63
Amniotic fluid abnormalities and Rh isoimmunization Rand Al-Shayeb
Amniotic fluid abnormalities and Rh isoimmunization
Rand Al-Shayeb
Amniotic fluid abnormalities
Amniotic fluid Definition • Is the liquid that surrounds the fetus after the first few weeks of
gestation. During much of pregnancy, AF is derived almost entirely from the fetus and has a number of functions that are essential for normal growth and development.
Amniotic fluid Functions 1. It helps to protect the fetus from trauma to the maternal abdomen.
2. It cushions the umbilical cord from compression between the fetus and uterus.
3. It has antibacterial properties that provide some protection from infection.
4. It serves as a reservoir of fluid and nutrients for the fetus.
5. Permit movement of the fetus while preventing limb contracture hence normal postural development.
6. It provides the necessary fluid, space, and growth factors to permit normal development of the fetal lungs and musculoskeletal and gastrointestinal systems.
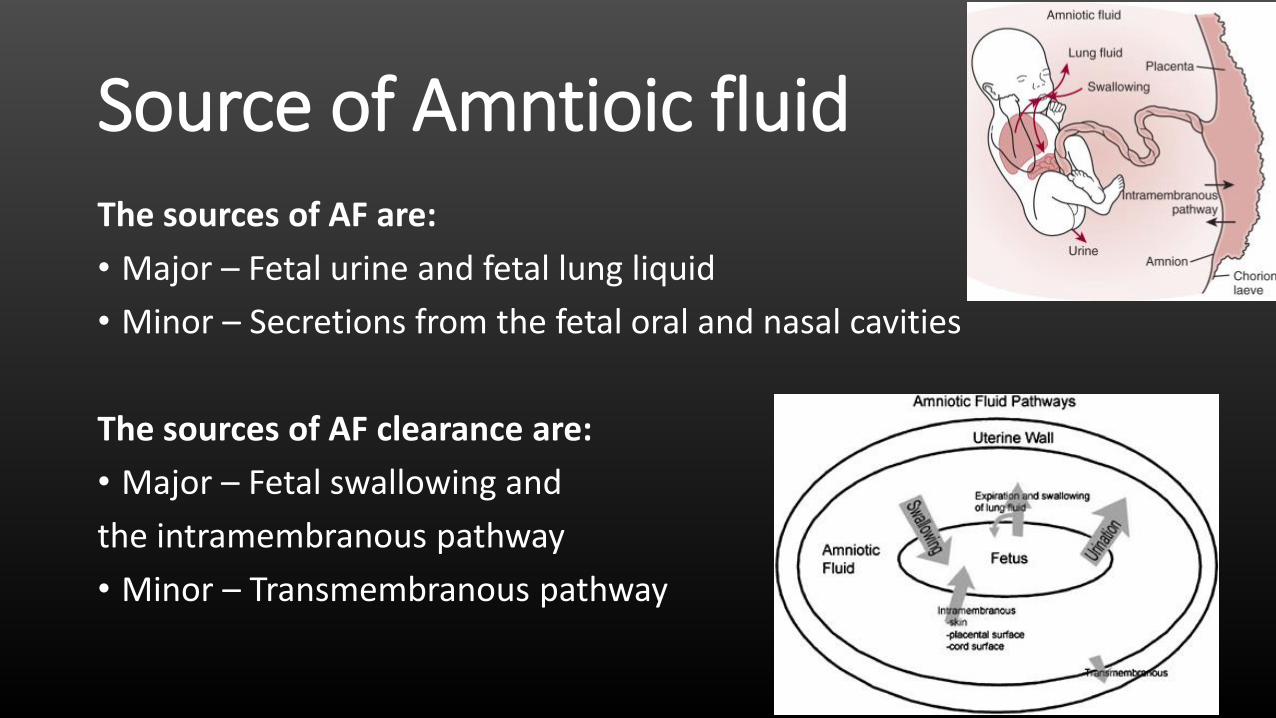
Source of Amntioic fluid The sources of AF are:
• Major – Fetal urine and fetal lung liquid
• Minor – Secretions from the fetal oral and nasal cavities
The sources of AF clearance are:
• Major – Fetal swallowing and
the intramembranous pathway
• Minor – Transmembranous pathway
Assessment of amniotic fluid volume Ultrasound examination is the only practical clinical method of
assessing AFV :
1. Single deepest pocket (SDP)
2. Amniotic fluid index (AFI)

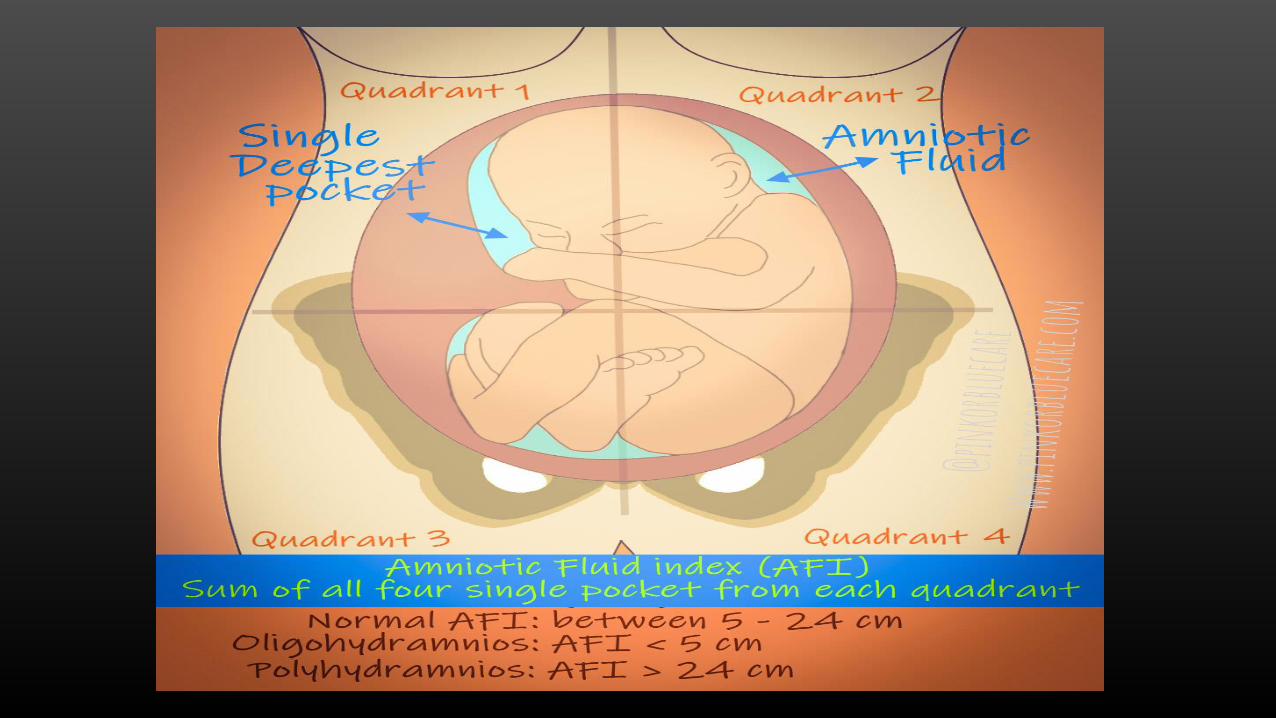
Single deepest pocket The SDP (also called the maximum vertical pocket [MVP] or the largest
vertical pocket) is the vertical dimension in centimeters of the largest pocket of amniotic fluid not persistently containing umbilical cord or fetal extremities and measured at a right angle to the uterine contour. The horizontal component of the vertical dimension must be at least 1 cm.
