Anatomical Risk Factors for Intraoperative Cerebrospinal Fluid Leaks During Transsphenoidal Surgery for Pituitary Adenomas Alvaro Campero 1,2 , Juan F. Villalonga 2,3 , Armando Basso 4 - BACKGROUND: Cerebrospinal fluid (CSF) fistulas are among the most clinically important and frequent compli- cations of transsphenoidal surgery for pituitary adenomas. Between the adenoma and the CSF, a “barrier” exists that consists of £3 elements. These, from cephalad to caudad, are the arachnoid, dura mater (sellar diaphragm), and pituitary glandular tissue. The objective of the present study was to determine whether the presence or absence of any of these 3 anatomical elements would be associated with the devel- opment of an intraoperative CSF fistula. - METHODS: From November 2016 to June 2018, 40 patients with pituitary adenomas underwent surgery, by trans- sphenoidal endonasal access, under a microscope. All procedures were filmed in 3 dimensions. The intraoperative findings and preoperative magnetic resonance images were analyzed and compared. The patients who had developed a fistula were compared against those who had not. - RESULTS: In 20 patients, glandular tissue was identified between the tumor and subarachnoid space. In 13, dura mater was evident, and in 7, only the arachnoid was noted. An intraoperative CSF fistula occurred in 6 patients, all of whom had the arachnoid as the only barrier. The presence of a fistula was significantly more likely statistically for patients with an arachnoid-only barrier than for those with any other barrier composition (P < 0.001). - CONCLUSIONS: The anatomical architecture forming the roof of the pituitary fossa is an important determinant of intraoperative CSF fistula risk. When the barrier consists of only the arachnoid, the risk will be significantly greater than when the barrier contains additional elements. Pre- operative magnetic resonance imaging would be useful to determine the type of the existing barrier. INTRODUCTION C ephalous cerebrospinal fluid (CSF) fistulas are 1 of the most clinically important and frequent complications of transsphenoidal surgery for pituitary adenomas, 1 whether performed using microscopic techniques, 2 assisted endoscopy, 3 or endoscopy alone. 4,5 Several risk factors for CSF fistulas have been described. 2 In addition, several reports have proposed a range of surgical techniques designed to prevent this complication. 6-20 To date, however, no contemporary studies have reported on how the anatomical structure of the subarachnoid tumorespace interface might be a determinant of intraoperative CSF fistula risk. Between the adenoma and the CSF is a “barrier” composed of 3 anatomical structures. Progressing from cephalad to caudad, these 3 structures are the arachnoid, dura mater (i.e., sellar diaphragm), and pituitary glandular tissue. Of these 3 elements, the only one that is present in every person is the arachnoid. The aim of the present study was to determine, by retrospec- tively analyzing 3-dimensional (3D) surgical videos and operative findings, whether the presence or absence of any of these 3 anatomical components of the "barrier" would be associated with the presence of an intraoperative CSF fistula. METHODS From November 2016 to June 2018, 40 patients with pituitary ade- nomas underwent surgery for adenoma resection. In each case, the Key words - CSF leak - Pituitary adenoma - Pituitary fossa - Risk factors - Trans-sphenoidal approach Abbreviations and Acronyms 3D: 3-Dimensional BMI: Body mass index CSF: Cerebrospinal fluid MRI: Magnetic resonance imaging From the 1 LINT, Facultad de Medicina, Universidad Nacional de Tucumán, Tucumán; 2 Jefe del Servicio de Neurocirugía, Hospital Padilla, Tucumán; 3 Departamento de Neurocirugía, FLENI, Buenos Aires; and 4 Universidad Nacional de Buenos Aires, Hospital de Clinicas, Buenos Aires, Argentina To whom correspondence should be addressed: Juan F. Villalonga, M.D. [E-mail: [email protected]] Citation: World Neurosurg. (2019). https://doi.org/10.1016/j.wneu.2018.12.094 Journal homepage: www.journals.elsevier.com/world-neurosurgery Available online: www.sciencedirect.com 1878-8750/$ - see front matter ª 2018 Elsevier Inc. All rights reserved. WORLD NEUROSURGERY -: e1-e10, - 2019 www.journals.elsevier.com/world-neurosurgery e1 Original Article
Transcript
Original Article
Anatomical Risk Factors for Intraoperative Cerebrospinal Fluid Leaks During
Transsphenoidal Surgery for Pituitary Adenomas
Alvaro Campero1,2, Juan F. Villalonga2,3, Armando Basso4
-BACKGROUND: Cerebrospinal fluid (CSF) fistulas areamong the most clinically important and frequent compli-cations of transsphenoidal surgery for pituitary adenomas.Between the adenoma and the CSF, a “barrier” exists thatconsists of£3 elements. These, fromcephalad to caudad, arethe arachnoid, dura mater (sellar diaphragm), and pituitaryglandular tissue. The objective of the present study was todeterminewhether the presence or absence of any of these 3anatomical elements would be associated with the devel-opment of an intraoperative CSF fistula.
