38
2017 YOU DECIDE Annual Enrollment October 17 – November 4, 2016
| Date post: | 06-Feb-2018 |
| Category: |
Documents |
| Upload: | truongnguyet |
| View: | 215 times |
| Download: | 1 times |

2017YOU DECIDE
Annual EnrollmentOctober 17 – November 4, 2016
www.GaBreeze.ga.gov
2017 You Decide
2
TABLE OF CONTENTSTABLE OF CONTENTSWelcome 3
General Eligibility and Enrollment Information EnrollmentandEligibility 4DependentsEligibleForCoverage 4SalaryforBenefitPurposes(AnnualBenefitBaseRate) 4Pre-TaxPremiumsHelpYouStretchYourDollars 5ImportantInformationIfYouAreANewEmployee 5AfterYouEnrollForCoverage 6WhenCoverageBegins 6ConfirmingYourChoices 6ToChangeYourDecisionsAtAnnualEnrollment 7ToChangeYourDecisionsOutsideAnnualEnrollment 7ContinuationofBenefitsDuringLeaveorEndofEmployment 8
Your Flexible Benefit OptionsDentalPlans 10Vision 14Employee,Spouse,andChildLifeInsuranceandAD&D 18Short-andLong-TermDisability 20Long-TermCare 22CriticalIllness 24LegalInsurance 27SpendingAccounts 29
Employee Checklist 32
HIPAA Privacy and Security Notice 33
Benefit Phone Directory 35
Terms and Conditions 36

www.GaBreeze.ga.gov
2017 You Decide
3
WelcmeWelcome toTHE STATE OF GEORGIA FLEXIBLE BENEFITS PROGRAM
TheStateofGeorgiaispleasedtoofferyouacompetitiveflexiblebenefitsprogramasanintegralpartofyourTotalRewardspackage.Your2017YOU DECIDEbookletgivesyouanopportunitytoreviewandunderstandtheseplans.Itsummarizestheoptionsavailabletoyouandyoureligibledependents,alongwithwhatyouneeddotoobtainthesebenefits.
Areyouplanningorexpectingthebirthoradoptionofachild?Gettingmarriedsoon?Areyoucaringforanagingparent?Isittimetostartthinkingaboutsupplementingyourretirement?Thesearejustsomeoflife’schangesthatcouldaffectthehealthcareandfinancialneedsofyouandyourfamily.
The2017planyearincludessomeenhancements,soreviewallyourmaterialscarefully.PleasereadtheYOU DECIDE booklettounderstandtheoptionsavailabletoyouandguideyouinmakingthechoicesthatbestmeetyourneeds.Makingtherightdecisionstodaycanmakearealdifferencetowardbuildingasecurefutureforyouandyourfamilytomorrow.
www.GaBreeze.ga.gov
2017 You Decide
4
Enrollment and Eligibility
YouareeligibletoparticipateintheFlexibleBenefitsProgramifyouare:• Afull-time,regularemployeewhoworksatleast
30hoursaweekandisexpectedtoworkforatleastninemonths.Employeeswhoworkinashelteredworkshoporworktransitionprogram,contingentemployees,temporaryemployees, andstudentemployeesarenoteligible.
• Apublicschoolteacher,workingatleast17.5hoursperweek,andemployedinaprofessionallycertifiedcapacity,workinghalftimeormoreandnot considered a “temporary” or “emergency” employee.
• Anemployeeofalocalschoolsystemholding anon-certificatedposition.YoumustbeeligibletoparticipateintheTeacher’sRetirementSystem(TRS)oritslocalequivalent,andyoumustworkaminimumof20hoursaweek(or60%ofthetimenecessarytocarryoutthedutiesoftheposition, ifthat’smorethan20hours).
• Anemployeeofalocalschoolsystemworkingatleast15hours(or60%ofthetimenecessarytocarryoutthedutiesofyourposition,ifthat’smorethan15hours)andyouareeligibletoparticipateinthePublicSchoolEmployees’RetirementSystem(PSERS).
• Anemployeeofacountyorregionallibrary andworkatleast17.5hoursperweek.
• Deemed eligible by Federal or Georgia law.
Ifyouaren’tsurewhetheryou’reeligible,contactyourHumanResources/PayrollOffice.
Dependents Eligible For Coverage
Eligibledependentsincludeyour:• Legalspouse.• Dependentchild/renwhoareunderage26.• Dependentchild/renwhoareage26oroverand
incapableofself-sustainingemploymentbyreasonofmentalincapacityorphysicaldisability.
• Dependentchild/renaredefinedasyouoryourspouse’snaturalorlegallyadoptedchild/ren.Toverifyeligibilityofnewlyaddeddependents,youmustprovidesupportingdocumentation(e.g.,birthcertificate,marriagecertificate),ifrequested.
Salary for Benefit Purposes (Annual Benefit Base Rate)
YourAnnualBenefitBaseRateincludesyourbase salaryandsalarysupplementsthatareregular,non-temporary,andnotmorethantheamountonwhichretirementcontributionsarecalculated.ThisamountisreflectedonGaBreezeandremainsconstantfortheentireplanyear.ItiscalculatedonyourdateofhireandupdatedeachOctober1thereafter(theBenefitCalculationDate).AnyadjustmentstoyourAnnualBenefitBaseRate,withtheexceptionoferrors(asdeterminedbythePlanAdministrator),shallbereflectedonthefollowingBenefitCalculationDateandeffectiveforthefollowingplanyear.Promotions,demotions,andadjustmentsduetocertificationsarenotdeemedtobeerrors.YourAnnualBenefitBaseRateisthepayusedtocalculateyourcoverageforemployeelife,AD&D,anddisabilityinsurance.
BenefitsareakeypartofyourTotalRewards.PleasenotethatyourAnnualBenefitsBaseRateasofOctober1maybedifferentfromyourregularsalary.
GENERAL ELIGIBILITY AND ENROLLMENT INFORMATION
The“TotalRewards”website,accessedthroughGaBreeze,hasbeenenhancedandisnowupdatedonamonthlybasis.Tocheckoutthenewsite,gotowww.team.ga.govandclickonMy Benefits followed by Flexible Benefits toaccessGaBreeze.ThenlookintheupperrighthandcornerforthelinktoYour Total Rewards.

