32
Anal Cancer Rob Glynne-Jones Mount Vernon Cancer Centre
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | elwin-scott |
| View: | 219 times |
| Download: | 0 times |

Anal Cancer
Rob Glynne-Jones Mount Vernon Cancer Centre on behalf of NCRI anal cancer subgroup

Aim to discuss
• The EORTC trials in anal cancer
• US and UK trials
• What we have learnt so far
• Where do we go from here?

Randomised trials • UKCCR ACT 1 CRT vs RT• EORTC 22861 CRT vs RT
• RTOG 8704/ECOG Role of MMC
• RTOG 98-11 Role of NACT/cisplat • ACCORD-03 Role of NACT cisplat/ RT dose • CRUK ACT 2 Role of cisplat vs MMC + maintenance 5FU/cisplat• EORTC Role of 5FU vs CDDP/MMC 22011-40014 not extended to phase III
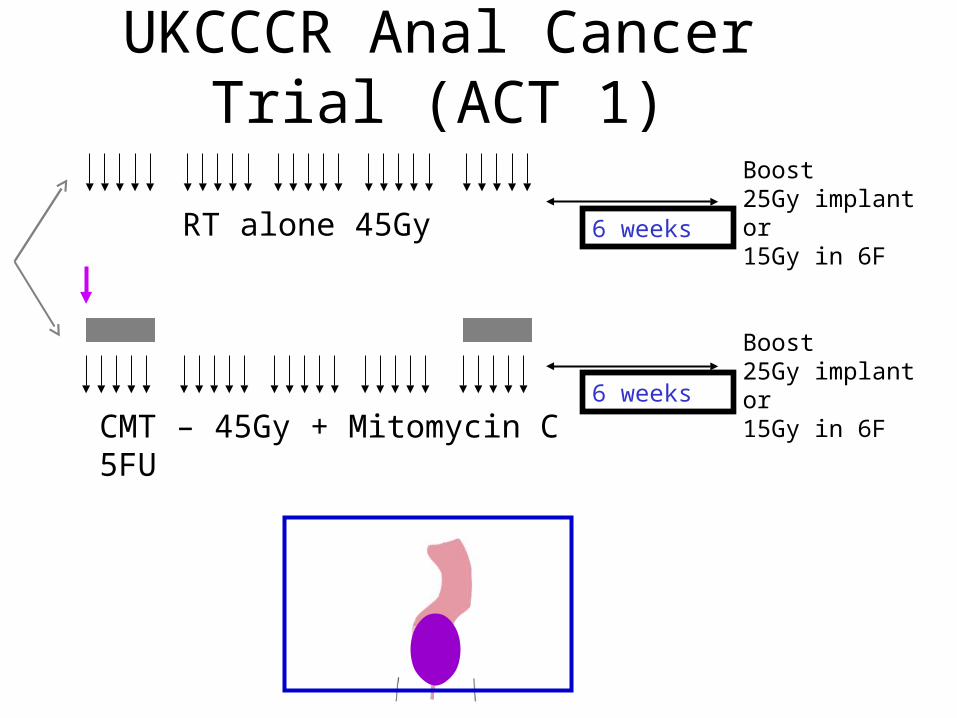
UKCCCR Anal Cancer Trial (ACT 1)
CMT – 45Gy + Mitomycin C 5FU
RT alone 45Gy
Boost25Gy implant or15Gy in 6F
Boost25Gy implant or15Gy in 6F
6 weeks
6 weeks

ACT I :Time to first local relapse
75
50
25
0
Per
cent
age
of p
atie
nts
havi
ng a
loca
l rel
apse
(%
)
0 2 4 6 8 10 12 14 16 18 20Time since randomisation (years)
RT aloneCMTHR 0.46, p<0.001

Colostomy-free survival


Effect of CD34 - RFS
Follow-up (years)
543210
Pro
gre
ssio
n-f
ree
ra
te (
%)
100
80
60
40
20
0
Follow-up (years)
543210P
rog
ress
ion
-fre
e r
ate
(%
)
100
80
60
40
20
0
RT armP=0.002
CRT armP=0.86
Mawdsley et al. (2004 GI ASCO)
1
234

