22
An uncommon route for an uncommon pathogen Brittany Folks, MD PGY2 Exempla Saint Joseph Hospital Denver, Colorado

An uncommon route for an uncommon pathogen
Brittany Folks, MD PGY2 Exempla Saint Joseph Hospital
Denver, Colorado

Q: What do a cow and a knee have in common?

The Patient
• 81 yo Hispanic gentleman • PMH: DM2, osteoarthritis of knees • Meds: diclofenac, ibuprofen, ASA, PPI,
multiple herbs and supplements • Social:
– No smoking, EtOH, or illicits – Resides in the US the majority of year – Travels to Chihuahua Mexico to his cattle ranch

The Presentation
• Chronic knee swelling 2/2 OA • Cough, hemoptysis, and weight loss for 2-3
months • Substernal CP, dyspnea, dizziness for 8 days • Progressive somnolence and fatigue for 2-3
days • ROS: + L hip pain, otherwise negative

The Exam
• VS normal • Bibasilar crackles • Normal heart sounds • No JVD • Pedal edema • Prepatellar L knee swelling • Oriented to self only

The Initial Work Up
• Na 130 • Cr 1.3 • Hb 12, Hct 36 • Trop 0.08 • BNP 200 • Lactate 1.3 • UA with small blood, trace LE, rare bacteria, 8
WBC



The Initial Course
• TTE obtained showed EF 50% with severe apical and septal hypokinesis, mild RV dilatation, grade I diastolic dysfunction
• ECG remained unchanged • Troponins negative x2 • Gently diuresed • Started on antibx for CAP
And Then…
• Antibx were broadened, antivirals were added • Transferred to ICU for worsening septic picture • Amphotericin was added with some
improvement initially • Developed progressive swelling of his knees
bilaterally • Liver enzymes became elevated • Decompensated and was placed on vent • Underwent bronchoscopy, LP, bone marrow bx,
joint fluid aspiration
The Work Up
• Mycoplasma • Hep A • Hep B • Hep C • HIV • Francisella • Parasite screen • Yersinia • Legionella • Leptospira • Chlamydia
• Coccidioides • Hantavirus • AFB • Brucella • Histoplasma • HSV • CMV • Coxiella • ANA • ANCA • Quantiferon
gold
• Sputum cx • Blood cx • Body fluid cx • Body fluid
analysis • MRI L spine • MRI hip • MRI brain • CT chest • CT abd • CT pelvis
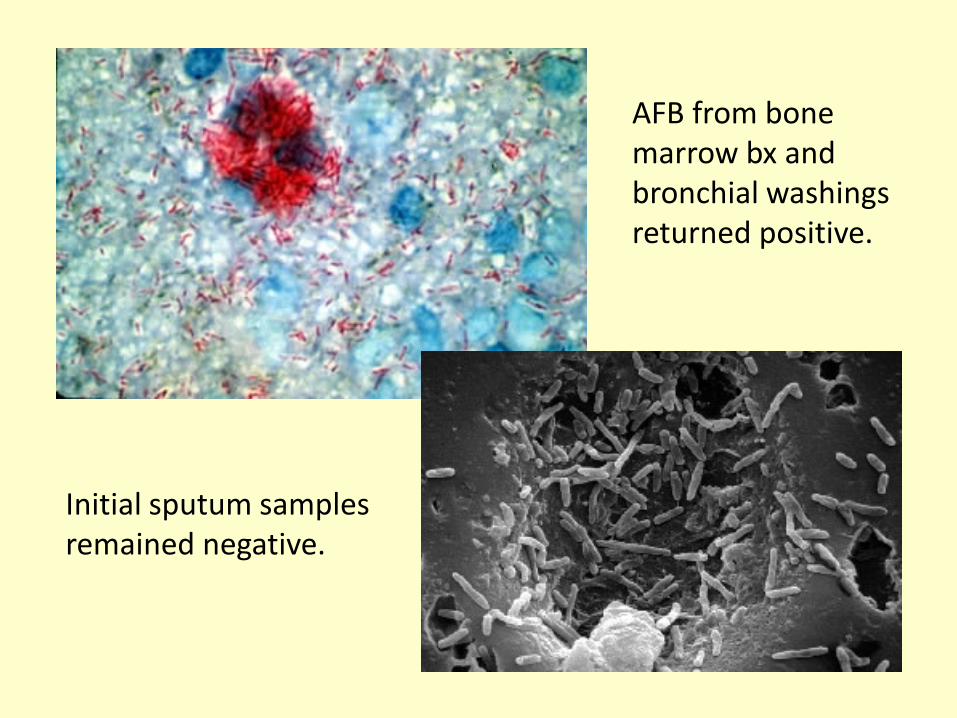
AFB from bone marrow bx and bronchial washings returned positive.
Initial sputum samples remained negative.
Q: What do a cow and a knee have in common? A: A needle.