The following interpretation of SDP:
• Oligohydramnios – Depth <2 cm
• Normal – Depth ≥2 cm and <8 cm
• Polyhydramnios – Depth ≥8 cm

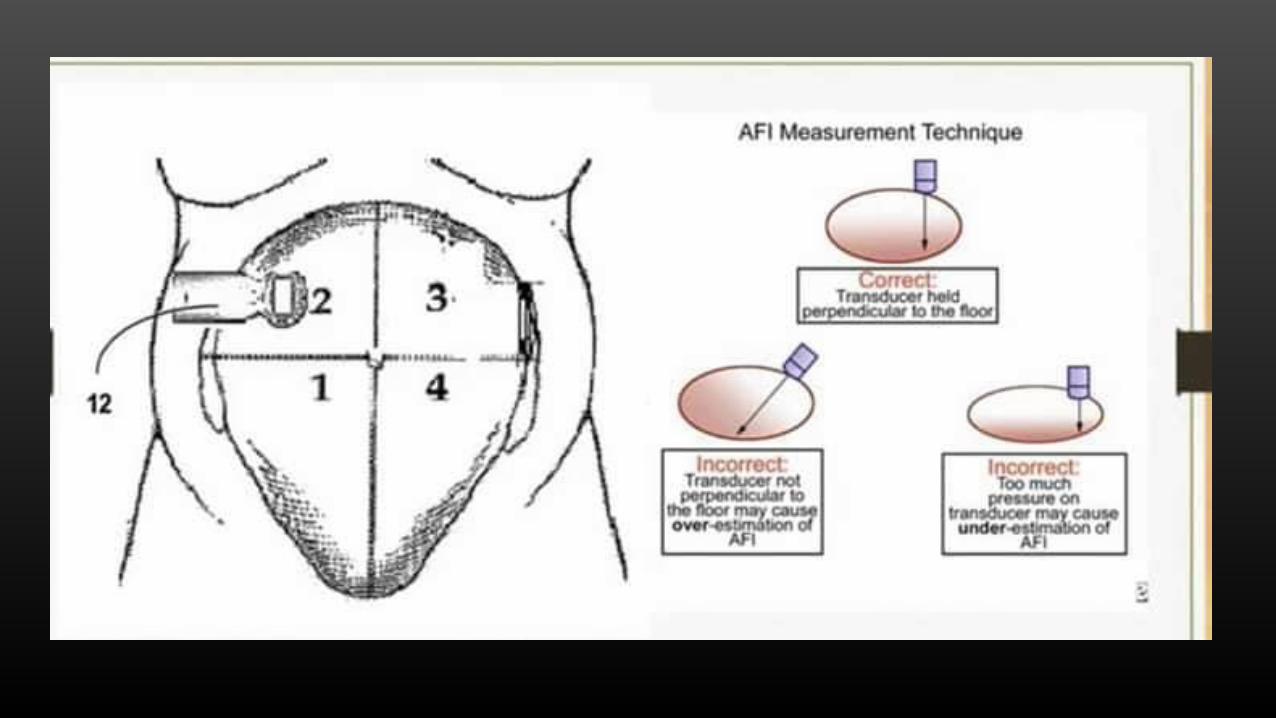
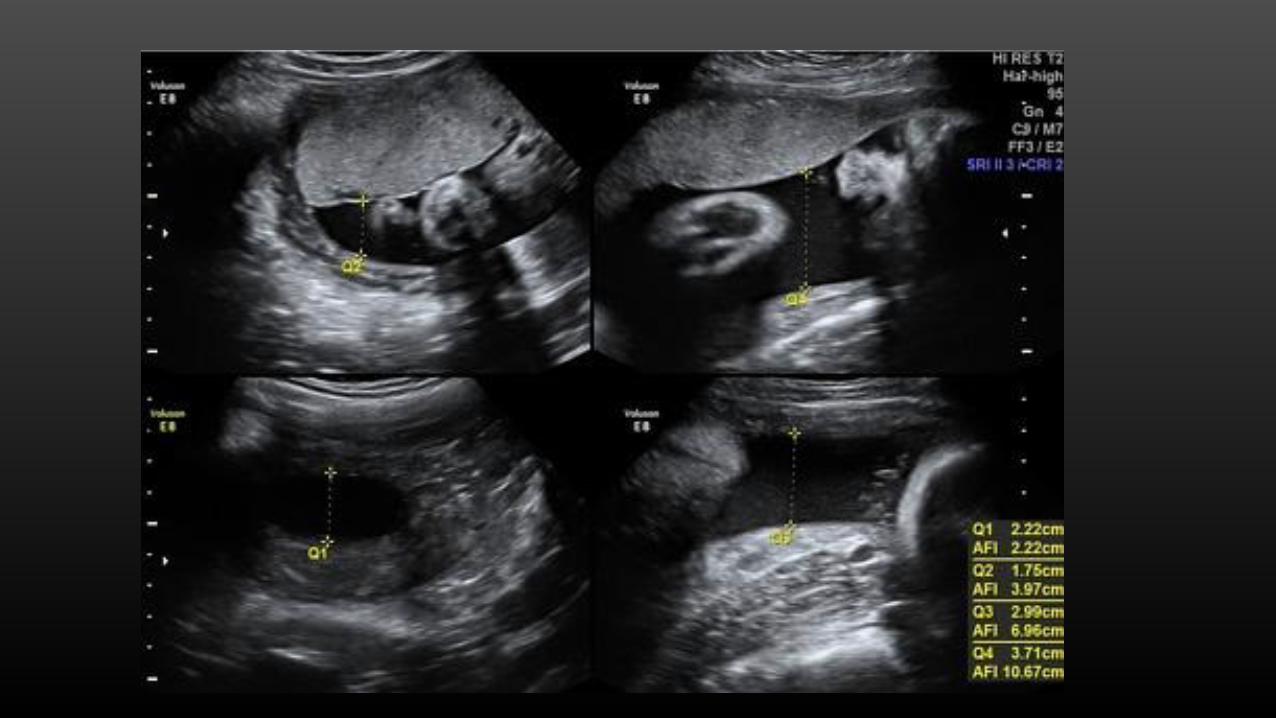
Amniotic fluid index The AFI is calculated by dividing the uterus into four quadrants using
the linea nigra for the right and left divisions and the umbilicus for the upper and lower quadrants. The maximal vertical amniotic fluid pocket diameter in each quadrant not containing cord or fetal extremities (on gray-scale examination) is measured in centimeters; the sum of these measurements is the AFI.
The following interpretation of AFI:
• Oligohydramnios – AFI ≤5 cm
• Normal – AFI >5 cm and <24 cm
• Polyhydramnios – AFI ≥24 cm
Oligohydramnios Definition: Oligohydramnios refers to amniotic fluid volume that is less than expected for gestational age.
Diagnosis:
Oligohydramnios may be suspected if :
