98
ANESTHESIA FOR OPHTHALMIC SURGERY AND COMPLICATIONS SHADAB
| Date post: | 07-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | shadab-kamal |
| View: | 156 times |
| Download: | 7 times |
ANESTHESIA FOR OPHTHALMIC SURGERY AND COMPLICATIONS
SHADAB

INTRODUCTION
Anesthesia for EYE surgery presents many unique challenges.
In addition to possessing technical expertise, the anesthesiologist must have detailed knowledge of ocular anatomy, physiology, and pharmacology.
INTRODUCTION Ocular anatomy Physiology of intraocular pressure and
effect of anesthetic drug on it, Systemic effects of ophthalmic drugs Technique of anaesthesia: advantage
and limitations Pre op evaluation General anaesthesia Complications Oculocardiac reflex and other reflex Specific considerations for eye
surgeries
Ophthalmic SurgeryChallenges for the anaesthesiologist
are Akinesia Analgesia Minimal Bleeding Awareness of drug interactions Regulation of intraocular pressure Prevention of the oculocardiac
reflex Management of oculocardiac reflex Control of intraocular gas
expansion Smooth emergence
Ophthalmic Surgery
Why these patient have a particular challenge to the anesthesiologist?
The combination of a full stomach and an
open-globe injury, both of which
conditions are problematic for the
anesthesiologist.
Any drug or manoeuvre that raises intra-
ocular pressure (lOP) can cause
extrusion of the vitreous humor and loss
of vision.

Ocular Anatomy

APPLIED ANATOMY OF THE ORBIT

APPLIED ANATOMY OF THE ORBIT
The orbit
♦ Four-sided bony pyramid
♦ Base pointing anteriorly
♦ Apex posteromedialiy.
♦ The medial wall of the right and left orbits are parallel to each other
♦ The mean distance from the inferior orbital margin to The apex is 55 mm. (This has important implications when injections are made into the orbit.)
APPLIED ANATOMY OF THE ORBIT
Movement of the globe is controlled by
the six extra-ocular muscles.
The eye is hollow sphere with a rigid
wall.
Intraocular pressure 12—20 mmHg
Ophthalmic surgery can be intraocular
or extraocular procedures, each has
different anaesthetic requirements.
APPLIED ANATOMY OF THE ORBIT
Squeezing and closing of the eyelids
These are controlled by the zygomatic
branch of the facial nerve (VII), which
supplies the motor innervation to the
orbicularis oculi muscle.
The facial nerve also supplies
secretomotor parasympathetic fibres to
the lacrimal glands, and glands of the
nasal and palatine mucosa.

APPLIED ANATOMY OF THE ORBIT
How is aqueous humor formed and eliminated?
a clear fluid that occupies the anterior and posterior chambers of the eye.
Its total volume is 0.3 ml. produced primarily in the posterior chamber circulates through the pupil to the anterior
chamber, passes through the Schlemmn’s canal.
drains into the episcleral veins and finally into the cavernous sinus or jugular venous sinus.
Physiology of IntraocuIar Pressure

