An economic comparison of surgical and medical therapy in patients with secondary hyperparathyroidism—the German perspective Ralph Schneider, MD, a Georgios Kolios, MD, b Benjamin M. Koch, a Emilio Dom ınguez Fernandez, MD, c Detlef K. Bartsch, MD, a and Katja Schlosser, MD, a Marburg, Bremen, and Hannover, Germany Background. Treatment options for secondary hyperparathyroidism were significantly amended with the introduction of cinacalcet and paricalcitol. Limitations of resources in public health systems demand detailed analyses of accruing costs. The aim of this study was to compare the costs of these new treatment modalities to surgery. Methods. Patients who underwent initial parathyroidectomy (n = 91) and patients treated with cina- calcet or paricalcitol (n = 100) at an ambulatory dialysis center between 01/2003 and 12/2006 were analyzed. The revenues of both therapies for the funding agencies were calculated by a cost-cost analysis. The real arising costs of the supplier were analyzed and compared to the revenues. Results. Treatment costs for cinacalcet (60 mg/day/year) were 5828.40V and 4485.20V for paricalcitol (15 mg/week/year). Revenues for inpatient surgical treatment according to the German DRG system were 3755.38V/case. Additionally, costs for postoperative ambulatory therapies were 545.05V for the first year and 384.97V for the following. Conclusion. Due to linearly increases, expenses of medical treatment with cinacalcet for more than 9 months or paricalcitol for more than 12 months exceeded the costs of surgical therapy. The indication of these new medical therapies should be restricted to patients as an interim solution ahead of surgery or in patients considered unfit for surgery. (Surgery 2010;148:1091-9.) From the Department of Visceral, Thoracic and Vascular Surgery, a Philipps University, Marburg, Department of Plastic, Reconstructive and Aesthetic Surgery, b University of Bremen, and Department of General, Visceral and Vascular Surgery, c Clinical Centre Nordstadt, Hannover, Germany SECONDARY HYPERPARATHYROIDISM (sHPT) is a common sequel of chronic kidney disease (CKD) developing in response to high phosphate, low calcium and low 1,25-dihydroxyvitamin D 3 (calcitriol) levels. High levels of parathyroid hormone (PTH) accelerate bone turnover, with efflux of calcium and phosphate leading to vascular calcifications and renal osteopathy. 1 Until the beginning of this century, the medical treat- ment of sHPT comprised the application of calcitriol and calcium-based phosphate binders. A successful kidney transplantation is the only causal treatment available to correct the abnormalities in mineral metabolism. 2 However, limited availability of kidney transplants or high comorbidities preventing trans- plantation led to a high percentage of patients requiring operative intervention with total parathy- roidectomy (PTX) with autotransplantation or subtotal PTX, both worldwide accepted equivalent standard procedures in the surgical treatment of sHPT. 3 The introduction of vitamin D analogs and calcimimetics in 2004 and 2005 was considered as a ‘‘breakthrough’’ in the medical treatment of sHPT. 4 Vitamin D analogs such as paricalcitol (ZemplarÒ) inhibit PTH gene transcription and parathyroid hyperplasia and have the advantage of a reduced calcemic activity when compared to vitamin D. Sev- eral such analogs are now in use, and analogs with even greater selectivity than those currently available are in development. 5 However, the role of vitamin D analogs and PTX needs to be re-evaluated in the calcimimetic era. 6 Cinacalcet (SensiparÒ/MimparaÒ) is the first of the new class of calcimimetic drugs approved for the treatment of sHPT. Calcimimetics suppress the R.S. and G.K. contributed equally to this work. Accepted for publication December 18, 2010. Reprint requests: Ralph Schneider, MD, Philipps University Marburg, Department of Visceral, Thoracic and Vascular Sur- gery, Baldingerstrasse, 35043 Marburg, Germany. E-mail: [email protected]. 0039-6060/$ - see front matter Ó 2010 Mosby, Inc. All rights reserved. doi:10.1016/j.surg.2010.09.009 SURGERY 1091
Transcript
R.S. and
Accepte
ReprintMarburggery, BRalph.S
0039-60
� 2010
doi:10.1
An economic comparison of surgicaland medical therapy in patients withsecondary hyperparathyroidism—theGerman perspectiveRalphSchneider,MD,aGeorgiosKolios,MD,b BenjaminM.Koch,a EmilioDom�ınguez Fern�andez,MD,c
Detlef K. Bartsch, MD,a and Katja Schlosser, MD,a Marburg, Bremen, and Hannover, Germany
Background. Treatment options for secondary hyperparathyroidism were significantly amended with theintroduction of cinacalcet and paricalcitol. Limitations of resources in public health systems demanddetailed analyses of accruing costs. The aim of this study was to compare the costs of these new treatmentmodalities to surgery.Methods. Patients who underwent initial parathyroidectomy (n = 91) and patients treated with cina-calcet or paricalcitol (n = 100) at an ambulatory dialysis center between 01/2003 and 12/2006 wereanalyzed. The revenues of both therapies for the funding agencies were calculated by a cost-cost analysis.The real arising costs of the supplier were analyzed and compared to the revenues.Results. Treatment costs for cinacalcet (60 mg/day/year) were 5828.40V and 4485.20V for paricalcitol(15 mg/week/year). Revenues for inpatient surgical treatment according to the German DRG system were3755.38V/case. Additionally, costs for postoperative ambulatory therapies were 545.05V for the firstyear and 384.97V for the following.Conclusion. Due to linearly increases, expenses of medical treatment with cinacalcet for more than 9months or paricalcitol for more than 12 months exceeded the costs of surgical therapy. The indication ofthese new medical therapies should be restricted to patients as an interim solution ahead of surgery or inpatients considered unfit for surgery. (Surgery 2010;148:1091-9.)
