AN EXAMINATION OF THE RELATIONSHIP BETWEEN STAFF BEHAVIOUR AND STRESS LEVELS IN RESIDENTIAL CARE John Rose South Wales Training Course in Clinical Psychology, Whitchurch Hospital, CardijJ CF4 7XB Ellen Mullan Slade House, Headlington, Oxford Professor Ben (C.) Fletcher The Business School, University of Hertfordshire, Herts Paper accepted June I994 Abstract This paper examines the relationship between levels of stress and the observed performance at work of direct care staff in one community unit and two group homes for people with learning disabilities. Staff completed a questionnaire which measured their levels of stress and factors which they perceived could have influenced them. Staff were observed in detail at work and asked to report on levels of stress during these observation periods. No significant differences in levels of stress were found between the staff in group homes and community units. There was greater staff/resident interaction in the group homes, suggesting that quality improvements in residential environments can be achieved without affecting staff stress. A number of factors, particularly relationships with other staff and management, are discussed as of vital importance in influencing stress levels. Introduction Recently there has been an increasing recognition of the importance of staff in the care of people with learning disabilities (e.g. Allen et al., 1991; Ayrshire & Arran Health Board, 1991; Browner et al., 1987; Canton et al., 1988; Power & Sharpe, 1988; Rose, 1993; Thompson, 1987). This interest is to be welcomed as staff are in a position to have profound influences on the lives of the people they serve. 0952-9608/94/04 0312-16 $6.00/0 MENTAL HANDICAP RESEARCH 0 1994 J. Rose, E. Mullan & B. Fletcher Vol. 7, No. 4, 1994 3 12
Transcript
AN EXAMINATION OF THE RELATIONSHIP BETWEEN STAFF BEHAVIOUR AND STRESS
LEVELS IN RESIDENTIAL CARE
John Rose South Wales Training Course in Clinical Psychology, Whitchurch
Hospital, CardijJ CF4 7XB
Ellen Mullan Slade House, Headlington, Oxford
Professor Ben (C.) Fletcher The Business School, University of Hertfordshire, Herts
Paper accepted June I994
Abstract This paper examines the relationship between levels of stress and the observed performance at work of direct care staff in one community unit and two group homes for people with learning disabilities. Staff completed a questionnaire which measured their levels of stress and factors which they perceived could have influenced them. Staff were observed in detail at work and asked to report on levels of stress during these observation periods. No significant differences in levels of stress were found between the staff in group homes and community units. There was greater staff/resident interaction in the group homes, suggesting that quality improvements in residential environments can be achieved without affecting staff stress.
A number of factors, particularly relationships with other staff and management, are discussed as of vital importance in influencing stress levels.
Introduction
Recently there has been an increasing recognition of the importance of staff in the care of people with learning disabilities (e.g. Allen et al., 1991; Ayrshire & Arran Health Board, 1991; Browner et al., 1987; Canton et al., 1988; Power & Sharpe, 1988; Rose, 1993; Thompson, 1987). This interest is to be welcomed as staff are in a position to have profound influences on the lives of the people they serve.
0952-9608/94/04 0312-16 $6.00/0 MENTAL HANDICAP RESEARCH
0 1994 J. Rose, E. Mullan & B. Fletcher Vol. 7, No. 4, 1994
3 12
STRESS LEVELS 313
Unfortunately due to differences in methodology, it has been difficult to draw any unifying themes from these studies except perhaps to conclude that working with people who have learning disabilities is generally moderately stressful and that a large number of factors such as type of work, management practices and type of resident, can influence stress levels. One recent study investigated unqualified direct care staff working in three different types of residence (Rose, 1993). Staff working in a hospital were compared with two community settings: small group homes and larger community units. This involved measuring levels of stress (or more precisely strain) and other factors which have been shown to influence strain levels. A questionnaire, based on Payne’s (1979), ‘demands, supports, constraints’ model of occupational stress was given to the staff. Relatively high levels of strain were found in the hospital and small group home settings, with lower levels of strain in the community units. A number of reasons for these differences were noted including organisational problems and resource deficiencies in the hospital; isolation and interpersonal problems posed the greatest problem in small group homes.