1. Uterine size is less than expected for dates .
2. If fetal movements are decreased .
3. Difficult to feel fetal parts.
4. By history of leakage of fluid.
5. It may also be suspected based on incidental ultrasonographic findings .
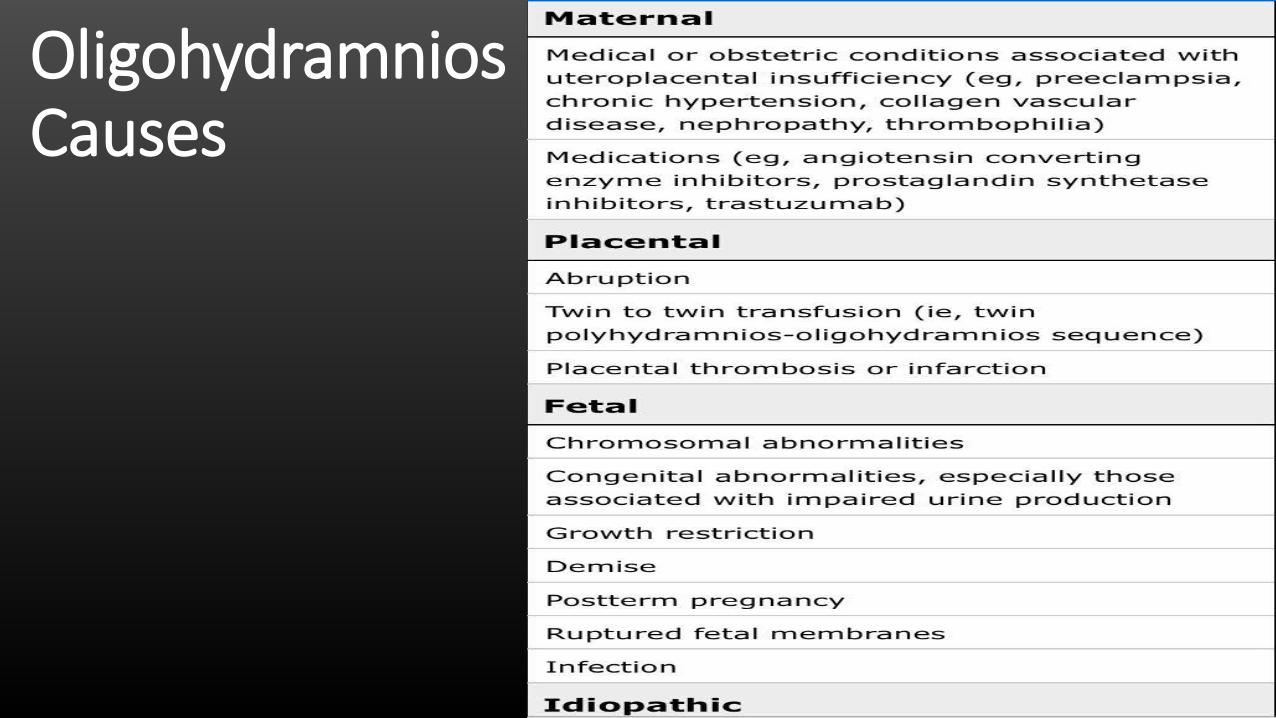
Oligohydramnios Causes

Oligohydramnios Complications • Fetal death.
• Intrauterine growth restriction.
• Limb contractures (if oligohydramnios begins early in the pregnancy) [Talipes and torticollis]
• Delayed or incomplete lung maturation (if oligohydramnios begins early in the pregnancy).
• Inability of the fetus to tolerate labor, leading to the need for cesarean delivery.
Risk of complications depends on how much amniotic fluid is present and what the cause is.
Oligohydramnios Management 1. Identification of cause.
2. Serial ultrasonography to determine AFI and monitor fetal growth.
3. Nonstress testing or biophysical profile.
4. If the causes is PROM management according to guidelines
5. If the cause is Post-term confirm date and Bishop score, presence of meconium or not ?
6. Oral hydration
Oligohydramnios 7. Amnioinfusion is a method in which isotonic fluid is instilled into
the uterine cavity.
• It is primarily used as a treatment in order to correct fetal heart rate changes caused by umbilical cord compression (indicated by variable deceleration seen on Cardiotocography)
• In severe cases of Oligohydramnios, amnioinfusion may be performed prophylactically to prevent umbilical cord compression.
• It has also been used to reduce the risk of meconium aspiration syndrome, though evidence of benefit is mixed.
Polyhydramnios
Definition: Polyhydramnios refers to an excess of amniotic fluid for gestational age.
Diagnosis:
Polyhydramnios may be suspected if :
1. On U/S AFI is more than or equal 24 cm , largest pool more than 8 cm
Presentation • Large for dates uterus ,
distended out of proportion to the gestational age (increased SFH).
• Unstable lie
• Abnormal presentation
• Difficulty feeling the fetal parts
• Difficulty hearing the fetal heart
• Shiny skin ,Dilated veins
• Fluid thrill • Abdominal discomfort and
distension, if sever maybe present as difficulty in breathing and painful uterine contraction
• Oedema • Increased varicose veins and
hemorrhoids
Polyhydramnios Causes Maternal
• Diabetes.
• Chorioangioma.
• Arteriovenous fistula.
Placental
• Hemangioma
Idiopathic
Fetal
• Multiple gestation (in monochorionic twins it may be twin-to-twin transfusion syndrome).
• Oesophageal atresia/tracheo-oesophageal fistula.
• Duodenal atresia.
• Neuromuscular fetal condition (preventing swallowing).
• Anencephaly.
Polyhydramnios Complications 1. Maternal respiratory compromise
2. Prelabor rupture of membranes
3. Preterm labor and delivery
4. Fetal malposition
5. Macrosomia (potentially leading to shoulder dystocia)
6. Umbilical cord prolapse
7. Abruptio placentae upon rupture of membranes
8. Longer second stage of labor
9. Postpartum uterine atony
10. High risk of Cesarean Section
Polyhydramnios Management • Establishing the cause and determining fetal prognosis, Exclude abnormality
through detailed anomaly scan
• Relieving the discomfort of the mother (if necessary by amniodrainage) and assessing the risk of preterm labor due to uterine overdistension.
