45
AMARO. AMOLENDA. ANDAL. ANG. ANG CASE CONFERENCE
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | annis-pitts |
| View: | 216 times |
| Download: | 0 times |

AMARO. AMOLENDA. ANDAL. ANG. ANG
CASE CONFERENCE

General Data
M.C. 14, Female April 29, 1996 Filipino Roman Catholic Sampaloc, Manila
Informant: Patient and Mother Reliability: Good

Chief Complaint
Fever

History of Present Illness
Patient experienced fever graded > 40°C Paracetamol 500 mg/tab Q4 Ibuprofen 200 mg/capsule
Provided temporary relief.
Bifrontal Headache non-radiating, graded 3/10
(+) Non projectile vomiting of previously ingested food (1 episode)
(+) loss of appetite (-) Epistaxis, Abdominal Pain (-) Gum Bleeding, Dizziness (-) Cough, Colds, Dysuria, Diarrhea
4 DAYS PTC

History of Present Illness
Persistence of Fever Ibuprofen 200 mg
It provided temporary relief of symptoms.
(+) Loss of appetite (-) Epistaxis, Abdominal Pain,
Dizziness, Vomiting, Gum Bleeding (-) Cough, Colds, Dysuria,
Diarrhea
1 DAY PTC
History of Present Illness
Persistence of Fever Ibuprofen 200mg/capsule
Provided temporary relief of symptoms
(+) Myalgia, Loss of appetite (-) Epistaxis, Abdominal Pain (-) Dizziness, Gum Bleeding,
Vomiting (-) Cough, Colds, Dysuria,
Diarrhea
3 hoursPTC

Review of Systems
General:, (-) weight loss/gain Skin: (-) rash, pigmentation Head: (-) visual difficulties, lacrimation,
aural discharge, nasal discharge Cardiovascular: (-) cyanosis, orthopnea Respiratory: see HPI Gastrointestinal: see HPI

Review of Systems
Genitourinary: (-) oliguria, hematuria Endocrine: (-) heat/cold intolerance,
palpitations, polyuria, polydipsia, polyphagia
Nervous: (-) convulsions, tremors, sleep problems
Hematologic: (-) easy bruisability, bleeding manifestation
24 Hour Food Recall
Bobby in table form po plus kCal and RENI
Ung kapanipaniwala… remember my loss of appetite since 4 days PTC. Pero wag nmn sobrang baba kc baka sabihin dpt i-admit. TNX

Past Medical History
Dysentery (2005) Confined in Hospital ng Sampaloc

Menstrual History
Menarche: 13 y/o Interval: Every 28-30 days Duration: 5-7 days Amount: 3 fully soaked napkins LMP: Aug 7-11, 2010 PMP: July 5-10, 2010

Immunizations
Incomplete with unrecalled dates BCG: 1 HepB: 3 DPT/OPV: 3 (without booster) Measles: 1 MMR: (unrecalled)
Family Profile (BOBBY AYUSIN MO PO ITO PLS.. TABLE FORM)
Father MC Age: 44 College Graduate Operator Healthy
Mother JC Age:44 College undergrad Housewife Healthy
Brother JC Age: 23 College undergraduate Healthy
Sister: JC Age: 21 College undergrad Housewife Healthy

Family History
(+) HPN, Paternal relatives (+) Ovarian CA, maternal grandmother

Socioeconomic and Environmental Profile
Housing Condition: 2 storey house, made up of wood, well lit
and well ventilated. Patient consumed mineral water.Garbage is collected everyday and they practice segregation. They have 2 pet dogs and no factories nearby. The family’s average monthly income amounts to >P10, 000
Psychosocial History
Home: Lives with both parents, 2 siblings and her sister’s family.
Has good relationship with other family members. Education:
Currently a 2nd year H.S. student at Ramon Magsaysay H.S. Good school performance, and gets along with teachers
and classmates. Eating:
Eats 3x a day + snacks Activities:
Part of Manila City Dance Scholars Listens to acoustic music, watches TV, and surfs the net.

Psychosocial History
Drugs: Denies illicit drug use Non smoker Non alcoholic beverage drinker
Suicide No suicidal ideation
Sexual No boyfriends Denies any sexual encounter
Safety Follows traffic rules and regulations

Physical Exam
General Survey: Conscious, coherent, ill looking, not in Cardiopulmonary distress, well nourished, and mildly dehydrated
Vital Signs- BP: 110/80, CR: 95, RR: 21, Temp: 36.5 °C
Ht: 155 cm (Z-score 0) Wt: 41.3 kg (Z- score ?) BMI: 17.2 (Z-score -1)

