-RELEASE TABLET
60 MG ORAL SUSTAINED-RELEASE TABLET
1 MG / ML ORAL SYRUP
5 MG / ML ORAL SYRUP
10 MG / ML ORAL SYRUP
0000214592800000622133
00002145936
00002146126
00002085895
00001916394
00002138018
00000725765
00000725757
00000725749
00000999995
00002247698
00002247699
00002247700
00002247701
00002247694
00002241377
00000776181
00000776203
00000607762
00000607770
00000690783
HYDROMORPHONE HPDILAUDID-HP
HYDROMORPHONE HP 20
HYDROMORPHONE HP 50
DILAUDID STERILE POWDER
PMS-HYDROMORPHONE
DEMEROL
MEPERIDINE HYDROCHLORIDE
MEPERIDINE HYDROCHLORIDE
MEPERIDINE HYDROCHLORIDE
METHADONE
METADOL
METADOL
METADOL
METADOL
METADOL
METADOL CONCENTRATE
M.O.S.-SR
M.O.S.-SR
RATIO-MORPHINE
RATIO-MORPHINE
RATIO-MORPHINE
SDZPUR
SDZ
SDZ
PUR
PMS
SAV
SDZ
SDZ
SDZ
XXX
PAL
PAL
PAL
PAL
PAL
PAL
VCL
VCL
RPH
RPH
RPH
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.08
2.7860 2.9992
4.5100
13.1500
75.4032
2.9640
0.1616
0.9600
1.0100
1.0699
0.0000
0.1689
0.5627
0.9003
1.6879
0.1017
0.3676
0.4960
0.8744
0.0151
0.0602
0.1931
77 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
(OPIATE AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
MORPHINE HCL
MORPHINE SULFATE
20 MG / ML ORAL SYRUP
5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
25 MG ORAL TABLET
30 MG ORAL TABLET
50 MG ORAL TABLET
15 MG ORAL SUSTAINED-RELEASE TABLET
30 MG ORAL SUSTAINED-RELEASE TABLET
60 MG ORAL SUSTAINED-RELEASE TABLET
100 MG ORAL SUSTAINED-RELEASE TABLET
200 MG ORAL SUSTAINED-RELEASE TABLET
10 MG ORAL EXTENDED-RELEASE CAPSULE
15 MG ORAL EXTENDED-RELEASE CAPSULE
30 MG ORAL EXTENDED-RELEASE CAPSULE
00000690791
000005946520000200977300002014203
000005946440000200976500002014211
00002014238
0000059463600002009749
00002014254
0000067596200002009706
00002350815000023027640000224479000002015439
00002350890000023027720000224479100002014297
00002350912000023027800000224479200002014300
000023509200000230279900002014319
000023509470000230280200002014327
00002019930
00002177749
00002019949
RATIO-MORPHINE
STATEXM.O.S. SULFATEMS.IR
STATEXM.O.S. SULFATEMS.IR
MS.IR
STATEXM.O.S. SULFATE
MS.IR
STATEXM.O.S. SULFATE
MORPHINE SRNOVO-MORPHINE SRSANDOZ MORPHINE SRMS CONTIN
MORPHINE SRNOVO-MORPHINE SRSANDOZ MORPHINE SRMS CONTIN
MORPHINE SRNOVO-MORPHINE SRSANDOZ MORPHINE SRMS CONTIN
MORPHINE SRNOVO-MORPHINE SRMS CONTIN
MORPHINE SRNOVO-MORPHINE SRMS CONTIN
M-ESLON
M-ESLON
M-ESLON
RPH
PALVCLPUR
PALVCLPUR
PUR
PALVCL
PUR
PALVCL
SNSTEVSDZPUR
SNSTEVSDZPUR
SNSTEVSDZPUR
SNSTEVPUR
SNSTEVPUR
ETP
ETP
ETP
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.08
0.5489
0.1182 0.1214 0.1333
0.1828 0.1876 0.2075
0.3698
0.2419 0.2482
0.4741
0.3709 0.3807
0.3550 0.3550 0.3550 0.7310
0.5486 0.5486 0.5486 1.1062
0.9628 0.9628 0.9628 1.9490
1.5853 1.5853 2.9713
2.9473 2.9473 5.5244
0.3208
0.3706
0.5531
78 EFFECTIVE APRIL 1, 2012
$
$$$
$$$
$
$$
$
$$
$$$$
$$$$
$$$$
$$$
$$$
$
$
$
(OPIATE AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
MORPHINE SULFATE
OPIUM/ BELLADONNA
60 MG ORAL EXTENDED-RELEASE CAPSULE
100 MG ORAL EXTENDED-RELEASE CAPSULE
200 MG ORAL EXTENDED-RELEASE CAPSULE
10 MG ORAL SUSTAINED-RELEASE CAPSULE
20 MG ORAL SUSTAINED-RELEASE CAPSULE
50 MG ORAL SUSTAINED-RELEASE CAPSULE
100 MG ORAL SUSTAINED-RELEASE CAPSULE
1 MG / ML ORAL SYRUP
5 MG / ML ORAL SYRUP
20 MG / ML ORAL DROPS
50 MG / ML ORAL DROPS
0.5 MG / ML INJECTION
1 MG / ML INJECTION
10 MG / ML INJECTION
15 MG / ML INJECTION
25 MG / ML INJECTION
50 MG / ML INJECTION
5 MG RECTAL SUPPOSITORY
10 MG RECTAL SUPPOSITORY
20 MG RECTAL SUPPOSITORY
30 MG RECTAL SUPPOSITORY
65 MG * 15 MG RECTAL SUPPOSITORY
00002019957
00002019965
00002177757
00002242163
00002184435
00002184443
00002184451
00000591467
00000591475
00000621935
00000705799
00002021056
00002021048
00000392588
00000392561
00000676411
00000617288
00000632228
00000632201
00000596965
00000639389
00001901869
M-ESLON
M-ESLON
M-ESLON
KADIAN
KADIAN
KADIAN
KADIAN
STATEX
STATEX
STATEX
STATEX
MORPHINE LP EPIDURAL
MORPHINE LP EPIDURAL
MORPHINE SULFATE
MORPHINE SULFATE
MORPHINE HP 25
MORPHINE HP 50
STATEX
STATEX
STATEX
STATEX
SANDOZ OPIUM & BELLADONNA
ETP
ETP
ETP
ABB
ABB
ABB
ABB
PAL
PAL
PAL
PAL
SDZ
SDZ
SDZ
SDZ
SDZ
SDZ
PAL
PAL
PAL
PAL
SDZ
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.08
0.9817
2.1128
4.2254
0.3680
0.7151
1.3145
2.2926
0.0200
0.0803
0.4980
0.9464
1.1420
2.2841
0.9900
1.0050
2.8900
3.9900
1.6690
1.8640
2.2190
2.4340
2.8800
79 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
(OPIATE AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
OXYCODONE HCL
OXYCODONE HCL/ ACETAMINOPHEN
5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
5 MG ORAL CONTROLLED-RELEASE TABLET
10 MG ORAL CONTROLLED-RELEASE TABLET
15 MG ORAL CONTROLLED-RELEASE TABLET
20 MG ORAL CONTROLLED-RELEASE TABLET
30 MG ORAL CONTROLLED-RELEASE TABLET
40 MG ORAL CONTROLLED-RELEASE TABLET
60 MG ORAL CONTROLLED-RELEASE TABLET
80 MG ORAL CONTROLLED-RELEASE TABLET
10 MG RECTAL SUPPOSITORY
20 MG RECTAL SUPPOSITORY
2.5 MG * 325 MG ORAL TABLET
5 MG * 325 MG ORAL TABLET
0000231997700000789739
000023199850000044394800002240131
000023199930000226298300002240132
00002258129
0000220244100002372525
0000232319200002372533
0000237279700002202468
0000232320600002372541
0000237256800002202476
0000232321400002372576
0000237258400002202484
00000392480
00000392472
00001916491
000023246280000191654800002361361000006081650000230789800001916475
PMS-OXYCODONESUPEUDOL
PMS-OXYCODONESUPEUDOLOXY-IR
PMS-OXYCODONESUPEUDOLOXY-IR
OXYCONTIN
OXYCONTINOXYNEO
OXYCONTINOXYNEO
OXYNEOOXYCONTIN
OXYCONTINOXYNEO
OXYNEOOXYCONTIN
OXYCONTINOXYNEO
OXYNEOOXYCONTIN
SUPEUDOL
SUPEUDOL
PERCOCET DEMI
APO-OXYCODONEENDOCETOXYCODONE/ACETRATIO-OXYCOCETSANDOZ-OXYCODONE ACETPERCOCET
PMSSDZ
PMSSDZPUR
PMSSDZPUR
PUR
PURPUR
PURPUR
PURPUR
PURPUR
PURPUR
PURPUR
PURPUR
SDZ
SDZ
BMS
APXBMSSNSRPHSDZBMS
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
28:00
28:08.08
0.1332 0.1332
0.2283 0.2283 0.4150
0.3965 0.3965 0.7213
0.6772
0.9438 0.9438
1.1395 1.1395
1.4158 1.4179
1.8705 1.8705
2.4537 2.4618
3.3862 3.3862
4.5322 4.5472
2.2612
2.8700
0.6299
0.1285 0.1285 0.1285 0.1285 0.1285 0.7706
80 EFFECTIVE APRIL 1, 2012
$$
$$$
$$$
$
$$
$$
$$
$$
$$
$$
$$
$
$
$
$$$$$$
(OPIATE AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
OXYCODONE HCL/ ASA
BUPRENORPHINE HCL/ NALOXONE HYDROCHLORIDE DIHYDRATE
PENTAZOCINE HCL
PENTAZOCINE LACTATE
PRIMIDONE
CLOBAZAM
5 MG * 325 MG ORAL TABLET
2 MG (BASE) * 0.5 MG (BASE) ORAL SUBLINGUAL TABLET
8 MG (BASE) * 2 MG (BASE) ORAL SUBLINGUAL TABLET
50 MG (BASE) ORAL TABLET
30 MG / ML INJECTION
125 MG ORAL TABLET
250 MG ORAL TABLET
10 MG ORAL TABLET
00000608157
00002295695
00002295709
00002137984
00002241976
00000399310
00000396761
000022446380000223833400002244474
RATIO-OXYCODAN
SUBOXONE
SUBOXONE
TALWIN
TALWIN
PRIMIDONE
PRIMIDONE
APO-CLOBAZAMNOVO-CLOBAZAMPMS-CLOBAZAM
RPH
RBC
RBC
SAV
HSP
AAP
AAP
APXTEVPMS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANALGESICS AND ANTIPYRETICS
ANALGESICS AND ANTIPYRETICS
ANTICONVULSANTS
ANTICONVULSANTS
28
28
28
28
:00
:00
:00
:00
28:08.08
28:08.12
28:12.04
28:12.08
0.3879
2.6700
4.7300
0.4662
1.7660
0.0594
0.0935
0.2153 0.2153 0.2153
81 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$$$
(OPIATE AGONISTS)
(OPIATE PARTIAL AGONISTS)
(BARBITURATES)
(BENZODIAZEPINES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CLONAZEPAM
PHENYTOIN
PHENYTOIN SODIUM
0.25 MG ORAL TABLET
0.5 MG ORAL TABLET
1 MG ORAL TABLET
2 MG ORAL TABLET
50 MG ORAL CHEWABLE TABLET
6 MG / ML ORAL SUSPENSION
25 MG / ML ORAL SUSPENSION
30 MG ORAL CAPSULE
100 MG ORAL CAPSULE
50 MG / ML INJECTION
00002179660
0000217788900002270641000022309500000223902400002145227000022369480000204870100002207818000021036560000223396000000382825
00002270668000021452350000204872800002233982
000021778970000227067600002230951000022390250000214524300002048736000021037370000223398500000382841
00000023698
00000023442
0000225089600000023450
00000022772
00000022780
00000780626
PMS-CLONAZEPAM
APO-CLONAZEPAMCO CLONAZEPAMMYLAN-CLONAZEPAMNOVO-CLONAZEPAMPHL-CLONAZEPAMPHL-CLONAZEPAM-RPMS-CLONAZEPAMPMS-CLONAZEPAM-RRATIO-CLONAZEPAMSANDOZ CLONAZEPAMRIVOTRIL
CO CLONAZEPAMPHL-CLONAZEPAMPMS-CLONAZEPAMSANDOZ CLONAZEPAM
APO-CLONAZEPAMCO CLONAZEPAMMYLAN-CLONAZEPAMNOVO-CLONAZEPAMPHL-CLONAZEPAMPMS-CLONAZEPAMRATIO-CLONAZEPAMSANDOZ CLONAZEPAMRIVOTRIL
DILANTIN INFATABS
DILANTIN-30
TARO-PHENYTOINDILANTIN-125
DILANTIN
DILANTIN
PHENYTOIN SODIUM
PMS
APXCOBMYPTEVPHHPHHPMSPMSRPHSDZHLR
COBPHHPMSSDZ
APXCOBMYPTEVPHHPMSRPHSDZHLR
PFI
PFI
TARPFI
PFI
PFI
SDZ
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTICONVULSANTS
ANTICONVULSANTS
28
28
:00
:00
28:12.08
28:12.12
0.0719
0.1166 0.1166 0.1166 0.1166 0.1166 0.1166 0.1166 0.1166 0.1166 0.1166 0.2131
0.1860 0.1860 0.1860 0.1860
0.2010 0.2010 0.2010 0.2010 0.2010 0.2010 0.2010 0.2010 0.3673
0.0778
0.0429
0.0311 0.0505
0.0568
0.0789
2.6300
82 EFFECTIVE APRIL 1, 2012
$
$$$$$$$$$$$
$$$$
$$$$$$$$$
$
$
$$
$
$
$
(BENZODIAZEPINES)
(HYDANTOINS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ETHOSUXIMIDE
METHSUXIMIDE
CARBAMAZEPINE
250 MG ORAL CAPSULE
50 MG / ML ORAL SYRUP
300 MG ORAL CAPSULE
200 MG ORAL TABLET
100 MG ORAL CHEWABLE TABLET
200 MG ORAL CHEWABLE TABLET
200 MG ORAL SUSTAINED-RELEASE TABLET
400 MG ORAL SUSTAINED-RELEASE TABLET
20 MG / ML ORAL SUSPENSION
00000022799
00000023485
00000022802
00000402699000007827180000204256800000010405
00002231542000022618550000224440300000369810
00002231540000022618630000224440400000665088
00002241882000022315430000226183900000773611
00002241883000022315440000226184700000755583
0000236739400002194333
ZARONTIN
ZARONTIN
CELONTIN
APO-CARBAMAZEPINENOVO-CARBAMAZNU-CARBAMAZEPINETEGRETOL
PMS-CARBAMAZEPINESANDOZ CARBAMAZEPINETARO-CARBAMAZEPINETEGRETOL
PMS-CARBAMAZEPINESANDOZ CARBAMAZEPINETARO-CARBAMAZEPINETEGRETOL
MYLAN-CARBAMAZEPINE CRPMS-CARBAMAZEPINE-CRSANDOZ CARBAMAZEPINE CRTEGRETOL CR
MYLAN-CARBAMAZEPINE CRPMS-CARBAMAZEPINE-CRSANDOZ CARBAMAZEPINE CRTEGRETOL CR
TARO-CARBAMAZEPINETEGRETOL
ERF
ERF
ERF
APXTEVNXPNOV
PMSSDZTARNOV
PMSSDZTARNOV
MYPPMSSDZNOV
MYPPMSSDZNOV
TARNOV
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTICONVULSANTS
ANTICONVULSANTS
28
28
:00
:00
28:12.20
28:12.92
0.3443
0.0688
0.6378
0.0795 0.0795 0.0795 0.4157
0.0770 0.0770 0.0770 0.1710
0.1520 0.1520 0.1520 0.3374
0.1887 0.1887 0.1887 0.4191
0.3774 0.3774 0.3774 0.8381
0.0541 0.0807
83 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$$$$
$$$$
$$$$
$$$$
$$$$
$$
(SUCCINIMIDES)
(MISCELLANEOUS ANTICONVULSANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
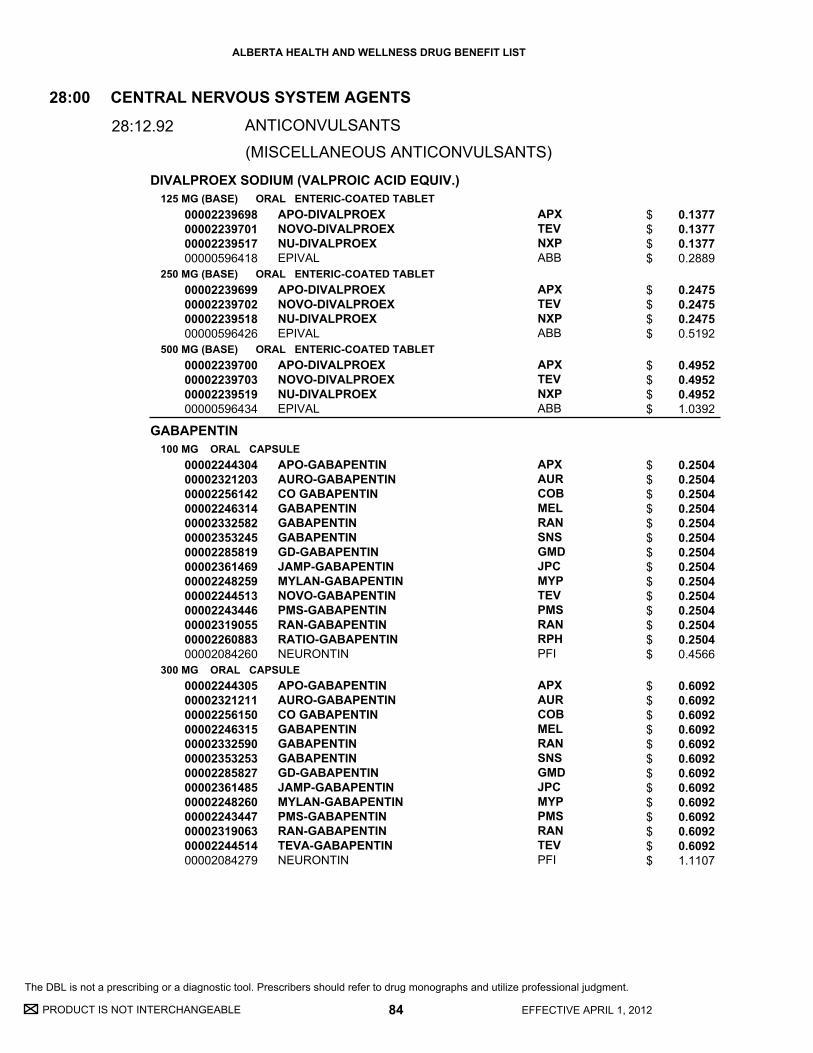
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DIVALPROEX SODIUM (VALPROIC ACID EQUIV.)
GABAPENTIN
125 MG (BASE) ORAL ENTERIC-COATED TABLET
250 MG (BASE) ORAL ENTERIC-COATED TABLET
500 MG (BASE) ORAL ENTERIC-COATED TABLET
100 MG ORAL CAPSULE
300 MG ORAL CAPSULE
00002239698000022397010000223951700000596418
00002239699000022397020000223951800000596426
00002239700000022397030000223951900000596434
0000224430400002321203000022561420000224631400002332582000023532450000228581900002361469000022482590000224451300002243446000023190550000226088300002084260
00002244305000023212110000225615000002246315000023325900000235325300002285827000023614850000224826000002243447000023190630000224451400002084279
APO-DIVALPROEXNOVO-DIVALPROEXNU-DIVALPROEXEPIVAL
APO-DIVALPROEXNOVO-DIVALPROEXNU-DIVALPROEXEPIVAL
APO-DIVALPROEXNOVO-DIVALPROEXNU-DIVALPROEXEPIVAL
APO-GABAPENTINAURO-GABAPENTINCO GABAPENTINGABAPENTINGABAPENTINGABAPENTINGD-GABAPENTINJAMP-GABAPENTINMYLAN-GABAPENTINNOVO-GABAPENTINPMS-GABAPENTINRAN-GABAPENTINRATIO-GABAPENTINNEURONTIN
APO-GABAPENTINAURO-GABAPENTINCO GABAPENTINGABAPENTINGABAPENTINGABAPENTINGD-GABAPENTINJAMP-GABAPENTINMYLAN-GABAPENTINPMS-GABAPENTINRAN-GABAPENTINTEVA-GABAPENTINNEURONTIN
APXTEVNXPABB
APXTEVNXPABB
APXTEVNXPABB
APXAURCOBMELRANSNSGMDJPCMYPTEVPMSRANRPHPFI
APXAURCOBMELRANSNSGMDJPCMYPPMSRANTEVPFI
CENTRAL NERVOUS SYSTEM AGENTS
ANTICONVULSANTS
28:00
28:12.92
0.1377 0.1377 0.1377 0.2889
0.2475 0.2475 0.2475 0.5192
0.4952 0.4952 0.4952 1.0392
0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.2504 0.4566
0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 0.6092 1.1107
84 EFFECTIVE APRIL 1, 2012
$$$$
$$$$
$$$$
$$$$$$$$$$$$$$
$$$$$$$$$$$$$
(MISCELLANEOUS ANTICONVULSANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
GABAPENTIN
LAMOTRIGINE
400 MG ORAL CAPSULE
25 MG ORAL TABLET
100 MG ORAL TABLET
150 MG ORAL TABLET
5 MG ORAL CHEWABLE TABLET
0000224430600002321238000022561690000224631600002332604000023532610000228583500002361493000022482610000224451500002243448000023190710000226090500002084287
00002245208000023430100000226549400002248232000022468970000224335200002142082
00002245209000023430290000226550800002248233000022468980000224335300002142104
00002245210000023430370000226551600002248234000022468990000224696300002142112
00002240115
APO-GABAPENTINAURO-GABAPENTINCO GABAPENTINGABAPENTINGABAPENTINGABAPENTINGD-GABAPENTINJAMP-GABAPENTINMYLAN-GABAPENTINNOVO-GABAPENTINPMS-GABAPENTINRAN-GABAPENTINRATIO-GABAPENTINNEURONTIN
APO-LAMOTRIGINELAMOTRIGINEMYLAN-LAMOTRIGINENOVO-LAMOTRIGINEPMS-LAMOTRIGINERATIO-LAMOTRIGINELAMICTAL
APO-LAMOTRIGINELAMOTRIGINEMYLAN-LAMOTRIGINENOVO-LAMOTRIGINEPMS-LAMOTRIGINERATIO-LAMOTRIGINELAMICTAL
APO-LAMOTRIGINELAMOTRIGINEMYLAN-LAMOTRIGINENOVO-LAMOTRIGINEPMS-LAMOTRIGINERATIO-LAMOTRIGINELAMICTAL
LAMICTAL
APXAURCOBMELRANSNSGMDJPCMYPTEVPMSRANRPHPFI
APXSNSMYPTEVPMSRPHGSK
APXSNSMYPTEVPMSRPHGSK
APXSNSMYPTEVPMSRPHGSK
GSK
CENTRAL NERVOUS SYSTEM AGENTS
ANTICONVULSANTS
28:00
28:12.92
0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 0.7259 1.3236
0.2088 0.2088 0.2088 0.2088 0.2088 0.2088 0.4108
0.8354 0.8354 0.8354 0.8354 0.8354 0.8354 1.6398
1.2530 1.2530 1.2530 1.2530 1.2530 1.2530 2.4167
0.1752
85 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$$$
$$$$$$$
$$$$$$$
$$$$$$$
$
(MISCELLANEOUS ANTICONVULSANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
LEVETIRACETAM
TOPIRAMATE
250 MG ORAL TABLET
500 MG ORAL TABLET
750 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
000022859240000237167700002274183000023533420000229610100002247027
000022859320000237168500002274191000023533500000229612800002247028
000022859400000237169300002274205000023533690000229613600002247029
000022796140000234580300002370972000022877650000231564500002263351000022488600000227118400002262991000022600500000235685600002230893
00002312085
000022796300000234583800002370980000022877730000231565300002263378000022488610000227119200002263009000022600690000235686400002230894
APO-LEVETIRACETAMAVA-LEVETIRACETAMCO LEVETIRACETAMLEVETIRACETAMPMS-LEVETIRACETAMKEPPRA
APO-LEVETIRACETAMAVA-LEVETIRACETAMCO LEVETIRACETAMLEVETIRACETAMPMS-LEVETIRACETAMKEPPRA
APO-LEVETIRACETAMAVA-LEVETIRACETAMCO LEVETIRACETAMLEVETIRACETAMPMS-LEVETIRACETAMKEPPRA
APO-TOPIRAMATEAURO-TOPIRAMATEAVA-TOPIRAMATECO TOPIRAMATEMINT-TOPIRAMATEMYLAN-TOPIRAMATENOVO-TOPIRAMATEPHL-TOPIRAMATEPMS-TOPIRAMATESANDOZ TOPIRAMATETOPIRAMATETOPAMAX
PMS-TOPIRAMATE
APO-TOPIRAMATEAURO-TOPIRAMATEAVA-TOPIRAMATECO TOPIRAMATEMINT-TOPIRAMATEMYLAN-TOPIRAMATENOVO-TOPIRAMATEPHL-TOPIRAMATEPMS-TOPIRAMATESANDOZ TOPIRAMATETOPIRAMATETOPAMAX
APXAVACOBSNSPMSUCB
APXAVACOBSNSPMSUCB
APXAVACOBSNSPMSUCB
APXAURAVACOBMPIMYPTEVPHHPMSSDZSNSJAI
PMS
APXAURAVACOBMPIMYPTEVPHHPMSSDZSNSJAI
CENTRAL NERVOUS SYSTEM AGENTS
ANTICONVULSANTS
28:00
28:12.92
0.9632 0.9632 0.9632 0.9632 0.9632 1.7859
1.1739 1.1739 1.1739 1.1739 1.1739 2.1959
1.6254 1.6254 1.6254 1.6254 1.6254 3.0404
0.6615 0.6615 0.6615 0.6615 0.6615 0.6615 0.6615 0.6615 0.6615 0.6615 0.6615 1.3746
1.0674
1.2537 1.2537 1.2537 1.2537 1.2537 1.2537 1.2537 1.2537 1.2537 1.2537 1.2537 2.6053
86 EFFECTIVE APRIL 1, 2012
$$$$$$
$$$$$$
$$$$$$
$$$$$$$$$$$$
$
$$$$$$$$$$$$
(MISCELLANEOUS ANTICONVULSANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
TOPIRAMATE
VALPROIC ACID
VIGABATRIN
200 MG ORAL TABLET
15 MG ORAL CAPSULE
25 MG ORAL CAPSULE
250 MG ORAL CAPSULE
500 MG ORAL ENTERIC-COATED CAPSULE
50 MG / ML ORAL SYRUP
500 MG ORAL TABLET
500 MG ORAL POWDER PACKET
000022796490000234584600002370999000022877810000231566100002263386000022488620000227120600002263017000022678370000235687200002230896
00002239907
00002239908
00002238048000021846480000210063000002237830000022307680000223971400000443840
0000221832100002229628
00002238370000022368070000214006300000443832
00002065819
00002068036
APO-TOPIRAMATEAURO-TOPIRAMATEAVA-TOPIRAMATECO TOPIRAMATEMINT-TOPIRAMATEMYLAN-TOPIRAMATENOVO-TOPIRAMATEPHL-TOPIRAMATEPMS-TOPIRAMATESANDOZ TOPIRAMATETOPIRAMATETOPAMAX
TOPAMAX SPRINKLE
TOPAMAX SPRINKLE
APO-VALPROICMYLAN-VALPROICNOVO-VALPROICNU-VALPROICPMS-VALPROIC ACIDSANDOZ VALPROICDEPAKENE
NOVO-VALPROICPMS-VALPROIC ACID E.C.
APO-VALPROICPMS-VALPROIC ACIDRATIO-VALPROICDEPAKENE
SABRIL
SABRIL
APXAURAVACOBMPIMYPTEVPHHPMSSDZSNSJAI
JAI
JAI
APXMYPTEVNXPPMSSDZABB
TEVPMS
APXPMSRPHABB
LUI
LUI
CENTRAL NERVOUS SYSTEM AGENTS
ANTICONVULSANTS
28:00
28:12.92
1.9845 1.9845 1.9845 1.9845 1.9845 1.9845 1.9845 1.9845 1.9845 1.9845 1.9845 3.8904
1.2551
1.3174
0.2584 0.2584 0.2584 0.2584 0.2584 0.2584 0.5452
0.5197 0.5197
0.0577 0.0577 0.0577 0.1136
0.9110
0.9110
87 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$
$
$
$$$$$$$
$$
$$$$
$
$
(MISCELLANEOUS ANTICONVULSANTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
MOCLOBEMIDE
PHENELZINE SULFATE
TRANYLCYPROMINE SULFATE
DULOXETINE HYDROCHLORIDE
100 MG ORAL TABLET
150 MG ORAL TABLET
300 MG ORAL TABLET
15 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
30 MG (BASE) ORAL DELAYED RELEASE CAPSULE
60 MG (BASE) ORAL DELAYED RELEASE CAPSULE
000022321480000223974600002237111
0000223215000002239747
0000224045600002239748
00000476552
00001919598
00002301482
00002301490
APO-MOCLOBEMIDENOVO-MOCLOBEMIDENU-MOCLOBEMIDE
APO-MOCLOBEMIDENOVO-MOCLOBEMIDE
APO-MOCLOBEMIDENOVO-MOCLOBEMIDE
NARDIL
PARNATE
CYMBALTA
CYMBALTA
APXTEVNXP
APXTEV
APXTEV
ERF
GSK
LIL
LIL
(MONOAMINE OXIDASE INHIBITORS)
(SELECTIVE SEROTONIN- AND NOREPINEPHRINE-REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.04.12
28:16.04.16
0.2520 0.2520 0.2520
0.3647 0.3647
0.7161 0.7161
0.3828
0.4041
2.0173
4.0351
88 EFFECTIVE APRIL 1, 2012
$$$
$$
$$
$
$
$
$
ANTIDEPRESSANTS
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
VENLAFAXINE HCL37.5 MG (BASE) ORAL EXTENDED-RELEASE CAPSULE
75 MG (BASE) ORAL EXTENDED-RELEASE CAPSULE
150 MG (BASE) ORAL EXTENDED-RELEASE CAPSULE
00002331683000023043170000236002000002310279000022750230000227854500002273969000023103170000235471300002237279
00002331691000023043250000236003900002310287000022750310000227855300002273977000023103250000235472100002237280
00002331705000023043330000236004700002310295000022750580000227856100002273985000023103330000235474800002237282
APO-VENLAFAXINE XRCO VENLAFAXINE XRGD-VENLAFAXINE XRMYLAN-VENLAFAXINE XRNOVO-VENLAFAXINE XRPMS-VENLAFAXINE XRRATIO-VENLAFAXINE XRSANDOZ VENLAFAXINE XRVENLAFAXINE XREFFEXOR XR
APO-VENLAFAXINE XRCO VENLAFAXINE XRGD-VENLAFAXINE XRMYLAN-VENLAFAXINE XRNOVO-VENLAFAXINE XRPMS-VENLAFAXINE XRRATIO-VENLAFAXINE XRSANDOZ VENLAFAXINE XRVENLAFAXINE XREFFEXOR XR
APO-VENLAFAXINE XRCO VENLAFAXINE XRGD-VENLAFAXINE XRMYLAN-VENLAFAXINE XRNOVO-VENLAFAXINE XRPMS-VENLAFAXINE XRRATIO-VENLAFAXINE XRSANDOZ VENLAFAXINE XRVENLAFAXINE XREFFEXOR XR
APXCOBGMDMYPTEVPMSRPHSDZSNSWAY
APXCOBGMDMYPTEVPMSRPHSDZSNSWAY
APXCOBGMDMYPTEVPMSRPHSDZSNSWAY
(SELECTIVE SEROTONIN- AND NOREPINEPHRINE-REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.04.16
0.5438 0.5438 0.5438 0.5438 0.5438 0.5438 0.5438 0.5438 0.5438 0.9935
1.0876 1.0876 1.0876 1.0876 1.0876 1.0876 1.0876 1.0876 1.0876 1.9875
1.1483 1.1483 1.1483 1.1483 1.1483 1.1483 1.1483 1.1483 1.1483 2.0981
89 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$
$$$$$$$$$$
$$$$$$$$$$
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
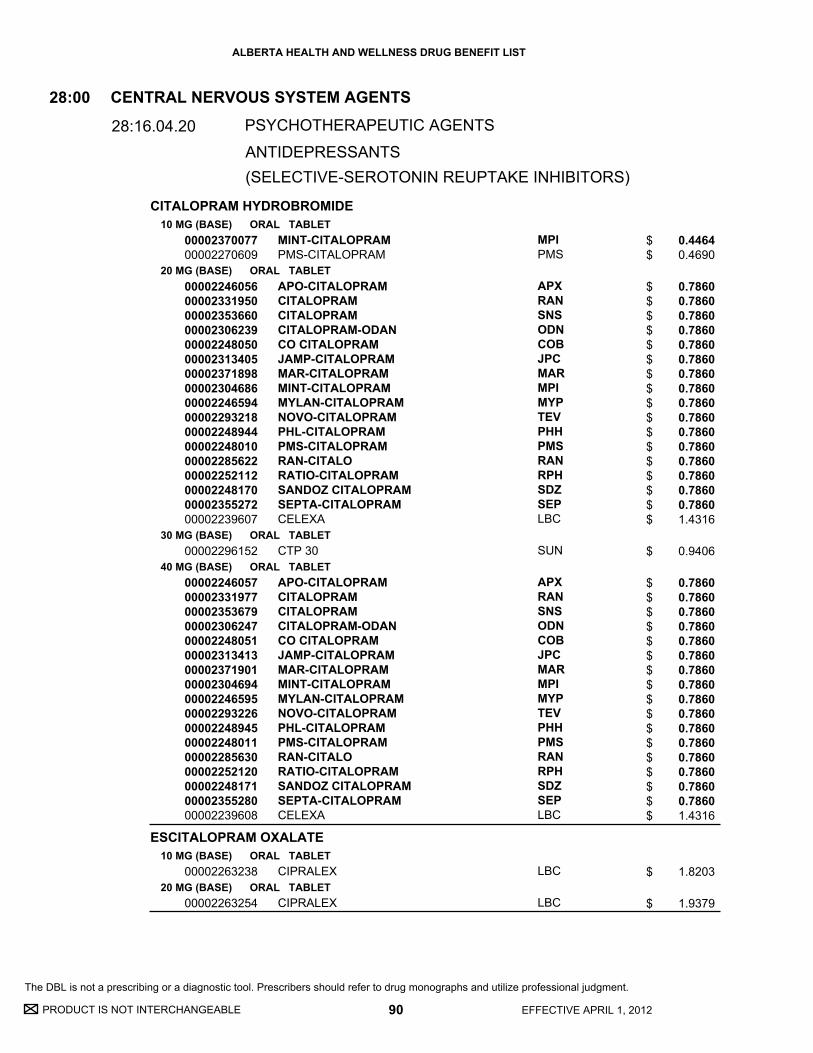
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CITALOPRAM HYDROBROMIDE
ESCITALOPRAM OXALATE
10 MG (BASE) ORAL TABLET
20 MG (BASE) ORAL TABLET
30 MG (BASE) ORAL TABLET
40 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
20 MG (BASE) ORAL TABLET
0000237007700002270609
0000224605600002331950000023536600000230623900002248050000023134050000237189800002304686000022465940000229321800002248944000022480100000228562200002252112000022481700000235527200002239607
00002296152
0000224605700002331977000023536790000230624700002248051000023134130000237190100002304694000022465950000229322600002248945000022480110000228563000002252120000022481710000235528000002239608
00002263238
00002263254
MINT-CITALOPRAMPMS-CITALOPRAM
APO-CITALOPRAMCITALOPRAMCITALOPRAMCITALOPRAM-ODANCO CITALOPRAMJAMP-CITALOPRAMMAR-CITALOPRAMMINT-CITALOPRAMMYLAN-CITALOPRAMNOVO-CITALOPRAMPHL-CITALOPRAMPMS-CITALOPRAMRAN-CITALORATIO-CITALOPRAMSANDOZ CITALOPRAMSEPTA-CITALOPRAMCELEXA
CTP 30
APO-CITALOPRAMCITALOPRAMCITALOPRAMCITALOPRAM-ODANCO CITALOPRAMJAMP-CITALOPRAMMAR-CITALOPRAMMINT-CITALOPRAMMYLAN-CITALOPRAMNOVO-CITALOPRAMPHL-CITALOPRAMPMS-CITALOPRAMRAN-CITALORATIO-CITALOPRAMSANDOZ CITALOPRAMSEPTA-CITALOPRAMCELEXA
CIPRALEX
CIPRALEX
MPIPMS
APXRANSNSODNCOBJPCMARMPIMYPTEVPHHPMSRANRPHSDZSEPLBC
SUN
APXRANSNSODNCOBJPCMARMPIMYPTEVPHHPMSRANRPHSDZSEPLBC
LBC
LBC
(SELECTIVE-SEROTONIN REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.04.20
0.4464 0.4690
0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 1.4316
0.9406
0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 0.7860 1.4316
1.8203
1.9379
90 EFFECTIVE APRIL 1, 2012
$$
$$$$$$$$$$$$$$$$$
$
$$$$$$$$$$$$$$$$$
$
$
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FLUOXETINE HCL
FLUVOXAMINE MALEATE
10 MG (BASE) ORAL CAPSULE
20 MG (BASE) ORAL CAPSULE
4 MG / ML (BASE) ORAL LIQUID
50 MG ORAL TABLET
100 MG ORAL TABLET
0000221635300002242177000022860680000223781300002216582000021927560000222348100002177579000022413710000224348600002018985
000022163610000236453000002242178000022860760000223781400002216590000021927640000222350300002177587000022413740000224348700000636622
00002231328
000022313290000236376300002255529000022399530000223119200002240682000022184530000224705400001919342
000022313300000236377100002255537000022399540000223119300002240683000022184610000224705500001919369
APO-FLUOXETINECO FLUOXETINEFLUOXETINEMYLAN-FLUOXETINENOVO-FLUOXETINENU-FLUOXETINEPHL-FLUOXETINEPMS-FLUOXETINERATIO-FLUOXETINE HYDROCHLORIDESANDOZ FLUOXETINEPROZAC
APO-FLUOXETINEAVA-FLUOXETINECO FLUOXETINEFLUOXETINEMYLAN-FLUOXETINENOVO-FLUOXETINENU-FLUOXETINEPHL-FLUOXETINEPMS-FLUOXETINERATIO-FLUOXETINE HYDROCHLORIDESANDOZ FLUOXETINEPROZAC
APO-FLUOXETINE
APO-FLUVOXAMINEAVA-FLUVOXAMINECO FLUVOXAMINENOVO-FLUVOXAMINENU-FLUVOXAMINEPMS-FLUVOXAMINERATIO-FLUVOXAMINESANDOZ FLUVOXAMINELUVOX
APO-FLUVOXAMINEAVA-FLUVOXAMINECO FLUVOXAMINENOVO-FLUVOXAMINENU-FLUVOXAMINEPMS-FLUVOXAMINERATIO-FLUVOXAMINESANDOZ FLUVOXAMINELUVOX
APXCOBSNSMYPTEVNXPPHHPMSRPHSDZLIL
APXAVACOBSNSMYPTEVNXPPHHPMSRPHSDZLIL
APX
APXAVACOBTEVNXPPMSRPHSDZABB
APXAVACOBTEVNXPPMSRPHSDZABB
(SELECTIVE-SEROTONIN REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.04.20
1.0807 1.0807 1.0807 1.0807 1.0807 1.0807 1.0807 1.0807 1.0807 1.0807 1.9757
1.0112 1.0112 1.0112 1.0112 1.0112 1.0112 1.0112 1.0112 1.0112 1.0112 1.0112 1.9772
0.5859
0.4952 0.4952 0.4952 0.4952 0.4952 0.4952 0.4952 0.4952 0.8750
0.8902 0.8902 0.8902 0.8902 0.8902 0.8902 0.8902 0.8902 1.5730
91 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$
$$$$$$$$$$$$
$
$$$$$$$$$
$$$$$$$$$
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PAROXETINE HCL
SERTRALINE HCL
20 MG (BASE) ORAL TABLET
30 MG (BASE) ORAL TABLET
40 MG (BASE) ORAL TABLET
25 MG (BASE) ORAL CAPSULE
50 MG (BASE) ORAL CAPSULE
00002240908000022627540000224801300002248557000022484510000228285200002247751000022478110000226943000001940481
0000224090900002262762000022480140000224855800002248452000022828600000224775200002247812000022547780000226944900001940473
00002293749
0000223828000002287390000022736830000224251900002240485000022458240000224483800002374552000022451590000235352000002132702
0000223828100002287404000022736910000224252000002240484000022458250000224483900002374560000022451600000235353900001962817
APO-PAROXETINECO PAROXETINEMYLAN-PAROXETINENOVO-PAROXETINEPAROXETINEPAROXETINEPMS-PAROXETINERATIO-PAROXETINESANDOZ PAROXETINEPAXIL
APO-PAROXETINECO PAROXETINEMYLAN-PAROXETINENOVO-PAROXETINEPAROXETINEPAROXETINEPMS-PAROXETINERATIO-PAROXETINESANDOZ PAROXETINESANDOZ PAROXETINEPAXIL
PMS-PAROXETINE
APO-SERTRALINECO SERTRALINEGD-SERTRALINEMYLAN-SERTRALINENOVO-SERTRALINEPHL-SERTRALINEPMS-SERTRALINERAN-SERTRALINESANDOZ SERTRALINESERTRALINEZOLOFT
APO-SERTRALINECO SERTRALINEGD-SERTRALINEMYLAN-SERTRALINENOVO-SERTRALINEPHL-SERTRALINEPMS-SERTRALINERAN-SERTRALINESANDOZ SERTRALINESERTRALINEZOLOFT
APXCOBMYPTEVMELSNSPMSRPHSDZGSK
APXCOBMYPTEVMELSNSPMSRPHSDZSDZGSK
PMS
APXCOBGMDMYPTEVPHHPMSRANSDZSNSPFI
APXCOBGMDMYPTEVPHHPMSRANSDZSNSPFI
(SELECTIVE-SEROTONIN REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.04.20
1.0017 1.0017 1.0017 1.0017 1.0017 1.0017 1.0017 1.0017 1.0017 1.9410
1.0647 1.0647 1.0647 1.0647 1.0647 1.0647 1.0647 1.0647 1.0647 1.0647 2.0622
2.2454
0.4826 0.4826 0.4826 0.4826 0.4826 0.4826 0.4826 0.4826 0.4826 0.4826 0.9054
0.9651 0.9651 0.9651 0.9651 0.9651 0.9651 0.9651 0.9651 0.9651 0.9651 1.8107
92 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$
$$$$$$$$$$$
$
$$$$$$$$$$$
$$$$$$$$$$$
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SERTRALINE HCL
TRAZODONE HCL
100 MG (BASE) ORAL CAPSULE
50 MG ORAL TABLET
75 MG ORAL TABLET
100 MG ORAL TABLET
150 MG ORAL TABLET
0000223828200002287412000022737050000224252100002240481000022458260000224484000002374579000022451610000235354700001962779
000021476370000223168300002144263000021653840000193722700002348772
00002237339
000021476450000223168400002144271000021653920000193723500002348780
00002147653000021442980000216540600002348799
APO-SERTRALINECO SERTRALINEGD-SERTRALINEMYLAN-SERTRALINENOVO-SERTRALINEPHL-SERTRALINEPMS-SERTRALINERAN-SERTRALINESANDOZ SERTRALINESERTRALINEZOLOFT
APO-TRAZODONEMYLAN-TRAZODONENOVO-TRAZODONENU-TRAZODONEPMS-TRAZODONETRAZODONE
PMS-TRAZODONE
APO-TRAZODONEMYLAN-TRAZODONENOVO-TRAZODONENU-TRAZODONEPMS-TRAZODONETRAZODONE
APO-TRAZODONE DNOVO-TRAZODONENU-TRAZODONE-DTRAZODONE
APXCOBGMDMYPTEVPHHPMSRANSDZSNSPFI
APXMYPTEVNXPPMSSNS
PMS
APXMYPTEVNXPPMSSNS
APXTEVNXPSNS
(SELECTIVE-SEROTONIN REUPTAKE INHIBITORS)
(SEROTONIN MODULATORS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.04.20
28:16.04.24
1.0114 1.0114 1.0114 1.0114 1.0114 1.0114 1.0114 1.0114 1.0114 1.0114 1.8974
0.2214 0.2214 0.2214 0.2214 0.2214 0.2214
0.3506
0.3956 0.3956 0.3956 0.3956 0.3956 0.3956
0.5812 0.5812 0.5812 0.5812
93 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$
$$$$$$
$
$$$$$$
$$$$
ANTIDEPRESSANTS
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
AMITRIPTYLINE HCL
CLOMIPRAMINE HCL
DESIPRAMINE HCL
DOXEPIN HCL
10 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
75 MG ORAL TABLET
10 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
10 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
75 MG ORAL TABLET
10 MG (BASE) ORAL CAPSULE
25 MG (BASE) ORAL CAPSULE
50 MG (BASE) ORAL CAPSULE
75 MG (BASE) ORAL CAPSULE
00000335053
00000335061
00000335088
00000754129
000020407860000224481600000330566
000020407780000224481700000324019
000020407510000224481800000402591
00002216248
00002216256
00002216264
00002216272
0000204999600000024325
000020500050000191342500000024333
000020500130000191343300000024341
000020500210000191344100000400750
ELAVIL
ELAVIL
ELAVIL
ELAVIL
APO-CLOMIPRAMINECO CLOMIPRAMINEANAFRANIL
APO-CLOMIPRAMINECO CLOMIPRAMINEANAFRANIL
APO-CLOMIPRAMINECO CLOMIPRAMINEANAFRANIL
APO-DESIPRAMINE
APO-DESIPRAMINE
APO-DESIPRAMINE
APO-DESIPRAMINE
APO-DOXEPINSINEQUAN
APO-DOXEPINNOVO-DOXEPINSINEQUAN
APO-DOXEPINNOVO-DOXEPINSINEQUAN
APO-DOXEPINNOVO-DOXEPINSINEQUAN
AAP
AAP
AAP
AAP
APXCOBSUN
APXCOBSUN
APXCOBSUN
APX
APX
APX
APX
APXERF
APXTEVERF
APXTEVERF
APXTEVERF
(TRICYCLICS AND OTHER NOREPINEPHRINE-REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.04.28
0.0714
0.1302
0.2523
0.3907
0.1626 0.1626 0.2973
0.2215 0.2215 0.4052
0.4078 0.4078 0.7460
0.3804
0.3804
0.6704
0.8915
0.1889 0.2768
0.1860 0.1860 0.3377
0.3450 0.3450 0.6250
0.4953 0.4953 0.9047
94 EFFECTIVE APRIL 1, 2012
$
$
$
$
$$$
$$$
$$$
$
$
$
$
$$
$$$
$$$
$$$
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
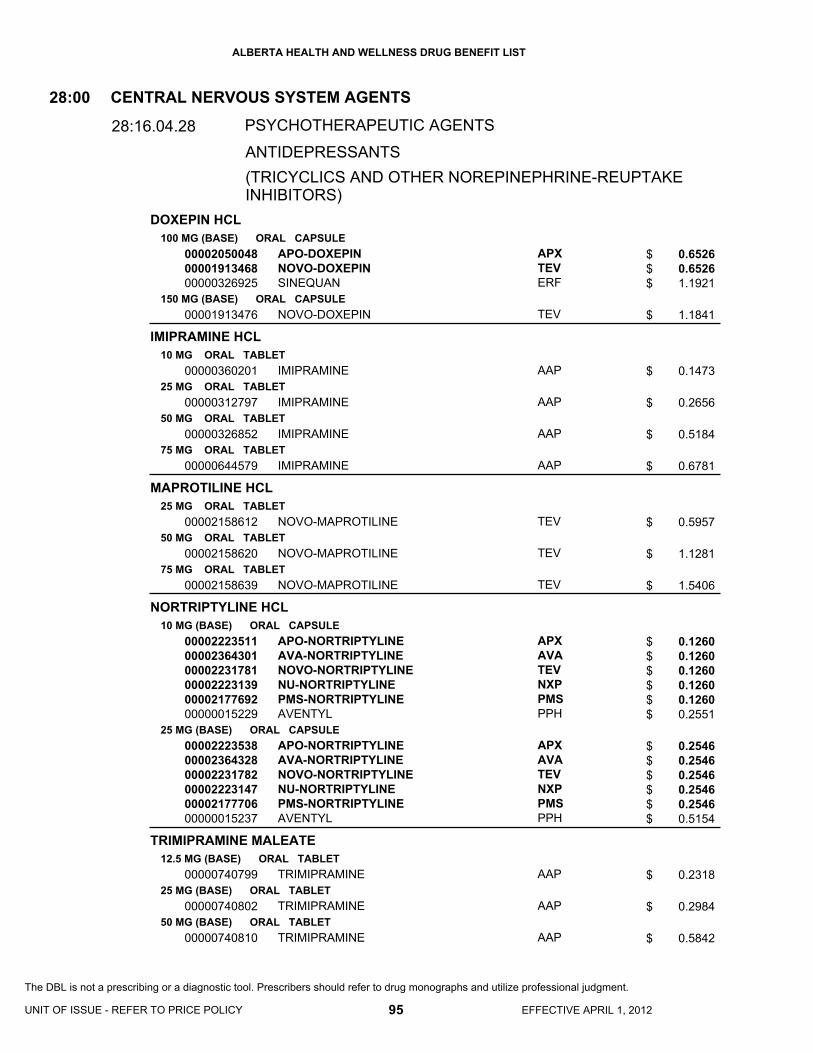
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DOXEPIN HCL
IMIPRAMINE HCL
MAPROTILINE HCL
NORTRIPTYLINE HCL
TRIMIPRAMINE MALEATE
100 MG (BASE) ORAL CAPSULE
150 MG (BASE) ORAL CAPSULE
10 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
75 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
75 MG ORAL TABLET
10 MG (BASE) ORAL CAPSULE
25 MG (BASE) ORAL CAPSULE
12.5 MG (BASE) ORAL TABLET
25 MG (BASE) ORAL TABLET
50 MG (BASE) ORAL TABLET
000020500480000191346800000326925
00001913476
00000360201
00000312797
00000326852
00000644579
00002158612
00002158620
00002158639
000022235110000236430100002231781000022231390000217769200000015229
000022235380000236432800002231782000022231470000217770600000015237
00000740799
00000740802
00000740810
APO-DOXEPINNOVO-DOXEPINSINEQUAN
NOVO-DOXEPIN
IMIPRAMINE
IMIPRAMINE
IMIPRAMINE
IMIPRAMINE
NOVO-MAPROTILINE
NOVO-MAPROTILINE
NOVO-MAPROTILINE
APO-NORTRIPTYLINEAVA-NORTRIPTYLINENOVO-NORTRIPTYLINENU-NORTRIPTYLINEPMS-NORTRIPTYLINEAVENTYL
APO-NORTRIPTYLINEAVA-NORTRIPTYLINENOVO-NORTRIPTYLINENU-NORTRIPTYLINEPMS-NORTRIPTYLINEAVENTYL
TRIMIPRAMINE
TRIMIPRAMINE
TRIMIPRAMINE
APXTEVERF
TEV
AAP
AAP
AAP
AAP
TEV
TEV
TEV
APXAVATEVNXPPMSPPH
APXAVATEVNXPPMSPPH
AAP
AAP
AAP
(TRICYCLICS AND OTHER NOREPINEPHRINE-REUPTAKE INHIBITORS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.04.28
0.6526 0.6526 1.1921
1.1841
0.1473
0.2656
0.5184
0.6781
0.5957
1.1281
1.5406
0.1260 0.1260 0.1260 0.1260 0.1260 0.2551
0.2546 0.2546 0.2546 0.2546 0.2546 0.5154
0.2318
0.2984
0.5842
95 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$
$
$
$
$
$
$
$
$$$$$$
$$$$$$
$
$
$
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TRIMIPRAMINE MALEATE
BUPROPION HCL
L-TRYPTOPHAN
100 MG (BASE) ORAL TABLET
75 MG (BASE) ORAL CAPSULE
100 MG ORAL SUSTAINED-RELEASE TABLET
150 MG ORAL SUSTAINED-RELEASE TABLET
150 MG ORAL EXTENDED-RELEASE TABLET
300 MG ORAL EXTENDED-RELEASE TABLET
250 MG ORAL TABLET
500 MG ORAL TABLET
750 MG ORAL TABLET
1 G ORAL TABLET
500 MG ORAL CAPSULE
00000740829
00002070987
00002363399000023253730000228565700002275074
0000236340200002313421000022856650000227508200002237825
00002275090
00002275104
00002239326
000022485380000224033300002029456
00002239327
000022485390000223725000000654531
000022485400000224033400000718149
TRIMIPRAMINE
TRIMIPRAMINE
AVA-BUPROPION SRPMS-BUPROPION SRRATIO-BUPROPION SRSANDOZ BUPROPION SR
AVA-BUPROPION SRPMS-BUPROPION SRRATIO-BUPROPION SRSANDOZ BUPROPION SRWELLBUTRIN SR
WELLBUTRIN XL
WELLBUTRIN XL
TRYPTAN
APO-TRYPTOPHANRATIO-TRYPTOPHANTRYPTAN
TRYPTAN
APO-TRYPTOPHANRATIO-TRYPTOPHANTRYPTAN
APO-TRYPTOPHANRATIO-TRYPTOPHANTRYPTAN
AAP
AAP
AVAPMSRPHSDZ
AVAPMSRPHSDZVCL
VCL
VCL
VCL
APXRPHVCL
VCL
APXRPHVCL
APXRPHVCL
(TRICYCLICS AND OTHER NOREPINEPHRINE-REUPTAKE INHIBITORS)
(MISCELLANEOUS ANTIDEPRESSANTS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.04.28
28:16.04.92
0.9968
0.7863
0.3365 0.3365 0.3365 0.3365
0.5040 0.5040 0.5040 0.5040 0.9356
0.5573
1.1150
0.3998
0.4289 0.4289 0.7996
1.1996
0.8579 0.8579 1.5994
0.4289 0.4289 0.7996
96 EFFECTIVE APRIL 1, 2012
$
$
$$$$
$$$$$
$
$
$
$$$
$
$$$
$$$
ANTIDEPRESSANTS
ANTIDEPRESSANTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
MIRTAZAPINE
ARIPIPRAZOLE
CLOZAPINE
15 MG ORAL TABLET
30 MG ORAL TABLET
45 MG ORAL TABLET
2 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
15 MG ORAL TABLET
20 MG ORAL TABLET
30 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
0000225609600002273942
000022866290000236293700002252279000023706890000225611800002259354000022487620000225060800002243910
00002256126
00002322374
00002322382
00002322390
00002322404
00002322412
00002322455
000022480340000224724300000894737
00002305003
MYLAN-MIRTAZAPINEPMS-MIRTAZAPINE
APO-MIRTAZAPINEAVA-MIRTAZAPINEMIRTAZAPINEMIRTAZAPINEMYLAN-MIRTAZAPINENOVO-MIRTAZAPINEPMS-MIRTAZAPINESANDOZ MIRTAZAPINEREMERON
MYLAN-MIRTAZAPINE
ABILIFY
ABILIFY
ABILIFY
ABILIFY
ABILIFY
ABILIFY
APO-CLOZAPINEGEN-CLOZAPINECLOZARIL
GEN-CLOZAPINE
MYPPMS
APXAVAMELSNSMYPTEVPMSSDZMFC
MYP
BMS
BMS
BMS
BMS
BMS
BMS
APXMYPNOV
MYP
(MISCELLANEOUS ANTIDEPRESSANTS)
(ATYPICAL ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.04.92
28:16.08.04
0.3750 0.3750
0.6944 0.6944 0.6944 0.6944 0.6944 0.6944 0.6944 0.6944 1.2989
1.1576
2.9140
3.2800
3.7800
3.7800
3.7800
3.7800
0.6594 0.6594 1.0127
1.3188
97 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$$$$$$$$
$
$
$
$
$
$
$
$$$
$
RESTRICTED BENEFIT - This Drug Product is a benefit for patients 15 to 17 years of age inclusive for the treatment of schizophrenia.
RESTRICTED BENEFIT - This Drug Product is a benefit for patients 15 to 17 years of age inclusive for the treatment of schizophrenia.
ANTIDEPRESSANTS
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CLOZAPINE
OLANZAPINE
100 MG ORAL TABLET
200 MG ORAL TABLET
2.5 MG ORAL TABLET
5 MG ORAL TABLET
7.5 MG ORAL TABLET
10 MG ORAL TABLET
000022480350000224724400000894745
00002305011
000022817910000237343200002325659000023378780000227671200002372819000023031160000231034100002229250
000022818050000237344000002325667000023378860000227672000002372827000023031590000231036800002229269
000022818130000237345900002325675000023378940000227673900002372835000023031670000231037600002229277
000022818210000237346700002325683000023379080000227674700002372843000023031750000231038400002229285
APO-CLOZAPINEGEN-CLOZAPINECLOZARIL
GEN-CLOZAPINE
APO-OLANZAPINEAVA-OLANZAPINECO OLANZAPINEMYLAN-OLANZAPINENOVO-OLANZAPINEOLANZAPINEPMS-OLANZAPINESANDOZ OLANZAPINEZYPREXA
APO-OLANZAPINEAVA-OLANZAPINECO OLANZAPINEMYLAN-OLANZAPINENOVO-OLANZAPINEOLANZAPINEPMS-OLANZAPINESANDOZ OLANZAPINEZYPREXA
APO-OLANZAPINEAVA-OLANZAPINECO OLANZAPINEMYLAN-OLANZAPINENOVO-OLANZAPINEOLANZAPINEPMS-OLANZAPINESANDOZ OLANZAPINEZYPREXA
APO-OLANZAPINEAVA-OLANZAPINECO OLANZAPINEMYLAN-OLANZAPINENOVO-OLANZAPINEOLANZAPINEPMS-OLANZAPINESANDOZ OLANZAPINEZYPREXA
APXMYPNOV
MYP
APXAVACOBMYPTEVSNSPMSSDZLIL
APXAVACOBMYPTEVSNSPMSSDZLIL
APXAVACOBMYPTEVSNSPMSSDZLIL
APXAVACOBMYPTEVSNSPMSSDZLIL
(ATYPICAL ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.08.04
2.6446 2.6446 4.0614
5.2892
1.0568 1.0568 1.0568 1.0568 1.0568 1.0568 1.0568 1.0568 1.9320
2.1135 2.1135 2.1135 2.1135 2.1135 2.1135 2.1135 2.1135 3.8640
3.1703 3.1703 3.1703 3.1703 3.1703 3.1703 3.1703 3.1703 5.7960
4.2270 4.2270 4.2270 4.2270 4.2270 4.2270 4.2270 4.2270 7.7280
98 EFFECTIVE APRIL 1, 2012
$$$
$
$$$$$$$$$
$$$$$$$$$
$$$$$$$$$
$$$$$$$$$
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
OLANZAPINE
QUETIAPINE FUMARATE
15 MG ORAL TABLET
5 MG ORAL DISINTEGRATING TABLET
10 MG ORAL DISINTEGRATING TABLET
25 MG (BASE) ORAL TABLET
50 MG ORAL TABLET
100 MG (BASE) ORAL TABLET
150 MG (BASE) ORAL TABLET
0000228184800002325691000023379160000227675500002372851000023031830000231039200002238850
00002360616000023275620000232134300002352974000023031910000232777500002243086
00002360624000023275700000232135100002352982000023032050000232778300002243087
000023139010000231608000002330415000023078040000228423500002296551000023531640000231399500002236951
00002361892
000023139280000231609900002330423000023078120000228424300002296578000023531720000231400200002236952
00002284251
APO-OLANZAPINECO OLANZAPINEMYLAN-OLANZAPINENOVO-OLANZAPINEOLANZAPINEPMS-OLANZAPINESANDOZ OLANZAPINEZYPREXA
APO-OLANZAPINE ODTCO OLANZAPINE ODTNOVO-OLANZAPINE ODOLANZAPINE ODTPMS-OLANZAPINE ODTSANDOZ OLANZAPINE ODTZYPREXA ZYDIS
APO-OLANZAPINE ODTCO OLANZAPINE ODTNOVO-OLANZAPINE ODOLANZAPINE ODTPMS-OLANZAPINE ODTSANDOZ OLANZAPINE ODTZYPREXA ZYDIS
APO-QUETIAPINECO QUETIAPINEJAMP-QUETIAPINEMYLAN-QUETIAPINENOVO-QUETIAPINEPMS-QUETIAPINEQUETIAPINESANDOZ QUETIAPINESEROQUEL
PMS-QUETIAPINE
APO-QUETIAPINECO QUETIAPINEJAMP-QUETIAPINEMYLAN-QUETIAPINENOVO-QUETIAPINEPMS-QUETIAPINEQUETIAPINESANDOZ QUETIAPINESEROQUEL
NOVO-QUETIAPINE
APXCOBMYPTEVSNSPMSSDZLIL
APXCOBTEVSNSPMSSDZLIL
APXCOBTEVSNSPMSSDZLIL
APXCOBJPCMYPTEVPMSSNSSDZAZC
PMS
APXCOBJPCMYPTEVPMSSNSSDZAZC
TEV
(ATYPICAL ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.08.04
6.3405 6.3405 6.3405 6.3405 6.3405 6.3405 6.3405
11.5918
1.6890 1.6890 1.6890 1.6890 1.6890 1.6890 3.8427
3.3750 3.3750 3.3750 3.3750 3.3750 3.3750 7.6786
0.2975 0.2975 0.2975 0.2975 0.2975 0.2975 0.2975 0.2975 0.5520
0.5614
0.7936 0.7936 0.7936 0.7936 0.7936 0.7936 0.7936 0.7936 1.4728
1.4203
99 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$
$$$$$$$
$$$$$$$
$$$$$$$$$
$
$$$$$$$$$
$
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
QUETIAPINE FUMARATE200 MG (BASE) ORAL TABLET
300 MG (BASE) ORAL TABLET
000023139360000231611000002330458000023078390000228427800002296594000023531990000231401000002236953
000023139440000231612900002330466000023078470000228428600002296608000023532020000231402900002244107
APO-QUETIAPINECO QUETIAPINEJAMP-QUETIAPINEMYLAN-QUETIAPINENOVO-QUETIAPINEPMS-QUETIAPINEQUETIAPINESANDOZ QUETIAPINESEROQUEL
APO-QUETIAPINECO QUETIAPINEJAMP-QUETIAPINEMYLAN-QUETIAPINENOVO-QUETIAPINEPMS-QUETIAPINEQUETIAPINESANDOZ QUETIAPINESEROQUEL
APXCOBJPCMYPTEVPMSSNSSDZAZC
APXCOBJPCMYPTEVPMSSNSSDZAZC
(ATYPICAL ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.08.04
1.5935 1.5935 1.5935 1.5935 1.5935 1.5935 1.5935 1.5935 2.9584
2.3252 2.3252 2.3252 2.3252 2.3252 2.3252 2.3252 2.3252 4.3156
100 EFFECTIVE APRIL 1, 2012
$$$$$$$$$
$$$$$$$$$
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RISPERIDONE0.25 MG ORAL TABLET
0.5 MG ORAL TABLET
1 MG ORAL TABLET
00002282119000023671730000228258500002359529000023717660000235979000002282240000022826900000225843900002252007000022809060000232830500002332051000023568800000230365500002240551
00002282127000023671810000228259300002359537000023717740000235980400002282259000022641880000225844700002252015000022809140000232831300002332078000023568990000230366300002240552
00002282135000023672030000228260700002359545000023717820000235981200002282267000022641960000225845500002252023000022809220000232832100002332086000023569020000227980000002025280
APO-RISPERIDONEAVA-RISPERIDONECO RISPERIDONEJAMP-RISPERIDONEMAR-RISPERIDONEMINT-RISPERIDONMYLAN-RISPERIDONENOVO-RISPERIDONEPHL-RISPERIDONEPMS-RISPERIDONERAN-RISPERIDONERAN-RISPERIDONERISPERIDONERISPERIDONESANDOZ RISPERIDONERISPERDAL
APO-RISPERIDONEAVA-RISPERIDONECO RISPERIDONEJAMP-RISPERIDONEMAR-RISPERIDONEMINT-RISPERIDONMYLAN-RISPERIDONENOVO-RISPERIDONEPHL-RISPERIDONEPMS-RISPERIDONERAN-RISPERIDONERAN-RISPERIDONERISPERIDONERISPERIDONESANDOZ RISPERIDONERISPERDAL
APO-RISPERIDONEAVA-RISPERIDONECO RISPERIDONEJAMP-RISPERIDONEMAR-RISPERIDONEMINT-RISPERIDONMYLAN-RISPERIDONENOVO-RISPERIDONEPHL-RISPERIDONEPMS-RISPERIDONERAN-RISPERIDONERAN-RISPERIDONERISPERIDONERISPERIDONESANDOZ RISPERIDONERISPERDAL
APXAVACOBJPCMARMPIMYPTEVPHHPMSRANRANRANSNSSDZJAI
APXAVACOBJPCMARMPIMYPTEVPHHPMSRANRANRANSNSSDZJAI
APXAVACOBJPCMARMPIMYPTEVPHHPMSRANRANRANSNSSDZJAI
(ATYPICAL ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.08.04
0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.2615 0.5815
0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.4379 0.9741
0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 0.6048 1.3457
101 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$$$$$
$$$$$$$$$$$$$$$$
$$$$$$$$$$$$$$$$
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
RISPERIDONE2 MG ORAL TABLET
3 MG ORAL TABLET
4 MG ORAL TABLET
00002282143000023672110000228261500002359553000023717900000235982000002282275000022642180000225846300002252031000022809300000232834800002332094000023569100000227981900002025299
00002282151000023672380000228262300002359561000023718040000235983900002282283000022642260000225847100002252058000022809490000232836400002332108000023569290000227982700002025302
00002282178000023672460000228263100002359588000023718120000235984700002282291000022642340000225849800002252066000022809570000232837200002332116000023569370000227983500002025310
APO-RISPERIDONEAVA-RISPERIDONECO RISPERIDONEJAMP-RISPERIDONEMAR-RISPERIDONEMINT-RISPERIDONMYLAN-RISPERIDONENOVO-RISPERIDONEPHL-RISPERIDONEPMS-RISPERIDONERAN-RISPERIDONERAN-RISPERIDONERISPERIDONERISPERIDONESANDOZ RISPERIDONERISPERDAL
APO-RISPERIDONEAVA-RISPERIDONECO RISPERIDONEJAMP-RISPERIDONEMAR-RISPERIDONEMINT-RISPERIDONMYLAN-RISPERIDONENOVO-RISPERIDONEPHL-RISPERIDONEPMS-RISPERIDONERAN-RISPERIDONERAN-RISPERIDONERISPERIDONERISPERIDONESANDOZ RISPERIDONERISPERDAL
APO-RISPERIDONEAVA-RISPERIDONECO RISPERIDONEJAMP-RISPERIDONEMAR-RISPERIDONEMINT-RISPERIDONMYLAN-RISPERIDONENOVO-RISPERIDONEPHL-RISPERIDONEPMS-RISPERIDONERAN-RISPERIDONERAN-RISPERIDONERISPERIDONERISPERIDONESANDOZ RISPERIDONERISPERDAL
APXAVACOBJPCMARMPIMYPTEVPHHPMSRANRANRANSNSSDZJAI
APXAVACOBJPCMARMPIMYPTEVPHHPMSRANRANRANSNSSDZJAI
APXAVACOBJPCMARMPIMYPTEVPHHPMSRANRANRANSNSSDZJAI
(ATYPICAL ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.08.04
1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 1.2075 2.6863
1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 1.8113 4.0297
2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 2.4150 5.3733
102 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$$$$$
$$$$$$$$$$$$$$$$
$$$$$$$$$$$$$$$$
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RISPERIDONE
RISPERIDONE TARTRATE
ZIPRASIDONE HYDROCHLORIDE MONOHYDRATE
HALOPERIDOL
0.5 MG ORAL DISINTEGRATING TABLET
1 MG ORAL DISINTEGRATING TABLET
2 MG ORAL DISINTEGRATING TABLET
3 MG ORAL DISINTEGRATING TABLET
4 MG ORAL DISINTEGRATING TABLET
1 MG / ML (BASE) ORAL SOLUTION
20 MG (BASE) ORAL CAPSULE
40 MG (BASE) ORAL CAPSULE
60 MG (BASE) ORAL CAPSULE
80 MG (BASE) ORAL CAPSULE
0.5 MG ORAL TABLET
1 MG ORAL TABLET
00002247704
0000229178900002247705
0000229179700002247706
0000237069700002268086
0000237070000002268094
00002280396000023643440000227926600002236950
00002298597
00002298600
00002298619
00002298627
0000039679600000363685
0000039681800000363677
RISPERDAL M-TAB
PMS-RISPERIDONE ODTRISPERDAL M-TAB
PMS-RISPERIDONE ODTRISPERDAL M-TAB
PMS-RISPERIDONE ODTRISPERDAL M-TAB
PMS-RISPERIDONE ODTRISPERDAL M-TAB
APO-RISPERIDONEAVA-RISPERIDONEPMS-RISPERIDONERISPERDAL
ZELDOX
ZELDOX
ZELDOX
ZELDOX
APO-HALOPERIDOLNOVO-PERIDOL
APO-HALOPERIDOLNOVO-PERIDOL
JAI
PMSJAI
PMSJAI
PMSJAI
PMSJAI
APXAVAPMSJAI
PFI
PFI
PFI
PFI
APXTEV
APXTEV
(ATYPICAL ANTIPSYCHOTICS)
(BUTYROPHENONES)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.08.04
28:16.08.08
0.8009
0.7725 1.1073
1.5281 2.1903
2.2913 3.2841
3.0638 4.3914
0.7727 0.7727 0.7727 1.5177
1.8251
2.0907
2.0907
2.0907
0.0360 0.0360
0.0614 0.0614
103 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$
$$
$$
$$
$$$$
$
$
$
$
$$
$$
RESTRICTED BENEFIT - This product is a benefit for patients 18 years of age and older for the management of the manifestations of schizophrenia and related psychotic disorders, as well as in severe dementia for the short-term symptomatic management of inappropriate behavior due to aggression and/or psychosis.
ANTIPSYCHOTICS
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
HALOPERIDOL
HALOPERIDOL DECANOATE
CHLORPROMAZINE HCL
FLUPHENAZINE DECANOATE
FLUPHENAZINE HCL
2 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
5 MG / ML INJECTION
50 MG / ML (BASE) INJECTION
100 MG / ML (BASE) INJECTION
25 MG (BASE) ORAL TABLET
50 MG (BASE) ORAL TABLET
100 MG (BASE) ORAL TABLET
25 MG / ML (BASE) INJECTION
25 MG / ML INJECTION
100 MG / ML INJECTION
1 MG ORAL TABLET
2 MG ORAL TABLET
0000039682600000363669
0000039683400000363650
0000046369800000713449
00000768820
00000808652
00002130297
00002130300
00000232823
00000232807
00000232831
00000743518
00002239636
0000224257000000755575
00000405345
00000410632
APO-HALOPERIDOLNOVO-PERIDOL
APO-HALOPERIDOLNOVO-PERIDOL
APO-HALOPERIDOLNOVO-PERIDOL
NOVO-PERIDOL
HALOPERIDOL
HALOPERIDOL LA
HALOPERIDOL LA
NOVO-CHLORPROMAZINE
NOVO-CHLORPROMAZINE
NOVO-CHLORPROMAZINE
CHLORPROMAZINE HCL
FLUPHENAZINE OMEGA
FLUPHENAZINE OMEGAMODECATE CONCENTRATE
APO-FLUPHENAZINE
APO-FLUPHENAZINE
APXTEV
APXTEV
APXTEV
TEV
SDZ
SDZ
SDZ
TEV
TEV
TEV
SDZ
OMG
OMGBMS
APX
APX
(BUTYROPHENONES)
(PHENOTHIAZINES)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.08.08
28:16.08.24
0.1050 0.1050
0.1487 0.1487
0.1330 0.1330
0.6624
4.8300
7.3600
14.7177
0.1816
0.2078
0.4000
1.1100
4.9794
29.7800 29.7800
0.1739
0.2252
104 EFFECTIVE APRIL 1, 2012
$$
$$
$$
$
$
$
$
$
$
$
$
$
$$
$
$
ANTIPSYCHOTICS
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FLUPHENAZINE HCL
METHOTRIMEPRAZINE HCL
METHOTRIMEPRAZINE MALEATE
PERICYAZINE
PERPHENAZINE
PIPOTIAZINE PALMITATE
THIOPROPERAZINE MESYLATE
5 MG ORAL TABLET
25 MG / ML (BASE) INJECTION
2 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
25 MG (BASE) ORAL TABLET
50 MG (BASE) ORAL TABLET
5 MG ORAL CAPSULE
10 MG ORAL CAPSULE
20 MG ORAL CAPSULE
10 MG / ML ORAL DROPS
2 MG ORAL TABLET
4 MG ORAL TABLET
8 MG ORAL TABLET
16 MG ORAL TABLET
25 MG / ML INJECTION
50 MG / ML INJECTION
10 MG (BASE) ORAL TABLET
00000405361
00001927698
00002238403
00002238404
00002238405
00002238406
00001926780
00001926772
00001926764
00001926756
00000335134
00000335126
00000335118
00000335096
00001926667
00001926675
00001927639
APO-FLUPHENAZINE
NOZINAN
APO-METHOPRAZINE
APO-METHOPRAZINE
APO-METHOPRAZINE
APO-METHOPRAZINE
NEULEPTIL
NEULEPTIL
NEULEPTIL
NEULEPTIL
PERPHENAZINE
PERPHENAZINE
PERPHENAZINE
PERPHENAZINE
PIPORTIL L4
PIPORTIL L4
MAJEPTIL
APX
SAV
APX
APX
APX
APX
ERF
ERF
ERF
ERF
AAP
AAP
AAP
AAP
SAV
SAV
ERF
(PHENOTHIAZINES)
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
28:00
28:16.08.24
0.1720
3.5873
0.0685
0.0991
0.2547
0.3857
0.2025
0.3299
0.5075
0.3997
0.0673
0.0815
0.0894
0.1370
17.2645
55.6635
0.5850
105 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TRIFLUOPERAZINE HCL
FLUPENTIXOL DECANOATE
FLUPENTIXOL DIHYDROCHLORIDE
THIOTHIXENE
ZUCLOPENTHIXOL ACETATE
ZUCLOPENTHIXOL DECANOATE
1 MG (BASE) ORAL TABLET
2 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
20 MG (BASE) ORAL TABLET
20 MG / ML INJECTION
100 MG / ML INJECTION
0.5 MG ORAL TABLET
3 MG ORAL TABLET
2 MG ORAL CAPSULE
5 MG ORAL CAPSULE
10 MG ORAL CAPSULE
50 MG / ML INJECTION
200 MG / ML INJECTION
00000345539
00000312754
00000312746
00000326836
00000595942
00002156032
00002156040
00002156008
00002156016
00000024430
00000024449
00000024457
00002230405
00002230406
TRIFLUOPERAZINE
TRIFLUOPERAZINE
TRIFLUOPERAZINE
TRIFLUOPERAZINE
TRIFLUOPERAZINE
FLUANXOL DEPOT
FLUANXOL DEPOT
FLUANXOL
FLUANXOL
NAVANE
NAVANE
NAVANE
CLOPIXOL ACUPHASE
CLOPIXOL DEPOT
AAP
AAP
AAP
AAP
AAP
LBC
LBC
LBC
LBC
ERF
ERF
ERF
LBC
LBC
(PHENOTHIAZINES)
(THIOXANTHENES)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
28
28
:00
:00
28:16.08.24
28:16.08.32
0.1440
0.1890
0.2503
0.2999
0.5998
7.7250
38.6248
0.2669
0.5764
0.3409
0.3794
0.4747
16.0326
16.0326
106 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$
$
$
$
$
$
$
$
ANTIPSYCHOTICS
ANTIPSYCHOTICS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ZUCLOPENTHIXOL DIHYDROCHLORIDE
LOXAPINE HCL
LOXAPINE SUCCINATE
PIMOZIDE
DEXTROAMPHETAMINE SULFATE
10 MG (BASE) ORAL TABLET
25 MG (BASE) ORAL TABLET
50 MG / ML (BASE) INJECTION
2.5 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
25 MG (BASE) ORAL TABLET
50 MG (BASE) ORAL TABLET
2 MG ORAL TABLET
4 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL SUSTAINED-RELEASE CAPSULE
15 MG ORAL SUSTAINED-RELEASE CAPSULE
00002230402
00002230403
00002169991
00002242868
00002230837
00002230838
00002230839
00002230840
0000224543200000313815
0000224543300000313823
00001924516
00001924559
00001924567
CLOPIXOL
CLOPIXOL
LOXAPAC
XYLAC
XYLAC
XYLAC
XYLAC
XYLAC
APO-PIMOZIDEORAP
APO-PIMOZIDEORAP
DEXEDRINE
DEXEDRINE
DEXEDRINE
LBC
LBC
SDZ
MMT
MMT
MMT
MMT
MMT
APXPHH
APXPHH
PAL
PAL
PAL
(THIOXANTHENES)
(MISCELLANEOUS ANTIPSYCHOTICS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
PSYCHOTHERAPEUTIC AGENTS
PSYCHOTHERAPEUTIC AGENTS
ANOREXIGENIC AGENTS & RESPIRATORY AND CEREBRAL STIMULANTS
28
28
28
:00
:00
:00
28:16.08.32
28:16.08.92
28:20.04
0.4123
1.0307
7.5700
0.1891
0.1773
0.2951
0.4574
0.5914
0.3093 0.3093
0.4136 0.4671
0.6179
0.8864
1.0837
107 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$$
$$
$
$
$
ANTIPSYCHOTICS
ANTIPSYCHOTICS
(AMPHETAMINES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
METHYLPHENIDATE HCL
PHENOBARBITAL
5 MG ORAL TABLET
10 MG ORAL TABLET
20 MG ORAL TABLET
20 MG ORAL EXTENDED-RELEASE TABLET
15 MG ORAL TABLET
30 MG ORAL TABLET
60 MG ORAL TABLET
100 MG ORAL TABLET
5 MG / ML ORAL ELIXIR
00002234749
000022493240000058499100000005606
000022493320000058500900000005614
000022666870000232031200000632775
00000178799
00000178802
00000178810
00000178829
00000645575
PMS-METHYLPHENIDATE
APO-METHYLPHENIDATEPMS-METHYLPHENIDATERITALIN
APO-METHYLPHENIDATEPMS-METHYLPHENIDATERITALIN
APO-METHYLPHENIDATE SRSANDOZ METHYLPHENIDATERITALIN SR
PHENOBARB
PHENOBARB
PHENOBARB
PHENOBARB
PHENOBARB
PMS
APXPMSNOV
APXPMSNOV
APXSDZNOV
PPH
PPH
PPH
PPH
PPH
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANOREXIGENIC AGENTS & RESPIRATORY AND CEREBRAL STIMULANTS
ANXIOLYTICS, SEDATIVES, AND HYPNOTICS
28
28
:00
:00
28:20.92
28:24.04
0.0995
0.1590 0.1590 0.3804
0.3536 0.3536 0.6647
0.3564 0.3564 0.6674
0.0874
0.1040
0.1410
0.1930
0.1167
108 EFFECTIVE APRIL 1, 2012
$
$$$
$$$
$$$
$
$
$
$
$
(MISCELLANEOUS ANOREXIGENIC AGENTS & RESPIRATORYAND CEREBRAL STIMULANTS)
(BARBITURATES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ALPRAZOLAM
BROMAZEPAM
CHLORDIAZEPOXIDE HCL
CHLORDIAZEPOXIDE HCL/ CLIDINIUM BROMIDE
CLORAZEPATE DIPOTASSIUM
DIAZEPAM
0.25 MG ORAL TABLET
0.5 MG ORAL TABLET
1.5 MG ORAL TABLET
3 MG ORAL TABLET
6 MG ORAL TABLET
5 MG ORAL CAPSULE
10 MG ORAL CAPSULE
25 MG ORAL CAPSULE
5 MG * 2.5 MG ORAL CAPSULE
3.75 MG ORAL CAPSULE
7.5 MG ORAL CAPSULE
15 MG ORAL CAPSULE
2 MG ORAL TABLET
5 MG ORAL TABLET
0000234919100000865397000021375340000191348400000548359
0000234920500000865400000021375420000191349200000548367
00002177153
000021771610000223058400000518123
000021771880000223058500000518131
00000522724
00000522988
00000522996
0000061845400000115630
00000860689
00000860700
00000860697
00000405329
00000362158
ALPRAZOLAMAPO-ALPRAZMYLAN-ALPRAZOLAMNOVO-ALPRAZOLXANAX
ALPRAZOLAMAPO-ALPRAZMYLAN-ALPRAZOLAMNOVO-ALPRAZOLXANAX
APO-BROMAZEPAM
APO-BROMAZEPAMNOVO-BROMAZEPAMLECTOPAM
APO-BROMAZEPAMNOVO-BROMAZEPAMLECTOPAM
APO-CHLORDIAZEPOXIDE
APO-CHLORDIAZEPOXIDE
APO-CHLORDIAZEPOXIDE
APO-CHLORAXLIBRAX
APO-CLORAZEPATE
APO-CLORAZEPATE
APO-CLORAZEPATE
APO-DIAZEPAM
APO-DIAZEPAM
SNSAPXMYPTEVPFI
SNSAPXMYPTEVPFI
APX
APXTEVHLR
APXTEVHLR
APX
APX
APX
APXVCL
APX
APX
APX
APX
APX
CENTRAL NERVOUS SYSTEM AGENTS
ANXIOLYTICS, SEDATIVES, AND HYPNOTICS
28:00
28:24.08
0.0760 0.0760 0.0760 0.0760 0.2672
0.0920 0.0920 0.0920 0.0920 0.3196
0.0693
0.0882 0.0882 0.1644
0.1288 0.1288 0.2402
0.0679
0.1070
0.1658
0.2330 0.3305
0.1476
0.1926
0.3856
0.0508
0.0650
109 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$
$$$$$
$
$$$
$$$
$
$
$
$$
$
$
$
$
$
(BENZODIAZEPINES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DIAZEPAM
FLURAZEPAM HCL
LORAZEPAM
MIDAZOLAM HCL
10 MG ORAL TABLET
5 MG / ML INJECTION
5 MG / ML INJECTION EMULSION
15 MG ORAL CAPSULE
30 MG ORAL CAPSULE
0.5 MG ORAL TABLET
1 MG ORAL TABLET
2 MG ORAL TABLET
0.5 MG ORAL SUBLINGUAL TABLET
1 MG ORAL SUBLINGUAL TABLET
2 MG ORAL SUBLINGUAL TABLET
5 MG / ML (BASE) INJECTION
00000405337
00000399728
00002065614
00000521698
00000521701
0000065574000002351072000007111010000072818700002041413
0000065575900002351080000006377420000072819500002041421
0000065576700002351099000006377500000072820900002041448
00002041456
00002041464
00002041472
00002240286
APO-DIAZEPAM
DIAZEPAM
DIAZEMULS
APO-FLURAZEPAM
APO-FLURAZEPAM
APO-LORAZEPAMLORAZEPAMNOVO-LORAZEMPMS-LORAZEPAMATIVAN
APO-LORAZEPAMLORAZEPAMNOVO-LORAZEMPMS-LORAZEPAMATIVAN
APO-LORAZEPAMLORAZEPAMNOVO-LORAZEMPMS-LORAZEPAMATIVAN
ATIVAN
ATIVAN
ATIVAN
MIDAZOLAM
APX
SDZ
PFI
APX
APX
APXSNSTEVPMSWAY
APXSNSTEVPMSWAY
APXSNSTEVPMSWAY
WAY
WAY
WAY
SDZ
CENTRAL NERVOUS SYSTEM AGENTS
ANXIOLYTICS, SEDATIVES, AND HYPNOTICS
28:00
28:24.08
0.0867
0.7850
1.2286
0.1166
0.1364
0.0359 0.0359 0.0359 0.0359 0.0386
0.0447 0.0447 0.0447 0.0447 0.0481
0.0699 0.0699 0.0699 0.0699 0.0751
0.1153
0.1449
0.2254
4.1000
110 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$$$$$
$$$$$
$$$$$
$
$
$
$
(BENZODIAZEPINES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
NITRAZEPAM
OXAZEPAM
TEMAZEPAM
TRIAZOLAM
BUSPIRONE HCL
5 MG ORAL TABLET
10 MG ORAL TABLET
10 MG ORAL TABLET
15 MG ORAL TABLET
30 MG ORAL TABLET
15 MG ORAL CAPSULE
30 MG ORAL CAPSULE
0.125 MG ORAL TABLET
0.25 MG ORAL TABLET
10 MG ORAL TABLET
00002245230000022340030000222965400000511528
00002245231000022340070000222965500000511536
00000402680
00000402745
00000402737
00002225964000022448140000223009500000604453
00002225972000022448150000223010200000604461
00000808563
00000808571
00002211076000022314920000220767200002230942
APO-NITRAZEPAMSANDOZ NITRAZEPAMNITRAZADONMOGADON
APO-NITRAZEPAMSANDOZ NITRAZEPAMNITRAZADONMOGADON
APO-OXAZEPAM
APO-OXAZEPAM
APO-OXAZEPAM
APO-TEMAZEPAMCO TEMAZEPAMNOVO-TEMAZEPAMRESTORIL
APO-TEMAZEPAMCO TEMAZEPAMNOVO-TEMAZEPAMRESTORIL
APO-TRIAZO
APO-TRIAZO
APO-BUSPIRONENOVO-BUSPIRONENU-BUSPIRONEPMS-BUSPIRONE
APXSDZVCLVCL
APXSDZVCLVCL
APX
APX
APX
APXCOBTEVSUN
APXCOBTEVSUN
APX
APX
APXTEVNXPPMS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANXIOLYTICS, SEDATIVES, AND HYPNOTICS
ANXIOLYTICS, SEDATIVES, AND HYPNOTICS
28
28
:00
:00
28:24.08
28:24.92
0.0731 0.0731 0.0750 0.1602
0.1093 0.1093 0.1122 0.2397
0.0420
0.0660
0.0900
0.1102 0.1102 0.1102 0.2085
0.1326 0.1326 0.1326 0.2524
0.1496
0.2502
0.5957 0.5957 0.5957 0.5957
111 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$$$
$
$
$
$$$$
$$$$
$
$
$$$$
(BENZODIAZEPINES)
(MISCELLANEOUS ANXIOLYTICS, SEDATIVES, AND HYPNOTICS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CHLORAL HYDRATE
HYDROXYZINE HCL
ZOPICLONE
100 MG / ML ORAL SYRUP
10 MG ORAL CAPSULE
25 MG ORAL CAPSULE
50 MG ORAL CAPSULE
2 MG / ML ORAL SYRUP
50 MG / ML INJECTION
5 MG ORAL TABLET
7.5 MG ORAL TABLET
00000792659
0000064605900000738824
0000064602400000738832
0000064601600000738840
0000074181700000024694
00000742813
0000224507700002363534000022719310000229661600002251450000022434260000226791800002246534000022575720000234412200002216167
00002218313000023635420000227195800002238596000022514690000222827000002240606000022679260000224248100002008203000022575800000228244500001926799
PMS-CHLORAL HYDRATE
APO-HYDROXYZINENOVO-HYDROXYZIN
APO-HYDROXYZINENOVO-HYDROXYZIN
APO-HYDROXYZINENOVO-HYDROXYZIN
PMS-HYDROXYZINEATARAX
HYDROXYZINE HCL
APO-ZOPICLONEAVA-ZOPICLONECO ZOPICLONEMYLAN-ZOPICLONENOVO-ZOPICLONEPMS-ZOPICLONERAN-ZOPICLONERATIO-ZOPICLONESANDOZ ZOPICLONEZOPICLONEIMOVANE
APO-ZOPICLONEAVA-ZOPICLONECO ZOPICLONEMYLAN-ZOPICLONENOVO-ZOPICLONENU-ZOPICLONEPMS-ZOPICLONERAN-ZOPICLONERATIO-ZOPICLONERHOVANESANDOZ ZOPICLONEZOPICLONEIMOVANE
PMS
APXTEV
APXTEV
APXTEV
PMSERF
SDZ
APXAVACOBMYPTEVPMSRANRPHSDZSNSSAV
APXAVACOBMYPTEVNXPPMSRANRPHSDZSDZSNSSAV
CENTRAL NERVOUS SYSTEM AGENTS
ANXIOLYTICS, SEDATIVES, AND HYPNOTICS
28:00
28:24.92
0.0455
0.1116 0.1116
0.1425 0.1425
0.2068 0.2068
0.0436 0.0558
4.7500
0.2231 0.2231 0.2231 0.2231 0.2231 0.2231 0.2231 0.2231 0.2231 0.2231 1.1116
0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 0.4685 1.4035
112 EFFECTIVE APRIL 1, 2012
$
$$
$$
$$
$$
$
$$$$$$$$$$$
$$$$$$$$$$$$$
(MISCELLANEOUS ANXIOLYTICS, SEDATIVES, AND HYPNOTICS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
LITHIUM CARBONATE
NARATRIPTAN HCL
RIZATRIPTAN BENZOATE
150 MG ORAL CAPSULE
150 MG ORAL CAPSULE
300 MG ORAL CAPSULE
300 MG ORAL CAPSULE
600 MG ORAL CAPSULE
1 MG (BASE) ORAL TABLET
2.5 MG (BASE) ORAL TABLET
10 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL DISINTEGRATING TABLET
10 MG (BASE) ORAL DISINTEGRATING TABLET
000022428370000221613200000461733
0000224283700002013231
000022428380000221614000000236683
0000224283800000406775
00002216159
0000231429000002237820
000023143040000232232300002237821
00002240521
00002240518
00002240519
APO-LITHIUM CARBONATEPMS-LITHIUM CARBONATECARBOLITH
APO-LITHIUM CARBONATELITHANE
APO-LITHIUM CARBONATEPMS-LITHIUM CARBONATECARBOLITH
APO-LITHIUM CARBONATELITHANE
PMS-LITHIUM CARBONATE
NOVO-NARATRIPTANAMERGE
NOVO-NARATRIPTANSANDOZ NARATRIPTANAMERGE
MAXALT
MAXALT RPD
MAXALT RPD
APXPMSVCL
APXERF
APXPMSVCL
APXERF
PMS
TEVGSK
TEVSDZGSK
MFC
MFC
MFC
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTIMANIC AGENTS
ANTIMIGRAINE AGENTS
28
28
:00
:00
28:28
28:32.28
0.0532 0.0532 0.1279
0.0532 0.1095
0.0533 0.0533 0.0993
0.0533 0.1091
0.1429
6.7151 15.2344
7.0760 7.0760
16.0575
15.2201
15.2201
15.2201
113 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$$
$$$
$$
$
$$
$$$
$
$
$
RESTRICTED BENEFIT - This product is a benefit for patients 18 to 64 years of age inclusive for the treatment of acute migraine attacks in patients where other standard therapy has failed. (Refer to Criteria for Special Authorization of Select Drug Products of the List for eligibility in patients 65 years of age and older; and Criteria for Special Authorization of Select Drug Products in the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
RESTRICTED BENEFIT - This product is a benefit for patients 18 to 64 years of age inclusive for the treatment of acute migraine attacks in patients where standard therapy has failed. (Refer to Criteria for Special Authorization of Select Drug Products of the List for eligibility in patients 65 years of age and older; and Criteria for Special Authorization of Select Drug Products of the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
(SELECTIVE SEROTONIN AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SUMATRIPTAN HEMISULFATE
SUMATRIPTAN SUCCINATE
5 MG / DOSE (BASE) NASAL UNIT DOSE SPRAY
20 MG / DOSE (BASE) NASAL UNIT DOSE SPRAY
50 MG (BASE) ORAL TABLET
100 MG (BASE) ORAL TABLET
6 MG / SYR (BASE) INJECTION SYRINGE
00002230418
00002230420
000023662580000226891400002286823000022865210000226838800002257890000022564360000226302500002212153
00002366266000022689220000223936700002286831000022865480000226839600002257904000022564440000226303300002212161
0000236169800002212188
IMITREX
IMITREX
AVA-SUMATRIPTANMYLAN-SUMATRIPTANNOVO-SUMATRIPTAN DFSUMATRIPTANAPO-SUMATRIPTANCO SUMATRIPTANPMS-SUMATRIPTANSANDOZ SUMATRIPTANIMITREX DF
AVA-SUMATRIPTANMYLAN-SUMATRIPTANNOVO-SUMATRIPTANNOVO-SUMATRIPTAN DFSUMATRIPTANAPO-SUMATRIPTANCO SUMATRIPTANPMS-SUMATRIPTANSANDOZ SUMATRIPTANIMITREX DF
SUMATRIPTAN SUN (0.5 ML)IMITREX (0.5 ML)
GSK
GSK
AVAMYPTEVSNSAPXCOBPMSSDZGSK
AVAMYPTEVTEVSNSAPXCOBPMSSDZGSK
SPGGSK
CENTRAL NERVOUS SYSTEM AGENTS
ANTIMIGRAINE AGENTS
28:00
28:32.28
15.4648
15.9148
8.9350 8.9350 8.9350 8.9350 8.9364 8.9364 8.9364 8.9364
16.2935
9.8433 9.8433 9.8433 9.8433 9.8433 9.8442 9.8442 9.8442 9.8442
17.9491
30.8600 47.3968
114 EFFECTIVE APRIL 1, 2012
$
$
$$$$$$$$$
$$$$$$$$$$
$$
RESTRICTED BENEFIT - This product is a benefit for patients 18 to 64 years of age inclusive for the treatment of acute migraine attacks in patients where other standard therapy has failed. (Refer to Criteria for Special Authorization of Select Drug Products of the List for eligibility in patients 65 years of age and older; and Criteria for Special Authorization of Select Drug Products of the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
RESTRICTED BENEFIT - This product is a benefit for patients 18 to 64 years of age inclusive for the treatment of acute migraine attacks in patients where other standard therapy has failed. (Refer to Criteria for Special Authorization of Select Drug Products of the List for eligibility in patients 65 years of age and older, and Criteria for Special Authorization of Select Drug Products in the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
(SELECTIVE SEROTONIN AGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ZOLMITRIPTAN
PIZOTIFEN MALATE
AMANTADINE HCL
2.5 MG ORAL TABLET
2.5 MG ORAL DISPERSIBLE TABLET
5 MG / DOSE NASAL UNIT DOSE SPRAY
0.5 MG (BASE) ORAL TABLET
100 MG ORAL CAPSULE
10 MG / ML ORAL SYRUP
0000236903600002324229000023629880000231396000002238660
00002324768000023629960000234254500002243045
00002248993
00000329320
0000213920000001990403
00002022826
MYLAN-ZOLMITRIPTANPMS-ZOLMITRIPTANSANDOZ ZOLMITRIPTANTEVA-ZOLMITRIPTANZOMIG
PMS-ZOLMITRIPTAN ODTSANDOZ ZOLMITRIPTAN ODTTEVA-ZOLMITRIPTAN ODZOMIG RAPIMELT
ZOMIG
SANDOMIGRAN
MYLAN-AMANTADINEPMS-AMANTADINE HYDROCHLORIDE
PMS-AMANTADINE HYDROCHLORIDE
MYPPMSSDZTEVAZC
PMSSDZTEVAZC
AZC
PAL
MYPPMS
PMS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTIMIGRAINE AGENTS
ANTIMIGRAINE AGENTS
ANTIPARKINSONIAN AGENTS
28
28
28
:00
:00
:00
28:32.28
28:32.92
28:36.04
6.5597 6.5597 6.5597 6.5597
14.8887
6.5621 6.5621 6.5621
14.8887
14.8887
0.3875
0.5179 0.5179
0.1005
115 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$
$$$$
$
$
$$
$
RESTRICTED BENEFIT - This product is a benefit for patients 18 to 64 years of age inclusive for the treatment of acute migraine attacks in patients where other standard therapy has failed. (Refer to Criteria for Special Authorization of Select Drug Products of the List for eligibility in patients 65 years of age and older; and Criteria for Special Authorization of Select Drug Products of the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
(SELECTIVE SEROTONIN AGONISTS)
(MISCELLANEOUS ANTIMIGRAINE AGENTS)
(ADAMANTANES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
BENZTROPINE MESYLATE
ETHOPROPAZINE HCL
PROCYCLIDINE HCL
TRIHEXYPHENIDYL HCL
ENTACAPONE
LEVODOPA/ BENSERAZIDE HCL
1 MG ORAL TABLET
2 MG ORAL TABLET
1 MG / ML INJECTION
50 MG (BASE) ORAL TABLET
2.5 MG ORAL TABLET
5 MG ORAL TABLET
0.5 MG / ML ORAL ELIXIR
2 MG ORAL TABLET
5 MG ORAL TABLET
200 MG ORAL TABLET
50 MG * 12.5 MG (BASE) ORAL CAPSULE
100 MG * 25 MG (BASE) ORAL CAPSULE
200 MG * 50 MG (BASE) ORAL CAPSULE
00000706531
0000042685700000587265
00002238903
00001927744
00000649392
00000587354
00000587362
00000545058
00000545074
00002243763
00000522597
00000386464
00000386472
PMS-BENZTROPINE
BENZTROPINEPMS-BENZTROPINE
BENZTROPINE OMEGA
PARSITAN
PMS-PROCYCLIDINE
PMS-PROCYCLIDINE
PMS-PROCYCLIDINE
TRIHEXYPHENIDYL
TRIHEXYPHENIDYL
COMTAN
PROLOPA 50-12.5
PROLOPA 100-25
PROLOPA 200-50
PMS
PMSPMS
OMG
ERF
PMS
PMS
PMS
AAP
AAP
NOV
HLR
HLR
HLR
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTIPARKINSONIAN AGENTS
ANTIPARKINSONIAN AGENTS
ANTIPARKINSONIAN AGENTS
28
28
28
:00
:00
:00
28:36.08
28:36.12
28:36.16
0.0450
0.0450 0.0450
7.5000
0.2237
0.0624
0.1248
0.2516
0.0397
0.0718
1.7414
0.2996
0.4932
0.8280
116 EFFECTIVE APRIL 1, 2012
$
$$
$
$
$
$
$
$
$
$
$
$
$
(ANTICHOLINERGIC AGENTS)
(CATECHOL-O-METHYLTRANSFERASE (COMT) INHIBITORS)
(DOPAMINE PRECURSORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
LEVODOPA/ CARBIDOPA
LEVODOPA/ CARBIDOPA/ ENTACAPONE
BROMOCRIPTINE MESYLATE
100 MG * 10 MG ORAL TABLET
100 MG * 25 MG ORAL TABLET
250 MG * 25 MG ORAL TABLET
100 MG * 25 MG ORAL SUSTAINED-RELEASE TABLET
200 MG * 50 MG ORAL SUSTAINED-RELEASE TABLET
50 MG * 12.5 MG * 200 MG ORAL TABLET
75 MG * 18.75 MG * 200 MG ORAL TABLET
100 MG * 25 MG * 200 MG ORAL TABLET
125 MG * 31.25 MG * 200 MG ORAL TABLET
150 MG * 37.5 MG * 200 MG ORAL TABLET
2.5 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL CAPSULE
00002195933000022444940000218283100000355658
00002195941000022444950000218282300000513997
00002195968000022444960000218285800000328219
0000227287300002028786
00000870935
00002305933
00002337827
00002305941
00002337835
00002305968
00002087324
00002230454
APO-LEVOCARBNOVO-LEVOCARBIDOPANU-LEVOCARBSINEMET 100/10
APO-LEVOCARBNOVO-LEVOCARBIDOPANU-LEVOCARBSINEMET 100/25
APO-LEVOCARBNOVO-LEVOCARBIDOPANU-LEVOCARBSINEMET 250/25
LEVOCARB CRSINEMET CR 100/25
SINEMET CR 200/50
STALEVO
STALEVO
STALEVO
STALEVO
STALEVO
APO-BROMOCRIPTINE
APO-BROMOCRIPTINE
APXTEVNXPMFC
APXTEVNXPMFC
APXTEVNXPMFC
AAPMFC
MFC
NOV
NOV
NOV
NOV
NOV
APX
APX
(ERGOT-DERIVATIVE-DOPAMINE RECEPTOR AGONISTS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTIPARKINSONIAN AGENTS
ANTIPARKINSONIAN AGENTS
28
28
:00
:00
28:36.16
28:36.20.04
0.2365 0.2365 0.2365 0.4554
0.3532 0.3532 0.3532 0.6800
0.3943 0.3943 0.3943 0.7591
0.5126 0.7374
1.3603
1.7219
1.7219
1.7219
1.7219
1.7219
0.9782
1.4644
117 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$$$$
$$$$
$$
$
$
$
$
$
$
$
$
(DOPAMINE PRECURSORS)
DOPAMINE RECEPTOR AGONISTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
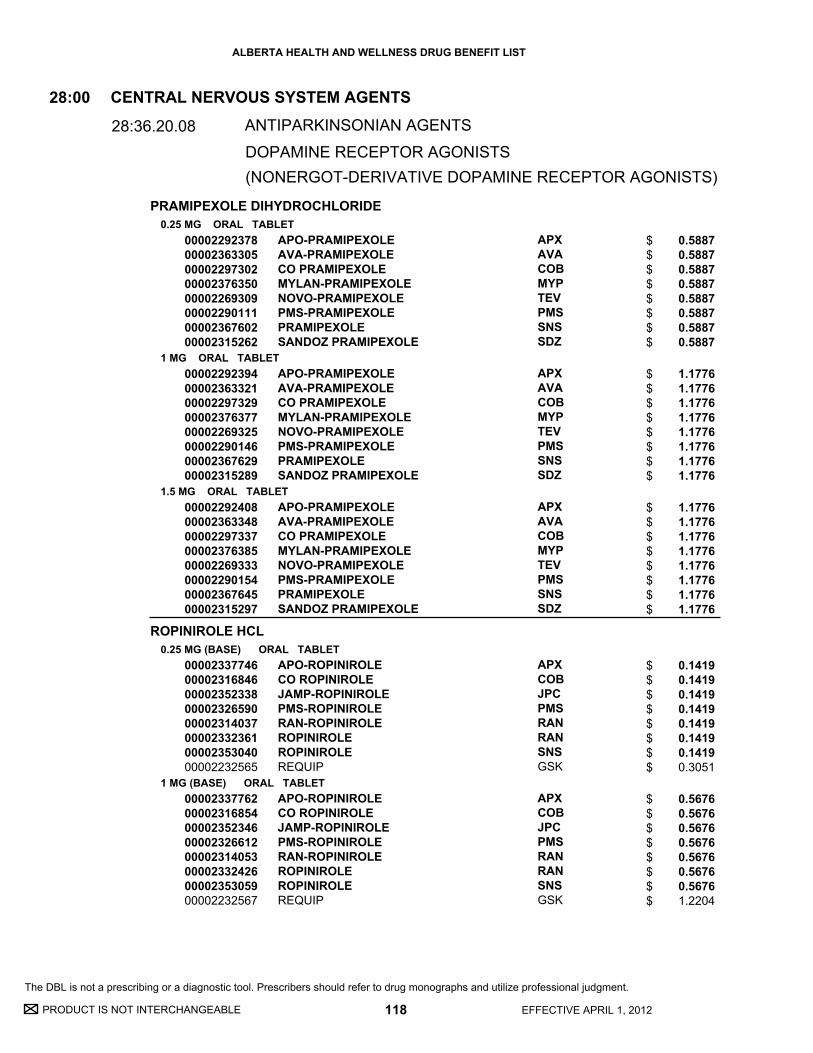
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PRAMIPEXOLE DIHYDROCHLORIDE
ROPINIROLE HCL
0.25 MG ORAL TABLET
1 MG ORAL TABLET
1.5 MG ORAL TABLET
0.25 MG (BASE) ORAL TABLET
1 MG (BASE) ORAL TABLET
0000229237800002363305000022973020000237635000002269309000022901110000236760200002315262
0000229239400002363321000022973290000237637700002269325000022901460000236762900002315289
0000229240800002363348000022973370000237638500002269333000022901540000236764500002315297
0000233774600002316846000023523380000232659000002314037000023323610000235304000002232565
0000233776200002316854000023523460000232661200002314053000023324260000235305900002232567
APO-PRAMIPEXOLEAVA-PRAMIPEXOLECO PRAMIPEXOLEMYLAN-PRAMIPEXOLENOVO-PRAMIPEXOLEPMS-PRAMIPEXOLEPRAMIPEXOLESANDOZ PRAMIPEXOLE
APO-PRAMIPEXOLEAVA-PRAMIPEXOLECO PRAMIPEXOLEMYLAN-PRAMIPEXOLENOVO-PRAMIPEXOLEPMS-PRAMIPEXOLEPRAMIPEXOLESANDOZ PRAMIPEXOLE
APO-PRAMIPEXOLEAVA-PRAMIPEXOLECO PRAMIPEXOLEMYLAN-PRAMIPEXOLENOVO-PRAMIPEXOLEPMS-PRAMIPEXOLEPRAMIPEXOLESANDOZ PRAMIPEXOLE
APO-ROPINIROLECO ROPINIROLEJAMP-ROPINIROLEPMS-ROPINIROLERAN-ROPINIROLEROPINIROLEROPINIROLEREQUIP
APO-ROPINIROLECO ROPINIROLEJAMP-ROPINIROLEPMS-ROPINIROLERAN-ROPINIROLEROPINIROLEROPINIROLEREQUIP
APXAVACOBMYPTEVPMSSNSSDZ
APXAVACOBMYPTEVPMSSNSSDZ
APXAVACOBMYPTEVPMSSNSSDZ
APXCOBJPCPMSRANRANSNSGSK
APXCOBJPCPMSRANRANSNSGSK
(NONERGOT-DERIVATIVE DOPAMINE RECEPTOR AGONISTS)
CENTRAL NERVOUS SYSTEM AGENTS
ANTIPARKINSONIAN AGENTS
28:00
28:36.20.08
0.5887 0.5887 0.5887 0.5887 0.5887 0.5887 0.5887 0.5887
1.1776 1.1776 1.1776 1.1776 1.1776 1.1776 1.1776 1.1776
1.1776 1.1776 1.1776 1.1776 1.1776 1.1776 1.1776 1.1776
0.1419 0.1419 0.1419 0.1419 0.1419 0.1419 0.1419 0.3051
0.5676 0.5676 0.5676 0.5676 0.5676 0.5676 0.5676 1.2204
118 EFFECTIVE APRIL 1, 2012
$$$$$$$$
$$$$$$$$
$$$$$$$$
$$$$$$$$
$$$$$$$$
DOPAMINE RECEPTOR AGONISTS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ROPINIROLE HCL
SELEGILINE HCL
PIZOTIFEN MALATE
2 MG (BASE) ORAL TABLET
5 MG (BASE) ORAL TABLET
5 MG ORAL TABLET
1 MG (BASE) ORAL TABLET
0000233777000002316862000023523540000232662000002314061000023324340000235306700002232568
0000233780000002316870000023523620000232663900002314088000023324420000235307500002232569
00002230641000022310360000206808700002230717
00000511552
APO-ROPINIROLECO ROPINIROLEJAMP-ROPINIROLEPMS-ROPINIROLERAN-ROPINIROLEROPINIROLEROPINIROLEREQUIP
APO-ROPINIROLECO ROPINIROLEJAMP-ROPINIROLEPMS-ROPINIROLERAN-ROPINIROLEROPINIROLEROPINIROLEREQUIP
APO-SELEGILINEMYLAN-SELEGILINENOVO-SELEGILINENU-SELEGILINE
SANDOMIGRAN DS
APXCOBJPCPMSRANRANSNSGSK
APXCOBJPCPMSRANRANSNSGSK
APXMYPTEVNXP
PAL
(NONERGOT-DERIVATIVE DOPAMINE RECEPTOR AGONISTS)
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
CENTRAL NERVOUS SYSTEM AGENTS
ANTIPARKINSONIAN AGENTS
ANTIPARKINSONIAN AGENTS
MISCELLANEOUS CENTRAL NERVOUS SYSTEM AGENTS
28
28
28
:00
:00
:00
28:36.20.08
28:36.32
28:92
0.6244 0.6244 0.6244 0.6244 0.6244 0.6244 0.6244 1.3426
1.7192 1.7192 1.7192 1.7192 1.7192 1.7192 1.7192 3.6963
1.2650 1.2650 1.2650 1.2650
0.6434
119 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$
$$$$$$$$
$$$$
$
DOPAMINE RECEPTOR AGONISTS
(MONOAMINE OXIDASE B INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

