41
Alzheimer’s Disease The Amyloid Theory: Time to Move on. Prepared and Presented by Aly H. Abayazeed, MBchB Neuroradiology Fellow
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | lukas-stain |
| View: | 213 times |
| Download: | 0 times |

Alzheimer’s DiseaseThe Amyloid Theory: Time to
Move on.Prepared and Presented byAly H. Abayazeed, MBchB
Neuroradiology Fellow

What We Will Talk About?
The History.
Why is it important ?
How is it diagnosed clinically ?
What is the role of Radiology ?
What are AD genetics ?
What is the Amyloid Theory and Why is it failing us ?
What’s next and how can Radiology be part of the future ?

The History

The History

The Problem

The Disease
4.5 million in the US.
Incidence doubles every 5 years after age 60.
14 million individuals by 2050.
Most leading cause to nursing home placement.
140 billion dollars/year (health care, nursing home and lost productivity)

The Clinical Diagnosis

The Clinical DiagnosisProgressive dementia.
Early onset or Late onset (95%).
Begins with isolated memory impairment.
Declarative memory domain most profoundly affected early.
Diagnosis: progressive deficit in more than one cognitive domain, usually memory plus another, after other possible causes of dementia have been excluded. “possible” or “probable”.1
1. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’sdisease: report of the NINCDS-ADRDA work group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease.Neurology1984;34:939–944.

Amnestic MCI
Considered to be the earliest form of AD.
Within 5 years about 80% of aMCI convert to AD.
Non-memory MCI syndromes are likely early manifestation of other dementias.

The Radiology Factor

The Amyloid Theory (overview)

The Radiology FactorExclusion
Lymphoma NPH Heubner

The Radiology FactorDiagnostic
Structural
1. Visual Assessment

The Radiology FactorDiagnostic
Structural
2. ROI Tissue Volume Measurement
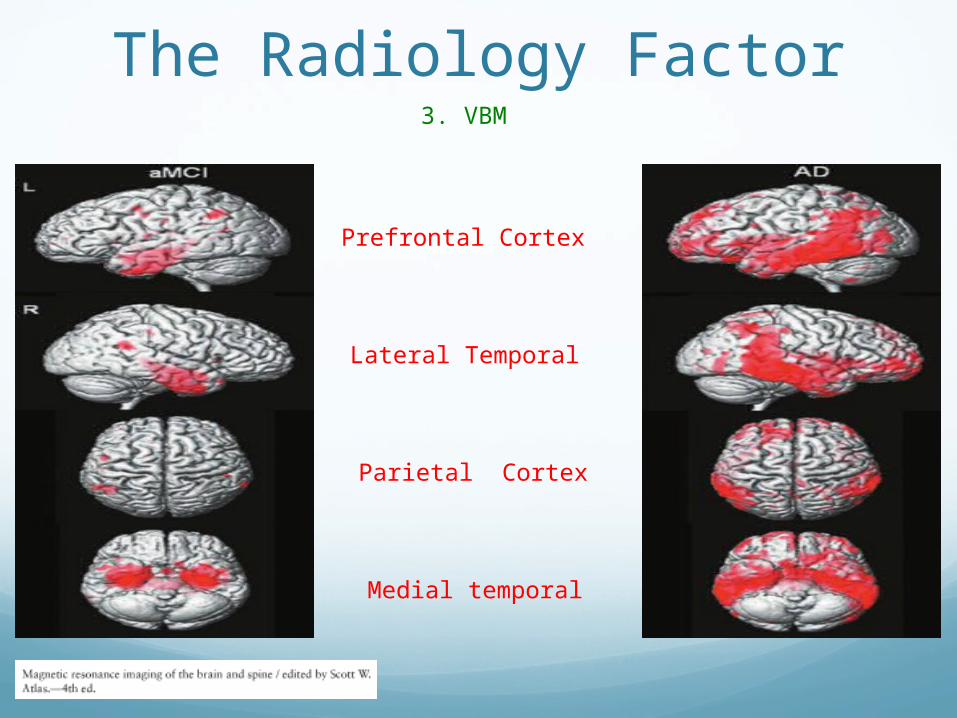
The Radiology Factor3. VBM
Lateral Temporal
Prefrontal Cortex
Parietal Cortex
Medial temporal

