21
Amy Sheide Clinical Informaticist 3M Health Information Systems USA Achieving Data Standardization in Health Information Exchange and Quality Measurement
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | phoebe-bates |
| View: | 217 times |
| Download: | 0 times |

Amy Sheide
Clinical Informaticist
3M Health Information Systems
USA
Achieving Data Standardization in Health Information Exchange and Quality Measurement

AbstractThis presentation reviewsthe benefits and challenges of achieving and maintaining interoperability.
Specifically, it showcases successful implementation of a centralized terminology server in health information exchange, biosurveillance and quality measurement.

Exchange
Interpret
Share
Understand
Background“Interoperability describes the extent to which systems and devices can exchange data, and interpret that shared data. For two systems to be interoperable, they must be able to exchange data and subsequently present that data such that it can be understood by a user.”http://www.himss.org/library/interoperability-standards/what-is

Benefits of interoperability Delivery of High Quality Cost Effective
CareProcess
ImprovementCoordination Across
Care SettingsMedical Error
Reduction
Providing care within clinical
guidelines
A complete health history
Accurate medication
Lists
Examining variation in physician practice
Allergy and adverse
reaction lists
Vaccine history

“The complexity of patient data in electronic medial records, coupled with expectations that these data facilitate clinical decision making, healthcare cost effectiveness, medical error reduction, and evidence based medicine, makes obvious the role of standardized terminologies as a foundation for comparable and consistent representation of patient information.”
-Pathak and Chute, Division of Biomedical Statistics and Informatics, Mayo Clinic
Pathak, J., & Chute, C. G. (2010). Analyzing categorical information in two publicly available drug terminologies: RxNorm and NDF-RT. Journal of the American Medical Informatics Association, 17(4), 432-439.

EHR
MU is centere
d around CollectingExchanging &Reporting
structured
clinical data and
leveraging
CEHRT to do it
Drivers for interoperability in the US•The 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act has the goal of using certified electronic health record technology (CEHRT) to promote patient safety and interoperability between and within health care systems.
•The initiative in HITECH Act are also known as Meaningful Use (MU).
• How do you obtain and implement the standards?• Are the current standards robust to function in current
clinical workflows? • Standard terminology is free but how much does it cost
to implement and understand?• How is your organization going to share data elements
that don’t have a standard code?
Reaching the interoperability target• Governing bodies have defined
structured data requirements with standard terminology
• Limitations and challenges exist in adopting these standards
Current State

Challenges in interoperabilityStandardizati
on
Multiple Standard Terminologies
Variable Versions
Gaps in Standard Terminologies
Integration
Variable Release Formats
Synonymous concepts with
different Identifiers
Unidirectional Data Translation
Organization
Flat Lists of Codes
Variation in Granularity
Significant effort to maintain mappings
Centralized Terminology Server (CTS) solution • Metadata repository which
enables the translation and integration of healthcare data
• Standardized terminology vocabulary compliance
• Knowledge Base to understand how data is represented and structured across the organization
Addresses the simple questions that are hardest to manage,“ What does it mean, where is it from, and how does it relate to
everything else!”

CTS components
• Terminology consulting • Integration of local codes
• Interoperability
• Translation between source and target system
• Browsing and Runtime Services
• Terminology and mapping container
• Search and browse content• Mapping tools
• Delivery of standard terminologies in a consistent consumable format
• Update to the standards content• Local content Content Software
Mapping Services
Web Service
APIs