34:00 Dental A
gents
34:00
Dental Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SODIUM FLUORIDE2.21 MG ORAL CHEWABLE TABLET
5.56 MG / ML ORAL DROPS00000575569
00000610100
FLUOR-A-DAY
FLUOR-A-DAY
PMS
PMS
DENTAL AGENTS34:00
34:00
0.0932
0.1864
121 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

36:00 Diagnostic A
gents
36:00
Diagnostic Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
THYROTROPIN ALFA0.9 MG / VIAL INJECTION
00002246016 THYROGEN GZM
DIAGNOSTIC AGENTS
THYROID FUNCTION
36:00
36:60
1363.7200
123 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

40:00 Electrolytic, Caloric, and W
ater Balance
40:00
Electrolytic, Caloric, and Water Balance

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
LACTULOSE
MAGNESIUM GLUCOHEPTONATE
MAGNESIUM GLUCONATE
POTASSIUM CHLORIDE (K+)
POTASSIUM CHLORIDE (K+)(CL-)
POTASSIUM CITRATE (K+)
SODIUM ACID PHOSPHATE/ SODIUM BICARBONATE/ POTASSIUM BICARBONATE
CALCIUM POLYSTYRENE SULPHONATE
667 MG / ML ORAL SYRUP
100 MG / ML ORAL SOLUTION
500 MG ORAL TABLET
8 MEQ ORAL SUSTAINED-RELEASE TABLET
20 MEQ ORAL SUSTAINED-RELEASE TABLET
8 MEQ ORAL SUSTAINED-RELEASE CAPSULE
1.33 MEQ / ML ORAL LIQUID
25 MEQ ORAL EFFERVESCENT TABLET
500 MG (BASE) * 469 MG (BASE) * 123 MG (BASE) ORAL EFFERVESCENT TABLET
ORAL POWDER
0000224281400002295881000007034860000085440900002331551
00000026697
00000555126
0000060288400000074225
00000713376
00002042304
0000223860400001918303
00002085992
00000225819
00002017741
APO-LACTULOSEJAMP-LACTULOSEPMS-LACTULOSERATIO-LACTULOSETEVA-LACTULOSE
ROUGIER MAGNESIUM
MAGLUCATE
APO-KSLOW K
K-DUR
MICRO-K EXTENCAPS
PMS - POTASSIUM CHLORIDEK-10 ORAL LIQUID
K-LYTE
PHOSPHATE-NOVARTIS
RESONIUM CALCIUM
APXJPCPMSRPHTEV
ROG
PMS
APXNOV
MFC
PAL
PMSGSK
WSP
NOV
SAV
ELECTROLYTIC, CALORIC, AND WATER BALANCE
ELECTROLYTIC, CALORIC, AND WATER BALANCE
ELECTROLYTIC, CALORIC, AND WATER BALANCE
AMMONIA DETOXICANTS
REPLACEMENT PREPARATIONS
ION-REMOVING AGENTS
40
40
40
:00
:00
:00
40:10
40:12
40:18.18
0.0145 0.0145 0.0145 0.0145 0.0145
0.0200
0.1253
0.0899 0.1586
0.2052
0.0930
0.0146 0.0169
0.5550
0.7372
0.3811
125 EFFECTIVE APRIL 1, 2012
$ 0.0899
UNIT OF ISSUE - REFER TO PRICE POLICY
MAC pricing has been applied based on the lowest unit cost for an 8 mEq (K+) oral sustained-release tablet: APO-K.
$$$$$
$
$
$$
$
$
$$
$
$
$
(POTASSIUM-REMOVING AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SODIUM POLYSTYRENE SULFONATE
AMILORIDE HCL
HYDROCHLOROTHIAZIDE
HYDROCHLOROTHIAZIDE/ AMILORIDE HCL
HYDROCHLOROTHIAZIDE/ TRIAMTERENE
250 MG / ML ORAL SUSPENSION
ORAL POWDER
30 G / ENM RECTAL RETENTION ENEMA
5 MG ORAL TABLET
12.5 MG ORAL TABLET
25 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
50 MG * 5 MG ORAL TABLET
25 MG * 50 MG ORAL TABLET
00000769541
0000075533800002026961
00000769533
00002249510
00002274086
000003268440000236396800000021474
000003128000000236397600000021482
00000644552
000007844000000193721900000886106
000004417750000053265700000865532
PMS-SODIUM POLYSTYRENE SULF.
PMS-SODIUM POLYSTYRENE SULF.KAYEXALATE
PMS-SOD POLYSTYR SULF (120 ML)
MIDAMOR
PMS-HYDROCHLOROTHIAZIDE
APO-HYDROAVA-HYDROCHLOROTHIAZIDENOVO-HYDRAZIDE
APO-HYDROAVA-HYDROCHLOROTHIAZIDENOVO-HYDRAZIDE
APO-HYDRO
APO-AMILZIDENOVAMILORNU-AMILZIDE
APO-TRIAZIDENOVO-TRIAMZIDENU-TRIAZIDE
PMS
PMSSAV
PMS
AAP
PMS
APXAVATEV
APXAVATEV
APX
APXTEVNXP
APXTEVNXP
ELECTROLYTIC, CALORIC, AND WATER BALANCE
ELECTROLYTIC, CALORIC, AND WATER BALANCE
ELECTROLYTIC, CALORIC, AND WATER BALANCE
ION-REMOVING AGENTS
DIURETICS
DIURETICS
40
40
40
:00
:00
:00
40:18.18
40:28.16
40:28.20
0.1306
0.1696 0.1973
15.3608
0.2921
0.0338
0.0395 0.0395 0.0395
0.0551 0.0551 0.0551
0.1232
0.1917 0.1917 0.1917
0.0608 0.0608 0.0608
126 EFFECTIVE APRIL 1, 2012
$
$$
$
$
$
$$$
$$$
$
$$$
$$$
(POTASSIUM-REMOVING AGENTS)
(POTASSIUM-SPARING DIURETICS)
(THIAZIDE DIURETICS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CHLORTHALIDONE
INDAPAMIDE HEMIHYDRATE
METOLAZONE
PROBENECID
SULFINPYRAZONE
50 MG ORAL TABLET
1.25 MG (BASE) ORAL TABLET
2.5 MG (BASE) ORAL TABLET
2.5 MG ORAL TABLET
500 MG ORAL TABLET
200 MG ORAL TABLET
00000360279
000022452460000224006700002239619
000022236780000215348300002231184000022235970000223962000000564966
00000888400
00000294926
00000441767
CHLORTHALIDONE
APO-INDAPAMIDEMYLAN-INDAPAMIDEPMS-INDAPAMIDE
APO-INDAPAMIDEMYLAN-INDAPAMIDENOVO-INDAPAMIDENU-INDAPAMIDEPMS-INDAPAMIDELOZIDE
ZAROXOLYN
BENURYL
SULFINPYRAZONE
AAP
APXMYPPMS
APXMYPTEVNXPPMSSEV
SAV
VCL
AAP
ELECTROLYTIC, CALORIC, AND WATER BALANCE
ELECTROLYTIC, CALORIC, AND WATER BALANCE
DIURETICS
URICOSURIC AGENTS
40
40
:00
:00
40:28.24
40:40
0.1335
0.1877 0.1877 0.1877
0.2933 0.2933 0.2933 0.2933 0.2933 0.5238
0.2082
0.5676
0.3222
127 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$
$$$$$$
$
$
$
(THIAZIDE-LIKE DIURETICS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
48:00 Respiratory Tract A
gents
48:00
Respiratory Tract Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
MONTELUKAST SODIUM
ZAFIRLUKAST
10 MG (BASE) ORAL TABLET
4 MG (BASE) ORAL CHEWABLE TABLET
5 MG (BASE) ORAL CHEWABLE TABLET
4 MG (BASE) ORAL GRANULE
20 MG ORAL TABLET
000023746090000236822600002373947000023285930000235552300002238217
0000237760800002354977000023303850000235550700002243602
0000237761600002354985000023303930000235551500002238216
0000235861100002247997
00002236606
APO-MONTELUKASTMYLAN-MONTELUKASTPMS-MONTELUKAST FCSANDOZ MONTELUKASTTEVA-MONTELUKASTSINGULAIR
APO-MONTELUKASTPMS-MONTELUKASTSANDOZ MONTELUKASTTEVA-MONTELUKASTSINGULAIR
APO-MONTELUKASTPMS-MONTELUKASTSANDOZ MONTELUKASTTEVA-MONTELUKASTSINGULAIR
SANDOZ MONTELUKASTSINGULAIR
ACCOLATE
APXMYPPMSSDZTEVMFC
APXPMSSDZTEVMFC
APXPMSSDZTEVMFC
SDZMFC
AZC
RESPIRATORY TRACT AGENTS
ANTI-INFLAMMATORY AGENTS
48:00
48:10.24
1.0641 1.0641 1.0641 1.0641 1.0641 2.4238
0.6562 0.6562 0.6562 0.6562 1.4904
0.7245 0.7245 0.7245 0.7245 1.6503
0.6562 1.4904
0.8054
129 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$
$$$$$
$$$$$
$$
$
RESTRICTED BENEFIT - This product is a benefit for patients 6 to 18 years of age inclusive for the prophylaxis and treatment of asthma. (For eligibility in patients over 18 years of age refer to Criteria for Special Authorization of Select Drug Products of the List, and Criteria for Special Authorization of Select Drug Products in the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
RESTRICTED BENEFIT - This product is a benefit for patients 2 to 18 years of age inclusive for the prophylaxis and treatment of asthma.
RESTRICTED BENEFIT - This product is a benefit for patients 6 to 18 years of age inclusive for the prophylaxis and treatment of asthma. (For eligibility in patients over 18 years of age refer to Criteria for Special Authorization of Select Drug Products of the List, and Criteria for Special Authorization of Select Drug Products in the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
RESTRICTED BENEFIT - This product is a benefit for patients 2 to 18 years of age inclusive for the prophylaxis and treatment of asthma.
RESTRICTED BENEFIT - This product is a benefit for patients 12 to 18 years of age inclusive for the prophylaxis and treatment of asthma. (For eligibility in patients over 18 years of age refer to the Criteria for Special Authorization of Select Drug Products of the List, and Criteria forSpecial Authorization of Select Drug Products in the Alberta Human Services Drug Benefit Supplement for eligibility in Alberta Human Services and Alberta Seniors (AISH) clients.)
(LEUKOTRIENE MODIFIERS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
SODIUM CROMOGLYCATE
ACETYLCYSTEINE
100 MG ORAL CAPSULE
1 % INHALATION SOLUTION
20 % INHALATION SOLUTION
00000500895
00002046113
0000224309800002091526
NALCROM
PMS-SODIUM CROMOGLYCATE
ACETYLCYSTEINEMUCOMYST
SAV
PMS
SDZWSP
RESPIRATORY TRACT AGENTS
RESPIRATORY TRACT AGENTS
ANTI-INFLAMMATORY AGENTS
MUCOLYTIC AGENTS
48
48
:00
:00
48:10.32
48:24
1.5347
0.7696
0.6800 0.7200
130 EFFECTIVE APRIL 1, 2012
$
$
$$
(MAST-CELL STABILIZERS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

52:00 Eye, Ear, Nose and Throat (EEN
T) Preparations
52:00
Eye, Ear, Nose and Throat (EENT) Preparations

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CIPROFLOXACIN HCL
ERYTHROMYCIN
GENTAMICIN SULFATE
NEOMYCIN SULFATE/ POLYMYXIN B SULFATE/ GRAMICIDIN
OFLOXACIN
TOBRAMYCIN
TRIFLURIDINE
0.3 % (BASE) OPHTHALMIC SOLUTION
0.5 % OPHTHALMIC OINTMENT
0.3 % (BASE) OPHTHALMIC SOLUTION
0.3 % (BASE) OPHTHALMIC OINTMENT
0.3 % (BASE) OTIC SOLUTION
0.25 % * 10,000 UNIT / ML * 0.03 MG / ML OTIC/OPHTHALMIC SOLUTION
0.3 % OPHTHALMIC SOLUTION
0.3 % OPHTHALMIC SOLUTION
0.3 % OPHTHALMIC OINTMENT
1 % OPHTHALMIC SOLUTION
0000225393300001945270
00001912755
0000051219200002229440
00002230888
0000051218400002229441
00000807435
000022483980000225257000002143291
000022395770000224175500000513962
00000614254
0000224852900000687456
PMS-CIPROFLOXACINCILOXAN
PMS-ERYTHROMYCIN
GARAMYCINSANDOZ GENTAMICIN SULFATE
SANDOZ GENTAMICIN SULFATE
GARAMYCINSANDOZ GENTAMICIN SULFATE
OPTIMYXIN PLUS
APO-OFLOXACINPMS-OFLOXACINOCUFLOX
PMS-TOBRAMYCINSANDOZ TOBRAMYCINTOBREX
TOBREX
SANDOZ TRIFLURIDINEVIROPTIC
PMSALC
PMS
MFCSDZ
SDZ
MFCSDZ
SDZ
APXPMSALL
PMSSDZALC
ALC
SDZVCL
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTI-INFECTIVES
ANTI-INFECTIVES
52
52
:00
:00
52:04.04
52:04.20
1.1280 2.1825
1.2959
0.4060 0.4060
1.5357
1.0320 1.0320
0.8230
0.9920 0.9920 2.6295
1.0029 1.0029 1.8743
2.6583
3.2520 3.2666
131 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$$
$
$$
$
$$$
$$$
$
$$
(ANTIBACTERIALS)
(ANTIVIRALS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
BECLOMETHASONE DIPROPIONATE
BUDESONIDE
CIPROFLOXACIN HCL/ DEXAMETHASONE
DEXAMETHASONE
DEXAMETHASONE SODIUM PHOSPHATE
FLUNISOLIDE
FLUOROMETHOLONE
FLUOROMETHOLONE ACETATE
HYDROCORTISONE ACETATE
MOMETASONE FUROATE
50 MCG / DOSE NASAL METERED DOSE SPRAY
100 MCG / DOSE NASAL METERED DOSE AEROSOL
100 MCG / DOSE NASAL METERED DOSE SPRAY
0.3 % * 0.1 % OTIC SUSPENSION
0.1 % OPHTHALMIC SUSPENSION
0.1 % OPHTHALMIC OINTMENT
0.1 % OTIC/OPHTHALMIC SOLUTION
0.025 % NASAL SPRAY
0.1 % OPHTHALMIC SUSPENSION
0.25 % OPHTHALMIC SUSPENSION
0.1 % OPHTHALMIC SUSPENSION
2.5 % OPHTHALMIC OINTMENT
50 MCG / DOSE NASAL METERED DOSE SPRAY
000022387960000217271200002238577
00002035324
00002230648
00002252716
00000042560
00000042579
00000739839
00002239288
00002238568
00000707511
00000756784
00001980661
00002238465
APO-BECLOMETHASONEMYLAN-BECLO AQ.NU-BECLOMETHASONE
RHINOCORT TURBUHALER
MYLAN-BUDESONIDE AQ
CIPRODEX
MAXIDEX
MAXIDEX
SANDOZ DEXAMETHASONE SOD. PHOSPHATE
APO-FLUNISOLIDE
PMS-FLUOROMETHOLONE
FML FORTE
FLAREX
CORTAMED
NASONEX
APXMYPNXP
AZC
MYP
ALC
ALC
ALC
SDZ
APX
PMS
ALL
ALC
SDZ
MFC
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTI-INFLAMMATORY AGENTS
52:00
52:08.08
0.0613 0.0613 0.0613
0.1266
0.1006
3.8198
1.7325
2.6840
1.4060
0.5940
1.7880
2.8229
1.9575
6.2000
0.2065
132 EFFECTIVE APRIL 1, 2012
$$$
$
$
$
$
$
$
$
$
$
$
$
$RESTRICTED BENEFIT - This product is a benefit for patients 3 to 12 years of age inclusive for the treatment of seasonal allergic rhinitis or perennial allergic rhinitis.
(CORTICOSTEROIDS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PREDNISOLONE ACETATE
BETAMETHASONE SODIUM PHOSPHATE/ GENTAMICIN SULFATE
DEXAMETHASONE/ FRAMYCETIN SULFATE/ GRAMICIDIN
DEXAMETHASONE/ NEOMYCIN SULFATE/ POLYMYXIN B SULFATE
DEXAMETHASONE/ TOBRAMYCIN
FLUMETHASONE PIVALATE/ CLIOQUINOL
PREDNISOLONE ACETATE/ SULFACETAMIDE SODIUM
0.12 % OPHTHALMIC SUSPENSION
1 % OPHTHALMIC SUSPENSION
0.1 % (BASE) * 0.3 % (BASE) OTIC/OPHTHALMIC SOLUTION
0.5 MG / ML * 5 MG / ML * 0.05 MG / ML OTIC/OPHTHALMIC SOLUTION
1 MG / ML * 3.5 MG / ML (BASE) * 6,000 UNIT / ML OPHTHALMIC SUSPENSION
1 MG / G * 3.5 MG / G (BASE) * 6,000 UNIT / G OPHTHALMIC OINTMENT
0.1 % * 0.3 % OPHTHALMIC SUSPENSION
0.1 % * 0.3 % OPHTHALMIC OINTMENT
0.02 % * 1 % OTIC SOLUTION
0.2 % * 10 % OPHTHALMIC SUSPENSION
0.2 % * 10 % OPHTHALMIC OINTMENT
0000191618100000299405
000007004010000191620300000301175
0000068221700002244999
0000224792000002224623
00000042676
00000358177
00000778907
00000778915
00000074454
00000807788
00000307246
SANDOZ PREDNISOLONE ACETATEPRED MILD
RATIO-PREDNISOLONESANDOZ PREDNISOLONE ACETATEPRED FORTE
GARASONESANDOZ PENTASONE
SANDOZ OPTICORTSOFRACORT
MAXITROL
MAXITROL
TOBRADEX
TOBRADEX
LOCACORTEN VIOFORM
BLEPHAMIDE
BLEPHAMIDE S.O.P.
SDZALL
RPHSDZALL
MFCSDZ
SDZSAV
ALC
ALC
ALC
ALC
PAL
ALL
ALL
(COMBINATION ANTI-INFECTIVE/CORTICOSTEROID AGENTS)
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTI-INFLAMMATORY AGENTS
ANTI-INFLAMMATORY AGENTS
52
52
:00
:00
52:08.08
52:08.08.00
1.3450 1.9307
1.9400 1.9400 5.6846
1.2813 1.2813
1.3000 2.0063
2.1420
2.9861
2.1930
3.2311
1.4790
2.8620
3.6611
133 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$$
$$
$$
$
$
$
$
$
$
$
(CORTICOSTEROIDS)
CORTICOSTEROIDS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DICLOFENAC SODIUM
KETOROLAC TROMETHAMINE
LIDOCAINE HCL
PROPARACAINE HCL
ATROPINE SULFATE
CYCLOPENTOLATE HCL
HOMATROPINE HYDROBROMIDE
TROPICAMIDE
0.1 % OPHTHALMIC SOLUTION
0.5 % OPHTHALMIC SOLUTION
2 % ORAL LIQUID
0.5 % OPHTHALMIC SOLUTION
1 % OPHTHALMIC SOLUTION
1 % OPHTHALMIC SOLUTION
2 % OPHTHALMIC SOLUTION
5 % OPHTHALMIC SOLUTION
0.5 % OPHTHALMIC SOLUTION
1 % OPHTHALMIC SOLUTION
00001940414
000022458210000224746100001968300
0000196882300000001686
00000035076
00000035017
00000252506
00000000779
00000000787
00000000981
00000001007
VOLTAREN OPHTHA
APO-KETOROLACRATIO-KETOROLACACULAR
LIDODAN VISCOUSXYLOCAINE VISCOUS
ALCAINE
ISOPTO ATROPINE
CYCLOGYL
ISOPTO HOMATROPINE
ISOPTO HOMATROPINE
MYDRIACYL
MYDRIACYL
ALC
APXRPHALL
ODNAZC
ALC
ALC
ALC
ALC
ALC
ALC
ALC
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTI-INFLAMMATORY AGENTS
LOCAL ANESTHETICS
MYDRIATICS
52
52
52
:00
:00
:00
52:08.20
52:16
52:24
2.7090
2.0160 2.0160 3.6120
0.0525 0.1021
0.6751
0.6750
0.9075
0.6863
0.8175
0.9413
1.2113
134 EFFECTIVE APRIL 1, 2012
$
$$$
$$
$
$
$
$
$
$
$
(NONSTEROIDAL ANTI-INFLAMMATORY AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
BENZYDAMINE HCL
COMPOUND PRESCRIPTION
EPINEPHRINE HCL
PHENYLEPHRINE HCL
BRIMONIDINE TARTRATE
BETAXOLOL HCL
0.15 % ORAL RINSE
ORAL
ORAL
1 MG / ML TOPICAL SOLUTION
2.5 % OPHTHALMIC SOLUTION
0.2 % OPHTHALMIC SOLUTION
0.25 % (BASE) OPHTHALMIC SUSPENSION
000022390440000231042200002229777
00000999209
00000999109
00000155365
00000465763
0000226007700002246284000022430260000230542900002236876
00001908448
APO-BENZYDAMINENOVO-BENZYDAMINEPMS-BENZYDAMINE
COMPD-CHLORHEX. MOUTH RINSE (ANY CONCENTRATION, NOT 0.12%)
COMPD-CHLORHEX. MOUTH RINSE (ANY CONCENTRATION, NOT 12%)
ADRENALIN
MYDFRIN
APO-BRIMONIDINEPMS-BRIMONIDINERATIO-BRIMONIDINESANDOZ BRIMONIDINEALPHAGAN
BETOPTIC S
APXTEVPMS
XXX
XXX
ERF
ALC
APXPMSRPHSDZALL
ALC
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
MOUTHWASHES AND GARGLES
VASOCONSTRICTORS
ANTIGLAUCOMA AGENTS
ANTIGLAUCOMA AGENTS
52
52
52
52
:00
:00
:00
:00
52:28
52:32
52:40.04
52:40.08
0.0218 0.0218 0.0218
0.0000
0.0000
0.5961
1.0912
1.9869 1.9869 1.9869 1.9869 3.5480
2.4725
135 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$
$
$
$
$$$$$
$
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
(ALPHA-ADRENERGIC AGONISTS)
(BETA-ADRENERGIC AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
LEVOBUNOLOL HCL
TIMOLOL MALEATE
ACETAZOLAMIDE
BRINZOLAMIDE
DORZOLAMIDE HCL
METHAZOLAMIDE
0.25 % OPHTHALMIC SOLUTION
0.5 % OPHTHALMIC SOLUTION
0.25 % (BASE) OPHTHALMIC SOLUTION
0.5 % (BASE) OPHTHALMIC SOLUTION
0.25 % (BASE) OPHTHALMIC LONG ACTING GELLAN SOLUTION
0.5 % (BASE) OPHTHALMIC LONG ACTING GELLAN SOLUTION
250 MG ORAL TABLET
1 % OPHTHALMIC SUSPENSION
2 % (BASE) OPHTHALMIC SOLUTION
50 MG ORAL TABLET
0000203115900002241715
00002237991000020311670000224171600000637661
00000755826000008937730000208335300002166712
00000755834000020833450000216672000000451207
00002171880
00002171899
00000545015
00002238873
00002296055000023163070000221620500002269090
00002245882
RATIO-LEVOBUNOLOLSANDOZ LEVOBUNOLOL
PMS-LEVOBUNOLOLRATIO-LEVOBUNOLOLSANDOZ LEVOBUNOLOLBETAGAN
APO-TIMOPMYLAN-TIMOLOLPMS-TIMOLOLSANDOZ TIMOLOL MALEATE
APO-TIMOPPMS-TIMOLOLSANDOZ TIMOLOL MALEATETIMOPTIC
TIMOPTIC-XE
TIMOPTIC-XE
ACETAZOLAMIDE
AZOPT
APO-DORZOLAMIDESANDOZ DORZOLAMIDETRUSOPTTRUSOPT (PRESERVATIVE-FREE)
METHAZOLAMIDE
RPHSDZ
PMSRPHSDZALL
APXMYPPMSSDZ
APXPMSSDZMFC
MFC
MFC
AAP
ALC
APXSDZMFCMFC
AAP
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTIGLAUCOMA AGENTS
ANTIGLAUCOMA AGENTS
52
52
:00
:00
52:40.08
52:40.12
1.1760 1.1760
1.5550 1.5550 1.5550 3.5368
1.5500 1.5500 1.5500 1.5500
1.8600 1.8600 1.8600 3.6348
3.8799
4.6408
0.1330
3.5307
1.6875 1.6875 3.8585 3.8639
0.5178
136 EFFECTIVE APRIL 1, 2012
$$
$$$$
$$$$
$$$$
$
$
$
$
$$$$
$
(BETA-ADRENERGIC AGENTS)
(CARBONIC ANHYDRASE INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CARBACHOL
PILOCARPINE HCL
BIMATOPROST
LATANOPROST
TRAVOPROST
BRIMONIDINE TARTRATE/ TIMOLOL MALEATE
BRINZOLAMIDE/ TIMOLOL MALEATE
1.5 % OPHTHALMIC SOLUTION
3 % OPHTHALMIC SOLUTION
1 % OPHTHALMIC SOLUTION
2 % OPHTHALMIC SOLUTION
4 % OPHTHALMIC SOLUTION
4 % OPHTHALMIC GEL
OPHTHALMIC SOLUTION
0.005 % OPHTHALMIC SOLUTION
0.004 % OPHTHALMIC SOLUTION
0.2 % * 0.5 % (BASE) OPHTHALMIC SOLUTION
1 % * 0.5 % (BASE) OPHTHALMIC SUSPENSION
00000000655
00000000663
00000000841
00000000868
00000000884
00000575240
00002324997
00002296527000022547860000237304100002231493
00002318008
00002248347
00002331624
ISOPTO CARBACHOL
ISOPTO CARBACHOL
ISOPTO CARPINE
ISOPTO CARPINE
ISOPTO CARPINE
PILOPINE HS
LUMIGAN RC 0.01%
APO-LATANOPROSTCO LATANOPROSTGD-LATANOPROSTXALATAN
TRAVATAN Z
COMBIGAN
AZARGA
ALC
ALC
ALC
ALC
ALC
ALC
ALL
APXCOBGMDPFI
ALC
ALL
ALC
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTIGLAUCOMA AGENTS
ANTIGLAUCOMA AGENTS
ANTIGLAUCOMA AGENTS
52
52
52
:00
:00
:00
52:40.20
52:40.28
52:40.92
0.7576
0.9113
0.2303
0.2655
0.3000
2.8103
11.6272
5.3264 5.3264 5.3264
11.8364
11.9110
4.3129
4.6053
137 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$$$$
$
$
$
(MIOTICS)
(PROSTAGLANDIN ANALOGS)
(MISCELLANEOUS ANTIGLAUCOMA AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DORZOLAMIDE HCL/ TIMOLOL MALEATE
LATANOPROST/ TIMOLOL MALEATE
TRAVOPROST/ TIMOLOL MALEATE
APRACLONIDINE HCL
2 % (BASE) * 0.5 % (BASE) OPHTHALMIC SOLUTION
0.005 % * 0.5 % (BASE) OPHTHALMIC SOLUTION
0.004 % * 0.5 % (BASE) OPHTHALMIC SOLUTION
0.5 % OPHTHALMIC SOLUTION
0000225869200002299615000023443510000232052500002240113
00002246619
00002278251
00002076306
COSOPT PRESERVATIVE-FREEAPO-DORZO-TIMOPSANDOZ DORZOLAMIDE/ TIMOLOLTEVA-DORZOTIMOLCOSOPT
XALACOM
DUO TRAV
IOPIDINE
MFCAPXSDZTEVMFC
PFI
ALC
ALC
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
ANTIGLAUCOMA AGENTS
MISCELLANEOUS EENT DRUGS
52
52
:00
:00
52:40.92
52:92
2.3675 2.5569 2.5569 2.5569 5.8454
13.3948
13.4212
4.7858
138 EFFECTIVE APRIL 1, 2012
$$$$$
$
$
$
(MISCELLANEOUS ANTIGLAUCOMA AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RANIBIZUMAB
2.3 MG / VIAL INJECTION00002296810 LUCENTIS NOV
EYE, EAR, NOSE, AND THROAT (EENT) PREPARATIONS
MISCELLANEOUS EENT DRUGS
52:00
52:92
1693.1250
139 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
For this product - pricing has been established on a per vial basis.$
RESTRICTED BENEFIT - This product is a benefit when prescribed by a registered prescriber conditional to the following criteria.
"For the treatment of neovascular (wet) age-related macular degeneration (AMD) if all of the following circumstances apply to the eye to be treated:- The best corrected visual acuity (BCVA) is between 6/12 (20/40) and 6/96 (20/320)- There is active disease activity (choroidal neovascularization) and no permanent structural damage to the central fovea- The lesion size is less than or equal to 12 disc areas in greatest linear dimension- There is evidence of recent (< 3 months) presumed disease progression (blood vessel growth, as indicated by fluoroscein angiography, optical coherence tomography (OCT) or recent visual acuity changes)- No concurrent verteporfin PDT treatment- Injection will be by a qualified ophthalmologist with experience in intravitreal injections.
The interval between the doses should be no shorter than one month.
Treatment with ranibizumab should be continued only in people who maintain adequate response to therapy.
Ranibizumab should be discontinued if any one of the following occur:- Reduction in BCVA in the treated eye to less than 15 letters (absolute) on 2 consecutive visitsin the treated eye, attributed to AMD in the absence of other pathology,- Reduction in BCVA of 30 letters or more compared to either baseline and/or best recorded level since baseline as this may indicate either poor treatment effect or adverse event or both.- There is evidence of deterioration of the lesion morphology despite optimum treatment over three consecutive visits."
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