From the Department of Visceral, Thoracic and Vascular Surgery,a Philipps University, Marburg, Departmentof Plastic, Reconstructive and Aesthetic Surgery,b University of Bremen, and Department of General, Visceraland Vascular Surgery,c Clinical Centre Nordstadt, Hannover, Germany
SECONDARY HYPERPARATHYROIDISM (sHPT) is a commonsequel of chronic kidney disease (CKD) developingin response to high phosphate, low calcium and low1,25-dihydroxyvitamin D3 (calcitriol) levels. Highlevels of parathyroid hormone (PTH) acceleratebone turnover, with efflux of calcium and phosphateleading to vascular calcifications and renal osteopathy.1
Until the beginning of this century, themedical treat-ment of sHPT comprised the application of calcitrioland calcium-based phosphate binders. A successfulkidney transplantation is the only causal treatmentavailable to correct the abnormalities in mineral
G.K. contributed equally to this work.
d for publication December 18, 2010.
requests: Ralph Schneider, MD, Philipps University, Department of Visceral, Thoracic and Vascular Sur-aldingerstrasse, 35043 Marburg, Germany. E-mail:[email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
016/j.surg.2010.09.009
metabolism.2 However, limited availability of kidneytransplants or high comorbidities preventing trans-plantation led to a high percentage of patientsrequiring operative intervention with total parathy-roidectomy(PTX)withautotransplantationor subtotalPTX, both worldwide accepted equivalent standardprocedures in the surgical treatment of sHPT.3
The introduction of vitamin D analogs andcalcimimetics in 2004 and 2005 was considered as a‘‘breakthrough’’ in the medical treatment of sHPT.4
Vitamin D analogs such as paricalcitol (Zemplar�)inhibit PTH gene transcription and parathyroidhyperplasia and have the advantage of a reducedcalcemic activity when compared to vitamin D. Sev-eral such analogs are now in use, and analogs witheven greater selectivity than those currently availableare in development.5 However, the role of vitamin Danalogs and PTX needs to be re-evaluated in thecalcimimetic era.6
Cinacalcet (Sensipar�/Mimpara�) is the first ofthe new class of calcimimetic drugs approved for thetreatment of sHPT. Calcimimetics suppress the
secretion of PTH by sensitizing the parathyroidcalcium receptor to extracellular calcium.2 Com-bined with higher doses of calcium-based oral phos-phate binders, it is mostly well tolerated and alreadyconsidered as an effective alternative to standardmedical treatments such as vitamin D derivatives to-gether with non--calcium-based oral phosphatebinders.2 Clinical trials demonstrated cinacalcet tobe effective in suppressing PTH secretion in uremicpatients with severe sHPT in whom formerly PTXmight have been considered. Therefore, calcimi-metics were claimed to be an alternative to PTX.2
However, evidence for an impact on clinical eventssuch as mortality, cardiovascular events or fracturesis based on short-term post hoc analyses7 and mostof the trials with cinacalcet are supported by the in-dustry merchandising this drug. Whether the appli-cation of cinacalcet will translate in improvedoutcomes remains to be demonstrated and ade-quately powered prospective controlled random-ized studies independently performed fromindustrial influence are needed.6 Reports aboutPTX rates before and after the introduction of ei-ther one of these new drugs are unavailable andthe rate of patients requiring PTX after unsuccess-ful treatment with either calcimimetics or vitaminD analogs needs to be evaluated.8 At present, the ris-ing costs of vitamin D analogs and cinacalcet are re-funded without any restrictions in Germany, andconsecutively decision-making between medical orsurgical therapy often depends on personal inter-ests and experiences of both patients andnephrologists.
To the best of our knowledge, no analysis isavailable comparing the costs of the surgical treat-ment and the costs of these new medical treat-ments with either cinacalcet or paricalcitol.
The aim of this study was to obtain objectiveinformation allowing a transparent estimation ofcosts associated with cinacalcet or paricalcitolmedication as well as with surgical therapy tofind out which therapy is more cost effective.Consequently, the results should facilitate thedecision-making process in reference to resources,regulations, and developmental processes.