www.GaBreeze.ga.gov
2017 You Decide
5
Pre-Tax Premiums Help You Stretch Your Dollars
TheFlexibleBenefitsProgramallowsyoutosaveontaxeswhileyoupayforyourbenefits.Pre-taxpremiumsreduceyourtaxableincome–which,inturn,reducesyourtaxes.That’sbecausecertainpremiums(dental,vision,and,atyourdirection,lifeinsurance),andSpendingAccountcontributionsaretakenoutofyourpaybefore federal and state income taxesandSocialSecurity(FICA)taxesarewithheld.
Theresult?Yourtaxableincomeislowerandso areyourtaxes.Italsomeansyouhavemorein yourpaycheck–ormoretospendonbenefitsthanyouwouldifyou’dpaidthesamepremiumswithpost-taxdollars.
Important Information for New Hires
Ifyouareanewemployee,lookcarefullyatthoseFlexibleBenefitsthatofferone-timeopportunities.
• New Hire Electronic Enrollment Youwillreceiveanenrollmentworksheet,mailed
toyourhomeaddress,toprepareyoutoenroll.Youcanselectyourbenefitsusingtheemployeewebsite, www.GaBreeze.ga.gov or by accessing theTeamGeorgiaConnection(www.team.ga.gov)byclickingFlexible BenefitsundertheMy Benefitstab,orcallingtheGaBreezeBenefitsCenterat1-877-342-7339.
• Dental Thereisasix-monthwaitingperiodforMajor
servicesundertheSelectPlanandasix-monthwaitingperiodforMajorandOrthoservicesundertheSelectPlusplan.TheDHMOoptiondoesnothavewaitingperiodsorlateenrollmentpenalties,butrequiresthatyouuseaDHMOnetworkprovider. Go to www.cigna.com for a list of DHMOnetworkproviders.
• Spending Accounts YourcontributionstoSpendingAccountswillstart
onthe15thdayofyourfirstfullcalendarmonthofemployment.Formonthlypayrolls,thefullreductionwillbetakenonceamonthafteryourfirstfullcalendarmonthofemployment.Yourtotalcontributionstoeachaccountareproratedbythenumberofmonthsyouparticipateintheseoptions,uptothemaximummonthlyamountallowedforeachaccount.Onceyouenroll,youmaysubmitclaimsforservicesincurredonorafterthefirstofthemonthafteryouhavecompletedonefullcalendarmonthofemployment.
• Long-Term Care Youhaveaone-timeopportunitytosignup
forLong-TermCareinsurancewithoutprovidingevidenceofinsurability.
• Employee Life, Spouse Life, and Child Life Youhaveaone-timeopportunitytochoose
designatedlevelsofemployeeandspouselifeinsurancecoveragewithoutprovidingevidence ofinsurability.PleaseseetheEmployee,Spouse,andChildLifesectionforspecificlimits.
• Employee Critical Illness and Spousal Critical Illness Youhaveaone-timeopportunitytosignupforguaranteedlevelsofCriticalIllnessinsurance,upto$30,000,withoutprovidingevidence of insurability.Coverageforchildrenisincluded withtheEmployeeBenefit.
Youalsohaveaone-timeopportunitytosignupforSpousalCriticalIllnesscoverage,guaranteedupto$30,000,withoutprovidingevidenceofinsurability.

www.GaBreeze.ga.gov
2017 You Decide
6
GeneralEligibilityandEnrollmentInformation• Disability Duringyournew-hireeligibilityperiod,youhave
aone-timeopportunitytosignupforlong-termdisabilitycoveragewithoutprovidingevidenceofinsurability.Ifyoudonotenrollwithinthis30-dayperiod,youwillneedtocompleteanevidenceofinsurabilityform.Yourrequestedlong-termdisabilitycoveragewillnotbecomeeffectiveuntilyourevidenceofinsurabilityisapprovedbyStandardInsuranceCompany(TheStandard).
Duringyournew-hireeligibilityperiod,youhaveaone-timeopportunitytosignupforshort-termdisabilitycoveragewithoutbeingsubjecttoalateentrantwaitingperiod(LateEnrollmentPenalty). Ifyoudonotenrollwithinthis30-dayperiod, youwillbesubjecttotheLateEnrollmentPenalty.
• Other Coverage Therearenomedicalunderwritingrequirements
atanytimeforlegalinsurance,AD&D,spendingaccounts,anddentalandvisionbenefits.
After You Enroll For Coverage
Besuretoconsideryouroptionscarefullywhenyoufirstenroll.IfyoudeclineordropsomeofyourStatecoveragesandwanttopickthemupagaininafutureAnnualEnrollment,youmayhavetoproveinsurabilitythroughmedicalunderwritingtobecoveredagain,orhavetocompletelongerwaitingperiodstoreceivefullbenefits.
When Coverage Begins
Ifyouareanewemployee,yourbenefitselection(s)andanynecessaryformsmustbecompletednolaterthan30daysafteryourhiredate.Yourcoveragewillbeginonthefirstdayofthemonthafteryouhavecompletedafullcalendarmonthofcontinuousemployment.
CoveragefornewoptionsselectedduringAnnualEnrollmentwillbeginonJanuary1stofthefollowingyear,aslongasyouhavemetallcontractualandadministrativerequirements.
Yournewspendingaccountreductionsbeginonthe15thofthemonth;otherpremiumsaretakenat theendofthemonth(forsemi-monthlypayperiods).Thesedatesmaynotapplyifyourdepartmenthasadifferentpayschedule.PleasecheckwithyourHumanResources/PayrollOfficeformoreinformation.Seespecificplandescriptions forinformationaboutwhenyourcoveragebegins.
Confirming Your Choices
Youareresponsibleforselectingthebenefitsyouwantbyeither:• EnteringselectionsontheGaBreezewebsite,or• CallingtheGaBreezeBenefitsCenterand
verbalizingyourselections.
Itiscrucialthatyouprintyourconfirmationandverifyyourselectionsbeforetheendoftheenrollmentperiod.ThebenefitelectionsreflectedontheStatementwillbeineffectfortheentireplanyear.TheConfirmationStatementdoesnotguaranteeyourcoverageforplansthatrequiresubmissionofadditionalinformation.Ifyouhavenotcompletedandsubmittedtheformsorotherinformationrequiredforyourselectedplan(s),thechoicesshownonyourConfirmationStatementmaynotbevalid.