-METHODS: From November 2016 to June 2018, 40 patientswith pituitary adenomas underwent surgery, by trans-sphenoidal endonasal access, under a microscope. Allprocedures were filmed in 3 dimensions. The intraoperativefindings and preoperative magnetic resonance images wereanalyzed and compared. The patients who had developed afistula were compared against those who had not.
-RESULTS: In 20 patients, glandular tissue was identifiedbetween the tumor and subarachnoid space. In 13, duramater was evident, and in 7, only the arachnoid was noted.An intraoperative CSF fistula occurred in 6 patients, all ofwhom had the arachnoid as the only barrier. The presenceof a fistula was significantly more likely statistically forpatients with an arachnoid-only barrier than for those withany other barrier composition (P < 0.001).
-CONCLUSIONS: The anatomical architecture formingthe roof of the pituitary fossa is an important determinant ofintraoperative CSF fistula risk. When the barrier consists ofonly the arachnoid, the risk will be significantly greater
Abbreviations and Acronyms3D: 3-DimensionalBMI: Body mass indexCSF: Cerebrospinal fluidMRI: Magnetic resonance imaging
WORLD NEUROSURGERY-: e1-e10, - 2019
than when the barrier contains additional elements. Pre-operative magnetic resonance imaging would be useful todetermine the type of the existing barrier.
INTRODUCTION
ephalous cerebrospinal fluid (CSF) fistulas are 1 of themost clinically important and frequent complications of
Ctranssphenoidal surgery for pituitary adenomas,1 whether
performed using microscopic techniques,2 assisted endoscopy,3 orendoscopy alone.4,5 Several risk factors for CSF fistulas have beendescribed.2 In addition, several reports have proposed a range ofsurgical techniques designed to prevent this complication.6-20 Todate, however, no contemporary studies have reported on how theanatomical structure of the subarachnoid tumorespace interfacemight be a determinant of intraoperative CSF fistula risk.Between the adenoma and the CSF is a “barrier” composed of�3
anatomical structures. Progressing from cephalad to caudad, these3 structures are the arachnoid, dura mater (i.e., sellar diaphragm),and pituitary glandular tissue. Of these 3 elements, the only one thatis present in every person is the arachnoid.The aim of the present study was to determine, by retrospec-
tively analyzing 3-dimensional (3D) surgical videos and operativefindings, whether the presence or absence of any of these 3anatomical components of the "barrier" would be associated withthe presence of an intraoperative CSF fistula.
METHODS
From November 2016 to June 2018, 40 patients with pituitary ade-nomas underwent surgery for adenoma resection. In each case, the
From the 1LINT, Facultad de Medicina, Universidad Nacional de Tucumán, Tucumán; 2Jefe delServicio de Neurocirugía, Hospital Padilla, Tucumán; 3Departamento de Neurocirugía, FLENI,Buenos Aires; and 4Universidad Nacional de Buenos Aires, Hospital de Clinicas, BuenosAires, Argentina
To whom correspondence should be addressed: Juan F. Villalonga, M.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2019).https://doi.org/10.1016/j.wneu.2018.12.094
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
surgeon used the transsphenoidal endonasal route andmicroscopictechniques. All surgeries were performed by the same surgeon(A.C.) and filmed in 3 dimensions (Blackmagic Micro Cinemacameras; 1920 � 1080, 1080p24 frames per second; constructed byBlackmagic Design, PortMelbourne, Victoria, Australia). Accordingto the intraoperativefindings of the tumorecistern interface, 2 typesof “barriers” were identified: 1 consisting of the arachnoid, sellardiaphragm, and/or pituitary glandular tissue (i.e. a “strong” barrier)and 1 consisting only of the arachnoid (i.e. a “weak” barrier). Theintraoperative findings and preoperative magnetic resonanceimaging (MRI) findings were compared using a specific MRI pro-tocol for the sellar region. The MRI protocol included sagittal andcoronal slices from T1-weighted volumetric sequences, with andwithout contrast, and axial and sagittal slices of the sellar regionfrom T2-weighted, fluid-attenuated inversion recovery, diffusion-weighted imaging, and echo spin gradient sequences (Signa HDxt1.5T Resonator [GE Healthcare, Chicago, Illinois, USA]).21 TheKodak Carestream PACSeClient Suite, version 10, software(Kodak, Rochester, New York, USA) was used to measure the“barrier.” The measurements were taken in the cephalocaudal di-rection on different serial sections of the coronary and sagittalplanes.For statistical analysis, the patients were divided into 2 groups:
those with a barrier <1 mm in width on the preoperative MRIscans and those with a barrier >1 mm in width measured on theT1-weighted volumetric sequences. All 3D videos and MRI scanswere evaluated by the senior author (A.B.).