MATERIALS AND METHODS
Data of the present study refer to a retrospectiveanalysis of a prospective database regarding thepatients who underwent surgery and to a retro-spective review of outpatient files of patients whoreceived a medical therapy with either cinacalcetor paricalcitol in 2 dialysis centers.
The inpatient surgical sector taken for economicevaluation comprised all patients with advanced
sHPT who underwent initial PTX between January2003 and January 2006 at a tertiary referral surgicalcenter (n = 91). The standard surgical procedurewas a total PTX with a parathyroid autotransplanta-tion into the forearm.
The costs of surgical therapy comprised inpa-tient costs, as well as costs for special postoperativeambulatory measures including blood examina-tions and calcium and calcitriol supplementation.The revenues were calculated on the basis of theGerman diagnosis related grouping (DRG) calcu-lation system, where base-case values are multi-plied with a relative weight. To find out if theinpatient surgical therapy can be performed cost-covering, the real arising costs for the supplier(hospital) were analyzed and compared to therevenues. An activity-based costing approach basedon clinical pathways, which allocated the individ-ual and overhead costs to processes, was chosen foran appropriate real cost accounting. Therefore,primary, secondary, and tertiary processes weredefined.
Primary processes comprised main activitiesincluding personal and material costs, whichwere directly related to the treatment. The nursingrelated activity was calculated summarizing thedaily allocation of each patient with correlatedworking minutes. Nursing related activitiescomprised admission examinations, transport ofpatients (x-ray, electrocardiogram, operation thea-ter), preoperative preparation of patients as well asdocumentation and other nursing activities on theward. Nursing efforts in the operation theater weredefined in a special ‘‘operation pathway’’ includingthe efforts of 1 anesthetic and 2 surgical nurses.The personnel costs of the nurses were calculatedon the basis of the salaries and the workingminutes at 0.50V per minute. The physician re-lated activity was calculated on the working min-utes for every process per patient on the ward(interviews, examinations, ward rounds, documen-tations). In the operation theater, the efforts of 2surgeons and 1 anesthetist were taken into consid-eration. The calculated minutes were multipliedwith personnel costs on the basis of the meansalaries of 2 residents (1 surgeon and 1 anesthetist)and 1 consultant of 1.05V per minute. Materialcosts were calculated considering wound dressingmaterials, surgical drapes, anesthetic materials,and drugs and disposable items like clips andsutures, as well as costs for sterilization of surgicalinstruments. The working minutes of physiciansand nurses on the ward were extrapolated fromestimates based on interviews to all nurses andphysicians involved in the care of patients with
0
5
10
15
20
25
30
35
40
2003 2004 2005 2006 2007 2008 2009Years
Nu
mb
er o
f p
atie
nts
u
nd
erg
oin
g in
itia
l P
TX
fo
r s
HP
T
Fig 1. Number of patients undergoing initial PTX forsHPT per year.
SurgeryVolume 148, Number 6
Schneider et al 1093
sHPT. The working minutes in the operationtheater were extrapolated as the mean of theprecise data provided by both the surgical andanesthetic protocols of all 91 patients who under-went a PTX.
Secondary processes comprised personal andmaterial costs provided by other departments ofthe hospital. The costs of medical functional ser-vices such as laboratory, radiology, pathology,nuclear medicine, and others were calculatedaccording to a catalog listing the equivalence-numeral-calculations of the German Hospital So-ciety (DKG-NT-table), where a point system ofinpatient and outpatient services for hospitals isdepicted. Every department is given a score whichis calculated on the total costs for the departmentdivided by the sum of all scores provided over aperiod of 1 year. Afterwards this score is mul-tiplied with the points of the DKG-NT-table.The files of all patients who underwent surgerywere screened for these services, and the costsfor every service in each patient were calcu-lated. The mean costs were used for the finalcalculation.
Tertiary processes were defined as activities ofthe hospital infrastructure without direct relationto the treatment (technical service, kitchen, clean-ing service, energy costs). These estimates refer tothe costs which arise for any patient admitted tothe hospital per treatment day independentlyfrom the reason of admission. The sum of alloverhead costs of 2006 was divided by the sum ofall treatment days of 2006 and multiplied by theindividual hospital stay of each of the 91 patientswho underwent surgery. The mean costs were usedfor the final calculation.
These primary, secondary, and tertiary processeswere summarized for every individual patient inorder to optimally display the clinical pathways andthen to calculate the real costs for the inpatienttherapy.
Costs for reoperations due to postoperative com-plications or recurrent/persistent disease wereadded into the calculation. A reoperation rate of5%was chosen as a result of a follow-up study not yetpublished concerning 479 patients who underwentsurgery at our department between the years 1976and 2003. This study revealed a rate of persistentsHPTof 0.6% and a rate of recurrent sHPTof 4.6%after a mean follow-up of 57.6 months.
Patients who underwent initial PTX for sHPT inthe following years (2007--2009) were counted toachieve information about the trend in thenumbers of PTX performed in the era after theinitiation of vitamin D analogs and calcimimetics.