ACT II Factorial DesignChemoradiation Comparison
MMC 5FU CRT No
maintenance
CisP 5FU CRT No
maintenance MMC 5FU CRT
+Maintenance
CisP 5FU CRT
+Maintenance
MMCN=472
CisPN=468
versus
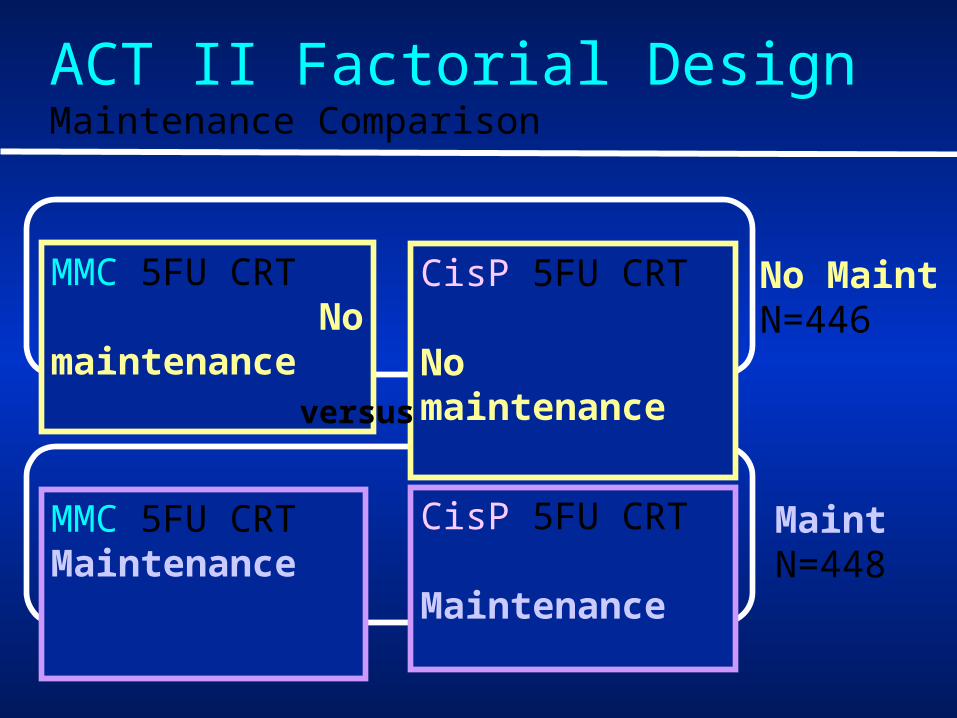
MMC 5FU CRT No maintenance
CisP 5FU CRT No maintenance
MMC 5FU CRT Maintenance
CisP 5FU CRT Maintenance
No MaintN=446
Maint N=448
versus
ACT II Factorial DesignMaintenance Comparison

Chemoradiation Regimens
1 2 3 4 5RT week
5FU
MMC
1 2 3 4 5RT week
5FU
CisP
1000mg/m2 d1-4 & 29-3224 hour continuous iv infusion
12mg/m2 d1 onlyiv bolus, max single dose 20 mg
60mg/m2 d1 & 29 iv infusion
1000mg/m2 d1-4 & 29-3224 hour continuous iv infusion
6
6

