Complex humanitarianemergencies: contextA disaster is the result of a vast ecologicalbreakdown between a population and theenvironment, on such a vast scale that thedemands exceed available resources (Gunn,2003). The disaster situation overwhelmsthe response capacity of the a¡ected com-munity and causes disruption and disinteg-ration of the social fabric by prohibitingthe survivors from functioning normally(Pe¤ rez-Sales, 2004). Traditionally, disastersare categorised as either natural disasters(such as earthquakes or £oods) or man-made disasters (such as technologicaldisasters, environmental disasters, terroristacts, armed con£icts or refugee crises). How-ever, this historical dichotomy is losing itsutility. For example, the impact of ‘natural’disasters is often compounded when occur-ring in already fragile ecological or politicalcontexts, while armed con£icts and massivedisplacements are, in turn, fuelled by eco-logical factors such as population pressure,and struggles for control over scarce naturalresources such as fertile land and water.Many disasters do not have a single cause.The 2010 earthquake in Haiti occurred in acontext characterised by social inequalities,
rized reproduction of this article is prohibited.195
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarian
grossly ine⁄cient public services and illprepared physical infrastructures. As aresult, the earthquake had a much moredevastating impact than it would have hadin a politically stable, high income countrywith fully functional public services. Forthese situations, the term complex humani-
tarian emergency was coined, speci¢cally todescribe settings in which multiple, oftenhistorically and politically determined,aetiological factors both predispose an areato disaster, and mitigate its outcomes.Complex humanitarian emergencies areoften characterised by factors such as:dislocation of populations, destruction ofsocial networks and ecosystems, insecuritya¡ecting civilians and others not engagedin ¢ghting, and abuses of human rights(Leaning, Briggs, & Chen, 1999). In suchmultidimensional disasters, natural andman-made factors are closely intertwined.High levels of violence and social insecurity,in particular, threaten the capacity of thepopulation to sustain livelihood and life(Zwi & Ugalde,1991).
Complex humanitarianemergencies: three phases ofassistanceThe conventional classi¢cation for thesequence of humanitarian assistance usesthree phases: relief, rehabilitation anddevelopment. Activities included in therelief phase aim to provide essential servicesto those whose survival is threatened. Thisphase is followed by rehabilitation, in whichbasic services such as schools, health care,andwater supply are restored, and damagedinfrastructure is rebuilt. Finally, the assist-ance can focus onbroader goals, such as eco-nomic growth, improving living standardsand creation of wealth and social capital(Ryscavage, 2003). While this relief^rehabilitation^development continuum is
meant to organise the post disaster responsein a logical way, there are fundamental£awswith it in complex humanitarian emer-gencies. For example, this continuum tendsto obscure the social, macro-economic andenvironmental factors contributing to thedisaster in these settings, and it may serveto legitimate restoration of a socially andmorally unjust, fragile status quo.Documents that provide consensus frame-works to guide humanitarian responsesafter disasters, emphasise community basedapproaches and the need to reinforce theresponses of the local population (IASC,2007; The Sphere Project, 2011). Typically,these frameworks limit their scope to theresponses occurring in themidst ofan emergency,generally the ¢rst months after a disaster.Within one to two years after an emergency,many organisations have ended theirprogrammes and moved to new emergencysettings. The changing nature of humani-tarian emergencies, however, from shortterm emergencies in con¢ned areas to pro-longed emergencies in large geographicalareas, need a di¡erent approach, withdue attention given to capacity buildingof national sta¡ and public institutions(Salama et al., 2004). In this post disasterphase, the need for new leaders and uncon-ventional approaches may arise. This cancall into question the status quo of ‘how things
were always done’, and may lead to rethinkingand rede¢ning public service delivery.The in£ux of local and foreign quali¢edprofessionals, and the provision of aidfunds, can provide additional factors tocreate opportunities for change, if theopportunities are seized at the rightmoment. This requires the use of long termperspectives that go beyond immediateservices delivery, and aim to restore andrestructure the systems that provide theseservices (deJong, 2002).
rized reproduction of this article is prohibited.
Copyrig
Ventevogel et al.