The ambulatory medical sector comprised allpatients who were treated with cinacalcet orparicalcitol in 2 dialysis centers (n = 100) betweenJanuary 2003 and January 2006. The costs of bothmedical therapies for the funding agencies werecalculated depending on their dosage and on costsfor laboratory measures. Considering a typical dis-count of 5% for funding agencies, the costs werecorrespondingly reduced. The dosages per patientwere analyzed, leading to a mean dosage of 60mg/day for cinacalcet and of 3 ml/week for paricalci-tol. The costs were summarized per month over atime period of 2 years. Physical or other examina-tions which were necessary due to dialysis werenot taken into consideration.
An analysis comparing the costs for surgical andthe costs for medical therapies was then performed(cost-cost analysis).
RESULTS
Ninety-one patients with sHPT who underwentinitial PTX between January 2003 and January 2006were analyzed. Of these 91 patients, 29 had a failedtreatment attempt with cinacalcet or paricalcitolprior to surgery. The number of patients whounderwent initial parathyroid surgery for sHPTdecreased from 37 in 2003 to 28 in 2004, 21 in2005, and 5 in 2006. The number of initial PTX forsHPT increased thereafter with 12, 13, and 20patients in the years 2007, 2008 and 2009, respec-tively (Fig 1). The mean duration of hospital stay ofthe patients considered for economic evaluationwas 7.3 ± 4.31 days. One patient had to undergo acervical revision for persistent sHPT due to amissedfifth gland within the carotid sheath. Within afollow-up period of 3 years after surgery, 2 patients
Table I. Revenues for our hospital for the treatment of sHPT
Year DRG text DRG codeRelativeweights
Base-case-value (V)
Revenue/case (V)
Numberof patients
Overallrevenue (V)
2003 ‘‘Parathyroid surgery’’ or ‘‘otherdisorders resulting from impairedrenal tubular function’’ or‘‘secondary hyperparathyroidismof renal origin’’
K05Z901ZL09B
1.1791.4792.137
3169.83 3737.234688.186773.93
3511
130 830.034 688.186 773.93
Average revenue per case (2003) 3 845.002004 ‘‘Procedures on the thyroid the
parathyroids or the thyroglottic duct’’or ‘‘other procedures for kidneyand urinary tract disorders’’
L09BK12Z
1.4051.390
3054.43 4291.474245.66
820
34 331.7984 913.15
Average revenue per case (2004) 4 258.752005 ‘‘Parathyroid disorders’’ or ‘‘Procedures
on the thyroid the parathyroids orthe thyroglottic duct’’ or ‘‘Otherdisorders resulting from impairedrenal tubular function’’ or‘‘secondary hyperparathyroidismof renal origin’’
K11ZL09BL18ZK64C901D
1.2571.1691.3310.6761.879
2954.71 3714.073454.063932.721997.385551.90
611112
22 284.4237 994.623 932.721 997.3811 103.80
Average revenue per case (2005) 3 681.572006 ‘‘Parathyroid disorders’’ or ‘‘procedures
on the thyroid the parathyroids orthe thyroglottic duct’’ or‘‘parathyroid procedures’’
K11ZL09BX06B
1.2171.2851.146
2806.35 3415.333606.163216.08
221
6 830.667 212.323 216.08
Average revenue per case (2006) 3 451.81Mean revenues per case for the whole period, calculated from the mean annual revenues and
the number of patients treated per year3 559.79± 484.22
SurgeryDecember 2010
1094 Schneider et al
developed recurrent sHPT at the parathyroid auto-graft and had to undergo an autograft reduction.
The ambulatory medical sector comprised 50patients who were treated with cinacalcet and 50patients who were treated with paricalcitol in 2dialysis centers (n = 100) between 01/2003 and01/2006. An interview with the nephrologists incharge addressing the outcome of these 100 pa-tients revealed a high lost to follow-up rate of18%, another 13% underwent PTX after a meanmedical treatment duration of 25.6 months with ei-ther cinacalcet or paricalcitol, 38% achieved a sig-nificant (>50%) reduction in PTH levels, and 31%patients exhibited minor or no response regardingPTH. The latter are considered unfit for surgery,refuse surgical intervention, or are already sched-uled for PTX in the meantime.
The calculation of the mean annual inpatientrevenues is shown in Table I. The mean revenuesper case for the whole period, calculated from themean annual revenues and the number of patientstreated per year, were 3559.79V ± 484.22V. Consid-ering a reoperation rate of 5% due to postoperativecomplications or recurrent/persistent disease therevenues increased to 3755.38V for Germany. Addi-tional costs for postoperative ambulatory therapies
were 545.05V for the first and maximum 384.97Vfor the following year. The sensitivity analyses con-sidering the different base-case values estimated a‘‘worst-case’’ revenue of 3589.77V and a ‘‘best-case’’ revenue of 3983.96V.
