November I949 GARDNER: Angiocardiography 553 yet there may be no radiological evidence of the site and size of the affected area. Even if a shadow is seen, it is usually ill-defined, and in the single posterior view, which is usually all that is available, there is no evidence of a pyramidal shape. If it is as small as i cm. it may be more or less circular, but when larger its ill-defined margins are often partly masked by a superadded pleural effusion. When studying a skiagram of the lungs in a patient with cardiac disease, it must not be for- gotten that other pathological conditions may co- exist. For instance, a bronchial neoplasm may arise in a patient with long-standing, but well. compensated, mitral stenosis; while ordinary inflanmmatory conditions may occur in the lungs independently of the cardiac lesion. A coal miner with pneumonokoniosis may develop mitral stenosis, in which case it may be difficult to differentiate the shadows of the pneumonokoniosis from those of a possible haemosiderosis. It is therefore essential to consider the X-ray appear- ances from a broad angle of general medicine. BIBLIOGRAPHY BING, R. J. (I949), Amer. Heart. J., 38, I. BROCK, R. C. (I949), Brit. Med. 7., 2, 399. DAVIES, C. E., and STEINER, R. E. (I949), Brit. Heart J., Ix, 126. HODGES, P. C., and EYSTER, J. A. E. (1926), Arch. Int. Med., 706. HODGES, P. C., EYSTER, J. A. E., and BOURNE, G. (I949), 'An Introduction to Cardiology,' London. McGREGOR, M. (I949), Brit. .7. Radiol., 22, 459. ROESLER, H. (I943), ' Clinical Roentgenology of the Cardio- Vascular System.' Illinois. SIMON, G. (I939), Proc. Roy. Soc. Med., 23, 1157. SMITH, K. SHIRLEY, and WOOD, F. G. (I949), Brit. Heart Y., 1I, 257. ANGIOCARDIOGRAPHY By FRANCES GARDNER, M.D., M.R.C.P. From the Cardiac Department of the Royal Free Hospital Angiocardiography is now an established diagnostic procedure in the fields of thoracic and cardiac surgery. By intravenous injection of an opaque substance combined with rapid serial radiography it is possible to study the heart chambers and great vessels during life. The method was conceived more than 20 years ago, though its application in clinical medicine is recent. Improvements in radiological technique have encouraged wider use of the procedure but the interest in the diagnosis of congenital heart disease and the advances in its treatment, are mainly responsible for modern development of this method of investigation. History In 1929 Forssman first injected an opaque substance into the living human heart. Like later workers in this field, notably Ameuille (1936), Forssman used sodium iodide for the intravenous injection. In the quantity and concentration employed this substance gave good angiograms of the pulmonary arteriat tree, but it was not suf- ficiently opaque to outline the heart chambers or the aorta. For this reason little progress was made in this method of investigation until Castellanos (I938) and his co-workers in Cuba introduced the organic iodides as the contrast medium. With 35 per cent. neoiopax these workers were able to show the right heart chambers and the aorta and its larger branches in children with cyanotic con- genital heart disease. But, because of dilution in the pulmonary circulation, satisfactory angio- cardiograms of the left heart in acyanotic conditions could not be obtained. In 1938 Robb and Steinberg prepared and used a 70 per cent. aqueous solution of the diethanol- amine salt of 3, 5-diiodo-4-pyridone-N-acetic acid for the intravenous injection. With this substance they were able to outline, first, the right heart chambers and pulmonary arteries and later the left heart and aorta. The introduction of multiple cassette-changing devices has enhanced the value of angiocardiography, but in other respects the procedure described by Robb and Steinberg is more satisfactory than any other and is in general use today. Contrast Media Diodone or diodrast, the material originally prepared by Robb and Steinberg, is still the most widely employed contrast medium in angio- Protected by copyright. on January 11, 2022 by guest. http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.25.289.553 on 1 November 1949. Downloaded from
Transcript
November I949 GARDNER: Angiocardiography 553
yet there may be no radiological evidence of thesite and size of the affected area. Even if a shadowis seen, it is usually ill-defined, and in the singleposterior view, which is usually all that is available,there is no evidence of a pyramidal shape. If it isas small as i cm. it may be more or less circular,but when larger its ill-defined margins are oftenpartly masked by a superadded pleural effusion.When studying a skiagram of the lungs in a
patient with cardiac disease, it must not be for-gotten that other pathological conditions may co-
exist. For instance, a bronchial neoplasm mayarise in a patient with long-standing, but well.compensated, mitral stenosis; while ordinaryinflanmmatory conditions may occur in the lungsindependently of the cardiac lesion. A coalminer with pneumonokoniosis may develop mitralstenosis, in which case it may be difficult todifferentiate the shadows of the pneumonokoniosisfrom those of a possible haemosiderosis. It istherefore essential to consider the X-ray appear-ances from a broad angle of general medicine.
