16
Volume 3 Issue 6 November/December 2015 An International, Open Access, Peer reviewed, Bi-Monthly Journal

Volume 3 Issue 6 November/December 2015
An International, Open Access, Peer reviewed,
Bi-Monthly Journal

Editorial
Editor-in-Chief
Chethana G S [email protected]
www.jobb.co.in
Advisory Board
Dr. S.M. Gopinath, Phd HOD, Dept of Biotechnology, Acharya Institute of Technology, Bangalore, INDIA
Dr. Vedamurthy A.B. Phd
Professor, P.G. Department of Studies in Biotechnology and Microbiology, Karnatak
University, Dharwad, India
Dr. Hari Venkatesh K Rajaraman MD(Ay), PGDHM Manager, R&D, Sri Sri Ayurveda Trust, Bangalore, INDIA
R. Rajamani, M.Sc.,M.Phil.,B.Ed. Co-Principle Investigator, SSIAR, Bangalore, INDIA
Dr. Pravina Koteshwar, MBBS, MD Director, Academic Programs, ICRI, India
Editorial Board
Dr. Pushpinder Kaur, Phd Research Associate, CSIR-Institute of Microbial Technology Sector,
Chandigarh, INDIA
Dr. Kavita Sharma, Phd Senior Scientist, Research and Development, Pharmacology Division,
Sigma Test and Research Centre, New Delhi, INDIA
Dr. Kasim Sakran Abass, Phd Associate Professor, College of Nursing,
University of Kirkuk, Kirkuk, IRAQ
Dr. Ashutosh Chaturvedi (BAMS, PEC Diabetes care)
Resident & M.D Scholar, Department of Panchakarma, SDMCAH - Hassan

Index – JOBB, Volume 3, Issue 6 - November/December 2015
Medical Biotechnology
BLEEDING PATTERN OF WOMEN USING HORMONAL CONTRACEPTIVES:
A PHARMACOVIGILANCE STUDY
Huma Dilshad, Rabia Ismail, Mohammad Harris Shoaib, Safila Naveed 319-326
Medical Biotechnology
SIMPLE UV SPECTROPHOTOMETRIC ASSAY OF NORFLOXACIN FORMULATION AND THEIR
COMPARATIVE STUDY
Safila Naveed, Sidra Sajid 327-331
Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
BLEEDING PATTERN OF WOMEN USING HORMONAL CONTRACEPTIVES:
A PHARMACOVIGILANCE STUDY
Research article
_______________________________
Huma Dilshad1, 2*
, Rabia Ismail1,
Mohammad Harris Shoaib1
Safila Naveed1, 2
_____________________________ 1Faculty of Pharmacy, University of
Karachi
2Faculty of Pharmacy, Jinnah
University for Women, Pakistan
*Corresponding Author: Email:
ABSTRACT:
In this study we compared the breakthrough bleeding, due to the use
of monophasic COC contains 0.15mg Levonorgestrol+0.03mg Ethinyl
estradiol (EE/LNG) with an injectable contraceptive Depot medroxy
progesterone (Depo Provera) comprising 150mg/mL of
medroxyprogestrone acetate (DMPA). The study was carried out in
family planning departments of different clinical settings and hospitals
in Karachi. Females maintained on hormonal type contraceptives were
invited and reviewed for their reproductive health and history. The
investigation includes over 12970 women, maintained on different
methods of contraceptives, out of which 1130 women were using
hormonal contraceptives. Total, 847 females were received allocated
treatment Depo-Provera verses Combined Oral Contraceptives n=498
vs n= 349 per group respectively). There are less bleeding/spotting
days recognized by women receiving DMPA than females using COCs.
Data divided into two groups: Group I (n=349) were the users of Drug-
I combined estrogen-progestin oral contraceptives were more likely to
show breakthrough bleeding than Group II (n=498) women maintained
on Drug-II Depot medroxy progesterone acetate (odds ratio [OR],
0.739; 95% confidence interval [CI], (0.56-1.97). The odd ratio of
breakthrough bleeding (BTB) for women in Age –I (19-35 years) odds
ratio [OR], 1.026 at 95% confidence interval [CI], (0.780 -1.350). This
increased risk was more observed in Duration -II, with odds ratio [OR],
1.74; 95% confidence interval [CI], with lower and upper CI limit
(1.55- 1.80). Patient education regarding early warning symptoms of
breakthrough bleeding, and lack of withdrawal bleeding adds an
additional margin of safety and reduces patient questions and
uncertainties. Long-term contraception with hormonal contraceptives
causes the maximum menstrual disturbances.
Keywords: Hormonal contraception, Bleeding pattern, COCs (Combine Oral Contraceptives), DMPA
(Depotmedroxyprogestrone acetate).