Health Information Exchange (HIE) use case
Goal: Make patient lab results available to any provider regardless
of performing laboratory
Standardization:Map labs to Standard
Terminology
Integration:Translate Standard
Terminology back to Source
Lab
Organization:Location to Store
the Mappings
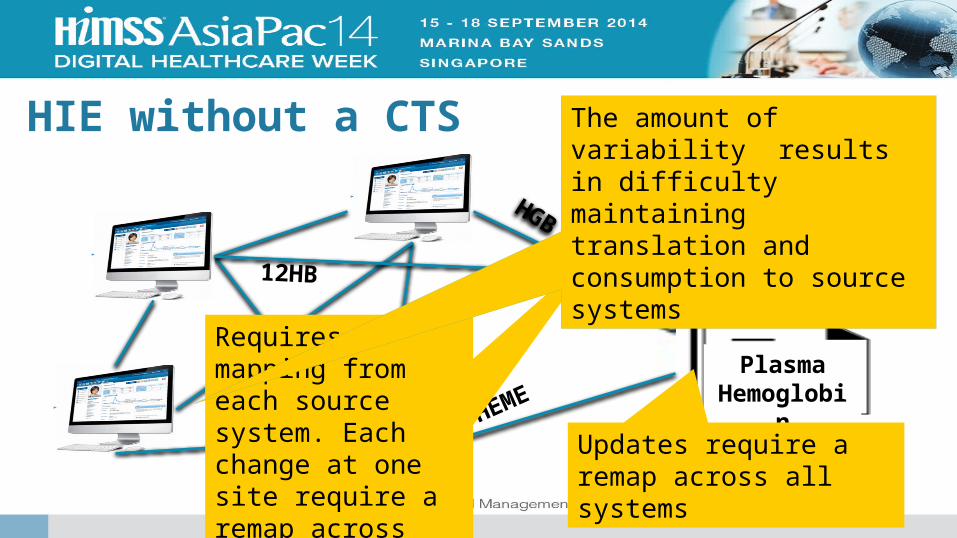
HIE without a CTS
HGB
HEME
12HB
HPLAS Plasma
Hemoglobin
Requires mapping from each source system. Each change at one site require a remap across systems.
Updates require a remap across all systems
The amount of variability results in difficulty maintaining translation and consumption to source systems
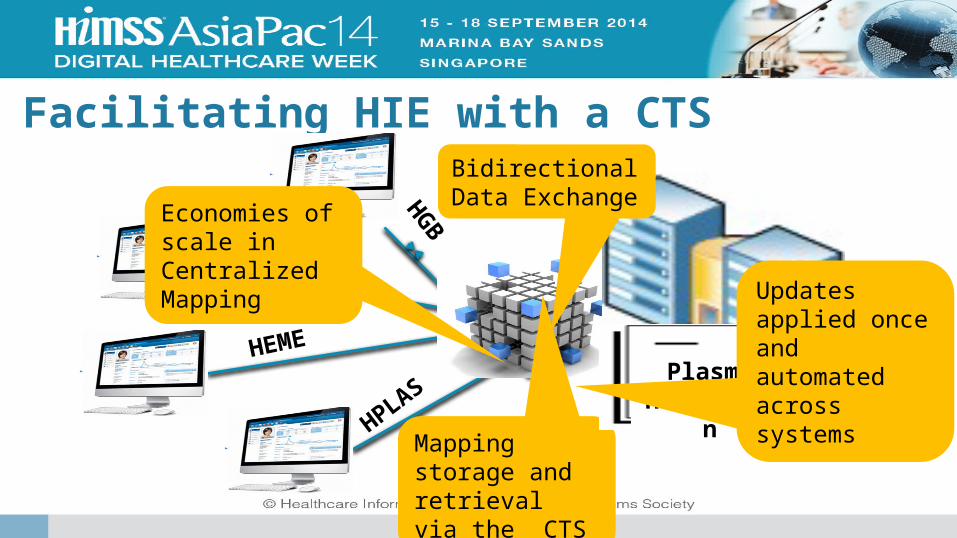
Facilitating HIE with a CTS
HGB
12HB
HEME
HPLAS
Mapping storage and retrieval via the CTS
Bidirectional Data Exchange
Economies of scale in Centralized Mapping
Plasma Hemoglob
in
Updates applied once and automated across systems
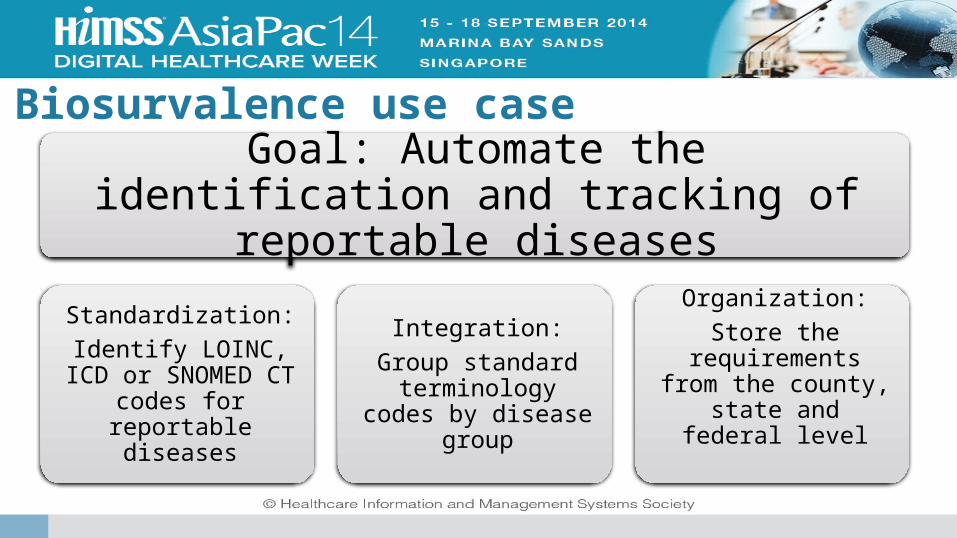
Biosurvalence use case
Goal: Automate the identification and tracking of reportable diseases
Standardization:Identify LOINC, ICD
or SNOMED CT codes for reportable
diseases
Integration:Group standard
terminology codes by disease group
Organization:Store the
requirements from the county, state and federal level
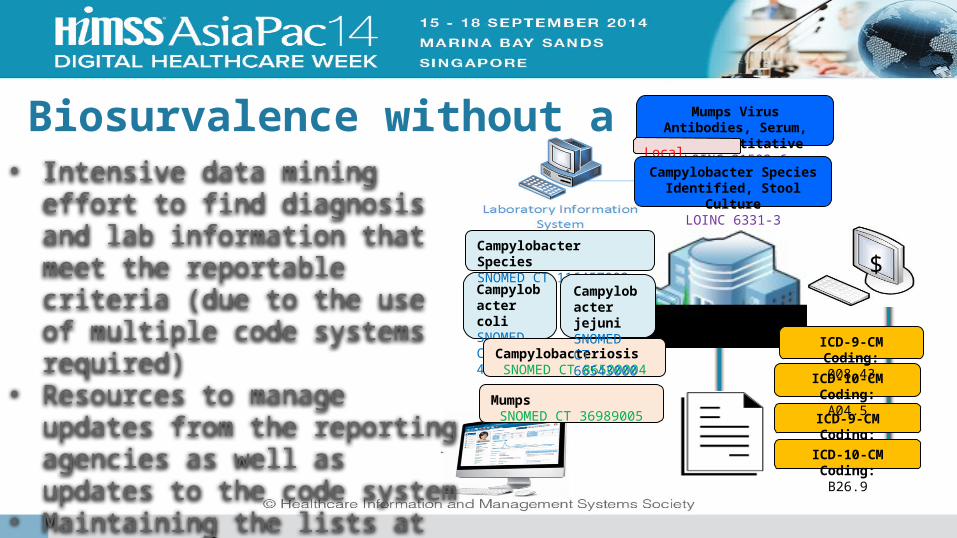
Biosurvalence without a CTS• Intensive data mining effort to find
diagnosis and lab information that meet the reportable criteria (due to the use of multiple code systems required)
