67
1 An introduction to diagnostic microbiology Dr Patrick Kimmitt HCPC registered Clinical Microbiologist
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | sof9555555 |
| View: | 27 times |
| Download: | 3 times |
1
An introduction to diagnostic microbiology
Dr Patrick Kimmitt
HCPC registered Clinical Microbiologist

2
Aims of this session
• To give an overview of the principles and practice of diagnostic microbiology
• To contrast investigations of the 4 general groups of pathogens
• To consider the reasons why so many different types of test are used
• To use the respiratory tract to illustrate different approaches to the investigation of pathogens

Recap
• I am assuming you have read the documents provided?
• You should have a basic understanding of the use of bacterial culture media, different types of media and why different types are needed
• You should also understand approaches to the diagnosis of viral pathogens and why and how they are used
3

Some extra help
• Check out my YouTube channel DrKimmitt for podcasts to support your learning on this module
• These podcasts + more can be found at www.drkimmitt.co.uk
• Please use the module site discussion board
4
5
We are making some assumptions about you
• That you know that there are 4 groups of human pathogens!
• That you know their biological characteristics!• That you know the important diseases that they
cause!• That you know the symptoms of these diseases
are due to the interaction between these pathogens and our immune system!
6
Some general principles
• The Standard Operating Procedures employed by many laboratories for the investigation of infectious diseases are well established.
• They are based on accumulated experience about which pathogens are most likely to cause a patient’s symptoms and the predictable properties of these pathogens
7
Normal flora
• Some parts of our bodies are sterile and so the presence of any microorganism may be significant
• Other parts have a normal flora that may make detection of a pathogen more difficult
• The site of infection may therefore influence the laboratory approach

8
Types of microbiological investigations
• Traditionally: M, C + S• Can try to see the pathogen – microscopy • Can try to grow the pathogen – isolation or
culture• Can investigate whether or not an isolated
pathogen is susceptible (sensitive) to an antibiotic
9
Bacteria
• Can they be seen using a microscope?• Can they be easily grown in vitro?• Can sensitivity tests be performed?
• Yes, if stained – light microscopy• Yes, using solid agar media• Yes, widely tested

10
Viruses
• Can they be seen microscopically?• Can they be easily grown in vitro?• Can sensitivity tests be performed?
• Only with electron microscopy• Only by using cell culture• Not using typical methods
11
Fungi
• Can they be seen microscopically?• Can they be grown in vitro?• Can sensitivity tests be performed?
• Yes, they are larger than bacteria• Yes, on different solid agar media• Yes, in a similar way to testing bacteria
12
Parasites
• Can they be seen with a microscope?• Can they be grown in vitro?• Can sensitivity tests be performed?
• Yes, staining for protozoa, not worms• Possible, but rarely attempted• Rarely attempted.
13
Culture media
• Please see notes in Blackboard and YouTube podcasts

14
Immunological tests
• Serology /serologic tests• Based on antibody-antigen reactions• Early tests were developed to detect the
presence (or absence) of antibodies in a patient’s peripheral blood
• Later tests can now also detect the presence of antigens associated with particular pathogens
• There are a whole range of these and they may be available as commercial kits and be highly automated
15
Types of serological tests
• Complement fixation test (CFTs): of great historic importance but less so today
• Agglutination tests: recognition of Ag by Ab results in a visible clumping of the complex
• Latex agglutination + Haemagglutination: by attaching the Ag to latex particles or RBCs, agglutination is easier to detect
• Precipitation tests: Ab and Ag allowed to diffuse towards each other in a gel; positive reaction results in visible lines of precipitation
16
Antibody vs antigen screening
• You must know the difference between an antibody and an antigen
• Antibody screening was introduced first but ultimately is of little value to patient management in most cases – why?
• Detection of pathogen-specific antigen indicates that a pathogen is present in a patient sample

17
Other serological tests
• Enzyme-Linked Immunosorbent Assay• An example of a ‘modern’ test that is
widely used:• Can detect antigen or antibody, can
distinguish different antibody classes e.g. IgM or IgG (why might this be important?)
• Can be automated• High specificity + sensitivity