RESULTS
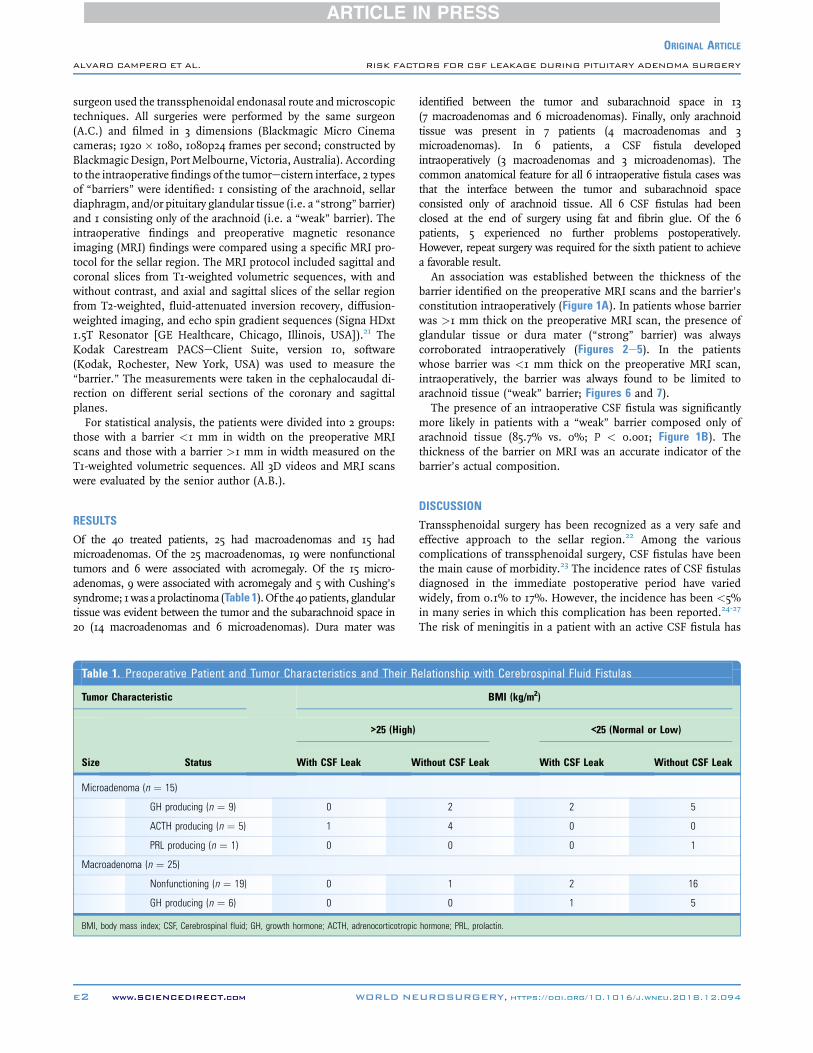
Of the 40 treated patients, 25 had macroadenomas and 15 hadmicroadenomas. Of the 25 macroadenomas, 19 were nonfunctionaltumors and 6 were associated with acromegaly. Of the 15 micro-adenomas, 9 were associated with acromegaly and 5 with Cushing’ssyndrome; 1was aprolactinoma (Table 1).Of the 40patients, glandulartissue was evident between the tumor and the subarachnoid space in20 (14 macroadenomas and 6 microadenomas). Dura mater was
Table 1. Preoperative Patient and Tumor Characteristics and Their R
Tumor Characteristic
Size Status
>25 (High)
With CSF Leak W
Microadenoma (n ¼ 15)
GH producing (n ¼ 9) 0
ACTH producing (n ¼ 5) 1
PRL producing (n ¼ 1) 0
Macroadenoma (n ¼ 25)
Nonfunctioning (n ¼ 19) 0
GH producing (n ¼ 6) 0
BMI, body mass index; CSF, Cerebrospinal fluid; GH, growth hormone; ACTH, adrenocorticotropic
e2 www.SCIENCEDIRECT.com WORLD NE
identified between the tumor and subarachnoid space in 13(7 macroadenomas and 6 microadenomas). Finally, only arachnoidtissue was present in 7 patients (4 macroadenomas and 3microadenomas). In 6 patients, a CSF fistula developedintraoperatively (3 macroadenomas and 3 microadenomas). Thecommon anatomical feature for all 6 