1 Abstract of dissertation entitled “An evidence-based protocol of gum chewing in preventing postoperative paralytic ileus in adult patients after abdominal surgeries” Submitted by Li Fong Ming for the degree of Master of Nursing at The University of Hong Kong in July 2015
Transcript
1
Abstract of dissertation entitled
“An evidence-based protocol of gum chewing in
preventing postoperative paralytic ileus in adult
patients after abdominal surgeries”
Submitted by
Li Fong Ming
for the degree of Master of Nursing
at The University of Hong Kong
in July 2015
2
Postoperative paralytic ileus is a very common complication following
with abdominal surgeries. It has been affecting a lot of patients in the local
setting. It is also a difficult situation for the health care providers.
In many studies, the use of chewing gum has been shown to be an
effective method for the prevention of postoperative ileus. It is significant in
helping patients to resume their bowel function in an easy and harmless way. It
is hopeful that this innovation can help more patients in the local setting.
In this regard, this translational research aims at developing an evidence-
based protocol on using chewing gum in the prevention of postoperative
paralytic ileus for adult patients after abdominal surgeries. A systematic search
for relevant literatures was performed with the use of three electronic
databases. Five relevant studies were found. Critical appraisal on the relevant
studies was conducted. The level of evidence extracted from the studies was
graded according to the Scottish Intercollegiate Guidelines Network (SIGN) and
were synthesized to establish the protocol for patients in the proposed setting.
The implementation potential of the protocol was assessed in terms of the
transferability, feasibility, and cost benefit ratio. An implementation and
evaluation plan was established for comprehensive evidenced-based protocol
development.
The successful implementation of the protocol will be beneficial for the
patients undergoing abdominal surgeries as it may prevent them from ileus,
minimizing their suffering and hasten their recovery.
3
“An evidence-based protocol of gum chewing in
preventing postoperative paralytic ileus in adult
patients after abdominal surgeries”
by
Li Fong Ming
B. Nurs. H. K. U.
A dissertation submitted in partial fulfillment of the requirements for
the Degree of Master of Nursing
at The University of Hong Kong
July 2015
4
Declaration
I declare that this thesis represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a
thesis, dissertation on report submitted to this University or to any other
institution for a degree, diploma or other qualification.
Signed
Li Fong Ming
5
Acknowledgement
I would like to express my sincere gratitude towards Dr. William Li, my
dissertation supervisor, for his professional advice and unreserved support in
helping me to complete this dissertation. I would also like to thank the teachers
in this master study that enlightened my vision for the future.
I would also grateful to my family, friends, classmates and my fellow
colleagues who shared my happiness and encouraged me throughout my whole
Among all review studies, they record the time from the time patient return from
recovery room until their first bowel sound heard. The time record is measured in
terms of hour. Comparison between control group (CG) and intervention
group (IG) were made. All resulted in a shorter time in the intervention group for
the first bowel sound. The shorter mean time of IG from the five studies varies
from 3.92 (24.3%)hours to 26.2 (29.3%)hours. After analysis, the protocol will
be regarded as successful if the patients under the chewing gum protocol have
25% faster in time for first bowel sound compared with patients without
chewing gum treatment.
Time of postoperative first flatus
In the review studies, the time reported from patients under chewing gum
protocol for their first flatus is commonly faster than patients with normal
practice. The shorter mean time of IG from the five studies varies from 6.07
(18.8%) hours to 14.8 (18.5%)hours. After analysis, the protocol will be regarded
as successful if the patients under the chewing gum protocol have 18%
45
faster in time for first flatus compared with patients without chewing gum
treatment.
Satisfaction level of patients and healthcare provider
All numeric data will be collected and analyzed with SD and mean.
Comments from the last question of both set of questionnaire will be remarked
for discussion during meeting. It is expected that over 75% of patients and
healthcare providers are satisfactory to the chewing gum protocol.
46
Chapter 8: Conclusion
Conclusion
The chewing gum protocol is feasible and transferable. It is harmless with
low cost. It is a noninvasive, which is favorable for patients with postoperative
ileus (POI). Although there is still data showing not all patients receive effect
from it, it brings no complication. It is worth to apply the protocol so as to
reduce POI in patients.
Establishing the chewing gum protocol can help patients, health care staff
and also the medical system. There is not much extra skill and workload for staff.
There is not much expenditure for the medical system as well. However, it brings
much more comfort and recovery to patients. By fine-tuning the protocol from
time to time, it is believed that the chewing gum protocol will be considered as
an easy prevention for POI.
47
Appendix
48
Appendix 1: Table of evidence Citation/
Study Design/
Country of study
Evidence level
Subject Characteristics
Intervention
Control
Outcomes
measures/Length of follow up
Effect size
Interpretation
Ertas (2013) Influence of gum chewing on postoperative bowel activity after complete staging surgery for gynecological malignancies: A randomized controlled trail, Gynecologic oncology 131 (2013) 118-122
• RCT • Turkey
1(+) • n=152 • Mean age=
52.05
Standard normal care
Began chewing gum on postop D1 and chew gum three times daily. Each chewing lasts 30min.
Standard normal care
1. Time to first bowel movement (h)
2. Postop first flatus time (h)
Length of FU
Period from the end of surgery until the time patient has bowel sound return.
1. The mean time to bowel movement in IG is 8.6 (h) faster than CG.
2. The mean time of first flatus in IG is 9.6 (h) faster than CG.
Gum chewing early in the postoperative period following elective total abdominal hysterectomy and systematic retroperitoneal lymphadenectomy hastens time to bowel motility.
