48
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
| Date post: | 26-Mar-2018 |
| Category: |
Documents |
| Upload: | vuongkhanh |
| View: | 216 times |
| Download: | 0 times |

Critical Care in
Obstetrics:
An Innovative and Integrated Model for
Learning the Essentials

Peripartum Cardiomyopathy
Leo R. Brancazio, M.D.
Division of Maternal-Fetal Medicine
Department of Obstetrics & Gynecology
Duke University Medical Center

I have no conflicts of interest to disclose
I will be discussing one off-label or
investigational drug: bromocriptine in the
management of peripartum cardiomyopathy
Disclosure

Learning Objectives
Background
Etiologies/ Pathophysiology
Diagnosis
Treatment/ Management
Prognosis/ Future Pregnancies
Summary
Evidence
Outline

Review current epidemiology of
peripartum cardiomyopathy (PPCM)
Understand pathophysiology of PPCM
Discuss signs, symptoms, and diagnosis of
PPCM
Discuss management and prognosis of
PPCM
Learning Objectives

Background

Development of heart failure in last month of
pregnancy or up to 6 months postpartum
Absence of preexisting heart disease
Indeterminate cause
Echocardiographic findings
(a, together with b or c; or all 3)
A. LV end-diastolic dimension >2.7 cm/m2
B. M-mode fractional shortening < 30 %
C. LV ejection fraction < 0.45%
Diagnostic Criteria
Demakis, J. G., & Rahimtoola, S. H. (1971). Peripartum cardiomyopathy. Circulation, 44(5), 964-968.
Manolio, T. A., Baughman, K. L., Rodeheffer, R., et al. (1992). Prevalence and etiology of idiopathic dilated
cardiomyopathy (summary of a National Heart, Lung, and Blood Institute workshop. Am J Cardiol, 69(17), 1458-1466.

True incidence unknown
Wide variation worldwide
Population differences
Estimates 18-333/100,000 births
In the United states: ~ 1/2066-1/4025 live
births
Clinical presentation highly variable
Incidence
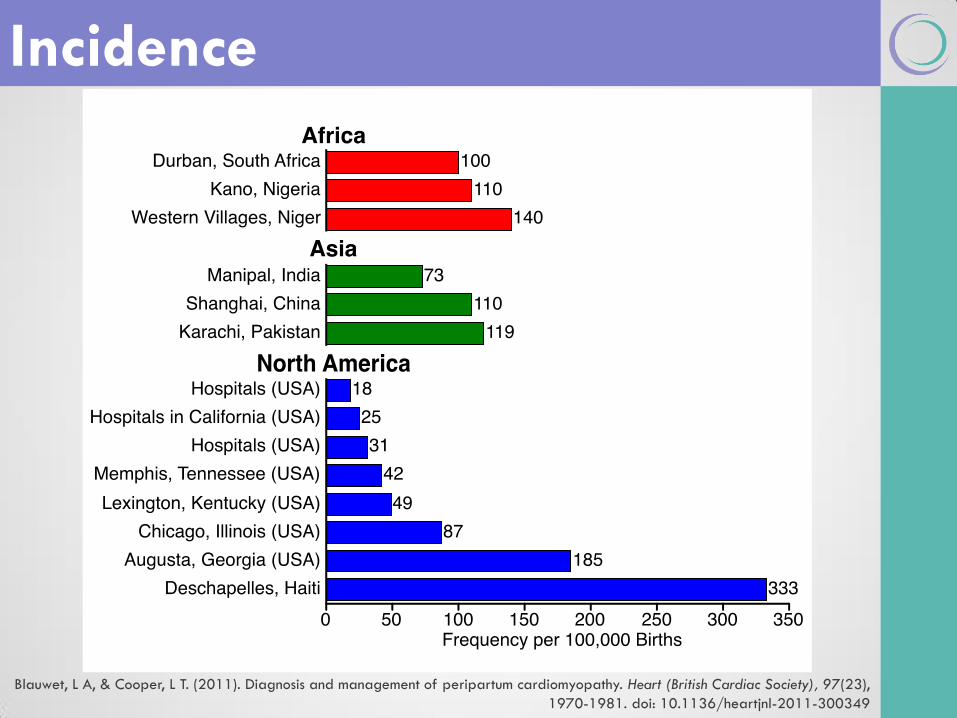
Blauwet, L A, & Cooper, L T. (2011). Diagnosis and management of peripartum cardiomyopathy. Heart (British Cardiac Society), 97(23),
1970-1981. doi: 10.1136/heartjnl-2011-300349
Incidence