These results are interesting but, as with all of the other research in this area, they only represent the perceptions of staff. They do not provide an indication of what staff actually do and the quality of service provided. Moreover, they do not give any clear indication as to how job content may have differed across settings and how this may influence staff.
There are a number of potential differences in job specification between different types of residential care. For example, some staff are required to cook meals for residents. Some staff ‘sleep in’ while other units employ waking night staff. Research has confirmed more subtle differences in the nature of work performed by staff in different residential settings. Abraham, Lindsay & Lawrenson (1991), found that the amount of staff involvement in clients’ personal care decreased from hospital to more community based services. Housekeeping activities were also more frequently performed in the smaller residential services than in the hospital or by community nurses.
Research in occupational psychology has shown that job design is important in other types of job. For example, workers with relatively routine jobs have improved their psychological health when given more responsibility and a greater variety of tasks (Kemp et al., 1983; Wall, 1978; Wall & Clegg, 1981). In order to develop the work with staff it was felt important to collect data on staff behaviour to determine how this can influence both staff stress levels and the experience of residents.
314 MENTAL HANDICAP RESEARCH
Observational Studies in Residential Settings
There have been a number of observational studies focusing on the behaviour of people with learning disabilities in residential settings (e.g. Dalgleish & Mathews, 1981; Mansell & Beasley, 1989; Moores & Grant, 1976; Hewson, 1991; Rose et al., 1993). Resident observation has also been complemented by the observation of staff behaviour (e.g. Evans et al., 1990; Landesman-Dwyer et al., 1981; Porterfield et al., 1981; Raynes et al., 1979) and staff have been observed in their own right. The majority of studies of staff behaviour have reported low rates of interaction and engagement of residents by staff (e.g. Bensberg & Barnett, 1966; Burg et a/., 1979; Landesman-Dwyer et al., 1980; Repp & Barton, 1980; Wood, 1989).
Some recent studies have suggested higher levels of interaction. Orlowska et al. (1991) found that interactions between staff and residents in a small group home were twice as likely as those between staff (47.3% compared to 25.9% of the observations). Felce et al. (1991) presented data suggesting that staff in small group homes tend to spend more time interacting with residents compared to staff in large community units and hospitals. However, individual staff-to-resident interaction was closely linked to the size of staff/client groups, with larger groups resulting in relatively less staff contact. Not surprisingly, far fewer large groups were found in group homes than in community units and hospitals. Indeed, the two main findings of this study were that improvement in staff performance and client behaviour arising from the addition of staff to a client group of given size were minimal and, secondly, that when one or two staff were together, improvements in the level of staff interactions and client adaptive functioning occurred as the client group decreased in size and the number of staff remained constant. This supports the findings of a number of other earlier studies (e.g. Harris et al., 1974; Mansell et al., 1982; Repp & Barton, 1980; Tizard et al., 1972) and provides a strong argument for the development of services where small groups predominate.
While considerable attention has been devoted to staff/resident interaction, interactions between staff have been largely ignored or thought to be undesirable (Gunzburg, 1989), with little data to substantiate this assumption. Orlowska et al., (1991) have recently examined the content of interactions between staff and found them to be largely work related. This provides some support for the importance of interaction between staff in developing an efficient and cohesive staff team, the efficient implementation of work procedures and providing a model for resident behaviour.
A number of studies have suggested that clients with characteristics perceived as more favorable by staff (e.g. a lower degree of disability,
STRESS LEVELS 315
younger and with fewer years of institutionalisation) lead to staff devoting disproportionately more time to these clients (Dailey et al., 1974; Paton & Stirling, 1974; Pettipher & Mansell, 1994; Pratt et al., 1976).
Another group of studies has compared staff behaviour in different environments. For example, Felce et al. (1980) found that senior staff were more likely to interact with clients in large institutions than in small homes, whereas the opposite was the case for more junior staff. This may be an important finding in favour of the small homes where there are larger numbers of junior staff.