Physical Exam
Skin: flushed skin with dry lips. Good skin turgor, no active dermatoses, and (+) Tourniquet test
Eyes/Ears/Nose/Throat: Pink palpebral conjunctivae, anicteric sclerae, pupils 3-4 mm ERTL / No tragal tenderness, no ear discharge, (+) retained cerumen on both ears / non hyperemic PPA, moist buccal mucosa, no gum bleeding, no mouth sores, no palatal petechiae
Physical Exam
Neck: Supple neck, no palpable cervical lymph nodes
Lungs/Chest: Symmetrical chest expansion, no retractions or alar flaring, normal AP diameter, no cyanosis, no clubbing, tactile fremiti are equal on both lung fields, resonant on all lung fields. vocal fremiti are equal on both lung fields. clear breath sounds

Physical Exam
Cardiovascular:Dynamic precordium, AB at 5th LICS MCL, no heaves, lifts, and murmurs, S1>S2 at the apex, S2>S1 at the base
Abdomen: Flabby abdomen, normoactive bowel sounds, no masses, no direct and indirect tenderness, liver and spleen not palpable
Musculoskeletal: No inflammation and pain on both knees, no limitation of motion

Physical Exam
Spine: Midline, No deformities along the vertebra
Pulse: full and equal on all extremities External genitalia: no clitoromegaly Tanner stage: Breast bud:2 Pubic Hair: 2
Physical Examination
• Neurologic Examination– Conscious, coherent, oriented to three spheres– Opens eye spontaneously, Oriented, Obeys
command– No anosmia– 20/40 on L and R eyes, (+) confrontation,
midline gaze, (+) direct and consensual light reflex, intact pupillary light reflex, (+) ROR
– EOMs full and equal– Can feel light touch equally on the forehead,
cheeks, mandibular area
Physical Examination
• Neurologic Examination– Can raise both eyebrows, can frown, smile,
and can puff out both cheeks– No hearing deficits, no lateralization– Uvula midline, rises on phonation– Can raise shoulder against resistance on
the left– Tongue midline on protrusion
Physical Examination
• Neurologic Examination– MMT 5/5 on all extremities– Can perform FTNT and APST– Sensitive to pain, temperature, light touch,
and vibration– DTRs ++ on all extremities, (-) Babinski
Salient Features
14 y/o, Female Sampaloc, Manila 4 day Fever Bifrontal Headache Vomiting (1 episode) (-) Epistaxis, Abdominal Pain, Dizziness, Gum
Bleeding (+) Loss of appetite, Myalgia (-) Cough, Colds, Dysuria, Diarrhea Flushed skin with dry lips Good skin turgor (+) Tourniquet test No palatal petechiae
APPROACH TO DIAGNOSIS
A presenting manifestation pointing to the least number of diseases
Fever with Constitutional
Symptoms
Dengue Hemorrhagic FeverInfluenzaTyphoid FeverLeptospirosis