intraoperative fistula cases wasthat the interface between the tumor and subarachnoid spaceconsisted only of arachnoid tissue. All 6 CSF fistulas had beenclosed at the end of surgery using fat and fibrin glue. Of the 6patients, 5 experienced no further problems postoperatively.However, repeat surgery was required for the sixth patient to achievea favorable result.An association was established between the thickness of the
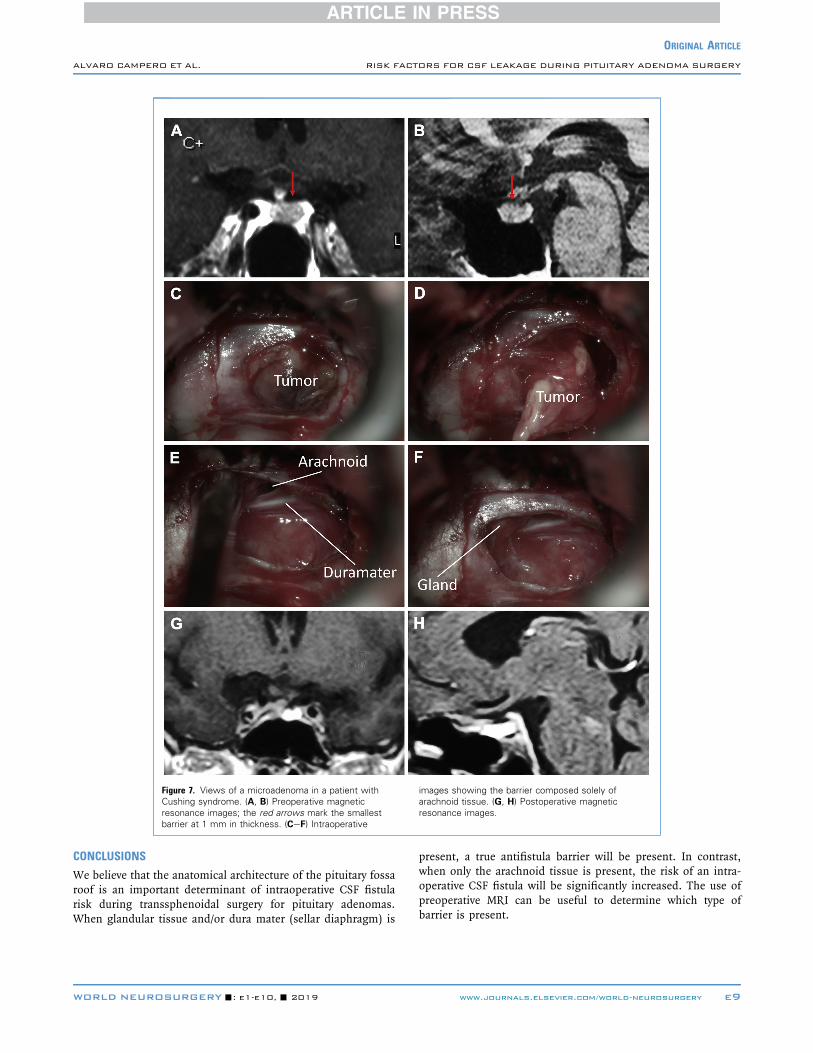
barrier identified on the preoperative MRI scans and the barrier’sconstitution intraoperatively (Figure 1A). In patients whose barrierwas >1 mm thick on the preoperative MRI scan, the presence ofglandular tissue or dura mater (“strong” barrier) was alwayscorroborated intraoperatively (Figures 2e5). In the patientswhose barrier was <1 mm thick on the preoperative MRI scan,intraoperatively, the barrier was always found to be limited toarachnoid tissue (“weak” barrier; Figures 6 and 7).The presence of an intraoperative CSF fistula was significantly
more likely in patients with a “weak” barrier composed only ofarachnoid tissue (85.7% vs. 0%; P < 0.001; Figure 1B). Thethickness of the barrier on MRI was an accurate indicator of thebarrier’s actual composition.