Footnote: h=hours; IG=intervention group; CG=control group
49
Citation/ Study
Design/ Country of
study
Evidence level
Subject Characteristics
Intervention
Control
Outcomes
measures/Length of follow up
Effect size
Interpretation
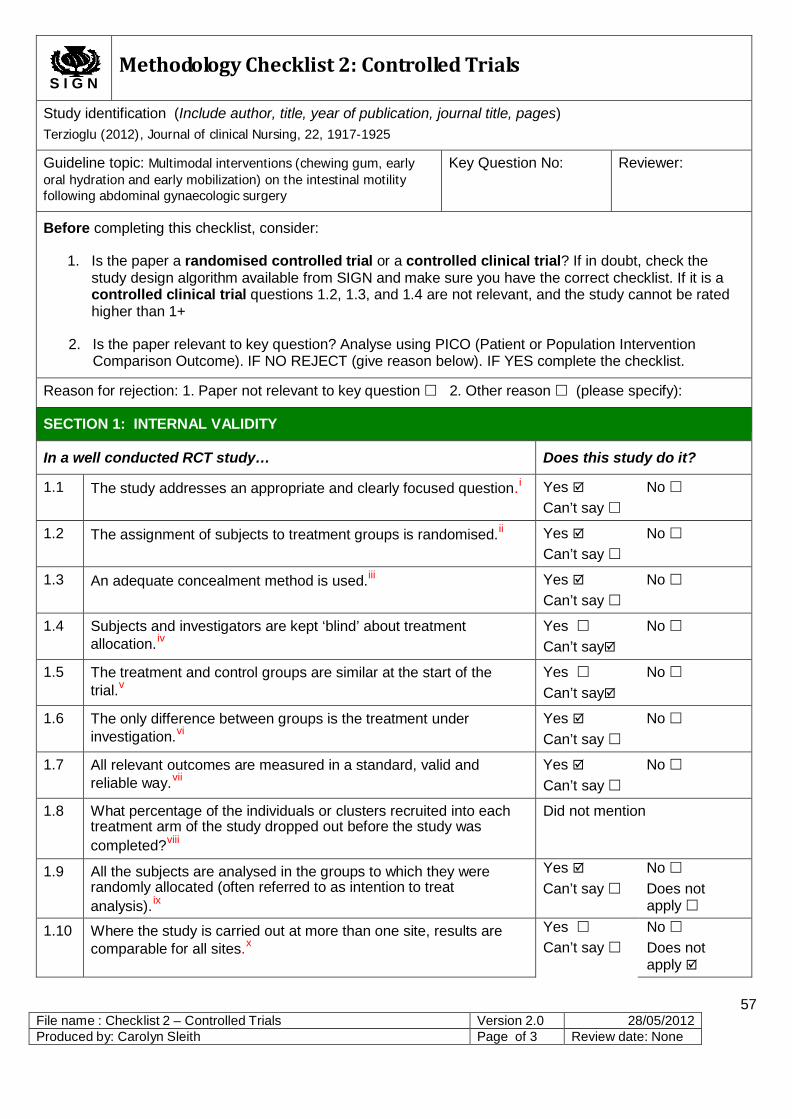
Terzioglu (2012) Multimodal interventions (chewing gum, early oral hydration and early mobilization) on the intestinal motility following abdominal gynaecologic surgery, Journal of clinical Nursing, 22, 1917-1925
• RCT • Turkey
1(+) • n=60 • Aged 50 or
below= 73.3%; aged 51 or above= 26.7%
Standard normal care
Chewing sugarless gum for a period of 15minutes once every 2 hours after the operation, which was ceased between 00:00 and 08:00.
Standard normal care
1. Time of first bowel sound (h)
2. Time of first passage of flatus (h)
Length of FU
Period from the end of surgery until the time patient has bowel sound return.
1. The mean time of first bowel sound in IG is 3.92 (h) faster than CG.
2. The mean time of first flatus in IG is 6.07(h) faster than CG.
Chewing gum is an effective method in preventing paralytic ileus after gynaecological surgeries with significant improvement in patients’ comfort.
Footnote: h=hours; IG=intervention group; CG=control group
50
Citation/ Study
Design/ Country of
study
Evidence level
Subject Characteristics
Intervention
Control
Outcomes
measures/Length of follow up
Effect size
Interpretation
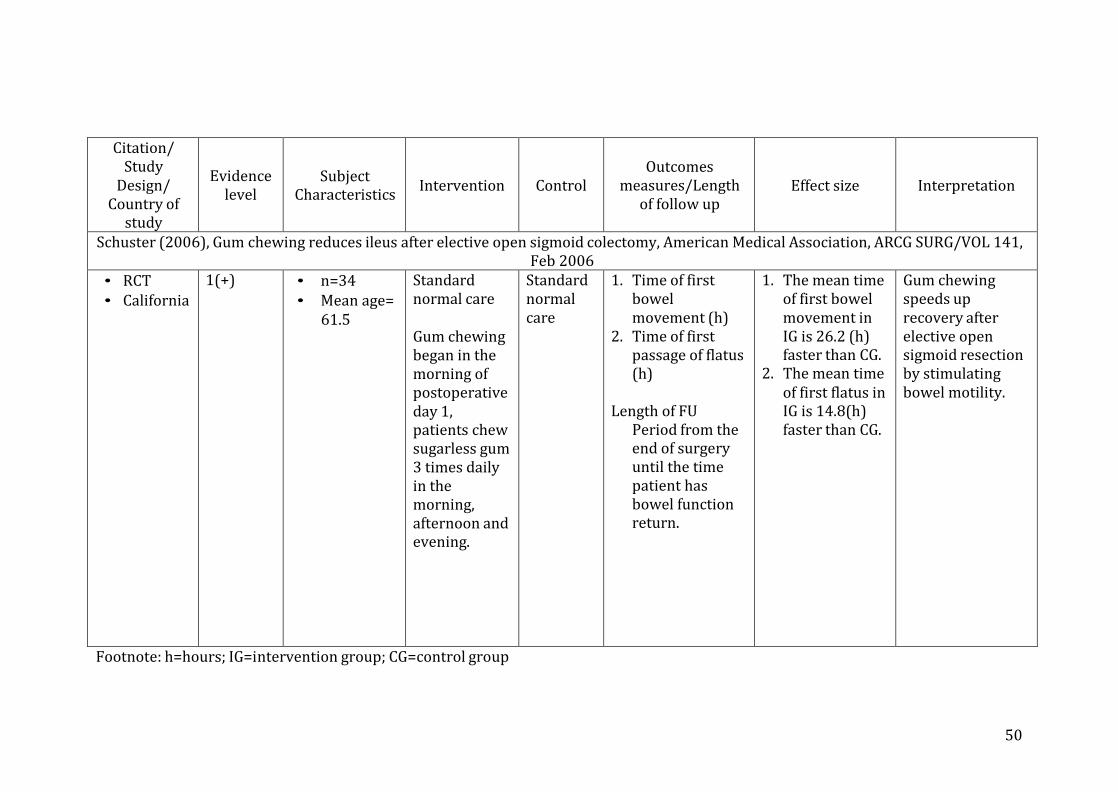
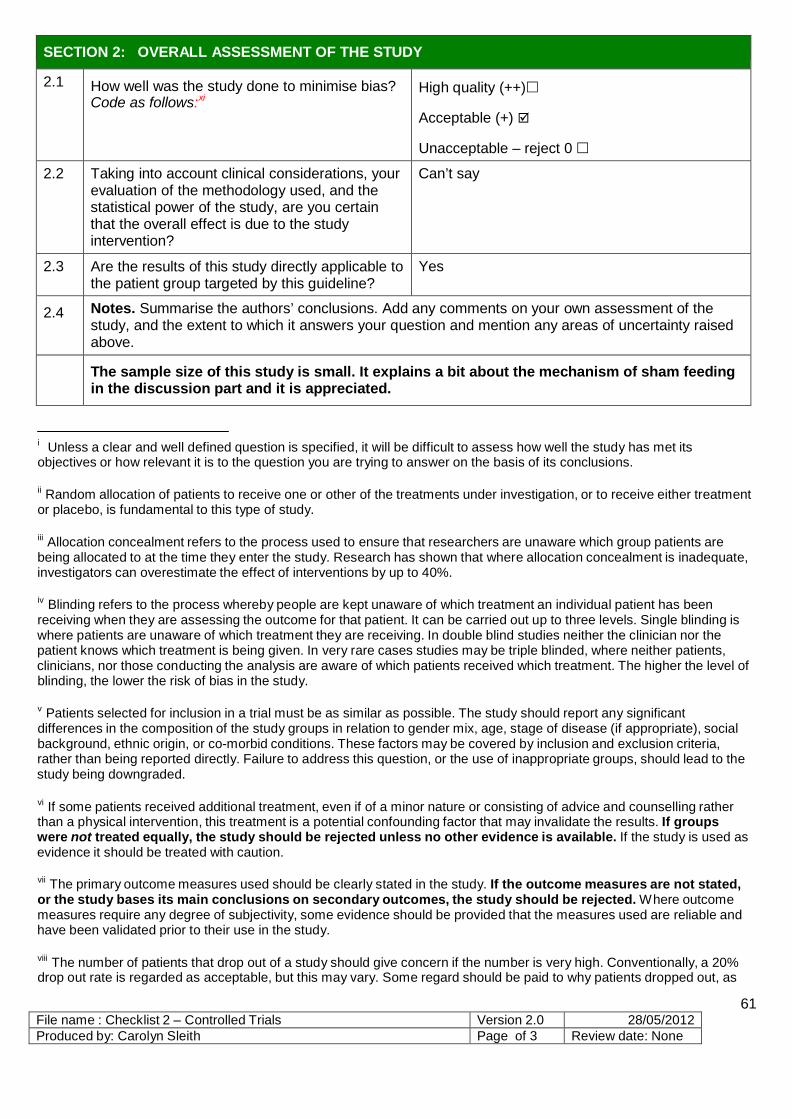