____________________________________________________________________________________
INTRODUCTION Research proved risks related with hormonal
contraception have driven women’s interest and changed
the approach for using hormone especially during
preceding decade (Andrist LC. 1998; Hunter MS et al.,
1997). The Women’s Health Initiative (WHI) study
outcomes proved the risk of using conventional
hormones, specifically Premarin®and Provera®
(Rossouw JE et al., 2002). Increased risk of coronary

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
events, breast cancer, stroke and blood clots are
associated with the use of estrogen combined with
progestin. Moreover females prescribed hormonal
contraception frequently stop it prior to long-term
advantages was identified. Weight gain and undesirable
side effects are the major reasons for discontinuation and
almost one third to two third of females stopping it during
initial two years (Vihtamaki T et al., 1999; Newton KM
et al., 1997; Tonkelaar I et al., 2000; Bjorn N et al.,
1997). Mainly the side effects are associated with the
synthetic progestin portion, and the most frequent
unwanted effects are bloating, irregular bleeding and
breast tenderness (Ettinger B et al., 1999). Other reasons
for discontinuation include risk of cancer and suggestion
by a physician. The most frequent side effect of every
form of hormonal contraceptive is abnormal uterine
bleeding. However this bleeding is not often dangerous
several females take it worrisome and frequently stop
hormonal contraception due to irregular bleeding and
other unwanted side effects (Sangi-Haghpeykar H et al.,
1996; Paul C et al., 1997). Irregular uterine bleeding has
become more frequent when oral contraceptives contain
lower doses of estrogen, which are incapable to maintain
endometrial integrity (Kaunitz AM 1998).
Progestin-induced decidualization and endometrial
atrophy associated with OCPs are the most frequent
reason of breakthrough bleeding. Increased dose and
potency of estrogen and progestin, decreases the
occurrence of breakthrough bleeding [Sulak P et al.,
1999]. Unusual uterine bleeding is associated with the
ratio of progestin to estrogen (Stubblefield PG 1994).
Moreover every woman metabolizes hormone in a
different way (Wallach M et al., 2000). These types of
factors cause more difficulties to elucidate the study
results. The management of irregular uterine bleeding in
females using combined OCPs starts with Psychotherapy
concerning compliance (Hatcher RA et al., 1998). OCs
inhibits ovulation and provide tremendous contraceptive
efficacy (Sitruk-Ware R 2006; Koetsawang et al., 1980;
Hirvonen E et al., 1990; Kivinen S et al., 1996;
Schubert W et al., 1987; Serup J et al., 1979).
In clinical trials, the monophasic and biphasic forms of
oral contraceptives are unacceptable for cycle control
(Sitruk-Ware R 2006; Hirvonen E et al., 1990; Kivinen
S et al., 1996; Schubert W et al., 1987; Serup J et al.,
1979) which may cause elevated rate of early
discontinuation as compare to products contain ethinyl
estradiol. Allied complications have included menstrual
disturbances, breakthrough bleeding/spotting (Kivinen S
et al., 1996; Schubert W et al., 1987) an improved
number of spotting or bleeding days for each cycle
(Hirvonen E et al., 1990) and extended bleeding (Wenzl
R et al., 1993). Depo-Provera (Depot medroxy
progesterone acetate) is an injection containing 150mg
progestin and administered intramuscularly that sustain
proper contraceptive efficacy for about 14 weeks. High
dose of progestin is inhibited ovulation in majority of
women (Hatcher RA. 1998). Merely 0.3% of females get
pregnancy during the first year of using Depo-Provera
injection (Trussell J. 1998). Breakthrough bleeding
means flow of blood at an unpredicted time throughout
the menstrual cycle and it requires to use tampon /sanitary
napkins. Surprising bleeding that does not need any safety
or protection is called as spotting (Thorneycroft IH.
1999).
Management of Irregular Uterine Bleeding
COMBINED ORAL CONTRACEPTIVE PILLS
Abnormal uterine bleeding occurs in 30% women
during first month of using combined oral contraceptives
pills (COCPs), this frequency decreases with the time.
The management of irregular uterine bleeding associated
with COCPs starts with counseling (Wallach M et al.,
2000; Hatcher RA et al., 1998). If bleeding sustain after
three months of pill use so that patient will be treated with
non-steroidal anti inflammatory drugs (NSAID) or
supplemental estrogen (Hatcher RA et al., 1998).
PROGESTIN-ONLY CONTRACEPTIVE
METHODS
Unusual uterine bleeding is commonly associated with
progestin-only contraceptives. Depo-Provera injection
contains higher dose of progestin. During first year of use
the incidents of irregular bleeding occur in 70% females
using injectable contraceptives (Hatcher RA et al.,
1998).
