92
Pharmacology I Ali Jaber, Ph.D. MS in Pharmacy MS in Pharmaceutical Chemistry Chapter 1 1

Pharmacology I
Ali Jaber, Ph.D.
MS in Pharmacy
MS in Pharmaceutical Chemistry
Chapter 1
1

Pharmacology, Definitions What is Pharmacology?
pharmakon = drug
logos = the study of
“A branch of medical sciences that study drugs and their action on living
organisms”
Pharmacology = the study of drugs what they do and how they do it
≠ Pharmacy: the health profession that deals with the preparation and dispensing of
(prescription) medications
2

Receptor
“A specific protein in either the plasma membrane or interior of a target
cell with which a chemical messenger/drug combines”
Pharmacology, Definitions
Drug
“Any substance that brings about a change in biologic function through its
chemical actions”
Dose
“The amount of a drug (mg/kg) to be administered at one time”
Mechanism of Action
“The ways by which drugs can produce therapeutic effects”
“Drug” has many definitions
Webster’s Dictionary: “a substance intended for use in the diagnosis, cure, mitigation, treatment or prevention
of disease”
3
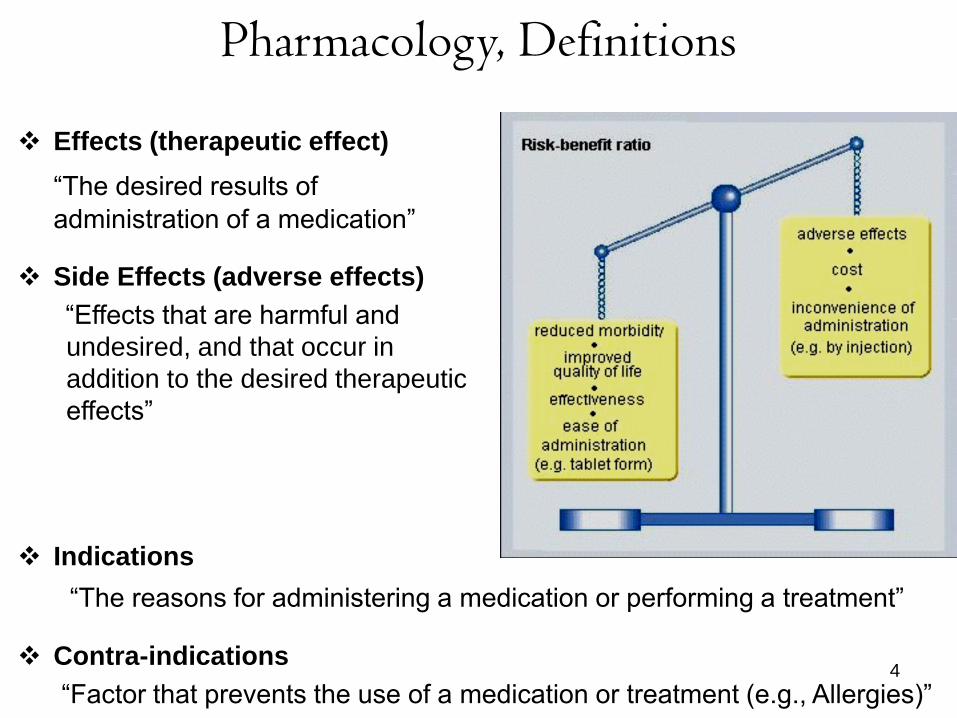
Indications
“The reasons for administering a medication or performing a treatment”
Contra-indications
“Factor that prevents the use of a medication or treatment (e.g., Allergies)”
Pharmacology, Definitions
Effects (therapeutic effect)
“The desired results of
administration of a medication”
Side Effects (adverse effects)
“Effects that are harmful and
undesired, and that occur in
addition to the desired therapeutic
effects”
4

Drug Sources 1. Plant Sources: Obtained from plant parts or products. Seeds, stem,
roots, leaves, resin, and other parts yield these drugs. Examples include digoxin from digitalis and morphine from opium.
5
Drug Sources
4. Mineral Sources: Some drugs are prepared from minerals, for example,
lithium carbonate (an antipsychotic), MgSO4 (a laxative)
5. Synthetic Sources: Laboratories duplicate natural processes, and may
modify the products. Frequently this can eliminate side effects and
increase the potency of the drug. Examples include sulfonamides, and aspirin.
6. Recombinant proteins: Proteins that are synthesized by expression of
cloned genes in recombinant cells, such as interferons, antibodies
3. From micro-organisms (fungi, bacteria) Penicillin was discovered by
Alexander Fleming in 1928 as a product of penicillium notatum (a mold
growing in his lab)
6
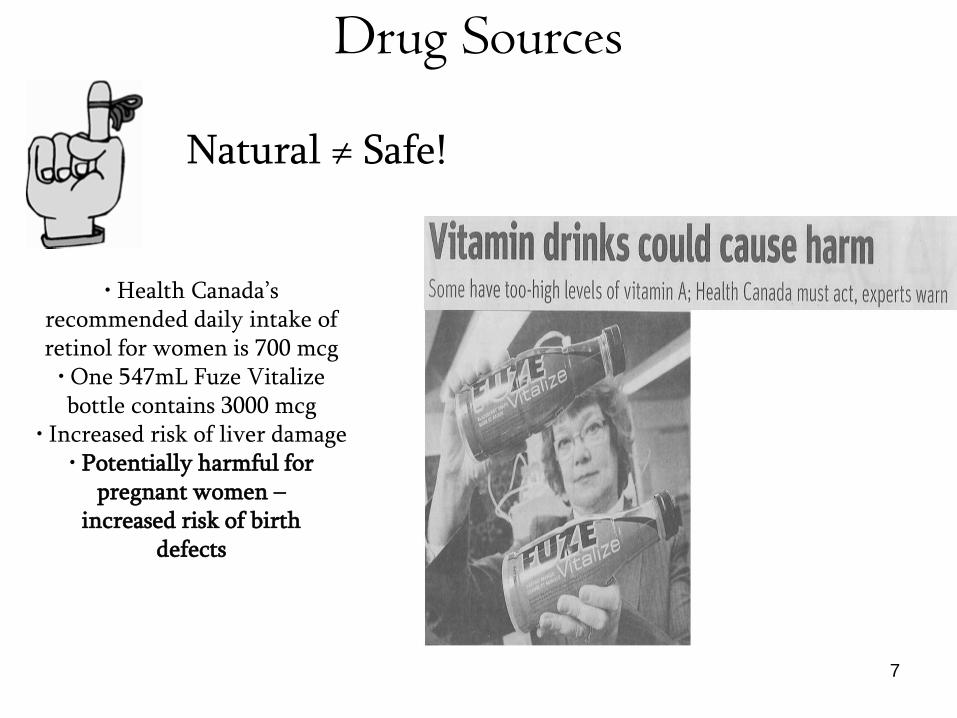
Drug Sources
Natural ≠ Safe!
• Health Canada’s recommended daily intake of retinol for women is 700 mcg
• One 547mL Fuze Vitalize bottle contains 3000 mcg
• Increased risk of liver damage • Potentially harmful for
pregnant women – increased risk of birth
defects
7

Drug Nomenclature
One drug…many names
Brand or trade name (proprietary) is developed by the company requesting
approval for the drug and identifies it as the exclusive property of that company.
Example 1: Metrogyl® is the trade name for metronidazole.
Example 2: Amoxil® is the trade name for amoxycillin.
Example 3: Celebrex® is the trade name for Celecoxib.
Example: the chemical name 2-methyl-5-nitroimidazole-l-ethanol is
metronidazole.
Chemical name represents the exact description of the drug’s chemical
composition important only for chemists,pharmacist
Generic name (non-proprietary name)
- simpler than the chemical name and
- derived from the chemical name itself
- easier to remember
8

Drug Nomenclature
One drug…many names
Chemical name: (+-)-2-(p-isobutylphenyl) propionic acid
Generic name: Ibuprofen Brand names: Advil®, Motrin®
Chemical name: Ethyl 4-(8-chloro-5,6-dihydro-11Hbenzo[
5,6]cyclohepta[1,2-b]pyridin-11-ylidine)-1- piperidinecarboxylate
Generic name: Loratadine Brand name: Claritin®
9

Pharmacokinetics (in Greek: "pharmacon" meaning drug, and "kinetikos"
meaning putting in motion)
The study of the movement of drugs in the body, including the processes
of absorption, distribution, metabolism and excretion (ADME)
The drug should be in an adequate concentration at the site of action to
produce its effects. This depends on ADME.
Pharmacokinetics (PK)
Pharmacodynamics (PD) The study of the action or effects of drugs on living organisms
Pharmacokinetics vs Pharmacodynamics
What the drug does to the body What the body does to the drug
Pharmacology has 2 arms
10