• Polyhydramnios due to maternal diabetes needs urgent investigation, as it often suggests high maternal blood glucose levels. In this context, polyhydramnios should correct itself when the mother’s glycaemic control is optimized
• Twin-to-twin transfusion syndrome is a rare cause of acute polyhydramnios. The condition may be rapidly fatal for both twins; amniodrainage and removal by laser of the placental vascular connections

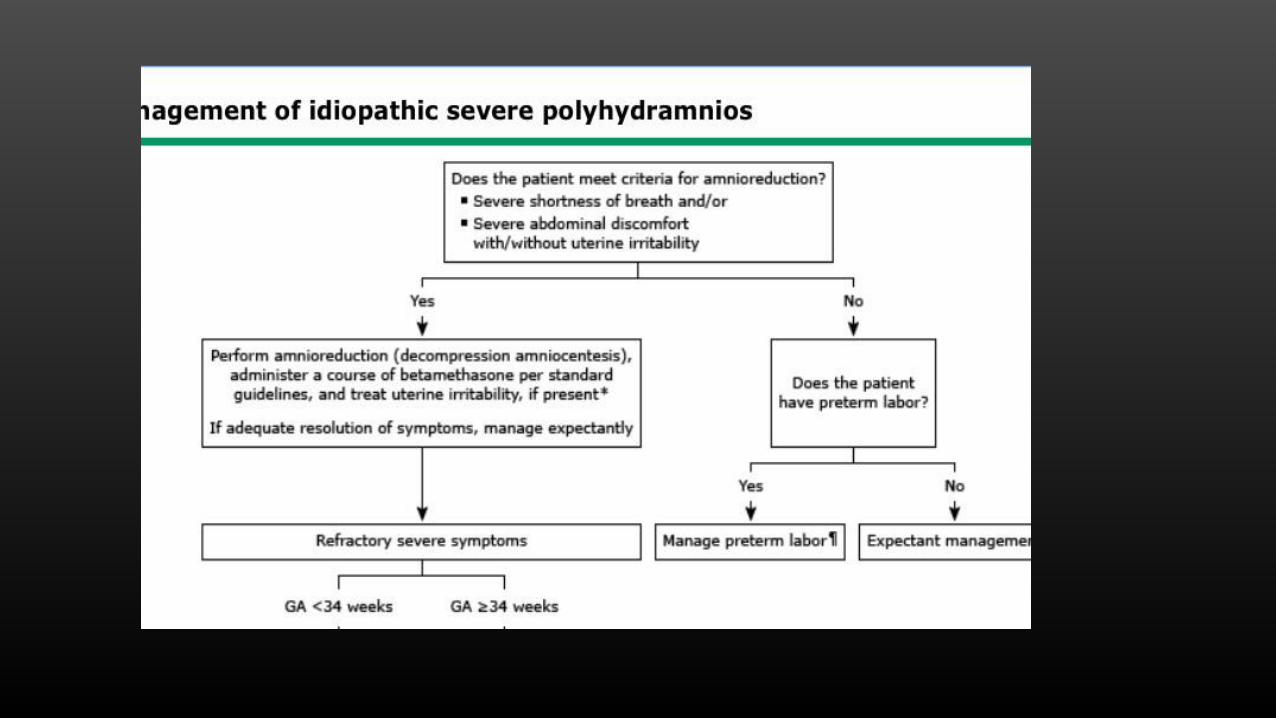
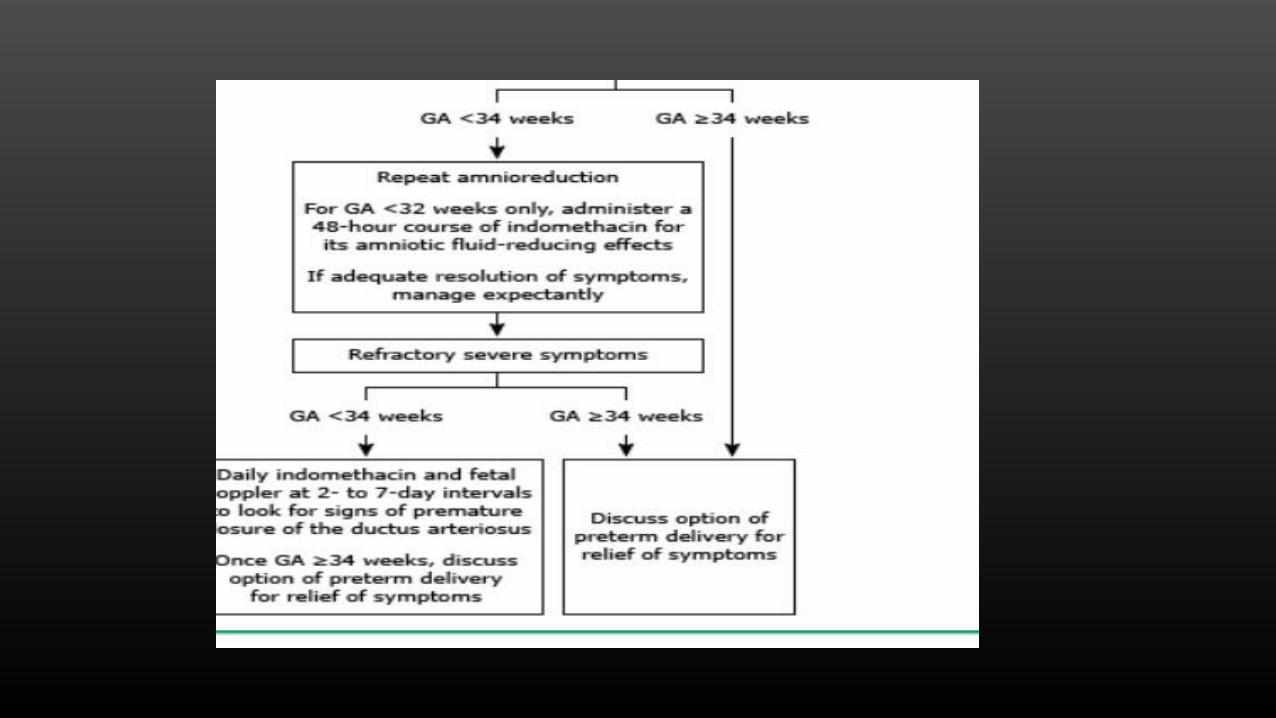
All patients — We perform antepartum fetal monitoring in all patients with idiopathic polyhydramnios:
• For mild to moderate polyhydramnios, we perform a biophysical profile (BPP) with the nonstress test (NST) component upon diagnosis and then every 1 to 2 weeks until 37 weeks, and then weekly from 37 weeks to delivery.
