22
An Approach to Rheumatologic Diagnosis, Osteoarthritis, and Fibromyalgia Roderick Fields, M.D.
An Approach to Rheumatologic Diagnosis, Osteoarthritis, and
Fibromyalgia
Roderick Fields, M.D.

Quick Notes on Age, Sex, and Distribution Specificities
How to make the diagnosis before seeing the patient

Age and Sex Specificities
• Young female: Think RA, SLE, Fibromyalgia
• Older female: Think OA, RA (bimodal presentation, Polymyalgia Rheumatica, Gout (over 50 y/o, gout prevalence in females equal to that in males
• Young male: Think Reactive Arthritis, RA, Gout
• Older male: Think OA, Gout, Pseudogout

Distribution Specificities
• Lower Extremity: HLAB27 related arthritis, gout
• Root Joints: Polymyalgia Rheumatica
• Symmetric Small Joint: RA, SLE
• Axial Pain: HLAB27 related, tumor, infection
• 1st MTP (Podagra): Gout, bunion, Pseudogout, reactive arthritis

Distribution Specificities (continued)
• Unilateral inflamed wrist: Pseudogout (look for calcification in the triangular fibrocartilage)
• 1st CMJs, DIPs, Hips, Knees: Primary OA
Osteoarthritis
• Primary
• Secondary
• Post Traumatic

Primary Osteoarthritis
• Older males and females
• Distribution: DIPs (Heberden’s nodes), PIPs (Bouchard’s nodes, Hips, Knees (medial compartment initially as opposed to lateral compartment involvement in inflammatory disease)
• Genetically determined
• Most common arthritis in world (40 million in U.S.) No disease modifying therapy available

Osteoarthritis Hands

Osteoarthritis of Hip
Secondary Osteoarthritis
• Osteoarthritis in atypical areas
• Primary OA does not occur in the ankles, wrists, MCPs, shoulders (glenohumeral articulation), or elbows.
• Usually crystal induced: Gout, Pseudogout, basic calcium phosphate.
• Radiologic clues: MCP Hooks, chondrocalcinosis, joint space loss without erosions

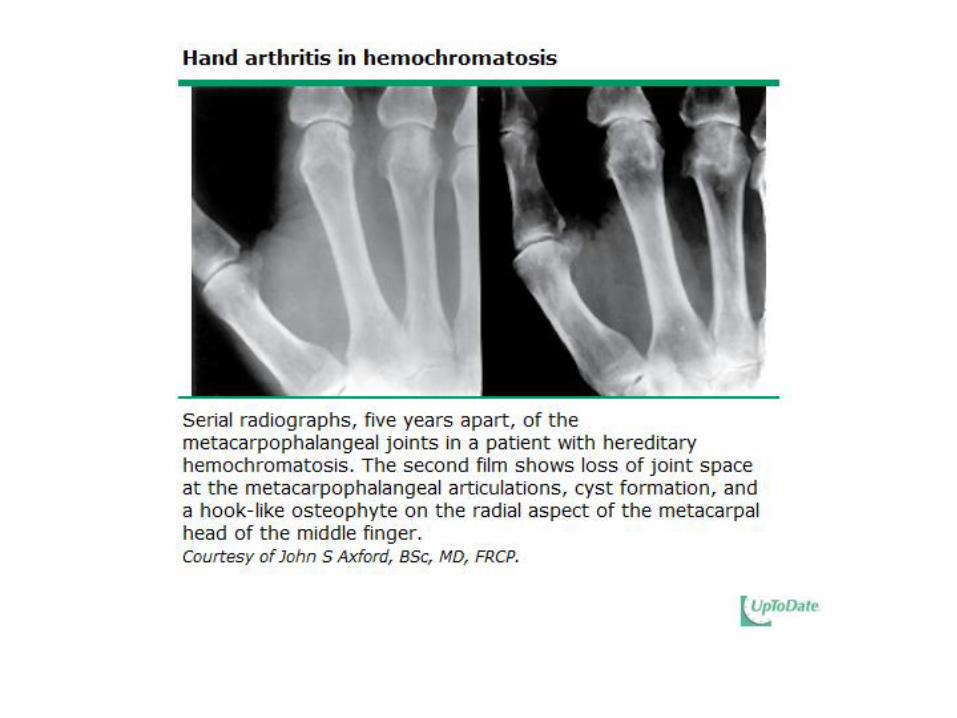

Look for Associated Metabolic Diseases in Secodary Osteoarthritis
• Pseudogout associated with hemochromatosis, hyperparathyroidism, Wilson’s Disease
• Gout
Diffuse Musculoskeletal Pain Syndrome (AKA Fibromyalgia)
• Diffuse pain involving muscle and joints
• High Prevalence in young female patients presenting to rheumatology office
• Neuropathic pain symptomatology
• Associated with sleep disorder (interruption or non-restful sleep)
• Trigger points on physical exam
• Absence of joint swelling
ACR Preliminary Diagnostic Criteria for Fibromyalgia
• Widespread pain index (WPI) greater than or equal to 7 and symptom severity (SS) scale score greater than or equal to 5 or WPI 3-6 and SS scale score greater than or equal to 9.
• Symptoms have been present at a similar level for at least 3 months
• The patient does not have a disorder that would otherwise explain the pain.

Differential Diagnosis of Fibromyalgia
• RA, SLE, myositis, polymyalgia rheumatica (in older patients)
• Hypothyroidism (common)
• Hepatitis C
• Paraneoplastic disease in older patients

Screening Lab Evaluation for a Patient with Rheumatologic Complaints
• CBC, CMP (metabolic profile), CPK
• UA
• T4, TSH
• RF, anti-CCP, ANA, HLAB27
• Sed rate, CRP
• Hepatitis Panel

Treatment of Osteoarthritis
• NSAIDs (Risk of ulcer, stroke, and MI – Counsel the patient). Chronic use not recommended.
• Analgesics (acetaminophen, tramadol, low dose narcotic analgesics)
• Injection (steroids, hyperviscosity agents)
• Surgery
Treatment of Fibromyalgia
• Low dose tricyclics at hs
• Cyclobenzaprine hs
• Duloxetine
• Lyrica (or neurontin)
• Aerobic exercise
• CPAP in OSA patient

Lupus Arthritis

Rheumatoid Arthritis

Rheumatoid Arthritis Hip

















