Anna Sommers † Julia Paradise ‡ Carolyn Miller * † Center for Studying Health System Change ‡ Kaiser Commission on Medicaid and the Uninsured * Independent consultant Presentation at State Health Research & Policy Interest Group Meeting, Seattle June 11, 2011 Physician Willingness and Resources to See New Medicaid Patients: Perspectives of Primary Care Physicians
Transcript
Anna Sommers †Julia Paradise ‡Carolyn Miller *
† Center for Studying Health System Change
‡ Kaiser Commission on Medicaid and the Uninsured
* Independent consultant
Presentation at State Health Research & Policy Interest Group Meeting, SeattleJune 11, 2011
Physician Willingness and Resources to See New Medicaid Patients:
Perspectives of Primary Care Physicians
Center for Studying Health System Change – www.hschange.org
ACA places new pressures on the Medicaid program
Center for Studying Health System Change – www.hschange.org
Extends Medicaid eligibility to most people up to 133% of FPL 16 million people will gain Medicaid coverage 25% increase over current enrollment
Raises Medicaid payment rates for primary care services delivered by primary care physicians to Medicare payment levels.
Temporary (2013 and 2014) Rates for specialty services remain unchanged.
2
Center for Studying Health System Change – www.hschange.org
Study Objective
Describe willingness and resources of primary care physicians to accept new Medicaid patients.
For Medicaid policy, willingness to treat patients just as critical to understand as physician capacity.
First study to combine data on these two dimensions.
3
Center for Studying Health System Change – www.hschange.org
Survey Data
2008 Center for Studying Health System Change (HSC) Health Tracking Physician Survey
Nationally representative sample of U.S. physicians
Self-administered mail survey
Provide direct patient care (20+ hrs per week)
62% response rate
More information:
Strouse et al. 2009, www.hschange.org
4
Center for Studying Health System Change – www.hschange.org
Survey Data
Analytic sample
Primary care physicians (PCPs) based on self-report
internal medicine
family medicine
general practice
Excludes if practiced most hours on hospital staff or in ED
1,460 PCPs
5
Center for Studying Health System Change – www.hschange.org
Methods PCPs ranked by level of participation in Medicaid
High-share Medicaid 26% or more of practice revenue from Medicaid
Moderate-share Medicaid 6-25% of practice revenue from Medicaid Accept new Medicaid patients
High-share Medicare (“Medicare”) 26% or more of practice revenue from Medicare Accept new Medicare patients Revenue from Medicaid 1% or more
Low and no-share Medicaid – none of the above
6
Center for Studying Health System Change – www.hschange.org
In-depth Follow-up Interviews
15 PCPs were interviewed in Summer 2010, after the ACA became law:
Various markets represented (eg. low-income urban, small town, suburban middle-income).
7
Center for Studying Health System Change – www.hschange.org
Low- and No- Share Medicaid
33.4%
High-ShareMedicare
19.0%
Moderate-Share Medicaid
29.1%
High-ShareMedicaid
18.5%
Figure 1Percent Distribution of Primary Care Physicians
by Level of Medicaid Participation, 2008
Note: Sample excludes pediatricians and physicians who work most hours on hospital staff or in emergency room.Source: 2008 HSC Health Tracking Physician Survey
High- and Moderate-
Share Medic-aid +
Medicare PCPs
66.6%
8
Center for Studying Health System Change – www.hschange.org
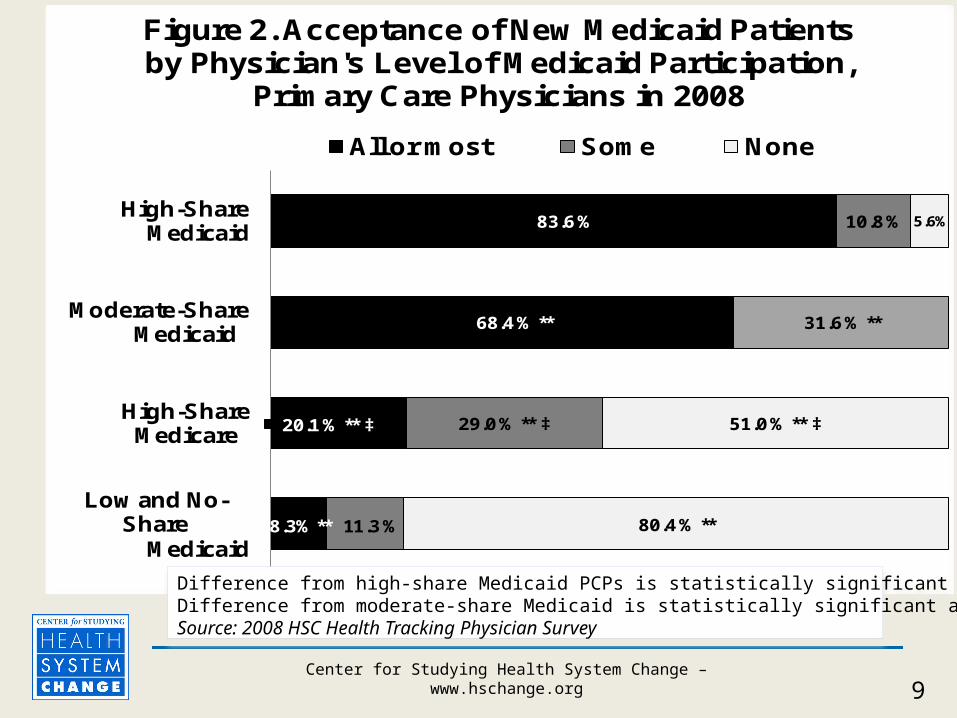
8.3% **
20.1 % ** ‡
68.4 % **
83.6 %
11.3 %
29.0 % ** ‡
31.6 % **
10.8 %
