Freedom Health PlansWhen it comes to health insurance, you want choice, value and dependability. Freedom Health Plans offer four quality options, including an HSA-qualified high-deductible health plan. This brochure must be accompanied by insert IHCHS 041 0609EH. IHCHS 539 0111 .org The IHC Group is an insurance organization composed of Independence Holding Company (NYSE: IHC) and its operating subsidiaries. The IHC Group has been providing life, health and stop-loss insurance solutions for over 25 years. For information about The IHC Group, visit www.ihcgroup.com. The Freedom Health Plans are available only to members of Communicating for America, Inc. Membership is optional for residents of Kansas and Montana. The Freedom Health Plans are underwritten by Companion Life Insurance Company. Companion Life is not a member of The IHC Group. January 2011 EH online only
Freedom Health Plans When it comes to health insurance, you want choice, value and dependability.
Freedom Health Plans offer four quality options, including anHSA-qualified high-deductible health plan.
This brochure must be accompanied by insert IHCHS 041 0609EH.
IHCHS 539 0111
.org
The IHC Group is an insurance organization composedof Independence Holding Company (NYSE: IHC) andits operating subsidiaries. The IHC Group has beenproviding life, health and stop-loss insurance solutionsfor over 25 years. For information about The IHC Groupvisit www.ihcgroup.com .
The Freedom Health Plans are available only to membeof Communicating for America, Inc. Membership isoptional for residents of Kansas and Montana.
The Freedom Health Plans are underwritten byCompanion Life Insurance Company. Companion Life
24-hour coverageCoverage is available 24 hours per day and includes work-related injuries or illnesses, unless those charges arecovered by workers’ compensation or you are required by law to be covered by workers’ compensation.
Air, water and land ambulanceCoverage includes ambulance services by air, water and land subject to the plan deductible and coinsurance.
Waiver of pre-existing condition limitationIf you fully disclose an existing medical condition on the application that is not specifically excluded fromcoverage, the Freedom Health Plan will consider a claim for that condition without applying the pre-existingcondition limitation.
Generation to generationCovered dependents have the option to purchase their own similar plan, regardless of their health history, whenthey reach 26 years of age or when they can no longer be considered a dependent on your plan. If your childdevelops a chronic condition, this important benefit will allow him or her to keep their health insurance coverage.
Centers of Excellence for transplant servicesAll plans include access to a national Center of Excellence network for organ transplants. This specialized networkconsists of top-rated providers in terms of the number of specific transplants performed and their success rates.The network ensures that if you need these services, you receive the highest level of care through expertise,patient advocacy and care management.
All Freedom Health Plans allow you to choose your health care providers. However, benefits are paid differentlybased on your selection of either a PPO plan or a traditional indemnity plan.
PPO plansOffice visit copays and negotiated discounts are available through PPO network plans. Because Freedom HealthPlans offer more than 50 PPO networks nationwide, you can choose a network in your area that includes yourphysicians and hospitals. Network providers have agreed to offer services at a reduced or discounted price.You realize these savings through a lower monthly premium, higher benefits and reduced out-of-pocket costs.
Forced providers – Certain providers such as radiologists, pathologists, anesthesiologists and assistantsurgeons may have relationships with network facilities but have chosen not to join the network.
Understanding that you are not always able to select these providers when admitted to an in-networkhospital, the Freedom Health Plan will consider charges for these “forced providers” at the in-networkbenefit level. Covered charges will be based on reasonable and customary charges, if both the hospitaland admitting physician participate in your selected PPO network.
Emergency care – If emergency medical attention is needed, you can receive care without worryingabout finding an in-network provider. Charges resulting from emergency services received from anout-of-network provider will be considered in-network. Transfer to an in-network facility or providermust be arranged within 48 hours or as soon as the transfer can take place without detriment toyour health.
Traditional plansOffering the greatest freedom in provider choice, traditional indemnity plans allow you to visit any health careprovider without network restrictions. While benefits are not subject to different in-network or out-of-networklimits, covered charges are subject to a reasonable and customary amount. The reasonable and customaryamount is determined by the typical amount charged for a certain procedure within a geographic area. If theamount charged for a covered service is above the reasonable and customary amount, you are responsible forthe excess charges.
