152 DENTISTRYTODAY.COM • JANUARY 2012 INTRODUCTION Nowadays, a great premium is placed on aesthetics with cosmetic solutions being sought by the parents of adolescent pa- tients at very early ages. Conventional orthodontics plays a huge part in satisfying this demand in adolescents, but cannot always provide all the answers. In cases such as partial anodontia, peg lateral incisors, misshapen and malformed teeth, additional aesthetic improvements have to be provided by a variety of restora- tive procedures. Whenever possible in ado- lescents, these techniques should be mini- mally, if at all, invasive. Gingival tissues con- tinue to mature and change shape during this period, as do skeletal changes through skull growth, and therefore, as a general rule, any restorations placed should be viewed as providing a solution in the medi- um term until early adulthood. Restorations placed subgingivally for aesthetics at an early age are soon likely to appear supragin- givally and require probable replacement especially in the high lip line case. Con - sequently, simple direct composite place- ment techniques have evolved to provide this medium-term aesthetic solution. Limitations of Direct Placement Composites Direct placement of composites as a filling and cosmetic bonding material has been available for many years and it is not with- in the scope of this article to review the chemistry and clinical techniques associat- ed with these materials. As a general rule, indirect bonding, when used to close diastemas, can provide an excel- lent and predictable aesthetic result. The case in Figure 1 shows how more advanced and extensive space closure cases can prove too complex when using the direct technique— poor slanted midline closure, disproportion- ately shaped teeth, and a particularly disap- pointing emergence profile. Although vari- ous techniques have been advocated, includ- ing the use of various space closure celluloid formers to overcome these problems, the final results in the authors’ hands can still be unpredictable. It is the opinion of the au - thors that these complex cases are more easi- ly, cheaply, and predictably restored with indirectly custom-fabricated composite me- sial/distal space closure veneers (or chips, as they are sometimes called) (Figures 2 to 4). Although this technique can also be car- ried out using porcelain chips, the degree of tooth preparation required to achieve an imperceptible join between the tooth and porcelain, along with associated problems of color matching and cost preclude their use in the medium-term in teenagers and are ideally provided in the early adolescent age group upward. CASE REPORT Diagnosis and Treatment Planning The 16-year-old patient seen in Figures 5a to 5c presented for a cosmetic opinion toward the completion of his orthodontic treat- ment. In the lower arch, both central inci- sors were congenitally absent, and ortho- dontic tooth movement had provided a one-toothed space for restoration. His age precluded implant placement and the inter- im proposed solution of the provision of a conventional Maryland bridge was accept- ed by the patient and his mother. The aesthetic problems in the maxillary arch were more complex. Both lateral inci- sors were malformed as well as misshapen. All 4 incisors were wider at the necks than at the incisal edge, with both canines rela- tively pointed. As tooth positioning follow- ing orthodontics was excellent for aesthet- ics and lip support, further treatment to bring the teeth together would have been counterproductive. Finally the patient and his mother were adamant that whichever technique was chosen to improve aesthet- ics, it was to be minimally if at all invasive. The patient additionally requested that tooth whitening be carried out prior to the restorative phase of treatment, and his exist- ing Raintree Essix Orthodontic Retainers (DENTSPLY International) were used as trays for “at-home” whitening using 15% Carba- mide Peroxide Gel (Ultradent Products). Study casts were taken and mounted with a face-bow on a semi-adjustable articu- lator (Dentatus). The case was studied with particular respect to the proposed space clo- sure and the maintenance of the correct crown width to length ratio of 75% and cor- responding Golden Proportion ratios for remaining teeth. Although minimum/no preparation veneers (eg, Lumineers) were an option if crown length was to be increased, this approach was not the preferred choice of the patient. Tom Bereznicki, BDS (Edin) Lola Welch An Alternative Approach to Cosmetic Space Closure continued on page 154 AESTHETICS Figure 1. An example of poor aesthetics with direct composite bonding. Figure 2. A pretreatment aesthetic dilemma presented by the excessively large diastemas. Figure 3. The case following Invisalign orthodontic tooth movement. (Courtesy of Dr. R. Edwards.) Figure 4. The case upon completion of indirect com- posite.