56:00 Gastrointestinal D
rugs
56:00
Gastrointestinal Drugs

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DIPHENOXYLATE HCL/ ATROPINE SULFATE
URSODIOL
LIPASE/ AMYLASE/ PROTEASE
2.5 MG * 0.025 MG ORAL TABLET
250 MG ORAL TABLET
500 MG ORAL TABLET
8,000 UNIT * 30,000 UNIT * 30,000 UNIT ORAL TABLET
16,000 UNIT * 60,000 UNIT * 60,000 UNIT ORAL TABLET
8,000 UNIT * 30,000 UNIT * 30,000 UNIT ORAL CAPSULE
4,000 UNIT * 12,000 UNIT * 12,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
4,500 UNIT * 20,000 UNIT * 25,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
8,000 UNIT * 30,000 UNIT * 30,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
10,000 UNIT * 30,000 UNIT * 30,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
10,000 UNIT * 33,200 UNIT * 37,500 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
12,000 UNIT * 39,000 UNIT * 39,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
16,000 UNIT * 48,000 UNIT * 48,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
20,000 UNIT * 55,000 UNIT * 55,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
20,000 UNIT * 65,000 UNIT * 65,000 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
25,000 UNIT * 74,000 UNIT * 62,500 UNIT ORAL CAPSULE (ENTERIC-COATED PELLET)
00000036323
0000227349700002238984
0000227350000002245894
00002230019
00002241933
00000263818
00000789445
00002203324
00000502790
00000789437
00002200104
00002045834
00000789429
00000821373
00002045869
00001985205
LOMOTIL
PMS-URSODIOL CURSO
PMS-URSODIOL CURSO DS
VIOKASE
VIOKASE 16
COTAZYM
PANCREASE MT 4
ULTRASE MS4 MICROSPHERES
COTAZYM ECS 8
PANCREASE MT 10
CREON 10 MINIMICROSPHERES
ULTRASE MT12 MINITABLETS
PANCREASE MT 16
COTAZYM ECS 20
ULTRASE MT20 MINITABLETS
CREON 25 MINIMICROSPHERES
PFI
PMSAXC
PMSAXC
AXC
AXC
ORG
JAI
AXC
ORG
JAI
ABB
AXC
JAI
ORG
AXC
ABB
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTIDIARRHEA AGENTS
CHOLELITHOLYTIC AGENTS
DIGESTANTS
56
56
56
:00
:00
:00
56:08
56:14
56:16
0.4784
0.8808 1.4729
1.6708 2.7937
0.2488
0.3817
0.1866
0.4897
0.2436
0.3368
1.2239
0.2723
0.4764
1.9580
0.8830
0.8255
0.8507
141 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$
$$
$
$
$
$
$
$
$
$
$
$
$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DIMENHYDRINATE
PROCHLORPERAZINE
DOLASETRON MESYLATE
GRANISETRON HCL
ONDANSETRON
10 MG / ML INJECTION
50 MG / ML INJECTION
5 MG ORAL TABLET
10 MG ORAL TABLET
5 MG / ML INJECTION
10 MG RECTAL SUPPOSITORY
100 MG ORAL TABLET
1 MG (BASE) ORAL TABLET
4 MG ORAL DISINTEGRATING TABLET
8 MG ORAL DISINTEGRATING TABLET
00000392731
00000392537
00000886440
00000886432
00000789747
00000789720
00002231379
0000230889400002185881
00002239372
00002239373
DIMENHYDRINATE I.V.
DIMENHYDRINATE I.M.
APO-PROCHLORAZINE
APO-PROCHLORAZINE
PROCHLORPERAZINE
SANDOZ PROCHLORPERAZINE
ANZEMET
GRANISETRONKYTRIL
ZOFRAN ODT
ZOFRAN ODT
SDZ
SDZ
APX
APX
SDZ
SDZ
SAV
AAPHLR
GSK
GSK
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTIEMETICS
ANTIEMETICS
56
56
:00
:00
56:22.08
56:22.20
0.3520
1.1500
0.1659
0.2025
1.0450
1.2500
31.3448
13.5000 19.3500
14.0707
21.4699
142 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$
$$
$
$
(ANTIHISTAMINES)
(5-HT3 RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ONDANSETRON HCL DIHYDRATE4 MG (BASE) ORAL TABLET
8 MG (BASE) ORAL TABLET
0.8 MG / ML (BASE) ORAL SOLUTION
2 MG / ML (BASE) INJECTION
2 MG / ML (BASE) INJECTION
0000228818400002296349000023136850000237173100002305259000022978680000226405600002306212000022786180000225818800002312247000022785290000227431000002213567
0000228819200002296357000023136930000237175800002305267000022978760000226406400002306220000022786260000225819600002312255000022785370000227432900002213575
0000229196700002229639
000022655240000227942800002271761
000022794360000226553200002271788
00002213745
APO-ONDANSETRONCO ONDANSETRONJAMP-ONDANSETRONMAR-ONDANSETRONMINT-ONDANSETRONMYLAN-ONDANSETRONNOVO-ONDANSETRONONDANSETRON-ODANPHL-ONDANSETRONPMS-ONDANSETRONRAN-ONDANSETRONRATIO-ONDANSETRONSANDOZ ONDANSETRONZOFRAN
APO-ONDANSETRONCO ONDANSETRONJAMP-ONDANSETRONMAR-ONDANSETRONMINT-ONDANSETRONMYLAN-ONDANSETRONNOVO-ONDANSETRONONDANSETRON-ODANPHL-ONDANSETRONPMS-ONDANSETRONRAN-ONDANSETRONRATIO-ONDANSETRONSANDOZ ONDANSETRONZOFRAN
ONDANSETRONZOFRAN
ONDANSETRON (PRESERVATIVE FREE)ONDANSETRON (UNPRESERVED)ONDANSETRON OMEGA (PRESERVATIVE FREE)
ONDANSETRON (PRESERVED)ONDANSETRON (WITH PRESERVATIVE)ONDANSETRON OMEGA (WITH PRESERVATIVE)ZOFRAN
APXCOBJPCMARMPIMYPTEVODNPHHPMSRANRPHSDZGSK
APXCOBJPCMARMPIMYPTEVODNPHHPMSRANRPHSDZGSK
AAPGSK
TEVSDZOMG
SDZTEVOMG
GSK
GASTROINTESTINAL DRUGS
ANTIEMETICS
56:00
56:22.20
7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450 7.5450
14.4028
11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 11.5166 21.9773
1.4614 2.1975
5.9429 5.9429 5.9429
5.9429 5.9429 5.9429
10.6124
143 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$$$$$$
$$$$$$$$$$$$$$
$$
$$$
$$$
$
(5-HT3 RECEPTOR ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
APREPITANT
APREPITANT/ APREPITANT
DOXYLAMINE SUCCINATE/ PYRIDOXINE HCL
NABILONE
CIMETIDINE
80 MG ORAL CAPSULE
80 MG * 125 MG ORAL CAPSULE
10 MG * 10 MG ORAL SUSTAINED-RELEASE TABLET
0.5 MG ORAL CAPSULE
1 MG ORAL CAPSULE
200 MG ORAL TABLET
300 MG ORAL TABLET
400 MG ORAL TABLET
600 MG ORAL TABLET
800 MG ORAL TABLET
00002298791
00002298813
00000609129
00002256193
00000548375
00000584215
00000487872000022274440000058241700000865818
00000600059000022274520000060367800000865826
00000600067000022274600000060368600000865834
0000074949400002227479
EMEND
EMEND TRI-PACK
DICLECTIN
CESAMET
CESAMET
APO-CIMETIDINE
APO-CIMETIDINEMYLAN-CIMETIDINENOVO-CIMETINENU-CIMET
APO-CIMETIDINEMYLAN-CIMETIDINENOVO-CIMETINENU-CIMET
APO-CIMETIDINEMYLAN-CIMETIDINENOVO-CIMETINENU-CIMET
APO-CIMETIDINEMYLAN-CIMETIDINE
MFC
MFC
DUI
VCL
VCL
APX
APXMYPTEVNXP
APXMYPTEVNXP
APXMYPTEVNXP
APXMYP
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTIEMETICS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
56
56
:00
:00
56:22.92
56:28.12
30.1800
30.1800
1.3406
3.3353
6.6704
0.0860
0.0860 0.0860 0.0860 0.0860
0.1350 0.1350 0.1350 0.1350
0.1720 0.1720 0.1720 0.1720
0.2530 0.2530
144 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$$$$
$$$$
$$$$
$$
RESTRICTED BENEFIT - This drug product must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates).
RESTRICTED BENEFIT - This drug product must be prescribed by the Directors of Alberta Health Services - Cancer Care "Cancer Centres" (or their designates).
(MISCELLANEOUS ANTIEMETICS)
(HISTAMINE H2-ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
FAMOTIDINE
NIZATIDINE
20 MG ORAL TABLET
40 MG ORAL TABLET
150 MG ORAL CAPSULE
300 MG ORAL CAPSULE
00001953842000023739200000235110200002196018000020221330000202419500000710121
00001953834000023739390000235111000002196026000020221410000202420900000710113
00002220156000022404570000217771400000778338
00002220164000022404580000217772200000778346
APO-FAMOTIDINEAVA-FAMOTIDINEFAMOTIDINEMYLAN-FAMOTIDINENOVO-FAMOTIDINENU-FAMOTIDINEPEPCID
APO-FAMOTIDINEAVA-FAMOTIDINEFAMOTIDINEMYLAN-FAMOTIDINENOVO-FAMOTIDINENU-FAMOTIDINEPEPCID
APO-NIZATIDINENOVO-NIZATIDINEPMS-NIZATIDINEAXID
APO-NIZATIDINENOVO-NIZATIDINEPMS-NIZATIDINEAXID
APXAVASNSMYPTEVNXPMFC
APXAVASNSMYPTEVNXPMFC
APXTEVPMSMMT
APXTEVPMSMMT
GASTROINTESTINAL DRUGS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
56:00
56:28.12
0.5896 0.5896 0.5896 0.5896 0.5896 0.5896 1.1092
1.0612 1.0612 1.0612 1.0612 1.0612 1.0612 2.0254
0.5052 0.5052 0.5052 1.0189
0.9154 0.9154 0.9154 1.8135
145 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$
$$$$$$$
$$$$
$$$$
(HISTAMINE H2-ANTAGONISTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
RANITIDINE HCL
MISOPROSTOL
150 MG (BASE) ORAL TABLET
300 MG (BASE) ORAL TABLET
15 MG / ML (BASE) ORAL SOLUTION
25 MG / ML (BASE) INJECTION
100 MCG ORAL TABLET
200 MCG ORAL TABLET
00000733059000022485700000236737800002207761000008285640000086573700002245782000022424530000233648000002353016000008288230000224322900002212331
000007330670000224857100002367386000022077880000082855600000865745000022457830000224245400002336502000023530240000224323000002212358
0000228083300002242940
0000225671100002212366
00002244022
00002244023
APO-RANITIDINECO RANITIDINEMYL-RANITIDINEMYLAN-RANITIDINENOVO-RANIDINENU-RANITPHL-RANITIDINEPMS-RANITIDINERAN-RANITIDINERANITIDINERATIO-RANITIDINESANDOZ RANITIDINEZANTAC
APO-RANITIDINECO RANITIDINEMYL-RANITIDINEMYLAN-RANITIDINENOVO-RANIDINENU-RANITPHL-RANITIDINEPMS-RANITIDINERAN-RANITIDINERANITIDINESANDOZ RANITIDINEZANTAC
APO-RANITIDINENOVO-RANIDINE
RANITIDINEZANTAC
MISOPROSTOL
MISOPROSTOL
APXCOBMYPMYPTEVNXPPHHPMSRANSNSRPHSDZGSK
APXCOBMYPMYPTEVNXPPHHPMSRANSNSSDZGSK
APXTEV
SDZGSK
AAP
AAP
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
56
56
:00
:00
56:28.12
56:28.28
0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800 0.1800
0.3600 0.3600 0.3600 0.3600 0.3600 0.3600 0.3600 0.3600 0.3600 0.3600 0.3600 0.3600
0.1174 0.1174
1.3310 1.5050
0.2778
0.4626
146 EFFECTIVE APRIL 1, 2012
$$$$$$$$$$$$$
$$$$$$$$$$$$
$$
$$
$
$
(HISTAMINE H2-ANTAGONISTS)
(PROSTAGLANDINS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
SUCRALFATE
LANSOPRAZOLE
LANSOPRAZOLE/ AMOXICILLIN TRIHYDRATE/ CLARITHROMYCIN
1 G ORAL TABLET
200 MG / ML ORAL SUSPENSION
15 MG ORAL DELAYED RELEASE CAPSULE
30 MG ORAL DELAYED RELEASE CAPSULE
30 MG * 500 MG (BASE) * 500 MG ORAL TABLET/CAPSULE
00002125250000020457020000213482900002100622
00002103567
0000229381100002357682000023538300000228051500002165503
0000229383800002357690000023538490000228052300002165511
00002238525
APO-SUCRALFATENOVO-SUCRALATENU-SUCRALFATESULCRATE
SULCRATE SUSPENSION PLUS
APO-LANSOPRAZOLELANSOPRAZOLEMYLAN-LANSOPRAZOLENOVO-LANSOPRAZOLEPREVACID
APO-LANSOPRAZOLELANSOPRAZOLEMYLAN-LANSOPRAZOLENOVO-LANSOPRAZOLEPREVACID
HP-PAC ( KIT )
APXTEVNXPAXC
AXC
APXSNSMYPTEVABB
APXSNSMYPTEVABB
ABB
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
56
56
:00
:00
56:28.32
56:28.36
0.2942 0.2942 0.2942 0.6138
0.1115
1.1200 1.1200 1.1200 1.1200 2.0000
1.1200 1.1200 1.1200 1.1200 2.0000
84.2700
147 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$
$
$$$$$
$$$$$
$
Please note: For individuals who require alternative administration (capsules to be opened and intact delayed release granules to be sprinkled on applesauce and swallowed immediately or mixed in water or apple juice and administered through a nasogastric tube) application for coverage for the Prevacid brand may be made using the Drug Special Authorization Request Form (ABC 20061), indicating a requirement for alternative administration.
(PROTECTANTS)
(PROTON-PUMP INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
OMEPRAZOLE
PANTOPRAZOLE
10 MG ORAL CAPSULE/SUSTAINED RELEASE TABLET
20 MG ORAL CAPSULE/SUSTAINED RELEASE TABLET
40 MG ORAL ENTERIC-COATED TABLET
0000232942500002296438
00002230737
000022450580000232943300002295415
0000234869100002320851
00002310260
00002374870
00002260867
00002296446
0000084650300002190915
000022672330000229292000002363429000023004860000229958500002285487000023098660000237080800002307871000023050460000230108300002229453
MYLAN-OMEPRAZOLE (CAPSULE)SANDOZ OMEPRAZOLE (SUSTAINED-RELEASE CAPSULE)LOSEC (SUSTAINED-RELEASE TABLET)
APO-OMEPRAZOLE (CAPSULE)MYLAN-OMEPRAZOLE (CAPSULE)NOVO-OMEPRAZOLE (DELAYED RELEASE TABLET)OMEPRAZOLE (CAPSULE)PMS-OMEPRAZOLE (SUSTAINED-RELEASE CAPSULE)PMS-OMEPRAZOLE DR (DELAYED RELEASETABLET)RAN-OMEPRAZOLE (DELAYED RELEASE TABLET)RATIO-OMEPRAZOLE (SUSTAINED-RELEASE TABLET)SANDOZ OMEPRAZOLE (SUSTAINED-RELEASE CAPSULE)LOSEC (SUSTAINED-RELEASE CAPSULE)LOSEC (SUSTAINED-RELEASE TABLET)
TECTAAPO-PANTOPRAZOLEAVA-PANTOPRAZOLECO PANTOPRAZOLEMYLAN-PANTOPRAZOLENOVO-PANTOPRAZOLEPANTOPRAZOLEPANTOPRAZOLEPMS-PANTOPRAZOLERAN-PANTOPRAZOLESANDOZ PANTOPRAZOLEPANTOLOC
MYPSDZ
AZC
APXMYPTEV
SNSPMS
PMS
RAN
RPH
SDZ
AZCAZC
NYCAPXAVACOBMYPTEVMELSNSPMSRANSDZNYC
GASTROINTESTINAL DRUGS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
56:00
56:28.36
0.8167 0.8167
1.9565
1.1000 1.1000 1.1000
1.1000 1.1000
1.1000
1.1000
1.1000
1.1000
1.1825 2.4585
0.8062 1.2135 1.2135 1.2135 1.2135 1.2135 1.2135 1.2135 1.2135 1.2135 1.2135 2.2363
148 EFFECTIVE APRIL 1, 2012
$$
$
$$$
$$
$
$
$
$
$$
$$$$$$$$$$$$
(PROTON-PUMP INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
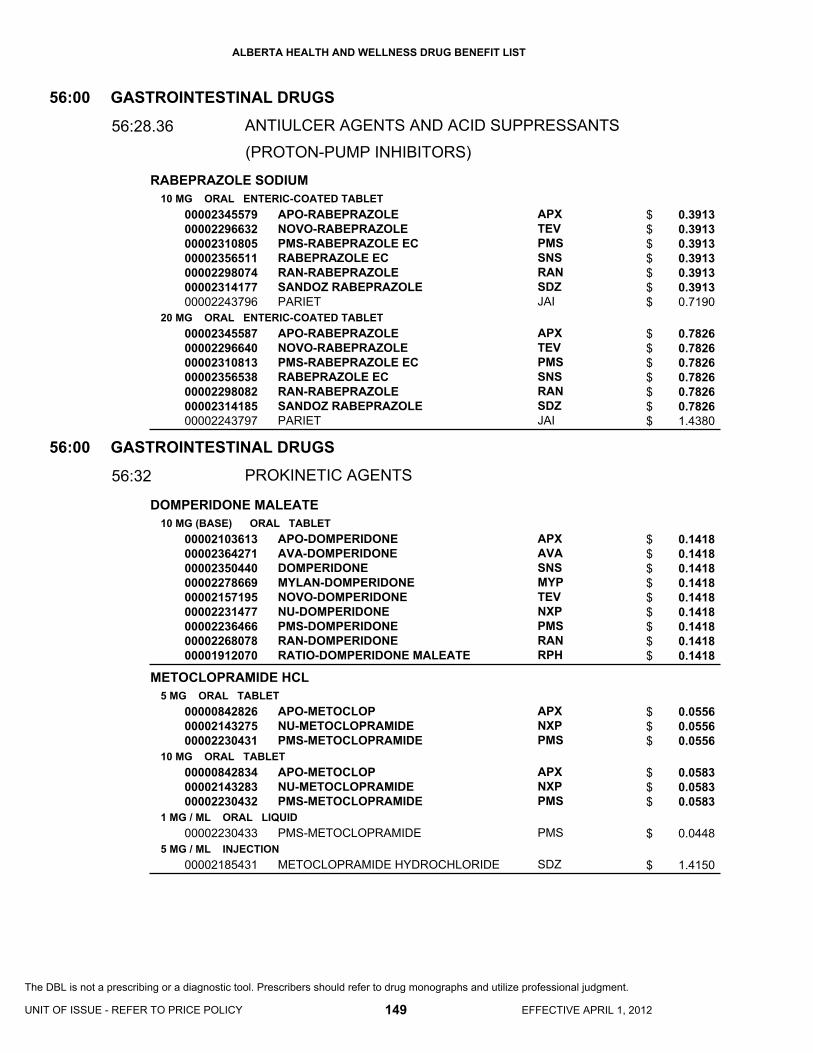
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
RABEPRAZOLE SODIUM
DOMPERIDONE MALEATE
METOCLOPRAMIDE HCL
10 MG ORAL ENTERIC-COATED TABLET
20 MG ORAL ENTERIC-COATED TABLET
10 MG (BASE) ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
1 MG / ML ORAL LIQUID
5 MG / ML INJECTION
00002345579000022966320000231080500002356511000022980740000231417700002243796
00002345587000022966400000231081300002356538000022980820000231418500002243797
000021036130000236427100002350440000022786690000215719500002231477000022364660000226807800001912070
000008428260000214327500002230431
000008428340000214328300002230432
00002230433
00002185431
APO-RABEPRAZOLENOVO-RABEPRAZOLEPMS-RABEPRAZOLE ECRABEPRAZOLE ECRAN-RABEPRAZOLESANDOZ RABEPRAZOLEPARIET
APO-RABEPRAZOLENOVO-RABEPRAZOLEPMS-RABEPRAZOLE ECRABEPRAZOLE ECRAN-RABEPRAZOLESANDOZ RABEPRAZOLEPARIET
APO-DOMPERIDONEAVA-DOMPERIDONEDOMPERIDONEMYLAN-DOMPERIDONENOVO-DOMPERIDONENU-DOMPERIDONEPMS-DOMPERIDONERAN-DOMPERIDONERATIO-DOMPERIDONE MALEATE
APO-METOCLOPNU-METOCLOPRAMIDEPMS-METOCLOPRAMIDE
APO-METOCLOPNU-METOCLOPRAMIDEPMS-METOCLOPRAMIDE
PMS-METOCLOPRAMIDE
METOCLOPRAMIDE HYDROCHLORIDE
APXTEVPMSSNSRANSDZJAI
APXTEVPMSSNSRANSDZJAI
APXAVASNSMYPTEVNXPPMSRANRPH
APXNXPPMS
APXNXPPMS
PMS
SDZ
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTIULCER AGENTS AND ACID SUPPRESSANTS
PROKINETIC AGENTS
56
56
:00
:00
56:28.36
56:32
0.3913 0.3913 0.3913 0.3913 0.3913 0.3913 0.7190
0.7826 0.7826 0.7826 0.7826 0.7826 0.7826 1.4380
0.1418 0.1418 0.1418 0.1418 0.1418 0.1418 0.1418 0.1418 0.1418
0.0556 0.0556 0.0556
0.0583 0.0583 0.0583
0.0448
1.4150
149 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$
$$$$$$$
$$$$$$$$$
$$$
$$$
$
$
(PROTON-PUMP INHIBITORS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
MESALAZINE
OLSALAZINE SODIUM
PINAVERIUM BROMIDE
TRIMEBUTINE MALEATE
500 MG ORAL SUSTAINED-RELEASE TABLET
400 MG ORAL ENTERIC-COATED TABLET
500 MG ORAL ENTERIC-COATED TABLET
800 MG ORAL ENTERIC-COATED TABLET
500 MG RECTAL SUPPOSITORY
1 G RECTAL SUPPOSITORY
1,000 MG RECTAL SUPPOSITORY
1 G / ENM RECTAL ENEMA
2 G / ENM RECTAL ENEMA
4 G / ENM RECTAL ENEMA
250 MG ORAL CAPSULE
50 MG ORAL TABLET
100 MG ORAL TABLET
100 MG ORAL TABLET
200 MG ORAL TABLET
00002099683
000023514630000217192900001997580
0000211278700001914030
00002267217
00002112760
00002153564
00002242146
00002153521
00002112795
0000215355600002112809
00002063808
00001950592
00002230684
00002245663
0000224566400000803499
PENTASA
5-AMINOSALICYLIC ACIDNOVO-5 ASAASACOL
SALOFALKMESASAL
ASACOL 800
SALOFALK
PENTASA
SALOFALK
PENTASA (1G/100ML)
SALOFALK (2G/60G)
PENTASA (4G/100 ML)SALOFALK (4G/60G)
DIPENTUM
DICETEL
DICETEL
TRIMEBUTINE
TRIMEBUTINEMODULON
FEI
SNSTEVWCC
AXCGSK
WCC
AXC
FEI
AXC
FEI
AXC
FEIAXC
UCB
ABB
ABB
AAP
AAPAXC
GASTROINTESTINAL DRUGS
GASTROINTESTINAL DRUGS
ANTI-INFLAMMATORY AGENTS
MISCELLANEOUS GI DRUGS
56
56
:00
:00
56:36
56:92
0.5987
0.3972 0.3972 0.5848
0.5778 0.6745
1.1368
1.2773
1.7200
1.8761
3.9775
4.1150
4.7945 6.9878
0.5698
0.3533
0.6160
0.2892
0.5235 0.7119
150 EFFECTIVE APRIL 1, 2012
$
$$$
$$
$
$
$
$
$
$
$$
$
$
$
$
$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

60:00 Gold C
ompounds
60:00
Gold Compounds
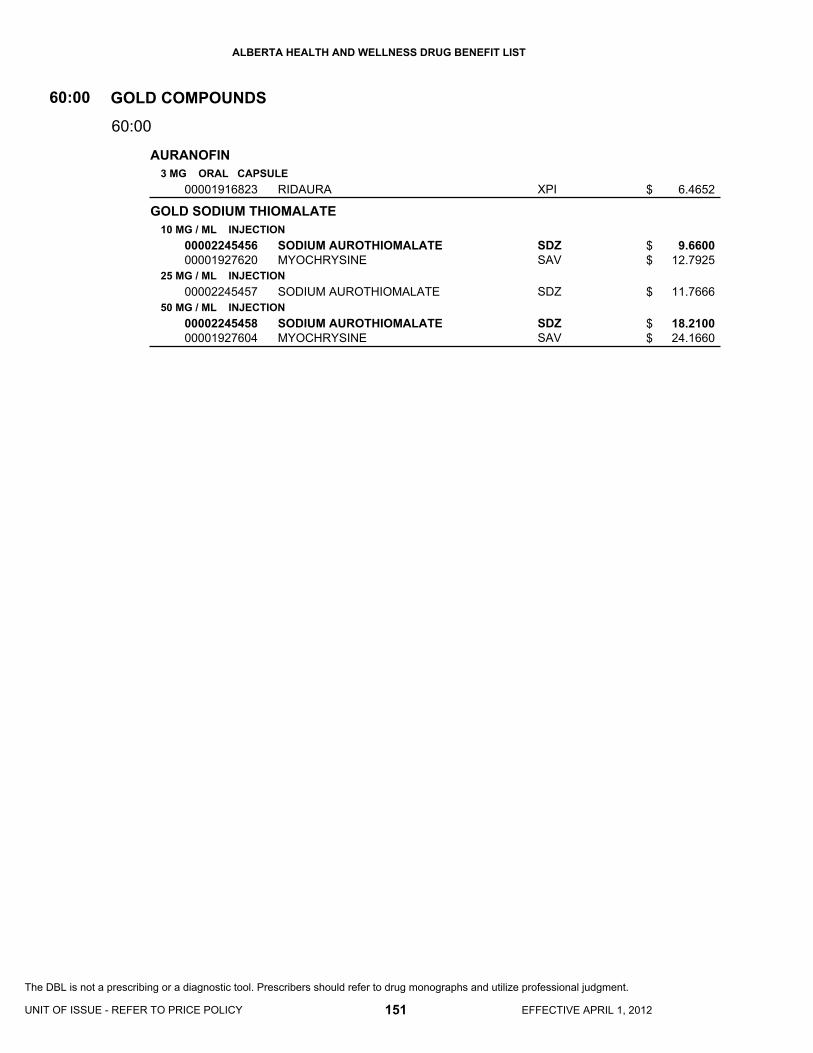
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
AURANOFIN
GOLD SODIUM THIOMALATE
3 MG ORAL CAPSULE
10 MG / ML INJECTION
25 MG / ML INJECTION
50 MG / ML INJECTION
00001916823
0000224545600001927620
00002245457
0000224545800001927604
RIDAURA
SODIUM AUROTHIOMALATEMYOCHRYSINE
SODIUM AUROTHIOMALATE
SODIUM AUROTHIOMALATEMYOCHRYSINE
XPI
SDZSAV
SDZ
SDZSAV
GOLD COMPOUNDS60:00
60:00
6.4652
9.6600 12.7925
11.7666
18.2100 24.1660
151 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$
$
$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

64:00 Heavy M
etal Antagonists
64:00
Heavy Metal Antagonists

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DEFEROXAMINE MESYLATE
PENICILLAMINE
500 MG / VIAL INJECTION
2 G / VIAL INJECTION
250 MG ORAL CAPSULE
000022416000000224205500001981242
000022470220000224345000001981250
00000016055
DESFERRIOXAMINE MESILATEPMS-DEFEROXAMINEDESFERAL
DESFERRIOXAMINE MESILATEPMS-DEFEROXAMINEDESFERAL
CUPRIMINE
HSPPMSNOV
HSPPMSNOV
ATP
HEAVY METAL ANTAGONISTS64:00
64:00
8.0535 8.0535
15.0352
32.3514 32.3514 60.3935
3.8450
153 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$$$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

68:00 Horm
ones and Synthetic Substitutes
68:00
Hormones and Synthetic Substitutes

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
COMPOUND PRESCRIPTION
BECLOMETHASONE DIPROPIONATE
BETAMETHASONE SODIUM PHOSPHATE/ BETAMETHASONE ACETATE
BUDESONIDE
CICLESONIDE
CORTISONE ACETATE
50 MCG / DOSE METERED DOSE AEROSOL
100 MCG / DOSE METERED DOSE AEROSOL
3 MG / ML (BASE) * 3 MG / ML INJECTION
100 MCG / DOSE METERED INHALATION POWDER
200 MCG / DOSE METERED INHALATION POWDER
400 MCG / DOSE METERED INHALATION POWDER
0.125 MG / ML INHALATION SUSPENSION
0.25 MG / ML INHALATION SUSPENSION
0.5 MG / ML INHALATION SUSPENSION
100 MCG / DOSE METERED DOSE AEROSOL
200 MCG / DOSE METERED DOSE AEROSOL
25 MG ORAL TABLET
00000999111
00000999212
00002242029
00002242030
00000028096
00000852074
00000851752
00000851760
00002229099
00001978918
00001978926
00002285606
00002285614
00000280437
COMPOUND HORMONES (ESTROGEN PROGEST TESTOSTERONE)
COMPOUND HORMONES (ESTROGEN PROGEST TESTOSTERONE)
QVAR CFC-FREE
QVAR CFC-FREE
CELESTONE SOLUSPAN
PULMICORT TURBUHALER
PULMICORT TURBUHALER
PULMICORT TURBUHALER
PULMICORT NEBUAMP
PULMICORT NEBUAMP
PULMICORT NEBUAMP
ALVESCO
ALVESCO
CORTISONE ACETATE
XXX
XXX
MEP
MEP
MFC
AZC
AZC
AZC
AZC
AZC
AZC
NYC
NYC
VCL
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
ADRENALS
68
68
:00
:00
68:00
68:04
0.0000
0.0000
0.1574
0.3148
10.3140
0.1661
0.3395
0.5986
0.2304
0.4606
0.9213
0.3991
0.6598
0.3440
155 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$
$
$
$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DEXAMETHASONE
DEXAMETHASONE SODIUM PHOSPHATE
FLUDROCORTISONE ACETATE
FLUTICASONE PROPIONATE
HYDROCORTISONE
HYDROCORTISONE SODIUM SUCCINATE
0.5 MG ORAL TABLET
0.75 MG ORAL TABLET
2 MG ORAL TABLET
4 MG ORAL TABLET
4 MG / ML (BASE) INJECTION
10 MG / ML (BASE) INJECTION
0.1 MG ORAL TABLET
50 MCG / DOSE METERED DOSE AEROSOL
125 MCG / DOSE METERED DOSE AEROSOL
250 MCG / DOSE METERED DOSE AEROSOL
250 MCG / DOSE METERED INHALATION POWDER
500 MCG / DOSE METERED INHALATION POWDER
10 MG ORAL TABLET
20 MG ORAL TABLET
100 MG / VIAL (BASE) INJECTION
250 MG / VIAL (BASE) INJECTION
500 MG / VIAL (BASE) INJECTION
000022610810000196497600002240684
00001964968
00002279363
00002250055000019640700000224068700000489158
0000066422700001977547
0000078390000000874582
00002086026
00002244291
00002244292
00002244293
00002237246
00002237247
00000030910
00000030929
0000087252000000030600
0000087253900000030619
0000087861800000030627
APO-DEXAMETHASONEPMS-DEXAMETHASONERATIO-DEXAMETHASONE
PMS-DEXAMETHASONE
PMS-DEXAMETHASONE
APO-DEXAMETHASONEPMS-DEXAMETHASONERATIO-DEXAMETHASONEDEXASONE
DEXAMETHASONE SODIUM PHOSPHATEDEXAMETHASONE SODIUM PHOSPHATE
PMS-DEXAMETHASONE SODIUM PHOSPDEXAMETHASONE SODIUM PHOSPHATE
FLORINEF
FLOVENT HFA
FLOVENT HFA
FLOVENT HFA
FLOVENT DISKUS
FLOVENT DISKUS
CORTEF
CORTEF
HYDROCORTISONE SOD. SUCCINATESOLU-CORTEF
HYDROCORTISONE SOD. SUCCINATESOLU-CORTEF
HYDROCORTISONE SOD. SUCCINATESOLU-CORTEF
APXPMSRPH
PMS
PMS
APXPMSRPHVCL
SDZCYT
PMSSDZ
PAL
GSK
GSK
GSK
GSK
GSK
PFI
PFI
TEVPFI
TEVPFI
TEVPFI
HORMONES AND SYNTHETIC SUBSTITUTES
ADRENALS
68:00
68:04
0.1751 0.1751 0.1751
0.4728
0.4389
0.7673 0.7673 0.7673 0.8468
1.6900 1.6900
1.2830 4.5600
0.2468
0.2144
0.3698
0.7396
0.7396
1.4789
0.1642
0.2963
2.0000 3.8810
3.4000 6.7340
5.1000 10.1780
156 EFFECTIVE APRIL 1, 2012
$$$
$
$
$$$$
$$
$$
$
$
$
$
$
$
$
$
$$
$$
$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
HYDROCORTISONE SODIUM SUCCINATE
METHYLPREDNISOLONE
METHYLPREDNISOLONE ACETATE
METHYLPREDNISOLONE ACETATE/ LIDOCAINE HCL
METHYLPREDNISOLONE SODIUM SUCCINATE
PREDNISOLONE SODIUM PHOSPHATE
1 G / VIAL (BASE) INJECTION
4 MG ORAL TABLET
16 MG ORAL TABLET
20 MG / ML INJECTION
40 MG / ML INJECTION
80 MG / ML INJECTION
40 MG / ML INJECTION
80 MG / ML INJECTION
40 MG / ML * 10 MG / ML INJECTION
40 MG / VIAL (BASE) INJECTION
125 MG / VIAL (BASE) INJECTION
500 MG / VIAL (BASE) INJECTION
1 G / VIAL (BASE) INJECTION
1 MG / ML (BASE) ORAL LIQUID
0000087862600000030635
00000030988
00000036129
00001934325
0000224540000000030759
0000224540600000030767
0000224540700001934333
0000224540800001934341
00000260428
0000223189300002063719
0000223189400002063727
000022318950000003067800002063700
000022412290000003613700002063697
0000224553200002230619
HYDROCORTISONE SOD. SUCCINATESOLU-CORTEF
MEDROL
MEDROL
DEPO-MEDROL
METHYLPREDNISOLONE ACETATEDEPO-MEDROL
METHYLPREDNISOLONE ACETATEDEPO-MEDROL
METHYLPREDNISOLONE ACETATE (P)DEPO-MEDROL (PRESERVED)
METHYLPREDNISOLONE ACETATE (P)DEPO-MEDROL (PRESERVED)
DEPO-MEDROL WITH LIDOCAINE
METHYLPREDNISOLONE SOD SUCCIN.SOLU-MEDROL ACT-O-VIAL (WITH PRESERVATIVE)
METHYLPREDNISOLONE SOD SUCCIN.SOLU-MEDROL ACT-O-VIAL (WITH PRESERVATIVE)
METHYLPREDNISOLONE SOD SUCCIN.SOLU-MEDROLSOLU-MEDROL ACT-O-VIAL (WITH PRESERVATIVE)
METHYLPREDNISOLONE SOD SUCCIN.SOLU-MEDROLSOLU-MEDROL ACT-O-VIAL (WITH PRESERVATIVE)
PMS-PREDNISOLONEPEDIAPRED
TEVPFI
PFI
PFI
PFI
SDZPFI
SDZPFI
SDZPFI
SDZPFI
PFI
TEVPFI
TEVPFI
TEVPFIPFI
TEVPFIPFI
PMSSAV
HORMONES AND SYNTHETIC SUBSTITUTES
ADRENALS
68:00
68:04
8.6000 17.0555
0.3713
1.0701
2.5585
4.7250 5.7405
9.0300 11.0964
4.5150 5.5482
6.9900 8.4882
6.4928
3.6000 6.5263
8.5000 15.4939
18.6000 38.0670 38.8312
31.0000 58.3510 59.5224
0.0863 0.1365
157 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$
$
$$
$$
$$
$$
$
$$
$$
$$$
$$$
$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PREDNISONE
TRIAMCINOLONE ACETONIDE
DANAZOL
TESTOSTERONE CYPIONATE
TESTOSTERONE ENANTHATE
DESOGESTREL/ ETHINYL ESTRADIOL
1 MG ORAL TABLET
5 MG ORAL TABLET
50 MG ORAL TABLET
10 MG / ML INJECTION
40 MG / ML INJECTION
50 MG ORAL CAPSULE
100 MG ORAL CAPSULE
200 MG ORAL CAPSULE
100 MG / ML INJECTION
200 MG / ML INJECTION
0.15 MG * 0.03 MG ORAL TABLET
0.15 MG * 0.03 MG ORAL TABLET
0000059819400000271373
00000312770
00000550957
0000222954000001999761
000019775630000222955000001999869
00002018144
00002018152
00002018160
0000224606300000030783
00000029246
0000231719200002042487
000023172060000204247900002042533
APO-PREDNISONEWINPRED
APO-PREDNISONE
APO-PREDNISONE
TRIAMCINOLONE ACETONIDEKENALOG-10
TRIAMCINOLONE ACETONIDE USPTRIAMCINOLONE ACETONIDEKENALOG-40
CYCLOMEN
CYCLOMEN
CYCLOMEN
TESTOSTERONE CYPIONATEDEPO-TESTOSTERONE CYPIONATE
DELATESTRYL
APRI 21MARVELON (21 DAY)
APRI 28MARVELON (28 DAY)ORTHO-CEPT (28 DAY)
APXVCL
APX
APX
SDZWSD
CYTSDZWSD
SAV
SAV
SAV
SDZPFI
VCL
BARMFC
BARMFCJAI
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
ADRENALS
ANDROGENS
CONTRACEPTIVES
68
68
68
:00
:00
:00
68:04
68:08
68:12
0.1072 0.1113
0.0401
0.1735
2.6760 3.2423
5.5000 6.0000 7.5320
0.9726
1.4432
2.3062
2.3580 2.9000
10.2663
0.5436 0.6586
0.4077 0.4939 0.6555
158 EFFECTIVE APRIL 1, 2012
$$
$
$
$$
$$$
$
$
$
$$
$
$$
$$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DESOGESTREL/ ETHINYL ESTRADIOL/ DESOGESTREL/ ETHINYL ESTRADIOL/ DESOGESTREL/ ETHINYL ESTRADIOL
DROSPIRENONE/ ETHINYL ESTRADIOL
ETHYNODIOL DIACETATE/ ETHINYL ESTRADIOL
LEVONORGESTREL
LEVONORGESTREL/ ETHINYL ESTRADIOL
LEVONORGESTREL/ ETHINYL ESTRADIOL/ LEVONORGESTREL/ETHINYL ESTRADIOL/ LEVONORGESTREL/ ETHINYL ESTRADIOL
NORETHINDRONE
NORETHINDRONE ACETATE/ ETHINYL ESTRADIOL
0.1 MG * 0.025 MG * 0.125 MG * 0.025 MG * 0.15 MG * 0.025 MG ORAL TABLET
3 MG * 0.03 MG ORAL TABLET
2 MG * 30 MCG ORAL TABLET
0.75 MG ORAL TABLET
52 MG INTRAUTERINE INSERT
100 MCG * 20 MCG ORAL TABLET
150 MCG * 30 MCG ORAL TABLET
100 MCG * 20 MCG ORAL TABLET
150 MCG * 30 MCG ORAL TABLET
50 MCG * 30 MCG * 75 MCG * 40 MCG * 125 MCG * 30 MCG ORAL TABLET
0.35 MG ORAL TABLET
1 MG * 20 MCG ORAL TABLET
1.5 MG * 0.03 MG ORAL TABLET
0000225723800002272903
0000226173100002261723
0000047152600000469327
00002241674
00002243005
0000229853800002236974
0000229594600002042320
0000229854600002236975
0000229595400002042339
0000070750300000707600
00000037605
0000034383800000315966
0000035302700000297143
LINESSA 28LINESSA 21
YASMIN 28YASMIN 21
DEMULEN 30 (28 DAY)DEMULEN 30 (21 DAY)
PLAN B
MIRENA SYSTEM
AVIANE 21ALESSE (21 DAY)
PORTIA 21MIN-OVRAL (21 DAY)
AVIANE 28ALESSE (28 DAY)
PORTIA 28MIN-OVRAL (28 DAY)
TRIQUILAR (28 DAY)TRIQUILAR (21 DAY)
MICRONOR (28 DAY)
MINESTRIN 1/20 (28 DAY)MINESTRIN 1/20 (21 DAY)
LOESTRIN 1.5/30 (28 DAY)LOESTRIN 1.5/30 (21 DAY)
MFCMFC
BAIBAI
PFIPFI
DUR
BHP
BARWAY
BARWAY
BARWAY
BARWAY
BHPBHP
JAI
PALPAL
PALPAL
HORMONES AND SYNTHETIC SUBSTITUTES
CONTRACEPTIVES
68:00
68:12
0.4678 0.6238
0.4546 0.6063
0.5087 0.6340
8.6000
354.3308
0.4636 0.7556
0.4636 0.7556
0.3477 0.5666
0.3477 0.5666
0.5629 0.7505
0.6555
0.4653 0.6205
0.4653 0.6205
159 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$
$$
$
$
$$
$$
$$
$$
$$
$
$$
$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
NORETHINDRONE/ ETHINYL ESTRADIOL
NORETHINDRONE/ ETHINYL ESTRADIOL/ NORETHINDRONE/ ETHINYL ESTRADIOL
NORETHINDRONE/ ETHINYL ESTRADIOL/ NORETHINDRONE/ ETHINYL ESTRADIOL/ NORETHINDRONE/ ETHINYL ESTRADIOL
NORGESTIMATE/ ETHINYL ESTRADIOL
NORGESTIMATE/ ETHINYL ESTRADIOL/ NORGESTIMATE/ ETHINYL ESTRADIOL/ NORGESTIMATE/ ETHINYL ESTRADIOL
CONJUGATED ESTROGENS
0.5 MG * 0.035 MG ORAL TABLET
1 MG * 0.035 MG ORAL TABLET
0.5 MG * 0.035 MG * 1 MG * 0.035 MG ORAL TABLET
0.5 MG * 0.035 MG * 0.75 MG * 0.035 MG * 1 MG * 0.035 MG ORAL TABLET
0.25 MG * 0.035 MG ORAL TABLET
0.18 MG * 0.025 MG * 0.215 MG * 0.025 MG * 0.25 MG * 0.025 MG ORAL TABLET
0.18 MG * 0.035 MG * 0.215 MG * 0.035 MG * 0.25 MG * 0.035 MG ORAL TABLET
0.3 MG ORAL TABLET
0.625 MG ORAL TABLET
1.25 MG ORAL TABLET
0.625 MG / G VAGINAL CREAM
00002187094000021870860000034073100000317047
000021992970000219750200002189062000021890540000037283800000372846
0000218711600002187108
0000060296500000602957
0000199287200001968440
0000225858700002258560
0000202942100002028700
00002043394
0000026547000002043408
00002043424
00002043440
BREVICON 0.5/35 (28 DAY)BREVICON 0.5/35 (21 DAY)ORTHO 0.5/35 (28 DAY)ORTHO 0.5/35 (21 DAY)
SELECT 1/35 (28 DAY)SELECT 1/35 (21 DAY)BREVICON 1/35 (28 DAY)BREVICON 1/35 (21 DAY)ORTHO 1/35 (28 DAY)ORTHO 1/35 (21 DAY)
SYNPHASIC (28 DAY)SYNPHASIC (21 DAY)
ORTHO 7/7/7 (28 DAY)ORTHO 7/7/7 (21 DAY)
CYCLEN (28 DAY)CYCLEN (21 DAY)
TRI-CYCLEN LO 28TRI-CYCLEN LO 21
TRI-CYCLEN (28 DAY)TRI-CYCLEN (21 DAY)
PREMARIN
C.E.S.PREMARIN
PREMARIN
PREMARIN
PFIPFIJAIJAI
PFIPFIPFIPFIJAIJAI
PFIPFI
JAIJAI
JAIJAI
JAIJAI
JAIJAI
WAY
VCLWAY
WAY
WAY
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
CONTRACEPTIVES
ESTROGENS AND ANTIESTROGENS
68
68
:00
:00
68:12
68:16.04
0.4358 0.5810 0.6555 0.8741
0.2942 0.3925 0.4358 0.5810 0.6555 0.8741
0.4004 0.5340
0.6555 0.8741
0.6555 0.8741
0.4712 0.6281
0.6555 0.8741
0.3117
0.1090 0.3117
0.3117
0.6740
160 EFFECTIVE APRIL 1, 2012
$$$$
$$$$$$
$$
$$
$$
$$
$$
$
$$
$
$
(ESTROGENS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ESTRADIOL-17B
NORETHINDRONE ACETATE/ ESTRADIOL-17B
0.5 MG ORAL TABLET
1 MG ORAL TABLET
2 MG ORAL TABLET
0.06 % TRANSDERMAL GEL
25 MCG/DAY TRANSDERMAL PATCH
37.5 MCG/DAY TRANSDERMAL PATCH
50 MCG/DAY TRANSDERMAL PATCH
75 MCG/DAY TRANSDERMAL PATCH
100 MCG/DAY TRANSDERMAL PATCH
10 MCG VAGINAL TABLET
25 MCG VAGINAL TABLET
2 MG VAGINAL SLOW-RELEASE RING
140 MCG/DAY * 50 MCG/DAY TRANSDERMAL PATCH
250 MCG/DAY * 50 MCG/DAY TRANSDERMAL PATCH
00002225190
00002148587
00002148595
00002238704
00002245676000022437220000075684900002247499
00002243999
00002246967000022437240000224400000002231509
000022469680000224400100002247500
00002246969000022440020000075679200002231510
00002325462
00002241332
00002168898
00002241835
00002241837
ESTRACE
ESTRACE
ESTRACE
ESTROGEL
ESTRADOT 25 (0.39 MG/PTH)OESCLIM 25 (5 MG/PTH)ESTRADERM-25 (2 MG/PTH)CLIMARA 25 (2 MG/PTH)
ESTRADOT 37.5 (0.585 MG/PTH)
SANDOZ ESTRADIOL DERM 50 (4 MG/PTH)OESCLIM 50 (10 MG/PTH)ESTRADOT 50 (0.78 MG/PTH)CLIMARA 50 (3.9 MG/PTH)
SANDOZ ESTRADIOL DERM 75 (6 MG/PTH)ESTRADOT 75 (1.17 MG/PTH)CLIMARA 75 (5.7 MG/PTH)
SANDOZ ESTRADIOL DERM 100 (8 MG/PTH)ESTRADOT 100 (1.56 MG/PTH)ESTRADERM-100 (8.0 MG/PTH)CLIMARA 100 (7.8 MG/PTH)
VAGIFEM
VAGIFEM
ESTRING
ESTALIS (2.7*.62 MG/PTH)
ESTALIS (4.8*.51 MG/PTH)
SHB
SHB
SHB
MFC
NOVTPINOVBHP
NOV
SDZTPINOVBHP
SDZNOVBHP
SDZNOVNOVBHP
NNA
NNA
PAL
NOV
NOV
HORMONES AND SYNTHETIC SUBSTITUTES
ESTROGENS AND ANTIESTROGENS
68:00
68:16.04
0.1287
0.2486
0.4390
0.3134
2.8055 2.8285 3.5731 5.2863
2.8249
2.4125 2.8377 3.0094 5.6464
2.5875 3.2278 6.0200
2.7375 3.4103 4.3121 6.3667
3.2133
3.2133
65.3934
3.3170
3.3170
161 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$$$$
$
$$$$
$$$
$$$$
$
$
$
$
$
(ESTROGENS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
CLOMIPHENE CITRATE
ACARBOSE
METFORMIN HCL
50 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
500 MG ORAL TABLET
850 MG ORAL TABLET
0000089372200002091879
00002190885
00002190893
00002167786000023645060000225772600002242794000023533770000214876500002045710000021628220000222356200002269031000022429740000224682000002099233
000022297850000236451400002257734000023533850000222965600002230475000022295170000224258900002269058000022429310000224682100002162849
SEROPHENECLOMID
GLUCOBAY
GLUCOBAY
APO-METFORMINAVA-METFORMINCO METFORMINMETFORMINMETFORMINMYLAN-METFORMINNOVO-METFORMINNU-METFORMINPMS-METFORMINRAN-METFORMINRATIO-METFORMIN HYDROCHLORIDESANDOZ METFORMIN FCGLUCOPHAGE
APO-METFORMINAVA-METFORMINCO METFORMINMETFORMINMYLAN-METFORMINNOVO-METFORMINNU-METFORMINPMS-METFORMINRAN-METFORMINRATIO-METFORMIN HYDROCHLORIDESANDOZ METFORMIN FCGLUCOPHAGE
SROSAV
BAI
BAI
APXAVACOBMELSNSMYPTEVNXPPMSRANRPHSDZSAV
APXAVACOBSNSMYPTEVNXPPMSRANRPHSDZSAV
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
ESTROGENS AND ANTIESTROGENS
ANTIDIABETIC AGENTS
ANTIDIABETIC AGENTS
68
68
68
:00
:00
:00
68:16.12
68:20.02
68:20.04
5.3623 5.9779
0.2840
0.3933
0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.1216 0.2920
0.2040 0.2040 0.2040 0.2040 0.2040 0.2040 0.2040 0.2040 0.2040 0.2040 0.2040 0.3803
162 EFFECTIVE APRIL 1, 2012
$$
$
$
$$$$$$$$$$$$$
$$$$$$$$$$$$
(ESTROGEN AGONISTS-ANTAGONISTS)
(ALPHA-GLUCOSIDASE INHIBITORS)
(BIGUANIDES)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
INSULIN ASPART
INSULIN DETEMIR
INSULIN GLARGINE
INSULIN GLULISINE (RDNA ORIGIN)
INSULIN HUMAN BIOSYNTHETIC (ISOPHANE)
INSULIN HUMAN BIOSYNTHETIC (REGULAR)
INSULIN HUMAN BIOSYNTHETIC (REGULAR)/ INSULIN HUMAN BIOSYNTHETIC (ISOPHANE)
INSULIN LISPRO
100 UNIT / ML INJECTION
100 UNIT / ML INJECTION
100 UNIT / ML INJECTION
100 UNIT / ML INJECTION
100 UNIT / ML INJECTION
100 UNIT / ML INJECTION
30 UNIT / ML * 70 UNIT / ML INJECTION
40 UNIT / ML * 60 UNIT / ML INJECTION
50 UNIT / ML * 50 UNIT / ML INJECTION
100 UNIT / ML INJECTION
0000224539700002244353
00002271842
000022456890000225193000002294338
000022794600000227947900002294346
00002024225000005877370000202426800001959239
00002024233000005867140000202428400001959220
00002024217000007958790000202524800001959212
00002024314
00002024322
0000222970400002229705
NOVORAPIDNOVORAPID CARTRIDGE
LEVEMIR CARTRIDGE
LANTUSLANTUS CARTRIDGELANTUS PEN
APIDRAAPIDRA CARTRIDGEAPIDRA PEN
NOVOLIN GE NPHHUMULIN NNOVOLIN GE NPH CARTRIDGEHUMULIN N CARTRIDGE/KWIKPEN
NOVOLIN GE TORONTOHUMULIN RNOVOLIN GE TORONTO CARTRIDGEHUMULIN R CARTRIDGE
NOVOLIN GE 30/70HUMULIN 30/70NOVOLIN GE 30/70 CARTRIDGEHUMULIN 30/70 CARTRIDGE
NOVOLIN GE 40/60 CARTRIDGE
NOVOLIN GE 50/50 CARTRIDGE
HUMALOGHUMALOG CARTRIDGE/KWIKPEN
NNANNA
NNA
SAVSAVSAV
SAVSAVSAV
NNALILNNALIL
NNALILNNALIL
NNALILNNALIL
NNA
NNA
LILLIL
HORMONES AND SYNTHETIC SUBSTITUTES
ANTIDIABETIC AGENTS
68:00
68:20.08
2.7920 3.7733
6.6787
6.4306 6.4529 6.4529
2.6338 3.4722 3.5117
2.1930 2.3291 2.8580 3.0476
2.1930 2.3291 2.8687 3.0476
2.1930 2.3291 2.8553 3.0476
2.9240
2.9240
2.9143 3.9022
163 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$$$
$$$
$$$$
$$$$
$$$$
$
$
$$
(INSULINS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
INSULIN LISPRO/ INSULIN LISPRO PROTAMINE
REPAGLINIDE
GLICLAZIDE
25 % * 75 % INJECTION
50 % * 50 % INJECTION
0.5 MG ORAL TABLET
1 MG ORAL TABLET
2 MG ORAL TABLET
80 MG ORAL TABLET
30 MG ORAL SUSTAINED-RELEASE TABLET
60 MG ORAL SUSTAINED-RELEASE TABLET
00002240294
00002240297
0000235566300002321475000023549260000235745300002239924
0000235567100002321483000023549340000235746100002239925
0000235569800002321491000023549420000235748800002239926
000022452470000236351800002287072000022295190000223810300000765996
0000229779500002242987
00002356422
HUMALOG MIX 25 CARTRIDGE/KWIKPEN
HUMALOG MIX 50 CARTRIDGE/KWIKPEN
APO-REPAGLINIDECO REPAGLINIDEPMS-REPAGLINIDESANDOZ REPAGLINIDEGLUCONORM
APO-REPAGLINIDECO REPAGLINIDEPMS-REPAGLINIDESANDOZ REPAGLINIDEGLUCONORM
APO-REPAGLINIDECO REPAGLINIDEPMS-REPAGLINIDESANDOZ REPAGLINIDEGLUCONORM
APO-GLICLAZIDEAVA-GLICLAZIDEGLICLAZIDEMYLAN-GLICLAZIDENOVO-GLICLAZIDEDIAMICRON
GLICLAZIDE MRDIAMICRON MR
DIAMICRON MR
LIL
LIL
APXCOBPMSSDZNNA
APXCOBPMSSDZNNA
APXCOBPMSSDZNNA
APXAVASNSMYPTEVSEV
AAPSEV
SEV
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
ANTIDIABETIC AGENTS
ANTIDIABETIC AGENTS
ANTIDIABETIC AGENTS
68
68
68
:00
:00
:00
68:20.08
68:20.16
68:20.20
3.9022
3.9021
0.1339 0.1339 0.1339 0.1339 0.3126
0.1392 0.1392 0.1392 0.1392 0.3250
0.1446 0.1446 0.1446 0.1446 0.3376
0.2242 0.2242 0.2242 0.2242 0.2242 0.4004
0.1405 0.1510
0.2719
164 EFFECTIVE APRIL 1, 2012
$
$
$$$$$
$$$$$
$$$$$
$$$$$$
$$
$
(INSULINS)
(MEGLITINIDES)
(SULFONYLUREAS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
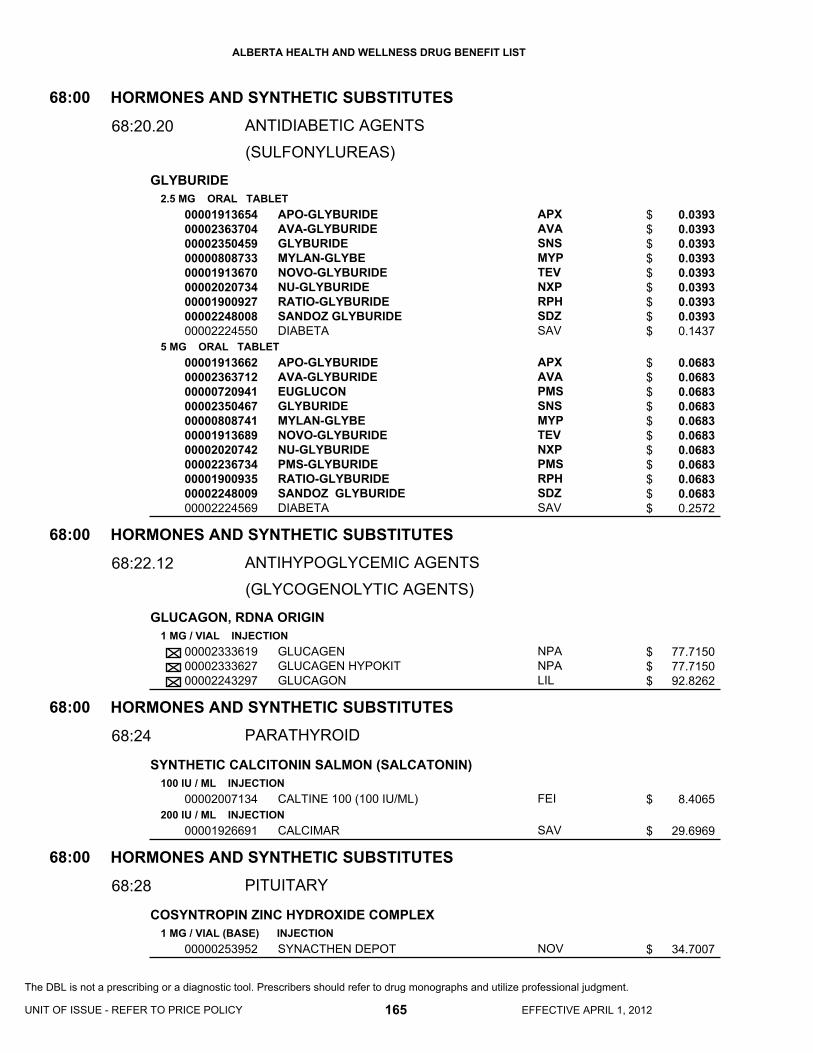
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
GLYBURIDE
GLUCAGON, RDNA ORIGIN
SYNTHETIC CALCITONIN SALMON (SALCATONIN)
COSYNTROPIN ZINC HYDROXIDE COMPLEX
2.5 MG ORAL TABLET
5 MG ORAL TABLET
1 MG / VIAL INJECTION
100 IU / ML INJECTION
200 IU / ML INJECTION
1 MG / VIAL (BASE) INJECTION
000019136540000236370400002350459000008087330000191367000002020734000019009270000224800800002224550
0000191366200002363712000007209410000235046700000808741000019136890000202074200002236734000019009350000224800900002224569
000023336190000233362700002243297
00002007134
00001926691
00000253952
APO-GLYBURIDEAVA-GLYBURIDEGLYBURIDEMYLAN-GLYBENOVO-GLYBURIDENU-GLYBURIDERATIO-GLYBURIDESANDOZ GLYBURIDEDIABETA
APO-GLYBURIDEAVA-GLYBURIDEEUGLUCONGLYBURIDEMYLAN-GLYBENOVO-GLYBURIDENU-GLYBURIDEPMS-GLYBURIDERATIO-GLYBURIDESANDOZ GLYBURIDEDIABETA
GLUCAGENGLUCAGEN HYPOKITGLUCAGON
CALTINE 100 (100 IU/ML)
CALCIMAR
SYNACTHEN DEPOT
APXAVASNSMYPTEVNXPRPHSDZSAV
APXAVAPMSSNSMYPTEVNXPPMSRPHSDZSAV
NPANPALIL
FEI
SAV
NOV
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
ANTIDIABETIC AGENTS
ANTIHYPOGLYCEMIC AGENTS
PARATHYROID
PITUITARY
68
68
68
68
:00
:00
:00
:00
68:20.20
68:22.12
68:24
68:28
0.0393 0.0393 0.0393 0.0393 0.0393 0.0393 0.0393 0.0393 0.1437
0.0683 0.0683 0.0683 0.0683 0.0683 0.0683 0.0683 0.0683 0.0683 0.0683 0.2572
77.7150 77.7150 92.8262
8.4065
29.6969
34.7007
165 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$$$$$
$$$$$$$$$$$
$$$
$
$
$
(SULFONYLUREAS)
(GLYCOGENOLYTIC AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
DESMOPRESSIN ACETATE
MEDROXYPROGESTERONE ACETATE
PROGESTERONE
0.1 MG ORAL TABLET
0.2 MG ORAL TABLET
10 MCG / DOSE NASAL METERED DOSE SPRAY
150 MCG / DOSE NASAL METERED DOSE SPRAY
0.1 MG / ML NASAL SOLUTION
4 MCG / ML INJECTION
2.5 MG ORAL TABLET
5 MG ORAL TABLET
10 MG ORAL TABLET
100 MG ORAL TABLET
50 MG / ML INJECTION
150 MG / ML INJECTION
100 MG ORAL CAPSULE
50 MG / ML INJECTION
00002284030000022877300000230436800000824305
00002284049000022877490000230437600000824143
0000224246500000836362
00002237860
00000402516
00000873993
000022447260000222128400000708917
000022447270000222129200000030937
000022772980000222130600000729973
00002267640
00000030848
0000232225000000585092
00002166704
00001977652
APO-DESMOPRESSINNOVO-DESMOPRESSINPMS-DESMOPRESSINDDAVP
APO-DESMOPRESSINNOVO-DESMOPRESSINPMS-DESMOPRESSINDDAVP
DESMOPRESSINDDAVP
OCTOSTIM
DDAVP
DDAVP
APO-MEDROXYNOVO-MEDRONEPROVERA
APO-MEDROXYNOVO-MEDRONEPROVERA
APO-MEDROXYNOVO-MEDRONEPROVERA
APO-MEDROXY
DEPO-PROVERA
MEDROXYPROGESTERONE ACETATEDEPO-PROVERA
PROMETRIUM
PROGESTERONE
APXTEVPMSFEI
APXTEVPMSFEI
AAPFEI
FEI
FEI
FEI
APXTEVPFI
APXTEVPFI
APXTEVPFI
APX
PFI
SDZPFI
MFC
CYT
HORMONES AND SYNTHETIC SUBSTITUTES
HORMONES AND SYNTHETIC SUBSTITUTES
PITUITARY
PROGESTINS
68
68
:00
:00
68:28
68:32
0.7956 0.7956 0.7956 1.4208
1.5912 1.5912 1.5912 2.8415
1.4160 2.0296
16.5980
20.2960
10.8145
0.0794 0.0794 0.1758
0.1569 0.1569 0.3474
0.3169 0.3169 0.7051
1.2057
5.7392
22.0000 29.6086
1.0910
6.3000
166 EFFECTIVE APRIL 1, 2012
$$$$
$$$$
$$
$
$
$
$$$
$$$
$$$
$
$
$$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
DESSICATED THYROID
LEVOTHYROXINE SODIUM
LIOTHYRONINE SODIUM
30 MG ORAL TABLET
60 MG ORAL TABLET
125 MG ORAL TABLET
0.025 MG ORAL TABLET
0.05 MG ORAL TABLET
0.075 MG ORAL TABLET
0.088 MG ORAL TABLET
0.1 MG ORAL TABLET
0.112 MG ORAL TABLET
0.125 MG ORAL TABLET
0.137 MG ORAL TABLET
0.15 MG ORAL TABLET
0.175 MG ORAL TABLET
0.2 MG ORAL TABLET
0.3 MG ORAL TABLET
5 MCG (BASE) ORAL TABLET
25 MCG (BASE) ORAL TABLET
00000023949
00000023957
00000023965
00002172062
0000221319200002172070
00002172089
00002172097
0000221320600002172100
00002171228
00002172119
00002233852
0000221321400002172127
00002172135
0000221322200002172143
00002172151
00001919458
00001919466
THYROID
THYROID
THYROID
SYNTHROID
ELTROXINSYNTHROID
SYNTHROID
SYNTHROID
ELTROXINSYNTHROID
SYNTHROID
SYNTHROID
SYNTHROID
ELTROXINSYNTHROID
SYNTHROID
ELTROXINSYNTHROID
SYNTHROID
CYTOMEL
CYTOMEL
ERF
ERF
ERF
ABB
TPIABB
ABB
ABB
TPIABB
ABB
ABB
ABB
TPIABB
ABB
TPIABB
ABB
KNG
KNG
HORMONES AND SYNTHETIC SUBSTITUTES
THYROID AND ANTITHYROID AGENTS
68:00
68:36.04
0.0575
0.0705
0.1012
0.0865
0.0310 0.0594
0.0935
0.0935
0.0381 0.0732
0.0987
0.0999
0.1687
0.0421 0.0784
0.1071
0.0446 0.0837
0.1154
1.0555
1.1473
167 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$$
$
$
$$
$
$
$
$$
$
$$
$
$
$
(THYROID AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
METHIMAZOLE
PROPYLTHIOURACIL
5 MG ORAL TABLET
50 MG ORAL TABLET
100 MG ORAL TABLET
00000015741
00000010200
00000010219
TAPAZOLE
PROPYL-THYRACIL
PROPYL-THYRACIL
PAL
PAL
PAL
HORMONES AND SYNTHETIC SUBSTITUTES
THYROID AND ANTITHYROID AGENTS
68:00
68:36.08
0.2503
0.2160
0.3380
168 EFFECTIVE APRIL 1, 2012
$
$
$
(ANTITHYROID AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

80:00 Serums, Toxoids and Vaccines
80:00
Serums, Toxoids and Vaccines

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ALLERGY SERUM
HEPATITIS B VACCINE (RECOMBINANT)
INJECTION
10 MCG / ML INJECTION
20 MCG / ML INJECTION
00000999981
00000749486
00001919431
ALLERGY SERUM
RECOMBIVAX-HB
ENGERIX-B
XXX
MFC
GSK
SERUMS, TOXOIDS, AND VACCINES
SERUMS, TOXOIDS, AND VACCINES
SERUMS
VACCINES
80
80
:00
:00
80:04
80:12
0.0000
21.3500
22.7792
169 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