Schuster (2006), Gum chewing reduces ileus after elective open sigmoid colectomy, American Medical Association, ARCG SURG/VOL 141, Feb 2006
• RCT • California
1(+) • n=34 • Mean age=
61.5
Standard normal care
Gum chewing began in the morning of postoperative day 1, patients chew sugarless gum 3 times daily in the morning, afternoon and evening.
Standard normal care
1. Time of first bowel movement (h)
2. Time of first passage of flatus (h)
Length of FU
Period from the end of surgery until the time patient has bowel function return.
1. The mean time of first bowel movement in IG is 26.2 (h) faster than CG.
2. The mean time of first flatus in IG is 14.8(h) faster than CG.
Gum chewing speeds up recovery after elective open sigmoid resection by stimulating bowel motility.
Footnote: h=hours; IG=intervention group; CG=control group
51
Citation/ Study
Design/ Country of
study
Evidence level
Subject Characteristics
Intervention
Control
Outcomes
measures/Length of follow up
Effect size
Interpretation
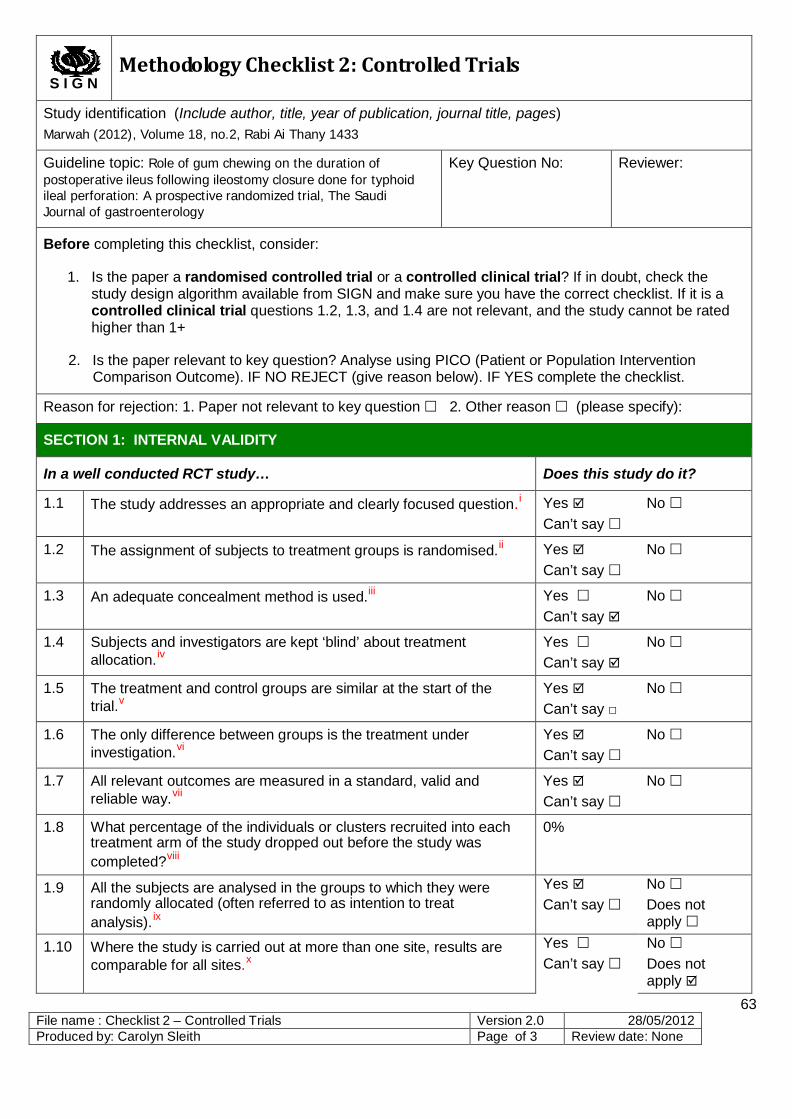
Marwah (2012), Role of gum chewing on the duration of postoperative ileus following ileostomy closure done for typhoid ileal perforation: A prospective randomized trial, The Saudi Journal of gastroenterology, Volume 18, no.2, Rabi Ai Thany 1433
• RCT • India
1(+) • n=100 • Mean age=
38.42
Standard normal care
To chew sugar-free gum 3 times per day for 1 hour each time, starting from 6 hours after the surgery until the passage of first flatus.