Routes of drug administration طرق إعطاء األدوة
• Which route to use? 3 factors to consider
1 size, water vs lipid solubility, pH stability
2. consciousness, ability to follow instructions,
age, other medications
3. urgency of situation, local vs systemic effects
11

Routes of drug administration طرق إعطاء األدوة
12
Local ومحلةSystemic تنقسم طرق اعطاء الدواء إلى نظامة
بالحقن ParenteralوEnteral وتنقسم الطرق النظامة إلى معوة

Enteral administration of drugs الطرق المعوة العطاء األدوة
Enteral (GI tract)
•Oralالطرق األكثر استخداما إلتاء الدواء
وهذا . إنها الطرقة األكثر تعقدا وتوفر امتصاصا بطئا وغر منتظم
عن أن مرور الدواء إلى الدم بطء إلى حد ما بسبب الحاجة إلى
عبور القناة الهضمة المعوة بالكامل ثم الوصول إلى الغشاء
. المخاط االثن عشر الذي متلك القدرة القصوى على االمتصاص
تم امتصاص بعض األدوة أضا بكمات صغرة من الغشاء المخاط ف المعدة
13
Enteral administration of drugs الطرق المعوة العطاء األدوة
Enteral (GI tract)
•Oral الفوائد
أمن وسهل االستعمال ومقبول من المرضى
ال صدمة حساسة وله تؤثرات أقل سمة
السلبات
ال صلح لحاالت الطارئة
غر منتظم ألنه ال مكن تحدد كمة تركزالدواء ف الدم بالضبط نظرا لوجود العدد من العوامل المسببة للتداخل ومنها
الحلول ، المعلقات ، الكبسوالت ، األقراص : اشكال الدواء تملح الدواء وتعدد األشكال: لعوامل الفزائة والكمائةا
, الحركة المعوة, تؤثر المرور األول: العوامل الفزولوجة الطعام
14

Enteral administration of drugs الطرق المعوة العطاء األدوة
Enteral (GI tract)
•Sublingual تحت اللسان
وضع الدواء تحت اللسان أو بن الخد واللثة سمح بانتشاره مباشرة إلى
الشعرات الدموة، مما عط تؤثرا سرعا للدواء وجنبه أثر التعرض
.إلفرازات المعدة واألمعاء وأثر المرور بالكبد
الفوائد
امتصاص سرع
تجنب المرور بالكبد
السلبات
تقرحات مع الوقت
ال مكن إعطاء أدوة شددة المرورة15
Enteral administration of drugs الطرق المعوة العطاء األدوة
Enteral (GI tract)
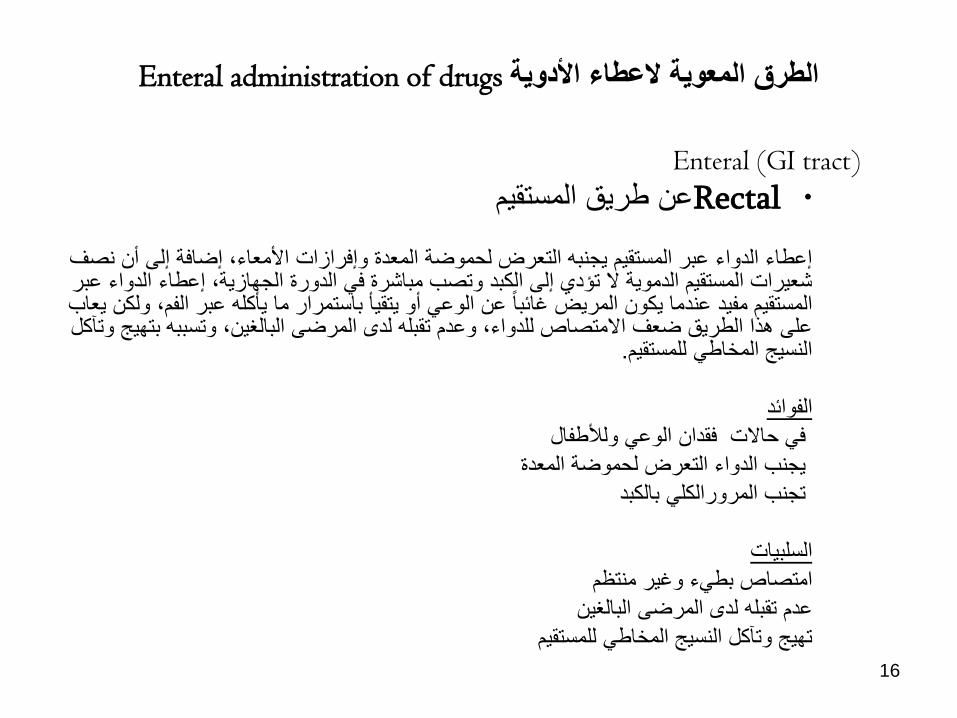
•Rectal عن طرق المستقم
إعطاء الدواء عبر المستقم جنبه التعرض لحموضة المعدة وإفرازات األمعاء، إضافة إلى أن نصف شعرات المستقم الدموة ال تإدي إلى الكبد وتصب مباشرة ف الدورة الجهازة، إعطاء الدواء عبر المستقم مفد عندما كون المرض غائبا عن الوع أو تقؤ باستمرار ما ؤكله عبر الفم، ولكن عاب على هذا الطرق ضعف االمتصاص للدواء، وعدم تقبله لدى المرضى البالغن، وتسببه بتهج وتآكل
.النسج المخاط للمستقم
الفوائد ف حاالت فقدان الوع ولألطفال جنب الدواء التعرض لحموضة المعدة تجنب المرورالكل بالكبد
السلبات امتصاص بطء وغر منتظم
عدم تقبله لدى المرضى البالغن تهج وتآكل النسج المخاط للمستقم
16

2.Parenteral administration of drugs المسارات الحقنةالعطاء األدوة
17
تم استخدام إبرة لحقن الدواء مباشرة إلى داخل الجسد، تستخدم الحقن
إلعطاء األدوة الت ال تمتص جدا ف األمعاء أو األدوة الت ال تتحمل
بئة القناة الهضمة، وف حاالت إعطاء العالج لمرضى فاقدي الوع أو
الحاجة لبداة سرعة للتؤثر العالج، أو الحاجة للحفاظ على تركز
محدد من الدواء داخل الجسد

2.Parenteral administration of drugs المسارات الحقنةالعطاء األدوة
• الحقن ف الورد: عد الحقن ف الورد أكثر الطرق الحقنة استخداما خاصة لألدوة الت ال مكن تعاطها عبر الفم، وللحقن ف الورد مزاا عدة، فهو تح
إصال الدواء مباشرة إلى الدورة الجهازة مما ضمن بداة سرعة للتؤثر
الدوائ، وضبط محكم لمستوى الدواء ف بالزما الدم، ولكن عاب عله إمكانة
.تسبب الحقن لترسب مكونات الدم أو تحللها
الحقن ف العضل: تح الحقن ف العضل إمكانة إطالة التؤثر العالج بسبب االنتشار .البطء للدواء من موقع الحقنة إلى الشعرات الدموة المجاورة
الحقن تحت الجلد: تمز الحقن تحت الجلد عن الحقن ف الورد بتقلل الحقن تحت الجلد وأطولمخاطر تحلل الدم أو تخثره، ولكنه تح تؤثر عالج أبطؤ
18

First-Pass Effect تأثر المرور األول
عن طرق الكبد حث نخفض تركز الدواء بشكل هو ظاهرة حول أض األدوة •
)الدورة الدموة الكبرى(كبر قبل أن صل الدورة الجهازة
قد تم استقالب الدواء المعطى عن طرق الفم على نطاق واسع عن طرق الكبد • )تؤثر تمرر أول عال(قبل الوصول إلى الدورة الجهازة
تجنب الكبد ، مما منع التؤثر األول من الحدوث -المعطى بالورد -نفس الدواء •
، والمزد من الدواء صل إلى الدورة الدموة
19

First-pass effect is the metabolism of a drug by the liver before its systemic
availability
Drug Routes and First-Pass Effects
20

Topical Routeموضع
• Skin (including transdermal patches)
• Eyes
• Ears
• Nose: Nicotin and Calcitonin
• Lungs (inhalation): aerosol for asthma and BPCO
• Vagina
21
ملخص
22

Phases of Drug Therapy مراحل العالج الدوائ
المراحل الت تإثر على العالج الدوائ
Pharmaceutic Phase المرحلة الصدالنة Pharmacokinetic Phase مرحلة الحركة الدوائة Pharmacodynamic Phase مرحلة الدنامكة الدوائة
23