Mental health and psychosocialsupport in complexhumanitarian emergenciesAttention to mental health and psychosocialsupport (MHPSS) in the aftermath ofdisasters is relatively new, and has led to¢erce and often polarised debates aboutwhat kind of mental health care and psycho-social support needs to be organised (Ager,Strang & Wessells, 2006; Galappatti, 2003;van Ommeren, Morris, & Saxena, 2006;Williamson & Robinson, 2006). The widelydiverging views among MHPSS prac-titioners working in complex humanitarianemergencies contributed heavily to poorcoordination across approaches, resultingin fragmented services and a lack of com-prehensive support. The wide range ofopinions about what should be done ispartly related to the absence of a solid baseof evidence on the results of MHPSS inter-ventions in complex humanitarian emer-gencies (Wessells & van Ommeren, 2008).The need to create such an evidence base isobvious (Tol et al., 2011), yet too often, inter-vention strategies are employed where thee¡ectiveness is not at all clear. It is also, asyet, unclear how emergency MHPSS maycontribute to lasting mental health reformsin the post disaster/post con£ict phases,and whether the e¡orts during emergenciesactually do lead to an improved mentalhealth care delivery for the population (All-den et al., 2009). MHPSS service providersin complex humanitarian emergencies canlearn from experiences elsewhere in thedeveloping world, and, in turn, may providedata that are useful for the emerging globalmental health movement.
Mental health, an emergingglobal priorityMental health is becoming a globalhealth priority because of the relative high
prevalence of mental disorders and theassociated disability (Prince et al., 2007).Among the most prevalent mental disordersare: depression, schizophrenia and alcoholor drug abuse disorders (World HealthOrganization, 2005).While non-communic-able diseases, including mental disorders,already pose a substantial global economicburden, this burden is expected to rise morethan double in the next two decades.Withinthis group of noncommunicable disorders,the most important contributors to theglobal economic burden are mental healthconditions and cardiovascular disease(Bloom et al., 2011). In low income countries,the resources for mental health care arevery limited, typically less than 1% of analready low health care budget (Saxenaet al., 2007). Although there has been alobby to promote mental health care in thedevelopment agenda in low incomecountries, there are also major challengesabout how to integrate mental health careinto health sector reform plans. Some ofthese challenges include: engaging mentalhealth professionals in general health sectorreforms; strengthening the links betweenmental health and social development; andintensifying resource mobilisation (Jenkinset al., 2010). One key to improving mentalhealth in communities is to look beyondnarrowly de¢ned health care systems.Treat-ment of mental disorders requires more thanjust individual therapies for the su¡erers.They should also foster the inclusion of men-tal health interventions into general healthsystems, thereby strengthening policies(Jenkins et al., 2011), as well as foster integ-ration of mental health aspects in generalsocial policies to improve the wellbeing ofthe population (Friedli, 2009). A recentconsensus seeking exercise among hundredsof researchers, advocates and clinicians,identi¢ed themost urgent research priorities
rized reproduction of this article is prohibited.197
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarian
for improving the lives of people withmental illness around the world. The ¢vemost important areas to be researched arerelated to:1) strengthening themental healthcomponent in the training of all health carepersonnel, 2) integrating screening and corepackages of services into routine primaryhealth care,3) reducing the cost and improv-ing the supply of e¡ective medications, 4)providing e¡ective and a¡ordable com-munity based care and rehabilitation,and 5) improving children’s access to evi-dence based careby trained health providersin low andmiddle income countries (Collinset al., 2011).One of the main strategies to improveaccess of the population to mental healthservices is to integrate such services withinthe general health care system, and to avoidstand-alone systems based on specialisedpsychiatric hospitals. Integrating mentalhealth services into primary health care(PHC) is often considered the most viableway of ensuring that people get the mentalhealth care they need (World HealthOrganization & Wonca, 2008). Primaryhealth care is de¢ned as the ¢rst level ofhealth system contact with the population.It includes various aspects, such as: healthpromotion, prevention, care for commonillnesses, and management of on-goingchronic health problems. Primary healthservices act as the principal point of consul-tation for patients within a health caresystem, and depending on the conditions ofthe system in the area, and the type ofstructure, it can be carried out by a doctor,nurse, midwife, community health worker,traditional healer, or members of the groupor the community. There is no single bestpractice model for the integration of mentalhealth care into PHC that ¢ts all contexts.In documenting 11 examples of successfulintegration of mental health care into
primary care, only one country, Uganda,was a post con£ict or post emergencysetting (World Health Organization &Wonca, 2008). Among the basic require-ments to make the integration a success areelements such as adapting mental healthpolicies, ensuring that primary care workersare adequately trained, organisingappropri-ate supervision, ensuring that primary careworkers are not burdened with unrealisticamounts of tasks, and making specialistmental health care professionals andfacilities available to support primary care.One important practical lessonwas the needto collaborate with other government nonhealth sectors, nongovernmental organis-ations (NGOs) and community networks.The World Health Organization haslaunched the comprehensive mental healthGap Action Programme (mhGAP) toaddress this lack of care, especially in lowand middle income countries, for peoplesu¡ering from mental, neurological andsubstance use disorders. This includes anintervention guide with evidence basedmental health interventions for generalhealth workers (World Health Organiz-ation, 2010). There is now an urgent needto use these available tools on a largerscale, and to document what we canlearn from the process to scale up mentalhealth services in low resource settings(Eaton et al., 2011).