www.GaBreeze.ga.gov
2017 You Decide
7
CompareyourpaycheckstatementswithyourConfirmationStatement.Deductionsshouldmatchtheconfirmedchoices.Shouldyoufindanydiscrepencies,itisyourresponsibilitytonotifyyourHumanResources/PayrollOfficeimmediately.AnychangesinbenefitsmustbeinaccordancewithIRS§125,EmployeeBenefitsPlanCouncilrulesandregulationsandbeapprovedbyplanadministrators.
To Change Your Decisions at Annual Enrollment
EachAnnualEnrollment,youcanchangeyourbenefitdecisionsbasedonwhichoftheavailableoptionsarebestforyouandyourfamily.Remember,thisisanannualagreementallowingtheStatetopurchaseselectedbenefitsforyou,asdescribedinthisbooklet,throughpre-taxpremiums.(Note:notallbenefitsareavailableonapre-taxbasis.)Youwill notbeabletochangebenefitelectionsuntilthe nextAnnualEnrollment–unlessyouhaveaqualifyingchangeinstatus,asdescribedinthe TermsandConditions.
Fornewhires,ifyouhavemadeyourbenefitdecisionsontheGaBreezewebsiteandwishto makeachangewithinyour30-dayenrollmentwindow,youwillneedtocontacttheGaBreezeBenefitsCenterat1-877-342-7339.
To Change Your Decisions Outside of Annual Enrollment
Qualifying Change in Status EventIngeneral,theInternalRevenueServiceprohibitsyoufromchangingcoverageelections,orenrollinginorcancelingcoverageundertheFlexibleBenefitsProgram,outsideofAnnualEnrollment.However,therulesoftheInternalRevenueServiceandtheEmployeeBenefitsPlanCouncildopermityoutochangecoverage,enroll,orcancelcoverageincertainlimitedcircumstances,ifthechangecorrespondstoaqualifyingchangeinstatusevent.
YourrequestforenrollmentorachangeincoverageundertheFlexibleBenefitsProgrammustbeenteredontheGaBreezewebsite,orbycallingtheGaBreezeBenefitsCenter,within30daysafterthequalifyingevent.Therewillbenorefundofpremiumspaidintotheplanwhenatimelychangeisnotmade.
Generally,benefitchangeswillgointoeffectonthefirstdayofthemonthfollowingtherequestwhenthepayrolldeductionischangedtoreflectyournewchoices.Forsomebenefits,however,whenyouchangecoveragebasedontheacquisitionofdependents,theeffectivedateforthecoveragemayberetroactivetothedateofthequalifyingevent,ormaybethefirstofthemonthfollowingtherequesttochangecoverage.
30-Day WindowIfyouhaveaqualifyingchangeinstatus,theIRSallowsyoualimitedperiod–30days–tomakeapplicablebenefitchanges.Inmostcases(e.g.,birthoradoption),ifyoumakeyourbenefitchangeswithinthe30-daywindow,theywillbebackdatedtothedateofthequalifyingevent.Ifyoudonotdosowithin30days,youwillhavetowaituntilthefollowingAnnualEnrollmenttoupdateyourbenefits.
Examples of Qualifying Changes in Status• Marriageordivorce• Birth,adoption,orlegalguardianship• Deathofadependent• LossofspousalcoverageFor more information, see Terms and Conditions, pp. 36-37.
www.GaBreeze.ga.gov
2017 You Decide
8
Separation From Service
• Unpaid Leave Whenyougoonleavewithoutpay,youwill
receiveabillfromGaBreezeforyourbenefitscoverage.Ifyoudonotcontinuepayingthesepremiums,yourbenefitswillbecancelledandyoumaybesubjecttopenaltiesandwaitingperiodswhenyouseektoreinstatethem.YoumayalsoberequiredtowaituntilthenextAnnualEnrollmentperiodtore-enroll.BesuretoreviewPlanDescriptionsforeachoption.UnpaidFamilyMedicalLeave(FML)andMilitaryLeavewillbehandledinaccordancewithapplicablelaws.
• Retirement Itistheemployee’sresponsibilitytocontactthe
providerdirectly,withintherequiredtimeframe,tocontinuecoverageforEmployee/Spouse/ChildLife,AD&D,Long-TermCare,Long-TermDisability,Employee/SpouseCriticalIllness,orLegalInsurance,asapplicable.Ifyouretireandarecurrentlyenrolledindental,yourcoveragewillcontinueautomatically.Ifyouwishtocancelyourdentalcoverage,contacttheGaBreezeBenefits
Center.(Pleasenotethat,oncecancelled,dentalcoveragecannotbereinstated.)Ifyouwish,youmaycontinueyourHealthCareSpendingAccount(HCSA)throughCOBRA.
• Breaks in Employment IfyouleaveactiveStateemploymentbutreturn
withina30-dayperiodduringthesameplanyear,yourpreviousbenefitchoiceswillremainineffectunlessyoureportaqualifyingchangeinstatusevent.IfyouleaveactiveStateemploymentandreturninthesameplanyearbeyonda30-dayperiod,youwillbetreatedasanewhireandmustmakenewbenefitelections.Ifyouretiredandarearehirereturningtoabenefits-eligibleposition,youmustre-electdentalinordertocontinuecoverage.
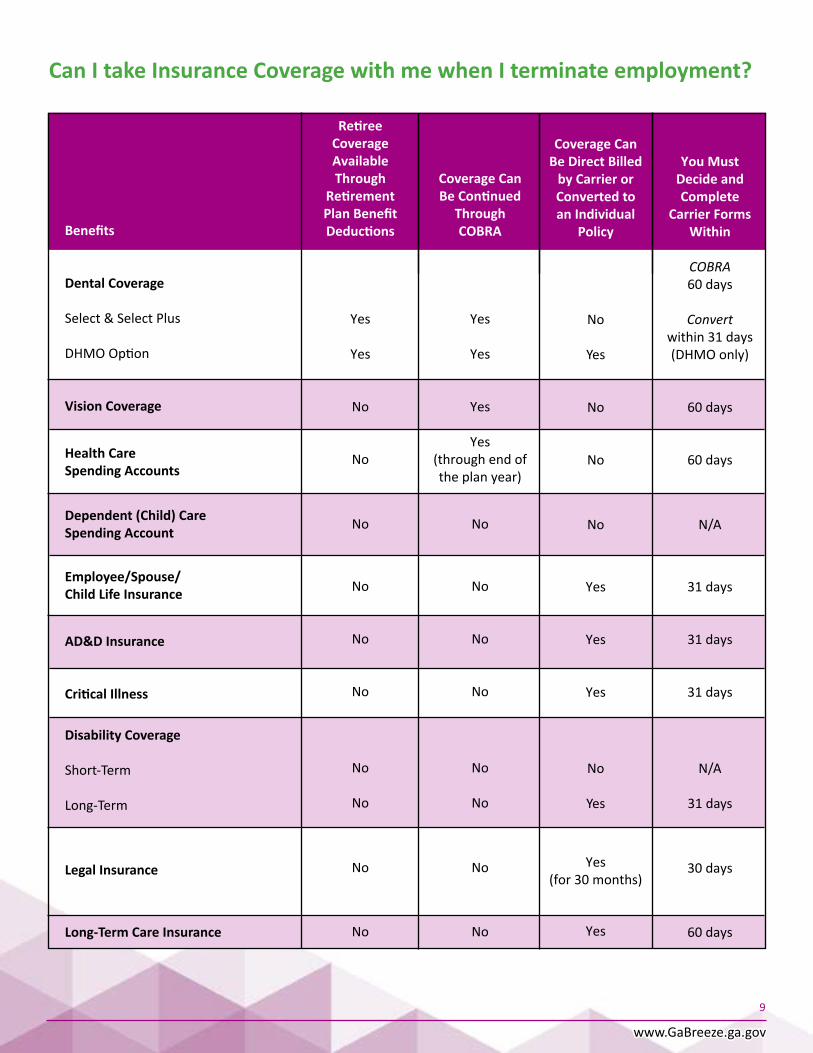
• Termination of Employment IfyoustopworkingfortheState,yourbenefits
typicallyend30daysafteryourmostrecentpremiumorcontributionhasbeenpaid.Seep.9foralistofbenefitseligibletobecontinued,onapost-taxbasis,eitherthroughCOBRAorbyarrangementwithacarrier.
www.GaBreeze.ga.gov
9
Can I take Insurance Coverage with me when I terminate employment?
Benefits
Dental Coverage
Select&SelectPlus
DHMOOption
Vision Coverage
Health CareSpending Accounts
Dependent (Child) Care Spending Account
Employee/Spouse/Child Life Insurance
AD&D Insurance
Critical Illness
Disability Coverage
Short-Term Long-Term
Legal Insurance
Long-Term Care Insurance
Retiree Coverage Available Through
Retirement Plan Benefit Deductions
Yes
Yes
No
No
No
No
No
No
No
No
No
No
Coverage Can Be Continued
Through COBRA
Yes
Yes
Yes
Yes(throughendof theplanyear)
No
No
No
No
No
No
No
No
You Must Decide and Complete
Carrier Forms Within
COBRA 60days
Convert within31days(DHMOonly)
60days
60days
N/A
31days
31days
31days
N/A
31days
30days
60days
Coverage Can
Be Direct Billed by Carrier or Converted to an Individual
Policy
No
Yes
No
No
No
Yes
Yes
Yes
No
Yes
Yes(for30months)
Yes