Pharmaceutic Phase المرحلة الصدالنة
– Drug absorption of various preparations
• Liquids Fastest
• Powders
• Tablets
• Enteric-coated tablets Slowest
ال وجد مرحلة صدالنة عن طرق الحقن
تدرس كفة تؤثر مختلف أشكال االدوة على الدنامكة الدوائة
والحركة الدوائة
24

Pharmacokinetics حركة الدواء
الحركة الدوائة ه جزء من علم الصدلة الذي درس آلات
• Absorptionاالمتصاص الوضع الذي دخل فه الدواء الجسم
• Distribution :التوزع • خروج الدواء من مجرى الدم وتوزعه ف أجزاء الجسم• Metabolism األض
تم استقالب الدواء وتعدله من قبل أعضاء معنة مثل الكبد والكلى • Excretion االقصاء الطرقة الت ترك بها الدواء الجسم
25
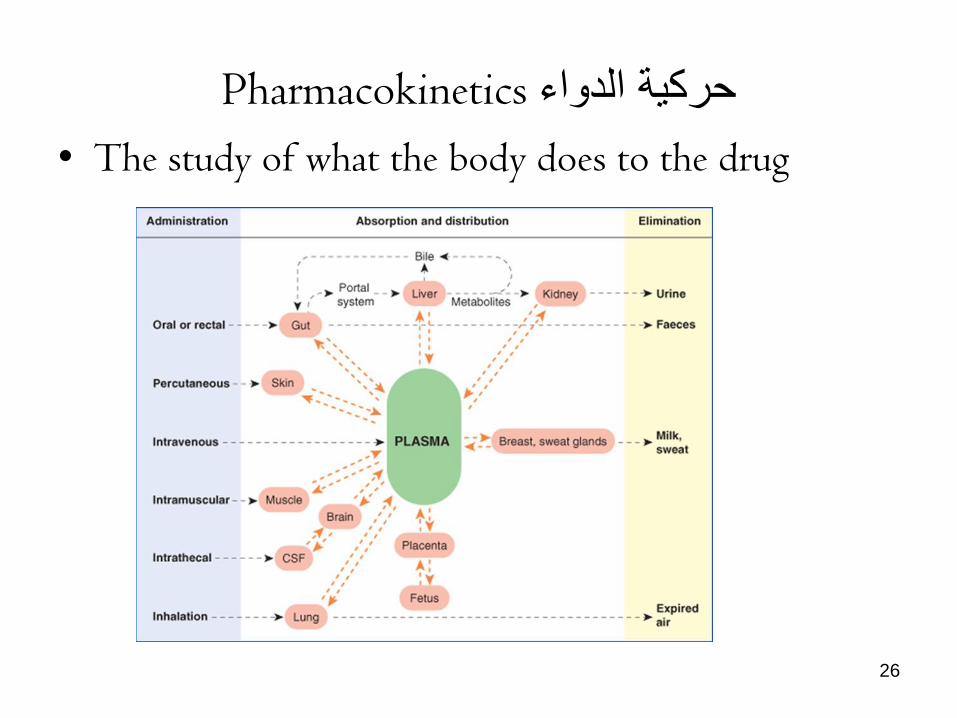
Pharmacokinetics حركة الدواء
• The study of what the body does to the drug
26

Pharmacokinetics حركة الدواء
• The study of what the body does to the drug
27

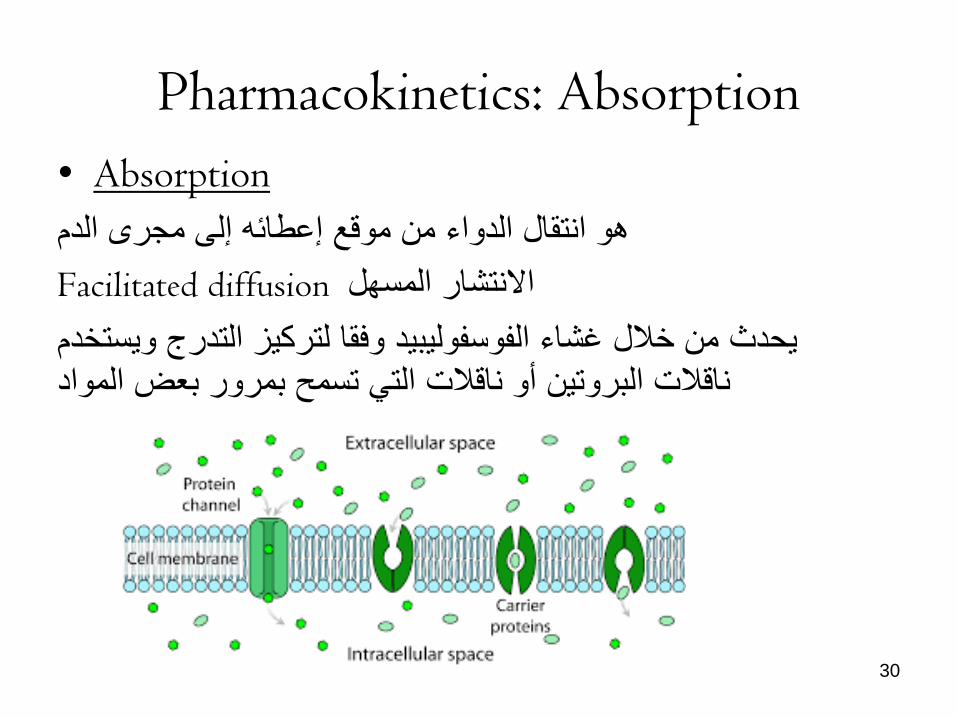
Pharmacokinetics: Absorption
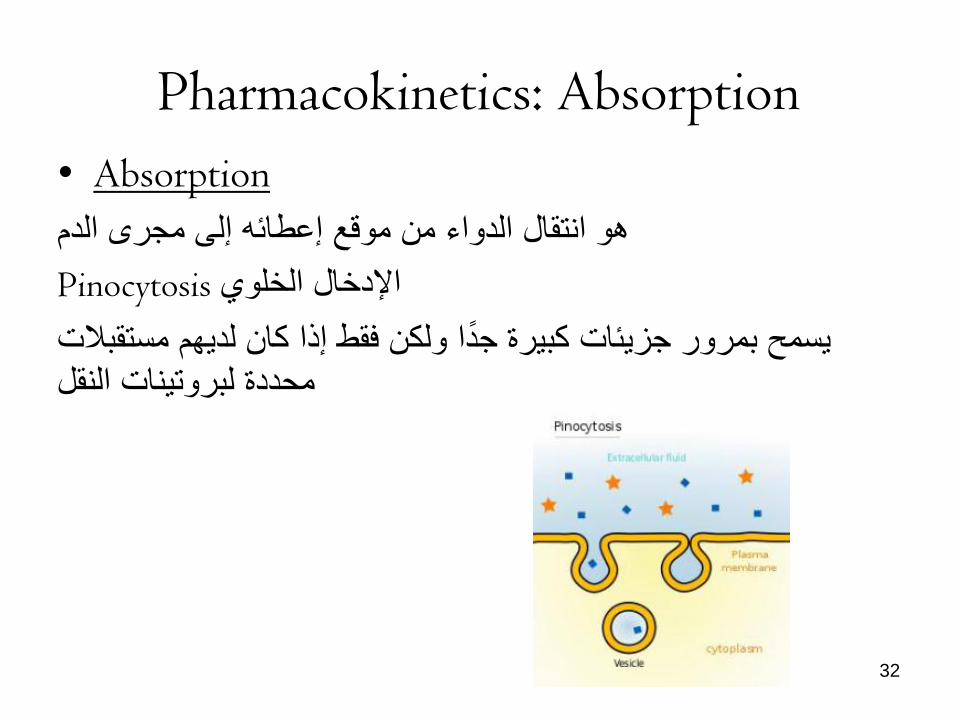
• Absorption
هو انتقال الدواء من موقع إعطائه إلى مجرى الدم
االمتصاص عتمد على طرق اعطاء الدواء ف الورد هو إجمال
:طرق لعبور الدواء من خالل األغشة البولوجة 5هناك
Simple diffusion االنتشار البسط
هذه ه الطرقة األكثر استخداما للجسمات القابلة للذوبان ف الدهون
والت مكن أن تمر عادة عبر غشاء الخلة بحسب تدرج التركز
28

Pharmacokinetics: Absorption
• Absorption
هو انتقال الدواء من موقع إعطائه إلى مجرى الدم
Filtration الترشح
ه عبارة عن مرور الجزئات القابلة للذوبان ف الماء من خالل
الت تم نقلها من خالل القنوات األونة المناسبة وفقا لتدرج . األغشة
التركز
29
Pharmacokinetics: Absorption
• Absorption
هو انتقال الدواء من موقع إعطائه إلى مجرى الدم
Facilitated diffusion االنتشار المسهل
حدث من خالل غشاء الفوسفولبد وفقا لتركز التدرج وستخدم ناقالت البروتن أو ناقالت الت تسمح بمرور بعض المواد
30

