An effective primary health care as the bedrock of a healthy nation: wither Nigeria? Dr. MC Asuzu (Professor of Public Health & Community Medicine, COM, UI, Ibadan) (Consultant Clinical Epidemiologist, Community & Occupational Physician, UCH, Ibadan) (President, Society for Public Health Professionals of Nigeria, SPHPN) Dept. of Community Medicine, College of Medicine, University of Ibadan, University College Hospital, Ibadan. Nigeria. (Being a keynote address at the inaugural conference of AMOHN at Ikeja, Lagos. 6/11/14)
Transcript
An effective primary health care as the bedrock of a healthy nation:
wither Nigeria?
Dr. MC Asuzu(Professor of Public Health & Community Medicine, COM, UI, Ibadan)
(Consultant Clinical Epidemiologist, Community & Occupational Physician, UCH, Ibadan)(President, Society for Public Health Professionals of Nigeria, SPHPN)
Dept. of Community Medicine,College of Medicine, University of Ibadan,
University College Hospital,Ibadan. Nigeria.
(Being a keynote address at the inaugural conference of AMOHN at Ikeja, Lagos. 6/11/14)
Order of presentation
• Gratitude to God for this event & to those who invited me
• The premise of this lecture, its appropriateness and history to date
• Our colonial heritage in this regard• Where we are now with it all• What we must do if we are to be serious with
ourselves in these regards• Some concluding remarks
Opening and gratitudes
• Gratitude to God for such an auspicious event• Gratitude to those who invited me• Why this event is about the most auspicious
event of my entire professional life – travel through neurosurgery, etc, to DPH/CM & to this!
• Auspicious Lagos colony, Lagos State, Ebola and now today for this event that will be a watershed in the history of modern PH, CM, CH, MOH & PHC/HFA in Nigeria!
The premise of this lecture
• Alma-Ata, PHC, HFA and their 5 antecedents• 1986, 1988, the Riga conference and its
clarifications and finalistic assertions; after?• Recall of PHC 6 principal and subsidiary
principles; totality and 8 minimum service components; and the nature of the training, organization, functions & leadership necessary to achieve it; else we deceive ourselves
Our colonial legacies in DPH & after• 1897, 1925, 1958, 1960/63/66 and our colonial
and immediate post colonial heritages and practices of Statutory PH/CM/CH; Strachan, Oluwole & Salami, etc. Manuwa…Otolorin.
• 1970, 1975/80 and following in relation with DPH, CM/H and PHC to date.
• Contrast DPH & CM/H in the UK from social reformers and people-serving politicians up to its final origin from within the profession(s) & the immediate problems thereafter to date
• Best practices of DPH/CM&H & PHC in the best practices
Self created problems & growing
• Stunted and decaying MOH and now dead Surgeon-General practices and culture; and the JOHESU & other aftermaths
• Destroyed school health services• Battle-ground environmental health issues• 8th principal principle of PHC only partially and
largely wrongly applied in regard of auxiliaries in spite of the obvious good intentions
• The mysterious Ebola blessing to wake us up from our slumber
What states desiring PHC/HFA must do• Establish the office of MOH for all the LGAs, train
and learn how to administer them properly.• Establish the offices of the district and zone
community nurse-midwives, train and learn how to administer them properly.
• Learn the proper nature of the medical and health practices and their teams & assist to have them run well, with all the adequate provisions thereof
• Lend a voice & hands in the national reforms that are needed in these regards
For Lagos State in particular• Know your history and place as the pace-setter
for DPH, CM&H and MOH in the country• Learn of your place as the only proven capable
federating state/unit in this country and be humbly proud and self sustaining thereof.
• Recognize the new-age fresh leadership that you have again started to show in this regard with the Ebola disease and its immediate aftermath.
• Learn how you may advance in these regards and endeavour to do so
Sir. (Dr.) Samuel A Manuwa as Nigeria’s first indigenous “Surgeon-General” (I-GM&HS)
Community Nursing-midwifery in Rewa Medical division of Fiji, 1999.
