48
GLOMERULONEPHRITIS Ali aL-ahrash, MD, PhD Azzawyia kidney center
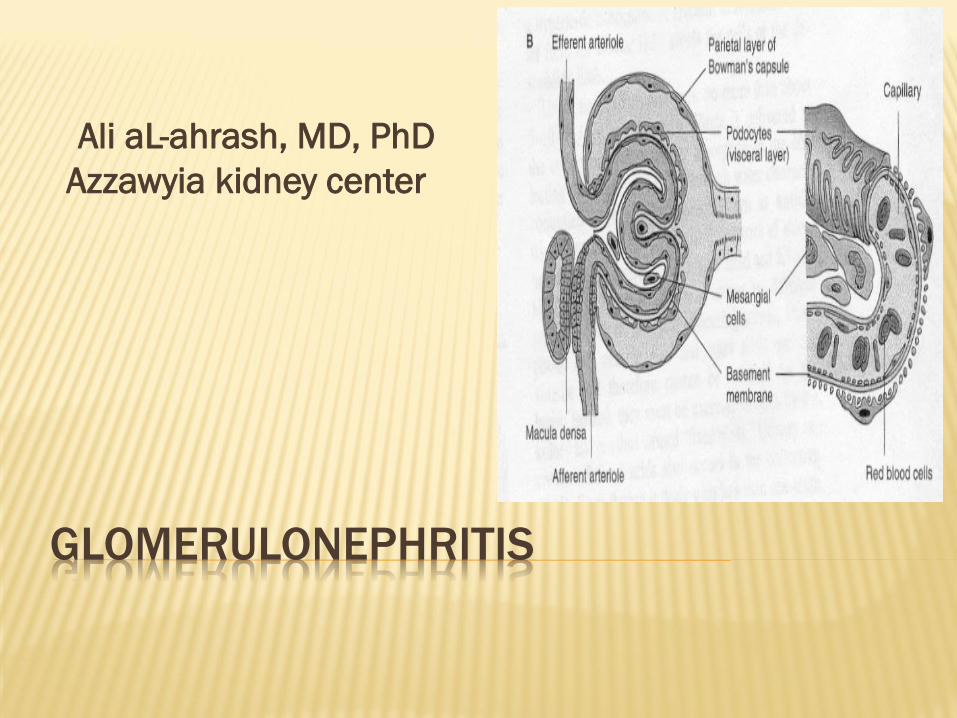
GLOMERULONEPHRITIS
Ali aL-ahrash, MD, PhD
Azzawyia kidney center

DEFINITION
A group of disorders in which:
Symmetrical involvement of both kidneys
Glomerular injury caused by immune depositin
Renal involvement as part of systemic diseases

characterized by inflammation either of the
glomeruli or small blood vessels in the kidneys,
but not all diseases necessarily have an
inflammatory component.
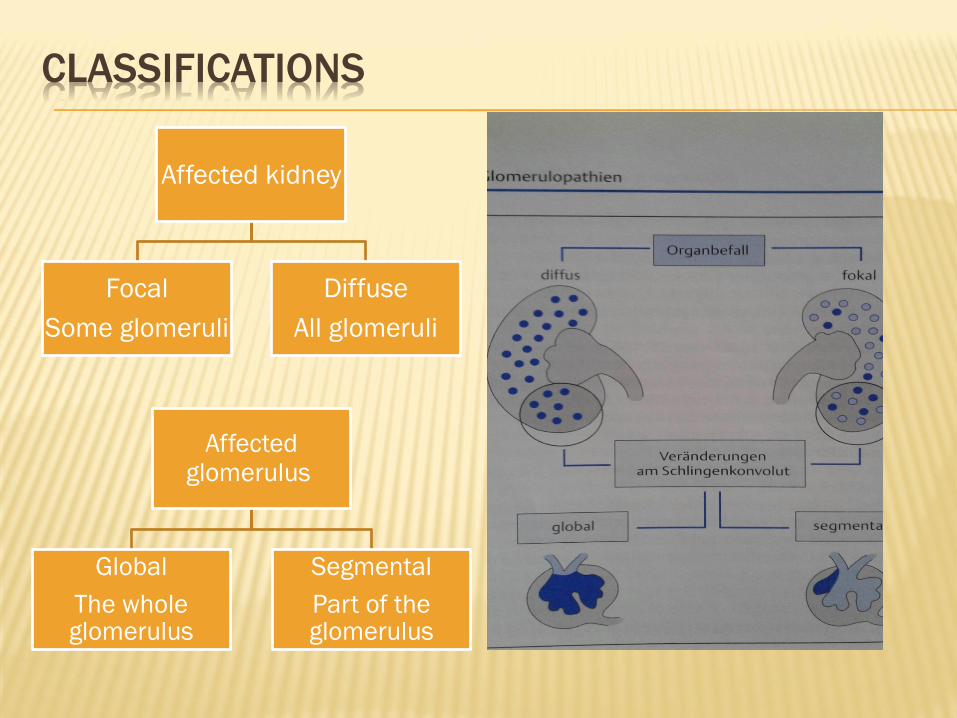
CLASSIFICATIONS
Affected kidney
Focal
Some glomeruli
Diffuse
All glomeruli
Affected glomerulus
Global
The whole glomerulus
Segmental
Part of the glomerulus