www.GaBreeze.ga.gov
2017 You Decide
10
YOUR FLEXIBLE BENEFIT OPTIONS
DentalYoucanchooseamongthreedentalplans:• CignaDentalCare®(DHMO)• Delta Dental Select • DeltaDentalSelectPlus
Eachhasdifferentpaymentschedulesandproviders.Closelyreviewtheseplanstodeterminewhichonebestfitstheneedsofyouandyourfamily.Usethecomparisonchartinthisguidetolearnabouttheplans.Duetoavailability,yourbestbenefitoptionmaydependonwhereyouliveorwork,sobesuretochecktheavailabilityofdentistscarefully.Forexample:
• Cigna Dental Care® (DHMO) –designedspecificallyforemployeeswholiveorworkinmetropolitanAtlantaandotherdesignatedareas.
• Delta Dental Select and Delta Dental Select Plus–forotheremployeesthroughoutGeorgia
Cigna Dental Care ® (DHMO) Plan
Cigna Dental Care® (DHMO)planfeatures:
• Nodeductiblestopaybeforeyoucanuse yourplan
• Noannualdollarmaximumsthatlimitbenefits• Noclaimformstofile• NoIDcardsrequiredtoreceivecare• Noagelimitonsealantstopreventcavities• Noreferralsrequiredtovisitanetwork
orthodontistorforchildrenunderseven tovisitanetworkpediatricdentist
TheCignaDHMOisavailabletoemployeeswholiveorworkinmetropolitanAtlantaandotherdesignatedareas.WiththeCignaDHMO,you’llknowexactlywhatyou’llpay(“copays”)forcoveredservices–evenforspecialtycarewithareferralapprovedforpayment.JustchooseageneraldentistfromtheCignaDHMOnetworkatenrollmentandvisitthatdentistforallyourdentalcareneeds.Networkdentistsaren’tallowedtochargeyoumorethantheco-payforcoveredservices.Mostpreventiveservices,suchasexams,x-raysandcleanings,arecovered100%(frequencylimitsmayapply).Dentaltreatments,suchasfillings,crownsandrootcanalsarecoveredatreduced,fixedco-pays.
Keep in mind that there is no out-of-network coverage with a DHMO plan.ButfindinganetworkdentistnearyouiseasywhenyouusetheProvider Directory at www.cigna.comandclickonFind a Doctoratthetopofthescreen.ThenselectIf your insurance plan is offered through work.Next,clickFind a . . . Dentist.Enterthegeographiclocationyouwanttosearch–bycity,state,orzipcode.Clickon Select a Plan, and select Cigna Dental Care HMO undertheDental Planssection.Then,pressChoose. Yourcoveredfamilymemberscaneachselecttheirowngeneraldentists.Afteryouenroll,youcanchangeyourgeneraldentistatanytime–onlineorbyphone.
• Cigna Dental Oral Health Integration Program® Thisprogramreimbursesout-of-pocketcosts
forspecificdentalservicesusedtotreatorhelppreventgumdiseaseandtoothdecay.Theprogramisforpeoplewithcertainmedicalconditionsthatmaybeimpactedbydentalcare.
Theonlyrequirementisthatyou’recurrentlybeingtreatedbyadoctorforheartdisease,stroke,diabetes,headandneckcancerradiation,maternity,chronickidneydisease,ororgantransplant.
ForadditionalinformationregardingCigna’s OralHealthIntegrationProgram,pleasevisit www.cigna.com.

www.GaBreeze.ga.gov
2017 You Decide
11
Cigna Dental Care DHMO Plan
In Network
Reduced,fixed,presetchargesforallcoveredservices.SeeyourpatientChargeScheduleforSpecificCharges(amalgam[silver]fillingsonly)
Reduced,fixed,presetchargesforallcoveredservices.SeeyourpatientChargeScheduleforSpecificCharges(amalgam[silver]fillingsonly)
Reduced,fixed,presetchargesforallcoveredservices.SeeyourpatientChargeScheduleforSpecificCharges
Reduced,fixed,presetchargesforallcoveredservices.SeeyourpatientChargeScheduleforSpecificCharges
NONE
NoMaximum
NoWaitingPeriod
Benefits & Covered Services
Type IDiagnostic&PreventiveServicesOralExams,Cleanings,X-rays,
Type IIBasic Services Fillings,RootCanals,Extractions,Scalingand RootPlanning,RepairstoDentures,Bridges and Crowns Sealants
Type IIIMajorCrowns,Dentures,Bridgework, SurgicalPeriodontal
Orthodontic BenefitsCephalometricX-rays,TreatmentXtudy,Bands,Appliances
Annual Deductible
Maximum Benefits
Waiting Period for Benefits