Physiology of IntraocuIar Pressure
The eye is hollow sphere with a rigid wall.
intraocular pressure 12—20 mm Hg
If the contents of the sphere increase, the intraocular pressure rise.
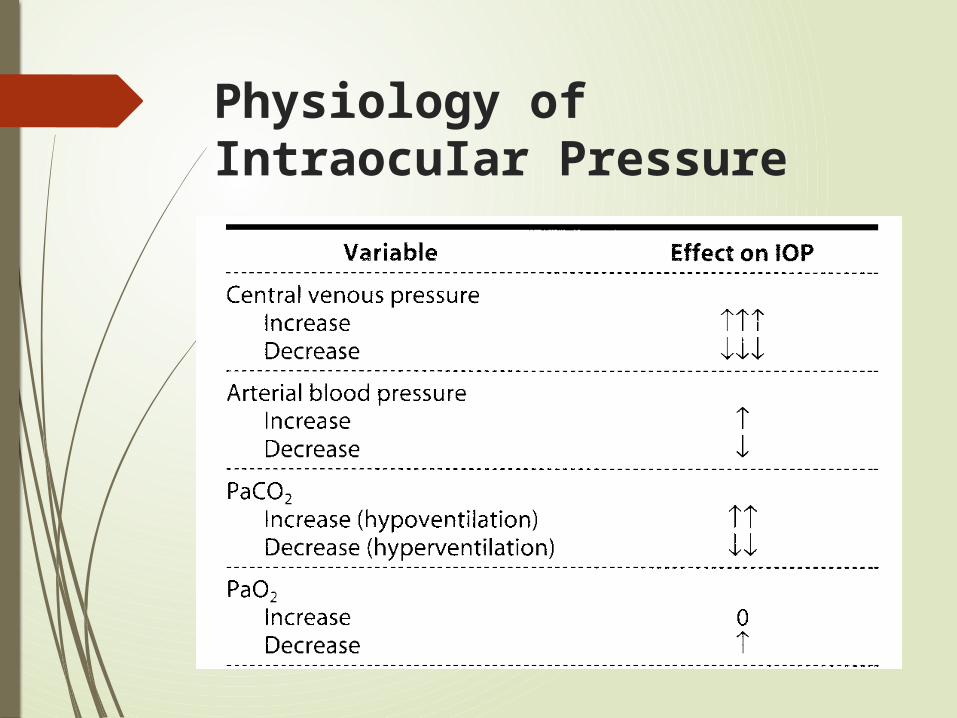
Physiology of IntraocuIar Pressure
Physiology of IntraocuIar Pressure
Any anaesthetic event that alters these parameters can affect intraocular pressure
Laryngoscopy Intubation Airway obstruction Coughing Trendelenburg position

Effect of Anesthetic Drugson intraocuIar Pressure
Effect of Anesthetic Drugs
Most anesthetic drugs either lower or have no effect on intraocular pressure

Inhaled Anesthetics
Inhalational anesthetics decrease intraocular pressure in proportion to the depth of anesthesia.
The decrease has multiple causes:
1. A drop in blood pressure reduces choroidal volume
2. Relaxation of the extraocular muscles lowers wall tension
3. pupillary constriction facilitates aqueous outflow.
Intravenous anesthetics
Intravenous anesthetics drugs
decrease intraocular pressure
Exception is ketamine, which usually
raises arterial blood pressure and
does not relax extraocular muscles.
Muscle relaxants
Succinylcholine increases intraocular
pressure by 5—10 mm Hg for 5—10
minutes principally through
prolonged contracture of the
extraocular muscles.
Nondepolarizing muscle relaxants do
not increase intraocular pressure.

The effect of anesthetic agents on intraocular pressure (lOP).

SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS

SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Topical ophthalmic drugs can be absorbed through the conjunctiva, or they drain through the nasolacrimal duct and be absorbed through the nasal mucosa.
Usage of topical medications can have implications for the anesthesiologist.

SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Atropine Used to produce mydriasis and
cyclopiegia. The 1% solution contains 0.2 to 0.5
mg of atropine per drop. Systemic reactions, include
tachycardia, flushing, thirst, dry skin, and agitation.
Atropine is contraindicated in closed-angle glaucoma.
SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Scopolamine One drop of the 0.5% solution has
0.2 mg of scopolamine. CNS excitement can be treated with
physostigmine, 0.015 mg/kg IV, repeated one or two times in a 15- minute period.
It is contraindicated in closed-angle glaucoma.

SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Phenylephrine Hydrochloride Phenylephrine hydrochloride is used
to produce capillary decongestion and pupillary dilatation.
Applied to the cornea, it can cause palpitations, nervousness, tachycardia, headache, nausea and vomiting, severe hypertension, reflex bradycardia, and subarachnoid hemorrhage.
Solutions of 2.5%, 5%, and 10% (6.25 mg phenylephrine per drop) are available.

SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Epinephrine Topical 2% epinephrine will decrease
aqueous secretion, improve outflow, and lower intraocular pressure in open-angie glaucoma.
Side-effects include hypertension, palpitations, fainting, pallor, and tachycardia.
The effects last about 15 minutes. One drop of 2% solution contains 0.5
to 1 mg of epinephrine.

SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Timolol Maleate (Tinwptic)
Timolol maleate is a beta-blocker used in
the treatment of chronic glaucoma.
Side- effects include light-headedness,
fatigue, disorientation, depressed CNS
function, and exacerbation of asthma.
Bradycardia, bronchospasm, and
potentiation of systemic beta-blockers can
occur.
SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Acetylcholine
Acetylcholine can be injected
intraoperatively into the anterior
chamber to produce miosis.
Side-effects are due to its
parasympathetic action they include
hypotension, bradycardia, and
bronchospasm.
SYSTEMIC EFFECTSOF OPHTHALMIC DRUGS
Echothiophate Iodide (Phosplzolfne Iodide) A cholinesterase inhibitor,
echothiophate iodide is used as a miotic agent.
prolong the effect of both succinyicholine and ester-type local anesthetics.
Levels of pseudocholinesterase decrease by 80% after 2 weeks on the drug.
Succinyicholine and ester-type local anesthetics should be avoided.

Anesthesia for Ophthalamic Surgery

TECHNIQUES OF ANESTHESIA
Facial nerve block
Retrobulbar block
Peribulbar block
Sub Tenon block
Topical anesthesia
General anesthesia
GENERAL VERSUS LOCAL ANESTHESIA
The choice of general versus local anesthesia is made on the basis of the duration of the surgery, the relative risks and benefits of
each technique for the patient, patient preference.
Neither technique has been shown to be safer.
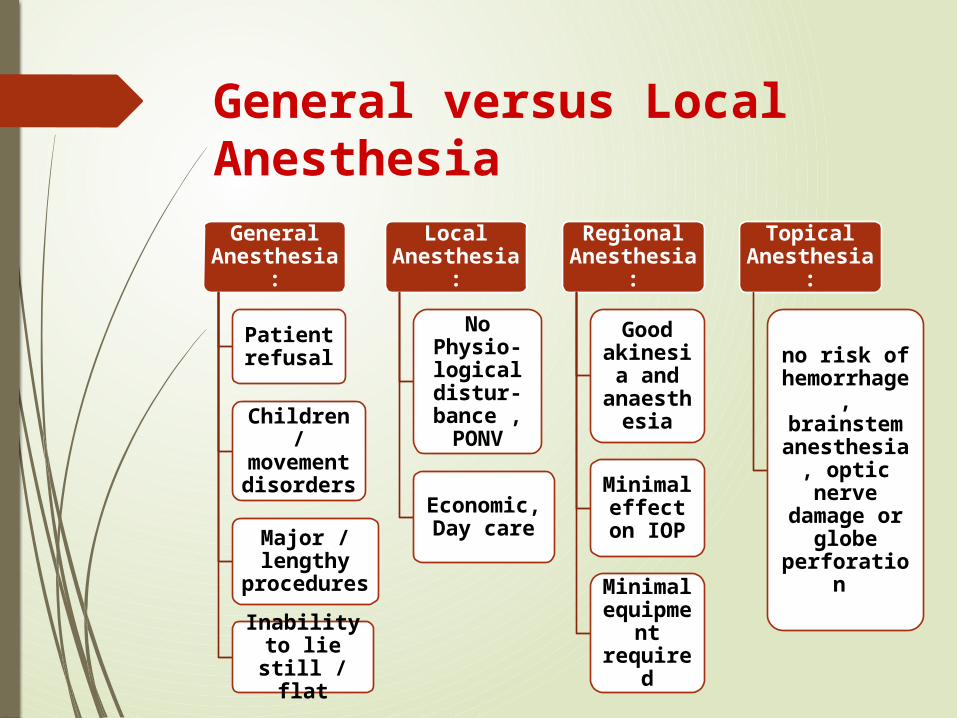
General versus Local AnesthesiaGeneral
Anesthesia:
Patient refusal
Children / movemen
t disorders
Major / lengthy
procedures
Inability to lie still /
flat
Local Anesthesia
:
No Physio-logical distur-bance , PONV
Economic, Day care
Regional Anesthesia
:
Good akinesia
and anaesth
esia
Minimal effect on
IOP
Minimal equipme
nt required
Topical Anesthesia
:
no risk of hemorrhage, brainstem anesthesia, optic nerve damage or
globe perforation

