136
| Date post: | 22-Mar-2018 |
| Category: |
Documents |
| Upload: | truongkhue |
| View: | 215 times |
| Download: | 0 times |


and symptoms

Page 3
CLINICAL PROCEDURES AND GUIDELINES
FOREWORD
This is the pocket edition of the clinical procedures and guidelines,developed for the ambulance sector of New Zealand. It is a summary ofthe comprehensive version
These clinical procedures and guidelines are for use by Wellington FreeAmbulance (WFA) personnel, with current authority to practice, whenproviding clinical care to patients on behalf of WFA. They have beendeveloped by the National Ambulance Sector Clinical Working Group(NASCWG) and are issued to individual clinical personnel by the MedicalDirector of Wellington Free Ambulance
These clinical procedures and guidelines expire at the beginning of 2016at which time they will be formally updated and reissued.They remain theintellectual property of the National Ambulance Sector Clinical WorkingGroup and may be recalled or updated at any time. Any persons otherthan WFA personnel using these clinical procedures and guidelines do soat their own risk. NASCWG and WFA will not be responsible for anyloss, damage or injury suffered by any person or persons as a result of, orarising out of, the use of these clinical procedures and guidelines bypersons other than WFA personnel
Page 4

Page 5
NASCWG members at the time of publication∙ Dr Andy Swain, Medical Director,Wellington Free Ambulance∙ Mark Bailey, Clinical Effectiveness Manager,WFA∙ Dr Alison Drewry, Director Defence Health, NZ Defence Force∙ Dr Craig Ellis, Deputy Medical Director, St John∙ Dr Tony Smith (Chair), Medical Director, St John∙ Steve Mann, Clinical Education Delivery Manager, St John
Comments and enquiriesClinical personnel should contact their appropriate Manager. Otherswishing to make formal comments or enquiries should contact
Chair of the National Ambulance Sector Clinical Working Groupc/o Ambulance New Zealand, PO Box 714,Wellington

Page 6Page 6
This is the CPG version control page. This page will be updated toindicate which pages in the CPGs have been updated and which versionis the most current
Printerd pocket edition all pages are dated March 2014
Comprehensive and electronic versions all pages should be datedDecember 2014

Page 7

Page 8

Page 9

Page 10

Page 11

Page 12

1.2 AUTHORITY TO PRACTICE
Ambulance and Defence Force personnel cannot legally supply oradminister prescription medicines to patients unless they have authorityto practice, or they are Registered Health Practitioners with this abilitydescribed within their scope of practice by their registering authority. Inaddition, services restrict the use of some items of clinical equipment andsome clinical interventions to specific personnel
Authority to practice is the granting of authorisation to a specific personto supply or administer prescription medicines to patients, or to usespecific items of clinical equipment, or to perform specific interventionsunder the oversight of the medical director. All clinical care provided topatients (beyond first aid) must comply with these clinical proceduresand guidelines. Personnel may not use these clinical procedures andguidelines without individual authority to do so
Authority to practice is granted at a specified practice level (listed onpages 14 and 15). Under each practice level is listed a delegated scope ofpractice. A delegated scope of practice defines the medicines andinterventions that designated personnel may administer or use whenproviding patient care. Ordinary interventions not formally describedwithin any delegated scope of practice can be performed by all personnel.Colour bars to the left of treatment steps in each guideline serve as areminder of the minimum practice level for that intervention.These barscorrespond to colours in the top row of the table on pages 14 and 15
Page 13

Page 14

Page 15

Page 16

Page 17

Page 18Page 18
Page 19
2.1 GENERAL PRINCIPLES OF TREATMENT
Although not listed with each section, all patients require a primary andsecondary survey with appropriate intervention as required
Unless otherwise specified, the medicine doses and fluid volumesdescribed in these guidelines are for adults and children weighing 50kg ormore. See the paediatric pages for paediatric dosing
All medicines have universal contraindications and as such they are notrepeatedly listed with each individual medicine. These are:
∙ Known allergy to the medicine or its constituents∙ Pregnancy (particularly first trimester) is a relative contraindication
for most medicines and as such they should not be administeredunless there is a very strong indication to do so
Specific contraindications are listed in section 11 of this book, whilecautions are listed in the comprehensive edition. Most sections containalerts to some (generally not all) contraindications and cautions to assistpersonnel
With the exception of sodium bicarbonate, drugs that are indicated forIV administration may be administered IO if such access is available

Page 20
2.2 OXYGEN ADMINISTRATION
Few sections contain specific instructions on oxygen and clinicaljudgement is required. Oxygen does not necessarily provide benefit andshould usually only be given if the patient has:
• An SpO2 less than 94% on air (exception – see CORD section) or• Airway obstruction or• Respiratory distress (exception – see CORD section) or• Shock or• Inability to obey commands from TBI or• Smoke inhalation
Use the simplest device and lowest flow rates to achieve the desiredSpO2. If pulse oximetry is unreliable or unavailable, give oxygen asappropriate based on the above bullet points
The oxygen flow rates to be used are:• Nasal prongs 1-4 L/min• Simple mask 6-8 L/min• Nebulised mask 8 L/min• Reservoir mask 10-15 L/min• Manual ventilation bag 10-15 L/min