BIBLIOGRAPHYBING, R. J. (I949), Amer. Heart. J., 38, I.BROCK, R. C. (I949), Brit. Med. 7., 2, 399.DAVIES, C. E., and STEINER, R. E. (I949), Brit. Heart J., Ix,
126.HODGES, P. C., and EYSTER, J. A. E. (1926), Arch. Int. Med.,
706.HODGES, P. C., EYSTER, J. A. E., and BOURNE, G. (I949),'An Introduction to Cardiology,' London.McGREGOR, M. (I949), Brit. .7. Radiol., 22, 459.ROESLER, H. (I943), ' Clinical Roentgenology of the Cardio-
Vascular System.' Illinois.SIMON, G. (I939), Proc. Roy. Soc. Med., 23, 1157.SMITH, K. SHIRLEY, and WOOD, F. G. (I949), Brit. Heart
From the Cardiac Department of the Royal Free Hospital
Angiocardiography is now an establisheddiagnostic procedure in the fields of thoracic andcardiac surgery. By intravenous injection of anopaque substance combined with rapid serialradiography it is possible to study the heartchambers and great vessels during life. Themethod was conceived more than 20 years ago,though its application in clinical medicine isrecent. Improvements in radiological techniquehave encouraged wider use of the procedure butthe interest in the diagnosis of congenital heartdisease and the advances in its treatment, aremainly responsible for modern development ofthis method of investigation.
HistoryIn 1929 Forssman first injected an opaque
substance into the living human heart. Like laterworkers in this field, notably Ameuille (1936),Forssman used sodium iodide for the intravenousinjection. In the quantity and concentrationemployed this substance gave good angiograms ofthe pulmonary arteriat tree, but it was not suf-ficiently opaque to outline the heart chambers orthe aorta. For this reason little progress was madein this method of investigation until Castellanos
(I938) and his co-workers in Cuba introduced theorganic iodides as the contrast medium. With35 per cent. neoiopax these workers were able toshow the right heart chambers and the aorta andits larger branches in children with cyanotic con-genital heart disease. But, because of dilution inthe pulmonary circulation, satisfactory angio-cardiograms ofthe left heart in acyanotic conditionscould not be obtained.
In 1938 Robb and Steinberg prepared and useda 70 per cent. aqueous solution of the diethanol-amine salt of 3, 5-diiodo-4-pyridone-N-acetic acidfor the intravenous injection. With this substancethey were able to outline, first, the right heartchambers and pulmonary arteries and later theleft heart and aorta. The introduction of multiplecassette-changing devices has enhanced the valueof angiocardiography, but in other respects theprocedure described by Robb and Steinberg ismore satisfactory than any other and is in generaluse today.
Contrast MediaDiodone or diodrast, the material originally
prepared by Robb and Steinberg, is still the mostwidely employed contrast medium in angio-
cardiography. The 75 per cent. solution of neoio-pax is used, but is less satisfactory because of itstendency to give rise to pain in the arm andshoulder during injection.
Diodone is freely miscible with blood, relativelyinert and excreted rapidly, unchanged, by thekidneys. It produces transitory peripheral vaso-dilatation and slight fall in blood pressure. Onreaching the systemic circulation it invariably givesrise to an unpleasant sensation of intense heat,often accompanied by a throbbing headache andoccasionally by nausea and vomiting. Localizedvenous thrombosis at the site of injection iscommon and infrequently erythematous or urti-carial eruptions occur. The toxic dose for man isnot known, but 1.5 gm./kilo is thought to beentirely safe (Robb and Steinberg, I939). Onseveral occasions we have employed larger quanti-ties and there have been no unpleasantsequelae.
Sensitivity to diodone is occasionally en-countered and intravenous, intradermal and intra-ocular tests are employed to exclude sensitivesubjects. Our practice is to inject i ml. diodonediluted in 20 ml. saline intravenously. On threeoccasions this has been followed by a vasovagalattack and the investigation was abandoned.Sensitivity tests are not, however, infallible. Twopatients who showed no reaction with the intra-venous test experienced transitory intense dys-pnoea when the diodone reached the pulmonarycirculation.
Although Robb (I947) has reported no serioussequelae in more than I,500 patients, deaths havefollowed angiocardiography in some instances(Taussig and Bing, 1949). Recently Dotter andJackson (I949) have reported 26 fatalities in a totalof 6,824 patients submitted to this procedure.The high incidence of cyanotic congenital heartdisease among the patients investigated probablyaccounts for the considerable mortality rate. Thereis little doubt, however, that in any seriously illsubject angiocardiography involves some risk andit is our practice to defer it in such patients, unlessit is expected to influence the immediate treatment.