84:00 Skin and Mucous M
embrane A
gents
84:00
Skin and Mucous Membrane Agents

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
COMPOUND PRESCRIPTION
COMPOUND PRESCRIPTION
FUSIDIC ACID
GENTAMICIN SULFATE
METRONIDAZOLE
TOPICAL
TOPICAL
TOPICAL
TOPICAL
2 % TOPICAL CREAM
0.1 % (BASE) TOPICAL CREAM
0.1 % (BASE) TOPICAL OINTMENT
0.75 % TOPICAL CREAM
1 % TOPICAL CREAM
0.75 % TOPICAL LOTION
1 % TOPICAL GEL
00000999119
00000999112
00000999219
00000999213
00000999103
00000999203
00000586668
00000805386
00000805025
00002226839
0000224291900002156091
00002248206
00002297809
COMPOUND - RETINOIC ACID (TRETINOIN) (TOPICAL)MISCELLANEOUS TOPICAL COMPOUND
COMPOUND - RETINOIC ACID (TRETINOIN) (TOPICAL)MISCELLANEOUS TOPICAL COMPOUND
COMPOUND-ANTI-INFECTIVE (TOPICAL)
COMPOUND-ANTI-INFECTIVE (TOPICAL)
FUCIDIN
RATIO-GENTAMICIN SULFATE
RATIO-GENTAMICIN SULFATE
METROCREAM
ROSASOLNORITATE
METROLOTION
METROGEL
XXX
XXX
XXX
XXX
XXX
XXX
LEO
RPH
RPH
GAL
GSKSAV
GAL
GAL
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFECTIVES
ANTI-INFECTIVES
84
84
84
:00
:00
:00
84:00
84:04
84:04.04
0.0000
0.0000
0.0000
0.0000
0.0000
0.0000
0.6581
0.4301
0.3729
0.5183
0.5593 0.5815
0.5183
0.6285
171 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$$
$
$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
(ANTIBACTERIALS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
METRONIDAZOLE
METRONIDAZOLE/ NYSTATIN
MUPIROCIN
NEOMYCIN SULFATE/ POLYMYXIN B SULFATE
SODIUM FUSIDATE
TERBINAFINE HCL
KETOCONAZOLE
10 % VAGINAL CREAM
100 MG / G * 20,000 UNIT / G VAGINAL CREAM
500 MG * 100,000 UNIT VAGINAL OVULE
2 % TOPICAL CREAM
2 % TOPICAL OINTMENT
40 MG / ML (BASE) * 200,000 UNIT / ML IRRIGATION SOLUTION
2 % TOPICAL OINTMENT
1 % TOPICAL CREAM
1 % TOPICAL SOLUTION
2 % TOPICAL CREAM
00001926861
00001926845
00001926829
00002239757
0000227998300001916947
00000666157
00000586676
00002031094
00002238703
00002245662
FLAGYL
FLAGYSTATIN
FLAGYSTATIN
BACTROBAN
TARO-MUPIROCINBACTROBAN
NEOSPORIN
FUCIDIN
LAMISIL
LAMISIL
KETODERM
SAV
SAV
SAV
GKC
TARGKC
GSK
LEO
NOV
NOV
TPT
(ALLYLAMINES)
(AZOLES)
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFECTIVES
ANTI-INFECTIVES
ANTI-INFECTIVES
84
84
84
:00
:00
:00
84:04.04
84:04.08.04
84:04.08.08
0.2496
0.6104
3.3572
0.5481
0.3453 0.5481
1.8127
0.6581
0.5573
0.5657
0.3431
172 EFFECTIVE APRIL 1, 2012
$
$
$
$
$$
$
$
$
$
$
(ANTIBACTERIALS)
ANTIFUNGALS
ANTIFUNGALS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
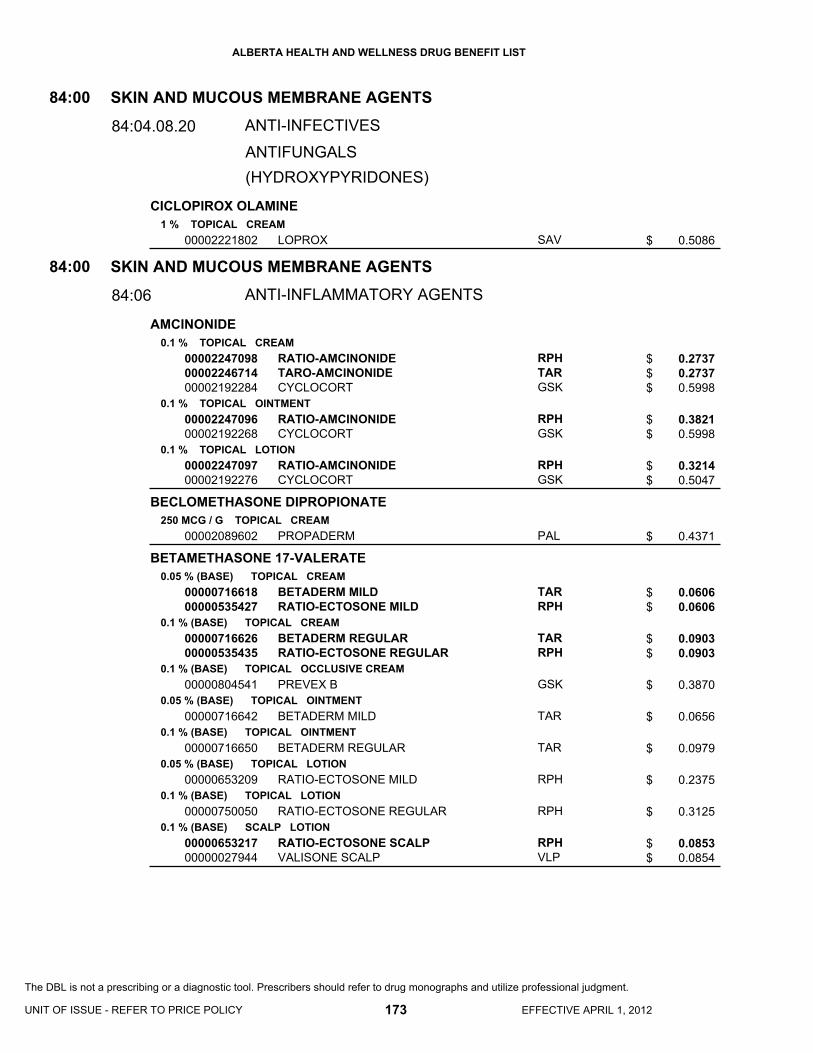
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CICLOPIROX OLAMINE
AMCINONIDE
BECLOMETHASONE DIPROPIONATE
BETAMETHASONE 17-VALERATE
1 % TOPICAL CREAM
0.1 % TOPICAL CREAM
0.1 % TOPICAL OINTMENT
0.1 % TOPICAL LOTION
250 MCG / G TOPICAL CREAM
0.05 % (BASE) TOPICAL CREAM
0.1 % (BASE) TOPICAL CREAM
0.1 % (BASE) TOPICAL OCCLUSIVE CREAM
0.05 % (BASE) TOPICAL OINTMENT
0.1 % (BASE) TOPICAL OINTMENT
0.05 % (BASE) TOPICAL LOTION
0.1 % (BASE) TOPICAL LOTION
0.1 % (BASE) SCALP LOTION
00002221802
000022470980000224671400002192284
0000224709600002192268
0000224709700002192276
00002089602
0000071661800000535427
0000071662600000535435
00000804541
00000716642
00000716650
00000653209
00000750050
0000065321700000027944
LOPROX
RATIO-AMCINONIDETARO-AMCINONIDECYCLOCORT
RATIO-AMCINONIDECYCLOCORT
RATIO-AMCINONIDECYCLOCORT
PROPADERM
BETADERM MILDRATIO-ECTOSONE MILD
BETADERM REGULARRATIO-ECTOSONE REGULAR
PREVEX B
BETADERM MILD
BETADERM REGULAR
RATIO-ECTOSONE MILD
RATIO-ECTOSONE REGULAR
RATIO-ECTOSONE SCALPVALISONE SCALP
SAV
RPHTARGSK
RPHGSK
RPHGSK
PAL
TARRPH
TARRPH
GSK
TAR
TAR
RPH
RPH
RPHVLP
(HYDROXYPYRIDONES)
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFECTIVES
ANTI-INFLAMMATORY AGENTS
84
84
:00
:00
84:04.08.20
84:06
0.5086
0.2737 0.2737 0.5998
0.3821 0.5998
0.3214 0.5047
0.4371
0.0606 0.0606
0.0903 0.0903
0.3870
0.0656
0.0979
0.2375
0.3125
0.0853 0.0854
173 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$
$$
$$
$
$$
$$
$
$
$
$
$
$$
ANTIFUNGALS
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
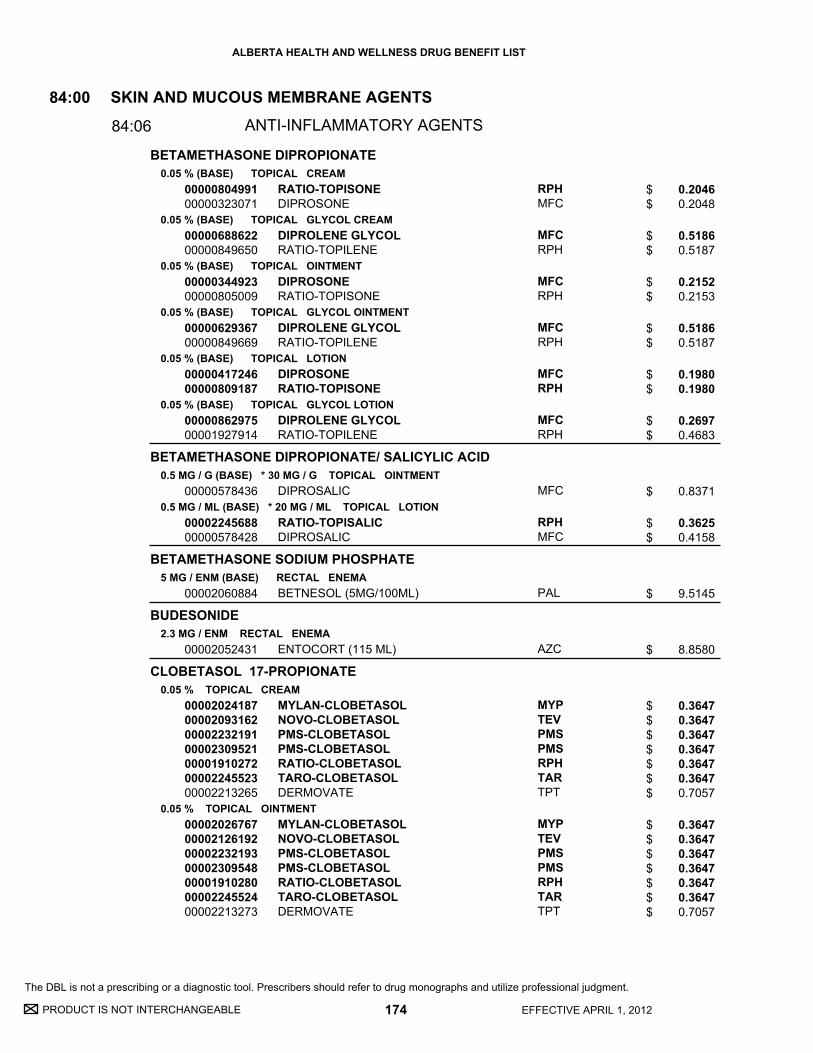
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
BETAMETHASONE DIPROPIONATE
BETAMETHASONE DIPROPIONATE/ SALICYLIC ACID
BETAMETHASONE SODIUM PHOSPHATE
BUDESONIDE
CLOBETASOL 17-PROPIONATE
0.05 % (BASE) TOPICAL CREAM
0.05 % (BASE) TOPICAL GLYCOL CREAM
0.05 % (BASE) TOPICAL OINTMENT
0.05 % (BASE) TOPICAL GLYCOL OINTMENT
0.05 % (BASE) TOPICAL LOTION
0.05 % (BASE) TOPICAL GLYCOL LOTION
0.5 MG / G (BASE) * 30 MG / G TOPICAL OINTMENT
0.5 MG / ML (BASE) * 20 MG / ML TOPICAL LOTION
5 MG / ENM (BASE) RECTAL ENEMA
2.3 MG / ENM RECTAL ENEMA
0.05 % TOPICAL CREAM
0.05 % TOPICAL OINTMENT
0000080499100000323071
0000068862200000849650
0000034492300000805009
0000062936700000849669
0000041724600000809187
0000086297500001927914
00000578436
0000224568800000578428
00002060884
00002052431
00002024187000020931620000223219100002309521000019102720000224552300002213265
00002026767000021261920000223219300002309548000019102800000224552400002213273
RATIO-TOPISONEDIPROSONE
DIPROLENE GLYCOLRATIO-TOPILENE
DIPROSONERATIO-TOPISONE
DIPROLENE GLYCOLRATIO-TOPILENE
DIPROSONERATIO-TOPISONE
DIPROLENE GLYCOLRATIO-TOPILENE
DIPROSALIC
RATIO-TOPISALICDIPROSALIC
BETNESOL (5MG/100ML)
ENTOCORT (115 ML)
MYLAN-CLOBETASOLNOVO-CLOBETASOLPMS-CLOBETASOLPMS-CLOBETASOLRATIO-CLOBETASOLTARO-CLOBETASOLDERMOVATE
MYLAN-CLOBETASOLNOVO-CLOBETASOLPMS-CLOBETASOLPMS-CLOBETASOLRATIO-CLOBETASOLTARO-CLOBETASOLDERMOVATE
RPHMFC
MFCRPH
MFCRPH
MFCRPH
MFCRPH
MFCRPH
MFC
RPHMFC
PAL
AZC
MYPTEVPMSPMSRPHTARTPT
MYPTEVPMSPMSRPHTARTPT
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFLAMMATORY AGENTS
84:00
84:06
0.2046 0.2048
0.5186 0.5187
0.2152 0.2153
0.5186 0.5187
0.1980 0.1980
0.2697 0.4683
0.8371
0.3625 0.4158
9.5145
8.8580
0.3647 0.3647 0.3647 0.3647 0.3647 0.3647 0.7057
0.3647 0.3647 0.3647 0.3647 0.3647 0.3647 0.7057
174 EFFECTIVE APRIL 1, 2012
$$
$$
$$
$$
$$
$$
$
$$
$
$
$$$$$$$
$$$$$$$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CLOBETASOL 17-PROPIONATE
COMPOUND PRESCRIPTION
DESONIDE
DESOXIMETASONE
DIFLUCORTOLONE VALERATE
FLUOCINONIDE
HALOBETASOL PROPIONATE
0.05 % SCALP LOTION
TOPICAL
TOPICAL
0.05 % TOPICAL CREAM
0.05 % TOPICAL OINTMENT
0.05 % TOPICAL CREAM
0.25 % TOPICAL CREAM
0.1 % TOPICAL CREAM
0.1 % TOPICAL OINTMENT
0.05 % TOPICAL CREAM
0.05 % TOPICAL EMOLLIENT CREAM
0.05 % TOPICAL OINTMENT
0.05 % TOPICAL GEL
0.05 % TOPICAL CREAM
0000221621300002232195000019102990000224552200002213281
00000999107
00000999207
00002229315
00002229323
00002221918
00002221896
0000058782600000587818
00000587834
00000716863
00000598933
00002236996
00002236997
00001962701
MYLAN-CLOBETASOLPMS-CLOBETASOLRATIO-CLOBETASOLTARO-CLOBETASOLDERMOVATE
COMPOUND-CORTICOSTEROIDS - TOPICAL
COMPOUND-CORTICOSTEROIDS - TOPICAL
PMS-DESONIDE
PMS-DESONIDE
TOPICORT MILD
TOPICORT
NERISONENERISONE OILY
NERISONE
LYDERM
TIAMOL
LYDERM
LYDERM
ULTRAVATE
MYPPMSRPHTARTPT
XXX
XXX
PMS
PMS
SAV
SAV
GSKGSK
GSK
TPT
TPT
TPT
TPT
VCL
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFLAMMATORY AGENTS
84:00
84:06
0.3184 0.3184 0.3184 0.3184 0.6160
0.0000
0.0000
0.3085
0.2992
0.5020
0.7235
0.4239 0.4243
0.4239
0.2835
0.2637
0.3652
0.3703
0.8590
175 EFFECTIVE APRIL 1, 2012
UNIT OF ISSUE - REFER TO PRICE POLICY
$$$$$
$
$
$
$
$
$
$$
$
$
$
$
$
$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
HYDROCORTISONE
HYDROCORTISONE 17-VALERATE
HYDROCORTISONE ACETATE
HYDROCORTISONE ACETATE/ PRAMOXINE HCL
HYDROCORTISONE ACETATE/ PRAMOXINE HCL/ ZINC SULFATE
HYDROCORTISONE ACETATE/ UREA
1 % TOPICAL CREAM
2.5 % TOPICAL CREAM
1 % TOPICAL OCCLUSIVE CREAM
0.5 % TOPICAL OINTMENT
1 % TOPICAL OINTMENT
1 % TOPICAL LOTION
2.5 % TOPICAL LOTION
100 MG / ENM RECTAL ENEMA
0.2 % TOPICAL CREAM
0.2 % TOPICAL OINTMENT
0.5 % TOPICAL CREAM
1 % TOPICAL CREAM
10 % RECTAL FOAM
1 % * 1 % RECTAL FOAM
10 MG * 20 MG * 10 MG RECTAL SUPPOSITORY
0.5 % * 1 % * 0.5 % RECTAL OINTMENT
1 % * 10 % TOPICAL CREAM
1 % * 10 % TOPICAL LOTION
00000192597
00000595799
00000804533
00000716685
00000716693
0000057854100000192600
0000085671100000595802
0000023031600002112736
00002242984
00002242985
00000716820
00000716839
00000579335
00000363014
0000224085100002242797
0000223446600002247692
00000503134
00000560022
EMO-CORT
EMO-CORT
PREVEX HC
CORTODERM MILD
CORTODERM REGULAR
SARNA HCEMO-CORT
SARNA HCEMO-CORT
HYCORT (100MG/60ML)CORTENEMA (100MG/60ML)
HYDROVAL
HYDROVAL
HYDERM
HYDERM
CORTIFOAM
PROCTOFOAM-HC
PROCTODAN-HCSANDOZ ANUZINC HC PLUS
PROCTODAN-HCSANDOZ ANUZINC HC PLUS
UREMOL-HC
UREMOL-HC
GSK
GSK
GSK
TAR
TAR
GSKGSK
GSKGSK
VCLAXC
TPT
TPT
TAR
TAR
PAL
DUI
ODNSDZ
ODNSDZ
GSK
GSK
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFLAMMATORY AGENTS
84:00
84:06
0.1847
0.2523
0.2878
0.1474
0.0422
0.1008 0.1706
0.1949 0.2257
5.6745 7.2234
0.1312
0.1312
0.1806
0.0395
6.1365
1.7815
0.7826 0.7826
0.5218 0.5218
0.1877
0.1044
176 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$$
$$
$$
$
$
$
$
$
$
$$
$$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
HYDROCORTISONE ACETATE/ ZINC SULFATE
MOMETASONE FUROATE
TRIAMCINOLONE ACETONIDE
BETAMETHASONE DIPROPIONATE/ CLOTRIMAZOLE
COMPOUND PRESCRIPTION
10 MG * 10 MG RECTAL SUPPOSITORY
0.5 % * 0.5 % RECTAL OINTMENT
0.1 % TOPICAL CREAM
0.1 % TOPICAL OINTMENT
0.1 % TOPICAL LOTION
0.1 % TOPICAL CREAM
0.5 % TOPICAL CREAM
0.1 % TOPICAL OINTMENT
0.1 % DENTAL PASTE
0.05 % (BASE) * 1 % TOPICAL CREAM
000022363990000060779700002242798
000021284460000060778900002247691
0000236715700000851744
000022481300000226474900000851736
0000226638500000871095
0000071696000002194058
00002194066
00002194031
00001964054
00000611174
00000999110
00000999211
ANODAN-HCRATIO-HEMCORT H.C.SANDOZ ANUZINC HC
ANODAN-HCRATIO-HEMCORT H.C.SANDOZ ANUZINC HC
TARO-MOMETASONEELOCOM
RATIO-MOMETASONETARO-MOMETASONEELOCOM
TARO-MOMETASONEELOCOM
TRIADERM REGULARARISTOCORT R
ARISTOCORT C
ARISTOCORT R
ORACORT
LOTRIDERM
COMBINATION ANTI-INFECTIVE /CORTICOSTEROID
COMBINATION ANTI-INFECTIVE /CORTICOSTEROID
ODNRPHSDZ
ODNRPHSDZ
TARMFC
RPHTARMFC
TARMFC
TARVLP
VLP
VLP
TAR
MFC
XXX
XXX
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFLAMMATORY AGENTS
ANTI-INFLAMMATORY AGENTS
84
84
:00
:00
84:06
84:06.00
0.6075 0.6075 0.6075
0.4130 0.4130 0.4130
0.5262 0.6796
0.3353 0.3353 0.6112
0.3124 0.4556
0.0650 0.1397
1.2387
0.1435
1.1703
0.7295
0.0000
0.0000
177 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$$
$$$
$$
$$$
$$
$$
$
$
$
$
$
$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
(COMBINATION ANTI-INFECTIVE/ANTI-INFLAMMATORY AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
HYDROCORTISONE/ CINCHOCAINE HCL/ FRAMYCETIN SULFATE/ ESCULIN
LIDOCAINE
LIDOCAINE HCL
COMPOUND PRESCRIPTION
METHOXSALEN
5 MG * 5 MG * 10 MG * 10 MG RECTAL SUPPOSITORY
5 MG / G * 5 MG / G * 10 MG / G * 10 MG / G RECTAL OINTMENT
5 % TOPICAL OINTMENT
2 % TOPICAL JELLY
TOPICAL
TOPICAL
10 MG ORAL CAPSULE
10 MG / ML TOPICAL LOTION
000022478820000222639100002242528
00002247322000022263830000224252700002223252
0000208379500000001961
00000001694
00000999104
00000999204
0000025265400001946374
00001907476
PROCTOLRATIO-PROCTOSONESANDOZ PROCTOMYXIN HC
PROCTOLRATIO-PROCTOSONESANDOZ PROCTOMYXIN HCPROCTOSEDYL
LIDODANXYLOCAINE
XYLOCAINE JELLY
COMPOUND- SALICYLIC ACID (TOPICAL)
COMPOUND- SALICYLIC ACID (TOPICAL)
OXSORALEN ULTRAOXSORALEN
OXSORALEN
ODNRPHSDZ
ODNRPHSDZAXC
ODNAZC
AZC
XXX
XXX
VCLVCL
VCL
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
SKIN AND MUCOUS MEMBRANE AGENTS
ANTI-INFLAMMATORY AGENTS
ANTIPRURITICS AND LOCAL ANESTHETICS
KERATOLYTIC AGENTS
DEPIGMENTING AND PIGMENTING AGENTS
84
84
84
84
:00
:00
:00
:00
84:06.00
84:08
84:28
84:50.06
0.6487 0.6487 0.6487
0.4577 0.4577 0.4577 0.8410
0.1548 0.2918
0.4515
0.0000
0.0000
0.4745 0.6370
1.6211
178 EFFECTIVE APRIL 1, 2012
$$$
$$$$
$$
$
$
$
$$
$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
(COMBINATION ANTI-INFECTIVE/ANTI-INFLAMMATORY AGENTS)
(PIGMENTING AGENTS)
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
5-FLUOROURACIL
ACITRETIN
AMINOBENZOATE POTASSIUM
AZELAIC ACID
CALCIPOTRIOL
CALCIPOTRIOL MONOHYDRATE/ BETAMETHASONE DIPROPIONATE
CALCIPOTRIOL/ BETAMETHASONE DIPROPIONATE
COLLAGENASE
ISOTRETINOIN
PODOFILOX
50 MG / G TOPICAL CREAM
10 MG ORAL CAPSULE
25 MG ORAL CAPSULE
500 MG ORAL TABLET
500 MG ORAL CAPSULE
15 % TOPICAL GEL
50 MCG / G TOPICAL CREAM
50 MCG / G TOPICAL OINTMENT
50 MCG / ML SCALP SOLUTION
50 MCG / G (BASE) * 0.5 MG / G (BASE) TOPICAL GEL
50 MCG / G * 0.5 MG / G TOPICAL OINTMENT
250 UNIT / G TOPICAL OINTMENT
10 MG ORAL CAPSULE
40 MG ORAL CAPSULE
0.5 % TOPICAL SOLUTION
00000330582
00002070847
00002070863
00000550175
00000611271
00002270811
00002150956
00001976133
00002194341
00002319012
00002244126
00002063670
0000058234400002257955
0000058235200002257963
00002074788
EFUDEX
SORIATANE
SORIATANE
POTABA
POTABA
FINACEA
DOVONEX
DOVONEX
DOVONEX
XAMIOL
DOVOBET
SANTYL
ACCUTANECLARUS
ACCUTANECLARUS
WARTEC
VCL
ACV
ACV
GLE
GLE
BAI
LEO
LEO
LEO
LEO
LEO
HPC
HLRMYP
HLRMYP
PAL
SKIN AND MUCOUS MEMBRANE AGENTS
MISCELLANEOUS SKIN AND MUCOUS MEMBRANE AGENTS
84:00
84:92
0.8976
1.9935
3.5015
0.3914
0.2976
0.6450
0.8126
0.7886
0.8162
1.5482
1.5436
2.9167
1.0011 1.0011
2.0428 2.0428
14.2610
179 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$
$
$
$
$
$
$
$
$
$$
$$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
TAZAROTENE0.05 % TOPICAL GEL
0.1 % TOPICAL GEL00002230784
00002230785
TAZORAC
TAZORAC
ALL
ALL
SKIN AND MUCOUS MEMBRANE AGENTS
MISCELLANEOUS SKIN AND MUCOUS MEMBRANE AGENTS
84:00
84:92
1.4203
1.4203
180 EFFECTIVE APRIL 1, 2012
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

86:00 Smooth M
uscle Relaxants
86:00
Smooth Muscle Relaxants

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
OXYBUTYNIN CHLORIDE
AMINOPHYLLINE
OXTRIPHYLLINE
OXTRIPHYLLINE/ GUAIFENESIN
THEOPHYLLINE
2.5 MG ORAL TABLET
5 MG ORAL TABLET
1 MG / ML ORAL SYRUP
25 MG / ML INJECTION
20 MG / ML ORAL ELIXIR
20 MG / ML * 10 MG / ML ORAL ELIXIR
100 MG ORAL SUSTAINED-RELEASE TABLET
200 MG ORAL SUSTAINED-RELEASE TABLET
300 MG ORAL SUSTAINED-RELEASE TABLET
400 MG ORAL SUSTAINED-RELEASE TABLET
600 MG ORAL SUSTAINED-RELEASE TABLET
5.3 MG / ML ORAL LIQUID
00002240549
000021635430000223080000002230394000021585900000235023800002240550
00002223376
00000497193
0000079294200000476366
00000476374
00000692689
00000692697
00000692700
00002014165
00002014181
00001966219
PMS-OXYBUTYNIN
APO-OXYBUTYNINMYLAN-OXYBUTYNINNOVO-OXYBUTYNINNU-OXYBUTYNOXYBUTYNINPMS-OXYBUTYNIN
PMS-OXYBUTYNIN
AMINOPHYLLINE
PMS-OXTRIPHYLLINECHOLEDYL
CHOLEDYL EXPECTORANT
APO-THEO LA
APO-THEO LA
APO-THEO LA
UNIPHYL
UNIPHYL
THEOLAIR
PMS
APXMYPTEVNXPSNSPMS
PMS
HSP
PMSERF
ERF
APX
APX
APX
PUR
PUR
MEP
SMOOTH MUSCLE RELAXANTS
SMOOTH MUSCLE RELAXANTS
GENITOURINARY SMOOTH MUSCLE RELAXANTS
RESPIRATORY SMOOTH MUSCLE RELAXANTS
86
86
:00
:00
86:12
86:16
0.1428
0.2485 0.2485 0.2485 0.2485 0.2485 0.2485
0.1183
0.4411
0.0325 0.0395
0.0791
0.1300
0.1350
0.1400
0.5354
0.6484
0.0271
181 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$$$$$$
$
$
$$
$
$
$
$
$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

88:00 Vitamins
88:00
Vitamins
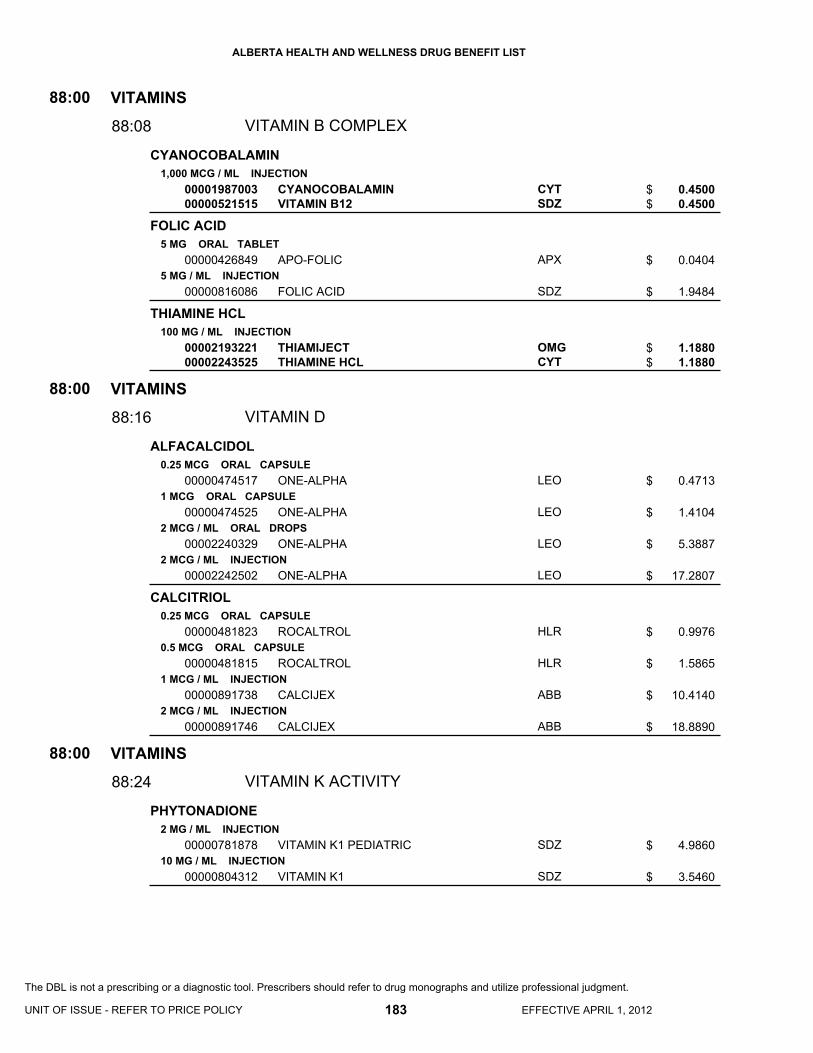
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
CYANOCOBALAMIN
FOLIC ACID
THIAMINE HCL
ALFACALCIDOL
CALCITRIOL
PHYTONADIONE
1,000 MCG / ML INJECTION
5 MG ORAL TABLET
5 MG / ML INJECTION
100 MG / ML INJECTION
0.25 MCG ORAL CAPSULE
1 MCG ORAL CAPSULE
2 MCG / ML ORAL DROPS
2 MCG / ML INJECTION
0.25 MCG ORAL CAPSULE
0.5 MCG ORAL CAPSULE
1 MCG / ML INJECTION
2 MCG / ML INJECTION
2 MG / ML INJECTION
10 MG / ML INJECTION
0000198700300000521515
00000426849
00000816086
0000219322100002243525
00000474517
00000474525
00002240329
00002242502
00000481823
00000481815
00000891738
00000891746
00000781878
00000804312
CYANOCOBALAMINVITAMIN B12
APO-FOLIC
FOLIC ACID
THIAMIJECTTHIAMINE HCL
ONE-ALPHA
ONE-ALPHA
ONE-ALPHA
ONE-ALPHA
ROCALTROL
ROCALTROL
CALCIJEX
CALCIJEX
VITAMIN K1 PEDIATRIC
VITAMIN K1
CYTSDZ
APX
SDZ
OMGCYT
LEO
LEO
LEO
LEO
HLR
HLR
ABB
ABB
SDZ
SDZ
VITAMINS
VITAMINS
VITAMINS
VITAMIN B COMPLEX
VITAMIN D
VITAMIN K ACTIVITY
88
88
88
:00
:00
:00
88:08
88:16
88:24
0.4500 0.4500
0.0404
1.9484
1.1880 1.1880
0.4713
1.4104
5.3887
17.2807
0.9976
1.5865
10.4140
18.8890
4.9860
3.5460
183 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$
$
$$
$
$
$
$
$
$
$
$
$
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
PIPRADROL HCL/ THIAMINE HCL/ RIBOFLAVIN/ PYRIDOXINE HCL/ NIACINAMIDE/ CHOLINE/ INOSITOL
0.04 MG / ML * 0.22 MG / ML * 0.11 MG / ML * 0.04 MG / ML * 1.11 MG / ML * 2.22 MG / ML * 2.22 MG / ML ORAL LIQUID
00002103052 ALERTONIC ODN
VITAMINS
MULTIVITAMIN PREPARATIONS
88:00
88:28
0.0643
184 EFFECTIVE APRIL 1, 2012
$
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

92:00 Miscellaneous Therapeutic A
gents
92:00
Miscellaneous Therapeutic Agents
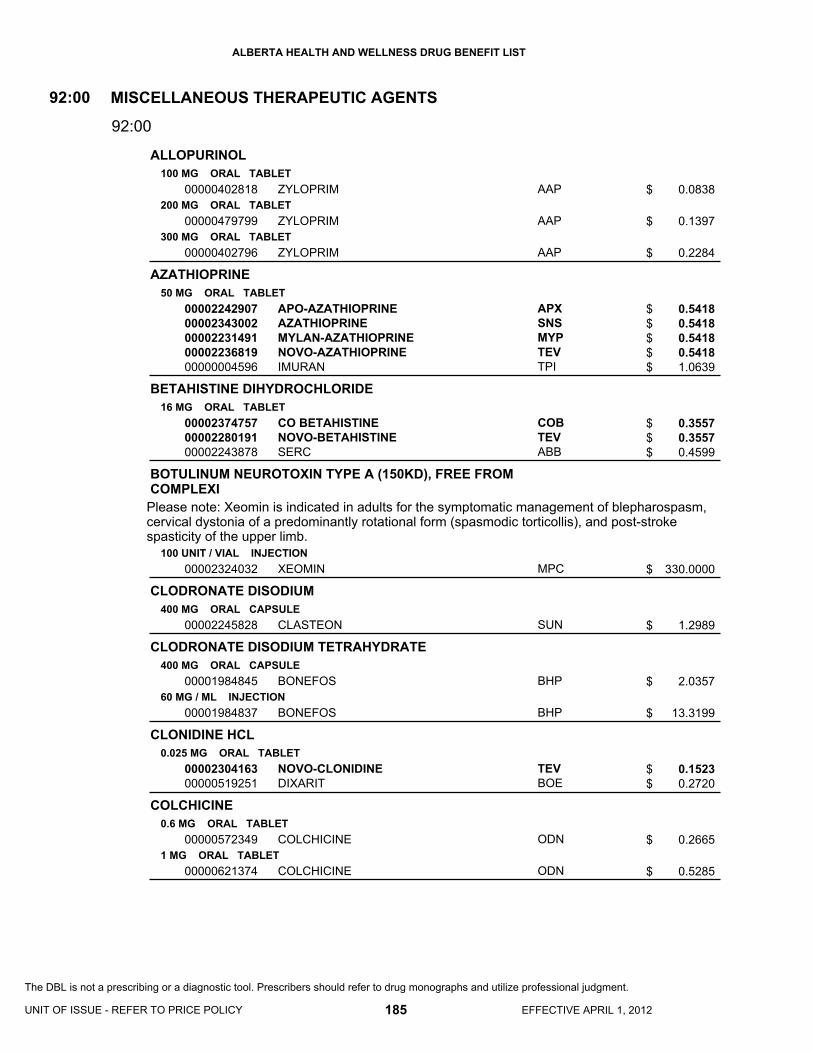
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
ALLOPURINOL
AZATHIOPRINE
BETAHISTINE DIHYDROCHLORIDE
BOTULINUM NEUROTOXIN TYPE A (150KD), FREE FROM COMPLEXI
CLODRONATE DISODIUM
CLODRONATE DISODIUM TETRAHYDRATE
CLONIDINE HCL
COLCHICINE
100 MG ORAL TABLET
200 MG ORAL TABLET
300 MG ORAL TABLET
50 MG ORAL TABLET
16 MG ORAL TABLET
100 UNIT / VIAL INJECTION
400 MG ORAL CAPSULE
400 MG ORAL CAPSULE
60 MG / ML INJECTION
0.025 MG ORAL TABLET
0.6 MG ORAL TABLET
1 MG ORAL TABLET
00000402818
00000479799
00000402796
0000224290700002343002000022314910000223681900000004596
000023747570000228019100002243878
00002324032
00002245828
00001984845
00001984837
0000230416300000519251
00000572349
00000621374
ZYLOPRIM
ZYLOPRIM
ZYLOPRIM
APO-AZATHIOPRINEAZATHIOPRINEMYLAN-AZATHIOPRINENOVO-AZATHIOPRINEIMURAN
CO BETAHISTINENOVO-BETAHISTINESERC
XEOMIN
CLASTEON
BONEFOS
BONEFOS
NOVO-CLONIDINEDIXARIT
COLCHICINE
COLCHICINE
AAP
AAP
AAP
APXSNSMYPTEVTPI
COBTEVABB
MPC
SUN
BHP
BHP
TEVBOE
ODN
ODN
MISCELLANEOUS THERAPEUTIC AGENTS92:00
92:00
0.0838
0.1397
0.2284
0.5418 0.5418 0.5418 0.5418 1.0639
0.3557 0.3557 0.4599
330.0000
1.2989
2.0357
13.3199
0.1523 0.2720
0.2665
0.5285
185 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$
$$$$$
$$$
$
$
$
$
$$
$
$
Please note: Xeomin is indicated in adults for the symptomatic management of blepharospasm,cervical dystonia of a predominantly rotational form (spasmodic torticollis), and post-stroke spasticity of the upper limb.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
PRODUCT IS NOT INTERCHANGEABLE
COMPOUND PRESCRIPTION
DIMETHYL SULFOXIDE
ETIDRONATE DISODIUM
ETIDRONATE DISODIUM/ CALCIUM CARBONATE
FLUNARIZINE HCL
LEUCOVORIN CALCIUM
INJECTION
INJECTION
ORAL
ORAL
50 % BLADDER IRRIGATION SOLUTION
200 MG ORAL TABLET
400 MG * 500 MG ORAL TABLET
5 MG (BASE) ORAL CAPSULE
5 MG (BASE) ORAL TABLET
10 MG / ML INJECTION
00000999114
00000999215
00000999999
00000999216
00000999214
00000999113
0000224323100000493392
0000224868600002245330
0000226386600002353210000022473230000232419900002176017
00002246082
00002170493
00002087316
MISCELLANEOUS INJECTABLE COMPOUND
MISCELLANEOUS INJECTABLE COMPOUND
MISCELLANEOUS COMPOUND
MISCELLANEOUS COMPOUND
MISCELLANEOUS ORAL COMPOUND
MISCELLANEOUS ORAL COMPOUND
DIMETHYL SULFOXIDE IRRIGATIONRIMSO-50
CO ETIDRONATEMYLAN-ETIDRONATE
CO ETIDROCALETIDROCALMYLAN-ETI-CAL-CAREPACNOVO-ETIDRONATECALDIDROCAL
FLUNARIZINE
LEDERLE LEUCOVORIN CALCIUM
LEUCOVORIN CALCIUM
XXX
XXX
XXX
XXX
XXX
XXX
SDZALV
COBMYP
COBSNSMYPTEVWCC
AAP
WAY
TEV
MISCELLANEOUS THERAPEUTIC AGENTS92:00
92:00
0.0000
0.0000
0.0000
0.0000
0.0000
0.0000
1.1840 1.1900
0.8257 0.8257
0.2808 0.2808 0.2808 0.2808 0.5235
0.7744
6.6605
10.9270
186 EFFECTIVE APRIL 1, 2012
$
$
$
$
$
$
$$
$$
$$$$$
$
$
$
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
To be used when the compound has been procured from a licensed compounding and repackaging pharmacy and dispensed by a licensed community pharmacy.
To be used when the compound has been prepared and dispensed by a licensed community pharmacy.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
NAFARELIN ACETATE
ONABOTULINUMTOXINA
PAMIDRONATE DISODIUM
PENTOSAN POLYSULFATE SODIUM
LEFLUNOMIDE
2 MG / ML (BASE) NASAL SOLUTION
INJECTION
30 MG / VIAL INJECTION
60 MG / VIAL INJECTION
90 MG / VIAL INJECTION
100 MG ORAL CAPSULE
10 MG ORAL TABLET
20 MG ORAL TABLET
00002188783
00001981501
00002244550000022649510000224966900002059762
0000224455100002264978
00002244552000022649860000224968500002059789
00002029448
0000225649500002351668000022612510000228396400002241888
0000225650900002351676000022612780000228397200002241889
SYNAREL
BOTOX (50/100/200 UNITS/VIAL)
PAMIDRONATE DISODIUMPAMIDRONATE DISODIUMPAMIDRONATE DISODIUM OMEGAAREDIA
PAMIDRONATE DISODIUMPAMIDRONATE DISODIUM
PAMIDRONATE DISODIUMPAMIDRONATE DISODIUMPAMIDRONATE DISODIUM OMEGAAREDIA
ELMIRON
APO-LEFLUNOMIDELEFLUNOMIDENOVO-LEFLUNOMIDESANDOZ LEFLUNOMIDEARAVA
APO-LEFLUNOMIDELEFLUNOMIDENOVO-LEFLUNOMIDESANDOZ LEFLUNOMIDEARAVA
PFI
ALL
HSPSDZOMGNOV
HSPSDZ
HSPSDZOMGNOV
JAI
APXSNSTEVSDZSAV
APXSNSTEVSDZSAV
MISCELLANEOUS THERAPEUTIC AGENTS
MISCELLANEOUS THERAPEUTIC AGENTS
DISEASE-MODIFYING ANTIRHEUMATIC AGENTS
92
92
:00
:00
92:00
92:36
38.4172
3.5700
82.1860 82.1860 82.1860
179.4498
123.2790 123.2791
246.5581 246.5581 246.5581 538.3492
1.7786
6.0417 6.0417 6.0417 6.0417
11.7221
6.0417 6.0417 6.0417 6.0417
11.7275
187 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$
$
$$$$
$$
$$$$
$
$$$$$
$$$$$
For the products within the following three groupings, pricing has been established on a per vialbasis.
RESTRICTED BENEFIT - This product is a benefit for the treatment of rheumatoid arthritis when prescribed by a Specialist in Rheumatology or Internal Medicine.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

94:00 Devices
94:00
Devices

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST
AEROSOL HOLDING CHAMBER
AEROSOL HOLDING CHAMBER/MASK
DEVICE
DEVICE
INFANT DEVICE
PEDIATRIC DEVICE
ADULT DEVICE
DEVICE
0000099001400000990095
000009900800000099008900000990088000009901000000099009900000990091
000009900810000099001500000990096
00000990092
000009900820000099001600000990097
00000990093
0000099001700000990098
00000990094
00000999949
SPACE CHAMBEROPTICHAMBER ADVANTAGE II (CHAMBER ONLY)VORTEXAEROCHAMBER AC BOYZ CHAMBERAEROCHAMBER AC GIRLZ CHAMBERAEROCHAMBER AC BOYZ CHAMBERAEROCHAMBER AC GIRLZ CHAMBERAEROCHAMBER PLUS FLOW-VU W/ MOUTHPIECE
VORTEX BABY WHIRL INFANT MASKSPACE CHAMBER INFANT MASKOPTICHAMBER ADVANTAGE II (WITH SMALL MASK)AEROCHAMBER PLUS FLOW-VU W/ SMALL MASK
VORTEX SPINNER PEDIATRIC MASKSPACE CHAMBER PEDIATRIC MASKOPTICHAMBER ADVANTAGE II (WITH MEDIUM MASK)AEROCHAMBER PLUS FLOW-VU W/ MEDIUMMASK
SPACE CHAMBER ADULT MASKOPTICHAMBER ADVANTAGE II (WITH LARGEMASK)AEROCHAMBER PLUS FLOW-VU W/ LARGE MASK
SEREVENT DISKHALER
KGHACM
KGHTMITMITMITMITMI
KGHKGHACM
TMI
KGHKGHACM
TMI
KGHACM
TMI
GSK
DEVICES94:00
94:00
12.9000 15.6000
20.9600 21.5400 21.5400 23.5500 23.5500 23.5500
9.1400 13.9800 26.8000
37.6700
9.1400 13.9800 26.8000
37.6700
13.9800 29.6000
39.8600
5.8695
189 EFFECTIVE APRIL 1, 2012UNIT OF ISSUE - REFER TO PRICE POLICY
$$
$$$$$$
$$$
$
$$$
$
$$
$
$
RESTRICTED BENEFIT - Coverage is limited to one aerosol holding chamber per plan participant per year.
RESTRICTED BENEFIT - Coverage is limited to one of each size (infant, pediatric, adult) aerosol holding chamber mask or chamber w/ mask per plan participant per year.
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.

Appendices
Appendices
Abbreviations Pharmaceutical Manufacturers

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST APPENDIX 1 - ABBREVIATIONS
Appendix 1 Abbreviations
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 190 EFFECTIVE APRIL 1, 2012
ASA ........................................... acetylsalicylic acid ENM ........................................... enema FC .............................................. film coated G ................................................ gram(s) HCL............................................ hydrochloride
HR .............................................. hour IU ............................................... international unit(s) MCG........................................... microgram MEQ ........................................... milliequivalent
MG ............................................. milligram ML .............................................. millilitre PTH ............................................ patch SYR............................................ syringe
W................................................ with % ................................................ percent

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST APPENDIX 2 - PHARMACEUTICAL MANUFACTURERS
Appendix 2 Pharmaceutical Manufacturers
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 191 EFFECTIVE APRIL 1, 2012
0BA
AAP AA Pharma Inc. ABB Abbott Laboratories Limited ACV Actavis ACM Auto Control Medical Inc. ACP Accel Pharma Inc. AHI Accord Healthcare Inc. ALC Alcon Canada Inc. ALL Allergan Inc. ALV Alveda Pharmaceuticals Inc. AMG Amgen Inc. API Alexion Pharmaceuticals, Inc. APX Apotex Inc. ASP Astellas Pharma Canada, Inc. ATP Aton Pharma Inc. AUR Auro Pharma Inc. AVA Avanstra Inc. AXC Axcan Pharma Inc. AZC AstraZeneca Canada Inc.
1BB BAI Bayer Inc. BAR Barr laboratories, Inc. BAX Baxter Corporation BHP Bayer Healthcare Pharmaceuticals BIO Biogen Idec Canada Inc BMS Bristol-Myers Squibb BOE Boehringer Ingelheim (Canada) Ltd. BVM Biovitrum AB
2BC COB Cobalt Pharmaceuticals Inc. COR Corepharma LLC CYT Cytex Pharmaceuticals Inc.
3BD DUI Duchesnay Inc. DUR Duramed Pharmaceuticals Inc.
4BE ERF ERFA Canada Inc. ETP Ethypharm Inc.
5BF FAB Fournier/Abbott Laboratories Limited FEI Ferring Inc.
6BG GAL Galderma Canada Inc. GIL Gilead Sciences Inc. GKC GlaxoSmithKline Consumer Healthcare
GLE Glenwood Laboratories Canada Ltd. GMD Genmed, a Division of Pfizer Canada Inc. GSK GlaxoSmithKline GZM Genzyme Canada Inc.
7BH HLR Hoffman-La Roche Limited HPC Healthpoint Canada ULC HSP Hospira Healthcare Corporation 8BJ JAI Janssen Inc. JHP JHP Pharmaceuticals, LLC JPC Jamp Pharma Corporation
9BK KGH Kego Healthcare KNG King Pharmaceuticals Canada Inc.
10BL LBC Lundbeck Canada Inc. LEO Leo Pharma Inc. LIL Eli Lilly Canada Inc. LUI Lundbeck Inc.
11BM MAR Marcan Pharmaceuticals Inc MEL Meliapharm Inc. MEP Medicis Pharmaceutical Corporation MFC Merck Canada Inc. MLI Merus Labs Inc. MMT MM Therapeutics Inc. MPC Merz Pharma Canada Ltd. MPI Mint Pharmaceuticals Inc. MYP Mylan Pharmaceuticals ULC
12BN NNA Novo Nordisk Canada Inc. NOV Novartis Pharmaceuticals Canada Inc. NPA Novo Nordisk Canada/Paladin Labs NTI Nucro-Technics Incorporated NXP Nu-Pharm Inc. NYC Nycomed Canada Inc.
13BO ODN Odan Laboratories Ltd. OMG Omega Laboratories Ltd. ORG Organon Canada Ltd.
14BP PAL Paladin Labs Inc. PAT Patriot, a Division of Janssen Inc. PFI Pfizer Canada Inc. PHH Pharmel Inc.

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST REFRESHED APPENDIX 2 - PHARMACEUTICAL MANUFACTURERS
Appendix 2 Pharmaceutical Manufacturers
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 192 EFFECTIVE APRIL 1, 2012
PMS Pharmascience Inc. PPC Pharmaceutical Partners of Canada, a
Division of Abraxis Bioscience Inc. PPH Pendopharm Inc. PUR Purdue Pharma
15BR
RAN Ranbaxy Pharmaceuticals Canada Inc RBC Reckitt Benckiser (Canada) Inc. ROG Rougier Pharma Inc. (Div. of ratiopharm) RPH ratiopharm
16BS SAV Sanofi-Aventis SDZ Sandoz Canada Inc. SEP Septa Pharmaceuticals Inc. SEV Servier Canada Inc. SHB Shire Canada Inc. SNS Sanis Health Inc. SPG Sun Pharma Global Fze SRO EMD Serono Canada Inc. STM Sterimax Inc. SUN Sunovion Pharmaceutical Inc.
T TAK Takeda Canada, Inc. TAR Taro Pharmaceuticals Inc. TCI Tercica, Inc. TEV Teva Canada Limited TMI Trudell Medical International TMP Teva Canada Innovation TPI Triton Pharma Inc. TPT Taropharma, a Div. of Taro
Pharmaceuticals Inc.
17BU
UCB UCB Pharma Canada Inc.
18BV VCL Valeant Canada Limittee/Limited VLP Valeo Pharma Inc.
19BW WAY Wyeth Pharmaceuticals WCC Warner Chilcott Canada Co. WSD Westwood Squibb (Div. Bristol-Myers Squibb
Canada) WSP Wellspring Pharmaceutical Canada Corp.
20BX XPI Xediton Pharmaceuticals Inc. XXX Miscellaneous Manufacturers
21BZ ZMC Zymcan Pharmaceuticals Inc.

Indices
Indices
Alphabetical List of Pharmaceutical Products
Numerical List by Drug Identification Number

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 193
NUMERIC
282 .................................................................................... 75 282 MEP ........................................................................... 75 292 .................................................................................... 75 5-AMINOSALICYLIC ACID ………………………………150 5-FLUOROURACIL ......................................................... 179
A
ABATACEPT ............................................................ SEC 3.6 ABILIFY ............................................................................. 97 ACARBOSE .................................................................... 162 ACCEL PIOGLITAZONE ........................................ SEC 3.71 ACCOLATE ..................................................................... 129 ACCOLATE ............................................................ SEC 3.92 ACCUPRIL ........................................................................ 60 ACCUPRIL ........................................................................ 61 ACCURETIC 10/12.5 ........................................................ 61 ACCURETIC 20/12.5 ........................................................ 61 ACCURETIC 20/25 ........................................................... 61 ACCUTANE .................................................................... 179 ACEBUTOLOL .................................................................. 46 ACEBUTOLOL HCL .......................................................... 46 ACENOCOUMAROL ......................................................... 27 ACETAZOLAMIDE .......................................................... 136 ACETYLCYSTEINE ........................................................ 130 ACITRETIN ..................................................................... 179 ACLASTA ............................................................... SEC 3.92 ACTEMRA (10 ML) ................................................ SEC 3.87 ACTEMRA (20 ML) ................................................ SEC 3.87 ACTEMRA (4 ML) .................................................. SEC 3.87 ACTONEL .............................................................. SEC 3.74 ACTOS ................................................................... SEC 3.71 ACULAR .......................................................................... 134 ACYCLOVIR ..................................................................... 16 ADALAT XL ....................................................................... 53 ADALIMUMAB ....................................................... SEC 3.13 ADEFOVIR DIPIVOXIL ..................................................... 16 ADRENALIN .................................................................... 135 ADRENALIN ...................................................................... 24 ADVAIR 100 DISKUS ........................................................ 24 ADVAIR 125 ...................................................................... 23 ADVAIR 250 ...................................................................... 23 ADVAIR 250 DISKUS ........................................................ 24 ADVAIR 500 DISKUS ........................................................ 24 AEROCHAMBER AC BOYZ CHAMBER ......................... 189 AEROCHAMBER AC GIRLZ CHAMBER ........................ 189 AEROCHAMBER PLUS FLOW-VU W/ LARGE MASK ... 189 AEROCHAMBER PLUS FLOW-VU W/ MOUTHPIECE .. 189 AEROCHAMBER PLUS FLOW-VU W/ SMALL MASK ... 189
AEROSOL HOLDING CHAMBER .................................... 189 AEROSOL HOLDING CHAMBER/MASK ........................ 189 AGGRENOX ...................................................................... 30 AIROMIR CFC-FREE ......................................................... 23 ALCAINE .......................................................................... 134 ALDACTAZIDE 25 ............................................................. 67 ALDACTAZIDE 50 ............................................................. 67 ALDACTONE ..................................................................... 67 ALDARA ................................................................. SEC 3.46 ALENDRONATE .................................................... SEC 3.14 ALENDRONATE SODIUM ..................................... SEC 3.14 ALENDRONATE SODIUM/ VITAMIN D3 ............... SEC 3.15 ALENDRONATE-FC .............................................. SEC 3.14 ALERTEC .............................................................. SEC 3.58 ALERTONIC..................................................................... 184 ALESSE (21 DAY) ........................................................... 159 ALESSE (28 DAY) ........................................................... 159 ALFACALCIDOL .............................................................. 183 ALFUZOSIN HCL ................................................... SEC 3.15 ALLERGY SERUM ........................................................... 169 ALLOPURINOL ................................................................ 185 ALPHAGAN ..................................................................... 135 ALPRAZOLAM ................................................................. 109 ALPROSTADIL .................................................................. 43 ALTACE (CAPSULE) ......................................................... 61 ALTACE (CAPSULE) ......................................................... 62 ALTACE HCT ..................................................................... 62 ALVESCO ........................................................................ 155 AMANTADINE HCL ......................................................... 115 AMCINONIDE .................................................................. 173 AMERGE ......................................................................... 113 AMERGE ............................................................... SEC 3.60 AMILORIDE HCL ............................................................. 126 AMINOBENZOATE POTASSIUM .................................... 179 AMINOPHYLLINE ............................................................ 181 AMIODARONE................................................................... 34 AMIODARONE HCL .......................................................... 34 AMITRIPTYLINE HCL ........................................................ 94 AMLODIPINE ..................................................................... 52 AMLODIPINE BESYLATE ................................................. 52 AMOXICILLIN ......................................................................8 AMOXICILLIN ......................................................................9 AMOXICILLIN SUGAR-REDUCED ......................................9 AMOXICILLIN TRIHYDRATE...............................................8 AMOXICILLIN TRIHYDRATE...............................................9 AMOXICILLIN TRIHYDRATE/ CLAVULANATE
POTASSIUM ...................................................................9 AMPHOTERICIN B ............................................................ 15

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 194 EFFECTIVE APRIL 1, 2012
AMPICILLIN ........................................................... SEC 3.15 AMPICILLIN SODIUM ....................................................... 10 AMPICILLIN SODIUM ......................................................... 9 ANAFRANIL ...................................................................... 94 ANAKINRA ............................................................. SEC 3.17 ANAPROX ......................................................................... 74 ANAPROX DS ................................................................... 74 ANDRIOL ............................................................... SEC 3.84 ANDROCUR .......................................................... SEC 3.21 ANDROCUR DEPOT ............................................. SEC 3.21 ANDRODERM (2.5 MG/DAY) ................................ SEC 3.84 ANDRODERM (5 MG/DAY) ................................... SEC 3.84 ANODAN-HC .................................................................. 177 ANZEMET ....................................................................... 142 APIDRA ........................................................................... 163 APIDRA CARTRIDGE ..................................................... 163 APIDRA PEN .................................................................. 163 APO-ACEBUTOLOL ......................................................... 46 APO-ACYCLOVIR ............................................................. 16 APO-ALENDRONATE ............................................ SEC 3.14 APO-ALFUZOSIN .................................................. SEC 3.15 APO-ALPRAZ ................................................................. 109 APO-AMILZIDE ............................................................... 126 APO-AMIODARONE ......................................................... 34 APO-AMLODIPINE ........................................................... 52 APO-AMOXI ........................................................................ 8 APO-AMOXI ........................................................................ 9 APO-AMOXI CLAV.............................................................. 9 APO-ATENIDONE............................................................. 47 APO-ATENOL ................................................................... 46 APO-ATENOL ................................................................... 47 APO-ATORVASTATIN ...................................................... 36 APO-AZATHIOPRINE ..................................................... 185 APO-AZITHROMYCIN ........................................................ 7 APO-BACLOFEN .............................................................. 25 APO-BECLOMETHASONE ............................................. 132 APO-BENZYDAMINE ...................................................... 135 APO-BISOPROLOL .......................................................... 47 APO-BRIMONIDINE ........................................................ 135 APO-BROMAZEPAM ...................................................... 109 APO-BROMOCRIPTINE ................................................. 117 APO-BUSPIRONE .......................................................... 111 APO-CALCITONIN ................................................. SEC 3.83 APO-CANDESARTAN ...................................................... 63 APO-CAPTO ..................................................................... 56 APO-CARBAMAZEPINE ................................................... 83 APO-CARVEDILOL ........................................................... 48 APO-CEFADROXIL................................................ SEC 3.19 APO-CEFPROZIL ............................................................... 4 APO-CEFUROXIME ............................................................ 5 APO-CEPHALEX ................................................................ 3 APO-CHLORAX .............................................................. 109
APO-CHLORDIAZEPOXIDE ............................................ 109 APO-CILAZAPRIL .............................................................. 56 APO-CILAZAPRIL .............................................................. 57 APO-CILAZAPRIL/HCTZ ................................................... 57 APO-CIMETIDINE ............................................................ 144 APO-CIPROFLOX .................................................. SEC 3A.2 APO-CIPROFLOX .................................................. SEC 3A.3 APO-CITALOPRAM ........................................................... 90 APO-CLINDAMYCIN .......................................................... 13 APO-CLOBAZAM ............................................................... 81 APO-CLOMIPRAMINE ....................................................... 94 APO-CLONAZEPAM .......................................................... 82 APO-CLONIDINE ............................................................... 40 APO-CLOPIDOGREL ............................................ SEC 3.20 APO-CLORAZEPATE ...................................................... 109 APO-CLOZAPINE .............................................................. 97 APO-CLOZAPINE .............................................................. 98 APO-CYCLOBENZAPRINE ............................................... 25 APO-CYCLOSPORINE .......................................... SEC 3.21 APO-DESIPRAMINE .......................................................... 94 APO-DESMOPRESSIN ................................................... 166 APO-DEXAMETHASONE ................................................ 156 APO-DIAZEPAM .............................................................. 109 APO-DIAZEPAM .............................................................. 110 APO-DICLO ....................................................................... 70 APO-DICLO SR ................................................................. 70 APO-DIFLUNISAL .............................................................. 71 APO-DILTIAZ ..................................................................... 53 APO-DILTIAZ CD ............................................................... 54 APO-DILTIAZ TZ ................................................................ 54 APO-DILTIAZ TZ ................................................................ 55 APO-DIPYRIDAMOLE (FC) ............................................... 43 APO-DIVALPROEX ........................................................... 84 APO-DOMPERIDONE ..................................................... 149 APO-DORZO-TIMOP ....................................................... 138 APO-DORZOLAMIDE ...................................................... 136 APO-DOXAZOSIN ............................................................. 44 APO-DOXEPIN .................................................................. 94 APO-DOXEPIN .................................................................. 95 APO-DOXY ........................................................................ 11 APO-ENALAPRIL ............................................................... 57 APO-ENALAPRIL ............................................................... 58 APO-ENALAPRIL MALEATE/HCTZ .................................. 58 APO-FAMOTIDINE .......................................................... 145 APO-FENO-MICRO ........................................................... 35 APO-FENO-SUPER ........................................................... 35 APO-FENO-SUPER (TABLET) .......................................... 35 APO-FENOFIBRATE ......................................................... 35 APO-FINASTERIDE ............................................... SEC 3.40 APO-FLUCONAZOLE ........................................................ 14 APO-FLUNISOLIDE ......................................................... 132 APO-FLUOXETINE ............................................................ 91

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 195
APO-FLUPHENAZINE .................................................... 104 APO-FLUPHENAZINE .................................................... 105 APO-FLURAZEPAM ....................................................... 110 APO-FLURBIPROFEN ...................................................... 71 APO-FLUTAMIDE .................................................. SEC 3.41 APO-FLUVOXAMINE ........................................................ 91 APO-FOLIC ..................................................................... 183 APO-FOSINOPRIL ............................................................ 58 APO-FUROSEMIDE .......................................................... 41 APO-GABAPENTIN .......................................................... 84 APO-GABAPENTIN .......................................................... 85 APO-GEMFIBROZIL ......................................................... 35 APO-GLICLAZIDE........................................................... 164 APO-GLYBURIDE ........................................................... 165 APO-HALOPERIDOL ...................................................... 103 APO-HALOPERIDOL ...................................................... 104 APO-HYDRALAZINE ........................................................ 41 APO-HYDRO .................................................................. 126 APO-HYDROXYQUINE .................................................... 17 APO-HYDROXYZINE ...................................................... 112 APO-IBUPROFEN............................................................. 71 APO-INDAPAMIDE ......................................................... 127 APO-INDOMETHACIN ...................................................... 71 APO-IPRAVENT................................................................ 22 APO-ISMN ........................................................................ 42 APO-K ............................................................................. 125 APO-KETOCONAZOLE .................................................... 14 APO-KETOROLAC ......................................................... 134 APO-KETOROLAC ........................................................... 72 APO-LACTULOSE .......................................................... 125 APO-LAMOTRIGINE ......................................................... 85 APO-LANSOPRAZOLE ................................................... 147 APO-LATANOPROST ..................................................... 137 APO-LEFLUNOMIDE ...................................................... 187 APO-LEVETIRACETAM .................................................... 86 APO-LEVOCARB ............................................................ 117 APO-LEVOFLOXACIN ........................................... SEC 3A.4 APO-LISINOPRIL .............................................................. 59 APO-LISINOPRIL/HCTZ ................................................... 60 APO-LITHIUM CARBONATE .......................................... 113 APO-LORAZEPAM ......................................................... 110 APO-LOVASTATIN ........................................................... 37 APO-MEDROXY ............................................................. 166 APO-METFORMIN .......................................................... 162 APO-METHOPRAZINE ................................................... 105 APO-METHOTREXATE .................................................... 19 APO-METHYLPHENIDATE ............................................ 108 APO-METHYLPHENIDATE SR ...................................... 108 APO-METOCLOP ........................................................... 149 APO-METOPROLOL ......................................................... 49 APO-METOPROLOL (TYPE L) ......................................... 49 APO-METOPROLOL SR ................................................... 49
APO-MINOCYCLINE ......................................................... 12 APO-MIRTAZAPINE .......................................................... 97 APO-MOCLOBEMIDE ....................................................... 88 APO-MONTELUKAST ..................................................... 129 APO-MONTELUKAST ........................................... SEC 3.59 APO-NABUMETONE ......................................................... 72 APO-NADOL ...................................................................... 49 APO-NAPRO-NA ............................................................... 74 APO-NAPRO-NA DS ......................................................... 74 APO-NAPROXEN .............................................................. 72 APO-NAPROXEN .............................................................. 73 APO-NAPROXEN EC ........................................................ 73 APO-NITRAZEPAM ......................................................... 111 APO-NIZATIDINE ............................................................ 145 APO-NORFLOX ................................................................. 10 APO-NORTRIPTYLINE ...................................................... 95 APO-OFLOXACIN ............................................................ 131 APO-OLANZAPINE ............................................................ 98 APO-OLANZAPINE ............................................................ 99 APO-OLANZAPINE ODT ................................................... 99 APO-OMEPRAZOLE (CAPSULE) ................................... 148 APO-ONDANSETRON .................................................... 143 APO-ORCIPRENALINE ..................................................... 23 APO-OXAZEPAM ............................................................ 111 APO-OXYBUTYNIN ......................................................... 181 APO-OXYCODONE ........................................................... 80 APO-PANTOPRAZOLE ................................................... 148 APO-PAROXETINE ........................................................... 92 APO-PEN-VK .......................................................................8 APO-PENTOXIFYLLINE SR .............................................. 31 APO-PIMOZIDE ............................................................... 107 APO-PINDOL ..................................................................... 50 APO-PIOGLITAZONE ............................................ SEC 3.71 APO-PIROXICAM .............................................................. 74 APO-PRAMIPEXOLE ....................................................... 118 APO-PRAVASTATIN ......................................................... 38 APO-PRAZO ...................................................................... 44 APO-PREDNISONE ......................................................... 158 APO-PROCHLORAZINE ................................................. 142 APO-PROPAFENONE ....................................................... 33 APO-PROPRANOLOL ....................................................... 50 APO-QUETIAPINE ........................................................... 100 APO-QUETIAPINE ............................................................. 99 APO-QUININE ................................................................... 18 APO-RABEPRAZOLE ...................................................... 149 APO-RALOXIFENE ................................................ SEC 3.73 APO-RAMIPRIL (CAPSULE) ............................................. 61 APO-RAMIPRIL (CAPSULE) ............................................. 62 APO-RANITIDINE ............................................................ 146 APO-REPAGLINIDE ........................................................ 164 APO-RISEDRONATE ............................................ SEC 3.74 APO-RISPERIDONE ........................................................ 101
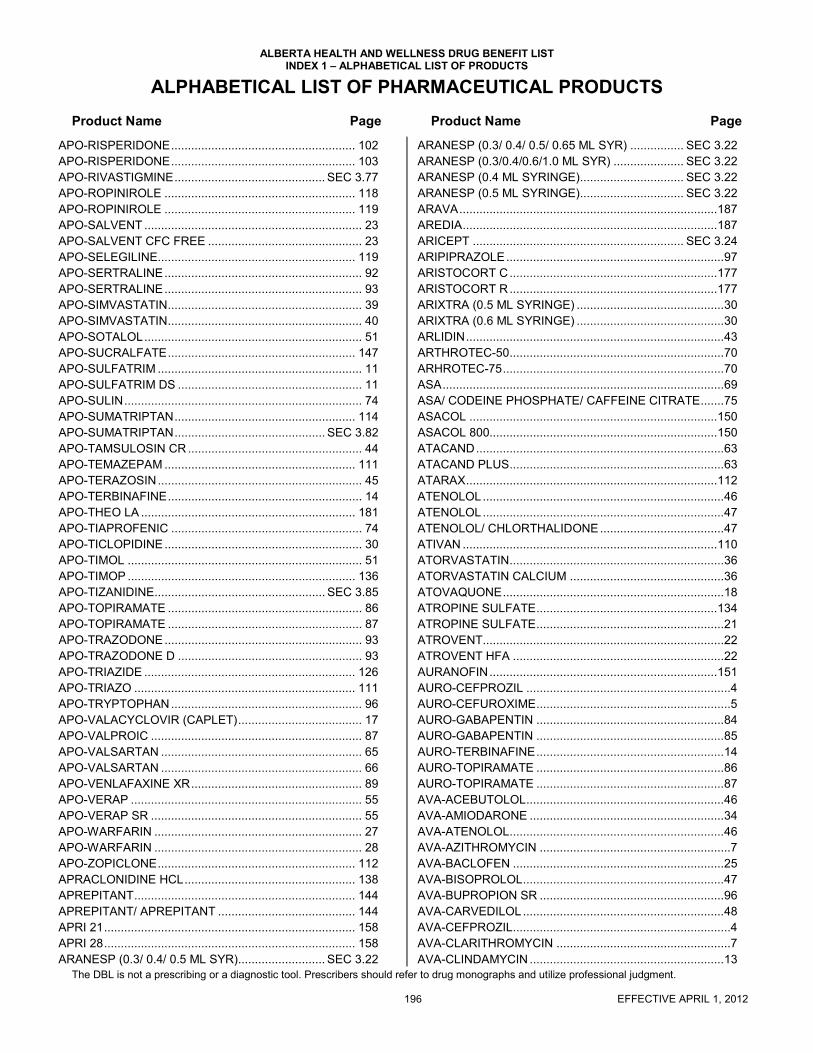
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 196 EFFECTIVE APRIL 1, 2012
APO-RISPERIDONE ....................................................... 102 APO-RISPERIDONE ....................................................... 103 APO-RIVASTIGMINE ............................................. SEC 3.77 APO-ROPINIROLE ......................................................... 118 APO-ROPINIROLE ......................................................... 119 APO-SALVENT ................................................................. 23 APO-SALVENT CFC FREE .............................................. 23 APO-SELEGILINE........................................................... 119 APO-SERTRALINE ........................................................... 92 APO-SERTRALINE ........................................................... 93 APO-SIMVASTATIN .......................................................... 39 APO-SIMVASTATIN .......................................................... 40 APO-SOTALOL ................................................................. 51 APO-SUCRALFATE ........................................................ 147 APO-SULFATRIM ............................................................. 11 APO-SULFATRIM DS ....................................................... 11 APO-SULIN ....................................................................... 74 APO-SUMATRIPTAN ...................................................... 114 APO-SUMATRIPTAN ............................................. SEC 3.82 APO-TAMSULOSIN CR .................................................... 44 APO-TEMAZEPAM ......................................................... 111 APO-TERAZOSIN ............................................................. 45 APO-TERBINAFINE .......................................................... 14 APO-THEO LA ................................................................ 181 APO-TIAPROFENIC ......................................................... 74 APO-TICLOPIDINE ........................................................... 30 APO-TIMOL ...................................................................... 51 APO-TIMOP .................................................................... 136 APO-TIZANIDINE................................................... SEC 3.85 APO-TOPIRAMATE .......................................................... 86 APO-TOPIRAMATE .......................................................... 87 APO-TRAZODONE ........................................................... 93 APO-TRAZODONE D ....................................................... 93 APO-TRIAZIDE ............................................................... 126 APO-TRIAZO .................................................................. 111 APO-TRYPTOPHAN ......................................................... 96 APO-VALACYCLOVIR (CAPLET) ..................................... 17 APO-VALPROIC ............................................................... 87 APO-VALSARTAN ............................................................ 65 APO-VALSARTAN ............................................................ 66 APO-VENLAFAXINE XR ................................................... 89 APO-VERAP ..................................................................... 55 APO-VERAP SR ............................................................... 55 APO-WARFARIN .............................................................. 27 APO-WARFARIN .............................................................. 28 APO-ZOPICLONE ........................................................... 112 APRACLONIDINE HCL ................................................... 138 APREPITANT .................................................................. 144 APREPITANT/ APREPITANT ......................................... 144 APRI 21 ........................................................................... 158 APRI 28 ........................................................................... 158 ARANESP (0.3/ 0.4/ 0.5 ML SYR).......................... SEC 3.22
ARANESP (0.3/ 0.4/ 0.5/ 0.65 ML SYR) ................ SEC 3.22 ARANESP (0.3/0.4/0.6/1.0 ML SYR) ..................... SEC 3.22 ARANESP (0.4 ML SYRINGE)............................... SEC 3.22 ARANESP (0.5 ML SYRINGE)............................... SEC 3.22 ARAVA ............................................................................. 187 AREDIA ............................................................................ 187 ARICEPT ............................................................... SEC 3.24 ARIPIPRAZOLE ................................................................. 97 ARISTOCORT C .............................................................. 177 ARISTOCORT R .............................................................. 177 ARIXTRA (0.5 ML SYRINGE) ............................................ 30 ARIXTRA (0.6 ML SYRINGE) ............................................ 30 ARLIDIN ............................................................................. 43 ARTHROTEC-50 ................................................................ 70 ARHROTEC-75 .................................................................. 70 ASA .................................................................................... 69 ASA/ CODEINE PHOSPHATE/ CAFFEINE CITRATE ....... 75 ASACOL .......................................................................... 150 ASACOL 800.................................................................... 150 ATACAND .......................................................................... 63 ATACAND PLUS ................................................................ 63 ATARAX ........................................................................... 112 ATENOLOL ........................................................................ 46 ATENOLOL ........................................................................ 47 ATENOLOL/ CHLORTHALIDONE ..................................... 47 ATIVAN ............................................................................ 110 ATORVASTATIN ................................................................ 36 ATORVASTATIN CALCIUM .............................................. 36 ATOVAQUONE .................................................................. 18 ATROPINE SULFATE ...................................................... 134 ATROPINE SULFATE ........................................................ 21 ATROVENT........................................................................ 22 ATROVENT HFA ............................................................... 22 AURANOFIN .................................................................... 151 AURO-CEFPROZIL .............................................................4 AURO-CEFUROXIME ..........................................................5 AURO-GABAPENTIN ........................................................ 84 AURO-GABAPENTIN ........................................................ 85 AURO-TERBINAFINE ........................................................ 14 AURO-TOPIRAMATE ........................................................ 86 AURO-TOPIRAMATE ........................................................ 87 AVA-ACEBUTOLOL ........................................................... 46 AVA-AMIODARONE .......................................................... 34 AVA-ATENOLOL ................................................................ 46 AVA-AZITHROMYCIN .........................................................7 AVA-BACLOFEN ............................................................... 25 AVA-BISOPROLOL ............................................................ 47 AVA-BUPROPION SR ....................................................... 96 AVA-CARVEDILOL ............................................................ 48 AVA-CEFPROZIL .................................................................4 AVA-CLARITHROMYCIN ....................................................7 AVA-CLINDAMYCIN .......................................................... 13