18
Other serological tests
• Immunofluorescence• Uses a pathogen specific antibody to
detect the presence of antigen on the surface of the pathogen
• The antibody is labelled with a fluorescent molecule at its non-binding end
• Antigen-antibody complexes are detected by fluorescence microscopy

19
Clinical specimens
• Successful microbiological investigations rely heavily on the correct specimen being taken from the patient
• Must be transported rapidly to the laboratory in a sterile container
• Must be taken from the site at correct time• Some specimens are easier to collect than
others
20
‘Sampling sites’
• Sites that should be sterile• Blood• Cerebrospinal fluid• Tissues• Lower respiratory tract• Bladder
• Sites with normal flora• Mouth + nose• Upper respiratory tract• Gastrointestinal tract (except stomach)• Female genital tract• Urethra

21
Specimens
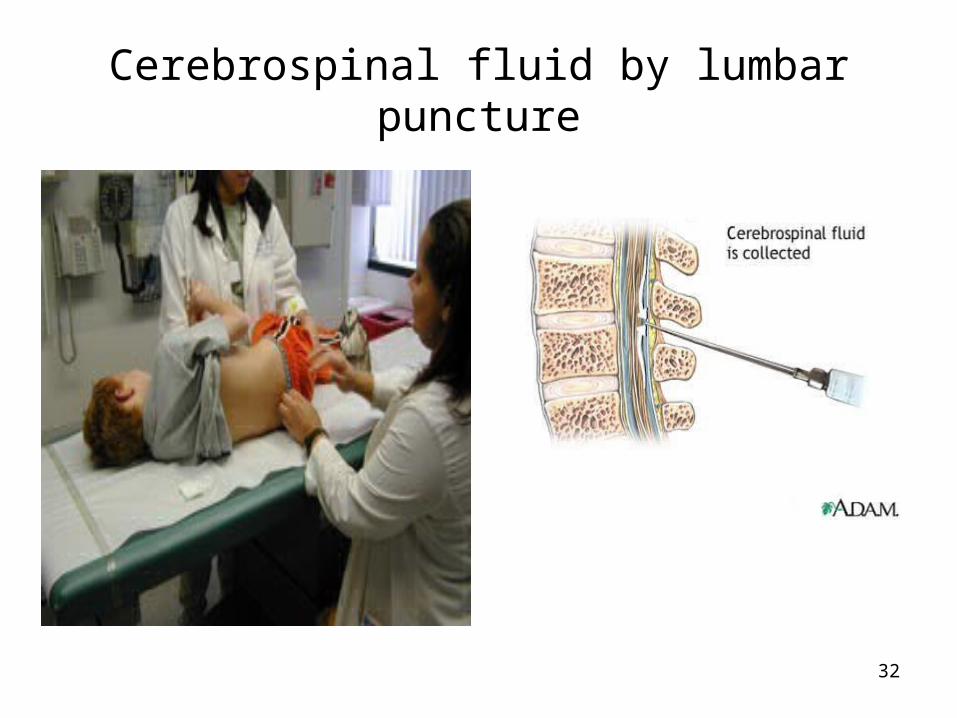
• Gastrointestinal tract• Urinary tract• L. respiratory tract• Skin• U. respiratory tract• Urethra• Cerebrospinal fluid• Tissues• Cardiovascular• Abscess
• S*** a.k.a. faeces or stool• Midstream urine• Sputum• Skin swab• Swabs• Urethral swab• Lumbar puncture: CSF• Biopsy, aspirate• Blood• Pus
22
Processing of specimens
• On arrival, specimen is processed by type, e.g. based on whether it is urine, faeces etc or on what type of swab it is.
• Processing really means deciding on the appropriate tests to carry out
• Microbiologists will know the type of pathogen, or normal flora likely to be present
• Also need some clinical information to help with decisions
23
Likely pathogens
• Early decision needs to be taken on the likely pathogen
• Is it likely to be a bacterium, fungus, virus or parasite?
• Is most likely to be a bacterium or virus • Depending on the decision, in UK,
specimen will be sent to Virology lab. or Bacteriology lab. (will cover fungi + parasites)