Pharmacokinetics: Absorption
• Absorption
هو انتقال الدواء من موقع إعطائه إلى مجرى الدم
Active Transport النقل النشط
النقل ضد تدرج التركز
31
Pharmacokinetics: Absorption
• Absorption
هو انتقال الدواء من موقع إعطائه إلى مجرى الدم
Pinocytosis اإلدخال الخلوي
سمح بمرور جزئات كبرة جدا ولكن فقط إذا كان لدهم مستقبالت محددة لبروتنات النقل
32
Pharmacokinetics: Absorption
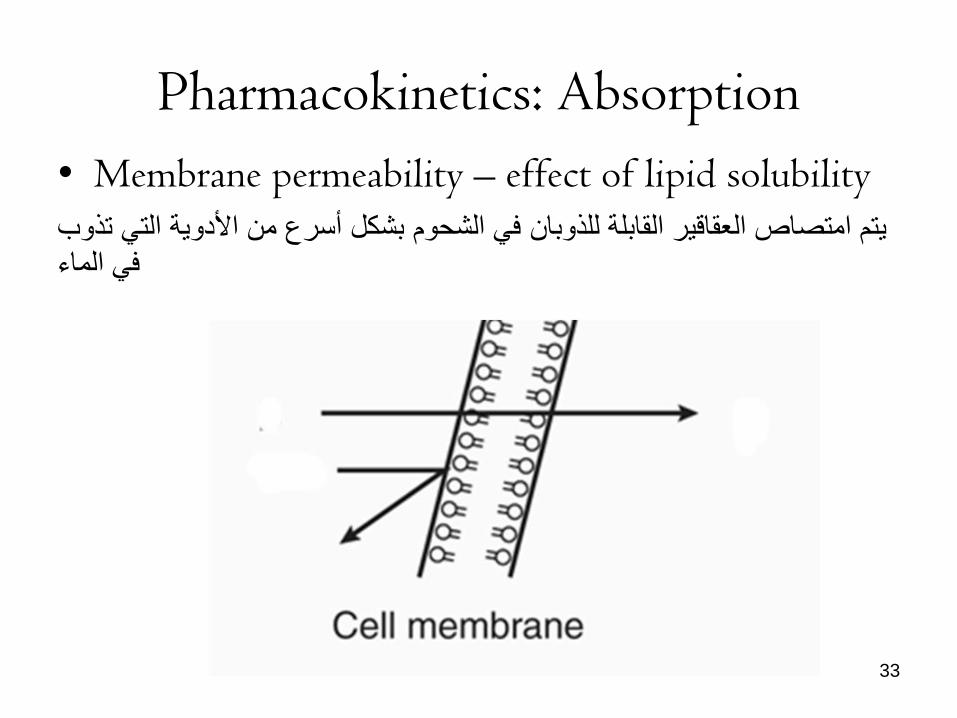
• Membrane permeability – effect of lipid solubility
تم امتصاص العقاقر القابلة للذوبان ف الشحوم بشكل أسرع من األدوة الت تذوب ف الماء
33

Pharmacokinetics: Absorption
-Membrane permeability – effect of pH
• exist –معظم األدوة ه أحماض ضعفة أو قواعد ضعفةin equilibrium between protonated & unprotonated, charged & uncharged species
HA H+ + A- B + H+ BH+
Weak base drug weak acid drug
34

Pharmacokinetics: Absorption
-Membrane permeability – effect of pH
• فقط األنواع غر المشحونة ستعبر الغشاء
35

العوامل المادة الت تإثر على امتصاص االدوة
• Administration route of the drug: Enteral, Parenteral
• Drug formulation: Chewable, enteric coated (breakdown
occurs in small intestine), slow release capsules
• Food or fluids administered with the drug: Orange juice – enhances absorption of iron taken orally
Caffeina decreses absorption of iron taken orally
• Blood flow تدفق الدم
كلما زاد تدفق الدم ارتفعت القدرة على امتصاص الدواء إلى الدورة الدموة
هذه ه إحدى العوامل الت تجعل االمتصاص المعوي لالدوة اكبر مقارنة
بالمعدة بالفعل هناك تدفق للدم الى األول أكثرمن الثان
36

العوامل المادة الت تإثر على امتصاص االدوة
الكلة المتاحة لالمتصاصالمساحة •
إضافةأكبر ف األمعاء وتحدد قدرة امتصاص ه
التالمس مع سطح االمتصاصوقت •
إذا كان هناك عوامل تسرع عبورا سرعا جدا ، فمن غر الممكن االمتصاص
الصحح للدواء ، والعكس بالعكس أي عنصر عوق المرور من المعدة الى األمعاء
سرع الالودي العبور ، وعوق المرور الودي، . وثر سلبا على االمتصاص باإلضافة إلى اي وجبة كبرة
37

Pharmacokinetics:Bioavailability التوافر البولوج
–Bioavailability التوافر البولوج تم تعرف التوافر البولوج على أنه الجزء من الدواء الذي صل
إلى الدم ف صورة غر معدلة كمائا بغض النظر عن طرقة اعطاإه
منح الحقن الوردي التوافر البولوج للدواء بنسبة ١٠٠
%
38
Bioavailability التوافر البولوج
:الت تإثر على التوافر البولوجالعوامل تؤثر المرور األول
الدواءذوبان
عدم االستقرار الكمائ
حجم الجسمات ، شكل المحلول : طبعة المستحضرات الصدالنة
الملح ، تعدد أشكال الكرستال ، وجود السواغات
39

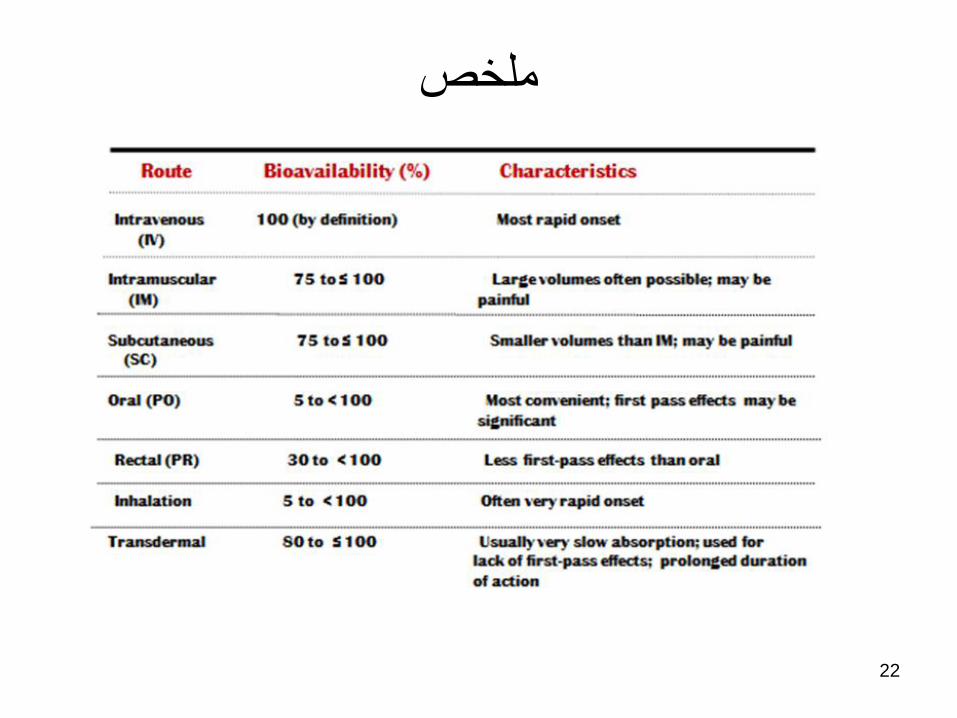
Route Bioavailability (%) Characteristics
Intravenous 100 (by definition) Most rapid onset
(IV)
Intramuscular 75 to ≤ 100 Large volumes often possible; may be
(IM) painful
Subcutaneous 75 to ≤ 100 Smaller volumes than IM; may be painful
(SC)
Oral (PO) 5 to < 100 Most convenient; first pass effects may be
significant
Rectal (PR) 30 to < 100 Less first-pass effects than oral
Inhalation 5 to < 100 Often very rapid onset
Transdermal 80 to ≤ 100 Usually very slow absorption; used for
lack of first-pass effects; prolonged duration
of action
40