CAUSES
Unknown
Antigen derived from:
bacteria, B, HS, staph, salmonella
virus, measles, mumps, HBV
parasite, malaria, schistosoma
drugs, penicellamin
from the host it self, SLE,malignant tumor

If the body failed to clear the circulating immune
complexes or dose not have the ability to produce
appropriate antibodies these mechanisms are
triggered by:
Complement activation
Fibrin deposition
Platlet aggregation
Inflammation with neutrophil-dependent mechanism
Activation of kinin system
Primary GN are intrinsic to the kidney.
Secondary GN are associated with certain
infections (bacterial, viral or parasitic
pathogens), drugs, systemic disorders (SLE,
vasculitis), or diabetes.
PATHOLOGY
The pathological mechanisms are:
Immune complex deposition or
insitu immune complex formation,
the antigens are :
Exogenous, e.g bacteria, virus
Endogenous, antibody against host DNA
Deposition of the anti basement membrane
antibodies, e.g GPS
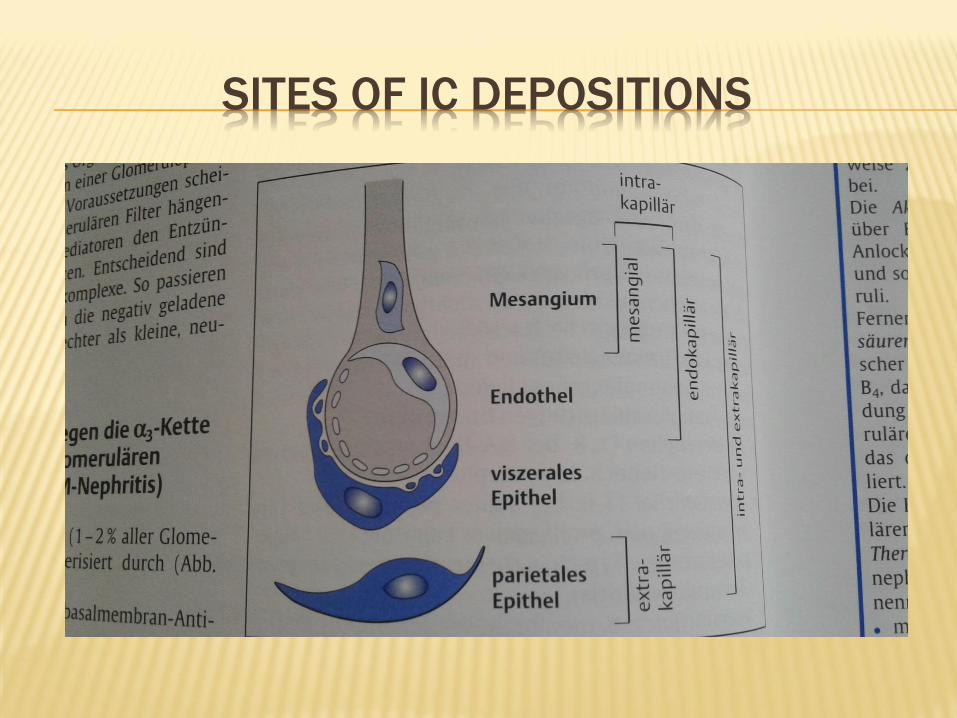
SITES OF IC DEPOSITIONS