MATERIAL AND METHODS The study was carried out in family planning centers,
established by Government of Pakistan in different
clinical settings of Karachi and was conducted on young
females, maintained on hormonal contraceptives
including oral pills and Injectable (Depo) for at least two
years with the following chemical composition,
Combined oral contraceptives (COC) containing
0.15mg Levonorgestrol + 0.03mg Ethinyl
estradiol.
Depo-Provera (Depo), an injectable consisting of

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
150mg/mL Medroxyprogestrone Acetate.
Study population A cohort of 12214 women, between 19 to 49 years of
age, between January 2012 and December 2013 was
identified. The selection of the subjects was done on the
basis of following inclusion and exclusion criteria. The
selected subjects maintained on these agents, were
thoroughly evaluated for minor side effects and data was
recorded on predesigned data collection form. The data
collection form was constructed on the basis of such
similar studies conducted by several researchers like
(Talisuna AO et al., 2006; Stergachis A et al., 2010 and
Kuemmerle et al., 2011). Those females who were
qualifying inclusion criteria evaluated for their
reproductive history. Healthy females aged 19–49 years
looking for contraception participated in this study. The
exclusion criteria for this study is included the pregnancy;
incident of b3 menstrual cycles due to childbirth, abortion
/lactation; present use of an intrauterine device; obesity
(body mass index N30 kg/m2); hypersensitivity to any of
the hormonal drug ingredients.
Study assessments
All through study period, participants were requisite to
record tablet intake and bleeding events. Parameters for
bleeding patterns were assessed for every 3-months
reference period (as suggested by the World Health
Organization). Reference Period 1 is 1-90 days of
treatment; Reference Period 2 is next three months (day
91-180) of treatment. Eight Reference Periods were
included in this study. Parameters of bleeding pattern
observed in this study are the number of bleeding/spotting
days and the extent and duration of bleeding/spotting
events.
Statistical analysis:
Statistical analysis was performed by means of age
group, treatment group and duration of treatment. In this
study 457 women aged 19–35 years and 390 women aged
36–49 years per treatment group (total participants = 847)
were selected to estimate of the number of females
required to conduct exact specific comparisons between
treatment groups and between age groups during whole
treatment period for the number of bleeding/spotting days
per reference period.
RESULTS AND DISCUSSION
Table 1: (CROSSTAB AND CHI SQUARE TEST OF COMBINED ORAL CONTRACEPTIVE (COCs)
VERSES DEPO –PROVERA FOR Breakthrough bleeding
EFFECT OF DRUGS
Breakthrough Bleeding TOTAL P-Value
B.BleedingYes B.Bleeding No
COCs(Drug-I) Count 218 179 397
0.031
% B.Bleeding 43.8% 51.3% 46.9%
Depo-
Provera(Drug-II)
Count 280 170 450
% B.Bleeding 56.2% 48.7% 53.1%
Total Count 498 349 847
% B.Bleeding 100% 100% 100%
EFFECT OF AGE
Breakthrough Bleeding TOTAL P-Value
B.Bleeding Yes B.Bleeding No
Age-I ( years)
19-35
Count 270
187
457
0.830
% B.Bleeding 54.2% 53.6% 54.0%
Age-II(years)
36-49
Count 228 162
390
% B.Bleeding 45.8% 46.4% 46.0%
Total Count 498 349 847
% B.Bleeding 100% 100% 100%

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
EFFECT OF DURATION
Breakthrough Bleeding TOTAL P-Value
B.BleedingYes B.Bleeding No
Duration-I
6months-1 year
Count 144 123
267
0.041
% B.Bleeding 28.9% 35.2% 31.5%
Duration-II
1year-2 years
Count 354 226
580
% B.Bleeding 71.1% 64.8% 68.5%
Total Count 498 349 847
% B.Bleeding 100% 100% 100%
Table 2: (LOGISTIC REGRESSION PREDICTING BREAK THROUGH BLEEDING BETWEEN
DIFFERENT DRUGS, AGE GROUP AND DURATION)
Description DRUGS
(Drug-I (COCs)
Drug-II (Depo-Provera)
AGE
Age-I(19-35)
Age-II (36-49)
DURATION (Duration-
I (6months-1 year)
Duration-II (1year-2years)
Number of
reported cases
847
847
847
Omnibus Tests
of Model
Coefficient s
Chi-Square
p-value
Chi-Square p-value
Chi-Square p-value
4.65 0.031 0.033 0.855 3.78 0.042
Variables in the
Equation
Drugs verses Nausea Age verses Nausea Duration verses Nausea
Odds Ratio
(Exp β)
95% CI Odds Ratio
(Exp β)
95% CI Odds Ratio
(Exp β)
95% CI
Lower –
Upper
Lower –
Upper
Lower - Upper
0.739
0.56 – 1.97 1.026 0.780-
1.350
1.74 1.55-1.80
p-Value 0.031 0.855 0.04
DISCUSSION:
When Drug I (n=397) was compared with Drug II
(n=450) and were observed for the presence of
breakthrough bleeding i.e. 218/397 (43.8%) and 280/450
(56.2%) cases were found respectively and statistical
significance was observed by chi-square test (p=0.031)
(Table 1). Omnibus test was also applied which showed
overall significance of the model with the chi-square
value of 4.653. The value of odd ratio (β) obtained was
0.746 showed that the odd of breakthrough bleeding
(BTB) of Drug I was 0.746 times greater than Drug-II
with 95% confidence interval limit 0.56-1.97. Fig 2 shows
comparison of breakthrough bleeding using both drugs.
