AN EXPERIMENTAL INVESTIGATION OF THE EFFECTIVENESS OF ASSERTION TRAINING WITH ALCOHOLICS by STEVEN M. HIRSCH, B.A. A DISSERTATION IN PSYCHOLOGY Submitted to the Graduate Faculty of Texas Tech University in Partial Fulfillment of the Requirements for the Degree of DOCTOR OF PHILOSOPHY May, 19 75
Transcript
AN EXPERIMENTAL INVESTIGATION OF THE EFFECTIVENESS
OF ASSERTION TRAINING WITH ALCOHOLICS
by
STEVEN M. HIRSCH, B.A.
A DISSERTATION
IN
PSYCHOLOGY
Submitted to the Graduate Faculty of Texas Tech University in Partial Fulfillment of the Requirements for
the Degree of
DOCTOR OF PHILOSOPHY
May, 19 75
c I V — \ (I -' *.
73
ACKNOWLE DGMENTS
I am sincerely grateful to my chairman. Dr. Jack L.
Bodden for his support and direction in this dissertation
project. Special appreciation and my deepest thanks go to
Dr. Robert P. Anderson for his constant encouragement and
concern. I greatly appreciated the statistical expertise
of Dr. Frank Lawlis and Dr. Douglas Chatfield and the
helpful critiques offered by Dr. Bruce Mattson. I am
also deeply indebted to Robert von Rosenberg, M.A., of
the Big Spring State Hospital, and Caren Phelan, Ph.D.,
of the San Antonio State Hospital, for their invaluable
efforts in making this study possible. I should also like
to extend a special note of thanks to the numerous profes
sionals of the Texas Department of Mental Health and Mental
Retardation who gave so freely of their time and expertise
in making this project a reality. Finally, the granting of
research funds from the Texas Commission on Alcoholism, to
assist with data collection, was deeply appreciated.
11
TABLE OF CONTENTS
ACKNOWLEDGMENTS ' ii
LIST OF TABLES V
I. INTRODUCTION 1
Review of the Literature 6
Statement of the Problem . . . . . . . . . 54
II. METHODOLOGY 5 8
Subjects 58
Instrumentation . 5 8
Procedure 64
Control Group 65
Minimal Assertive Training Group 66
Assertive Training Group 6 7
Hypotheses 6 8
Statistical Analyses . . . . . 69
III. RESULTS 70
Demographic-Drinking Data Form 70
Hypothesis 1 73
Hypothesis 2 75
Hypothesis 3 76
Hypothesis 4 ' 82
IV. DISCUSSION . . . . . . . . . 84
Research Hypotheses 84
Theoretical Implications . 9 4
111
Programmatic and Research Implications . . 9 7
V. SUMMARY AND CONCLUSIONS 10 4
REFERENCES 10 8
APPENDIX . 115
A. Demographic Drinking Data Form 116
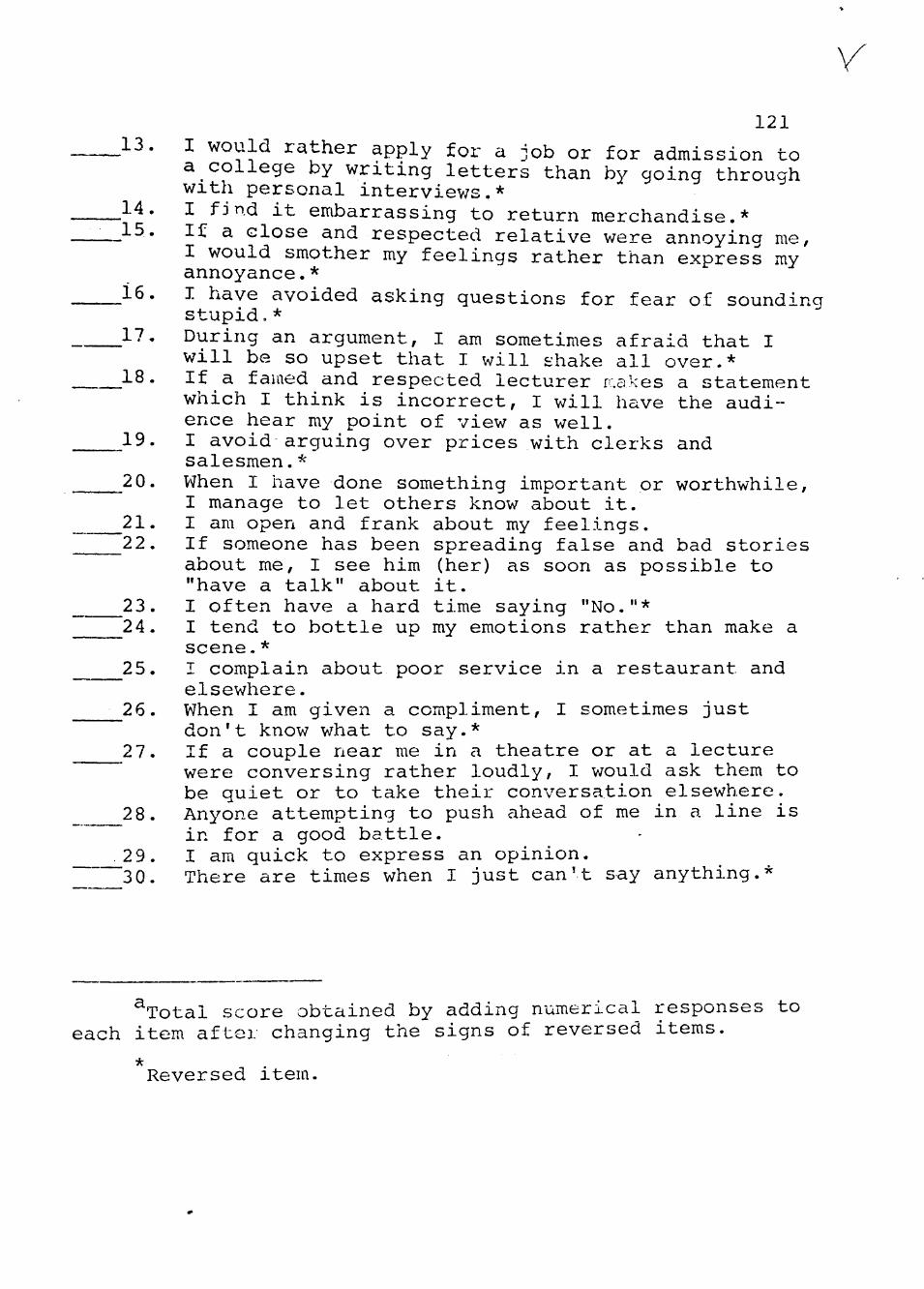
B. Rathus Assertiveness Scale . . . . . 120
C. Behavioral Assertiveness Test . . . . . . . . 122
D. Scoring Sheet for Behavior Assertiveness Test 125
E. Assertive Behavior Index 127
IV
LIST OF TABLES
1. Demographic-Drinking Data 70
2. Correlation of RAS Scores of Alcoholics with Five Variables 74
3. Rathus Pre-Posttest Means and Standard Deviations for Treatment and Control Groups 75
4. Analysis of Covariance Results of RAS Scores for Treatment and Control Groups . . . . 76
5. Response Latency Means and Standard Deviations for Treatment and Control Groups 77
6. Analysis of Variance Results of Response Latency Scores for Treatment and Control Groups 77
7. Response Duration Means and Standard Deviations for Treatment and Control Groups in Seconds 78
8. Analysis of Variance Results of Response Duration Scores for Treatment and Control Groups 79
9. Rater's Means, Standard Deviations and Inter-Rater Reliability of BAT 80
10. Average Total Assertiveness Means and Standard Deviations for Treatment and Control Groups 80
11. Analysis of Variance of Mean Assertiveness Scores on the BAT for Treatment and Control Groups 81
12. ABI Means and Standard Deviations for Treatment and Control Groups 82
V
CHAPTER I
INTRODUCTION
Alcoholism has long been a major health problem in
this country, directly affecting an estim.ated nine million
individuals and their families. It has become increasingly
evident that legal sanctions and moral pressures have not
provided an adequate remedy for this problem. Moreover,
it is estimated that treatment of alcoholic individuals
with present techniques would fill every existing hospital
bed and require the full-time services of every physician
in the Nation. Consequently, solution of this problem must
ultimately lie in the development of improved prevention
and treatment techniques.
In recent years there has been a movement av/ay from
a generalized "psychotherapy" treatment for emotional,
intellectual, or behavioral disorders in favor of a more
specific approach v/hich matches treatment and therapist
with client and problem. Clients who benefit from therapy
regardless of the type of treatment they undergo, often
state that they have become less inhibited, more outspoken,
and able to stand up for their rights. Most recently, a
growing number of clinicians (Blake, 19 65; Martorano, 19 74;
Miller, Hersen, Eisler, & Hilsman, 1974) have recognized
that various procedures subsumed under the heading of
assertive training can be effectively utilized to help
alcoholic clients achieve a greater degree of self-esteem
and emotional freedom.
The therapeutic technique called assertive training
has been in existence for about 15 years (Wolpe, 1958).
Practitioners have customarily employed it in one-to-one
therapeutic situations with persons for whom nonassertive-
ness or unassertiveness was part of their problem. Over
the last 3 or 4 years behavior change agents have expanded
the technique to the treatment of groups of unassertive
individuals. It is this modality of treatment which is
the subject of the present research.
Assertive behavior refers to all socially acceptable
expressions of personal rights and feelings (Wolpe &
Lazarus, 1966). It is the action of declaring oneself,
of stating, "this is who I am and what I think and feel."
Being assertive includes the honest, appropriate and rela
tively straightforward expression of such negative feelings
as anger, dissatisfaction, and resentment, as well as the
expression of such positive feelings as love, affection,
and praise. Alberti and Emmons (19 70) perhaps summarized
it best when they said that assertive behavior is that
"which enables a person to act in his own best interest,
to stand up for himself without undue anxiety, to express
his rights without denying the rights of others" (p. 7).
The rationale for training in assertion is presented
by Wolpe (19 69) as follows:
Assertive training . . . is required for patients who in interpersonal contexts have unadaptive anxiety responses that prevent them from saying or doing V7hat is reasonable and right . . . suppression of feeling may lead to a continuing inner turmoil which may produce somatic symptoms and even pathological changes in predisposed organs. (p. 61)
A variety of component techniques including advice, exhorta
tion, coaching, social modeling, role playing, behavioral
rehearsal, graded exercises, and homework assignments are
used during the full course of assertive training. Although
Wolpe emphasized the principle of "reciprocal inhibition" in
his earlier writing (Wolpe, 1958), in his more recent writ
ings (Wolpe, 19 69, 19 70) the importance of operant condi
tioning (reinforcement and shaping) during assertive
training has been acknowledged.
Increased assertiveness, therefore, is assumed by
Wolpe to benefit the client in two v;ays:
1. It is thought that more assertive behavior will
instill in the client a greater feeling of well-being. This
proposal is related to the "reciprocal inhibition" view that
'assertive behavior is very similar to deep muscle relaxation
in being physiologically antagonistic to anxiety.
2. It is assumed that, by behaving in a more assertive
manner, the client will bring about positive changes in be
havior of others toward him, and thus be better able to
achieve significant social (as well as material) rewards
and, in fact, control his own destiny. In theory, therefore,
the individual achieves both internal and external positive
feedback from appropriate assertive responses.
The assertive training approach to psychotherapy is
based on a response acquisition model of treatment (McFall
& Twentyman, 1973). Within this model, unadaptive behaviors
are interpreted in terms of the absence of specific response
skills. The therapeutic objective of assertive training
with alcoholics is to provide clients with direct training
in precisely those interpersonal and social skills deficient
in their response repertoire.
Very little attention is given to eliminating existing maladaptive behavior; instead, it is assumed that as skillful, adaptive responses are acquired, rehearsed and reinforced, the previous maladaptive responses will be displaced and will disappear. (McFall & Twentyman, 19 73, p. 199)
As positive rewarding behaviors are practiced and developed,
they will compete with and eventually replace alcoholic
avoidance and escape.
In contrast to psychodrama (Corsini, 1966; Moreno,
1946) or attitude change research (Elms, 1969) where the
focus is on the modification of abstract emotional or
cognitive processes, assertive training procedures are
r
designed to modify definite observable behaviors. Asser
tive training, in effect, permits clients to simulate
problem situations and to practice new ways of responding
without concern or anxiety for the immediate real-life
consequences of their experimental behavior. Only after
clients develop proficiency and confidence in their
responses do they attempt to transfer them to real-life
situations.
Clinical evidence (Miller et al., 1974) suggests that
interpersonal situations requiring an alcoholic to respond
assertively (i.e., direct expression of personal rights
and feelings) are often stressful and frequently lead to
as a generalized trait, Wolpe views it as being specific
to situations and emotions.
3. Wolpe is more concerned with the possible inter
personal consequences (especially negative) of assertive
acts.
Wolpe's (1958, 1969, 1971) main focus, however, was
upon the reduction of anxiety. Assertive responses, like
sexual and relaxation responses, are inhibitory of anxiety
in his well-known classical conditioning model of learning.
Cure of social anxiety (which inhibits appropriate social
expressions) involves a counter-conditioning of the anxiety
of eliciting the inhibited assertive response through
persuasion, instructions, and cognitive restructuring.
The augmented emotions accompanying assertiveness inhibit
the anxiety response habit, and the motor act of assertion
is increased in frequency by its reinforcing consequences
in daily life (e.g., control of a social situation).
Today much of Wolpe's explanation of behavior change
via reciprocal inhibition is in question (Lang, 1969;
Meichenbaum, 1971; Spence, 1971), but his pioneer work in
assertive training is still important. His basic treatment
techniques can be found in the repertoire of many therapists
(a) encouraging the outward expression of feelings of anger,
etc.; (b) directly instructing the client how to act asser
tively; and (c) rehearsing the needed behavior with the
client.
Another pioneer in training people in assertive
behavior is Arnold Lazarus. He stressed the idea of "emo
tional freedom" of which assertiveness is a subunit.
Training in emotional freedom implies the recognition and appropriate expression of each and every affective state . . . assertive behavior will denote only that aspect of emotional freedom that concerns standing up for one's rights. (1971, p. 116)
In Behavior Therapy Techniques (1966), he and Wolpe described
three techniques which La2;arus has continued to elaborate
upon in subsequent writings (Lazarus, 1966; Piaget & Lazarus,
1969): (a) behavior rehearsal, (b) graded structure, and
(c) cognitive restructuring.
