1 Anne Arundel County Mental Health Agency, Inc PO Box 6675, MS 3230 Sponsor of Anne Arundel County’s Web Site: www.aamentalhealth.org 1 Truman Parkway, Suite 101 information website: www.networkofcare.org Email: [email protected]Annapolis, MD 21401 Phone: 410-222-7858 Francis A. Sullivan, LCSW-C, Executive Director Fax: 410-222-7881 CRISIS INTERVENTION SERVICES I. Request For Proposal (RFP) Overview A. Purpose The purpose of this RFP is to identify a mental health provider to operate Crisis Intervention Services (CIS) that consist of Mobile Crisis Teams (MCTs), Hospital Diversion, and 10 Urgent Care psychiatric evaluation slots per week as part of Anne Arundel County’s Crisis Response System (CRS). The CRS is part of a larger Community Behavioral Health System. It is designed with an operations hub and three (3) levels of interventions (See Appendix A, Community Mental Health Services). The CRS consists of the following: Mobile Crisis Teams, Hospital Diversion, the Operations Center, Consumer Outreach, Entitlements, and Care Coordination, and Urgent Care. The CRS was created with the goal of improving community response to persons with mental illness who experience a crisis. It was designed to develop a systemically integrated approach that would assist the police and fire officers who frequently are the first to be called for a wide variety of crises. At first, the above was accomplished by using MCTs consisting of two mental health professionals who carry police radios and have received police training about 911 operations, police procedures, and safety protocols. In 2008 a second goal, Hospital Diversion (HD), was added. The goal of HD was to decrease the number of repeat visits to an Emergency Department (ED), reduce unnecessary in-patient admissions, lower average length of stay of those admissions, and reduce the number of persons re- admitted within 30 days. Hospital Diversion staffing is included as part of the Mobile Crisis Teams. The expectation of the Anne Arundel County Mental Health Agency, (AACMHA), also known as the Core Service Agency (CSA), is that MCTs will respond to the EDs or inpatient units as part of Hospital Diversion. The Operations Center (OPS), including the telephone warmline, data collection, and care management, will be carved out of the existing CRS grants and will be staffed and managed directly by the CSA as follows: 1. The CRS program director position will be a CSA staff person. 2. The Operations Director will be a CSA staff person. 3. A Care Coordinator with at least a B.A. degree will coordinate, monitor, collect data, complete and manage reports on High Utilization Frequent Emergency Department (HUFED) consumers.
Transcript
1
Anne Arundel County Mental Health Agency, Inc PO Box 6675, MS 3230 Sponsor of Anne Arundel County’s Web Site: www.aamentalhealth.org 1 Truman Parkway, Suite 101 information website: www.networkofcare.org Email: [email protected] Annapolis, MD 21401 Phone: 410-222-7858 Francis A. Sullivan, LCSW-C, Executive Director Fax: 410-222-7881
CRISIS INTERVENTION SERVICES
I. Request For Proposal (RFP) Overview
A. Purpose
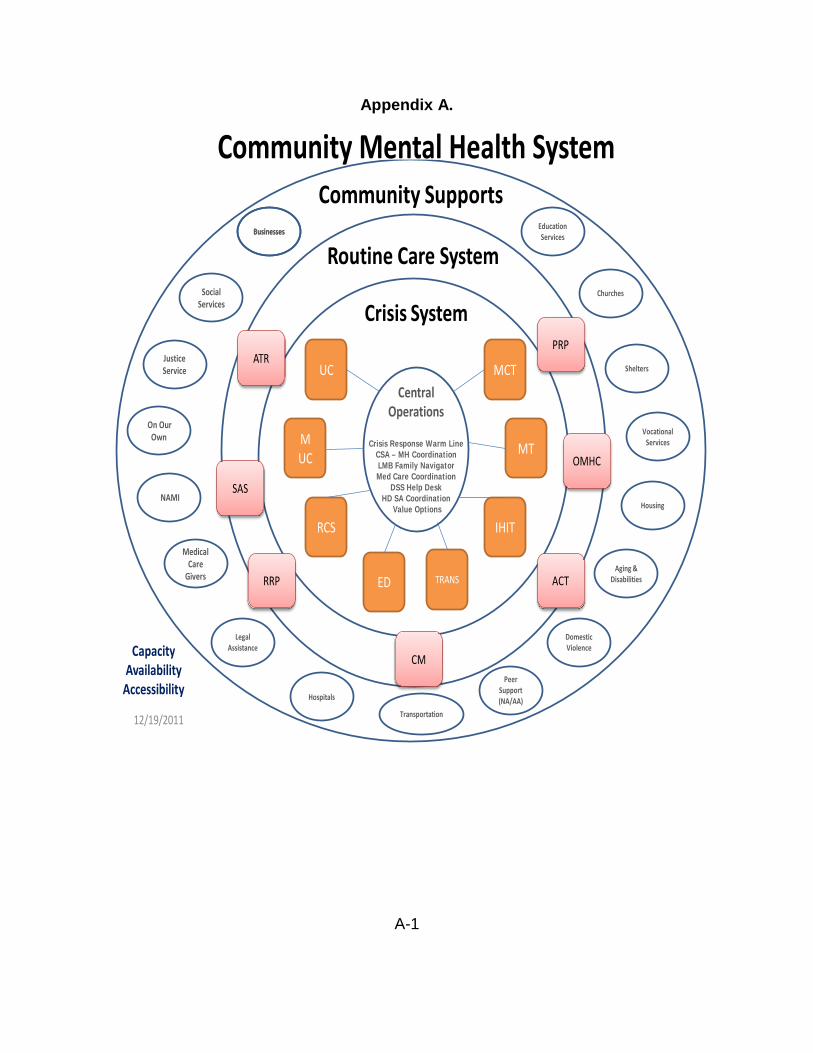
The purpose of this RFP is to identify a mental health provider to operate Crisis Intervention Services (CIS) that consist of Mobile Crisis Teams (MCTs), Hospital Diversion, and 10 Urgent Care psychiatric evaluation slots per week as part of Anne Arundel County’s Crisis Response System (CRS). The CRS is part of a larger Community Behavioral Health System. It is designed with an operations hub and three (3) levels of interventions (See Appendix A, Community Mental Health Services). The CRS consists of the following: Mobile Crisis Teams, Hospital Diversion, the Operations Center, Consumer Outreach, Entitlements, and Care Coordination, and Urgent Care. The CRS was created with the goal of improving community response to persons with mental illness who experience a crisis. It was designed to develop a systemically integrated approach that would assist the police and fire officers who frequently are the first to be called for a wide variety of crises. At first, the above was accomplished by using MCTs consisting of two mental health professionals who carry police radios and have received police training about 911 operations, police procedures, and safety protocols. In 2008 a second goal, Hospital Diversion (HD), was added. The goal of HD was to decrease the number of repeat visits to an Emergency Department (ED), reduce unnecessary in-patient admissions, lower average length of stay of those admissions, and reduce the number of persons re-admitted within 30 days. Hospital Diversion staffing is included as part of the Mobile Crisis Teams. The expectation of the Anne Arundel County Mental Health Agency, (AACMHA), also known as the Core Service Agency (CSA), is that MCTs will respond to the EDs or inpatient units as part of Hospital Diversion. The Operations Center (OPS), including the telephone warmline, data collection, and care management, will be carved out of the existing CRS grants and will be staffed and managed directly by the CSA as follows:
1. The CRS program director position will be a CSA staff person. 2. The Operations Director will be a CSA staff person. 3. A Care Coordinator with at least a B.A. degree will coordinate, monitor,
collect data, complete and manage reports on High Utilization Frequent Emergency Department (HUFED) consumers.
4. The current number of telephone warmline full-time employees will be maintained at seven.
5. Staff to provide administrative and data functions and support will be a part of OPS.
6. A consultant Psychiatrist will provide case consultations by phone and/or live case conferences.
7. If the CSA cannot develop an agreement to use Department of Aging and Disabilities to provide transportation between service components or to and from clinical services, a driver and vehicle will be provided by the CSA as part of the Operations Center.
8. Consumer Outreach, Entitlements, and Care Coordination (COECC) services will not be rebid. The provider, Partnership Development Group (PDG), will be expected to be a consistent partner of CIS, particularly in assisting with Care Coordination and entitlements follow-up.
9. 10 slots for Urgent Care psychiatric evaluations will be required by the successful bidder for use by the OPS staff and are included in this one RFP.
B. Applicant Qualifications
Applicants must meet the following criteria to be eligible for funding:
1. Be a state-certified and/or licensed mental health treatment provider and must be in good standing with the Office of Health Care Quality (OHCQ) and/or the AACMHA. Copies of all applicable state certifications and licenses and any OHCQ Site Visit Reports, including statements of deficiencies, must be included as an Appendix.
2. Have organizational capacity to bill the fee-for-service Public Mental Health System, i.e., collect revenue from the State of Maryland Administrative Service Organization (ASO).
3. Have the ability to assist with persons in stress, experiencing issues related to trauma, and be certified to conduct Critical Incident Stress Management (CISM) debriefings or defusings.
4. Have a commitment to provide high quality services to the diverse population of Anne Arundel County.
C. Proposal Timeframes and Specifications1
a. Timeline
a. Pre-bid Conference - 04/19/13, 1:00 p.m., Department of Health, 1 Harry Truman Parkway, Annapolis, MD 21401, Partnership
Conference Room. Attendance by applicants is strongly recommended. All interested applicants are encouraged to send questions in advance of the conference to the AACMHA email at [email protected]. In the Subject line list Questions to RFP. Questions received prior to the pre- bid conference will be answered at the conference, as well as questions posed at the conference. Full
1 Anticipated dates, subject to change at the sole discretion of the Anne Arundel County Mental Health Agency
3
responses to all questions will be posted on the AACMHA website (www.aamentalhealth.org).
b. Proposal Submission Deadline – Monday, May 13, 2013 by 3:00 p.m. c. RFP Review Committee Pick-up – Tuesday, May 14, 2013 d. RFP Review Committee Meeting - Wednesday, May 22, 2013, 10:00
a.m., Department of Health, 1 Harry Truman Parkway, Annapolis, MD 21401, Partnership Conference Room.
e. RFP Decision presented to the Board of Directors for approval – Tuesday, May 28, 2013
f. Contract Award – Wednesday, May 29, 2013 g. Work Commences – Monday, July 1, 2013
D. Contract Terms of Agreement and Funding
It is anticipated that funding will be available for Fiscal Year 2014 (July 1, 2013 to June 30, 2014). AACMHA anticipates stable or increased funding in future years. AACMHA may annually renew the contract awarded as a result of this RFP for up to four years.
II. Scope of Service
As a result of the CRS reorganization, the AACMHA is issuing this Request for Proposals (RFP) for Crisis Intervention Services (CIS). CIS consists of three services: Mobile Crisis Teams, Hospital Diversion, and Urgent Psychiatric Evaluation Availability.