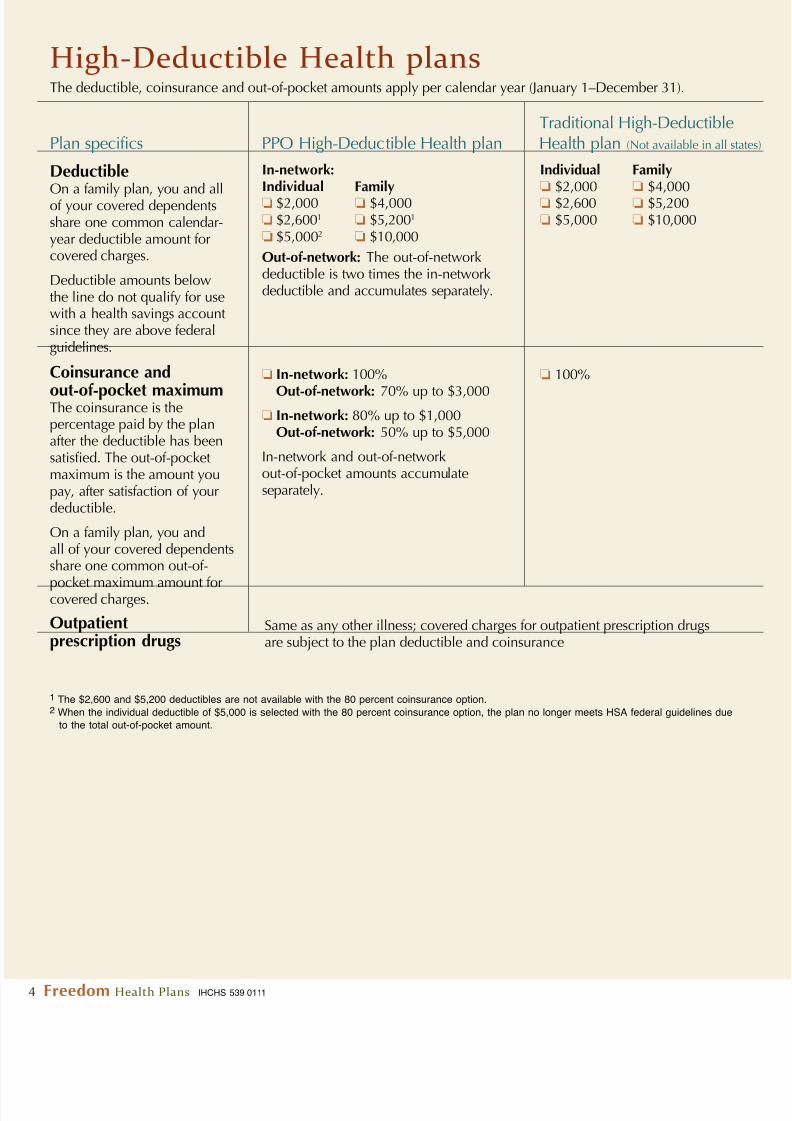
High-Deductible Health plansThe deductible, coinsurance and out-of-pocket amounts apply per calendar year (January 1–December 31).
Traditional High-DeductiblePlan specifics PPO High-Deductible Health plan Health plan (Not available in all sta
1 The $2,600 and $5,200 deductibles are not available with the 80 percent coinsurance option.2 When the individual deductible of $5,000 is selected with the 80 percent coinsurance option, the plan no longer meets HSA federal guidelines due
to the total out-of-pocket amount.
Deductible
On a family plan, you and allof your covered dependentsshare one common calendar-year deductible amount forcovered charges.
Deductible amounts belowthe line do not qualify for usewith a health savings accountsince they are above federalguidelines.