IMMUNE COMPLEX DEPOSITION
NO
MC GN
FSGS
YES
MGN
IGA
MPGN
RPGN

HISTOLOGICAL CLASSIFICATIONS
1 Thin Basement Membrane Disease
2 Non Proliferative 2.1 Minimal change GN (also known as Minimal
Change Disease)
2.2 Focal Segmental Glomerulosclerosis (FSGS)
2.3 Membranous glomerulonephritis
3 Proliferative 3.1 IgA nephropathy (Berger's disease)
3.2 Post-infectious
3.3 Membranoproliferative/mesangiocapillary GN
3.4 Rapidly progressive glomerulonephritis

THIN BASEMENT MEMBRANE DISEASE
BENIGN FAMILIAL HEMATURIA

WHAT HAPPENED AFTER IMMUNE RESPONSE?
Cellular changes
proliferative
Glomerular cells enlargment
Inflammatory cells infiltration(exudative)
Non proliferative

MINIMAL CHANGE DISEASE
90% OF CHILDREN, 10% OF ADULT cause of NS
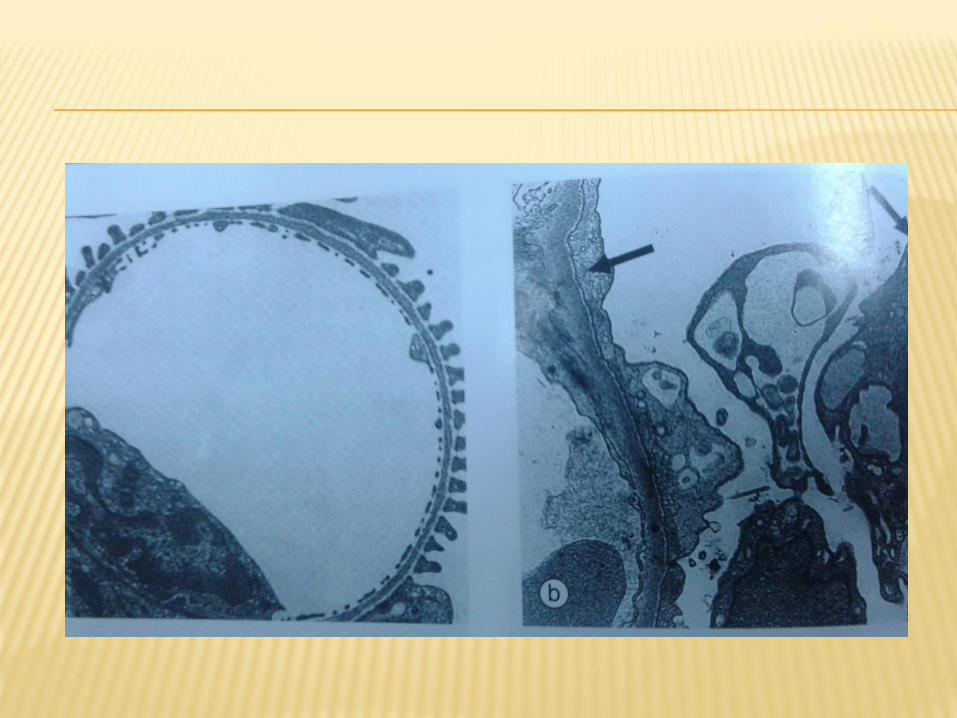
Absence of histologic abnormality on LM, fusion
of foot process of podocytes on EM
T cell mediated immunity against glomerular
epithelium (NO immune complex deposition)