A. Mobile Crisis Teams (MCT) a. Four (4) Mobile Crisis Teams (MCT), each consisting of either two licensed
or one licensed and one Masters level unlicensed/intern staff, is required. Each team operates an average of 40 hours per week, and coverage hours and days will be based upon the Anne Arundel Police Department (AAPD) needs. These four MCTs are expected to provide overnight coverage and Hospital Diversion as part of their MCT duties. An MCT Coordinator should be specified and should provide direct service. Shifts are defined as an average coverage of 8.5 hours per day each. Coverage hours and days will be based upon the Anne Arundel County Police Department needs. However coverage for 17 hours per day, seven days per week must be available. The teams are also expected to be available to provide follow-up community-based visits in at least 5% of the call-outs. These follow-up Community Stabilization Services (CSS) are considered billable and should be reflected in the budget. A plan to assure adequate staff to meet these requirements must be outlined. The successful bidder will assure the teams have sufficient vehicles and supplies to support the requirements of this RFP. The teams are expected to provide clinical support to the OPS phone counselors when the MCTs are not working on an active case.
b. Overnight Coverage for MCTs - A licensed Master’s Level Clinician will be available on call midnight to 8:00 a.m., seven days per week, to respond to MCT requests by the AAPD. Response to a calls, if requested by police, is to
4
be in less than one hour from time of request to arrival on site, unless physical distance is more than 25 miles from the Crownsville, Maryland CRS site.
B. Hospital Diversion and Emergency Department (ED) – as part of the MCT a licensed experienced clinician is expected to respond to hospital ED or in-patient units seven days per week when there is reason to believe a person with Medical Assistance (MA), Primary Adult Care (PAC) or an uninsured person might be diverted or transferred to a lesser restrictive service.
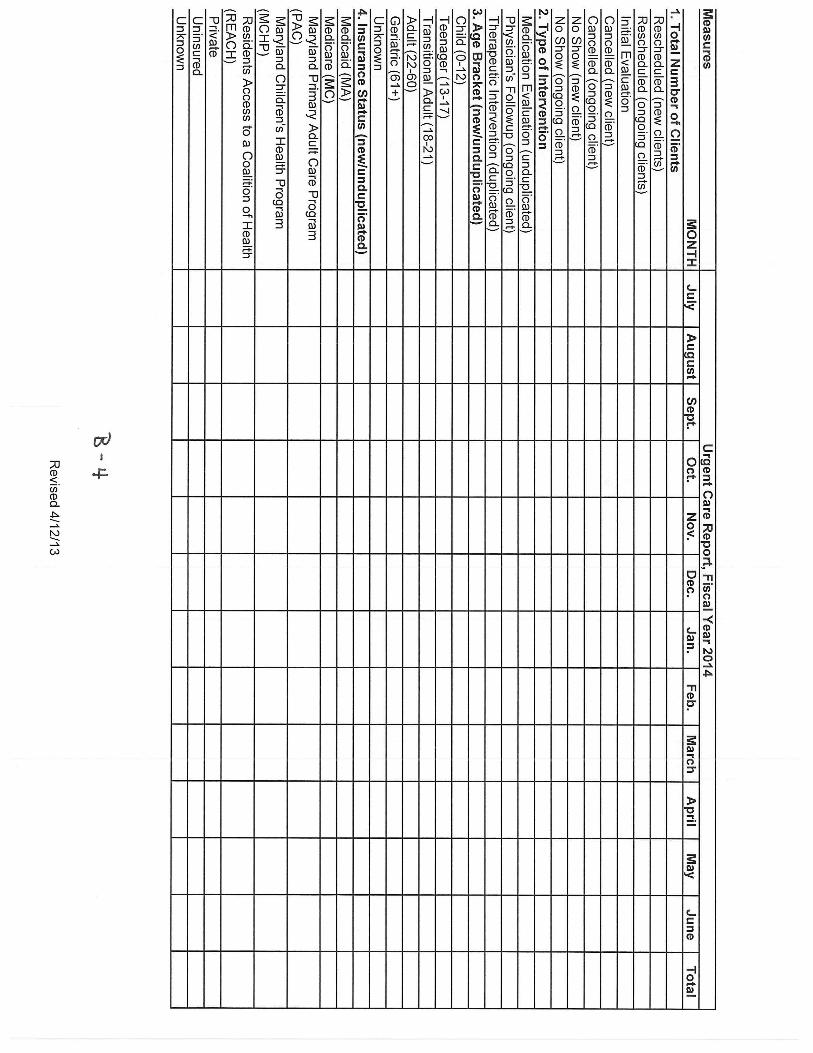
C. Urgent Psychiatric Evaluation Availability - The successful bidder should describe how CIS will provide or subcontract for 10 psychiatric evaluation slots per week with a Psychiatrist or a Clinical Nurse Specialist licensed to prescribe psychiatric medications. It is anticipated that most of these services can be billed to MA or other insurance, particularly after January 1, 2014. The successful bidder shall describe how they shall screen, assess, link or provide needed medical services as part of the psychiatric evaluation and Crisis Stabilization Plan (CSP).
D. Space and Logistics - The CRS is currently housed in the Winterode Building on
the grounds of the Crownsville Hospital Center. By July 1, 2013, the date of the beginning of the commencement of work under the contract award resulting from this RFP, the Operations Center and the MCT base office space will be co-located on the second floor of the Winterode Building. The co-location of MCT and OPS is considered a primary element of integration and is a major deliverable.