Standard normal care
1. Time of first bowel sound (h)
2. Time of first passage of flatus (h)
Length of FU
Period from the end of surgery until the time patient has bowel sound return.
1. The mean time of first bowel sound in IG is 7.92(h) faster than CG.
2. The mean time of first flatus in IG is 14.64(h) faster than CG.
Gum chewing shows significance in reducing the duration of POI after laparotomy for ileostomy closure, which was done for typhoid perforation peritonitis.
Footnote: h=hours; IG=intervention group; CG=control group
52
Citation/ Study
Design/ Country of
study
Evidence level
Subject Characteristics
Intervention
Control
Outcomes
measures/Length of follow up
Effect size
Interpretation
Chol (2011) Chewing gum has a stimulatory effect on bowel motility in patients after open or robotic radical cystectomy for bladder cancer: A prospective randomized comparative study, Urology. 2011 Apr;77(4):884-90. doi: 10.1016
• RCT • Korea
1(+) • n=64 • Mean age= 64
Standard normal care
To chew sugar-free gum 3 times per day for 30min each time until the passage of first flatus.
Standard normal care
1. Time of first bowel sound (h)
2. Time of first passage of flatus (h)
Length of FU
Period from the end of surgery until the time patient has bowel sound return.
1. The mean time of first bowel sound in IG is 16.6 (h) faster than CG.
2. The mean time of first flatus in IG is 12.4 (h) faster than CG.
Chewing gum has stimulatory effects on bowel motility after cystectomy and urinary diversion. It is safe and could be used for postoperative ileus.
Footnote: h=hours; IG=intervention group; CG=control group
Appendix 2 SIGN Checklist
2.1 Ertas (2013), Gynecologic oncology 131 (2013) 118-122 2.2 Terzioglu (2012), Journal of clinical Nursing, 22, 1917-1925 2.3 Schuster (2006), American Medical Association, ARCG SURG/VOL 141, Feb 2006 2.4 Marwah (2012), Volume 18, no.2, Rabi Ai Thany 1433 2.5 Hoon Chol, (2011) Urology 2011 Apr;77(4):884-90. doi: 10.1016
53
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages) Ertas (2013), Gynecologic oncology 131 (2013) 118-122
Guideline topic: Influence of gum chewing on postoperative bowel activity after complete staging surgery for gynecological malignancies: A randomized controlled trail
Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study…
Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i Yes No
Can’t say
1.2 The assignment of subjects to treatment groups is randomised.ii Yes No Can’t say
1.3 An adequate concealment method is used.iii Yes No Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation.iv
Yes No Can’t say
1.5 The treatment and control groups are similar at the start of the trial.v
Yes No Can’t say □
1.6 The only difference between groups is the treatment under investigation.vi
Yes No Can’t say
1.7 All relevant outcomes are measured in a standard, valid and reliable way.vii
Yes No Can’t say
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?viii
1.97%
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).ix
Yes No Can’t say Does not
apply
1.10 Where the study is carried out at more than one site, results are comparable for all sites.x
Yes Can’t say
No Does not apply
54
File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1
How well was the study done to minimise bias? Code as follows:xi
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Can’t say
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
There is significant different difference between IG and CG. The patients are not blind but it is blind to the assessors. It may be possible to make it blind to patients in this study as well.
i Unless a clear and well defined question is specified, it will be difficult to assess how well the study has met its objectives or how relevant it is to the question you are trying to answer on the basis of its conclusions.
ii Random allocation of patients to receive one or other of the treatments under investigation, or to receive either treatment or placebo, is fundamental to this type of study.
iii Allocation concealment refers to the process used to ensure that researchers are unaware which group patients are being allocated to at the time they enter the study. Research has shown that where allocation concealment is inadequate, investigators can overestimate the effect of interventions by up to 40%.
iv Blinding refers to the process whereby people are kept unaware of which treatment an individual patient has been receiving when they are assessing the outcome for that patient. It can be carried out up to three levels. Single blinding is where patients are unaware of which treatment they are receiving. In double blind studies neither the clinician nor the patient knows which treatment is being given. In very rare cases studies may be triple blinded, where neither patients, clinicians, nor those conducting the analysis are aware of which patients received which treatment. The higher the level of blinding, the lower the risk of bias in the study.
v Patients selected for inclusion in a trial must be as similar as possible. The study should report any significant differences in the composition of the study groups in relation to gender mix, age, stage of disease (if appropriate), social background, ethnic origin, or co-morbid conditions. These factors may be covered by inclusion and exclusion criteria, rather than being reported directly. Failure to address this question, or the use of inappropriate groups, should lead to the study being downgraded.
vi If some patients received additional treatment, even if of a minor nature or consisting of advice and counselling rather than a physical intervention, this treatment is a potential confounding factor that may invalidate the results. If groups were not treated equally, the study should be rejected unless no other evidence is available. If the study is used as evidence it should be treated with caution.
vii The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
viii The number of patients that drop out of a study should give concern if the number is very high. Conventionally, a 20% drop out rate is regarded as acceptable, but this may vary. Some regard should be paid to why patients dropped out, as
55 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
well as how many. It should be noted that the drop out rate may be expected to be higher in studies conducted over a long period of time. A higher drop out rate will normally lead to downgrading, rather than rejection of a study.