LIMITATIONS…
General Anesthesia:
Eye surgery necessitates
positioning the anesthesiologist away from the
patient’s airway
Patients at extremes of age
Pediatric patients : associated congenital
disorders (eg: rubella syndrome, Down syndrome).Co-morbidity in
elderly: esp. Diabetes,
hypertension and coronary artery
diseaseOphthalmic
drugs
Local Anesthesia:
Complications , Allergy to drug
Skill of anaesthetist
Shortness of breath on
lying down, chronic cough
Parkinson’s disease
Eye Trauma
Topical Anesthesia:
lack of eye
akinesis
treatment of
uncomplicated
cataracts only
PREOPERATIVE EVALUATION Eye surgery patients are a high-risk
group Extremes of Age Other risk factors, such as diabetes,
hypertension, and atherosclerosis The anesthesiologist's goal is to
prepare the patient to present an acceptable risk at surgery.
Acceptable risk is determined by the medical care team with the informed consent of the patient.

HISTORY
Previous hospitalizations and surgical procedures Allergies and drug sensitivities
A current list of medications Patient factors that could
influence anesthetic management include dementia, deafness, language difficulty, restless legs syndrome, obstructive sleep apnea, tremors, dizziness, and claustrophobia.
PHYSICAL EXAMINATIONS
Check for signs of major cardiac or pulmonary decompensation.
Particular attention should be paid to positioning issues, such as severe scoliosis or orthopnea.
CARDIOVASCULAR EVALUATION
The American Heart Association and American College of Cardiology published guidelines for perioperative cardiovascular evaluation for noncardiac surgery.
Ophthalmic procedures such as cataract extraction are specifically identified as low-risk procedures.
For these procedures, evaluation is focused on patients with major clinical predictors of risk.

HYPERTENSION
Severe hypertension may lead to perioperative complications.
It would be prudent to reschedule elective procedures in patients with sustained stage 3 hypertension until after 2 weeks of antihypertensive therapy.

PULMONARY CONSIDERATIONS
Ophthalmic procedures generally require that the patient lie flat comfortably and quietly.
Preoperative risk reduction strategies include cessation of cigarette smoking, treatment of airflow obstruction with bronchodilators or steroids, and administration of antibiotics for respiratory infections.
Patients should be assessed for sleep apnea. Intravenous sedation is often contraindicated in these patients.

ENDOCRINE CONSIDERATIONS
Severe hyperglycemia and hypoglycemia should be avoided.
A fasting blood glucose should be checked preoperatively.
Insulin therapy should be used, if needed, to maintain blood glucose at 150 to 250 mg/dL.
The potential for autonomic neuropathy needs to be considered, especially when elevating the patient from the supine position.
ENDOCRINE CONSIDERATIONS
Patients on long-term steroid therapy generally do not require “stress-dose” steroid treatment for ophthalmic surgery.
The patient should be given his or her normal steroid dose on the day of surgery.
Unexpected hypotension, fatigue, and nausea may be signs of a patient who needs additional steroid
ANTICOAGULATION
Perioperative management of anticoagulants involves weighing the relative risks of thrombotic against possible hemorrhagic complications. That depends on the following: The degree of anticoagulation. The hemorrhagic potential of the
surgical procedure as in orbital and oculoplastic surgery; of intermediate probability in vitreoretinal, glaucoma, and corneal transplant surgery; and least likely in cataract surgery.
INVESTIGATIONS
Electrocardiogram: New chest pain, decreased exercise tolerance, palpitations, near-syncope, fatigue, or dyspnea. Tachycardia, bradycardia, or irregular pulse on examination.
Serum electrolytes: History of severe vomiting or diarrhea, poor oral intake, changes in diuretic management, or arrhythmia. Critical results: Sodium less than 120 mEq/L or greater than 158 mEq/L. Potassium less than 2.8 mEq/L or greater than 6.2 mEq/L.
INVESTIGATIONS
Urea nitrogen: Signs or symptoms of renal decompensation. Critical result: Greater than 104 mg/dL.
Serum glucose: Polydipsia, polyuria, or weight loss. Critical results: Less than 46 mg/dL or greater than 484 mg/dL.
Hematocrit/hemoglobin: History of bleeding, poor oral intake, fatigue, decreased exercise tolerance, or tachycardia. Critical results: Hematocrit less than 18% or greater than 61%. Hemoglobin less than 6.6 mg/dL or greater than 19.9 mg/dL

