OBSTETRICS Amniotic fluid infection, inflammation, and colonization in preterm labor with intact membranes C. Andrew Combs, MD, PhD; Michael Gravett, MD; Thomas J. Garite, MD; Durlin E. Hickok, MD, MPH; Jodi Lapidus, PhD; Richard Porreco, MD; Julie Rael, RN; Thomas Grove, PhD; Terry K. Morgan, MD, PhD; William Clewell, MD; Hugh Miller, MD; David Luthy, MD; Leonardo Pereira, MD; Michael Nageotte, MD; Peter A. Robilio, MD; Stephen Fortunato, MD; Hyagriv Simhan, MD; Jason K. Baxter, MD; Erol Amon, MD; Albert Franco, MD; Kenneth Trofatter, MD; Kent Heyborne, MD; for the ProteoGenix/Obstetrix Collaborative Research Network OBJECTIVE: The purpose of this study was to compare intraamniotic inflammation vs microbial invasion of the amniotic cavity (MIAC) as predictors of adverse outcome in preterm labor with intact membranes. STUDY DESIGN: Interleukin-6 (IL-6) was measured in prospectively collected amniotic fluid from 305 women with preterm labor. MIAC was defined by amniotic fluid culture and/or detection of microbial 16S ribosomal DNA. Cases were categorized into 5 groups: infection (MIAC; IL-6, 11.3 ng/mL); severe inflammation (no MIAC; IL-6, 11.3 ng/mL); mild inflammation (no MIAC; IL-6, 2.6-11.2 ng/mL); colonization (MIAC; IL-6, <2.6 ng/mL); negative (no MIAC; IL-6, <2.6 ng/mL). RESULTS: The infection (n ¼ 27) and severe inflammation (n ¼ 36) groups had similar latency (median, <1 day and 2 days, respectively) and similar rates of composite perinatal morbidity and mortality (81% and 72%, respectively). The colonization (n ¼ 4) and negative (n ¼ 195) groups had similar outcomes (median latency, 23.5 and 25 days; composite morbidity and mortality rates, 21% and 25%, respectively). The mild inflammation (n ¼ 47) groups had outcomes that were intermediate to the severe inflammation and negative groups (median latency, 7 days; composite morbidity and mortality rates, 53%). In logistic regression adjusting for gestational age at enrollment, IL-6 11.3 and 2.6-11.2 ng/mL, but not MIAC, were associated significantly with composite morbidity and mortality rates (odds ratio [OR], 4.9; 95% confidence interval [CI], 2.2e11.2, OR, 3.1; 95% CI, 1.5e6.4, and OR, 1.8; 95% CI, 0.6e5.5, respectively). CONCLUSION: We confirmed previous reports that intraamniotic inflammation is associated with adverse perinatal outcomes whether or not intraamniotic microbes are detected. Colonization without inflammation appears relatively benign. Intraamniotic inflammation is not simply present or absent but also has degrees of severity that correlate with adverse outcomes. We propose the designation amni- otic inflammatory response syndrome to denote the adverse outcomes that are associated with intraamniotic inflammation. Key words: chorioamnionitis, intraamniotic infection, intraamniotic inflammation, microbial invasion of the amniotic cavity, morbidity, preterm birth, preterm labor Cite this article as: Combs CA, Gravett M, Garite TJ, et al. Amniotic fluid infection, inflammation, and colonization in preterm labor with intact membranes. Am J Obstet Gynecol 2014;210:125.e1-15. From the Center for Research, Education, and Quality, Mednax, Inc., Sunrise, FL (Drs Combs and Garite and Ms Rael); Obstetrix Medical Group, San Jose, CA (Dr Combs); University of Washington Medical Center, Seattle, WA (Drs Gravett and Robilio); ProteoGenix, Inc., Costa Mesa, CA (Drs Hickok and Grove); Oregon Health and Science University, Portland, OR (Drs Lapidus, Morgan, and Pereira); Obstetrix Medical Group of Colorado, Denver, CO (Drs Porreco and Heyborne and Ms Rael); Obstetrix Medical Group, Phoenix Perinatal Associates, Phoenix, AZ (Dr Clewell); Obstetrix Medical Group of Arizona, Tucson, AZ (Dr Miller); Obstetrix Medical Group of Washington, Seattle, WA (Dr Luthy); Obstetrix Medical Group, Southern California, Long Beach, CA (Dr Nageotte); Perinatal Research Group, Nashville, TN (Dr Fortunato); University of Pittsburgh, Pittsburgh, PA (Dr Simhan); Thomas Jefferson University, Philadelphia, PA (Dr Baxter); St. Louis University School of Medicine, St. Louis, MO (Dr Amon); Carolinas Medical Center, Charlotte, NC (Dr Franco); and University Medical Center, Greenville, SC (Dr Trofatter). Received July 29, 2013; revised Oct. 20, 2013; accepted Nov. 20, 2013. Supported by a research grant from ProteoGenix, Inc; statistical analyses supported by Hologic, Inc. Each author had grant support, consulting arrangements, employment, or equity interests with the sponsor, ProteoGenix, Inc. C.A.C. and T.J.G. have served on advisory boards; J.L. has a consulting arrangement, and J.K.B. has an unrelated research grant with Hologic, Inc, which acquired ProteoGenix in 2010. Presented at the 33rd annual meeting of the Society for Maternal-Fetal Medicine, San Francisco, CA, Feb. 11-16, 2013. Reprints not available from the authors. 0002-9378/$36.00 ª 2014 Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.ajog.2013.11.032 FEBRUARY 2014 American Journal of Obstetrics & Gynecology 125.e1 Research www. AJOG.org
Transcript
Research www.AJOG.org
OBSTETRICS
Amniotic fluid infection, inflammation, and colonization inpreterm labor with intact membranesC. Andrew Combs, MD, PhD; Michael Gravett, MD; Thomas J. Garite, MD; Durlin E. Hickok, MD, MPH;Jodi Lapidus, PhD; Richard Porreco, MD; Julie Rael, RN; Thomas Grove, PhD; Terry K. Morgan, MD, PhD;William Clewell, MD; Hugh Miller, MD; David Luthy, MD; Leonardo Pereira, MD; Michael Nageotte, MD;Peter A. Robilio, MD; Stephen Fortunato, MD; Hyagriv Simhan, MD; Jason K. Baxter, MD; Erol Amon, MD;Albert Franco, MD; Kenneth Trofatter, MD; Kent Heyborne, MD; for the ProteoGenix/Obstetrix CollaborativeResearch Network
OBJECTIVE: The purpose of this study was to compare intraamniotic that were intermediate to the severe inflammation and negative
inflammation vs microbial invasion of the amniotic cavity (MIAC)as predictors of adverse outcome in preterm labor with intactmembranes.
STUDY DESIGN: Interleukin-6 (IL-6) was measured in prospectivelycollected amniotic fluid from 305 women with preterm labor.MIAC was defined by amniotic fluid culture and/or detection ofmicrobial 16S ribosomal DNA. Cases were categorized into5 groups: infection (MIAC; IL-6, �11.3 ng/mL); severe inflammation(no MIAC; IL-6, �11.3 ng/mL); mild inflammation (no MIAC; IL-6,2.6-11.2 ng/mL); colonization (MIAC; IL-6, <2.6 ng/mL); negative(no MIAC; IL-6, <2.6 ng/mL).
RESULTS: The infection (n ¼ 27) and severe inflammation (n ¼ 36)groups had similar latency (median, <1 day and 2 days, respectively)and similar rates of composite perinatal morbidity and mortality(81% and 72%, respectively). The colonization (n¼ 4) and negative(n ¼ 195) groups had similar outcomes (median latency, 23.5 and25 days; composite morbidity and mortality rates, 21% and 25%,respectively). The mild inflammation (n¼ 47) groups had outcomes
From the Center for Research, Education, and Quality, Mednax, Inc., SunrisSan Jose, CA (Dr Combs); University of Washington Medical Center, Seattle(Drs Hickok and Grove); Oregon Health and Science University, Portland, ORDenver, CO (Drs Porreco andHeyborne andMsRael); ObstetrixMedical GrouGroup of Arizona, Tucson, AZ (Dr Miller); Obstetrix Medical Group of WashingLong Beach, CA (Dr Nageotte); Perinatal Research Group, Nashville, TN (DrJefferson University, Philadelphia, PA (Dr Baxter); St. Louis University SchoolNC (Dr Franco); and University Medical Center, Greenville, SC (Dr Trofatter).
Received July 29, 2013; revised Oct. 20, 2013; accepted Nov. 20, 2013.
Supported by a research grant from ProteoGenix, Inc; statistical analyses su
Each author had grant support, consulting arrangements, employment, or ehave served on advisory boards; J.L. has a consulting arrangement, and J.KProteoGenix in 2010.
Presented at the 33rd annual meeting of the Society for Maternal-Fetal Medi
Reprints not available from the authors.