In behavior rehearsal the client repeatedly practices
assertive responses, such as telling a mother-in-law to stop
being so obtrusive, until he is relatively comfortable in
saying the words. If the target behavior is so anxiety
provoking that the individual would be unlikely ever to
Some less threatening behavior in a graded hierarchy of
assertive situations is rehearsed first until the client
is successful in its performance. Then he moves closer to
practicing the target behavior itself and ultimately to
performing it in his real-life situation.
10
Lazarus (19 71) believed that using a graded structure
of tasks in therapy can be therapeutic itself. Structure
gives a person a knowledge of what leads to what and of
the steps in the solution of a problem. It allows him to
attend to and concern himself with the "right things" in
therapy. The graded aspect lets a person have a sense of
achievement and fulfillment that results from a step-by-
step progress. Much like programmed learning, graded
structure allows the client to get a sense of mastery over
his problem via active participation, immediate reinforce
ment and feedback concerning results.
Unassertive persons (as well as others) cause unneces
sary grief for themselves because of faulty anxiety-arousing
conceptions regarding the social situation at hand. They
repeatedly tell themselves that they cannot handle a situa
tion, or that they are inferior persons and so doom them
selves to maladaptive behavior.
The bulk of therapeutic endeavors may be said to center around the correction of misconceptions. The people who consult us tend to view innocuous events as extremely noxious, and may disregard objectively noxious situations. Therapy often strives to show people how to separate subjective from objective dangers. Thereafter, the emphasis is on avoiding or coping with objectively hazardous events while ignoring the innocuous situations. (Lazarus, 1971, p. 165)
The first "do-it-yourself" manual of assertive training
was written by Alberti and Emmons (19 70) for both profession
als and laymen. The authors' premise was that men are
11
created equal and so have a right to personal dignity
without untoward fear in social interactions. They pro
posed to help their readers develop a more adequate reper
toire of assertive behaviors in order that these persons
can have a greater range of choices of self-fulfilling
behaviors in a number of situations. This freedom to choose
responses should enable a person to escape from his con
stricted pattern of behaviors and move to a fuller human
life.
Alberti and Emmons distinguished for their readers
aggressive, assertive, and nonassertive behaviors. The
aggressively behaving person enhances himself and achieves
his goals at the expense of others. He chooses for others,
deprecating him and leaving him hurt and without achieving
his goals. The nonassertive person is inhibited, self-
denying, and so does not achieve his goals. He allows
others to choose for him and ends up being anxious, hurt,
and full of suppressed rage. The assertive person behaves
in a self-enhancing way to achieve his goals. He makes
choices for himself and he allows the other person to pursue \
his goa ls as well.
Alberti and Emmons distinguished between a situation-
ally nonassertive person and a generally nonassertive one.
The former exhibits behavior that is generally adequate
but is ineffective in specific situations. The generally
t "' »
12
nonassertive person usually has low self-esteem, feels
inadequate, and is anxious in most all social situations.
These individuals may require special psychological help ^^
in addition to assertive training.
The authors prescribed a 14-step assertive training
procedure. First, clients receive an explanation from the
therapist of why they have a right to be assertive. There
after, they undergo a problem-solving process which incor
porates role playing, behavior rehearsal, and modeling. The '
therapist provides feedback and reward to the client in a
graded structure procedure similar to the one suggested by
Lazarus (19 71). Alberti and Emmons suggested instructing
clients in the principles of self-reinforcement so that
behaviors will be maintained and generalized in the absence
of the therapist. They also recommended the use of treatment
in a group, citing such advantages as being able to share
with others who have the same problems (cf. Yalom, 19 70, on
"Universality"), helpful modeling from others in the group,
a more realistic social learning environment, and increased
feedback.
Manuel Smith (19 75) has recently published a book on
systematic assertive therapy which is entitled When I Say No,
I Feel Guilty. The author has a somewhat different slant
toward assertive training than what Alberti and Emmons have
described. Smith appeared to use less modeling, coaching.
13
and behavior rehearsal, but instead he tended to focus on
the verbal content of an assertive message. He described
a number of training dialogues which cover many everyday
situations such as returning purchases, handling criticism,
asking for a raise, meeting new people at parties, and
learning how to say no without anger, fear or guilt. The
main focus of the book was directed toward the teaching of
verbal techniques such as "broken record," "fogging,"
"negative assertion," etc. with the basic notion of helping
clients learn how to out manipulate the manipulators.
Techniques of Assertive Training
Assertive training techniques are not as standardized
as many other^behavior therapy techniquesJ nor have they
been carefully investigated. Assertive training takes on
many different forms, but is generally applied in the fol
lowing manner. Generally, a first step in teaching asser
tive behavior requires that the client be aware of how he
comes across (awareness = response - ability). When the
therapist, using situations which are drawn from the
client's life, carefully distinguishes among assertive,
aggressive, and nonassertive behavior, the client usually
realizes quickly that he has an assertive problem. The
therapist must explore all areas of difficulty to determine
the controlling factors--the situational and personal vari
ables that raise anxieties and decrease the client's ability
14
to behave assertively. Obtaining a good clinical history
is often an important part in determining those areas
where the patient is having problems.
A major goal of assertive training is building a
personal belief system which v/ill help the client to support
and justify his acting assertively. This is important so
that the client believes in his right to act assertively
even when he may be unjustly criticized, and can counteract
his own irrational guilt that often occurs as a result of
having asserted himself. An important part of this belief
system concerns the patient's acceptance of certain basic
interpersonal rights. Didactic explanations are very useful,
explaining the differences between nonassertive behavior,
aggressive behavior, and assertive behavior.
NON-ASSERTIVE BEHAVIOR
Actor
Self-denying
Inhibited Does not achieve desired goal(s)
ASSERTIVE BEHAVIOR
Actor
Self-enhancing
Expressive May achieve desired goal(s)
AGGRESSIVE BEHAVIOR
Actor
Self-enhancing at expense of another
Expressive Achieves desired goal(s) by hurting others
Allows others to Chooses for self Chooses for others choose for him
Hurt, anxious Feels good about Depreciates others self
15
Acted Upon
Guilty or angry, depreciates actor
Achieves desired goal(s) at actor's expense
Acted Upon
Self-enhancing expressive
May achieve desired goal(s)
Acted Upon
Self-denying, hurt defensive, humiliated
Does not achieve desired goal(s)
(Alberti & Emmons, 1970, p. 24)
In the initial stages of assertive training, the
therapist stresses the negative effects (frustration,
resentment, lack of satisfaction) of patient's nonassertive
behavior, hov; such behavior is learned and how more appro
priate assertive responses can be conditioned with resulting
feelings of personal well-being, relief, and interpersonal
satisfaction. This procedure is an attempt to change the
client's attitude toward his behavior. The therapist briefly
describes the method and rationale of assertive training and
discusses some of the techniques that will be used.
A commonly used technique in assertive training is
behavior rehearsal (V7olpe, 1969). This is a procedure which
requires the client to act out relevant interpersonal inter
actions. Initially the client demonstrates behavior which
is typical for him in a given situation. The therapist then
supplies corrective feedback, support, and verbal reinforce
ment. By repeated practice, the client reduces his anxiety
and develops a sense of mastery over interpersonal situations
which previously caused difficulty. The therapist used the
16
principle of successive approximations to help shape the
client's behavior. Role rehearsal, in which the client
models the behavior of the significant other and the
therapist assumes the client's role, may also be employed.
Clients in a group receive feedback from each other and
from the therapist on their practice behaviors. They will
encourage and support one another's progress. The use of
video-tape feedback can be a particularly powerful technique
in changing client's behavior.
In a lengthy interaction, the therapist should
determine that each segment can be mastered by the client
with little or no anxiety before proceeding to the next
segment of interaction. In an interaction involving the
expression of negative feelings, it is helpful to have the
client begin with a relatively mild response. He should,
however, be given stronger responses in case the initial
response is ineffective. In rehearsing the expression of
negative feelings, it should be pointed out that feedback
pertaining to annoying or hurtful behaviors on the part of
the other person is far superior to personal attacks, which
are often irrelevant and have the effect of backing the
other into a corner. Clients are asked to try target
behavior(s) in their real life settings and report the,
success or failure in their next session. Needless to
say, the client must be considered potentially capable
•I ^
17
of completing the assignment within prescribed time limits
(Fensterheim, 1972).
Modeling is a technique based on principles of
imitative learning. When used in combination with feed
back and instruction, the necessity of individuals dis
covering the most effective response through trial and
error is eliminated. In his research, Bandura (1969, 1971)
had established that modeling and guided participation is
one of the most effective methods of modifying anxiety-
based avoidance behavior. According to this method, the
therapist models behavior for the client and preferably
has others model it as well. The client then practices
the model's behavior with coaching from the therapist in
a graduated sequence of behaviors from the easiest to the
most difficult. Favorable reinforcement categories are
established to maintain the new behaviors. Kanfer and
Phillips (1970) clarified this observational learning
process further by noting that the observer of modeled
behavior benefits most from the modeling if (a) information
presented by the model is explicit, (b) it occurs during
acquisition, and (c) the model increases his own effective
ness over trial blocks.
Alberti and Emmons (19 70) have indicated that a group
atmosphere is effective and possibly superior to individual
treatment in assertive training. A group provides consensus
' 18
for what behavior is appropriately assertive in a situation,
multiple models, and massive social reinforcement. Con
frontation between group members on here-and-now behaviors
may provide opportunities for practicing assertive behavior
"in vivo." Groups of extremely withdrawn individuals may
benefit from nonthreatening warm-up exercises, e.g., greet
tion, and related techniques have enjoyed success in the
modification of a number of problem behaviors (Bandura,
1971; Bandura, Blanchard, & Ritter, 1969). Until recently,
however, controlled empirical studies of the usage of these
techniques for the modification of unassertive behaviors
have been scarce. The following section will present a
review of those studies which have been reported.
•?/• II
20
Controlled Research on Assertive Training
The effects of assertive training and its component
techniques have been examined in a number of group analogue
and clinical outcome studies. Lazarus (1966) conducted one
of the initial studies in the area. He compared the effi
cacy of four 30-minute sessions of behavior rehearsal,
direct advice, and nondirective therapy with respect to
improvement in the management of specific interpersonal
problems. All the subjects in the experiment were clients
of Lazarus. The results revealed that behavior rehearsal
was almost twice as effective as direct advice and the
nondirective treatment procedure fared v/orst of all. The
outcome measure of effectiveness was a statement by the
patient that he or she was behaving adaptively in the area
which had previously been the problem. Lazarus administered
the treatment for the three groups and acknowledged "the
possibility of experimenter bias," but he argued that the
superiority of behavior rehearsal is predicted on a
theoretical basis.
Friedman (1968, 1971) conducted an analogue study in
which the following treatments were compared: modeling,
modeling plus role playing, directed role playing, impro
vised role playing, assertive script, and nonassertive
script. In a treatment period of 8 to 10 minutes per
subject, Friedman shov/ed the subject how to assert himself
21
when harassed by another student in a scene set in a
library. The teaching device was a script containing
the dialogue of the interchange between students.
Primary measures, used pre- and posttest in Friedman's
study were the Action Situation Inventory (ASI) and a Sum
Assertion score (SA). The former was a questionnaire
which consisted of 10 possible threatening behavioral
situations and six alternate reactions to them. Subjects
were to rate the reaction which would best describe their
behavior in the setting (ratings from "not assertive" to
"very assertive"). The SA was a behavioral m.easure con
sisting of ratings by judges on 2 4 categories of the
subject's behavior and an audiotape interaction between
him or her and an accomplice of the experimenter. The
subject was given examples of assertive behavior and told
to act assertively in the ensuing interaction. He also was
told that he was being tape recorded, watched through a
one-way mirror, and being rated. A stressful role play
social situation was then created in which an accomplice
of the experimenter entered a room and obnoxiously inter
fered for 6 minutes with a task on which the subject was
working--solving a cube puzzle. The judges later scored
the subject's behavior in one of 15 categories. Subjects
were included in the experiment who made six or fewer
assertive responses on this measure.
-^mHf0''' -''•mmmmm^mamaKS,.'•
22
There were five treatment conditions and a control
group in Friedman's study: Directed Role Playing, in
which the subjects rehearsed audibly the role of the
harassed student in the presence of an accomplice of the
experimenter who was the instigating student. Subjects
read their responses from a prepared script. The Improvised
Role Playing condition was the same as the previous one
except that the subjects improvised the harassed student's
responses instead of reading them. In the Live Modeling
condition, subjects observed models enacting the role of
harassed and instigating students. Students in the Model
ing and Directed Role Playing condition combined the
activities of the Live Modeling and Directed Role Playing
subjects already described. In the Assertive Script condi-
tion subjects simply read the script. The control group
read scripts not involving assertive behavior.
Differential effects for treatment were demonstrated
only on the behavioral measure (SA). ASI results proved
to be insignificant. According to the SA data, subjects
in all treatm.ent conditions increased in mean assertiveness
scores over those of the controls; however, the Modeling
and Directed Role Playing group subjects, as predicted,
improved most. The second most powerful treatment proved
to be Live Modeling. Interestingly enough, even subjects
who simply read scripts portraying assertive responses
improved significantly in assertiveness.
23
In his discussion, Friedman (19 71) claimed that the
covert rehearsal responses generated by the assertive
information conveyed to the subjects in the modeling,
directed role playing, and assertive script conditions
were presumably used as internal cues for verbal assertive
ness and thus account for most of the changes in these
three conditions.
Wlien m.odeling was combined with directed role playing, the hypothesized mediating variables to account for the efficacy of modeling and directed role playing (covert perceptual cognitive images, covert rehearsal, overt rehearsal) may summate; and consequently foster greater changes in assertiveness than in either of these conditions separately or in the assertive script condition. (1971, p.'l66)
One intriguing aspect of this study is that marked
behavioral changes were obtained vzith only 10 minutes of
treatment. Investigations of behaviors more difficult to
execute are needed before Friedman's conclusions can be
accepted v/ithout reservations.
The major effort to study assertive training pro
cedures experimentally has been undertaken by McFall and
his colleagues at the University of Wisconsin (McFall &
1973). Their basic treatment techniques have been a stan
dardized audiotaped, semi-automated laboratory analogue of
behavior rehearsal. They have employed a consistent
paradigm across studies varying the specific training
24
methods. The target behavior was limited to saying "no"
to unreasonable demands. This has greatly limited the
generalizations which may be drawn from their findings,
but allows for a focused, more precisely measured core
variable.