DISCUSSION
Transsphenoidal surgery has been recognized as a very safe andeffective approach to the sellar region.22 Among the variouscomplications of transsphenoidal surgery, CSF fistulas have beenthe main cause of morbidity.23 The incidence rates of CSF fistulasdiagnosed in the immediate postoperative period have variedwidely, from 0.1% to 17%. However, the incidence has been <5%in many series in which this complication has been reported.24-27
The risk of meningitis in a patient with an active CSF fistula has
Figure 1. Statistical data regarding the barrier. (A) Threshold of the barrieron preoperative magnetic resonance imaging (MRI) and compositionintraoperatively. (B) Presence of intraoperative cerebrospinal fluid (CSF)fistulas and composition of the barrier intraoperatively.
ORIGINAL ARTICLE
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
been 19%.28 In addition, the placement of a lumbar drainage tube isan invasive procedure that carries its own risks.29
Our team has found it useful to differentiate, in the registries,between intraoperative and postoperative fistula rates. Stricklandet al.1 reported a series of patients, 37.4% of whom developed anintraoperative fistula and 2.6% still had a fistula postoperatively.In our series, the corresponding rates were 15.0% and 2.5%.Currently, several techniques for CSF anti-fistula reconstruction
for use with the endoscopic endonasal approach are being greatlypromoted.6-20 These have included multiple layers; combining fat,fascia lata, and septal cartilage; pedunculated flaps; dural sub-stitutes; and nonautologousmaterials.28 In addition, other reportedstudies have had, as their primary objective, the early identificationof CSF fistulas and, for example, assessed the utility of intrathecalfluorescein dye to demonstrate an intraoperative fistula30 and thepresence of pneumocephalus on postoperative computedtomography,31 among others.Of the studies that reported the preoperative determinants of CSF
fistula development, the study by Lobatto et al.32 deserves specialmention. After conducting a systematic review of the reporteddata, they analyzed each factor in sequence, beginning with thedemographic and morphometric factors (e.g., age, gender, andbody mass index), tumor characteristics (e.g., size or volume,extent, histopathologic features), and treatment-related factors(e.g., previous surgery, use of radiation, surgeon learning curve).
WORLD NEUROSURGERY-: e1-e10, - 2019
They concluded that the only risk factor consistently associated witha greater risk of CSF fistula was intraventricular extension of thetumor.32 Other studies have supported the hypothesis that a highbody mass index (BMI) is an independent risk factor for CSFfistula formation.23,33 In our experience, a high BMI was not a sig-nificant and independent risk factor because only one patient with ahigh BMI developed an intraoperative CSF fistula (Table 1).Regarding the surgeon’s learning curve as a risk factor for CSFfistula, several investigative groups have studied this as an issueof interest, with many considering 100 procedures necessary for asurgeon to achieve a stable surgical plateau.34
We believe that the structure of the interphase between thetumor and the sellar cistern might be more important than thesize or suprasellar extension of the tumor in the genesis of anintraoperative CSF fistula. To the best of our knowledge, however,the present study is the first to consider anatomical factors aspotential predictors of intraoperative CSF fistulas.
Sellar Anatomy: A New Predictive FactorThe anatomy of the roof of the pituitary fossa is highly variable.35 Ina previous study of the sellar diaphragm anatomy, performed using20 adult cadavers, the opening of the diaphragm was classified assmall (<4 mm) in 20% of cases, intermediate (4e8 mm) in 40%,and large (>8 mm)in 40%.35 This anatomical knowledge,together with the intraoperative findings from the present series,have aroused our interest in the systematic study of the anatomyof the pituitary fossa roof in the context of hypophysis adenomasto determine whether the same variability in barrier compositionplays a predictive role similar to that for CSF fistulas.From our intraoperative findings, their correlation with the
preoperative MRI findings, and the later corroboration by a se-nior neurosurgeon (A.B.) examining the 3D videos of the pro-cedures, we believe that between the tumor and thesubarachnoid space just 3 tissues will be interposed: glandularpituitary tissue and the dura mater of the sellar diaphragm, withthe presence of both inconsistent, and the arachnoid, which willalways be present. Therefore, the only constant component ofthe interface between the tumor and the CSF will be thearachnoid.In all 6 patients in our series who developed a CSF fistula
intraoperatively, a weak barrier, consisting only of the arachnoid,was identified at the tumoreCSF interface. Moreover, these were 6of just 7 patients with this anatomical architecture, resulting in ahigh percentage (87%) that significantly greater than the 0% rateobserved for all other patients, with �99.9% confidence(P < 0.001).