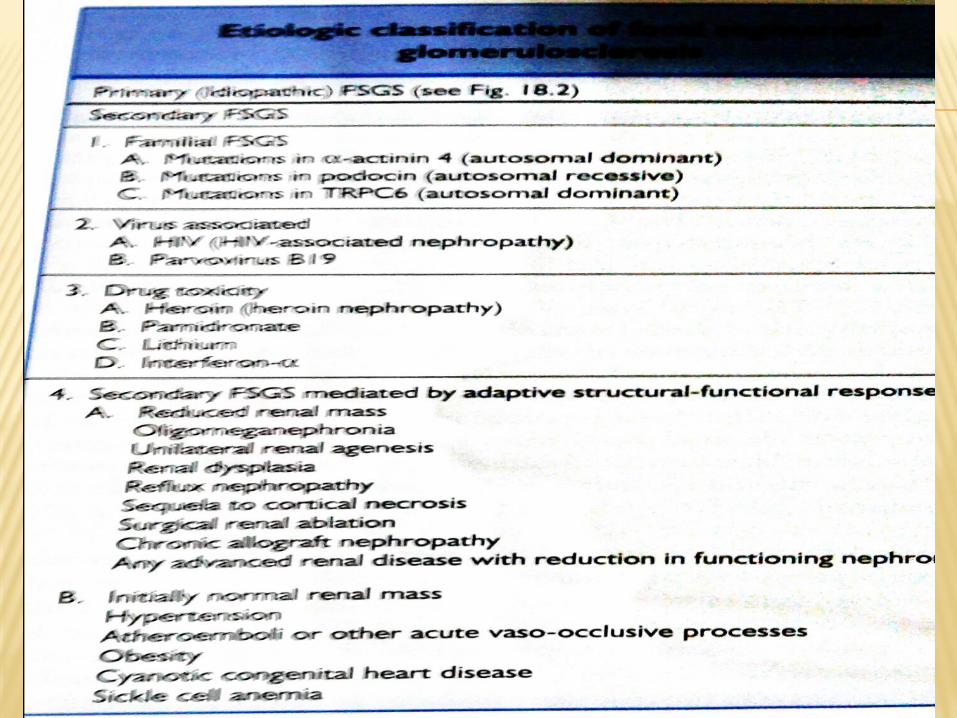
FOCAL SEGMENTAL GLOMERULOSCLEROSIS
(FSGS)
Increase incidence in both child & adult
More in males
More in blacks
In US the most common cause of GN leading to End stage CKD
HTN is found in 30-50% of child &adult
Presence of some permeability factors are responsible for recurrence of the disease after transplant
Majority will proceed for End stage ,5-25% got spontaneous remission