ACT II EndpointsChemoradiation (CRT) comparison
Primary Endpoints • Complete response rate at 6
months• Acute Toxicity (CTC Grade 3 & 4)
Maintenance comparison Primary Endpoint• Recurrence Free Survival
Both comparisons Secondary Endpoints• Colostomy Rate• Cause-specific & Overall survival
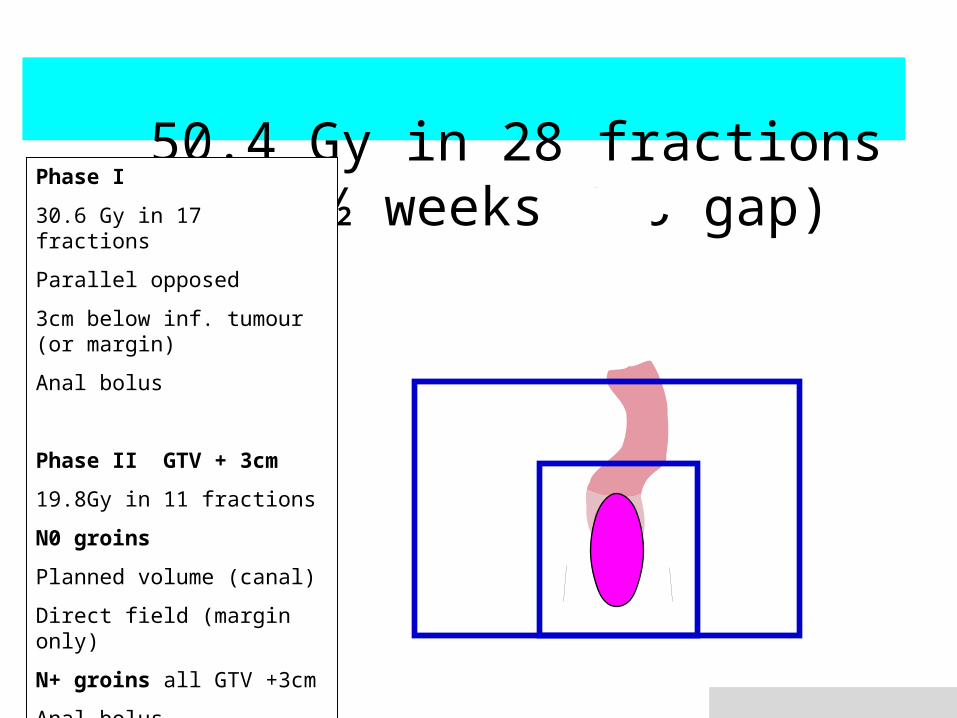
50.4 Gy in 28 fractions over 5 ½ weeks
(no gap)Phase I
30.6 Gy in 17 fractions
Parallel opposed
3cm below inf. tumour (or margin)
Anal bolus
Phase II GTV + 3cm
19.8Gy in 11 fractions
N0 groins
Planned volume (canal)
Direct field (margin only)
N+ groins all GTV +3cm
Anal bolus

Mean Doses Received• PTV primary 51.37Gy ± 0.84 (95% CI) • PTV inguinal nodes 51.41Gy ± 1.54
• Uninvolved inguinal 36.53Gy ± 3.38 • Uninvolved external iliac 34.28Gy + 5.63
• Femoral heads 47.32Gy ± 3.45
Aggarwal A, et al., Radiother Oncol. 2012 Jun;103(3):341-6

Tumour Stage
MMC(472)
CisP(468)
T stageT1 T2 49% (232) 54% (254)T3 T4 48% (225) 44% (205)TX 15 13
N StageNode negative 63% (297) 62% (290)Node positive 32% (150) 33% (155)NX 25 23
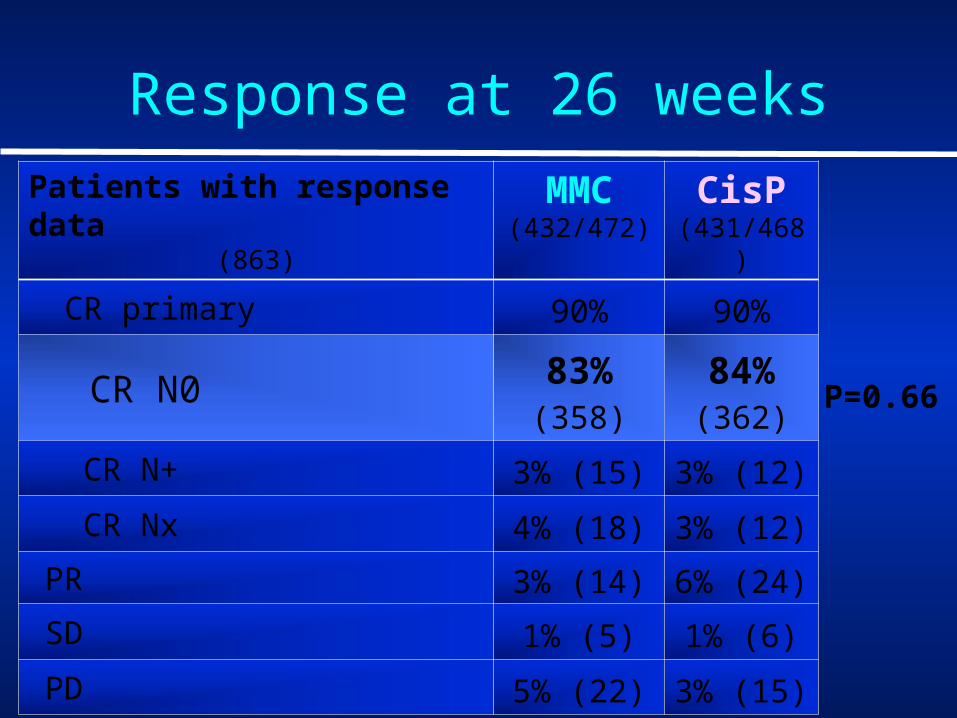
Response at 26 weeksPatients with response data
(863)
MMC(432/472)
CisP(431/468)
CR primary 90% 90%
CR N0 83% (358)
84% (362)
CR N+ 3% (15) 3% (12)
CR Nx 4% (18) 3% (12)
PR 3% (14) 6% (24)
SD 1% (5) 1% (6)
PD 5% (22) 3% (15)
P=0.66