E. Support Services Menu - The CSA has already published a menu of support
services (See Appendix E, Crisis Services and Price Matrix). The CSA has budgeted $500,000 for payments for services of various types. The CSA encourages bidders to partner with shelters, mental health, substance abuse, medical, and/or Psychiatric Rehabilitation programs to develop effective use of these services with the ultimate goal of reducing ED visits and inpatient psychiatric hospitalizations. It is expected that any billable service through the Public Mental Health system will be billed accordingly. These 10 Urgent Care psychiatric evaluations (II. Items 3) are exclusive of services that are provided via Appendix E, Crisis Services and Price Matrix. These slots are to be made available and filled only by persons referred by the OPS Coordinator.
III. Statement of Need
There are several theoretical concepts underpinning the Anne Arundel County Crisis Response System (CRS), including: A. No Wrong Door - The Operations Center (OPS), is considered a major entry
point into services for persons seeking information or presenting as being in immediate need of behavioral help or intervention. OPS includes a telephone “warmline”, a comprehensive resource directory, and staff persons with comprehensive knowledge of local resources and how to access them. It also includes the ability to collect data, and to provide care coordination for persons in crisis. This service will be carved out of the existing CRS grants and will be staffed and managed directly by the CSA. The CRS program director position will
5
become a CSA staff person. The Operations Director will be a CSA staff person. A Care Coordinator with at least a B.A. degree will coordinate, monitor, collect data, complete and manage reports on High Utilizer Frequent Emergency Department (HUFED) consumers. The current number of Telephone Full Time Employees (FTEs) will be maintained. Staff(s) sufficient to provide administrative, data functions, and support will be a part of OPS. A consultant Psychiatrist will provide case consultations by phone and/or case conferences. If the CSA cannot develop an agreement to use Department of Aging and Disabilities to provide transportation between service components or to/from clinical services, a driver and vehicle will be provided by the CSA as part of the Operations Center.
B. Sequential Intercept Concept - Ideally, OPS is the hub of mental health service coordination. The telephone Warmline is a source of information and coordination, and a “No Wrong Door” entry or intercept point. www.networkofcare.org, an information and recovery-oriented resource for the public and system users, will be maintained as a way of enabling families and consumers to use services early and effectively. MCT is a second intercept point and the EDs a third. The fourth is the central booking at the Detention Center, and the fifth is the Court. The fourth and fifth points of this model are not funded by this RFP. The successful bidder should address the method of maximizing the use of OPS, MCT, and ED interventions to stabilize persons in mental health crises and ensure, to the extent possible, that the person gets the mental health and support services needed to maintain themselves in the community.
C. Integrated Care Systems - The experience of CRS since 1999 is that crises come in all forms. Furthermore persons in crisis usually have numerous problems and factors affecting the precipitation of the crisis and the form it takes. Experience confirms that treating the right condition at the right time with the right intervention is the right thing to do. It is vital to have crisis hotlines, mobile teams, care coordination, and multiple resources as part of a crisis system. It is just as important to have a community service system that can follow up after the crisis is over. Equally important is a robust system of community supports and communication in a recovery-oriented approach to maintaining wellness. This concept as it is applied in Anne Arundel County is found in Appendix A, Community Mental Health System.
D. Statistics - The current reports are found in Appendix B, Data Reports. Other reports will be required but are not provided as they are required by outside funding sources and should be expected to change throughout the duration of the contract period.
E. Physical Plant - The ideal physical layout is similar to the Haven for Hope Campus in San Antonio, Texas (See Appendix C, Ideal Campus). This ideal campus has job training and employment counseling, behavioral health, residential, legal, food services, medical, and other services essential to the homeless, behaviorally disturbed, physically ill, and legally involved. All services in the ideal model are in close physical proximity. Anne Arundel County currently has no such place. However, the CSA has several options for office and program space that should be addressed in the RFP response. These are:
6
a. The Winterode Building on the Crownsville Hospital grounds is a County Building. The successful bidder may opt to use the second floor which will be leased to the CSA. The first floor may or may not be available for programming. If the basement or 3rd floor is to be used, the cost of making the space habitable and appropriate for patient care must be addressed.
b. The Phillips Building on the Crownsville Grounds was vacated on or about April 1, 2013 by Second Genesis. This space may be available, partially or in full. The bidder may address how this space could be renovated to be used for purposes of this RFP. Because the CSA has no funds for renovation or rent, the source and amount of in-kind donations must be addressed. The cost of utilities is allocated by the square foot. This cost would be identified if any bidder expresses an interest.
c. Bidders may opt to locate, rent or purchase other space for use. If this option is selected, the bidder must identify and validate any in-kind donations or funding sources that are identified. Also, if this option is chosen, the bidder must address the co-location of the OPS, MCTs and other services specified in the RFP response. Also, a description of how the location and configuration of the building would facilitate integrated and effective treatment must be included in the response.
IV. Deliverables
The following are deliverables for MCT, HD, and Urgent Care Assessments (UC).
A. Mobile Crisis Teams
1. Four (4) Mobile Crisis Teams (MCT), each consisting of either two licensed or one licensed and one Masters level unlicensed/intern staff, is required. Each of these teams operate an average of 40 hours per week, coverage hours and days will be based upon the Anne Arundel County Police Department needs. The licensed staff on the MCTs are expected to provide overnight coverage and Hospital Diversion as part of their MCT duties. A total of 8 FTEs comprise the MCTs.
2. One FTE MCT Coordinator should be specified. The coordinator will have at least 50% direct service duties and 50% administrative (Although the MCT Coordinator is not included as part of the required 8 FTEs for the MCTs, he/she can be a team member up to 50% of his/her time).
3. These teams are also expected to be available to provide follow-up Community Stabilization Services (CSS) visits for at least 5% of the call- outs.