• For severe polyhydramnios, we perform the BPPs (including NST) every week from diagnosis until delivery. In interpreting the BPP score, clinicians should be cautious about conclusions of fetal well-being with a borderline score (6/8) since the two points for amniotic fluid volume (AFV) in these cases are not reassuring.

Rhesus isoimmunization

Rhesus system • Contains 45 different antigens
• The most clinically relevant; D, c and E
• In practice; only anti-D + anti-c cause HDFN, others rarely give rise to problem and anti-D is much more common than anti-c.
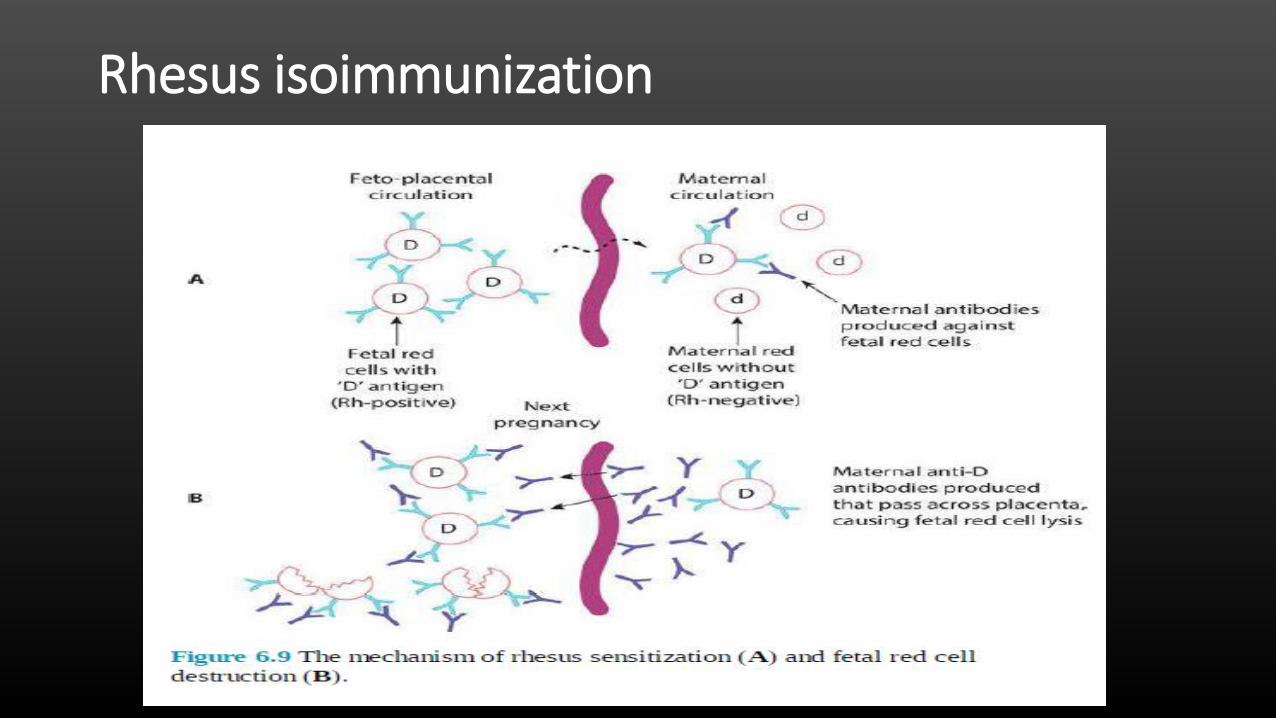
Rhesus isoimmunization • Occurrence of HDFN as a result of rhesus isoimmunization involves
three key stages
1. Firstly, a rhesus-negative mother must conceive a baby who has inherited the rhesus-positive phenotype from the father.
2. Secondly, fetal cells must gain access to the maternal circulation in a sufficient volume to provoke a maternal antibody response.
3. Finally, maternal antibodies must cross the placenta and cause immune destruction of red cells in the fetus.
Pathophysiology
• Rhesus disease does not affect a first pregnancy as the primary response is usually weak and consists primarily of immunoglobulin IgM antibodies that do not cross the placenta.
• However, in a subsequent pregnancy with a rhesus-positive baby, rhesus-positive red cells pass from the baby to the maternal circulation and cause maternal resensitization
• On this occasion, the B-cells produce a much larger response, this time of IgG antibodies that can cross the placenta to the fetal circulation.