ACT II Compliance & Toxicity
• Radiotherapy – 92% MMC vs 90% CisP - total dose 50.4Gy– ~3% >7 days interruptions
• Chemotherapy - weeks 1 & 5 – 75% MMC vs 72% CisP full dose weeks 1 & 5
• Acute toxicity – 58% MMC vs 60% CisP Grade 3 – 13% MMC vs 12% CisP Grade 4 – 71% MMC vs 72% CisP combined Grade 3/4

CR at 26 weeks
Difference (95% CI)
P value
MMC CisP83%
(358/432)84%
(362/431)+1% (-3.8 to 6.1) p =0.66
No Maint
Maint
82%(337/409)
85% (348/410)
+3% (-2.6 to 7.5)p = 0.34
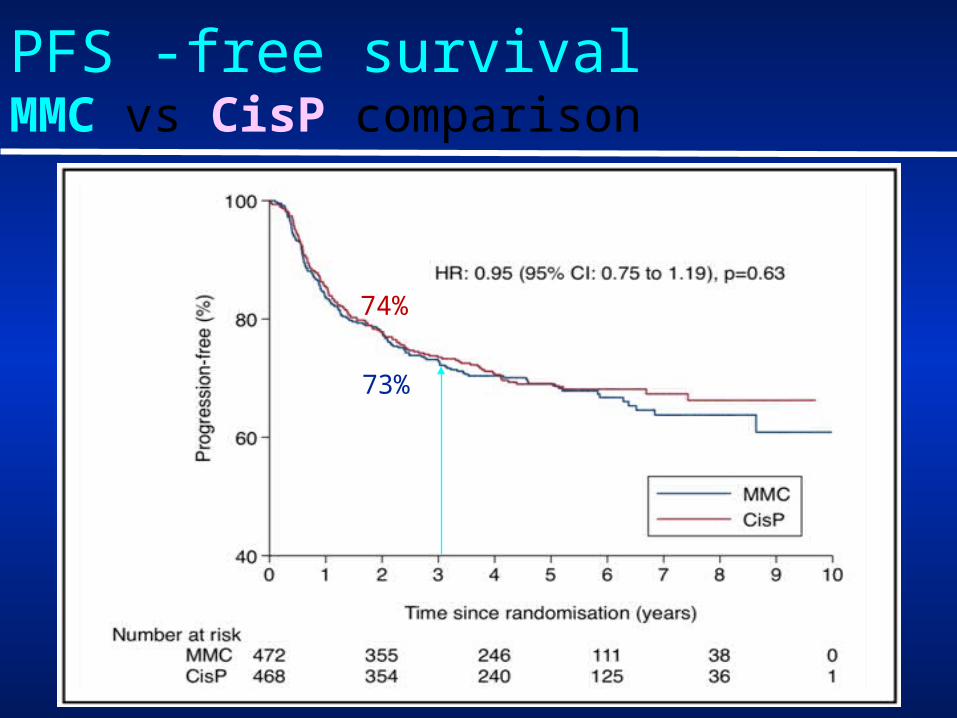
PFS -free survivalMMC vs CisP comparison
73%
74%