0002-9378/$36.00 � ª 2014 Mosby, Inc. All rights reserved. � http://dx.doi.org/10.1
groups (median latency, 7 days; composite morbidity and mortalityrates, 53%). In logistic regression adjusting for gestational age atenrollment, IL-6 �11.3 and 2.6-11.2 ng/mL, but not MIAC, wereassociated significantly with composite morbidity and mortalityrates (odds ratio [OR], 4.9; 95% confidence interval [CI],2.2e11.2, OR, 3.1; 95% CI, 1.5e6.4, and OR, 1.8; 95% CI,0.6e5.5, respectively).
CONCLUSION: We confirmed previous reports that intraamnioticinflammation is associated with adverse perinatal outcomes whetheror not intraamniotic microbes are detected. Colonization withoutinflammation appears relatively benign. Intraamniotic inflammation isnot simply present or absent but also has degrees of severity thatcorrelate with adverse outcomes. We propose the designation amni-otic inflammatory response syndrome to denote the adverse outcomesthat are associated with intraamniotic inflammation.
Key words: chorioamnionitis, intraamniotic infection, intraamnioticinflammation, microbial invasion of the amniotic cavity, morbidity,preterm birth, preterm labor
Cite this article as: Combs CA, Gravett M, Garite TJ, et al. Amniotic fluid infection, inflammation, and colonization in preterm labor with intact membranes. Am J ObstetGynecol 2014;210:125.e1-15.
e, FL (Drs Combs and Garite and Ms Rael); Obstetrix Medical Group,, WA (Drs Gravett and Robilio); ProteoGenix, Inc., Costa Mesa, CA(Drs Lapidus, Morgan, and Pereira); Obstetrix Medical Group of Colorado,p, Phoenix Perinatal Associates, Phoenix, AZ (Dr Clewell); ObstetrixMedicalton, Seattle, WA (Dr Luthy); Obstetrix Medical Group, Southern California,Fortunato); University of Pittsburgh, Pittsburgh, PA (Dr Simhan); Thomasof Medicine, St. Louis, MO (Dr Amon); Carolinas Medical Center, Charlotte,
pported by Hologic, Inc.
quity interests with the sponsor, ProteoGenix, Inc. C.A.C. and T.J.G..B. has an unrelated research grant with Hologic, Inc, which acquired
cine, San Francisco, CA, Feb. 11-16, 2013.
016/j.ajog.2013.11.032
FEBRUARY 2014 American Journal of Obstetrics & Gynecology 125.e1
I mation are well-documented causesof preterm labor with intact fetalmembranes, especially at very earlygestational ages.1 Cultures for microor-ganisms in amniotic fluid demonstratemicrobial invasion of the amniotic cavity(MIAC) in 20-60% of women with pre-term labor at <28 weeks of gestationand 10-25% at 28-32 weeks of gesta-tion.2-4 Culture-proven MIAC is associ-ated with short latency to delivery andhigh rates of perinatal morbidity andmortality.2-5
Even with culture-negative amnioticfluid, however, women in preterm laboroften have intraamniotic inflammation,which is evidenced by elevated amnioticfluid levels of inflammatory markerssuch as interleukin-6 (IL-6),3,5-11 otherproinflammatory cytokines and che-mokines,6,10-13 tumor necrosis factoralpha,4,6,10,14 or matrix metallo-proteinase-8 (MMP-8).15-17 Whether ornot the amniotic fluid culture is positive,intraamniotic inflammation is associ-ated with short latency3-5,7,9,12-18 andhigh rates of perinatal morbidity andmortality.3-5,14,17,18
One explanation for the morbiditythat is associated with culture-negativeintraamniotic inflammation is thatmany cases actually have MIAC but thatthe amniotic fluid cultures are falselynegative. Using polymerase chain reac-tion (PCR) amplification, several groupshave demonstrated prokaryotic 16Ssubunit ribosomal RNA or the DNAcoding for it (rDNA) in amniotic fluid inmany culture-negative preterm laborcases.19-26 The microbes that are identi-fied by 16S PCR techniques are oftenfacultative organisms that are difficult toculture with standard techniques. Pre-term labor cases with 16S PCR-provenMIAC have similar outcomes to caseswith culture-proven MIAC,19-21,23-25
which suggests true infection and notsimply detection of nonviable microbialdegradation products.
In principle, MIAC and the intra-amniotic inflammatory response aredistinct entities. In the simplest model,each of them can be either present orabsent; therefore, states of amnioticfluid are possible: (1) infection (MIAC
125.e2 American Journal of Obstetrics & Gynecol
and inflammatory response both pre-sent), (2) inflammation (inflammatoryresponse present, MIAC absent); (3)colonization (MIAC present, inflamma-tory response absent); (4) negative (bothabsent).Moreover, the inflammatory response
is not simply present or absent but is acontinuum. A recent report suggestedthat clinical outcomes correlated withgradations in inflammatory responsethat varied from “no” to “minimal” to“severe,” with categories defined by thenumber of biomarkers that are presentin amniotic fluid.27 To our knowledge,there has been no previous report thathas investigated whether the severity ofoutcomes might be graded similarlybased on the concentration of a singleinflammatory marker.The aims of the present investigation
were to compare the outcomes of pre-term labor in women with intraamnioticinfection, inflammation, or colonizationand to examine whether the outcomesare related to the severity of the inflam-matory response as defined by intra-amniotic IL-6 levels.
MATERIALS AND METHODS
This report involved a subset of subjectsfrom a larger multicenter study, the goalof which was to develop a noninvasivetest to screen for intraamniotic infectionbased on cervicovaginal proteins. Theprotocol was approved by the local in-stitutional review board at each par-ticipating site.
Inclusion/exclusion criteriaWe included consenting women whowere at least 18 years old with singletonpregnancies at 15.0-36.9 weeks of ges-tation in spontaneous preterm laborwith intact fetal membranes and whounderwent amniocentesis to evaluate forintraamniotic infection and to measureamniotic fluid IL-6. Preterm labor wasdefined as regular uterine contractionsplus at least 1 of the following: cervicaldilation �2 cm; cervical length bytransvaginal sonography �30 mm; or apositive cervicovaginal fetal fibronectintest. The protocol required cervicallength by transvaginal sonography orfetal fibronectin test only if cervical
ogy FEBRUARY 2014
dilation was <2 cm. Each of theparticipating sites was a tertiary perinatalcenter where amniocentesis was offeredroutinely to women with preterm labor,although several centers restricted theprocedure to <34 weeks of gestation.Exclusion criteria were ruptured mem-branes, major fetal anomaly, fetal aneu-ploidy, or a medical indication forpreterm birth.
SpecimensAmniotic fluid was obtained by trans-abdominal amniocentesis with the use ofsonographic guidance and antisepticskin preparation. A 5-mL aliquot wassent to the local hospital laboratory forassessment of glucose concentration,white blood cell count (WBC), Gramstain, and aerobic and anaerobic culture,which included genital mycoplasmas atsome laboratories. A 10-mL aliquot ofamniotic fluid was frozen at e80�C and
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
Research Obstetrics www.AJOG.org
shipped to the central laboratory atProteoGenix, Inc (Costa Mesa, CA).
If delivery occurred at the study hos-pital, a full-thickness placental biopsythat included chorionic plate and asegment of umbilical cord within 2-3 cmfrom the placental insertion site wereobtained and fixed in formalin. Biopsyspecimens were interpreted by a placentalpathologist (T.K.M.) who was blinded toclinical and laboratory findings.
Additional specimens that were ob-tained as part of the parent study but werenot considered for the present studyincluded samples of maternal plasma,cervicovaginal secretions, urine at en-rollment, and cord blood at delivery.
TreatmentManagement of preterm labor, durationof hospitalization, route of delivery,diagnosis and management of infection,and other clinical decisions were leftto the discretion of the caregivers andnot specified by the protocol. The only
125.e4 American Journal of Obstetrics & Gynecol
study-specific procedures were the col-lection of specimens: the extra aliquot ofamniotic fluid, cervicovaginal swabs,maternal plasma and urine, cord blood,and placental biopsy specimens. Care-givers had access to local hospital labo-ratory results but were blinded to allresults from the central laboratory.