4. Assure the teams have sufficient vehicles and supplies to support the requirements of this RFP.
5. For overnight coverage the MCT is expected to respond to Police Department calls. Response to a call, if requested by Police, is to be in less than one hour from time of request to arrive on site, unless physical distance is more than 25 miles from the Crownsville, Maryland CRS site.
6. Provide a minimum of 40 trainings per year to police, fire, hospital, and other agencies in the county regarding effective use of CRS and MCT.
7
7. Provide a block of formal training delivered as part of the AAPD Training Academy.
8. Develop and implement a plan to assure adequate minimal staff works shifts to meet these requirements specified.
9. Hospital and Emergency Department (ED) Diversion - As part of the MCTs responsibility, the teams are to respond to hospital ED or inpatient units when there is reason to believe a person with Medical Assistance (MA), Primary Adult Care (PAC), or uninsured might be diverted or transferred to a lesser restrictive service.
10. The MCT members are expected to assist OPS telephone staff with clinical support, if needed. MCT members are also expected to further assist OPS telephone staff when not actively managing open cases.
11. Urgent Psychiatric Evaluations
a. Provide or subcontract for 10 psychiatric evaluation slots per week with a Psychiatrist or a Clinical Nurse Specialist licensed to prescribe psychiatric medications. These evaluations are exclusive of services that are provided via Appendix D, Crisis Services and Price Matrix. However, these slots are to be made available and filled only by persons referred by the OPS Coordinator.
b. Report revenue collections and efforts to bill for these services to MA or other insurance.
c. Provide a system to screen, assess, link or provide needed medical services as part of the psychiatric assessment and Crisis Stabilization Plan (CSP).
12. Space and Logistics
a. Co-location of MCT and OPS in a geographic location that facilitates prompt responses to the AAPD calls for MCT.
b. Demonstration of a plan and commitment to developing appropriate and adequate space that is conducive to the CRS mission outlined in this RFP.
13. Data and Administration
a. Provide records and data as required by the CSA. The successful bidder will input patient information in real time directly into the system purchased and maintained by the CSA. The information required will include but is not limited to patient name and appropriate demographics as defined by the CSA, referral source, and all releases and resolution of the crisis and/ or subsequent activity of the patient. If clinical information is entered into the system and deemed a client's medical record, the electronic medical record (EMR) will remain the property of the successful bidder and only management staff at the CSA will have access to that portion of the data in order to coordinate care at the system level, or to identity trends and other managerial functions. All OPS phone counselors and other staff identified by the CSA as requiring access to the
8
general database will be permitted limited access as needed to perform their duties at CRS. The successful bidder may use the CSA system for the patient’s medical record, if desired, and the CSA will pay for this use for up to 10 users (nine line staff and one management staff).
Training will be provided by the CSA at the beginning of the contract on one single day, and once annually thereafter for each year of the contract renewal. It is the expectation that the successful bidder will have sufficient staff present on the agreed to training day so that the staff is proficient in the use of the computer system and is able to adequately train any new employees hired by the successful bidder, if the hiring occurs prior to the next scheduled training. The successful bidder may choose to use any computerized medical record of their choice to download the data from their system into the CSA system, but the CSA system is to be used for real time encounters.
If the successful bidder chooses to use a different EMR for CRS, the
successful bidder will use an EMR that is compatible with the system in use by the CSA and capable of transferring the successful bidders other EMR data into the CSA system. This capability must be available on the first day of the contract. If this capability is inadequate or malfunctions in any way, the successful bidder will use the EMR capability of the CSA system until such time as the successful bidder demonstrates that another system is available to satisfy this requirement in a reliable manner. Reliable in this context is defined as a data dump that is error free in at least 99 percent of all attempts and there is 100 percent accuracy in all fields transferred.
b. Agree to assign staff for coordination meetings with other service
providers, as necessary, to comply with funding and monitoring agents.
V. Outcomes
The following are the minimum expectations of the components in this RFP. It should be expected that other elements could be added and/or these outcomes modified as the system is refined. A. Mobile Crisis Teams
1. Coverage for 24 hours a day, seven days a week, 365 days per year. 2. 1872 MCT responses per year. 3. 1235 police initiated responses per year. 4. 40 community agency trainings per year to police, fire, hospital and other
agencies in the county regarding the effective use of the CRS and MCTs. 5. At least one block of training delivered as part of the AAPD Training
Academy. 6. At least 72 Community Stabilization Services visits to at least 50 persons. 7. Favorable AAPD satisfaction ratings, (Rating Instrument will be provided by
the CSA).
9
8. 15 minute response to scene of AAPD dispatch request for at least 85% of dispatches.