Usefulness of Knowing the Anatomical Risk FactorWe believe consider that identifying those patients with a high riskof developing an intraoperative CSF fistula preoperatively would beuseful for surgical planning and choosing the best technique. Forexample, one could plan the type of flap to be created and foreseewhich materials would be necessary for the reconstructive phase.The latter is especially important in developing countries owing tothe limited availability of certain resources (e.g., synthetic seal-ants). In addition, the knowledge of a high risk of an intra-operative CSF fistula in relationship to the patient’s own anatomycould be important when discussing their case with the patient
Figure 2. Views of a patient with a nonfunctioningmacroadenoma. (A, B) Preoperative magneticresonance images; the yellow arrows indicate thebarrier, which captured contrast with a thickness >1
mm. (CeF) Intraoperative images showing the barriercomposed of glandular tissue. (G, H) Postoperativemagnetic resonance images.
ORIGINAL ARTICLE
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
(e.g., postoperative nasal symptoms, operative time, postoperativeCSF fistula risk) and could have legal implications in the post-operative period.At present, with the advances in MRI, various structures of the
sellar region can be identified, and the barrier located at the roofof the pituitary fossa can be measured. This would useful for
e4 www.SCIENCEDIRECT.com WORLD NE
estimating the risk of intraoperative CSF leaks and explaining suchrisks to the patient.
Endoscopic View of Pituitary Fossa Roof: The Next StepIn 1963, Guiot et al.36 first proposed the use of the endoscope as partof the transnasorhinoseptal microsurgical approach to explore the
Figure 3. Views of a macroadenoma in an acromegalicpatient in the context of an empty sella turcica. (A, B)Preoperative magnetic resonance images; the yellowarrows indicate the barrier, which captured contrast
with a thickness >1 mm. (CeF) Intraoperative imagesshowing the barrier composed of glandular tissue. (G,H) Postoperative magnetic resonance images.
ORIGINAL ARTICLE
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
sellar contents. However, this idea remained unrecognized until thefurther contribution of Apuzzo et al.36 in 1977. The use of theendoscope in transsphenoidal surgery was reconsidered as aresult of advances in optical technology that permitted the
WORLD NEUROSURGERY-: e1-e10, - 2019
development of adequate endoscopic instrumentation and thewidespread use of endoscopes in nasal and paranasal sinussurgery by otolaryngologists. Some investigators have describedan endoscope-assisted technique (i.e., the use of the endoscope
Figure 4. Views of a patient with a nonfunctioningmacroadenoma. (A, B) Preoperative magneticresonance images; the yellow arrows indicate thebarrier, which captured contrast with a thickness >1
mm. (CeF) Intraoperative images showing the barriercomposed of dura mater. (G, H) Postoperativemagnetic resonance images.
ORIGINAL ARTICLE
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
to complement the microscope in the early or late stages of atraditional procedure). “Pure” endoscopic endonasal trans-sphenoidal surgery, with the endoscope used alone throughout theapproach to visualize the surgical trajectory and the surgical targetarea, has been described in detail by Jho and Carrau.36
e6 www.SCIENCEDIRECT.com WORLD NE
The endoscopic endonasal technique brings advantages to thepatient (e.g., less nasal traumatism, less postoperative pain), tothe surgeon (e.g., wider and closer view of the surgical target area,increased scientific activity, smoothing of interdisciplinary coop-eration), and to the institution (e.g., shorter postoperative hospital
Figure 5. Views of a microadenoma in an acromegalicpatient. (A, B) Preoperative magnetic resonanceimages; the yellow arrows indicate the barrier, whichcaptured contrast with a thickness >1 mm. (CeF)
Intraoperative images showing the barrier composed ofdura mater. (G, H) Postoperative magnetic resonanceimages.
ORIGINAL ARTICLE
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
stay, increased case load).37 However, the endoscopic endonasaltechnique has some limits. This procedure is technicallydemanding and requires some additional specific endoscopicskills. The endoscope provides a 2-dimensional view, and thesurgeon must overcome the inferior depth perception using
WORLD NEUROSURGERY-: e1-e10, - 2019
“in-and-out” movements of the endoscope with the aim of iden-tifying the main surgical landmarks. However, in the presence of apresellar or conchal sphenoid sinus, which will provide a paucityof anatomical landmarks, use of an image-guidance neuro-navigation system could be very useful to guide the procedure.37
Figure 6. Views of a macroadenoma in an acromegalicpatient. (A, B) Preoperative magnetic resonanceimages; the red arrows mark the barrier, which was <1
mm thick. (CeF) Intraoperative images showing thebarrier composed solely of arachnoid tissue. (G, H)Postoperative magnetic resonance images.
ORIGINAL ARTICLE
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
Our patients underwent surgery with the microscopictechnique, and our series was evaluated retrospectively, withall the imperfections that this method presents. New studieswith a greater casuistry and using the endoscopic techniquewould serve to corroborate the conclusions proposed in
e8 www.SCIENCEDIRECT.com WORLD NE
the present study. It is not minor to note that anintraoperative CSF leak is the consequence, at least insome cases, of an anatomical defect of the roof of the pituitaryfossa of the patient and not the technique used by theneurosurgeon.
