Global Development Network Strengthening Institutions to Improve Public Expenditure Accountability Cost-Effectiveness of Voluntary Counseling and Testing (VCT) and Provider-initiated Testing and Counseling (PITC) in a Hospital-Based Clinic in Indonesia Adiatma Y.M. Siregar Dindin Komarudin Pipit Pitriyan Center for Economics and Development Studies (CEDS), Padjadjaran University March, 2013
Transcript
Global Development NetworkStrengthening Institutions to Improve Public Expenditure Accountability
Cost-Effectiveness
of Voluntary Counseling
and Testing (VCT) and
Provider-initiated Testing
and Counseling (PITC)
in a Hospital-Based Clinic
in Indonesia
Adiatma Y.M. SiregarDindin KomarudinPipit PitriyanCenter for Economics and Development Studies (CEDS), Padjadjaran University
March, 2013
The Global Development Network (GDN) is an International Organization that builds research capacity in development globally. GDN supports researchers in developing and transition countries to generate and share high quality applied social science research to inform policymaking and advance social and economic development. Founded in 1999, GDN is headquartered in New Delhi, with offices in Cairo and Washington DC.
This Research Paper has been prepared as part of the research which was conducted under the GDN Global Research Project “Strengthening Institutions to Improve Public Expenditure Accountability”, implemented in partnership with Results for Development Institute (R4D), USA with the aim of building and strengthening institutional capacity for public expenditure analysis across developing and transitional countries. The Global Research Project is fully funded by the Department for International Development (DFID), UK. The views expressed in this publication are those of the author(s) alone.
Abstract The HIV epidemic in Indonesia is among the fastest growing in Asia and calls for scaling up of interventions. Two current interventions are Voluntary Counseling and Testing (VCT) and Provider-initiated Testing and Counseling (PITC). Scaling up these two interventions, however, must be analyzed from an economic framework, given the limited existing budget. There are two main concerns: (1) the issue of extending the coverage of VCT through PITC which has not been economically analyzed, and (2) economic evaluation studies on both interventions are limited. Methods: The cost estimation is based on a previous study on the costs of delivering VCT which is adapted to estimate the cost of delivering hospital-based VCT and PITC. The effectiveness study is also adapted from a previous study on the natural decline of CD4 cell count on HIV-positive clients, both intravenous drug users (IDUs) and non-IDUs, in terms of life-years saved. Results: Most clients are in their productive age. The unit cost per HIV-positive person detected differs by US$37. The time gained by utilizing VCT compared to PITC for IDUs is less than that of non-IDUs. The Incremental Cost-Effectiveness Ratio (ICER) of performing VCT as compared to PITC for unit cost per HIV-positive case is higher for non-IDUs as compared to IDUs. Discussion: VCT has the benefit of early detection as compared to PITC. The unit costs of VCT and PITC per HIV-positive case for each service shows higher costs for PITC than VCT. The ICER based on unit costs per HIV-positive case for both IDUs and non–IDUs shows that providing VCT will result in less cost in gaining more life years. Although the results show that VCT seems to be more cost-effective than PITC, the unique characteristics of PITC should also be considered. We suggest that PITC may not be the best scaling-up measure replacing VCT, but may complement it. Keywords: HIV, Cost-effectiveness, Economic Evaluation, IDUs, VCT, PITC. JEL classification: I14, I18
4