McFall and his associates are the only researchers in
the area of assertive training who have attempted to system
atically determine which components of assertive training
are more effective.
Tv7o opposing research strategies can be taken in investigating psychotherapy techniques. On the one hand, an investigator can start with a fully developed treatment system and proceed to dismantle it (Lang, 1959), systematically eliminating individual treatment components and measuring the associated decrements in treatment effects. In this manner, the relative contribution of each component to the total system can be assessed. The dismantling strategy is most appropriate for structured and established systems composed of a number of treatment components.
Alternatively, an investigator can follow a constructive strategy. In this case, he starts by isolating the most fundamental or theoretically significant treatment component and assesses its effect on behavior. Then, building on this base, new treatm.ent components are systematically added to determine-whether they significantly enhance the fundamental treatment effects.
Effective components are retained. This constructive strategy is most appropriate for studying complex, nonsystematic techniques that are loosely organized around a central treatment mechanism, e.g., behavioral rehearsal. One advantage of the constructive strategy is that it can lead to the development of an empirically based technique which is ultimately more powerful than the one initially giving rise to the research. (McFall & Marston, 1970, p. 302)
•WF
25
The first study of a series (McFall & Marston, 1970)
compared the effects of behavior rehearsal (with and without
tape-recorded feedback) with placebo therapy and a no-
adversive stimulation, i.e., shakes and DT's, drinking
behavior is automatically and continuously reinforced.
Although this analysis may seem simplistic, it has provided
the basis for a great deal of scientific investigation as
evidenced by an excellent review of 8 8 studies by Cappell
and Herman (1972). They found that the tension-reduction
hypothesis of alcohol has been tested in a wide variety of
experimental situations, in a number of different species
and with varying degrees of sophistication in experimental
methodology and design. Much of the data is equivocal and
sometimes contradictory, although supportive results were
found in the area of conflict and experimental neurosis
(Cappell & Herman, 1972).
/
47
From a social learning point of view, alcoholics are
people who have acquired, through differential reinforce
ment and modeling experiences, alcohol consumption as a
widely generalized response to aversive stimulation (Vogel-
Sprott, 1967). Therapeutic attention would therefore be
most profitably directed toward reducing the level of
aversive stimulation experienced by individuals and toward
eliminating alcohol stress responses either directly or,
preferably, by establishing alternative modes of coping.
Given more effective and rewarding means of dealing with
environmental demands, individuals will have less need to
resort to self-anesthetization against everyday experiences.
Research by Gross and Carpenter (19 71) indicated that
226 hospitalized alcoholics scored significantly lower than
the general population on the E and H factors of the Sixteen
Personality Factor Questionnaire. A person who scores low
on the E factor tends to give v/ay to others, to be docile,
and to conform. He is often dependent, submissive, and
overly accommodating. Similarly a person who scores low
on the H factor tends to be shy, withdrawing, cautious,
restrained, retiring, a "wallflower." He tends to be slow
and impeded in speech and in expressing himself. These two
factors seem to be closely related to the concept of asser
tiveness and unassertiveness. Further research needs to be
conducted to determine if in fact alcoholics are more
assertive than the general population.
48
Drawing on 10 years of research into the psychological
meaning of alcohol consumption, McClelland, David, Kalin,
and VTanner (19 72) have developed a theory of alcoholism
which in some respects gives added validity to the idea of
using assertive training v;ith alcoholic patients. They
attempted to explain som.e of the variations in rates of
heavy drinking in terms of their pov er concern theory. For
example, why should middle-aged men drink more heavily than
younger or older men? They answered rhis question with the
following explanation.
Generally speaking, more strength and assertiveness is expected of mi.ddle-aged men with heavy family and work responsibilities than of either younger or older men. Yet this increase in responsibility is associated with a regular physical decline in potency both in the sexual and aggressive senses of the term. What is more likely than that men faced with high demands for assertiveness and a lessening capacity should turn more often to the artificial sense of increased potency that drinking produces? (p. 296)
McClelland and his associates reported on a pilot
attempt to help alcoholics by socializing their power needs.
Although they arrived at their theory of drinking behavior
quite independently of a behavioristic model, it is interest
ing to note that several of their specialized treatmient
approaches utilized role playing in ccial and interpersonal
situations and other strategies which are not uncommon to
assertive training. Follow-up of four alcoholic subjects
showed that the socialization treatment program "was clearly
49
of some benefit." They called for additional research
comparing their theory of personalized power with other
treatment approaches to see which is more effective.
Many researchers have attempted to define the
"alcoholic personality." However, in 1950, Sutherland,
Schroeder, and Tordella reviewed the literature related
to the hypothesis that alcoholism is caused by personality
traits. They concluded that no satisfactory evidence had
been found to warrant the contention that persons of one
type are more likely to become alcoholics than persons of
another type. In 1957, Syme reviewed another 7 years of
psychological studies and concluded again that there was
no evidence of a definable alcoholic personality upon which
alcoholism is likely to develop. There are, though, certain
characteristics that do appear to be quite common in a
majority of alcoholics. Catanzaro (1968) has enumerated
the following characteristics: (a) anger over dependency,
(b) inability to express emotions adequately, (c) high level
of anxiety in interpersonal relations, (d) emotional imma
feelings of isolation, (j) perfectionism, (k) guilt, (1) com-
pulsiveness, and (m) sex-role confusion. Several of these
characteristics appear to be directly related to the need
for assertive training with alcoholics.
50 /
Inability to express emotions adequately is common in alcoholics, and is also rather prominent in people suffering from depression. Alcoholics are in general very sensitive people. Consequently, they tend to build up feelings of anger at even minor rejections or frustrations. In addition, they find it very hard to deal adequately with their great wealth of angry feelings. They often find it difficult to talk out their feelings, and therefore either hold them inside or explosively let them out in an argument or fight. One of the main aims of therapy is to help the alcoholic learn to express his feelings verbally. (Catanzaro, 1968, p. 16)
Alcohol's ability to reduce a high level of anxiety in personal relations has caused Dr. Jellinek to dub alcohol "a social lubricant." Many alcoholics, early in their disease, use alcohol as a drug for calming anxious and insecure feelings which arise at social gatherings. Thus, as their inability to deal with people effectively becomes more pronounced, they need increasing amounts to blot out their increasingly unpleasant reality. (p. 17)
Feelings of isolation are the natural outgrov7th of his inability to get along with people. As the alcoholic continues drinking, his behavior and conversation become less acceptable to those about him, and consequently, his family and friends begin isolating him from their social circle. (p. 18)
-The three above mentioned characteristics appear to
show that assertive training procedures may be very useful
in developing social and interpersonal skills in alcoholics
By providing alcoholics direct training in precisely those
interpersonal and social skills lacking in their behavior,
it is hypothesized that they will have less need to resort
to alcohol.
Miller, Hersen, Eisler, and Hilsman (1974) attempted
to design a study to evaluate the role of stressful inter
personal encounters on the etiology of alcohol abuse.
51 V
They hypothesized that when confronted with interpersonal
would increase their rate of responding to obtain alcohol
on an operant task. On the other hand, it was hypothesized
that social drinkers would not show this relationship. The
subjects for this experiment consisted of eight alcoholics
and eight nonalcoholics hospitalized at a Veteran's Admin
istration Hospital.
The social stress condition consisted of everyday life
experiences in which the subjects were to act assertively.
After the subjects responded, the experimenter would tell
the subjects that their performance was very poor compared
to other patients and that they apparently have let people
boss them around and that they don't stand up for their
rights. The subjects were then confronted by two experi
menters with their social, parental, or vocational inade
quacies. Pulse rate was obtained immediately prior to and
following these interactions. Both alcoholics and social
drinkers significantly increased their pulse rates as the
function of the stress conditions. The results of the study
revealed that exposure to interpersonal encounters requiring
assertive responses increased alcohol consumption in chronic
alcoholic subjects. By contrast, social drinkers did not
exhibit increased alcohol consumption under stressful
conditions.
52^
These data corroborate findings . . . in that alcoholics do not seem to have a lower tolerance for social stress than non-alcoholics. Rather, as a function of his prior experience, the alcoholics have learned to respond to stressful situations by consuming alcohol whereas the non-alcoholic has learned a variety of more adaptive responses (e.g., being appropriately assertive). (Miller, Hersen, Eisler, & Hilsman, 1974, p. 71)
Martorano (19 74) suggested that if alcoholics were
given an alternative behavior to drinking as a vehicle for
emotional expression, they might be able to decrease their
drinking. In an unique experiment, Martorano set out to
investigate the interrelationships among alcohol consump
tion, mood, and social contact in four male alcoholics.
V7ithin each of three periods (Baseline, Experimental Period
I, and Experimental Period II), 6 days of drinking were
programmed during which subjects could buy alcohol, social
interactions, or closed circuit TV communications time with
points that they had previously earned at the operant console
or by participating in assertive and nonassertive training
tasks. The results showed that assertive training benefited
alcoholic subjects by increasing their social desirability
and activity and by decreasing resentment built up through
suppression of anger. The study also suggested that the
positive changes experienced by these men from assertive
training were not maintained once the drinking began. Fol
lowing assertive training, the men were more likely to
externalize'anger and less likely to feel guilty about it.
53
Since this study utilized a within-subjects, small N design, \ /
the author felt the results of the study should be inter
preted with caution.
Burtle, Whitlock, and Franks (19 74) in a pilot research
project with 16 women alcoholics, indicated that training
and techniques of social interaction played an important
role in the restoration of self-esteem and as a means of
helping women alcoholics maintain their sobriety. Follow-up
questionnaires returned by 10 subjects indicated that some
of the gains from the behavioral program were maintained
after 16 weeks. It is difficult to determine the extent to
which assertive training positively affected the outcome
since the design of the study did not utilize a control
group and assertive training V7as confounded with other be
havioral techniques; however, the results are encouraging.
Eisler, Miller, Hersen, and Alford (19 74) reported the
effects of assertive training on marital interaction. Three
couples were videotaped while discussing their marital con
flicts before and after husbands received training in asser
tive expression. In the context of role-played interpersonal
encounters, assertive training consisted of instructions,
behavior rehearsal, coaching, and feedback. In all three
in the husband's assertiveness. In two of the three cases,
increased assertiveness produced marked changes in the
54 ,/
couple's marital interactions. One of the most interesting
aspects of the author's article was the fact that one of the
husbands had a 6-year history of heavy sporadic drinking
following episodes of intense marital conflict. Several
issues involved in the marital discord were: the discipline
of his 21-year~old retarded daughter, the amount of time
he spent at home with his wife, and frequent arguments about
whether he could have a few beers to relax in the evening
without becoming inebriated. Breath alcohol levels taken
weekly for 6 weeks prior to assertive training ranged from
.01% to .20% with a mean of .08%. For 6 weekly intervals
following training, the levels ranged from .00% to .04% with
a mean of .02%. Thus, it appears that training the husband
to be assertive in simulated marital encounters did general
ize to actual marital interactions. Not only did changes
in the husband's assertive behavior transfer to the inter
action with his V7ife but also they led to a decrease in the
amount of alcohol he consumed. Although this finding
relates to only one case, it is indicative of the potential
effectiveness of assertive training with alcoholics.
Statement of the Problem
Purpose and Scope of the Study
The study had several major objectives. The first
objective was to delineate and better define the parameters
of unassertiveness-assertiveness in alcoholics as compared
55
to normals. The second objective of the study was to
demonstrate that assertive training can be an effective
technique in modifying unassertive behavior in alcoholics.
The design of the study not only attempted to show that
unassertive thoughts and attitudes can be changed, but
that the actual behavior of alcoholics in situations
requiring assertive responses could be modified.
Basically, the study attempted to determine whether
alcoholics can be trained to behave more assertively
following an assertive training program. Because this
study was the first in a planned series of experiments, it
did not answer several important questions. The first of
these questions relates to the issue of transfer of train
ing once the patient has returned to the community. The
second and possibly the most important question is whether
assertive training in fact helps alcoholics maintain their
sobriety. Although this question will not be answered in
the present study, data regarding type, frequency, and
quantity of alcohol consumed were gathered in the hope of
doing a 1 year follow-up on all subjects (see Appendix A).
Importance of the Study
The significance of this study was twofold. First,
it dealt with the nation's third largest health problem.
In this country, the age-old problem of excessive drinking
is taking a disturbing new turn for the v'orsc. In the last
56
10 years, per capita consumption of alcohol in the United
States has increased approximately 26% (Chafetz, 1974).
More and more of the nation's young people are becoming
addicted to the most devastating drug of all—alcohol.
About 1 in 10 of the 95 million Americans who drink are
either full-fledged or at least serious problem drinkers.
The dollar cost of alcoholism may be as much as 25 billion
a year, much of it from lost work time in business, industry,
and government (Chafetz, 1974).
The second major importance of the study was that it
represented a movement av7ay from a generalized treatment
philosophy for alcoholism to a more specific approach which
matches treatment and therapist with client and problem.
It is generally recognized by practitioners in the field
of alcoholism that since multiple factors seem to contribute
to alcoholism, multiple approaches are necessary to promote
human well-being and to enhance human dignity in order to
prevent and treat alcoholism (Chafetz, 1974). Recognizing
the wealth of therapeutic approaches available today for
alcoholic patients, treatment staffs are studying the best
way to assign patients to treatment modes most suited to
their psychological and physical needs. An example of this
viewpoint is a study conducted by Kissin, Platz, and Su
(19 72) entitled "Selective Factors in Treatment Choice and
Outcome in Alcoholics." After an initial social interviev;
•-y:\ -^^ff^\
57
and psychological testing, over 450 alcoholic men were
assigned randomly to one of four treatment conditions. In
general, the investigators found that the success rate of
the treatment condition was directly correlated with the
number of treatment options offered to the patient.
If we conclude that the general population of alcoholics includes different types who would do better in different kinds of treatment, then the more types of treatment offered to a random group, the greater the overall success rate should be. This hypothesis was bcrne out, (Kissin, Platz, & Su, 1972, p, 782)
Kissin's study suggested that an eclectic approach
tailored to individual needs is likely to yield the greatest
benefit to persons abusing alcohol and if treatment programs
are to be truly effective for a large population of their
clients, then specialized and individualized treatments need
to be developed and applied.
b.-..:
CHAPTER II
METHODOLOGY
Subjects
The population from which subjects were selected for
this study was defined by the following criteria: chronic
state hospitalized alcoholics, at least 7 years of school
ing, scoring in the lower 50th percentile on the Rathus
Assertiveness Scale, nonpsychotic, with at least low
average level of verbal functioning. Chronic alcoholism
here implied a relatively long (a year or more) period of
regular alcohol abuse, with the manifestation of withdrawal
symptoms upon termination of drinking episodes. One hundred
and two subjects at two state hospitals were randomly
assigned to the three treatment groups with 34 subjects
in each group. Another and separate group of 123 state
hospitalized alcoholics was randomly chosen as the stan
dardization group for the self-report measure used in this
study.