Costs of primary processes arising from nursingrelated activities were 571.50V per case assuming663 working minutes per patient on the ward and480 minutes per surgery in the operation theater.Time for physician relatedworkwas 243minutes perpatient on the ward and 541 minutes in the oper-ation theater resulting in a total amount of 823.20Vper case (Fig 2). Material costs were 643.66V percase. Costs of 1118.27V ± 650.40V per case werecalculated for secondary processes and of 685.89V± 407.45V per case for tertiary processes. The sum-mation of the costs for primary, secondary andtertiary processes revealed 3842.52V per case asthe real arising costs for the inpatient surgicaltreatment.
The mean revenues from the agencies for ourhospital were 3912.99V per case, leading to a cost-covering situation with a mean benefit of 70.47Vper case over all years analyzed (Table II). Neitherthe costs of the operative treatment nor the costsof the medical therapy varied over the years
Fig 2. Timeline of primary processes to physician and nurse related activities to estimate the real arising costs.
SurgeryVolume 148, Number 6
Schneider et al 1095
analyzed. However, the revenues decreased over theyears mainly attributed to a reduction of the base-case values. The cost-revenue relation per case forevery year analyzed is depicted in Table II. However,the cost-revenue analysis per year observed revealedan increasing unprofitable relation between thesemeasures, leading to resumed negotiations betweenthe hospital, the funding agencies, and the nephrol-ogists in charge to compile a treatment plan in theaim to regain a cost-covering situation.
The costs of the ambulatory medical therapiesmainly depended on the dosages of the drugs.Cinacalcet (28 tablets/package) was offered with30, 60, and 90 mg at 232.72V, 421.47V, and627.39V, respectively. Paricalcitol was offered inpackages containing 5 3 1-ml (5 mg/ml) at130.47V and 5 3 2 ml (5 mg/ml) at 251.29V.Monthly and yearly costs for cinacalcet and par-icalcitol are displayed in Tables III and IV.
The cost-intensive inpatient hospital stay causedhigher expenses for the surgical therapy within thefirstmonths. Due to linearly rising costs and lifelongapplication of the drugs the surgical expenses wereexceeded by cinacalcet after 9 months and byparicalcitol after 12 months (Fig 3). The postopera-tive costs remained almost constant within the out-patient period. These costs were depended on thedosages of calcium and vitamin D supplementationand the numbers of laboratory measures needed tocontrol calcium and PTH levels and are displayed inTables V and VI. We additionally performed a
sensitivity analysis considering different dosages ofthe drugs to differentiate between best and worst-case scenarios. In the worst case scenarios all pa-tients were treated with the highest dosage of eachdrug (cinacalcet 180 mg, paricalcitol 3 3 2 ml). Incontrast, the best case scenario was basedon the low-est dosages of each drug (cinacalcet 30mg, paricalci-tol 1 3 1-ml). The costs of surgical therapy wereexceeded by the costs for cinacalcet in the worstcase scenario after 3 months (Fig 4, A) and for par-icalcitol after 6 months (Fig 4, B). Based on the bestcase scenario surgical therapy has to be preferredfrom an economic point of view after 16 months(C) treatment with cinacalcet and after 31 months(D) treatment with paricalcitol.
DISCUSSION
According to the third National Health andNutrition Examination Survey, CKD affected asmany as 19 million adults in the U.S. in 2003, with20 million more at risk.9 The economic burdenassociated with CKD was recently analyzed in anobservational study of 13,796 predialytic pa-tients,10 the determined costs to treat CKD relatedcomorbidities were almost twice of those treatingCKD alone ($14,000 vs $8,000) and the cumulativecosts of CKD plus comorbidities were greater thantheir simple sum ($26,000 vs $22,000). However,these findings underscored the importance of anactive treatment of underlying risk factors forcomorbidities.10
Table II. The cost-revenue relation per case for every year analyzed
2003--2006 2003/2004 2005 2006
Mean revenue per case 3912.99 4258.75 3681.57 3451.81Mean cost per case 3842.52 3842.52 3842.52 3842.52Mean cost-revenue relation per case 70.47 416.23 �160.95 �390.71
All costs are in Euros.