Background The HIV epidemic in Indonesia is one of the fastest spreading epidemics in Asia, and it is estimated that without an acceleration in prevention strategies, the HIV-positive population will grow to 482,800 by 2014 (UNAIDS, 2007; MoH, 2008). From 2004 to 2009, the cumulative number of reported AIDS cases rose from 2,682 to 19,973. Cases of HIV infection were reported from 16 out of 33 provinces in 2004, and increased to 32 out of 33 provinces in 2009. Within this period, both drug injection and sexual transmission were the main modes of transmission (NAC [a], 2009). In response to this, HIV/AIDS control efforts have increased considerably in Indonesia in recent years (Siregar, et al., 2009), with voluntary counseling and testing (VCT) being a key component in the national strategic plan (Afriandi, et al., 2009). VCT offers an entry point for the treatment of HIV-positive individuals, and is instrumental in preventing the further spread of the disease by reducing risk behavior among tested individuals (UNAIDS, 2001). The number of VCT centers increased from 25 in 2004 to 547 in mid-2009 (NAC [a], 2010). Between 2004 and 2007, there was an increase in the incidence of VCT delivered to high-risk groups, especially injecting drug users (IDUs), from 18 to 41 percent (Integrated Biological-Behavioral Surveillance, 2007, cited in NAC [b], 2010). To complement the ongoing VCT effort, provider-initiated HIV testing and counseling (PITC) is also available to improve access to care by HIV-infected patients and strengthen national HIV/AIDS control efforts. PITC is recommended by health care providers as a standard component of medical care which will help arrive at clinical decisions and medical treatment according to a person’s HIV status. It also aims to increase the number of patients tested, to detect unsuspected HIV-infected clients attending health facilities, and presents an opportunity to ensure that HIV is more systematically diagnosed in health care facilities (Leelukkanaveera, et al., 2010; WHO, 2007; Becker et al., 2009). Both interventions will be elaborated later. There are two concerns which relate to the interventions and arise from policy and academic points of view. The former concern arises from the idea of extending the coverage of VCT through PITC, so that the latter will not merely complement VCT. Given the limited budget for HIV/AIDS in Indonesia (Siregar, et al., 2009), and the varied health condition of clients accessing either service, scaling up VCT by replacing it with PITC warrants investigation to explore whether this option is economically feasible. The second concern is at an academic level; although VCT and PITC are important interventions, economic evaluation of both interventions in Asia is limited, as pointed out by Walker (2003). Currently, evidence on costs of VCT only includes two studies in Thailand (Teerawattananon et al., 2005; HITAP, 2008), one study at the South-east Asian sub-regional level (Hogan et al., 2005), and one in India (Dandona et al., 2008). There is at present only one economic evaluation comparing VCT and PITC in Thailand (Leelukkanaveera, et al., 2010). To our knowledge, there is no research on the cost-effectiveness of VCT and PITC in Indonesia. This paper tries to address these concerns through a cost-effectiveness study comparing VCT and PITC in Indonesia, based mainly on the number of HIV-positive cases detected and the benefit of early detection. This study is unique for two reasons. First, it provides the first such study in Indonesia, which is an important input for rational decision-making on the scaling up of service delivery (Siregar et al., 2009). Second, the study also estimates the relevant program costs which are typically ignored in economic analysis (Johns et al., 2003), and the costs for patients seeking and undergoing VCT and PITC. Both program costs and patient costs are significant when making the decision to scale up VCT and PITC services.
5
Methods Study Setting: The study combines the results of a study by Siregar et al. (2010) and Meijerink (unpublished) under the IMPACT project, and the results of our own research. The IMPACT project is collaboration between one university in Indonesia (Universitas Padjadjaran) and three European universities. All studies have been conducted at clinics located at and associated with Hasan Sadikin hospital, a teaching and provincial top-referral public hospital for West Java (with a population of approximately 40 million). The clinics studied are the hospital clinic, Methadone Maintenance Treatment (MMT), and a prison-based clinic (which conducts all HIV-related services in collaboration with Hasan Sadikin hospital).