A closer look at mental healthinterventions in emergencies:what should be done?There is an important and large gapbetween the rapidly increasing knowledgebase on community mental health care inlow and middle income countries, and themental health and psychosocial work that isactually done in emergencies (Allden et al.,2009). One important challenge in planning
rized reproduction of this article is prohibited.
Copyrig
Ventevogel et al.
mental health services in complex emer-gencies is how to ensure that the servicehas immediate, measurable bene¢ts, whileat the same time building a model that is-sustainable and ultimately integratedwithin the broader primary health service(Silove,2004b).TheWorld Health Organiz-ation advocates strengthening pre-existingmental health services. Particularly afterthe most acute distress has decreased, andthe most basic needs have been addressed,e¡orts should be directed towardsestablishing a more comprehensive rangeof community based mental health inter-ventions, ensuring that 1) people withsevere mental disorders (e.g. psychosis,severe depression) have access to e¡ectivecare in the community, 2) mental healthcare is available within general healthsettings and 3) links to outside the formalhealth sector are established and madefunctional. This last point could include,for example, training and supervisingof social workers, teachers, communityleaders, and, when feasible, and traditionalhealers (van Ommeren, Saraceno, &Saxena,2004).Many papers published on mental healthproblems in humanitarian emergenciesfocus on the prevalence of mental disorders,with a strong emphasis on posttraumaticstress disorder (PTSD) and depression.Reported prevalence ¢gures of depressionand PTSD vary widely between surveysof con£ict a¡ected populations.While thismay be a result of contextual factors,such as the extent of exposure to adversity,they are also strongly a¡ected bymethodological di¡erences (Rodin & vanOmmeren, 2009). Trauma focused surveysare also often unable to identify the e¡ectsof a complex emergency on a population’sability to care for itself (Ager, 2002), or toidentify locally used cultural expressions
on the lack of wellbeing (Miller, Kulkarni,& Kushner, 2006). Prevalence rates ofsevere mental disorders, such as psychosisand bipolar disorder, are largely unknown.A rough estimation is that a humanitariancrisis leads to an increase of the prevalenceof severe mental disorders from 2^3% to3^4% in the ¢rst 12 months, and forcommon mental disorders from anestimated 10% at baseline (pre-crisis) to20% (van Ommeren, Saxena, & Saraceno,2005). In striking contrast to the impressiveamount of scienti¢c papers on prevalence¢gures in complex emergencies, is thedearth of papers describing the outcome ofactual interventions to tackle such pro-blems. The published literature is skewedtowards psychological interventions forPTSD. This emphasis on trauma relatedmental problems is not consistent with thekind of programmes that are usually imple-mented, and for which there is an urgentneed to assess the e¡ectiveness. MHPSSinterventions initiated by external actors,such as international NGOs, frequently arenot well connected to existing systems ofcare. A recent survey of 160 reports of actualinterventions found that the vast majority ofthem took place and were funded outsideexisting systems of care, such as nationalmental health care systems (Tol et al., 2011).A World Bank report in 2005 identi¢edthis lack of systematic documentation ofmental health and psychosocial inter-ventions in post emergency and postcon£ict settings as the major obstacle tomore e¡ective and better targeted interven-tions (Baingana, Bannon, & Thomas, 2005).Others have called for a public discussion onthe results of assessments and evaluations ofmental health activities in complex humani-tarian emergencies, so that lessons canbe learnt for future interventions (Mollicaet al., 2004).