Developing Staff Performance
It has been suggested that additional consistent programmes of reinforcement may be necessary for staff to maintain levels of interaction and practise the skills they have learnt. Repp et al. (1987) describe four basic strategies: Monetary Feedback; Self Monitoring; Verbal Feedback; and Publicly Posted Data. These have all been used to increase the frequency and quality of interactions between staff and their clients.
Other interventions, notably room management and a number of similar strategies (e.g. Coburn, 1989; Coles & Blunden, 1981; Porterfield et al., 1980; Wood, 1989, have manipulated organisational arrangements to increase interactions, amongst other things by using staff to effectively subdivide existing groups so that optimum use can be made of staff availability. When these interventions have not been maintained con- sistently, a decrease in staff performance has been noted.
The Study
There are clearly important features of a job, such as staff group size, job variety, job role and resident characteristics that could influence levels of staff stress. The aims of the current study were therefore to see if any further evidence could be found for the higher levels of stress previously reported in group homes compared to community units (Rose, 1993). For example, could it be that there are increased staff/resident interaction levels in group homes that may contribute to increased stress levels of staff. Or could there be greater staff/staff interaction in community units that may act to reduce stress levels? Data on the range and variety of activities performed by staff was collected to see if these influence staff stress levels. These factors were investigated while attempting to keep others such as client characteristics and role in job (only direct care staff were investigated) constant.
316 MENTAL HANDICAP RESEARCH
Method
Settings
A subgroup of the residences that had been used in previous research (Rose, 1993) were chosen to participate in this project. After an approach was made through management, one community unit was identified for study. This consisted of three adjacent bungalows (two with six and one with seven full time residents; one bungalow with six beds had an additional respite care bed). Two group homes were identified for comparison, consisting of ordinary houses both with four full time residents. All residences were managed as part of the NHS.
Resident characteristics
.4n attempt was made to select homes and units with residents who had similar characteristics. Initial comparison was made using a brief screening assessment called the resident profile (Thomas & Ponton, 1992). This was then followed by a more detailed assessment using part 1 of the Adaptive Behaviour Scale (Nihara et al., 1974). Staff who knew the person well, or staff and the resident concerned completed the assessment with one of the authors assisting.
Five of the eight residents in the group homes were male and three female. Seven of the nineteen permanent residents in the community unit were female and twelve male.
Table 1 Adaptive behaviour scale scores for residents
IF PD EA LD NT DA VA SD R S Total
Group Homes Average 43 14 3.5 15 3 7 1 9 2.5 13 1 1 1 Range (7-82) (5-24) (1-9) (2-28) (0-10) (0-15) (0-6) (1-20) (0-6) (2-24) (22-207)
Community Units Average 44 14 1 14 I 4 1 7 1.5 I 1 99 Range
Key: IF = Independent Functioning P D =Physical Development
EA =Economic Activity NT =Number and Time VA = Vocational Activity R = Responsibility S = Socialisation
LD = Language Development DA = Domestic Activity SD = Self Direction
STRESS LEVELS 317
When permanent residents were compared between group homes and community unit there were no significant differences in age profiles. Mean age in the community unit was 54, with a range from 24 to 81 years old. In the group homes, mean age was 41 with a range of 22 to 76 years old. Table 1 shows the average scores and ranges obtained from the ABS for both individual scales and totals. No significant differences were found when total scores were compared using t-tests.
Staff investigations
As in previous research, only direct care staff were involved in the project, that is staff without nursing qualifications and management responsibility (on nursing grades A-C), as it was felt that qualified individuals may have different concerns. There were 34 staff on these grades in the community unit and group homes involved in the study. No domestic staff or cooks were employed in any of the residences. Direct care staff were initially approached through a staff meeting and individuals who did not attend were contacted separately. All aspects of the project were explained and the voluntary nature of participation emphasised.
Background characteristics
Four men and thirteen women returned questionnaires from the community unit and three men and seven women returned questionnaires from the group homes. Comparisons using the chi-squared test 0, <0.05) indicated no differences in background characteristics between community unit and group home staff except for marital status. The average age was approximately 34 years old in the community units and 24 years old in the group homes. This probably accounted for more of the staff being married in the community unit than the group homes (nine compared to one). There was only one single person in the community unit sample and six in the group homes, the remainder being divorced, widowed or separated.