Study Sites:
Hospital Clinic (Teratai Clinic) This clinic is situated in Hasan Sadikin hospital and delivers both general medical services and HIV-related services such as VCT, PITC, ART (antiretroviral treatment), and STI (sexually transmitted infection). It is frequented by both the general population and high- risk groups, mostly IDUs. The number of visits for HIV-related services is very high and the clinic currently operates at full capacity. It generates its own revenues through user fees, but also relies on government, hospital, and donor funding. This clinic is included in both studies by Siregar and Meijerink. MMT Clinic The MMT clinic in Hasan Sadikin hospital was established in May 2006 and is still running. It is one of the 24 MMT service points across the country and opens every day from morning till noon. The clinic works closely with the HIV clinic in the hospital. This clinic is included in the study by Meijerink. Prison Clinic This clinic is within the premises of a prison for drug users, including IDUs. All tests and HIV-related services are delivered in collaboration with Hasan Sadikin hospital: the HIV tests are conducted at Hasan Sadikin hospital, where HIV-positive prisoners also receive ART. This clinic is included in the study by both Siregar and Meijerink. The Interventions:
Voluntary Counseling and Testing (VCT) Traditional VCT focuses on walk-in clients and offers specialized counseling sessions tailored to the risk behavior of individual patients. The VCT service is voluntary and confidential, shared only between the counselor and the client. An individual is considered to have undergone VCT if he/she has followed the whole procedure; i.e. Pre-test counseling, HIV test, and post-test counseling. Counseling is defined as professional advice and suggestions given to an individual with problems. This is delivered by counselors who are members of the staff and have the ability to counsel with complete and comprehensive understanding of HIV/AIDS. Post-test counseling specifically focuses on risk reduction and “positive living”, regardless of the results (Surdo, 2007; RSHS, 2008). The aim of VCT is, first, to help those individuals at risk of HIV or PLWHA (people living with HIV/AIDS) to lead a healthier and safer life through psychological support to the individual and his/her family. Second, VCT attempts to reduce the risk of infection through information-sharing on
6
risk behavior, and to assist and support clients in developing a healthy lifestyle. Finally, VCT is also aimed at ensuring effective and early treatment (RSHS, 2008). Figure 1 depicts the VCT procedure in Teratai clinic in Hasan Sadikin Hospital. Figure 1: VCT Procedure in Hasan Sadikin Hospital
Adapted from Hasan Sadikin Hospital Bandung VCT Procedure (2008). Provider-Initiated Testing and Counseling (PITC) To complement the ongoing VCT program, provider-initiated HIV testing and counseling (PITC) is provided to improve access to care by HIV-infected patients and contribute to the success of national HIV/AIDS control efforts. PITC refers to HIV testing and counseling which is recommended by health care providers to clients as a standard component of medical care, diagnostic testing, and/or a routine offer. It aims to enable specific clinical decisions to be made, and/or specific medical services to be performed with knowledge of the person’s HIV status; this is because providers need HIV diagnosis in order to provide quality care for their patients. The intervention also aims to increase the number of patients tested, early detection, and detection of unsuspected HIV-infected clients attending health facilities. It also presents an opportunity to ensure that HIV is more systematically diagnosed in health care facilities (Leelukkanaveera, et al., 2010; WHO, 2007; Becker et al., 2009; Surdo, 2007; RSHS, 2008). Figure 2 describes the procedure of PITC in Hasan Sadikin hospital.
From within Hospital:
- In-patient care
- Out-patient care
- Emergency unit
- MCU
- Laboratory
From outside hospital
Hospital clinic
Registration
Pre-test counseling
Ready for test
Laboratory
Results
Post-test counseling
No
Advise the client to make
another visit on an agreed
schedule
Yes
Informed consent
signing
Filling test request
form
7
Figure 2: PITC Procedure in Hasan Sadikin Hospital