Premedication and AnaesthesiaThe immediate unpleasant effects of diodone
can be mitigated to some extent by sedation;phenobarbitone or nembutal and nepenthe aresatisfactory in adults and in most acyanotic con-ditions in children. In children with cyanoticcongenital heart disease, on the other hand, theunpleasant sensation of heat and the intense head-ache occur early and are often very severe becausethe diodone is shunted directly into the systemiccirculation. Moreover, these children are often
seriously ill and any manipulation or fright mayinduce a fatal cyanotic attack. -In these circum.stances, therefore, angiocardiography, if deemedessential, is best performed under generalanaesthesia.
Technique of InjectionThis has been fully described by Robb and
Steinberg (1939) and only some details of theprocedure require special emphasis.The object of the injection is to produce an
opaque intravascular bolus which will in turnoutline each heart chamber and the great vessels.This can only be accomplished if a sufficientquantity of diodone is injected in a short time.Dilution of the contrast medium with venousblood inevitably occurs, even with rapid injection,,and may prevent clear definition of the cardiacchambers if only a small quantity is used. Largequantities, injected over a period of three orfour seconds, are equally unsatisfactory, since theangiocardiograms produced in this way consist ofa mass of confusing shadows where right and leftheart chambers and pulmonary and systemicvessels are superimposed.The rate of injection should be at least 30 ml.
per second and this speed can only be attained ifthe internal diameter of the cannula and the nozzleof the syringe are at least 2 mm. (--14 B.S.W.G.).Further, some form of locking device should beincorporated in the nozzle of the syringe to preventleakage during the injection. This is effected inthe special Robb cannula by the Luer-Lok, and inthis country syringes and cannulae with bayonetfixings can be obtained.The quantity of diodone injected depends on
the size of the patient and the size of the heart.In children 20 ml. is often sufficient. In adultswith large hearts and in obese subjects amountsup to 70 ml. may be required. Our experiencesuggests, however, that there is nothing to begained by increasing the quantity if the durationof the injection exceeds two seconds.The right median basilic vein is selected for the
injection if the superior vena cava is right-sided.In children the vein must be exposed and thecannula tied in, but in adults it is better to thrustthe trocar and cannula directly into the vein.The injection may be made with the patient
supine or erect. The former position is essentialin anaesthetized or heavily sedated subjects, butwhenever possible the upright position is to bepreferred. Not only does this allow, of less dis-tortion of the heart shadow, but in the uprightposition kinking of the subclavian vein at thethoracic inlet, which may interfere with rapidinjection, is more easily avoided.
November I949554P
rotected by copyright. on January 11, 2022 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.553 on 1 N
FIG. i.-Normal heart, child aged 4i years, antero-posterior position. I-second film showing superiorvena cava, right auricle, right auricular appendageand pulmonary trunk.
2 -
PA
FIG. 2.-Normal heart, child aged 41 years, antero-posterior position. ij-second film showing rightauricle and auricular appendage, right ventricle,pulmonary trunk, and right and left pulmonaryarteries.
ABBREVIATIONS IN DIAGRAMS
SVC Superior vena cava.IVC Inferior vena cava.
RA Right auricle.R. A. App. Right auricular appendage.RV Right ventricle.MPA Main pulmonary artery.RPA Right pulmonary artery.LPA Left pulmonary artery.LA Left auricle.L. A. App. Left auricular appendage.LV Left ventricle.AA Aorta.Cor. Sinus Coronary Sinus.
FIG. 3.-Normal heart, child aged 4i years, antero-posterior position. 31-second film showing pul-monary veins, left auricle, left ventricle and aortaand its branches.
W Att W e t ^oF
LV
FIG. 4.-Normal heart, child aged 41 years, antero-posterior position. 4A-second film showing leftauricle and auricular appendage, left ventricle andaorta.
FIG. 5.-Normal heart, woman aged 38, left anterioroblique position. i-second film showing superiorvena cava, right auricle, auricular appendage andcoronary sinus, right ventricle and pulmonary trunk.
...........i0t
FIG. 6.-Normal heart, woman aged 38, left anterioroblique position. 3-second film showing rightventricle, pulmonary trunk and its right and leftbranches.