Similarly when Age -I (n=457) was compared with Age-II
(n=390) were observed for the presence of breakthrough
bleeding 270/457 (54.2%) and 228/390 (45.8%) cases
were observed respectively and statistical insignificance
was observed by chi-square test (P=0.830) (Table 1). By
using Omnibus test overall significance of the model was
obtained with the chi-square value of 0.033. The value of
odd ratio (β) obtained was 1.026 showed non-significant
results between Age and Break through Bleeding, as the
p-value is >0.05 and 95% (CI) confidence interval limit of

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
1.077- 1.895. Fig 3 shows breakthrough bleeding in
different age group.
When Duration I (n=267) was compared with
Duration-II (n=580) was observed for the presence of
breakthrough bleeding 144/267 (28.9%) and 354/580
(71.1%) were observed respectively and statistical
significance was observed by chi-square test (p=0.041)
(Table 1). We used Omnibus test to analyze the
association between side/adverse effect and duration that
showed overall significance of the model where the chi-
square value of 3.78. However the value of odd ratio (β)
was 1.74 showing that the odd of breakthrough bleeding
of Duration-II was 1.74 times greater than Duration-I with
95% confidence interval limit of 1.55- 1.80. Fig 1 shows
time period for Breakthrough bleeding.
CONCLUSION Abnormal menstrual patterns are most probably
produce discontinuation of hormonal contraception in
females. These disturbances include breakthrough
bleeding/spotting although bleeding due to missed
withdrawal is associated with existing levels of estrogen
and concealed endometrium.
Since breakthrough bleeding recovers with the time
and clinicians must educate women about benefits of
hormonal contraceptives as proper counseling can
discourage the misperceptions to encourage more women
to use contraception during child bearing age. For the
development of efficient treatment it is necessary to have
the knowledge of basic mechanism of bleeding. It is also
essential to review the approaches to the assessment and
treatment of abnormal bleeding associated with the use of
contraceptives.
Fig 1: Time period for Breakthrough bleeding

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
Fig 2: Comparison of breakthrough bleeding using both drugs
Fig 3: Breakthrough bleeding in different age group

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
REFERENCES
Andrist LC (1998). The impact of media attention,
familyhistory, politics and maturation on
women’sdecisions regarding hormone replacement
therapy.Health Care Women Int. 19:243-260.
Bjorn N, Backstrom T (1997). Compliance to HRT:
thesignificance of negative side effects and
moodsymptoms. Abstract: Eighth Annual Meeting
ofNAMS. Menopause. 4:283.
Den Tonkelaar I, Oddens BJ (2000). Determinants of
longterm hormone replacement therapy and reasons
forearly discontinuation. Obstet Gynecol. 95:507-512.
Ettinger B, Pressman A, Silver P(1999). Effect of ageon
reasons for initiation and discontinuationof hormone
replacement therapy. Menopause. 6:282-289.
Hatcher RA, Guillebaud J. The pill: combined oral
contraceptives. In: Hatcher RA. Contraceptive
technology. 17th ed. rev. New York: Ardent Media,
1998:405–66.
Hunter MS, O’Dea I, Britten N (1997). Decision-
makingand hormone replacement therapy: a
qualitativeanalysis. Soc Sci Med. 45:1541-1548.
Hatcher RA (1998). Depo-Provera, Norplant, and
progestin- only pills. In: Hatcher RA. Contraceptive
technology. 17th ed. rev. New York: Ardent Media. 467-
509.
Hatcher RA, Guillebaud J.(1998). The pill: combined oral
contraceptives. In: Hatcher RA. Contraceptive
technology. 17th ed. rev. New York: Ardent Media. 405-
66.