Instrumentation
Four instruments were used; they were a demographic-
drinking data form, a self-report in nature, a behavioral
measure, and an unobtrusive rating of assertiveness.
Demographic-Drinking Data Form (DDDF). The DDDF
(see Appendix A) v7as developed to secure data relevant to
58
59
a description of the sample as well as to provide baseline
data regarding type, quantity and frequency of alcohol
consumed. This was important for several reasons. First,
it gave relevant data as to the populations to which the
results may be generalized (external validity). Secondly,
the data would be extremely useful in determining which
treatment significantly affected the quantity and frequency
of alcohol consumed should a follow-up be done at a later
time.
Rathus Assertiveness Scale (RAS). Rathus (1973b) " • • • • - I - - - T - T l I I I I • « 11 11 I I J» I I I I I . . I I I. •• _ . . I l l . • • .1 . • _ . . . . . . t J i M
developed a 30-item scale (see Appendix B) that is based
in part on assertive questions previously used by Wolpe
and Lazarus (1966) and Wolpe (1969). Each statement is
rated with a Likert Scale ranging from +3 to -3. The
possible total score can range from -90 to +90. Test-retest
reliability of the RAS was determined by administering the
instrument to 6 8 undergraduate college men and women ranging
in age from 17 to 27, and then retesting them after 8 weeks
passed. The mean pretest score was .2941; the standard
deviation was 29.121. Mean posttest score was 1.6176,and
the standard deviation was 2 7.6 319. A Pearson product-
moment correlation coefficient was run between respondents'
pre- and posttest scores yielding an £ of .7782 (£<.01),
indicating moderate to high stability of test scores over
a 2-month period. Split-half reliability yielded an r of
Vl9f
60
.772 3 (£ < .01) suggesting the quality measured by the RAS
possesses moderate homogeneity.
The validity of the RAS was established by comparing
self-reported RAS scores to two external measure of asser
tiveness. In the first validity study, 6 7 subjects who had
taken the RAS were rated on a 17-item rating schedule by
someone they knew well, A Pearson product-moment correla
tion coefficient was then computed. RAS scores correlated
significantly (£ < ,01) with each of the scales comprising
an assertiveness factor, RAS scores thus serve as a valid
indicator of respondents' assertiveness in terms of the
impression they make on other people (Rathus, 1973b),
Another index of RAS's validity was determined by
comparing subjects' RAS scores with ratings of their re
sponses to five taped interpersonal situations requiring
an assertive response, A Pearson product-moment correlation
coefficient was computed between the RAS scores-and the
scores from the audiotaped sessions yielding an r of .7049
(£ < .01). Thus, RAS scores are also valid in terms of
impartial raters' impressions of the behavior that subjects
report they would exhibit in specific social encounters
(Rathus, 19 73b).
Behavior Assertiveness Test (BAT). Suggested by
similar devices used by McFall and Marston (1970), McFall
and Lillesand (1971), McFall and Twentyman (1973), Friedman
ifi«1
61
(1968), and Eisler et al. (1973), the BAT aimed to assess
the subjects' reactions to role-played threatening or irri
tating social or interpersonal situations involving com
binations of (a) standing up for one's rights, (b) expressing
one's feelings honestly and directly, and (c) showing anger
in a provoking situation. Subjects were presented with 10
tape-recorded stimulus situations (see Appendix C) requiring
assertive responses. They were instructed to respond to
each situation as if it were actually happening to them.
The siibjects' responses were tape-recorded by a
second tape recorder and analyzed at a later date by three
raters. ' The subjects' responses were scored in terms of
response latency, response duration, and on a six point
scale of overall assertiveness (see Appendix D) utilized
by Weiskott (19 75). Since Weiskott showed that the rating
scale of assertiveness had high inter-rater reliability
(ranging from .95 to .97), it was not deemed necessary to
establish inter-rater reliability prior to the actual use
of the instrument in the study. The three raters were given
an intensive 2-hour training session to acquaint them with
the use of the scoring instrument. The possible scoring
for each of the 10 situations ranged from a 6 (a very asser
tive response) to a 1 (a totally unassertive response). The
total assertive score on the BAT could thus range from 60
(perfectly assertive in each situation) to a low of 10
(extremely passive and unassertive in each situation).
62
The response latency for each subject was determined
by totaling the length of time between a bell sounding
(indicating a subject could respond) and when the subject
actually began responding. Each of the 10 role-played
situations allowed the subject a maximum of 20 seconds in
which to make his response. The response duration was
determined by totaling the actual amount of time the
subject spoke during each of the situations.
Since all the previous behavioral role-playing tests
had been constructed for either college students or psy
chiatric populations, it was necessary to construct a
behavioral test which was appropriate for an alcoholic
population. The items for the BAT were selected in several
ways. First, items which had appeared in other behavioral
role-playing tests were used if they were appropriate for
the population of subjects being tested. For example,
situations involving college roommates were excluded.
Secondly, a sample of 45 alcoholics in the state hospital
were asked to write down those situations in their life in
which they had the most difficulty being assertive. Those
situations which appeared most frequently were included in
the study. The following is an example of one item which
appeared in the final version of the BAT.
Narrative: Imagine that this morning you took your
car to a local Exxon station and you
63
explicitly told the mechanic to give you
a simple tune-up. The bill should have
been about $20. It is now later in the
afternoon and you're at the station to
pick up your car. The mechanic is walking
over to you.
Mechanic: "Okay, let me make out a ticket for you.
The tune-up was $12 for parts and $8 for
labor. Uh, grease and oil job was $6.
Antifreeze was $5. Uh, $4 for a new oil
filter. And uh, $5 for rotating the
tires. That's $40 in all. Will this be
cash or charge?"
Bell sounds and subject begins responding.
20 seconds
Stop if you have not finished responding!
Assertive Behavior Index (ABI). This rating instrument
(see Appendix E) was specifically developed for this study.
The instrument attempted to measure a number of verbal and
nonverbal components of assertiveness such as eye contact,
facial expression, body movement, loudness of voice, and
fluency of voice. Each of the eight variables was scored
on a five point scale ranging from -2 to +2. The negative
end of the scale represented the unassertive aspect of the
64
variable while the positive end represented the aggressive
aspect of the variable. The center point (zero) represented
the appropriately assertive aspect of the variable. Possi-
bile scores ranged from -16 to +16.
All subjects, after completion of their 2 weeks in
the study, were individually interviev7ed regarding their
plans for returning home after discharge from the hospital.
These interviews generally lasted about 15 minutes and were
conducted by psychologists, alcoholism counselors, and
social workers not directly related to the study. Upon
termination of the interview, the staff member completed
the ABI, rating the patient's behavior during the previous
interview.
Procedure
Data collection for the investigation was accomplished
during a 5-month period from November, 19 74 through March,
19 75. Prior to the start of the actual study, the Rathus
Assertiveness Scale was randomly given to 123 alcoholics at
three state hospitals. The results of this testing were
tabulated and the standardization/normalization data were
used to spotlight unassertive subjects for inclusion in the
study and to test the first hypothesis. The mean Rathus
Assertiveness score was calculated for this sample of 12 3
alcoholics and found to be -5.04. This information was
subsequently used.to identify patients for inclusion in the
f-wi'-^y;: •^mmmammmmmmm^-"' ''"'•*' -^ws^sm.»i
65
second phase of the study. During a 4-month period,
almost all alcoholic patients at Big Spring State Hospital
and San Antonio State Hospital were administered the RAS.
All subjects were detoxified and free from major physical
problems when the RAS was administered. If a patient
scored -5 (50th percentile) or below on the RAS and met
the other criteria for inclusion in the study, he was
randomly assigned to either one of the two treatment groups
or the control group. The 50th percentile was an arbitrary
cut-off point, but it did help assure that subjects included
in the study tended toward unassertiveness, at least as
measured by the Rathus Assertiveness Scale,
The trainers for the treatment groups consisted of
four Masters level psychologists and counselors, two from
each state hospital. All treatments were conducted by
co-trainers. Prior to the start of the study, the four
trainers were brought.together for an intensive 3-day
workshop on assertive therapy.
Control Group
The subjects in the Control group were allowed to
participate in all alcoholism unit treatment and activities
except those involving assertive training. Subjects in the
Control group were posttested with RAS, BAT, and ABI after
2 weeks. Assertive treatment was not given to the Control
66
s u b j e c t s a f t e r t e r m i n a t i o n of t h e s t u d y s i n c e fo l lov7-up
d a t a w i l l be g a t h e r e d .
Minimal Assertive Training Group * ' " * ' " * * " " •• I • I l i a , • P i l l —T— I • . , • • W B i f c u M . i m i n i ami i — ^ • • • ^ ^ • l ^
Subjects in the Minimal Assertive Training group, in
addition to the regular treatment program, received 2 hours
of didactic presentation and group discussion on hov7 each
person could behave more assertively. This treatment group
was an open-ended group, that is, clients came into the
group and stayed for two sessions. The size of the group
fluctuated from week to week as new clients entered and
other clients who met the criterion of two sessions left.
The first session was an elaboration of the problem. Each
subject explored the situational determinants of his non-
assertiveness, distinguishing when he/she could perform or
could not perform satisfactorily and specifying the critical
factors. Toward the end of the session, the therapist
offered the following general interpretationsof subject's
inhibitions: "You are too concerned with what other people
think of you. You must stop worrying about making everyone
like you and stand up for your rights!" This theme was
elaborated in terms of each subject's particular problem
and each subject was then encouraged to overcome his/her
unassertiveness in daily life activities.
The second session came at least 1 week later and
continued to explore the same basic theme. Successful
67
and unsuccessful attempts made by patients during the week
were discussed and analyzed. Part of the session was
devoted to a didactic lecture on the unassertive-assertive-
aggressive continuum, helping each patient realize situa
tions when he/she could act more assertively. Subjects
were given a common sense explanation of why they behaved
unassertively and they were taught how to discriminate
between assertive and unassertive behavior. They were
strongly encouraged to behave assertively. At the end of
2 weeks, subjects were posttested with the RJ-iS, BAT, and
ABI.
Assertive Training Group
The subjects in this treatment group received, in
addition to the regular treatment program, 10 hours of
assertive training over a 2-week period. This treatment
group was also an open-ended group. Clients entered the
group and stayed for a total of 10 sessions. The size of
the group fluctuated from day to day as new clients
entered and other clients who met the criterion of 10
sessions left. The counselors leading this group utilized
all the components of assertive training: modeling, coach
ing, role playing, role reversal, instructions, behavior
rehearsal, feedback, graded-structured exercises, and
homework assignments. Each subject was asked to discuss
situations in his/her own life which were proving
m^
68
problematic. Much of the focus of this group was to develop
skills in precisely those aspects of unassertiveness in
which the client was having difficulty. Subjects were
given a theoretical rationale for their treatment and they
were strongly encouraged to begin behaving assertively.
At the end of 2 weeks, siobjects were posttested with the
RAS, BAT, and ABI,
Hypotheses
In accordance with the previously stated objectives
of this study, there were four major hypotheses specifically
considered in this experiment. The hypotheses are stated
in the null form,
1. There is no difference between the assertiveness
of alcoholics and that of "normals," as expressed
by scores obtained on the Rathus Assertiveness
Scale.
2. There is no difference between pre- and post-
assertiveness scores, for all the groups as mea
sured by the Rathus Assertiveness Scale,
3. There is no significant difference between groups
regarding the effectiveness of the treatments as
measured by elements of the Behavioral Assertive
ness Test (response latency, response duration,
and total assertiveness scores).
69
4, There is no significant difference betv7een groups
regarding the effectiveness of the treatments as
measured by the Assertive Behavior Index.
Statistical Analyses
The first hypothesis was tested by means of a t test
between the standardization group of alcoholic subjects on
the RAS and a group of college students ("normals") reported
by R.thus (19 73b) . The second hypothesis V7as tested by
using an analysis of covariance design. The third hypothe
sis was tested by a Kruskal-Wallis one-way analysis of
variance by ranks for response latency, follov7ed by the
Mann-Whitney U Test. Response duration and total assertive
ness scores were analyzed by a one-way analysis of variance.
The fourth hypothesis was tested by using a one-way analysis
of variance design. The analyses of the second, third, and
fourth hypotheses V7ere followed by Duncan's Multiple Range
Test (Kirk, 1968). Additional data from the RAS were analyzed
via correlational methods to help determine if age, sex,
number of admissions, length of stay, and educational level
affect assertiveness scores on the RAS.
CHAPTER III
RESULTS
For purposes of clarity, this chapter is divided into
five sections corresponding to the Demographic-Drinking Data
Form and the four stated hypotheses of the study.
Demographic-Drinking Data Form
Relevant means and percentages on the data gathered
from the Demographic Drinking Data Form (DDDF) are presented
in Table 1 for the entire sample of 102 alcoholics involved
in the assertive training component of the research project.
TABLE 1
DEMOGRAPHIC-DRINKING DATA
1. Sex: Male = 85% Female = 1 5 %
2. Mean Educational Level = 11.04
3. Mean Age = 4 7
4. Marital Status: 9% Never Married 2 7% Married Living with Spouse 6% V7idowed
44% Divorced/Annulled 14% Separated
5. Mean number of times clients had been hospitalized for alcohol-related problems during previous 30 days = .66
6. Mean number of days clients had been in state hospitals at the time of the RAS pretest = 8.13 days
70
71
TABLE 1—Continued
7. Mean number of days clients drank during previous 30 days = 20,08 days
The third hypothesis was concerned with the impact of
the assertive treatments on the Behavioral Assertiveness
Test. Since the BAT was composed of three elements, each
is reported separately.
Response Latency
Prior to computing the analysis of variance for
Response Latency, each subject's total latency score in
seconds was transformed by a logarithmic transformation
(x' '-^ log-,f x) to achieve greater normality. The means
77
and standard deviations of the transformed scores are
presented in Table 5.
TABLE 5
RESPONSE LATENCY MEANS AND STANDARD DEVIATIONS FOR TREATMENT AND CONTROL GROUPS
Group Mean SD
Assertive Training
Minimal Assertive Training
Control
1.2445
1.3347
1.4156
.1867
.2086
.2477
*N = 34 for each group.