Distribution توزع األدوة ف الجسم
-The process by which drug reversibly leaves the
bloodstream
توزع الدواء هو العملة الت تسمح لجزئات الدواء بالمرور من مجرى الدم
إلى الجسم وه خطوة أساسة تسمح االدوة باالتصال بهاكل الخالا المستهدفة
• drug moves between body compartments
• drug reaches the site of action (receptors)
41
هذه العملة تعتمد على
هكل او تركبة الدواء .1
من الواضح أن االدوة الت تذوب ف الدهون قادرة على عبور
جدار الشعرات الدموة دون مشاكل على عكس االدوة المحبة
للماء الت لدها محدودة أكثرف االنتشار بسبب استحالة عبورها طبقة الدهون ف األغشة

Distributionالتوزع Effect of blood flow:
• Areas of rapid distribution: heart, liver,
kidneys, brain
• Areas of slow distribution: muscle, skin, fat
42
تدفق الدم.2تم توزع الدواء باكثر سرعة وكمة أكبر ف االعضاء الت
كون فها تدفق الدم أكبر القلب ، الكبد ، الكلى ، المخ: مناطق التوزع السرع• العضالت والجلد والدهون: مناطق التوزع البطء•
Distribution توزع األدوة ف الجسم
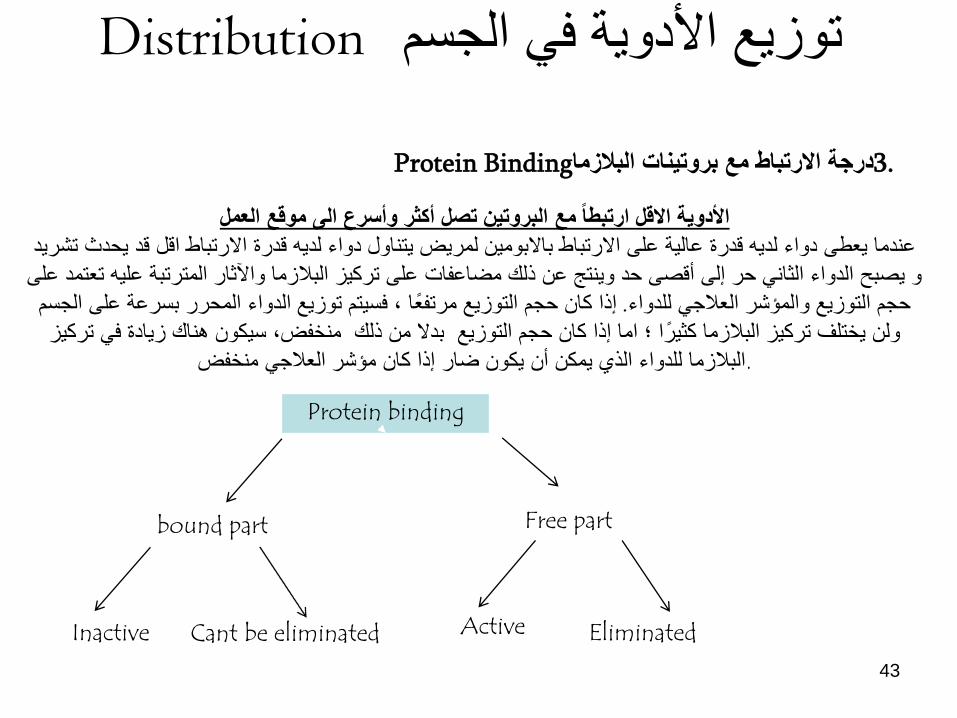
Protein Bindingدرجة االرتباط مع بروتنات البالزما .3
43
األدوة االقل ارتبطا مع البروتن تصل أكثر وأسرع الى موقع العملعندما عطى دواء لده قدرة عالة على االرتباط باالبومن لمرض تناول دواء لده قدرة االرتباط اقل قد حدث تشرد
و صبح الدواء الثان حر إلى أقصى حد ونتج عن ذلك مضاعفات على تركز البالزما واآلثار المترتبة عله تعتمد على
إذا كان حجم التوزع مرتفعا ، فستم توزع الدواء المحرر بسرعة على الجسم . حجم التوزع والمإشر العالج للدواء
ولن ختلف تركز البالزما كثرا ؛ اما إذا كان حجم التوزع بدال من ذلك منخفض، سكون هناك زادة ف تركز
.البالزما للدواء الذي مكن أن كون ضار إذا كان مإشر العالج منخفض Protein binding
bound part Free part
Inactive Cant be eliminated Active Eliminated

Distribution
44
Protein Bindingدرجة االرتباط مع بروتنات البالزما تصنف االدوة المرتبطة بالبروتن
1جزئة ل 1)مكن أن تكون رابطة منخفضة السعة 1. ( ألبومن
(ألبومن 1جزئات مختلفة ل )أو قدرة عالة 2.Weakly protein bound drug Highly protein bound drug

Displacement
45

Volume of distribution (Vd) حجم التوزع
What is volume of distribution? ا ، بل هو ثابت تناسب ربط كمة الدواء ف الجسم بتركزه ف الدم • ا حقق لس حجما فسولوج
وزع الدواء خارج الدم والجسم(: ل ٤٢< )حجم التوزع كبر
السوائل ف األنسجة
المخدرات لدها توزع محدود ، عادة(: ل ٤٢≥)حجم التوزع صغر
قتصر على الدم أو السوائل الفسولوجة
• The magnitude of Vd indicates the extent of drug distribution in the body, but not the location Large Vd (>42 L): drug distributes outside blood and body fluids into tissues Small Vd (≤42 L): drug has limited distribution, typically restricted to blood or physiological fluids
46

Metabolism استقالب الدواء (Also Known As Biotransformation)
the irreversible biotransformation of drug
makes it more polar to ↑ renal (urinary) excretion
التحول األحائ او االستقالب هو عملة تحول الدواء إلى جزيء أكثر ذوبانا ف الماء بطرقة تسمح بطرحه من الجسم من خالل الكلة
تحدث هذه العملة بشكل رئس ف الكبد وهو الجهاز الرئس لعملة التحول األحائ ، ولكن هناك أضا مواقع أخرى أقل أهمة مثل المشمة واألمعاء
47

Metabolism استقالب الدواء (Also Known As Biotransformation)
:هناك عدة إمكانات للنتائج بعد استقالب الدواء
هذا إالطارتتبعه معظم األدوة= الدواء الفعال صبح غر فعال . 1
حالة الهرون الذي تحول إلى مورفن= الدواء الفعال بقى فعال . 2
حالة بعض األدوة مثل الكورتزون = الدواء غر فعال صبح فعال . 3 والبردنزون
حالة الباراستامول= الدواء الفعال صبح سام . 4
48

Metabolism استقالب الدواء (Also Known As Biotransformation)
49
تتضمن هذه التفاعالت التحلل المائ ، األكسدة ، االختزال ، : تفاعالت المرحلة األولى
هدروكسل ، التصفة الت تحول الدواء إلى مستقلب أكثر قابلة للذوبان ف الماء عن طرق
-كشف أو إنشاء مجموعات وظفة قطبة مثل OH ، - SH2 ، - NH2.
تفاعالت االقتران بشكل رئس مع جزئات ترتبط بالمجموعات القطبة : 2تفاعالت المرحلة
عموما العنصر . الت تم إنشاإها سابقا مع الوظفة دائما لجعل المستقلب أكثر قابلة للذوبان
الرئس المستخدم هو حمض الجلوكورونك ولكن من الممكن أضا استخدام حمض الكبرتك ،
والنتجة ه عموما مركب غر نشط. حمض الخلك أو حمض أمن

Metabolism
Phase I: cytochrome P450 enzymes
A superfamily of related enzymes that add on or
uncover small polar groups (–OH, –NH2, –COOH) to increase water solubility
تختلف النظم األنزمة المسإولة عن التحول األحائ ومكن تقسمها إلى أقسام
P-450حث حتل الستوكروم اإلنزمات المكروسومة
الدور المحوري للعملة والت تحفز بشكل أساس تفاعالت األكسدة أو االقتران
االنزمات الغرمكروسومة الت تحفز بعض التحلل المائ واإلقتران
50

Metabolism
Phase II: conjugative enzymes
Mediated by various non-P450
liver enzymes
• covalently add large, polar,
endogenous molecules to Phase I metabolite
• ensures that metabolite is ready for excretion
(glucuronide, glutathione, sulfate,
acetate, amino acids etc)
51

Metabolism
P450 enzyme induction and inhibition • some P450 enzymes can be induced or inhibited by
other drugs, foods, pregnancy or disease
هناك العدد من المواد الت مكن أن تعمل كمعززات إنزمة أو مثبطات
Inducers زادة النشاط االستقالب لألنزمات
(ex: alcohol)
Inhibition: تقلل النشاط االستقالب لألنزمات
(ex: grapefruit juice)
- Primary cause of drug interactions
- Requires drug dosing to be increased or decreased
52