Coinsurance and
out-of-pocket maximumThe coinsurance is thepercentage paid by the planafter the deductible has beensatisfied. The out-of-pocketmaximum is the amount youpay, after satisfaction of yourdeductible.
On a family plan, you andall of your covered dependentsshare one common out-of-
Choice and Traditional plansThe deductible, coinsurance and out-of-pocket amounts apply per calendar year (January 1–December 31).
Plan specifics Choice PPO Traditional (Not available in all states
Physician office copayAfter copay, plan covers100 percent of the coveredcharges for in-network physician
office visits including: examination,consultation and minor officesurgery. Diagnostic tests, laband X-rays are subject to theplan deductible and coinsurance.Copays do not accumulate towardsatisfaction of your deductibleor out-of-pocket maximum.
DeductibleThe family deductible is amaximum of three individualdeductible amounts.
Coinsurance andout-of-pocket maximumThe coinsurance is thepercentage paid by the plan afterthe deductible has been satisfied.The out-of-pocket maximum isthe amount you pay, aftersatisfaction of your deductible.
Hospital or skilled nursingdeductible,1 per confinement
Emergency roomdeductible,1 per visit
Outpatient prescriptiondrugs
$100(Waived if admitted to the hospital immediately following emergency room visit.)
$250 deductible* then $15 copay for generic drugs or $25 copay and80% coinsurance for brand name drugs* Maximum of three prescription deductibles per family, per calendar year. This deductible does notaccumulate toward satisfaction of the plan deductible or out-of-pocket maximums.
1 Confinement and emergency room deductibles do not accumulate toward satisfaction of the plan deductible or out-of-pocket maximum.
No copay; covered charges aresubject to the plan deductibleand coinsurance
❏ $2,500
❏ $5,000
70% to $6,000
$250
In-network:$25Out-of-network: Covered charges aresubject to the out-of-network deductibleand coinsurance
In-network:❏ $1,500❏ $2,500❏ $5,000❏ $10,000
The out-of-network deductible is twotimes the in-network deductible andaccumulates separately.
In accordance with the Patient Protection and Affordable Care Act, the Freedom Health Plan will cover preventiveservices rated with an “A” or “B” by the United States Preventive Services Task Force (USPSTF). For an updated list of
covered services visit www.uspreventiveservicestaskforce.org.For PPO plans, in-network covered preventive services are paid at 100 percent with no required copay, deductible orcoinsurance. Out-of-network preventive services are not covered.
For traditional plans, covered preventive services are paid at 100 percent with no required deductible or coinsurance.
Optional benefits
Outpatient supplemental accident coverageAccidents happen, even to the most careful. Additional first dollar coverage is available through this optional accidentbenefit. Select one of three benefit amounts for coverage of an accident that is treated within 72 hours, on anoutpatient basis. Follow-up care is also included for up to 90 days. This benefit is available for an unlimited numberof covered accidents.
Benefit amount per accident Deductible* per accident ❏ $500 $50 ❏ $1,000 $50 ❏ $2,000 $150
* Deductible does not accumulate toward satisfaction of the plan deductible or out-of-pocket maximum.
Term Life InsuranceLife insurance is available in increments of $10,000 up to a total of $50,000. This life insurance benefit is payable aslong as the Freedom Health Plan is inforce at the time of death. Protect your family with the funds to maintain theirlifestyle and continue their health insurance coverage. (Life insurance is not available to residents of Kansas.)
Limited benefitsBenefits listed below apply per covered person.
Non-surgical back treatment (including chiropractic care)Covered charges for non-surgical back treatment are payable up to 10 visits per calendar year and are subject toyour medical plan deductible and coinsurance.
Skilled nursing facility careAfter your deductible has been satisfied, covered medical charges will be paid at the coinsurance level up to amaximum of $100 per day.
Home health careCovered charges are payable up to a maximum of 21 visits per calendar year, subject to your medical plandeductible and coinsurance.
Hospice careAfter your deductible has been satisfied, covered medical charges for hospice care will be paid at 100 percent forup to six months. The plan will also cover bereavement support services for the insured person’s family during thethree-month period following death, up to $250.