Average length of service in the community unit tended to be longer (26 months) than in the group homes (16 months). This may be related to better career structure, with unqualified staff being able to obtain higher grading (and therefore pay) in the community unit than in the group homes. There was little difference in the amount of training they reported, with 14 out of 17 communityunit staff and nine out of ten group home staff reporting some training. Training generally consisted of short in-service courses either at or near to their base. Common topics included Social Role Valorisation, Challenging Rehaviour, Teaching Skills, Epilepsy and Sexuality.
318 MENTAL HANDICAP RESEARCH
Questionnaire measures
Staff were first asked to complete a general stress questionnaire similar to that used in the previous research. This asked for details of background characteristics, demands, supports/constraints and a strain measure. Thirty- three demand items and twenty-three supports/constraints items were identified. Questions were constructed so that individuals could rate levels of demand on scales from one to five. A similar rating was used for the supports/constraints items but here ratings of four and five signified levels of support and one and two levels of constraint, three being a neutral rating. A rating of zero for both types of items enabled the participant to indicate that the item was not relevant to them. Stress was measured by the ‘Thoughts and Feelings Index’ (Flectcher, 1989). Details of individual items are found in Rose (1993). The questionnaire was completed and returned anonymously, but a note was made of the house or bungalow in which the individual worked. The return rates for this questionnaire were high, 17 out of 22 (77%) for the community unit staff and 10 out of 12 (83%) for the group home staff.
Observational measures
Arrangements were made between the researchers and staff to observe individual staff at work. A protocol for observation was devised which was based on that used by Cherniss (1986), and is available on request from the first author. The observations were collected using Psion organisers programmed for a 30-second momentary time sample. Software developed for resident observation (Beasley, Hewson & Mansell, 1989) was recoded, so that it could be used to observe staff. In total three observers were used to collect the data.
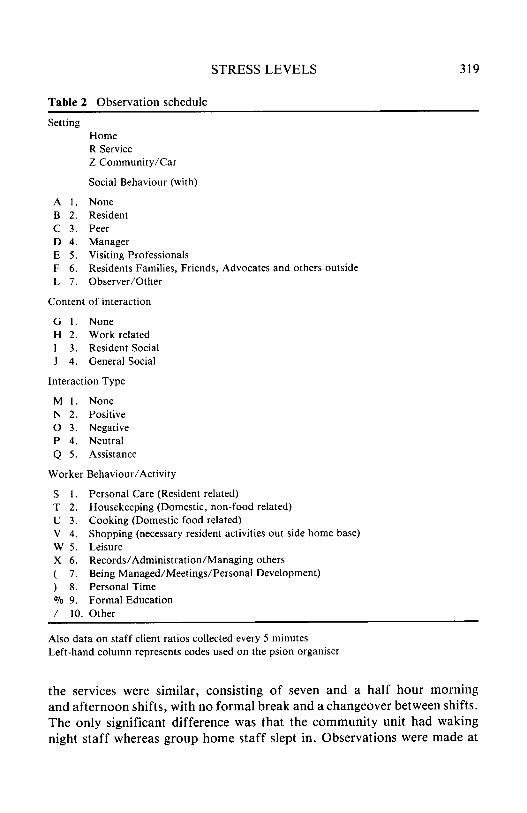
The observation schedule required a judgement as to who the member of staff being observed was interacting with (if anyone), the content of the interaction, the type of interaction, and what activity the member of staff being observed was involved in. A note was also made of the setting in which the observation was made e.g. inside or outside the home. Headings for the codes used are shown in Table 2. A more complete description of the codes and definitions are available from me first author. Staff/client numbers were recorded every five minutes.
Observation schedules
Individual staff were observed for 90-minute periods with a short break at 45 minutes to facilitate the concentration of observers. Shift patterns in
STRESS LEVELS 319
Table 2 Observation schedule
Setting Home R Service Z Community/Car
Social Behaviour (with)
A 1. None B 2. Resident C 3. Peer D 4. Manager E 5 . Visiting Professionals F 6 . Residents Families, Friends, Advocates and others outside L 7. Observer/Other
Content of interaction
G 1 . None H 2. Work related I 3 . Resident Social J 4. General Social
Interaction Type
M 1. None N 2. Positive 0 3. Negative P 4. Neutral Q 5 . Assistance
Worker Behaviour/Activity
S 1. Personal Care (Resident related) T 2. u 3. v 4. w 5 . X 6 . ( 7. ) 8. VO 9. / 10.