Figure 7. Views of a microadenoma in a patient withCushing syndrome. (A, B) Preoperative magneticresonance images; the red arrows mark the smallestbarrier at 1 mm in thickness. (CeF) Intraoperative
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
CONCLUSIONS
We believe that the anatomical architecture of the pituitary fossaroof is an important determinant of intraoperative CSF fistularisk during transsphenoidal surgery for pituitary adenomas.When glandular tissue and/or dura mater (sellar diaphragm) is
WORLD NEUROSURGERY-: e1-e10, - 2019
present, a true antifistula barrier will be present. In contrast,when only the arachnoid tissue is present, the risk of an intra-operative CSF fistula will be significantly increased. The use ofpreoperative MRI can be useful to determine which type ofbarrier is present.
ALVARO CAMPERO ET AL. RISK FACTORS FOR CSF LEAKAGE DURING PITUITARY ADENOMA SURGERY
REFERENCES14. Hadad G, Bassagas
A novel reconstructiv
1. Strickland BA, Lucas J, Harris B, et al. Identifica-tion and repair of intraoperative cerebrospinalfluid leaks in endonasal transsphenoidal pituitarysurgery: surgical experience in a series of 1002patients. J Neurosurg. 2018;129:425-429.
2. Hardy J. Transsphenoidal microsurgery of thenormal and pathological pituitary. Clin Neurosurg.1969;16:185-217.
3. Jho H, Carrau R. Endoscopy assisted trans-sphenoidal surgery for pituitary adenoma. ActaNeurochir (Wien). 1996;138:1416-1425.
4. Cappabianca P, Alfieri A, de Divitiis E. Endo-scopic endonasal transsphenoidal approach to thesella: towards functional endoscopic pituitarysurgery (FEPS). Minim Invasive Neurosurg. 1998;41:66-73.
5. Jho H, Carrau R. Endoscopic endonasal trans-sphenoidal surgery: experience with fifty patients.J Neurosurg. 1997;87:44-51.
6. Bergsneider M, Xue K, Suh JD, Wang MB. Barrier-limited multimodality closure for reconstructionof wide sellar openings. Oper Neurosurg. 2011;71:68-76.
7. Cappabianca P, Esposito F, Magro F, et al. Naturaabhorret a vacuo—use of fibrin glue as a filler andsealant in neurosurgical “dead spaces”: technicalnote. Acta Neurochir (Wien). 2010;152:897-904.
8. Cho JM, Ahn JY, Chang JH, Kim SH. Prevention ofcerebrospinal fluid rhinorrhea after trans-sphenoidal surgery by collagen fleece coated withfibrin sealant without autologous tissue graft orpostoperative lumbar drainage. Oper Neurosurg.2011;68:130-137.
9. Duntze J, Litré CF, Graillon T, et al. Rhinorrhéecérébrospinale après chirurgie hypophysaireendoscopique trans-sphénoïdale: réflexions après337 patients. Neurochirurgie. 2012;58:241-245.
11. Freyschlag CF, Goerke SA, Obernauer J,Kerschbaumer J, Thomé C, Seiz M. A sandwichtechnique for prevention of cerebrospinal fluidrhinorrhea and reconstruction of the sellar floorafter microsurgical transsphenoidal pituitary sur-gery. J Neurol Surg A Cent Eur Neurosurg. 2015;77:229-232.
13. Goljo E, Kinberg E, Stepan K, et al. Reconstruc-tion of a skull base defect after endoscopicendonasal resection of a pituitary adenoma:sphenoid mucosal flaps. Am J Otolaryngol. 2018;39:253-256.
e10 www.SCIENCEDIRECT.com
teguy L, Carrau RL, et al.e technique following endo-
15. Luginbuhl AJ, Campbell PG, Evans J, Rosen M.Endoscopic repair of high-flow cranial base de-fects using a bilayer button. Laryngoscope. 2010;120:876-880.
16. Magro E, Graillon T, Lassave J, et al. Complica-tions related to the endoscopic endonasal trans-sphenoidal approach for nonfunctioning pituitarymacroadenomas in 300 consecutive patients.World Neurosurg. 2016;89:442-453.
17. Nishioka H, Izawa H, Ikeda Y, Namatame H,Fukami S, Haraoka J. Dural suturing for repair ofcerebrospinal fluid leak in transnasal trans-sphenoidal surgery. Acta Neurochir (Wien). 2009;151:1427-1431.