Central laboratory methodsAmniotic fluid IL-6 concentration wasassayed with a quantitative sandwichenzyme immunoassay (Quantikine ELISA#D6050; R&D Systems, Minneapolis,MN).Cultures of amniotic fluid were per-
formed on an aliquot of amniotic fluidthat had been sent to reference labora-tories at the University of Washington(through May 2008) or Focus Di-agnostics Inc (Cypress, CA; after June2008). Broth enrichment techniqueswere used to detect low levels of aerobicand anaerobic bacteria, including genitalmycoplasmas, as described elsewhere.2
ogy FEBRUARY 2014
PCR for amniotic fluid 16S rDNAwasperformed on DNA that was extractedwith the use of an FFTE kit and Maxwell16 system (Promega, Madison, WI). Theoptimized PCR reaction included uni-versal 16S rDNA primers 5F and 531R(Invitrogen Life Technologies, Carlsbad,CA). All extraction runs included knownpositive and negative controls that weregenerated by spiking the water samplewith Staphylococcus aureus. Positive sam-ples, which were identified by the pres-ence of amplicon of 460-560 base pair,were ligated into the pCR4 TOPO vectorand transformed into Escherichia coliTOP10 cells with the use of the TOPO-TAcloning kit (Invitrogen Life Technol-ogies). After overnight incubation onampicillin-containing agar, up to 24clones per sample were selected. Plasmidswere isolated from bacterial colonies withthe QIAprep Spin kit (Qiagen Sciences,Germantown, MD). Inserts from 24plasmids that were generated from eachpositive PCR were sequenced with an AB
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
www.AJOG.org Obstetrics Research
3730xl sequencer (Applied Biosystems,Foster City, CA) with the custom primersBac16S_8F2 and Bac16S_R518. For bac-terial identification, bidirectional se-quences were processed with MicroSeqanalysis software (Applied Biosystems),and MicroSeq ID 16S rDNA 500 Libraryv2.0. Ureaplasma urealyticum and Snea-thia sanguinegens sequences were addedto create custom libraries.
Groups defined by amniotic fluidresultsTo define groups, we used the cut-offamniotic fluid IL-6 concentrations of11.3 ng/mL5,18 and 2.6 ng/mL3 that hadbeen determined by previous in-vestigators. MIAC was defined by apositive 16S rDNA result and/or a posi-tive culture from either the local hospitaland/or reference laboratory.
For analysis, cases were divided into 5groups based on amniotic fluid results:(1) infection group: MIAC plus IL-6concentration of �11.3 ng/mL; (2) se-vere inflammation group: no MIAC, IL-6 concentration of �11.3 ng/mL; (3)mild inflammation group: no MIAC,
IL-6 concentration of 2.6-11.2 ng/mL;(4) colonization group: MIAC, IL-6concentration of <2.6 ng/mL; and (5)negative group: no MIAC, IL-6 concen-tration of <2.6 ng/mL. These groupswere compared regarding baseline char-acteristics, pregnancy outcomes, andneonatal outcomes.
DefinitionsClinical chorioamnionitis was defined asantenatal maternal fever (�100.4�F)plus either maternal leukocytosis (WBC>15,000/mm3), uterine tenderness topalpation, and/or fetal tachycardia (base-line fetal heart rate >160 beats/min).Histologic chorioamnionitis was de-
fined by the presence of neutrophilsthat marginated into the placental cho-rionic plate; funisitis was defined by thepresence of neutrophils in the umbilicalcord vessel walls.28
Composite perinatal morbidity anddeath was defined as any �1 the fol-lowing events: stillbirth, neonatal death,respiratory distress syndrome, grade 3 or4 intraventricular hemorrhage, necro-tizing enterocolitis, or culture-positive
FEBRUARY 2014 Ameri
neonatal sepsis. Neonatal outcomeswere assessed from birth to 28 days oflife or until hospital discharge, which-ever came first.
Statistical analysesBetween-group differences were testedwith c2 or Fisher exact test for categoricvariables, t test and analysis of variancefor continuous variables (with log-transformation as appropriate), andlog-rank test for time-to-event curves.Multivariable logistic regression analyseswere performed to examine predictorsof short latency, composite perinatalmorbidity and mortality rates, or com-posite morbidity andmortality rates thatexcluded respiratory distress syndromeand were adjusted for gestational age atenrollment or gestational age at delivery.One set of regression models includedMIAC (present or absent) and amnioticfluid IL-6 concentration (�11.3, 2.6-11.2, or <2.6 ng/mL) as predictors.Another set of models included the5 defined groups as predictors. Proba-bility values of < .05 were consideredsignificant.
RESULTS
From September 2007 through No-vember 2009, 338 women who met allthe inclusion criteria were enrolled at 16sites. Of these, 18 women withdrew orwere lost to follow-up evaluation, and15 were excluded because of inadequatespecimens, which left 305 women for theanalyses presented here. The number ofwomen at each site and the gestationalages at amniocentesis are tabulated inTable 1.
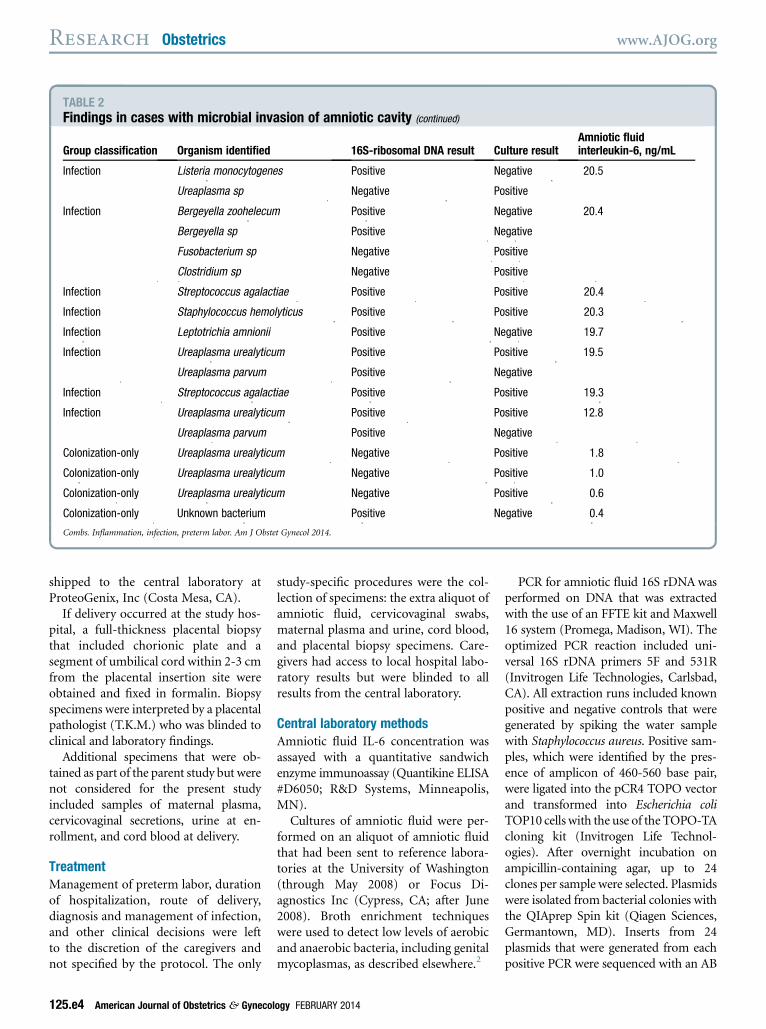
Groups defined by amniotic fluidresultsMIAC was found in 31 of 305 women(10.1%). As summarized in Table 2, 20of these cases (65%) were both 16SrDNA PCR-positive and culture-positive;6 cases (19%) were PCR-positive butculture-negative, and 5 cases (16%) wereculture-positive but PCR-negative.
The distribution of amniotic fluidIL-6 concentrations that was used in thedesignation of the 5 groups is shown inFigure 1. IL-6 concentration of �11.3ng/mL was found in 63 cases (20.7%),
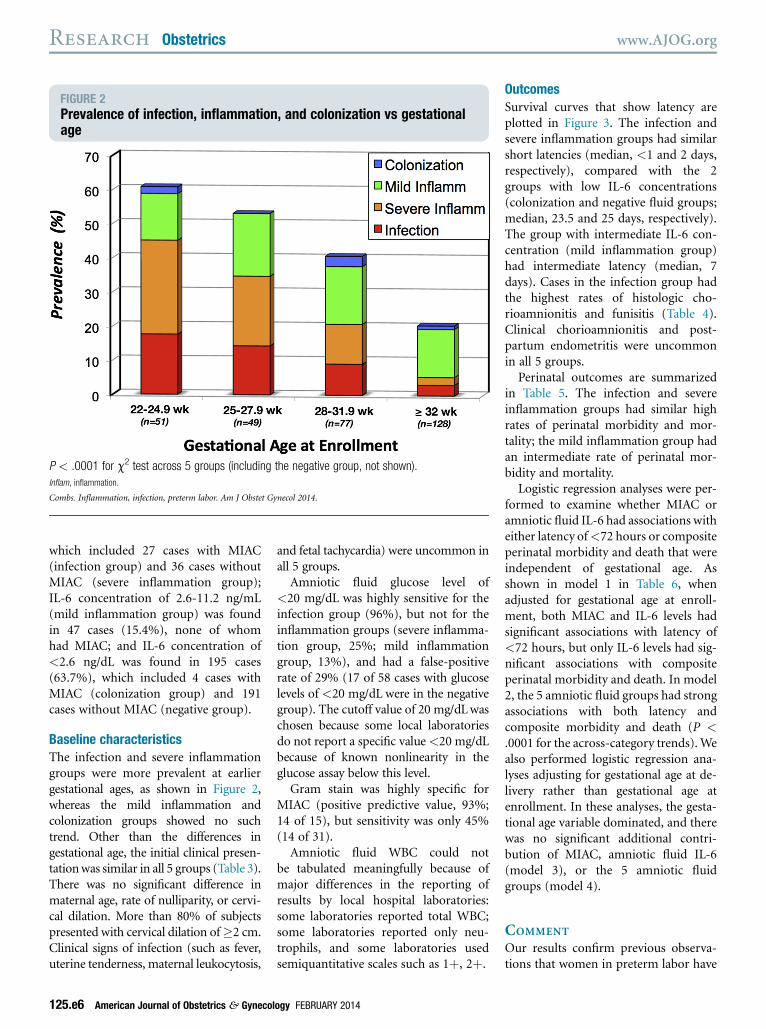
FIGURE 2Prevalence of infection, inflammation, and colonization vs gestationalage
P < .0001 for c2 test across 5 groups (including the negative group, not shown).Inflam, inflammation.