Housekeeping (Domestic, non-food related) Cooking (Domestic food related) Shopping (necessary resident activities out side home base) Leisure Records/Administration/Managing others Being Managed/Meetings/Personal Development) Personal Time Formal Education Other
Also data on staff client ratios collected every 5 minutes Left-hand column represents codes used on the psion organiser
the services were similar, consisting of seven and a half hour morning and afternoon shifts, with no formal break and a changeover between shifts. The only significant difference was that the community unit had waking night staff whereas group home staff slept in. Observations were made at
3 20 MENTAL HANDICAP RESEARCH
different times on different days with different members of staff being observed. However, a general plan was followed for each house whereby all of the times between 7.30am, when staff started the morning shift, up until 10.00pm, when staff finished the evening shift, would be observed once on a weekday (i.e., nine observations). Three additional observations were made at weekends to try and provide a representative cross section of a week's work. This meant that 12 observations were made in each house (totalling 18 hours). In total 54 hours of observation were conducted in the community unit and 36 hours of observation in the group homes. Out of the total staff group of 34, only two declined to participate in the study. Other staff were observed between one and four times.
Summary frequencies of each code from each observation were taken and collated. Comparisons were then made between observations made in group homes and community unit. Total means for each set of observations were calculated and the data was compared using t-tests. Average staff/client ratios were compared in the same way.
Reliability
Two observers were present for reliability checks for nine hours in the community unit (16.6% of observations) and three hours in the group homes (8.3 "0 of observations). Inter-rater reliabilities were calculated for individual observation sessions using a programme that calculates both percentage agreement and Kappa for each variable (Martin, 1992). Inter- observer agreement was high ranging between 86% and 100% for each variable. Kappa values were also generally acceptable with the large majority exceeding 0.8. A few values were in the range 0.6-0.8 for particular observation periods. This generally coincided with unusual events such as a visit to a restaurant.
However, there were some instances of large disagreement with codes that were generally low scoring or that had not occurred frequently in a particular observation period. For example, one rater may have used one code once during an observation with no corresponding coding by the other rater. Codes where this occurred included positive interaction, assistance; general social interaction; being managed, and meetings. However, there were other examples of good agreement for these codes. When the data were combined across all sessions relating to a setting, Kappa values were reasonable for all codes, ranging from 0.75 to 1 .O. All percentage agreements were in excess of 88%.
STRESS LEVELS 32 1
Immediate monitoring of stress levels
On completion of the observation period, the person observed was requested to complete a brief questionnaire which asked them to rate their levels of stress and other associated factors during the period of observation (Table 3). Staff were also given the opportunity to comment on any aspect of the research, both verbally and in writing. The questionnaire was completed and returned to the observer before they left the house or unit.
Table 3 Items included on the post observation questionnaire Unstressful
Unpressurised Satisfied
Interesting 1 felt Included
Work was not challenging Relationships with
colleagues were good Demands of residents
were low Demands of Boss
were low Support from Boss
was high I felt clear about
my duties Observation did not
influence my behaviour
Stressful* Pressurised Unsatisfied Boring I felt Isolated Work was challenging Relationships with colleagues were difficult Demands of residents were great Demands of Boss were high Support from Boss was low 1 felt unclear about my duties Observation influenced my behaviour
~~ ~ ~~
Staff were asked to reply using a seven-point Likert scale. * This item was asked twice, once relating to the period of observation and once relating to the whole shift. On other items staff were only asked to comment on the period of observation.
Results
Levels of strain
The score on the depression and anxiety scales of the ‘Thoughts and Feelings Index’ (Fletcher, 1989) showed that the overall levels of depression and general anxiety reported by group home staff were lower than those reported by community unit staff (Table 4).