9. Growth of Emergency Petition (EP) pickups equal to or greater than the growth rate of the past two years.
10. Total number of Community Stabilization Services billed through any other source.
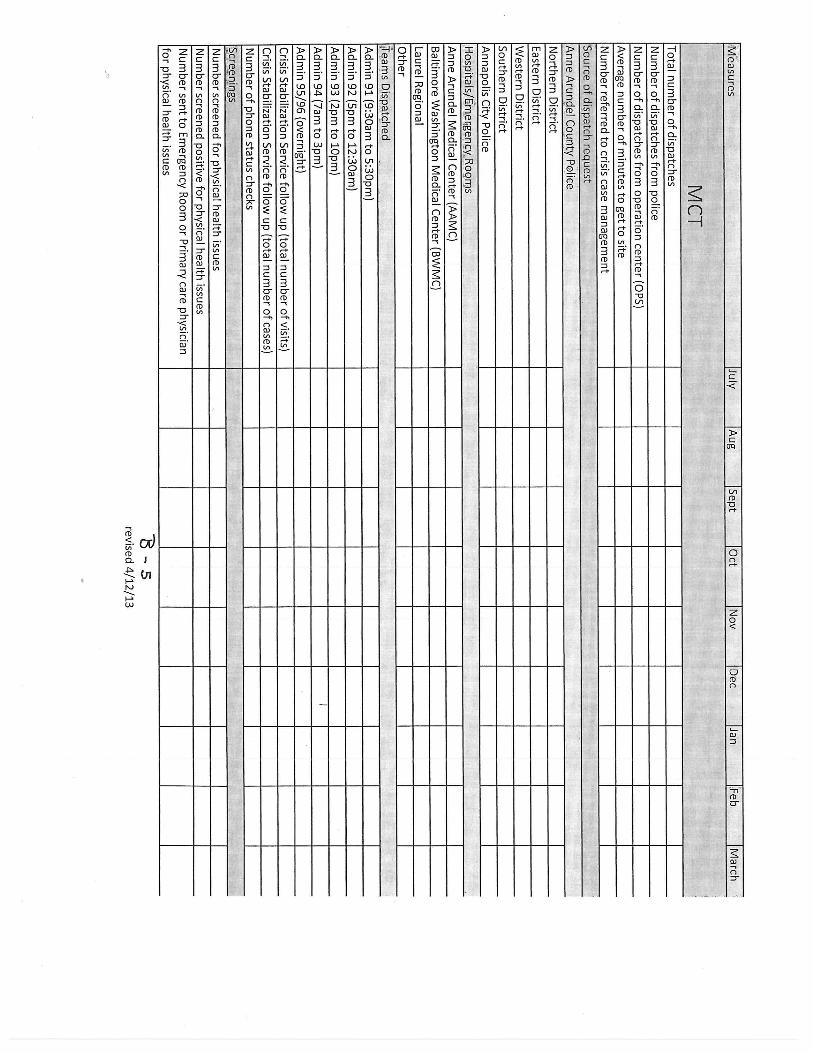
B. Hospital Diversion Reporting – Year one will be primarily data collection. Subsequent contract years will include expectations that Hospital Diversion will impact the data collected in year one. The following data will be collected:
1. Number of Emergency Department responses. 2. Number of inpatient responses. 3. Number of cases opened. 4. Number and percentage of persons identified as needing inpatient
hospitalization and number and percentage of persons diverted to other services.
5. Number of persons refusing MCT assessment.
C. 10 Weekly Urgent Psychiatric Evaluations Reporting 1. Number of evaluation slots allocated. 2. Number of appointments scheduled. 3. Number of appointments kept. 4. Number requiring medications. 5. Number screened positive for medical issues. 6. Number screened positive for substance use issues.
VI. Procurement Process
A. General 1. The issuing Office is:
Anne Arundel County Mental Health Agency, Inc. 1 Harry S Truman Parkway Suite 101 Annapolis, Maryland 21401 410 222-7858 The Issuing Officer is Francis A. Sullivan, LCSW-C, Executive Director.
B. Duration of Offer The offeror agrees to be bound by its technical and price proposals for a period of
60 days from the proposal closing date, during which time AACMHA may request clarification or corrections for the purpose of evaluation. Amendments or clarifications requested by AACMHA shall not affect the remainder of the proposals, but only that portion so amended or clarified.
C. Cost of Proposal Preparation
Any costs incurred by offerors in preparing or submitting proposals are the sole responsibility of the offerors. AACMHA will not reimburse any offeror for any
10
costs incurred in making a proposal or subsequent pre-contract discussions, presentations, or negotiations.
D. Selection and Ad Hoc Committee A committee will be formed to review the proposals, score them, and recommend a selection to the AACMHA Board of Directors Contract Committee. Final acceptance of the deliverables will be made by AACMHA and the AACMHA Board of Directors.
E. Proposal Submission
1. Form of Proposal - Proposals will be received from each offeror in separate sealed packages grouped and marked as follows:
“Anne Arundel County Crisis Intervention Services – Technical Proposal.”
Include Offerors Name and Date of Proposal
2. A separate proposal in a separate sealed package grouped and marked as follows:
“Anne Arundel County Crisis Intervention Services – Price Proposal” Include Offerors Name, Date of Proposal
F. Freedom of Information 1. Offerors should give specific attention to the identification of those portions
of their proposals that they deem to be confidential proprietary information or trade secrets and provide any justification why such material, upon request, should not be discussed by AACMHA under the Maryland Public Information Act, State Government Article, Sections 10-611 et seq. annotated Code of Maryland.
2. Offerors are advised that the mere assertion of confidentiality is not sufficient to make matters confidential under the act. Information is confidential only if it is customarily so regarded in the trade and/or the withholding of the data would serve an objectively recognized private interest sufficiently compelling as to override the general disclosure policy of the act. In determining whether or not information designated as such is proprietary, AACMHA will follow the direction provided by the attorney when responding to requests for information contained in proposals.
3. It may be necessary that the entire contents of the proposal of the selected offeror be made available and reproduced for the purpose of examination and discussion by a broad range of interested parties.
VII. Technical Proposal Criteria
A. Overview
The proposal should address all points outlined in this RFP, and should be clear and precise in response to the information and requirements described. A transmittal letter should accompany the technical proposal. The sole purpose of this letter is to transmit the proposal. It should be brief and signed by an individual
11
who is authorized to commit the offeror to the services and requirements as stated in this RFP.