Adapted from Hasan Sadikin Hospital Bandung PITC Procedure (2008). Cost Estimation: The cost estimation of delivering VCT in a hospital clinic is derived and adapted from a research study by Siregar et al. (2010). The research estimates the costs of VCT in four different settings: hospital clinic, community HIV clinic, community STI clinic, and prison clinic. We took the results of VCT costs in the hospital clinic in our analysis. This includes health care costs (costs related to the consumption of resources in the health care system), and non-health care costs (costs incurred by the patient for seeking and undergoing care) of delivering hospital-based VCT service. The health care costs for PITC are calculated by using a similar method from the same study by Siregar, et al. (2010), as well as a study by Afriandi, et al. (2009) which incorporates micro-costing (Drummond, et al., 2005). Relevant health care costs were estimated on the basis of service utilization and service cost data. The data on service utilization were retrieved from the hospital clinic’s records, including information on the number of PITC cases and resources used. All resources used and salaries paid were listed and estimated on the basis of clinical records, interviews with medical staff, government standards or market price. Costs to the clinic consist of recurrent and capital costs. Personnel recurrent costs were estimated on the basis of their actual wage or estimated by using government salary scales (issued by Ministry of Finance in 2007). Other recurrent costs such as the cost of medical and administration services utilized during the year of observation
Doctor on duty in in-patient care
suspects of HIV/ AIDS
1. Doctor offers testing
2. Gives information on pre-test:
a. Infection
b. HIV prevention Agree
Not agree:
Suggestion to
take VCT
Informed consent
signing
VCT/
counseling
Blood sample intake:
Related doctor or Teratai clinic staff
Laboratory
Results disclosed by related doctor or
Teratai clinic staff Positive
Negative Follow up
8
were estimated using both actual and market prices. Laboratory costs were estimated using the current service charge. Capital costs, which include training and workshops for the clinic staff, were obtained from their actual budget or government records. Market prices were used to estimate other capital costs, which include the cost of equipment, furniture, as well as start-up costs. Capital costs were subsequently calculated per year on the basis of the life-span of the capital items. The costs of utilities were omitted (i.e. water and electricity). Non-health care costs (i.e. patient costs) for PITC were estimated based on the results of the study by Siregar, et al. (2010) as the socio-economic characteristics of the clients using VCT and PITC are roughly similar. Patient costs included information on demographic characteristics, travel and travel time, the monthly income of the client, the average number of daily working hours, and monthly expenditure. All costs were measured in rupiah, and converted to US$ using the current exchange rate (IMF, 2010). Effectiveness Measurement: The measurement of effectiveness was based on the model developed by Meijerink et al., using the CD4 cell count data for clients attending the hospital clinic. The model predicts the natural decline of the CD4 cell count of an HIV-positive person, either IDUs or non-IDUs, based on their CD4 cell count during the time of HIV testing. The decline of CD4 cell numbers is a very accurate and meaningful parameter to monitor the natural course of HIV infection. HIV antibodies are measured using different commercially available rapid tests. The hospital laboratory also uses immunoassays, with external quality control showing 100 percent accuracy (National Serology Reference Laboratory, Australia). CD4 cell measurements are performed at the hospital laboratory using Facscount flowcytometry (BD Biosciences, Jakarta, Indonesia). Data were derived from a cohort of 1,464 randomly selected HIV-infected patients attending the three urban clinics between August 2007 and August 2010. The Effectiveness Modeling (Study by Meijerink, et al.) All adults (≥16 years) with HIV infection between August 2007 and August 2010 who had not yet been exposed to ART were selected for the study. For the linear mixed model to describe the natural decline of CD4 cells over time, all patients who had subsequently undergone a CD4 cell count measurement at least one month apart were included. To meet all criteria for linear regression, all CD4 cell counts were transformed to the square root scale. The effect of IDU on the decline of CD4 cells was determined with an interaction-term between IDU and time (IDU*t). A constant variable was added to the model to account for the variability in CD4 cell decline, which is independent of other variables. The correlation between CD4 cell counts as measured and predicted by the model was determined and expressed as the coefficient of determination (R2). This model predicts that a decline from 350 to 200 CD4cells/µl would take an average of 20 months in patients with a history of IDU, compared with 38 months in patients without a history of IDU (a difference of 18 months). This indicates that people with a history of injected drug use progress 1.9 times faster from 350 to 200 CD4cells/µl. The study, however, is limited by the fact that half of our patients had had CD4 counts measured only twice. Despite limitations, however, the study by Meijerink, et al. still concludes that IDU accelerates the natural decline of CD4 cells in HIV-infected patients. The findings indicate that the progression of HIV should be monitored carefully in IDU patients, and that earlier initiation of ART should be considered for this risk group.