Metabolism
P450 enzyme induction and inhibition
Enzyme inhibition
• Other drugs
• Combination drugs
• Liver disease
• Impaired blood circulation in person with heart disease
• Infant with immature livers
53

Metabolism
Oral route is variable
54

Half-life (T1/2) عمر النصف الحوي
• Serum half-life or elimination half-life is the time it takes the serum concentration of the drug to reach 50% of the administered dose
• A measure of the rate at which drugs are removed from the body
٪ 50هو الوقت الذي ستغرقه تركز الدواء ف الدم للوصول إلى •
لماذا هذا مهم؟انه مقاس سرعة إزالة األدوة من الجسم•
تطلب دواء بنصف عمر قصر جرعات أكثر تكرار•
تطلب دواء بنصف عمر طول جرعات أقل تكرارا•
55

Half-life (T1/2) عمر النصف الحوي
نصف عمر الدواء عوامل تزد
تضاإل تدفق الدم الكلوي أو الكبدي•
امراض الكلى•
ة• مرض كبدي أو مثبطات إنزمة كبد
عوامل تنقص نصف عمر الدواء
تدفق الدم الكبدي•
نقص االرتباط باأللبومن•
تحفز او تسرع االستقالب•
56
Excretionازالة االدوة
57
ا :تختلف طرق التخلص من الدواء ولكن بعضها لعب دورا أساس البول. 1 البراز. 2 استنفاد الهواء. 3
العرق/ الحلب . 4
البول هو الوسلة الرئسة للتخلص من المستقلبات الدوائة المعدلة بالكبد •الدواء عند وصول المادة الصفراوة الت تحتوي من تعتبر البراز مهمة للتخلص•
ا عن طرق دخول الدورة الدموة على مستقلبات دوائة مكن إعادة امتصاصها جزئ
، وف جزء منها تم طرحها ف البرازEnterohepatic circulationالكبدة
Excretionازالة االدوة
58
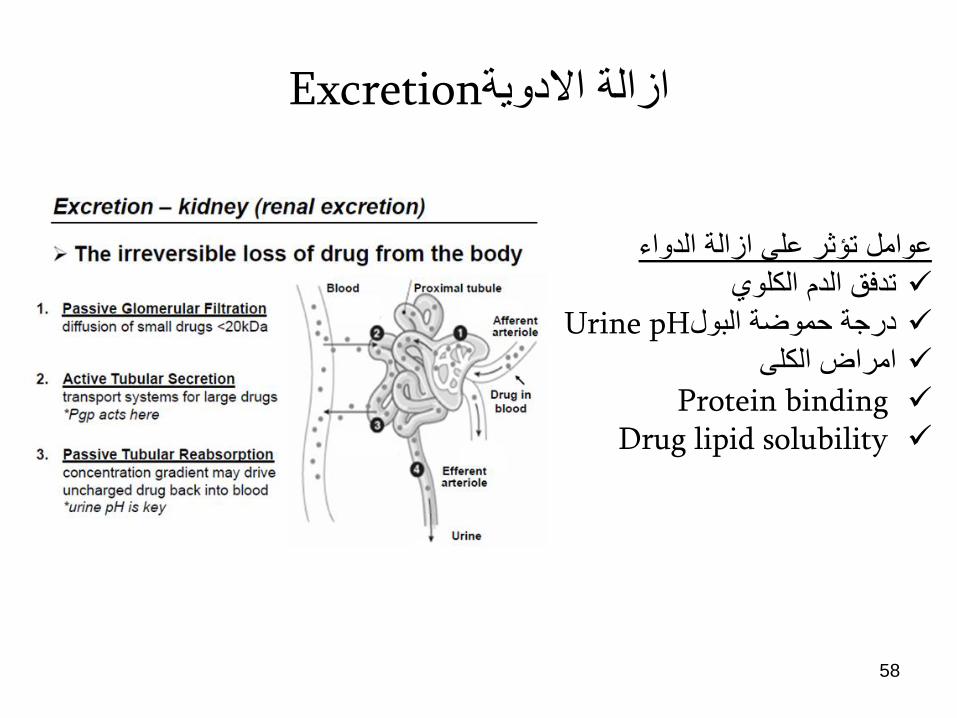
عوامل تإثر على ازالة الدواء تدفق الدم الكلوي درجة حموضة البول Urine pH امراض الكلى Protein binding Drug lipid solubility

Onset, Peak, and Duration
59
Onsetالبداةالوقت الذي ستغرقه الدواء الستنباط استجابة
عالجة Peak القمة
الوقت الذي ستغرقه الدواء للوصول إلى
أقصى استجاباته العالجةالزمنة المدة Duration
الوقت الذي كون فه تركز الدواء كافا
للحصول على استجابة عالجة

How does the drug know where to go?
1)drug circulates throughout bodyin the blood
2)encounters receptors for which it has affinity
3)Binds
4) pharmacological response
60
Pharmacodynamics الدنامكة الدوائة
تهتم الدنامكات الدوائة بتحلل العملات الت رتبط بها الدواء بالمستقبالت ، واألحداث الجزئة الت تلها
.وأخرا التؤثرات البولوجة الناتجة عنها على الفرد
“What the drug does to the body”.
ما فعله الدواء للجسم
61

Pharmacodynamics:
Mechanisms of Action of Drugs • Receptor interaction
• Enzyme interaction
• Nonspecific
interactions
62
مثل التفاعل على المستوى الخلوي
بن الدواء ومكونات خلوة ، مثل
بروتنات غشاء الخلة ، أو اإلنزمات ،
.أو المستقبالت ، عمل الدواء
مكن للدواء تعدل وظفة الخلة أو سرعة اداء الوظفة ، ولكن ال
مكن له خلق وظفة جددة للخلة أو لألنسجة المستهدفة

Pharmacodynamics:
Simplification of drug mechanisms (action)
Drug
Receptor Drug – receptor complex
Biologic alteration
Pharmacologic effect(s)
63

Pharmacodynamics:
• What are receptors?
• Receptors are located on the surface of or within cells
64

Pharmacodynamics:
• There are 4 main classes of receptors
Intracellular phosphorylation
Change in membrane potential or [ion]
Intracellular 2nd messengers
Altered transcription
INTRACELLULAR EFFECTS
PHARMACOLOGIC EFFECTS 65
Pharmacodynamics:
• What binds to the receptors?
• Most receptors have naturally occurring (endogenous) molecules that bind to them
• Exogenous (foreign( molecules can be designed to bind to the same receptor rational drug design
Example ~ Endorphins (endogenous)
Morphine (exogenous) Bind opiate receptors
in brain
66
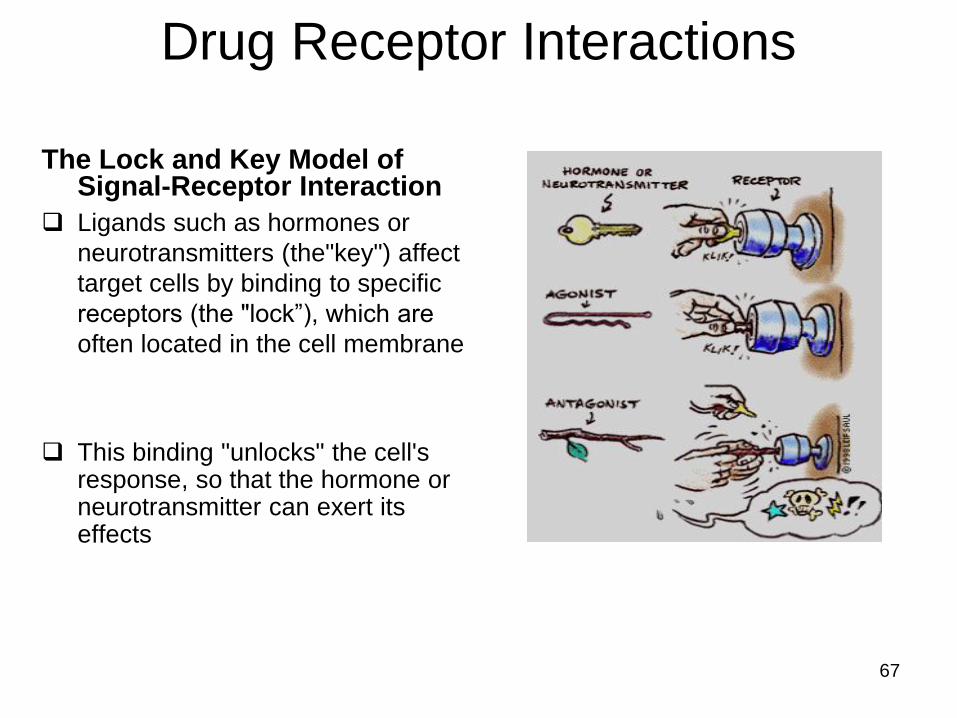
The Lock and Key Model of Signal-Receptor Interaction
Ligands such as hormones or
neurotransmitters (the"key") affect
target cells by binding to specific
receptors (the "lock”), which are
often located in the cell membrane
This binding "unlocks" the cell's response, so that the hormone or neurotransmitter can exert its effects
Drug Receptor Interactions
67