rized reproduction of this article is prohibited.199
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarian
How trying to help can makethings worse: the example ofSri LankaIn the aftermath of some humanitarianemergencies, the in£ux of organisationsand groups providing all kinds of assistancecan be quite overwhelming. More to thepoint, they may also inadvertently under-mine existing assistance structures, and dis-credit local ways of coping with adversity.This has been poignantly described in posttsunami Sri Lanka, where delivering ofmental health care and psychosocial supportin a¡ected areas was compromised by themassive destruction of infrastructure, anddi⁄culties coordinating responses betweenmany organisations were involved (Ashraf,2005). A Sri Lankan psychiatrist, Ganesan(2006), saw dozens of experts in mentalhealth and psychosocial support being‘parachuted’ in to the east coast of Sri Lankato start a multitude of trauma- focussedactivities, while there was far less attentiongiven to much more urgent social workprojects and programmes to care for thosewith severe mental disorders such as psy-chosis. In his chapter ‘The wave that brought
PTSD to Sri Lanka’, Watters (2010) providesdisconcerting examples of the rather toxiccombination of cultural naivete¤ and thetherapeutic arrogance of many of theseexperts. Humanitarian interventions, suchas mental health training of local sta¡,may amount to the imposition of westernconcepts of distress and disorder, to popu-lations with di¡erent ways of understandinghuman su¡ering (Abramowitz, 2010). More-over, the e¡orts of outsiders to providemental health assistance tends to obscurethe e¡orts by local stakeholders (Fernando,Pedersen, &Weerackody, 2010).There is alsoa risk that NGO programmes take awaymental health professionals from the publicsystem. As Ganesan (2011) mentions in this
issue, he was the only psychiatrist in theheaviest a¡ected area of Sri Lanka posttsunami, and felt pressured by externalagencies and the media to decrease the timehe spent treating people with severe mentaldisorders, and to favour trauma focusedinterventions of the newly started pro-grammes instead.
How something good may comeout of a disaster: the example ofSri LankaFortunately, there are also good exampleswhere mental health interventions in thesetting of complex humanitarian emer-gencies have had long lasting, positivee¡ects on mental health service delivery.Again, Sri Lanka may serve as an example.The ¢nancial aid generated as a responseto the tsunami boosted the developmentof community centred, and therefore decen-tralised, mental health care in Sri Lanka.For example, in the northern town ofJa¡na, local organisations and authoritiesformed a joint Mental HealthTask Force inthe ¢rst months after the disaster, in orderto coordinate their activities (van der Veen& Somasundaram, 2006). The ad hoc taskforce was later transformed into a formalintrasectoral, coordinating body for localgovernmental and NGOs involved inmental health and psychosocial work, andcontinued to be a driving force for improv-ingMHPSS services in the area (Krishnaku-mar, Sivayokan, & Somasundaram, 2008).Prior to the tsunami, in the north-easternareas of Sri Lanka, there was a long historyof protracted armed con£ict. There, localmental health workers had already startedinnovative mental health services withinsecondary and primary care. The WorldHealth Organization advised using thismodel for other districts in Sri Lanka (Sara-ceno& vanOmmeren,2003). Unfortunately,
rized reproduction of this article is prohibited.
Copyrig
Ventevogel et al.