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 197
AVA-DICLOFENAC ........................................................... 70 AVA-DICLOFENAC SR ..................................................... 70 AVA-DOMPERIDONE ..................................................... 149 AVA-ENALAPRIL .............................................................. 57 AVA-ENALAPRIL .............................................................. 58 AVA-FAMOTIDINE .......................................................... 145 AVA-FENOFIBRATE MICRO ............................................ 35 AVA-FLUOXETINE ........................................................... 91 AVA-FLUVOXAMINE ........................................................ 91 AVA-FUROSEMIDE .......................................................... 41 AVA-GLICLAZIDE ........................................................... 164 AVA-GLYBURIDE ........................................................... 165 AVA-HYDROCHLOROTHIAZIDE ................................... 126 AVA-IRBESARTAN ........................................................... 63 AVA-IRBESARTAN ........................................................... 64 AVA-IRBESARTAN/HCTZ ................................................ 64 AVA-LEVETIRACETAM .................................................... 86 AVA-LEVOFLOXACIN ........................................... SEC 3A.4 AVA-LISINOPRIL HCT ...................................................... 60 AVA-LOVASTATIN............................................................ 37 AVA-METFORMIN .......................................................... 162 AVA-METOPROLOL ......................................................... 49 AVA-METOPROLOL (TYPE L) ......................................... 49 AVA-MIRTAZAPINE .......................................................... 97 AVA-NAPROXEN .............................................................. 73 AVA-NAPROXEN EC ........................................................ 73 AVA-NORFLOXACIN ........................................................ 10 AVA-NORTRIPTYLINE ..................................................... 95 AVA-OLANZAPINE ........................................................... 98 AVA-PANTOPRAZOLE ................................................... 148 AVA-PIOGLITAZONE ............................................ SEC 3.71 AVA-PRAMIPEXOLE ...................................................... 118 AVA-RAMIPRIL (TABLET) ................................................ 61 AVA-RAMIPRIL (TABLET) ................................................ 62 AVA-RISEDRONATE ............................................. SEC 3.74 AVA-RISPERIDONE ....................................................... 101 AVA-RISPERIDONE ....................................................... 102 AVA-RISPERIDONE ....................................................... 103 AVA-SOTALOL ................................................................. 51 AVA-SUMATRIPTAN ...................................................... 114 AVA-SUMATRIPTAN ............................................. SEC 3.82 AVA-TAMSULOSIN CR .................................................... 44 AVA-TOPIRAMATE........................................................... 86 AVA-TOPIRAMATE........................................................... 87 AVA-VALSARTAN............................................................. 65 AVA-VALSARTAN............................................................. 66 AVA-VALSARTAN HCT .................................................... 66 AVA-ZOPICLONE ........................................................... 112 AVALIDE 150/12.5 ............................................................ 64 AVALIDE 300/12.5 ............................................................ 64 AVANDAMET ......................................................... SEC 3.79 AVANDIA ............................................................... SEC 3.78
AVAPRO ............................................................................ 63 AVAPRO ............................................................................ 64 AVELOX ................................................................. SEC 3A.5 AVENTYL ........................................................................... 95 AVIANE 21 ....................................................................... 159 AVIANE 28 ....................................................................... 159 AVODART .............................................................. SEC 3.24 AVONEX (30 MCG) SEC………………………………….. 2.10 AVONEX PS/PEN (30 MCG/0.5 ML)………………. SEC 2.10 AXID ................................................................................. 145 AZARGA .......................................................................... 137 AZATHIOPRINE ............................................................... 185 AZELAIC ACID................................................................. 179 AZITHROMYCIN ..................................................................7 AZITHROMYCIN .................................................... SEC 3.17 AZOPT ............................................................................. 136 AZTREONAM......................................................... SEC 3.17
B
BACLOFEN ........................................................................ 25 BACLOFEN ........................................................................ 26 BACTROBAN ................................................................... 172 BARACLUDE ..................................................................... 16 BECLOMETHASONE DIPROPIONATE .......................... 132 BECLOMETHASONE DIPROPIONATE .......................... 155 BECLOMETHASONE DIPROPIONATE .......................... 173 BELLADONNA/ ERGOTAMINE TARTRATE/
PHENOBARBITAL ......................................................... 21 BELLERGAL SPACETABS ................................................ 21 BENAZEPRIL ..................................................................... 56 BENAZEPRIL HCL ............................................................. 56 BENTYLOL ........................................................................ 21 BENURYL ........................................................................ 127 BENZACLIN ........................................................... SEC 3.19 BENZOYL PEROXIDE ........................................... SEC 3.18 BENZTROPINE ................................................................ 116 BENZTROPINE MESYLATE............................................ 116 BENZTROPINE OMEGA ................................................. 116 BENZYDAMINE HCL ....................................................... 135 BETADERM MILD ............................................................ 173 BETADERM REGULAR ................................................... 173 BETAGAN ........................................................................ 136 BETAHISTINE DIHYDROCHLORIDE .............................. 185 BETAMETHASONE 17-VALERATE ................................ 173 BETAMETHASONE DIPROPIONATE ............................. 174 BETAMETHASONE DIPROPIONATE/ CLOTRIMAZOLE177 BETAMETHASONE DIPROPIONATE/ SALICYLIC ACID174 BETAMETHASONE SODIUM PHOSPHATE ................... 174
BETAMETHASONE SODIUM PHOSPHATE/ BETAMETHASONE ACETATE 155

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 198 EFFECTIVE APRIL 1, 2012
BETAMETHASONE SODIUM PHOSPHATE/ GENTAMICIN SULFATE .................................................................... 133
BETASERON (0.3 MG)………………………….…... SEC 2.10 BETAXOLOL HCL ........................................................... 135 BETNESOL (5MG/100ML) .............................................. 174 BETOPTIC S ................................................................... 135 BEZAFIBRATE .................................................................. 35 BEZALIP ........................................................................... 35 BIAXIN ................................................................................ 7 BIAXIN BID ......................................................................... 7 BIAXIN XL ........................................................................... 7 BIMATOPROST .............................................................. 137 BISOPROLOL FUMARATE .............................................. 47 BLEPHAMIDE ................................................................. 133 BLEPHAMIDE S.O.P. ...................................................... 133 BONEFOS ....................................................................... 185 BOTOX (50/100/200 UNITS/VIAL) .................................. 187 BOTULINUM NEUROTOXIN TYPE A (150KD), FREE FROM
COMPLEXI .................................................................. 185 BREVICON 0.5/35 (21 DAY) ........................................... 160 BREVICON 0.5/35 (28 DAY) ........................................... 160 BREVICON 1/35 (21 DAY) .............................................. 160 BREVICON 1/35 (28 DAY) .............................................. 160 BRICANYL TURBUHALER ............................................... 24 BRIMONIDINE TARTRATE ............................................ 135 BRIMONIDINE TARTRATE/ TIMOLOL MALEATE ......... 137 BRINZOLAMIDE ............................................................. 136 BRINZOLAMIDE/ TIMOLOL MALEATE .......................... 137 BROMAZEPAM ............................................................... 109 BROMOCRIPTINE MESYLATE ...................................... 117 BUDESONIDE ................................................................ 132 BUDESONIDE ................................................................ 155 BUDESONIDE ................................................................ 174 BUDESONIDE ....................................................... SEC 3.18 BUDESONIDE/ FORMOTEROL FUMARATE DIHYDRATE
...................................................................................... 22 BUPRENORPHINE HCL/ NALOXONE HYDROCHLORIDE
DIHYDRATE ................................................................. 81 BUPROPION HCL............................................................. 96 BUSCOPAN ...................................................................... 21 BUSERELIN ACETATE ......................................... SEC 3.18 BUSPIRONE HCL ........................................................... 111 BUTALBITAL/ CAFFEINE/ ASA ........................................ 69 BUTALBITAL/ CODEINE PHOSPHATE/ ASA/ CAFFEINE ........................................................................ 75
C
C.E.S. .............................................................................. 160 CABERGOLINE ..................................................... SEC 3.18 CAFERGOT ...................................................................... 24 CALCIJEX ....................................................................... 183
CALCIMAR ...................................................................... 165 CALCIPOTRIOL ............................................................... 179 CALCIPOTRIOL MONOHYDRATE/ BETAMETHASONE
DIPROPIONATE .......................................................... 179 CALCIPOTRIOL/ BETAMETHASONE DIPROPIONATE . 179 CALCITRIOL .................................................................... 183 CALCIUM POLYSTYRENE SULPHONATE .................... 125 CALTINE 100 (100 IU/ML) ............................................... 165 CANCIDAS ............................................................ SEC 3.19 CANDESARTAN CILEXETIL ............................................. 63 CANDESARTAN CILEXETIL/ HYDROCHLOROTHIAZIDE63 CAPTOPRIL ....................................................................... 56 CARBACHOL ................................................................... 137 CARBAMAZEPINE ............................................................ 83 CARBOLITH..................................................................... 113 CARDIZEM CD .................................................................. 54 CARDURA ......................................................................... 44 CARNITOR ............................................................ SEC 3.56 CARVEDILOL .................................................................... 48 CASPOFUNGIN ..................................................... SEC 3.19 CATAPRES ........................................................................ 40 CAYSTON .............................................................. SEC 3.17 CEDOCARD-SR ................................................................ 42 CEFADROXIL ........................................................ SEC 3.19 CEFAZOLIN .........................................................................3 CEFAZOLIN SODIUM ..........................................................3 CEFIXIME ............................................................................5 CEFOTAXIME SODIUM ......................................................5 CEFPROZIL .........................................................................4 CEFTAZIDIME .....................................................................5 CEFTIN ................................................................................5 CEFTRIAXONE FOR INJECTION USP ...............................5 CEFTRIAXONE SODIUM ....................................................5 CEFUROXIME AXETIL ........................................................5 CEFZIL .................................................................................4 CELEBREX ............................................................ SEC 3.19 CELECOXIB........................................................... SEC 3.19 CELESTONE SOLUSPAN ............................................... 155 CELEXA ............................................................................. 90 CELONTIN ......................................................................... 83 CEPHALEXIN ......................................................................3 CEPHALEXIN ......................................................................4 CESAMET ........................................................................ 144 CHAMPIX ............................................................... SEC 3.90 CHAMPIX (STARTER PACK) ................................ SEC 3.91 CHLORAL HYDRATE ...................................................... 112 CHLORAMPHENICOL SODIUM SUCCINATE ....................6 CHLORDIAZEPOXIDE HCL ............................................ 109 CHLORDIAZEPOXIDE HCL/ CLIDINIUM BROMIDE ...... 109 CHLOROMYCETIN ..............................................................6 CHLOROQUINE PHOSPHATE ......................................... 17 CHLORPROMAZINE HCL ............................................... 104

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 199
CHLORTHALIDONE ....................................................... 127 CHOLEDYL ..................................................................... 181 CHOLEDYL EXPECTORANT ......................................... 181 CHOLESTYRAMINE RESIN ............................................. 34 CICLESONIDE ................................................................ 155 CICLOPIROX OLAMINE ................................................. 173 CILAZAPRIL ...................................................................... 56 CILAZAPRIL ...................................................................... 57 CILAZAPRIL/ HYDROCHLOROTHIAZIDE ....................... 57 CILOXAN ........................................................................ 131 CIMETIDINE ................................................................... 144 CIPRALEX ........................................................................ 90 CIPRO .................................................................... SEC 3A.1 CIPRO .................................................................... SEC 3A.2 CIPRO .................................................................... SEC 3A.3 CIPRODEX ..................................................................... 132 CIPROFLOXACIN .................................................. SEC 3A.1 CIPROFLOXACIN .................................................. SEC 3A.2 CIPROFLOXACIN .................................................. SEC 3A.3 CIPROFLOXACIN HCL ................................................... 131 CIPROFLOXACIN HCL .......................................... SEC 3A.2 CIPROFLOXACIN HCL .......................................... SEC 3A.3 CIPROFLOXACIN HCL/ DEXAMETHASONE ................ 132 CITALOPRAM ................................................................... 90 CITALOPRAM HYDROBROMIDE .................................... 90 CITALOPRAM-ODAN ....................................................... 90 CLAFORAN ......................................................................... 5 CLARITHROMYCIN ............................................................ 7 CLARUS .......................................................................... 179 CLASTEON ..................................................................... 185 CLAVULIN-125F ................................................................. 9 CLAVULIN-200 ................................................................... 9 CLAVULIN-250F ................................................................. 9 CLAVULIN-400 ................................................................... 9 CLAVULIN-500F ................................................................. 9 CLAVULIN-875 ................................................................... 9 CLIMARA 100 (7.8 MG/PTH) .......................................... 161 CLIMARA 25 (2 MG/PTH) ............................................... 161 CLIMARA 50 (3.9 MG/PTH) ............................................ 161 CLIMARA 75 (5.7 MG/PTH) ............................................ 161 CLINDAMYCIN ................................................................. 13 CLINDAMYCIN (60 & 120 ML) .......................................... 13 CLINDAMYCIN HCL ......................................................... 13 CLINDAMYCIN PALMITATE HCL..................................... 13 CLINDAMYCIN PHOSPHATE .......................................... 13 CLINDAMYCIN PHOSPHATE/ BENZOYL PEROXIDE
………………………………………………………..SEC 3.19 CLINDOXYL ........................................................... SEC 3.19 CLOBAZAM ...................................................................... 81 CLOBETASOL 17-PROPIONATE .................................. 174 CLOBETASOL 17-PROPIONATE .................................. 175 CLODRONATE DISODIUM ............................................ 185
CLODRONATE DISODIUM TETRAHYDRATE ................ 185 CLOMID ........................................................................... 162 CLOMIPHENE CITRATE ................................................. 162 CLOMIPRAMINE HCL ....................................................... 94 CLONAZEPAM .................................................................. 82 CLONIDINE HCL ............................................................. 185 CLONIDINE HCL ............................................................... 40 CLOPIDOGREL BISULFATE ................................. SEC 3.20 CLOPIXOL ....................................................................... 107 CLOPIXOL ACUPHASE .................................................. 106 CLOPIXOL DEPOT .......................................................... 106 CLORAZEPATE DIPOTASSIUM ..................................... 109 CLOXACILLIN SODIUM .................................................... 10 CLOZAPINE ....................................................................... 97 CLOZAPINE ....................................................................... 98 CLOZARIL ......................................................................... 97 CLOZARIL ......................................................................... 98 CO ALENDRONATE .............................................. SEC 3.14 CO AMLODIPINE ............................................................... 52 CO ATENOLOL.................................................................. 46 CO ATENOLOL.................................................................. 47 CO ATORVASTATIN ......................................................... 36 CO AZITHROMYCIN ...........................................................7 CO AZITHROMYCIN ............................................. SEC 3.17 CO BETAHISTINE ........................................................... 185 CO CABERGOLINE ............................................... SEC 3.18 CO CANDESARTAN .......................................................... 63 CO CILAZAPRIL ................................................................ 56 CO CILAZAPRIL ................................................................ 57 CO CIPROFLOXACIN ........................................... SEC 3A.2 CO CIPROFLOXACIN ........................................... SEC 3A.3 CO CITALOPRAM ............................................................. 90 CO CLOMIPRAMINE ......................................................... 94 CO CLONAZEPAM ............................................................ 82 CO CLOPIDOGREL ............................................... SEC 3.20 CO DILTIAZEM CD ............................................................ 54 CO DILTIAZEM T ............................................................... 54 CO DILTIAZEM T ............................................................... 55 CO ENALAPRIL ................................................................. 57 CO ENALAPRIL ................................................................. 58 CO ETIDROCAL .............................................................. 186 CO ETIDRONATE ............................................................ 186 CO FINASTERIDE ................................................. SEC 3.40 CO FLUCONAZOLE .......................................................... 14 CO FLUOXETINE .............................................................. 91 CO FLUVOXAMINE ........................................................... 91 CO GABAPENTIN .............................................................. 84 CO GABAPENTIN .............................................................. 85 CO IRBESARTAN .............................................................. 63 CO IRBESARTAN .............................................................. 64 CO IRBESARTAN/HCT ..................................................... 64 CO LATANOPROST ........................................................ 137
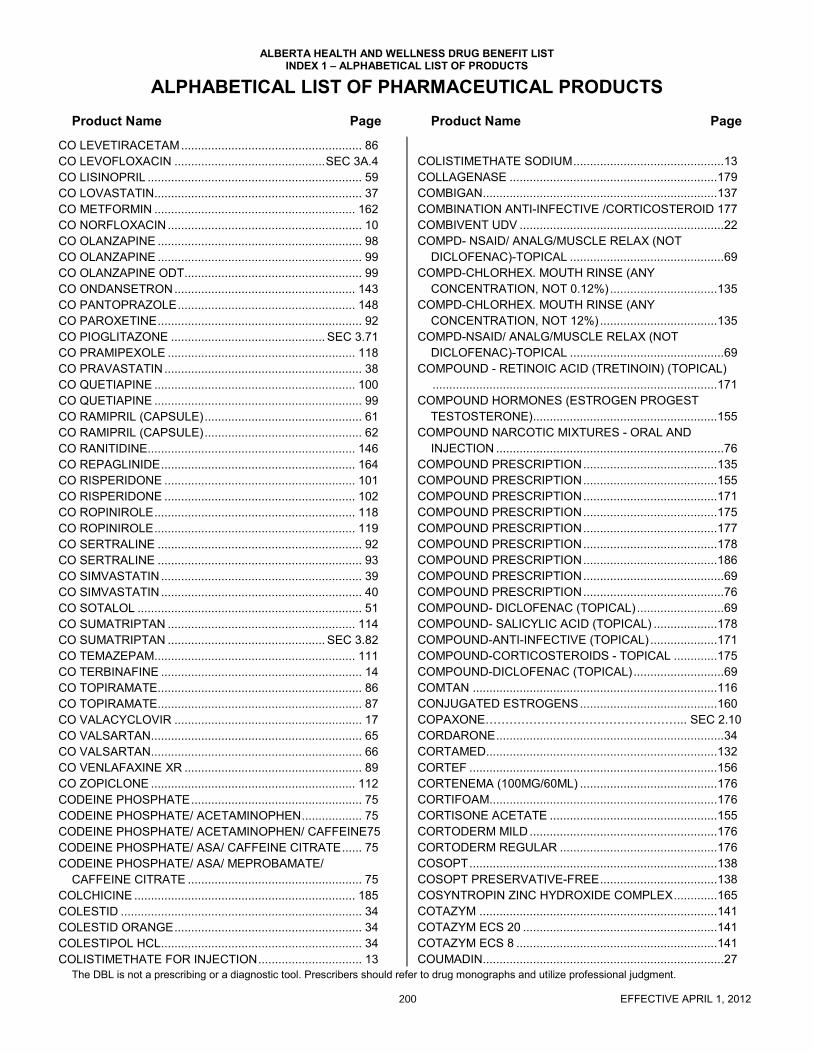
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 200 EFFECTIVE APRIL 1, 2012
CO LEVETIRACETAM ...................................................... 86 CO LEVOFLOXACIN ............................................. SEC 3A.4 CO LISINOPRIL ................................................................ 59 CO LOVASTATIN.............................................................. 37 CO METFORMIN ............................................................ 162 CO NORFLOXACIN .......................................................... 10 CO OLANZAPINE ............................................................. 98 CO OLANZAPINE ............................................................. 99 CO OLANZAPINE ODT ..................................................... 99 CO ONDANSETRON ...................................................... 143 CO PANTOPRAZOLE ..................................................... 148 CO PAROXETINE ............................................................. 92 CO PIOGLITAZONE .............................................. SEC 3.71 CO PRAMIPEXOLE ........................................................ 118 CO PRAVASTATIN ........................................................... 38 CO QUETIAPINE ............................................................ 100 CO QUETIAPINE .............................................................. 99 CO RAMIPRIL (CAPSULE) ............................................... 61 CO RAMIPRIL (CAPSULE) ............................................... 62 CO RANITIDINE.............................................................. 146 CO REPAGLINIDE .......................................................... 164 CO RISPERIDONE ......................................................... 101 CO RISPERIDONE ......................................................... 102 CO ROPINIROLE ............................................................ 118 CO ROPINIROLE ............................................................ 119 CO SERTRALINE ............................................................. 92 CO SERTRALINE ............................................................. 93 CO SIMVASTATIN ............................................................ 39 CO SIMVASTATIN ............................................................ 40 CO SOTALOL ................................................................... 51 CO SUMATRIPTAN ........................................................ 114 CO SUMATRIPTAN ............................................... SEC 3.82 CO TEMAZEPAM............................................................ 111 CO TERBINAFINE ............................................................ 14 CO TOPIRAMATE............................................................. 86 CO TOPIRAMATE............................................................. 87 CO VALACYCLOVIR ........................................................ 17 CO VALSARTAN............................................................... 65 CO VALSARTAN............................................................... 66 CO VENLAFAXINE XR ..................................................... 89 CO ZOPICLONE ............................................................. 112 CODEINE PHOSPHATE ................................................... 75 CODEINE PHOSPHATE/ ACETAMINOPHEN .................. 75 CODEINE PHOSPHATE/ ACETAMINOPHEN/ CAFFEINE75 CODEINE PHOSPHATE/ ASA/ CAFFEINE CITRATE ...... 75 CODEINE PHOSPHATE/ ASA/ MEPROBAMATE/
CAFFEINE CITRATE .................................................... 75 COLCHICINE .................................................................. 185 COLESTID ........................................................................ 34 COLESTID ORANGE ........................................................ 34 COLESTIPOL HCL............................................................ 34 COLISTIMETHATE FOR INJECTION ............................... 13
COLISTIMETHATE SODIUM ............................................. 13 COLLAGENASE .............................................................. 179 COMBIGAN...................................................................... 137 COMBINATION ANTI-INFECTIVE /CORTICOSTEROID 177 COMBIVENT UDV ............................................................. 22 COMPD- NSAID/ ANALG/MUSCLE RELAX (NOT
DICLOFENAC)-TOPICAL .............................................. 69 COMPD-CHLORHEX. MOUTH RINSE (ANY
CONCENTRATION, NOT 0.12%) ................................ 135 COMPD-CHLORHEX. MOUTH RINSE (ANY
CONCENTRATION, NOT 12%) ................................... 135 COMPD-NSAID/ ANALG/MUSCLE RELAX (NOT
DICLOFENAC)-TOPICAL .............................................. 69 COMPOUND - RETINOIC ACID (TRETINOIN) (TOPICAL)
..................................................................................... 171 COMPOUND HORMONES (ESTROGEN PROGEST
TESTOSTERONE) ....................................................... 155 COMPOUND NARCOTIC MIXTURES - ORAL AND
INJECTION .................................................................... 76 COMPOUND PRESCRIPTION ........................................ 135 COMPOUND PRESCRIPTION ........................................ 155 COMPOUND PRESCRIPTION ........................................ 171 COMPOUND PRESCRIPTION ........................................ 175 COMPOUND PRESCRIPTION ........................................ 177 COMPOUND PRESCRIPTION ........................................ 178 COMPOUND PRESCRIPTION ........................................ 186 COMPOUND PRESCRIPTION .......................................... 69 COMPOUND PRESCRIPTION .......................................... 76 COMPOUND- DICLOFENAC (TOPICAL) .......................... 69 COMPOUND- SALICYLIC ACID (TOPICAL) ................... 178 COMPOUND-ANTI-INFECTIVE (TOPICAL) .................... 171 COMPOUND-CORTICOSTEROIDS - TOPICAL ............. 175 COMPOUND-DICLOFENAC (TOPICAL) ........................... 69 COMTAN ......................................................................... 116 CONJUGATED ESTROGENS ......................................... 160 COPAXONE…………………………………………... SEC 2.10 CORDARONE .................................................................... 34 CORTAMED..................................................................... 132 CORTEF .......................................................................... 156 CORTENEMA (100MG/60ML) ......................................... 176 CORTIFOAM.................................................................... 176 CORTISONE ACETATE .................................................. 155 CORTODERM MILD ........................................................ 176 CORTODERM REGULAR ............................................... 176 COSOPT .......................................................................... 138 COSOPT PRESERVATIVE-FREE ................................... 138 COSYNTROPIN ZINC HYDROXIDE COMPLEX ............. 165 COTAZYM ....................................................................... 141 COTAZYM ECS 20 .......................................................... 141 COTAZYM ECS 8 ............................................................ 141 COUMADIN........................................................................ 27

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 201
COUMADIN ....................................................................... 28 COVERSYL ....................................................................... 60 COVERSYL PLUS ............................................................ 60 COVERSYL PLUS HD ...................................................... 60 COZAAR ........................................................................... 64 CREON 10 MINIMICROSPHERES ................................. 141 CREON 25 MINIMICROSPHERES ................................. 141 CRESTOR ......................................................................... 38 CTP 30 .............................................................................. 90 CUPRIMINE .................................................................... 153 CYANOCOBALAMIN ...................................................... 183 CYCLEN (21 DAY) .......................................................... 160 CYCLEN (28 DAY) .......................................................... 160 CYCLOBENZAPRINE ....................................................... 25 CYCLOBENZAPRINE HCL ............................................... 25 CYCLOCORT .................................................................. 173 CYCLOGYL ..................................................................... 134 CYCLOMEN .................................................................... 158 CYCLOPENTOLATE HCL .............................................. 134 CYCLOSPORINE ................................................... SEC 3.21 CYKLOKAPRON ............................................................... 31 CYMBALTA ....................................................................... 88 CYPROTERONE.................................................... SEC 3.21 CYPROTERONE ACETATE .................................. SEC 3.21 CYTOMEL ....................................................................... 167 CYTOVENE ...................................................................... 17
D
DALACIN C ....................................................................... 13 DALACIN C PALMITATE .............................................. 13 DALACIN C PHOSPHATE ................................................ 13 DALTEPARIN SODIUM .................................................... 28 DALTEPARIN SODIUM .................................................... 29 DANAPAROID SODIUM ........................................ SEC 3.21 DANAZOL ....................................................................... 158 DANTRIUM ....................................................................... 25 DANTROLENE SODIUM .................................................. 25 DAPSONE ......................................................................... 15 DARAPRIM ....................................................................... 17 DARBEPOETIN ..................................................... SEC 3.22 DARIFENACIN HYDROBROMIDE ........................ SEC 3.22 DDAVP ............................................................................ 166 DEFERASIROX ..................................................... SEC 3.23 DEFEROXAMINE MESYLATE ....................................... 153 DELATESTRYL ............................................................... 158 DEMEROL ........................................................................ 77 DEMULEN 30 (21 DAY) .................................................. 159 DEMULEN 30 (28 DAY) .................................................. 159 DENOSUMAB ........................................................ SEC 3.23
DEPAKENE ....................................................................... 87 DEPO-MEDROL .............................................................. 157 DEPO-MEDROL (PRESERVED) ..................................... 157 DEPO-MEDROL WITH LIDOCAINE ................................ 157 DEPO-PROVERA ............................................................ 166 DEPO-TESTOSTERONE CYPIONATE ........................... 158 DERMOVATE .................................................................. 174 DERMOVATE .................................................................. 175 DESFERAL ...................................................................... 153 DESFERRIOXAMINE MESILATE .................................... 153 DESIPRAMINE HCL .......................................................... 94 DESMOPRESSIN ............................................................ 166 DESMOPRESSIN ACETATE ........................................... 166 DESOGESTREL/ ETHINYL ESTRADIOL ........................ 158 DESOGESTREL/ ETHINYL ESTRADIOL/ DESOGESTREL/
ETHINYL ESTRADIOL/ DESOGESTREL/ ETHINYL ESTRADIOL ................................................................. 159
DESONIDE ...................................................................... 175 DESOXIMETASONE ....................................................... 175 DESSICATED THYROID ................................................. 167 DETROL LA ........................................................... SEC 3.87 DEVICE ............................................................................ 189 DEXAMETHASONE ......................................................... 132 DEXAMETHASONE ......................................................... 156 DEXAMETHASONE SODIUM PHOSPHATE .................. 132 DEXAMETHASONE SODIUM PHOSPHATE .................. 156 DEXAMETHASONE/ FRAMYCETIN SULFATE/
GRAMICIDIN................................................................ 133 DEXAMETHASONE/ NEOMYCIN SULFATE/ POLYMYXIN B
SULFATE ..................................................................... 133 DEXAMETHASONE/ TOBRAMYCIN ............................... 133 DEXASONE ..................................................................... 156 DEXEDRINE .................................................................... 107 DEXIRON ........................................................................... 27 DEXTROAMPHETAMINE SULFATE ............................... 107 DIABETA .......................................................................... 165 DIAMICRON..................................................................... 164 DIAMICRON MR .............................................................. 164 DIAZEMULS..................................................................... 110 DIAZEPAM ....................................................................... 109 DIAZEPAM ....................................................................... 110 DIAZOXIDE ........................................................................ 41 DICETEL .......................................................................... 150 DICLECTIN ...................................................................... 144 DICLOFENAC SODIUM ................................................... 134 DICLOFENAC SODIUM ..................................................... 70 DICLOFENAC SODIUM SR ............................................... 70 DICLOFENAC SODIUM/ MISOPROSTOL ........................ 70 DICYCLOMINE HCL .......................................................... 21 DICYCLOMINE HYDROCHLORIDE .................................. 21 DIDROCAL ...................................................................... 186 DIFLUCAN ......................................................................... 14

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 202 EFFECTIVE APRIL 1, 2012
DIFLUCAN ............................................................. SEC 3.41 DIFLUCORTOLONE VALERATE ................................... 175 DIFLUNISAL ..................................................................... 71 DIGOXIN ........................................................................... 34 DIGOXIN PEDIATRIC ....................................................... 34 DIHYDROERGOTAMINE (DHE) ....................................... 24 DIHYDROERGOTAMINE MESYLATE .............................. 24 DILANTIN .......................................................................... 82 DILANTIN INFATABS ....................................................... 82 DILANTIN-125 ................................................................... 82 DILANTIN-30 ..................................................................... 82 DILAUDID ......................................................................... 76 DILAUDID STERILE POWDER ........................................ 77 DILAUDID-HP ................................................................... 77 DILTIAZEM HCL ............................................................... 53 DILTIAZEM HCL ............................................................... 54 DILTIAZEM HCL ............................................................... 55 DIMENHYDRINATE ........................................................ 142 DIMENHYDRINATE I.M. ................................................. 142 DIMENHYDRINATE I.V. .................................................. 142 DIMETHYL SULFOXIDE ................................................. 186 DIMETHYL SULFOXIDE IRRIGATION ........................... 186 DIODOQUIN ..................................................................... 17 DIOVAN ............................................................................ 65 DIOVAN ............................................................................ 66 DIOVAN-HCT .................................................................... 66 DIPENTUM ..................................................................... 150 DIPHENHYDRAMINE ......................................................... 1 DIPHENHYDRAMINE HCL ................................................. 1 DIPHENOXYLATE HCL/ ATROPINE SULFATE ............. 141 DIPROLENE GLYCOL .................................................... 174 DIPROSALIC .................................................................. 174 DIPROSONE ................................................................... 174 DIPYRIDAMOLE ............................................................... 43 DIPYRIDAMOLE/ ASA ...................................................... 30 DISOPYRAMIDE ............................................................... 33 DIVALPROEX SODIUM (VALPROIC ACID EQUIV.) ........ 84 DIXARIT .......................................................................... 185 DOLASETRON MESYLATE ........................................... 142 DOMPERIDONE ............................................................. 149 DOMPERIDONE MALEATE ........................................... 149 DONEPEZIL HCL ................................................... SEC 3.24 DORZOLAMIDE HCL ...................................................... 136 DORZOLAMIDE HCL/ TIMOLOL MALEATE .................. 138 DOSTINEX ............................................................. SEC 3.18 DOVOBET ....................................................................... 179 DOVONEX ...................................................................... 179 DOXAZOSIN MESYLATE ................................................. 44 DOXEPIN HCL .................................................................. 94 DOXEPIN HCL .................................................................. 95 DOXYCYCLINE ................................................................ 11
DOXYCYCLINE HYCLATE ................................................ 11 DOXYLAMINE SUCCINATE/ PYRIDOXINE HCL ............ 144 DROSPIRENONE/ ETHINYL ESTRADIOL ...................... 159 DULOXETINE HYDROCHLORIDE .................................... 88 DUO TRAV ...................................................................... 138 DUTASTERIDE ...................................................... SEC 3.24
E
ECULIZUMAB ........................................................ SEC 3.29 EDECRIN ........................................................................... 41 EFFEXOR XR .................................................................... 89 EFUDEX .......................................................................... 179 ELAVIL ............................................................................... 94 ELMIRON ......................................................................... 187 ELOCOM ......................................................................... 177 ELTROXIN ....................................................................... 167 EMEND ............................................................................ 144 EMEND TRI-PACK .......................................................... 144 EMO-CORT...................................................................... 176 ENABLEX .............................................................. SEC 3.22 ENALAPRIL MALEATE ...................................................... 57 ENALAPRIL MALEATE ...................................................... 58 ENALAPRIL MALEATE/ HYDROCHLOROTHIAZIDE ....... 58 ENBREL ................................................................. SEC 3.37 ENDOCET ......................................................................... 80 ENGERIX-B ..................................................................... 169 ENOXAPARIN SODIUM .................................................... 29 ENTACAPONE ................................................................ 116 ENTECAVIR....................................................................... 16 ENTOCORT ........................................................... SEC 3.18 ENTOCORT (115 ML) ...................................................... 174 ENTROPHEN 10 ................................................................ 69 EPINEPHRINE ................................................................... 24 EPINEPHRINE HCL ......................................................... 135 EPINEPHRINE HCL ........................................................... 24 EPIPEN .............................................................................. 24 EPIPEN JR ........................................................................ 24 EPIVAL .............................................................................. 84 EPOETIN ALFA ..................................................... SEC 3.29 EPOETIN ALFA ..................................................... SEC 3.30 EPREX ................................................................... SEC 3.29 EPREX (0.3 ML SYRINGE) ................................... SEC 3.30 EPREX (0.4 ML SYRINGE) ................................... SEC 3.30 EPREX (0.5 ML SYRINGE) ................................... SEC 3.30 EPREX (0.6 ML SYRINGE) ................................... SEC 3.30 EPREX (0.8 ML SYRINGE) ................................... SEC 3.30 EPREX (1 ML SYRINGE) ...................................... SEC 3.30 EPROSARTAN MESYLATE .............................................. 63 EPROSARTAN MESYLATE/ HYDROCHLOROTHIAZIDE 63 ERGOLOID MESYLATES .................................................. 24

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 203
ERGOTAMINE TARTRATE/ CAFFEINE ........................... 24 ERTAPENEM ......................................................... SEC 3.31 ERYC .................................................................................. 6 ERYTHRO-BASE ................................................................ 6 ERYTHRO-EC .................................................................... 6 ERYTHRO-ES ..................................................................... 6 ERYTHRO-S ....................................................................... 6 ERYTHROMYCIN ........................................................... 131 ERYTHROMYCIN ............................................................... 6 ERYTHROMYCIN ESTOLATE ........................................... 6 ERYTHROMYCIN ETHYLSUCCINATE .............................. 6 ERYTHROMYCIN STEARATE ........................................... 6 ERYTHROMYCIN/ TRETINOIN ............................. SEC 3.31 ESCITALOPRAM OXALATE ............................................. 90 ESTALIS (2.7*.62 MG/PTH) ............................................ 161 ESTALIS (4.8*.51 MG/PTH) ............................................ 161 ESTRACE ....................................................................... 161 ESTRADERM-100 (8.0 MG/PTH) ................................... 161 ESTRADERM-25 (2 MG/PTH) ........................................ 161 ESTRADIOL-17B ............................................................ 161 ESTRADOT 100 (1.56 MG/PTH) .................................... 161 ESTRADOT 25 (0.39 MG/PTH) ...................................... 161 ESTRADOT 37.5 (0.585 MG/PTH).................................. 161 ESTRADOT 50 (0.78 MG/PTH) ...................................... 161 ESTRADOT 75 (1.17 MG/PTH) ...................................... 161 ESTRING ........................................................................ 161 ESTROGEL ..................................................................... 161 ETANERCEPT ....................................................... SEC 3.37 ETHACRYNIC ACID ......................................................... 41 ETHOPROPAZINE HCL ................................................. 116 ETHOSUXIMIDE ............................................................... 83 ETHYNODIOL DIACETATE/ ETHINYL ESTRADIOL...... 159 ETIDROCAL .................................................................... 186 ETIDRONATE DISODIUM .............................................. 186 ETIDRONATE DISODIUM/ CALCIUM CARBONATE ..... 186 ETODOLAC ...................................................................... 71 EUFLEX ................................................................. SEC 3.41 EUGLUCON .................................................................... 165 EVISTA .................................................................. SEC 3.73 EXELON ................................................................. SEC 3.77 EXJADE ................................................................. SEC 3.23 EXTAVIA (0.3 MG)…………………………………… SEC 2.10 EZETIMIBE ............................................................ SEC 3.37 EZETROL ............................................................... SEC 3.37
F
FAMOTIDINE .................................................................. 145 FEBUXOSTAT ....................................................... SEC 3.38 FELODIPINE ..................................................................... 52 FELODIPINE..................................................................... 53
FENOFIBRATE .................................................................. 35 FENOFIBRATE MICRO ..................................................... 35 FENOFIBRATE-S .............................................................. 35 FENOFIBRATE-S (TABLET).............................................. 35 FENTANYL ............................................................ SEC 3.38 FENTANYL ............................................................ SEC 3.39 FENTANYL CITRATE ............................................ SEC 3.39 FILGRASTIM.......................................................... SEC 3.40 FINACEA ......................................................................... 179 FINASTERIDE ....................................................... SEC 3.40 FIORINAL .......................................................................... 69 FIORINAL-C 1/2 ................................................................. 75 FIORINAL-C 1/4 ................................................................. 75 FLAGYL ........................................................................... 172 FLAGYL ............................................................................. 18 FLAGYSTATIN................................................................. 172 FLAREX ........................................................................... 132 FLECAINIDE ...................................................................... 33 FLECAINIDE ACETATE .................................................... 33 FLOCTAFENINE ................................................................ 71 FLORINEF ....................................................................... 156 FLOVENT DISKUS .......................................................... 156 FLOVENT HFA ................................................................ 156 FLUANXOL ...................................................................... 106 FLUANXOL DEPOT ......................................................... 106 FLUCONAZOLE ................................................................. 14 FLUCONAZOLE ..................................................... SEC 3.41 FLUCONAZOLE OMEGA .................................................. 14 FLUDROCORTISONE ACETATE .................................... 156 FLUMETHASONE PIVALATE/ CLIOQUINOL.................. 133 FLUNARIZINE.................................................................. 186 FLUNARIZINE HCL ......................................................... 186 FLUNISOLIDE.................................................................. 132 FLUOCINONIDE .............................................................. 175 FLUOR-A-DAY ................................................................. 121 FLUOROMETHOLONE ................................................... 132 FLUOROMETHOLONE ACETATE .................................. 132 FLUOXETINE..................................................................... 91 FLUOXETINE HCL ............................................................ 91 FLUPENTIXOL DECANOATE ......................................... 106 FLUPENTIXOL DIHYDROCHLORIDE ............................. 106 FLUPHENAZINE DECANOATE....................................... 104 FLUPHENAZINE HCL ...................................................... 104 FLUPHENAZINE HCL ...................................................... 105 FLUPHENAZINE OMEGA ............................................... 104 FLURAZEPAM HCL ......................................................... 110 FLURBIPROFEN ............................................................... 71 FLUTAMIDE ........................................................... SEC 3.41 FLUTICASONE PROPIONATE........................................ 156 FLUVASTATIN SODIUM ................................................... 37 FLUVOXAMINE MALEATE ................................................ 91
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 204 EFFECTIVE APRIL 1, 2012
FML FORTE .................................................................... 132 FOLIC ACID .................................................................... 183 FONDAPARINUX SODIUM .............................................. 30 FORADIL ........................................................................... 22 FORMOTEROL FUMARATE ............................................ 22 FORMOTEROL FUMARATE DIHYDRATE ....................... 23 FORTAZ .............................................................................. 5 FOSAMAX .............................................................. SEC 3.14 FOSAVANCE ......................................................... SEC 3.15 FOSINOPRIL .................................................................... 58 FOSINOPRIL SODIUM ..................................................... 58 FRAGMIN .......................................................................... 28 FRAGMIN (0.2 ML SYRINGE) .......................................... 28 FRAGMIN (0.3 ML SYRINGE) .......................................... 28 FRAGMIN (0.4 ML SYRINGE) .......................................... 28 FRAGMIN (0.5 ML SYRINGE) .......................................... 28 FRAGMIN (0.6 ML SYRINGE) .......................................... 28 FRAGMIN (0.72 ML SYRINGE) ........................................ 29 FRAXIPARINE (.3-1ML SYR) ........................................... 29 FRAXIPARINE FORTE (.6-1ML SYR) .............................. 29 FUCIDIN .......................................................................... 171 FUCIDIN .......................................................................... 172 FUNGIZONE IV ................................................................. 15 FUROSEMIDE .................................................................. 41 FUSIDIC ACID ................................................................ 171
G
GABAPENTIN ................................................................... 84 GABAPENTIN ................................................................... 85 GALANTAMINE HYDROBROMIDE ....................... SEC 3.41 GANCICLOVIR SODIUM .................................................. 17 GARAMYCIN .................................................................. 131 GARASONE .................................................................... 133 GD-AMLODIPINE.............................................................. 52 GD-ATORVASTATIN ........................................................ 36 GD-AZITHROMYCIN .......................................................... 7 GD-GABAPENTIN............................................................. 84 GD-GABAPENTIN............................................................. 85 GD-LATANOPROST ....................................................... 137 GD-SERTRALINE ............................................................. 92 GD-SERTRALINE ............................................................. 93 GD-VENLAFAXINE XR ..................................................... 89 GEMFIBROZIL .................................................................. 35 GEN-CLOZAPINE ............................................................. 97 GEN-CLOZAPINE ............................................................. 98 GENTAMICIN ...................................................................... 3 GENTAMICIN SULFATE ................................................. 131 GENTAMICIN SULFATE ................................................. 171 GENTAMICIN SULFATE ..................................................... 3 GLICLAZIDE ................................................................... 164
GLICLAZIDE MR .............................................................. 164 GLUCAGEN ..................................................................... 165 GLUCAGEN HYPOKIT .................................................... 165 GLUCAGON..................................................................... 165 GLUCAGON, RDNA ORIGIN ........................................... 165 GLUCOBAY ..................................................................... 162 GLUCONORM ................................................................. 164 GLUCOPHAGE ................................................................ 162 GLYBURIDE .................................................................... 165 GLYCOPYRROLATE ......................................................... 21 GOLD SODIUM THIOMALATE ........................................ 151 GOLIMUMAB ......................................................... SEC 3.45 GOSERELIN ACETATE ......................................... SEC 3.45 GRANISETRON ............................................................... 142 GRANISETRON HCL ....................................................... 142
H
HALOBETASOL PROPIONATE ...................................... 175 HALOPERIDOL................................................................ 103 HALOPERIDOL................................................................ 104 HALOPERIDOL DECANOATE ........................................ 104 HALOPERIDOL LA .......................................................... 104 HEPARIN LEO ................................................................... 29 HEPARIN LOCK FLUSH .................................................... 29 HEPARIN SODIUM ............................................................ 29 HEPATITIS B VACCINE (RECOMBINANT) .................... 169 HEPSERA .......................................................................... 16 HEPTOVIR ......................................................................... 15 HOMATROPINE HYDROBROMIDE ................................ 134 HP-PAC ( KIT )................................................................. 147 HUMALOG ....................................................................... 163 HUMALOG CARTRIDGE/KWIKPEN ............................... 163 HUMALOG MIX 25 CARTRIDGE/KWIKPEN ................... 164 HUMALOG MIX 50 CARTRIDGE/KWIKPEN ................... 164 HUMATROPE ........................................................ SEC 3.80 HUMIRA ................................................................. SEC 3.13 HUMULIN 30/70 ............................................................... 163 HUMULIN 30/70 CARTRIDGE ......................................... 163 HUMULIN N ..................................................................... 163 HUMULIN N CARTRIDGE/KWIKPEN .............................. 163 HUMULIN R ..................................................................... 163 HUMULIN R CARTRIDGE ............................................... 163 HYCORT (100MG/60ML) ................................................. 176 HYDERGINE ...................................................................... 24 HYDERM ......................................................................... 176 HYDRALAZINE HCL .......................................................... 41 HYDROCHLOROTHIAZIDE............................................. 126 HYDROCHLOROTHIAZIDE/ AMILORIDE HCL ............... 126 HYDROCHLOROTHIAZIDE/ SPIRONOLACTONE ........... 67 HYDROCHLOROTHIAZIDE/ TRIAMTERENE ................. 126

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 205
HYDROCORTISONE ...................................................... 156 HYDROCORTISONE ...................................................... 176 HYDROCORTISONE 17-VALERATE ............................. 176 HYDROCORTISONE ACETATE .................................... 132 HYDROCORTISONE ACETATE .................................... 176 HYDROCORTISONE ACETATE/ PRAMOXINE HCL ..... 176 HYDROCORTISONE ACETATE/ PRAMOXINE HCL/ ZINC
SULFATE .................................................................... 176 HYDROCORTISONE ACETATE/ UREA ......................... 176 HYDROCORTISONE ACETATE/ ZINC SULFATE ......... 177 HYDROCORTISONE SOD. SUCCINATE ....................... 156 HYDROCORTISONE SOD. SUCCINATE ....................... 157 HYDROCORTISONE SODIUM SUCCINATE ................. 156 HYDROCORTISONE SODIUM SUCCINATE ................. 157 HYDROCORTISONE/ CINCHOCAINE HCL/ FRAMYCETIN
SULFATE/ ESCULIN ................................................... 178 HYDROMORPH CONTIN ................................................. 76 HYDROMORPHONE ........................................................ 76 HYDROMORPHONE HCL ................................................ 76 HYDROMORPHONE HCL ................................................ 77 HYDROMORPHONE HP .................................................. 77 HYDROMORPHONE HP 20 ............................................. 77 HYDROMORPHONE HP 50 ............................................. 77 HYDROVAL .................................................................... 176 HYDROXYCHLOROQUINE SULFATE ............................. 17 HYDROXYZINE HCL ...................................................... 112 HYOSCINE BUTYLBROMIDE .......................................... 21 HYTRIN ............................................................................. 45 HYZAAR ............................................................................ 65 HYZAAR DS ...................................................................... 65
I
IBUPROFEN ..................................................................... 71 IMDUR .............................................................................. 42 IMIPENEM/ CILASTATIN SODIUM........................ SEC 3.46 IMIPRAMINE ..................................................................... 95 IMIPRAMINE HCL ............................................................. 95 IMIQUIMOD ........................................................... SEC 3.46 IMITREX .......................................................................... 114 IMITREX ................................................................. SEC 3.81 IMITREX (0.5 ML) ........................................................... 114 IMITREX (0.5 ML) .................................................. SEC 3.82 IMITREX DF .................................................................... 114 IMITREX DF ........................................................... SEC 3.82 IMOVANE ........................................................................ 112 IMURAN .......................................................................... 185 INDAPAMIDE HEMIHYDRATE ....................................... 127 INDERAL-LA ..................................................................... 50 INDOMETHACIN............................................................... 71 INDOMETHACIN............................................................... 72
INFLIXIMAB ........................................................... SEC 3.54 INFUFER ........................................................................... 27 INHIBACE .......................................................................... 56 INHIBACE .......................................................................... 57 INHIBACE PLUS ................................................................ 57 INNOHEP ........................................................................... 29 INNOHEP (0.25 ML SYRINGE) ......................................... 29 INNOHEP (0.35 ML SYRINGE) ......................................... 29 INNOHEP (0.45 ML SYRINGE) ......................................... 29 INNOHEP (0.5 ML SYRINGE) ........................................... 29 INNOHEP (0.7 ML SYRINGE) ........................................... 30 INNOHEP (0.9 ML SYRINGE) ........................................... 30 INSULIN ASPART ............................................................ 163 INSULIN DETEMIR .......................................................... 163 INSULIN GLARGINE ....................................................... 163 INSULIN GLULISINE (RDNA ORIGIN) ............................ 163 INSULIN HUMAN BIOSYNTHETIC (ISOPHANE) ............ 163 INSULIN HUMAN BIOSYNTHETIC (REGULAR) ............. 163 INSULIN HUMAN BIOSYNTHETIC (REGULAR)/ INSULIN
HUMAN BIOSYNTHETIC (ISOPHANE) ....................... 163 INSULIN LISPRO ............................................................. 163 INSULIN LISPRO/ INSULIN LISPRO PROTAMINE ........ 164 INVANZ .................................................................. SEC 3.31 INVEGA SUSTENNA (0.5 ML SYR) ...................... SEC 3.64 INVEGA SUSTENNA (0.75 ML SYR) .................... SEC 3.64 INVEGA SUSTENNA (1 ML SYR) ......................... SEC 3.64 INVEGA SUSTENNA (1.5 ML SYR) ...................... SEC 3.64 IODOQUINOL .................................................................... 17 IOPIDINE ......................................................................... 138 IPRATROPIUM BROMIDE ................................................ 22 IPRATROPIUM BROMIDE .................................... SEC 3.54 IPRATROPIUM BROMIDE/ SALBUTAMOL SULFATE ..... 22 IRBESARTAN .................................................................... 63 IRBESARTAN .................................................................... 64 IRBESARTAN/ HYDROCHLOROTHIAZIDE ...................... 64 IRBESARTAN/HCTZ .......................................................... 64 IRON DEXTRAN COMPLEX.............................................. 27 ISDN .................................................................................. 42 ISOPTIN SR ....................................................................... 55 ISOPTO ATROPINE ........................................................ 134 ISOPTO CARBACHOL .................................................... 137 ISOPTO CARPINE ........................................................... 137 ISOPTO HOMATROPINE ................................................ 134 ISOSORBIDE DINITRATE ................................................. 42 ISOSORBIDE-5-MONONITRATE ...................................... 42 ISOTRETINOIN ................................................................ 179 ITRACONAZOLE ............................................................... 14 ITRACONAZOLE ................................................... SEC 3.54
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 206 EFFECTIVE APRIL 1, 2012
J
JAMP-AMLODIPINE ......................................................... 52 JAMP-ATENOLOL ............................................................ 46 JAMP-ATENOLOL ............................................................ 47 JAMP-CITALOPRAM ........................................................ 90 JAMP-FINASTERIDE ............................................. SEC 3.40 JAMP-FOSINOPRIL .......................................................... 58 JAMP-GABAPENTIN ........................................................ 84 JAMP-GABAPENTIN ........................................................ 85 JAMP-LACTULOSE ........................................................ 125 JAMP-LISINOPRIL ............................................................ 59 JAMP-METOPROLOL-L ................................................... 49 JAMP-ONDANSETRON .................................................. 143 JAMP-PIOGLITAZONE .......................................... SEC 3.71 JAMP-PRAVASTATIN ....................................................... 38 JAMP-QUETIAPINE ........................................................ 100 JAMP-QUETIAPINE .......................................................... 99 JAMP-RAMIPRIL (CAPSULE) .......................................... 61 JAMP-RAMIPRIL (CAPSULE) .......................................... 62 JAMP-RISPERIDONE ..................................................... 101 JAMP-RISPERIDONE ..................................................... 102 JAMP-ROPINIROLE ....................................................... 118 JAMP-ROPINIROLE ....................................................... 119 JAMP-SIMVASTATIN ........................................................ 39 JAMP-SIMVASTATIN ........................................................ 40 JAMP-TERBINAFINE ........................................................ 14
K
K-10 ORAL LIQUID ......................................................... 125 K-DUR ............................................................................. 125 K-LYTE ............................................................................ 125 KADIAN ............................................................................. 79 KAYEXALATE ................................................................. 126 KENALOG-10 .................................................................. 158 KENALOG-40 .................................................................. 158 KEPPRA ............................................................................ 86 KETOCONAZOLE ............................................................. 14 KETOCONAZOLE ........................................................... 172 KETODERM .................................................................... 172 KETOPROFEN ................................................................. 72 KETOPROFEN SR............................................................ 72 KETOPROFEN-E .............................................................. 72 KETOROLAC TROMETHAMINE .................................... 134 KETOROLAC TROMETHAMINE ...................................... 72 KETOTIFEN FUMARATE ................................................... 1 KINERET ................................................................ SEC 3.17 KYTRIL ............................................................................ 142
L
L-TRYPTOPHAN ............................................................... 96 LABETALOL HCL .............................................................. 48 LABETALOL HYDROCHLORIDE ...................................... 48 LACOSAMIDE........................................................ SEC 3.54 LACOSAMIDE........................................................ SEC 3.55 LACTULOSE .................................................................... 125 LAMICTAL ......................................................................... 85 LAMISIL ............................................................................. 14 LAMISIL ........................................................................... 172 LAMIVUDINE ..................................................................... 15 LAMOTRIGINE .................................................................. 85 LANREOTIDE ACETATE ....................................... SEC 3.55 LANSOPRAZOLE ............................................................ 147 LANSOPRAZOLE/ AMOXICILLIN TRIHYDRATE/
CLARITHROMYCIN ..................................................... 147 LANTUS ........................................................................... 163 LANTUS CARTRIDGE ..................................................... 163 LANTUS PEN................................................................... 163 LASIX ................................................................................. 41 LASIX SPECIAL ................................................................. 41 LATANOPROST .............................................................. 137 LATANOPROST/ TIMOLOL MALEATE ........................... 138 LECTOPAM ..................................................................... 109 LEDERLE LEUCOVORIN CALCIUM ............................... 186 LEFLUNOMIDE ................................................................ 187 LESCOL ............................................................................. 37 LESCOL XL ....................................................................... 37 LEUCOVORIN CALCIUM ................................................ 186 LEUPROLIDE ACETATE ....................................... SEC 3.55 LEVAQUIN ............................................................. SEC 3A.4 LEVEMIR CARTRIDGE ................................................... 163 LEVETIRACETAM ............................................................. 86 LEVOBUNOLOL HCL ...................................................... 136 LEVOCARB CR ............................................................... 117 LEVOCARNITINE .................................................. SEC 3.56 LEVODOPA/ BENSERAZIDE HCL .................................. 116 LEVODOPA/ CARBIDOPA .............................................. 117 LEVODOPA/ CARBIDOPA/ ENTACAPONE .................... 117 LEVOFLOXACIN .................................................... SEC 3A.4 LEVONORGESTREL ....................................................... 159 LEVONORGESTREL/ ETHINYL ESTRADIOL ................ 159 LEVONORGESTREL/ ETHINYL ESTRADIOL/
LEVONORGESTREL/ ETHINYL ESTRADIOL/ LEVONORGESTREL/ ETHINYL ESTRADIOL ............ 159
LEVOTHYROXINE SODIUM ........................................... 167 LIBRAX ............................................................................ 109 LIDOCAINE ...................................................................... 178 LIDOCAINE HCL .............................................................. 134 LIDOCAINE HCL .............................................................. 178

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 207
LIDODAN ........................................................................ 178 LIDODAN VISCOUS ....................................................... 134 LINESSA 21 .................................................................... 159 LINESSA 28 .................................................................... 159 LINEZOLID ............................................................. SEC 3.56 LIORESAL ......................................................................... 25 LIORESAL D.S. ................................................................. 25 LIORESAL INTRATHECAL ............................................... 25 LIORESAL INTRATHECAL ............................................... 26 LIOTHYRONINE SODIUM .............................................. 167 LIPASE/ AMYLASE/ PROTEASE ................................... 141 LIPIDIL MICRO ................................................................. 35 LIPIDIL SUPRA ................................................................. 35 LIPIDIL SUPRA (TABLET) ................................................ 35 LIPITOR ............................................................................ 36 LISINOPRIL ...................................................................... 59 LISINOPRIL/ HYDROCHLOROTHIAZIDE ........................ 60 LISINOPRIL/HCTZ (TYPE Z) ........................................... 60 LITHANE ......................................................................... 113 LITHIUM CARBONATE ................................................... 113 LOCACORTEN VIOFORM .............................................. 133 LOESTRIN 1.5/30 (21 DAY) ............................................ 159 LOESTRIN 1.5/30 (28 DAY) ............................................ 159 LOMOTIL ........................................................................ 141 LONITEN ........................................................................... 41 LOPRESOR ...................................................................... 49 LOPRESOR SR ................................................................ 49 LOPROX ......................................................................... 173 LORAZEPAM .................................................................. 110 LOSARTAN POTASSIUM ................................................. 64 LOSARTAN POTASSIUM/ HYDROCHLOROTHIAZIDE .. 65 LOSEC (SUSTAINED-RELEASE CAPSULE) ................. 148 LOSEC (SUSTAINED-RELEASE TABLET) .................... 148 LOTENSIN ........................................................................ 56 LOTRIDERM ................................................................... 177 LOVASTATIN .................................................................... 37 LOVENOX ......................................................................... 29 LOVENOX (0.3 ML SYRINGE) ......................................... 29 LOVENOX (0.4 - 1 ML SYRINGE) .................................... 29 LOVENOX HP (0.8ML/1ML SYRINGE)............................. 29 LOXAPAC ....................................................................... 107 LOXAPINE HCL .............................................................. 107 LOXAPINE SUCCINATE ................................................. 107 LOZIDE ........................................................................... 127 LUCENTIS ...................................................................... 139 LUMIGAN RC 0.01% ....................................................... 137 LUPRON ................................................................ SEC 3.55 LUPRON DEPOT ................................................... SEC 3.55 LUVOX .............................................................................. 91 LYDERM ......................................................................... 175
M
M-ESLON ........................................................................... 78 M-ESLON ........................................................................... 79 M.O.S. SULFATE ............................................................... 78 M.O.S.-SR .......................................................................... 77 MACROBID ........................................................................ 18 MAGLUCATE ................................................................... 125 MAGNESIUM GLUCOHEPTONATE ............................... 125 MAGNESIUM GLUCONATE ............................................ 125 MAJEPTIL ........................................................................ 105 MAPROTILINE HCL ........................................................... 95 MAR-AMLODIPINE ............................................................ 52 MAR-ATENOLOL ............................................................... 46 MAR-ATENOLOL ............................................................... 47 MAR-CITALOPRAM ........................................................... 90 MAR-ONDANSETRON .................................................... 143 MAR-RISPERIDONE ....................................................... 101 MAR-RISPERIDONE ....................................................... 102 MAR-SIMVASTATIN .......................................................... 39 MAR-SIMVASTATIN .......................................................... 40 MARVELON (21 DAY) ..................................................... 158 MARVELON (28 DAY) ..................................................... 158 MAVIK ................................................................................ 62 MAXALT ........................................................................... 113 MAXALT ................................................................. SEC 3.78 MAXALT RPD .................................................................. 113 MAXALT RPD ........................................................ SEC 3.78 MAXIDEX ......................................................................... 132 MAXITROL ....................................................................... 133 MEBENDAZOLE ..................................................................3 MEDROL .......................................................................... 157 MEDROXYPROGESTERONE ACETATE ....................... 166 MEFENAMIC...................................................................... 72 MEFENAMIC ACID ............................................................ 72 MEGACE OS ......................................................... SEC 3.57 MEGESTROL......................................................... SEC 3.57 MEGESTROL ACETATE ....................................... SEC 3.57 MEPERIDINE HCL ............................................................. 77 MEPERIDINE HYDROCHLORIDE .................................... 77 MEPRON ........................................................................... 18 MEROPENEM........................................................ SEC 3.58 MERREM ............................................................... SEC 3.58 MESALAZINE .................................................................. 150 MESASAL ........................................................................ 150 MESTINON ........................................................................ 21 MESTINON-SR .................................................................. 21 METADOL .......................................................................... 77 METADOL CONCENTRATE.............................................. 77 METFORMIN ................................................................... 162 METFORMIN HCL ........................................................... 162

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 208 EFFECTIVE APRIL 1, 2012
METHADONE ................................................................... 77 METHADONE COMPOUND ............................................. 77 METHADONE HCL ........................................................... 77 METHAZOLAMIDE ......................................................... 136 METHIMAZOLE .............................................................. 168 METHOTREXATE ............................................................. 19 METHOTREXATE SOD. (PRESERVED) .......................... 19 METHOTREXATE SOD.(UNPRESERVED) ..................... 19 METHOTREXATE SODIUM ............................................. 19 METHOTRIMEPRAZINE HCL ........................................ 105 METHOTRIMEPRAZINE MALEATE ............................... 105 METHOXSALEN ............................................................. 178 METHSUXIMIDE ............................................................... 83 METHYLDOPA ................................................................. 40 METHYLPHENIDATE HCL ............................................. 108 METHYLPREDNISOLONE ............................................. 157 METHYLPREDNISOLONE ACETATE ............................ 157 METHYLPREDNISOLONE ACETATE (P) ...................... 157 METHYLPREDNISOLONE ACETATE/ LIDOCAINE HCL157 METHYLPREDNISOLONE ACETATE/ NEOMYCIN
SULFATE/ ALUMINUM CHLORHYDROXIDE COMPLEX/ SULFUR ............................................................. SEC 3.58
METHYLPREDNISOLONE SOD SUCCIN. ..................... 157 METHYLPREDNISOLONE SODIUM SUCCINATE ........ 157 METOCLOPRAMIDE HCL .............................................. 149 METOCLOPRAMIDE HYDROCHLORIDE ...................... 149 METOLAZONE ............................................................... 127 METOPROLOL ................................................................. 49 METOPROLOL TARTRATE ............................................. 49 METROCREAM .............................................................. 171 METROGEL .................................................................... 171 METROLOTION .............................................................. 171 METRONIDAZOLE ......................................................... 171 METRONIDAZOLE ......................................................... 172 METRONIDAZOLE ........................................................... 18 METRONIDAZOLE/ NYSTATIN ...................................... 172 MEVACOR ........................................................................ 37 MEXILETINE HCL ............................................................. 33 MIACALCIN ............................................................ SEC 3.83 MICARDIS ......................................................................... 65 MICARDIS PLUS .............................................................. 65 MICRO-K EXTENCAPS .................................................. 125 MICRONOR (28 DAY) ..................................................... 159 MIDAMOR ....................................................................... 126 MIDAZOLAM ................................................................... 110 MIDAZOLAM HCL ........................................................... 110 MIDODRINE ...................................................................... 22 MIDODRINE HCL.............................................................. 22 MIGRANAL ....................................................................... 24 MIN-OVRAL (21 DAY) ..................................................... 159 MIN-OVRAL (28 DAY) ..................................................... 159 MINESTRIN 1/20 (21 DAY) ............................................. 159
MINESTRIN 1/20 (28 DAY) .............................................. 159 MINITRAN 0.2 .................................................................... 43 MINITRAN 0.4 .................................................................... 43 MINITRAN 0.6 .................................................................... 43 MINOCYCLINE .................................................................. 12 MINOCYCLINE HCL .......................................................... 12 MINOXIDIL ......................................................................... 41 MINT-AMLODIPINE ........................................................... 52 MINT-ATENOL ................................................................... 46 MINT-ATENOL ................................................................... 47 MINT-CIPROFLOXACIN ........................................ SEC 3A.2 MINT-CIPROFLOXACIN ........................................ SEC 3A.3 MINT-CITALOPRAM .......................................................... 90 MINT-ONDANSETRON ................................................... 143 MINT-PIOGLITAZONE ........................................... SEC 3.71 MINT-PRAVASTATIN ........................................................ 38 MINT-RISPERIDON ......................................................... 101 MINT-RISPERIDON ......................................................... 102 MINT-SIMVASTATIN ......................................................... 39 MINT-SIMVASTATIN ......................................................... 40 MINT-TOPIRAMATE .......................................................... 86 MINT-TOPIRAMATE .......................................................... 87 MIRENA SYSTEM ........................................................... 159 MIRTAZAPINE ................................................................... 97 MISCELLANEOUS COMPOUND .................................... 186 MISCELLANEOUS INJECTABLE COMPOUND .............. 186 MISCELLANEOUS ORAL COMPOUND .......................... 186 MISCELLANEOUS TOPICAL COMPOUND .................... 171 MISOPROSTOL ............................................................... 146 MOCLOBEMIDE ................................................................ 88 MODAFINIL............................................................ SEC 3.58 MODECATE CONCENTRATE......................................... 104 MODULON ....................................................................... 150 MOGADON ...................................................................... 111 MOMETASONE FUROATE ............................................. 132 MOMETASONE FUROATE ............................................. 177 MONOPRIL ........................................................................ 58 MONTELUKAST SODIUM ............................................... 129 MONTELUKAST SODIUM ..................................... SEC 3.59 MORPHINE HCL ................................................................ 77 MORPHINE HCL ................................................................ 78 MORPHINE HP 25 ............................................................. 79 MORPHINE HP 50 ............................................................. 79 MORPHINE LP EPIDURAL ............................................... 79 MORPHINE SR .................................................................. 78 MORPHINE SULFATE ....................................................... 78 MORPHINE SULFATE ....................................................... 79 MOXIFLOXACIN HCL ............................................ SEC 3A.5 MS CONTIN ....................................................................... 78 MS.IR ................................................................................. 78 MUCOMYST .................................................................... 130 MUPIROCIN..................................................................... 172

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 209
MYCOBUTIN .......................................................... SEC 3.73 MYDFRIN ........................................................................ 135 MYDRIACYL ................................................................... 134 MYL-RANITIDINE ........................................................... 146 MYLAN-ACEBUTOLOL ..................................................... 46 MYLAN-ACEBUTOLOL (TYPE S)..................................... 46 MYLAN-ACYCLOVIR ........................................................ 16 MYLAN-ALENDRONATE ....................................... SEC 3.14 MYLAN-ALPRAZOLAM ................................................... 109 MYLAN-AMANTADINE ................................................... 115 MYLAN-AMIODARONE .................................................... 34 MYLAN-AMLODIPINE ....................................................... 52 MYLAN-AMOXICILLIN ........................................................ 8 MYLAN-ATENOLOL.......................................................... 46 MYLAN-ATENOLOL.......................................................... 47 MYLAN-ATORVASTATIN ................................................. 36 MYLAN-AZATHIOPRINE ................................................ 185 MYLAN-AZITHROMYCIN ................................................... 7 MYLAN-BACLOFEN ......................................................... 25 MYLAN-BECLO AQ. ....................................................... 132 MYLAN-BUDESONIDE AQ ............................................. 132 MYLAN-CAPTOPRIL ........................................................ 56 MYLAN-CARBAMAZEPINE CR ........................................ 83 MYLAN-CARVEDILOL ...................................................... 48 MYLAN-CILAZAPRIL ........................................................ 56 MYLAN-CILAZAPRIL ........................................................ 57 MYLAN-CIMETIDINE ...................................................... 144 MYLAN-CIPROFLOXACIN .................................... SEC 3A.2 MYLAN-CIPROFLOXACIN .................................... SEC 3A.3 MYLAN-CITALOPRAM ..................................................... 90 MYLAN-CLARITHROMYCIN .............................................. 7 MYLAN-CLINDAMYCIN .................................................... 13 MYLAN-CLOBETASOL ................................................... 174 MYLAN-CLOBETASOL ................................................... 175 MYLAN-CLONAZEPAM .................................................... 82 MYLAN-CLOPIDOGREL ........................................ SEC 3.20 MYLAN-COMBO STERINEBS .......................................... 22 MYLAN-CYCLOBENZAPRINE ......................................... 25 MYLAN-DOMPERIDONE ................................................ 149 MYLAN-DOXAZOSIN ........................................................ 44 MYLAN-ENALAPRIL ......................................................... 57 MYLAN-ENALAPRIL ......................................................... 58 MYLAN-ETI-CAL-CAREPAC .......................................... 186 MYLAN-ETIDRONATE .................................................... 186 MYLAN-FAMOTIDINE ..................................................... 145 MYLAN-FENOFIBRATE MICRO ....................................... 35 MYLAN-FINASTERIDE .......................................... SEC 3.40 MYLAN-FLUCONAZOLE .................................................. 14 MYLAN-FLUOXETINE ...................................................... 91 MYLAN-FOSINOPRIL ....................................................... 58 MYLAN-GABAPENTIN ...................................................... 84
MYLAN-GABAPENTIN ...................................................... 85 MYLAN-GALANTAMINE ER .................................. SEC 3.41 MYLAN-GEMFIBROZIL ..................................................... 35 MYLAN-GLICLAZIDE ....................................................... 164 MYLAN-GLYBE................................................................ 165 MYLAN-HYDROXYCHLOROQUINE ................................. 17 MYLAN-INDAPAMIDE ..................................................... 127 MYLAN-IPRATROPIUM ..................................................... 22 MYLAN-IPRATROPIUM STERINEBS ................... SEC 3.54 MYLAN-IRBESARTAN ....................................................... 63 MYLAN-IRBESARTAN ....................................................... 64 MYLAN-LAMOTRIGINE ..................................................... 85 MYLAN-LANSOPRAZOLE ............................................... 147 MYLAN-LEVOFLOXACIN ...................................... SEC 3A.4 MYLAN-LISINOPRIL .......................................................... 59 MYLAN-LISINOPRIL HCTZ ............................................... 60 MYLAN-LOVASTATIN ....................................................... 37 MYLAN-METFORMIN ...................................................... 162 MYLAN-METOPROLOL ..................................................... 49 MYLAN-METOPROLOL (TYPE L) ..................................... 49 MYLAN-MINOCYCLINE ..................................................... 12 MYLAN-MIRTAZAPINE ..................................................... 97 MYLAN-MONTELUKAST ................................................. 129 MYLAN-MONTELUKAST ....................................... SEC 3.59 MYLAN-NABUMETONE .................................................... 72 MYLAN-NAPROXEN EC ................................................... 73 MYLAN-NIFEDIPINE EXTENDED RELEASE.................... 53 MYLAN-NITRO .................................................................. 42 MYLAN-OLANZAPINE ....................................................... 98 MYLAN-OLANZAPINE ....................................................... 99 MYLAN-OMEPRAZOLE (CAPSULE) ............................... 148 MYLAN-ONDANSETRON ................................................ 143 MYLAN-OXYBUTYNIN .................................................... 181 MYLAN-PANTOPRAZOLE .............................................. 148 MYLAN-PAROXETINE ...................................................... 92 MYLAN-PIOGLITAZONE ....................................... SEC 3.71 MYLAN-PRAMIPEXOLE .................................................. 118 MYLAN-PRAVASTATIN ..................................................... 38 MYLAN-QUETIAPINE ...................................................... 100 MYLAN-QUETIAPINE ........................................................ 99 MYLAN-RAMIPRIL (CAPSULE)......................................... 61 MYLAN-RAMIPRIL (CAPSULE)......................................... 62 MYLAN-RANITIDINE ....................................................... 146 MYLAN-RISEDRONATE ........................................ SEC 3.74 MYLAN-RISPERIDONE ................................................... 101 MYLAN-RISPERIDONE ................................................... 102 MYLAN-RIVASTIGMINE ........................................ SEC 3.77 MYLAN-SALBUTAMOL STERINEBS P.F. ......................... 23 MYLAN-SELEGILINE ....................................................... 119 MYLAN-SERTRALINE ....................................................... 92 MYLAN-SERTRALINE ....................................................... 93 MYLAN-SIMVASTATIN ...................................................... 39