322 MENTAL HANDICAP RESEARCH
Table 4 Scores obtained on the general anxiety and depression scale for community unit and group home staff
No. staff General Anxiety Depression in sample score score
Community Unit 17 Group Home 10 Community Unit 47 (Rose, 1993) Group Home 3 1 (Rose, 1993)
9.35 7.80 8.59
9.77
8.18 7.70 7.37
8.52
Differences in demands and supports/constraints
A number of significant differences were (t-test; p < 0.05) noted between responses of staff in the community unit and those in group homes in respect of the demands and supports/constraints items on the general stress questionnaire. These are shown in Table 5 .
Table 5 Significant differences between community unit and group home staff on demands and support/constraint items 0, < 0.05)
Demand
Keeping up to standards of nurse in charge Certain individual staff Large number of jobs The paperwork Being moved between houses Lack of results Having too few staff on shift
Community Unit Group Home
2.94 1.60
3.29 3.23 2.94 2.76 3.23 3.23
1.55 2.11 1.87 1.75 2.40 4.30*
Support
From colleagues 3.76 4.70
Doctor 3.47 4.00** O T 3.13 4.50**
Regular IPP’s or reviews 3.88 4.44
Knowing role in job and NHS 4.00 3.44***
* The only item group home staff found more demanding. * * Only applicable to one house. *** The only support found t o be significantly greater by community unit staff.
STRESS LEVELS 323
Table 6a Total interactions Community Unit Houses
None 47.59 Residents 28.58 Colleagues 17.76 Boss 4.71 Visiting Professionals 0.37 Residents Families etc. 0.54 Observer (other) 0.65
38.72* 44.48** 10.37* 2.78 I . 15 (all one house) 5.17 0.44
Table 6b Content of interaction Community Unit Group Homes
None Work Related General Social
47.82 49.72
2.91
38.82* 59.21** 2.35
Table 6c Interaction type Community Unit Group Homes
The major findings from the observational measures (Table 6) were that group home staff were generally more interactive than community unit staff @<0.05): they interacted far more with residents than community unit staff (p<O.Ol), whereas community unit staff tended to interact far more with their peers (pc0.05).
There were also significantly more ‘work related interactions’ in group homes that is, interaction with residents, combined with work related interactions with other workers etc. The relative proportions of interaction types were similar, with positive and negative interactions being at a low level in all environments.
When examining worker activities, community unit staff were significantly less likely than those in group homes to be involved in leisure activities with clients and they were more likely to be observed while being managed or in meetings (p<O.O5) . A number of other differences did not reach statistical significance. These included staff being involved in more cooking in the community unit and taking more breaks (personal time). Staff and client groups tended to be significantly larger in the community unit (both p<O.Ol), with generally more favourable ratios in the group homes.
Staff ratings immediately after observation
The analysis of staff ratings in the questionnaire immediately following observations showed only one significant difference between the two groups (t-test p<O.O5): staff in the group homes felt their boss to be significantly more supportive, when present, than community unit staff.
It is interesting to note that the effects of observation were not considered to be intrusive by either group. This was rated 2.16 in group homes and 2.20 in the community unit, on a scale from one (low influence) to seven (high influence). There were very few written or verbal comments about the research, except those relating to the process of observation. These were generally of the type ‘it was much easier than I thought it would be’ or ‘after the first few minutes observation did not bother me’.
Discussion
Perhaps the most interesting finding in this study is that the two group homes in this study do not follow the general trend of those surveyed in earlier work (Rose, 1993; Table 4) and are apparently less stressful places to
STRESS LEVELS 325
work than the community unit. Statistical comparison confirms a lower level of general anxiety in the homes in this study to those previously surveyed.
This finding was tempered by the fact that there did seem to be some differences in the type of staff employed (in terms of marital status and age), which may have tended to produce lower stress ratings in these group homes. Different characteristics of residents may also have influenced the results.