GENERAL ANESTHESIA
PREMEDICATION
An effective antiemetic should be used
to decrease PONV. Eg- Ondansetron
Opioids are avoided as they contribute
to PONV.
Benzodiazepines are given.

Pretreatment regimens to control the sympathetic response to tracheal intubation:
i.v. lidocaine (1.5 mg/kg) i.v. remifentanil(0.5 to 0.1 µg/kg) i.v. fentanyl (1 to 3 µg/kg) 3 to 5
minutes before induction. i.v alfentanil (20 µg/kg) Oral clonidine (5 µg/kg) 2 hours
before induction
GENERAL ANESTHESIA
INDUCTION The choice of induction technique for
eye surgery usually depends more on
the patient’s medical problems
the patient’s eye disease
the type of surgery contemplated.
GENERAL ANESTHESIA
Intravenous agents: Propofol , Thiopental and Etomidate.
Volatile Agents: can be used, minimal PONV.
Coughing during intubation: avoided by a deep level of anesthesia and profound paralysis.
The IOP response: to laryngoscopy and endotracheal intubation can be blunted.
LMA: can also be used. Less changes in IOP.

AIRWAY MANAGEMENT
For measurement of intraocular pressure (IOP)- maintenance of spontaneous respiration via a facemask should be used, as intubation will raise the intraocular pressure.
Examination under anaesthesia (EUA)-spontaneous respiration through a reinforced laryngeal mask airway (LMA)
It has the advantages of reduced coughing at the end of the surgery and controlled ventilation with the use of muscle relaxants is possible.
AIRWAY MANAGEMENT
Intraocular surgery requires a still eye with low intraocular pressure and the airway is best managed by intubation with paralysis and controlled ventilation.
Access to the airway will be restricted during the surgery so it is important to secure the tracheal tube firmly.
A preformed south facing RAE tube is ideal, but this may be too long in neonates; a reinforced flexible tracheal tube (ETT) may be preferable in this situation.

GENERAL ANESTHESIA
RELAXATION- A nondepolarising muscle relaxant is
used instead of succinylcholine because the latter increases intraocular pressure.
However, the rise in IOP is small by succinylcholine than the fall caused by intravenous induction agent, and also considering risk of aspiration succinylcholine can be used in an emergency case.

MAINTENANCE
Where halothane is used there is an increased risk of dysrhythmias, particularly where eye preparations containing atropine or adrenaline are used, and in the presence of hypercapnia.
Isoflurane or sevoflurane may be preferable.
Total intravenous anaesthesia (TIVA) with propofol has advantages in reducing the risk of postoperative nausea and vomiting (PONV) since propofol has anti-emetic effects.
Remifentanil can reduce volatile requirements.

USE OF NITROUS OXIDE
The use of nitrous oxide in eye surgery is limited by two factors.
Increase the risk of PONV, and in ophthalmic procedures there is a high incidence of PONV
Secondly, nitrous oxide diffuses from the blood into gas filled spaces in the body.
It should be avoided in vitreoretinal detachment surgery where intraocular gas bubbles of sulphur hexachloride or perfluropropane are introduced into the eye to tamponade detached surfaces.

Effect of intraocular gas expansion
If nitrous oxide is used for a patient who has had recent vitreoretinal surgery (the bubble may last several weeks), or if it is commenced mid procedure, it can cause a significant rise in intraocular pressure with resultant ischaemic damage.
Alternatively, if nitrous oxide was used from the start of the anaesthetic, prior to placement of the gas bubble, it will diffuse out of the bubble on completion of the anaesthetic, and the bubble will shrink and risk re-detachment
Intraocular gas expansion
Prevention: discontinue nitrous 15-20 mins
prior to injection. Avoid nitrous oxide 5 days after air
and 10 days after sulfur hexachloride injection.
In case of perfluoropropane avoid nitrous for atleast a month, or until the bubble is resorbed.