ix In practice, it is rarely the case that all patients allocated to the intervention group receive the intervention throughout the trial, or that all those in the comparison group do not. Patients may refuse treatment, or contra-indications arise that lead them to be switched to the other group. If the comparability of groups through randomisation is to be maintained, however, patient outcomes must be analysed according to the group to which they were originally allocated irrespective of the treatment they actually received. (This is known as intention to treat analysis.) If it is clear that analysis was not on an intention to treat basis, the study may be rejected. If there is little other evidence available, the study may be included but should be evaluated as if it were a non-randomised cohort study.
x In multi-site studies, confidence in the results should be increased if it can be shown that similar results were obtained at the different participating centres.
xi Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias, Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
56 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages) Terzioglu (2012), Journal of clinical Nursing, 22, 1917-1925
Guideline topic: Multimodal interventions (chewing gum, early oral hydration and early mobilization) on the intestinal motility following abdominal gynaecologic surgery
Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study…
Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i Yes No
Can’t say
1.2 The assignment of subjects to treatment groups is randomised.ii Yes No
Can’t say
1.3 An adequate concealment method is used.iii Yes No Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation.iv
Yes No Can’t say
1.5 The treatment and control groups are similar at the start of the trial.v
Yes No Can’t say
1.6 The only difference between groups is the treatment under investigation.vi
Yes No Can’t say
1.7 All relevant outcomes are measured in a standard, valid and reliable way.vii
Yes No Can’t say
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?viii
Did not mention
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).ix
Yes No Can’t say Does not
apply
1.10 Where the study is carried out at more than one site, results are comparable for all sites.x
Yes Can’t say
No Does not apply
57
File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1
How well was the study done to minimise bias? Code as follows:xi
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Can’t say
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
Chewing gum may have its optimal effectiveness in preventing POI when using together with other intervention such as early oral hydration and early mobilization. Drop out rate from this study should be mentioned.
i Unless a clear and well defined question is specified, it will be difficult to assess how well the study has met its objectives or how relevant it is to the question you are trying to answer on the basis of its conclusions.
ii Random allocation of patients to receive one or other of the treatments under investigation, or to receive either treatment or placebo, is fundamental to this type of study.
iii Allocation concealment refers to the process used to ensure that researchers are unaware which group patients are being allocated to at the time they enter the study. Research has shown that where allocation concealment is inadequate, investigators can overestimate the effect of interventions by up to 40%.
iv Blinding refers to the process whereby people are kept unaware of which treatment an individual patient has been receiving when they are assessing the outcome for that patient. It can be carried out up to three levels. Single blinding is where patients are unaware of which treatment they are receiving. In double blind studies neither the clinician nor the patient knows which treatment is being given. In very rare cases studies may be triple blinded, where neither patients, clinicians, nor those conducting the analysis are aware of which patients received which treatment. The higher the level of blinding, the lower the risk of bias in the study.
v Patients selected for inclusion in a trial must be as similar as possible. The study should report any significant differences in the composition of the study groups in relation to gender mix, age, stage of disease (if appropriate), social background, ethnic origin, or co-morbid conditions. These factors may be covered by inclusion and exclusion criteria, rather than being reported directly. Failure to address this question, or the use of inappropriate groups, should lead to the study being downgraded.
vi If some patients received additional treatment, even if of a minor nature or consisting of advice and counselling rather than a physical intervention, this treatment is a potential confounding factor that may invalidate the results. If groups were not treated equally, the study should be rejected unless no other evidence is available. If the study is used as evidence it should be treated with caution.
vii The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
58 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
viii The number of patients that drop out of a study should give concern if the number is very high. Conventionally, a 20% drop out rate is regarded as acceptable, but this may vary. Some regard should be paid to why patients dropped out, as well as how many. It should be noted that the drop out rate may be expected to be higher in studies conducted over a long period of time. A higher drop out rate will normally lead to downgrading, rather than rejection of a study.
ix In practice, it is rarely the case that all patients allocated to the intervention group receive the intervention throughout the trial, or that all those in the comparison group do not. Patients may refuse treatment, or contra-indications arise that lead them to be switched to the other group. If the comparability of groups through randomisation is to be maintained, however, patient outcomes must be analysed according to the group to which they were originally allocated irrespective of the treatment they actually received. (This is known as intention to treat analysis.) If it is clear that analysis was not on an intention to treat basis, the study may be rejected. If there is little other evidence available, the study may be included but should be evaluated as if it were a non-randomised cohort study.
x In multi-site studies, confidence in the results should be increased if it can be shown that similar results were obtained at the different participating centres.
xi Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias, Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
59 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages) Schuster (2006), American Medical Association, ARCG SURG/VOL 141, Feb 2006
Guideline topic: Gum chewing reduces ileus after elective open sigmoid colectomy
Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study…
Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i Yes No
Can’t say
1.2 The assignment of subjects to treatment groups is randomised.ii Yes No
Can’t say
1.3 An adequate concealment method is used.iii Yes No Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation.iv
Yes No Can’t say
1.5 The treatment and control groups are similar at the start of the trial.v
Yes No Can’t say □
1.6 The only difference between groups is the treatment under investigation.vi
Yes No Can’t say
1.7 All relevant outcomes are measured in a standard, valid and reliable way.vii
Yes No Can’t say
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?viii
0%
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).ix
Yes No Can’t say Does not
apply
1.10 Where the study is carried out at more than one site, results are comparable for all sites.x
Yes Can’t say
No Does not apply
60 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1
How well was the study done to minimise bias? Code as follows:xi
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Can’t say
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The sample size of this study is small. It explains a bit about the mechanism of sham feeding in the discussion part and it is appreciated.
i Unless a clear and well defined question is specified, it will be difficult to assess how well the study has met its objectives or how relevant it is to the question you are trying to answer on the basis of its conclusions.
ii Random allocation of patients to receive one or other of the treatments under investigation, or to receive either treatment or placebo, is fundamental to this type of study.
iii Allocation concealment refers to the process used to ensure that researchers are unaware which group patients are being allocated to at the time they enter the study. Research has shown that where allocation concealment is inadequate, investigators can overestimate the effect of interventions by up to 40%.