Hirvonen E, Vartiainen E, Kulmala Y (1990). A
multicenter trial with a new OC using a natural estradiol
and cyproterone acetate for women over 35. Adv
Contracep. 6:248.
Kaunitz AM (1998). Oral contraceptive estrogen dose
considerations. Contraception. 58(3 suppl):S15–21.
Kivinen S, Saure A.(1996). Efficacy and tolerability of a
combined oral contraceptive containing 17 beta-estradiol
and desogestrel. Eur J Contracept Reprod Health
Care.1:183.
Koetsawang S, Mandlekar AV, Krishna UR (1980).A
randomized, double-blind study of two combined oral
contraceptives containing the same progestogen, but
different estrogens. World Health Organization Task
Force on Oral Contraception. Contraception. 21:445-59.
Kuemmerle A, Dodoo AN, Olsson S, Van Erps J, Burri C
(2011) Assessment of global reporting of adverse drug
reactions for anti-malarials, including artemisinin-based
combination therapy, to the WHO Programme for
International Drug Monitoring. Malar J 10: 57.
Paul C, Skegg DC, Williams S (1997). Depot
medroxyprogesterone acetate. Patterns of use and reasons
for discontinuation. Contraception. 56:209–14.
Newton KM, LaCroix AZ, Leveille SG (1997). Women’s
beliefs and decisions about hormonereplacement therapy.
J Womens Health. 6:459-465.
Rossouw JE, Anderson GL, Prentice RL (2002).Risks and
benefits of estrogen plus progestin inhealthy
postmenopausal women: principal resultsFrom the
Women’s Health Initiative randomizedcontrolled trial.
JAMA. 288:321-333.
Sangi-Haghpeykar H, Poindexter A N Bate-man L,
Ditmore JR (1996). Experiences of injectable
contraceptive users in an urban setting. Obstet Gynecol.
88:227–33.
Serup J, Bostofte E, Larsen S, Westergaard J, Lebech PE
(1979). Natural oestrogens for oral contraception. Lancet.
2:471-2.
Schubert W, Cullberg G (1987). Ovulation inhibition with
17 beta-estradiol cyclo-octyl acetate and desogestrel. Acta
Obstet Gynecol Scand. 66:543-7.
Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 319-326 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
Sitruk-Ware R(2006). New progestagens for
contraceptive use. Hum Reprod Update. 12:169-78.
Stubblefield PG (1994). Menstrual impact of
contraception. Am J Obstet Gynecol. 170(5 pt 2):1513–22.
Sulak P, Lippman J, Siu C, Massaro J, Godwin A (1999).
Clinical comparison of triphasic norgestimate/35
micrograms ethinyl estradiol and monophasic
norethindrone acetate/20 micrograms ethinyl estradiol.
Contraception. 59:161–6.
Stergachis A, Bartlein RJ, Dodoo A, Nwokike J, Kachur
SP (2010). A situational analysis of pharmacovigilance
plans in the Global Fund Malaria and U.S. President's
Malaria Initiative proposals. Malar J 9: 148.
Talisuna AO, Staedke SG, D'Alessandro U (2006)
Pharmacovigilance of antimalarial treatment in Africa: is
it possible? Malar J 5: 50.
Thorneycroft IH (1999). Cycle control with oral
contraceptives:a review of the literature. Am J Obstet
Gynecol. 80(2 pt 2):280-7.
Trussell J (1998). Contraceptive efficacy. In: Hatcher
RA.Contraceptive technology. 17th ed. rev. New York:
Ardent Media, 779-99.
Wenzl R, Bennink HC, van Beek A, Spona J, Huber J
(1993). Ovulation inhibition with a combined oral
contraceptive containing 1 mg micronized 17 beta-
estradiol. Fertil Steril. 60:616-9.
Vihtamaki T, Savilahti R, Tuimala R (1999). Why
dopostmenopausal women discontinue
hormonereplacement therapy? Maturitas. 33:99-105.
Wallach M, Grimes DA, Chaney EJ, Totowa, N.J.: Emron
(2000). Approach to common side effects. In: Modern
oral contraception: updates from The Contraception
Report. 70–6.
Citation of this article: Huma Dilshad, Safila Naveed, Rabia Ismail, Mohammad Harris Shoaib.
Bleeding pattern of women using hormonal contraceptives: A Pharmacovigilance study. Journal
and Biotechnology and Biosafety. 3(6):319-326
Source of Support: Nil Conflict of Interest: None Declared

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 327-331 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
SIMPLE UV SPECTROPHOTOMETRIC ASSAY OF NORFLOXACIN
FORMULATION AND THEIR COMPARATIVE STUDY
Research article ___________________________________
Safila Naveed1*, Sidra Sajid
2
___________________________________
Faculty of pharmacy, Jinnah University for
women, Karachi.