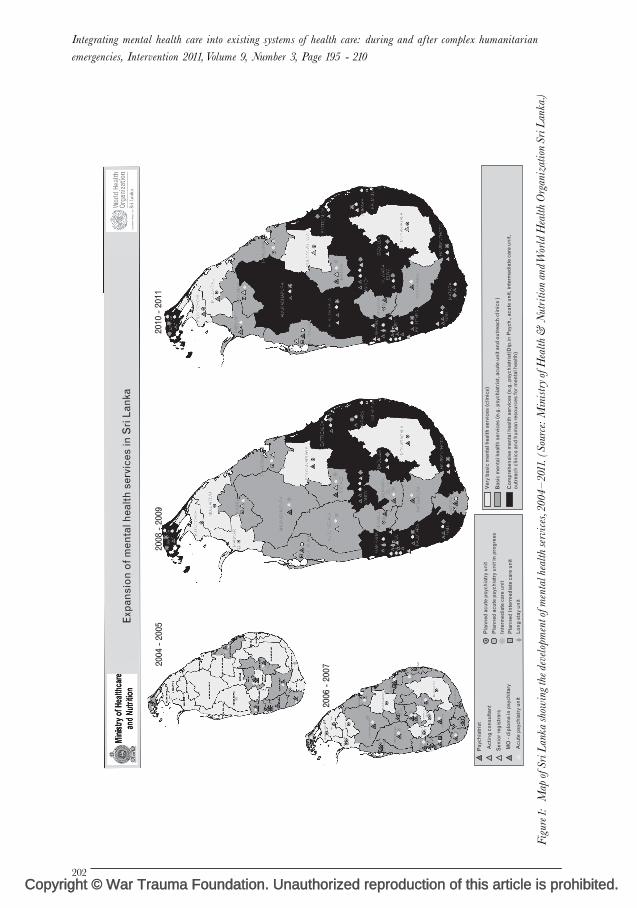
donors were initially uninterested, that isuntil the 2004 Asian tsunami. The suddenavailability of funds for mental health careprompted the development of a nationalmental health policy that encourageddecentralisation of service, and that wasde facto based on the innovative workdeveloped in the con£ict a¡ected areasin the north east (Saraceno, 2005). Theincreased awareness of the importance ofmental health care after the tsunami,prompted the establishment of decentralisedmental health services integrated intogeneral health care, and led to training ofgeneral health workers to provide treatmentfor people with mental health problems inthe tsunami a¡ected areas (Mahoneyet al., 2006). Several years after the tsunami,there are still mental health services inseven tsunami a¡ected districts of SriLanka, run by the Ministry of Health(WHO, 2008). A map of the diversityand spread of mental health servicesshows the improvements quite dramatically(Figure 1).
The importance of documentingexperiencesThe brief examples of Sri Lanka abovemay serve to highlight the importance ofdescribing the process of how interventionsin these settings, often starting with a reliefperspective, can lead to more fundamentalchanges in mental health service delivery.Perhaps there are many experiences ofmental health care being integrated intoexisting systems of care during humani-tarian emergencies, but to our knowledge,they are rarely documented. Edited volumeson mental health in post war and postcon£ict settings pay limited attention toaspects related to the integration of mentalhealth care into existing systems, and focus
instead on the development of NGO basedservices. Or they describe the immediatemental health response without taking alonger term perspective, while in turn,books on mental health care developmentin resource poor settings often do notaddress the speci¢c context of humanitarianemergencies.There are many reports of successful mentalhealth training of general health workersin humanitarian settings (Budosan, 2011;Budosan et al., 2007; Henderson et al.,2006; Mohit et al., 1999; Sadik et al., 2011;Ventevogel & Kortmann, 2004). Thesearticles usually describe how it was feasibleto install basic mental health care skills ingeneral healthworkers. However, we are leftwith the question of what happened after?Some articles describe how attempts tostart primary mental health services withinprimary care proved feasible within theproject period, showing clear increases ofnumbers of patients receiving treatment(Budosan & Jones, 2009; Jones et al., 2007a;Jones et al., 2009; Somasundaram et al.,1999; Souza, Yasuda, & Cristofani, 2009).Yet, most of these publications focus ondirect output (building mental health skillsin sta¡, increasing the number of patientsin treatment) with less attention to a sys-tematic description of how these inter-ventions could contribute to long lastingchanges in public mental health servicesdelivery. It is rare to ¢nd published docu-mentation on how mental health projects,that started in the aftermath of a humani-tarian emergency, moved from a projectwith an initial focus on relieving immediatesu¡ering to long term programmes tostrengthen mental health care services.There are exceptions. In the 1980 s inGuinea-Bissau, then recovering from an18 year long war of independence, a com-munity mental health programme was set
rized reproduction of this article is prohibited.201
up to train primary health care workersin mental health, and the evolution of thisprogramme was described for a periodcovering more than a decade (de Jong,1996). InTimor Leste, overwhelmed by thee¡ects of mass violence, displacement anddestruction of infrastructure after its violentcessation from Indonesia in 1999, a mentalhealth care programme with a strongcommunity oriented outlook was describedfor a period covering more than a decade(Silove et al., 2011). In Afghanistan, afterthe fall of the Taliban in 2001, NGO ledmental health projects started with theaim of integrating mental health into exist-ing governmental health care services.Several NGOs and the WHO contributedto curriculum development and advocacyfor the inclusion of mental health intothe Basic Package of Health Services(Ventevogel, Faiz & van Mierlo, 2011).There are however many more complexhumanitarian emergencies in which govern-ments, local organisations and internationalNGO design and implement mental healthprogrammes. Unfortunately, little is knownabout these experiences. For example, inAceh, the emergency programme by aninternational NGO after the 2004 tsunami(Jones et al., 2007) was later taken overby another international NGO with astrong focus on development. The healthauthorities made annual budgetary allo-cation to continue the primary healthcentre based community mental healthservices, but this experience has not yetbeen documented (A. Mohanraj, personalcommunication). Much of the experienceof organisations that actually make thetransition from emergency relief to theadoption and promotion of structuralchanges in service delivery for people withmental disorders, remain undocumented tothis day.