Page 21

Page 22Page 22

Page 23

Page 24

Page 25

2.4 STATUS CODES
Status codes are a numerical means of describing an assessmentof the severity of a patient’s condition
They are qualitative, require clinical judgement and are allocated topatients after taking into account their illness or injuries, their vitalsigns and the potential threat to their life
They are not altered by the mechanism of injury, the physicalenvironment (e.g. trapped or not trapped) or the age of the patient
Status Condition Triage tagStatus zero Dead Black/whiteStatus one Immediate threat to life RedStatus two Potential threat to life OrangeStatus three Unlikely threat to life GreenStatus four No threat to life Green
Page 26

Page 27

Page 28

Page 29

Page 30

Page 31

Page 32

Page 33

Page 34

Page 35

Page 36

Page 37

Page 38

Page 39

Page 40

Page 41

Page 42

Page 43

Page 44

Page 45

Page 46

Page 47

Page 48

Page 49

Page 50

Page 51

Page 52

Page 53

Page 54

Page 55

Page 56

Page 57

Page 58

Page 59

Page 60

Page 61
Page 62

Page 63

Page 64

Page 65

Page 66

Page 67

Page 68

Page 69

Page 70

Page 71

Page 72

Page 73

Page 74

Page 75

Page 76

Page 77

Page 78

Page 79

Page 80

Page 81Page 81

Page 82

Page 83Page 83

Page 84

Page 85

Page 86

Page 87

Page 88

All patients with head trauma causing loss of consciousness should beadvised that they need to be transported to the emergency departmentfor observation.Where a patient refuses transport the following adviceshould be given to them and, wherever possible, to a responsibleaccompanying adult
Problems could arise within the first 24 hours. Someone needs to bewith you during that time.You, or the person looking after you, mustphone 111 and ask for an ambulance if any of the following develop
•You have a headache that gets worse•You are drowsy or difficult to wake up•You have difficulty recognising people or places•You have any vomiting•You behave unusually or seem confused•You have seizures or fits•You have weak arms or legs, or are unsteady on your feet•You have slurred speech
Page 89

Page 90

Page 91

Page 92

Page 93

Page 94

Page 95Page 95

Page 96

Page 97

Page 98

Page 99Page 99

Page 100

Page 101

Page 102

Page 103

Page 104

Page 105

Weight (kg)• Under 1 year old 5
• 1 10 years old 2 × (age in years + 4)
• 11 14 years old 3 × age in years
For age 1 year and older, round patient weight (known or calculated) tothe nearest 10kg before using the tables in each CPG or on the followingpages
• Newborn to 1 year 3 4 (uncuffed), 2 3 (cuffed)
• 1 year and over (age in years / 4) + 4 (uncuffed)
Endotracheal tube Length at Lips (LAL) (cm)• Newborn 6 + weight in kg
• Under 1 year ETT size × 3
• 1 year and over (age in years / 2) + 12
Endotracheal tube (ETT) size
10.1 PAEDIATRIC EQUIPMENT AND DRUG DOSE
For children, the dose of drugs, defibrillation energy, and fluidtherapy are based on body weight. If the body weight is unknown,it can be estimated from the child’s age using the followingAdvanced Paediatric Life Support (APLS) formulae
Page 106
(age in years / 4) + 3.5 (cuffed)

Notes• These formulae are a guide only, individual children may be lighter or
heavier than predicted by the APLS formulae.They may also requirea different ETT size, LAL, or defibrillation energy than that derivedfrom the formulae
• If drugs are administered, or a paediatric patient is intubated ordefibrillated, the patient's estimated/calculated weight must berecorded together with drug dose(s), ETT size, LAL, energy settings,etc.
• All children greater than 14 years or greater than 45kg can be givenadult doses
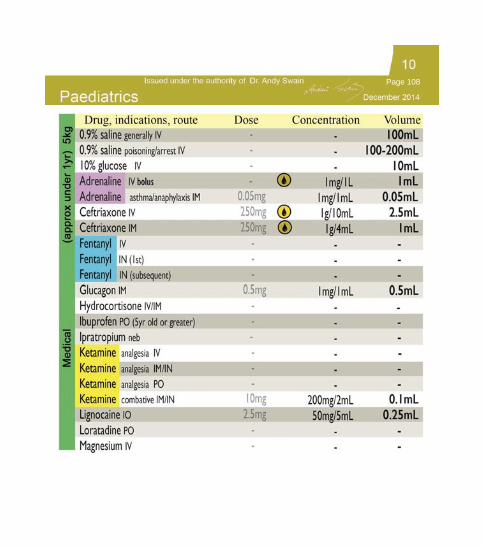
PAEDIATRIC DRUG DOSES
The following pages contain tables of paediatric drug doses.These tablesare provided to assist you in applying your knowledge and training.Theycannot incorporate all administration information, so a strong knowledgeof each drug is still required.They indicate the calculated dose for a givenpatient weight, the concentration of solution that should be obtained, andthe volume that should be administered from that solution. For amore detailed explanation consult the comprehensive edition
Drug administration errors have occurred where paramedics haveadminstered a listed volume "straight" rather than from the specifiedconcentration of solution. Entries that are highlighted red are drugs thatare frequently involved in administration errors
Page 107
Page 108