Corresponding author: [email protected],
ABSTRACT
Norfloxacin belongs to flouoroquinolones class of
antibiotics. Its structure is related to nalidixic acid. The
purpose of following study was to develop an easy, less
time consuming and economically affordable UV
Spectrophotometric method for assay of Norfloxacin in
tablet formulation and comparison of two brands of
Norfloxacin tablets. This assay procedure based on the
absorbance measurements of 2 brands of Norfloxacin
400mg tablet available in market at wavelength of
294nm.These two brands are taken and their solutions of
100ppm, 50ppm, 25ppm, 12.5 and 6.25ppm is prepared.
Results obtained by regression equation and regression
line. Percent assay is calculated by taking absorbance of
sample and standard solutions of 12.5ppm to predict the
availability of drug in both brands i.e. 98.27% and
102.6%. Results indicates that both brands meet USP/BP
limit.
Key words: Norfloxacin, UV spectrophotometer, Assay
_________________________________________________________________________________
INTRODUCTION
Figure 1: Structure of Norfloxacin
Molecular weight: 319.33
Norfloxacin (NFX) l-ethyl-6-fluoro-1,4-di-hydro-4-
oxo-7-(1-piperazinyl)-3-quinoline carboxylic acid, is a
synthetic antifluoroquinolon (Prapaporn B et al.,
2002). It is a synthetic drug was the firstly selected drug
for the treatment of diseases caused by Ecoli,
Salmonella, Campylobacter, V. cholera, Shigella and V.
cholera (Murakawa GJ et al., 2003). The drug is also
prescribed for optical infections as well as gonorrhea
and infection urinary tract (Van Bambeke et al., 2005).
The dose usually recommended is 400mg two times
daily. Half-life of NFX in plasma and serum is
measured3-4 hours and only approx bioavailability of
oral dose is 30–40%. Norfloxacin, aflouroquinolone
antibacterial agent structurally related nalidixic acid,
Merck Index (2001).
Following are few developed methods for assay of
Norfloxacin. The UV spectrophotometer was used for

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 327-331 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
the determination of the Norfloxacin in tablets at
wavelength 337nm using 0.05M NaOH as solvent
(Stankov, M et al., 1993). A reversed-phase high-
performance liquid chromatographic assay for
Norfloxacin (NFLX) has been developed. The method
gave good linearity (r2≥0.999) in the range 1–20μg/mL
using a Lichrosorb-RP-8 column (10μm, 20cm×g
4.6mm) at wavelength (278nm) at normal temperature.
Above method is also useful for the analysis of photo
degraded NFLX samples, and was useful to study the
photo-stability of NFLX tablets under different
conditions i.e., UV light, sunlight light or fluorescent
light (Córdoba-Borrego et al., 1999). To measure the
quantity or the content of Norfloxacin in its tablet by
UV spectrophotometer, the assay was carried out at the
wavelength of maximum absorption in hydrochloric
acid solution 0.1mol/L (Samanidou, V. F et al., 2003).
A simple titration method is also used for
Norfloxacin analysis as weight and crushes tablet equal
to 250mg of Norfloxacin. Dissolve in 80mL of
anhydrous acetic acid and titrate with 0.1N per chloric
acid, crystal violet used as indicator.
MATERIALS AND METHODS
UV visible 1601 Shimadzu double beam
spectrophotometer was used to measurement of Spectra.
The solvents which were used for the assay was
distilled water.
Wavelength Selection
About 100 to 6.25ppm of Norfloxacin was accurately
prepared in water. These solutions were scanned in the
200-400nm UV regions. The wavelength kept was
294nm and this wavelength was adopted for absorbance
measurement.
Standard Stock solution
Accurately weighed 10mg of Norfloxacin standard was
transferred to a volumetric flask and add sufficient
methanol to produce 100mL. This was sonicated 5 min
to dissolve it. Make up volume up to 100mL with water.
Transfer 6.25mL from stock solution to 50mL
volumetric flask and make up volume with water.
Sample preparation
Two different brands of Norfloxacin from the
marketed sample were weighed and crushed uniformly
with the help of a mortar and pestle. By calculating the
average weighed sample powder equivalent to 10mg of
Norfloxacin was transferred into a volumetric flask
containing 10mL water. The solutions were sonicated
for about 5 min and then make up volume up to 100ml
with water. Now transfer 6.25mL from stock solution
into 50mL volumetric flask and make up volume with
water (Safila N, 2014).
PROCEDURE After preparation of standard and tablet solutions,
strength of solution 12.5ppm in 50mL Absorbance of
the sample preparation and standard preparation in 1cm
cell at the wavelength of maximum. Absorbance at
about 294nm using a spectrophotometer, using the
blank solution, calculate the quantity in mg, of
Norfloxacin per tablet.