Mental, nervous and chemical dependency disorders Outpatient mental, nervous and chemical dependencyMaximum benefit of $25 per visit, subject to your medical plan deductible and coinsurance. Outpatientdetoxification services and supplies are not covered.
Inpatient mental, nervous and chemical dependencyMaximum benefit of $250 per day subject to your medical plan deductible and coinsurance. For inpatienchemical dependency, benefits are limited to inpatient detoxification in connection with a therapyprogram and rehabilitative services.
Organ transplants If a Center of Excellence is utilized:
Covered transplant charges are subject to the plan’s calendar-year maximum of $2,000,000. Also, atravel expense allowance is included for up to $5,000 for one companion, or two companions if theinsured is a minor.
If a Center of Excellence is not utilized:Covered organ transplant services are subject to a maximum benefit of $250,000 per transplant.
Important information about your planPre-certification requirementsThe plan requires that the followingservices and supplies be pre-certified:• all proposed inpatient hospital
confinements• all proposed stays in an extended care
or skilled care nursing facility• all proposed home health services• all proposed hospice services• complications of pregnancy (must be
pre-certified within seven days of diagnosis)
For the Choice PPO plan and theTraditional plan:• prescription drug orders for growth
hormones, immunosuppressants, AZTor HIV antiretroviral medication, “off label” use, orphan drugs, investigativenew drugs and Group C cancer drugs.
• outpatient prescription drugs thatrequire pre-certification are also
subject to the pre-existing conditionlimitation. See the certificate for fulldetails.
In non-emergency situations you mustcontact the pre-certification serviceat least seven days before incurringexpenses on account of any of theabove occurrences. You simply call thepre-certification service listed on yourhealth plan identification card. They willcontact your physician for any necessaryadditional information. In an emergency,you should go directly to the hospital to
receive immediate care. If you are thenadmitted as an inpatient in the hospital,you must contact the pre-certificationservice within 48 hours of admission,or as soon as reasonably possible. Yourphysician must verify that an emergencyexisted.
If you do not pre-certify an inpatienthospital stay as outlined above orcomplications of pregnancy, you will beresponsible for up to an additional $500deductible per occurrence. If you donot pre-certify any of the medicationslisted above, then no benefits arepayable toward their cost. If you followpre-certification requirements, theseadditional deductible amounts will bewaived.
Definition of apre-existing conditionA pre-existing condition means abodily injury or sickness for which theindividual received medical treatment(including the taking of medicineprescribed by a physician), advice orconsultation, or which produced distinct
symptoms that would have causedan ordinarily prudent person to seekmedical diagnosis or treatment duringthe 12 months immediately precedingthe effective date of the coveredperson’s insurance.
Coordination of benefits
Coordination of benefit (“COB”) appliesto the plan when an insured or theinsured’s covered dependent has healthcare coverage under more than oneplan. If the COB provision applies, theorder of benefit determination rulesshould be looked at first according tothe policy. The rules state whether theplan is a primary plan or secondaryplan as to another plan covering theperson. When the plan is a primaryplan, its benefits are determined beforethose of the other plan and withoutconsidering the other plan’s benefits.
When the plan is a secondary plan,its benefits are determined after thoseof the other plan and may be reducedbecause of the other plan’s benefits.With respect to covered personswho are eligible for coverage underMedicare, a benefit otherwise payableunder the policy shall be reduced bythe amount of any similar Medicarebenefit so that the total reimbursementswith respect to an insured personor his eligible dependents shall notexceed 100 percent of such person’sapproved Medicare expenses otherwisereimbursable under the policy.
Dependent coverageEligible dependents include an insured’sspouse and all children from birth toage 26. Coverage will not terminatefor a child who is or becomes, priorto the date insurance would normallyterminate, mentally retarded orphysically handicapped to the extentthat the child is unable to maintain self-sustaining employment and remainschiefly dependent upon the insured forsupport, provided satisfactory proof of
such dependent’s capacity is submittedto the company not later than 31 daysafter attainment of the limiting age.