Effect on the fetus and neonate
• Placental transfer of Anti-D IgG is possible
• Transfer is slow initially, rising from 20 weeks until term
• At term, IgG levels in fetus can exceed levels in the mother
• IgG attaches to the D antigen on fetal RBCs
• Antibody-antigen complex formed then destroyed by the reticuloendothelial system (spleen and liver)
• Fetus is at risk of anemia, may lead to hydrops and death
Pathophysiology
• Anti D antibodies remain for life
• In subsequent pregnancy
• If the fetus is Rh D positive
• A small FMH will elicit a big maternal immune response
• Production of Anti-D IgG antibodies
• Will cross the placenta to fetal circulation
• Hemolysis of fetal Rh +ve RBCs in the spleen and liver
Pathophysiology
In case of prior Rh-D disease, it either
• Recurs with the same severity OR
• Becomes progressively more severe
If previous fetal hydrops
• Risk in subsequent pregnancies: 90%
• Develops at same GA or earlier than in previous pregnancy
Rhesus isoimmunization • Risk of sensitization depends largely upon the following 3 factors:
1. Volume of transplacental hemorrhage 2. Extent of the maternal immune response 3. Presence of ABO incompatibility (protective factor)
Sensitizing events During pregnancy and delivery
• Miscarriage. Ectopic. Molar. Surgical Mx of miscarriage
• Chorionic villous sampling, Amniocentesis, Cordocentesis
• Antepartum haemorrhage
• External cephalic version
• Trauma to gravid uterus
• Delivery: vaginal and CS
Other sensitizing events
• Transfusion of RhD +ve blood: Mismatched blood or stem cells
• Needle injection contaminated with RhD +ve RBC
Rhesus isoimmunization
How does the fetus respond? If hemolysis is mild • Compensates by increasing erythropoiesis If hemolysis is severe (severe fetal anemia) • Extramedullary hematopoiesis • Portal hypertension • Hypoalbuminemia • Hyperbilirubinemia • Heart failure (hydrops fetalis) • IUFD Hyperbilirubinemia causes CNS damage • Neonatal encephalopathy • kernicterus


Screening

Screening • Identify women at risk to prevent immunisation
• Identify women already have D alloimmunity in order to identify at risk fetuses
• Maternal booking visit blood tests should include blood group & Rh determination
• If Rh –ve: test for Anti-D antibodies • If Anti- Antibodies are negative:
• Mother is not sensitized
• A further check for antibodies at 28-30 weeks
• Prevention is recommended (Anti-D Ig prophylaxis)
• If Ant-D antibodies are positive: • Mother is sensitized either known or new
• Management of alloimmunisation started
Screening
Prevention of sensitization
Principles of prevention Avoid exposure
• Rh appropriate transfusion
• Avoid contaminated needles
Prevent sensitization
• Anti-D immunoglobulins prophylaxis
• Given within 72 hours of sensitizing event
• Anti-D immunoglobulins ‘mop up’ any circulating rhesus-positive cells before an immune response is excited in the mother.
Limit sensitization if already exposed
• Anti-D after sensitizing events (<72 hours)

Routine antenatal anti-D prophylaxis
Routine prophylaxis can be given as:
Antenatally
• 2 doses of anti-D at 28 weeks & at 34 weeks OR
• A single dose either at 28 weeks or 34 weeks
Give Anti-D
• After a potentially sensitizing event
• May use Kleihauer test to calculate dose in indicated: how much fetal blood entered the maternal circulation to calculate the the amount of anti-d to give [not routinely done]
Kleihauer - Betke test (Acid elusion test) • A method of quantifying feto–maternal hemorrhage (FMH), % fetal
RBC in maternal circulation
• Have a threshold of 5 mL of FMH to be positive
• Amount of FMH to cause immunization: 0.01-0.03 ml
• Therefore • It is NOT a test to determine if there is FMH, but to better estimate
the amount of FMH • If positive, it is used to determine additional Anti-D over the
standard 150 to 300 mcg that should be administered • 300 mcg Anti-D protects against 30 ml of fetal cells
Guideline for anti‐D Routine Antenatal Anti‐D Prophylaxis • Administered regardless of and in addition to any anti‐D that may have been
given for a potentially sensitizing event Following birth • Baby’s ABO & Rh D status checked on cord blood • If baby is D +ve, a previously non‐sensitised mother, should be offered at
least 500 IU of anti‐D Ig within 72 h • If indicated, maternal blood should be tested for the size of FMH to adjust
extra dose(s) of Anti-D needed For IUFD • May not be able to obtain fetal blood sample • Anti‐D Ig should be administered to D -ve, previously non‐sensitised mother
within 72 h of the Dx of IUFD, irrespective of the time of subsequent delivery
Guideline for anti‐D
Threatened miscarriage before 12 weeks
• Rh D antigen reported on fetal RBC as early as GA: 7.5 wk
• FMH happened in 3–11% of women with threatened
• Miscarriage from GA of 7 to 13 weeks
• Consider Anti-D when bleeding is heavy, repeated, associated with abdominal pain and close to 12 weeks.
• Consider: ectopic pregnancy, molar pregnancy, therapeutic termination of pregnancy
• Dose: 250 IU
For potentially sensitizing events between 12 and 20 weeks gestation
• A minimum dose of 250 IU should be administered within 72 hours of the event and a Kleihauer test should be performed. Further anti-D can be given if indicated by the Kleihauer test.
For potentially sensitizing events after 20 weeks’ gestation:
• a minimum anti-D Ig dose of 500 IU should be administered within 72 hours of the event. Further anti-D can be given if indicated by the Kleihauer test.