RESULTS AND DISCUSSIONS
Using spectrophotometer on both brands of
Norfloxacin tablets during the study carried out
pharmaceutical assay. Table-1.1 shows brand as A and
B identification and % assay of both brands i.e. 98.27%
and 102.6% respectively. Table 1.2 and 1.3 shows
absorbance of brand A and brand B respectively.
Graphical representation of linearity of equation and
regression value for both brands given in figure 2 and 3.
These results indications that Absorbance is directly
proportional to concentration thus, it obeys to Beers
lambert law. Our research group work on different
assay method those were useful for pharmacy
professionals (Safila et al., 2014,15).

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 327-331 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
TABLE 1.1: SHOWS % ASSAY OF TWO BRANDS
Brand ID ABS at 294nm % Assay
Brand A 0.342 98.27%
Brand B 0.358 102.6%
Standard (Norfloxacin) 0.348 --------
TABLE 1.2: SHOWS ABS OF BRAND A AT DIFFERENT CONC.
Conc ppm Abs
100 2.42
50 1.25
25 0.718
12.5 0.342
6.25 0.17
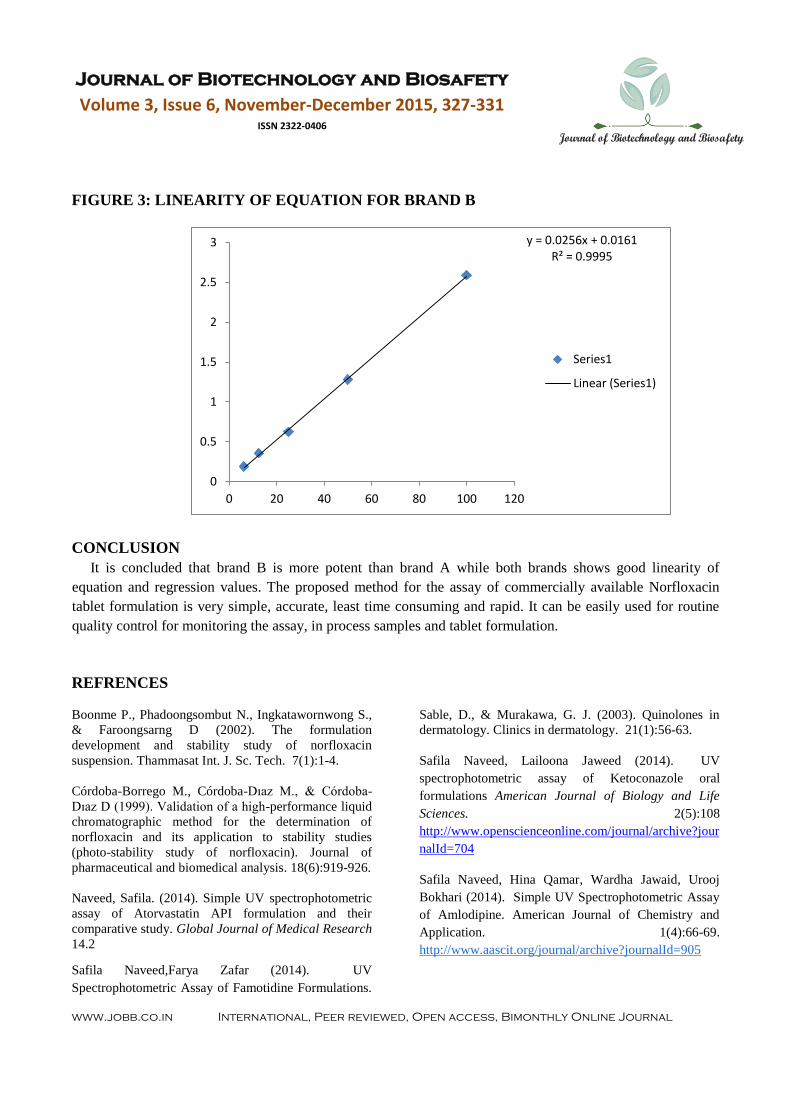
TABLE1.3: SHOWS ABS OF BRAND B AT DIFFERENT CONC.
Conc ppm Abs
100 2.59
50 1.28
25 0.625
12.5 0.358
6.25 0.19
FIGURE 2: LINEARITY OF EQUATION FOR BRAND A
y = 0.0237x + 0.0606 R² = 0.9982
0
0.5
1
1.5
2
2.5
3
0 20 40 60 80 100 120
Series1
Linear (Series1)
Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 327-331 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
FIGURE 3: LINEARITY OF EQUATION FOR BRAND B
CONCLUSION
It is concluded that brand B is more potent than brand A while both brands shows good linearity of
equation and regression values. The proposed method for the assay of commercially available Norfloxacin
tablet formulation is very simple, accurate, least time consuming and rapid. It can be easily used for routine
quality control for monitoring the assay, in process samples and tablet formulation.