24
Benches
• Depending on type of investigation selected, specimen is assigned to a particular ‘bench’ e.g. ‘urine bench’
• There, the appropriate techniques are performed by biomedical scientists who will follow appropriate SOPs
• They should also receive appropriate clinical information

25
Typical benches/areas
• Urine• Faeces• Respiratory for swabs• Wounds• Blood cultures• MRSA• Tuberculosis

26
Upper respiratory tract
• Upper respiratory tract• Mainly swabs • Mainly bacterial pathogens• Some fungi• Extensive normal flora
27
Lower respiratory tract
• Lower respiratory tract• Pneumonia or Tuberculosis• High risk sputum• Must use a specialised lab and safety
cabinet for Category 3 containment
28
Some other clinical specimens

29
Swabs
• Very widely used and come in a variety of types

30
Faeces (Stool)
• The stool sample is often ‘improperly formed’……………

31
Pus
32
Cerebrospinal fluid by lumbar puncture

34
Blood cultures

Automation
• A few years ago labs who could afford it started using machines such as the VITEK II system
• This is semi-automated and can perform a full ID and sensitivity test in 4 hours
• Previously this took 24 hours or more
35

Automation
• Companies such as Kiestra are introducing fully automated microbiology labs
• Systems will inoculate, incubate and read plates
• MALDI-TOF is being used for rapid identification of pathogens
• A concern for the existing workforce!
36
37
Molecular testing
• Detection of nucleic acid of pathogens DNA or RNA
• Polymerase Chain Reaction including Real-time PCR and Reverse transcriptase PCR
• There are a number of other molecular technologies also in use e.g. NASBA, Reverse Hybridisation, SDA etc...