Termination of insuranceCoverage will terminate on the earliestof the following:
1. The date of termination of the policy;
2. The next premium due date after thecompany receives written request toterminate coverage of the insuredperson under the policy;
3. The last premium due date prior to agrace period, if the premium then dueis not paid within the grace period;
4. The date the insured person has beendetermined by the company to havecommitted an act of fraud or made anintentional misrepresentation of
material fact under the terms of thepolicy;
5. The first date following 90 daysadvance written notice by thecompany to the insured when thecompany may lawfully discontinueoffering coverage under the policyin the state where the certificatewas issued;
6. The first date following 180 daysadvance written notice by thecompany to the insured whenthe company may lawfully
discontinue offering all healthinsurance coverage in the individualmarket in the state were the certificatewas issued;
7. The date the coverage is determinedto be a small employer health planpursuant to governing law; or
8. The date of the insured’s death.
Covered chargesMeans expenses for medical servicesand supplies actually incurred as aresult of a bodily injury or sickness by
or on behalf of a covered person whilecoverage under the policy is inforcewith respect to such covered person andwhich:
1. are medically necessary for thetreatment of a bodily injury orsickness and which have beenrecommended and prescribed bya physician;
2. are not in excess of the necessary,reasonable and customary chargesmade for the services performed ormaterials furnished, or are not inexcess of such charges as would havebeen made in the absence of thisinsurance;
3. are not excluded from coverage bythe terms of the policy; and
4. do not exceed any amounts payableunder the terms of the policy.
Rate guaranteeInitial monthly premiums are based onseveral factors, including age, spouse’sage (if applicable), the number of children covered under the plan, andhome address.
The company guarantees that rateswill not change for the initial 12months of coverage from the insured’s
effective date unless one or more of thefollowing events occur during that time:• A move to a new residence by the
insured• You change your benefit options• The number of covered dependents
changes
PremiumThe rates used to determine the initialpremiums due under the policy willbe the company’s published rates.Premiums are payable to the companyor its authorized administrator.
Premiums will be determined by, butnot limited to, such factors as the tableof premiums and applicable fees thenin effect and by the current attainedage, place of residence, and experienceclass of the covered persons.
The company reserves the right tochange premiums, on a class basis,under the coverage on any premiumdue date by giving the insured at least31 days prior written notice.
No benefits shall be payable under thepolicy for (may vary by state):
1. Expenses incurred by or for acovered person in connectionwith a pre-existing condition for12 months after the effective dateas shown on the validation pagefor that covered person. No claimfor covered charges incurred morethan 12 months after a coveredperson’s effective date will bereduced or denied solely on thegrounds that the charge is due toa pre-existing condition, unless thecondition is excluded or limited
by name or specific description inan amendatory endorsement that isattached to the certificate. Thislimitation shall not apply to adependent child who is adoptedor placed for adoption before age18; however, expenses incurredbefore adoption or placement foradoption will not be covered.
2. Any confinement, treatment, service,supply or prescription which is: (a)not necessitated by a bodily injury orsickness, (b) not authorized by aphysician; (c) not medicallynecessary; (d) not necessary,reasonable, and customary; or (e) notincurred while coverage is inforce.
3. Pregnancy, including freestanding
birthing center services, certifiednurse midwives, certified nurseanesthesiologist, midwives licensedpursuant to state law and statelicensed birth centers.
4. Experimental or investigationalmedical treatment.
5. Voluntary abortions.
6. Bodily injury or sickness whicharises out of or in the course of any employment for wage or profitfor any person required to becovered under any workers’
compensation law.
7. Any confinement, treatment, serviceor supply provided by a governmentowned or operated facility, unless thecovered person is legally required topay the charges incurred.
8. Bodily injury or sickness resultingfrom war or any act of war (declaredor undeclared).
9. Charges incurred while on activeduty with any military, naval or airforce of any country or international
organization.10. Newborn nursery care.
11. Routine well-baby care, unlessthe service is rated with an “A” or“B” by the United States PreventiveServices Task Force.
