American College of American College of Surgeons Presenter Surgeons Presenter Disclosure Slide Disclosure Slide Chang Shu 2010 Clinical Congress American College of Surgeons ♦ Division of Education
Transcript
American College of Surgeons American College of Surgeons Presenter Disclosure SlidePresenter Disclosure Slide
Chang Shu
2010 Clinical CongressAmerican College of Surgeons ♦ Division of Education
Endovascular Repair of Standford Type B Aortic Dissections with
Severe Complications
Endovascular Repair of Standford Type B Aortic Dissections with
Severe Complications
Chang ShuDepartment of Vascular Surgery, Xiang-Ya Second
Hospital, Central-South University, China
Chang ShuDepartment of Vascular Surgery, Xiang-Ya Second
Hospital, Central-South University, China
Clinical Materials
2003.2—2009.12 Among 290 Stanford type B AD patients, 65 (22.4%) patients Male: 43 Female: 22 Age of 42.6±10.7years (range 34-71 years), Presented with severe complications,
The Range of oxygen saturation index: 85%-67%The Range of oxygen saturation index: 85%-67%
To be supported by respirator: 7 (7/29)To be supported by respirator: 7 (7/29)
Combined with ischemia of the viscera: 3 (3/29)Combined with ischemia of the viscera: 3 (3/29)
To be diagnosed respiratory failure: 10 (10/29)To be diagnosed respiratory failure: 10 (10/29)
Result
1
2
3
4
Mortality: 0%Mortality: 0%
hydrothorax to be totally absorbed : 22 cases, 28days-11 months after the stent-graft treatment hydrothorax to be totally absorbed : 22 cases, 28days-11 months after the stent-graft treatment
Respiratory support after operation: 7 (7/29). Range: 2-9 daysRespiratory support after operation: 7 (7/29). Range: 2-9 days
Six (6/29) progressive increasing hydrothorax after the procedure: drainage tube to be used:1. Puncture drainage 5.