Next generation sequencing
• For labs who can afford it new sequencing platforms can sequence the genome of a microorganism within a few hours
• In the not too distant future this may become part of the routine work of the Biomedical Scientist
• Sequence the genome, ID, susceptibility and epidemiological information available in ‘real-time’
38
39
Whatever the techniques, the end results should be the same!
• A report on presence or absence of a pathogen/pathogens
• The identification of the pathogen(s)• Some guidance given to clinician on
appropriate antibiotic to be used if treatment is needed
Tuberculosis
• Chronic respiratory infection (+ sometimes other sites) where the causative organism resides in the lungs, withstands phagocytosis and causes fibrosis and necrosis of lung tissue
• Caused by Mycobacterium tuberculosis • Has a thick waxy cell wall containing
mycolic acids which resists phagocytosis
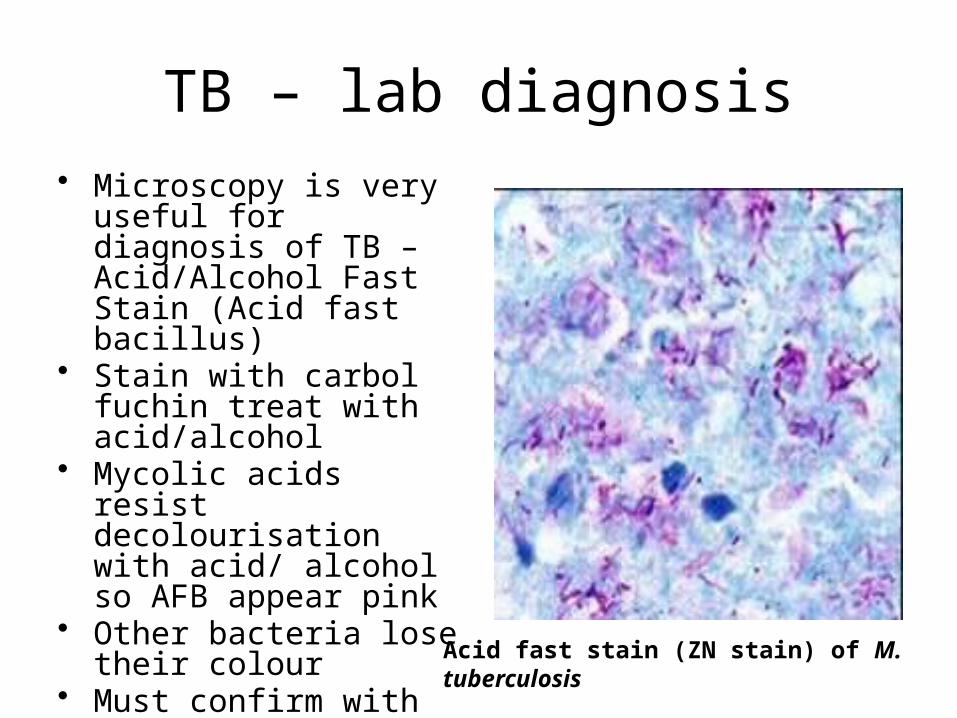
TB – lab diagnosis• Microscopy is very useful
for diagnosis of TB – Acid/Alcohol Fast Stain (Acid fast bacillus)
• Stain with carbol fuchin treat with acid/alcohol
• Mycolic acids resist decolourisation with acid/ alcohol so AFB appear pink
• Other bacteria lose their colour
• Must confirm with culture
Acid fast stain (ZN stain) of M. tuberculosis
