morphological feature related to AF is the presence of inflammatory cells in the atrial myocar-
dium [11]. Despite observed association between elevated plasma levels of inflammatory mark-
ers and AF, it is still not determined whether inflammation is a systemic or local phenomenon
reflecting an active inflammatory process in the heart [18]. A role of inflammation and myo-
cardial inflammatory infiltrate was suggested by morphological studies and by clinical studies
that monitored serum levels of inflammatory cytokines in patients with AF [18, 19]. Histologi-
cal findings supporting the association between inflammation and AF have been reported in
several animal [20, 21] as well as human studies [11, 22–24]. Other reports have shown a corre-
lation between the level of fibrosis and infiltration of atrial myocardium by inflammatory cells
[25]. However, the above studies focused on inflammatory cells in general and were usually
limited to one atrium only or to single pathological condition related to AF. It is not known
whether the inflammatory cells are a marker of local reaction to tissue injury caused by factors
leading to AF or whether they actively participate in the maintenance of AF due to direct cyto-
toxic or pro-fibrotic effects [26] or indirectly due to released cytokines that may promote
arrhythmogenesis [21]. The aims of this study were the following: 1) to characterize and quan-
tify immune cell populations in human atrial myocardium of patients undergoing open heart
surgery with AF and in sinus rhythm (SR); 2) to identify regional differences in terms of
immune cell populations in atrial myocardium of patients undergoing open heart surgery; 3)
to correlate atrial immune cell populations with markers of systemic inflammation or AF risk
factors.
Materials and methods
Patients
We used bioptic material from 46 patients (19 with long-term persistent AF and 27 in SR),
which were hospitalized in Institute for Clinical and Experimental Medicine in Prague. We
included patients who underwent coronary artery bypass surgery or valve surgery and who
agreed to participate in the study (S1 Table). Patients who presented with sepsis, active endo-
carditis, permanent cardiostimulation, dominating atrial flutter or postincisional supraventric-
ular tachycardia on ECG were excluded. The study conformed to the principles presented in
the Declaration of Helsinki. Ethics committee of the Institute for Clinical and Experimental
Medicine in Prague approved the study protocol. Only those patients who signed a written
informed consent were included into the study.
Tissue sampling, histological and immunohistochemical analysis
Tissue samples were obtained during open-heart surgery and processed as described previ-
ously [27]. Immunohistochemistry was used to visualize CD45, CD3, CD68-KP1, DC-SIGN
(DC-specific ICAM-3 grabbing nonintegrin), mast cell tryptase and CD20 in these samples
(S2 Table).
Histomorphometry
To quantify CD45+cells, CD3+cells, CD68-KP1+cells and mast cells we used the program
Image J 1.44p (National Institutes of Health, USA). Image sampling was performed as de-
scribed in [27]. Only immunoreactive cells within the myocardium were counted manually
and labeled in the image analysis program to make sure that no cell is counted twice. The fre-
quency of cells was expressed as the number of cells per square millimeter. Those, who per-
formed image analysis were blinded to patient characteristics.
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 3 / 13
Statistical analysis
The values of morphometric analyses are expressed as a mean±SD. The range of values is also
provided. Statistical testing of the morphometric analysis comparing values from AF and SR
groups in various anatomical locations was performed using a non-parametric test—Mann–
Whitney U test. Statistical significance of differences between the patient groups in various
patient characteristics was tested using Student’s t-test, Fisher’s exact test, or chi-square test
where appropriate. Statistical programs used for these analyses were Microsoft Office Excel,
InStat and Statistica. A value of P< 0.05 was considered significant.
Results
Patient characteristics
S1 Table shows characteristics of the patient population in detail. The group of patients suffer-
ing from AF was 7 years older on average. Patients from AF group had higher left and right
atrial volumes. Left atrial volume was on average almost doubled in subjects with AF. On the
other hand, patients in SR had more often coronary artery disease. There was no difference in
NYHA class, diabetes, arterial hypertension, anemia and renal insufficiency between both
patient groups. E/E ‘ratio, non-invasive estimate of left atrial pressure and markers of systemic
inflammation (CRP, leukocyte count) were similar between patients with AF and SR.