Emergencies: risks andopportunities for strengtheningexisting mental health caresystemsComplex humanitarian emergencies createboth enormous challenges and opportunitiesfor structural improvement of mental healthservices. A discursive reading of the pub-lished literature led us to identify the follow-ing opportunities and challenges for thedevelopment of sustainable mental healthservices, during and after complex humani-tarian emergencies:
Risks
1. C
rize
reating parallel systems
The breakdown of often already weakand ine⁄cient public services oftenprompts aid organisations to startservices by themselves.While there maynot always be an alternative, the risk isthat unsustainable programmes arecreated, with the result that instead ofsupporting the public system, it mayundermine it. Interventions may focuson one particular type of ‘mentaldisorder’, while ignoring that the spec-trum of mental health problems incomplex emergencies is much broader(Summer¢eld,1999). If separate servicesare started, it is often challengingNGOs to make the transition towardsintegrated, horizontal programming(deJong, 2007).
2. I
nterventions by outsiders may ignore what
people do themselves
Humanitarian interventions maysilence, or marginalise, local perspect-ives and local views (Abramowitz &Kleinman, 2008). The acceptable, ordominant form of healing communitiesafter mass upheaval, is expected to comefrom humanitarian aid and this tends toobscure the healing the social wounds of war.
d reproduction of this article is prohibited.203
Copyright
Integrating mental health care into existing systems of health care: during and after complex humanitarian
In other words, how communitiesthemselves mobilise their own social,and other resources, in order to recoverin their own time and in their own way(Last, 2000).
3. M
edicalising non pathological distress and
social problems
TheWorldHealthOrganizationwarnsofthe risk of misapplication of the medicalmodel by general health workers withbasic training in mental health care(van Ommeren et al., 2004). This hasbeen documented as a real problem incomplex humanitarian emergencies,such as Afghanistan (Ventevogel, Faiz,& vanMierlo, 2011).
4. O
verburdening general health workers with
skills and knowledge they cannot useGeneral health workers in overloadedhealth care facilities have limitedtime for each encounter, and often donot have the time to go deeper intothe presented complaints and thereforemiss mental health disorders thatpresent as physical problems (Afanaet al., 2002).
5. P
roviding insu⁄cient supervision andfollowup
training
Systematic supervision and training,preferably attached to existing institu-tions, is an essential ingredient ofcapacity building, but may also be givenlimited attention in practice (Silove,2004a).
Many of these risks are not speci¢c to thesituation of complex humanitarian emer-gencies, but may become more pronouncedand urgent in such emergencies. Similarly,the unusual context of complex humani-tarian emergencies can also provide oppor-tunities that, again, may not be speci¢cfor these contexts, but may be morepronounced.
Some complex humanitarian emergen-cies, particularly those involving acutenatural disasters such as earthquakes ortsunamis, may generate many millionsof dollars in emergency relief. This isusually distributed by multilateralagencies and foreign governments, andtranslated into short term projects byinternationalNGOs.The unprecedentedamount of funding, in an otherwisedisadvantaged or marginalised region,can provide opportunities to start newinitiatives that boost mental health care.