Six (6/29) progressive increasing hydrothorax after the procedure: drainage tube to be used:1. Puncture drainage 5.
Complications after endoluminal treatment
Pleural thickening: 6.
Pulmonary atelectasis: 2
Lung consolidation combined with chest dent: 2
Conclusion
Endovascular therapy is safe and effective for
the cases of acute Stanford type B aortic
dissection with hydrothorax.
The reasonable drainage of hydrothorax after
stent-graft deployed is a must for the patient
suffered from respiratory failure.
The early treatment Is very important to the patient
with dissection combined with hydrothorax.
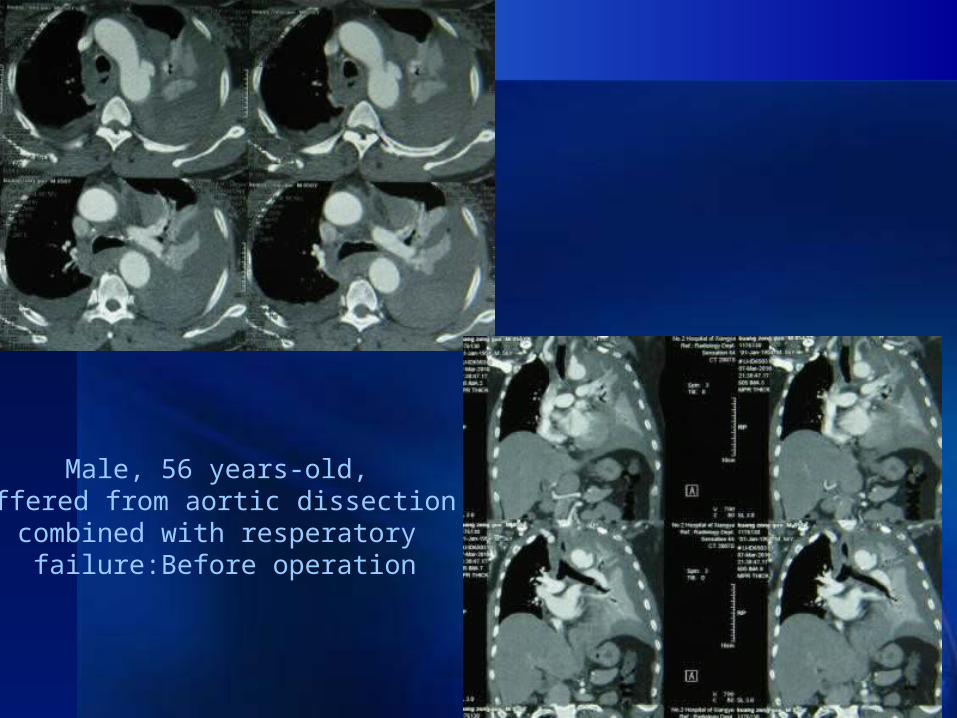
Male, 56 years-old,Suffered from aortic dissection
combined with resperatory failure:Before operation
After operation, 3 months later
Male, 56 years-old,Suffered
from aortic dissection
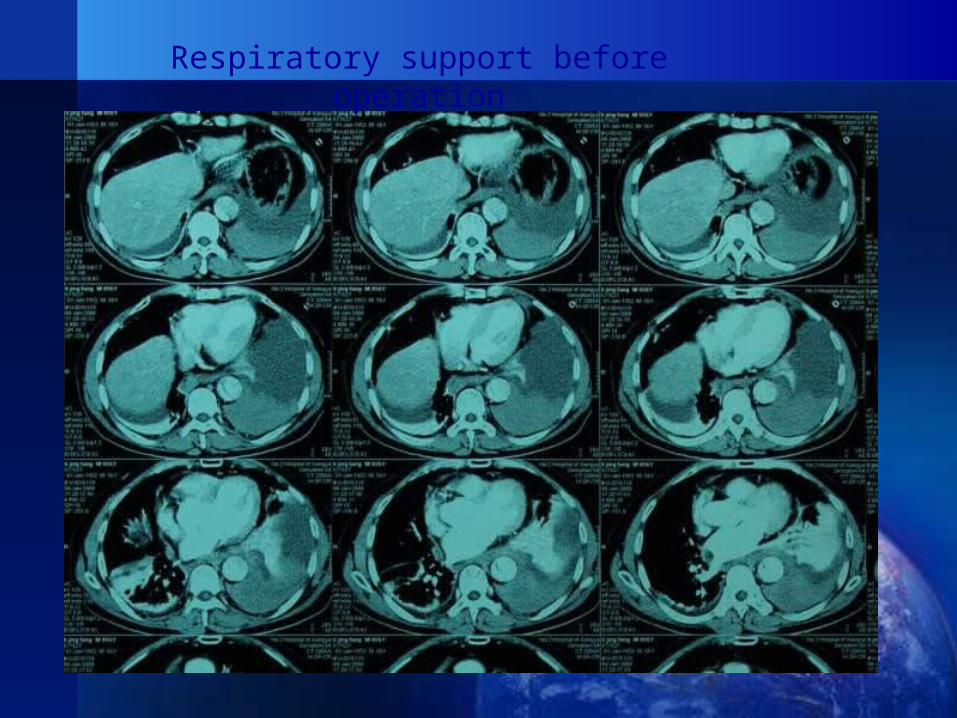
Respiratory support before operation
Three months later, false lumenAlmost disppeared,
Lung consolidation combined with chest dent
Male, 63 years-old, breath supported by the machine before operation
Three days later after deploy the stent-graft
11 months later, false lumen disspeared, and the chest is very clean for we drainge it after deployed the stent-graft
Combined with acute kidney failure
Seven aortic dissection combined with kidney failure:
6 patients had been given hemodialysis before being treated by stent-graft (3days-2 weeks)
1 patient suffered from kidney failure for 2 days
Result
All patients survived: 3 (3/7) patients need hemodialysis after the
endoluminal treatment for 3-7days. 4( 4/7) patients need not hemodialysis after the
stent-graft deployed, the DSA shows the instantly blood supply of the renal artery for the true lumen opened.