Harper, Margaret A, Meyer, Robert E, & Berg, Cynthia J. (2012). Peripartum cardiomyopathy: population-based birth prevalence and 7-
year mortality. Obstet Gynecol, 120(5), 1013-1019. doi: 10.1097/AOG.0b013e31826e46a1
Incidence by ICD
both over estimates
and misses cases
Incidence likely
1/2066-1/4025 live
births nationwide
Incidence
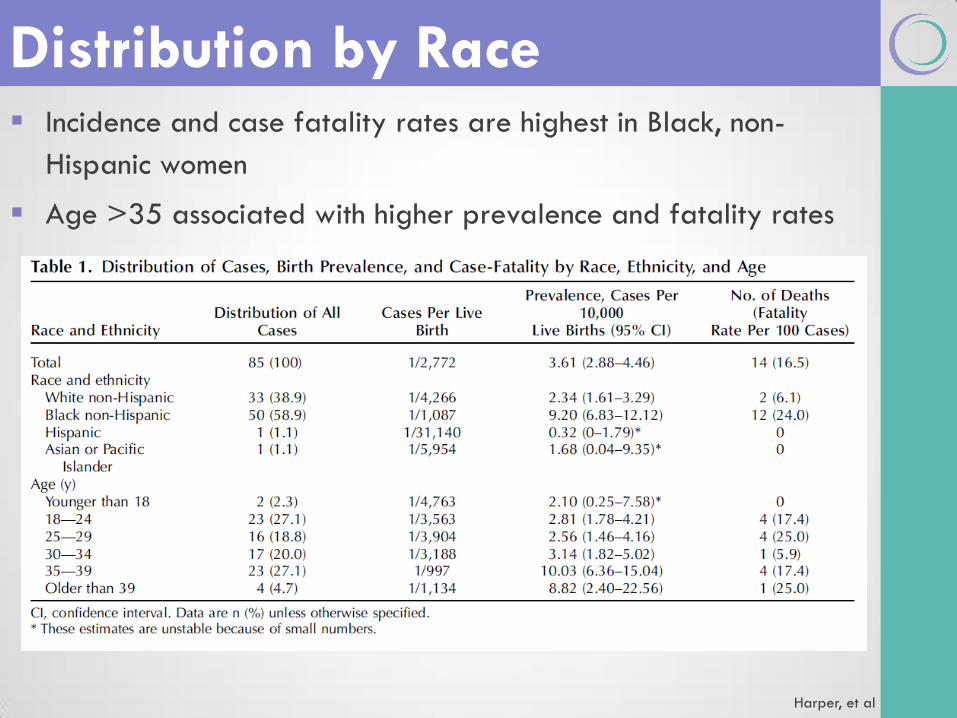
Harper, et al
Incidence and case fatality rates are highest in Black, non-
Hispanic women
Age >35 associated with higher prevalence and fatality rates
Distribution by Race

Risk Factors
Blauwet, L A, & Cooper, L T. (2011). Diagnosis and management of peripartum cardiomyopathy. Heart (British Cardiac Society), 97(23),
1970-1981. doi: 10.1136/heartjnl-2011-300349
Probable Risk Factors Proposed Risk Factors
Emerging Risk Factors
PPCM
Twin
Pregnancy
High Parity
High Gravidity
Extremes of
Reproductive Age
Prolonged
Tocolysis Preeclampsia
Genetics
Obesity
Smoking
Hypertension
Malnutrition
Cocaine Abuse
African Ancestry
Socioeconomic
Status