2. P
ossibilities to involve di¡erent categories of
health workers in mental health activities
Themassiveneedsarising inemergenciesmay lead health authorities to acceptpiloting new initiatives formental healthcare provision, including the training ofgeneral health workers, the use of para-medical sta¡ and working closely withcommunities. Mental health care shouldbe linked with other sectors, outside thehealth care system in order to becomee¡ective on a community level (WorldHealth Organization, 2003). Perhaps themost powerful interventions to improvethe mental health status of people inimpoverished circumstances are outsidethe formal health sector. Interventionsdealing with mental health can playan important role in e¡ective postcon£ict reconciliation and reconstruc-tion (Baingana, Bannon, & Thomas,2005). The in£ux of organisations withcommunity focused orientations maymake help to improve such inter-sectorallinks.
3. I
ncluding mental health care in health sector
reforms
Mental health care should not beisolated from other parts of health care.
It needs to be linked with other, moregeneral approaches to strengthen thehealth care sector, including aspects suchas general health sector reform andresults based ¢nancing. Emergenciesoften lead to health sector reforms, andin several post con£ict settings, such asAfghanistan, Somalia and Liberia, thishas led to the incorporation of mentalhealth into minimum packages of care(Ventevogel et al., 2002). Health policymakers are also more likely to acceptand implement mental health carereforms (Munir et al., 2004; PanduSetiawan & Viora, 2006)
This Special Issue of Intervention documentsa variety of examples from mental healthprogrammes in the aftermath of naturaldisasters and armed con£ict. Some of themain lessons learned are described in theclosing article of this issue (Pe¤ rez-Saleset al., 2011). We hope it will contribute tobuilding an evidence base for integratingmental health care into existing systems ofhealth care, in complex humanitarianemergencies.
AcknowledgementsThe authors would like to thank Julian Eaton,
Ananda Galappatti, Andrew Mohanraj and
Mark van Ommeren for their comments on
earlier versions of this paper.
ReferencesAbramowitz, S. &Kleinman, A. (2008). Humani-
tarian intervention and cultural translation:
a review of the IASC Guidelines on Mental
Health and Psychosocial Support in Emer-
gency Settings. Intervention, 6(3/4), 219-227.
Abramowitz, S. A. (2010). Trauma and humani-
tarian translation in Liberia: the tale of open
mole.Culture,Medicine&Psychiatry, 34,353-379.
War Trauma Foundation. Unautho
Afana, AH., Dalgard, OS., Bjertness, E. &
Grunfeld, B. (2002). The ability of general
practitioners to detect mental disorders
among primary care patients in a stressful
environment: Gaza Strip. Journal of Public
HealthMedicine, 24(4), 326-331.
Ager, A. (2002). Psychosocial needs in complex
emergencies. Lancet, 360(Suppl), s43-s44.
Ager, A., Strang, A. & Wessells, M. (2006).
Integrating psychosocial issues in humani-
tariananddevelopment assistance:A response
to Williamson and Robinson. Intervention, 4,
29-31.
Allden,K., Jones, L.,Weissbecker, I.,Wessells,M.,
Bolton, P., Betancourt, TS. & Sumathipala,
A. (2009). Mental health and psychosocial
support in crisis and con£ict: report of the
mental health working group. Prehospital &
DisasterMedicine, 24(Suppl 2), s217-s227.
Ashraf, H. (2005).Tsunami wreaks mental health
havoc. BulletinWorld Health Organization, 83(6),
405-406.
Baingana, F., Bannon, I. & Thomas, R. (2005).
Mental health and con£icts. Conceptual Framework
and Approaches.Washington, DC:World Bank.
Bloom, DE., Ca¢ero, ET., Jane¤ -Llopis, E.,
Abrahams-Gessel, S., Bloom, LR., Fathima,
S. & Weinstein, C. (2011).The Global Economic
Burden of Non-communicable Diseases. Geneva:
World Economic Forum.
Budosan, B. (2011). Mental health training of
primaryhealthcareworkers: case reports from
Sri Lanka, Pakistan and Jordan. Intervention,
9(2),125-136.
Budosan, B., & Jones, L. (2009). Evaluation of
e¡ectiveness of mental health training
rized reproduction of this article is prohibited.205
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarian






























![Monochromatic Camping Event Flyer - Redefining Refuge · • 4 event tickets with VIP Experience and early access PROSECCO | $1,000 [Rede!ning Refuge] is a 501 C (3) Organization.](https://static.documents.pub/doc/80x56/5f379ab501171d23cb625c86/monochromatic-camping-event-flyer-redefining-refuge-a-4-event-tickets-with-vip.jpg)