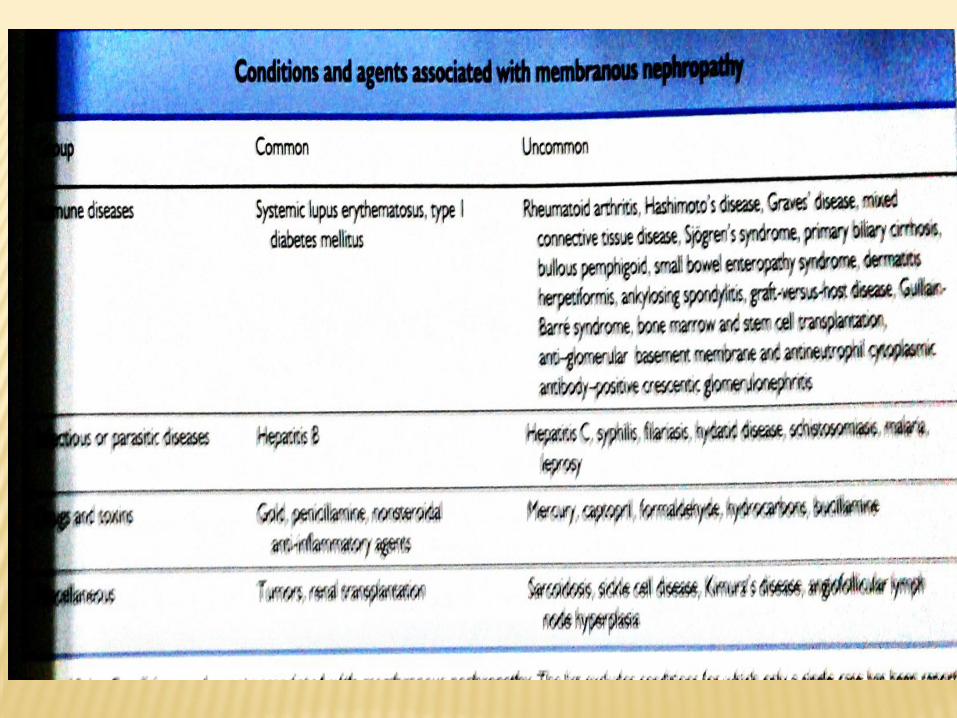
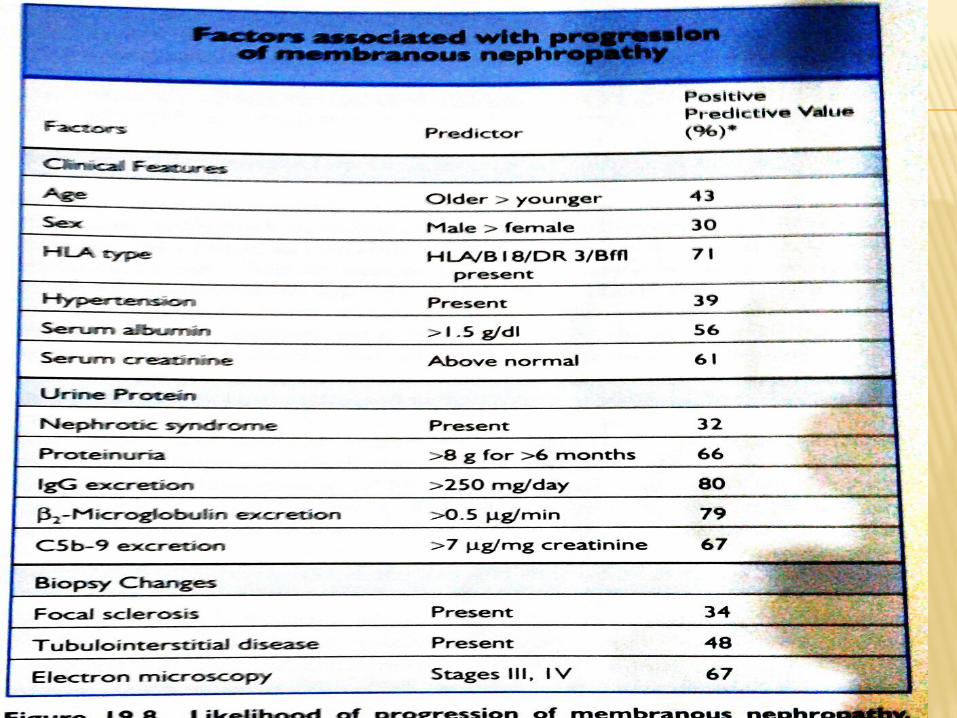
MEMBRANOUS GLOMERULONEPHRITIS
Thickning of glomerular basal membrane
Characterized histological by deposition of IgG &IC on subepithelial space as a spikes
70-80% primary, 20-30% secondary
Uncommon in chlidren less than 5%
Leading cause of NS (30-50%)
30% spontnous remission, 30% progress to end stage, 30% stable, 10% died due to non renal causes