Overall Survival CR vs Not CR week 26
93%
61%

ACT II – Conclusions
• Excellent CR rate at 6 months - 83% v 84% - no difference MMC/Cisp
• No difference in colostomy rate• No difference in PFS• 60% of pts not in CR at 11 weeks
achieved CR at 26 weeks.• We recommend assessment at 26
weeks in future trials
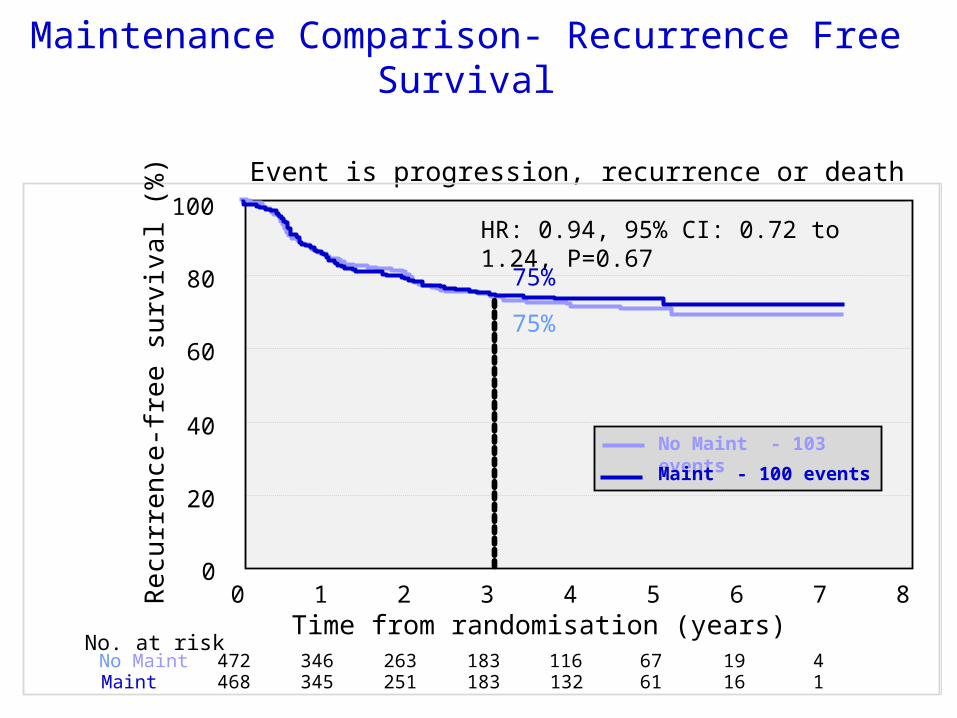
Maintenance Comparison- Recurrence Free Survival
Event is progression, recurrence or death
0
20
40
60
80
100
Re
curr
en
ce-f
ree
surv
iva
l (%
)
Maint 468 345 251 183 132 61 16 1472 346 263 183 116 67 19 4No Maint
No. at risk
0 1 2 3 4 5 6 7 8Time from randomisation (years)
No Maint - 103 events
Maint - 100 events
HR: 0.94, 95% CI: 0.72 to 1.24, P=0.67
75%
75%

0
20
40
60
80
100
Ove
rall
surv
ival
(%
)
448 361 278 203 138 71 22 3Maint446 369 278 198 125 67 19 4No Maint
No. at risk
0 1 2 3 4 5 6 7 8Time from randomisation (years)
HR: 0.81, 95% CI: 0.57 to 1.13, P=0.21
84%
85%
No Maint - 74 events
Maint - 60 events
Maintenance Comparison - Overall Survival
HR: 0.81, 95% CI: 0.57 to 1.13, P=0.21