Drug Receptor Interactions
1) Drugs can be Agonist
“A chemical messenger that binds to a receptor and triggers the cell’s
response
AGONISTS have:
1. AFFINITY for the receptor (they bind to it)
2. INTRINSIC ACTIVITY (binding elicits a response)
Agonists can be either
1. Endogenous (ex: adrenalin)
2. Exogenous (ex: dobutamine) Both rate
68

Drug Receptor Interactions
2) Drugs can be Antagonist (receptor blockers or inhibitors)
"A molecule that competes for a receptor with a chemical messenger normally
present in the body.
1. have AFFINITY (bind the receptor)
2. LACK intrinsic activity (no response)
The antagonist binds to the receptor but does not trigger the cell’s response”
69

Drug Receptor Interactions
Antagonist example
Claritin®: an antagonist that blocks histamine receptors
→ allergy treatment
70

Pharmacodynamics:
• An exception to the rule • a few drugs work via non-receptor mechanisms, for example:
Antacids - purely chemical basis via acid
neutralization in the stomach
Osmotic diuretics - promote urine
excretion by altering water flow in the
kidney independent of receptors
71

Important implications of drug-receptor interaction
drugs can potentially alter rate of any body/brain function
drugs cannot impart entirely new functions to cells
drugs do not create effects, only modify ongoing ones
drugs can allow for effects outside of normal physiological range
72
الدواء مكن أن غر سرعة اداء أي وظفة ف الجسم
ال مكن لألدوة خلق وظائف جددة تماما
للخالا ال تخلق االدوة آثارا جددة ، بل تعدلها فقط
مكن لألدوة أن تنتج تؤثرات خارج نطاق
الفسولوجة الطبعة

Pharmacologic effects – side effects
“A drug without side effects isn’t really a drug”
Side Effects/Adverse Effects
Mild, tolerable, subside on their own
(ex: GI disturbances)
Potentially life threatening & sustained
(ex: seizures)
Risks vs benefits must be carefully weighed → Therapeutic Index
73
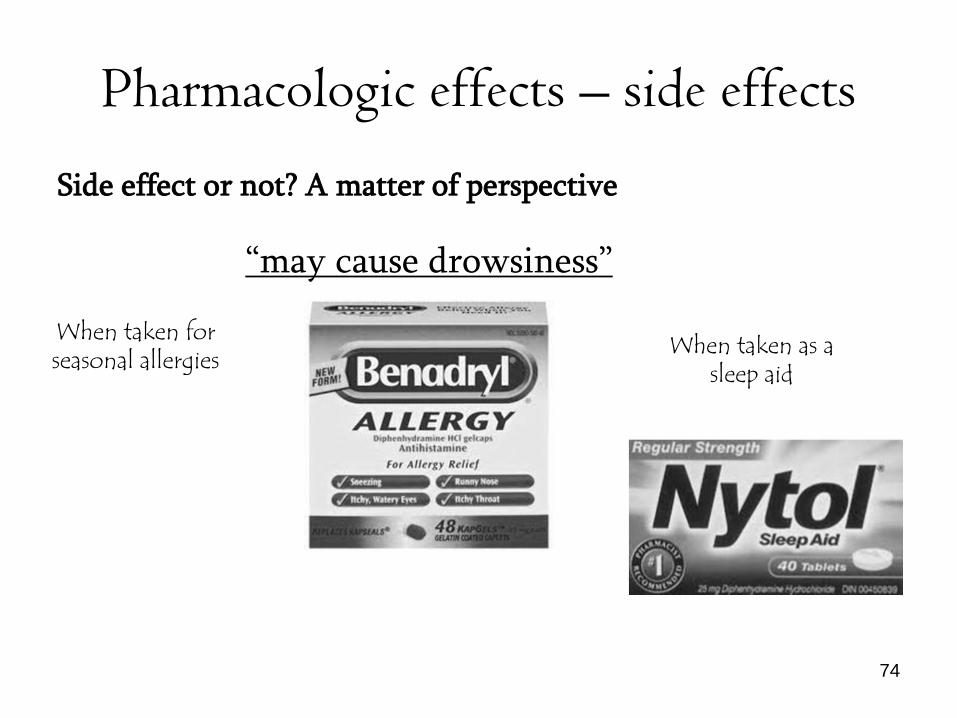
Pharmacologic effects – side effects
Side effect or not? A matter of perspective
“may cause drowsiness”
When taken for seasonal allergies
When taken as a sleep aid
74
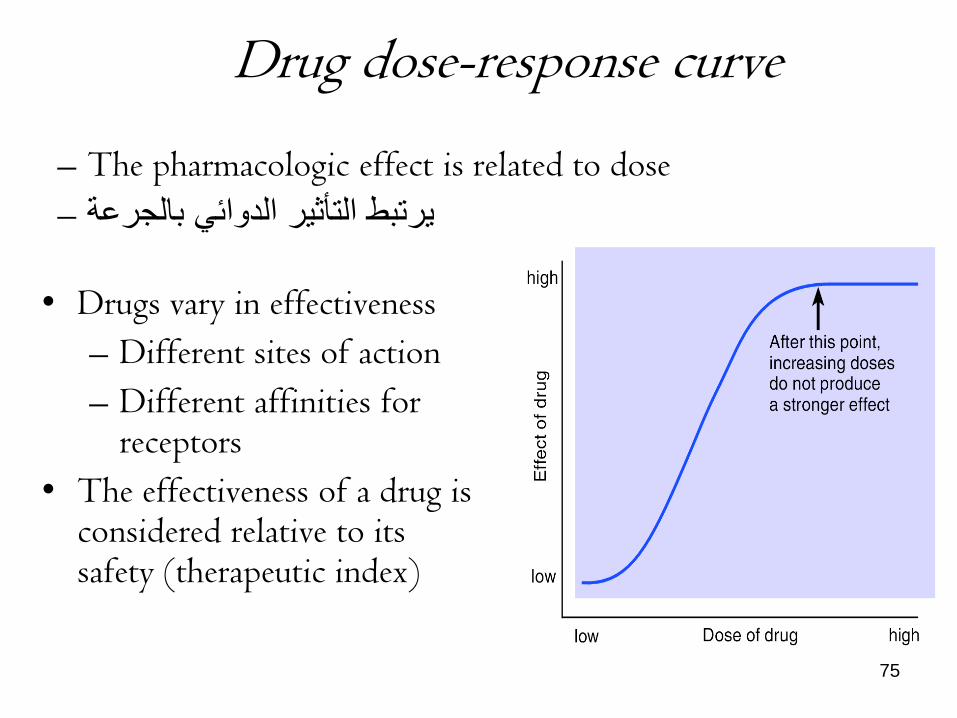
Drug dose-response curve
• Drugs vary in effectiveness
– Different sites of action
– Different affinities for receptors
• The effectiveness of a drug is considered relative to its safety (therapeutic index)
– The pharmacologic effect is related to dose
– رتبط التؤثر الدوائ بالجرعة
75

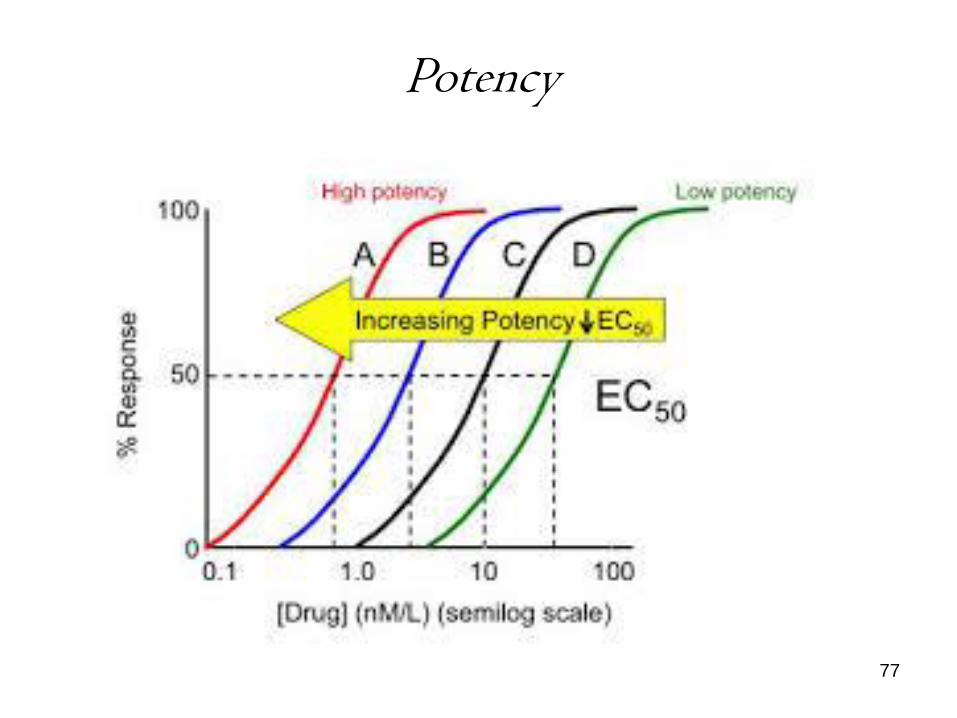
Potency • Relative strength of response
for a given dose
– Effective concentration
(EC50) is the concentration
of an agonist needed to
elicit half of the maximum
biological response of the
agonist
– The potency of an agonist
is inversely related to its
EC50 value
• D-R curve shifts left with
greater potency
76
الجرعة الفعالة ه مقاس لكمة الدواء المطلوبة إلنتاج تؤثر
بحجم معن
الدواء الى السار تمتع بقدر أكبر من الفعالة
Potency
77