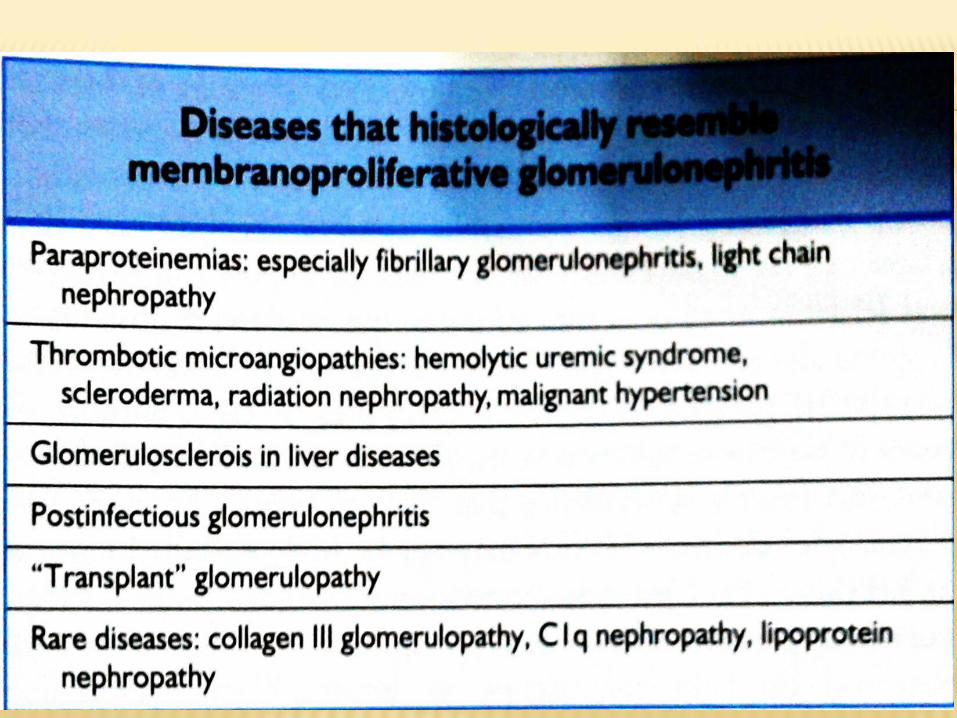
MEMBRANOPROLIFERATIVE/
MESANGIOCAPILLARY GN
Diffuse proliferation of capillary loops
Hypocomplementimia GN
Idiopathic or secondary to chronic infection, cryoglobulinemia or systemic immune disorder
Type I; subendothelial depostion
Type II (DDD); mesangial and glomerular basement membrane deposition
Type III; subendo & subepithelial deposition with marked disruption of basement membrane

Idiopathic MPGN carry poor prognosis in both
untreated child &adullt, it progress to end stage
Has high recurrence rate after tx


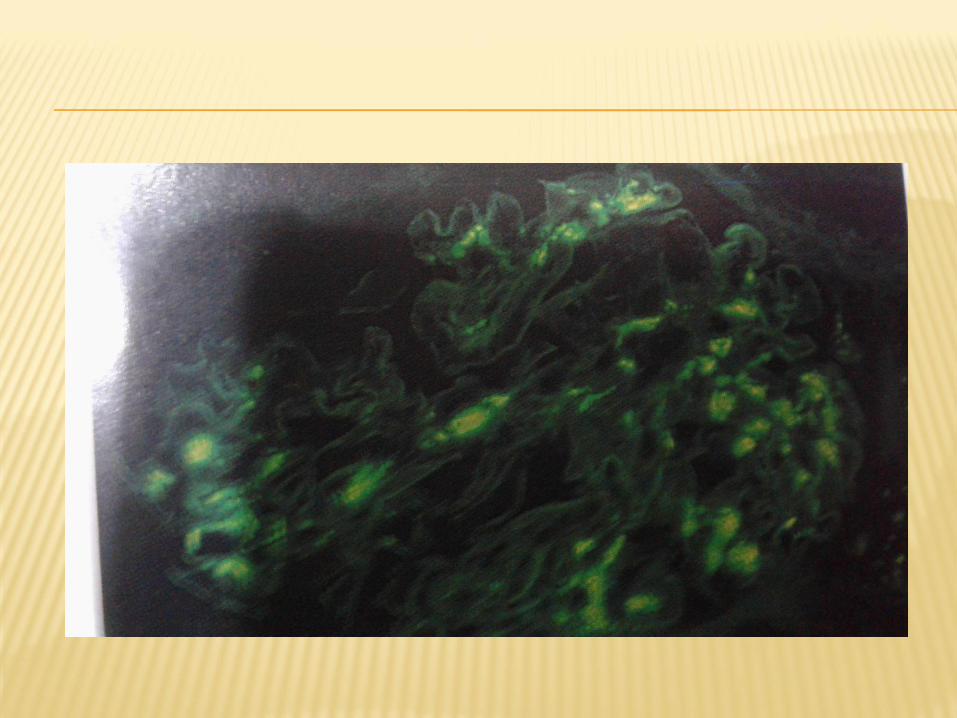
IgA nephropathy (Berger's disease)
Mesangial proliferation due to massive IgAdeposition
10-40% of renal biopsies
Disease of men between 20-40 ys
Diagonosis by immunoflurecent microscope
More prevalent in westren &Asia
Benign recurrent hematuria was used befor
Its an important cause of end stage
Macroscopic Hematuria &HTN following URTI
Reccure after tx