Table III. Dosage dependent costs of medical treatment with cinacalcet
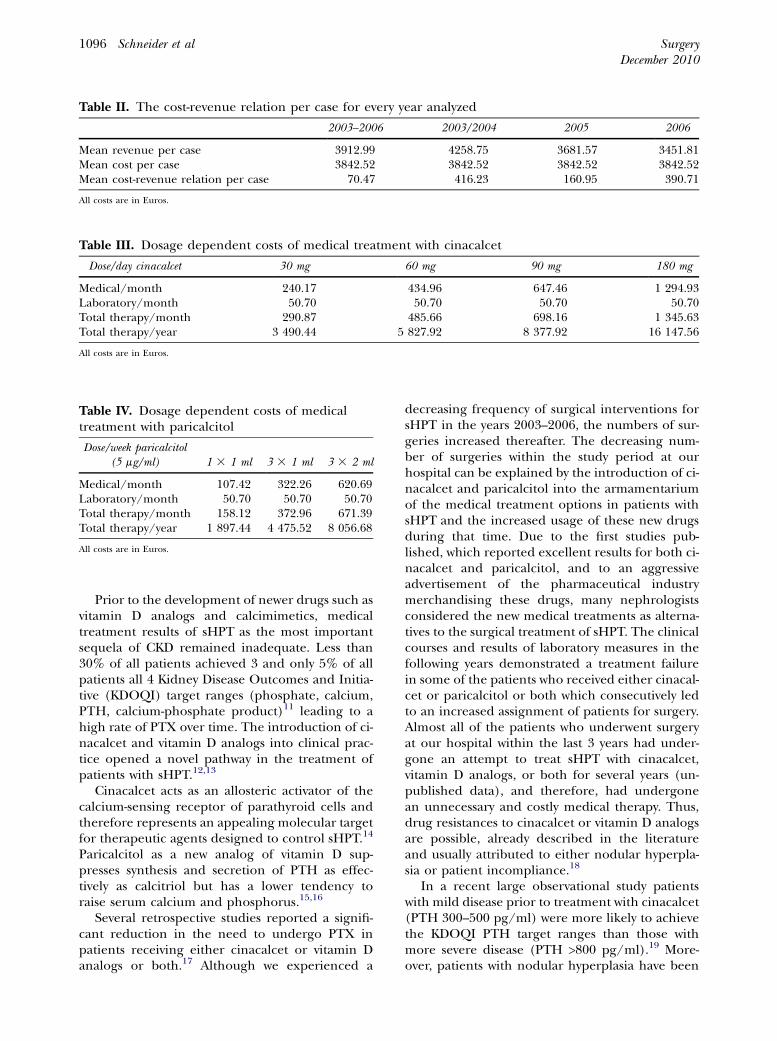
Prior to the development of newer drugs such asvitamin D analogs and calcimimetics, medicaltreatment results of sHPT as the most importantsequela of CKD remained inadequate. Less than30% of all patients achieved 3 and only 5% of allpatients all 4 Kidney Disease Outcomes and Initia-tive (KDOQI) target ranges (phosphate, calcium,PTH, calcium-phosphate product)11 leading to ahigh rate of PTX over time. The introduction of ci-nacalcet and vitamin D analogs into clinical prac-tice opened a novel pathway in the treatment ofpatients with sHPT.12,13
Cinacalcet acts as an allosteric activator of thecalcium-sensing receptor of parathyroid cells andtherefore represents an appealing molecular targetfor therapeutic agents designed to control sHPT.14
Paricalcitol as a new analog of vitamin D sup-presses synthesis and secretion of PTH as effec-tively as calcitriol but has a lower tendency toraise serum calcium and phosphorus.15,16
Several retrospective studies reported a signifi-cant reduction in the need to undergo PTX inpatients receiving either cinacalcet or vitamin Danalogs or both.17 Although we experienced a
decreasing frequency of surgical interventions forsHPT in the years 2003--2006, the numbers of sur-geries increased thereafter. The decreasing num-ber of surgeries within the study period at ourhospital can be explained by the introduction of ci-nacalcet and paricalcitol into the armamentariumof the medical treatment options in patients withsHPT and the increased usage of these new drugsduring that time. Due to the first studies pub-lished, which reported excellent results for both ci-nacalcet and paricalcitol, and to an aggressiveadvertisement of the pharmaceutical industrymerchandising these drugs, many nephrologistsconsidered the new medical treatments as alterna-tives to the surgical treatment of sHPT. The clinicalcourses and results of laboratory measures in thefollowing years demonstrated a treatment failurein some of the patients who received either cinacal-cet or paricalcitol or both which consecutively ledto an increased assignment of patients for surgery.Almost all of the patients who underwent surgeryat our hospital within the last 3 years had under-gone an attempt to treat sHPT with cinacalcet,vitamin D analogs, or both for several years (un-published data), and therefore, had undergonean unnecessary and costly medical therapy. Thus,drug resistances to cinacalcet or vitamin D analogsare possible, already described in the literatureand usually attributed to either nodular hyperpla-sia or patient incompliance.18
In a recent large observational study patientswith mild disease prior to treatment with cinacalcet(PTH 300--500 pg/ml) were more likely to achievethe KDOQI PTH target ranges than those withmore severe disease (PTH >800 pg/ml).19 More-over, patients with nodular hyperplasia have been
- €
500 €
1.000 €
1.500 €
2.000 €
2.500 €
3.000 €
3.500 €
4.000 €
4.500 €
5.000 €
5.500 €
6.000 €
6.500 €
7.000 €
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
months
co
sts
Surgery (average base-case-value nationwide)Paricalcitol (5μg/ml) 3 x 1ml/weekCinacalcet 60mg/day
Fig 3. Average treatment costs of treatment modalities over time.
Table V. Costs for calcitriol and calciumsupplementation within the postoperativeambulatory setting
Drug Costs Calcitriol (vitamin D) Calcium
Per day .53 .19Per week 3.73 1.33Per month 16.18 5.78Per year 194.18 69.35
All costs are in Euros.