The differences in demands and support/constraint items between the group homes in the current study and those in the earlier study (Rose, 1993), suggest that the current staff groups were functioning more effectively as teams with staff feeling less isolated and other staff being perceived as less demanding, having higher morale and being more supportive. Support from their manager was also perceived as relatively high. In one home in the current study the work of external professionals seemed to be a significant support. While conducting the observations, the questionnaire replies of staff were confirmed anecdotally, with these group homes proving to be particularly pleaseant places for staff to work and residents to live. In contrast, when compared to the previous research, results from the community unit were generally similar, if not slightly more stressful and demanding places to work.
The current research has tended to confirm previous findings (Felce et al., 1991) of greater staff/resident interaction and less staff/staff interaction where there were smaller groups of staff and residents (that is in group homes rather than in the larger residences). However, the lower contact with colleagues and manager could generally predispose group home staff to stress. Even though there was clearly no evidence for this here, this needs further investigation.
General levels of interaction were higher in group homes and this may be said to be indicative of a higher quality of service in these residences. Also the greater staff/resident interaction recorded in the group homes, where there were smaller resident groups would translate into many more contacts for individual residents, with very few of these interactions being negative.
On close examination of the interaction data it is important to note that the staff interactions were predominantly work-related. No categorisation of such interactions were attempted, but during observation it was clear these interactions were important, both for the general functioning of the house and to the residents to whom the majority of them were addressed. Even though it could be argued that non-work interactions may have been reduced with an observer present, few of the staff gave the impression that they had significantly altered their behaviour, and indeed reported little effect on their behaviour. It could also be said that the social interaction that did occur was an important part of team building for staff (particularly
326 MENTAL HANDICAP RESEARCH
as there were no official breaks on shift) and may have provided a model for residents.
It seems that workers in group homes tend to spend more time on leisure activities than their peers in the community unit. The ability of staff to engage in more leisure with clients may be explained by more opportunity due to their locations in the community and more favourable staff ratios.
Staff in the community unit tended to spend their time in meetings, cooking and in personal time (breaks etc.). The greater size and complexity of the community unit organisation and the proximity of management probably account for the extra meetings. Extra cooking could probably be accounted for by relatively fewer staff cooking for larger numbers. Staff in the community unit also probably engaged in much more housework as waking night staff in this unit were supposed to do housework whereas group home staff slept in. Both groups of staff engaged in similar amounts of housework during the day. Again, this could be explained by proportionally fewer staff being available in community units. Community unit staff may be more concerned with housekeeping functions, due to a lower staff/client ratio or due to a different style of approach to their work.
The greater amount of time spent on personal breaks in the community unit may be due to the slightly larger groups of staff and greater opportunities to talk with colleagues.
Some broad recommendations for the future can be made for both types of accommodation. It would be hoped that community units could be replaced by group homes. However, great care must be taken to provide adequate staffing levels to ensure a quality service can be maintained (staff in better staffed group homes perceived more demands arising from low staffing levels). Special attention needs to be given to management support (probably by managers actually working in the houses with staff) and team building with staff to ensure a cohesive, low stress service.
Even though the group homes have been shown to provide a high quality, lower stress service, great care must be taken to ensure that inter-staff and staff-management relationships are maintained. This could be done in a number of ways, such as providing routine feedback to staff, holding more regular team meeetings and examining particular aspects of their work. It would also be important to provide cover during any long term gaps in staffing as the loss of a single staff member in a small group, for any length of time, could increase the pressure on other staff members dramatically.
This research has examined the link between worker behaviour and stress. It has not been able to replicate previous findings, which suggests a degree of variability between individual residences. More work of this kind needs to be done. The study of ‘high’ and ‘low’ stress residences may provide clearer
STRESS LEVELS 327
indications of what are the most important factors that influence staff stress in residential care. It would also be useful to study other factors such as resident characteristics, particularly challenging behaviour, and how these can influence stress levels. The current research has suggested a number of factors, particularly those associated with relationships between staff, that are influential in regulating levels of stress.
Perhaps most importantly it has also shown that high quality residential services for people with learning disabilities, as represented by the group homes in this study, do not necessarily have to be provided at the expense of staff stress levels.
Acknowledgements
Thanks are due to the staff who took part in the project and the residents who let us enter into their homes. We are also grateful for the assistance and encouragement of the management of Oxfordshire Learning Disabilities (NHS) Trust.