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
Research Obstetrics www.AJOG.org
which included 27 cases with MIAC(infection group) and 36 cases withoutMIAC (severe inflammation group);IL-6 concentration of 2.6-11.2 ng/mL(mild inflammation group) was foundin 47 cases (15.4%), none of whomhad MIAC; and IL-6 concentration of<2.6 ng/dL was found in 195 cases(63.7%), which included 4 cases withMIAC (colonization group) and 191cases without MIAC (negative group).
Baseline characteristicsThe infection and severe inflammationgroups were more prevalent at earliergestational ages, as shown in Figure 2,whereas the mild inflammation andcolonization groups showed no suchtrend. Other than the differences ingestational age, the initial clinical presen-tationwas similar in all 5 groups (Table 3).There was no significant difference inmaternal age, rate of nulliparity, or cervi-cal dilation. More than 80% of subjectspresented with cervical dilation of�2 cm.Clinical signs of infection (such as fever,uterine tenderness, maternal leukocytosis,
125.e6 American Journal of Obstetrics & Gynecol
and fetal tachycardia) were uncommon inall 5 groups.Amniotic fluid glucose level of
<20 mg/dL was highly sensitive for theinfection group (96%), but not for theinflammation groups (severe inflamma-tion group, 25%; mild inflammationgroup, 13%), and had a false-positiverate of 29% (17 of 58 cases with glucoselevels of <20 mg/dL were in the negativegroup). The cutoff value of 20 mg/dLwaschosen because some local laboratoriesdo not report a specific value<20 mg/dLbecause of known nonlinearity in theglucose assay below this level.Gram stain was highly specific for
MIAC (positive predictive value, 93%;14 of 15), but sensitivity was only 45%(14 of 31).Amniotic fluid WBC could not
be tabulated meaningfully because ofmajor differences in the reporting ofresults by local hospital laboratories:some laboratories reported total WBC;some laboratories reported only neu-trophils, and some laboratories usedsemiquantitative scales such as 1þ, 2þ.
ogy FEBRUARY 2014
OutcomesSurvival curves that show latency areplotted in Figure 3. The infection andsevere inflammation groups had similarshort latencies (median, <1 and 2 days,respectively), compared with the 2groups with low IL-6 concentrations(colonization and negative fluid groups;median, 23.5 and 25 days, respectively).The group with intermediate IL-6 con-centration (mild inflammation group)had intermediate latency (median, 7days). Cases in the infection group hadthe highest rates of histologic cho-rioamnionitis and funisitis (Table 4).Clinical chorioamnionitis and post-partum endometritis were uncommonin all 5 groups.
Perinatal outcomes are summarizedin Table 5. The infection and severeinflammation groups had similar highrates of perinatal morbidity and mor-tality; the mild inflammation group hadan intermediate rate of perinatal mor-bidity and mortality.
Logistic regression analyses were per-formed to examine whether MIAC oramniotic fluid IL-6 had associations witheither latency of<72 hours or compositeperinatal morbidity and death that wereindependent of gestational age. Asshown in model 1 in Table 6, whenadjusted for gestational age at enroll-ment, both MIAC and IL-6 levels hadsignificant associations with latency of<72 hours, but only IL-6 levels had sig-nificant associations with compositeperinatal morbidity and death. In model2, the 5 amniotic fluid groups had strongassociations with both latency andcomposite morbidity and death (P <.0001 for the across-category trends).Wealso performed logistic regression ana-lyses adjusting for gestational age at de-livery rather than gestational age atenrollment. In these analyses, the gesta-tional age variable dominated, and therewas no significant additional contri-bution of MIAC, amniotic fluid IL-6(model 3), or the 5 amniotic fluidgroups (model 4).
COMMENT
Our results confirm previous observa-tions that women in preterm labor have
N/A, analysis of variance was not performed because amniotic fluid interleukin-6 was used to define the groups; the difference between the infection and severe inflammation groups was significantat P ¼ .002 (t test on log-transformed values).
a Comparison of subjects across all 5 groups with analysis of variance or c2 test; Fisher exact test was used in lieu of c2 for clinical signs of infection because of the small counts; b Data are givenas mean� SD; c N¼ 27, 35, 46, 4, and 191 for the 5 groups, respectively, because of missing values; d N¼ 24, 30, 46, 4, and 167 for the 5 groups, respectively, because of missing values;e N ¼ 3 for the colonization group and n ¼ 190 for the negative fluid group because of missing values; f Data are given as geometric mean and SD.
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
www.AJOG.org Obstetrics Research
high rates of intraamniotic infection andinflammation, especially at early gesta-tional ages.2-4 We also confirm thatintraamniotic inflammation, which isevidenced by high IL-6 levels, is asso-ciated with short latency and high ratesof perinatal morbidity and mortalitywhether or not microbes are detected inthe amniotic fluid.3,4
We present 4 novel findings: (1) In theinflammation groups, the absence ofMIAC was shown not only by negativeamniotic fluid cultures as in previousreports but also by negative 16S rDNAPCR. (2) The degree of inflammation(mild or severe) as categorized by a single
biomarker (IL-6 concentration) corre-lated with the rate of perinatal morbidityand mortality. (3) The amniotic fluidcolonization group had similar outcomesto the negative group. (4) Amniotic fluidIL-6 level was stronger than MIAC asa predictor of composite perinatal mor-bidity and death in the logistic reg-ressions, but IL-6 concentration was nolonger predictive after adjustment forgestational age at delivery.
Intraamniotic infection (MIAC plushigh IL-6)As in previous reports, we found thatmost cases of intraamniotic infection
FEBRUARY 2014 Ameri
are occult, that is, not associatedwith clinically evident chorioamnioni-tis.2-4,19,22,23,25 In some of these cases,the short latency may have been a re-flection of caregivers’ responses to am-niotic fluid Gram stains, glucose levels,WBC, or other signs of infection. In theremainder, however, the short latencylikely reflected the natural history ofintraamniotic infection.
Intraamniotic inflammation withoutMIACWe confirm previous findings thatculture-negative intraamniotic inflam-mation is associated with short latency
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
Research Obstetrics www.AJOG.org
and perinatal morbidity and death.3-5,18
However, a negative culture does notexclude MIAC adequately because manyintraamniotic bacteria in preterm laborare resistant to culture.19-26 In the pre-sent study, we evaluated amniotic fluidby both sensitive culture techniques andby 16S rDNA. Previous investigatorsfound that 16S-positive cases hadsimilar outcomes to culture-positivecases; however, they did not report theoutcomes of those with elevated in-flammatory markers but who werenegative for both 16S PCR and cultureas a distinct group.20,24,25 We found thatthis group (severe inflammation group)had similar outcomes to those withintraamniotic infection. The short la-tency in these cases must reflect thenatural history of intraamniotic in-flammation and not the caregivers’responses to the diagnosis of inflam-mation because caregivers had no accessto IL-6 results.
125.e8 American Journal of Obstetrics & Gynecol
What triggers intraamniotic inflam-mation in the absence of intraamnioticmicrobes? One possibility is that in-flammation is the response to microbialinvasion of extraamniotic compart-ments such as the decidua,29 mem-branes,8,11,30 or placenta.31,32 Anotherpossibility is that the inflammatory res-ponse might be triggered by noninfec-tious insults such as trauma, ischemia,33
or abruption.34
We confirm an earlier report that theoutcomes of intraamniotic inflamma-tion are not “all-or-nothing” but havegrades of severity that correlate with thelevels of intraamniotic inflammatorymediators.27 The previous report basedseverity on the number of biomarkersthat were present (severe inflammation if3 or 4 markers; minimal inflammation if1 or 2markers). We find that severity canbe based instead on the concentration ofa single marker, amniotic fluid IL-6.High levels of IL-6, with MIAC
ogy FEBRUARY 2014
(infection group) or without MIAC(severe inflammation group), wereassociated with short latencies and highrates of perinatal morbidity and mor-tality, whereas intermediate levels of IL-6(mild inflammation group) were asso-ciated with intermediate latency andperinatal morbidity and death. Thesefindings are supported by another recentreport that concluded that IL-6 alone orMMP-8 alone had equivalent diagnosticperformance to the 4-biomarker scoringsystem in the identification of MIAC orintraamniotic inflammation.35
It is likely that mild inflammation inour cases represents an early stage ina process that progresses to severeinflammation over a period of days toweeks. In a monkey model of pretermlabor that was induced by intraamnioticinoculation of bacteria, for example,levels of bacteria and cytokines rise pro-gressively over time and correlate withthe onset of uterine contractions.36-39
However, it is also possible that mildinflammation might remain mild overtime and simply have a slower time-course of progression to delivery. Ourdata do not allow us to distinguish thesepossibilities because we did not performserial amniocenteses.