SurgeryVolume 148, Number 6
Schneider et al 1097
reported to have a higher risk for cinacalcet resis-tance.20 Thus, the severity of sHPT and the degreeof nodular transformation potentially induce thedevelopment of resistance to the new drugs.
Very few reports exist about the proposed lengthof treatment and dosage titration for cinacalcet orparicalcitol to achieve KDOQI targets.17 These arti-cles report successful reductions in PTH already af-ter 3 months of treatment.11,19-21 Accordingly, theNational Institute for Health and Clinical Excel-lence of the United Kingdom recommended a con-tinuation of medication only in patients whoachieved a reduction in PTH levels of 30% ormore within 4 months of treatment, includingdose escalation if appropriate.22
Our study demonstrated that the costs for sur-gical therapy were exceeded by the linearly risingcosts for medical therapy already after a 9-monthtreatment with cinacalcet and after a 12-monthtreatment with paricalcitol. Our findings are inaccordance to those of Narayan et al who foundthe surgical intervention to be more cost effectiveafter 8 months when compared to a treatment withcinacalcet.23 In addition, Narayan showed thatPTX was more cost effective after 16 to 19 monthseven after calculating a combination of maximum
possible surgical costs and minimum cinacalcetcosts.23 To the best of our knowledge, this is thefirst study which provides a detailed cost-cost anal-ysis together with an estimate of the real arisingcosts concerning the treatment options in patientswith sHPT. Based on our results one has to suggestthat medical therapy may be optimal in patientswith an anticipated short time on dialysis therapy(<12 months) and mild sHPT. This group includespatients with a high expected mortality due to co-morbid illness or poor general health, patientswho expect to undergo transplantation in lessthan 1 year, dialysis patients with living donors,and those who do decline operative therapy,respectively. However, it is not known whether con-trol of PTH will be sustained after cessation of cina-calcet or paricalcitol. It is possible that underlyingdisease progression still occurs or that effectivenessmay not be sustained over the long-term.24 More-over, cinacalcet is not approved in patients afterkidney transplantation and it needs to be eluci-dated how many of those requiring pretransplantcinacalcet will have to undergo PTX or necessitateongoing costly off-label administered cinacalcettherapy thereafter.
Because our study referred to 2 different med-ical treatment arms, the group of patients observedwas unfortunately too small and heterogeneous togain reliable data about the treatment successes.To evaluate the outcome of these treatments,prospective randomized multicenter trials with astructured follow-up protocol have to be con-ducted. However, the wise use of medical resourcesis paramount to delivering cost-effective care andour study adds a helpful piece of information toenable the development of a reasonable durationand dosage recommendation for the medical
Table VI. Costs for laboratory measures within the postoperative ambulatory setting
Laboratory parameters
TotalCalcium PTH
Costs/laboratory measure (V) 2.76 33.12 35.88Number of laboratory measures in the 1st year postsurgery 78 2 80Total costs for laboratory measures in the 1st year
postsurgery (V)215.28 66.24 281.52
Number of laboratory measures in the 2nd yearpostsurgery
20 2 22
Total costs for laboratory measures in the 2nd yearpostsurgery (V)
55.20 66.24 121.44
Fig 4. Sensitivity analysis considering different dosages of the drugs compared to costs for surgical therapy over time.
SurgeryDecember 2010
1098 Schneider et al
therapies. A combination of our results and theresults of future prospective trials comparing thesuccess of medical and surgical treatments willhelp to facilitate the ever pressing challenge tosurgeons in choosing the right patient to undergosurgery, choosing the right surgical technique, andthen making the operative treatment more suc-cessful, less complicated, and less expensive.
In conclusion, sHPT is an important sequela ofCKD. The treatment options of sHPT have ex-panded substantially in the last years, with vitaminD analogs and calcimimetics being the most recentaddition. From an economic point of view surgicaltherapy should be preferred whenever possible.Especially in patients with only little effect onimproving mineral balance by cinacalcet or
vitamin D analogs, a prolongation of medicaltherapy over the recommended length of 4months seems to be unjustifiable and should notbe remunerated by the funding agencies. Random-ized studies are needed to predict which patientswill most likely gain benefit from early parathyroidsurgery in order to avoid unnecessary, prolonged,and costly medical therapy.
REFERENCES
1. Schlieper G, Floege J. Calcimimetics in CKD-results from re-cent clinical studies. Pediatr Nephrol 2008;23:1721-8.
2. Lewin E, Wang W, Olgaard K. Reversibility of experimentalsecondary hyperparathyroidism.Kidney Int 1997;52:1232-41.
3. Schlosser K, Veit JA, Witte S, Fern�andez ED, Victor N, Knae-bel HP, et al. Comparison of total parathyroidectomy
SurgeryVolume 148, Number 6
Schneider et al 1099
without autotransplantation and without thymectomy ver-sus total parathyroidectomy with autotransplantation andwith thymectomy for secondary hyperparathyroidism: TO-PAR PILOT-Trial. Trials 2007;8:22.