www.GaBreeze.ga.gov
2017 You Decide
12
Delta Dental Select and Delta Dental Select Plus IfyouchooseaSelectorSelectPlusplanwith DeltaDental:
• Youmaygotoanydentist.
• IfyouvisitaDeltaDentalPPOnetworkdentist,theyacceptreducedfeesforcoveredservices,soyou’llusuallypaytheleastwhenyouvisitaPPOnetworkdentist.ThisprovisionalsoensuresthatDeltaDentalPPOdentistswon’tbalance-billyouthedifferencebetweenthecontractedamountandtheirusualfee.
• Ifyouvisitnon-DeltaDentalnetworkdentists,theycanbalancebillyouthedifferencebetweentheamountofbenefitspayablebyDeltaDental andthedentistchargeforthatservice.
• Note:Orthodontiaservicesforadultsanddependentchildrenareavailableonlythrough theSelectPlusPlan.
Important Information for Select and Select Plus Options
Six (6) Month Wait PeriodAllNewHiresaresubjecttotheSix(6)MonthWaitPeriodforMajor(TypeIII)andOrthodontiaservices(foradultsandchildrenundertheSelectPlusPlan).
Ifacurrentemployeeselectsdentalforthefirsttime,theyandanyeligibledependentswillberequiredtomeettheSix(6)MonthWaitPeriodforTypeIIIandOrthodontiaservices(foradultsandchildrenundertheSelectPlusPlan).
IfanemployeeswitchesfromtheSelecttotheSelectPlusoption,theyandanyeligibledependentswillberequiredtomeettheSix(6)MonthWaitPeriodforTypeIIIandOrthodontiaservices(foradultsandchildrenundertheSelectPlusPlan).
www.GaBreeze.ga.gov
13
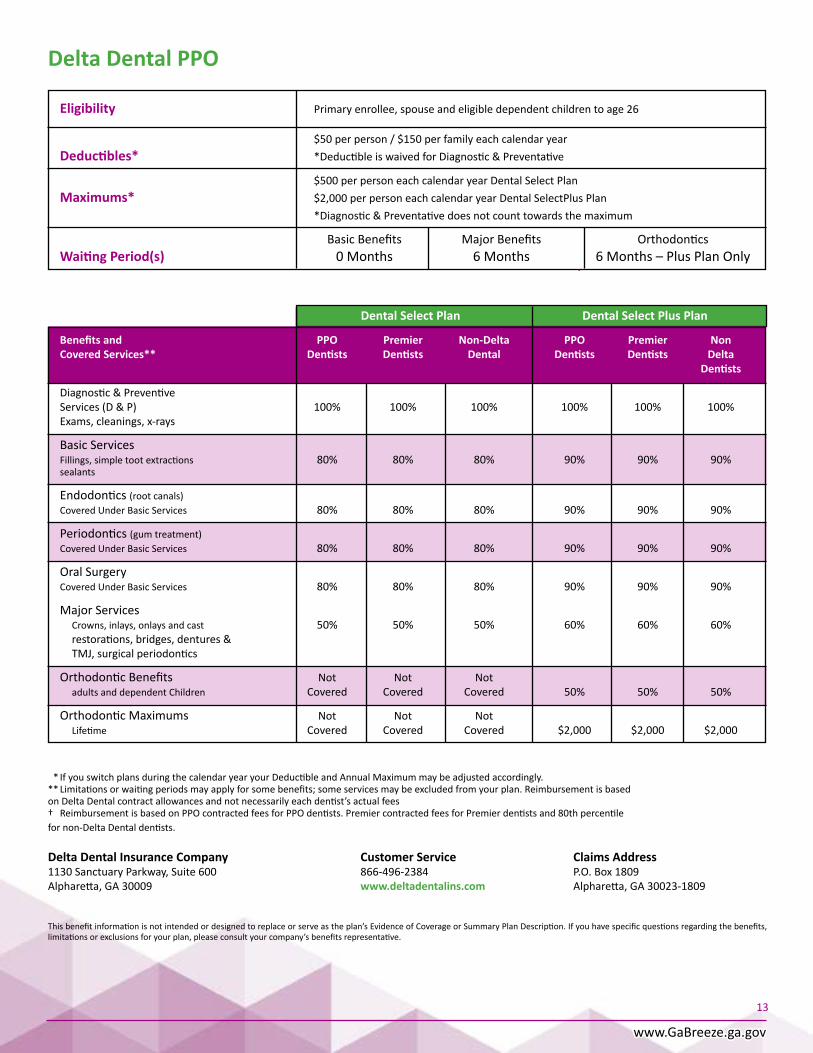
Delta Dental PPO
Eligibility Primaryenrollee,spouseandeligibledependentchildrentoage26
$50perperson/$150perfamilyeachcalendaryearDeductibles* *DeductibleiswaivedforDiagnostic&Preventative
$500perpersoneachcalendaryearDentalSelectPlanMaximums* $2,000perpersoneachcalendaryearDentalSelectPlusPlan *Diagnostic&Preventativedoesnotcounttowardsthemaximum
BasicBenefits MajorBenefits OrthodonticsWaiting Period(s) 0Months 6Months 6Months–PlusPlanOnly
*IfyouswitchplansduringthecalendaryearyourDeductibleandAnnualMaximummaybeadjustedaccordingly.**Limitationsorwaitingperiodsmayapplyforsomebenefits;someservicesmaybeexcludedfromyourplan.Reimbursementisbased onDeltaDentalcontractallowancesandnotnecessarilyeachdentist’sactualfees† ReimbursementisbasedonPPOcontractedfeesforPPOdentists.PremiercontractedfeesforPremierdentistsand80thpercentile fornon-DeltaDentaldentists.
Delta Dental Insurance Company Customer Service Claims Address1130SanctuaryParkway,Suite600 866-496-2384 P.O.Box1809Alpharetta,GA30009 www.deltadentalins.com Alpharetta,GA30023-1809
Thisbenefitinformationisnotintendedordesignedtoreplaceorserveastheplan’sEvidenceofCoverageorSummaryPlanDescription.Ifyouhavespecificquestionsregardingthebenefits,limitationsorexclusionsforyourplan,pleaseconsultyourcompany’sbenefitsrepresentative.
Dental Select Plan Dental Select Plus Plan
Benefits and PPO Premier Non-Delta PPO Premier Non Covered Services** Dentists Dentists Dental Dentists Dentists Delta Dentists
Diagnostic&Preventive Services(D&P) 100% 100% 100% 100% 100% 100% Exams,cleanings,x-rays
Basic Services Fillings,simpletootextractions 80% 80% 80% 90% 90% 90% sealants
Endodontics(rootcanals) CoveredUnderBasicServices 80% 80% 80% 90% 90% 90%
Periodontics(gumtreatment) CoveredUnderBasicServices 80% 80% 80% 90% 90% 90%
OralSurgery CoveredUnderBasicServices 80% 80% 80% 90% 90% 90%
MajorServices Crowns, inlays, onlays and cast 50% 50% 50% 60% 60% 60% restorations,bridges,dentures& TMJ,surgicalperiodontics
OrthodonticBenefits Not Not Not adultsanddependentChildren Covered Covered Covered 50% 50% 50%
OrthodonticMaximums Not Not Not Lifetime Covered Covered Covered $2,000 $2,000 $2,000

www.GaBreeze.ga.gov
2017 You Decide
14
VisionVisioncoverageisavailablethroughBlueCrossBlueShieldofGeorgia.Youhaveachoicebetweentwoplanoptions–VisionSelectPlanandVisionSelectPlusPlan.Bothplansofferthesefeatures:• Coveredexamsandmaterials• Statewideaccesstoanetworkofproviders• Noclaimstofilefor“in-network”benefits• Benefitsfor“out-of-network”providers.
TheBlueCrossBlueShieldorGeorgiaVisionCareparticipatingprovidernetworkincludesbothprivatepracticeophthalmologistsandretailchains.Manyproviders–includingretailchains–areopeneveningsandweekends.ParticipatingretailchainprovidersincludeLensCrafters,TargetOptical,JCPenneyOptical,SearsOptical,Walmart,PearleVision,and1-800-Contacts,amongothers.
Tolocateparticipatingprivateproviders,justgotowww.bcbsga.com:• ClickFind a Doctor• ChooseyourState(GA)• Scroll down to Vision and select Blue View Vision.
Your Plan Options
• Vision Select Plan TheVisionSelectPlancoversstandardsingle
visionandstandardlinedmulti-focallensesforglasses.Cosmeticlensoptions,suchastinting,UVcoating,andtransitionallensesarenotcovered,butareavailableatdiscountedrates.
Certainstandardcontactlenses,includingdailywear,anduptofourboxesofstandardsinglevisiondisposablecontacts,arecoveredinfullbycopays.UndertheVisionSelectPlan,ifyoupurchasecontactsthatarenotamongBlueCrossBlueShieldofGeorgiaVision’s“coveredinfull”selection,youwillreceiveanannual$105allowancetowardthepurchaseofcontactlenses,andprofessionalservices(e.g.,fitandfollow-up).
Toreceivethefull$105allowanceundertheVisionSelectPlan,youmustreceiveyourexam,fitting,andevaluationduringasinglevisittothesamenetworkprovider.Theallowancewillapplyonlytoonepurchaseperplanyear.
Ifyouuseanon-networkprovider,youmustsubmitallreceiptsatthesametime.Anybalanceremaining,andnotusedduringtheplanyearwhenthepurchaseoccurred,willbeforfeited.
• Important Information for the Vision Select Plan Benefitsareprovidedevery12monthsforexams,
lensesand/orcontacts,andforframes,basedonthelastdateofservice.Theout-of-networkallowanceforcontactlensesis$105.
Note:Benefitservicelimitationsarecalculatedonacalendaryear.Example:ifyoureceiveexamservicesinMarch,youwillbeeligibletoreceiveanotherexaminJanuaryofthefollowingyear.
Ifyouchoosecontactlenses,nobenefitswillbeavailableforcoveredeyeglasslensesduringthatperiod.