B. Format of Proposal
Complete Appendix F, RFP Submission Checklist. Each offeror is required to submit a package which must bear the name of the offeror and the closing date for proposals on the outside of the package. This package should consist of an original and five copies of the entire proprosal. 1. Executive Summary
The offeror shall condense and highlight the contents of the Technical Proposal in a separate section entitled Executive Summary. The summary shall provide a broad understanding of the objectives, the requirements of the RFP, the scope of work, the contents of the proposal, and any related issues.
2. Proposed Services - Work Plan
The offeror shall provide a detailed discussion of the offeror's approach, methods, techniques, tasks, work plan for addressing the requirements outlined in the scope of work, and any additional requirements that might be identified by the offeror. The proposal must fully explain how the proposed services will satisfy the requirements of this RFP, including all significant tasks, aspects, or issues that will be examined to fulfill the scope of work. A time-phased schedule by tasks should be included for meeting the proposed objective, along with a breakdown of proposed staff assignments, and time requirements by task. The offeror should demonstrate a full understanding of the purpose and expectations and complexities of the project and how the objective may best be accomplished. The total scope of effort and resources proposed by the offeror should be convincing and consistent with the view and nature of the engagement. The offeror should demonstrate the required objectivity.
3. Project Organization and Management
The offeror shall demonstrate the capability to successfully manage and complete the contract, including an outline of the overall management concepts and methodologies to be employed by the offeror and a project management plan which includes project control mechanisms, and quality control procedures. Key management individuals responsible for coordinating with the AACMHA should be identified. The offeror must meet periodically with AACMHA staff and render periodic progress reports for the purpose of administering the contract. Offeror shall also participate in the client tracking process developed by AACMHA, collecting and submitting relevant data, as required. The offeror shall also address the transition and employment of existing agency-based staff.
12
4. Experience and Qualifications of Offeror
References and descriptions of previous similar engagements should be provided, (all references should include a contact person familiar with the offeror's work and the appropriate telephone number) as well as demonstrated ability of the offeror to successfully provide sufficient qualified backup staff.
5. Personnel Capability Clearly identify the proposed project team, the assignment of work activities, and the experience, qualifications, and education of the staff to be assigned. It is essential that the offeror assign and provide sufficient qualified staff assigned in an appropriate mix who has experience in aspects related to the objectives and scope of the proposal. The offeror should explain to what extent backup professional personnel are available to substitute for loss of professional personnel identified as necessary in the proposal.
VIII. Price Proposal Criteria
A. Overview
The proposal should address all points outlined in this RFP, and should be clear and precise in response to the information and requirements described. A transmittal letter should accompany the price proposal. The sole purpose of this letter is to transmit the proposal. It should be brief and signed by an individual who is authorized to commit the offeror to the services and requirements as stated in this RFP.
B. Format of Price Proposal
Each offeror is required to submit a Price Proposal which must bear the name of the offeror and the closing date for proposals on the outside of the package. Inside this package (an original and five copies) shall be the offeror's Price Proposal. For purposes of scoring the price proposal, “offer” is considered to be DHMH grant funds only. The budget in its entirety, including all other revenue, will be considered as part of the technical submission for completion and qualitative elements.
1. Overall Budget
An overall budget (on the appropriate forms) shall be submitted. All other sources of revenues anticipated should be detailed in the submitted budget.
2. Personnel Detail Page (See Appendix D, Additional Budget Instructions).
A personnel detail page, including the qualifications and titles of staff, the hours/days of employment anticipated, the salary per hour/day, and any agency adjustments should be detailed. All consultant costs should be
13
detailed including type of consultant, if known, and an hourly rate for each consultant hired.
3. Collections
Use of, and ability to bill and collect Medicare, Medicaid, and third party payments should be documented.
IX. Proposal Evaluation Criteria
A. Overview
An Ad Hoc Committee shall first review any submitted technical portions for compliance with essential technical requirements as expressed in this RFP. Proposals will be studied in depth and evaluated, first for technical content without consideration of costs, then for costs. Technical considerations will receive 55% relative weight in the evaluation process and costs will carry 45% relative weight. The proposals and scores of the top contenders, along with the Ad Hoc Committee recommendations, will be forwarded to the AACMHA Contract Committee for review and final determination.
B. Evaluation Method
Acceptable Offers
Each member of the Ad Hoc Committee will complete a preliminary technical evaluation. All offerors who receive a rating of 80% or more of total points possible on the technical proposal evaluation from a majority of the Ad Hoc Committee will be considered to have an acceptable offer and will receive consideration of their price proposal. Technical factors will be weighted as follows:
a. Strength of overall approach 5%
b. Work Plan and Approach to Deliverables and Goals 30%
c. Project Organization, Management, In-kind services/donations, Organizational infrastructure 35% d. Experience and qualifications 10% e. Personnel Capabilities 20%
Unacceptable Offers
The offerors for whom a majority of the Ad Hoc Committee evaluates with a technical rating of less than 80% of the total possible points will be considered unacceptable and will not be considered further. Their price proposal will not be considered.
14
Technical Scores
Relative values will be established by the following computation for the technical scores of each of the proposals being considered.
Average Number of Technical Rating Points - Individual Proposal
----------------------------------------------------------------- = X (Technical Score)
Average Number of Technical Rating Points - Highest Rated Proposal
Price Score
Those proposals that receive a technical relative value score of 80 or higher will be assigned a financial relative score by the following computation:
Lowest Offer
----------------------------------------------------------------- = Y (Price Score) Individual Offer
Final Score
The individual proposal will then be scored using the formula:
.55X + .45Y = FINAL SCORE
Appendix A.