Transcript
152
DENTISTRYTODAY.COM • JANUARY 2012
INTRODUCTIONNowadays, a great premium is placed onaesthetics with cosmetic solutions beingsought by the parents of adolescent pa -tients at very early ages. Conventionalorthodontics plays a huge part in satisfyingthis demand in adolescents, but cannotalways provide all the answers.In cases such as partial anodontia, peg
lateral incisors, misshapen and malformedteeth, additional aesthetic improvementshave to be provided by a variety of restora-tive procedures. Whenever possible in ado-lescents, these techniques should be mini-mally, if at all, invasive. Gingival tissues con-tinue to mature and change shape duringthis period, as do skeletal changes throughskull growth, and therefore, as a generalrule, any restorations placed should beviewed as providing a solution in the medi-um term until early adulthood. Restorationsplaced subgingivally for aesthetics at anearly age are soon likely to appear supragin-givally and require probable replacementespecially in the high lip line case. Con -sequently, simple direct composite place-ment techniques have evolved to providethis medium-term aesthetic solution.
Limitations of Direct Placement Composites
Direct placement of composites as a fillingand cosmetic bonding material has beenavailable for many years and it is not with-in the scope of this article to review thechemistry and clinical techniques associat-ed with these materials.As a general rule, indirect bonding, when
used to close diastemas, can provide an excel-lent and predictable aesthetic result. The casein Figure 1 shows how more advanced andextensive space closure cases can prove toocomplex when using the direct technique—poor slanted midline closure, disproportion-ately shaped teeth, and a particularly disap-pointing emergence profile. Although vari-ous techniques have been advocated, includ-ing the use of various space closure celluloidformers to overcome these problems, thefinal results in the authors’ hands can still beunpredictable. It is the opinion of the au -thors that these complex cases are more easi-ly, cheaply, and predictably restored with
indirectly custom-fabricated composite me -sial/distal space closure veneers (or chips, asthey are sometimes called) (Figures 2 to 4).Although this technique can also be car-
ried out using porcelain chips, the degree oftooth preparation required to achieve an
imperceptible join between the tooth andporcelain, along with associated problems ofcolor matching and cost preclude their usein the medium-term in teenagers and areideally provided in the early adolescent agegroup upward.
CASE REPORTDiagnosis and Treatment Planning
The 16-year-old patient seen in Figures 5a to5c presented for a cosmetic opinion towardthe completion of his orthodontic treat-ment. In the lower arch, both central inci-sors were congenitally absent, and ortho-dontic tooth movement had provided aone-toothed space for restoration. His ageprecluded implant placement and the inter-im proposed solution of the provision of aconventional Maryland bridge was accept-ed by the patient and his mother.The aesthetic problems in the maxillary
arch were more complex. Both lateral inci-sors were malformed as well as misshapen.All 4 incisors were wider at the necks thanat the incisal edge, with both canines rela-tively pointed. As tooth positioning follow-ing orthodontics was excellent for aesthet-ics and lip support, further treatment tobring the teeth together would have beencounterproductive. Finally the patient andhis mother were adamant that whichevertechnique was chosen to improve aesthet-ics, it was to be minimally if at all invasive.The patient additionally requested that
tooth whitening be carried out prior to therestorative phase of treatment, and his exist-ing Raintree Essix Orthodontic Retainers(DENTSPLY International) were used as traysfor “at-home” whitening using 15% Carba -mide Peroxide Gel (Ultradent Products).Study casts were taken and mounted
with a face-bow on a semi-adjustable articu-lator (Dentatus). The case was studied withparticular respect to the proposed space clo-sure and the maintenance of the correctcrown width to length ratio of 75% and cor-responding Golden Proportion ratios forremaining teeth. Although minimum/nopreparation veneers (eg, Lumineers) were anoption if crown length was to be in creased,this approach was not the preferred choiceof the patient.