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 210 EFFECTIVE APRIL 1, 2012
MYLAN-SIMVASTATIN ..................................................... 40 MYLAN-SOTALOL ............................................................ 51 MYLAN-SUMATRIPTAN ................................................. 114 MYLAN-SUMATRIPTAN ........................................ SEC 3.82 MYLAN-TAMSULOSIN ..................................................... 44 MYLAN-TERBINAFINE ..................................................... 14 MYLAN-TICLOPIDINE ...................................................... 30 MYLAN-TIMOLOL ........................................................... 136 MYLAN-TIZANIDINE .............................................. SEC 3.85 MYLAN-TOPIRAMATE ..................................................... 86 MYLAN-TOPIRAMATE ..................................................... 87 MYLAN-TRAZODONE ...................................................... 93 MYLAN-VALACYCLOVIR (CAPLET) ................................ 17 MYLAN-VALPROIC........................................................... 87 MYLAN-VALSARTAN HCTZ ............................................. 66 MYLAN-VENLAFAXINE XR .............................................. 89 MYLAN-VERAPAMIL ........................................................ 55 MYLAN-VERAPAMIL SR .................................................. 55 MYLAN-WARFARIN .......................................................... 27 MYLAN-WARFARIN .......................................................... 28 MYLAN-ZOLMITRIPTAN ................................................ 115 MYLAN-ZOLMITRIPTAN ....................................... SEC 3.93 MYLAN-ZOPICLONE ...................................................... 112 MYOCHRYSINE.............................................................. 151
N
NABILONE ...................................................................... 144 NABUMETONE ................................................................. 72 NADOLOL ......................................................................... 49 NADROPARIN CALCIUM ................................................. 29 NAFARELIN ACETATE ................................................... 187 NALCROM ...................................................................... 130 NAPROSYN ...................................................................... 73 NAPROSYN E ................................................................... 73 NAPROSYN SR ................................................................ 73 NAPROXEN ...................................................................... 72 NAPROXEN ...................................................................... 73 NAPROXEN EC ................................................................ 73 NAPROXEN SODIUM ....................................................... 74 NAPROXEN SODIUM DS ................................................. 74 NARATRIPTAN HCL ....................................................... 113 NARATRIPTAN HCL .............................................. SEC 3.60 NARDIL ............................................................................. 88 NASONEX ....................................................................... 132 NAVANE ......................................................................... 106 NEO-MEDROL ACNE ............................................ SEC 3.58 NEOMYCIN SULFATE/ POLYMYXIN B SULFATE......... 172 NEOMYCIN SULFATE/ POLYMYXIN B SULFATE/
GRAMICIDIN ............................................................... 131 NEORAL ................................................................ SEC 3.21
NEOSPORIN.................................................................... 172 NEOSTIGMINE BROMIDE ................................................ 21 NERISONE ...................................................................... 175 NERISONE OILY ............................................................. 175 NEULASTA (0.6 ML SYRINGE) ............................. SEC 3.64 NEULEPTIL ..................................................................... 105 NEUPOGEN........................................................... SEC 3.40 NEURONTIN ...................................................................... 84 NEURONTIN ...................................................................... 85 NIFEDIPINE ....................................................................... 53 NITOMAN .............................................................. SEC 3.85 NITRAZADON .................................................................. 111 NITRAZEPAM .................................................................. 111 NITRO-DUR 0.2 ................................................................. 43 NITRO-DUR 0.4 ................................................................. 43 NITRO-DUR 0.6 ................................................................. 43 NITRO-DUR 0.8 ................................................................. 43 NITROFURANTOIN ........................................................... 18 NITROGLYCERIN .............................................................. 42 NITROGLYCERIN .............................................................. 43 NITROL .............................................................................. 42 NITROLINGUAL PUMPSPRAY ......................................... 42 NITROSTAT ....................................................................... 42 NIZATIDINE ..................................................................... 145 NORETHINDRONE ......................................................... 159 NORETHINDRONE ACETATE/ ESTRADIOL-17B .......... 161 NORETHINDRONE ACETATE/ ETHINYL ESTRADIOL .. 159 NORETHINDRONE/ ETHINYL ESTRADIOL ................... 160 NORETHINDRONE/ ETHINYL ESTRADIOL/
NORETHINDRONE/ ETHINYL ESTRADIOL ............... 160 NORETHINDRONE/ ETHINYL ESTRADIOL/
NORETHINDRONE/ ETHINYL ESTRADIOL/ NORETHINDRONE/ ETHINYL ESTRADIOL ............... 160
NORFLOXACIN ................................................................. 10 NORGESTIMATE/ ETHINYL ESTRADIOL ...................... 160 NORGESTIMATE/ ETHINYL ESTRADIOL/
NORGESTIMATE/ ETHINYL ESTRADIOL/ NORGESTIMATE/ ETHINYL ESTRADIOL .................. 160
NORITATE ....................................................................... 171 NORPROLAC ........................................................ SEC 3.72 NORTRIPTYLINE HCL ...................................................... 95 NORVASC ......................................................................... 52 NOVAMILOR.................................................................... 126 NOVAMOXIN .......................................................................8 NOVAMOXIN .......................................................................9 NOVAMOXIN SUGAR-REDUCED .......................................9 NOVO-5 ASA ................................................................... 150 NOVO-ACEBUTOLOL ....................................................... 46 NOVO-ACYCLOVIR ........................................................... 16 NOVO-ALENDRONATE ........................................ SEC 3.14 NOVO-ALFUZOSIN PR ......................................... SEC 3.15

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 211
NOVO-ALPRAZOL .......................................................... 109 NOVO-AMIODARONE ...................................................... 34 NOVO-AMLODIPINE ........................................................ 52 NOVO-AMPICILLIN................................................ SEC 3.15 NOVO-ATENOL ................................................................ 46 NOVO-ATENOL ................................................................ 47 NOVO-ATENOLTHALIDONE ............................................ 47 NOVO-ATORVASTATIN ................................................... 36 NOVO-AZATHIOPRINE .................................................. 185 NOVO-AZITHROMYCIN ..................................................... 7 NOVO-BENZYDAMINE ................................................... 135 NOVO-BETAHISTINE ..................................................... 185 NOVO-BISOPROLOL ....................................................... 47 NOVO-BROMAZEPAM ................................................... 109 NOVO-BUSPIRONE ....................................................... 111 NOVO-CAPTORIL............................................................. 56 NOVO-CARBAMAZ........................................................... 83 NOVO-CEFADROXIL ............................................. SEC 3.19 NOVO-CHLOROQUINE .................................................... 17 NOVO-CHLORPROMAZINE ........................................... 104 NOVO-CILAZAPRIL .......................................................... 56 NOVO-CILAZAPRIL .......................................................... 57 NOVO-CILAZAPRIL/HCTZ ............................................... 57 NOVO-CIMETINE ........................................................... 144 NOVO-CIPROFLOXACIN ...................................... SEC 3A.2 NOVO-CIPROFLOXACIN ...................................... SEC 3A.3 NOVO-CITALOPRAM ....................................................... 90 NOVO-CLAVAMOXIN ......................................................... 9 NOVO-CLINDAMYCIN ...................................................... 13 NOVO-CLOBAZAM ........................................................... 81 NOVO-CLOBETASOL ..................................................... 174 NOVO-CLONAZEPAM ...................................................... 82 NOVO-CLONIDINE ......................................................... 185 NOVO-CLONIDINE ........................................................... 40 NOVO-CLOXIN ................................................................. 10 NOVO-CYCLOPRINE ....................................................... 25 NOVO-DESMOPRESSIN ................................................ 166 NOVO-DIFENAC ............................................................... 70 NOVO-DIFENAC SR ......................................................... 70 NOVO-DIFLUNISAL FC .................................................... 71 NOVO-DILTAZEM ............................................................. 53 NOVO-DILTAZEM CD ....................................................... 54 NOVO-DILTIAZEM HCL ER .............................................. 54 NOVO-DILTIAZEM HCL ER .............................................. 55 NOVO-DIVALPROEX ........................................................ 84 NOVO-DOMPERIDONE ................................................. 149 NOVO-DOXAZOSIN ......................................................... 44 NOVO-DOXEPIN .............................................................. 94 NOVO-DOXEPIN .............................................................. 95 NOVO-DOXYLIN ............................................................... 11 NOVO-ENALAPRIL ........................................................... 57 NOVO-ENALAPRIL ........................................................... 58
NOVO-ENALAPRIL/HCTZ ................................................. 58 NOVO-ETIDRONATECAL ............................................... 186 NOVO-FAMOTIDINE ....................................................... 145 NOVO-FENOFIBRATE MICRONIZED ............................... 35 NOVO-FENOFIBRATE-S ................................................... 35 NOVO-FENOFIBRATE-S (TABLET) .................................. 35 NOVO-FENTANYL 100 .......................................... SEC 3.39 NOVO-FENTANYL 25 ............................................ SEC 3.38 NOVO-FENTANYL 50 ............................................ SEC 3.39 NOVO-FENTANYL 75 ............................................ SEC 3.39 NOVO-FINASTERIDE ............................................ SEC 3.40 NOVO-FLUCONAZOLE ..................................................... 14 NOVO-FLUOXETINE ......................................................... 91 NOVO-FLURPROFEN ....................................................... 71 NOVO-FLUTAMIDE ............................................... SEC 3.41 NOVO-FLUVOXAMINE ...................................................... 91 NOVO-FOSINOPRIL .......................................................... 58 NOVO-FURANTOIN .......................................................... 18 NOVO-GABAPENTIN ........................................................ 84 NOVO-GABAPENTIN ........................................................ 85 NOVO-GEMFIBROZIL ....................................................... 35 NOVO-GLICLAZIDE ........................................................ 164 NOVO-GLYBURIDE ......................................................... 165 NOVO-HYDRAZIDE ......................................................... 126 NOVO-HYDROXYZIN ...................................................... 112 NOVO-INDAPAMIDE ....................................................... 127 NOVO-IPRAMIDE .............................................................. 22 NOVO-KETOCONAZOLE .................................................. 14 NOVO-KETOROLAC ......................................................... 72 NOVO-KETOTIFEN .............................................................1 NOVO-LAMOTRIGINE ....................................................... 85 NOVO-LANSOPRAZOLE ................................................ 147 NOVO-LEFLUNOMIDE .................................................... 187 NOVO-LEVOCARBIDOPA ............................................... 117 NOVO-LEVOFLOXACIN ........................................ SEC 3A.4 NOVO-LEXIN .......................................................................3 NOVO-LEXIN .......................................................................4 NOVO-LISINOPRIL (TYPE P)............................................ 59 NOVO-LISINOPRIL (TYPE Z) ............................................ 59 NOVO-LISINOPRIL/HCTZ (TYPE P) ................................. 60 NOVO-LISINOPRIL/HCTZ (TYPE Z) ................................. 60 NOVO-LORAZEM ............................................................ 110 NOVO-LOVASTATIN ......................................................... 37 NOVO-MAPROTILINE ....................................................... 95 NOVO-MEDRONE ........................................................... 166 NOVO-METFORMIN ........................................................ 162 NOVO-METHACIN ............................................................. 71 NOVO-METOPROL ........................................................... 49 NOVO-METOPROL (FC) ................................................... 49 NOVO-MEXILETINE .......................................................... 33 NOVO-MINOCYCLINE ...................................................... 12 NOVO-MIRTAZAPINE ....................................................... 97

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 212 EFFECTIVE APRIL 1, 2012
NOVO-MOCLOBEMIDE .................................................... 88 NOVO-MORPHINE SR ..................................................... 78 NOVO-NABUMETONE ..................................................... 72 NOVO-NADOLOL ............................................................. 49 NOVO-NAPROX ............................................................... 72 NOVO-NAPROX ............................................................... 73 NOVO-NAPROX EC ......................................................... 73 NOVO-NAPROX SODIUM ................................................ 74 NOVO-NAPROX SODIUM DS .......................................... 74 NOVO-NARATRIPTAN ................................................... 113 NOVO-NARATRIPTAN .......................................... SEC 3.60 NOVO-NIZATIDINE......................................................... 145 NOVO-NORFLOXACIN ..................................................... 10 NOVO-NORTRIPTYLINE .................................................. 95 NOVO-OLANZAPINE ........................................................ 98 NOVO-OLANZAPINE ........................................................ 99 NOVO-OLANZAPINE OD ................................................. 99 NOVO-OMEPRAZOLE (DELAYED RELEASE TABLET) 148 NOVO-ONDANSETRON ................................................. 143 NOVO-OXYBUTYNIN ..................................................... 181 NOVO-PANTOPRAZOLE ............................................... 148 NOVO-PAROXETINE ....................................................... 92 NOVO-PEN-VK ................................................................... 8 NOVO-PERIDOL ............................................................. 103 NOVO-PERIDOL ............................................................. 104 NOVO-PINDOL ................................................................. 50 NOVO-PIOGLITAZONE ......................................... SEC 3.71 NOVO-PIROCAM .............................................................. 74 NOVO-PRAMIPEXOLE ................................................... 118 NOVO-PRANOL ................................................................ 50 NOVO-PRAVASTATIN ...................................................... 38 NOVO-PRAZIN ................................................................. 44 NOVO-PROFEN................................................................ 71 NOVO-QUETIAPINE ....................................................... 100 NOVO-QUETIAPINE ......................................................... 99 NOVO-QUININE................................................................ 18 NOVO-RABEPRAZOLE .................................................. 149 NOVO-RALOXIFENE ............................................. SEC 3.73 NOVO-RAMIPRIL (CAPSULE) ......................................... 61 NOVO-RAMIPRIL (CAPSULE) ......................................... 62 NOVO-RANIDINE ........................................................... 146 NOVO-RISEDRONATE .......................................... SEC 3.74 NOVO-RISPERIDONE .................................................... 101 NOVO-RISPERIDONE .................................................... 102 NOVO-RIVASTIGMINE .......................................... SEC 3.77 NOVO-RYTHRO EES ......................................................... 6 NOVO-RYTHRO ESTOLATE .............................................. 6 NOVO-SELEGILINE........................................................ 119 NOVO-SEMIDE ................................................................. 41 NOVO-SERTRALINE ........................................................ 92 NOVO-SERTRALINE ........................................................ 93 NOVO-SIMVASTATIN ....................................................... 39
NOVO-SIMVASTATIN ....................................................... 40 NOVO-SOTALOL ............................................................... 51 NOVO-SPIROTON ............................................................. 67 NOVO-SPIROZINE ............................................................ 67 NOVO-SUCRALATE ........................................................ 147 NOVO-SUMATRIPTAN .................................................... 114 NOVO-SUMATRIPTAN .......................................... SEC 3.82 NOVO-SUMATRIPTAN DF .............................................. 114 NOVO-SUMATRIPTAN DF .................................... SEC 3.82 NOVO-SUNDAC ................................................................ 74 NOVO-TAMSULOSIN ........................................................ 44 NOVO-TEMAZEPAM ....................................................... 111 NOVO-TERAZOSIN ........................................................... 45 NOVO-TERBINAFINE ........................................................ 14 NOVO-TIAPROFENIC ....................................................... 74 NOVO-TICLOPIDINE ......................................................... 30 NOVO-TIMOL .................................................................... 51 NOVO-TOPIRAMATE ........................................................ 86 NOVO-TOPIRAMATE ........................................................ 87 NOVO-TRAZODONE ......................................................... 93 NOVO-TRIAMZIDE .......................................................... 126 NOVO-TRIMEL .................................................................. 11 NOVO-TRIMEL DS ............................................................ 11 NOVO-VALPROIC ............................................................. 87 NOVO-VENLAFAXINE XR ................................................. 89 NOVO-VERAMIL SR .......................................................... 55 NOVO-WARFARIN ............................................................ 27 NOVO-WARFARIN ............................................................ 28 NOVO-ZOPICLONE ......................................................... 112 NOVOLIN GE 30/70 ......................................................... 163 NOVOLIN GE 30/70 CARTRIDGE ................................... 163 NOVOLIN GE 40/60 CARTRIDGE ................................... 163 NOVOLIN GE 50/50 CARTRIDGE ................................... 163 NOVOLIN GE NPH .......................................................... 163 NOVOLIN GE NPH CARTRIDGE .................................... 163 NOVOLIN GE TORONTO ................................................ 163 NOVOLIN GE TORONTO CARTRIDGE .......................... 163 NOVORAPID.................................................................... 163 NOVORAPID CARTRIDGE ............................................. 163 NOZINAN ......................................................................... 105 NU-ACEBUTOLOL ............................................................. 46 NU-ACYCLOVIR ................................................................ 16 NU-AMILZIDE .................................................................. 126 NU-AMOXI ...........................................................................8 NU-AMOXI ...........................................................................9 NU-BACLO ........................................................................ 25 NU-BECLOMETHASONE ................................................ 132 NU-BUSPIRONE .............................................................. 111 NU-CAPTO ........................................................................ 56 NU-CARBAMAZEPINE ...................................................... 83 NU-CEPHALEX....................................................................3 NU-CIMET ....................................................................... 144

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 213
NU-COTRIMOX................................................................. 11 NU-COTRIMOX DS........................................................... 11 NU-CYCLOBENZAPRINE ................................................. 25 NU-DICLO ......................................................................... 70 NU-DILTIAZ ...................................................................... 53 NU-DILTIAZ-CD ................................................................ 54 NU-DIVALPROEX ............................................................. 84 NU-DOMPERIDONE ....................................................... 149 NU-DOXYCYCLINE .......................................................... 11 NU-FAMOTIDINE ............................................................ 145 NU-FLUOXETINE ............................................................. 91 NU-FLURBIPROFEN ........................................................ 71 NU-FLUVOXAMINE .......................................................... 91 NU-GEMFIBROZIL............................................................ 35 NU-GLYBURIDE ............................................................. 165 NU-IBUPROFEN ............................................................... 71 NU-INDAPAMIDE............................................................ 127 NU-INDO ........................................................................... 71 NU-KETOCON .................................................................. 14 NU-KETOROLAC .............................................................. 72 NU-LEVOCARB .............................................................. 117 NU-METFORMIN ............................................................ 162 NU-METOCLOPRAMIDE ................................................ 149 NU-METOP ....................................................................... 49 NU-MOCLOBEMIDE ......................................................... 88 NU-NAPROX ..................................................................... 72 NU-NAPROX ..................................................................... 73 NU-NORTRIPTYLINE ....................................................... 95 NU-OXYBUTYN .............................................................. 181 NU-PEN-VK ........................................................................ 8 NU-PINDOL ...................................................................... 50 NU-PIROX ......................................................................... 74 NU-PRAZO ....................................................................... 44 NU-RANIT ....................................................................... 146 NU-SELEGILINE ............................................................. 119 NU-SOTALOL ................................................................... 51 NU-SUCRALFATE .......................................................... 147 NU-SULINDAC .................................................................. 74 NU-TERAZOSIN ............................................................... 45 NU-TIAPROFENIC ............................................................ 74 NU-TICLOPIDINE ............................................................. 30 NU-TIMOLOL .................................................................... 51 NU-TRAZODONE ............................................................. 93 NU-TRAZODONE-D .......................................................... 93 NU-TRIAZIDE ................................................................. 126 NU-VALPROIC .................................................................. 87 NU-VERAP ........................................................................ 55 NU-ZOPICLONE ............................................................. 112 NYLIDRIN HCL ................................................................. 43 NYSTATIN ........................................................................ 15
O
OCTOSTIM ...................................................................... 166 OCTREOTIDE........................................................ SEC 3.60 OCTREOTIDE ACETATE ...................................... SEC 3.60 OCTREOTIDE ACETATE ...................................... SEC 3.61 OCTREOTIDE ACETATE OMEGA ........................ SEC 3.60 OCUFLOX ........................................................................ 131 OESCLIM 25 (5 MG/PTH) ................................................ 161 OESCLIM 50 (10 MG/PTH) .............................................. 161 OFLOXACIN .................................................................... 131 OFLOXACIN .......................................................... SEC 3A.5 OLANZAPINE .................................................................... 98 OLANZAPINE .................................................................... 99 OLANZAPINE ODT ............................................................ 99 OLESTYR LIGHT ............................................................... 34 OLESTYR REGULAR ........................................................ 34 OLMESARTAN MEDOXOMIL............................................ 42 OLMESARTAN MEDOXOMIL/ HYDROCHLOROTHIAZIDE
....................................................................................... 42 OLMETEC .......................................................................... 42 OLMETEC PLUS ............................................................... 42 OLSALAZINE SODIUM .................................................... 150 OMALIZUMAB ....................................................... SEC 3.63 OMEPRAZOLE ................................................................ 148 OMEPRAZOLE (CAPSULE) ............................................ 148 OMNITROPE ......................................................... SEC 3.80 ONABOTULINUMTOXINA ............................................... 187 ONDANSETRON ............................................................. 142 ONDANSETRON ............................................................. 143 ONDANSETRON (PRESERVATIVE FREE) .................... 143 ONDANSETRON (PRESERVED) .................................... 143 ONDANSETRON (UNPRESERVED) ............................... 143 ONDANSETRON (WITH PRESERVATIVE) .................... 143 ONDANSETRON HCL DIHYDRATE ............................... 143 ONDANSETRON OMEGA (PRESERVATIVE FREE) ...... 143 ONDANSETRON OMEGA (WITH PRESERVATIVE) ...... 143 ONDANSETRON-ODAN .................................................. 143 ONE-ALPHA .................................................................... 183 ONGLYZA .............................................................. SEC 3.79 OPIUM/ BELLADONNA ..................................................... 79 OPTICHAMBER ADVANTAGE II (CHAMBER ONLY) ..... 189 OPTICHAMBER ADVANTAGE II (WITH LARGE MASK) 189 OPTICHAMBER ADVANTAGE II (WITH MEDIUM MASK)
..................................................................................... 189 OPTICHAMBER ADVANTAGE II (WITH SMALL MASK) 189 OPTIMYXIN PLUS ........................................................... 131 ORACORT ....................................................................... 177 ORAP ............................................................................... 107 ORCIPRENALINE SULFATE ............................................. 23 ORENCIA ................................................................. SEC 3.6

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 214 EFFECTIVE APRIL 1, 2012
ORGARAN ............................................................. SEC 3.21 ORTHO 0.5/35 (21 DAY) ................................................. 160 ORTHO 0.5/35 (28 DAY) ................................................. 160 ORTHO 1/35 (21 DAY) .................................................... 160 ORTHO 1/35 (28 DAY) .................................................... 160 ORTHO 7/7/7 (21 DAY) ................................................... 160 ORTHO 7/7/7 (28 DAY) ................................................... 160 ORTHO-CEPT (28 DAY) ................................................. 158 OXAZEPAM .................................................................... 111 OXEZE TURBUHALER ..................................................... 23 OXSORALEN .................................................................. 178 OXSORALEN ULTRA ..................................................... 178 OXTRIPHYLLINE ............................................................ 181 OXTRIPHYLLINE/ GUAIFENESIN .................................. 181 OXY-IR .............................................................................. 80 OXYBUTYNIN ................................................................. 181 OXYBUTYNIN CHLORIDE ............................................. 181 OXYBUTYNIN CHLORIDE .................................... SEC 3.63 OXYCODONE HCL ........................................................... 80 OXYCODONE HCL/ ACETAMINOPHEN .......................... 80 OXYCODONE HCL/ ASA .................................................. 81 OXYCODONE/ACET ........................................................ 80 OXYCONTIN ..................................................................... 80 OXYNEO ........................................................................... 80
P
PALIPERIDONE PALMITATE ................................ SEC 3.64 PAMIDRONATE DISODIUM ........................................... 187 PAMIDRONATE DISODIUM OMEGA ............................. 187 PANCREASE MT 10 ....................................................... 141 PANCREASE MT 16 ....................................................... 141 PANCREASE MT 4 ......................................................... 141 PANECTYL ......................................................................... 1 PANOXYL 10 ......................................................... SEC 3.18 PANOXYL 20 ......................................................... SEC 3.18 PANTOLOC .................................................................... 148 PANTOPRAZOLE ........................................................... 148 PAPAVERINE HCL ................................................ SEC 3.64 PARIET ........................................................................... 149 PARNATE ......................................................................... 88 PAROXETINE ................................................................... 92 PAROXETINE HCL ........................................................... 92 PARSITAN ...................................................................... 116 PAT-GALANTAMINE ER ....................................... SEC 3.41 PAXIL ................................................................................ 92 PEDIAPRED ................................................................... 157 PEGASYS (0.5 ML SYRINGE) .......................................... 16 PEGASYS (0.5 ML SYRINGE) ............................... SEC 3.66 PEGASYS RBV (KIT) ............................................. SEC 3.68 PEGETRON (KIT) .................................................. SEC 3.70
PEGETRON REDIPEN (KIT) ................................. SEC 3.70 PEGFILGRASTIM .................................................. SEC 3.64 PEGINTERFERON ALFA-2A ............................................. 16 PEGINTERFERON ALFA-2A ................................. SEC 3.66 PEGINTERFERON ALFA-2A/ RIBAVIRIN ............. SEC 3.68 PEGINTERFERON ALFA-2B/ RIBAVIRIN ............. SEC 3.70 PENICILLAMINE .............................................................. 153 PENICILLIN G SODIUM ......................................................8 PENICILLIN V POTASSIUM ................................................8 PENTASA ........................................................................ 150 PENTASA (1G/100ML) .................................................... 150 PENTASA (4G/100 ML) ................................................... 150 PENTAZOCINE HCL ......................................................... 81 PENTAZOCINE LACTATE ................................................ 81 PENTOSAN POLYSULFATE SODIUM ........................... 187 PENTOXIFYLLINE ............................................................. 31 PEPCID ............................................................................ 145 PERCOCET ....................................................................... 80 PERCOCET DEMI ............................................................. 80 PERICYAZINE ................................................................. 105 PERINDOPRIL ERBUMINE ............................................... 60 PERINDOPRIL ERBUMINE/ INDAPAMIDE HEMIHYDRATE
....................................................................................... 60 PERPHENAZINE ............................................................. 105 PHENELZINE SULFATE ................................................... 88 PHENOBARB................................................................... 108 PHENOBARBITAL ........................................................... 108 PHENYLEPHRINE HCL ................................................... 135 PHENYTOIN ...................................................................... 82 PHENYTOIN SODIUM ....................................................... 82 PHL-AMLODIPINE ............................................................. 52 PHL-ATENOLOL ................................................................ 46 PHL-ATENOLOL ................................................................ 47 PHL-AZITHROMYCIN ..........................................................7 PHL-BACLOFEN ................................................................ 25 PHL-CARVEDILOL ............................................................ 48 PHL-CITALOPRAM ............................................................ 90 PHL-CLONAZEPAM .......................................................... 82 PHL-CLONAZEPAM-R ...................................................... 82 PHL-FLUOXETINE ............................................................ 91 PHL-ONDANSETRON ..................................................... 143 PHL-PIOGLITAZONE ............................................ SEC 3.71 PHL-RANITIDINE ............................................................. 146 PHL-RISPERIDONE ........................................................ 101 PHL-RISPERIDONE ........................................................ 102 PHL-SERTRALINE ............................................................ 92 PHL-SERTRALINE ............................................................ 93 PHL-SIMVASTATIN ........................................................... 39 PHL-SIMVASTATIN ........................................................... 40 PHL-TOPIRAMATE ............................................................ 86 PHL-TOPIRAMATE ............................................................ 87 PHOSPHATE-NOVARTIS ............................................... 125

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 215
PHYTONADIONE............................................................ 183 PILOCARPINE HCL ........................................................ 137 PILOCARPINE HCL .......................................................... 21 PILOPINE HS .................................................................. 137 PIMOZIDE ....................................................................... 107 PINAVERIUM BROMIDE ................................................ 150 PINDOLOL ........................................................................ 50 PINDOLOL/ HYDROCHLOROTHIAZIDE .......................... 50 PIOGLITAZONE HCL ............................................. SEC 3.71 PIOGLITAZONE HYDROCHLORIDE .................... SEC 3.71 PIPERACILLIN AND TAZOBACTAM ..................... SEC 3.72 PIPERACILLIN SODIUM/ TAZOBACTAM SODIUMSEC 3.72 PIPERACILLIN SODIUM/TAZOBACTAM SODIUMSEC 3.72 PIPORTIL L4 ................................................................... 105 PIPOTIAZINE PALMITATE ............................................. 105 PIPRADROL HCL/ THIAMINE HCL/ RIBOFLAVIN/
PYRIDOXINE HCL/ NIACINAMIDE/ CHOLINE/ INOSITOL .............................................................................. 184 PIROXICAM ...................................................................... 74 PIZOTIFEN MALATE ...................................................... 115 PIZOTIFEN MALATE ...................................................... 119 PLAN B ........................................................................... 159 PLAQUENIL SULFATE ..................................................... 17 PLAVIX ................................................................... SEC 3.20 PLENDIL ........................................................................... 52 PLENDIL ........................................................................... 53 PMS - POTASSIUM CHLORIDE ..................................... 125 PMS-ALENDRONATE-FC ..................................... SEC 3.14 PMS-AMANTADINE HYDROCHLORIDE ....................... 115 PMS-AMIODARONE ......................................................... 34 PMS-AMLODIPINE ........................................................... 52 PMS-AMOXICILLIN............................................................. 8 PMS-AMOXICILLIN............................................................. 9 PMS-ATENOLOL .............................................................. 46 PMS-ATENOLOL .............................................................. 47 PMS-ATORVASTATIN ...................................................... 36 PMS-AZITHROMYCIN ........................................................ 7 PMS-AZITHROMYCIN ........................................... SEC 3.17 PMS-BACLOFEN .............................................................. 25 PMS-BENZTROPINE ...................................................... 116 PMS-BENZYDAMINE ..................................................... 135 PMS-BISOPROLOL .......................................................... 47 PMS-BRIMONIDINE ....................................................... 135 PMS-BUPROPION SR ...................................................... 96 PMS-BUSPIRONE .......................................................... 111 PMS-CARBAMAZEPINE ................................................... 83 PMS-CARBAMAZEPINE-CR ............................................ 83 PMS-CARVEDILOL........................................................... 48 PMS-CHLORAL HYDRATE ............................................ 112 PMS-CILAZAPRIL ............................................................. 56 PMS-CILAZAPRIL ............................................................. 57 PMS-CIPROFLOXACIN .................................................. 131 PMS-CIPROFLOXACIN ......................................... SEC 3A.2
PMS-CIPROFLOXACIN ......................................... SEC 3A.3 PMS-CITALOPRAM ........................................................... 90 PMS-CLARITHROMYCIN ....................................................7 PMS-CLOBAZAM .............................................................. 81 PMS-CLOBETASOL ........................................................ 174 PMS-CLOBETASOL ........................................................ 175 PMS-CLONAZEPAM ......................................................... 82 PMS-CLONAZEPAM-R ...................................................... 82 PMS-CLOPIDOGREL ............................................ SEC 3.20 PMS-CYCLOBENZAPRINE ............................................... 25 PMS-DEFEROXAMINE ................................................... 153 PMS-DESMOPRESSIN ................................................... 166 PMS-DESONIDE ............................................................. 175 PMS-DEXAMETHASONE ................................................ 156 PMS-DEXAMETHASONE SODIUM PHOSP ................... 156 PMS-DICLOFENAC ........................................................... 70 PMS-DICLOFENAC-SR ..................................................... 70 PMS-DILTIAZEM CD ......................................................... 54 PMS-DOMPERIDONE ..................................................... 149 PMS-DOXAZOSIN ............................................................. 44 PMS-ENALAPRIL .............................................................. 57 PMS-ENALAPRIL .............................................................. 58 PMS-ERYTHROMYCIN ................................................... 131 PMS-FENOFIBRATE MICRO ............................................ 35 PMS-FENTANYL MTX ........................................... SEC 3.38 PMS-FENTANYL MTX ........................................... SEC 3.39 PMS-FINASTERIDE .............................................. SEC 3.40 PMS-FLUCONAZOLE ........................................................ 14 PMS-FLUOROMETHOLONE........................................... 132 PMS-FLUOXETINE ............................................................ 91 PMS-FLUTAMIDE .................................................. SEC 3.41 PMS-FLUVOXAMINE ........................................................ 91 PMS-GABAPENTIN ........................................................... 84 PMS-GABAPENTIN ........................................................... 85 PMS-GEMFIBROZIL .......................................................... 35 PMS-GLYBURIDE ........................................................... 165 PMS-HYDROCHLOROTHIAZIDE .................................... 126 PMS-HYDROMORPHONE ................................................ 76 PMS-HYDROMORPHONE ................................................ 77 PMS-HYDROXYZINE ...................................................... 112 PMS-INDAPAMIDE .......................................................... 127 PMS-IPRATROPIUM ......................................................... 22 PMS-IPRATROPIUM ............................................. SEC 3.54 PMS-IPRATROPIUM (1ML) ................................... SEC 3.54 PMS-IPRATROPIUM (2ML) ................................... SEC 3.54 PMS-IRBESARTAN ........................................................... 63 PMS-IRBESARTAN ........................................................... 64 PMS-IRBESARTAN-HCTZ ................................................ 64 PMS-ISMN ......................................................................... 42 PMS-KETOPROFEN ......................................................... 72 PMS-LACTULOSE ........................................................... 125 PMS-LAMOTRIGINE ......................................................... 85

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 216 EFFECTIVE APRIL 1, 2012
PMS-LEVETIRACETAM ................................................... 86 PMS-LEVOBUNOLOL ..................................................... 136 PMS-LEVOFLOXACIN ........................................... SEC 3A.4 PMS-LISINOPRIL.............................................................. 59 PMS-LITHIUM CARBONATE .......................................... 113 PMS-LORAZEPAM ......................................................... 110 PMS-LOVASTATIN ........................................................... 37 PMS-METFORMIN.......................................................... 162 PMS-METHYLPHENIDATE ............................................ 108 PMS-METOCLOPRAMIDE ............................................. 149 PMS-METOPROLOL-L ..................................................... 49 PMS-MINOCYCLINE ........................................................ 12 PMS-MIRTAZAPINE ......................................................... 97 PMS-MONTELUKAST .................................................... 129 PMS-MONTELUKAST ........................................... SEC 3.59 PMS-MONTELUKAST FC ............................................... 129 PMS-MONTELUKAST FC ...................................... SEC 3.59 PMS-NAPROXEN ............................................................. 73 PMS-NAPROXEN EC ....................................................... 73 PMS-NIZATIDINE ........................................................... 145 PMS-NORFLOXACIN ....................................................... 10 PMS-NORTRIPTYLINE ..................................................... 95 PMS-NYSTATIN................................................................ 15 PMS-OFLOXACIN........................................................... 131 PMS-OLANZAPINE........................................................... 98 PMS-OLANZAPINE........................................................... 99 PMS-OLANZAPINE ODT .................................................. 99 PMS-OMEPRAZOLE (SUSTAINED-RELEASE CAPSULE)
.................................................................................... 148 PMS-OMEPRAZOLE DR (DELAYED RELEASE TABLET)
.................................................................................... 148 PMS-ONDANSETRON ................................................... 143 PMS-OXTRIPHYLLINE ................................................... 181 PMS-OXYBUTYNIN ........................................................ 181 PMS-OXYCODONE .......................................................... 80 PMS-PANTOPRAZOLE .................................................. 148 PMS-PAROXETINE .......................................................... 92 PMS-PINDOLOL ............................................................... 50 PMS-PIOGLITAZONE ............................................ SEC 3.71 PMS-PIROXICAM ............................................................. 74 PMS-PRAMIPEXOLE ...................................................... 118 PMS-PRAVASTATIN ........................................................ 38 PMS-PREDNISOLONE ................................................... 157 PMS-PROCYCLIDINE .................................................... 116 PMS-QUETIAPINE.......................................................... 100 PMS-QUETIAPINE............................................................ 99 PMS-RABEPRAZOLE EC ............................................... 149 PMS-RALOXIFENE................................................ SEC 3.73 PMS-RAMIPRIL (CAPSULE) ............................................ 61 PMS-RAMIPRIL (CAPSULE) ............................................ 62 PMS-RAMIPRIL-HCTZ ...................................................... 62 PMS-RANITIDINE ........................................................... 146
PMS-REPAGLINIDE ........................................................ 164 PMS-RISEDRONATE ............................................ SEC 3.74 PMS-RISPERIDONE ....................................................... 101 PMS-RISPERIDONE ....................................................... 102 PMS-RISPERIDONE ....................................................... 103 PMS-RISPERIDONE ODT ............................................... 103 PMS-RIVASTIGMINE ............................................ SEC 3.77 PMS-ROPINIROLE .......................................................... 118 PMS-ROPINIROLE .......................................................... 119 PMS-SALBUTAMOL .......................................................... 23 PMS-SALBUTAMOL POLYNEB ........................................ 23 PMS-SERTRALINE ............................................................ 92 PMS-SERTRALINE ............................................................ 93 PMS-SIMVASTATIN .......................................................... 39 PMS-SIMVASTATIN .......................................................... 40 PMS-SOD POLYSTYR SULF (120 ML) ........................... 126 PMS-SODIUM CROMOGLYCATE .................................. 130 PMS-SODIUM POLYSTYRENE SULF. ........................... 126 PMS-SOTALOL.................................................................. 51 PMS-SULFASALAZINE ..................................................... 11 PMS-SUMATRIPTAN ...................................................... 114 PMS-SUMATRIPTAN ............................................ SEC 3.82 PMS-TERAZOSIN .............................................................. 45 PMS-TERBINAFINE .......................................................... 14 PMS-TIMOLOL ................................................................ 136 PMS-TOBRAMYCIN ........................................................ 131 PMS-TOPIRAMATE ........................................................... 86 PMS-TOPIRAMATE ........................................................... 87 PMS-TRAZODONE ............................................................ 93 PMS-URSODIOL C .......................................................... 141 PMS-VALACYCLOVIR (CAPLET) ..................................... 17 PMS-VALPROIC ACID ...................................................... 87 PMS-VALPROIC ACID E.C. .............................................. 87 PMS-VANCOMYCIN .......................................................... 12 PMS-VENLAFAXINE XR ................................................... 89 PMS-VERAPAMIL SR ........................................................ 55 PMS-ZOLMITRIPTAN ...................................................... 115 PMS-ZOLMITRIPTAN ............................................ SEC 3.93 PMS-ZOLMITRIPTAN ODT ............................................. 115 PMS-ZOLMITRIPTAN ODT ................................... SEC 3.93 PMS-ZOPICLONE ........................................................... 112 PODOFILOX .................................................................... 179 PORTIA 21 ....................................................................... 159 PORTIA 28 ....................................................................... 159 POTABA .......................................................................... 179 POTASSIUM CHLORIDE (K+) ......................................... 125 POTASSIUM CHLORIDE (K+)(CL-) ................................ 125 POTASSIUM CITRATE (K+) ............................................ 125 PRAMIPEXOLE ............................................................... 118 PRAMIPEXOLE DIHYDROCHLORIDE ........................... 118 PRAVACHOL ..................................................................... 38 PRAVASTATIN .................................................................. 38

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 217
PRAVASTATIN SODIUM .................................................. 38 PRAZOSIN HCL ................................................................ 44 PRED FORTE ................................................................. 133 PRED MILD ..................................................................... 133 PREDNISOLONE ACETATE .......................................... 133 PREDNISOLONE ACETATE/ SULFACETAMIDE SODIUM
.................................................................................... 133 PREDNISOLONE SODIUM PHOSPHATE ..................... 157 PREDNISONE ................................................................ 158 PREMARIN ..................................................................... 160 PREVACID ...................................................................... 147 PREVEX B ...................................................................... 173 PREVEX HC ................................................................... 176 PRIMAQUINE PHOSPHATE ............................................ 17 PRIMAXIN .............................................................. SEC 3.46 PRIMIDONE ...................................................................... 81 PRINIVIL ........................................................................... 59 PRINZIDE ......................................................................... 60 PROBENECID ................................................................ 127 PROCAINAMIDE HCL ...................................................... 33 PROCAN SR ..................................................................... 33 PROCHLORPERAZINE .................................................. 142 PROCTODAN-HC ........................................................... 176 PROCTOFOAM-HC ........................................................ 176 PROCTOL ....................................................................... 178 PROCTOSEDYL ............................................................. 178 PROCYCLIDINE HCL ..................................................... 116 PROGESTERONE .......................................................... 166 PROGLYCEM ................................................................... 41 PROLIA .................................................................. SEC 3.23 PROLOPA 100-25 ........................................................... 116 PROLOPA 200-50 ........................................................... 116 PROLOPA 50-12.5 .......................................................... 116 PROMETHAZINE ................................................................ 1 PROMETHAZINE HCL ........................................................ 1 PROMETRIUM ................................................................ 166 PROPADERM ................................................................. 173 PROPAFENONE HCL ....................................................... 33 PROPARACAINE HCL .................................................... 134 PROPRANOLOL HCL ....................................................... 50 PROPYL-THYRACIL ....................................................... 168 PROPYLTHIOURACIL .................................................... 168 PROSCAR ............................................................. SEC 3.40 PROSTIGMIN ................................................................... 21 PROSTIN VR .................................................................... 43 PROTOPIC ............................................................ SEC 3.83 PROTOPIC ............................................................ SEC 3.84 PROVERA ....................................................................... 166 PROZAC ........................................................................... 91 PULMICORT NEBUAMP ................................................ 155 PULMICORT TURBUHALER .......................................... 155 PYRIDOSTIGMINE BROMIDE ......................................... 21
PYRIMETHAMINE ............................................................. 17
Q
QUETIAPINE ................................................................... 100 QUETIAPINE ..................................................................... 99 QUETIAPINE FUMARATE ............................................... 100 QUETIAPINE FUMARATE ................................................. 99 QUINAGOLIDE ...................................................... SEC 3.72 QUINAPRIL HCL ................................................................ 60 QUINAPRIL HCL ................................................................ 61 QUINAPRIL HCL/ HYDROCHLOROTHIAZIDE ................. 61 QUININE SULFATE ........................................................... 18 QVAR CFC-FREE ............................................................ 155
R
RABEPRAZOLE EC ......................................................... 149 RABEPRAZOLE SODIUM ............................................... 149 RALOXIFENE HCL ................................................ SEC 3.73 RAMIPRIL .......................................................................... 61 RAMIPRIL .......................................................................... 62 RAMIPRIL (CAPSULE) ...................................................... 61 RAMIPRIL (CAPSULE) ...................................................... 62 RAMIPRIL/ HYDROCHLOROTHIAZIDE ............................ 62 RAN-AMLODIPINE ............................................................ 52 RAN-ATENOLOL ............................................................... 46 RAN-ATENOLOL ............................................................... 47 RAN-ATORVASTATIN ....................................................... 36 RAN-CARVEDILOL ............................................................ 48 RAN-CEFPROZIL ................................................................4 RAN-CIPROFLOX .................................................. SEC 3A.2 RAN-CIPROFLOX .................................................. SEC 3A.3 RAN-CITALO ..................................................................... 90 RAN-DOMPERIDONE ..................................................... 149 RAN-ENALAPRIL ............................................................... 57 RAN-ENALAPRIL ............................................................... 58 RAN-FENTANYL MATRIX ..................................... SEC 3.38 RAN-FENTANYL MATRIX ..................................... SEC 3.39 RAN-FINASTERIDE ............................................... SEC 3.40 RAN-FOSINOPRIL ............................................................. 58 RAN-GABAPENTIN ........................................................... 84 RAN-GABAPENTIN ........................................................... 85 RAN-IRBESARTAN HCTZ ................................................. 64 RAN-LISINOPRIL ............................................................... 59 RAN-METFORMIN ........................................................... 162 RAN-OMEPRAZOLE (DELAYED RELEASE TABLET) ... 148 RAN-ONDANSETRON .................................................... 143 RAN-PANTOPRAZOLE ................................................... 148 RAN-PRAVASTATIN ......................................................... 38 RAN-RABEPRAZOLE ...................................................... 149
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 218 EFFECTIVE APRIL 1, 2012
RAN-RAMIPRIL (CAPSULE) ............................................ 61 RAN-RAMIPRIL (CAPSULE) ............................................ 62 RAN-RANITIDINE ........................................................... 146 RAN-RISPERIDONE ....................................................... 101 RAN-RISPERIDONE ....................................................... 102 RAN-ROPINIROLE ......................................................... 118 RAN-ROPINIROLE ......................................................... 119 RAN-SERTRALINE ........................................................... 92 RAN-SERTRALINE ........................................................... 93 RAN-SIMVASTATIN .......................................................... 39 RAN-SIMVASTATIN .......................................................... 40 RAN-TAMSULOSIN .......................................................... 44 RAN-VALSARTAN ............................................................ 65 RAN-ZOPICLONE ........................................................... 112 RANIBIZUMAB ................................................................ 139 RANITIDINE .................................................................... 146 RANITIDINE HCL ............................................................ 146 RATIO-ACLAVULANATE .................................................... 9 RATIO-ACLAVULANATE 125F ........................................... 9 RATIO-ACLAVULANATE 250F ........................................... 9 RATIO-ACYCLOVIR ......................................................... 16 RATIO-ALENDRONATE ........................................ SEC 3.14 RATIO-AMCINONIDE ..................................................... 173 RATIO-AMIODARONE ...................................................... 34 RATIO-AMLODIPINE ........................................................ 52 RATIO-ATENOLOL ........................................................... 46 RATIO-ATENOLOL ........................................................... 47 RATIO-ATORVASTATIN ................................................... 36 RATIO-AZITHROMYCIN ..................................................... 7 RATIO-BACLOFEN ........................................................... 25 RATIO-BRIMONIDINE .................................................... 135 RATIO-BUPROPION SR ................................................... 96 RATIO-CARVEDILOL ....................................................... 48 RATIO-CEFUROXIME ........................................................ 5 RATIO-CIPROFLOXACIN ...................................... SEC 3A.2 RATIO-CIPROFLOXACIN ...................................... SEC 3A.3 RATIO-CITALOPRAM ....................................................... 90 RATIO-CLARITHROMYCIN ................................................ 7 RATIO-CLOBETASOL .................................................... 174 RATIO-CLOBETASOL .................................................... 175 RATIO-CLONAZEPAM ..................................................... 82 RATIO-CODEINE .............................................................. 75 RATIO-DEXAMETHASONE ............................................ 156 RATIO-DILTIAZEM CD ..................................................... 54 RATIO-DOMPERIDONE MALEATE ............................... 149 RATIO-ECTOSONE MILD .............................................. 173 RATIO-ECTOSONE REGULAR ...................................... 173 RATIO-ECTOSONE SCALP ........................................... 173 RATIO-EMTEC-30 ............................................................ 75 RATIO-FENOFIBRATE MC .............................................. 35 RATIO-FENTANYL ................................................ SEC 3.38 RATIO-FENTANYL ................................................ SEC 3.39
RATIO-FINASTERIDE ........................................... SEC 3.40 RATIO-FLUOXETINE HYDROCHLORIDE ........................ 91 RATIO-FLUVOXAMINE ..................................................... 91 RATIO-GABAPENTIN ........................................................ 84 RATIO-GABAPENTIN ........................................................ 85 RATIO-GENTAMICIN SULFATE ..................................... 171 RATIO-GLYBURIDE ........................................................ 165 RATIO-HEMCORT H.C. ................................................... 177 RATIO-INDOMETHACIN ................................................... 72 RATIO-IPRA SAL UDV ...................................................... 22 RATIO-IPRATROPIUM UDV.................................. SEC 3.54 RATIO-IRBESARTAN ........................................................ 63 RATIO-IRBESARTAN ........................................................ 64 RATIO-IRBESARTAN HCTZ.............................................. 64 RATIO-KETOROLAC ....................................................... 134 RATIO-LACTULOSE ........................................................ 125 RATIO-LAMOTRIGINE ...................................................... 85 RATIO-LENOLTEC NO.2 ................................................... 75 RATIO-LENOLTEC NO.3 ................................................... 75 RATIO-LENOLTEC NO.4 ................................................... 75 RATIO-LEVOBUNOLOL .................................................. 136 RATIO-LISINOPRIL P ........................................................ 59 RATIO-LISINOPRIL Z ........................................................ 59 RATIO-LOVASTATIN ......................................................... 37 RATIO-METFORMIN HYDROCHLORIDE ....................... 162 RATIO-METHOTREXATE SODIUM .................................. 19 RATIO-MOMETASONE ................................................... 177 RATIO-MORPHINE ............................................................ 77 RATIO-MORPHINE ............................................................ 78 RATIO-NYSTATIN ............................................................. 15 RATIO-OMEPRAZOLE (SUSTAINED-RELEASE TABLET)
..................................................................................... 148 RATIO-ONDANSETRON ................................................. 143 RATIO-OXYCOCET ........................................................... 80 RATIO-OXYCODAN .......................................................... 81 RATIO-PAROXETINE ........................................................ 92 RATIO-PIOGLITAZONE ........................................ SEC 3.71 RATIO-PREDNISOLONE ................................................ 133 RATIO-PROCTOSONE ................................................... 178 RATIO-RANITIDINE ......................................................... 146 RATIO-RISEDRONATE ......................................... SEC 3.74 RATIO-RIVASTIGMINE ......................................... SEC 3.77 RATIO-SALBUTAMOL ....................................................... 23 RATIO-SALBUTAMOL SULF U.D.P.F. .............................. 23 RATIO-SALBUTAMOL UNI DOSE P.F. ............................. 23 RATIO-SALBUTAMOL UNIT DOSE P.F ............................ 23 RATIO-SOTALOL .............................................................. 51 RATIO-TAMSULOSIN ........................................................ 44 RATIO-TECNAL ................................................................. 69 RATIO-TECNAL-C 1/2 ....................................................... 75 RATIO-TECNAL-C 1/4 ....................................................... 75 RATIO-TERAZOSIN .......................................................... 45

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 219
RATIO-TOPILENE .......................................................... 174 RATIO-TOPISALIC ......................................................... 174 RATIO-TOPISONE.......................................................... 174 RATIO-TRYPTOPHAN ...................................................... 96 RATIO-VALPROIC ............................................................ 87 RATIO-VENLAFAXINE XR ............................................... 89 RATIO-ZOPICLONE ....................................................... 112 REBIF (0.5 ML SYRINGE)…………………………... SEC 2.10 REBIF (1.5 ML CARTRIDGE) ………………………SEC 2.10 REBIF (INITIATION PACK)…………………………. SEC 2.10 RECOMBIVAX-HB .......................................................... 169 REMERON ........................................................................ 97 REMICADE ............................................................ SEC 3.54 REMINYL ER ......................................................... SEC 3.41 RENEDIL ........................................................................... 52 RENEDIL ........................................................................... 53 REPAGLINIDE ................................................................ 164 REQUIP .......................................................................... 118 REQUIP .......................................................................... 119 RESONIUM CALCIUM .................................................... 125 RESTORIL ...................................................................... 111 RHINOCORT TURBUHALER ......................................... 132 RHO-NITRO PUMPSPRAY .............................................. 42 RHOTRAL ......................................................................... 46 RHOVANE ...................................................................... 112 RIDAURA ........................................................................ 151 RIFABUTIN ............................................................ SEC 3.73 RILUTEK ................................................................ SEC 3.73 RILUZOLE .............................................................. SEC 3.73 RIMSO-50 ....................................................................... 186 RISEDRONATE ..................................................... SEC 3.74 RISEDRONATE SODIUM ...................................... SEC 3.74 RISPERDAL .................................................................... 101 RISPERDAL .................................................................... 102 RISPERDAL .................................................................... 103 RISPERDAL CONSTA ........................................... SEC 3.75 RISPERDAL M-TAB ........................................................ 103 RISPERIDONE ............................................................... 101 RISPERIDONE ............................................................... 102 RISPERIDONE ............................................................... 103 RISPERIDONE ...................................................... SEC 3.75 RISPERIDONE TARTRATE ............................................ 103 RITALIN .......................................................................... 108 RITALIN SR .................................................................... 108 RITUXAN ............................................................... SEC 3.76 RITUXIMAB ............................................................ SEC 3.76 RIVAROXABAN ................................................................ 30 RIVASTIGMINE HYDROGEN TARTRATE ............ SEC 3.77 RIVOTRIL .......................................................................... 82 RIZATRIPTAN BENZOATE ............................................ 113 RIZATRIPTAN BENZOATE ................................... SEC 3.78 ROCALTROL .................................................................. 183
ROPINIROLE ................................................................... 118 ROPINIROLE ................................................................... 119 ROPINIROLE HCL ........................................................... 118 ROPINIROLE HCL ........................................................... 119 ROSASOL ........................................................................ 171 ROSIGLITAZONE MALEATE ................................ SEC 3.78 ROSIGLITAZONE MALEATE/ METFORMIN HCL . SEC 3.79 ROSUVASTATIN CALCIUM .............................................. 38 ROUGIER MAGNESIUM ................................................. 125 RYTHMODAN .................................................................... 33 RYTHMOL ......................................................................... 33
S
SABRIL .............................................................................. 87 SAIZEN .................................................................. SEC 3.80 SAIZEN (1.5 ML) .................................................... SEC 3.80 SAIZEN (2.5 ML) .................................................... SEC 3.80 SALAGEN .......................................................................... 21 SALAZOPYRIN .................................................................. 11 SALAZOPYRIN EN-TABS ................................................. 11 SALBUTAMOL ................................................................... 23 SALBUTAMOL SULFATE .................................................. 23 SALMETEROL XINAFOATE .............................................. 23 SALMETEROL XINAFOATE/
FLUTICASONE PROPIONATE..................................... 23 SALMETEROL XINAFOATE/
FLUTICASONE PROPIONATE..................................... 24 SALOFALK ...................................................................... 150 SALOFALK (2G/60G) ....................................................... 150 SALOFALK (4G/60G) ....................................................... 150 SANDOMIGRAN .............................................................. 115 SANDOMIGRAN DS ........................................................ 119 SANDOSTATIN ...................................................... SEC 3.60 SANDOSTATIN LAR .............................................. SEC 3.61 SANDOZ FLUOXETINE .................................................... 91 SANDOZ GLYBURIDE ................................................... 165 SANDOZ ALENDRONATE .................................... SEC 3.14 SANDOZ ALFUZOSIN ........................................... SEC 3.15 SANDOZ AMIODARONE ................................................... 34 SANDOZ AMLODIPINE ..................................................... 52 SANDOZ ANUZINC HC ................................................... 177 SANDOZ ANUZINC HC PLUS ......................................... 176 SANDOZ ATENOLOL ........................................................ 46 SANDOZ ATENOLOL ........................................................ 47 SANDOZ ATORVASTATIN ................................................ 36 SANDOZ AZITHROMYCIN ..................................................7 SANDOZ BISOPROLOL .................................................... 47 SANDOZ BRIMONIDINE ................................................. 135 SANDOZ BUPROPION SR ................................................ 96 SANDOZ CALCITONIN NS ................................... SEC 3.83

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 220 EFFECTIVE APRIL 1, 2012
SANDOZ CANDESARTAN ............................................... 63 SANDOZ CARBAMAZEPINE ............................................ 83 SANDOZ CARBAMAZEPINE CR...................................... 83 SANDOZ CEFPROZIL ........................................................ 4 SANDOZ CIPROFLOXACIN .................................. SEC 3A.2 SANDOZ CIPROFLOXACIN .................................. SEC 3A.3 SANDOZ CITALOPRAM ................................................... 90 SANDOZ CLARITHROMYCIN ............................................ 7 SANDOZ CLONAZEPAM .................................................. 82 SANDOZ CLOPIDOGREL ..................................... SEC 3.20 SANDOZ CYCLOSPORINE ................................... SEC 3.21 SANDOZ DEXAMETHASONE SOD. PHOSPHATE ....... 132 SANDOZ DICLOFENAC ................................................... 70 SANDOZ DICLOFENAC SR ............................................. 70 SANDOZ DILTIAZEM CD ................................................. 54 SANDOZ DILTIAZEM T .................................................... 54 SANDOZ DILTIAZEM T .................................................... 55 SANDOZ DORZOLAMIDE .............................................. 136 SANDOZ DORZOLAMIDE/ TIMOLOL ............................ 138 SANDOZ ENALAPRIL ....................................................... 57 SANDOZ ENALAPRIL ....................................................... 58 SANDOZ ESTRADIOL DERM 100 (8 MG/PTH) ............. 161 SANDOZ ESTRADIOL DERM 50 (4 MG/PTH) ............... 161 SANDOZ ESTRADIOL DERM 75 (6 MG/PTH) ............... 161 SANDOZ FELODIPINE ..................................................... 52 SANDOZ FELODIPINE ..................................................... 53 SANDOZ FENOFIBRATE S .............................................. 35 SANDOZ FENOFIBRATE S (TABLET) ............................. 35 SANDOZ FENTANYL PATCH ............................... SEC 3.38 SANDOZ FENTANYL PATCH ............................... SEC 3.39 SANDOZ FINASTERIDE ........................................ SEC 3.40 SANDOZ FLUOXETINE .................................................... 91 SANDOZ FLUVOXAMINE ................................................. 91 SANDOZ GENTAMICIN SULFATE ................................. 131 SANDOZ GLYBURIDE .................................................... 165 SANDOZ INDOMETHACIN ............................................... 71 SANDOZ INDOMETHACIN ............................................... 72 SANDOZ IRBESARTAN ................................................... 63 SANDOZ IRBESARTAN ................................................... 64 SANDOZ IRBESARTAN HCT ........................................... 64 SANDOZ LEFLUNOMIDE ............................................... 187 SANDOZ LEVOBUNOLOL .............................................. 136 SANDOZ LEVOFLOXACIN .................................... SEC 3A.4 SANDOZ LISINOPRIL ....................................................... 59 SANDOZ LISINOPRIL HCT .............................................. 60 SANDOZ LOVASTATIN .................................................... 37 SANDOZ METFORMIN FC ............................................. 162 SANDOZ METHYLPHENIDATE ..................................... 108 SANDOZ METOPROLOL (TYPE L) .................................. 49 SANDOZ METOPROLOL SR ........................................... 49 SANDOZ MINOCYCLINE ................................................. 12 SANDOZ MIRTAZAPINE .................................................. 97
SANDOZ MONTELUKAST .............................................. 129 SANDOZ MONTELUKAST .................................... SEC 3.59 SANDOZ MORPHINE SR .................................................. 78 SANDOZ NARATRIPTAN ................................................ 113 SANDOZ NARATRIPTAN ...................................... SEC 3.60 SANDOZ NITRAZEPAM .................................................. 111 SANDOZ OLANZAPINE .................................................... 98 SANDOZ OLANZAPINE .................................................... 99 SANDOZ OLANZAPINE ODT ............................................ 99 SANDOZ OMEPRAZOLE (SUSTAINED-RELEASE
CAPSULE) ................................................................... 148 SANDOZ ONDANSETRON ............................................. 143 SANDOZ OPIUM & BELLADONNA ................................... 79 SANDOZ OPTICORT ....................................................... 133 SANDOZ PANTOPRAZOLE ............................................ 148 SANDOZ PAROXETINE .................................................... 92 SANDOZ PENTASONE ................................................... 133 SANDOZ PINDOLOL ......................................................... 50 SANDOZ PIOGLITAZONE ..................................... SEC 3.71 SANDOZ PRAMIPEXOLE ............................................... 118 SANDOZ PRAVASTATIN .................................................. 38 SANDOZ PREDNISOLONE ACETATE ........................... 133 SANDOZ PROCHLORPERAZINE ................................... 142 SANDOZ PROCTOMYXIN HC ........................................ 178 SANDOZ QUETIAPINE ................................................... 100 SANDOZ QUETIAPINE ..................................................... 99 SANDOZ RABEPRAZOLE ............................................... 149 SANDOZ RAMIPRIL (TABLET) ......................................... 61 SANDOZ RAMIPRIL (TABLET) ......................................... 62 SANDOZ RANITIDINE ..................................................... 146 SANDOZ REPAGLINIDE ................................................. 164 SANDOZ RISEDRONATE ..................................... SEC 3.74 SANDOZ RISPERIDONE ................................................ 101 SANDOZ RISPERIDONE ................................................ 102 SANDOZ RIVASTIGMINE ..................................... SEC 3.77 SANDOZ SALBUTAMOL ................................................... 23 SANDOZ SERTRALINE ..................................................... 92 SANDOZ SERTRALINE ..................................................... 93 ANDOZ SIMVASTATIN ...................................................... 39 SANDOZ SIMVASTATIN ................................................... 40 SANDOZ SOTALOL ........................................................... 51 SANDOZ SUMATRIPTAN ............................................... 114 SANDOZ SUMATRIPTAN ..................................... SEC 3.82 SANDOZ TAMSULOSIN .................................................... 44 SANDOZ TAMSULOSIN CR .............................................. 44 SANDOZ TERBINAFINE ................................................... 14 SANDOZ TICLOPIDINE ..................................................... 30 SANDOZ TIMOLOL MALEATE ........................................ 136 SANDOZ TOBRAMYCIN ................................................. 131 SANDOZ TOPIRAMATE .................................................... 86 SANDOZ TOPIRAMATE .................................................... 87 SANDOZ TRIFLURIDINE ................................................ 131

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 221
SANDOZ VALPROIC ........................................................ 87 SANDOZ VALSARTAN ..................................................... 65 SANDOZ VALSARTAN ..................................................... 66 SANDOZ VALSARTAN HCT ............................................. 66 SANDOZ VENLAFAXINE XR ............................................ 89 SANDOZ ZOLMITRIPTAN .............................................. 115 SANDOZ ZOLMITRIPTAN ..................................... SEC 3.93 SANDOZ ZOLMITRIPTAN ODT ..................................... 115 SANDOZ ZOLMITRIPTAN ODT ............................ SEC 3.93 SANDOZ ZOPICLONE .................................................... 112 SANDOZ-OXYCODONE ACET ........................................ 80 SANTYL .......................................................................... 179 SARNA HC ...................................................................... 176 SAXAGLIPTIN HCL................................................ SEC 3.79 SECTRAL .......................................................................... 46 SELECT 1/35 (21 DAY) ................................................... 160 SELECT 1/35 (28 DAY) ................................................... 160 SELEGILINE HCL ........................................................... 119 SEPTA-AMLODIPINE ....................................................... 52 SEPTA-CITALOPRAM ...................................................... 90 SEPTRA ............................................................................ 11 SERC .............................................................................. 185 SEREVENT ....................................................................... 23 SEREVENT DISKHALER ................................................ 189 SEREVENT DISKUS ......................................................... 23 SEROPHENE .................................................................. 162 SEROQUEL .................................................................... 100 SEROQUEL ...................................................................... 99 SERTRALINE .................................................................... 92 SERTRALINE .................................................................... 93 SERTRALINE HCL............................................................ 92 SERTRALINE HCL............................................................ 93 SIMPONI ................................................................ SEC 3.45 SIMVASTATIN .................................................................. 39 SIMVASTATIN .................................................................. 40 SINEMET 100/10 ............................................................ 117 SINEMET 100/25 ............................................................ 117 SINEMET 250/25 ............................................................ 117 SINEMET CR 100/25 ...................................................... 117 SINEMET CR 200/50 ...................................................... 117 SINEQUAN ....................................................................... 94 SINEQUAN ....................................................................... 95 SINGULAIR ..................................................................... 129 SINGULAIR ............................................................ SEC 3.59 SINTROM .......................................................................... 27 SLOW K .......................................................................... 125 SODIUM ACID PHOSPHATE/ SODIUM BICARBONATE/
POTASSIUM BICARBONATE .................................... 125 SODIUM AUROTHIOMALATE ........................................ 151 SODIUM CROMOGLYCATE .......................................... 130 SODIUM FLUORIDE ....................................................... 121 SODIUM FUSIDATE ....................................................... 172
SODIUM POLYSTYRENE SULFONATE ......................... 126 SODIUM TETRADECYL SULFATE ................................... 43 SOFRACORT................................................................... 133 SOLIFENACIN SUCCINATE.................................. SEC 3.80 SOLIRIS ................................................................. SEC 3.29 SOLU-CORTEF ............................................................... 156 SOLU-CORTEF ............................................................... 157 SOLU-MEDROL ............................................................... 157 SOLU-MEDROL ACT-O-VIAL (WITH PRESERVATIVE) . 157 SOMATROPIN ....................................................... SEC 3.80 SOMATROPIN R-DNA ORIGIN ............................. SEC 3.80 SOMATULINE AUTOGEL (0.3 ML SYRINGE) ...... SEC 3.55 SOMATULINE AUTOGEL (0.5 ML SYRINGE) ...... SEC 3.55 SORIATANE .................................................................... 179 SOTALOL HCL .................................................................. 51 SPACE CHAMBER .......................................................... 189 SPACE CHAMBER ADULT MASK .................................. 189 SPACE CHAMBER INFANT MASK ................................. 189 SPACE CHAMBER PEDIATRIC MASK ........................... 189 SPIRIVA ............................................................................. 22 SPIRONOLACTONE .......................................................... 67 SPORANOX ....................................................................... 14 SPORANOX ........................................................... SEC 3.54 STALEVO ........................................................................ 117 STATEX ............................................................................. 78 STATEX ............................................................................. 79 STELARA (0.5 ML VIAL OR SYRINGE) ................ SEC 3.89 STERILE CEFAZOLIN SODIUM ..........................................3 STIEVA-A ............................................................... SEC 3.87 STIEVA-A ............................................................... SEC 3.88 STIEVA-A FORTE .................................................. SEC 3.87 STIEVAMYCIN FORTE .......................................... SEC 3.31 STIEVAMYCIN MILD ............................................. SEC 3.31 STIEVAMYCIN REGULAR .................................... SEC 3.31 SUBOXONE ....................................................................... 81 SUCRALFATE ................................................................. 147 SULCRATE ...................................................................... 147 SULCRATE SUSPENSION PLUS ................................... 147 SULFACET-R......................................................... SEC 3.81 SULFAMETHOXAZOLE/ TRIMETHOPRIM ....................... 11 SULFASALAZINE .............................................................. 11 SULFINPYRAZONE ......................................................... 127 SULFUR/ SULFACETAMIDE SODIUM ................. SEC 3.81 SULINDAC ......................................................................... 74 SUMATRIPTAN ............................................................... 114 SUMATRIPTAN ..................................................... SEC 3.82 SUMATRIPTAN HEMISULFATE ..................................... 114 SUMATRIPTAN HEMISULFATE ........................... SEC 3.81 SUMATRIPTAN SUCCINATE .......................................... 114 SUMATRIPTAN SUCCINATE ................................ SEC 3.82 SUMATRIPTAN SUN (0.5 ML)......................................... 114 SUMATRIPTAN SUN (0.5 ML)............................... SEC 3.82