The results of the analysis of variance for Response
Latency scores are reported in Table 6.
TABLE 6
ANALYSIS OF VARIANCE RESULTS OF RESPONSE LATENCY SCORES FOR TREATMENT AND CONTROL GROUPS
Source
Group
Error
Total
*£ < .006.
Sum of Squares
.498
4.618
5.116
d£
2
99
101
Mean Squares
.249
.046
F
5. 34*
78
Duncan's Multiple Range Test was used to carry out
pair-wise comparisons across groups. The Assertive Train
ing group had a significantly shorter Response Latency than
the Control group (p < .01), but not significantly shorter
than the Minimal Assertive Training group. The means for
the Minimal Assertive Training and Control groups were not
statistically different from each other. The null hypothe
sis of no difference between groups was rejected and the
data were supportive of the effectiveness of Assertive
Training in reducing the Response Latency of subjects on a
role-played test of assertiveness over that of a Control
group,
Response Duration
The means and standard deviations for Response Duration
are presented in Table 7.
TABLE 7
RESPONSE DUR7\TI0N MEANS AND STANDARD DEVIATIONS FOR TREATMENT AND CONTROL GROUPS IN SECONDS
Group Mean SD
Assertive Training
Minimal Assertive Training
Control
8 8 . 1 1
6 5 . 1 1
5 8 . 88
3 4 . 0 9
3 4 . 3 6
3 0 . 8 2
*N = 34 for each group.
79
The results of the analysis of variance for Response
Duration are reported in Table 8.
TABLE 8
ANALYSIS OF VARIANCE RESULTS OF RESPONSE DURATION SCORES FOR TREATxMENT AND CONTROL GROUPS
Source ,^^^ °^ df /^^^ F Squares — Squares —
Group 16122.59 2 8061.29 7.34*
Error 108704.59 99 1098.02
Total 124827.18 101
*£ < .001.
Duncan's Multiple Range Test was used to carry out * -
pair-wise comparisons across groups. The Assertive Training
group spoke significantly longer on the BAT than either the
Minimal Assertive Training or the Control groups (p < .01),
The null hypothesis of no difference between groups was
therefore rejected. The Minimal Assertive Training and
Control groups were essentially statistically similar to
each other. The results of the data were supportive of the
effectiveness of Assertive Training in increasing the quan
tity of verbalization on a role-played test of assertiveness
80
Total Assertiveness Scores
Inter-rater reliability data for the Total Assertive
ness Scores on the BAT are presented in Table 9,
TABLE 9
RATER'S MEANS, STANDARD DEVIATIONS AND INTER-RATER RELIABILITY OF BAT
Rater Mean SD Pearson-Product Moment
Correlations
3 3 . 9 4
3 3 . 4 8
1 1 . 3 0
1 1 , 2 3
Rater 1 with Rater 2 £ = ,9 34
Rater 2 with Rater 3 r = ,9 36
35,43 12,73 Rater 3 with Rater 1 r = ,9 43
It can be seen from the data in Table 9 that there is
a high degree of inter-rater reliability for the Total
Assertiveness scores on the BAT. The Total Assertiveness
Score means and standard deviations for the groups are
presented in Table 10.
TABLE 10
AVERAGE TOTAL ASSERTIVENESS MEANS AND STANDARD DEVIATIONS FOR TREATMENT AND CONTROL GROUPS
Group
Assertive Training
Minimal Assertive Training
Control
*N 34 for each group.
Mean SD
4 2 . 9 1
3 2 . 1 7
2 7 . 5 5
1 1 . 4 0
1 1 . 9 4
1 1 . 6 8
81
Analysis of variance was computed for the Mean
Total Assertiveness Scores on the BAT and the results are
reported in Table 11.
TABLE 11
ANALYSIS OF VARIANCE OF MEAN ASSERTIVENESS SCORES ON THE BAT FOR TREATMENT AND CONTROL GROUPS
Source / ^ °f df /^^^ F Squares — Squares —
Group 4219.19 2 2109.59 23.75*
Error 8800.05 99 88.88
Total 13019.25 101
*£ < .0000001.
Duncan's Multiple Range Test was used to carry out
pair-wise comparisons across groups. Each of the groups was
homogeneous with itself. The Assertive Training group
scored significantly more assertive on the BAT than either
the Minimal Assertive Training or Control groups (£ < .01).
In addition, the Minimal Assertive Training group scored
significantly higher on the BAT than the Control group
(£ < .05). The null hypothesis of no difference between
groups was therefore rejected.
82
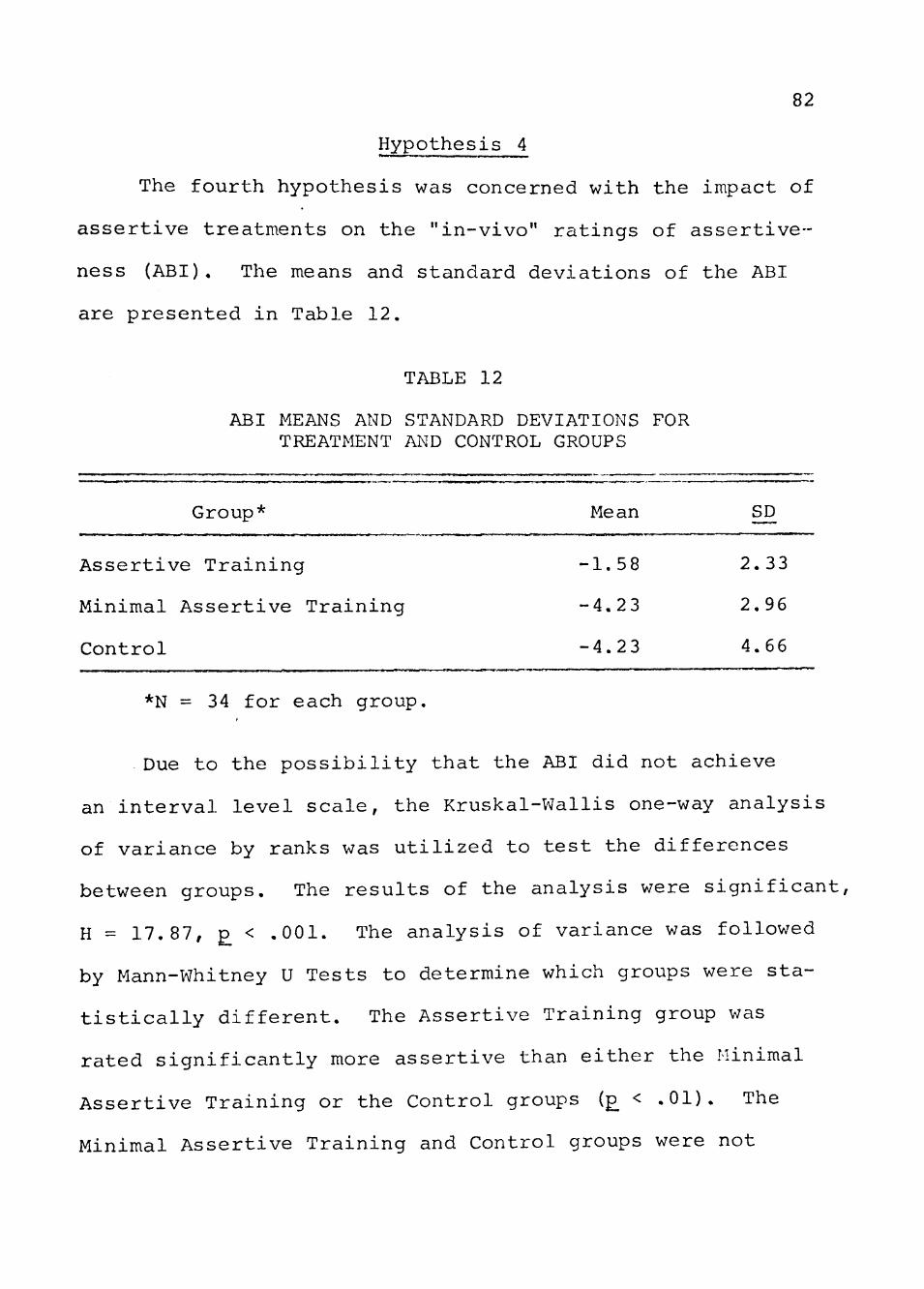
Hypothesis 4
The fourth hypothesis was concerned with the impact of
assertive treatments on the "in-vivo" ratings of assertive
ness (ABI). The means and standard deviations of the ABI
are presented in Table 12.
TABLE 12
ABI MEANS AND STANDARD DEVIATIONS FOR TREATMENT AND CONTROL GROUPS
Group* Mean S£
Assertive Training -1.58 2.33
Minimal Assertive Training -4.23 2.96
Control -4.23 4.66
*N = 34 for each group.
Due to the possibility that the ABI did not achieve
an interval level scale, the Kruskal-Wallis one-way analysis
of variance by ranks was utilized to test the differences
between groups. The results of the analysis were significant,
H = 17.87, £ < .001. The analysis of variance was followed
by Mann-Whitney U Tests to determine which groups were sta
tistically different. The Assertive Training group was
rated significantly more assertive than either the Minimal
Assertive Training or the Control groups (£ < .01). The
Minimal Assertive Training and Control groups were not
83
significantly different from each other. The null hypothe
sis of no difference between groups was rejected.
CHAPTER IV
DISCUSSION
Data relevant to the research hypotheses were presented
in Chapter III. The results obtained were totally congruent
with V7hat had been expected. Discussion of these results
and their implications are presented in two sections: an
investigation cf the data regarding the research hypotheses
is followed by a presentation of the implications for fur
ther research.
Research Hypotheses — i , n i « i » f j « « w , I — ^ w — M .11 <•••••>• in II • •• — • ^ » w < w .11 M lattmi •»
Hypothesis 1
The null hypothesis of no significant differences in
assertiveness between alcoholics and "normals," as measured
by the RAS, V7as accepted. In accepting the null hypothesis,
several considerations need to be kept in mind. First, the
comparison sample of college students (Rathus, 1973b) used
in his study in considerably younger than the mean age of
47 years reported for the present sample of alcoholics. No
data are yet available regarding the relationship of age
and assertiveness in the general population. In addition,
the problems inherently associated ' - h using a relatively
small sample of college students as representative of the
"normal" population speak for themselves. Similarly, there
are external validity problem.s associated with utilizing a
84
85
sample of chronic state hospitalized alcoholics as represen
tative of the total alcoholic population.
Assertiveness as a variable is probably normally dis
tributed in state hospitalized alcoholics. It is likely
that alcoholics do not differ greatly from nonalcoholics in
their capacity to assert themselves and are able to stand
up for their rights without undue anxiety. Some do have
problems being too aggressive or hostile while others are,
conversely, too passive or unassertive. It is this latter
group which was the major focus of this research project.
The fact that state hospitalized alcoholics did not signifi
cantly differ from a comparison group in terms of a self-
report measure of assertiveness does not diminish the
importance of this research. The significance of this
study lies in its movement away from a generalized treatment
orientation for alcoholism to a more focused approach which
matches treatment and therapist with client and.problem.
Several issues surrounding the adequacy of the Rathus
Assertiveness S-cale as a measurement of assertiveness need
to be briefly discussed. First, the RAS is a relatively
gross measure of a person's self-reported attitude toward
his ov7n assertiveness. The extent to which a person's score
may be influenced by social desirability, response set and
the demand characteristics of the setting in which the RAS
is administered is unclear. Each of these factors may
86
contribute to lowered validity. Finally, there exists som.e
degree of disparity between a client's perception or self-
reported attitude of assertiveness and actual behavior as
noted in differences between the RAS, BAT and ABI. Cer
tainly, these factors restrict the generalizability of the
reported results.
Apparently, age, number of admissions,and sex did not
significantly affect the RAS scores in the standardization
sample of 12 3 alcoholics. The general expectation that
women tend to score more unassertively than men did not
materialize for the sample investigated. It is not sur
prising that assertiveness is significantly and positively
correlated with length of treatment (number of days hospi
talized) , since a large component of many treatment orienta-
tions is to encourage clients to be more expressive with
their feelings and to be less inhibited and more outspoken.
The effects of ongoing treatment probably account for the
correlation between RAS scores and number of days hospital
ized. The finding that clients with higher educational
levels tend to be m.ore assertive is interesting. Certainly,
the verbal skills learned in school should make assertive
ness somewhat easier for many individuals. An alternative
explanation may be that the people with higher levels of
education had less difficulty reading the RAS and conse
quently were able to answer the items more assertively.
87
Furthermore, clients with more education would be more
familiar with testing situations. It should be noted that
both the number of years of education and the number of
days hospitalized each account for only 4% of the variance.
Hypothesis 2
The second hypothesis was concerned with the effective
ness of assertive treatment on RAS scores. Although the
three groups were essentially similar prior to the start of
treatment, only the Assertive Training group scored signifi
cantly higher at the time of posttesting. In the course of
10 hours of assertive training, this group averaged one
standard deviation gain on the RAS. The results obtained on
this outcome measure clearly show the superiority of the
Assertive Training group in modifying the self-reported
attitudes of unassertive subjects.
Although the Minimal Assertive Training group showed
some pre-posttest gain on the RAS, it is somewhat surprising
that the group did not gain more than it did. One of the
major reasons for including the Minimal Assertive Training
group in the research design was to evaluate the effective
ness of essentially just telling someone to be more asser
tive and the impact this would have on a person's attitude.
It could also be argued that the small change noted for the
Minimal Assertive Training group is due to the implicit
88
demand characteristics of the experimental paradigm. In
other words, the pretesting experience plus talking about
assertiveness suggest that clients in the Minimal group
should show some improvement on the posttest. Furthermore,
the results from the previous hypothesis related to a slight
increase in assertiveness as a function of length of time
in treatment could also account for the slight pre-posttest
changes exhibited by the Minimal and Control groups. Cer
tainly the results obtained on this measure are totally
congruent with the results reported by Rathus (19 73a) in
which his placebo treatment group showed a similar slight
increase in pre-posttest scores.
Hypothesis 3
The overall results on the Behavioral Assertiveness
Test clearly showed the superiority of the Assertive Train
ing group in modifying unassertiveness in alcoholics. The
results of each element of the BAT will be discussed
separately.