www.GaBreeze.ga.gov
2017 You Decide
15
* If you choose contact lenses, no benefits will be available for covered eyeglass lenses during that period.
Vision Select Plan
COVERED SERVICES COPAYMENTS/MAXIMUMS
Network Providers Non-Network Providers
Eye ExamLimitedtooneexamper $10Copayment Reimbursedupto$40 MembereveryCalendarYear
Prescription Lenses $20CopaymentLimited to one set of lenses perMembereveryCalendarYear
Basic Lenses (Pair)• SingleVisionlenses Reimbursedupto$40• Bifocallenses Reimbursedupto$60• Trifocallenses Reimbursedupto$80• Lenticularlenses Reimbursedupto$80
Includes:• Factoryscratchcoating• Tint(solidandgradient)• PolycarbonateandPhotochromic
lenses(forchildrenunderage19)• UVcoatings
FramesLimitedtoonesetofframes NoCopayment Reimbursedupto$45perMembereverytwoyears AllowableAmountupto $130retailallowance
Prescription Contact Lenses* No Copayment (traditionalordisposable)
• Non-ElectiveContactLenses Coveredinfull Non-Networkproviders (OnceeveryCalendarYear) arereimbursedupto$210
• ElectiveContactLenses NoCopayment Non-Networkproviders (OnceeveryCalendarYear) $105retailallowance arereimbursedupto$105

www.GaBreeze.ga.gov
2017 You Decide
16
• Vision Select Plus Plan InadditiontothecoverageintheVisionSelect
Plan,theVisionSelectPlusPlanofferscosmeticlensoptionsforTints,UV,Polycarbonate,andBasicProgressivelenses.
Toreceivethefull$200allowanceundertheVisionSelectPlusPlan,youmustreceiveyourexam,fitting,andevaluationduringasinglevisittothesamenetworkprovider.Theallowance willapplyonlytoonepurchaseperplanyear. Youmustsubmitallreceiptsatthesametime. Anybalanceremaining,andnotusedduring theplanyearwhenthepurchaseoccurred, will be forfeited.
• Important Information for the Vision Select Plus Plan
BenefitsareprovidedeveryCalendarYearforexams,lensesand/orcontacts,andforframesmeasuredfromthelastdateofservice.Theout-of-networkallowanceforcontactlensesis$200.
Note:Benefitservicelimitationsarecalculatedonacalendaryear.Example:IfyoureceiveexamservicesinMarch,youwillbeeligibletoreceiveanotherexaminJanuaryofthefollowingyear.
IfyouchoosecoveredNon-ElectiveContactLensesorElectiveContactLenses,nobenefitswillbeavailableforcoveredeyeglasslensesinthatperiod.

www.GaBreeze.ga.gov
2017 You Decide
17
* If you choose contact lenses, no benefits will be available for covered eyeglass lenses during that period.
Vision Select Plus PlanCOVERED SERVICES COPAYMENTS/MAXIMUMS
Network Providers Non-Network Providers
Eye ExamLimitedtooneexamper $10Copayment Reimbursedupto$40MembereveryCalendarYear
Prescription LensesLimited to one set of lenses per MembereveryCalendarYear Basic Lenses (Pair) $25Copayment• SingleVisionlenses Reimbursedupto$40• Bifocallenses Reimbursedupto$60• Trifocallenses Reimbursedupto$80• Lenticularlenses Reimbursedupto$80
Includes the following Lens Options: • Factoryscratchcoating• UVcoating• Tint(solid&gradient)• Polycarbonatelenses• TransitionsPhotochromiclenses• Standard&PremiumProgressivelenses• StandardAnti-Reflectivecoating(Not
CoveredForNon-NetworkProviders) Frames Limitedtoonesetofframes NoCopayment Reimbursedupto$45perMembereveryCalendarYear AllowableAmountupto $150retailallowance
Prescription Contact Lenses* (traditionalordisposable) NoCopayment
• Non-ElectiveContactLenses Coveredinfull Non-Networkproviders (OnceeveryCalendarYear) arereimbursedupto$210
• ElectiveContactLenses NoCopayment Non-Networkproviders (OnceeveryCalendarYear) $200retailallowance arereimbursedupto$200
Still have questions? PleasecontactGeorgiaBreezeorBlueCrossBlueShieldofGeorgiaVisionCustomerServiceat1-855-556-4844.