• Resources to manage updates from the reporting agencies as well as updates to the code system
• Maintaining the lists at each level of reporting (county, state, federal)
ICD-9-CM Coding:072.9
MumpsSNOMED CT 36989005
ICD-10-CM Coding:B26.9
Campylobacter coliSNOMED CT 40614002
ICD-10-CM Coding:A04.5
Mumps Virus Antibodies, Serum, Semi-Quantitative
LOINC 31503-6Local Code: A
008.43Campylobacter Species Identified, Stool Culture
LOINC 6331-3
$
ICD-9-CM Coding:008.43Campylobacteriosis
SNOMED CT 86500004
Campylobacter SpeciesSNOMED CT 116457002
Campylobacter jejuniSNOMED CT 66543000
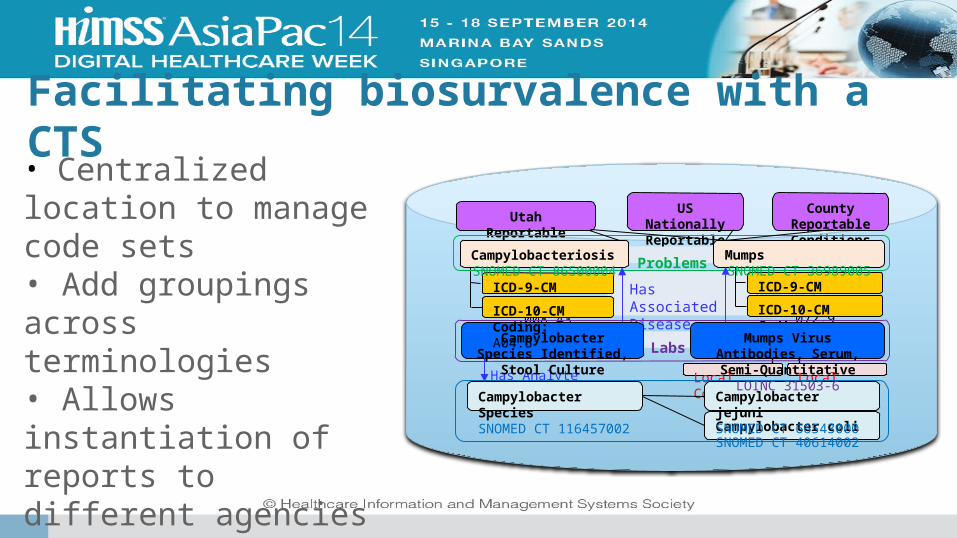
Facilitating biosurvalence with a CTS
Local Code: B008.43
Local Code: A008.43
Utah Reportable Conditions
US Nationally Reportable Conditions
Has Associated Disease
County Reportable Conditions
ICD-9-CM Coding:008.43
ProblemsICD-9-CM Coding:
072.9
MumpsSNOMED CT 36989005
ICD-10-CM Coding:B26.9
Has AnalyteNCID 76770
Campylobacter coliSNOMED CT 40614002
Labs
CampylobacteriosisSNOMED CT 86500004
Campylobacter Species Identified, Stool Culture
LOINC 6331-3
Campylobacter jejuniSNOMED CT 66543000
Campylobacter SpeciesSNOMED CT 116457002
ICD-10-CM Coding:A04.5
Mumps Virus Antibodies, Serum, Semi-Quantitative
LOINC 31503-6
• Centralized location to manage code sets• Add groupings across terminologies• Allows instantiation of reports to different agencies• Enterprise wide structured data integration