Tom Bereznicki,BDS (Edin)
Lola Welch
An Alternative Approach to Cosmetic Space Closure
continued on page 154
AESTHETICS
Figure 1. An example of poor aesthetics with direct
composite bonding.
Figure 2. A pretreatment aesthetic dilemma
presented by the excessively large diastemas.
Figure 3. The case following Invisalign orthodontic
tooth movement. (Courtesy of Dr. R. Edwards.)
Figure 4. The case upon completion of indirect com-
posite.
AESTHETICS154
Tooth size was analyzed by my tech-nician with Digital Callipers (Har borFreight Tools) and a diagnostic wax-upcarried out with IQ Compact OpaqueWax (Yeti Dental) without increasingtooth length (Figures 6 and 7), whileensuring that the theoretical demandsof the Golden Proportion were met. Thefollowing treatment plan was proposed:2 composite ve neers to address the issueof tooth width and the malformed buc-cal surfaces of the lateral incisors, aswell as the provision of indirect inter-proximal composite veneers on the cen-tral incisors to close the remainingdiastemas and mesially on both caninesto im prove their aesthetic appearance.The existing large overjet followingorthodontic treatment would ensurethat oc clusal stresses on the compositeres torations were minimal and chip-ping unlikely in everyday usage.The patient was informed that min-
imal preparation of the lateral incisorswould be necessary to im prove theirsurface morphology and provide finish-ing lines. In addition, the provision ofminimal depth grooves within enamelon the central incisor and canine teethwould be required to provide locationand seamless transition between thecomposite chips and enamel on thebuccal surfaces of the teeth. Similarcases were demonstrated to the patientand the treatment plan accepted.
Clinical TechniqueFollowing tooth whitening, colorswatches similar in shape to the finalrestorations were made in a variety ofcomposite combinations on the upperstudy model to trial fit on one of thecentral incisors. These swatches werelocated in turn and, without enameletching, bonded sequentially in placewith the chosen translucent compos-ite luting cement (Choice 2 Cement[BIS CO Dental Products]) to be used infinal bonding, until such time as thecorrect color match had beenachieved. The color combination wasnoted for future use during fabrica-tion of the final restorations.
While refining this technique inprevious cases, it became apparentthat the issue of the emergence profileand the creation of papillae could onlybe addressed by extending the veneerchips subgingivally to a featheredgemargin necessitating use of retractioncord prior to tooth preparation. Thedesign of the chips also required posi-tive location to ensure correct place-ment and positioning on the teethduring bonding. To satisfy this re -quirement, the shape of each chip wasextended over the incisal edge to pro-vide a location handle and cut awayonce bonding was completed.Following placement of gingival
retraction cord (Racestyptine Cord[Septodont]), the necessary minimaltooth reduction was carried out conven-tionally for the full veneers, and verti-cally on the buccal surfaces of the otherteeth and extending along the gingivalmargin just into the palatal surface inorder to provide a positive finishing line(Figures 8a and 8b). The final impres-sion was taken with Polyether Rubber(Impregum 6 Minute Hard [3M ESPE])in a custom tray. Temporary restora-tions were not required in this case.Then, the final impression was pouredin stone (Fuji Rock [GC America]) to fab-ricate the working model (Figure 9).For the laboratory stage of fabrica-
tion, an indirect composite systemwas chosen (Gradia [GC America]). Aseparator (Gradia Separator [GC Amer -ica]) was applied to the working modeland the chips fabricated to the previ-ously chosen shade combination: A1dentine combined with a superficiallayer of enamel E2 and IntensiveEnamel EI1. Translucent enamel wasused only on the locating handle. To ensure that the aesthetic
appearance achieved with the trialwax-up was duplicated, the dentaltechnician started by creating theideal shape and width of the fullveneers on both lateral incisors, fol-lowed by the space closure veneers(Figure 10) on the mesial surfaces ofthe canines and, finally, on the distalthen mesial surfaces of the centralincisors (Figure 11).The authors’ preferred composite
bonding system in cases such as thesecomprises of Uni-etch, One step Plus,Composite Activator, and Choice 2Cement (Translucent) (BISCO DentalProducts). Translucent cement wasused to ensure that the transitionbetween the enamel and compositechip would be imperceptible, common-ly known as the contact lens effect. Theuse of a shaded cement can often resultin the transition line being visible.