iv Blinding refers to the process whereby people are kept unaware of which treatment an individual patient has been receiving when they are assessing the outcome for that patient. It can be carried out up to three levels. Single blinding is where patients are unaware of which treatment they are receiving. In double blind studies neither the clinician nor the patient knows which treatment is being given. In very rare cases studies may be triple blinded, where neither patients, clinicians, nor those conducting the analysis are aware of which patients received which treatment. The higher the level of blinding, the lower the risk of bias in the study.
v Patients selected for inclusion in a trial must be as similar as possible. The study should report any significant differences in the composition of the study groups in relation to gender mix, age, stage of disease (if appropriate), social background, ethnic origin, or co-morbid conditions. These factors may be covered by inclusion and exclusion criteria, rather than being reported directly. Failure to address this question, or the use of inappropriate groups, should lead to the study being downgraded.
vi If some patients received additional treatment, even if of a minor nature or consisting of advice and counselling rather than a physical intervention, this treatment is a potential confounding factor that may invalidate the results. If groups were not treated equally, the study should be rejected unless no other evidence is available. If the study is used as evidence it should be treated with caution.
vii The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
viii The number of patients that drop out of a study should give concern if the number is very high. Conventionally, a 20% drop out rate is regarded as acceptable, but this may vary. Some regard should be paid to why patients dropped out, as
61 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
well as how many. It should be noted that the drop out rate may be expected to be higher in studies conducted over a long period of time. A higher drop out rate will normally lead to downgrading, rather than rejection of a study.
ix In practice, it is rarely the case that all patients allocated to the intervention group receive the intervention throughout the trial, or that all those in the comparison group do not. Patients may refuse treatment, or contra-indications arise that lead them to be switched to the other group. If the comparability of groups through randomisation is to be maintained, however, patient outcomes must be analysed according to the group to which they were originally allocated irrespective of the treatment they actually received. (This is known as intention to treat analysis.) If it is clear that analysis was not on an intention to treat basis, the study may be rejected. If there is little other evidence available, the study may be included but should be evaluated as if it were a non-randomised cohort study.
x In multi-site studies, confidence in the results should be increased if it can be shown that similar results were obtained at the different participating centres.
xi Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias, Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
62 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages) Marwah (2012), Volume 18, no.2, Rabi Ai Thany 1433
Guideline topic: Role of gum chewing on the duration of postoperative ileus following ileostomy closure done for typhoid ileal perforation: A prospective randomized trial, The Saudi Journal of gastroenterology
Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study…
Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i Yes No
Can’t say
1.2 The assignment of subjects to treatment groups is randomised.ii Yes No
Can’t say
1.3 An adequate concealment method is used.iii Yes No Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation.iv
Yes No Can’t say
1.5 The treatment and control groups are similar at the start of the trial.v
Yes No Can’t say □
1.6 The only difference between groups is the treatment under investigation.vi
Yes No Can’t say
1.7 All relevant outcomes are measured in a standard, valid and reliable way.vii
Yes No Can’t say
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?viii
0%
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).ix
Yes No Can’t say Does not
apply
1.10 Where the study is carried out at more than one site, results are comparable for all sites.x
Yes Can’t say
No Does not apply
63 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1
How well was the study done to minimise bias? Code as follows:xi
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The blinding is uncertain in this study.
i Unless a clear and well defined question is specified, it will be difficult to assess how well the study has met its objectives or how relevant it is to the question you are trying to answer on the basis of its conclusions.
ii Random allocation of patients to receive one or other of the treatments under investigation, or to receive either treatment or placebo, is fundamental to this type of study.
iii Allocation concealment refers to the process used to ensure that researchers are unaware which group patients are being allocated to at the time they enter the study. Research has shown that where allocation concealment is inadequate, investigators can overestimate the effect of interventions by up to 40%.
iv Blinding refers to the process whereby people are kept unaware of which treatment an individual patient has been receiving when they are assessing the outcome for that patient. It can be carried out up to three levels. Single blinding is where patients are unaware of which treatment they are receiving. In double blind studies neither the clinician nor the patient knows which treatment is being given. In very rare cases studies may be triple blinded, where neither patients, clinicians, nor those conducting the analysis are aware of which patients received which treatment. The higher the level of blinding, the lower the risk of bias in the study.
v Patients selected for inclusion in a trial must be as similar as possible. The study should report any significant differences in the composition of the study groups in relation to gender mix, age, stage of disease (if appropriate), social background, ethnic origin, or co-morbid conditions. These factors may be covered by inclusion and exclusion criteria, rather than being reported directly. Failure to address this question, or the use of inappropriate groups, should lead to the study being downgraded.
vi If some patients received additional treatment, even if of a minor nature or consisting of advice and counselling rather than a physical intervention, this treatment is a potential confounding factor that may invalidate the results. If groups were not treated equally, the study should be rejected unless no other evidence is available. If the study is used as evidence it should be treated with caution.
vii The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
viii The number of patients that drop out of a study should give concern if the number is very high. Conventionally, a 20% drop out rate is regarded as acceptable, but this may vary. Some regard should be paid to why patients dropped out, as
64 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
well as how many. It should be noted that the drop out rate may be expected to be higher in studies conducted over a long period of time. A higher drop out rate will normally lead to downgrading, rather than rejection of a study.
ix In practice, it is rarely the case that all patients allocated to the intervention group receive the intervention throughout the trial, or that all those in the comparison group do not. Patients may refuse treatment, or contra-indications arise that lead them to be switched to the other group. If the comparability of groups through randomisation is to be maintained, however, patient outcomes must be analysed according to the group to which they were originally allocated irrespective of the treatment they actually received. (This is known as intention to treat analysis.) If it is clear that analysis was not on an intention to treat basis, the study may be rejected. If there is little other evidence available, the study may be included but should be evaluated as if it were a non-randomised cohort study.
x In multi-site studies, confidence in the results should be increased if it can be shown that similar results were obtained at the different participating centres.