POST-INFECTIOUS GN
Charactarized by diffuse exudative
endocapillary GN after bacterial infection
sub epithelial electron dense deposition in a
form of humps
The AG is not well recognized, only
streptoccocal AG
It’s a disease of children
Ac. NS after 2 wks after throat or skin infection


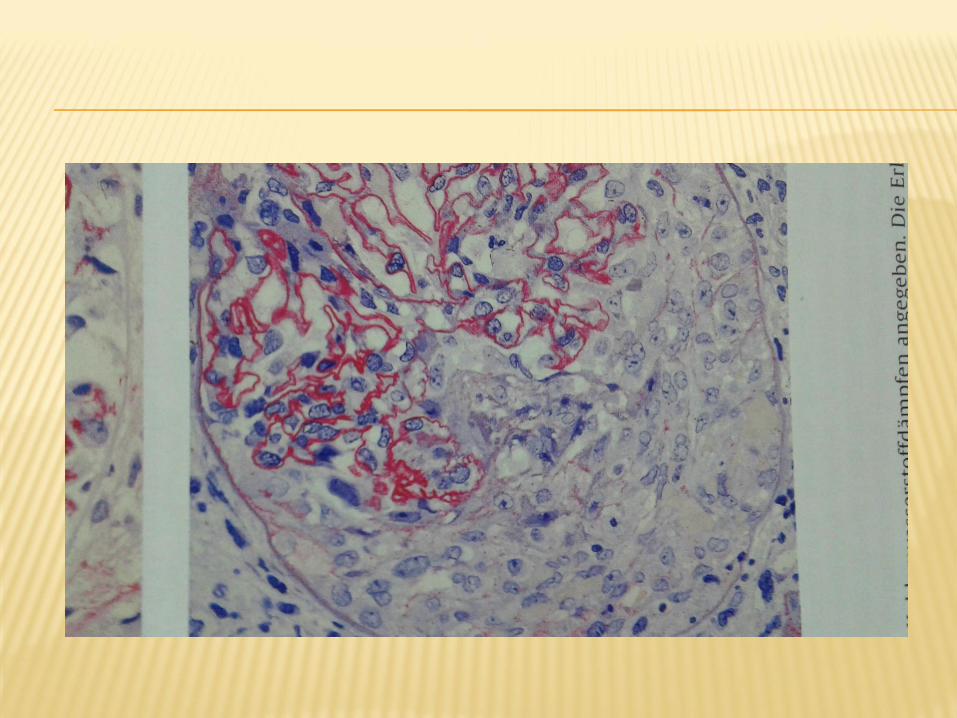
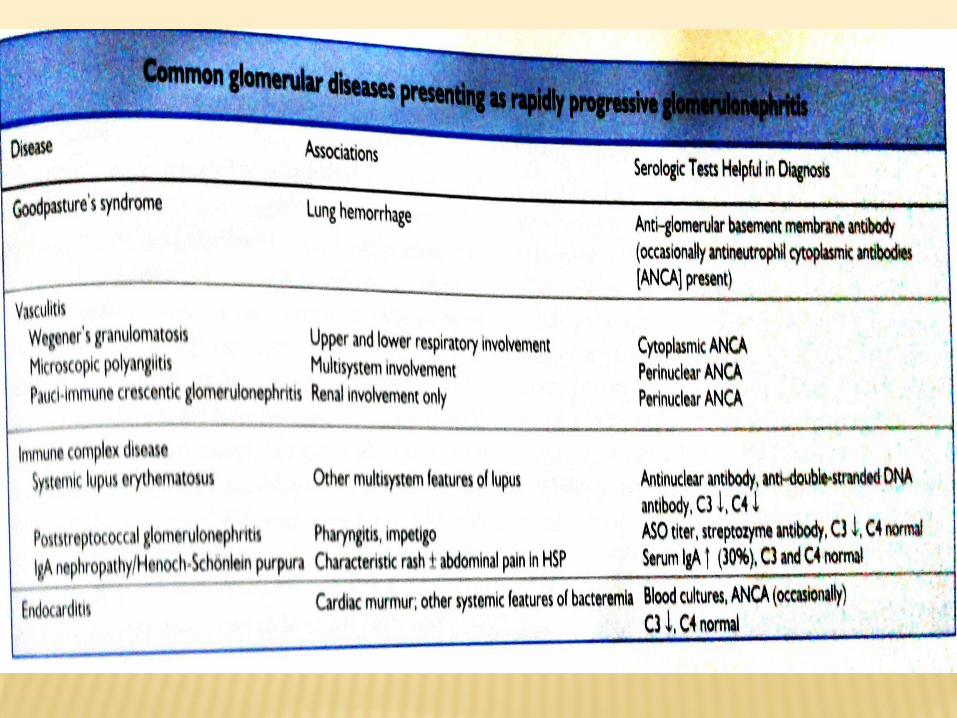
RAPIDLY PROGRESSIVE GLOMERULONEPHRITIS
Acute GN, followed by rapid drop of GFR in days
presence of intra &extra capillary proliferation in more than 50% of the glomerlulus in a form of crescent formation
Usually associated with system immune disease like, ANCA, ANA, Anti GBM Ab, SLE
Poor remission
Preservation of kidney size