Detection and quantification of CD45+ cells in the atrial myocardium
To visualize cells with a potential of an inflammatory process we used an antibody against a
pan-leukocyte marker CD45. This marker is common for cells of hematopoietic origin. Immu-
noperoxidase reaction revealed CD45+ cells in all samples analyzed from SR and AF group.
The immunoreactive cells were found in the whole thickness of the atrial wall regardless of
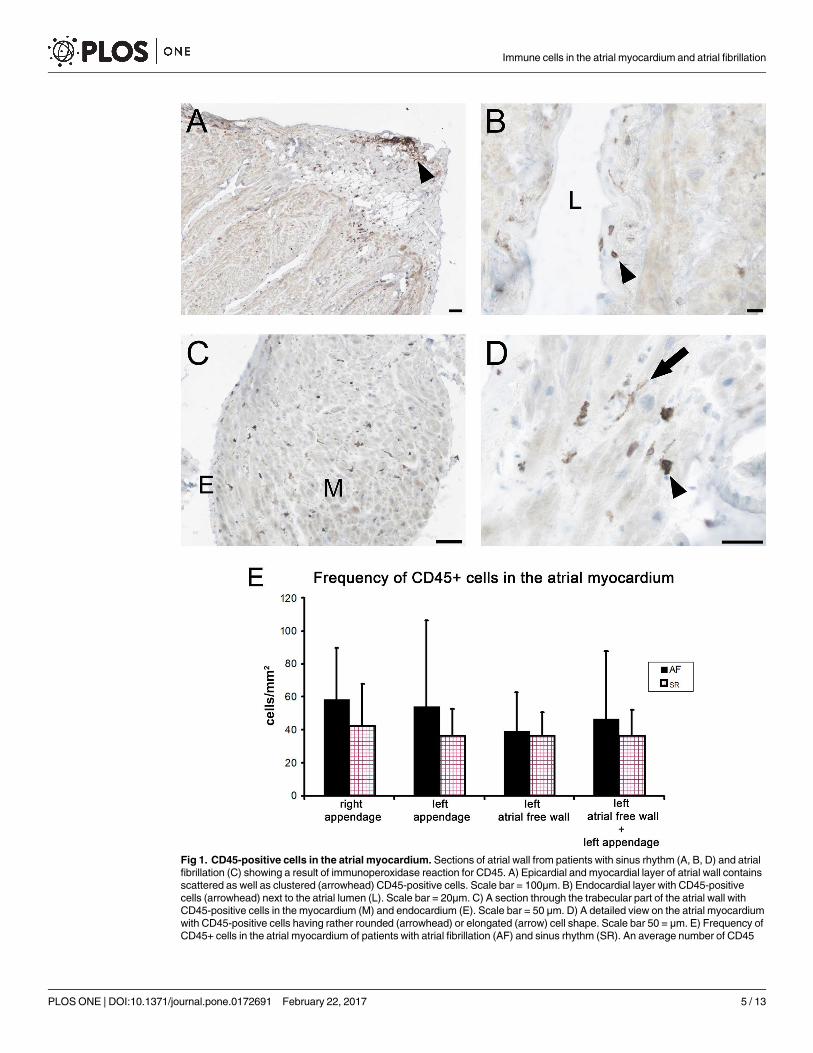
the anatomical location (Fig 1A–1D). In the epicardium, CD45+ cells often formed larger
clusters (Fig 1A). In the endocardium, these cells were scattered in the whole thickness of this
layer (Fig 1B), occasionally they also adhered to the endothelium from the luminal side (not
shown). The cells immunoreactive for CD45+ were found in the interstitial compartment of
the myocardium both in perimysium and in endomysium. Morphologically, the CD45+ cell
population appeared heterogeneous with cells having in general either rounded or elongated
cell bodies (Fig 1D). The CD45+ cells located in the myocardium were quantified in tissue sec-
tions of left and right atrial appendages and left atrial free wall. When samples from SR group
and AF group were compared there was a tendency for a higher frequency of CD45+ cells in
AF group, however, without reaching a statistical significance (Fig 1E). In the right atrial ap-
pendage, the average number of CD45+ cells per 1mm2 was 42.4±25.5 (range 12.2–103.8) in
the SR group and 58.4±31.3 (range 12.6–118.5) in the AF group. In the left atrial appendage,
the average number of CD45+ cells per 1mm2 was 36.1±16.7 (range 14.4–61.7) in the SR group
and 54.2±52.2 (range 17.8–186.2) in the AF group. In the left atrial free wall, the average num-
ber of CD45+ cells per 1mm2 was 36.2±14.2 (range 20.6–59.3) in the SR group and 39.0±23.7
(range 11.9–95.5) in the AF group. In the pooled samples from the whole left atrium, the aver-
age number of CD45+ cells per 1mm2 was 36.1±15.9 (range 14.3–61.7) in the SR group and
46.6±41.2 (range 11.9–186.2) in the AF group.
CD3-positive T-lymphocytes in the atrial myocardium
With the aim to characterize the inflammatory cell population further, we performed analysis
of different subpopulations of CD45+ cells. Thus, as a next step, T-lymphocytes were immu-