Who would have thought?!

M. bovis
• Carried by cattle and other mammals • 1-2% of TB cases in US, 10-15% in developing
countries • Risk factors: young age, residing in endemic
areas, Hispanics, immunosuppressed • Typically spread by aerosolized particles or
non-pasteurized dairy products • Has been found in blood samples of cattle
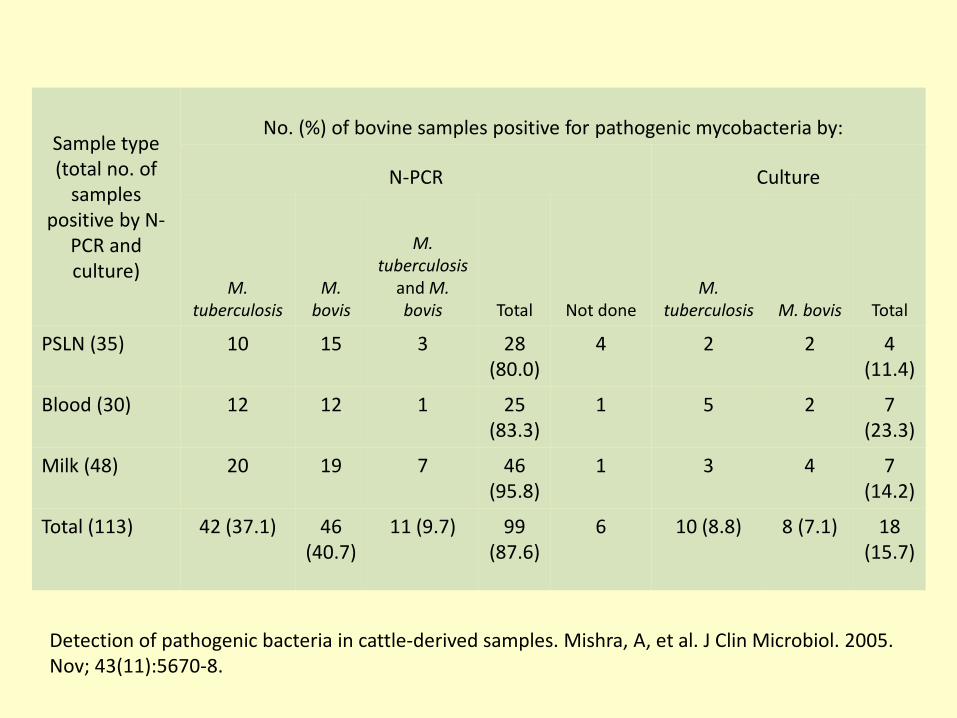
Sample type (total no. of
samples positive by N-
PCR and culture)
No. (%) of bovine samples positive for pathogenic mycobacteria by:
N-PCR Culture
M. tuberculosis
M. bovis
M. tuberculosis
and M. bovis Total Not done
M. tuberculosis M. bovis Total
PSLN (35) 10 15 3 28 (80.0)
4 2 2 4 (11.4)
Blood (30) 12 12 1 25 (83.3)
1 5 2 7 (23.3)
Milk (48) 20 19 7 46 (95.8)
1 3 4 7 (14.2)
Total (113) 42 (37.1) 46 (40.7)
11 (9.7) 99 (87.6)
6 10 (8.8) 8 (7.1) 18 (15.7)
Detection of pathogenic bacteria in cattle-derived samples. Mishra, A, et al. J Clin Microbiol. 2005. Nov; 43(11):5670-8.

M. bovis vs. M. tuberculosis
• Clinically and radiographically indistinguishable
• Extrapulmonary manifestations are more common with M. bovis
• Distinguished by DNA PCR • Differ in treatment regimen
– Both require 4 drug regimen – Levofloxacin instead of pyrazinamide

PCR products of various Mycobacteria DNA. Lanes 2 and 3 are M. tuberculosis; lane 5 is M. bovis. Bayraktar B, et al. J. Clin. Microbiol. 2011;49:3837-3841
The Course Continued
• Reintubated x1 • Tension pneumothorax requiring needle
thoracostomy and chest tube • Anteroapical MI with development of apical
thrombus • Developed atrial fibrillation with RVR • DVT at PICC site • At one point, made DNR and extubated
And Continued…
• PEG tube placed • L psoas fluid collection drained for possible
abscess • Discharged to SNF after 92 days • Rehospitalized x2 later that year
– 13 days for FTT, GIB – 8 days for sepsis with enterococcus bacteremia

And Continued…
• PEG tube placed • L psoas fluid collection drained for possible
abscess • Discharged to SNF after 92 days • Rehospitalized x2 later that year
– 13 days for FTT, GIB – 8 days for sepsis with enterococcus bacteremia
• But was back in Mexico the following spring!
Thank you.

