Colonization of amniotic fluidOur finding of a few cases of amnioticfluid colonization is consistent withpublished observations. In Table 7, wecompiled 16 studies of preterm laborthat reported on both MIAC and at least1 amniotic fluid marker of inflamma-tion.3-7,9,11,12,15-17,20,23,26,40 Ten of thestudies documented occasional casesthat we would classify as colonization(that is, MIAC with low levels of in-flammatory markers). When we pooledthe data, colonization was found inslightly>1% of all cases of preterm laboror nearly 9% of cases with MIAC. Noneof the other tabulated studies reportedoutcomes of the colonization cases. Wefound that those with colonization hadoutcomes similar to those with negativefluid, although our statistical power islimited by the small number of cases. Uurealyticum accounted for 3 of our 4cases of colonization. This organism is
Postpartum endometritis, n (%) 1 (4) 1 (3) 1 (2) 1 (25) 6 (3) .26a Comparison of subjects across all 5 groups with analysis of variance (gestational age), nonparametric analysis of variance (latency), or c2 test for other outcomes; for histologic chorioamnionitis,funisitis, and postpartum endometritis, the Fisher exact test was used because of small sample sizes; b Data are given as mean � SD; c N ¼ 26 in the infection group because of missing data;d Data are given as median (interquartile range) for latency; e N ¼ 26, 34, 37, 1, and 120 for the 5 groups, respectively, because of missing data.
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
www.AJOG.org Obstetrics Research
common in genital tract flora and un-likely to be a skin contaminant.
Recent evidence challenges the tradi-tional view that the normal intrauterineenvironment is sterile. With the use of16S PCR techniques, bacteria havebeen found in fetal membranes,30
placenta,31,32 and amniotic fluid41 in asubstantial fraction of pregnancies atcesarean delivery without labor, al-though these findings are contradictedby others.42,43 Amniotic fluid fromsecond-trimester genetic amniocentesisin asymptomatic women is culture-positive in 0.3-6.6% of cases44-47 and16S PCR-positive in 10-12%.48,49 Mostof these women carry their pregnanciesuneventfully and deliver at term withoutsequelae,47-49 which suggests coloniza-tion rather than infection. Some of thesewomen have elevated amniotic fluid in-flammatory markers, and these womenare at high risk of miscarriage or pretermbirth.50-54
Inflammation as the maindeterminant of outcomeThe logistic regressions (Table 6) dem-onstrate that IL-6 is more strongly
correlated with latency of <72 hoursand composite perinatal morbidity anddeath than is MIAC (models 1 and 2). Inother words, these adverse outcomes arerelated more closely to intraamnioticinflammation than to the presence ofmicrobes. The observation that the pre-dictive value of IL-6 did not persist afteradjustment for gestational age at delivery(models 3 and 4) suggests that the am-niotic inflammatory response is associ-ated with perinatal morbidity and deathprimarily because of its association withshort latency and early preterm deliveryrather than a direct contribution to fetalor neonatal inflammation. This wouldseem to refute the hypothesis that neo-nates who are born in the settingof intraamniotic inflammation neces-sarily fare worse than gestational ageematched neonates who are born with-out intraamniotic inflammation.The interplay between intraamniotic
bacteria and the inflammatory responsecan be summarized with a model thatinvolves 4 stages: homeostasis, in-citement, evolution, and resolution.55
We propose that some microbes, espe-cially Ureaplasmas and other genital
FEBRUARY 2014 Ameri
mycoplasmas, may exist at low levels inthe intrauterine milieu in many normalhuman pregnancies by colonizing thedecidua, placenta, fetal membranes, and,occasionally, the amniotic fluid. If theorganisms are kept in check by a low-level inflammatory response (homeo-stasis), such colonization has no adversesequelae for mother or fetus. However,in some cases, the balance may beupset by the unchecked proliferation oforganisms or by the invasion of moreaggressive strains. Such imbalancecould trigger a more vigorous in-flammatory response (incitement). Wepropose that the inflammatory re-sponse, not the microbial invasion,triggers the release of prostanoids thatcause contractions and cervical change,which are the clinical hallmarks ofpreterm labor (evolution). Once estab-lished, severe intraamniotic inflam-mation almost always progressesrapidly to delivery (resolution). It isunknown precisely what factors drivethe transitions between these stages,so it is unknown whether clinical in-terventions at early stages might makea different resolution possible, that
Culture proven neonatal sepsis, n (%) 6 (22) 6 (17) 4 (9) 0 6 (3) .001a Comparison of the subjects in the 5 groups by analysis of variance (birthweight) or Fisher exact test (morbidities); b Data are given as mean � SD.
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
Research Obstetrics www.AJOG.org
is, continuation of pregnancy ratherthan inexorable progression to pretermdelivery.
Amniotic inflammatory responsesyndromeIn critical care, the term systemic in-flammatory response syndrome is usedto denote the complex multiorgan re-sponse to systemic inflammation.56 Theadvantage of such a term over termssuch as sepsis or bacteremia is that theterminology emphasizes that the in-flammatory response is more directlyresponsible for much of the end-organdamage and other sequelae of infectionthan are the infecting organisms them-selves. This helps to focus clinicalattention on treatment of the host in-flammatory response in addition to thesimple eradication of the organisms.
The analogous term fetal inflamma-tory response syndrome describes the as-sociation between elevated fetal plasmaIL-6 levels and a spectrum of severeneonatal morbidities and death.57
We propose the term amniotic infla-mmatory response syndrome to describe
125.e10 American Journal of Obstetrics & Gynec
the relationship between elevatedamniotic fluid inflammatory markerssuch as IL-6 and a spectrum of adverseoutcomes that include early pretermbirth and perinatal morbidity anddeath. The term amniotic inflamma-tory response syndrome focuses atten-tion on intraamniotic inflammationrather than infection because the in-flammatory response may be moredirectly responsible than the presenceof microbes for a short latency andthe resultant perinatal morbidity anddeath.
Culture vs PCR for detection of MIACWe found some discordance betweenculture and PCR results. Among thecases with MIAC, 65% were positive byboth culture and PCR; 16%were positiveby culture only, and 19% were positiveby PCR only. These rates of concor-dance/discordance are similar to those ina previous study: 40%, 24%, and 36%,respectively.24
Cases with positive culture and nega-tive PCR are of special interest becauseit is often assumed that PCR is more
ology FEBRUARY 2014
sensitive than culture. However, vari-ous factors that include low bacterialloads or PCR inhibitors in body fluidsactually may render it less sensitive.In our series, 1 case had a positive cul-ture for Candida; the negative PCR inthis case is not surprising becauseCandida is eukaryotic and would notbe expected to have prokaryotic 16SrDNA. Both this case and 1 other withpositive culture, despite negative PCR,had elevated IL-6 levels (51.1 and71.7 ng/dL, respectively; Table 2) andwere classified as infection; both womendelivered within 72 hours. The other 3women with positive cultures, despitenegative PCR, all had U urealyticum(Table 2) with low colony counts(data not shown), had low IL-6 levels(< 1.8 ng/dL), and were classifiedas colonization; they had longer la-tencies. This does not imply that Ure-aplasma is always benign. Indeed,several other cases had U urealyticum,either in isolation or in mixed culture,with elevations of IL-6 levels (ie,infection; Table 2), and all had shortlatency.
Microbial invasion of amnioticcavity amniotic fluid interleukin-6
1.4 0.3e6.6 1.1 0.3e3.4
�11.3 ng/mL 0.2 0.1e0.9 0.9 0.3e2.8
2.6-11.3 ng/mL 1.2 0.4e3.6 0.6 0.2e2.5
<2.6 ng/mL Referent — Referent —
Model 4d
Infection 0.4 0.1e2.5 0.9 0.2e3.4
Severe inflammation 0.2 0.0e0.8 0.6 0.2e2.3
Mild inflammation 1.2 0.4e3.5 0.5 0.1e2.0
Colonization 0.2 0.0e16.1 N/A N/A
Negative Referent — Referent —
N/A, not applicable.
a Adjusted for gestational age at enrollment; b P � .005; c P � .001; d Adjusted for gestational age at delivery.
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
www.AJOG.org Obstetrics Research
We conclude that culture and PCR arecomplementary techniques in the de-tection of MIAC and that neither tech-nique alone can be relied on to excludeMIAC.