18. Patel MR, Stadler ME, Snyderman CH, et al. Howto choose? Endoscopic skull base reconstructiveoptions and limitations. J Neurol Surg B Skull Base.2010;20:397-402.
19. Pereira EA, Grandidge CA, Nowak VA, Cudlip SA.Cerebrospinal fluid leaks after transsphenoidalsurgery—effect of a polyethylene glycol hydrogeldural sealant. J Clin Neurosci. 2017;44:6-10.
20. Rivera-Serrano CM, Snyderman CH, Gardner P,et al. Nasoseptal “rescue” flap: a novel modifica-tion of the nasoseptal flap technique for pituitarysurgery. Laryngoscope. 2011;121:990-993.
21. Chung SB, Kwag KS, Kim ST, Park K, Kim JH,Kong DS. 3D T2-weighted turbo spin-echo MRsequence for identifying cerebrospinal fluid leakafter endoscopic endonasal pituitary surgery. ActaNeurochir (Wien). 2012;154:1499-1503.
23. Zhou Q, Yang Z, Wang X, et al. Risk factors andmanagement of intraoperative cerebrospinal fluidleaks in endoscopic treatment of pituitary ade-noma: analysis of 492 patients. World Neurosurg.2017;101:390-395.
24. Berker M, Hazer DB, Yücel T, et al. Complicationsof endoscopic surgery of the pituitary adenomas:analysis of 570 patients and review of the litera-ture. Pituitary. 2012;15:288-300.
25. Gondim JA, Almeida JP, De Albuquerque LA,Gomes E, Schops M, Mota JI. Endoscopic endo-nasal transsphenoidal surgery in elderly patientswith pituitary adenomas. J Neurosurg. 2015;123:31-38.
26. Gondim JA, Almeida JPC, De Albuquerque LA,et al. Endoscopic endonasal approach for pituitaryadenoma: surgical complications in 301 patients.Pituitary. 2011;14:174-183.
27. Sanders-Taylor C, Anaizi A, Kosty J, Zimmer LA,Theodosopoulos PV. Sellar reconstruction and
WORLD NEUROSURGERY, http
rates of delayed cerebrospinal fluid leak afterendoscopic pituitary surgery. J Neurol Surg B SkullBase. 2015;76:281-285.
28. Nix P, Tyagi A, Phillips N. Retrospective analysisof anterior skull base CSF leaks and endoscopicrepairs at Leeds. Br J Neurosurg. 2016;30:422-426.
29. Tien DA, Stokken JK, Recinos PF, Woodard TD,Sindwani R. Cerebrospinal fluid diversion inendoscopic skull base reconstruction: anevidence-based approach to the use of lumbardrains. Otolaryngol Clin North Am. 2016;49:119-129.
30. Jakimovski D, Bonci G, Attia M, et al. Incidenceand significance of intraoperative cerebrospinalfluid leak in endoscopic pituitary surgery usingintrathecal fluorescein. World Neurosurg. 2014;82:513-523.
31. Banu MA, Szentirmai O, Mascarenhas L, Salek AA,Anand VK, Schwartz TH. Pneumocephalus pat-terns following endonasal endoscopic skull basesurgery as predictors of postoperative CSF leaks.J Neurosurg. 2014;121:961-975.
32. Lobatto DJ, De Vries F, Najafabadi AHZ, et al.Preoperative risk factors for postoperative com-plications in endoscopic pituitary surgery: a sys-tematic review. Pituitary. 2018;21:84-97.
33. Dlouhy BJ, Madhavan K, Clinger JD, et al. Elevatedbody mass index and risk of postoperative CSFleak following transsphenoidal surgery.J Neurosurg. 2012;116:1311-1317.
34. Shikary T, Andaluz N, Meinzen-Derr J, Edwards C,Theodosopoulos P, Zimmer LA. Operativelearning curve after transition to endoscopictranssphenoidal pituitary surgery. World Neurosurg.2017;102:608-612.
35. Campero A, Martins C, Yasuda A, Rhoton AL Jr.Microsurgical anatomy of the diaphragma sellaeand its role in directing the pattern of growth ofpituitary adenomas. Neurosurgery. 2008;62:717-723.
36. Cappabianca P, Cavallo LM, de Divitis E. Endo-scopic endonasal transphenoidal surgery. Neuro-surgery. 2004;55:933-941.
Conflict of interest statement: The authors declare that thearticle content was composed in the absence of anycommercial or financial relationships that could be construedas a potential conflict of interest.
Received 22 September 2018; accepted 11 December 2018
Citation: World Neurosurg. (2019).https://doi.org/10.1016/j.wneu.2018.12.094