xi Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias, Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
65 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages) Hoon Chol, (2011) Urology 2011 Apr;77(4):884-90. doi: 10.1016
Guideline topic: Chewing gum has a stimulatory effect on bowel motility in patients after open or robotic radical cystectomy for bladder cancer: A prospective randomized comparative study
Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study…
Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i Yes No
Can’t say
1.2 The assignment of subjects to treatment groups is randomised.ii Yes No
Can’t say
1.3 An adequate concealment method is used.iii Yes No Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation.iv
Yes No Can’t say
1.5 The treatment and control groups are similar at the start of the trial.v
Yes No Can’t say □
1.6 The only difference between groups is the treatment under investigation.vi
Yes No Can’t say
1.7 All relevant outcomes are measured in a standard, valid and reliable way.vii
Yes No Can’t say
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?viii
6.25%
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).ix
Yes No Can’t say Does not
apply
1.10 Where the study is carried out at more than one site, results are comparable for all sites.x
Yes Can’t say
No Does not apply
66
File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1
How well was the study done to minimise bias? Code as follows:xi
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
Blinding is used in subjects but isn’t mentioned to investigators.
i Unless a clear and well defined question is specified, it will be difficult to assess how well the study has met its objectives or how relevant it is to the question you are trying to answer on the basis of its conclusions.
ii Random allocation of patients to receive one or other of the treatments under investigation, or to receive either treatment or placebo, is fundamental to this type of study.
iii Allocation concealment refers to the process used to ensure that researchers are unaware which group patients are being allocated to at the time they enter the study. Research has shown that where allocation concealment is inadequate, investigators can overestimate the effect of interventions by up to 40%.
iv Blinding refers to the process whereby people are kept unaware of which treatment an individual patient has been receiving when they are assessing the outcome for that patient. It can be carried out up to three levels. Single blinding is where patients are unaware of which treatment they are receiving. In double blind studies neither the clinician nor the patient knows which treatment is being given. In very rare cases studies may be triple blinded, where neither patients, clinicians, nor those conducting the analysis are aware of which patients received which treatment. The higher the level of blinding, the lower the risk of bias in the study.
v Patients selected for inclusion in a trial must be as similar as possible. The study should report any significant differences in the composition of the study groups in relation to gender mix, age, stage of disease (if appropriate), social background, ethnic origin, or co-morbid conditions. These factors may be covered by inclusion and exclusion criteria, rather than being reported directly. Failure to address this question, or the use of inappropriate groups, should lead to the study being downgraded.
vi If some patients received additional treatment, even if of a minor nature or consisting of advice and counselling rather than a physical intervention, this treatment is a potential confounding factor that may invalidate the results. If groups were not treated equally, the study should be rejected unless no other evidence is available. If the study is used as evidence it should be treated with caution.
vii The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
viii The number of patients that drop out of a study should give concern if the number is very high. Conventionally, a 20% drop out rate is regarded as acceptable, but this may vary. Some regard should be paid to why patients dropped out, as
67 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
well as how many. It should be noted that the drop out rate may be expected to be higher in studies conducted over a long period of time. A higher drop out rate will normally lead to downgrading, rather than rejection of a study.
ix In practice, it is rarely the case that all patients allocated to the intervention group receive the intervention throughout the trial, or that all those in the comparison group do not. Patients may refuse treatment, or contra-indications arise that lead them to be switched to the other group. If the comparability of groups through randomisation is to be maintained, however, patient outcomes must be analysed according to the group to which they were originally allocated irrespective of the treatment they actually received. (This is known as intention to treat analysis.) If it is clear that analysis was not on an intention to treat basis, the study may be rejected. If there is little other evidence available, the study may be included but should be evaluated as if it were a non-randomised cohort study.
x In multi-site studies, confidence in the results should be increased if it can be shown that similar results were obtained at the different participating centres.
xi Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias, Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
68 File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012 Produced by: Carolyn Sleith Page of 3 Review date: None
69
Appendix 3 Search history (Last search in May 2014)
PubMed (# Of citation)
CINAHL (# Of citation)
Mosby’s Nursing consult (# Of citation)
After keyword search (chewing gum + postoperative ileus)
61
23
11
After keyword search (sham feeding + postoperative ileus)
9
25
4
After keyword search (chewing gum + bowel movement)
37
107
19
After keyword search (chewing gum + postoperative care)
38
130
9
Total # of citations from keywords
145
285
43
Total # of citations from all databases: 473
After further screening of titles and abstracts
11
19
12
After reading full text
2
1
3
70
After checking reference
3
1
3
After removing duplicates
3
1
1
Total selected citations: 5
71
Incl
uded
El
igib
ility
Sc
reen
ing
Iden
tific
atio
n
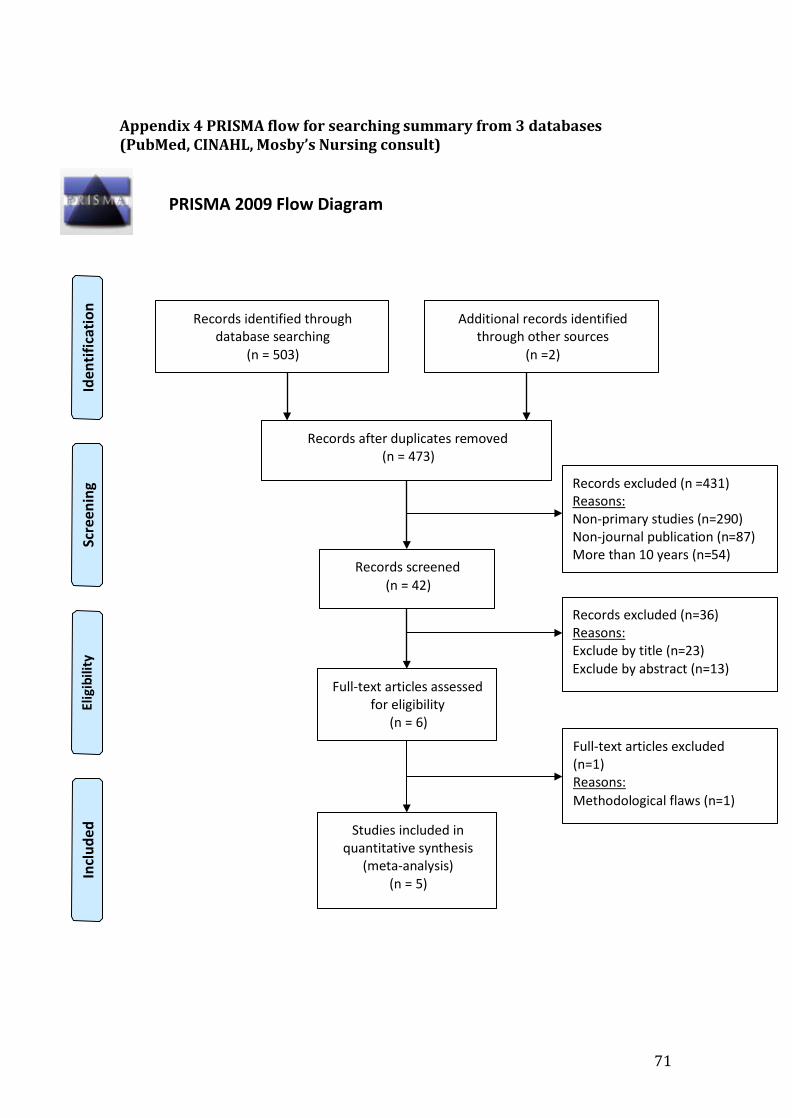
Appendix 4 PRISMA flow for searching summary from 3 databases (PubMed, CINAHL, Mosby’s Nursing consult)
PRISMA 2009 Flow Diagram
Records identified through database searching
(n = 503)
Additional records identified through other sources
(n =2)
Records after duplicates removed (n = 473)
Records screened (n = 42)
Records excluded (n =431) Reasons: Non-primary studies (n=290) Non-journal publication (n=87) More than 10 years (n=54)
Full-text articles assessed for eligibility
(n = 6)
Records excluded (n=36) Reasons: Exclude by title (n=23) Exclude by abstract (n=13) Full-text articles excluded (n=1) Reasons: Methodological flaws (n=1)
Studies included in quantitative synthesis
(meta-analysis) (n = 5)
72
Appendix 5
Time schedule for implementing the innovation
It is estimated that the new innovation will take 58 weeks for implementation and evaluation.