DENTISTRYTODAY.COM • JANUARY 2012
An Alternative Approach...continued from page 152
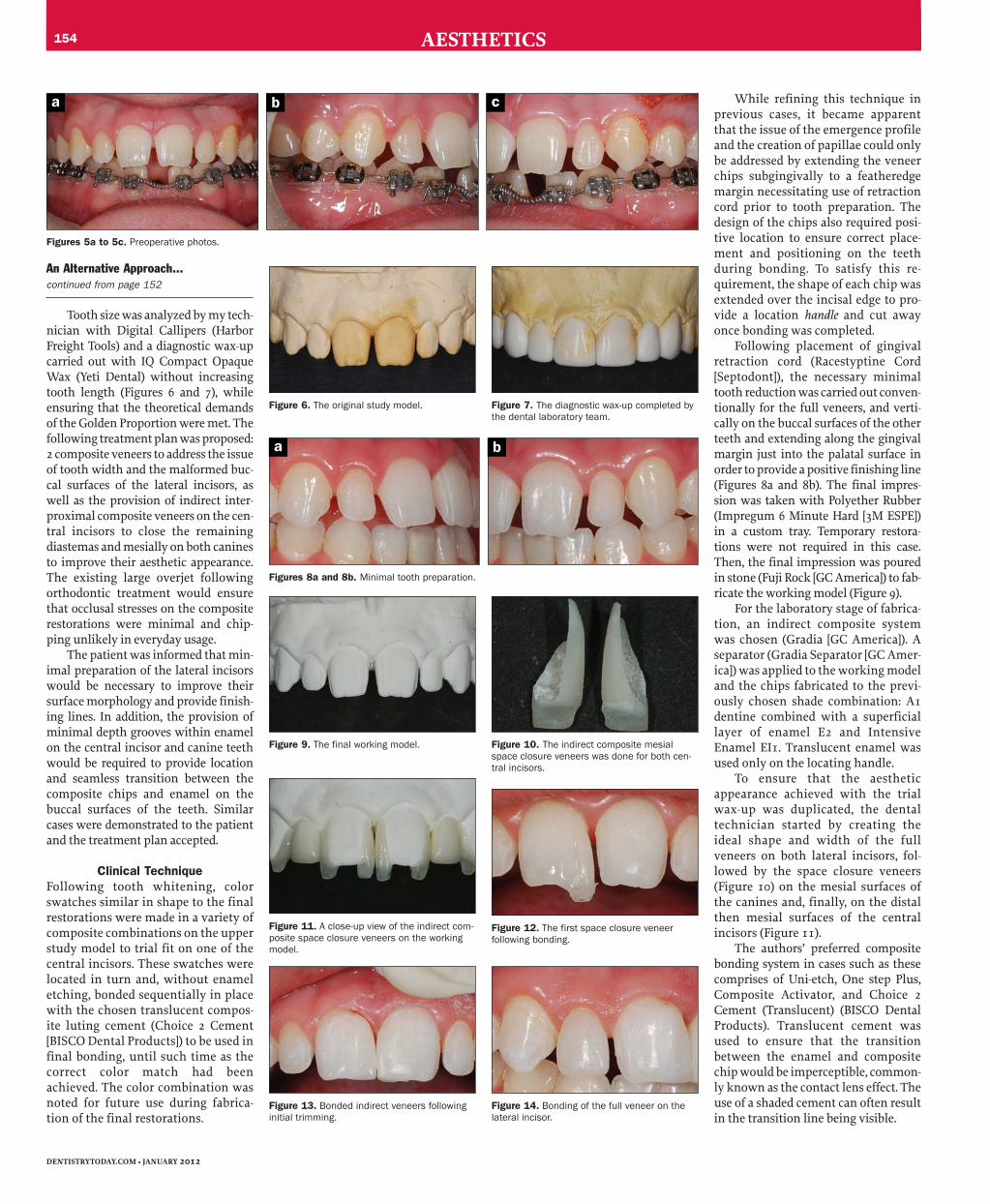
Figures 5a to 5c. Preoperative photos.