nohistochemically detected in atrial samples using an antibody against a marker CD3. Like
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 4 / 13
Fig 1. CD45-positive cells in the atrial myocardium. Sections of atrial wall from patients with sinus rhythm (A, B, D) and atrial
fibrillation (C) showing a result of immunoperoxidase reaction for CD45. A) Epicardial and myocardial layer of atrial wall contains
scattered as well as clustered (arrowhead) CD45-positive cells. Scale bar = 100μm. B) Endocardial layer with CD45-positive
cells (arrowhead) next to the atrial lumen (L). Scale bar = 20μm. C) A section through the trabecular part of the atrial wall with
CD45-positive cells in the myocardium (M) and endocardium (E). Scale bar = 50 μm. D) A detailed view on the atrial myocardium
with CD45-positive cells having rather rounded (arrowhead) or elongated (arrow) cell shape. Scale bar 50 = μm. E) Frequency of
CD45+ cells in the atrial myocardium of patients with atrial fibrillation (AF) and sinus rhythm (SR). An average number of CD45
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 5 / 13
CD45+ cells, T-lymphocytes were found in all samples from both SR and AF groups and were
localized in the whole atrial wall including myocardium (Fig 2), but were much less abundant
than CD45+ cells. The rounded morphology of CD3+ cells, which were found scattered in
endomysial and perimysial interstitial spaces corresponded to that of lymphocytes (Fig 2A).
The quantification of CD3+ T-lymphocytes revealed their significantly higher frequency in left
atrium of patients with AF. When samples of left atrial appendage and left atrial free wall were
pooled the difference between AF and SR group was statistically significant (Fig 2C). In the
right atrial appendage, the average number of CD3+ cells per 1mm2 was 6.5±6.0 (range 1.08–
26.8) in the SR group and 5.3±4.2 (range 1.2–15.3) in the AF group. In the left atrial append-
age, the average number of CD3+ cells per 1mm2 was 3.5±2.3 (range 1.1–8.4) in the SR group
and 8.6±10.1 (range 1.7–36.2) in the AF group. In the pooled samples from the whole left
atrium, the average number of CD3+ cells per 1mm2 was 3.5±2.2 (range 1.1–8.4) in the SR
group and 9.8±10.0 (range 1.7–36.2) in the AF group.