Items
Schedule
Formation of a program committee for the new innovation- the chewing gum
protocol
4 weeks
Planning for the innovation including communication plan
6 weeks
Staff briefing and training
6weeks
Trial running for the program
8 weeks
Implementation period
28 weeks
Evaluation of the programs
6 weeks
73
Appendix 6 Estimated set up cost and operational cost
Estimated set up cost for implementation for 58 weeks Items Calculation Amount
Sugarless gum HKD$ 0.1 x 225 x 15 x 3 HKD$ 1012.5
Stereoscopes HKD$ 25 x 30 (set) HKD$ 750
Staff training HKD$ 300 (hr) x 50 (staff) HKD$ 15,000
Extra staff (registered nurse)
HKD$ 30000 x 1 (staff) x 12.5 (salary of 50 weeks)
HKD$ 375,000
Information pamphlet HKD$ 0.1 x 225 (page) HKD$ 22.5
Total set up cost HKD$ 391,785
Estimated operational cost per month/4 weeks Items Calculation Amount
Sugarless gum HKD$ 0.1 (piece) x 25(patients) x 15 x 3 (basic consumption of gum)
HKD$ 112.5
Staff tutorial class HKD$300 (hr) x 3 (staff) HKD$ 900
patients weekly). 3. 255 patients for 36 weeks of implementation including pilot study test. 4. 15 days is estimated as the maximum time for the treatment per patient
as most patients will not need to exist 15 days of treatment. 5. Each patient consumes 3 gums daily. 6. Expense on extra staff may have minor variation depending on the
individual point of salary.
74
Appendix 7 Key to evidence statements and grades of recommendations by SCOTTISH INTERCOLLEGIATE GUIDELINES NETWORK
LEVEL OF EVIDENCE 1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias 1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias 1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias 2++ High quality systematic reviews of case control or cohort or studies H igh
quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal 2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal 2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal 3 Non-analytic studies, e.g. case reports, case series 4 Expert opinions
GRADES OF RECOMMENDATIONS A- At least one meta-analysis, systematic review, or RCT rated as 1++, and directly applicable to the target population; or A body of evidence consisting principally of studies rated as 1+, directly applicable to the target population, and demonstrating overall consistency of results B- A body of evidence including studies rated as 2++, directly applicable to the target population, and demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 1++ or 1+ C- A body of evidence including studies rated as 2+, directly applicable to the target population and demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 2++ D- Evidence level 3 or 4; or Extrapolated evidence from studies rated as 2+
Good practice points Recommended best practice based on the clinical experience of the guideline development group
Being cooperative in monitoring and reporting of flatus and discomfort
Yield useful data for the chewing gum protocol/ Patients beneficial from the protocol
78
Appendix 11 Guideline of gum chewing in preventing postoperative paralytic ileus in adult patients after abdominal surgeries
1. Objectives 1.1 To provide care for promoting optimal recovery from surgery 1.2 To minimize risk of postoperative paralytic ileus
2. Scope 2.1 The procedure covers all adult patients who aged 18 or above who have undergone abdominal surgery under general anesthesia.
3. Nursing intervention 3.1 Post-operative care day 1 3.1.1 check patient’s conscious level 3.1.2 check patient’s ability in chewing and reporting of flatus and discomfort 3.1.3 Medical officer prescribed chewing gum and nurse administrate it 3.2 Instruct patient to chew without swallowing the gum for 30 minutes 3.3 Observe for abnormality 3.4 Use timer for time control 3.5 Assist patient to discard chewing gum after 30 minutes 3.6 Repeat administrating chewing gum as scheduled for 3 times per day 3.7 Use stereoscope to check patients’ bowel sound hourly 3.8 Document hourly result properly, report if any abnormality 3.9 Provide call bell to patient, allow immediate report of flatus 3.10 Document date and time of first flatus 3.11 Ensure patient safety throughout procedures
4. Evaluation 4.1 Confirm patients’ bowel movement with doctors 4.2 Distributed evaluation form to patients 4.2.1 Provide instruction of filling the evaluation form 4.2.2 Allow privacy and sufficient time for filling form 4.3 Collect evaluation form for later analysis
79
Reference
80
1. Abd-El-Maeboud KH(2009) Gum chewing stimulates early return of bowel
motility after caesarean section. BJOG. 2009 Sep;116(10):1334-9.
2. Antosh DD (2013) A case-control study of risk factors for ileus and bowel
obstruction following benign gynecologic surgery. Int J Gynaecol Obstet.