TB - culture
• Problem – M. tuberculosis one of the slowest growing bacteria – mean generation time 12-18 hrs (compare with E. coli 20-30 mins)
• Use specialist medium - Lowenstein-Jensen (contains egg) and incubate for up to 8 weeks
• Use slopes not plates so the media doesn’t dry out
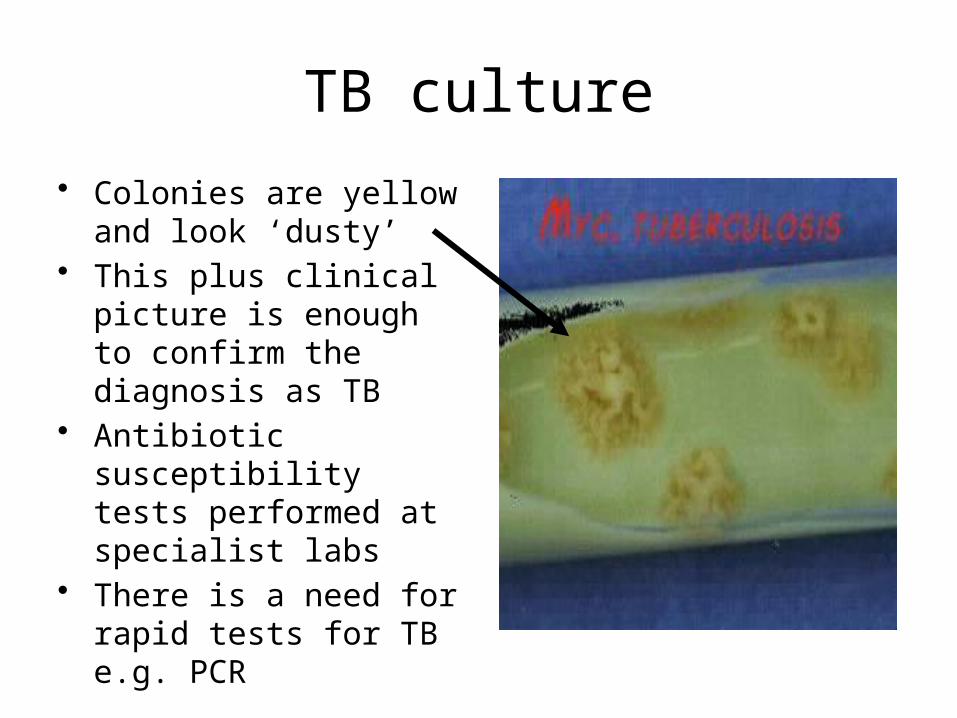
TB culture
• Colonies are yellow and look ‘dusty’
• This plus clinical picture is enough to confirm the diagnosis as TB
• Antibiotic susceptibility tests performed at specialist labs
• There is a need for rapid tests for TB e.g. PCR
Streptococcus pyogenes
• Causes a number of different infections including pharyngitis and Scarlet Fever (rare but increasing)
• Streptococcus contains many species, many reside in the URT as part of the normal flora – others are pathogenic
• Enterococcus is closely related and found in the gut
• We need to be able to distinguish between the different species and also to differentiate Streptococcus from Staphylococcus
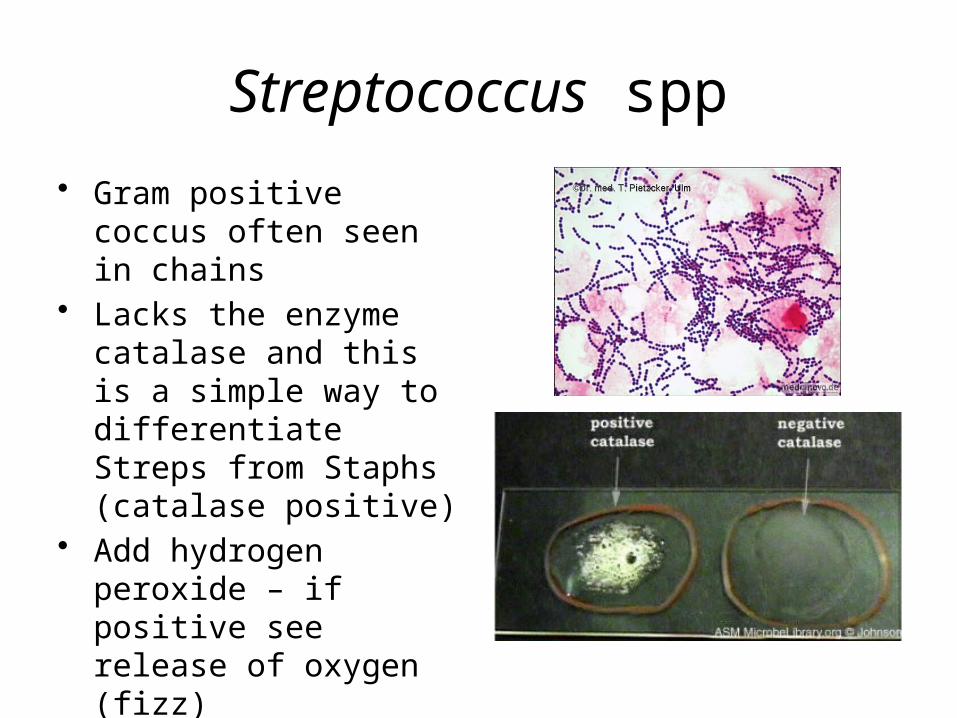
Streptococcus spp
• Gram positive coccus often seen in chains
• Lacks the enzyme catalase and this is a simple way to differentiate Streps from Staphs (catalase positive)
• Add hydrogen peroxide – if positive see release of oxygen (fizz)