80.4 % **
51.0 % ** ‡
5.6%
Low and No-Share
Medicaid
High-Share Medicare
Moderate-ShareMedicaid
High-ShareMedicaid
Figure 2. Acceptance of New Medicaid Patients by Physician's Level of Medicaid Participation,
Primary Care Physicians in 2008
All or most Some None
Difference from high-share Medicaid PCPs is statistically significant at *p<.05 and **p<.01. Difference from moderate-share Medicaid is statistically significant at †p<.05 and ‡p<.01.Source: 2008 HSC Health Tracking Physician Survey
9
Center for Studying Health System Change – www.hschange.org
High-share Medicaid PCPs: More in hospital-based offices and community health
centers (38 vs 17 and 6%). High- and moderate-share Medicaid PCPs:
More report hospital ownership interest (30 vs 19%). Located in areas with lower household income.
Medicare PCPs (vs high/moderate Medicaid): More in solo/2-physician practices (44 vs 26 and 32%).
Practice Type and Location by Level of Medicaid Participation
10
Center for Studying Health System Change – www.hschange.org
75.9%68.7%
27.8%
41.8%
78.1%
62.9%
17.6%**
41.4%
72.6%
44.9% **‡
11.5%**‡
32.7%*
All EMR Interpreter services
Lack of qualifiedspecialists in area
Inadequate time with patients
Figure 3. Resources and Constraints at Primary Care Physician's Main Practice
by Physician's Level of Medicaid Participation, 2008
Difference from high-share Medicaid PCPs is statistically significant at *p<.05 and **p<.01. Difference from moderate-share Medicaid is statistically significant at †p<.05 and ‡p<.01.Source: 2008 HSC Health Tracking Physician Survey
11
Center for Studying Health System Change – www.hschange.org
PCPs currently limiting Medicaid panel expected to revisit participation level after Medicaid expansion.
Most cited at least one issue besides payment that would be considered. Difficulty finding specialists, paperwork, time-burden of
non-medical needs are all factors. Some consider Medicare patients/program to be more
of a burden than Medicaid. Illness burden of new patients
Findings of In-depth Interviews: Willingness
12
Center for Studying Health System Change – www.hschange.org
PCPs most willing to accept new Medicaid patients are already serving many of them. Just as likely to use health IT, more likely to offer
other key supports. Practice in low-income areas. Report more constraints on time and difficulty
finding specialists. Supporting new capacity here might improve
access.
Summary and Discussion
13
Center for Studying Health System Change – www.hschange.org
Moderate-share Medicaid PCPs hold some promise for adding capacity in Medicaid: Practice in lower-income areas, use health IT,
some have other supports in place. Decision matrix and makers may be different
because practice settings are different. Addressing issues other than payment
(payment delays, prior authorization) may increase participation levels.
Summary and Discussion
14
Center for Studying Health System Change – www.hschange.org
High-share Medicare PCPs hold less promise for increasing capacity: More are in solo/2-physician practices. Fewer have key patient supports. Location in higher-income areas may be a barrier.
Payment increases in Medicaid and trends in hospital acquisition of practices may impact both willingness and capacity.
Summary and Discussion
15
Center for Studying Health System Change – www.hschange.org
Kaiser Family Foundationhttp://www.kff.org/medicaid/8178.cfm
Jointly released inMedicare & Medicaid Research Review (MMRR)
Publication of the Centers for Medicare & Medicaid Services, Center for Strategic Planninghttps://www.cms.gov/MMRR/