WORKING DIAGNOSIS
Acute Viral Infection to r/o Dengue Fever with probable signs
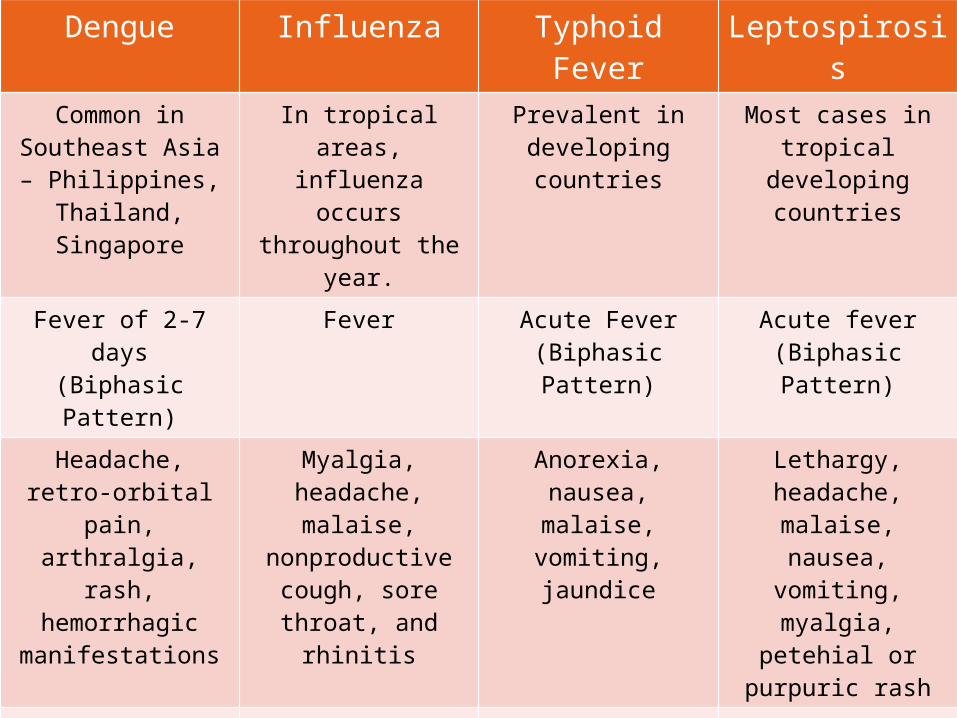
Dengue Influenza Typhoid Fever LeptospirosisCommon in
Southeast Asia – Philippines, Thailand, Singapore
In tropical areas, influenza occurs throughout the
year.
Prevalent in developing countries
Most cases in tropical
developing countries
Fever of 2-7 days(Biphasic Pattern)
Fever Acute Fever(Biphasic Pattern)
Acute fever(Biphasic Pattern)
Headache, retro-orbital pain,
arthralgia, rash, hemorrhagic
manifestations
Myalgia, headache, malaise,
nonproductive cough, sore throat, and
rhinitis
Anorexia, nausea, malaise, vomiting, jaundice
Lethargy, headache,
malaise, nausea, vomiting,
myalgia, petehial or purpuric rash
Rapid and weak pulses, narrow pulse pressure,
hypotension, cold clammy skin
In children, diarrhea may be a
feature.Tachycardia, signs
of mild volume depletion with dry
skin
Resembles AGE in young children
Bradycardia, hypotension, but
circulatory collapse
uncommon
Signs of plasma leakage – pleural effusion, ascites, hypoproteinemia
Regional lymphadenopathy
, splenomegaly
Conjunctival suffusion,
generalized lymphadenopathy
Diagnostic Plans
Complete blood cell count with Platelet
Complete Blood Count
Hemoconcentration (hematocrit increased 20%) – precedes shock
Thrombocytopenia (platelet count <100 x 109/L) are seen in dengue hemorrhagic fever or dengue shock syndrome and occur before defervescence and the onset of shock.
Leukopenia, often with lymphopenia, is observed near the end of the febrile phase of illness
Lymphocytosis, with atypical lymphocytes, commonly develops before defervescence or shock.
• Monitor CBC at least every 24 hours to facilitate early recognition of dengue hemorrhagic fever
Treatment Plans
Supportive Paracetamol 500mg/tab, 1 tablet PO every 4
hours for temperature >38.5 Oral rehydration solution 75 replace losses
volume per volume Increase oral fluid intake (water, soups, juice,
milk) Bed rest

Treatment Plans
Supportive: Avoid dark colored foods Watch out for warning signs (severe abdominal
pain, passage of black stools, bleeding into the skin or from the nose or gums, sweating, and cold skin )
Observe carefully for complications for at least 2 days after recovery from fever.
Treatment Plans
Preventive1.) Prevent mosquito bites:
Wear full-sleeve clothes and long dresses to cover the limbs.
Use of mosquito repellents Use of mosquito nets to protect babies, old
people and others who may rest during the day.
Permethrin (pyrethroid insecticide) treatment on mosquito nets, curtains to repel or kill mosquitoes.

Treatment Plans
Preventive2.) Prevent the multiplication of mosquitoes:
Mosquitoes which spread dengue live and breed in stagnant water in and around houses. Drain out the water from bottles, tanks, barrels, drums, buckets, etc.
All stored water containers should be kept covered at all times.

BRIEF DISCUSSION
Dengue Viral Replication Cycle Family Flaviviridae Genus Flavivirus Small, enveloped viruses containing a
single-stranded RNA genome of positive polarity
Vector: Aedes aegypti
Dengue Viral Replication Cycle Attachment to the cell surface Entry into the cytoplasm Translation of viral proteins Replication of the viral RNA genome Formation of virions (encapsidation) Release from the cell


Incubation Period
Symptoms typically develop between 4 and 7 days (3-14 days)

DENGUE FEVER
Acute febrile illness accompanied by: Headache Retroorbital pain Marked muscle and joint pains - "break-bone fever“
Fever typically lasts for 5-7 days Some patients display a biphasic ("saddleback")
fever curve, with the second febrile phase lasting 1-2 days
The febrile period may also be followed by a period of marked fatigue that can last for days to weeks
DENGUE FEVER
Constitutional symptoms Fever and headache Eye pain Body pain Joint pain
Rash Gastrointestinal symptoms
Nausea or vomiting Diarrhea
Respiratory tract symptoms Cough Sore throat Nasal congestion

DENGUE FEVER
Physical examination Non-specific Fever Rash – macular or maculopapular Conjunctival injection, pharyngeal
erythema, lymphadenopathy, and hepatomegaly
DENGUE FEVER
Laboratory findings Leukopenia Thrombocytopenia Serum aspartate transaminase (AST) levels
are frequently elevated
Thank You.

