Guideline for anti‐D

Management of Rh alloimmunisation
Management History
• Time of sensitization / event (if possible)
• Same or new partner (check his Rh-D status)
• If new partner is:
• Rh-D negative: No further action
• Rh-D positive : Mx
• If known sensitized, ask about previous pregnancies outcome; GA at onset, development of hydrops
• Tends to develop earlier and more severe
• Risk of recurrence of hydrops > 90%
• Determine fetal D antigen status (if possible) by
• Free fetal DNA in maternal blood from 8 weeks
• CVS or amniocentesis If free fetal DNA is not available
• Results and action
• If fetus is D –ve : no further action
• If fetus is D +ve : needs follow up; maternal Anti-D antibody titer
Management
Maternal Anti-D antibody titer
An anti-D level < 4 iu/ml
• HDFN unlikely
An anti-D level > 4 iu/ml but < 15 iu/ml
• Moderate risk of fetal anaemia
An anti-D level of > 15 iu/ml
• Can cause severe fetal anaemia
Anti-D levels should be measured
• Every 4 weeks up to 28 weeks
• Every 2 weeks until delivery
• Referral for fetal medicine once anti-D levels are > 4 iu/ml
Monitoring of pregnancies at risk of fetal anaemia If anti-D antibody titre is rising > 4 iu/ml, perform;
• Weekly Doppler study of the Middle cerebral artery (MCA) to measure peak systolic velocity (MCA PSV)
• Ultrasound scan (USS)
• Early feature of fetal anemia • MCA PSV > 1.5 multiple of the median • USS evidence of anemia (ascites is an early sign)
If anemia develops, consider intrauterine transfusion
Fetal Anemia Assessment for severity of fetal anemia 1. Middle cerebral artery-peak systolic velocity — Doppler assessment based on
the principle that the anemic fetus preserves oxygen delivery to the brain by increasing cerebral flow of low viscosity blood, The risk of anemia is highest in fetuses with a peak systolic velocity of 1.5 times the median or higher.
2. Spectral analysis of amniotic fluid — In the past, amniocentesis to determine amniotic fluid bilirubin levels was the usual method for indirectly estimating the severity of fetal anemia. Bilirubin present in amniotic fluid derives from fetal pulmonary and tracheal effluents and correlates with the degree of fetal hemolysis.
3. Fetal blood sampling — Ultrasound-directed fetal blood sampling (ie, percutaneous umbilical blood sampling, cordocentesis, funipuncture) allows direct access to the fetal circulation to obtain important laboratory values such as hematocrit, direct Coombs, fetal blood type, reticulocyte count, and platelet count.

Fetal anemia • Sign of fetal anemia features are not obvious unless the fetal hemoglobin is less than 6 g/dl.
1. Polyhydramnios.
2. Enlarged fetal heart.
3. Ascites and pericardial effusions.
4. Reduced fetal movements.
5. Hyperdynamic fetal circulation (can be detected by Doppler ultrasound by measuring increased velocities in the middle cerebral artery or aorta).
6. Abnormal CTG with reduced variability, eventually a ‘sinusoidal’ trace.
Monitoring of pregnancies at risk of fetal anaemia
Fetal hydrops • An overt sign of fetal anemia
• Defined as an ultrasound finding of fluid in two or more compartments:
• Ascites
• Pleural effusion
• Pericardial effusion
• Scalp oedema
• Skin oedema
Fetal anemia Treatment Delivery or Fetal blood transfusion. • Delivery of the fetus is an option if the fetus is sufficiently mature.
• When we deliver the fetus ?
• If there is no complications we wait until the 36 – 37 weeks
• If there is complications we try to keep the blood level of the fetus in normal values (by transfusion) until the age of 34 weeks then we do the delivery
Delivery Timing of delivery depend on
• The antibody levels / titers rate of rise
• If any fetal therapy has been required
• Consider steroids for lung maturity
Mode
• High risk; therefore continuous FHR monitoring
• Standard obstetrics indications
Place of delivery
• NICU well equipped unit
Intrauterine transfusion (IUT) • Once a decision has been made that the fetus is severely anemic and requires a blood
transfusion, the invasive procedure aims to first take a sample to confirm the anemia and then infuse the blood during a single puncture.
• Intra-vascular and Intra-peritonial
• May need to repeat several times
• Overall chance of survival of anemic fetus is 85% to 90% if transfused
Complication • Complication rate: 2% per IUT procedure
• Include: o PPROM o Preterm labour o Infection o Fetal distress , IUFD
Fetal anemia Transfused blood should be
1. RhD negative
2. Crossmatched with a maternal sample;
3. Densely packed (Hb usually around 30 g/L) so that small volumes are used
4. White cell depleted and irradiated;
5. Screened for infection including CMV.
Fetal anemia At delivery • If the baby is known to be anemic or has had multiple transfusions, a
neonatologist must be present at delivery should exchange transfusion be required.
• Blood must therefore always be ready for the delivery. All babies born to rhesus negative women should have cord blood taken at delivery for a blood count, blood group and indirect Coombs test.
Management of the neonate
• Early discharge is not advisable
• Regular assessment of neuro-behavioural state
• Observed for development of jaundice and / or anemia
• Regular assessment of bilirubin and Hb levels
• Encourage breast feeding
• Pregnancies with a minimal or no risk of fetal or neonatal anemia require no specific treatment

Thank you

