Response Latency. The data on Response Latency
shov7ed that the Assertive Training group had significantly
shorter reaction times to the 10 tape recorded situations
on the BAT than the Control group. Although the Control
and Minimal Assertive Training groups did not significantly
differ from each other, only the difference between Control
and Assertive Training groups reached a significant level
89
(p < .01). It is apparent that the practice and training
received by the Assertive Training group allowed them to
respond to the task more quickly. The fact that the
Assertive Training group showed less hesitation in their
responses suggests that their replies on the BAT were
more accessible and readily available for use in situations
requiring assertive responses.
Response Duration. The subjects in the Assertive
Training group talked significantly longer than either the
subjects in the Minimal or Control groups. The data for
Response Duration are extremely supportive of the effective
ness of Assertive Training in increasing the quantity of
verbalization on a role-played situational test of asser-
tiveness. The Assertive Training group averaged nearly 30
seconds more verbalization than the Control group. It
appears that the behavior rehearsal, modeling and coaching
which the Assertive Training group received significantly
affected the quantity of output on the BAT. Most situations
which require an assertive response cannot be adequately
handled by one- or two-v7ord responses, and persistence is
generally required in order to get one's point across.
The subjects in the Assertive Training group clearly demon
strated their superiority in this area.
Total Assertiveness Scores. The superiority of the
Assertive Training group was again demonstrated, as the
90
results showed that the Assertive Training group was rated
significantly more assertive than either the Minimal or
Control group. In addition, the Minimal Assertive Training
group scored significantly higher than the Control group.
Although both treatment groups gained over the Control
group, the magnitude of change for the Assertive Training
group was dramatic.
It is interesting and somev7hat surprising that the
Minimal Assertive Training gained significantly on this
behavioral measure while not showing such changes on the
self-reported attitudinal measure (PJ S). The significant
increase for the Minimal Assertive Training group over the
Control group on the BAT and not on the RAS might be ac
counted for in terms of the characteristics of the two
measures. The RAS is a self-report attitudinal measure
and may be less sensitive to change than behavioral mea
sures. Similar findings were also reported by McFall and
Marston (1970) and Hersen et al. (1973). There appears to
be some evidence for an "attitudinal lag" on self-report
measures in comparison to more behaviorally oriented mea
sures. Apparently, significant changes occurred for this
group with only 2 hours of treatment. The effectiveness of
discussion, didactic presentation and common sense explana
tions of why one behaves unassertively can be important in
effecting change. The positive change for the Minimal group
91
is consistent with the results reported by Friedman (19 71),
m which marked behavioral changes were obtained with only
10 minutes of treatment.
The use of the EAT as an instrument for measuring
assertiveness in subjects gained validity from this research.
The high inter-rater reliabilities showed that simulated
real-life situations are consistently and reliably obtained
across different raters. It was readily apparent from lis
tening to the tapes that the subjects became very emotionally
involved with the task. From a clinical point of view, the
BAT revealed much more information about the person than his
degree of assertiveness. It also highlighted other clinical
problems. • The manner in which a person dealt with signifi
cant others in his environment can become much clearer in
listening to 10 minutes of the BAT than several hours of
interviews or self-report. Male-female, marriage, and
other interpersonal problems as well as the way in which
a person deals with them stand out clearly in listening
clinically to many of the tapes. The BAT takes a relatively
short amount of time to administer (10 m.inutes) and can pro
vide a wealth of clinical information. After this research
project got underway, it became apparent that the use of
the BAT as a screening instrument would have been more
preferable than using the RAS.
92
The BAT has several features which make its use as a
screening instrument potentially more desirable than the
RAS. First, the client does not have to be able to read.
Secondly, the BAT provides more clinical information and
is usually well accepted by clients. Thirdly, the BAT
appears to tap actual behavior rather than self-reported
attitudes. The potential use of the BAT and similar
devices in treatment programs as a valuable diagnostic tool
cannot be underscored.
Hypothesis 4
The results of the Assertive Behavior Index clearly
demonstrated the superiority of the Assertive Training
group over either the Minimal Assertive Training or Control
groups. The data shov7ed that subjects receiving assertive
training behaved more assertively on a number of nonverbal
and verbal variables, such as eye contact, body language,
voice loudness, etc. While subjects in the Minimal Asser
tive Training group showed a significant increase in asser
tiveness over the Control group on the Total Assertiveness
Score of the BAT, they did not demonstrate this superiority
in an unobtrusive rating situation. In fact, the ABI means
for the Minimal and Control groups were identical. This
suggests that what the Minimal Assertive Training group
learned was a modification of the content of their responses
93
and not what Serber (1972) called a "command of style." He
defined lack of style as the inability to master appropriate
nonverbal, as well as verbal, components of behavior. Thus,
a person may say the right thing but come across in an
unassertive manner.
The feedback modeling, coaching, role playing and
behavior rehearsal received by the Assertive Training group
appears to have made a significant difference in the way
clients came across during the interviews in which they
were rated. The fact that this group of subjects was rated
more assertive has important significance. The 15-minute
interview was a real-life situation and the clients had no
idea that they were being rated. The fact that the ABI was
a nonobtrusive measure suggests that the cognitive or atti
tudinal expectancy effect which could have been operating
in the RAS and BAT would be greatly minimized. In other
words, the clients were not aware that assertiveness was
being evaluated and there was no reason to expect the client
to respond according to his conception of how an assertive
person behaves. Although the time lag between the assertive
training and the interviews was relatively short (several
days), the data are suggestive of transfer of training in
assertive skills.
It should be mentioned that although the ABI raters
were not directly connected with the research study, the
94
possibility of "experimenter bias" cannot be ruled out.
All the raters were full-time staff members on the Alcohol
ism Units and took part in the staffing of clients. It was
not always possible for the rater to rem.ain unaware of
which group a subject was in. The degree to which the
raters knew the client's treatment group and the extent
of bias that this knowledge may have had on the obtained
results cannot be adequately determined.
Theoretical Implications
In contrast to psychoanalysis and other more traditional
psychotherapies which focus on subjective behavior, i.e.,
thoughts and feelings, in order to effect change indirectly
in the client's overt behavior, assertive training focuses
directly on the client's overt behavior. The results ob
tained in this study are quite supportive of behavior therapy
and tend to challenge some of the basic assumptions of tradi
tional psychotherapies. In applying the assertive training
techniques used in this research, no attempt was made to
explore the genesis or dynamics of unassertiveness. In
addition, no effort was made to delve into the childhood
memories, unconscious processes, or client dreams. In fact,
reorganization of the client's personality was not a major
objective of the assertiveness training.
In a departure from "nondirective" psychotherapies,
in which a client is helped to understand the way he feels
95
and, consequently, is free to adopt more appropriate
behavior, assertive training follows through by providing
specific instruction, modeling, and behavior rehearsal.
Not only is a client helped to understand his situation,
but he is provided with specific techniques for the
development of alternative behaviors.
Behavior therapists conceive of psychiatric syndromes
as collections of faulty habits which can be best modified
if they become the direct focus of treatment. The role of
a behavior therapist is to help the client identify the
presenting problem in terms of observable behavior. After
a specific behavior pattern has been determined and the
conditions under which the maladaptive behavior is main
tained, the behavior therapist selects the potentially
most suitable and efficient methods developed and validated
in the experimental laboratory (McFall et al. , 1973). As
demonstrated in this study, this approach can effect signif
icant change within a relatively short period of time.
The assertive training techniques utilized in this
research project have some characteristics in common with
other types of behavior therapy groups. First, the asser
tive training group was organized on the basis that a common
modification technique was applicable to all the members.
Secondly, the group V7as highly structured and goal-oriented
with the primary objective being the amelioration of
96
unadaptive anxiety responses in social and interpersonal
situations. Thus, the goal of the assertive treatment was
similar to what Wolpe and Lazarus discussed (1966) as the
goal for many relaxation and systematic desensitization
groups. The major differences between these approaches
lie in the fact that assertive training techniques stress
an active orientation and the ability to communicate satis
factorily with others.
The assertive training procedures used in this study
also give added validity to the modeling work of Bandura
(1971) and to the skill deficit theories of McFall and his
associates. McFall views unassertiveness as a behavioral
deficit or lack of skill in otherwise normal people who are
over-polite or too civilized. Frequently, an individual is
quite able to engage in significant interchanges without
apparent anxiety, but consistently exhibits a woeful lack
of skill, resulting in failure to satisfy needs. Since the
major thrust of this study's assertive treatment was toward
skill building via coaching, modeling, and behavior rehears
al, the significant results obtained tend to reinforce the
theoretical notions of McFall. Actually, the results of
this study extend the work of McFall and his associates in
the behavioral techniques which they studied, since this
experiment used a more chronic, nonstudent population.
Furthermore, McFall only used semi-automated experimental
97
analogues of more fully developed clinical procedures,
while the assertive treatment in the present study was more
comprehensive in its approach.
The findings of this study are consistent with the
"tension reduction" model of alcoholism (Cappell & Herman,
19 72). Drinking alcohol may be one way that stress-induced
tension can be reduced. V7olpe (1958) views assertive be
havior as being physiologically antagonistic to anxiety and
tension. In the acting out of assertion, there is an
augmentation of the emotion at its core and the strength
this emotion thus acquired may enable it to inhibit the
concurrently evoked anxiety. Assertiveness may function
to reduce the tension build-up in stressful social situations
and consequently lower the need to use alcohol for tension
reduction. Certainly, the results of this study are con
sistent with the previously reported work of Miller,et al.
(1974) and Martorano (1974) in which interpersonal variables
may represent significant factors in determining the alco
holic's drinking as a function of stressful situations.
Programmatic and Research Implications
Recent developments in the application of learning
theory to therapy have been useful in designing behaviorally
oriented ward treatment programs, such as token economies
for the mentally ill and retarded. However, to date there
98
has been relatively little attempt to apply other techniques
of behavior therapy to state hospitalized alcoholics. A
partial explanation of this fact is that behavior modifi
cation techniques are frequently associated in the public
mind with the mechanistic human engineering of Orwell's
19_84_. Behaviorally oriented programs such as token econo
mies and adversive conditioning tend to reinforce the
stereotype of emphasis on external control. However,
clinical techniques developed and used by Wolpe, Lazarus,
and others, such as relaxation, desensitization and asser
tive training, combined with instruction about the affects
of rewards and punishments upon behavior, can greatly
increase clients' control over their internal and external
environments.
Seldom have attempts been made concurrently to train
socially acceptable behaviors in the place of heavy drinking.
This study represents a significant step forward in develop
ing a behavior modification program with an emphasis on
self-control. It has been shown in this study that the
assertive training method is more effective than a minimal
and a no-treatment control in inducing more assertive be
havior in a sample of chronic state hospitalized alcoholics.
It appears that encouraging a client to demand his rights,
to express his feelings, and to be generally outgoing is
certainly a step in the direction of fuller functioning.
99
The repertoire of coping techniques mastered by the asser
tive training groups should assist them in securing greater
satisfaction and gratification when they return home after
their hospital stay. Given more rewarding and effective
means of dealing with their environment, alcoholics should
be better able to maintain their sobriety.
The positive results obtained in this study also have
implications for the future development of alcoholism treat
ment programs. First, the results suggest that if one type
of behavioral program (assertive training) can be effective
in the amelioration of a specific problem area, then other
types of specialized treatment techniques can be developed
and applied. If future alcoholism programs are to be truly
effective for a large proportion of clients, then other
specialized techniques must be researched and adopted. The
need for multidisciplinary staff utilizing a broad range of
proven treatment modalities appears to be the only effec
tive way to treat chronic alcoholism.
Secondly, as more and more alcoholism programs apply
for alcoholism accreditation from the Joint Commission on
Accreditation of Hospitals, there exists a need for better
assessment techniques related to specific client problem
areas. The accreditation standards call for documentation
that individualized treatment plans are based on the
diagnostic assessment of a client's phychological-social
100
needs. The RAS, BAT, and ABI utilized in this study can
provide such documentation and justification. In addition,
the RAS, BAT, and ABI could be used in program evaluation,
also a requirement in the accreditation standards.
Finally, one aspect of the assertive training which
was not revealed in the reported statistics was the manner
in which the patients reacted to the Assertive Training
group. The clients frequently stated that the Assertive
Training group was their favorite group on the unit.
Clients responded well to the training and could readily
identify with the need for assertive training and understand
the relevance of the group to their lives. The quality of
the Assertive Training group was markedly different from
most of the other groups on the units. Clients were
interested and excited about being in the group. There
was a tremendous amount of "esprit de corps" among members
and the quantity and quality of interpersonal relationships
in the group remained consistently high. Members would
frequently volunteer to role-play situations and the amount
of "risking" behavior on the part of clients was, quite
frankly, extremely atypical for this chronic population.
It is noteworthy to mention that when the members of the
Assertive Training group at one hospital learned that the
group leader would be terminated at the conclusion of this
research grant, they started a petition for the hospital
to keep her on permc-inent Jy.
101
The major concern of this investigation was not with
the methodology of assertive training but rather in demon
strating that a relatively short amount of training could
have significant impact on the assertiveness of passive
alcoholics. The comparisons between the Control group and
Assertive Training group were by far the more important in
this study, although if this study were to be replicated,
it might be appropriate to equate the number of hours of
treatment the Minimal and Assertive groups received. It
might be argued by some that the reason the Assertive
Training group did so much better than the Minimal Asser
tive Training group was that its subjects received eight
additional hours of treatment. That possibility certainly
exists, but what is more important is the fact that the
Assertive Training group far exceeded the Control group.
Also related to this issue was the fact that the Minimal
Assertive Training group received no skill training. For
example, they had no opportunity to practice specific
assertive responses. Since the work of McFall and his
associates (1970, 1971, 1973) appears to indicate that
behavior rehearsal is the most powerful component of asser
tive training, the lack of practice rather than the length
of treatment the Minimal Assertive Training group received
might be the important factor.
Several research questions related to the usefulness
of assertive training for alcoholic clients remain to be
102
investigated. This study was limited to demonstrating that
unassertive behavior can adequately be modified through
the component techniques of assertive training. It did
not address itself to the issue of transfer of training
once the client leaves the state hospital and returns to
the community. Do the assertive skills hold up and for
how long? What is the impact of an appropriately assertive
person returning to a family situation in which he had
previously been quite passive? These questions and others
need to be researched in order to more fully evaluate the
effectiveness of assertive training.
The most important aspect of assertive training with
alcoholics is undoubtedly the impact such training has on
the frequency and quantity of alcohol consumed. Does
assertive training lead to a decrease in the amount of
alcohol consumed? Does it help alcoholic clients maintain
their sobriety? This experimenter is hopeful that a 1-year
follow-up will help answer some of these questions. As of
now, they remain unanswered.