Strengths and limitations of the studyStrengths of the study include the largenumber of subjects, which provided
statistical power to analyze outcomesbased on different levels of amnioticfluid IL-6. Another strength is the use ofboth culture and 16S rDNA PCR indefining MIAC.Limitations include the small number
of subjects with colonization, whichdiminished statistical power to com-pare outcomes with the other groups.
FEBRUARY 2014 Americ
Another limitation was the nonuniformreporting of amniotic fluid WBC bydifferent hospital laboratories, whichmade it impossible to combine andanalyze the results. Another limitationwas the inability to distinguish betweenvarious values of amniotic fluid glucose<20 mg/dL because some of the labo-ratories would not report specific values
Pooled data 278/2096 (13.3%) 24/2096 (1.1%) 24/278 (8.6%)
IL, interleukin; MIAC, microbial invasion of amniotic cavity; MMP, matrix metalloproteinase; PCR, polymerase chain reaction.
a Threshold not defined by original authors.
Combs. Inflammation, infection, preterm labor. Am J Obstet Gynecol 2014.
Research Obstetrics www.AJOG.org
below this level. Another limitation wasthat our techniques did not test for viralinvasion of the amniotic cavity, whichhas been documented in midtrimesteramniotic fluid in a small percentage ofasymptomatic women.58 However, thefrequency of viral infection in pretermlabor patients is unknown.
Clinical implicationsThe high rate of subclinical intra-amniotic infection does not imply thatantibiotics should be given routinely tounselected women in preterm labor. Inclinical trials, empiric antibiotic therapyhas been shown not to have benefit inpreterm labor with intact membranes59
and may increase the risk of neona-tal necrotizing enterocolitis60 and cere-bral palsy.61 It is unknown whether
125.e12 American Journal of Obstetrics & Gynec
antibiotics would be beneficial if targetedto MIAC.
Research implicationsControlled clinical trials are needed toaddress whether targeted antibiotictherapy is beneficial for the subgroup ofwomen in preterm labor with knownMIAC. Case reports have documentedthat such therapy can sometimes eradi-cate bacteria from the amniotic fluid inpatients with preterm labor,62-64 pretermrupture of membranes,65,66 or a sono-graphic short cervix,67,68 with subsequentcontinuation of pregnancy for weeks ormonths. But it is unclear whether thesecases were associated with intraamnioticinflammation (which we would classifyas infection) or not (which we wouldclassify as colonization). If the latter, ourresults would suggest that a benign course
ology FEBRUARY 2014
would have been expected even withoutsuch treatment.
Controlled clinical trials are needed toassess the possible benefits of the treat-ment of intraamniotic inflammationwith steroids, nonsteroidal antiinflam-matory drugs, and/or other immunemodulators in addition to antibiotics.In animal models of infection-inducedpreterm birth, salutary effects havebeen shown with dexamethasone,37 ibu-profen,37 the antiinflammatory cytokineinterleukin-10,69,70 and an antagonistof Toll-like receptor 4.71 In humans,corticosteroid treatment appears bene-ficial, even when given to women withclinical or histologic chorioamnionitis,72
perhaps because the favorable antiin-flammatory effects of steroids mayoutweigh any harm from their immu-nosuppressive effects.
To optimally select patients for suchtrials, it would first be useful to haverapid, reliable tests for intraamnioticinflammation and/or MIAC. In princi-ple, 16S rDNA PCR could be faster thanamniotic fluid culture, but this test is notreadily available for clinical use. Further,our results suggest that tests to detectinflammatory mediators such as IL-6may be more useful than tests to detectmicrobes. Rapid bedside tests for IL-6,MMP-8,73 and other inflammatory me-diators are theoretically possible but notyet clinically available. Tests that useproteomic profiling of amniotic fluid orcervicovaginal secretions show somepromise in the prediction of MIAC orintraamniotic inflammation74-76 but arenot clinically available.
We would hypothesize that antibioticand/or antiinflammatory treatmentwould be more successful if given duringthe stage of mild inflammation ratherthan severe inflammation.
CONCLUSION
In preterm labor with intact membranes,there is a high rate of intraamnioticinfection and inflammation, especially atearly gestational ages. Latency and peri-natal morbidity and death are relatedmore closely to the degree of the in-flammatory response than to the pres-ence or absence of microbes in theamniotic fluid. Microbial colonizationwithout inflammatory response may berelatively benign. -
ACKNOWLEDGMENTS
ProteoGenix/Obstetrix Collaborative ResearchNetworkInvestigative sites. Obstetrix Medical Group,Phoenix Perinatal Associates, Phoenix, AZ:William Clewell, MD; Banner Good SamaritanMedical Center, Phoenix, AZ: Melissa Ingersoll,RN, CRC; Banner Desert Samaritan MedicalCenter, Phoenix, AZ: Ana Braescu, RN, MS;Obstetrix Medical Group of Arizona, TucsonMedical Center, Tucson, AZ: Hugh Miller, MDand Diane Mercer, RN, CCRC; Obstetrix Medi-cal Group of Colorado, Presbyterian SaintLuke’s Hospital, Denver, CO: Richard Porreco,MD and Kent Heyborne, MD; Swedish MedicalCenter, Englewood, CO; Leslie Harden, RN,Julie Rael, RN, and Jeri Lech, RN; ObstetrixMedical Group of Washington, SwedishMedicalCenter, Seattle, WA: David Luthy, MD andTheresa Murray, RN; Obstetrix Medical Group,
San Jose Good Samaritan Hospital, San Jose,CA: C. Andrew Combs, MD, PhD, KimberlyMallory, RN, and Stacey Maguire, RN; OregonHealth and Science University, University Hos-pital, Portland, OR: Leonardo Pereira, MD andJanice Snyder, RNC; Obstetrix Medical Group,Southern California, Long Beach MemorialMedical Center, Long Beach, CA: MichaelNageotte,MD andChristine Preslicka, BSN, RN;Division of Maternal-Fetal Medicine, University ofWashington School of Medicine, UniversityHospital, Seattle, WA: Kristina Adams, MD,DrewRobilio,MD, andHopeClark, RN; PerinatalResearch Group, Centennial Women’s Hospital,Nashville, TN: Steven Fortunato, MD; MageeWomen’s Hospital, University of Pittsburgh,Pittsburgh, PA: Hyagriv Simhan, MD; Division ofMaternal-Fetal Medicine, Thomas JeffersonUniversity, Philadelphia, PA: Jason K. Baxter,MD, MSCP and Susan Weiner, PhD, MSN,RNC-OB, CNS; Department of Obstetrics andGynecology, St. Louis University School ofMedicine, St. Louis, MO: Erol Amon, MD;Department of Obstetrics and Gynecology,Carolinas Medical Center, Charlotte, NC: AlbertFranco, MD; Maternal-Fetal Medicine, GreenvilleHospital System, University Medical Center,Greenville, SC: Kenneth Trofatter, MD.Biostatistics. Oregon Health and ScienceUniversity, Portland, OR: Jodi Lapidus, PhD.Pathology. Oregon Health and Science Uni-versity, University Hospital, Portland, OR: TerryMorgan, MD.Principal investigator. Obstetrix MedicalGroup Center for Research, Education, andQuality, Campbell, CA: C. Andrew Combs, MD.Administration, Obstetrix CollaborativeResearch Network. Obstetrix Medical GroupCREQ, Steamboat Springs, CO: Thomas J.Garite, MD; Obstetrix Medical Group CREQ,Fountain Valley, CA: Kimberly Maurel, RN, MS;Obstetrix Medical Group CREQ, Gilbert, AZ:Diana Abril, RN, MSc; Obstetrix Medical Groupof Colorado, Denver, CO: Leslie Harden, RN andJulie Rael, RN.Administration, ProteoGenix. ProteoGenix,Inc, Costa Mesa, CA: Michael Gravett, MD, Sri-nivasa Nagalla, MD, Durlin Hickok, MD, DesireeHollemon, RN, and Xinfang Lu, MS.