12. Services and supplies for treatmentof: (a) the teeth; and (b) the gumsother than for tumors; and (c) anyother associated structuresprimarily in connection withthe treatment or replacement
of natural teeth; and (d) preventionor correction of teeth irregularitiesand malocclusion of jaws by wireappliances, braces or othermechanical aids, unless due to aninjury which occurs while coveredunder the policy to sound naturalteeth, provided that such treatmentis received within 90 days followingthe date of injury.
13. Treatment or surgery as the result of prognathism, retrognathism,micrognathism, or any treatment
or surgery to reposition the maxilla(upper jaw), mandible (lower jaw),or both maxilla and mandible,unless due to an injury, whichoccurs while covered under thepolicy to sound natural teeth,provided that such treatmentis received within 90 daysfollowing the date of injury.
14. Charges for treatment of temporo-mandibular joint (TMJ) dysfunction
15. Services or supplies to improve theappearance or self perception of acovered person, which does notrestore a bodily function, includingwithout limitation; cosmetic orplastic surgery, hair loss; or skinwrinkling.
16. Routine eye exams, glasses, visualtherapy, or contact lenses, exceptfor the first pair of glasses or lensesfor use after cataract surgery.
17. Hearing aids or the fitting thereof.
18. Charges incurred as a result of participation in a riot orinsurrection or the commission of a felony or while imprisoned.
19. Charges for radial keratotomy andradial keratectomy or othersimilar procedures, includinglaser-based procedures, that areperformed on the eyes.
20. Meridian therapy (acupuncture),except when used in lieu of an
anesthetic.21. Routine physical examinations,
immunizations, use of prophylacticinjections including gamma globu-lins and flu shots, and the well-chilcare including immunizations,unless the service is listed as an “Aor “B” by the United StatesPreventive Services Task Force.
22. Charges for treatment, paring orremoval of corns, calluses ortoenails (other than partial orcomplete removal of nail roots),
except when prescribed by anattending physician who istreating the covered person for ametabolic disease, such as diabetemellitus or a peripheral-vasculardisease such as arteriosclerosis,or treatment of the feet by postingor strapping, or range-of-motionstudies, or orthotics.
23. Treatments made in connectionwith obesity or weight reductionincluding wiring of the teeth and aforms of intestinal bypass surgery.
24. Charges for services rendered bya physician, nurse or other providerif such person: (a) is a close relativeof the covered person or (b) livesin the same household as thecovered person, or (c) is theemployer of the covered person,except for charges rendered while ahospital inpatient.
25. Charges incurred as the result of attempted suicide or intentionallyself-inflicted bodily injury orsickness while sane or insane.
26. Treatment for mental, nervous orchemical dependency disorders,except as provided under theLimited Major Medical benefitssection of the policy.
27. Charges related to or inconnection with: (a) proceduresto restore or enhance fertility; and(b) reversal of sterilization; (c) penile
implants; and (d) fertility andsterility studies.
28. Impregnation techniques such as:(a) artificial insemination, or (b)in vitro fertilization, including butnot limited to: artificialinsemination; in vitro fertilization,in vitro zygote, intrafallopiantransfers, gamete intrafallopiantransfer; genetic counseling; and allrelated charges.
29. Hospital and physician charges forweekend hospital admissions
occurring between noon on anyFriday and noon the followingSunday for non-emergencyprocedures, unless medicallynecessary or unless surgery isscheduled for the next day.
30. Congenital conditions, except withrespect to children covered frombirth.
31. Sexual reassignments or sexualdysfunctions or inadequacies.
32. Custodial care, regardless of whom
prescribes or renders such care.33. Services or supplies for which no
charge is made or for which thecovered person is not required topay.
34. Services received or suppliespurchased outside the United Statesunless the charges are incurredwhile traveling on business or forpleasure not to exceed 90 days,provided the procedure ortreatment is approved for usein the United States.
35. Charges related to or in connectionwith human organ or tissuetransplants or high dosechemotherapy administered inconnection therewith except asprovided under the Limited MajorMedical benefits section of thepolicy.