Clinical Quality Measure (CQM) use case
Goal: Identify groups of patients receiving or eligible for treatment
Standardization:Over 20 different
code systems required to
calculate CQMs
Integration:Manage multiple versions of value
sets and code systems
Organization:Link local codes
to CQM data elements and
measures
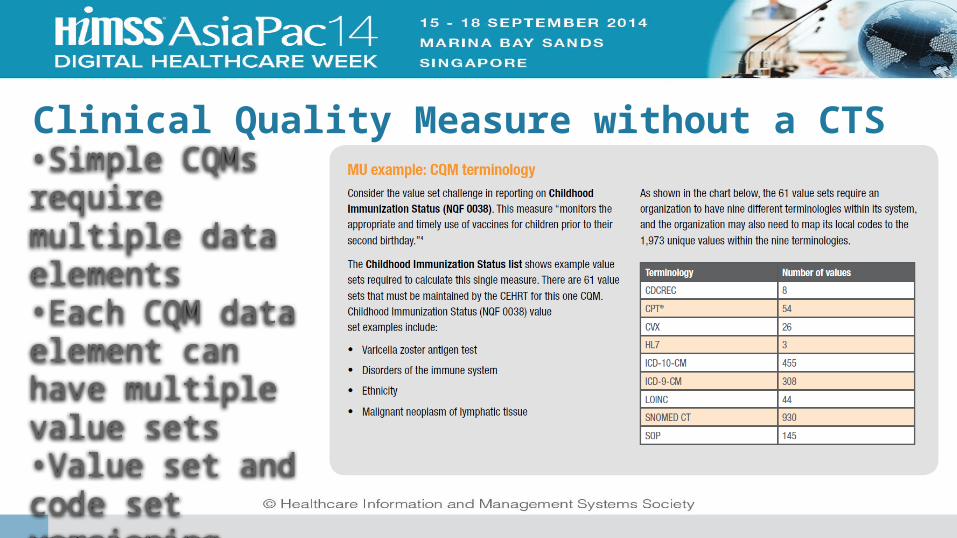
Clinical Quality Measure without a CTS•Simple CQMs require multiple data elements•Each CQM data element can have multiple value sets•Value set and code set versioning cause a high level of variability

Facilitating CQM with a CTS•Cost and process benefits in managing the complexity of data value sets and values •Technical benefit in accessing CQM content with APIs and runtime services•Versioning reduces variability of content

Achieving enterprise intelligence with a scalable CTS
Enterprise Intelligence
Accelerates implementation of electronic health records• Longitudinal patient
care record• Personal health
records
Enables structured clinical data capture, queries and analytics
• Data mining• Complex secondary
data use
Semantically interoperable data for exchange, analytics, decision support, alerts and reminders• Lower total cost of
ownership• Maximized
consistency, quality and efficiency of mapping

Questions

