REFRENCES
Boonme P., Phadoongsombut N., Ingkatawornwong S.,
& Faroongsarng D (2002). The formulation
development and stability study of norfloxacin
suspension. Thammasat Int. J. Sc. Tech. 7(1):1-4.
Córdoba-Borrego M., Córdoba-Dıaz M., & Córdoba-
Dıaz D (1999). Validation of a high-performance liquid
chromatographic method for the determination of
norfloxacin and its application to stability studies
(photo-stability study of norfloxacin). Journal of
pharmaceutical and biomedical analysis. 18(6):919-926.
Naveed, Safila. (2014). Simple UV spectrophotometric
assay of Atorvastatin API formulation and their
comparative study. Global Journal of Medical Research
14.2
Sable, D., & Murakawa, G. J. (2003). Quinolones in
dermatology. Clinics in dermatology. 21(1):56-63.
Safila Naveed, Lailoona Jaweed (2014). UV
spectrophotometric assay of Ketoconazole oral
formulations American Journal of Biology and Life
Sciences. 2(5):108
http://www.openscienceonline.com/journal/archive?jour
nalId=704
Safila Naveed, Hina Qamar, Wardha Jawaid, Urooj
Bokhari (2014). Simple UV Spectrophotometric Assay
of Amlodipine. American Journal of Chemistry and
Application. 1(4):66-69.
http://www.aascit.org/journal/archive?journalId=905
Safila Naveed,Farya Zafar (2014). UV
Spectrophotometric Assay of Famotidine Formulations.
y = 0.0256x + 0.0161 R² = 0.9995
0
0.5
1
1.5
2
2.5
3
0 20 40 60 80 100 120
Series1
Linear (Series1)

Journal of Biotechnology and Biosafety
Volume 3, Issue 6, November-December 2015, 327-331 ISSN 2322-0406
Journal of Biotechnology and Biosafety
www.jobb.co.in International, Peer reviewed, Open access, Bimonthly Online Journal
American Journal of Pharmacy and Pharmacology.
1(3):28-31.
http://www.aascit.org/journal/archive?journalId=922
Safila Naveed and Fatima Qamar (2014) Simple UV
spectrophotometric assay of Metronidazole Open
Access Library Journal. 1: e615:1-4.
http://dx.doi.org/10.4236/oalib.1100615
Safila Naveed, Hina Qamar, Wardha Jawaid, Urooj
Bokhari (2014) Simple UV spectrophotometric assay of
Glimepride Journal of Clinical Medicine. 2(4): 94
http://www.openscienceonline.com/journal/archive?jour
nalId=717
Safila Naveed, Hina Rehman, Fatima Qamar, Syeda
Zainab (2015). Method development of Perindopril
using UV spectrophotometer. International journal of
pharmaceutical Quality Assurance. 6(1)
http://ijpqa.com/#
Safila Naveed, Hina Rehman, Fatima Qamar, Syeda
Zainab (2015) Development of a spectrophotometric
method for the assay of Diclofenac potassium JIPBS. 2
(1): 7-11.
Samanidou V. F., Demetriou C. E., Papadoyannis I. N.
(2003). Direct determination of four fluoroquinolones,
enoxacin, norfloxacin, ofloxacin, and ciprofloxacin, in
pharmaceuticals and blood serum by HPLC. Analytical
and bioanalytical chemistry. 375(5): 623-629.
Stankov M., Stankov D., Milićević Z., Veselinović D.,
Djurdjević P (1993). Fluorometric and derivative
spectrophotometric determination of norfloxacin.
Spectroscopy letters. 26(9): 1709-1714.
Van Bambeke F., Michot J. M., Van Eldere J., &
Tulkens P. M (2005). Quinolones in 2005: an update.
Clinical Microbiology and infection. 11(4): 256-280.
Citation of this article: Safila Naveed, Sidra Sajid (2015). SIMPLE UV
SPECTROPHOTOMETRIC ASSAY OF NORFLOXACIN FORMULATION AND THEIR
COMPARATIVE STUDY. Journal and Biotechnology and Biosafety. 3(6):327-331
Source of Support: Nil Conflict of Interest: None Declared
![Hizbof habibabubakras sakran[slideshare]](https://static.documents.pub/doc/80x56/558bc658d8b42ac80a8b45cd/hizbof-habibabubakras-sakranslideshare.jpg)
