GENERAL ANESTHESIA
MONITORING & MAINTENANCE Eye surgery necessitates positioning
the anesthesiologist away from the patient’s airway, making pulse oximetry mandatory for all ophthalmologic procedures.
Continuous monitoring for breathing-circuit disconnections or unintentional extubation is also crucial.
The possibility of kinking and obstruction of the endotracheal tube can be minimised by using a reinforced or preformed right-angle endotracheal tube.

GENERAL ANESTHESIA
MONITORING & MAINTENANCE The possibility of dysrhythmias caused by
the oculocardiac reflex increases the importance of constantly scrutinizing the electrocardiograph.
most pediatric surgery, infant body temperature often rises during ophthalmic surgen’ because of head- to-toe draping and insignificant body-surface exposure.
End-tidal CO2 analysis helps differentiate this from malignant hyperthermia.
GENERAL ANESTHESIA
EXTUBATION & EMERGENCE A smooth emergence from general
anesthesia Deep level of anesthesia. Intravenous lidocaine (1.5 mg/kg)
prior to extubation. Severe postoperative pain is
unusual.

COMPLICATIONS
COMPLICATIONS OF REGIONAL ANAESTHESIA
Retrobulbar hemorrhage
Stimulation of OC reflex
Puncture of posterior globe
IV injection of LA brainstem anesthesia - (delayed
onset LOC and resp. depression)
Optic nerve trauma.

RETROBULBAR HAEMORRHAGE
Venous hemorrhages - spread slower
Arterial hemorrhages - rapid and taut orbital swelling with marked proptosis.
incidence-1% to 3%. Clinical suspicion: stained
conjunctiva and a proptotic globe
RETROBULBAR HAEMORRHAGE
MANAGEMENT Determine IOP Ophthalmoscopy
TREATMENT reduce orbital compartment
pressure, thereby IOP Osmotic diuretics Lateral canthotomy Orbital decompression
OCULOCARDIAC REFLEX
The Oculocardiac Reflex(OCR) is manifested by Bradycardia Bigeminy Ectopics Nodal rhythm Atrioventricular block Cardiac arrest
OCULOCARDIAC REFLEX
Caused By: Traction on the extraocular muscles
(medial rectus) Ocular manipulation Manual pressure on the globe
The OCR is seen during: Eye muscle surgery Detached retina repair Enucleation

OCULOCARDIAC REFLEX
Factors contributing to the incidence of the oculocardiac reflex:
Preoperative anxiety
Hypoxia
Hypercarbia
Increased vagal tone owing to age
OCULOCARDIAC REFLEX
Management stop stimulation by the surgeon
before the arrhythmia progresses to sinus arrest
Atropine (0.01 mg/kg IV) local injection of lidocaine near the
eye muscle
Ensure depth of general anesthesia normocapnia surgical manipulation is gentle.

OCULORESPIRATORY REFLEX
may cause shallow breathing, reduced respiratory rate and even full respiratory arrest.
Trigemino vagal reflex- connection exists between the trigeminal sensory nucleus and the pneumotactic centre in the pons and medullary respiratory centre.
Commonly seen in strabismus surgery
Atropine has no effect.

OCULOEMETIC REFLEX
It is likely responsible for the high
incidence of vomiting after squint surgery (60-90%).
Trigemino-vagal reflex with traction on the extraocular muscles stimulating the afferent arc.
Antiemetics may reduce the incidence, a regional block technique provides the best prophylaxis
BRAINSTEM ANAESTHESIA Amaurosis
Gaze Palsy (Ductional Defects),
Apnea Shivering Tachycardia and
Hypertension Dysphagia Loss Of
Consciousness Cardiac Arrest

BRAINSTEM ANAESTHESIA The onset of symptoms -delayed 2
to 40 minutes after injection.
Management: Early and prompt treatment 100% oxygen maintenance of vital signs tracheal intubation and controlled
ventilation

OCULAR PENETRATION AND PERFORATION
most common in the myopic, elongated globes.
Myopics with staphyloma. associated with the use of large,
dull needles. a sensation of "poking through
”during the placement of the needle.
sudden appearance of hypotony, vitreous hemorrhage or a diminished red reflex

OCULAR PENETRATION AND PERFORATION
Diagnosis -Indirect fundoscopy
The most common sequelae- Retinal detachment
Appropriate retinal surgery-to prevent the loss of vision.