9
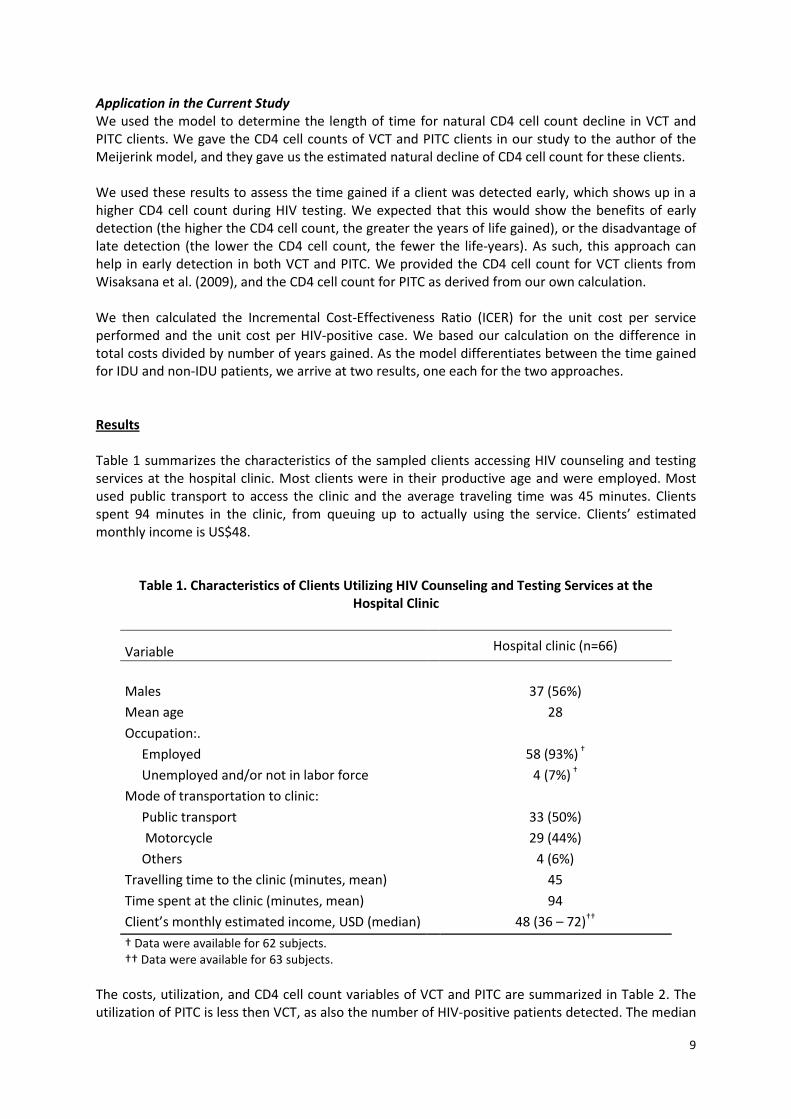
Application in the Current Study We used the model to determine the length of time for natural CD4 cell count decline in VCT and PITC clients. We gave the CD4 cell counts of VCT and PITC clients in our study to the author of the Meijerink model, and they gave us the estimated natural decline of CD4 cell count for these clients. We used these results to assess the time gained if a client was detected early, which shows up in a higher CD4 cell count during HIV testing. We expected that this would show the benefits of early detection (the higher the CD4 cell count, the greater the years of life gained), or the disadvantage of late detection (the lower the CD4 cell count, the fewer the life-years). As such, this approach can help in early detection in both VCT and PITC. We provided the CD4 cell count for VCT clients from Wisaksana et al. (2009), and the CD4 cell count for PITC as derived from our own calculation. We then calculated the Incremental Cost-Effectiveness Ratio (ICER) for the unit cost per service performed and the unit cost per HIV-positive case. We based our calculation on the difference in total costs divided by number of years gained. As the model differentiates between the time gained for IDU and non-IDU patients, we arrive at two results, one each for the two approaches. Results Table 1 summarizes the characteristics of the sampled clients accessing HIV counseling and testing services at the hospital clinic. Most clients were in their productive age and were employed. Most used public transport to access the clinic and the average traveling time was 45 minutes. Clients spent 94 minutes in the clinic, from queuing up to actually using the service. Clients’ estimated monthly income is US$48.
Table 1. Characteristics of Clients Utilizing HIV Counseling and Testing Services at the Hospital Clinic
† Data were available for 62 subjects. †† Data were available for 63 subjects.
The costs, utilization, and CD4 cell count variables of VCT and PITC are summarized in Table 2. The utilization of PITC is less then VCT, as also the number of HIV-positive patients detected. The median
10
CD4 cell count of VCT clients is far above the median CD4 cell count of PITC clients, while the annual costs in the year under study (including non- health care costs) for clients utilizing VCT is approximately triple that of PITC clients. The unit cost per service performed, however, does not differ significantly between the two services. The unit cost per HIV-positive client detected between the two services differs by US$37.