Efficacy
• Maximum possible effect Emax
• Indicated by peak of D-R curve
أقصى تؤثر فزولوج ناتج عن تفاعل الدواء
والمستقبل
78

Efficacy
79
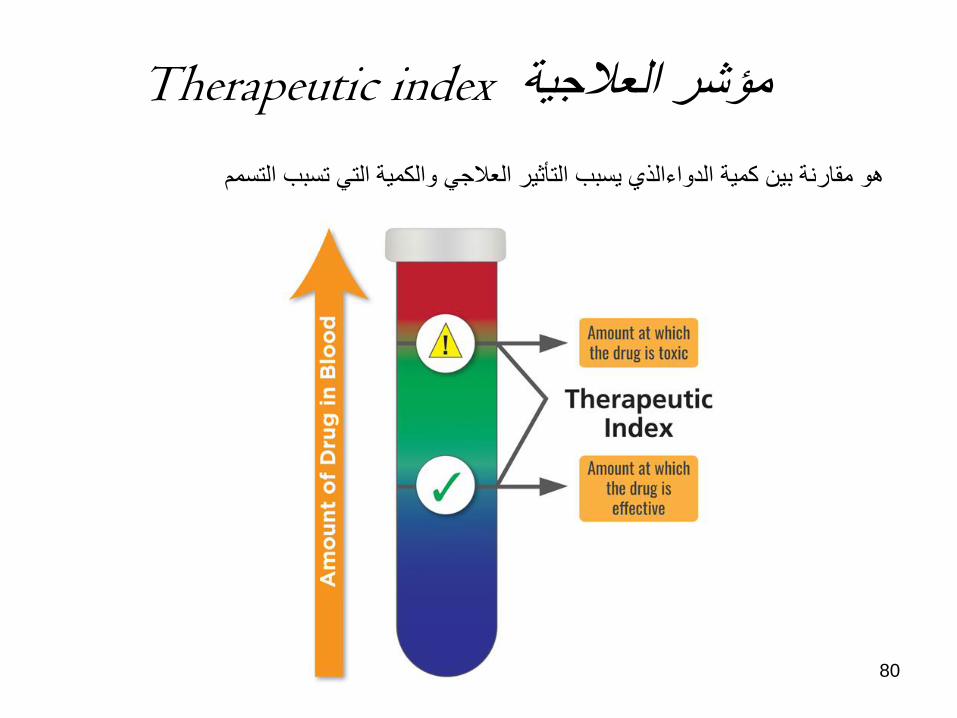
Therapeutic index مإشر العالجة
هو مقارنة بن كمة الدواءالذي سبب التؤثر العالج والكمة الت تسبب التسمم
ED50
80
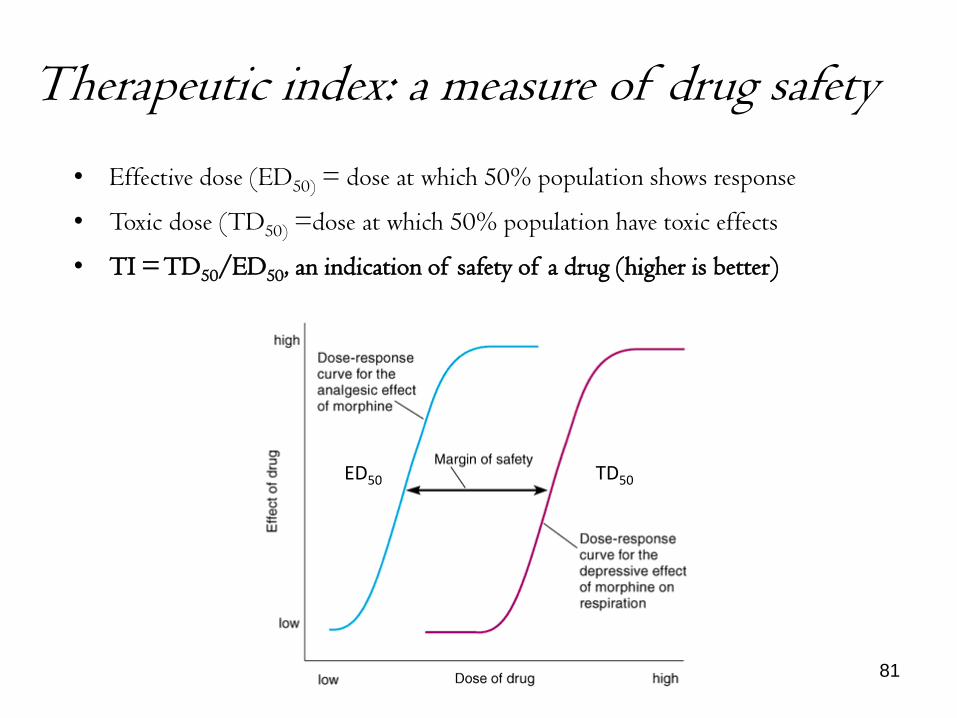
Therapeutic index: a measure of drug safety
• Effective dose (ED50) = dose at which 50% population shows response
• Toxic dose (TD50) =dose at which 50% population have toxic effects
• TI = TD50/ED50, an indication of safety of a drug (higher is better)
ED50 TD50
81

Therapeutic index: a measure of drug safety
Narrow TI Drugs • Digoxin • Lithium
• Phenobarbital • Vancomycin
• Warfarin
82
جب مراقبة تركز هذه األدوة ف الدم دائما
لتجنب التؤثرات السامة

Tolerance (desensitization)
• Decreased response to same dose with
repeated (constant) exposure
• Right-ward shift of D-R curve
• Sometimes occurs in an acute dose
(e.g. alcohol)
• Can develop across drugs (cross-
tolerance)
• Ex Diazepam, Morphine,
83

Mechanisms of Tolerance
• Pharmacokinetic
– changes in drug availability at site of action (decreased
bioavailability)
– Decreased absorption
– Increased binding to depot sites
• Pharmacodynamic
– Changes in drug-receptor interaction
– Down regulation of receptors
84

Sensitization
• Increased response to same dose with
repeated exposure
• or less drug needed to achieve same
effect
• Left-ward shift in D-R curve
• Sometimes occurs in an acute dose
(e.g. amphetamine)
• Can develop across drugs (cross-
sensitization)
85

• Pharmacokinetic and pharmacodynamic
– With pharmacokinetic drug interactions, one drug
affects the absorption, distribution, metabolism, or
excretion of another.
– With pharmacodynamic drug interactions, two drugs
have interactive effects in the brain.
– In terms of efficacy, there can be several types of
interactions between medications: additive, synergistic,
and antagonistic.
Drug-drug Interactions
86

Response
Hi
Lo
Time
A B
Additive Effects
A + B
The effect of two chemicals is equal to the sum of the effect of the two chemicals taken separately, eg., aspirin and motrin.
87

Response
Hi
Lo
Time
A B
A + B
Synergistic Effects
The effect of two chemicals taken together is greater than the sum of their separate effect at the same doses, e.g., alcohol and other drugs
88

Response
Hi
Lo
Time
A B
A + B
Antagonistic Effects
The effect of two chemicals taken together is less than the sum of their separate effect at the same doses ex NSAD with ACE inhibitors
89

• Variables that effect drug action
• Dosage of the drug refers to frequency, size, and
number of doses
• Route of administration does affect drug action
and client response
• Food
• Client Variables
-Age
-Gender
-Medical conditions
90
Drug – Diet interaction
• Food can slow absorption
• Food substances can react with certain drugs
• How to give medication is information
provided in your drug manual
91

92

