ACT II – Conclusions 2Maintenance comparison• Preliminary data shown 2009• Median follow-up now 5 years• No evidence of any difference in
PFS, cause specific survival or overall survival
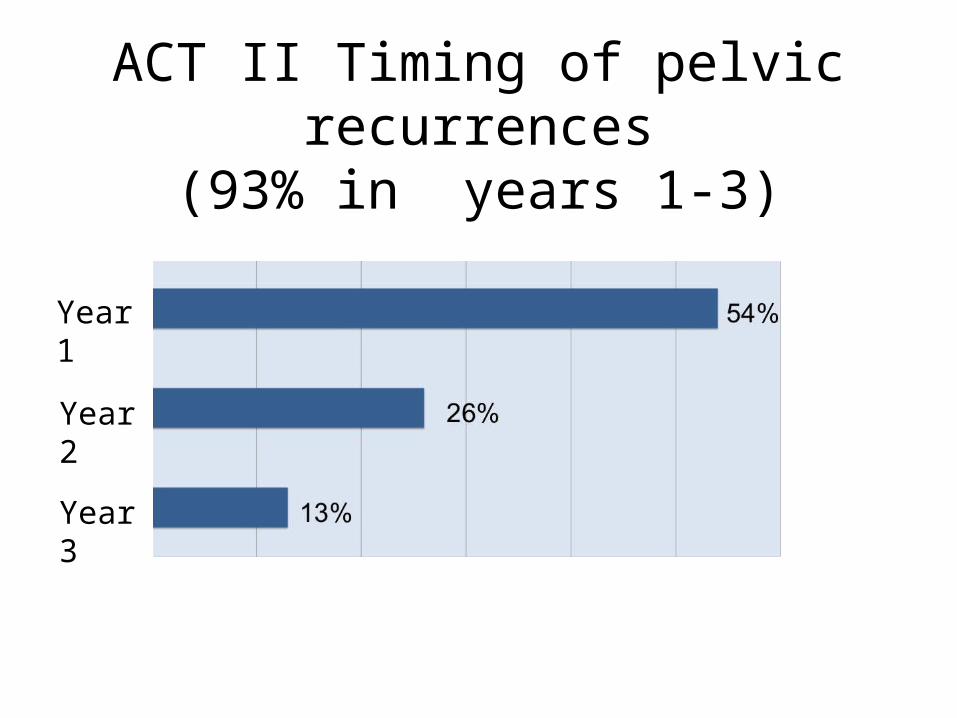
ACT II Timing of pelvic recurrences(93% in years 1-3)
Year 1
Year 2
Year 3

Site of relapse
Number % total relapses
PELVIC NO METS 133 64%
PELVIC WITH METS 30 14%
DISTANT METS ONLY 46 22%
TOTAL CRUDE PF (WITH OR WITHOUT METS)
163 78%
TOTAL RELAPSES 209
The pattern was similar for PF only and PF + mets (data not shown)

ACCORD- 03
• Locally advanced >4cm or N1 anal canal
• Therapeutic intensification – Induction chemotherapy– High dose radiotherapy
• Primary endpoint: colostomy-free-survival(CFS).
• Secondary endpoint : QoL, local control (LC), overall survival (OS), and cancer-specific survival.

ACCORD 03
low boost15 Gy
45 GyCDDP 5 FU 2 cycles
CTCDDP 5FU 2 cycles
high boost20-25 Gy
45 GyCDDP 5 FU 2 cycles
CTCDDP 5FU 2 cycles
low boost15 Gy
45 GyCDDP 5 FU 2 cycles
No CT
high boost20-25 Gy
45 GyCDDP 5 FU 2 cycles
No CT
R
70% 82% 77% 73%
5 years CFS

RTOG 9811 Time to Colostomy
Cisplat
MMC
RTOG 9811 Ajani JA et al JAMA 2008

MMC
Cisplatin
RTOG 9811 Ajani JA et al JAMA 2008
RTOG 9811 Disease Free Survival
Thoughts• No longer feasible to think that one size fits
all in anal cancer
• We improved
overall 3 year DFS from 54% (ACT I)
to 74% (ACT II)
• We took 7 years to do ACT II
• We probably need international collaboration for next studies
Radiotherapy strategies which need exploring• (1) Optimization of radiotherapy (optimal
dose/fractionation/concomitant boost/brachytherapy)
• (2) Optimal field sizes
• (3) Evaluation of new radiosensitization protocols (oxaliplatin, irinotecan, taxanes).
• (4) Optimization of radiotherapy techniques (IMRT/VMAT/Brachytherapy)

