CD68-KP1-positive cells in the atrial myocardium
Inflammatory cells including monocyte/macrophages and dendritic cells can be detected
using a marker CD68-KP1. Cells immunoreactive for CD68-KP1 were very frequent in all
atrial tissue samples from both AF and SR group. They were regularly detected in the myocar-
dium and had predominantly an elongated cell shape (Fig 2B). The quantitative analysis
revealed that CD68-KP1+ cell population was the most abundant inflammatory cell popula-
tion and they were more frequent in samples from patients with AF (Fig 2D). There was signif-
icantly higher number of CD68-KP1+ cells in the left appendage and in pooled samples of left
appendage and left atrial wall in patients with AF compared to patients with SR (Fig 2D). In
the right atrial appendage, the average number of CD68-KP1+ cells per 1mm2 was 44.3±19.3
(range 7.7–76.7) in the SR group and 52.0±27.0 (range 14.0–109.0) in the AF group. In the left
atrial appendage, the average number of CD68-KP1+ cells per 1mm2 was 40.8±24.4 (range
9.9–96.3) in the SR group and 67.2±25.0 (r[7]ange 41.6–122.4) in the AF group. In the pooled
samples from the whole left atrium, the average number of CD68-KP1+ cells per 1mm2 was
38.5±23.7 (range 9.9–96.3) in the SR group and 60.2±28.4 (range 18.0–122.4) in the AF group.
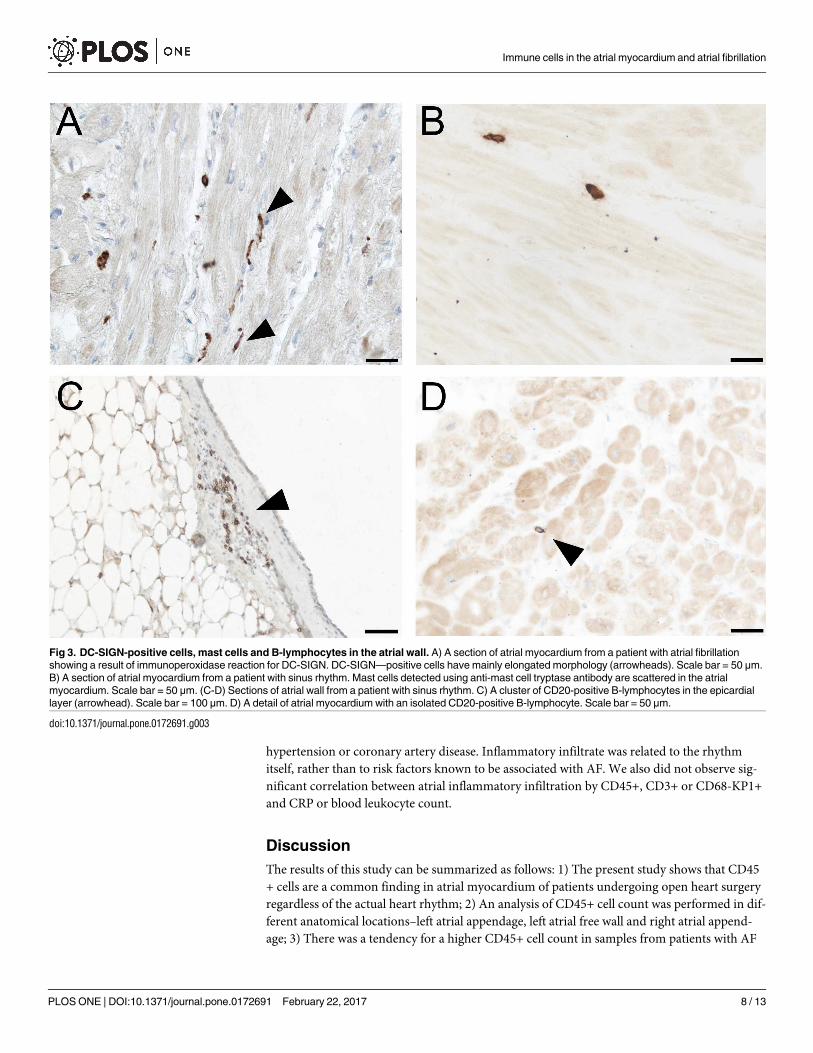
DC-SIGN-positive dendritic cells, mast cells and B-lymphocytes in the
atrial myocardium
Dendritic cells are among cells immunoreactive for CD68-KP1+. To confirm their presence in
the atrial myocardium of patients undergoing open heart surgery we performed an immuno-
histochemical detection of marker DC-SIGN, which labels immature dendritic cells. DC-
SIGN+ cells were found frequently in atrial myocardial samples from both AF and SR groups.