Differentiation of Streptococcus• First stage is to look at
the type of haemolysis on blood agar
• Haemolysins are produced which lyse red blood cells in the agar
• β-haemolysis is a clear zone around the colony
• α-haemolysis is uncomplete haemolysis and has a green tint
• S. pygoenes is β-haemolytic
Βeta-haemolysis
Alpha-haemolysis

β-Haemolytic Streptococcus
• This group can be further divided on the basis of their cell wall polysaccharides
• Known as Lancefield grouping – main groups are A, B, C, D, F & G
• Streptococcus pyogenes is group A
• Simple agglutination test using group specific antisera
Rebecca Lancefield 1895-1981

α-Haemolytic Streptococcus
• Also known as the ‘viridans’ group• Most are members of the URT flora but
can cause infections e.g. endocarditis• However there is one major pathogen in
this group – Streptococcus pneumoniae• Causes bronchitis and pneumonia (and
meningitis)• How do we differentiate this species from
the other members of the viridans group?

Streptococcus pneumoniae
• S. pneumoniae is sensitive to a chemical called optochin
• All the other viridans streps are resistant
• This is the basis for a simple test for S. pneumoniae – look for green colonies and a zone of no growth around the disc
Optochin - 4β,8α,9R)-6'-Ethoxy-10,11-dihydrocinchonan-9-ol
Influenza
• Causes flu which is primarily a disease of the upper respiratory tract
• In some cases it can cause pneumonia – life threatening
• There are two major forms of flu– Seasonal– Pandemic (e.g. swine flu)
• We need to be able to detect the presence of influenza virus and then the type of strain – typically use a nasopharyngeal aspirate

Diagnostic tests for influenza
Diagnostic test Time for result Problems
Electron microscopy 2-3 h Poor sensitivity, expensive instrument
Viral culture 3-10 days Slow, cumbersome
Immunofluorescence 2-4 h Insensitive, labour intensive
PCR 2-4 h Lack of expertise/ validation
Antibody detection 2-6 weeks Very slow
ELISA for virus antigen 2 h Uses expensive equipment
Immunochromatography 30 mins Insensitive

Virus cell culture• Certain mammalian cells
are susceptible to certain viruses – the virus kills the cells & produces a specific cytopathic effect (CPE)
• This is the basis of an important lab test for viruses - clinical samples are used to infect tissue culture lines
• Use a cells line that is susceptible to the virus to be detected
See virus induced CPEs here: http://www.microbiologybytes.com/video/virus.html
Virus cell culture

Virus cell culture
Immunofluorescence
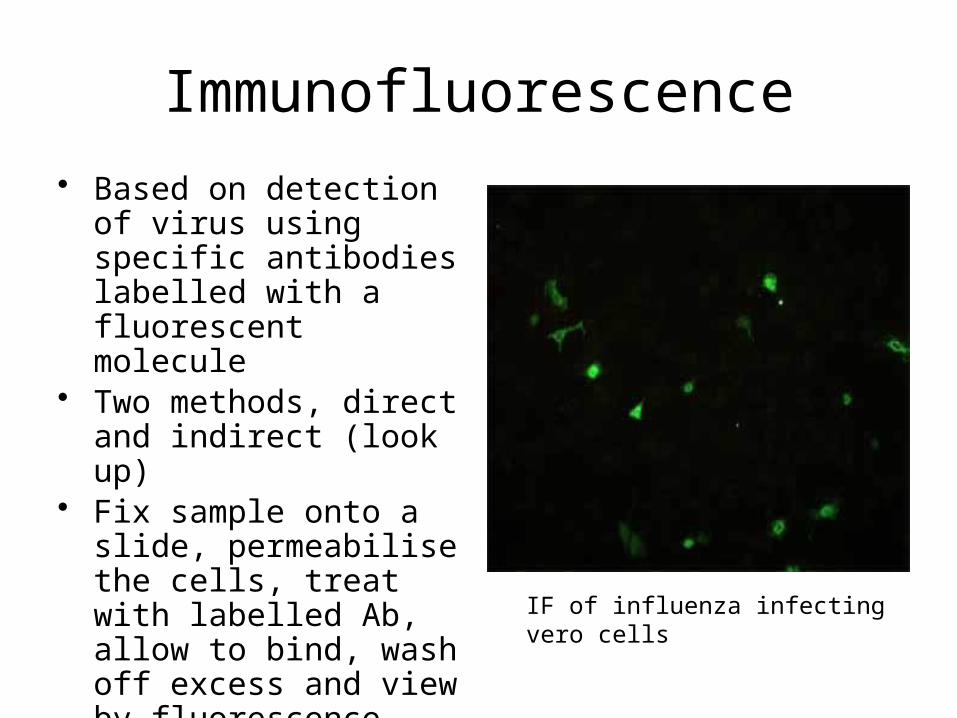
• Based on detection of virus using specific antibodies labelled with a fluorescent molecule
• Two methods, direct and indirect (look up)
• Fix sample onto a slide, permeabilise the cells, treat with labelled Ab, allow to bind, wash off excess and view by fluorescence microscopy
IF of influenza infecting vero cells
Serology
• Can determine the presence of infection by demonstrating an increase in influenza antibodies in patient serum
• Two samples required one during the illness (acute) and one 30 days later (convalescent)
• Measure antibody levels in both samples using an ELISA test
• An increase in convalescent titre indicates infection
• Alternatively use a test which specifically detected influenza IgM antibodies