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 222 EFFECTIVE APRIL 1, 2012
SUPEUDOL ...................................................................... 80 SUPRAX ............................................................................. 5 SUPREFACT ......................................................... SEC 3.18 SUPREFACT DEPOT ............................................ SEC 3.18 SUPREFACT INTRANASAL .................................. SEC 3.18 SYMBICORT 100 TURBUHALER ..................................... 22 SYMBICORT 200 TURBUHALER ..................................... 22 SYNACTHEN DEPOT ..................................................... 165 SYNAREL ....................................................................... 187 SYNPHASIC (21 DAY) .................................................... 160 SYNPHASIC (28 DAY) .................................................... 160 SYNTHETIC CALCITONIN SALMON (SALCATONIN) ... 165 SYNTHETIC CALCITONIN SALMON (SALCATONIN)
........................................................................... SEC 3.83 SYNTHROID ................................................................... 167
T
TACROLIMUS ........................................................ SEC 3.83 TACROLIMUS ........................................................ SEC 3.84 TALWIN ............................................................................. 81 TAMBOCOR ..................................................................... 33 TAMSULOSIN ................................................................... 44 TAMSULOSIN HCL ........................................................... 44 TAPAZOLE ..................................................................... 168 TARO-AMCINONIDE ...................................................... 173 TARO-CARBAMAZEPINE ................................................ 83 TARO-CLOBETASOL ..................................................... 174 TARO-CLOBETASOL ..................................................... 175 TARO-MOMETASONE ................................................... 177 TARO-MUPIROCIN......................................................... 172 TARO-PHENYTOIN .......................................................... 82 TARO-WARFARIN ............................................................ 27 TARO-WARFARIN ............................................................ 28 TAZAROTENE ................................................................ 180 TAZOCIN ............................................................... SEC 3.72 TAZORAC ....................................................................... 180 TECTA ............................................................................ 148 TEGRETOL ....................................................................... 83 TEGRETOL CR ................................................................. 83 TELMISARTAN ................................................................. 65 TELMISARTAN/ AMLODIPINE BESYLATE ...................... 65 TELMISARTAN/ HYDROCHLOROTHIAZIDE ................... 65 TEMAZEPAM .................................................................. 111 TENOFOVIR DISOPROXIL FUMARATE .......................... 15 TENORETIC 50/25........................................................... 47 TENORETIC 100/25.......................................................... 47 TENORMIN ....................................................................... 46 TENORMIN ....................................................................... 47 TENOXICAM ..................................................................... 74 TERAZOSIN ...................................................................... 45
TERAZOSIN HCL .............................................................. 45 TERBINAFINE ................................................................... 14 TERBINAFINE HCL ........................................................... 14 TERBINAFINE HCL ......................................................... 172 TERBUTALINE SULFATE ................................................. 24 TESTOSTERONE .................................................. SEC 3.84 TESTOSTERONE CYPIONATE ...................................... 158 TESTOSTERONE ENANTHATE ..................................... 158 TESTOSTERONE UNDECANOATE ..................... SEC 3.84 TETRABENAZINE ................................................. SEC 3.85 TETRACYCLINE ................................................................ 12 TETRACYCLINE HCL ........................................................ 12 TEVA-ATENOLOL ............................................................. 46 TEVA-CLOPIDOGREL ........................................... SEC 3.20 TEVA-DORZOTIMOL ....................................................... 138 TEVA-GABAPENTIN ......................................................... 84 TEVA-HYDROMORPHONE............................................... 76 TEVA-IRBESARTAN .......................................................... 63 TEVA-IRBESARTAN .......................................................... 64 TEVA-IRBESARTAN/HCTZ ............................................... 64 TEVA-LACTULOSE ......................................................... 125 TEVA-MONTELUKAST .................................................... 129 TEVA-MONTELUKAST .......................................... SEC 3.59 TEVA-TAMSULOSIN CR ................................................... 44 TEVA-TERAZOSIN ............................................................ 45 TEVA-VALSARTAN ........................................................... 65 TEVA-VALSARTAN ........................................................... 66 TEVA-VALSARTAN/HCTZ ................................................. 66 TEVA-ZOLMITRIPTAN .................................................... 115 TEVA-ZOLMITRIPTAN .......................................... SEC 3.93 TEVA-ZOLMITRIPTAN OD .............................................. 115 TEVA-ZOLMITRIPTAN OD .................................... SEC 3.93 TEVETEN .......................................................................... 63 TEVETEN PLUS ................................................................ 63 THEOLAIR ....................................................................... 181 THEOPHYLLINE .............................................................. 181 THIAMIJECT .................................................................... 183 THIAMINE HCL ................................................................ 183 THIOPROPERAZINE MESYLATE ................................... 105 THIOTHIXENE ................................................................. 106 THYROGEN ..................................................................... 123 THYROID ......................................................................... 167 THYROTROPIN ALFA ..................................................... 123 TIAMOL ............................................................................ 175 TIAPROFENIC ACID ......................................................... 74 TIAZAC .............................................................................. 54 TIAZAC .............................................................................. 55 TIAZAC XC ........................................................................ 53 TICLOPIDINE..................................................................... 30 TICLOPIDINE HCL ............................................................ 30 TIMOLOL MALEATE ........................................................ 136 TIMOLOL MALEATE .......................................................... 51

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 223
TIMOPTIC ....................................................................... 136 TIMOPTIC-XE ................................................................. 136 TINZAPARIN SODIUM ...................................................... 29 TINZAPARIN SODIUM ...................................................... 30 TIOTROPIUM BROMIDE MONOHYDRATE ..................... 22 TIZANIDINE HCL ................................................... SEC 3.85 TOBI .................................................................................... 3 TOBI PODHALER ............................................................... 3 TOBRADEX .................................................................... 133 TOBRAMYCIN ................................................................ 131 TOBRAMYCIN .................................................................... 3 TOBRAMYCIN SULFATE ................................................... 3 TOBREX ......................................................................... 131 TOCILIZUMAB ....................................................... SEC 3.87 TOLOXIN .......................................................................... 34 TOLOXIN PEDIATRIC ...................................................... 34 TOLTERODINE L-TARTRATE ............................... SEC 3.87 TOPAMAX ......................................................................... 86 TOPAMAX ......................................................................... 87 TOPAMAX SPRINKLE ...................................................... 87 TOPICORT ...................................................................... 175 TOPICORT MILD ............................................................ 175 TOPIRAMATE ................................................................... 86 TOPIRAMATE ................................................................... 87 TORADOL ......................................................................... 72 TRANDATE ....................................................................... 48 TRANDOLAPRIL ............................................................... 62 TRANEXAMIC ACID ......................................................... 31 TRANSDERM-NITRO 0.2 ................................................. 43 TRANSDERM-NITRO 0.4 ................................................. 43 TRANSDERM-NITRO 0.6 ................................................. 43 TRANYLCYPROMINE SULFATE ..................................... 88 TRAVATAN Z .................................................................. 137 TRAVOPROST ............................................................... 137 TRAVOPROST/ TIMOLOL MALEATE ............................ 138 TRAZODONE .................................................................... 93 TRAZODONE HCL............................................................ 93 TRENTAL .......................................................................... 31 TRETINOIN ............................................................ SEC 3.87 TRETINOIN ............................................................ SEC 3.88 TRI-CYCLEN (21 DAY) ................................................... 160 TRI-CYCLEN (28 DAY) ................................................... 160 TRI-CYCLEN LO 21 ........................................................ 160 TRI-CYCLEN LO 28 ........................................................ 160 TRIADERM REGULAR ................................................... 177 TRIAMCINOLONE ACETONIDE..................................... 158 TRIAMCINOLONE ACETONIDE..................................... 177 TRIAMCINOLONE ACETONIDE USP ............................ 158 TRIAZOLAM .................................................................... 111 TRIFLUOPERAZINE ....................................................... 106 TRIFLUOPERAZINE HCL ............................................... 106 TRIFLURIDINE ............................................................... 131
TRIHEXYPHENIDYL ........................................................ 116 TRIHEXYPHENIDYL HCL ............................................... 116 TRIMEBUTINE ................................................................. 150 TRIMEBUTINE MALEATE ............................................... 150 TRIMEPRAZINE TARTRATE...............................................1 TRIMETHOPRIM ............................................................... 18 TRIMIPRAMINE ................................................................. 95 TRIMIPRAMINE ................................................................. 96 TRIMIPRAMINE MALEATE ............................................... 95 TRIMIPRAMINE MALEATE ............................................... 96 TRINIPATCH 0.2 ................................................................ 43 TRINIPATCH 0.4 ................................................................ 43 TRINIPATCH 0.6 ................................................................ 43 TRIQUILAR (21 DAY) ...................................................... 159 TRIQUILAR (28 DAY) ...................................................... 159 TROMBOJECT .................................................................. 43 TROPICAMIDE ................................................................ 134 TROSEC ................................................................ SEC 3.88 TROSPIUM CHLORIDE ......................................... SEC 3.88 TRUSOPT ........................................................................ 136 TRUSOPT (PRESERVATIVE-FREE) .............................. 136 TRYPTAN .......................................................................... 96 TWINJECT AUTO INJECTOR ........................................... 24 TWYNSTA ......................................................................... 65 TYLENOL NO. 2 ................................................................ 75 TYLENOL NO. 3 ................................................................ 75 TYLENOL NO. 4 ................................................................ 75 TYLENOL WITH CODEINE ............................................... 75 TYSABRI ………………………………………………SEC 2.13
U
ULORIC ................................................................. SEC 3.38 ULTRASE MS4 MICROSPHERES .................................. 141 ULTRASE MT12 MINITABLETS ...................................... 141 ULTRASE MT20 MINITABLETS ...................................... 141 ULTRAVATE .................................................................... 175 UNIPHYL ......................................................................... 181 UREMOL-HC ................................................................... 176 UROMAX ............................................................... SEC 3.63 URSO ............................................................................... 141 URSO DS ......................................................................... 141 URSODIOL ...................................................................... 141 USTEKINUMAB ..................................................... SEC 3.89
V
VAGIFEM ......................................................................... 161 VAL-VANCO ...................................................................... 12 VALACYCLOVIR ................................................................ 17 VALCYTE ............................................................... SEC 3.90

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 224 EFFECTIVE APRIL 1, 2012
VALGANCICLOVIR HCL ........................................ SEC 3.90 VALISONE SCALP.......................................................... 173 VALPROIC ACID............................................................... 87 VALSARTAN ..................................................................... 65 VALSARTAN ..................................................................... 66 VALSARTAN/ HYDROCHLOROTHIAZIDE ...................... 66 VALTREX (CAPLET) ......................................................... 17 VANCOCIN ............................................................ SEC 3.90 VANCOMYCIN HCL .......................................................... 12 VANCOMYCIN HCL ............................................... SEC 3.90 VARENICLINE TARTRATE ................................... SEC 3.90 VARENICLINE TARTRATE/|
VARENICLINE TARTRATE .............................. SEC 3.91 VASERETIC ...................................................................... 58 VASOTEC ......................................................................... 57 VASOTEC ......................................................................... 58 VENLAFAXINE HCL ......................................................... 89 VENLAFAXINE XR............................................................ 89 VENTOLIN ........................................................................ 23 VENTOLIN HFA ................................................................ 23 VENTOLIN NEBULES P.F. ............................................... 23 VERAPAMIL HCL.............................................................. 55 VERMOX ............................................................................. 3 VESICARE ............................................................. SEC 3.80 VFEND ................................................................... SEC 3.91 VIBRAMYCIN .................................................................... 11 VIGABATRIN .................................................................... 87 VIMPAT .................................................................. SEC 3.54 VIMPAT .................................................................. SEC 3.55 VIOKASE ........................................................................ 141 VIOKASE 16 ................................................................... 141 VIREAD ............................................................................. 15 VIROPTIC ....................................................................... 131 VISKAZIDE 10/25.............................................................. 50 VISKAZIDE 10/50.............................................................. 50 VISKEN ............................................................................. 50 VITAMIN A ACID .................................................... SEC 3.87 VITAMIN A ACID .................................................... SEC 3.88 VITAMIN B12 .................................................................. 183 VITAMIN K1 .................................................................... 183 VITAMIN K1 PEDIATRIC ................................................ 183 VOLTAREN ....................................................................... 70 VOLTAREN OPHTHA ..................................................... 134 VOLTAREN SR ................................................................. 70 VORICONAZOLE ................................................... SEC 3.91 VORTEX ......................................................................... 189 VORTEX BABY WHIRL INFANT MASK ......................... 189 VORTEX SPINNER PEDIATRIC MASK ......................... 189
W
WARFARIN ........................................................................ 27 WARFARIN ........................................................................ 28 WARFARIN SODIUM ......................................................... 27 WARFARIN SODIUM ......................................................... 28 WARTEC ......................................................................... 179 WELLBUTRIN SR .............................................................. 96 WELLBUTRIN XL ............................................................... 96 WINPRED ........................................................................ 158
X
XALACOM ....................................................................... 138 XALATAN ......................................................................... 137 XAMIOL ........................................................................... 179 XANAX ............................................................................. 109 XARELTO .......................................................................... 30 XATRAL ................................................................. SEC 3.15 XEOMIN ........................................................................... 185 XOLAIR .................................................................. SEC 3.63 XYLAC ............................................................................. 107 XYLOCAINE..................................................................... 178 XYLOCAINE JELLY ......................................................... 178 XYLOCAINE VISCOUS ................................................... 134
Y
YASMIN 21 ...................................................................... 159 YASMIN 28 ...................................................................... 159
Z
ZADITEN ..............................................................................1 ZAFIRLUKAST ................................................................. 129 ZAFIRLUKAST ....................................................... SEC 3.92 ZANAFLEX ............................................................ SEC 3.85 ZANTAC ........................................................................... 146 ZARONTIN ......................................................................... 83 ZAROXOLYN ................................................................... 127 ZELDOX ........................................................................... 103 ZESTORETIC .................................................................... 60 ZESTRIL ............................................................................ 59 ZIPRASIDONE HYDROCHLORIDE MONOHYDRATE ... 103 ZITHROMAX ........................................................................7 ZITHROMAX .......................................................... SEC 3.17 ZOCOR .............................................................................. 39 ZOCOR .............................................................................. 40 ZOFRAN .......................................................................... 143 ZOFRAN ODT .................................................................. 142

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 1 – ALPHABETICAL LIST OF PRODUCTS
ALPHABETICAL LIST OF PHARMACEUTICAL PRODUCTS
Product Name Page Product Name Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 225
ZOLADEX .............................................................. SEC 3.45 ZOLADEX LA ......................................................... SEC 3.45 ZOLEDRONIC ACID .............................................. SEC 3.92 ZOLMITRIPTAN .............................................................. 115 ZOLMITRIPTAN ..................................................... SEC 3.93 ZOLOFT ............................................................................ 92 ZOLOFT ............................................................................ 93 ZOMETA CONCENTRATE .................................... SEC 3.92 ZOMIG ............................................................................ 115 ZOMIG ................................................................... SEC 3.93 ZOMIG RAPIMELT.......................................................... 115 ZOMIG RAPIMELT................................................. SEC 3.93 ZOPICLONE ................................................................... 112 ZOVIRAX .......................................................................... 16 ZUCLOPENTHIXOL ACETATE ...................................... 106 ZUCLOPENTHIXOL DECANOATE................................. 106 ZUCLOPENTHIXOL DIHYDROCHLORIDE .................... 107 ZYLOPRIM ...................................................................... 185 ZYPREXA ......................................................................... 98 ZYPREXA ......................................................................... 99 ZYPREXA ZYDIS .............................................................. 99 ZYVOXAM .............................................................. SEC 3.56

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS
DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
226 EFFECTIVE APRIL 1, 2012
00000000655 .......... 137 00000000663 .......... 137 00000000779 .......... 134 00000000787 .......... 134 00000000841 .......... 137 00000000868 .......... 137 00000000884 .......... 137 00000000981 .......... 134 00000001007 .......... 134 00000001686 .......... 134 00000001694 .......... 178 00000001961 .......... 178 00000004596 .......... 185 00000004774 ............ 17 00000005606 .......... 108 00000005614 .......... 108 00000009881 . SEC 3.64 00000010200 .......... 168 00000010219 .......... 168 00000010340 ............ 69 00000010383 ............ 27 00000010391 ............ 27 00000010405 ............ 83 00000015229 ............ 95 00000015237 ............ 95 00000015741 .......... 168 00000016055 .......... 153 00000020877 . SEC 3.15 00000020885 . SEC 3.15 00000021008 ............ 18 00000021016 ............ 18 00000021202 .............. 8 00000021261 ............ 17 00000021474 .......... 126 00000021482 .......... 126 00000022772 ............ 82 00000022780 ............ 82 00000022799 ............ 83 00000022802 ............ 83 00000023442 ............ 82 00000023450 ............ 82 00000023485 ............ 83 00000023698 ............ 82 00000023949 .......... 167 00000023957 .......... 167 00000023965 .......... 167 00000024325 ............ 94 00000024333 ............ 94 00000024341 ............ 94 00000024368 ............ 11
00000024430 .......... 106 00000024449 .......... 106 00000024457 .......... 106 00000024694 .......... 112 00000026697 .......... 125 00000027243 ............ 24 00000027944 .......... 173 00000028096 .......... 155 00000028606 ............ 67 00000029149 ............ 15 00000029246 .......... 158 00000030570 ............ 13 00000030600 .......... 156 00000030619 .......... 156 00000030627 .......... 156 00000030635 .......... 157 00000030678 .......... 157 00000030759 .......... 157 00000030767 .......... 157 00000030783 .......... 158 00000030848 .......... 166 00000030910 .......... 156 00000030929 .......... 156 00000030937 .......... 166 00000030988 .......... 157 00000035017 .......... 134 00000035076 .......... 134 00000036129 .......... 157 00000036137 .......... 157 00000036323 .......... 141 00000037605 .......... 159 00000037613 ............ 42 00000037621 ............ 42 00000042560 .......... 132 00000042579 .......... 132 00000042676 .......... 133 00000074225 .......... 125 00000074454 .......... 133 00000115630 .......... 109 00000125083 ............ 76 00000125121 ............ 76 00000155357 ............ 24 00000155365 .......... 135 00000176095 ............ 24 00000176141 ............ 21 00000176176 ............ 24 00000176192 ............ 75 00000176206 ............ 75 00000178799 .......... 108 00000178802 .......... 108
00000178810 .......... 108 00000178829 .......... 108 00000180408 ............ 67 00000192597 .......... 176 00000192600 .......... 176 00000195057 .SEC 3.58 00000225819 .......... 125 00000225851 ............ 13 00000226327 ............ 69 00000230316 .......... 176 00000232807 .......... 104 00000232823 .......... 104 00000232831 .......... 104 00000236683 .......... 113 00000252506 .......... 134 00000252654 .......... 178 00000253952 .......... 165 00000259527 ............ 40 00000260428 .......... 157 00000260436 ............ 13 00000262595 .............. 6 00000263699 .SEC 3.18 00000263818 .......... 141 00000265470 .......... 160 00000271373 .......... 158 00000280437 .......... 155 00000285455 ............ 67 00000291889 ............ 40 00000294926 .......... 127 00000297143 .......... 159 00000299405 .......... 133 00000301175 .......... 133 00000307246 .......... 133 00000312363 .............. 6 00000312738 ............ 18 00000312746 .......... 106 00000312754 .......... 106 00000312770 .......... 158 00000312797 ............ 95 00000312800 .......... 126 00000313815 .......... 107 00000313823 .......... 107 00000315966 .......... 159 00000317047 .......... 160 00000319511 ............ 18 00000323071 .......... 174 00000324019 ............ 94 00000326836 .......... 106 00000326844 .......... 126 00000326852 ............ 95
00000326925 ............ 95 00000328219 .......... 117 00000329320 .......... 115 00000330566 ............ 94 00000330582 .......... 179 00000335053 ............ 94 00000335061 ............ 94 00000335088 ............ 94 00000335096 .......... 105 00000335118 .......... 105 00000335126 .......... 105 00000335134 .......... 105 00000337420 ............ 71 00000337439 ............ 71 00000337730 ............ 41 00000337749 ............ 41 00000337757 ............ 10 00000337765 ............ 10 00000337773 ............ 10 00000340731 .......... 160 00000342084 .............. 4 00000342092 .............. 4 00000342106 .............. 4 00000342114 .............. 4 00000343838 .......... 159 00000344923 .......... 174 00000345539 .......... 106 00000353027 .......... 159 00000355658 .......... 117 00000358177 .......... 133 00000360201 ............ 95 00000360252 ............ 40 00000360260 ............ 40 00000360279 .......... 127 00000362158 .......... 109 00000362166 ............ 41 00000363014 .......... 176 00000363650 .......... 104 00000363669 .......... 104 00000363677 .......... 103 00000363685 .......... 103 00000363812 ............ 21 00000363839 ............ 21 00000369810 ............ 83 00000372838 .......... 160 00000372846 .......... 160 00000373036 SEC 3.18 00000382825 ............ 82 00000382841 ............ 82 00000386464 .......... 116

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 227
00000386472 .......... 116 00000391603 .............. 8 00000392472 ............ 80 00000392480 ............ 80 00000392537 .......... 142 00000392561 ............ 79 00000392588 ............ 79 00000392693 ............ 21 00000392731 .......... 142 00000392782 ............ 21 00000392812 ............ 21 00000396761 ............ 81 00000396788 ............ 41 00000396796 .......... 103 00000396818 .......... 103 00000396826 .......... 104 00000396834 .......... 104 00000397423 ............ 49 00000397431 ............ 49 00000399310 ............ 81 00000399728 .......... 110 00000400750 ............ 94 00000402516 .......... 166 00000402591 ............ 94 00000402680 .......... 111 00000402699 ............ 83 00000402737 .......... 111 00000402745 .......... 111 00000402753 ............ 50 00000402761 ............ 50 00000402788 ............ 50 00000402796 .......... 185 00000402818 .......... 185 00000405329 .......... 109 00000405337 .......... 110 00000405345 .......... 104 00000405361 .......... 105 00000406716 .............. 8 00000406724 .............. 8 00000406775 .......... 113 00000410632 .......... 104 00000417246 .......... 174 00000417270 ............ 50 00000417289 ............ 50 00000426830 ............ 40 00000426849 .......... 183 00000426857 .......... 116 00000441619 ............ 41 00000441627 ............ 41 00000441635 ............ 41
00000441651 ............ 71 00000441686 ............ 42 00000441694 ............ 42 00000441767 .......... 127 00000441775 .......... 126 00000443174 ............ 50 00000443832 ............ 87 00000443840 ............ 87 00000443948 ............ 80 00000445266 ............ 11 00000445274 ............ 11 00000445282 ............ 11 00000451207 .......... 136 00000452130 .............. 9 00000452149 .............. 9 00000453781 ............ 29 00000453811 ............ 29 00000455881 ............ 25 00000461733 .......... 113 00000463698 .......... 104 00000465763 .......... 135 00000469327 .......... 159 00000471526 .......... 159 00000474517 .......... 183 00000474525 .......... 183 00000476366 .......... 181 00000476374 .......... 181 00000476552 ............ 88 00000479799 .......... 185 00000481815 .......... 183 00000481823 .......... 183 00000487872 .......... 144 00000489158 .......... 156 00000493392 .......... 186 00000496480 ............ 50 00000496499 ............ 50 00000496502 ............ 50 00000497193 .......... 181 00000500895 .......... 130 00000502790 .......... 141 00000503134 .......... 176 00000503347 ............ 41 00000504335 ............ 50 00000506052 ............ 71 00000509558 ............ 24 00000510637 ............ 11 00000510645 ............ 11 00000511234 ............ 43 00000511528 .......... 111 00000511536 .......... 111
00000511552 .......... 119 00000512184 .......... 131 00000512192 .......... 131 00000513962 .......... 131 00000513997 .......... 117 00000514012 ............ 70 00000514497 ............ 41 00000514500 ............ 41 00000518123 .......... 109 00000518131 .......... 109 00000518182 .SEC 3.87 00000519251 .......... 185 00000521515 .......... 183 00000521698 .......... 110 00000521701 .......... 110 00000522597 .......... 116 00000522651 ............ 72 00000522678 ............ 72 00000522724 .......... 109 00000522988 .......... 109 00000522996 .......... 109 00000527033 ............ 41 00000532657 .......... 126 00000534560 ............ 49 00000535427 .......... 173 00000535435 .......... 173 00000544884 ............ 75 00000545015 .......... 136 00000545058 .......... 116 00000545066 ............ 18 00000545074 .......... 116 00000545678 .............. 6 00000548359 .......... 109 00000548367 .......... 109 00000548375 .......... 144 00000550086 ............ 11 00000550175 .......... 179 00000550957 .......... 158 00000555126 .......... 125 00000556734 .............. 3 00000559253 ............ 43 00000560022 .......... 176 00000564966 .......... 127 00000565350 ............ 72 00000567434 .............. 1 00000568627 ............ 50 00000568635 ............ 50 00000572349 .......... 185 00000575240 .......... 137 00000575569 .......... 121
00000577308 .............. 1 00000578428 .......... 174 00000578436 .......... 174 00000578541 .......... 176 00000578576 SEC 3.87 00000578657 ............ 24 00000579335 .......... 176 00000579718 ............ 29 00000580929 ............ 12 00000582344 .......... 179 00000582352 .......... 179 00000582417 .......... 144 00000583413 .............. 3 00000583421 .............. 3 00000584215 .......... 144 00000584223 ............ 43 00000584991 .......... 108 00000585009 .......... 108 00000585092 .......... 166 00000585114 ............ 71 00000586668 .......... 171 00000586676 .......... 172 00000586714 .......... 163 00000587265 .......... 116 00000587354 .......... 116 00000587362 .......... 116 00000587737 .......... 163 00000587818 .......... 175 00000587826 .......... 175 00000587834 .......... 175 00000587966 SEC 3.87 00000589861 ............ 73 00000590819 ............ 49 00000590827 ............ 70 00000591467 ............ 79 00000591475 ............ 79 00000592277 ............ 73 00000593435 ............ 75 00000593451 ............ 75 00000594377 ............ 67 00000594636 ............ 78 00000594644 ............ 78 00000594652 ............ 78 00000595799 .......... 176 00000595802 .......... 176 00000595942 .......... 106 00000596418 ............ 84 00000596426 ............ 84 00000596434 ............ 84 00000596612 .............. 1
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 228 EFFECTIVE APRIL 1, 2012
00000596965 ............ 79 00000598194 .......... 158 00000598461 ............ 11 00000598488 ............ 11 00000598933 .......... 175 00000600059 .......... 144 00000600067 .......... 144 00000600806 ............ 73 00000602884 .......... 125 00000602957 .......... 160 00000602965 .......... 160 00000603678 .......... 144 00000603686 .......... 144 00000603708 ............ 33 00000603716 ............ 33 00000604453 .......... 111 00000604461 .......... 111 00000605859 .............. 6 00000607142 .............. 6 00000607762 ............ 77 00000607770 ............ 77 00000607789 .......... 177 00000607797 .......... 177 00000608157 ............ 81 00000608165 ............ 80 00000608181 ............ 75 00000608203 ............ 75 00000608211 ............ 69 00000608238 ............ 69 00000608882 ............ 75 00000609129 .......... 144 00000610100 .......... 121 00000611158 ............ 71 00000611166 ............ 71 00000611174 .......... 177 00000611271 .......... 179 00000613215 ............ 67 00000613223 ............ 67 00000613231 ............ 67 00000614254 .......... 131 00000617288 ............ 79 00000618454 .......... 109 00000618632 ............ 49 00000618640 ............ 49 00000621374 .......... 185 00000621463 ............ 75 00000621935 ............ 79 00000622133 ............ 77 00000627097 ............ 73 00000627100 ............ 76
00000628115 .............. 8 00000628123 .............. 8 00000628131 .............. 9 00000628158 .............. 9 00000629340 ............ 71 00000629359 ............ 71 00000629367 .......... 174 00000632201 ............ 79 00000632228 ............ 79 00000632724 ............ 70 00000632732 ............ 70 00000632775 .......... 108 00000634506 ............ 16 00000636576 ............ 25 00000636622 ............ 91 00000637416 .............. 6 00000637661 .......... 136 00000637726 . SEC 3.41 00000637742 .......... 110 00000637750 .......... 110 00000638676 ............ 33 00000638684 ............ 33 00000638692 ............ 33 00000639389 ............ 79 00000641863 . SEC 3.88 00000642215 .............. 8 00000642223 .............. 8 00000642231 .............. 8 00000642886 ............ 74 00000642894 ............ 74 00000642975 ............ 34 00000644552 .......... 126 00000644579 ............ 95 00000645575 .......... 108 00000646016 .......... 112 00000646024 .......... 112 00000646059 .......... 112 00000648035 ............ 49 00000648043 ............ 49 00000649074 ............ 18 00000649392 .......... 116 00000652318 .............. 6 00000653209 .......... 173 00000653217 .......... 173 00000653241 ............ 75 00000653276 ............ 75 00000654531 ............ 96 00000655740 .......... 110 00000655759 .......... 110 00000655767 .......... 110
00000657182 ............ 67 00000657204 .SEC 3.87 00000657298 ............ 58 00000658855 ............ 49 00000662348 .SEC 3.87 00000663719 ............ 50 00000664227 .......... 156 00000665088 ............ 83 00000666157 .......... 172 00000670901 ............ 57 00000670928 ............ 58 00000670944 ............ 42 00000675962 ............ 78 00000676411 ............ 79 00000682020 .............. 6 00000682217 .......... 133 00000687456 .......... 131 00000688568 .............. 6 00000688622 .......... 174 00000690783 ............ 77 00000690791 ............ 78 00000692689 .......... 181 00000692697 .......... 181 00000692700 .......... 181 00000695696 ............ 74 00000695718 ............ 74 00000700401 .......... 133 00000703486 .......... 125 00000704423 .SEC 3.21 00000704431 .SEC 3.21 00000705438 ............ 76 00000705799 ............ 79 00000706531 .......... 116 00000707503 .......... 159 00000707511 .......... 132 00000707570 ............ 41 00000707600 .......... 159 00000708879 ............ 57 00000708917 .......... 166 00000710113 .......... 145 00000710121 .......... 145 00000711101 .......... 110 00000713376 .......... 125 00000713449 .......... 104 00000716618 .......... 173 00000716626 .......... 173 00000716642 .......... 173 00000716650 .......... 173 00000716685 .......... 176 00000716693 .......... 176
00000716820 .......... 176 00000716839 .......... 176 00000716863 .......... 175 00000716960 .......... 177 00000717274 SEC 3.46 00000717282 SEC 3.46 00000717568 .............. 8 00000718149 ............ 96 00000720941 .......... 165 00000725110 ............ 53 00000725250 ............ 11 00000725315 ............ 29 00000725323 ............ 29 00000725749 ............ 77 00000725757 ............ 77 00000725765 ............ 77 00000726540 ............ 11 00000726672 .............. 6 00000727520 ............ 29 00000727695 SEC 3.55 00000728187 .......... 110 00000728195 .......... 110 00000728209 .......... 110 00000729973 .......... 166 00000733059 .......... 146 00000733067 .......... 146 00000738824 .......... 112 00000738832 .......... 112 00000738840 .......... 112 00000739839 .......... 132 00000740675 ............ 50 00000740713 ............ 11 00000740721 ............ 42 00000740799 ............ 95 00000740802 ............ 95 00000740810 ............ 95 00000740829 ............ 96 00000741817 .......... 112 00000742554 ............ 55 00000742813 .......... 112 00000743518 .......... 104 00000745588 ............ 74 00000745596 ............ 74 00000749354 ............ 49 00000749486 .......... 169 00000749494 .......... 144 00000750050 .......... 173 00000751170 ............ 49 00000754129 ............ 94 00000755338 .......... 126

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 229
00000755575 .......... 104 00000755583 ............ 83 00000755826 .......... 136 00000755834 .......... 136 00000755842 ............ 51 00000755850 ............ 51 00000755869 ............ 51 00000755877 ............ 50 00000755885 ............ 50 00000755893 ............ 50 00000755907 ............ 53 00000756784 .......... 132 00000756792 .......... 161 00000756849 .......... 161 00000765953 ............ 41 00000765996 .......... 164 00000768715 .............. 3 00000768723 .............. 3 00000768820 .......... 104 00000769533 .......... 126 00000769541 .......... 126 00000771376 ............ 53 00000771384 ............ 53 00000773611 ............ 83 00000773689 ............ 46 00000773697 ............ 47 00000776181 ............ 77 00000776203 ............ 77 00000778338 .......... 145 00000778346 .......... 145 00000778354 ............ 74 00000778362 ............ 74 00000778389 ............ 74 00000778907 .......... 133 00000778915 .......... 133 00000779474 ............ 75 00000780626 ............ 82 00000781878 .......... 183 00000782327 . SEC 3.84 00000782459 ............ 70 00000782467 ............ 49 00000782475 ............ 49 00000782483 ............ 55 00000782491 ............ 55 00000782505 ............ 49 00000782718 ............ 83 00000783900 .......... 156 00000784354 ............ 74 00000784400 .......... 126 00000786535 ............ 76
00000786543 ............ 76 00000786616 ............ 24 00000788716 . SEC 3.90 00000789429 .......... 141 00000789437 .......... 141 00000789445 .......... 141 00000789720 .......... 142 00000789739 ............ 80 00000789747 .......... 142 00000790427 ............ 72 00000790435 ............ 72 00000792659 .......... 112 00000792667 ............ 15 00000792942 .......... 181 00000795852 ............ 37 00000795860 ............ 37 00000795879 .......... 163 00000800430 . SEC 3.90 00000803499 .......... 150 00000804312 .......... 183 00000804533 .......... 176 00000804541 .......... 173 00000804991 .......... 174 00000805009 .......... 174 00000805025 .......... 171 00000805386 .......... 171 00000807435 .......... 131 00000807788 .......... 133 00000808539 ............ 70 00000808547 ............ 70 00000808563 .......... 111 00000808571 .......... 111 00000808652 .......... 104 00000808733 .......... 165 00000808741 .......... 165 00000809187 .......... 174 00000816086 .......... 183 00000818658 ............ 45 00000818666 ............ 45 00000818674 ............ 45 00000818682 ............ 45 00000821373 .......... 141 00000824143 .......... 166 00000824305 .......... 166 00000828556 .......... 146 00000828564 .......... 146 00000828823 .......... 146 00000836273 . SEC 3.55 00000836362 .......... 166 00000839175 ............ 70
00000839183 ............ 70 00000839191 .SEC 3.60 00000839205 .SEC 3.60 00000839213 .SEC 3.60 00000839388 ............ 59 00000839396 ............ 59 00000839418 ............ 59 00000842648 ............ 49 00000842656 ............ 49 00000842664 ............ 72 00000842826 .......... 149 00000842834 .......... 149 00000846503 .......... 148 00000849650 .......... 174 00000849669 .......... 174 00000851736 .......... 177 00000851744 .......... 177 00000851752 .......... 155 00000851760 .......... 155 00000851779 ............ 52 00000851787 ............ 53 00000851795 ............ 57 00000852074 .......... 155 00000852384 ............ 43 00000854409 .......... 125 00000856711 .......... 176 00000860689 .......... 109 00000860697 .......... 109 00000860700 .......... 109 00000860808 ............ 23 00000862924 ............ 53 00000862932 ............ 53 00000862975 .......... 174 00000865397 .......... 109 00000865400 .......... 109 00000865532 .......... 126 00000865540 .............. 9 00000865559 .............. 9 00000865567 .............. 8 00000865575 .............. 8 00000865605 ............ 49 00000865613 ............ 49 00000865648 ............ 72 00000865656 ............ 73 00000865664 ............ 73 00000865710 ............ 11 00000865729 ............ 11 00000865737 .......... 146 00000865745 .......... 146 00000865761 ............ 74
00000865788 ............ 74 00000865818 .......... 144 00000865826 .......... 144 00000865834 .......... 144 00000865850 ............ 71 00000865869 ............ 71 00000865877 .............. 3 00000865885 .............. 3 00000868957 ............ 40 00000868965 .............. 5 00000868981 .............. 5 00000869007 ............ 50 00000869015 ............ 50 00000869023 ............ 50 00000869945 ............ 21 00000869953 ............ 21 00000869961 ............ 21 00000870420 ............ 18 00000870935 .......... 117 00000871095 .......... 177 00000872520 .......... 156 00000872539 .......... 156 00000872644 .............. 9 00000872652 .............. 9 00000873454 .............. 6 00000873993 .......... 166 00000874256 ............ 11 00000874582 .......... 156 00000878618 .......... 156 00000878626 .......... 157 00000878928 ............ 52 00000878936 ............ 52 00000882801 ............ 44 00000882828 ............ 44 00000882836 ............ 44 00000883751 .............. 8 00000884324 ............ 39 00000884332 ............ 39 00000884340 ............ 39 00000884359 ............ 40 00000884413 ............ 60 00000884502 SEC 3.55 00000885401 ............ 76 00000885428 ............ 76 00000885436 ............ 76 00000885444 ............ 76 00000885835 ............ 56 00000885851 ............ 56 00000886009 ............ 50 00000886017 ............ 70

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 230 EFFECTIVE APRIL 1, 2012
00000886033 ............ 55 00000886041 ............ 55 00000886068 ............ 53 00000886076 ............ 53 00000886106 .......... 126 00000886130 ............ 50 00000886149 ............ 50 00000886157 ............ 16 00000886432 .......... 142 00000886440 .......... 142 00000888346 . SEC 3.39 00000888400 .......... 127 00000890960 ............ 34 00000891738 .......... 183 00000891746 .......... 183 00000891835 ............ 14 00000893595 ............ 56 00000893609 ............ 56 00000893617 ............ 56 00000893625 ............ 56 00000893722 .......... 162 00000893749 ............ 38 00000893757 ............ 38 00000893773 .......... 136 00000894737 ............ 97 00000894745 ............ 98 00000895644 ............ 43 00000895652 ............ 43 00000895660 ............ 43 00000990014 .......... 189 00000990015 .......... 189 00000990016 .......... 189 00000990017 .......... 189 00000990080 .......... 189 00000990081 .......... 189 00000990082 .......... 189 00000990088 .......... 189 00000990089 .......... 189 00000990091 .......... 189 00000990092 .......... 189 00000990093 .......... 189 00000990094 .......... 189 00000990095 .......... 189 00000990096 .......... 189 00000990097 .......... 189 00000990098 .......... 189 00000990099 .......... 189 00000990100 .......... 189 00000999102 ............ 69 00000999103 .......... 171
00000999104 .......... 178 00000999105 ............ 69 00000999107 .......... 175 00000999108 ............ 76 00000999109 .......... 135 00000999110 .......... 177 00000999111 .......... 155 00000999112 .......... 171 00000999113 .......... 186 00000999114 .......... 186 00000999119 .......... 171 00000999202 ............ 69 00000999203 .......... 171 00000999204 .......... 178 00000999205 ............ 69 00000999207 .......... 175 00000999208 ............ 76 00000999209 .......... 135 00000999211 .......... 177 00000999212 .......... 155 00000999213 .......... 171 00000999214 .......... 186 00000999215 .......... 186 00000999216 .......... 186 00000999219 .......... 171 00000999949 .......... 189 00000999981 .......... 169 00000999995 ............ 77 00000999999 .......... 186 00001900927 .......... 165 00001900935 .......... 165 00001901869 ............ 79 00001905112 . SEC 3.31 00001907107 ............ 58 00001907115 ............ 58 00001907123 ............ 55 00001907476 .......... 178 00001908448 .......... 135 00001910140 ............ 46 00001910159 ............ 46 00001910167 ............ 46 00001910272 .......... 174 00001910280 .......... 174 00001910299 .......... 175 00001911473 ............ 56 00001911481 ............ 57 00001911627 ............ 16 00001911902 ............ 43 00001911910 ............ 43 00001911929 ............ 43
00001912038 ............ 71 00001912046 ............ 71 00001912054 ............ 47 00001912062 ............ 46 00001912070 .......... 149 00001912410 ............ 10 00001912429 ............ 10 00001912755 .......... 131 00001913425 ............ 94 00001913433 ............ 94 00001913441 ............ 94 00001913468 ............ 95 00001913476 ............ 95 00001913484 .......... 109 00001913492 .......... 109 00001913654 .......... 165 00001913662 .......... 165 00001913670 .......... 165 00001913689 .......... 165 00001913794 ............ 44 00001913808 ............ 44 00001913816 ............ 44 00001913824 ............ 56 00001913832 ............ 56 00001913840 ............ 56 00001913859 ............ 56 00001914030 .......... 150 00001916181 .......... 133 00001916203 .......... 133 00001916386 ............ 76 00001916394 ............ 77 00001916475 ............ 80 00001916491 ............ 80 00001916548 ............ 80 00001916823 .......... 151 00001916858 .............. 9 00001916874 .............. 9 00001916882 .............. 9 00001916947 .......... 172 00001917056 ............ 70 00001918303 .......... 125 00001918311 ............ 27 00001918338 ............ 27 00001918346 ............ 27 00001918354 ............ 28 00001918362 ............ 28 00001919342 ............ 91 00001919369 ............ 91 00001919431 .......... 169 00001919458 .......... 167
00001919466 .......... 167 00001919598 ............ 88 00001924516 .......... 107 00001924559 .......... 107 00001924567 .......... 107 00001925938 .............. 6 00001926292 .............. 1 00001926306 .............. 1 00001926454 ............ 42 00001926462 SEC 3.87 00001926470 SEC 3.87 00001926489 SEC 3.88 00001926543 ............ 46 00001926551 ............ 46 00001926578 ............ 46 00001926667 .......... 105 00001926675 .......... 105 00001926691 .......... 165 00001926713 ............ 43 00001926756 .......... 105 00001926764 .......... 105 00001926772 .......... 105 00001926780 .......... 105 00001926799 .......... 112 00001926829 .......... 172 00001926845 .......... 172 00001926861 .......... 172 00001926934 ............ 23 00001927604 .......... 151 00001927620 .......... 151 00001927639 .......... 105 00001927698 .......... 105 00001927744 .......... 116 00001927914 .......... 174 00001930672 .............. 8 00001930680 .............. 8 00001933345 .............. 9 00001933353 ............ 10 00001934139 ............ 72 00001934163 .............. 9 00001934171 .............. 9 00001934198 ............ 44 00001934201 ............ 44 00001934228 ............ 44 00001934317 ............ 55 00001934325 .......... 157 00001934333 .......... 157 00001934341 .......... 157 00001937219 .......... 126 00001937227 ............ 93

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 231
00001937235 ............ 93 00001940309 ............ 74 00001940414 .......... 134 00001940473 ............ 92 00001940481 ............ 92 00001942964 ............ 56 00001942972 ............ 56 00001942980 ............ 56 00001942999 ............ 56 00001945262 . SEC 3.31 00001945270 .......... 131 00001946374 .......... 178 00001947664 ............ 60 00001947672 ............ 60 00001947680 ............ 61 00001947699 ............ 61 00001947796 ............ 51 00001947818 ............ 51 00001947826 ............ 51 00001950592 .......... 150 00001953834 .......... 145 00001953842 .......... 145 00001958097 ............ 44 00001958100 ............ 44 00001958119 ............ 44 00001959212 .......... 163 00001959220 .......... 163 00001959239 .......... 163 00001962701 .......... 175 00001962779 ............ 93 00001962817 ............ 92 00001964054 .......... 177 00001964070 .......... 156 00001964968 .......... 156 00001964976 .......... 156 00001966197 ............ 33 00001966200 ............ 33 00001966219 .......... 181 00001968017 . SEC 3.40 00001968300 .......... 134 00001968440 .......... 160 00001968823 .......... 134 00001975447 ............ 10 00001976133 .......... 179 00001977547 .......... 156 00001977563 .......... 158 00001977652 .......... 166 00001978918 .......... 155 00001978926 .......... 155 00001979574 ............ 35
00001979582 ............ 35 00001980661 .......... 132 00001981242 .......... 153 00001981250 .......... 153 00001981501 .......... 187 00001984837 .......... 185 00001984845 .......... 185 00001984853 .............. 7 00001985205 .......... 141 00001986864 ............ 23 00001987003 .......... 183 00001990403 .......... 115 00001992872 .......... 160 00001997580 .......... 150 00001997602 ............ 25 00001997653 ............ 25 00001997750 ............ 17 00001997769 ............ 17 00001999761 .......... 158 00001999869 .......... 158 00002007134 .......... 165 00002007959 ............ 28 00002008203 .......... 112 00002009706 ............ 78 00002009749 ............ 78 00002009765 ............ 78 00002009773 ............ 78 00002010909 . SEC 3.40 00002011271 ............ 43 00002012472 ............ 29 00002013231 .......... 113 00002014165 .......... 181 00002014181 .......... 181 00002014203 ............ 78 00002014211 ............ 78 00002014238 ............ 78 00002014254 ............ 78 00002014297 ............ 78 00002014300 ............ 78 00002014319 ............ 78 00002014327 ............ 78 00002015439 ............ 78 00002015951 ............ 72 00002015994 . SEC 3.31 00002017237 ............ 73 00002017709 ............ 17 00002017741 .......... 125 00002017776 ............ 17 00002018144 .......... 158 00002018152 .......... 158
00002018160 .......... 158 00002018985 ............ 91 00002019884 ............ 57 00002019892 ............ 57 00002019906 ............ 58 00002019930 ............ 78 00002019949 ............ 78 00002019957 ............ 79 00002019965 ............ 79 00002020025 ............ 57 00002020661 ............ 71 00002020688 ............ 71 00002020726 ............ 71 00002020734 .......... 165 00002020742 .......... 165 00002021048 ............ 79 00002021056 ............ 79 00002022133 .......... 145 00002022141 .......... 145 00002022826 .......... 115 00002024152 .SEC 3.41 00002024187 .......... 174 00002024195 .......... 145 00002024209 .......... 145 00002024217 .......... 163 00002024225 .......... 163 00002024233 .......... 163 00002024268 .......... 163 00002024284 .......... 163 00002024314 .......... 163 00002024322 .......... 163 00002025248 .......... 163 00002025280 .......... 101 00002025299 .......... 102 00002025302 .......... 102 00002025310 .......... 102 00002026600 ............ 74 00002026767 .......... 174 00002026961 .......... 126 00002028700 .......... 160 00002028786 .......... 117 00002029421 .......... 160 00002029448 .......... 187 00002029456 ............ 96 00002031094 .......... 172 00002031116 ............ 14 00002031159 .......... 136 00002031167 .......... 136 00002035324 .......... 132 00002036282 ............ 34
00002036347 .............. 8 00002036355 .............. 8 00002039486 ............ 71 00002039494 ............ 71 00002039508 ............ 21 00002039532 ............ 46 00002039540 ............ 47 00002040751 ............ 94 00002040778 ............ 94 00002040786 ............ 94 00002041413 .......... 110 00002041421 .......... 110 00002041448 .......... 110 00002041456 .......... 110 00002041464 .......... 110 00002041472 .......... 110 00002041510 ............ 15 00002042231 ............ 50 00002042258 ............ 50 00002042266 ............ 50 00002042274 ............ 50 00002042304 .......... 125 00002042320 .......... 159 00002042339 .......... 159 00002042479 .......... 158 00002042487 .......... 158 00002042533 .......... 158 00002042568 ............ 83 00002042576 ............ 74 00002042584 ............ 74 00002043394 .......... 160 00002043408 .......... 160 00002043424 .......... 160 00002043440 .......... 160 00002044609 ............ 51 00002044617 ............ 51 00002044668 ............ 11 00002045702 .......... 147 00002045710 .......... 162 00002045729 ............ 60 00002045737 ............ 60 00002045834 .......... 141 00002045869 .......... 141 00002046113 .......... 130 00002046121 ............ 40 00002046148 ............ 40 00002046156 ............ 43 00002047454 ............ 14 00002048264 ............ 34 00002048272 ............ 34

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 232 EFFECTIVE APRIL 1, 2012
00002048493 ............ 71 00002048698 ............ 70 00002048701 ............ 82 00002048728 ............ 82 00002048736 ............ 82 00002049325 . SEC 3.45 00002049333 ............ 59 00002049376 ............ 59 00002049384 ............ 59 00002049392 . SEC 3.60 00002049961 ............ 47 00002049988 ............ 47 00002049996 ............ 94 00002050005 ............ 94 00002050013 ............ 94 00002050021 ............ 94 00002050048 ............ 95 00002052431 .......... 174 00002057778 ............ 52 00002058456 ............ 35 00002058464 ............ 35 00002059762 .......... 187 00002059789 .......... 187 00002060884 .......... 174 00002061562 ............ 37 00002061570 ............ 37 00002063662 ............ 18 00002063670 .......... 179 00002063697 .......... 157 00002063700 .......... 157 00002063719 .......... 157 00002063727 .......... 157 00002063735 ............ 25 00002063743 ............ 25 00002063786 . SEC 3.73 00002063808 .......... 150 00002064405 ............ 31 00002064472 ............ 11 00002064480 ............ 11 00002065614 .......... 110 00002065819 ............ 87 00002068036 ............ 87 00002068087 .......... 119 00002069571 ............ 23 00002070847 .......... 179 00002070863 .......... 179 00002070987 ............ 96 00002074788 .......... 179 00002076306 .......... 138 00002078627 ............ 16
00002078635 ............ 16 00002078651 ............ 16 00002080052 ............ 25 00002083345 .......... 136 00002083353 .......... 136 00002083523 ............ 35 00002083795 .......... 178 00002084090 ............ 12 00002084104 ............ 12 00002084228 ............ 51 00002084236 ............ 51 00002084260 ............ 84 00002084279 ............ 84 00002084287 ............ 85 00002085895 ............ 77 00002085992 .......... 125 00002086026 .......... 156 00002087316 .......... 186 00002087324 .......... 117 00002088398 ............ 25 00002088401 ............ 25 00002089602 .......... 173 00002091194 ............ 70 00002091526 .......... 130 00002091879 .......... 162 00002093162 .......... 174 00002097168 . SEC 3.54 00002097176 . SEC 3.54 00002097249 ............ 54 00002097257 ............ 54 00002097265 ............ 54 00002097273 ............ 54 00002099233 .......... 162 00002099683 .......... 150 00002099705 ............ 19 00002100509 ............ 71 00002100517 ............ 71 00002100622 .......... 147 00002100630 ............ 87 00002102978 ............ 21 00002103052 .......... 184 00002103087 ............ 21 00002103095 ............ 21 00002103567 .......... 147 00002103613 .......... 149 00002103656 ............ 82 00002103729 ............ 60 00002103737 ............ 82 00002106272 ............ 48 00002106280 ............ 48
00002108119 .............. 3 00002108127 .............. 3 00002108135 .............. 3 00002108143 ............ 12 00002108151 ............ 12 00002112736 .......... 176 00002112760 .......... 150 00002112787 .......... 150 00002112795 .......... 150 00002112809 .......... 150 00002122197 ............ 14 00002123274 ............ 60 00002123282 ............ 60 00002125250 .......... 147 00002125323 ............ 76 00002125331 ............ 76 00002125366 ............ 76 00002125382 ............ 76 00002125390 ............ 76 00002126192 .......... 174 00002126222 ............ 22 00002126559 ............ 42 00002126710 .............. 7 00002126753 ............ 49 00002126761 ............ 49 00002128446 .......... 177 00002129043 .SEC 3.21 00002130297 .......... 104 00002130300 .......... 104 00002131048 ............ 25 00002131056 ............ 25 00002131064 ............ 26 00002132621 ............ 28 00002132648 ............ 28 00002132664 ............ 28 00002132680 ............ 34 00002132699 ............ 34 00002132702 ............ 92 00002134829 .......... 147 00002136090 ............ 25 00002136104 ............ 25 00002136112 ............ 74 00002136120 ............ 74 00002137534 .......... 109 00002137542 .......... 109 00002137984 ............ 81 00002138018 ............ 77 00002139200 .......... 115 00002139332 ............ 25 00002139391 ............ 25
00002140063 ............ 87 00002142074 ............ 35 00002142082 ............ 85 00002142104 ............ 85 00002142112 ............ 85 00002143275 .......... 149 00002143283 .......... 149 00002143291 .......... 131 00002144263 ............ 93 00002144271 ............ 93 00002144298 ............ 93 00002144328 SEC 3.56 00002144336 SEC 3.56 00002144344 SEC 3.56 00002145227 ............ 82 00002145235 ............ 82 00002145243 ............ 82 00002145901 ............ 76 00002145928 ............ 77 00002145936 ............ 77 00002146126 ............ 77 00002146843 ............ 23 00002146851 ............ 23 00002146886 ............ 74 00002146894 ............ 46 00002146908 .............. 7 00002146959 ............ 35 00002147432 ............ 47 00002147602 ............ 46 00002147610 ............ 46 00002147629 ............ 46 00002147637 ............ 93 00002147645 ............ 93 00002147653 ............ 93 00002148587 .......... 161 00002148595 .......... 161 00002148765 .......... 162 00002150662 SEC 3.21 00002150670 SEC 3.21 00002150689 SEC 3.21 00002150697 SEC 3.21 00002150956 .......... 179 00002153483 .......... 127 00002153521 .......... 150 00002153556 .......... 150 00002153564 .......... 150 00002154412 ............ 23 00002154463 ............ 74 00002155907 ............ 53 00002155958 SEC 3A.2

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 233
00002155966 SEC 3A.3 00002155974 SEC 3A.3 00002155990 ............ 53 00002156008 .......... 106 00002156016 .......... 106 00002156032 .......... 106 00002156040 .......... 106 00002156091 .......... 171 00002157195 .......... 149 00002158574 ............ 11 00002158582 ............ 70 00002158590 .......... 181 00002158612 ............ 95 00002158620 ............ 95 00002158639 ............ 95 00002161737 SEC 3A.2 00002161745 SEC 3A.3 00002161753 SEC 3A.3 00002162415 ............ 73 00002162423 ............ 73 00002162431 ............ 73 00002162466 ............ 73 00002162644 ............ 72 00002162660 ............ 72 00002162695 ............ 17 00002162717 ............ 74 00002162725 ............ 74 00002162792 ............ 73 00002162806 ............ 43 00002162814 ............ 70 00002162822 .......... 162 00002162849 .......... 162 00002163527 ............ 43 00002163535 ............ 43 00002163543 .......... 181 00002163551 ............ 56 00002163578 ............ 56 00002163586 ............ 56 00002163594 ............ 56 00002163659 .............. 4 00002163667 .............. 4 00002163675 .............. 4 00002163683 .............. 4 00002163705 ............ 22 00002163772 ............ 51 00002163918 ............ 75 00002163926 ............ 75 00002163934 ............ 75 00002163942 ............ 75 00002165384 ............ 93
00002165392 ............ 93 00002165406 ............ 93 00002165503 .......... 147 00002165511 .......... 147 00002165546 ............ 46 00002165554 ............ 46 00002165562 ............ 46 00002166704 .......... 166 00002166712 .......... 136 00002166720 .......... 136 00002167786 .......... 162 00002167794 ............ 51 00002167840 ............ 29 00002168898 .......... 161 00002168979 . SEC 3.57 00002169649 . SEC 2.10 00002169991 .......... 107 00002170493 .......... 186 00002170698 ............ 19 00002170795 . SEC 3.72 00002170809 . SEC 3.72 00002170817 . SEC 3.72 00002171228 .......... 167 00002171791 ............ 46 00002171805 ............ 47 00002171848 ............ 25 00002171880 .......... 136 00002171899 .......... 136 00002171929 .......... 150 00002172062 .......... 167 00002172070 .......... 167 00002172089 .......... 167 00002172097 .......... 167 00002172100 .......... 167 00002172119 .......... 167 00002172127 .......... 167 00002172135 .......... 167 00002172143 .......... 167 00002172151 .......... 167 00002172577 ............ 72 00002172712 .......... 132 00002173360 ............ 23 00002174545 ............ 49 00002174553 ............ 49 00002176017 .......... 186 00002176084 .............. 1 00002177145 ............ 25 00002177153 .......... 109 00002177161 .......... 109 00002177188 .......... 109
00002177579 ............ 91 00002177587 ............ 91 00002177692 ............ 95 00002177706 ............ 95 00002177714 .......... 145 00002177722 .......... 145 00002177749 ............ 78 00002177757 ............ 79 00002177889 ............ 82 00002177897 ............ 82 00002179660 ............ 82 00002179679 ............ 74 00002179687 ............ 74 00002181479 ............ 57 00002182750 ............ 19 00002182777 ............ 19 00002182815 ............ 64 00002182823 .......... 117 00002182831 .......... 117 00002182858 .......... 117 00002182866 ............ 13 00002182874 ............ 64 00002182882 ............ 64 00002182955 ............ 19 00002182963 ............ 19 00002184435 ............ 79 00002184443 ............ 79 00002184451 ............ 79 00002184648 ............ 87 00002185407 ............ 35 00002185431 .......... 149 00002185881 .......... 142 00002187086 .......... 160 00002187094 .......... 160 00002187108 .......... 160 00002187116 .......... 160 00002188783 .......... 187 00002189054 .......... 160 00002189062 .......... 160 00002190885 .......... 162 00002190893 .......... 162 00002190915 .......... 148 00002192268 .......... 173 00002192276 .......... 173 00002192284 .......... 173 00002192756 ............ 91 00002192764 ............ 91 00002193221 .......... 183 00002194031 .......... 177 00002194058 .......... 177
00002194066 .......... 177 00002194198 ............ 15 00002194201 ............ 15 00002194333 ............ 83 00002194341 .......... 179 00002195917 SEC 3.57 00002195925 SEC 3.57 00002195933 .......... 117 00002195941 .......... 117 00002195968 .......... 117 00002196018 .......... 145 00002196026 .......... 145 00002197413 ............ 16 00002197421 ............ 16 00002197502 .......... 160 00002199270 SEC 3.85 00002199297 .......... 160 00002200104 .......... 141 00002200996 ............ 51 00002201038 SEC 3.14 00002202441 ............ 80 00002202468 ............ 80 00002202476 ............ 80 00002202484 ............ 80 00002203324 .......... 141 00002204517 ............ 46 00002204525 ............ 46 00002204533 ............ 46 00002205963 ............ 27 00002207621 ............ 16 00002207648 ............ 16 00002207656 ............ 16 00002207672 .......... 111 00002207761 .......... 146 00002207788 .......... 146 00002207818 ............ 82 00002208229 ............ 23 00002208237 ............ 23 00002208245 ............ 23 00002210320 ............ 34 00002210347 ............ 55 00002210355 ............ 55 00002210363 ............ 55 00002210428 ............ 51 00002210479 ............ 22 00002211076 .......... 111 00002211920 ............ 55 00002212021 .............. 7 00002212048 ............ 25 00002212153 .......... 114

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 234 EFFECTIVE APRIL 1, 2012
00002212153 . SEC 3.82 00002212161 .......... 114 00002212161 . SEC 3.82 00002212188 .......... 114 00002212188 . SEC 3.82 00002212218 .............. 5 00002212226 .............. 5 00002212234 .............. 5 00002212277 .............. 5 00002212285 .............. 5 00002212331 .......... 146 00002212358 .......... 146 00002212366 .......... 146 00002213192 .......... 167 00002213206 .......... 167 00002213214 .......... 167 00002213222 .......... 167 00002213265 .......... 174 00002213273 .......... 174 00002213281 .......... 175 00002213419 ............ 23 00002213427 ............ 23 00002213486 ............ 23 00002213567 .......... 143 00002213575 .......... 143 00002213745 .......... 143 00002214261 ............ 23 00002215136 . SEC 3.80 00002216132 .......... 113 00002216140 .......... 113 00002216159 .......... 113 00002216167 .......... 112 00002216205 .......... 136 00002216213 .......... 175 00002216221 . SEC 3.54 00002216248 ............ 94 00002216256 ............ 94 00002216264 ............ 94 00002216272 ............ 94 00002216345 ............ 21 00002216353 ............ 91 00002216361 ............ 91 00002216582 ............ 91 00002216590 ............ 91 00002217422 ............ 18 00002217481 ............ 59 00002217503 ............ 59 00002217511 ............ 59 00002218313 .......... 112 00002218321 ............ 87
00002218453 ............ 91 00002218461 ............ 91 00002218488 . SEC 3.58 00002218496 . SEC 3.58 00002218941 ............ 45 00002218968 ............ 45 00002218976 ............ 45 00002218984 ............ 45 00002219492 ............ 17 00002220156 .......... 145 00002220164 .......... 145 00002220172 ............ 37 00002220180 ............ 37 00002220407 . SEC 3.81 00002221284 .......... 166 00002221292 .......... 166 00002221306 .......... 166 00002221780 ............ 27 00002221802 .......... 173 00002221829 ............ 61 00002221837 ............ 61 00002221845 ............ 61 00002221853 ............ 62 00002221896 .......... 175 00002221918 .......... 175 00002221977 ............ 31 00002221985 ............ 52 00002221993 ............ 52 00002222000 ............ 53 00002222051 ............ 38 00002223139 ............ 95 00002223147 ............ 95 00002223252 .......... 178 00002223376 .......... 181 00002223481 ............ 91 00002223503 ............ 91 00002223511 ............ 95 00002223538 ............ 95 00002223562 .......... 162 00002223597 .......... 127 00002223678 .......... 127 00002223716 .............. 7 00002223724 .............. 7 00002223767 . SEC 3.72 00002223775 . SEC 3.72 00002224550 .......... 165 00002224569 .......... 165 00002224623 .......... 133 00002224690 ............ 41 00002224704 ............ 41
00002224720 ............ 41 00002224755 ............ 41 00002224801 ............ 33 00002224828 ............ 33 00002225085 .............. 5 00002225093 .............. 5 00002225107 .............. 5 00002225158 .SEC 3.18 00002225166 .SEC 3.18 00002225190 .......... 161 00002225905 .SEC 3.45 00002225964 .......... 111 00002225972 .......... 111 00002225980 ............ 35 00002226383 .......... 178 00002226391 .......... 178 00002226839 .......... 171 00002227444 .......... 144 00002227452 .......... 144 00002227460 .......... 144 00002227479 .......... 144 00002228270 .......... 112 00002228947 ............ 24 00002228955 .SEC 3.18 00002229080 ............ 72 00002229099 .......... 155 00002229250 ............ 98 00002229269 ............ 98 00002229277 ............ 98 00002229285 ............ 98 00002229293 .SEC 3.18 00002229315 .......... 175 00002229323 .......... 175 00002229440 .......... 131 00002229441 .......... 131 00002229452 ............ 72 00002229453 .......... 148 00002229515 ............ 29 00002229517 .......... 162 00002229519 .......... 164 00002229521 SEC 3A.2 00002229522 SEC 3A.3 00002229523 SEC 3A.3 00002229524 ............ 10 00002229526 ............ 54 00002229540 .......... 158 00002229550 .......... 158 00002229628 ............ 87 00002229639 .......... 143 00002229654 .......... 111
00002229655 .......... 111 00002229656 .......... 162 00002229704 .......... 163 00002229705 .......... 163 00002229755 ............ 29 00002229777 .......... 135 00002229778 ............ 51 00002229779 ............ 51 00002229781 ............ 54 00002229782 ............ 54 00002229783 ............ 54 00002229784 ............ 54 00002229785 .......... 162 00002229837 ............ 70 00002230019 .......... 141 00002230047 ............ 65 00002230089 SEC 3.41 00002230090 ............ 31 00002230095 .......... 111 00002230102 .......... 111 00002230104 SEC 3.41 00002230183 ............ 35 00002230201 ............ 72 00002230243 .............. 8 00002230244 .............. 8 00002230245 .............. 9 00002230246 .............. 9 00002230248 SEC 3.55 00002230359 ............ 33 00002230360 ............ 33 00002230394 .......... 181 00002230402 .......... 107 00002230403 .......... 107 00002230405 .......... 106 00002230406 .......... 106 00002230418 .......... 114 00002230418 SEC 3.81 00002230420 .......... 114 00002230420 SEC 3.81 00002230431 .......... 149 00002230432 .......... 149 00002230433 .......... 149 00002230454 .......... 117 00002230475 .......... 162 00002230476 ............ 35 00002230535 ............ 13 00002230540 ............ 13 00002230584 .......... 109 00002230585 .......... 109 00002230619 .......... 157

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 235
00002230641 .......... 119 00002230648 .......... 132 00002230661 ............ 74 00002230684 .......... 150 00002230711 ............ 36 00002230713 ............ 36 00002230714 ............ 36 00002230717 .......... 119 00002230730 .............. 1 00002230732 ............ 43 00002230733 ............ 43 00002230734 ............ 43 00002230735 ............ 12 00002230736 ............ 12 00002230737 .......... 148 00002230768 ............ 87 00002230784 .......... 180 00002230785 .......... 180 00002230800 .......... 181 00002230803 ............ 49 00002230804 ............ 49 00002230805 ............ 45 00002230806 ............ 45 00002230807 ............ 45 00002230808 ............ 45 00002230837 .......... 107 00002230838 .......... 107 00002230839 .......... 107 00002230840 .......... 107 00002230888 .......... 131 00002230893 ............ 86 00002230894 ............ 86 00002230896 ............ 87 00002230898 ............ 22 00002230942 .......... 111 00002230950 ............ 82 00002230951 ............ 82 00002230997 ............ 54 00002230998 ............ 54 00002230999 ............ 54 00002231015 ............ 18 00002231016 ............ 18 00002231036 .......... 119 00002231052 ............ 54 00002231053 ............ 54 00002231054 ............ 54 00002231061 ............ 14 00002231129 ............ 23 00002231135 . SEC 3.54 00002231136 ............ 22
00002231143 . SEC 3.17 00002231150 ............ 54 00002231151 ............ 54 00002231152 ............ 55 00002231154 ............ 55 00002231155 ............ 55 00002231171 ............ 28 00002231181 ............ 51 00002231182 ............ 51 00002231184 .......... 127 00002231192 ............ 91 00002231193 ............ 91 00002231244 . SEC 3.54 00002231245 . SEC 3.54 00002231328 ............ 91 00002231329 ............ 91 00002231330 ............ 91 00002231347 . SEC 3.54 00002231353 ............ 25 00002231379 .......... 142 00002231441 ............ 42 00002231457 ............ 62 00002231459 ............ 62 00002231460 ............ 62 00002231477 .......... 149 00002231478 ............ 29 00002231491 .......... 185 00002231492 .......... 111 00002231493 .......... 137 00002231504 ............ 70 00002231505 ............ 70 00002231506 ............ 70 00002231508 ............ 70 00002231509 .......... 161 00002231510 .......... 161 00002231529 SEC 3A.5 00002231531 SEC 3A.5 00002231532 SEC 3A.5 00002231536 ............ 50 00002231537 ............ 50 00002231539 ............ 50 00002231540 ............ 83 00002231542 ............ 83 00002231543 ............ 83 00002231544 ............ 83 00002231583 . SEC 3.30 00002231584 . SEC 3.30 00002231585 . SEC 3.30 00002231586 . SEC 3.30 00002231587 . SEC 3.30
00002231675 ............ 22 00002231683 ............ 93 00002231684 ............ 93 00002231689 ............ 48 00002231731 ............ 46 00002231733 ............ 47 00002231781 ............ 95 00002231782 ............ 95 00002231799 ............ 71 00002231800 ............ 72 00002231893 .......... 157 00002231894 .......... 157 00002231895 .......... 157 00002232043 .SEC 3.24 00002232044 .SEC 3.24 00002232148 ............ 88 00002232150 ............ 88 00002232191 .......... 174 00002232193 .......... 174 00002232195 .......... 175 00002232317 ............ 71 00002232318 ............ 71 00002232565 .......... 118 00002232567 .......... 118 00002232568 .......... 119 00002232569 .......... 119 00002232570 ............ 23 00002233005 ............ 57 00002233006 ............ 57 00002233007 ............ 58 00002233047 ............ 45 00002233048 ............ 45 00002233049 ............ 45 00002233050 ............ 45 00002233852 .......... 167 00002233960 ............ 82 00002233982 ............ 82 00002233985 ............ 82 00002234003 .......... 111 00002234007 .......... 111 00002234466 .......... 176 00002234502 ............ 45 00002234503 ............ 45 00002234504 ............ 45 00002234505 ............ 45 00002234510 ............ 75 00002234749 .......... 108 00002235134 .SEC 3.19 00002236399 .......... 177 00002236466 .......... 149
00002236507 ............ 25 00002236508 ............ 25 00002236564 ............ 29 00002236606 .......... 129 00002236606 SEC 3.92 00002236734 .......... 165 00002236783 ............ 23 00002236807 ............ 87 00002236819 .......... 185 00002236841 SEC 3A.4 00002236842 SEC 3A.4 00002236848 ............ 30 00002236876 .......... 135 00002236883 ............ 29 00002236913 ............ 29 00002236948 ............ 82 00002236950 .......... 103 00002236951 ............ 99 00002236952 ............ 99 00002236953 .......... 100 00002236963 ............ 25 00002236964 ............ 25 00002236974 .......... 159 00002236975 .......... 159 00002236978 ............ 14 00002236979 ............ 14 00002236996 .......... 175 00002236997 .......... 175 00002237111 ............ 88 00002237224 ............ 23 00002237225 ............ 23 00002237235 ............ 14 00002237246 .......... 156 00002237247 .......... 156 00002237250 ............ 96 00002237279 ............ 89 00002237280 ............ 89 00002237282 ............ 89 00002237313 ............ 12 00002237314 ............ 12 00002237319 SEC 2.10 00002237320 SEC 2.10 00002237339 ............ 93 00002237367 ............ 61 00002237368 ............ 61 00002237369 ............ 61 00002237370 ............ 14 00002237371 ............ 14 00002237514 SEC 3A.1 00002237560 ............ 30