Table 2. Summary of Costs and Utilization
Variable VCT PITC Number of services performed 421 147
Number of HIV (+) detected 167 47
CD4 cell count on HIV (+) (/mm3) 129 (26 – 338)† 9 (1 – 184)††
One-year service costs (US$) 33,455 11,233
Unit cost per service performed (US$) 79 76
Unit cost per HIV (+) case (US$) 191 228
† Median (IQR). †† Median (min – max).
Table 3 shows the time gained and ICER, divided into IDU and non-IDU. The logic behind time gained is as follows: The CD4 cell count median of clients who took VCT is 129cells/µl, whereas those who underwent PITC had a CD4 cell count median of 9cells/µl. By using the model developed by Meijerink et al., the time required for the CD4 cell count to naturally decline from 129cells/µl to 9cells/µl is two years for IDUs, and around three years for non-IDUs. Applying this logic to our study, it can be said that IDUs using VCT will have two years before the CD4 cell count reaches the level where clients usually need to opt for PITC. In the case of non-IDUs, VCT will save around three years. The ICER for unit cost per service performed is higher for IDUs as compared to non-IDUs. The opposite applies to the ICER for unit cost per HIV-positive case.
Table 3. Time Gained and Incremental Cost-Effectiveness Ratio (ICER)
Time gained for doing VCT instead of PITC based on CD4 cell count
IDUs 2 years
Non – IDUs 3.2 years
ICER (US$/year gain)
based on unit cost per service performed
IDUs 1.52 US$/life years gain
Non – IDUs 0.96 US$/life years gain
based on unit cost per HIV (+) case
IDUs -18 US$/life years gain
Non – IDUs -12 US$/life years gain
11
Discussion Although both VCT and PITC are accessed in the hospital clinic, their cost-effectiveness has not been measured in Indonesia. This paper addresses this gap and tries to provide information that might be relevant for policy. As mentioned, clients accessing HIV counseling and testing in the hospital clinic are in their productive age; therefore, early detection becomes crucial to ensure that there is no loss of productivity. It is clear from our study that VCT clients make use of the service at an earlier stage of HIV than those who access PITC based on their CD4 cell count. Therefore, VCT has the benefit of early detection as compared to PITC. Currently, PITC clients come to the hospital at a late and/or complicated stage rather than for HIV testing. At a PITC client’s level of CD4 cell count (9 cells/µl), it is likely that they suffer from severe opportunistic infection and relatively high frequency of complications (Barlett & Gallant, 2007), and, as such, require more medical treatment and incur more costs. VCT service costs in one year are approximately triple that of PITC, amounting to US$33,455. This is understandable since VCT is utilized by more clients. However, dividing the total cost by number of services utilized resulted in only a US$3 difference in unit cost per service. Furthermore, dividing VCT and PITC total costs by the number of HIV–positive cases for each service showed in the opposite picture. In this respect, the unit cost per HIV-positive client is higher for PITC than VCT. Combining this with the benefit of early detection, VCT seems to be more cost-effective than PITC. Exploring the results of time gained, we derive an important conclusion. As VCT detects HIV-positive clients at a much higher CD4 cell count than PITC clients, providing VCT will give the client a certain estimated time gain. In other words, detecting HIV-positive clients at an earlier stage (higher CD4 cell count, where clients usually undergo VCT) will give the clients more time for treatment before they reach the late and more severe stage of the disease (lower CD4 cell count, where clients usually take the HIV test). To this extent, VCT seems to give clients more years as compared to PITC, i.e. two years for IDUs and around three years for non-IDUs. We then combined the results for time gained with the costs data to calculate the ICER for IDU and non-IDU clients. The ICER based on unit cost per service performed is relatively low for both IDUs and non-IDUs, implying that spending more money on VCT might be more appropriate, given the relatively low cost to society and the benefit of life-years gained. The ICER based on unit cost per HIV-positive case for both IDUs and non-IDUs throws up an interesting finding. Leaning on VCT in this respect will actually result in a lower cost to gain more life-years. This finding suggests that VCT actually reduces the cost to the society in gaining a year of life. This finding, however, may need further research to confirm if it is indeed the case. All our findings indicate that VCT seems to be more cost-effective than PITC. However, the unique characteristic of PITC should also be taken into account. It is important to note that the first step in PITC is performed by physicians through diagnosis. Clients utilizing PITC might include those who suffer from opportunistic infections that occur during a late stage of HIV/AIDS, and visit the physicians for consultation without realizing that they may already be HIV infected. Thus, these clients may not undergo HIV testing if they are not advised by the physicians to undergo PITC (or, in some cases, VCT). This unique characteristic emphasizes the usefulness of PITC as a complement to VCT and should be maintained, even if PITC is less cost-effective. However, scaling up VCT by replacing it with PITC should be considered carefully and done with care and even further analysis.