They had the same morphology as the cells previously immunoreactive for CD68-KP1 antigen
(Fig 3A). Mast cells were detected using an antibody against mast cell tryptase.
Mast cells were quite rare in the atrial myocardium and they were found scattered as indi-
vidual cells in the endomysial compartment or in small groups in the perimysial spaces sur-
rounding bigger vessels (Fig 3B). There was a similar frequency of mast cells in the atrial
myocardium of patients in AF and SR group (not shown). B-lymphocytes were detected using
an antibody against CD20 marker in the atrial myocardium of patients in AF and SR group.
+ cells per square mm of cross-sectioned atrial myocardium is given +- SD. Right appendage–SR (n = 22), AF (n = 15); Left
appendage—SR (n = 8), AF (n = 8); Left atrial free wall—SR (n = 4), AF (n = 8); Left atrial free wall + left appendage—SR
(n = 12), AF (n = 16).
doi:10.1371/journal.pone.0172691.g001
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 6 / 13
CD20+ cells were occasionally found as small clusters in the epicardial layer (Fig 3C). In the
myocardium, these cells were very rare (Fig 3D).
Determinants of inflammatory cell populations other than cardiac rhythm
In the pooled cohort, variations of immune cell population were related to prevailing rhythm
(particularly for CD3 and CD68-KP1 markers). However, they did not significantly correlate
with mitral regurgitation grade, left atrial volume, E/E´ ratio, age, presence of diabetes,
Fig 2. CD3-positive T-lymphocytes and CD68-KP1-positive cells in the atrial myocardium. Sections of atrial myocardium from patients with atrial
fibrillation showing a result of immunoperoxidase reaction for CD3 and CD68-KP1. A) CD3-positive T-lymphocytes localized among atrial cardiomyocytes and
in the interstitial spaces (arrowheads). Scale bar = 50 μm. B) CD68-KP1-positive cells are found in the interstitium and have mainly elongated morphology
(arrowheads). Scale bar = 50 μm. C) Frequency of CD3-positive T-lymphocytes in the atrial myocardium of patients with atrial fibrillation (AF) and sinus rhythm
(SR). An average number of CD3-positive T-lymphocytes cells per square mm of cross-sectioned atrial myocardium is given +- SD. Right appendage–SR
(n = 17), AF (n = 11); Left appendage—SR (n = 8), AF (n = 10); Left atrial free wall + left appendage—SR (n = 9), AF (n = 16). *—p<0,05 D) Frequency of
CD68-KP1-positive cells in the atrial myocardium of patients with atrial fibrillation (AF) and sinus rhythm (SR). An average number of CD68-KP1-positive cells
per square mm of cross-sectioned atrial myocardium is given +- SD. Right appendage–SR (n = 22), AF (n = 9); Left appendage—SR (n = 11), AF (n = 9); Left
atrial free wall + left appendage—SR (n = 13), AF (n = 19). *—p<0,05
doi:10.1371/journal.pone.0172691.g002
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 7 / 13
hypertension or coronary artery disease. Inflammatory infiltrate was related to the rhythm
itself, rather than to risk factors known to be associated with AF. We also did not observe sig-
nificant correlation between atrial inflammatory infiltration by CD45+, CD3+ or CD68-KP1+
and CRP or blood leukocyte count.