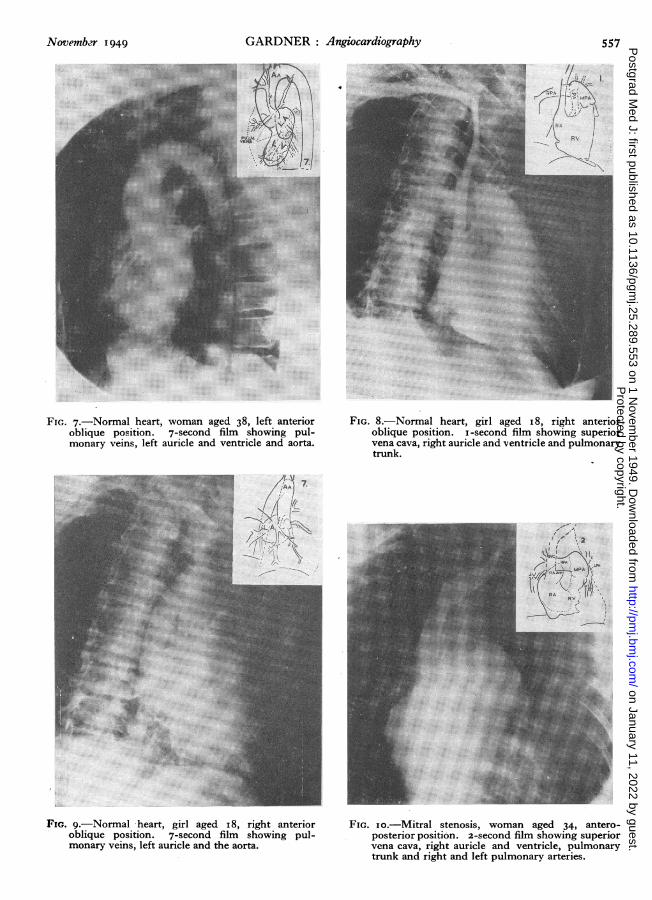
FIG. 7.-Normal heart, woman aged 38, left anterioroblique position. 7-second film showing pul-monary veins, left auricle and ventricle and aorta.
...
-u>(/-'N J
FIG. 8.-Normal heart, girl aged i8, right anterioroblique position. i-second film showing superiorvena cava, right auricle and ventricle and pulmonarytrunk.
7......
IL F
FIG. 9.-Normal heart, girl aged i 8, right anterioroblique position. 7-second film showing pul-monary veins, left auricle and the aorta.
- FAPA
-l--
FIG. io.-Mitral stenosis, woman aged 34, antero-posterior position. 2-second film showing superiorvena cava, right auricle and ventricle, pulmonarytrunk and right and left pulmonary arteries.
FIG. I2.-Mitral stenosis, child aged 8, left lateralposition. 2-second film showing right auricle andventricle and pulmonary trunk and right and leftpulmonary arteries.
PEAWs
FIG. 13.-Mitral stenosis, child aged 8, left lateralposition. 7-second film showing pulmonary veins,left auricle and ventricle and aorta.
*i
FIG. I4.-Syphilitic aortitis, man aged 56, left anterioroblique position. 9-second film showing aorticarch.
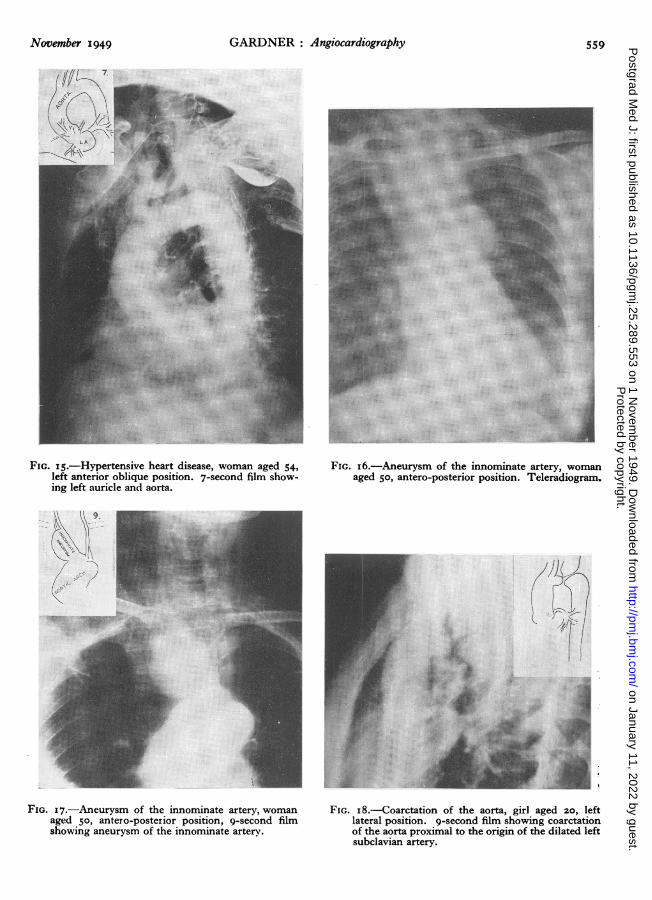
FIG. I5.-Hypertensive heart disease, woman aged 54left anterior oblique position. 7-second film show-ing left auricle and aorta.