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 236 EFFECTIVE APRIL 1, 2012
00002237600 ............ 46 00002237601 ............ 47 00002237618 ............ 53 00002237671 . SEC 3.21 00002237682 ............ 10 00002237701 ............ 30 00002237721 ............ 46 00002237722 ............ 46 00002237723 ............ 46 00002237770 . SEC 2.10 00002237791 ............ 55 00002237813 ............ 91 00002237814 ............ 91 00002237820 .......... 113 00002237820 . SEC 3.60 00002237821 .......... 113 00002237821 . SEC 3.60 00002237825 ............ 96 00002237830 ............ 87 00002237860 .......... 166 00002237885 ............ 46 00002237886 ............ 46 00002237887 ............ 46 00002237910 ............ 72 00002237921 ............ 55 00002237922 ............ 55 00002237923 ............ 63 00002237924 ............ 63 00002237925 ............ 64 00002237971 . SEC 3.80 00002237991 .......... 136 00002238048 ............ 87 00002238103 .......... 164 00002238171 .............. 8 00002238172 .............. 8 00002238216 .......... 129 00002238216 . SEC 3.59 00002238217 .......... 129 00002238217 . SEC 3.59 00002238280 ............ 92 00002238281 ............ 92 00002238282 ............ 93 00002238316 ............ 46 00002238318 ............ 47 00002238326 ............ 51 00002238327 ............ 51 00002238334 ............ 81 00002238370 ............ 87 00002238403 .......... 105 00002238404 .......... 105
00002238405 .......... 105 00002238406 .......... 105 00002238465 .......... 132 00002238525 .......... 147 00002238560 . SEC 3.41 00002238568 .......... 132 00002238577 .......... 132 00002238596 .......... 112 00002238604 .......... 125 00002238639 ............ 72 00002238645 ............ 75 00002238646 ............ 75 00002238660 .......... 115 00002238660 . SEC 3.93 00002238682 . SEC 3.20 00002238703 .......... 172 00002238704 .......... 161 00002238796 .......... 132 00002238829 .............. 9 00002238830 .............. 9 00002238831 .............. 9 00002238850 ............ 99 00002238873 .......... 136 00002238903 .......... 116 00002238984 .......... 141 00002238998 ............ 42 00002239024 ............ 82 00002239025 ............ 82 00002239028 . SEC 3.73 00002239044 .......... 135 00002239091 ............ 63 00002239092 ............ 63 00002239131 ............ 22 00002239146 . SEC 3.74 00002239170 . SEC 3.85 00002239193 ............ 15 00002239267 ............ 62 00002239288 .......... 132 00002239323 . SEC 3.61 00002239324 . SEC 3.61 00002239325 . SEC 3.61 00002239326 ............ 96 00002239327 ............ 96 00002239365 ............ 23 00002239366 ............ 23 00002239367 .......... 114 00002239367 . SEC 3.82 00002239372 .......... 142 00002239373 .......... 142 00002239505 . SEC 3.46
00002239517 ............ 84 00002239518 ............ 84 00002239519 ............ 84 00002239577 .......... 131 00002239607 ............ 90 00002239608 ............ 90 00002239619 .......... 127 00002239620 .......... 127 00002239627 ............ 22 00002239630 .............. 3 00002239636 .......... 104 00002239653 .SEC 3.84 00002239665 .SEC 3.58 00002239698 ............ 84 00002239699 ............ 84 00002239700 ............ 84 00002239701 ............ 84 00002239702 ............ 84 00002239703 ............ 84 00002239714 ............ 87 00002239744 ............ 30 00002239746 ............ 88 00002239747 ............ 88 00002239748 ............ 88 00002239757 .......... 172 00002239834 .SEC 3.55 00002239835 ............ 34 00002239864 ............ 35 00002239893 ............ 14 00002239907 ............ 87 00002239908 ............ 87 00002239924 .......... 164 00002239925 .......... 164 00002239926 .......... 164 00002239941 .SEC 3.19 00002239942 .SEC 3.19 00002239944 ............ 72 00002239951 ............ 35 00002239953 ............ 91 00002239954 ............ 91 00002240067 .......... 127 00002240071 ............ 34 00002240113 .......... 138 00002240114 ............ 29 00002240115 ............ 85 00002240131 ............ 80 00002240132 ............ 80 00002240205 ............ 27 00002240210 ............ 35 00002240286 .......... 110
00002240294 .......... 164 00002240297 .......... 164 00002240329 .......... 183 00002240332 ............ 40 00002240333 ............ 96 00002240334 ............ 96 00002240346 ............ 14 00002240432 ............ 63 00002240456 ............ 88 00002240457 .......... 145 00002240458 .......... 145 00002240481 ............ 93 00002240484 ............ 92 00002240485 ............ 92 00002240498 ............ 44 00002240499 ............ 44 00002240500 ............ 44 00002240518 .......... 113 00002240518 SEC 3.78 00002240519 .......... 113 00002240519 SEC 3.78 00002240521 .......... 113 00002240521 SEC 3.78 00002240549 .......... 181 00002240550 .......... 181 00002240551 .......... 101 00002240552 .......... 101 00002240588 ............ 44 00002240589 ............ 44 00002240590 ............ 44 00002240604 ............ 34 00002240606 .......... 112 00002240682 ............ 91 00002240683 ............ 91 00002240684 .......... 156 00002240687 .......... 156 00002240722 SEC 3.29 00002240769 ............ 65 00002240770 ............ 65 00002240774 SEC 3.19 00002240775 SEC 3.83 00002240807 ............ 14 00002240835 ............ 24 00002240836 ............ 24 00002240837 ............ 24 00002240851 .......... 176 00002240867 ............ 72 00002240908 ............ 92 00002240909 ............ 92 00002241007 ............ 65

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 237
00002241024 ............ 73 00002241112 . SEC 3.78 00002241113 . SEC 3.78 00002241114 . SEC 3.78 00002241163 ............ 24 00002241209 .............. 3 00002241210 .............. 3 00002241224 ............ 70 00002241229 .......... 157 00002241332 .......... 161 00002241371 ............ 91 00002241374 ............ 91 00002241377 ............ 77 00002241497 ............ 23 00002241600 .......... 153 00002241601 ............ 35 00002241602 ............ 35 00002241674 .......... 159 00002241704 ............ 35 00002241709 ............ 13 00002241710 ............ 13 00002241715 .......... 136 00002241716 .......... 136 00002241755 .......... 131 00002241818 ............ 64 00002241819 ............ 64 00002241820 ............ 12 00002241821 ............ 12 00002241835 .......... 161 00002241837 .......... 161 00002241882 ............ 83 00002241883 ............ 83 00002241888 .......... 187 00002241889 .......... 187 00002241900 ............ 66 00002241901 ............ 66 00002241927 . SEC 3.76 00002241933 .......... 141 00002241976 ............ 81 00002242029 .......... 155 00002242030 .......... 155 00002242055 .......... 153 00002242115 . SEC 3.77 00002242116 . SEC 3.77 00002242117 . SEC 3.77 00002242118 . SEC 3.77 00002242119 ............ 30 00002242146 .......... 150 00002242163 ............ 79 00002242177 ............ 91
00002242178 ............ 91 00002242320 ............ 34 00002242453 .......... 146 00002242454 .......... 146 00002242463 ............ 16 00002242464 ............ 16 00002242465 .......... 166 00002242471 . SEC 3.18 00002242472 ............ 34 00002242481 .......... 112 00002242502 .......... 183 00002242503 ............ 14 00002242518 . SEC 3.74 00002242519 ............ 92 00002242520 ............ 92 00002242521 ............ 93 00002242527 .......... 178 00002242528 .......... 178 00002242538 ............ 54 00002242539 ............ 54 00002242540 ............ 54 00002242541 ............ 54 00002242570 .......... 104 00002242572 . SEC 3.71 00002242573 . SEC 3.71 00002242574 . SEC 3.71 00002242589 .......... 162 00002242652 .............. 3 00002242656 .............. 5 00002242657 .............. 5 00002242680 ............ 27 00002242681 ............ 27 00002242682 ............ 27 00002242683 ............ 27 00002242684 ............ 28 00002242685 ............ 28 00002242686 ............ 28 00002242687 ............ 28 00002242692 ............ 29 00002242697 ............ 28 00002242728 ............ 44 00002242729 ............ 44 00002242730 ............ 44 00002242763 . SEC 3.73 00002242784 ............ 16 00002242794 .......... 162 00002242797 .......... 176 00002242798 .......... 177 00002242814 .......... 125 00002242821 . SEC 3.21
00002242837 .......... 113 00002242838 .......... 113 00002242868 .......... 107 00002242903 .SEC 3.37 00002242907 .......... 185 00002242919 .......... 171 00002242924 ............ 27 00002242925 ............ 27 00002242926 ............ 27 00002242927 ............ 28 00002242928 ............ 28 00002242929 ............ 28 00002242931 .......... 162 00002242940 .......... 146 00002242965 SEC 3A.5 00002242974 .......... 162 00002242984 .......... 176 00002242985 .......... 176 00002242987 .......... 164 00002243005 .......... 159 00002243026 .......... 135 00002243045 .......... 115 00002243045 .SEC 3.93 00002243077 .SEC 3.80 00002243078 .SEC 3.80 00002243086 ............ 99 00002243087 ............ 99 00002243097 ............ 36 00002243098 .......... 130 00002243116 ............ 18 00002243117 ............ 18 00002243127 ............ 37 00002243129 ............ 37 00002243158 .SEC 3.19 00002243180 ............ 35 00002243229 .......... 146 00002243230 .......... 146 00002243231 .......... 186 00002243239 .SEC 3.30 00002243297 .......... 165 00002243312 ............ 73 00002243313 ............ 73 00002243314 ............ 73 00002243324 ............ 33 00002243325 ............ 33 00002243338 ............ 54 00002243339 ............ 54 00002243340 ............ 54 00002243341 ............ 54 00002243350 .............. 9
00002243351 .............. 9 00002243352 ............ 85 00002243353 ............ 85 00002243400 SEC 3.30 00002243401 SEC 3.30 00002243403 SEC 3.30 00002243426 .......... 112 00002243432 ............ 73 00002243446 ............ 84 00002243447 ............ 84 00002243448 ............ 85 00002243450 .......... 153 00002243486 ............ 91 00002243487 ............ 91 00002243506 ............ 38 00002243507 ............ 38 00002243508 ............ 38 00002243518 ............ 45 00002243519 ............ 45 00002243520 ............ 45 00002243521 ............ 45 00002243525 .......... 183 00002243551 ............ 35 00002243552 ............ 35 00002243562 ............ 76 00002243587 ............ 30 00002243588 ............ 42 00002243602 .......... 129 00002243684 SEC 3.56 00002243722 .......... 161 00002243724 .......... 161 00002243763 .......... 116 00002243771 .............. 9 00002243789 ............ 22 00002243796 .......... 149 00002243797 .......... 149 00002243836 ............ 34 00002243878 .......... 185 00002243910 ............ 97 00002243942 ............ 63 00002243986 .............. 9 00002243987 .............. 9 00002243999 .......... 161 00002244000 .......... 161 00002244001 .......... 161 00002244002 .......... 161 00002244016 SEC 3.54 00002244021 ............ 63 00002244022 .......... 146 00002244023 .......... 146

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 238 EFFECTIVE APRIL 1, 2012
00002244107 .......... 100 00002244126 .......... 179 00002244148 . SEC 3.83 00002244149 . SEC 3.84 00002244265 . SEC 3.19 00002244266 . SEC 3.19 00002244291 .......... 156 00002244292 .......... 156 00002244293 .......... 156 00002244304 ............ 84 00002244305 ............ 84 00002244306 ............ 85 00002244324 . SEC 3.21 00002244344 ............ 65 00002244353 .......... 163 00002244393 .............. 5 00002244394 .............. 5 00002244403 ............ 83 00002244404 ............ 83 00002244462 ............ 27 00002244463 ............ 27 00002244464 ............ 27 00002244465 ............ 28 00002244466 ............ 28 00002244467 ............ 28 00002244474 ............ 81 00002244494 .......... 117 00002244495 .......... 117 00002244496 .......... 117 00002244513 ............ 84 00002244514 ............ 84 00002244515 ............ 85 00002244527 ............ 44 00002244528 ............ 44 00002244529 ............ 44 00002244550 .......... 187 00002244551 .......... 187 00002244552 .......... 187 00002244563 ............ 72 00002244612 . SEC 3.87 00002244613 . SEC 3.87 00002244638 ............ 81 00002244641 .............. 7 00002244646 .............. 9 00002244647 .............. 9 00002244680 ............ 71 00002244681 ............ 71 00002244726 .......... 166 00002244727 .......... 166 00002244756 .............. 7
00002244781 ............ 65 00002244782 ............ 65 00002244790 ............ 78 00002244791 ............ 78 00002244792 ............ 78 00002244798 ............ 19 00002244814 .......... 111 00002244815 .......... 111 00002244816 ............ 94 00002244817 ............ 94 00002244818 ............ 94 00002244838 ............ 92 00002244839 ............ 92 00002244840 ............ 93 00002244849 ............ 13 00002244999 .......... 133 00002245058 .......... 148 00002245077 .......... 112 00002245126 ............ 23 00002245127 ............ 23 00002245159 ............ 92 00002245160 ............ 92 00002245161 ............ 93 00002245208 ............ 85 00002245209 ............ 85 00002245210 ............ 85 00002245230 .......... 111 00002245231 .......... 111 00002245232 ............ 13 00002245233 ............ 13 00002245240 . SEC 3.77 00002245246 .......... 127 00002245247 .......... 164 00002245292 ............ 14 00002245293 ............ 14 00002245329 . SEC 3.14 00002245330 .......... 186 00002245385 ............ 22 00002245386 ............ 22 00002245397 .......... 163 00002245400 .......... 157 00002245406 .......... 157 00002245407 .......... 157 00002245408 .......... 157 00002245432 .......... 107 00002245433 .......... 107 00002245456 .......... 151 00002245457 .......... 151 00002245458 .......... 151 00002245522 .......... 175
00002245523 .......... 174 00002245524 .......... 174 00002245531 ............ 30 00002245532 .......... 157 00002245565 .SEC 3.15 00002245618 ............ 27 00002245618 .SEC 2.10 00002245623 .............. 9 00002245643 ............ 14 00002245644 ............ 14 00002245647 SEC 3A.2 00002245648 SEC 3A.3 00002245649 SEC 3A.3 00002245662 .......... 172 00002245663 .......... 150 00002245664 .......... 150 00002245669 ............ 23 00002245676 .......... 161 00002245688 .......... 174 00002245689 .......... 163 00002245777 .SEC 3.90 00002245782 .......... 146 00002245783 .......... 146 00002245821 .......... 134 00002245822 ............ 37 00002245823 ............ 37 00002245824 ............ 92 00002245825 ............ 92 00002245826 ............ 93 00002245828 .......... 185 00002245882 .......... 136 00002245894 .......... 141 00002245898 .SEC 3.21 00002245913 .SEC 3.17 00002245914 ............ 48 00002245915 ............ 48 00002245916 ............ 48 00002245917 ............ 48 00002245918 ............ 54 00002245919 ............ 54 00002245920 ............ 55 00002245921 ............ 55 00002245922 ............ 55 00002245972 .SEC 3.84 00002246010 ............ 49 00002246013 ............ 37 00002246014 ............ 37 00002246016 .......... 123 00002246026 .SEC 3.70 00002246030 .SEC 3.70
00002246056 ............ 90 00002246057 ............ 90 00002246063 .......... 158 00002246082 .......... 186 00002246194 ............ 34 00002246284 .......... 135 00002246314 ............ 84 00002246315 ............ 84 00002246316 ............ 85 00002246354 SEC 3.22 00002246355 SEC 3.22 00002246357 SEC 3.22 00002246358 SEC 3.22 00002246360 SEC 3.22 00002246534 .......... 112 00002246542 ............ 37 00002246543 ............ 37 00002246569 ............ 60 00002246581 ............ 46 00002246582 ............ 39 00002246583 ............ 39 00002246584 ............ 40 00002246585 ............ 40 00002246594 ............ 90 00002246595 ............ 90 00002246596 ............ 10 00002246619 .......... 138 00002246624 ............ 60 00002246691 ............ 17 00002246699 ............ 73 00002246700 ............ 73 00002246701 ............ 73 00002246714 .......... 173 00002246737 ............ 39 00002246793 ............ 22 00002246804 SEC 3A.4 00002246820 .......... 162 00002246821 .......... 162 00002246825 SEC 3A.2 00002246826 SEC 3A.3 00002246827 SEC 3A.3 00002246859 ............ 35 00002246860 ............ 35 00002246893 ............ 55 00002246894 ............ 55 00002246895 ............ 55 00002246896 SEC 3.74 00002246897 ............ 85 00002246898 ............ 85 00002246899 ............ 85

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 239
00002246955 ............ 66 00002246963 ............ 85 00002246967 .......... 161 00002246968 .......... 161 00002246969 .......... 161 00002247008 ............ 38 00002247009 ............ 38 00002247010 ............ 38 00002247011 ............ 39 00002247012 ............ 39 00002247013 ............ 39 00002247014 ............ 40 00002247015 ............ 40 00002247021 .............. 9 00002247022 .......... 153 00002247027 ............ 86 00002247028 ............ 86 00002247029 ............ 86 00002247054 ............ 91 00002247055 ............ 91 00002247056 ............ 37 00002247057 ............ 37 00002247073 . SEC 3.21 00002247074 . SEC 3.21 00002247085 . SEC 3.79 00002247086 . SEC 3.79 00002247087 . SEC 3.79 00002247096 .......... 173 00002247097 .......... 173 00002247098 .......... 173 00002247128 ............ 15 00002247162 ............ 38 00002247163 ............ 38 00002247164 ............ 38 00002247243 ............ 97 00002247244 ............ 98 00002247310 ............ 24 00002247322 .......... 178 00002247323 .......... 186 00002247339 SEC 3A.2 00002247340 SEC 3A.3 00002247341 SEC 3A.3 00002247373 . SEC 3.14 00002247423 .............. 7 00002247437 . SEC 3.31 00002247439 ............ 47 00002247440 ............ 47 00002247461 .......... 134 00002247499 .......... 161 00002247500 .......... 161
00002247521 . SEC 3.37 00002247573 .............. 7 00002247574 .............. 7 00002247585 . SEC 3.83 00002247655 ............ 38 00002247656 ............ 38 00002247657 ............ 38 00002247686 ............ 22 00002247691 .......... 177 00002247692 .......... 176 00002247694 ............ 77 00002247698 ............ 77 00002247699 ............ 77 00002247700 ............ 77 00002247701 ............ 77 00002247704 .......... 103 00002247705 .......... 103 00002247706 .......... 103 00002247749 ............ 14 00002247751 ............ 92 00002247752 ............ 92 00002247802 ............ 58 00002247803 ............ 58 00002247811 ............ 92 00002247812 ............ 92 00002247813 . SEC 3.24 00002247818 .............. 7 00002247819 .............. 7 00002247823 ............ 16 00002247828 ............ 39 00002247830 ............ 39 00002247831 ............ 40 00002247833 ............ 40 00002247856 ............ 38 00002247857 ............ 38 00002247858 ............ 38 00002247876 ............ 49 00002247882 .......... 178 00002247917 ............ 61 00002247918 ............ 61 00002247919 ............ 62 00002247920 .......... 133 00002247922 ............ 14 00002247933 ............ 48 00002247934 ............ 48 00002247935 ............ 48 00002247936 ............ 48 00002247945 ............ 61 00002247946 ............ 61 00002247947 ............ 62
00002247997 .......... 129 00002248008 .......... 165 00002248009 .......... 165 00002248010 ............ 90 00002248011 ............ 90 00002248013 ............ 92 00002248014 ............ 92 00002248034 ............ 97 00002248035 ............ 98 00002248050 ............ 90 00002248051 ............ 90 00002248077 ............ 16 00002248077 .SEC 3.66 00002248103 ............ 39 00002248104 ............ 39 00002248105 ............ 39 00002248106 ............ 40 00002248107 ............ 40 00002248130 .......... 177 00002248138 .............. 9 00002248170 ............ 90 00002248171 ............ 90 00002248182 ............ 38 00002248183 ............ 38 00002248184 ............ 38 00002248206 .......... 171 00002248232 ............ 85 00002248233 ............ 85 00002248234 ............ 85 00002248259 ............ 84 00002248260 ............ 84 00002248261 ............ 85 00002248262 SEC 3A.4 00002248263 SEC 3A.4 00002248296 .SEC 3.92 00002248347 .......... 137 00002248398 .......... 131 00002248437 SEC 3A.2 00002248438 SEC 3A.3 00002248439 SEC 3A.3 00002248440 .SEC 3.79 00002248441 .SEC 3.79 00002248451 ............ 92 00002248452 ............ 92 00002248472 .SEC 3.19 00002248529 .......... 131 00002248538 ............ 96 00002248539 ............ 96 00002248540 ............ 96 00002248557 ............ 92
00002248558 ............ 92 00002248570 .......... 146 00002248571 .......... 146 00002248572 ............ 37 00002248573 ............ 37 00002248639 SEC 3.60 00002248640 SEC 3.60 00002248641 SEC 3.60 00002248642 SEC 3.60 00002248686 .......... 186 00002248728 SEC 3.14 00002248730 SEC 3.14 00002248752 ............ 48 00002248753 ............ 48 00002248754 ............ 48 00002248756 SEC 3A.2 00002248757 SEC 3A.3 00002248758 SEC 3A.3 00002248762 ............ 97 00002248763 ............ 47 00002248764 ............ 47 00002248855 ............ 49 00002248856 .............. 7 00002248857 .............. 7 00002248860 ............ 86 00002248861 ............ 86 00002248862 ............ 87 00002248944 ............ 90 00002248945 ............ 90 00002248993 .......... 115 00002248993 SEC 3.93 00002249324 .......... 108 00002249332 .......... 108 00002249510 .......... 126 00002249669 .......... 187 00002249685 .......... 187 00002249790 SEC 3.64 00002250039 ............ 35 00002250055 .......... 156 00002250144 ............ 39 00002250152 ............ 39 00002250160 ............ 39 00002250179 ............ 40 00002250187 ............ 40 00002250497 ............ 52 00002250500 ............ 52 00002250527 ............ 37 00002250608 ............ 97 00002250896 ............ 82 00002251450 .......... 112

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 240 EFFECTIVE APRIL 1, 2012
00002251469 .......... 112 00002251515 ............ 61 00002251531 ............ 61 00002251574 ............ 61 00002251582 ............ 62 00002251930 .......... 163 00002252007 .......... 101 00002252015 .......... 101 00002252023 .......... 101 00002252031 .......... 102 00002252058 .......... 102 00002252066 .......... 102 00002252112 ............ 90 00002252120 ............ 90 00002252279 ............ 97 00002252309 ............ 48 00002252317 ............ 48 00002252325 ............ 48 00002252333 ............ 48 00002252570 .......... 131 00002252600 ............ 17 00002252716 .......... 132 00002252767 . SEC 3.20 00002253429 . SEC 3.68 00002253631 ............ 63 00002253933 .......... 131 00002254514 ............ 18 00002254522 ............ 18 00002254581 . SEC 3.70 00002254603 . SEC 3.70 00002254638 . SEC 3.70 00002254646 . SEC 3.70 00002254727 ............ 14 00002254778 ............ 92 00002254786 .......... 137 00002255340 .............. 7 00002255529 ............ 91 00002255537 ............ 91 00002255545 ............ 46 00002255553 ............ 47 00002255707 . SEC 3.75 00002255723 . SEC 3.75 00002255758 . SEC 3.75 00002256088 . SEC 3.17 00002256096 ............ 97 00002256118 ............ 97 00002256126 ............ 97 00002256134 ............ 47 00002256142 ............ 84 00002256150 ............ 84
00002256169 ............ 85 00002256177 ............ 47 00002256193 .......... 144 00002256436 .......... 114 00002256436 . SEC 3.82 00002256444 .......... 114 00002256444 . SEC 3.82 00002256460 . SEC 3.91 00002256479 . SEC 3.91 00002256487 . SEC 3.91 00002256495 .......... 187 00002256509 .......... 187 00002256711 .......... 146 00002256738 ............ 53 00002256746 ............ 53 00002256754 ............ 53 00002256762 ............ 53 00002256770 ............ 53 00002256797 ............ 59 00002256800 ............ 59 00002256819 ............ 59 00002257092 ............ 38 00002257106 ............ 38 00002257114 ............ 38 00002257238 .......... 159 00002257572 .......... 112 00002257580 .......... 112 00002257726 .......... 162 00002257734 .......... 162 00002257831 ............ 51 00002257858 ............ 51 00002257890 .......... 114 00002257890 . SEC 3.82 00002257904 .......... 114 00002257904 . SEC 3.82 00002257955 .......... 179 00002257963 .......... 179 00002258056 ............ 30 00002258102 . SEC 3.14 00002258110 . SEC 3.14 00002258129 ............ 80 00002258188 .......... 143 00002258196 .......... 143 00002258331 ............ 13 00002258358 ............ 13 00002258439 .......... 101 00002258447 .......... 101 00002258455 .......... 101 00002258463 .......... 102 00002258471 .......... 102
00002258498 .......... 102 00002258528 ............ 41 00002258560 .......... 160 00002258587 .......... 160 00002258595 .SEC 3.13 00002258692 .......... 138 00002259354 ............ 97 00002259605 ............ 52 00002259613 ............ 52 00002259893 .SEC 3.85 00002260050 ............ 86 00002260069 ............ 86 00002260077 .......... 135 00002260565 .SEC 3.63 00002260867 .......... 148 00002260883 ............ 84 00002260905 ............ 85 00002261081 .......... 156 00002261251 .......... 187 00002261278 .......... 187 00002261634 .............. 7 00002261642 .SEC 3.17 00002261715 .SEC 3.14 00002261723 .......... 159 00002261731 .......... 159 00002261766 .SEC 3.83 00002261782 ............ 50 00002261790 ............ 50 00002261804 ............ 50 00002261839 ............ 83 00002261847 ............ 83 00002261855 ............ 83 00002261863 ............ 83 00002261901 ............ 70 00002261928 ............ 70 00002261936 ............ 70 00002261944 ............ 70 00002261952 ............ 70 00002261960 ............ 70 00002261979 ............ 60 00002261987 ............ 60 00002261995 ............ 60 00002262177 ............ 14 00002262401 ............ 58 00002262428 ............ 58 00002262754 ............ 92 00002262762 ............ 92 00002262983 ............ 80 00002262991 ............ 86 00002263009 ............ 86
00002263017 ............ 87 00002263025 .......... 114 00002263025 SEC 3.82 00002263033 .......... 114 00002263033 SEC 3.82 00002263238 ............ 90 00002263254 ............ 90 00002263351 ............ 86 00002263378 ............ 86 00002263386 ............ 87 00002263866 .......... 186 00002264056 .......... 143 00002264064 .......... 143 00002264188 .......... 101 00002264196 .......... 101 00002264218 .......... 102 00002264226 .......... 102 00002264234 .......... 102 00002264749 .......... 177 00002264951 .......... 187 00002264978 .......... 187 00002264986 .......... 187 00002265273 ............ 27 00002265281 ............ 27 00002265303 ............ 27 00002265311 ............ 27 00002265338 ............ 28 00002265346 ............ 28 00002265494 ............ 85 00002265508 ............ 85 00002265516 ............ 85 00002265524 .......... 143 00002265532 .......... 143 00002265540 ............ 38 00002265826 .............. 7 00002266008 ............ 58 00002266016 ............ 58 00002266350 ............ 56 00002266369 ............ 56 00002266377 ............ 57 00002266385 .......... 177 00002266539 .............. 7 00002266547 .............. 7 00002266660 ............ 46 00002266687 .......... 108 00002266717 SEC 3.41 00002266725 SEC 3.41 00002266733 SEC 3.41 00002267217 .......... 150 00002267233 .......... 148

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 241
00002267470 ............ 47 00002267489 ............ 47 00002267640 .......... 166 00002267837 ............ 87 00002267845 .............. 7 00002267918 .......... 112 00002267926 .......... 112 00002267985 ............ 46 00002267993 ............ 47 00002268027 ............ 48 00002268035 ............ 48 00002268043 ............ 48 00002268051 ............ 48 00002268078 .......... 149 00002268086 .......... 103 00002268094 .......... 103 00002268205 ............ 24 00002268388 .......... 114 00002268388 . SEC 3.82 00002268396 .......... 114 00002268396 . SEC 3.82 00002268914 .......... 114 00002268914 . SEC 3.82 00002268922 .......... 114 00002268922 . SEC 3.82 00002269031 .......... 162 00002269058 .......... 162 00002269090 .......... 136 00002269198 . SEC 3.92 00002269201 . SEC 2.10 00002269252 ............ 39 00002269260 ............ 39 00002269279 ............ 39 00002269287 ............ 40 00002269295 ............ 40 00002269309 .......... 118 00002269325 .......... 118 00002269333 .......... 118 00002269430 ............ 92 00002269449 ............ 92 00002269627 ............ 10 00002270129 . SEC 3.14 00002270609 ............ 90 00002270625 ............ 51 00002270633 ............ 51 00002270641 ............ 82 00002270668 ............ 82 00002270676 ............ 82 00002270811 .......... 179 00002271184 ............ 86
00002271192 ............ 86 00002271206 ............ 87 00002271443 ............ 59 00002271451 ............ 59 00002271478 ............ 59 00002271605 ............ 54 00002271613 ............ 54 00002271621 ............ 55 00002271648 ............ 55 00002271656 ............ 55 00002271761 .......... 143 00002271788 .......... 143 00002271842 .......... 163 00002271931 .......... 112 00002271958 .......... 112 00002272059 . SEC 3.85 00002272083 . SEC 3.80 00002272113 ............ 52 00002272121 ............ 52 00002272695 ............ 22 00002272830 ............ 42 00002272873 .......... 117 00002272903 .......... 159 00002273217 . SEC 3.22 00002273225 . SEC 3.22 00002273373 ............ 52 00002273381 ............ 52 00002273497 .......... 141 00002273500 .......... 141 00002273551 ............ 35 00002273578 . SEC 3.63 00002273586 . SEC 3.63 00002273683 ............ 92 00002273691 ............ 92 00002273705 ............ 93 00002273918 ............ 56 00002273942 ............ 97 00002273969 ............ 89 00002273977 ............ 89 00002273985 ............ 89 00002274086 .......... 126 00002274183 ............ 86 00002274191 ............ 86 00002274205 ............ 86 00002274310 .......... 143 00002274329 .......... 143 00002274388 .............. 7 00002274396 .............. 7 00002274531 .............. 7 00002274728 . SEC 3.37
00002274833 ............ 59 00002274841 ............ 59 00002274868 ............ 59 00002274914 .SEC 3.71 00002274922 .SEC 3.71 00002274930 .SEC 3.71 00002275023 ............ 89 00002275031 ............ 89 00002275058 ............ 89 00002275066 .SEC 3.88 00002275074 ............ 96 00002275082 ............ 96 00002275090 ............ 96 00002275104 ............ 96 00002275279 .SEC 3.14 00002275287 .............. 7 00002275538 ............ 33 00002275546 ............ 33 00002276712 ............ 98 00002276720 ............ 98 00002276739 ............ 98 00002276747 ............ 98 00002276755 ............ 99 00002277263 .SEC 3.80 00002277271 .SEC 3.80 00002277298 .......... 166 00002278251 .......... 138 00002278359 .............. 7 00002278529 .......... 143 00002278537 .......... 143 00002278545 ............ 89 00002278553 ............ 89 00002278561 ............ 89 00002278588 .............. 7 00002278618 .......... 143 00002278626 .......... 143 00002278669 .......... 149 00002278677 ............ 22 00002278685 ............ 22 00002279215 .SEC 3.73 00002279266 .......... 103 00002279363 .......... 156 00002279428 .......... 143 00002279436 .......... 143 00002279460 .......... 163 00002279479 .......... 163 00002279614 ............ 86 00002279630 ............ 86 00002279649 ............ 87 00002279800 .......... 101
00002279819 .......... 102 00002279827 .......... 102 00002279835 .......... 102 00002279983 .......... 172 00002280132 ............ 52 00002280140 ............ 52 00002280191 .......... 185 00002280264 ............ 52 00002280272 ............ 53 00002280396 .......... 103 00002280442 ............ 56 00002280450 ............ 56 00002280469 ............ 57 00002280515 .......... 147 00002280523 .......... 147 00002280833 .......... 146 00002280906 .......... 101 00002280914 .......... 101 00002280922 .......... 101 00002280930 .......... 102 00002280949 .......... 102 00002280957 .......... 102 00002281260 ............ 14 00002281279 ............ 14 00002281392 ............ 44 00002281546 ............ 39 00002281554 ............ 39 00002281562 ............ 39 00002281570 ............ 40 00002281589 ............ 40 00002281708 SEC 2.10 00002281791 ............ 98 00002281805 ............ 98 00002281813 ............ 98 00002281821 ............ 98 00002281848 ............ 99 00002282097 .. SEC 3.6 00002282119 .......... 101 00002282127 .......... 101 00002282135 .......... 101 00002282143 .......... 102 00002282151 .......... 102 00002282178 .......... 102 00002282224 ............ 16 00002282240 .......... 101 00002282259 .......... 101 00002282267 .......... 101 00002282275 .......... 102 00002282283 .......... 102 00002282291 .......... 102

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 242 EFFECTIVE APRIL 1, 2012
00002282445 .......... 112 00002282585 .......... 101 00002282593 .......... 101 00002282607 .......... 101 00002282615 .......... 102 00002282623 .......... 102 00002282631 .......... 102 00002282690 .......... 101 00002282852 ............ 92 00002282860 ............ 92 00002282941 . SEC 3.38 00002282968 . SEC 3.39 00002282976 . SEC 3.39 00002282984 . SEC 3.39 00002283131 ............ 62 00002283158 ............ 62 00002283166 ............ 62 00002283174 ............ 62 00002283182 ............ 62 00002283395 . SEC 3.55 00002283409 . SEC 3.55 00002283417 . SEC 3.55 00002283778 ............ 56 00002283786 ............ 56 00002283794 ............ 57 00002283964 .......... 187 00002283972 .......... 187 00002284006 . SEC 3.14 00002284030 .......... 166 00002284049 .......... 166 00002284065 ............ 52 00002284073 ............ 52 00002284235 ............ 99 00002284243 ............ 99 00002284251 ............ 99 00002284278 .......... 100 00002284286 .......... 100 00002284383 ............ 52 00002284391 ............ 52 00002284421 ............ 38 00002284448 ............ 38 00002284456 ............ 38 00002284677 SEC 3A.4 00002284685 SEC 3A.4 00002284707 SEC 3A.4 00002284715 SEC 3A.4 00002284723 ............ 39 00002284731 ............ 39 00002284758 ............ 39 00002284766 ............ 40
00002284774 ............ 40 00002284987 ............ 57 00002285061 ............ 59 00002285088 ............ 59 00002285096 ............ 59 00002285118 ............ 59 00002285126 ............ 59 00002285134 ............ 59 00002285169 ............ 49 00002285177 ............ 49 00002285215 ............ 56 00002285223 ............ 57 00002285398 . SEC 3.58 00002285487 .......... 148 00002285606 .......... 155 00002285614 .......... 155 00002285622 ............ 90 00002285630 ............ 90 00002285649 SEC 3A.4 00002285657 ............ 96 00002285665 ............ 96 00002285819 ............ 84 00002285827 ............ 84 00002285835 ............ 85 00002285924 ............ 86 00002285932 ............ 86 00002285940 ............ 86 00002285959 ............ 16 00002285967 ............ 16 00002285975 ............ 16 00002286068 ............ 91 00002286076 ............ 91 00002286092 ............ 35 00002286246 ............ 46 00002286254 ............ 46 00002286262 ............ 46 00002286335 . SEC 3.14 00002286386 . SEC 2.13 00002286521 .......... 114 00002286521 . SEC 3.82 00002286548 .......... 114 00002286548 . SEC 3.82 00002286556 ............ 16 00002286564 ............ 16 00002286572 ............ 16 00002286629 ............ 97 00002286823 .......... 114 00002286823 . SEC 3.82 00002286831 .......... 114 00002286831 . SEC 3.82
00002287021 ............ 25 00002287048 ............ 25 00002287064 ............ 25 00002287072 .......... 164 00002287226 ............ 12 00002287234 ............ 12 00002287390 ............ 92 00002287404 ............ 92 00002287412 ............ 93 00002287420 .SEC 3.23 00002287439 .SEC 3.23 00002287447 .SEC 3.23 00002287498 ............ 27 00002287730 .......... 166 00002287749 .......... 166 00002287765 ............ 86 00002287773 ............ 86 00002287781 ............ 87 00002288044 ............ 35 00002288052 ............ 35 00002288087 .SEC 3.14 00002288109 .SEC 3.14 00002288184 .......... 143 00002288192 .......... 143 00002288346 ............ 36 00002288354 ............ 36 00002288362 ............ 36 00002288370 ............ 36 00002288680 .SEC 3.29 00002289083 ............ 35 00002289091 ............ 35 00002289199 ............ 59 00002289202 ............ 59 00002289229 ............ 59 00002289504 ............ 66 00002290111 .......... 118 00002290146 .......... 118 00002290154 .......... 118 00002290332 ............ 56 00002290340 ............ 56 00002291037 ............ 54 00002291045 ............ 54 00002291053 ............ 55 00002291061 ............ 55 00002291088 ............ 55 00002291134 ............ 56 00002291142 ............ 56 00002291150 ............ 57 00002291177 .SEC 3.90 00002291185 .SEC 3.90
00002291398 ............ 61 00002291401 ............ 61 00002291428 ............ 61 00002291436 ............ 62 00002291789 .......... 103 00002291797 .......... 103 00002291878 ............ 57 00002291886 ............ 57 00002291894 ............ 57 00002291908 ............ 58 00002291967 .......... 143 00002292173 ............ 34 00002292203 ............ 59 00002292211 ............ 59 00002292238 ............ 59 00002292270 .............. 5 00002292289 .............. 5 00002292378 .......... 118 00002292394 .......... 118 00002292408 .......... 118 00002292866 .............. 5 00002292874 .............. 5 00002292882 .............. 5 00002292920 .......... 148 00002292998 .............. 4 00002293005 .............. 4 00002293161 SEC 3.20 00002293218 ............ 90 00002293226 ............ 90 00002293528 .............. 4 00002293536 .............. 4 00002293579 .............. 4 00002293749 ............ 92 00002293811 .......... 147 00002293838 .......... 147 00002293943 .............. 4 00002293951 .............. 4 00002294230 ............ 59 00002294249 ............ 59 00002294257 ............ 59 00002294265 ............ 44 00002294273 ............ 14 00002294338 .......... 163 00002294346 .......... 163 00002294419 ............ 12 00002294427 ............ 12 00002294524 ............ 58 00002294532 ............ 58 00002294702 ............ 73 00002294710 ............ 73

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 243
00002294885 ............ 44 00002295121 ............ 44 00002295148 ............ 52 00002295261 ............ 36 00002295288 ............ 36 00002295296 ............ 36 00002295318 ............ 36 00002295369 ............ 61 00002295415 .......... 148 00002295482 ............ 61 00002295490 ............ 61 00002295504 ............ 61 00002295512 ............ 62 00002295695 ............ 81 00002295709 ............ 81 00002295822 ............ 17 00002295881 .......... 125 00002295946 .......... 159 00002295954 .......... 159 00002296055 .......... 136 00002296101 ............ 86 00002296128 ............ 86 00002296136 ............ 86 00002296152 ............ 90 00002296349 .......... 143 00002296357 .......... 143 00002296438 .......... 148 00002296446 .......... 148 00002296527 .......... 137 00002296551 ............ 99 00002296578 ............ 99 00002296594 .......... 100 00002296608 .......... 100 00002296616 .......... 112 00002296632 .......... 149 00002296640 .......... 149 00002296810 .......... 139 00002297205 .............. 3 00002297213 .............. 3 00002297302 .......... 118 00002297329 .......... 118 00002297337 .......... 118 00002297485 ............ 52 00002297493 ............ 52 00002297736 ............ 60 00002297744 ............ 60 00002297752 ............ 60 00002297795 .......... 164 00002297809 .......... 171 00002297841 ............ 65
00002297868 .......... 143 00002297876 .......... 143 00002297906 . SEC 3.71 00002297914 . SEC 3.71 00002297922 . SEC 3.71 00002298074 .......... 149 00002298082 .......... 149 00002298279 . SEC 3.71 00002298287 . SEC 3.71 00002298295 . SEC 3.71 00002298309 . SEC 3.91 00002298376 . SEC 3.74 00002298384 . SEC 3.74 00002298392 . SEC 3.74 00002298457 ............ 17 00002298538 .......... 159 00002298546 .......... 159 00002298570 ............ 44 00002298597 .......... 103 00002298600 .......... 103 00002298619 .......... 103 00002298627 .......... 103 00002298635 SEC 3A.4 00002298643 SEC 3A.4 00002298651 SEC 3A.4 00002298791 .......... 144 00002298813 .......... 144 00002299437 . SEC 3.60 00002299445 . SEC 3.60 00002299453 . SEC 3.60 00002299585 .......... 148 00002299615 .......... 138 00002299623 . SEC 3.72 00002299631 . SEC 3.72 00002299658 . SEC 3.72 00002299712 . SEC 3.14 00002299879 ............ 59 00002299887 ............ 59 00002299895 ............ 59 00002299933 ............ 57 00002299941 ............ 57 00002299968 ............ 57 00002299976 ............ 58 00002300036 ............ 57 00002300044 ............ 57 00002300052 ............ 57 00002300060 ............ 58 00002300079 ............ 57 00002300087 ............ 57 00002300095 ............ 57
00002300109 ............ 58 00002300222 ............ 58 00002300230 ............ 58 00002300486 .......... 148 00002300680 ............ 57 00002301083 .......... 148 00002301148 ............ 61 00002301156 ............ 61 00002301164 ............ 61 00002301172 ............ 62 00002301288 ............ 42 00002301407 .SEC 3.18 00002301423 .SEC 3.71 00002301431 .SEC 3.71 00002301458 .SEC 3.71 00002301482 ............ 88 00002301490 ............ 88 00002301768 ............ 60 00002301776 ............ 60 00002301784 ............ 60 00002302055 ............ 49 00002302136 ............ 60 00002302144 ............ 60 00002302152 ............ 60 00002302179 .............. 4 00002302187 .............. 4 00002302209 .SEC 3.74 00002302365 ............ 60 00002302373 ............ 60 00002302381 ............ 60 00002302616 ............ 70 00002302624 ............ 70 00002302632 ............ 47 00002302640 ............ 47 00002302675 ............ 36 00002302683 ............ 36 00002302691 ............ 36 00002302713 ............ 36 00002302764 ............ 78 00002302772 ............ 78 00002302780 ............ 78 00002302799 ............ 78 00002302802 ............ 78 00002302861 .SEC 3.71 00002302888 .SEC 3.71 00002302896 .SEC 3.71 00002302918 ............ 47 00002302926 ............ 47 00002302942 .SEC 3.71 00002302950 .SEC 3.71
00002302977 SEC 3.71 00002303027 SEC 3.20 00002303116 ............ 98 00002303124 SEC 3.71 00002303132 SEC 3.71 00002303140 SEC 3.71 00002303159 ............ 98 00002303167 ............ 98 00002303175 ............ 98 00002303183 ............ 99 00002303191 ............ 99 00002303205 ............ 99 00002303396 ............ 49 00002303418 ............ 49 00002303426 .............. 4 00002303434 .............. 4 00002303442 SEC 3.71 00002303450 SEC 3.71 00002303469 SEC 3.71 00002303647 ............ 46 00002303655 .......... 101 00002303663 .......... 101 00002303728 SEC 3A.2 00002303736 SEC 3A.3 00002303744 SEC 3A.3 00002304163 .......... 185 00002304317 ............ 89 00002304325 ............ 89 00002304333 ............ 89 00002304368 .......... 166 00002304376 .......... 166 00002304678 SEC 3.15 00002304686 ............ 90 00002304694 ............ 90 00002305003 ............ 97 00002305011 ............ 98 00002305046 .......... 148 00002305259 .......... 143 00002305267 .......... 143 00002305429 .......... 135 00002305585 SEC 3A.4 00002305933 .......... 117 00002305941 .......... 117 00002305968 .......... 117 00002305984 SEC 3.77 00002305992 SEC 3.77 00002306018 SEC 3.77 00002306026 SEC 3.77 00002306034 SEC 3.77 00002306042 SEC 3.77

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 244 EFFECTIVE APRIL 1, 2012
00002306050 . SEC 3.77 00002306069 . SEC 3.77 00002306212 .......... 143 00002306220 .......... 143 00002306239 ............ 90 00002306247 ............ 90 00002306905 . SEC 3.40 00002307669 . SEC 3.71 00002307677 . SEC 3.71 00002307723 . SEC 3.71 00002307804 ............ 99 00002307812 ............ 99 00002307839 .......... 100 00002307847 .......... 100 00002307871 .......... 148 00002307898 ............ 80 00002308444 . SEC 3.72 00002308452 . SEC 3.72 00002308460 . SEC 3.72 00002308894 .......... 142 00002308908 ............ 66 00002308916 ............ 66 00002308932 .............. 3 00002308959 .............. 3 00002308967 .............. 3 00002309521 .......... 174 00002309548 .......... 174 00002309866 .......... 148 00002310112 . SEC 3.40 00002310260 .......... 148 00002310279 ............ 89 00002310287 ............ 89 00002310295 ............ 89 00002310317 ............ 89 00002310325 ............ 89 00002310333 ............ 89 00002310341 ............ 98 00002310368 ............ 98 00002310376 ............ 98 00002310384 ............ 98 00002310392 ............ 99 00002310422 .......... 135 00002310503 ............ 61 00002310511 ............ 61 00002310538 ............ 61 00002310546 ............ 62 00002310805 .......... 149 00002310813 .......... 149 00002310899 ............ 36 00002310902 ............ 36
00002310910 ............ 36 00002310929 ............ 36 00002311283 . SEC 3.77 00002311291 . SEC 3.77 00002311305 . SEC 3.77 00002311313 . SEC 3.77 00002311658 ............ 63 00002311925 . SEC 3.38 00002312085 ............ 86 00002312247 .......... 143 00002312255 .......... 143 00002312298 . SEC 3.73 00002313405 ............ 90 00002313413 ............ 90 00002313421 ............ 96 00002313448 ............ 36 00002313456 ............ 36 00002313464 ............ 36 00002313472 ............ 36 00002313685 .......... 143 00002313693 .......... 143 00002313707 ............ 36 00002313715 ............ 36 00002313723 ............ 36 00002313731 ............ 57 00002313758 ............ 36 00002313901 ............ 99 00002313928 ............ 99 00002313936 .......... 100 00002313944 .......... 100 00002313960 .......... 115 00002313960 . SEC 3.93 00002313979 SEC 3A.4 00002313987 SEC 3A.4 00002313995 ............ 99 00002314002 ............ 99 00002314010 .......... 100 00002314029 .......... 100 00002314037 .......... 118 00002314053 .......... 118 00002314061 .......... 119 00002314088 .......... 119 00002314177 .......... 149 00002314185 .......... 149 00002314282 . SEC 3.15 00002314290 .......... 113 00002314290 . SEC 3.60 00002314304 .......... 113 00002314304 . SEC 3.60 00002314630 . SEC 3.38
00002314649 .SEC 3.39 00002314657 .SEC 3.39 00002314665 .SEC 3.39 00002314940 .SEC 3.15 00002315157 .............. 7 00002315165 .............. 7 00002315262 .......... 118 00002315289 .......... 118 00002315297 .......... 118 00002315424 SEC 3A.4 00002315432 SEC 3A.4 00002315440 SEC 3A.4 00002315645 ............ 86 00002315653 ............ 86 00002315661 ............ 87 00002315866 .SEC 3.15 00002315971 ............ 63 00002315998 ............ 63 00002316005 ............ 64 00002316013 ............ 64 00002316021 ............ 64 00002316048 ............ 64 00002316080 ............ 99 00002316099 ............ 99 00002316110 .......... 100 00002316129 .......... 100 00002316307 .......... 136 00002316390 ............ 63 00002316404 ............ 63 00002316412 ............ 64 00002316846 .......... 118 00002316854 .......... 118 00002316862 .......... 119 00002316870 .......... 119 00002316943 .SEC 3.41 00002316951 .SEC 3.41 00002316978 .SEC 3.41 00002316986 ............ 30 00002317060 ............ 63 00002317079 ............ 63 00002317087 ............ 64 00002317192 .......... 158 00002317206 .......... 158 00002317427 SEC 3A.2 00002317435 SEC 3A.3 00002317443 SEC 3A.3 00002317451 ............ 38 00002317478 ............ 38 00002317486 ............ 38 00002318008 .......... 137
00002318008 SEC 2.10 00002318261 SEC 2.10 00002318660 ............ 42 00002318679 ............ 42 00002318709 ............ 65 00002319012 .......... 179 00002319055 ............ 84 00002319063 ............ 84 00002319071 ............ 85 00002319403 ............ 76 00002319411 ............ 76 00002319438 ............ 76 00002319446 ............ 76 00002319616 ............ 42 00002319624 ............ 42 00002319632 ............ 42 00002319861 SEC 3.74 00002319977 ............ 80 00002319985 ............ 80 00002319993 ............ 80 00002320134 ............ 14 00002320312 .......... 108 00002320525 .......... 138 00002320673 SEC 3.89 00002320851 .......... 148 00002321149 ............ 53 00002321203 ............ 84 00002321211 ............ 84 00002321238 ............ 85 00002321343 ............ 99 00002321351 ............ 99 00002321475 .......... 164 00002321483 .......... 164 00002321491 .......... 164 00002321653 ............ 60 00002321858 ............ 52 00002321866 ............ 52 00002322250 .......... 166 00002322285 SEC 3.29 00002322323 .......... 113 00002322323 SEC 3.60 00002322374 ............ 97 00002322382 ............ 97 00002322390 ............ 97 00002322404 ............ 97 00002322412 ............ 97 00002322455 ............ 97 00002322579 SEC 3.40 00002323192 ............ 80 00002323206 ............ 80
ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 245
00002323214 ............ 80 00002324032 .......... 185 00002324199 .......... 186 00002324229 .......... 115 00002324229 . SEC 3.93 00002324563 . SEC 3.77 00002324571 . SEC 3.77 00002324598 . SEC 3.77 00002324601 . SEC 3.77 00002324628 ............ 80 00002324768 .......... 115 00002324768 . SEC 3.93 00002324776 . SEC 3.45 00002324784 . SEC 3.45 00002324946 ............ 36 00002324954 ............ 36 00002324962 ............ 36 00002324970 ............ 36 00002324997 .......... 137 00002325063 . SEC 3.80 00002325071 . SEC 3.80 00002325373 ............ 96 00002325462 .......... 161 00002325659 ............ 98 00002325667 ............ 98 00002325675 ............ 98 00002325683 ............ 98 00002325691 ............ 99 00002325942 SEC 3A.4 00002326477 . SEC 3.71 00002326485 . SEC 3.71 00002326493 . SEC 3.71 00002326590 .......... 118 00002326612 .......... 118 00002326620 .......... 119 00002326639 .......... 119 00002326760 ............ 52 00002326779 ............ 52 00002326787 ............ 52 00002326965 ............ 63 00002326973 ............ 63 00002327112 . SEC 3.38 00002327120 . SEC 3.38 00002327147 . SEC 3.39 00002327155 . SEC 3.39 00002327163 . SEC 3.39 00002327295 . SEC 3.74 00002327562 ............ 99 00002327570 ............ 99 00002327775 ............ 99
00002327783 ............ 99 00002328070 ............ 63 00002328089 ............ 63 00002328100 ............ 64 00002328305 .......... 101 00002328313 .......... 101 00002328321 .......... 101 00002328348 .......... 102 00002328364 .......... 102 00002328372 .......... 102 00002328461 ............ 63 00002328488 ............ 63 00002328496 ............ 64 00002328518 ............ 64 00002328526 ............ 64 00002328534 ............ 64 00002328593 .......... 129 00002328593 . SEC 3.59 00002329131 ............ 39 00002329158 ............ 39 00002329166 ............ 39 00002329174 ............ 40 00002329182 ............ 40 00002329204 .............. 4 00002329425 .......... 148 00002329433 .......... 148 00002329840 . SEC 3.17 00002330105 . SEC 3.38 00002330113 . SEC 3.38 00002330121 . SEC 3.39 00002330148 . SEC 3.39 00002330156 . SEC 3.39 00002330385 .......... 129 00002330393 .......... 129 00002330393 . SEC 3.59 00002330415 ............ 99 00002330423 ............ 99 00002330458 .......... 100 00002330466 .......... 100 00002330512 ............ 64 00002330520 ............ 64 00002330539 ............ 64 00002330881 .............. 7 00002330911 . SEC 3.17 00002330954 ............ 38 00002330962 ............ 38 00002330970 ............ 38 00002331004 ............ 58 00002331012 ............ 58 00002331020 ............ 39
00002331039 ............ 39 00002331047 ............ 39 00002331055 ............ 40 00002331063 ............ 40 00002331071 ............ 52 00002331098 ............ 52 00002331101 ............ 61 00002331128 ............ 61 00002331136 ............ 61 00002331144 ............ 62 00002331284 ............ 52 00002331292 ............ 52 00002331551 .......... 125 00002331624 .......... 137 00002331683 ............ 89 00002331691 ............ 89 00002331705 ............ 89 00002331748 ............ 17 00002331780 ............ 44 00002331934 ............ 52 00002331942 ............ 52 00002331950 ............ 90 00002331969 ............ 39 00002331977 ............ 90 00002331985 ............ 39 00002331993 ............ 39 00002332000 ............ 40 00002332019 ............ 40 00002332027 .............. 4 00002332035 .............. 4 00002332043 .............. 4 00002332051 .......... 101 00002332078 .......... 101 00002332086 .......... 101 00002332094 .......... 102 00002332108 .......... 102 00002332116 .......... 102 00002332132 SEC 3A.2 00002332140 SEC 3A.3 00002332159 SEC 3A.3 00002332167 ............ 59 00002332175 ............ 59 00002332183 ............ 59 00002332191 ............ 38 00002332205 ............ 38 00002332213 ............ 38 00002332299 ............ 61 00002332302 ............ 61 00002332310 ............ 61 00002332329 ............ 62
00002332361 .......... 118 00002332388 .............. 7 00002332396 .............. 7 00002332426 .......... 118 00002332434 .......... 119 00002332442 .......... 119 00002332566 ............ 58 00002332574 ............ 58 00002332582 ............ 84 00002332590 ............ 84 00002332604 ............ 85 00002332809 SEC 3.77 00002332817 SEC 3.77 00002332825 SEC 3.77 00002332833 SEC 3.77 00002332922 ............ 63 00002332957 ............ 63 00002333554 SEC 3.79 00002333619 .......... 165 00002333627 .......... 165 00002335700 ............ 34 00002335719 ............ 34 00002335727 ............ 34 00002336480 .......... 146 00002336502 .......... 146 00002336715 SEC 3.77 00002336723 SEC 3.77 00002336731 SEC 3.77 00002336758 SEC 3.77 00002337428 ............ 64 00002337436 ............ 64 00002337444 ............ 64 00002337495 ............ 65 00002337509 ............ 65 00002337517 ............ 66 00002337746 .......... 118 00002337762 .......... 118 00002337770 .......... 119 00002337800 .......... 119 00002337800 SEC 2.10 00002337827 .......... 117 00002337835 .......... 117 00002337878 ............ 98 00002337886 ............ 98 00002337894 ............ 98 00002337908 ............ 98 00002337916 ............ 99 00002339439 SEC 3.41 00002339447 SEC 3.41 00002339455 SEC 3.41

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 246 EFFECTIVE APRIL 1, 2012
00002339587 . SEC 3.71 00002339595 . SEC 3.71 00002340208 ............ 44 00002341379 . SEC 3.38 00002341387 . SEC 3.38 00002341395 . SEC 3.39 00002341409 . SEC 3.39 00002341417 . SEC 3.39 00002342138 ............ 62 00002342146 ............ 62 00002342154 ............ 62 00002342162 ............ 62 00002342170 ............ 62 00002342545 .......... 115 00002342545 . SEC 3.93 00002342855 ............ 12 00002342863 ............ 12 00002343002 .......... 185 00002343010 ............ 85 00002343029 ............ 85 00002343037 ............ 85 00002343045 ............ 30 00002343282 ............ 72 00002343541 . SEC 3.23 00002344025 ............ 27 00002344033 ............ 27 00002344041 ............ 27 00002344068 ............ 27 00002344076 ............ 28 00002344084 ............ 28 00002344114 ............ 28 00002344122 .......... 112 00002344351 .......... 138 00002344823 .............. 5 00002344831 .............. 5 00002345579 .......... 149 00002345587 .......... 149 00002345803 ............ 86 00002345838 ............ 86 00002345846 ............ 87 00002347245 .............. 4 00002347253 .............. 4 00002347261 .............. 4 00002347288 .............. 4 00002347296 ............ 63 00002347318 ............ 63 00002347326 ............ 64 00002347512 ............ 48 00002347520 ............ 48 00002347555 ............ 48
00002347571 ............ 48 00002348004 . SEC 3.20 00002348500 . SEC 3.40 00002348691 .......... 148 00002348705 ............ 36 00002348713 ............ 36 00002348721 ............ 36 00002348748 ............ 36 00002348772 ............ 93 00002348780 ............ 93 00002348799 ............ 93 00002349167 ............ 53 00002349191 .......... 109 00002349205 .......... 109 00002350092 . SEC 3.87 00002350106 . SEC 3.87 00002350114 . SEC 3.87 00002350122 . SEC 3.80 00002350130 . SEC 3.80 00002350149 . SEC 3.80 00002350238 .......... 181 00002350297 ............ 36 00002350319 ............ 36 00002350327 ............ 36 00002350335 ............ 36 00002350394 ............ 49 00002350408 ............ 49 00002350440 .......... 149 00002350459 .......... 165 00002350467 .......... 165 00002350475 ............ 45 00002350483 ............ 45 00002350491 ............ 45 00002350505 ............ 45 00002350750 ............ 72 00002350769 ............ 73 00002350777 ............ 73 00002350785 ............ 73 00002350793 ............ 73 00002350807 ............ 73 00002350815 ............ 78 00002350890 ............ 78 00002350912 ............ 78 00002350920 ............ 78 00002350947 ............ 78 00002350963 ............ 56 00002350971 ............ 56 00002350998 ............ 57 00002351013 ............ 74 00002351021 ............ 74
00002351072 .......... 110 00002351080 .......... 110 00002351099 .......... 110 00002351102 .......... 145 00002351110 .......... 145 00002351234 ............ 11 00002351242 ............ 11 00002351420 ............ 41 00002351439 ............ 41 00002351447 ............ 41 00002351463 .......... 150 00002351536 .SEC 3.20 00002351579 ............ 17 00002351668 .......... 187 00002351676 .......... 187 00002352230 ............ 57 00002352249 ............ 57 00002352257 ............ 57 00002352265 ............ 58 00002352338 .......... 118 00002352346 .......... 118 00002352354 .......... 119 00002352362 .......... 119 00002352397 ............ 70 00002352400 ............ 70 00002352648 ............ 28 00002352656 ............ 28 00002352664 ............ 28 00002352672 ............ 28 00002352680 ............ 29 00002352710 .............. 8 00002352729 .............. 8 00002352745 .............. 9 00002352753 .............. 9 00002352761 .............. 9 00002352788 .............. 9 00002352923 ............ 58 00002352931 ............ 58 00002352966 .SEC 3.14 00002352974 ............ 99 00002352982 ............ 99 00002353016 .......... 146 00002353024 .......... 146 00002353040 .......... 118 00002353059 .......... 118 00002353067 .......... 119 00002353075 .......... 119 00002353121 ............ 14 00002353164 ............ 99 00002353172 ............ 99
00002353199 .......... 100 00002353202 .......... 100 00002353210 .......... 186 00002353229 ............ 37 00002353237 ............ 37 00002353245 ............ 84 00002353253 ............ 84 00002353261 ............ 85 00002353318 SEC 3A.2 00002353326 SEC 3A.3 00002353334 SEC 3A.3 00002353342 ............ 86 00002353350 ............ 86 00002353369 ............ 86 00002353377 .......... 162 00002353385 .......... 162 00002353520 ............ 92 00002353539 ............ 92 00002353547 ............ 93 00002353660 ............ 90 00002353679 ............ 90 00002353687 SEC 3.74 00002353830 .......... 147 00002353849 .......... 147 00002354187 ............ 49 00002354195 ............ 49 00002354217 SEC 3.64 00002354225 SEC 3.64 00002354233 SEC 3.64 00002354241 SEC 3.64 00002354462 SEC 3.40 00002354705 ............ 17 00002354713 ............ 89 00002354721 ............ 89 00002354748 ............ 89 00002354926 .......... 164 00002354934 .......... 164 00002354942 .......... 164 00002354977 .......... 129 00002354985 .......... 129 00002354985 SEC 3.59 00002355043 SEC 3.40 00002355272 ............ 90 00002355280 ............ 90 00002355507 .......... 129 00002355515 .......... 129 00002355515 SEC 3.59 00002355523 .......... 129 00002355523 SEC 3.59 00002355663 .......... 164

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment.
EFFECTIVE APRIL 1, 2012 247
00002355671 .......... 164 00002355698 .......... 164 00002355752 ............ 54 00002355760 ............ 54 00002355779 ............ 54 00002355787 ............ 54 00002356058 . SEC 3.40 00002356422 .......... 164 00002356511 .......... 149 00002356538 .......... 149 00002356546 ............ 38 00002356554 ............ 38 00002356562 ............ 38 00002356570 ............ 35 00002356589 ............ 35 00002356651 ............ 65 00002356678 ............ 65 00002356686 ............ 66 00002356694 ............ 66 00002356708 ............ 66 00002356716 ............ 66 00002356724 ............ 66 00002356732 ............ 66 00002356759 ............ 65 00002356767 ............ 65 00002356775 ............ 66 00002356813 ............ 49 00002356821 ............ 49 00002356848 ............ 49 00002356856 ............ 86 00002356864 ............ 86 00002356872 ............ 87 00002356880 .......... 101 00002356899 .......... 101 00002356902 .......... 101 00002356910 .......... 102 00002356929 .......... 102 00002356937 .......... 102 00002356996 ............ 66 00002357003 ............ 66 00002357011 ............ 66 00002357038 ............ 66 00002357046 ............ 66 00002357070 ............ 14 00002357194 ............ 52 00002357208 ............ 52 00002357224 . SEC 3.40 00002357380 . SEC 3.38 00002357399 ............ 64 00002357402 ............ 64
00002357410 ............ 64 00002357453 .......... 164 00002357461 .......... 164 00002357488 .......... 164 00002357615 . SEC 3.54 00002357623 . SEC 3.54 00002357631 . SEC 3.55 00002357658 . SEC 3.55 00002357682 .......... 147 00002357690 .......... 147 00002357712 ............ 52 00002357720 ............ 52 00002357984 . SEC 3.74 00002358158 ............ 29 00002358166 ............ 29 00002358174 ............ 30 00002358182 ............ 30 00002358611 .......... 129 00002358921 . SEC 3.73 00002359316 . SEC 3.20 00002359502 ............ 76 00002359510 ............ 76 00002359529 .......... 101 00002359537 .......... 101 00002359545 .......... 101 00002359553 .......... 102 00002359561 .......... 102 00002359588 .......... 102 00002359790 .......... 101 00002359804 .......... 101 00002359812 .......... 101 00002359820 .......... 102 00002359839 .......... 102 00002359847 .......... 102 00002360020 ............ 89 00002360039 ............ 89 00002360047 ............ 89 00002360616 ............ 99 00002360624 ............ 99 00002360969 ............ 46 00002361027 SEC 3A.4 00002361035 SEC 3A.4 00002361361 ............ 80 00002361469 ............ 84 00002361485 ............ 84 00002361493 ............ 85 00002361531 ............ 59 00002361558 ............ 59 00002361566 ............ 59 00002361698 .......... 114
00002361698 .SEC 3.82 00002361892 ............ 99 00002362406 ............ 44 00002362651 ............ 52 00002362678 ............ 52 00002362848 .............. 4 00002362856 .............. 4 00002362864 .............. 4 00002362872 .............. 4 00002362880 ............ 60 00002362899 ............ 60 00002362902 ............ 60 00002362937 ............ 97 00002362945 ............ 60 00002362953 ............ 60 00002362961 ............ 60 00002362988 .......... 115 00002362988 .SEC 3.93 00002362996 .......... 115 00002362996 .SEC 3.93 00002363100 ............ 65 00002363119 ............ 65 00002363208 ............ 64 00002363216 ............ 64 00002363224 ............ 64 00002363232 .SEC 3.71 00002363240 .SEC 3.71 00002363259 .SEC 3.71 00002363267 ............ 61 00002363275 ............ 61 00002363283 ............ 61 00002363291 ............ 62 00002363305 .......... 118 00002363321 .......... 118 00002363348 .......... 118 00002363364 .............. 7 00002363372 .............. 7 00002363380 .............. 7 00002363399 ............ 96 00002363402 ............ 96 00002363429 .......... 148 00002363453 ............ 57 00002363461 ............ 57 00002363488 ............ 57 00002363496 ............ 58 00002363518 .......... 164 00002363534 .......... 112 00002363542 .......... 112 00002363674 ............ 51 00002363682 ............ 51
00002363704 .......... 165 00002363712 .......... 165 00002363763 ............ 91 00002363771 ............ 91 00002363798 ............ 46 00002363801 ............ 46 00002363828 ............ 46 00002363887 ............ 47 00002363895 ............ 47 00002363968 .......... 126 00002363976 .......... 126 00002364239 ............ 37 00002364247 ............ 37 00002364263 ............ 34 00002364271 .......... 149 00002364301 ............ 95 00002364328 ............ 95 00002364336 ............ 34 00002364344 .......... 103 00002364409 ............ 35 00002364506 .......... 162 00002364514 .......... 162 00002364530 ............ 91 00002364573 ............ 41 00002364581 ............ 41 00002364603 ............ 41 00002364719 ............ 13 00002364727 ............ 13 00002364816 SEC 3.74 00002364824 ............ 49 00002364832 ............ 49 00002364840 ............ 49 00002364859 ............ 49 00002364913 ............ 48 00002364921 ............ 48 00002364948 ............ 48 00002364956 ............ 48 00002365154 .............. 3 00002365359 ............ 63 00002365367 ............ 63 00002365383 SEC 3.40 00002365529 SEC 3.71 00002365537 SEC 3.71 00002365820 ............ 73 00002365839 ............ 73 00002365847 ............ 73 00002365855 ............ 73 00002365863 ............ 73 00002366231 ............ 44 00002366258 .......... 114

ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST INDEX 2 - NUMERICAL LIST BY DRUG IDENTIFICATION NUMBER
DRUG IDENTIFICATION NUMBERS OF PHARMACEUTICAL PRODUCTS DIN Page DIN Page DIN Page DIN Page
The DBL is not a prescribing or a diagnostic tool. Prescribers should refer to drug monographs and utilize professional judgment. 248 EFFECTIVE APRIL 1, 2012
00002366258 . SEC 3.82 00002366266 .......... 114 00002366266 . SEC 3.82 00002366304 ............ 10 00002366398 .............. 7 00002366665 ............ 70 00002366673 ............ 70 00002366681 ............ 70 00002366703 ............ 70 00002367068 ............ 66 00002367076 ............ 66 00002367084 ............ 66 00002367092 ............ 66 00002367106 ............ 66 00002367122 ............ 65 00002367130 ............ 65 00002367149 ............ 66 00002367157 .......... 177 00002367173 .......... 101 00002367181 .......... 101 00002367203 .......... 101 00002367211 .......... 102 00002367238 .......... 102 00002367246 .......... 102 00002367378 .......... 146 00002367386 .......... 146 00002367394 ............ 83 00002367564 ............ 46 00002367572 ............ 47 00002367602 .......... 118 00002367629 .......... 118 00002367645 .......... 118 00002368013 ............ 46 00002368021 ............ 46 00002368048 ............ 47 00002368226 .......... 129 00002368226 . SEC 3.59 00002368242 ............ 44 00002369036 .......... 115 00002369036 . SEC 3.93 00002370077 ............ 90 00002370255 . SEC 3.74 00002370441 ............ 54 00002370492 ............ 54 00002370506 ............ 55 00002370514 ............ 55 00002370522 ............ 55 00002370611 ............ 54 00002370638 ............ 54 00002370646 ............ 54
00002370654 ............ 54 00002370689 ............ 97 00002370697 .......... 103 00002370700 .......... 103 00002370735 ............ 48 00002370743 ............ 48 00002370751 ............ 48 00002370786 ............ 48 00002370808 .......... 148 00002370972 ............ 86 00002370980 ............ 86 00002370999 ............ 87 00002371022 ............ 65 00002371030 ............ 65 00002371049 ............ 65 00002371057 ............ 65 00002371413 ............ 25 00002371421 ............ 25 00002371529 ............ 65 00002371537 ............ 65 00002371545 ............ 66 00002371677 ............ 86 00002371685 ............ 86 00002371693 ............ 86 00002371715 ............ 52 00002371723 ............ 52 00002371731 .......... 143 00002371758 .......... 143 00002371766 .......... 101 00002371774 .......... 101 00002371782 .......... 101 00002371790 .......... 102 00002371804 .......... 102 00002371812 .......... 102 00002371820 . SEC 3.40 00002371898 ............ 90 00002371901 ............ 90 00002371987 ............ 46 00002371995 ............ 47 00002372347 ............ 63 00002372371 ............ 63 00002372398 ............ 64 00002372525 ............ 80 00002372533 ............ 80 00002372541 ............ 80 00002372568 ............ 80 00002372576 ............ 80 00002372584 ............ 80 00002372797 ............ 80 00002372819 ............ 98
00002372827 ............ 98 00002372835 ............ 98 00002372843 ............ 98 00002372851 ............ 99 00002372886 ............ 64 00002372894 ............ 64 00002372908 ............ 64 00002372932 ............ 39 00002372940 ............ 39 00002372959 ............ 39 00002372967 ............ 40 00002372975 ............ 40 00002373041 .......... 137 00002373203 ............ 36 00002373211 ............ 36 00002373238 ............ 36 00002373246 ............ 36 00002373319 ............ 63 00002373327 ............ 63 00002373335 ............ 64 00002373343 ............ 64 00002373351 ............ 64 00002373378 ............ 64 00002373432 ............ 98 00002373440 ............ 98 00002373459 ............ 98 00002373467 ............ 98 00002373734 ............ 66 00002373742 ............ 66 00002373750 ............ 66 00002373769 ............ 66 00002373777 ............ 66 00002373920 .......... 145 00002373939 .......... 145 00002373947 .......... 129 00002373947 .SEC 3.59 00002374552 ............ 92 00002374560 ............ 92 00002374579 ............ 93 00002374609 .......... 129 00002374609 .SEC 3.59 00002374757 .......... 185 00002374846 ............ 61 00002374854 ............ 61 00002374862 ............ 62 00002374870 .......... 148 00002375036 ............ 39 00002375044 ............ 39 00002375052 ............ 39 00002375060 ............ 40
00002375079 ............ 40 00002376350 .......... 118 00002376377 .......... 118 00002376385 .......... 118 00002376539 ............ 63 00002376547 ............ 63 00002376555 ............ 63 00002377608 .......... 129 00002377616 .......... 129 00002377616 SEC 3.59

















