21
FLORES, SONZA, SAMSON AMNIOTI C FLUID
| Date post: | 06-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | kamsteph012 |
| View: | 132 times |
| Download: | 1 times |

FLORES, SONZA, SAMSON
AMNIOTIC
FLUID
Amniotic fluid is present in the amnion, a membranous sac that surrounds the fetus
The primary functions of the fluid are to provide a protective cushion for the fetus, allow fetal movement, stablize the temperature to protect the fetus from extreme temperature changes, and to permit proper lung development
Volume
Amniotic fluid volume is regulated by a balance between the production of fetal urine and lung fluid and the absorption from fetal swallowing and intramembranous flow
Meconium - which is usually defined as a newborn’s first bowel movement, may be present in the amniotic fluid as the result of fetal intestinal secretions.
About 500 mls enter and leave the amniotic sac each hour.
gradual ↑ up to 36 weeks to around 600 to 1000 ml then↓ after that.
The normal range is wide but the approximate volumes are:
- 500 ml at 18 weeks - 800 ml at 34 weeks. - 600 ml at term.

Polyhydramnios
Failure of the fetus to begin swallowing results in excessive accumulation of amniotic fluid (polyhydramnios) and is an indication of fetal distress, often associated with neural tube disorders.
Polyhydramnios may be secondarily associated with fetal structural anomalies, cardiac arrhythmias, congenital infections, or chromosomal abnormalities.

Oligohydramnios
Increased fetal swallowing, urinary tract deformities, and membrane leakage are possible causes of decreased amniotic fluid (oligohydramnios).
Oligohydramnios may be associated with umbilical cord compression, resulting in decelerated heart rate and fetal death.
Chemical Composition
The placenta is the ultimate source of amniotic fluid water and solutes.
Amniotic fluid has a composition similar to that of the maternal plasma and contains a small amount of sloughed fetal cells from the skin, digestive system, and urinary tract.
These cells provide the basis for cytogenetic analysis. The fluid also contains biochemical substances that are produced by the fetus, such as bilirubin, lipids, enzymes, electrolytes, nitrogenous compounds, and proteins that can be tested to determine the health or maturity of the fetus.