Etiologies/
Pathophysiology
Inflammation
Infection
Abnormal immune response to pregnancy
Abnormal response to hemodynamic stress of
pregnancy
Increased myocyte apoptosis
Abnormal hormonal response
Increased adrenergic tone
Excessive prolactin production
Genetics
Proposed Etiologies
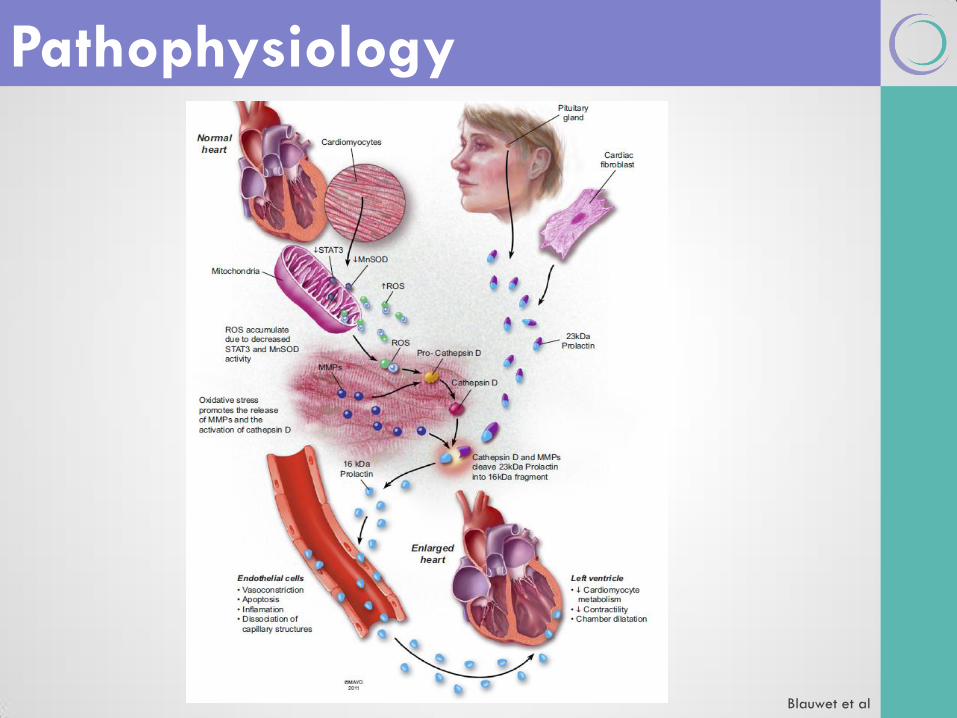
Pathophysiology
Blauwet et al

Prolactin
Hilfiker-Kleiner, D., Struman, I., Hoch, M., Podewski, E., & Sliwa, K. (2012). 16-kDa prolactin and bromocriptine in postpartum
cardiomyopathy. Curr Heart Fail Rep, 9(3), 174-182. doi: 10.1007/s11897-012-0095-7
16-kDA
Prolactin
23-kDA
Prolactin
Cathepsin D
(Vasoinhibin)

Prolactin
Hilfiker-Kleiner, D., Struman, I., Hoch, M., Podewski, E., & Sliwa, K. (2012). 16-kDa prolactin and bromocriptine in postpartum
cardiomyopathy. Curr Heart Fail Rep, 9(3), 174-182. doi: 10.1007/s11897-012-0095-7
Apoptosis
Migration
Inhibition
Leukocyte
Adhesion
Vaso-
dilatation
Inhibition
16K PRL
Impaired
Vessel
Maturation
Capase
3/8/9
NF-kB
eNOS
Proliferation
Inhibition
MAPKDelta /Notch
Ras-Tiam-Rac1
ICAM
VCAM
SELE
Diagnosis

Signs and Symptoms
Symptoms of PPCM
Dyspnea
Peripheral Edema
Fatigue
Orthopnea
Paroxysmal Nocturnal
dyspnea
Palpitations
Chest pain
Decreased exercise
tolerance
Anorexia
Persistent cough
Abdominal discomfort
Signs of PPCM
Pulmonary Rales
Loud P2
Third Heart Sound (S3) or
Gallop Rhythm
New Mitral Murmur
New Tricuspid Murmur
Lateral / Downward
Displacement of PMI
Jugular Venous Distension
Hepatojugular Reflux
Hepatomegaly
Peripheral Edema
Ascites
Blauwet et al