REFERENCES
1. Romero R, Espinoza J, Kusanovic JP, et al.The preterm parturition syndrome. BJOG2006;113(suppl 3):17-42.2. Watts DH, Krohn MA, Hillier SL,Eschenbach DA. The association of occult am-niotic fluid infection with gestational age andneonatal outcome among women in pretermlabor. Obstet Gynecol 1992;79:351-7.3. Yoon BH, Romero R, Moon JB, et al. Clinicalsignificance of intra-amniotic inflammation inpatients with preterm labor and intact mem-branes. Am J Obstet Gynecol 2001;185:1130-6.4. Hitti J, Tarczy-Hornoch P, Murphy J,Hillier SL, Aura J, Eschenbach DA. Amniotic fluid
FEBRUARY 2014 Americ
infection, cytokines, and adverse outcomeamong infants at 34 weeks’ gestation or less.Obstet Gynecol 2001;98:1080-8.5. Romero R, Yoon BH, Mazor M, et al. Thediagnostic and prognostic value of amniotic fluidwhite blood cell count, glucose, interleukin-6,and Gram stain in patients with preterm laborand intact membranes. Am J Obstet Gynecol1993;169:805-16.6. Hillier SL, Witkin SS, Krohn MA, Watts DH,Kiviat NB, Eschenbach DA. The relationship ofamniotic fluid cytokines and preterm delivery,amniotic fluid infection, histologic chorioamnio-nitis, and chorioamnion infection. Obstet Gyne-col 1993;81:941-8.7. Coultrip LL, Lien JM, Gomez R, Kapernick P,Khoury A, Grossman JH. The value of amnioticfluid interleukin-6 determination in patients withpreterm labor and intact membranes in thedetection of microbial invasion of the amnioticcavity. Am J Obstet Gynecol 1994;171:901-11.8. Andrews WW, Hauth JC, Goldenberg RL,Gomez R, Romero R, Cassell GH. Amniotic fluidinterleukin-6: correlation with upper genital tractmicrobial colonization and gestational age inwomen delivered after spontaneous laborversus indicated delivery. Am J Obstet Gynecol1995;173:606-12.9. Greci LS, Gilson GJ, Nevils B, Izquierdo LA,Qualls CR, Curet LB. Is amniotic fluid analysisthe key to preterm labor? A model usinginterleukin-6 for predicting rapid delivery. Am JObstet Gynecol 1998;179:172-8.10. Figueroa R, Garry D, Elimian A, Patel K,Sehgal PB, Tejani N. Evaluation of amniotic fluidcytokines in preterm labor and intact mem-branes. J Matern Fetal Neonatal Med 2005;18:241-7.11. Jacobsson B, Mattsby-Baltzer I, Hagberg H.Interleukin-6 and interleukin-8 in cervical andamniotic fluid: relationship to microbial invasionof the chorioamniotic membranes. BJOG 2005;112:719-24.12. JacobssonB,Mattsby-Baltzer I, AnderschB,et al. Microbial invasion and cytokine response inamniotic fluid in a Swedish population of womenin preterm labor. Acta Obstet Gynecol Scand2003;82:120-8.13. Yoneda S, Sakai M, Sasaki Y, Shiozaki A,Hidaka T, Saito S. Interleukin-8 and glucosein amniotic fluid, fetal fibronectin in vaginal se-cretions and preterm labor index based onclinical variables are optimal predictive markersfor preterm delivery in patients with intactmembranes. J Obstet Gynaecol Res 2007;33:38-44.14. Park KH, Yoon BH, Shim S-S, Jun JK,Syn HC. Amniotic fluid tumor necrosis factor-alpha is a marker for the prediction of early-onset neonatal sepsis in preterm labor. GynecolObstet Invest 2004;58:84-90.15. Angus SR, Segel SY, Hsu C-D, et al. Am-niotic fluid matrix metalloproteinase-8 indicatesintra-amniotic infection. Am J Obstet Gynecol2001;185:1232-8.16. Maymon E, Romero R, Chaiworapongsa T,et al. Amniotic fluid matrix metalloproteinase-8
in preterm labor with intact membranes. Am JObstet Gynecol 2001;185:1149-55.17. Kim SM, Romero R, Lee JH, et al. The fre-quency and clinical significance of intraamnioticinflammation in women with preterm uterinecontractility but without cervical changes: do thediagnostic criteria for preterm labor need to bechanged? J Matern Fetal Neonatal Med2012;25:1212-21.18. Romero R, Yoon BH, Kenney JS, Gomez R,Allison AC, Sehgal PB. Amniotic fluid interleukin-6 determinations are of diagnostic and prog-nostic value in preterm labor. Am J ReprodImmunol 1993;30:167-83.19. Markenson GR, Martin RK, Tillotson-Criss M, Foley KS, Stewart RS, Yancey M. Theuse of the polymerase chain reaction to detectbacteria in amniotic fluid in pregnanciescomplicated by preterm labor. Am J ObstetGynecol 1997;177:1471-7.20. Hitti J, Riley DE, Krohn MA, et al. Broad-spectrum bacterial rDNA polymerase chain re-action assay for detecting amniotic fluid infectionamongwomen in premature labor. Clin Infect Dis1997;24:1228-32.21. Oyarzun E, YamamotoM, Kato S, GomezR,Lizama L, Moenne A. Specific detection of 16micro-organisms in amniotic fluid by polymerasechain reaction and its correlation with pretermdelivery occurrence. Am J Obstet Gynecol1998;179:1115-9.22. Yoon BH, Romero R, Kim M, et al. Clinicalimplications of detection of Ureaplasma ure-alyticum in the amniotic cavity with the poly-merase chain reaction. Am J Obstet Gynecol2000;183:1130-7.23. Yoon BH, Romero R, Lim J-H, et al. Theclinical significance of detecting Ureaplasmaurealyticum by the polymerase chain reaction inthe amniotic fluid of patients with preterm labor.Am J Obstet Gynecol 2003;189:919-24.24. DiGiulio DB, Romero R, Amogan HP, et al.Microbial prevalence, diversity and abundancein amniotic fluid during preterm labor: a molec-ular and culture-based investigation. PLoS One2008;3:e3056.1-10.25. Han YW, Shen T, Chung P, Buhimschi IA,Buhimschi CS. Uncultivated bacteria as etiologicagents of intra-amniotic inflammation leading topreterm birth. J Clin Microbiol 2009;47:38-47.26. Marconi C, de Andrade Ramos BR,Peracoli JC, Donders GGG, da Silva MG. Am-niotic fluid interleukin-1 beta and interleukin-6,but not interleukin-8 correlate with microbial in-vasion of the amniotic cavity in preterm labor.Am J Reprod Immunol 2011;65:549-56.27. Buhimschi CS, Bhandari V, Hamar BD, et al.Proteomic profiling of the amniotic fluid to detectinflammation, infection, and neonatal sepsis.PLoS Med 2007;4:e18.28. Romero R, Salafia CM, Athanassiadis AP,et al. The relationship between acute inflamma-tory lesions of the pretermplacenta and amnioticfluid microbiology. Am J Obstet Gynecol1992;166:1382-8.29. Waldorf KM, Gravett MG, McAdams RM,et al. Choriodecidual group B streptococcal
125.e14 American Journal of Obstetrics & Gynec
inoculation induces fetal lung injury without intra-amniotic infection and preterm labor in Macacanemestrina. PLoS One 2011;6:e28972.30. Steel JH, Malatos S, Kennea N, et al. Bac-teria and inflammatory cells in fetal membranesdo not always cause preterm labor. Pediatr Res2005;57:404-11.31. Onderdonk AB, Delaney ML, DuBois AM,Allred EN, Leviton A, Extremely Low GestationalAge Newborns (ELGAN) Study Investigators.Detection of bacteria in placental tissues ob-tained from extremely low gestational age neo-nates. Am J Obstet Gynecol 2008;198:110.e1-7.32. OnderdonkAB,Hecht JL,McElrath TF, et al.Colonization of second-trimester placenta pa-renchyma. Am J Obstet Gynecol 2008;199:52.e1-10.33. Fry DE. Sepsis, systemic inflammatoryresponse, and multiple organ dysfunction: themystery continues. Am Surg 2012;78:1-8.34. Buhimschi CS, Schatz F, Krikun G,Buhimschi IA, Lockwood CJ. Novel insights intomolecular mechanisms of abruption-inducedpreterm birth. Expert Rev Mol Med 2010;12:e35.35. Romero R, Kadar NR, Miranda J, et al. Thediagnostic performance of the mass restricted(MR) score in the identification of microbial in-vasion of the amniotic cavity or intra-amnioticinflammation is not superior to amniotic fluidinterleukin-6. J Matern Fetal Neonatal Med2013. Epub ahead of print.36. Gravett MG, Witkin SS, Haluska GJ,Edwards JL, Cook MJ, Novy MJ. An experi-mental model for intraamniotic infection andpreterm labor in Rhesus monkeys. Am J ObstetGynecol 1994;171:1660-7.37. Gravett MG, Adams KM, Sadowsky DW,et al. Immunomodulators plus antibiotics delaypreterm delivery after experimental intraamnioticinfection in a nonhuman primate model. Am JObstet Gynecol 2007;197:518.e1-8.38. Novy MJ, Duffy L, Axthelm MK, et al. Ure-aplasma parvum or Mycoplasma hominis assole pathogens cause chorioamnionitis, pretermdelivery, and fetal pneumonia in Rhesus ma-caques. Reprod Sci 2009;16:56-70.39. Grigsby PL, Novy MJ, Sadowsky DW,et al. Maternal azithromycin therapy for Ure-aplasma intraamniotic infection delays pre-term delivery and reduces fetal lung injuryin a primate model. Am J Obstet Gynecol2012;207:475.e1-14.40. Rizzo G, Capponi A, Rinaldo D, Tedeschi D,Arduini D, Romanini C. Interleukin-6 concentra-tions in cervical secretions identify microbial in-vasion of the amniotic cavity in patients withpreterm labor and intact membranes. Am JObstet Gynecol 1996;175:812-7.41. Bearfield C, Davenport ES,Sivapathasundaram V, Allaker RP. Possibleassociation between amniotic fluid micro-organism infection and microflora in the mouth.BJOG 2002;109:527-33.42. Kim MJ, Romero R, Gervasi MT. Wide-spread microbial invasion of the chorioamniotic