Routine Care System
CentralOperations
Crisis System
CapacityAvailability
Accessibility
Community Mental Health System
MCT
MT
UC
RCS
Community Supports
MUC
SocialServices
Businesses
NAMI
Medical Care
Givers
Domestic Violence
Shelters
Churches
EducationServices
Legal Assistance
Aging &Disabilities
Housing
VocationalServices
Hospitals
Peer Support(NA/AA)
Crisis Response Warm LineCSA – MH CoordinationLMB Family NavigatorMed Care Coordination
DSS Help DeskHD SA Coordination
Value Options
Transportation
IHIT
Businesses
On Our Own
JusticeService
ED TRANS
PRP
OMHC
ATR
ACTRRP
SAS
CM
12/19/2011
A-1
A-2
D-1
Anne Arundel County Mental Health Agency, Inc PO Box 6675, MS 3230 Sponsor of Anne Arundel County’s Web Site: www.aamentalhealth.org 1 Truman Parkway, Suite 101 information website: www.networkofcare.org Email: [email protected] Annapolis, MD 21401 Phone: 410-222-7858 Francis A. Sullivan, LCSW-C, Executive Director Fax: 410-222-7881
APPENDIX D ADDITIONAL BUDGET INSTRUCTIONS
DHMH Form 432 is required to submit a detailed budget and budget narrative for this RFP. Forms are available via a link at www.aacountymentalhealth.org or directly on the DHMH Maryland website. All pages of the form are required. Please pay particular attention that the detail pages tie to the cover page (432B). Also, please pay strict attention to the salary and the consultant pages. For this RFP the following is required information. For your convenience, your organization may modify (add an additional column), if necessary, to provide the following data. Salary (This is required for EACH position listed on the salary back-up page, even if the position is support staff):
• Name of person filling the position. • Credentials of person filling the position, i.e., type of license, if applicable, and/or highest
degree held. • Dollar amount of salary PER HOUR and the dollar amount of the annualized salary. • The number of hours PER WEEK that the person is assigned to this particular project. • The % FTE (Full Time Employee) for the position. • The total DHMH funding requested. • The total funding for each position. HOTE: if the total funding is greater than the DHMH
funding requested, the in-kind or other revenue must be clearly identified on the 432H. • Page number of technical proposal where each position is listed.
Consultants For each consultant listed, please include the same information listed above, as well as, the duties expected of the consultant. NOTE: For both SALARY AND CONSULTANT please attach the appropriate pages of the
Technical Proposal where the positions are detailed. All positions should be clearly identified and must match the submitted salary and consultant detail. If there is a discrepancy, the proposal may be disqualified, or the AACMHA, at its discretion, may request clarification. The AACMHA assumes no responsibility for any misinterpretation of the number of staff members and their salaries assigned to this project. The forms are very clear and should match the technical proposals. Please attach a copy of the exact pages of the Technical Proposal describing the budget to the appropriate budget pages.
PO Box 6675, MS 3230 Sponsor of Anne Arundel County’s Web Site: www.aamentalhealth.org 1 Truman Parkway, Suite 101 information website: www.networkofcare.org Email: [email protected] Annapolis, MD 21401 Phone: 410-222-7858 Francis A. Sullivan, LCSW-C, Executive Director Fax: 410-222-7881
Appendix F
Please provide copies of the following documents, if applicable. If they are not available or not applicable, note as such. Incomplete proposals will not be considered.
1. Signed certification regarding Debarment, Suspension and other responsibility matters.
2. Articles of Incorporation.
3. By-Laws of your organization.
4. If your organization is a non-profit, proof from the Internal Revenue Service showing that your organization is exempt from income tax. (Copy of 501c(3) status.)
5. Copy of your organization’s general entity information showing that it is currently in good standing with the state of Maryland. (Use the following address to obtain an unpaid STAT certificate. https://sdatcert1.resiusa.org/certificate_net/)
6. Ascertain that entity is not on the List of OIG (Office of Inspector General) Excluded Individuals/Entities. http://oig.hhs.gov/fraud/exclusions.asp
7. Listing of names, titles, addresses, and phone numbers of your current Executive Director, Officers, and Board of Directors legally responsible for the organization’s affairs.
8. Annual Report/Audit or review for the previous two (2) fiscal years.
9. Board resolution approving submission of proposal.
10. Proof of financial capability to perform work requirements described in the RFP.
11. Adherence to Format/Outline/Guide provided in the RFP. *Note: Use of graphs/charts, etc. to facilitate the review process is encouraged. The Review Committee makes no assurance regarding the interpretation of the submission. Clear, concise narratives are encouraged with attention given to the format provided.
12. Proof of financial capability to perform work requirements described in the FRP.
13. Description of your organizational structure, including internal management controls.
14. Technical proposal which includes the following: • RFP mission statement with goals and objectives; • Knowledge of the population to be served; • Knowledge of the Maryland Public Mental Health System; • Your organization’s basic values and beliefs about mental health systems; • Detailed Work Plan; • Performance measures; • Implementation schedule; • Ability to respond requirements in a timely and cooperative manner; • Documentation procedures, including confidentiality and record security; • Internal Quality Assurance processes, including use of technology to improve
quality and efficiency. • Ability to prepare and obtain MOU’s with appropriate entities. • Letters of support, if applicable. • Copies of Tools (surveys, checklists, etc.) planned to be used while implementing
the service.
15. Price proposal detailing all staff and support costs associated with the project.
16. Resumes of personnel who will be assigned to the project.
17. Transmittal letter on Offeror’s stationary signed by authorized official.