......
..i{ .F....e
FIG. i6.-Aneurysm of the innominate artery, womanaged 5o, antero-posterior position. Teleradiogram.
I-O.......i~
!:N3>
FIG. 17.-Aneurysm of the innominate artery, womanaged 50, antero-posterior position, 9-second filmshowing aneurysm of the innominate arterv.
4/)
FIG. i8.-Coarctation of the aorta, girl aged 20, leftlateral position. 9-second film showing coarctationof the aorta proximal to the origin of the dilated leftsubclavian artery.
FIG. I 9.-Patent ductus arteriosus, girl aged 17 leftlateral position. Film showing bulge on the Xaorta,marked by arrow in the diagram.
2.
.. .. ... ...
FIG. 2C.-Eisenmenger complex, child aged 9, antero-posterior position. 2-second film showing simul-taneous filling of aorta and pulmonary trunk anddense pulmonary vascular markings.
VAL E.
FIG. 21.-Fallot's Tetralogy, child aged io, antero-posterior position. a-second film showing simul-taneous filling of aorta and pulmonary trunk andtranslucent lung fields. The dotted line in thediagram indicates the position of a catheter in theright pulmonary artery (from composite tracings).
The Circulation TimesIn normal children diodone may reach the
carotid arteries within four seconds of its injectioninto an antecubital vein and the difficulty of rapidfilm changing constitutes the chief problem ofangiocardiography. In adults, on the other hand,it may be 20 or more seconds before the aorta isoutlined and the problem here is to determine theoptimum times for the exposures. The arm-lungand arm-tongue circulation times are some indica-tion, provided the material employed is injectedthrough the large-bore syringe and cannula. Wehave found a modified arm-tongue time, deter-mined by injecting 5 gm. of saccharin diluted in2o ml. of saline, to be the most reliable guide tothe time when diodone first appears in the carotidarteries. Films taken one second before this timeand for I-2 seconds after it usually show the leftheart chambers and the aorta. But no way ofestimating the circulation time is infallible, ex-cepting only the injection of a full dose of diodoneitself, and in a few instances we have been forcedto employ this procedure.
CLINICAL APPLICATIONSThe Normal Angiocardiogram
Angiocardiographic studies in normal subjectshave been made in several centres (Robb andSteinberg, I940; Taylor and McGovern, 1943;Sussman and Grishman, I947; Chavez et al.,I947). These studies have confirmed in manyrespects and in a few have corrected the acceptedinterpretation, based on fluoroscopic study, of thecardiac contour. Further, by indicating the extentof the chambers lying within that contour, theyhave afforded a clearer conception of living cardiacanatomy. We have made angiocardiograms in aa small number of normal subjects in differentage groups in the three standard positions used atfluoroscopy. Not only have they shown somethingof the scope and limitations of the technique, butthey provide a useful standard by which to judgethe abnormal.
Antero-Posterior PositionIn the antero-posterior position the cardiac
chambers and both right and left auricularappendages are clearly defined and the anatomyof the systemic arteries arising from the arch ofthe aorta can generally be recognized. On theother hand, it is often difficult to determine withcertainty the exact position of the aortic andpulmonary valves because the former are super-imposed on the shadow of the left auricle and thelatter on that of the backwardly directed pul-monary trunk.
Figures I-4 are the antero-posterior angio-
cardiograms of a normal child aged 41 years. Thefilms are taken at one-second intervals, startinghalf a second after the beginning of the injection,and the first, second, fourth and fifth films of theseries are shown. The presence of diodone in thepulmonary artery and aorta, half a second andthree and a half seconds respectively, after thebeginning of the injection, is objective evidence ofthe rapid circulation times in these small subjects.
Left Anterior Oblique PositionThe main pulmonary artery and its left branch,
the arch of the aorta and the situation of the aorticvalves are seen best in this position and theventricular septum and the left heart chambers areusually, but not always, clearly defined. On theother hand, the right auricle and ventricle aresuperimposed and the pulmonary valves are rarelyseen because they overlie the root of the superiorvena cava and the right auricular appendage. Theright pulmonary artery is seen end on, and thedense rounded shadow indicating its origin is auseful landmark when the presence of the pul-monary arteries is in doubt.
Figures 5-7 illustrate the normal appearancesin the left anterior oblique position. In addition,they show two rather unusual features : in theone-second film a short segment of the coronarysinus is seen as a wide channel curving upwardsand backwards from the posterior mLrgin of theright auricle, and in the seven-second film a smallbulge di'+orts the usually smooth contour of theaortic arch at its junction with the descendingaorta.
Right Anterior Oblique PositionThe situation of the pulmonary valves is seen
better in this position than in any other. Theheart chambers are often well seen, but the rootof the aorta is rarely defined clearly because it issuperimposed on the shadows of the left auricleand the pulmonary veins.