ology FEBRUARY 2014
membranes is a consequence and not a causeof intraamniotic infection. Lab Invest 2009;89:924-36.43. Seong HS, Lee SE, Kang JH, Romero R,Yoon BH. The frequency of microbial invasion ofthe amniotic cavity and histologic chorioamnio-nitis in women at term with intact membranes inthe presence or absence of labor. Am J ObstetGynecol 2008;199:375.e1-5.44. Cassell GH, Davis RO, Waites KB, et al.Isolation of Mycoplasma hominis and Ure-aplasma urealyticum fromamniotic fluid at 16-20weeks of gestation: potential effect on outcomeof pregnancy. Sex Transm Dis 1983;10:294-302.45. Gray DJ, Robinson HB, Malone J,Thomson RB Jr. Adverse outcome in pregnancyfollowing amniotic fluid isolation of Ureaplasmurealyticum. Prenat Diagn 1992;12:111-7.46. Horowitz S, Mazor M, Romero R,Horowitz J, Glezerman M. Infection of the am-niotic cavity with Ureaplasma urealyticum in themidtrimester of pregnancy. J Reprod Med1995;40:375-9.47. Berg TG, Philpot KL, Welsh MS,Sanger WG, Smith CV. Ureaplasma/Myco-plasma-infected amniotic fluid: pregnancyoutcome in treated and nontreated patients.J Perinatol 1999;19:275-7.48. Gerber S, Vial Y, Hohlfeld P, Witkin SS.Detection of Ureaplasma urealyticum in second-trimester amniotic fluid by polymerase chain re-action correlates with subsequent preterm laborand delivery. J Infect Dis 2003;187:518-21.49. Perni SC, Vardhana S, Korneeva I, et al.Mycoplasma hominis and Ureaplasma ure-alyticum in midtrimester amniotic fluid: associa-tion with amniotic fluid cytokine levels andpregnancy outcome. Am J Obstet Gynecol2004;191:1382-6.50. Wenstrom KD, Andrews WW, Hauth JC,GoldenbergRL, DuBardMB, Cliver SP. Elevatedsecond-trimester amniotic fluid interleukin-6levels predict preterm delivery. Am J ObstetGynecol 1998;178:546-50.51. Bashiri A, Horowitz S, Huleihel M,Hackmon R, Dukler D, Mazor M. Elevated con-centrations of interleukin-6 in intra-amnioticinfection with Ureaplasma urealyticum inasymptomatic women during genetic amnio-centesis. ActaObstet Gynecol 1999;78:379-82.52. Thomakos N, Daskalakis G,Papapanagiotou A, PapantoniouN,Mesogitis S,Antsaklis A. Amniotic fluid interleukin-6 and tu-mor necrosis factor-a at mid-trimester geneticamniocentesis: relationship to intra-amnioticmicrobial invasion and preterm delivery. Eur JObstet Gynecol Reprod Biol 2010;148:147-51.53. Daskalakis G, Thomakos N,Papapanagiotou A, PapantoniouN,Mesogitis S,Antsaklis A. Amniotic fluid interleukin-18 at mid-trimester genetic amniocentesis: relationship tointra-amniotic microbial invasion and pretermdelivery. BJOG 2009;116:1743-8.54. Yoon BH, Oh S-Y, Romero R, et al. Anelevated amniotic fluidmatrix metalloproteinase-8 level at the time of mid-trimester genetic
amniocentesis is a risk factor for spontaneouspreterm delivery. Am J Obstet Gynecol2001;185:1162-7.55. McCall CE, Yoza B, Liu T, El Gazzar M.Gene-specific epigenetic regulation in seriousinfections with systemic inflammation. J InnateImmun 2010;2:395-405.56. American College of Chest Physicians/Society of Critical Care Medicine ConsensusConference. Definitions for sepsis and organfailure and guidelines for the use of innovativetherapies in sepsis. Crit Care Med 1992;20:864-74.57. Gomez R, Romero R, Ghezzi F, Yoon BH,Mazor M, Berry SM. The fetal inflammatoryresponse syndrome. Am J Obstet Gynecol1998;179:194-202.58. Gervasi MT, Romero R, Bracalente G. Viralinvasion of the amniotic cavity (VIAC) in themidtrimester of pregnancy. J Matern FetalNeonatal Med 2012;25:2002-13.59. Hutzal CE, Boyle EM, Kenyon SL, et al. Useof antibiotics for the treatment of pretermparturition and prevention of neonatal morbidity:ametaanalysis. Am JObstet Gynecol 2008;199:620.e1-8.60. Kenyon SL, Taylor DJ, Tarnow-Mordi W,ORACLE Collaborative Group. Broad-spectrumantibiotics for spontaneous preterm labour: theORACLE II randomised trial. Lancet 2001;357:989-94.61. Kenyon S, Pike K, Jones DR, et al. Child-hood outcomes after prescription of antibioticsto pregnant women with spontaneous pretermlabour: 7-year follow-up of the ORACLE II trial.Lancet 2008;372:1319-27.
62. Mazor M, Horowitz S, Meril T, Bar-Am I.Eradication of Ureaplasma urealyticum fromamniotic fluid. Isr J Med Sci 1992;28:296-8.63. Mazor M, Chaim W, Hershkowitz R,Wiznitzer A. Eradication of Viridans streptococcifrom the amniotic cavity with transplacentalantibiotic treatment. Arch Gynecol Obstet1994;255:147-51.64. Mazor M, Chaim W, Meirovitz M, Yohay D,Leiberman JR, Glezerman M. Eradication of vir-idans streptococci from the amniotic cavity byparenteral antibiotic administration: a casereport. J Reprod Med 1995;40:820-2.65. Romero R, Scioscia AL, Edberg SC,Hobbins JC. Use of parenteral antibiotic therapyto eradicate bacterial colonization of amnioticfluid in premature rupture of membranes. ObstetGynecol 1986;67(suppl):15S-7S.66. Romero R, Hagay Z, Nores J, SepulvedaW,MazorM. Eradication of Ureaplasmaurealyticumfrom the amniotic fluid with transplacental anti-biotic treatment. Am J Obstet Gynecol 1992;166:618-20.67. Hassan S, Romero R, Hendler I, et al.A sonographic short cervix as the only clini-cal manifestation of intra-amniotic infection.J Perinat Med 2006;34:13-9.68. Morency A-M, Rallu F, Laferriere C, Bujold E.Eradication of intra-amniotic Streptococcusmutans in a woman with a short cervix. J ObstetGynecol Can 2006;28:898-902.69. Terrone DA, Rinehart BK, Granger JP,Barrilleaux PS, Martin JN, Bennett WA. Inter-leukin-10 administration and bacterial endotoxin-induced preterm birth in a rat model. ObstetGynecol 2001;98:476-80.
FEBRUARY 2014 Americ
70. Rodts-Palenik S, Wyatt-Ashmead J,Pang Y, et al. Maternal infection-induced whitematter injury is reduced by treatment with inter-leukin-10. Am J Obstet Gynecol 2004;191:1387-92.71. Adams Waldorf KM, Persing D, Novy MJ,Sadowsky DW, Gravett MG. Pre-treatmentwith Toll-like receptor 4 antagonist inhibitslipopolysaccharide-induced preterm uterinecontractility, cytokines, and prostaglandins inrhesus monkeys. Reprod Sci 2008;15:121-7.72. Been JV, Degraeuwe PL, Kramer BW,Zimmerman LJI. Antenatal steroids and neonataloutcome after chorioamnionitis: a meta-anal-ysis. BJOG 2011;118:113-22.73. Kim KW, Romero R, Park HS, et al. A rapidmatrix metalloproteinase-8 bedside test forthe detection of intraamniotic inflammation inwomen with preterm premature rupture ofmembranes. Am J Obstet Gynecol 2007;197:292.e1-5.74. Gravett MG, Thomas A, Schneider KA, et al.Proteomic analysis of cervical-vaginal fluid:identification of novel biomarkers for detection ofintra-amniotic infection. J ProteomeRes 2007;6:89-96.75. Hitti J, Lapidus JA, Lu X, et al. Noninvasivediagnosis of intraamniotic infection: proteomicbiomarkers in vaginal fluid. Am JObstet Gynecol2010;203:32.e1-8.76. Holst R-M, Hagberg H, Wennerholm U-B,Skogstrand K, Thorsen P, Jacobsson B. Pre-diction of microbial invasion of the amnioticcavity in women with preterm labour: analysis ofmultiple proteins in amniotic and cervical fluids.BJOG 2011;118:240-9.