Enzyme Linked Immunosorbant Assay
• Can be used for detection of influenza antigen
• Will be covered in the Immunology module, please research this technology
69
Immunochromatography
• A.k.a. Lateral flow test• Simple, easy to use test involving adding sample
plus reagents to a solid matrix or card• Can be used as a Point of Care test to be
performed in the lab, on the ward, in the field or at home
• Point of care testing is becoming increasingly important and while attractive in principle there are important implications to be considered with this approach

Immunochromatography

Immunochromatography
• Patient sample dropped onto a membrane• Virus antigen forms an immunocomplex when it
comes into contact with antibody coated latex particles
• Capillary action moves the complex down the membrane where it contacts a detection antibody
• Binding triggers an enzymatic detection system an a visible colour change if the sample contains the virus
• e.g. QuickVue Influenza kit

Pneumocystis jiroveci
• Formerly known as Pneumocystis carinii this is a fungus which causes pneumonitis (PCP) almost exclusively in patients with HIV
• It was practically unknown before the HIV pandemic
• Causes life-threatening infection in HIV patient, not pathogenic in healthy individuals

PCP
• PCP is diagnosed by collecting a sample of sputum or bronchial washing
• Can perform immunofluorescence or staining with e.g. Grocott silver and observe characteristic morphology

Aspergillus
• The genus Aspergillus is a fungus which causes respiratory infection only in immunocompromised patients and special cases e.g. cystic fibrosis