CLINICAL PRESENTATION OF GN
it may present with;
isolated hematuria
and/or proteinuria
or as a nephrotic syndrome,
or nephritic syndrome,
or acute renal failure,
or chronic renal failure.




ACUTE NEPHRITIC SYNDROME
is a collection of signs (known as a syndrome) associated with disorders affecting the glomeruli.
It is characterized by having a thin glomerular basement membrane and small pores in the podocytes of the glomerulus,
leading to proteins and red blood cells to pass into the urine.
nephrotic syndrome is characterized by only proteins moving into the urine.
Both nephritic syndrome and nephrotic syndrome result in hypoalbuminemia due to protein albumin moving from the blood to the urine.

hematuria, with red blood cell (RBC) casts in
the urine
Proteinuria (<3.5 g/day)
Hypertension - mild
Uremia
oliguria (low urine output <400 mL/day)

CLINICAL PRESENTATION
Usually children with H/O 1-3 weeks URTI, otitis
media or cellulitis
Usually infection with group A beta HSC

INVESTIGATIONS
Urine for; RBC, Red cell castes, proteins
RFT
Throat swab for C/S
ASOT
ANA
C3
24 hrs urinary proteins
CXR
Renal biopsy

TREATMENT
Hospital management Daily in put /out put
Daily weighing
BP monitoring
Dietary control; protein in case of azotemia
Salt restriction
Fluid restriction
Diuretics therapy for HPN, fluid over load
Manag the life threatining complications like hypertensive encephalopathy, pulmonary oedema, uraemia accordingly
Prophylaxis therapy for individual at risk with penicillin
Needs follow up

BOOK SOURCES

