Another question regarding assertive training relates
to the types of clinical problems for V7hich these techniques
are appropriate. The focus of this research project was on
the amelioration of unassertive behavior in alcoholic clients
How can aggressive or hostile clients be helped? Are asser
tive techniques useful in changing aggressive/hostile
103
b e h a v i o r i n t o more a p p r o p r i a t e a s s e r t i v e behav io r? There
d e f i n i t e l y e x i s t s a need fo r f u tu r e r e s e a r c h i n t o t h e s e
a r e a s . The f i n d i n g s of t he p r e s e n t s tudy a re indeed h i g h l y
e n c o u r a g i n g , b u t only on the b a s i s of con t inued i n v e s t i
g a t i o n and outcome s t u d i e s can one expec t t o develop an
e f f e c t i v e and e f f i c i e n t t r e a t m e n t for a l coho l i sm.
CHAPTER V
SUMMARY AND CONCLUSIONS
One of the major objectives of this study was to
delineate the parameters of unassertiveness in alcoholics
as compared to normals. A random sample of 12 3 state hos
pitalized alcoholics were chosen as a standardization/
normalization group for the Rathus Assertiveness Scale
(RAS). The RAS is a self-report, paper and pencil measure
of a person's perceived assertiveness. This sample of 123
alcoholics was then compared to a group of college students
(normals). The results of the comparison revealed no
significant differences between assertiveness of state
hospitalized alcoholics and that of normals as measured
by scores obtained on the RAS.
Additional analyses of the data were done to determine
if-'age, sex, number of admissions to state hospital, number
of days in state hospital, and the number of years of edu
cation significantly correlated with the RAS scores in
the sample of alcoholics. The results showed that alco
holic clients tended to become more assertive the longer
they stayed in the state hospital and also that those
clients with higher educational levels tended to be more
assertive.
The second major objective of the study was to demon
strate that assertive training can be an effective technique
104
105
in modifying unassertive attitudes and behavior in alcoholic
clients. The subjects for this part of the study were a
separate group of 102 chronic state hospitalized alcoholics.
An equal number of subjects were randomly assigned into a
Control group. Minimal Assertive Training group and an
Assertive Training group based upon a subject scoring in
the lower 5 0th percentile on the RAS. The Control group
received the regular state hospital treatment program. The
Minimal Assertive Training group, in addition to the regu
lar state hospital program received two hours of didactic
presentation and group discussion on how each person could
behave more assertively. The subjects in the Assertive
Training group, in addition to the regular state hospital
program, received 10 hours of assertive training, utilizing
all the component techniques of assertion training such as
modeling, coaching, role playing, instructions, behavior
rehearsal and homework assignments. Clients in both the
Minimal and Assertive training groups were strongly en
couraged to begin behaving assertively. At the end of
two weeks, all subjects were posttested with the RAS. In
addition, clients were also posttested with a tape-recorded
situational test of assertive behavior and an unobtrusive
rating scale of assertiveness.
The results of the research shov7ed significant
pre-posttest changes for the Assertive Training group on
106
the RAS, but not for the Control or Minimal Assertive
Training groups. On the tape-recorded situational test of
assertive behavior, between group differences revealed a
similar superiority by the Assertive Training group over
the Control group in terms of response latency, response
duration, and ratings of assertiveness. Clients in the
Assertive Training group spoke more rapidly, spoke longer,
and responded more assertively to the role-played threaten
ing or irritating social and interpersonal situations they
encountered on the tape recorded task. In addition, the
Minimal Assertive Training group significantly improved
their assertiveness over the control group in their ratings
of assertiveness. Their improvement, however, was much
less dramatic than the Assertive Training group.
The final outcome measure used in the study consisted
of a rating instrument which attempted to measure a number
of verbal and nonverbal components of assertiveness, such
as eye contact, body posture, facial expressions, loudness
of voice, and voice rhythm. Each client V7as interviewed
regarding plans for returning home after discharge from the
hospital. The staff ratings of assertiveness showed signif
icant improvement for the Assertive Training group over
either the Minimal or Control groups. The overall results
of the study clearly demonstrated that group assertive
training can be an effective therapeutic technique for
rx;)difying unassertive attitudes and behavior in alcoholics.
107
Although this study did not directly address itself
to the issue of tremsfer of assertive skills once a client
leaves the state hospital and the effect such skill train
ing has on future alcohol consumption, the results are
extremely suggestive of the potential usefulness of asser
tion training in the treatment of alcoholism. It is hoped
that by providing unassertive alcoholics with the social
and interpersonal skills necessary to cope more effectively
with their environment that they will have less of a need
to resort to self-anesthetization and escape from everyday
life experiences. If alcoholics are given alternative
behaviors to drinking as a vehicle for emotional expression,
they might be able to decrease their drinking and to lead a
more comfortable, rewarding life.
REFERENCES
Alberti; R., & Emmons, M. Your perfect right. San Luis Obispo: Impact Books, 1970". ' ''
Bandura, A. Principles of behavior modification. New York: Holt, Rmehart, and Winston, 19 69.
Bandura, A. Psychotherapy based upon modeling principles. In A. E. Bergin & S. L. Garfield (Eds.), The handbook o^ psychotherapy and behavior change. New York:"~JoFn Wiley and Sons, 19 71.
Bandura, A., Blanchard, E. B., & Ritter, B. The relative efficacy of desensitization and mtodeling approaches for inducing behavioral, affective and attitudinal changes. Journal of Personality and Social Psycholoqy, 19 69, 12, TTT^lT. "' • — ' ^~
Bates, H. D. , &• Zimjnerman, S. F. Toward the development of a screening scale for assertive training. Psychological Reports, 1971, 2_8, 99-107. ^
Bergin, A. E. The evaluation of therapeutic outcomes. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of Psychotherapy and behavior change. New York: John Wiley and Sons, 19 71. '' "
Blake, B. G. The application of behavior therapy to the treatment of alcoholism. Behavior Research and Therapy, 1965, 3, 75-85.
Blake, B. G. A follow-up of alcoholics treated by behavior therapy. Behavior Research and Therapy, 196 7, 5, 89-94. ' " """
Burtle, v., V7hitlock, D. , & Franks, V. Modification of low self-esteem in women alcoholics: A behavior treatment approach. Psychotherapy: Theory, Research, and Practice, 1974, _11, 36-40.
Cappell, H. , & Herman, P. Alcohol ai J! tension reduction. Quarterly Journal of Studies on Alcohol, 19 72, 33, 33-64.
Catanzaro, R. J. Alcoholism: The total treatment approach. Springfield, 111.: Charles C ThoTiia's, 1968.
108
109
Chafetz, M. E. Alcohol and health: New knowledge. (USDHEW), preprint edition, June, 1974, NIAAA, Stock No. 1724-00399.
Conger, J. Alcoholism: Theory, problem, and challenge. II._ Reinforcement theory and the dynamics of alcoholism. Quarterly Journal of Studies on Alcohol, 1956, 17_, 2^6-36T, ' "
Corsini, R. Roleplaying in psychotherapy: A manual. Chicago: Aldine, 1966.
Doering, M., Hamlin, R., Everstine, L., Eigenbrode, C., Chambers, G., Wolpin, M., & Lackner, F. The use of training to increase intensity of angry verbalization. Psychological Monographs, 1962, 7£v37, V7hole No. 556).
Edwards, N. B. Case conference: Assertive training in a case of homosexual pedophillia. Journal of Behavior Therapy and Experimental Psychiatry, 1972, 2^ 55-63.
Eisler, R. M. , Miller, P. M., & Hersen, M. Components of assertive behavior. Journal of Clinical Psychology, 1973, 2^(3), 295-299. ~" "
Eisler, R. , Hersen, M. , & Miller, P. Effects of modeling on components of assertive behavior. Journal of Behavior Therapy and Experimental Psychiatry^ r9"73, £, 1-6. "" "^
Eisler, R. M., Miller, P. M., Hersen, M., & Alford, H. Effects of assertive training on marital interaction. Archives of General Psychiatry, 1974, 3£' 643-649.
Eisler, R. M., & Hersen, M. Behavioral techniques in family oriented crisis intervention. Archives of General Psychiatry, 1973, 2 ./ 111-116.
Ellis, A. Reason and emotion in psychotherapy. New York: Lyle Stuart, 1962.
Elms, A. Roleplaying, reward, and attitude change. New York: Van Norstrand, 1969.
Fensterheim, H. Behavior therapy: Assertive training in groups. In C. J. Sager & H. S. Kaplan (Eds.), Progress in group and family therapy. New York: Brunner/Mazel, TTTT.
110
Friedman, P. H. The effects of modeling and roleplaying on assertive behavior. Unpublished doctoral thesis. University of Wisconsin, 196 8.
Friedman, P. H. The effects of modeling and roleplaying on assertive behavior. In C. M. Franks (Ed.), Advances in behavior therapy. New York: Academic Press", 19 71.
Galassi, J., DeLo, J., Galassi, M., & Bastien, S. The college self-expression scale: A measure of assertiveness. Behavior Therapy, 1974, £, 165-171.
Gross, W. F., & Carpenter, L. L. Alcoholic personality: Reality or fiction? Psychological Report, 1971, 28, 375-378. "
Guilford, J. P. Fundamental statistics in psychology and education. New York: McGraw-Hill, 1965.
Hedquist, F. J. , & V7einhold, B. K. Behavioral group counseling with socially anxious and unassertive college students. Journal of Counseling Psychology, 19 70, r7, 237-242.
Hersen, M., Eisler, R. M., & Miller, P. M, Development of assertive responses: Clinical measurement and research considerations. Behavior Research and Therapy, 19 73, Ij., 505-521.
Hersen, M., Eisler, R., Miller, P., Johnson, M., & Pinkston, S. Effects of practice, instructions, and modeling on components of assertive behavior. Behavior Research and Therapy, 1973, 1_1, 443-451.
Kanfer, F., & Phillips, J. Learning foundations of behavior therapy. New York: John Wiley and~Sons, 19 70"
Kirk, R. E. Experimental design: Procedures for the behavioral sciences. Belmont, Calif,: Brooks/Cole, 1968.
Kissin, B., Platz, A., & Su, W. H. Selective factors in treatment choice and outcome in alcoholics. In N. K. Mello and J. H. Mendelson (Eds.), Recent advances in studies of alcoholism. Washington, D.C.: U.S. Govern-inent Printing Office, 19 72.
Lang, P. J. The mechanics of desensitization and the laboratory study of human fear. In C. M. Franks (Ed,), Behavior therapy: Appraisal and status. New York: McGraw-Ki i r ; l9"69.
Ill
Lazarus, A. A. Behavior rehearsal vs. non-directive therapy vs. advice in effecting behavior change. Behavior Research and Therapy, 1966, £, 209-212.
Lazarus, A. A. Behavior therapy and beyond. New York: McGraw-Hill, 1971. ~~~
Lewinsonn, P. M. , Weinstein, M. S., & Alper, T. A. Behavioral approach to the group treatment of depressed persons: A methodological contribution. Journal of Clinical Psychology, 1970, 2^^, 525-532.
Lisansky, E. Clinical research in alcoholism and the use of psychological tests: A reevaluation. In R. Fox (Ed.), Alcoholism: Behavioral research and therapeutic approaches. New York: Springer Publishing Co., 1967, 3-15.
Lomont, J., Gilner, F., Specter, N., & Skinner, K. Group assertion training and group insight therapies. Psychological Reports, 1969, Z5, 463-470.
Martinson, W. D., & Zerface, J. P. Comparison of individual counseling and a social program with nondaters. Journal of Counseling Psychology, 1970, Yl, 36-40.
Martorano, R. Mood and social perception in four alcoholics: Effects of drinking and assertion training. Quarterly Journal of Studies on Alcohol, 1974, 3_5.' 445-457.
McFall, R. M., & Lillesand, D. V, B. Behavioral rehearsal with modeling and coaching in assertive training: Assessment and training stimuli. (Mimeographed) University of Wisconsin, 1970.
McFall, R. M., & Lillesand, D. V. B. Behavior rehearsal with modeling and coaching in assertion training. Journal of Abnormal Psychology, 1971, 7_7/ 313-323.
McFall, R. M., & Marston, A. R. An experimental investigation of behavior rehearsal in assertive training. Journal of Abnormal Psychology, 1970, 76_, 295-303.
McFall, R. M., & Twentyman, C. T. Four experiments on the relative contributions of rehearsal, modeling, and coaching to assertion training. Journal of Abnormal Psychology, 1973, 8^, 199-218.
112 McClelland, D. C , Davis, W. N., Kaline, R. , & Wanner, E.
The drinking man. New York: The Free Press, 1972.
Meichenbaum, D. Cognitive factors in behavior modification: Modifying what clients say to themselves. Paper presented at Association for Advancement of Behavior Therapy. Washington, D.C., 1971.
Miller, A. G. Role playing: An alternative to deception? A review of the evidence. American Psychologist, 1972, 22, 623-636. ^
Miller, P. M. , Hersen, M., Eisler, R. M., & Hilsman, G. Effects of social stress on operant drinking of alcoholics and social drinkers. Behavior Research and Therapy, 1974, L2, 67-72. '
Moreno, J. Psychodrama. Vol. I. New York: Beacon House, 1946.
Neuman, D. Using assertive training. In J. D. Krumboltz & E. C. Thorenson (Eds,), Behavioral counseling: Cases and techniques. New York: Holt, Rinehart, and Winston, 1969, 433-441.
Patterson, R. L. Time-out and assertive training for a dependent child. Behavior Therapy, 1972, 2/ 466-468,
Piaget, G., & Lazarus, A. A. The use of rehearsal-desensitization. Psychotherapy, Research and Practice. 1969, 6_r 264-266.
Rathus, S. A. An experimental investigation of assertive training in a group setting. Journal of Behavior Therapy and Experimental Psychiatry, 1972, 2/ 81-86.
Rathus, S. A. Investigation of assertive behavior through videotape-mediated assertive models and directed practice. Behavior Research and Therapy, 1973, 12' 57-65. (a)
Rathus, S. A. A 30-item schedule for assessing assertive behavior. Behavior Therapy, 1973, A_, 398-406. (b)
Rehm, L. P., & Marston, A. R. Reduction of social anxiety through modification of self-reinforcement: An instigation therapy technique. Journal of Consulting and Clinical Psychology, 1968, 3Tr'565-574.