Discussion
The results of this study can be summarized as follows: 1) The present study shows that CD45
+ cells are a common finding in atrial myocardium of patients undergoing open heart surgery
regardless of the actual heart rhythm; 2) An analysis of CD45+ cell count was performed in dif-
ferent anatomical locations–left atrial appendage, left atrial free wall and right atrial append-
age; 3) There was a tendency for a higher CD45+ cell count in samples from patients with AF
Fig 3. DC-SIGN-positive cells, mast cells and B-lymphocytes in the atrial wall. A) A section of atrial myocardium from a patient with atrial fibrillation
showing a result of immunoperoxidase reaction for DC-SIGN. DC-SIGN—positive cells have mainly elongated morphology (arrowheads). Scale bar = 50 μm.
B) A section of atrial myocardium from a patient with sinus rhythm. Mast cells detected using anti-mast cell tryptase antibody are scattered in the atrial
myocardium. Scale bar = 50 μm. (C-D) Sections of atrial wall from a patient with sinus rhythm. C) A cluster of CD20-positive B-lymphocytes in the epicardial
layer (arrowhead). Scale bar = 100 μm. D) A detail of atrial myocardium with an isolated CD20-positive B-lymphocyte. Scale bar = 50 μm.
doi:10.1371/journal.pone.0172691.g003
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 8 / 13
and this difference was even more prominent when focusing on some specific subpopulations
of inflammatory cells in the atrial myocardium; 4) Both in case of CD3+ T-lymphocytes and
CD68-KP1+ cells there was a higher cell count in the samples from patients with AF, but only
in the left atrium.
Several studies have been published previously describing an elevated count of inflamma-
tory cells in the atria of patients suffering from AF [11, 15, 22–25, 28, 29]. In contrast to our
study, some papers evaluated samples only from either left or right atrium [22, 24, 28, 29] or
the analysis was performed on necroptic specimens [25]. The results of our study are in general
agreement with findings of the above studies performed on different patient populations.
Importantly, it shows that there is significantly larger immune cell count only in the left atrium
of patients suffering from AF. The reason for the differential response of atria in terms of
inflammatory cell infiltration might be explained by a differences in density of capillaries serv-
ing as an entrance port for immune cells to invade atrial interstitium. In our recent study per-
formed on the same patient groups, we reported a higher microvascular density in the left
atrium compared to the right atrium [27]. It was shown repeatedly that the most pronounced
morphological changes attributable to AF could be detected in the left posterior atrial wall
[17]. Since, in the present study, most samples of the left atrium originated from the left ap-
pendage and a smaller number from left atrial free wall, we could not evaluate them separately,
however the statistical significance of differences between CD3+ and CD68-KP1+ always
increased when the samples from both locations were pooled together.
In addition to above mentioned immune cell populations, we also evaluated the amount of
mast cells and B-lymphocytes. One experimental study suggested the crucial role of mast cells
for development of AF [21]. However, in our study we found only a small number of mast cells
in the atrial myocardium and there was no difference between AF and SR groups of patients.