12
Some cautious advice when interpreting our results: First, this study has evaluated highly contextualized VCT and PITC service delivery models, which may hamper generaliziation. Yet, the conceptual decision framework can be applied to other settings. Second, we estimated patient costs of seeking and undergoing care on the basis of (assumed) productivity losses—we may then have overestimated the total patient costs. Third, personnel costs in clinics may include inefficiencies in the delivery of VCT and PITC services, and we may have overestimated total costs; a time-motion study is warranted to accurately assess the resources required to scale up VCT and PITC services. Fourth, the effectiveness model is based on the data of clients utilizing HIV counseling and testing in the hospital clinic, which provide both VCT and PITC. Developing a specific model for each service may generate more appropriate results. Fifth, there might be bias in client selection. Further research with random sample selection in clinics for VCT and PITC separately is necessary. In conclusion, we recommend that the current policy of the Indonesian government of providing PITC to complement VCT be maintained. As of now, this seems to be the most appropriate approach, given the current situation in Indonesia where HIV has reached epidemic proportions. Replacing VCT with PITC within the context of scaling up seems to be a less favorable option, although further research with a different approach may prove otherwise. Acknowledgements We would like to thank the IMPACT project and the staff of the Hasan Sadikin hospital clinic for making the necessary data available to us for analysis. Thanks to Hinta Meijerink for her assistance in providing her model to be used in the effectiveness analysis. We acknowledge the financial support of the Global Development Network in this research.
13
References Afriandi, I., A.Y.M. Siregar, F. Meheus, T. Hidayat, A. Van der Ven, R. Van Crevel, and R. Baltussen. “Costs of Hospital-based Methadone Maintenance Treatment in HIV/AIDS Control Among Injecting Drug Users in Indonesia”. Health Policy 2010, 95: 67-73. doi:10.1016/j.healthpol.2009.11.003 Afriandi, A., T. Aditama, D. Mustikawati, M. Oktavia, and B. Alisjahbana. “HIV and Injecting Drug Use in Indonesia: Epidemiology and National Response”. Acta Medica Indonesiana, the Indonesian Journal of Internal Medicine, a Publication of the Indonesian Society of Internal Medicine, 2009, 41(supplement.1): 75 – 78 Bartlett, J.G. and J.E. Gallant. Medical Management of HIV Infection, Baltimore, Johns Hopkins University School of Medicine, 2007. Becker, J., L. Tsague, R. Sahabo and P. Twyman. “Provider-initiated Testing and Counseling (PITC) for HIV in Resource-limited Clinical Settings: Important Questions Unanswered”. Pan African Medical Journal, 2009, 3:4. http://www.panafrican-med-journal.com/content/editorial/3/4/ Dandona, L., S.G.P. Kumar, Y.K. Ramesh, M.C. Rao and A.A. Kumar. “Changing Cost of HIV Interventions in the Context of Scaling-up in India”. AIDS, 2008; 22: S43-S49; doi:10.1097/01.aids.0000327622.24232.aa Drummond, M.F., M.J. Sculpher and G.W.Torrance. Methods for the Economic Evaluation of Health Care Programmes. 3rd Edition. New York, Oxford University Press, 2005. General Directorate of Communicable Disease Control and Environmental Health, Ministry of Health, Republic of Indonesia (MOH-RI). “Mathematical Model of HIV Epidemic in Indonesia 2008 – 2014”, Jakarta, 2008. Health Intervention and Technology Assessment Program (HITAP). “The Potential of Provider-Initiated Voluntary HIV Counseling and Testing at Health Care Settings in Thailand, Final Report, December 2008, Thailand. Hogan, D.R., R. Baltussen, C. Hayashi, J.A. Lauer and J.A. Salomon. “Cost Effectiveness Analysis of Strategies to Combat HIV/AIDS in Developing Countries: Achieving the Millennium Development Goals for Health”. BMJ, 2005;doi:10.1136/bmj.38643.368692.68 (published 10 November 2005). International Monetary Fund. Representative Exchange Rates for Selected Currencies. Available from: http://www.imf.org/external/np/fin/data/rms_rep.aspx, accessed 22 June 2010. Johns, B., R. Baltussen and R. Hutubessy. “ Programme Costs in the Economic Evaluation of Health Interventions: Cost Effectiveness and Resource Allocation”, 2003; 1:1; http://www.resource-allocation.com/content/1/1/1 Leelukkanaveera, Y., P. Sithisarankul and N. Hirunsutthikul. “Provider-initiated HIV Counseling and Testing of Out-patients at Community Hospitals in Thailand: An Economic Evaluation using the Markov Model”. Asian Biomedicine, 2010, 4 (3); 479-84; http://www.asianbiomed.org/htdocs/previous/A20104479.pdf Meijerink, H., R. Wisaksana, S. Iskandar, B. Alisjahbana, M. den Heijer, A. van der Ven and R. van Crevel. “Injecting Drug Use is Associated with a More Rapid CD4 Cell Decline and a Higher Risk of Tuberculosis among HIV-infected Patients in Indonesia”. Unpublished.