113
Salter, A. Conditioned reflex therapy. New York: Capricorn Books, 1949, 1961.
Serber, M.^ Teaching the nonverbal components of assertive training. Journal of Behavior Therapy and Experimental Psychiatry, 1972, 2/ 179-183.
Smith, M. S. When I say no, I feel guilty. New York: The Dial Press, 1975. ~"
Spence, J. Behavior therapy and the treatment of anxiety: The role of instrumental response. Paper given at American Psychological Association, Washington, D.C., 1971.
Syme, L. Personality characteristics and the alcoholic: A critique of current studies. Quarterly Journal of Studies on Alcohol, 1957, 12' 288-302.
Strum, I. E. Implications of role playing methodology for clinical procedure. Behavior Therapy, 1971, 2^, 88-96.
Strum, I. E. Behavioristic aspects of psychodrama. Group Psychotherapy, 1965, 12, 50-64.
Sutherland, E. H. , Schroeder, H. G., & Tordella, C. L. Personality traits and the alcoholics; a critique of existing studies. Quarterly Journal of Studies on Alcohol, 1950, 11./ 547-561.
Veldman, D. J. Fortran programming for the behavioral sciences. New York: Holt, Rinehart, and Winston,1967 .
Vogel-Sprott, M. Alcoholism a learned behavior: Some hypotheses and research. In R. Fox (Ed.), Alcoholism: Behavioral research and therapeutic approaches. New York: Springer Publishing Co., 1967, 46-54.
Wagner, M. K. Comparative effectiveness of behavioral rehearsal and verbal reinforcement for effecting anger expressiveness. Psychological Reports, 1968, 22, 1079-1080. (a)
Wagner, M. K. Reinforcement of the expression of anger through role playing. Behavior Research and Therapy, 1968, 6, 91-96. (b)
114
Webb, E. J., Campbell, D. T., Schwartz, R. D., & Sechrest, L. Unobtrusive measures: Non-reactive research in the social science"sT Chicago: Rand McNally and Company, 1966.
Weinman, B., Selbert, P., Wallace, M., & Post, M. Inducing assertive behavior in chronic schizophrenics. Journal of Consulting and Clinical Psychology, 1972, 2i' 246-252.
Weiskott, G. Assertiveness, territoriality, and personal space behavior as a factor of group assertive training with a college population. Unpublished doctoral dissertation, The University of Texas at Austin, 1975.
Wolpe, J. Psychotherapy by reciprocal inhibition. Stanford: Stanford University Press, 1958,
Wolpe, J. The practice of behavior therapy. New York: Pergammon Press, 1969.
Wolpe, J. The instigation of assertive behavior: Transcripts from two cases. Journal of Behavior Therapy and Experimental Psychiatry, 1970, 1_, 145-151.
Wolpe, J. Neurotic depression: Experimental analog, clinical syndromes, and treatment. American Journal of Psychotherapy, 1971, 25.' 362-368.
Wolpe, J,, & Lazarus, A, A. .Behavior therapy techniques. Oxford: Pergammon Press, 1966,
Yalom, I. D. The theory and practice of group psychotherapy. New York: Basic Books, 1970.
Yates, A. J. Behavior therapy. New York: Wiley, 1970.
B. HOW many days did client drink during the past 30 days?
117
6. DRINKING QUANTITY AND FREQUENCY
A. About how often did client drink during the past 30 days:
BEER
Every day 5-6 days a week 3-4 days a week 1-2 days a week Less often than weekly None
WINE
Every day 5-6 days a week 3-4 days a v/eek 1-2 days a week Less often than weekly None
LIQUOR
Every day 5-6 days a week 3-4 days a week 2-2 days a week Less often than weekly None
(NOTE TO INTERVIEWER: Be sure to complete quantity for each type of drink.)
B. About how much did client drink in a typical day in which he drank?
BEER 6 quarts or more '5 quarts "4 quarts "3 quarts "1-2 quarts '1-3 glasses None
V7INE 5 fifths or more "3-4 fifths '2 fifths '1 fifth '2 water glasses or '3-5 wine glasses 1 water glass or '1-2 wine glasses None
LIQUOR 4 pints or more '3 pints '2 pints "l pint '8-10 shots or drinks '5-7 shots or drinks '3-4 shots or drinks '1-2 shots or drinks 'None
118
NOTE TO INTERVIEWER:
1 quart = three 11 oz. bottles (cans) or four 8 oz. glasses
1 fifth is a standard size bottle and is equal to about three 8 oz. water or six 4 oz. wine glasses. There are 5 fifths in a gallon or 2 1/2 fifths to a half gallon.
1 pint. = 16 oz. or just over ten 1 1/2 oz. shots. There are 2 pints in 1 quart and a little over 1 1/2 pints in a fifth.
7. BEHAVIORAL ASPECTS OF DRINKING
A. Number of times drunk
None 1-4 ^ 5-10 More than 10
E. Longest period between drinks
12 hours or more Less than 12 hours
C. Longest period of continued drinking
Less than 6 hours 6-12 hours More
than 12 hours
D. Number of days had a drink upon awakening
None 1-4 5-10 More than 10
E. Meals missed because of drinking
None 1-4 5-10 _More than 10
F. Drinking alone or with others
None Mostly with others Sometimes
alone, sometimes with other- _Mostly alone
G. Number of mem.ory lapses or "blackouts"
None 1-2 3-5 More than 5
119
H. Number of times had the "shakes"
l^one 1-2 3-5 More than 5
I. Number of nights had difficulty sleeping
None 1-2 3-5 More than 5
J. Number of quarrels with others while drinking
None 1-2 3-5 More than 5
K. Drinking while on job/during daily activities
No Yes
L. Days of work missed/days of inactivity because of drinking
None 1-2 3-5 More than 5
120
APPENDIX B: RATHUS ASSERTIVENESS SCALE
Age: Sex:
Approximately how many days have you been in the state hospital? Approximately how many times have you been admitted to the state hospital? Circle the last school grade you completed: 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Directions: Indicate how characteristic or descriptive each of the following statements is of you by using the code given below. Please answer each question as honestly as you can,
a +3 very characteristic of me, extremely descriptive +2 rather characteristic of me, quite descriptive +1 somewhat characteristic of me, slightly descriptive -1 somewhat uncharacteristic of me, slightly non-
descriptive -2 rather uncharacteristic of me, quite nondescriptive -3 very uncharacteristic of me, extremely nondescriptive
1. Most people seem to be more aggressive and assertive than I am.*
2. I have hesitated to make or accept dates because of shyne s s.*
3. When the food served at a restaurant is not done to my satisfaction, I complain about it to the waiter or waitress,
4. I am careful to avoid hurting other people s feel-ings, even when I feel that I have been injured.*
5. If a salesman has gone to considerable trouble to show me merchandise which is not quite suitable, I have a difficult time saying "No."*
6. When I am asked to do something, I insist upon knowing why.
7. There are times when I look for a good, vigorous argument.
8. I strive to get ahead as well as most people m my position.
9 To be honest, people often take advantage of me, 10. I enjoy starting conversations with new acquaint
ances and strangers. ^^^^^^ 11. I often don't know what to say to attractive persons
of the opposite sex.* -,-, ^ v. • ^r-c. 12. I will hesitate to make phone calls to business
establishments and institutions.*
121
13. I would rather apply for a job or for admission to a college by writing letters than by going through with personal interviev7S. *
14. I find it embarrassing to return merchandise.* 15. If a close and respected relative were annoying me,
I would smother my feelings rather than express my annoyance.*
16. I have avoided asking questions for fear of sounding stupid.*
27. During an argument, I am sometimes afraid that I will be so upset that I will shake all over.*
18. If a famed and respected lecturer rr.akes a statement which I think is incorrect, I will have the audience hear my point of view as well.
19. I avoid arguing over prices with clerks and salesmen.*
20. When I have done something important or worthwhile, I manage to let others know about it.
_21« I am open and frank about my feelings. 22. If someone has been spreading false and bad stories
about me, I see him (her) as soon as possible to "have a talk" about it.
23. I often have a hard time saying "No."* 24. I tend to bottle up my emotions rather than make a
scene,* 25. I complain about poor service in a restaurant and
elsewhere. 26. When I am given a compliment, I sometimes just
don't know V7hat to say.* 27. If a couple near me in a theatre or at a lecture
were conversing rather loudly, I would ask them to be quiet or to take their conversation elsewhere.
28. Anyone attempting to push ahead of me in a line is in for a good battle.
29. I am quick to express an opinion. '30. There are times when I just can't say anything.*
^Total score obtained by adding numerical responses to each item after changing the signs of reversed items.
*
Reversed item.
122 APPENDIX C: BEHAVIORAL ASSERTIVENESS TEST
1"
The purpose of today's procedure is to find out how you react to some, ordinary everyday situations that might happen outside the hospital. The idea is for you to respond just as if you were actually in that situation, whether at home, in a store or in a restaurant. For example, if I say that you are in a restaurant and the waitress approaches, try and imagine that you are really there.
I will narrate and describe a numuber of different situations After I have described a scene, one of the characters will speak to you. Ac: soon as this person is finished speaking, you will hear a bell. Immediately after hearing the bell,.I want you to respond to that person and say what you normally would say if you were in that situation. If you have any questions, be sure to ask them nov7 because once we start the person running the tape recorders will not be able to answer you.
(PAUSE)
Let's have one practice exercise to be sure you understand the instructions. Remember to respond as if you were really there in each situation.
(PRACTICE EXERCISE)
Narrator:
Wife:
You have just come home from a hard day's work dead tired. Your wife informs you that she has accepted an invitation for you both to visit some friends that evening. You are definitely not in the mood to go out.
"I just knew that you'd like to visit tonight, let's go right after dinner."
1, Narrator
Daughter
You are in the middle of watching your favorite TV show. Your daughter walks in and changes the TV channel as she does everytime you are watching TV.
"Let's V7atch this movie instead; it is suppose to be real good."
123 2. Narrator: This morning you took your car to the local
Exxon station and you clearly told the mechanic to give you a simple tune-up. The bill should have been around $20. It is now later in the afternoon and you are at the station to pick up your car. The mechanic IS walking over to you.
:l£2ll?-ili5_- "OK, let me make out a ticket for you. The tune-up was $12 for parts and $8 for labor. Uh, grease and oil job was $6. Antifreeze was $5. Uh, $4 for a nev7 oil filter, and uh, $5 for rotating the tires. That's $4 0. in all. Will this be cash or charge?"
- Narrator: You're in a restaurant with some friends. You order a very rare steak. The waitress brings a steak to the table which is so well done that it looks burned.
Waitress: "I hope you enjoy your dinner."
^' Nar.rator: You are in a crowded grocery store and are in a hurry. You had picked up one small item and you get in line to pay for it when a woman with a shopping cart full of groceries cuts in line right in front of you.
Woman: "You won't mind if I cut in here, will you? I*m late for an appointment,"
5. Nar.rator: Suppose you worked part-time in an office in the afternoon. At 4:35 one afternoon, as you v/ere looking forward to going home and anticipating your evening out wich some friends, your boss asked you to work overtime for that evening.
2oss^; "Vyould you mind working overtime this evening?"
6. Narrator: You almost finished painting some furniture v/hen you suddenly realize that you won't have enough to finish the job. The salesman at the hardware store W-:ongly advised you that a quart would be sufficient. You get in your car and rush back to the hardware store to buy another pint and arrive a few minutes before closing.
124
Salesman: "I'm sorry but you will have to come back tomorrow. I'm trying to close up a few minutes
Narrator:
8
Spouse:
Narrator:
Mechanic
Narrator
early today."
You have just punished your child for his inconsiderate behavior and told him that he must stay in his room for the rest of the afternoon. Your spouse feels sorry for him and tells him that he can go out and play,
"It's so nice outside; it is a shame to make him stay in his room,"
You left your car at 9:00 in the morning at the Goodyear Tire Dealer for a new set of tires. At 4:30 that afternoon you call to see if it is ready and they told you tliat it v/as. A friend, V7ho is going nearby, gives you a ride to the Goodyear Dealer and then leaves before you get your car, figuring that it would be ready.
"The blue Chevy? Nah, it's not ready. Come back tomorrow and we will have it ready for ya."
You go to a ball game with a reserved seat ticket. When you arrive you find a man has put his coat in the seat for which you have a reserved ticket. You ask him to remove his coat, and he tells you he is "saving that seat for a friend."
10
Man:
Narrator
Friend:
"I'm sorry that seat is saved."
You are talking with a friend who the night before embarrassed you at a party by revealing a very personal and confidential story you had told her sometime ago in private,
"Sorry I embarrassed you, but I just had to tell them, I mean it was such a funny story and well, sometimes I think you are too darn sensitive."
125
APPENDIX D: SCORING SHEET FOR BEHAVIOR ASSERTIVENESS TEST
fident; shows appropriate emotions spontaneously; pursues his demand or initiation strongly, recognizing reasonable limits; is insistent without being overbearing or self-righteous; his content is quite substantial or convincing.
A somewhat assertive response; the subject exhibits some confidence; shows guarded emotion; repeats a demand with some development of content; pushes his point, but not really enough; his content is moderately convincing.
A mildly assertive response; the subject simply states his demand or makes his initiation without much confidence or effect; the response, although assertive, is either very brief or very long, with the attitude of "trying to explain"; content is on the shallow side.
126
3 =? A mildly unassertive response; the subject shows some passivity; may induce some guilt in partner; is indirect in responding; content is on the shallow side; he is slightly hesitant; pursues his demand or initiation very awkwardly.
2 = A cover-up unassertive response; the subject anxiously repeats himself or i¥ jocular; gives phony, "hot-air" responses; finds some cause for agreement; shows a number of passive-aggressive signs; sounds like he's having difficulty handling the situation.
• ~ Totally unassertive response; the subject does not respond; gives an irrelevant response; is extremely passive-aggressive; completely fails to exercise his rights or initiate an interaction; agrees completely with partner.
127
APPENDIX E: ASSERTIVE BEHAVIOR INDEX
Date
Interviewer's Name_ Patient's Name
Before the_interview, read over the various categories of behavior listed below. Do not fill out this form durina the interview but keep the categories in your mind as you interview the patient. At the end of the interview, please complete the form. (Be sure to rate the patient in each of the eight areas listed below.) You have five possible~responses to choose from in each C£*tegory. Place a check mark (/) in the column which you feel best describes or captures the patient's behavior during the interview. (Make only one check mark for each category.)
!• Eye Contact: avoids contact most of time avoids contact sometimes ^appropriate frequently" staring ^constantly staring