www.GaBreeze.ga.gov
2017 You Decide
18
Employee, Spouse, Child Life, and Accidental Death & Dismemberment Insurance Ifyouwantlifeinsuranceprotection,orwanttosupplementthecoverageyoualreadyhave,you maychooseMetLifegrouptermcoverageunder theFlexibleBenefitsProgram.Theamountyou selectispaidtothebeneficiariesyounameto receivethesebenefitsshouldyoudiewhilethiscoverageisineffect.
Your 2017 Annual Enrollment• Employee Life Coverage–abilitytoelectbenefits
ofoneto10timesyourpay,upamaximumbenefitof$2,000,000.YouhavetheoptiontopaypremiumsforEmployeeLifeonapre-taxorpost-taxbasis.(Note:Coverageisreducedstartingatage65.)
Note:During2017AnnualEnrollment,youmayincreaseyourcoveragebyone-timespay,guaranteed,withouthavingtoprovideevidence ofinsurability.
• Premium Waiver–providescontinuationofEmployeeLifeinsuracewithoutpremiumpaymentshouldyoubecomedisabled.
• Will Preparation Service–allowsyoutoconsult,inpersonorviaphone,withaparticipatingHyattLegalplanattorney,whowillcompleteawill,livingwill,orpowerofattorneyforyouandyourlegalspouse,atnochargetoyou.
• Estate Resolution Services–givesyourbeneficiariesthesupportofaHyattLegalplanattorney,in-personorviatelephone,todiscussmattersrelatedtoprobatingyourestate.
If You are a New Employee
Asanewhire,youhaveaone-timeopportunitytoelectcertainlevelsofemployeeandspouselifeinsurance,guaranteed,withouthavingtoprovideevidenceofinsurability.
Coverageforyouisavailableinincrementsofyourpay–fromoneto10timespay,upto$2,000,000.Amountsofone-timespay,upto$200,000,areissued,guaranteed.Higherlevelsofcoveragewillbesubjecttoevidenceofinsurability.
Childlifeinsuranceandupto$30,000ofspouselifecoverageisalsoavailable,guaranteed,withoutneedtoprovideevidenceofinsurability.
• Spouse Life Insurance Ifyouchooseemployeelifeinsuranceforyourself,
youmayalsoselectcoverageforyourspouse.Spouselifeinsurancepremiumsarebasedon thecoveragelevelandyourage.YourpremiumsforSpouseLifearepaidonanpost-taxbasis. (Ifyouare65orolder,theamountofyourspouselifecoverageisreduced.)
SpouseLifecoveragecannotexceed100%ofyouramountofEmployeeLifecoverage.
Youarethebeneficiaryofspouselifeinsurancecoverageandwillreceivetheinsurancebenefit intheeventofyourspouse’sdeath.
• Child Life Insurance Ifyouchooselifeinsuranceforyourself,you
mayalsoelectchildlifeinsuranceforyourchild(ren)underage26.Thiscoverage,whichisissuedguaranteed(withoutneedformedicalunderwriting),ispaidforonanpost-taxbasis.
www.GaBreeze.ga.gov
2017 You Decide
19
Important Notes about Child Life: Childcoveragebeginsatlivebirth.Coveragefromlivebirthtosixmonthsisthelesseroftheelectedamountor$6,000.Fromsixmonthsofagetoage26,thefullelectedamountapplies.
• ChildLifecoveragecannotexceedyouramountofEmployeeLifebenefits.
• Youarethebeneficiaryofchildlifeinsurancecoverageandwillreceivethebenefitintheeventofthechild’sdeath.
• Accidental Death and Dismemberment Insurance TheFlexibleBenefitsProgramoffersaccidental
deathanddismemberment(AD&D)insurancetobepaidtoyouoryourbeneficiaryifyourinjuryordeathistheresultofacoveredaccident.Incaseofpermanentandtotaldisability,youareeligibleforAD&Dbenefitsifyourinjurypreventsyoufromworkingatanyjobforwhichyouarequalifiedbyeducation,training,orexperience.
Youmayelectcoverageinincrementsofyourpay
–fromoneto10timespay,upto$2,000,000.YourpremiumsforAD&Darepaidonapre-taxbasis.(Ifyouareage75orolder,thiscoverageisreduced.)
• Important Notes about Employee, Spouse, Child Life and AD&D Insurance
ThelifeandAD&DinsuranceamountsyouchoosewillbebasedonyourAnnualBenefitBaseRateasofOctober1.Thisamountisroundeduptothenexthigher$1,000,afteryoumultiplyyourcoverageandadjustforagereductions.
Ifyourcoverageselectionrequiresmedicalunderwriting,youwillneedtocompletetheonlineMetLifeStatementofHealthForm alongwithanyotherrequiredinformation.MetLifemustapproveyourapplicationbeforecoveragecantakeeffect.
Besuretodesignateyourbeneficiariesby
accessingtheGaBreezewebsiteorcallingtheGaBreezeBenefitsCenter.Also,youcanchangeandupdateyourbeneficiariesatanytime.
Please be advised.NopaperStatementofHealthFormwillbemailedfortheemployeeand/orthespousetocomplete.Anonlinepre-registrationprocesswillneedtobecompletedforaspouserequiringmedicalunderwritingbeforetheStatementofHealthFormwill be available online.
• ForinformationregardingconversionandportabilityofyourEmployeeLife,SpouseLife,ChildLifeinsurance,andAD&Dinsurances,contactMetLife,toll-free,at1-877-255-5862.
www.GaBreeze.ga.gov
2017 You Decide
20
Short and Long-Term DisabilityTohelpprovideincomeprotectionagainsttheunexpected,theFlexibleBenefitsProgramallows youtochoose:• Short-TermDisabilityinsuranceand/or• Long-TermDisabilityinsurance.
Short-Term Disability with Standard Insurance Company
Ifyouchooseshort-termdisability(STD)coverage,theplanwillworkincoordinationwithotherincomebenefitstoreplace60%ofyourAnnualBenefitBaseRateduringtheplanyearthedisabilitybegan,upto$1,000perweek.Ifyoureceiveotherbenefits(includingbutnotlimitedtoworkers’compensation,otherdisabilityplansand/orprogramsincludingtheStateretirementsystems,earningsfromworkyouperformwhiledisabled)whichreplaceatotalof60%ormoreofyourAnnualBenefitBaseRate,theshort-termdisabilityplanwillnotpayabenefitforthisdisability.
Your Options• Seven(7)DayBenefitWaitingPeriod• Thirty(30)DayBenefitWaitingPeriod
• How STD Works A late enrollment penalty will apply for late
entrantstotheSTDplan(employeeswhodo notelectSTDwithin30daysofemployment).
YourSTDbenefitsarecalculatedontheAnnualBenefitBaseRatethatisineffectduringtheplanyearyourdisabilitybegan,lessotherincomebenefits.Forexample,ifyourfirstdayofdisabilityisDecember3,2016,yourdisabilitybenefitwillbecalculatedfromthe2016AnnualBenefitBaseRate,notyour2017AnnualBenefitBaseRate.The2016AnnualBenefitBaseRateisbasedonyour
weeklyrateofearningsineffectonOctober1,2016,oryourhiredate,ifafterthisdate.
YourSTDbenefitscancontinueuntilyourecover,cease to be disabled, or are disabled for a maximumof150calendardaysoramaximumof173calendardays(dependingonthecoveragelevelyouhavechosen).
• What Is A Late Enrollment Penalty For Late Entrants?
Anemployeechoosingcoverageforthefirsttimemorethan30daysafterbeginningemploymentis considered a late entrant. For STD late entrantswhobecomedisabledduetophysicaldisease,pregnancy,ormentaldisorderduringthe12-monthperiodafterthedateyourSTDinsurancebecomeseffective,benefitswillnotbeginuntilafteryouhavebeencontinuouslydisabledfor60days,unlessyouhavebeeninsuredforatleast12consecutivemonths.ForSTDlateentrantswhosedisabilitiesbeginafterthis12monthperiod,benefitswillstartafterthebenefitwaitingperiod(sevenor30continuouscalendardays,asapplicable)issatisfied.
Whenchangingfromthe30-dayBenefitWaitingPeriodtotheseven-dayBenefitWaitingPeriod,yourBenefitWaitingPeriodforadisabilityresultingfromphysicaldisease,pregnancy,ormentaldisorderwillbeextendedto30days,untilyouhavebeeninsuredundertheseven-dayBenefitWaitingPeriodforatleast12consecutivemonths.Thisdoesnotapply toaccidentalinjuries.
• Enrolling For Short-Term Disability Coverage Yourpremiumswillbebasedonyourage,
coveragelevel,andAnnualBenefitBaseRate.Thispremiumisapost-taxdeduction–soyouwon’tpaytaxesonthebenefitsyoureceive.
NOTE: YoushouldcheckwithyourHumanResourcesOfficeand/ormanagerconcerningleavepolicieswhendisabled.AgencypolicymayimpactyoureligibilitytoreceiveShort-TermDisabilitybenefits.
www.GaBreeze.ga.gov
2017 You Decide
21
Long-Term Disability with Standard Insurance Company
TheFlexibleBenefitsProgram’sLong-TermDisability(LTD)coverageworkswithotherbenefitsyouareeligibletoreceive,includingbutnotlimitedtoSocialSecurity,Workers’Compensation,otherdisabilityplansbenefitandprograms,includingtheStateretirementsystems.Theplanassuresthatyourcombineddisabilitybenefitsandincomefromothersourceswillequal60%ofyourAnnualBenefitBaseRateupto$5,000permonth.Thereisaminimummonthlybenefitof$100.00.
• How Long LTD Benefits May Be Payable Ifyouqualifyforbenefits,theywillbeginafter
youhavebeendisabledfor180calendardays. LTDbenefitsendwhenyouarenolongerdisabledoryoureachyourSocialSecurityNormalRetirementAge.Benefitsfordisabilitiescausedbymentaldisorders,substanceabuseandotherlimitedconditionswillnotbepaidformorethantwoyears.Ifyoubecomedisabledafterreachingage61,anage-gradedmaximumbenefitperiodwill apply.
• Enrolling For Long-Term Disability Coverage Yourcostforlong-termdisabilitycoverageisbased
onyourage,yourFICAStatus,AnnualBenefitBaseRate,andwhetherornotyouareeligiblefordisabilitycoveragethroughanyStateofGeorgiaretirementplan,and/orthroughSocialSecurity.
LTDpremiumsarepaidwithpost-taxdollars.Anybenefitsyoureceivearenotconsideredtaxableincome.
Notethatotherexclusionsandlimitationsapplytothesecoverages.RefertotheCertificatesofInsuranceformoreinformation.
Ifyouhaveanyquestionsabouteligibilityorhowtheshort-termandlong-termdisabilityinsuranceplanswork,callTheStandardat1-888-641-7186.