• In the immunocompromised especially those who have undergone transplants can cause life-threatening infection.
• Fungi have characteristic structures so microscopy is useful in diagnosis
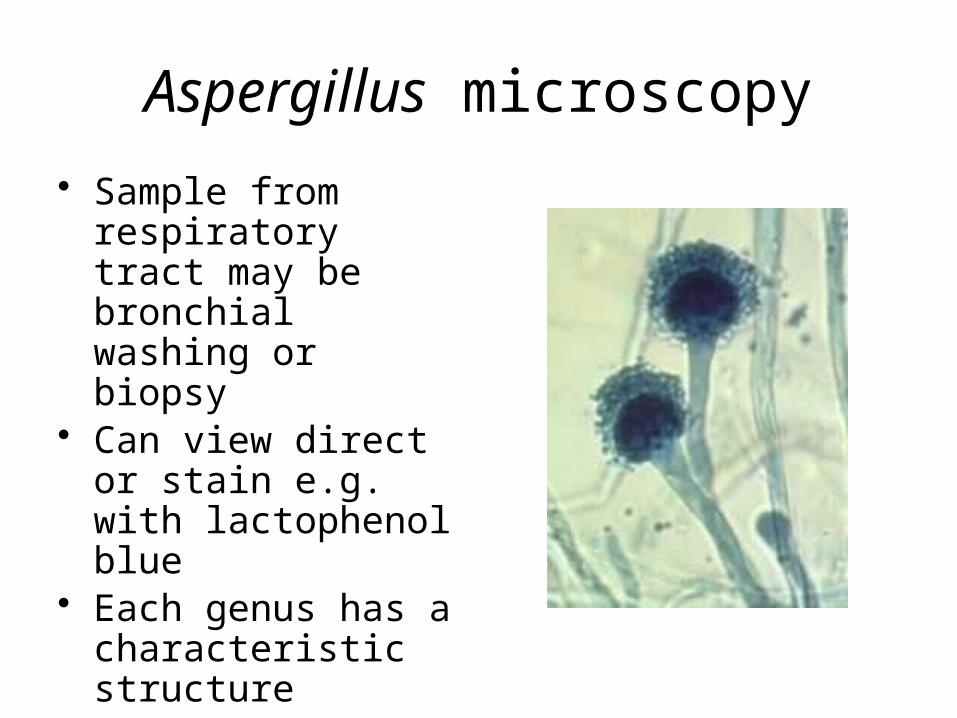
Aspergillus microscopy
• Sample from respiratory tract may be bronchial washing or biopsy
• Can view direct or stain e.g. with lactophenol blue
• Each genus has a characteristic structure
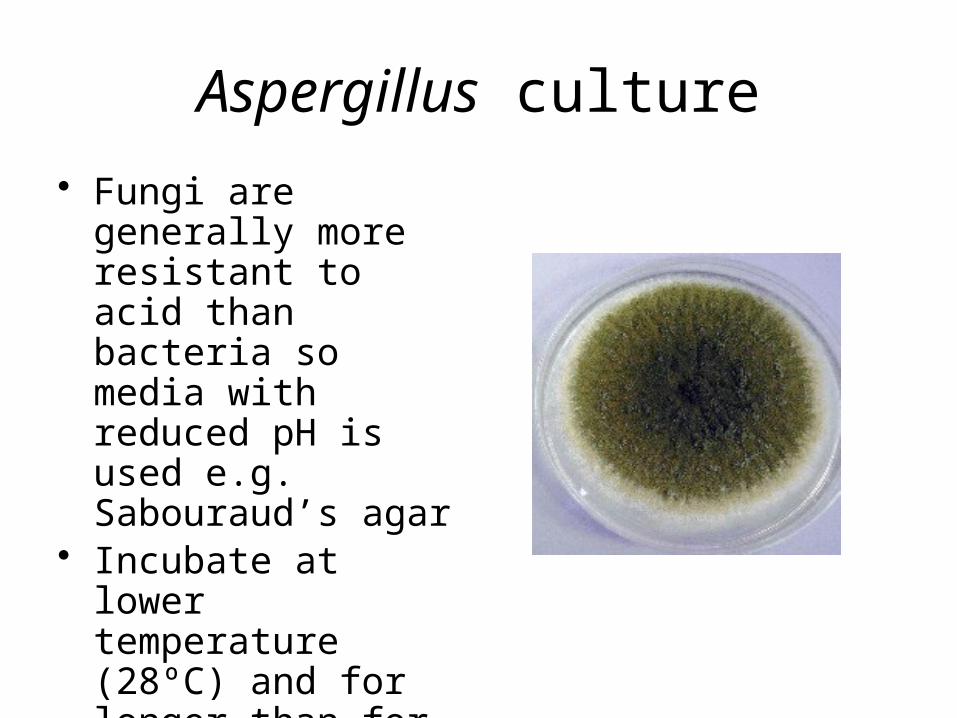
Aspergillus culture
• Fungi are generally more resistant to acid than bacteria so media with reduced pH is used e.g. Sabouraud’s agar
• Incubate at lower temperature (28ºC) and for longer than for bacteria
• ID by microscopy
What you need to know...
• You need to know what medical microbiologists do and how the lab is organised
• To understand and contrast how investigations of the four groups of pathogens is performed with reasons
• What types of samples are received and what are the considerations before samples are processed e.g. normal flora
77
What you need to know...
• Knowledge of the range of different tests available and the reasoning behind why some are used in SOPs but not others
• An understanding of the use of culture media including selective and enrichment media
• An understanding of the applications of immunological tests and their limitations
• Knowledge of what tests are available to detect bacterial, viral and fungal pathogens
78
Finally…
• What will the lab you may work in look like?
• Consider the impact of automation, molecular technologies and point of care testing
79

