FACIAL NERVE BLOCK COMPLICATIONS
Blocked at several points after exiting from the base of the skull from the stylomastoid foramen
Nadbath block, O'Brien procedure, Atkinson procedure
Disturbances of swallowing and respiratory difficulties
Horner's syndrome permanent facial nerve paralysis-longer
needles and hyaluronidase use of a single injection of a large
volume of LA

COMPLICATIONS ASSOCIATED WITH GENERAL ANAESTHESIA
PONV
Increase in IOP-extrusion of intraocular contents
Intraocular gas expansion
Pulmonary embolism
POST OPERATIVE NAUSEA AND VOMITING
Most common complication associated with outpatiet
The incidence in patients undergoing strabismus surgery -85%.
MANAGEMENT Metoclopromide i.v (10 mg) 5HT3 antagonists Dexamethasone i.v

Pulmonary Embolus
chief cause of postoperative ophthalmic surgery death
particularly a problem with long procedures (retinal and oculoplastic surgery) in the elderly.
from a leg deep venous thrombosis
Pneumatic leg compression devices

INTRAOCULAR GAS EXPANSION
Intravitreal air/SF6 injection: to flatten a detached retina and allow anatomically correct healing
Nitrous oxide:expansion of air bubble and rise in IOP
Prevention: discontinue nitrous 15-20 mins prior to injection
CONTROL OF INTRAOCULAR PRESSURE
Management of anesthesia for ophthalmic surgery requires control of IOP before, during, and after the procedure
Any anesthetic event that alters the following parameters can affect intraocular pressure laryngoscopy Intubation airway obstruction Coughing Trendelenburg position

Strategies to Prevent Increases in Intraocular PressureAvoid direct pressure on the globe
Patch eye with Fox shield
No retrobulbar or peribulbar injections
Avoid increases in central venous pressure
Prevent coughing during induction and intubation
deep level of anesthesia and relaxation
Avoid head-down positions
Extubate deeply asleep
Avoid pharmacological agents that increase IOP
Succinylcholine
Ketamine (?)

Specific Clinical Situations and Complications

Penetrating Eye Injuries
Balancing the need to prevent aspiration of gastric contents…
and prevention of sudden significant increases in IOP.

Penetrating Eye Injuries
Strategies to Prevent Increases in Intraocular Pressure (IOP). Avoid direct pressure on the globe No retrobulbar or peribulbar injections Careful face mask technique Prevent coughing during induction and
intubation Avoid head-down positions Avoid pharmacological agents that
increase IOP - Succinylcholine, Ketamine (?)
PENETRATING EYE INJURIES
Strategies to Prevent Aspiration Pneumonia.
Premedication by Metoclopramide and Histamine H2-receptor antagonists
Nonparticulate antacids
Evacuation of gastric contents by Nasogastric tube1
Rapid-sequence induction
Cricoid pressure
A rapid-acting induction agent like Succinylcholine,1rocuronium
Avoidance of positive-pressure ventilation
Intubation as soon as possible
Extubation awake

Pediatric Eye Injuries
Regional eye anesthesia- not suitable
Topical anesthetic cream:to start an intravenous line OR
Rapid, gentle induction of anesthesia by mask (with 7% to 8% sevoflurane).