Blauwet et al
Diagnosis - Adjunct Studies Rule out pneumonia
Rule out pneumothorax
Access for
Cardiac MRI
Useful when echo images are non-diagnostic
May provide prognostic information
Right Ventricular Biopsy
Useful with ventricular tachycardia or high grade failure
Patients who fail to respond to optimal medical therapy
Anemia
Thyroid disease
Liver disease
End stage renal disease
Infection
HIV
Electrolytes
NT-proBNP
hs-CRP

Treatment-
Compensated

Non-pharmaceutical
therapies
Low-sodium diet
≤ 2 liters fluid per day
Decreased activity
Antepartum
management
Beta-blocker
Carvedilol
Metoprolol extended
release
Vasodilator
Digoxin
Diuretic
LMWH for EF < 35%
Treatment (Compensated)
Heart Failure Society Of America. (2006). Johnson-Coyle et al. Lata, I. et al.
Postpartum therapy
Angiotensin-converting enzyme (ACE) inhibitor
Angiotensin-receptor blocker (if ACE inhibitor not tolerated)
± Nitrates or hydralazine
Loop Diuretic
Vasodilator
Aldosterone antagonist
Beta-blocker
Warfarin for EF < 35%
Treatment (Compensated)
Heart Failure Society Of America. (2006). Johnson-Coyle et al. Lata, I. et al.
ABCs
Loop diuretic
Vasodilator
Positive inotropic agents
Avoid beta-blockers
Heparin
Consider endomyocardial biopsy
Consider cardiac MRI
Assist devices
ECMO
Transplantation
Treatment (Decompensated)
Heart Failure Society Of America. (2006). Johnson-Coyle et al. Lata, I. et al.

Possible novel therapy for patients with
PPCM
Still should be considered experimental
May consider use in patients failing
conventional therapy or who are
severely compromised
Bromocriptine

Pilot study – Open-label randomized 10:10
Open-label randomized 10:10
8 weeks of bromocriptine therapy
Improved EF at 6 months vs. standard care
Decreased risk of composite poor outcomes
Bromocriptine
Sliwa et al

Treatment algorithm
Bachelier-Walenta et al.

Treatment algorithm
Bachelier-Walenta et al.

Treatment algorithm
Bachelier-Walenta et al.

Management
– Labor &
Delivery

If possible, delay until heart failure has
resolved (or is resolving)
Route of delivery- ideally vaginal
Decreased hemodynamic burden
Condition may not tolerated prolonged
induction
Supplemental oxygen
Left tilt
Labor & Delivery
Heart Failure Society Of America. (2006). Johnson-Coyle et al. Lata, I. et al.

Anesthesia - early epidural
Avoid tachycardia
Avoid hypotension
Careful fluid management
Continuous ECG
± Arterial catheter
± Pulmonary catheter
Intensive care 48 hours postpartum
Labor & Delivery
Heart Failure Society Of America. (2006). Johnson-Coyle et al. Lata, I. et al.

Prognosis

Older studies
50% recovery
25% stable but reduced cardiac function
25% deteriorate
Prognosis

Higher diagnosis and 6 month EF than other causes for
cardiomyopathy
Trend to greater change in EF in 6 months
PPCM vs. other CM
Cooper, L. T. et al