4. Felsenfeld AJ. Considerations for the treatment of second-ary hyperparathyroidism in renal failure. J Am Soc Nephrol1997;8:993-1004.
5. Brown AJ, Slatopolsky E. Drug insight: vitamin D analogs inthe treatment of secondary hyperparathyroidism in patientswith chronic kidney disease. Nat Clin Pract EndocrinolMetab 2007;3:134-44.
6. EvenepoelP.Calcimimetics inchronickidneydisease: evidence,opportunities and challenges. Kidney Int 2008;74:265-75.
7. Cunningham J, Danese M, Olson K, Klassen P, Chertow GM.Effects of the calcimimetic cinacalcet HCl on cardiovasculardisease, fracture, and health-related quality of life in sec-ondary hyperparathyroidism. Kidney Int 2005;68:1793-800.
8. Tominaga Y, Matsuoka S, Uno N. Surgical and medical treat-ment of secondary hyperparathyroidism in patients on con-tinuous dialysis. World J Surg 2009;33:2335-42.
9. Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prev-alence of chronic kidney disease and decreased kidneyfunction in the adult US population: Third NationalHealth and Nutrition Examination Survey. Am J KidneyDis 2003;41:1-12.
10. Joy MS, Karagiannis PC, Peyerl FW. Outcomes of secondaryhyperparathyroidism in chronic kidney disease and the di-rect costs of treatment. JManagCarePharm2007;13:397-411.
11. Portol�es J, Tato A, L�opez-S�anchez P, Gruss E, Cava F, Orti-gosa A, et al. [Cinacalcet in patients on peritoneal dialysiswith moderate to severe hyperparathyroidism resistant toconventional treatment, a one-year, prospective study].Nefrologia 2008;28:419-24.
12. Szczech LA. The impact of calcimimetic agents on the useof different classes of phosphate binders: results of recentclinical trials. Kidney Int Suppl 2004:S46-8.
13. Block GA. The impact of calcimimetics on mineral metabo-lism and secondary hyperparathyroidism in end-stage renaldisease. Kidney Int Suppl 2003:S131-6.
14. Nemeth EF, Steffey ME, Fox J. The parathyroid calcium re-ceptor: a novel therapeutic target for treating hyperparathy-roidism. Pediatr Nephrol 1996;10:275-9.
15. Lindberg J,Martin KJ, Gonz�alez EA, Acchiardo SR, Valdin JR,SoltanekC.A long-term,multicenter study of the efficacy andsafety of paricalcitol in end-stage renal disease. Clin Nephrol2001;56:315-23.
16. Llach F, Yudd M. Paricalcitol in dialysis patients withcalcitriol-resistant secondary hyperparathyroidism. Am JKidney Dis 2001;38:S45-50.
17. Lazar E, Hebert K, Poma T, Stankus N. Long-term outcomesof cinacalcet and paricalcitol titration protocol for treat-ment of secondary hyperparathyroidism. Am J Nephrol2007;27:274-8.
18. Fukagawa M, Taniguchi M. Can calcimimetics inhibit nodu-lar hyperplasia of parathyroid glands? Nephrol Dial Trans-plant 2008;23:407-8.
19. Ure~na P, Jacobson SH, Zitt E, Vervloet M, Malberti F, Ash-man N, et al. Cinacalcet and achievement of the NKF/K-DOQI recommended target values for bone and mineralmetabolism in real-world clinical practice--the ECHO obser-vational study. Nephrol Dial Transplant 2009;24:2852-9.
20. Hirai T, Nakashima A, Takasugi N, Yorioka N. Response ofsecondary hyperparathyroidism to cinacalcet depends onparathyroid size. Nephron Clin Pract 2010;114:c187-93.
21. Kakuta T, Tanaka R, Kanai G, Sawaya A, Hirukawa T, Sato A,et al. Can cinacalcet replace parathyroid intervention in se-vere secondary hyperparathyroidism? Ther Apher Dial2009;13(Suppl 1):S20-7.
22. National Institute for Health and Clinical Excellence.Understanding NICE guidance. Information for peoplewho use NHS services Cinacalcet for treating secondaryhyperparathyroidism in people with kidney disease whoare on dialysis. January 2007. Available at: http://www.nice.org.uk/nicemedia/pdf/TA117publicinfo.pdf.
23. Narayan R, Perkins RM, Berbano EP, Yuan CM, Neff RT,Sawyers ES, et al. Parathyroidectomy versus cinacalcethydrochloride-based medical therapy in the managementof hyperparathyroidism in ESRD: a cost utility analysis.Am J Kidney Dis 2007;49:801-13.
24. GarsideR, PittM, AndersonR,Mealing S, D’SouzaR, SteinK.Thecost-utility of cinacalcet in addition to standardcare com-pared to standard care alone for secondary hyperparathy-roidism in end-stage renal disease: a UK perspective.Nephrol Dial Transplant 2007;22:1428-36.