Figure 6. The original study model.
Figures 8a and 8b. Minimal tooth preparation.
Figure 7. The diagnostic wax-up completed by
the dental laboratory team.
Figure 11. A close-up view of the indirect com-
posite space closure veneers on the working
model.
Figure 9. The final working model. Figure 10. The indirect composite mesial
space closure veneers was done for both cen-
tral incisors.
Figure 12. The first space closure veneer
following bonding.
Figure 13. Bonded indirect veneers following
initial trimming.
Figure 14. Bonding of the full veneer on the
lateral incisor.
a b c
a b
AESTHETICS
Final PlacementIsolation was achieved with the place-ment of rubber dam, but the clinical pho-tographs shown are following sequen-tial cementation and removal of the rub-ber dam to give a clearer picture of theresults achieved with each clinical step.
Prior to etching, the teeth in -volved were thoroughly cleaned byspraying 50 μm oxide powder usingthe EtchMaster (Groman Dental) andall the powder thoroughly washed off.
Prior to bonding each full veneer andindividual chip, the tooth was isolat-ed from adjacent teeth with a cellu-loid matrix strip. Each surface wastreated sequentially with the manu-facturer’s recommended techniquewhich is common for all compositebonding systems; namely etching theenamel, thorough washing of theetchant gel, drying, then applicationof the bonding agent and subsequentlight-curing. The fit surface of eachchip was treated with composite acti-vator prior to the application of OneStep Plus but not light-cured. A thinlayer of cement was applied to the fitsurface and the veneer gently easedinto place and excess luting cementremoved with a sable brush prior tolight-curing. In the case of each chip,the handle was removed first and,along with the cemented veneers, pol-ished with composite finishing discsand rubber cups (Shofu Dental) priorto fitting the next one in the cement-ing sequence. Each subsequent chipwas trial fitted to ensure correct loca-tion and passive fit prior to furtherbonding. The cementation sequenceis shown in Figures 12 to 15.
The case pre- and postbonding isshown in Figures 16 and 17, and afterfitting the lower Maryland bridge inFigures 18 and 19. The final clinicalresults achieved are shown in Figures20 and 21.
CONCLUSIONThe suggested technique as outlined isvery predictable and it demonstratesboth excellent aesthetics and colormatching. Natural-looking gingivalpapillae, resulting from proper emer-gence profile, were created by the fab-ricated shape of the veneers and chips.The technique has the added benefit of
being simple and cost-effective asskilled dental technicians versed inthe art of indirect composites can easi-ly carry it out. Composites haveshown excellent and predictablelongevity, especially when bonded toenamel. If necessary, following thearrival of full dental maturity, thecomposite can easily be stripped offand replaced (utilizing the same tech-nique described herein) using anappropriate pressed ceramic material.
The clinical technique presentedin this article offers clinicians a sim-ple and effective method of fulfilling apatient’s requirement for a cost-effec-tive, predictable, noninvasive solu-tion to a complex aesthetic challengein adolescents.�
Dr. Bereznicki graduated from Edinburgh
Dental Hospital and School in 1976. He moved
to London and after various house surgeon
appointments at Guy’s Hospital and the Royal
Dental Hospital, he entered general practice
and started his own private practice in
Queensgate, London in 1982. Recently, he has
joined the Dawood and Tanner Dental Practice
in London as a member of the res torative team.
His area of special interest is aesthetic dentistry