Figures 8 and 9 illustrate the normalappearances in an i8-year-old girl in the rightoblique position.
Rheumatic Heart DiseaseAngiocardiographic studies in rheumatic heart
disease have been made by Grishman and Sussman(I944). These workers maintain that in mitralstenosis the pulmonary arc is formed in its upperpart by the pulmonary artery either alone or withits left branch, and in its lower part by the leftauricular appendage. In some of our patients,however, the appendage has appeared to besituated well within the cardiac silhouette and totake no part in the contour of the pulmonary arc.It is possible that in these instances the tip of the
November I 949P
rotected by copyright. on January 11, 2022 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.553 on 1 N
appendage contained blood clot or faulty timingof the exposures may have prevented its completedefinition.
Figures I0 and ii are the angiocardiograms ofa woman aged 34 with well-developed mitralstenosis. The pulmonary arc in this instance isformed entirely by the main pulmonary artery andits left branch and the left auricular appendage issome distance from the left border of the heart.Grishman and Sussman have shown that in
mitral stenosis the left auricle is enlarged in alldirections; it invariably contributes to the upperright cardiac contour and its forward enlargementresults in elongation and displacement of the out-flow tract of the right ventricle and the pulmonaryartery.The large left auricle is certainly the most
striking feature of angiocardiograms in mitralstenosis. It is appreciated most readily in the leftoblique or left lateral positions, where the forwardand upward enlargement is seen to displace theright heart chambers and the pulmonary artery.It is probably this elevation of the pulmonaryartery, so that it is directed upwards rather thanbackwards, that is primarily responsible for theprominent pulmonary arc so characteristic ofmitral stenosis.
Figures IX and 13, the angiocardiograms ofan 8-year-old child with mitral stenosis, illustratethe effect of enlargement of the left auricle on theanatomy of the right heart and pulmonary artery.
Syphilitic AortitisAngiocardiography has become a useful pro-
cedure in suspected syphilitic aortitis. FigureI4, the angiocardiogram of a 56-year-old man,shows the local bulging and loss of parallelism ofthe aortic walls, characteristic of specific aortitis.These features are readily distinguished from theuncoiled aorta of hypertensive heart disease(Figure I5), where the walls of the aorta aresmooth and the calibre decreases uniformly as thevessel is traced from its origin.
Aneurysm and Mediastinal TumourRobb and Steinberg (1940) were the first to
demonstrate the value of contrast media in thedifferential diagnosis of aneurysm and mediastinaltumour, and more recently Sussman (I948) haspublished an excellent study of this subject. Ananeurysm, unless completely thrombosed, becomesopaque at the same time as its vessel of origin. Atumour, on the other hand, though it may deformor displace the great vessels, does not becomeopaque. Figure i6 is the teleradiogram of a
woman aged 50 who complained of dysphagia.The shadow in the superior mediastinum suggestsan intrathoracic goitre, but the angiocardiogram(Figure I7) shows that it is, in fact, a thick-walled aneurysm of the innominate artery.
CONGENITAL HEART DISEASE
I. Acyanotic GroupCoarctation of the AortaWithin the last few years coarctation of the
aorta has become amenable to surgery in someinstances (Crafoord and Nylin, 1945). Diagnosisof this condition presents no difficulty and theindications for operation are based on clinical con-siderations, but the practicability of resectiondepends on the site and extent of the coarctation,and this can only be determined by angiocardio-graphy or thoracotomy. Several variations in theexact anatomy of the aortic arch may be en-countered and these have been discussed by Salenand Wiklund (1948). The commonest site ofmaximal stenosis is 2-3 cm. beyond the origin ofthe left subclavian artery, but in some instances itis immediately distal to the artery and rarely itmay be proximal to the latter.
Figure i8 is the angiocardiogram of a girlaged 2o years in whom the degree of coarctationas judged by the clinical findings was severe. Itis an example of the rare type of coarctationwhere the narrow segment is proximal to the leftsubclavian artery and the artery itself and thedistal aorta are dilated.
Isolated Valvular LesionsStenosis of the pulmonary or aortic valves has
been shown in only a few instances by angio-cardiography (Grishman et al., I947). Associatedanomalies, however, such as dilatation or hypo-plasia of the great vessels are easily demonstrated.
II. Arterio-Venous Shunts; Septal Defectsand Patent Ductus ArteriosusAngiocardiography may provide direct or in-
direct evidence of these anomalies. The directevidence is early filling of the left auricle orventricle from the right heart in atrial or ventricularseptal defect respectively (Keele; I948). Theindirect evidence of such defects and of patencyof the ductus arteriosus is the reappearance ofdiodone in the right heart chambers after it hasreached the left heart and aorta (Sussman andGrishman, 1947; Keele, 1948).