Before operation:The right renal false lumen
After deploy the stent-graft
Aortic dissection combined with paraplegia
Three patients suffered from paraplegia after aortic dissection happened. Only one patient had been given stent-graft treatment.
Male, 60 years-old. Suffered from aortic dissection 1 day, paraplegia happened, we gave him emergency stent-graft deployed, and drainage the spinal cord, use large dose of hormone. He can move his extremities after 4 hours later of the operation.
Before operation
2 weeks later of the stent-graft deployed
With ischemia of the celiac or SMA, Lower limbs
celiac trunk ischemia 10; Superior mesenteric artery ischemia 11;
(10 treated by stent-graft) Severe limb ischemia 5.
The true lumen is totally compressed by the false lumen, we have to put the guide wire from the subclavian to the femoral artery
26
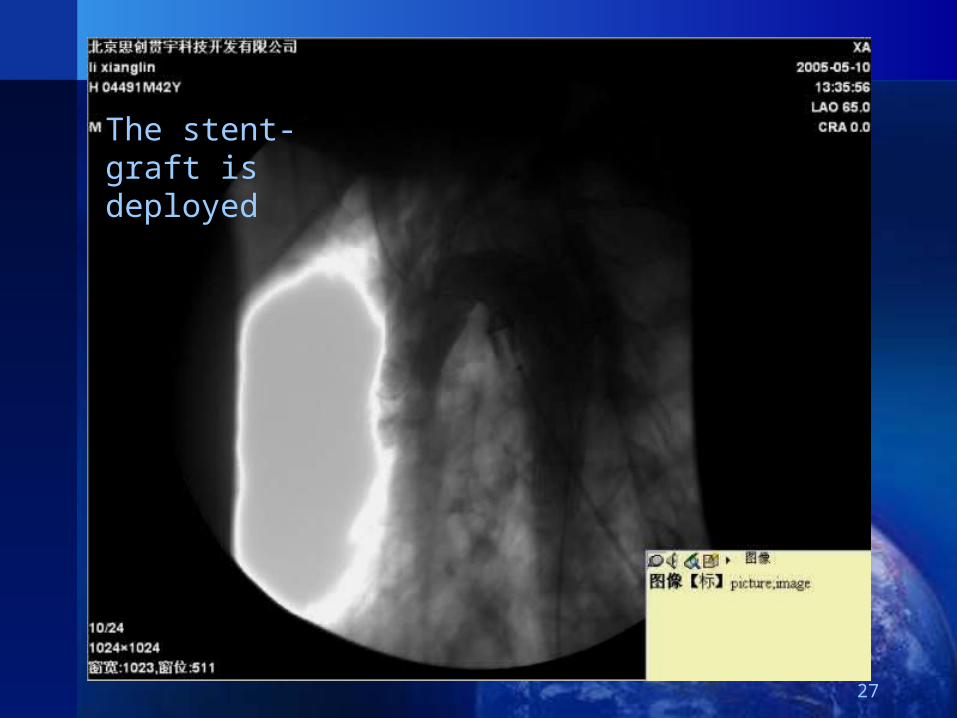
The stent-graft is deployed
27
The true lumen is opened, although some visceral arteries are still coming from the false lumen, the patients has no ischemia symptoms
28
Result
Limb and visceral ischemia disappeared gradually after endoluminal repair 1 to 14 days later, and the paraplegia patient begin to recover 4 hours later after stent-graft deployed. All endoluminal treatent patients were kept alive and the 3-86 months follow up showed that enlarged true lumen and thrombosis in the false lumen.
Conclusion
Emergency endovascular therapy is a safe and effective method to treat Standford type B AD combined with severe complications.