Greater percentage of PPCM patients with EF>50%
Percentage of patients with EF<30% similar between
etiologies
Distribution of EF in PPCM
Cooper, L. T et al
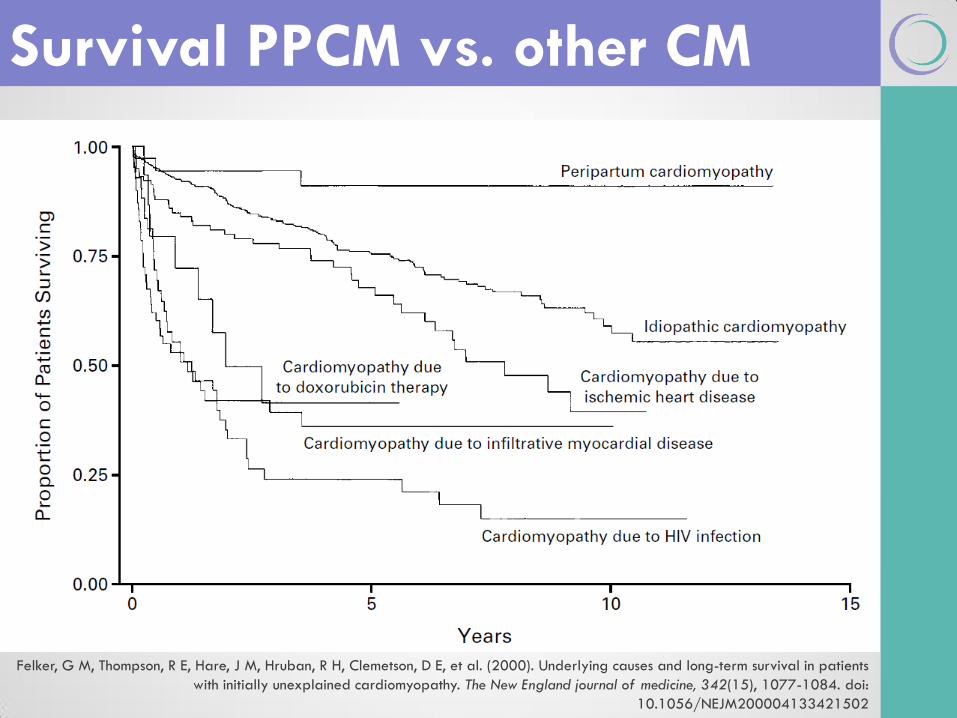
Felker, G M, Thompson, R E, Hare, J M, Hruban, R H, Clemetson, D E, et al. (2000). Underlying causes and long-term survival in patients
with initially unexplained cardiomyopathy. The New England journal of medicine, 342(15), 1077-1084. doi:
10.1056/NEJM200004133421502
Survival PPCM vs. other CM

Future Pregnancy Inadvisable

Elkayam, U et al.
Future Pregnancy Inadvisable

Future Pregnancy Inadvisable
Elkayam, U et al.

Summary
Summary
Widely variable incidence
Rule out other etiologies first
Better long term outcomes that other CM
etiologies
Future pregnancies are not recommended
regardless of recovery

Summary
Initial treatment includes diuretics, beta-
blockers, and inotropes
Consider Bromocriptine for those that do
not respond to maximum therapy
Consider delivery if fetus mature or
cardiac failure decompensated
Evidence

REFERENCES
• Bachelier-Walenta, Katrin, Hilfiker-Kleiner, Denise, & Sliwa, Karen. (2013). Peripartum
cardiomyopathy. Curr Opin Crit Care, 19(5), 397-403. doi: 10.1097/MCC.0b013e328364d7db
(Level III)
• Blauwet, L A, & Cooper, L T. (2011). Diagnosis and management of peripartum cardiomyopathy.
Heart (British Cardiac Society), 97(23), 1970-1981. doi: 10.1136/heartjnl-2011-300349 (Level
III)
• Cooper, L. T., Mather, P. J., Alexis, J. D., Pauly, D. F., et al. (2012). Myocardial recovery in
peripartum cardiomyopathy: prospective comparison with recent onset cardiomyopathy in men
and nonperipartum women. J Card Fail, 18(1), 28-33. doi: 10.1016/j.cardfail.2011.09.009
(Level II-2)
• Demakis, J. G., & Rahimtoola, S. H. (1971). Peripartum cardiomyopathy. Circulation, 44(5), 964-
968. Level III)
• Elkayam, U., Tummala, P. P., Rao, K., Akhter, M. W., Karaalp, I. S., Wani, O. R., et al. (2001).
Maternal and Fetal Outcomes of Subsequent Pregnancies in Women with Peripartum
Cardiomyopathy. The New England journal of medicine, 344(21), 1567–1571.
doi:10.1056/NEJM200105243442101(Level II-2)
• Felker, G M, Thompson, R E, Hare, J M, Hruban, R H, Clemetson, D E, et al. (2000). Underlying
causes and long-term survival in patients with initially unexplained cardiomyopathy. The New
England journal of medicine, 342(15), 1077-1084. doi: 10.1056/NEJM200004133421502 (Level
II-3)
Evidence