Pediatric Eye Injuries
stomach decompression-during surgery
To facilitate tolerance of the endotracheal tube and minimize bucking
1.narcotic: 10 to 20 minutes before the end of surgery
2.lidocaine (1.5 mg/kg) 5 minutes before extubation

Syringing and probing of nasolacrimal ducts
Anaesthetic considerations:
The surgical team may require placement of a topical vasoconstrictor onto the child’s nasal mucosa.
Hypotensive anaesthesia may be required to reduce bleeding.
The airway should be protected from blood, ideally with a throat pack, and the nasopharynx should be adequately suctioned out before extubation.
Opioids may be required for analgesia for this procedure.
The use of antimicrobial prophylaxis for those at risk of infective endocarditis is no longer routinely recommended for this procedure

STRABISMUS SURGERY
Problem the possible increased risk of malignant
hyperthermia the high incidence (PONV) the likelihood of an OCR
Solution avoid succinylcholine and halothane i.v lidocaine (1.5 mg/kg) low-dose ondansetron (50 µg/kg) dexamethasone (150 µg/kg) regimen
STRABISMUS SURGERY
Induction technique, method of airway control and choice of ventilation according to the preference of the anaesthetist.
Maintenance of anaesthesia is usually achieved with a volatile anaesthetic agent and air;
The use of total intravenous anaesthesia (TIVA) has been shown to reduce PONV.
Consider atropine 20mcg/kg IV or glycopyrolate 10mcg/kg IV as high incidence of oculocardiac reflex.
STRABISMUS SURGERY PONV is common postoperatively, up
to 50 – 75%. Giving two anti-emetic agents such
as ondansetron 0.1 mg/kg IV and dexamethasone 0.1-0.2 mg/kg IV can reduce this to 10%.
Ideally extubate in deep plane. Analgesia should include topical
tetracaine or oxybuprocaine, NSAIDS such as ibuprofen or diclofenac and paracetamol, unless contraindicated.
STRABISMUS SURGERY
Intraoperative opioids should be avoided due to the high incidence of PONV, but where necessary, consider the use of fentanyl.
A peribulbar block is effective for analgesic requirements and reduces PONV, possibly by blocking the ophthalmic division of the trigeminal nerve that passes to the vomiting centre in the medulla.
A sub-Tenon block performed intraoperatively by the surgeon can be very effective for analgesia.
VITREORETINAL SURGERY
Avoid nitrous oxide if an intraocular gas bubble is used.
Avoid nitrous oxide in patients who have had an intraocular bubble placed for several weeks after the procedure.
Controlled ventilation and paralysis should be considered for maintaining a still eye and avoiding raised IOP during the procedure.

VITREORETINAL SURGERY
This procedure is painful and analgesia including opioids should be considered.
Anti-emesis should be used routinely
Avoid raised IOP during extubation – extubate deep.
CONCLUSION
Anesthesia for eye surgery posses unique challenges.
Knowledge of ocular anatomy is important to prevent retrobulbar hemorrhage and other complications.
With intraocular procedures, profound akinesia and meticulous control of IOP are requisite.
However, with extraocular surgery, the significance of IOP fades, whereas concern about elicitation of the oculocardiac reflex assumes prominence.
CONCLUSION
Intraocular pressure are affected by physiological factors, anaesthetic drugs and technique. The regulation of IOP is important as increase in it can cause extrusion of the vitreous humor and loss of vision.
Ophthalmic drugs may significantly alter the patient’s reaction to anesthesia.
Regardless of the technique, ventilation and oxygenation must be monitored, and equipment to provide positive pressure ventilation must be immediately available .
CONCLUSION Goal of general anaesthesia is to
provide: Smooth intubation, Stable IOP, Avoidance of severe oculocardiac reflexes, A motionless field and Smooth emergence
The complications of ophthalmic anesthesia are rare and can be both vision- and life-threatening.
Complications involving the intraocular expansion of gas bubbles can be avoided by discontinuing nitrous oxide at least 15 min prior to the injection of air or SF6, or by avoiding the use of nitrous oxide entirely .











![Ophthalmic Complications of Bariatric Surgery · 2017-08-19 · ophthalmic complications have already occurred in patients after bariatric surgery [11, 13, 14]. Symptomatic vitamin](https://static.documents.pub/doc/80x56/5fab819e32d14352ae428938/ophthalmic-complications-of-bariatric-surgery-2017-08-19-ophthalmic-complications.jpg)