It is clear that the pressure differences whichnormally exist between the left and right sides ofthe heart should make direct visualization of thesedefects difficult. We have only seen this direct
562 November 1949P
rotected by copyright. on January 11, 2022 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.553 on 1 N
evidence in complicated anomalies where the shuntis from right to left and we have never seen it inan isolated atrial or ventricular septal defect.Recirculation of diodone, the indirect evidence ofintracardiac arterio-venous shunts, must, more-over, be diagnosed with caution. Where there is alarge left to right shunt, with or without pulmonaryincompetence, there is always much dilution ofdiodone in the right heart and pulmonary arteriesand these structures remain outlined for manyseconds after injection. Furthermore, in anycondition, diodone held up at the thoracic inlet byfaulty positioning of the arm may give rise to lateghost shadows of the right heart chambers. In asmall group of 20 patients with intracardiacarterio-venous shunts or a patent ductus arteriosuswe have not seen convincing evidence of re-circulation.
In persistent patency of the ductus arteriosusdirect evidence of the abnormal channel is rarelyseen but an abnormality of the contour of theaorta is said to be very constant (Sussman andGrishman, 1947). This is a local bulge or a moreextensive irregularity on the antero-inferior aspectof the arch at its junction with the descendingaorta. We have not seen an instance of patency ofthe ductus arteriosus where the outline of thispart of the aorta was normal, but we have seenlocal bulges in this situation in normal subjects(Figure 7). Further, it should be emphasizedthat, although the abnormality is easy to identifywhen the shunt is small, when it is large the aortamay be poorly defined owing to dilution of dio-done in the lesser circulation and the irregularityof its contour may be obscured by dense pul-monary vascular shadows.
Figure I9 illustrates the abnormal contour ofthe aorta in a I7-year-old girl with a patent ductusarteriosus.
III. Morbus CoeruleusThe most valuable contribution angiocardio-
graphy has made to modern cardiology is probablyin the field of cyanotic congenital heart disease.The advances in the surgery of this conditioninitiated by Blalock and Taussig (I945) in theUnited States and by Brock (1948) in this countrycall for accurate anatomical diagnosis.The surgical procedures are designed to increase
the blood supply to the lungs. The Blalock opera-tion is only feasible if both right and left pul-monary arteries and a systemic vessel, suitable foranastomosis, are present. Valvulotomy demandsa patent pulmonary trunk. In selecting cases suit-able for operation, therefore, it is necessary, first,to exclude those cyanosed patients in whom thepulmonary blood flow is adequate or increased
and, secondly, to establish the presence of thepulmonary arteries.
Angiocardiograms in patients with increasedpulmonary blood flow show dense pulmonaryvascular markings often for six or eight secondsafter the injection and there is no delay in fillingthe pulmonary arteries. By contrast, the trans-lucency of the lungs in children with diminishedpulmonary blood flow is striking; the pulmonaryarteries are seen in only one, or at the most in two,films of the series, and there is always some delayin their filling. The recognition of this delaydepends on a standard technique, and for thisreason the translucent appearance of the lungfields is probably more reliable evidence of pul-monary stenosis. In our experience' the exact siteof the pulmonary stenosis can rarely be determinedwith certainty by angiocardiography.The relative densities of the pulmonary and
aortic shadows are a rough measure of the rightto left shunt and the pulmonary blood flow. Slightaortic density suggests a small shunt, whereas adense aortic shadow is evidence of a large shuntand considerable pulmonary stenosis.The Eisenmenger complex is an example of
cyanotic heart disease with increased pulmonaryblood flow. Figure 20 is the two-second film ofa 9-year-old child with an abnormality of this type.Both the pulmonary arteries and the aorta arefilled with diodone and the solid density of theformer, compared with the slighter aortic shadow,suggests that the right to left shunt is not large.In this and subsequent films the dense vascularshadows in the lung fields are evidence of increasedpulmonary blood flow.
In cyanotic congenital heart disease withdiminished pulmonary blood flow the circulationto the alveoli is effected by pulmonary arteries,or by bronchial arteries and other collaterals, or,in some instances, by both pulmonary and bron-chial arteries. In the presence of pulmonarystenosis the pulmonary arteries fill from the rightventricle and they are always clearly seen inangiocardiograms, even if the stenosis be extreme.When, however, there is pulmonary atresia, thepulmonary arteries, if patent, fill from collateralvessels, and in these circumstances they may bedifficult to define. The ' hilar comma ' (Danelius,I942) of the left or right pulmonary artery canoften be recognized in teleradiograms of the chestand with experience it can be distinguished fromthe nodular hilar shadows characteristic of bron-chial arteries. But it is often impossible to makethis all-important distinction with certainty andit is pre-eminently for this reason that angio-cardiography has become an essential pre-opera-tive investigation in these patients. Campbell andHills (1950) have recently made a comprehensive
November I 949 563P
rotected by copyright. on January 11, 2022 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.553 on 1 N
study of this subject, based on a large number ofcases, and they have emphasized the distinctivefeatures of pulmonary and bronchial arteries.The Tetralogy of Fallot is the commonest
example of cyanotic congenital heart disease inwhich the blood supply to the lungs is inadequate.