Amniocentesis
Amniotic fluid is obtained by needle aspiration into the amniotic sac, a procedure called amniocentesis.
The procedure most frequently performed is a transabdominal amniocentesis
A thin, hollow needle is inserted through the mother’s abdomen into the mother’s uterus and into the amniotic sac to aspirate the amniotic fluid.
Vaginal amniocentesis may also be performed; however, this method carries a greater risk of infection
Indications for Performing Amniocentesis
Amniocentesis may be indicated at 15 to 18 weeks of gestation for the following conditions to determine early treatment or intervention: Mother’s age of 35 or more at
delivery Family history of chromosome
abnormalities, such as trisomy 21 (Down syndrome)
Parents carry an abnormal chromosome rearrangement
Earlier pregnancy or child with birth defect
Parent is a carrier of a metabolic disorder
History of genetic diseases such a sickle cell disease, Tay-Sachs disease, hemophilia, muscular dystrophy, sickle cell anemia, Huntington chorea, and cystic fibrosis
Elevated maternal serum alpha fetoprotein
Abnormal triple marker screening test
Previous child with a neural tube disorder such as spina bifida, or ventral wall defects (gastroschisis) •
Three or more miscarriages Evaluation of amniocentesis is indicated later in the pregnancy (20 to 42 weeks) to evaluate:
Fetal lung maturity Fetal distress Hemolytic disease of the
newborn caused by Rh blood type incompatibility
Infection
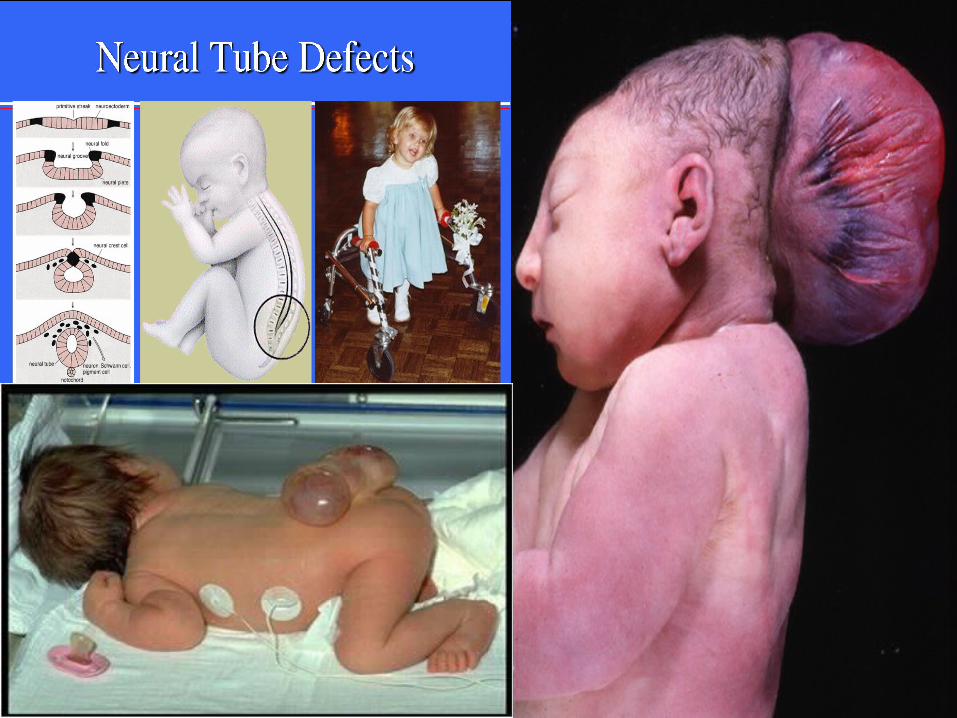
NEURAL TUBE DEFECTS
-increased levels of alpha-fetoprotein (AFP) in both the maternal circulation and the amniotic fluid can be indicative of fetal neural tube defects such as anencephaly and spina bifida.
AFP- major protein produced by the fetal liver during early gestation (prior to 18 weeks).
-found in the maternal serum due to the combined fetal-maternal circulations and in the amniotic fluid from diffusion and excretion of fetal urine.
-increased levels are found in the maternal serum and amniotic fluid when the skin fails to close over the neural tissue, as occurs in anencephaly and spina bifida.
Measurement of amniotic fluid AFP levels is indicated when maternal serum levels are elevated.
-Multiple Pregnancy-investigates when serum levels are elevated
-Normal values are based on the week of gestational age
-Fetus produces maximal AFP between 12-15 weeks of gestation
-Serum and amniotic fluid AFP levels are reported in terms of multiples of the median (MoM)
-Testing for AFP has been automated by the Access Immunoassay System.
-Elevated amniotic fluid AFP levels are followed by measurement of amniotic acetyl cholinesterase (AChE).
TEST FOR FETAL MATURITY
FETAL LUNG MATURITY
Respiratory Distress Syndrome (RDS)- most frequent complication of early delivery and is a cause of morbidity and mortality in the premature infant.
-caused by a lack of lung surfactant Lung surfactant- substance that normally appears in mature
lungs and allows the alveoli (air sacs of the lung) to remain open throughout the normal cycle of inhalation and exhalation.
-keeps the alveoli from collapsing by decreasing the surface tension and allows them to inflate with air more easily.
LECITHIN-SPHINGOMYELIN RATIO Lecithin
primary component of the surfactants (phospholipids, neutral lipids and proteins) that make up the alveolar lining and account for alveolar stability.
produced at a relatively low and constant rate until the 35th week of gestation Sphingomyelin- lipid that is produced at a constant rate after about 26
weeks’ gestation Lecithin and Sphingomyelin appear in the amniotic fluid in amounts
proportional to their concentration to their concentrations in the fetus. Prior to 35 weeks’ gestation the L/S ratio is usually less than 1.6 because
large amount of lecithin are not being produces at this time. It will rise to 2.0 or higher when lecithin production increases to prevent alveolar collapse.
Reaches 2.0- pre term delivery is considered to be a relatively safe procedure.
Falsely elevated- contaminated with blood or meconium Quantitative measurement- using thin-layer chromatography. *phosphatidyl glycerol immunoassays, fluorescence polarization, lamellar
body density procedures.

AMNIOSTAT-FLM Phosphatidyl glycerol- essential for
adequate lung maturity. Aminostat-FLM uses antisera specific for
phosphatidyl glycerol and is not affected by specimen contamination with blood and meconium.
FOAM STABILITY
“Foam” or “Shake” test- mechanical screening test, used to determine their presence.
Amniotic is mixed with 95% ethanol, shaken for 15 seconds, and allowed to sit undisturbed for 15 mins.
The presence of the bubbles indicates that a sufficient amount of phospholipid is available to reduce the surface tension of the fluid even in the presence of alcohol, an antifoaming agent.
MICROVISCOSITY: FLUORESCENCE POLARIZATION ASSAY
The presence of phospholipids decreases the microviscosity of the amniotic fluid
This change can be measured using the principle of fluorescence polarization employed by the Abbott TDx analyzer with the TDx/TDxFLxFLM II Assay System
TDx/TDxFLxFetal Lung Maturity II- reagentsystem for the quantitative measurement of the ratio of surfactant to albumin in amniotic fluid for assessment of lung maturity of the fetus.
LAMELLAR BODIES AND OPTICAL DENSITY
Lamellar Bodies- lamelled phospholipids that represent storage form of surfactant
the presence of lamellar bodies increases the OD of the amniotic fluid
lamellar body diameter is similar to that of small platelets
can be counted using resistance-pulse counting such as that employed by Coulter cell-counting instruments.


