REFERENCES – continued
• Habli, Mounira, O'Brien, Thomas, Nowack, Elizabeth, Khoury, Saeb, Barton, John R, &
Sibai, Baha. (2008). Peripartum cardiomyopathy: prognostic factors for long-term maternal
outcome. American journal of obstetrics and gynecology, 199(4), 415.e411-415. doi:
10.1016/j.ajog.2008.06.087 (Level II-3)
• Harper, Margaret A, Meyer, Robert E, & Berg, Cynthia J. (2012). Peripartum cardiomyopathy:
population-based birth prevalence and 7-year mortality. Obstet Gynecol, 120(5), 1013-
1019. doi: 10.1097/AOG.0b013e31826e46a1 (Level II-3)
• Heart Failure Society Of, America. (2006). Executive summary: HFSA 2006 Comprehensive
Heart Failure Practice Guideline. J Card Fail, 12(1), 10-38. doi:
10.1016/j.cardfail.2005.12.001(Level III)
• Hilfiker-Kleiner, D., Struman, I., Hoch, M., Podewski, E., & Sliwa, K. (2012). 16-kDa prolactin
and bromocriptine in postpartum cardiomyopathy. Curr Heart Fail Rep, 9(3), 174-182. doi:
10.1007/s11897-012-0095-7 (Level III)
• Johnson-Coyle, L., Jensen, L., Sobey, A., American College of Cardiology, Foundation, &
American Heart, Association. (2012). Peripartum cardiomyopathy: review and practice
guidelines. Am J Crit Care, 21(2), 89-98. doi: 10.4037/ajcc2012163 (Level III)
• Lata, I., Gupta, R., Sahu, S., & Singh, H. (2009). Emergency management of decompensated
peripartum cardiomyopathy. J Emerg Trauma Shock, 2(2), 124-128. doi: 10.4103/0974-
2700.50748 (Level III)
Evidence

REFERENCES – continued
• Manolio, T. A., Baughman, K. L., Rodeheffer, R., Pearson, T. A., Bristow, J. D., et al. (1992).
Prevalence and etiology of idiopathic dilated cardiomyopathy (summary of a National Heart,
Lung, and Blood Institute workshop. Am J Cardiol, 69(17), 1458-1466. (Level II-3)
• Natalie Bello, M. D., Iliana S Hurtado Rendon, M. D., & Zoltan Arany, M. P. (2013). Accepted
Manuscript. Journal of the American College of Cardiology, 1–35.
doi:10.1016/j.jacc.2013.08.717 (Level I)
• Patten, Ian S, Rana, Sarosh, Shahul, Sajid, Rowe, Glenn C, Jang, Cholsoon, et al. (2012).
Cardiac angiogenic imbalance leads to peripartum cardiomyopathy. Nature, 485(7398), 333-
338. doi: 10.1038/nature11040 (Level III)
• Sliwa, K, Blauwet, L, Tibazarwa, K, Libhaber, E, Smedema, J P, et al. (2010). Evaluation of
Bromocriptine in the Treatment of Acute Severe Peripartum Cardiomyopathy: A Proof-of-
Concept Pilot Study. Circulation, 121(13), 1465-1473. doi:
10.1161/CIRCULATIONAHA.109.901496 (Level I)
Evidence

Thank You for Your Attention!
Planning Committee
Mike Foley, Director Shad Deering, co-Director
Helen Feltovich, co-Director Bill Goodnight, co-Director
Loralei Thornburg, Content co-Chair Deirdre Lyell, Content co-Chair
Suneet Chauhan, Testing Chair Mary d’Alton
Daniel O’Keeffe Andrew Satin
Barbara Shaw

