Figure 2I is the two-second angiocardiogramof a io-year-old child. The aorta and pulmonaryartery are equally dense and the lung fields in thisand subsequent films are unusually translucent,suggesting considerable pulmonary stenosis. Theapproximate site of the stenosis, determined atright heart catheterization, is indicated in thediagram and the post-stenosis dilatation of thepulmonary artery is clearly seen in the angio-cardiogram. In the antero-posterior position therelation of both right and left subclavian arteriesto the pulmonary arteries is displayed and for thisreason it is the position of choice for angiocardio-graphy in uncomplicated Fallot's Tetralogy. Whenthe existence of pulmonary arteries is in doubtadditional films in the oblique position areessential.
Summary and ConclusionAdvances in the study of the living human
heart have been furthered by angiocardiographyand progress in this technique will add much to theunderstanding of the subject. At present inter-
pretation is often difficult, partly because exposuresare made too infrequently and partly because ofchanges in heart position and chamber size insystole and diastole. Improved radiological tech-nique, particularly means of making the exposuresat selected times in the cardiac cycle and simul-taneous exposures in the antero-posterior andoblique positions, will ease the difficulties andafford a clearer picture of the anatomy anddynamics of the heart in health and disease.
In the fields of thoracic and cardiac surgery,wider use of angiocardiography should decreasethe need for exploratory thoracotomy.
It is a pleasure to record my thanks to my seniorcolleague, Dr. Jenner Hoskin, for his help andencouragement in these investigations and to Drs.Ball and Zoob and Sister Kerrigan for theirassistance. I wish to thank Dr. Staveley forgenerous facilities in the X-ray Department andMr. Shepherd and his assistants for the photo-graphy.
I am greatly indebted to Dr. Maurice Campbellfor reading the script and for helpful criticism.
I am also indebted to the medical and surgicalstaff of the Royal Free and other hospitals whohave referred patients for angiocardiography.
BIBLIOGRAPHY
AMEUILLE, P., RONNEAUX, G., HINAULT, V., DEGREZand LEMOINE, J. M. (1936), Bull. et mim. Soc. mid. d. hop.de Paris, 60, 729.
BLALOCK, A., and TAUSSIG, H. B. (I945), J. Am. Med. Ass.,I28, I89.
BROCK, R. C. (1948), Brit. Med. J., , iizI.CAMPBELL, M., and HILLS, T. H. (I950), Brit. Heart. Y. In
the press.CASTELLANOS, A., PEREIRAS, R., and GARCIA, A. (I938),
Havana, La Propagandista.CHAVEZ, I., DORBECKER, N., and CELIS, A. (I947), Amer.
Heart Y., 33, 560.CRAFOORD, C., and NYLIN, G. (1945), J. Thoracic Surg.,
I4, 347-DANELIUS, G. (I942), Am. J. Roent., 47, 870.DOTTER, C. T., and JACKSON, F. (i949). Personal com-
munication.FORSSMANN, W. (1929), Klin. Wchnschr., 8, 2085.GRISHAM, A., and SUSSMAN, M. L. (1944), Am. J. Roent.,
S, 33.GRISHMAN A., STEINBERG, M. F., and SUSSMAN, M. L.
(1947), Med. Clin. N. Am., 31, 543.KEELE, K. D. (I947), Brit. J. Radiol., 21, 393.KEELE, K. D. (1947), Radiography, z5, I69.ROBB, G. P., and STEINBERG, I. (I939), Amer. J. Roent., 42, 14.ROBB, G. P., and STEINBERG, I. (1940), J. Am. Med. Ass.,
1I14, 474-ROBB, G. P. (I947). Personal communication.SALEN, E. F., and WIKLUND, Th. (I948), Acta. Radiol., 30, 299.SUSSMAN, M. L. (1947), Amer. J. Roent., 58, 584.SUSSMAN, M. L., and GRISHMAN, A. (I947), Advances in
Internal Medicine, by W. Dock and I. Snapper, New York;Vol. II, p. 102.
TAUSSIG, H. B., and BING, R. J. (i949), Amer. HeartJ., 37, 551.TAYLOR, H. K., and McGOVERN, T. (1943), 7. Am. Med. Ass.,