MRS: Depressed NAA and Elevated mI.
DTI: Increased ADC of water and Abnormal FA.
MR perfusion: DCE/DSC/more recently ASL modalities. Bilateral temporal parietal decrease in CBF.
fMRI: Task-activation fMRI in aMCI patients, and, Resting state fMRI for AD.
The Radiology Factor
Other Modalities

PIB, most commonly studied. Have a very short half life.
Frontal lobes, posterior cingulate and temporal parietal cortex. Cerebellum is control. 2 positive gyri are considered sufficient for the diagnosis.
Atrophy <−> PIB −> Cognitive decline.1
10-30% Cognitively normal have PIB uptake.
The Radiology FactorAmyloid Imaging

The Radiology Factor

The Radiology Factor

Normal anatomic variation between individuals limits the diagnostic utility of cross-sectional structural MRI obtained at a SINGLE point in time. LONGITUDINAL measures with serial MRIs is of better diagnostic value.
Rates of WHOLE brain atrophy in AD: 1.5 to 3%. Rates of HIPPOCAMPUS atrophy in AD: 4 to 6%
We need to develop automated techniques for GRAY matter VOLUME MEASUREMENTS and apply it to our clinical practice.
MRS: Depressed NAA and elevated mI. fMRI can show INCREASED activity in AD and aMCI patients.
ASL: Might be a helpful tool in the future.
Amyloid imaging: Sensitive but not specific. Doesn’t significantly change with progression of disease.
Cognitive decline MIRRORS structural atrophy where there is no increase in Amyloid deposition.
The Radiology FactorImaging Take Home Points

The Genetic Factor

The Amyloid Theory (overview)

How Does The Genetics Fit In The Amyloid Theory

The Genetic Factor

The Genetic Factor
Our data suggest that Alzheimer's disease is not a single entity, but rather results from genetic defects on chromosome 21 and from other genetic or no- genetic factors. “Conflicting Reports”

The Genetic Factor
Using this method, we identified two regions suggesting linkage: the proximal long arm of chromosome 19 (CH19) and the CH21 region of FAD linkage reported by St. George Hyslop et al. Application of standard likelihood (LOD score) analysis to these data support the possibility of an FAD gene locate on CH19, particularly in the late-onset FAD families.

The Genetic Factor
CONCLUSIONS:The APOE epsilon4 allele represents a major risk factor for AD in all ethnic groups studied, across all ages between 40 and 90 years, and in both men and women.

The Amyloid Theory

The Amyloid Theory

The Amyloid Theory

The FlawsThe association of neurofibrillary tangles more clearly relevant to the dementia of AD than the presence of amyloid containing neuritic plaques.1
Many drugs that were invented to remove or stop amyloid have failed to improve patient’s symptoms.
The amount of Amyloid deposition doesn’t correlate with the degree of volume atrophy (10mg in a 1400gm brain).
Only 2% of population have PSN mutations. Of those only 50% develop AD in their life time.
50% of APO E4/E4 who are 80-years-old lack AD. African Americans with APOE4 don’t show the disease. (Absent in Nigerian AD with matching controls).
1. Braak H, Braak E. Neuropathological staging of Alzheimer-related changes. Acta Neuropathol 1991;82:239–59

So What Do We Think Is Really Causing AD ?

The Vascular Theory

The Vascular Theory

The Vascular Theory

What Are We Doing AT UMASS ?

New England Stroke & Research Center
David Drachman MD Matthew Gounis PhD

The StudySimvastatin (40 mg/day) for one month.
Then add L-Arginine (2 gm qid) for a month.
Then add Tetrahydrobiopterin (BH4), 20 mg/kg for 2 months. So, for the last 2 months of the study he will be on all three drugs.
The statin increases endothelial nitric oxide production (eNOS) and function; the L-Arginine supplies nitrogen; and the BH4 is a critical cofactor for the process.
NOTCH is secreted by the endothelial cells in response to elevated eNOS.
ASL (PLD 1600, 1900, 2100ms) Time “0”, 1 month, 2 month and 4 month.

#1
#2
#3
#4
Sessio
n
Subject 1, ASL, PLD = 1600 ms

The Study Goals
To have better understanding of the underlying vascular pathogenesis of AD and to validate the vascular theory.
Proposal and trial of new treatment of AD.
To evaluate and establish the diagnostic and prognostic utility of ASL in the imaging of patients with AD.

Thank You

