Station District or zone PopulationCentral/Hq Medical & Health District (1)Nausori Health Centre Naulu Nursing Station Baulevu Nursing StationNamara Nursing Station Wainibokasi Medical & Health District (2)Wainibokasi Hospital (later CHC) Naililili Nursing Station Mokani Medical & Health District (3)Mokani Health Centre
Nausori ZoneKuku ZoneNageledamu ZoneDavuilevu ZoneZawani ZoneWainibuku DistrictNaulu DistrictBaulevu DistrictNamara District Wainibokasi ZoneNavaka ZoneNaililili District
Luvuluvu ZoneMokani Zone
531352125037680951036519467144753549 506133783644
48253889
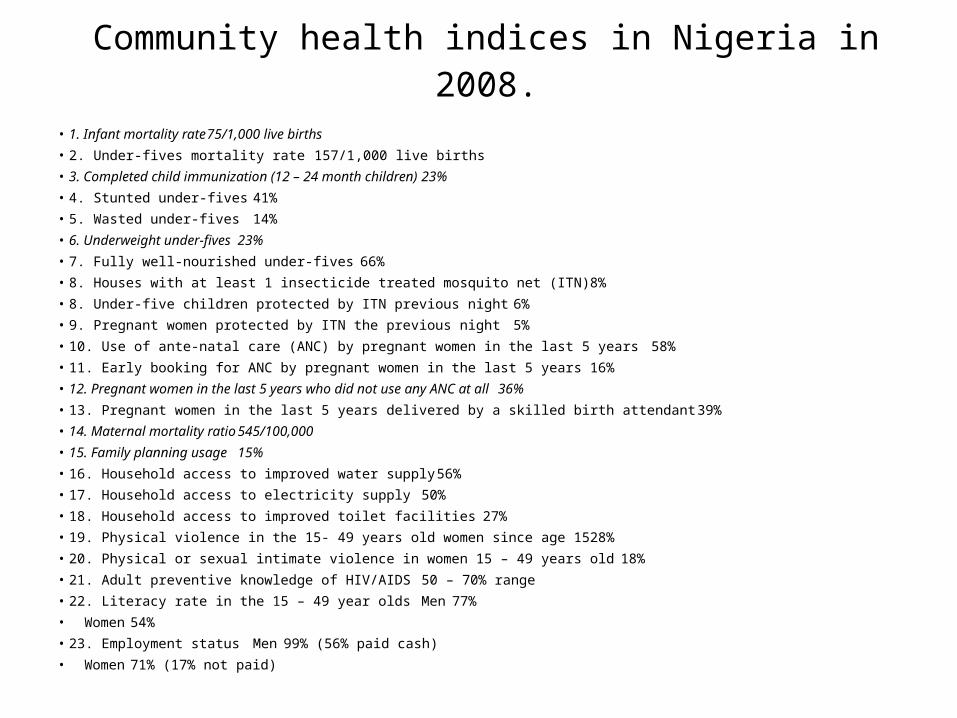
Community health indices in Nigeria in 2008.• 1. Infant mortality rate 75/1,000 live births• 2. Under-fives mortality rate 157/1,000 live births• 3. Completed child immunization (12 – 24 month children) 23%• 4. Stunted under-fives 41%• 5. Wasted under-fives 14%• 6. Underweight under-fives 23%• 7. Fully well-nourished under-fives 66%• 8. Houses with at least 1 insecticide treated mosquito net (ITN) 8%• 8. Under-five children protected by ITN previous night 6%• 9. Pregnant women protected by ITN the previous night 5%• 10. Use of ante-natal care (ANC) by pregnant women in the last 5 years 58%• 11. Early booking for ANC by pregnant women in the last 5 years 16%• 12. Pregnant women in the last 5 years who did not use any ANC at all 36%• 13. Pregnant women in the last 5 years delivered by a skilled birth attendant 39%• 14. Maternal mortality ratio 545/100,000• 15. Family planning usage 15%• 16. Household access to improved water supply 56%• 17. Household access to electricity supply 50%• 18. Household access to improved toilet facilities 27%• 19. Physical violence in the 15- 49 years old women since age 15 28%• 20. Physical or sexual intimate violence in women 15 – 49 years old 18%• 21. Adult preventive knowledge of HIV/AIDS 50 – 70% range• 22. Literacy rate in the 15 – 49 year olds Men 77%• Women 54%• 23. Employment status Men 99% (56% paid cash)• Women 71% (17% not paid)
Community health indices in Fiji in 1998• 1. Crude death rate 16/1,000• 2. Crude death rate 4/1,000• 3. Infant Mortality rate 11/1,000• 4. Maternal mortality rate <1/1,000• 5. Immunization rate – BCG/Polio O 99%• - DPT 3 96%• - HIB 3 85%• - Measles 88%• 6. Under-5s weight below 3rd percentile of normal 5%• 7. Contraceptive prevalence rate 37% of CBA• 8. Percentage of villages with own VHWs 11%• 9. Villages with self-owned dispensaries 37%• 10. Non-indigenous settlements with self-owned dispensaries 16%• 11. Villages with health committees 48%• 12. Communities with adequate water supply 76%• 13. Communities with adequate sewage disposal 77%• 14. Mean mosquito [premises] larval index 23%