Our data show rather moderate increase of immune cells in left atrial myocardium of
patients with AF compared to SR group of patients undergoing open heart surgery. In case of
CD3+ T-lymphocytes, we found diffuse infiltration mostly by isolated cells. Interestingly, in
contrast to an initial report [11], no inflammatory infiltrates were found in more recent study
analyzing atrial myocardium from patients with lone atrial fibrillation [7]. In the present
study, we were not able to detect active (acute) myocarditis according to current criteria [30,
31]. It seems likely that an elevated number of CD3+ and CD68-KP1+ cells in the left atrial
myocardium of patients with AF reflects certain level of inflammatory activation of myocardial
tissue due to the mechanical stress accompanying the atrial dilation [32, 33]. Expression of
inflammatory cytokines is another parameter of local inflammatory state. One study reported
that there was an increased production of TNF-alpha and IL-6 in the right atria of AF patients
with valvular disease compared to control group of SR patients with valvular disease [34]. A
more recent study demonstrated a higher expression of an inflammatory cell adhesion mole-
cule VCAM1 in myocardial capillaries of left atrial appendages of patients with AF compared
with autoptic SR controls [29]. Interestingly, while the former study also reported a higher col-
lagen volume fraction in patients with AF [34], no difference between AF patients and controls
was observed in the latter [29]. Fibrosis is considered by many authors as a hallmark of struc-
tural remodeling in AF [13–16] and can also cause remodeling of infiltrating subepicardial
fatty infiltrates [35]. However, there are also reports, where no statistical difference in collagen
volume fraction or fibrosis was found between AR and SR group of patient most likely due to a
variable influence of accompanying structural heart diseases [27, 29, 32, 36, 37]. The largest
immune cell population was formed by CD68-KP1+ cells of monocyte/macrophage lineage
corresponding largely to dendritic cells, which were immunoreactive to DC-SIGN. The role
of these cells that are also found in the normal myocardium [38] is still a matter of ongoing
research and these cells can have both beneficial as well as detrimental effects on the heart,
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 9 / 13
based on various pathophysiological circumstances [39, 40]. In a recent study it was demon-
strated that atrial myocarditis coincides with certain types of ventricular myocarditis [41], but
since we have no reports of ventricular myocarditis in our patients we are unable to relate an
increased number of CD3+ and CD68-KP1+ cells in the left atria of AF group to an inflamma-
tory process in other parts of the myocardium. Our goal was to quantify inflammatory cells in
the atrial myocardia. Although we observed inflammatory cells regularly in the endocardium
and epicardium regardless of the heart rhythm we did not perform a quantitative study in
these layers of the heart wall and thus future studies may demonstrate whether there is a corre-
lation between the number of these cells across the heart. There are several limitations result-
ing from the fact that we relied on material from bioptic samples. In addition, the small size of
our patient groups might affect our quantitative results. It was possible to safely harvest only
small bioptic samples and these could be obtained from only certain regions within the atria.
Only patients suffering from various structural heart diseases were compared.
Conclusions
Immunohistochemical analysis of tissue samples from patients undergoing open heart surgery
showed moderate and site-specific increase of inflammatory cells in the atrial myocardium of
patients with AF compared to those in SR. The most represented immune cell population was
CD3+ T-lymphocytes and CD68-KP1+ monocyte/macrophage subpopulation corresponding
mostly to dendritic cells. Mast cells and B-lymphocytes were less frequent. Only CD3+ and
CD68-KP1+ cells were elevated in the left atrium of patients with AF, while no inflammatory
foci were detected in the atrial myocardium. This local elevation of some CD45+ cell popula-
tions might reflect the progression of AF. More research has to be done to elucidate signifi-
cance of general pro-inflammatory state reported in patients with AF.
Supporting information
S1 Table. Characteristics of patients with AF and patients in SR.
(DOCX)
S2 Table. Characterization of antibodies used in the study.
(DOC)
Acknowledgments
We thank Bc. Ivana Kamenařova for the help with sample collection, Ms. Marcela Blazkeova
and Ing.Lucie Kosova for their excellent technical assistance.
Author Contributions
Conceptualization: TK JK VM J Pirk.
Data curation: TK MB VM.
Formal analysis: TK MB VM.
Funding acquisition: TK VM JK J Pirk.
Investigation: TK NS VM MB MD J Přidal KR.
Methodology: JK VM TK.
Project administration: TK VM JK J Pirk.
Immune cells in the atrial myocardium and atrial fibrillation
PLOS ONE | DOI:10.1371/journal.pone.0172691 February 22, 2017 10 / 13