Ministry of Health of Indonesia (MoH). Mathematical Model of HIV Epidemic in Indonesia, Jakarta, 2008 National AIDS Commission (NAC), Republic of Indonesia (a). National Strategy and Action Plan on HIV and AIDS 2010 – 2014, Jakarta, 2010. National AIDS Commission (NAC), Republic of Indonesia (b). Republic of Indonesia Country Report on the Follow up to the Declaration of Commitment on HIV/AIDS (UNGASS), Reporting Period 2008 – 2009, Jakarta, 2009. RSHS. Hasan Sadikin Hospital Bandung PITC Procedure, 2008. RSHS. Hasan Sadikin Hospital Bandung VCT Procedure, 2008. Siregar, A.Y.M., D. Komarudin, B. Leuwol, I. Afriandi, H. Djuhaeni and R. Baltussen. “Economic Aspect of HIV/AIDS Control and Injecting Drug Use in Indonesia”. Acta Medica Indonesiana, the Indonesian Journal of Internal Medicine, a Publication of the Indonesian Society of Internal Medicine, 2009, 41 (supplement1); 70 – 74. Siregar, A.Y.M., D. Komarudin, R. Wisaksana, R. van Crevel and R. Baltussen. “Costs and Outcomes of VCT Delivery Models in the Context of Scaling Up Services in Indonesia”. Tropical Medicine and International Health, 2010, 16(2): 193-99. Surdo, A. “Clinicians or Counselors? Challenges to the Scale-up of Provider-Initiated HIV Testing and Counseling”. Presented at USAID Mini-University, October 2007. Teerawattananon, Y., T. Vos, V. Tangcharoensathien and M. Mugford. “Cost-effectiveness of Models for Prevention of Vertical HIV Transmission—Voluntary Counseling and Testing and Choices of Drug Regimen. Cost Effectiveness and Resource Allocation”, 2005, 3:7;doi:10.1186/1478-7547-3-7. UNAIDS, WHO. AIDS Epidemic Update: December 2007. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organzation (WHO), 2007. UNAIDS. “The Impact of Voluntary Counselling and Testing: A Global Review and Challenges”. June 2001. Geneva, UNAIDS. Walker, D. “Cost and Cost-effectiveness of HIV/AIDS Prevention Strategies in Developing Countries: Is there an Evidence Base?” Health Policy and Planning 2003, 18 (1): 4-17. Wisaksana, R., B. Alijsahbana, R. Crevel, N. Kesumah, P. Sudjana. “Challenges in Delivering HIV-care in Indonesia: Experience from a Referral Hospital”. Acta Medica Indonesiana, the Indonesian Journal of Internal Medicine, Publication of the Indonesian Society of Internal Medicine, 2009, 41 (supplement1), 45 – 51. WHO. World Health Organization. “Guidance on Provider-initiated HIV Testing and Counseling in Health Facilities”, Switzerland, 2007. http://whqlibdoc.who.int/publications/2007/9789241595568_eng.pdf