Page 109

Page 110

Page 111

Page 112

Page 113

Page 114

Page 115

Page 116

Page 117

Page 118
10.2 OTHER PAEDIATRIC GUIDES
Page 118
December 2014

Page 119
WongBaker FACES pain scale
No hurt Hurts Hurts Hurts Hurts Hurtslittle bit little more even more whole lot worst
Page 119

Amiodarone• Known hypersensitivity or allergy to iodine• Pregnancy or lactation
Aspirin• Known hypersensitivity or allergy to salicylates• Recent gastric bleeding• Pregnancy• Children under 12 years old
The following is a summary of drug contraindications for quickreference. For the complete standing orders, refer to thecomprehensive edition of the CPGs
ALL DRUGS: allergy and 1st trimester pregnancyDrugs with no additional cautions are not listed
Ceftriaxone• Known hypersensitivity or allergy to cephalosporins• Consult if hypersensitivity or allergy to penicillin• Consult for children less than 1 year old
Page 120
Clopidogrel• Severe liver impairment• Active pathological bleeding (e.g. peptic ulcer or intracranial haemorrhage)• Breast feeding
Entonox• Decreased LOC• Suspected pneumothorax• Diagnosed bowel obstruction• Scuba diving in the last 24hrs
Fentanyl• Children under 1yr age• Unable to obey commands• Respiratory depression (includes active or poorly controlled asthma)• Premature labour• Myasthenia gravis

Glucagon• Insulin- or glucagon-growing tumours
Glyceryl trinitrate (GTN)• Systolic BP less than 100mmHg• HR less than 40 or greater than 150bpm• Erectile dysfunction medications
Heparin• Currently taking anti-coagulants
Hydrocortisone• Premature infants• Systemic fungal infections
Page 121
ALL DRUGS: allergy and 1st trimester pregnancy
Ibuprofen• Known hypersensitivity to ibuprofen and aspirin or other nonsteroidal anti-inflammatory drugs• On anticoagulants i.e. warfarin• Peptic ulcer or hiatus hernia• Renal failure• Third trimester pregnancy
Ipratropium bromide• Known hypersensitivity or allergy to atropine

Ketamine• Patients
where
a
significant elevation of blood pressure would constitute a risk For analgesia• Children under 1yr age• Unable to obey commands• Has active psychosis• Cardiac chest pain
Lignocaine• Known
hypersensitivity
or allergy to local anaesthetics• Localised inflammation or sepsis at the injection site, or septicaemia• Heart block (sinoatrial, atrioventricular, intraventricular)• Serious CNS disease (meningitis, cranial haemorrhage)
Loratadine• Pregnant
or
breast
feeding• Children under 1yr age• Taking erythromycin or roxithromycin - check QTc less than 500milliseconds
• Known
hypermagnesaemia
Page 122
ALL DRUGS: allergy and 1st trimester pregnancy
Midazolam• Hypersensitivity
or
allergy
to benzodiazepines• GCS<10 for the agitated patient• Airway problems• Myasthenia gravis
Magnesium sulphate

Morphine sulphate• Acute severe asthma/CORD Respiratory compromise or depression (especially with cyanosis)• Premature infants or during labour for the delivery of premature infants
Naloxone• Newborns born to opiate- abusers (may precipitate withdrawal
Ondansetron• Less than 1year old• Known contenital long QT
Oxygen• CORD - more than 88% SpO2
Oxytocin• Prolonged QT segment
Paracetamol• Liver impairment• Any drug overdose• If patient has taken any other medication containing paracetamol within past 4hrs
Prednisone• Active peptic ulcer
Page 123
ALL DRUGS: allergy and 1st trimester pregnancy
Suxamethonium• History or family history of malignant hyperthermia• Paraplegia/quadriplegia• Muscle disorder• Hyperkalaemia• Significant healing burns

Tenecteplase• Age > 75 years• Stroke or head injury within last 6 months• Previous major surgery or GI bleed within the last 2 months• Recent trauma or surgery of any form within the last 2 weeks (including extensive CPR)• Currently taking anticoagulant• Severe uncontrolled hypertension (systolic BP greater than 200mmHg)• Confirmed peptic ulcer disease with symptoms in the last 3 months
Page 124
ALL DRUGS: allergy and 1st trimester pregnancy
Ticagrelor• History of intracranial haemorrhage• Active bleeding• Severe hepatic impairment
Tramadol• Known hypersensitivity to tramadol or opioids• MAOI inhibitors within last 14 days• Epilepsy• Acute Intoxication
Tranexamic Acid• Subarachnoid haemorrhage• Active intravascular clotting e.g. DVT

Page 125




Page R-3

Page R-4

Page R-5

Page R-6

Page R-7

Page R-8

Page R-9

Page R-1 0

