36. Any education or training materials
including, but not limited to: painmanagement; the managementof asthma, heart disorders and othermedical disorders; prenatalscreening education, unless suchprograms or materials are offeredthrough our health carecoordination in conjunction with adisease management program.
37. Equipment, other than durablemedical equipment, including, butnot limited to: modifications tomotor vehicles or homes such as towheelchair lifts or ramps; water
therapy device, such as whirlpoolsor hot tubs; and exerciseequipment.
38. Any service or supply to eliminateor reduce a dependency or anaddiction to tobacco, including butnot limited to: nicotine withdrawalprograms; nicotine products, suchas transdermal patches and gums;hypnotism or goal-orientedbehavioral modification.
39. Any surgical removal of an organ ortissue unless medically necessary.
40. Treatment for home health careservices, except as provided in theLimited Major Medical benefits.
41. Treatment for hospice care servicesexcept as provided under theLimited Major Medical benefitssection of the policy.
42. Non-surgical back treatment,except as provided under theLimited Major Medical benefitssection of the policy.
43. Any service or supply in connectionwith the implant of an artificialorgan.
44. Personal convenience servicesor supplies including withoutlimitation: beauty or barberservices; radio and television;non-therapeutic massages;telephone charges; take homesupplies and guest meals; andmotel accommodations.
45. For high-deductible health plans:Any non-prescriptive medication or
prescription medication that isdeemed not medically necessary.For the Choice PPO and Traditionalplans: any non-prescriptivemedication.
46. Charges for voice training for a lisp.
47. Breast reduction surgery unlesssuch surgery was performed as partof a mastectomy due to breast
cancer.
48. For Choice PPO and Traditionalplans, outpatient prescription drugexclusions include:
a. Contraceptive devices orinjectables.
b. Over-the-counter drugs andproducts.
c. Fertility agents.d. Sexual performance
enhancement drugs (e.g. Viagra).e. Vitamins (other than prenatal).f. Anti-smoking aids (e.g. Nicorette,
Nicaderm, Habitrol).g. Hair loss medications (e.g.
sera, blood or blood plasma.i. Investigation use or experimental
drugs. j. Any charge for administration of
injectable insulin.k. Drugs covered under workers’
compensation.l. Anorectic drugs for diet control.m. Medication taken, prescribed or
administered while an inpatientat a hospital, rest home,sanitarium, skilled nursing facility,convalescent hospital, nursinghome or similar institution whichoperates a facility for dispensingpharmaceutical drugs.
n. Therapeutic devices orappliances, support garmentsand other non-medicinalsubstances regardless of intendeduse.
o. Homeopathic medications.p. Any drugs purchased outside the
United States of America.q. Any drug which requires
pre-certification, which is notpre-certified as described.
Satisfaction Guaranteed: If you are not completely satised with the health insurance coverage and have not led a claim, youmay return the certicate of coverage within 10 days of your receipt and receive a full premium refund.
The information in this brochure is an outline of the features, plan provisions, benets and other information about the Free-dom Health Plans. Plans offered may be subject to change. This brochure is not intended to serve as legal interpretation of the benets, which are provided under the Master Policy (CLI CH 3000 or CLI CH 3020 PPO) issued to Communicating forAmerica, Inc. in the District of Columbia. The exact provisions governing the insurance contract are contained in the MasterPolicy underwritten by Companion Life Insurance Company, in Columbia, South Carolina. Some provisions, benets, exclusionor limitations may vary depending on your state of residence. Certain terms and conditions apply. Any provision of this policythat is in conict with any applicable federal or state law is hereby amended to meet the minimum requirements of such law.For complete details about the Freedom Health Plans, please refer to the health insurance Certicate of Coverage (CLI CH 3010CERT or CLI CH 3030 PPO CERT).
Applicants should not cancel any existing insurance until they have been notied in writing that their new insurance is in effect
Freedom Health Plans are endorsed by Communicating for America, Inc.