www.GaBreeze.ga.gov
2017 You Decide
22
Long-Term CareLong-Term Care Insurance with Unum
Long-TermCare(LTC)referstoawiderangeofpersonalcare,health,andsocialservicesforpeopleofallageswhosufferachronicdiseaseorlong-lastingdisability.Theseservicescanbeprovidedinanursingfacility,anadultdaycarecenter,orathome,andcaninvolvesomenursingcare.Thecostforthiskindofcareistypicallyveryhigh–asmuchas$20,000peryearforhomecare,andfrom$20,000to$60,000annuallyforanursinghome.Generally,youhavetopaytheseexpensesoutofyourownpocket,becausemedicalinsuranceandMedicaredonotcoverlong-term care.
• Your Long-Term Care Options Youcanchoosefromoneofthreedailybenefit
levelsandthecorrespondingmonthlypremiumthatisrightforyourneedsandbudget.Theamountofthebenefitdependsontwofactors:wherecareisprovided–eitherinanursingfacility,orhome/day/assistedlivingfacility–andthedailydollarlevelofcoverageyouselect.Withanyoftheseoptions,benefitsarepaidonamonthlybasis.Themonthlybenefitisequalto100%ofyourelecteddailybenefitamountforcareprovidedinastate-licensednursinghomefacility,and60%ofyourelecteddailybenefitamountforcare provided in an assisted living facility or at home.Ifyouwish,youcanaddareducedpaid-upoptionand/oraninflationprotectionoption.
• Who Can Be Covered Thisplanisofferedtoyou,yourspouse,your
parents,oryourparents-in-law.“Parents”arebiological(natural),adoptive,orstep-parentsofeligibleemployeesorspouses.Yourspouse,parents,andparents-in-lawwillhavetocompleteamedicalunderwritingprocessandbeapprovedforLTCcoverage.Yourfamilymembers’premiumswillbebilleddirectlybyUnum.Yourpayrolldeductionwillbeforyourindividualcoverageonly.Youcanelectspouseorfamilycoverageevenifyoudonotenroll.
• When Benefits Are Paid Benefitsbeginaftera90-dayeliminationperiod
inwhichyouoracoveredfamilymemberhasaneligiblephysicalorcognitivedisability.Youqualifyforbenefitsifthedisabilitycreatesaneedforyoutoreceivecontinualhelpfromanotherpersontocarryoutanythreeofthesixactivitiesofdailyliving:bathing,dressing,toileting,transferring,continence,andeating.Becauselong-termcarepremiumsaretakenfromyourpost-taxincome,benefitsareprovidedtax-free.
• Please note: Apre-existingconditionlimitationwillapplytocoveragepurchasedonaguaranteed-issuebasis.Itwillnotapplytocoveragethatismedicallyunderwritten.Ifapre-existingconditionlimitationapplies,andlossiscausedby,contributedto,orresultsfromapre-existingconditionpresentsixmonthsbeforetheeffectivedateofcoverage,andoccursduringthefirstsixmonthsaftercoveragebegins,nobenefitwillbepayableuntilboththesix-monthperiodandthewaitingperiodhavebeenfulfilled.

www.GaBreeze.ga.gov
2017 You Decide
23
SpecifiedIllness• About Your Premiums and Enrolling YoupayforyourLTCcoverage,throughthe
convenienceofpayrolldeduction,withpost-taxdollars.Usingpost-taxpremiumdollarspermitsthebenefitsyoureceivetobepaidtax-free.PremiumcostsarebasedonyourageasoftheBenefitCalculationDate(October1)oryourhiredate,whicheverislater.Theyoungeryouarewhenyoupurchasethiscoverage,theloweryourpremiums.Yourfamilymembers’premiumsarebasedontheirageasofthedatetheyapplyforcoverage.TheywillpaypremiumsdirectlytoUnum.
IfyouareanewemployeeandenrollinLTCinsuranceduringyourinitialenrollmentperiod,youmayselectLTCwithnomedicalunderwritingrequirements.IfyouareacurrentemployeeenrollinginLTCforthefirsttime,oranemployeecurrentlyenrolledwhowantstoincreasebenefitlevels,addoptions,orarere-enrollingafterdiscontinuingcoverage,medicalunderwritingwillberequired.Coverageforyourspouseandothereligiblefamilymemberswillbemedicallyunderwritten.
Formoreinformationaboutlong-termcarecoverage,visit www.unuminfo.com/sogorcallUnumat1-888-SOG-FLEX(1-888-764-3539).
www.GaBreeze.ga.gov
2017 You Decide
24
Critical IllnessCritical Illness Plan with Aflac/CAIC
Thegroupcriticalillnessplanhelpsyouandyourfamilycopewith,andrecoverfrom,thefinancialstressofacriticalillnessorhealthcondition.
Employee Coverage Levels$5,000 $10,000 $20,000$30,000 $40,000 $50,000 • Lump-sumbenefitsarepaiddirectlytotheinsured
followingthediagnosisofeachcoveredcriticalillnessafteryouarehospital-confinedforsaidcondition.
• Ratescannotbeindividuallyincreasedduetochangeinage,health,orindividualclaim.
• Nomedicalunderwritingisrequiredforupto$30,000incoverage,andsimplifiedmedicalunderwriting,withonlyafewhealthquestions, forhigheramounts.
• Theplanisportable,subjecttocertainstipulations,soyoumaybeabletotakeyourcoveragewithyouifyouleaveyourjob.
• Benefitswillnotreduceduetoage.
Spouse Coverage Levels$5,000 $10,000 $20,000$30,000 $40,000 $50,000
• Nomedicalunderwritingisrequiredforupto$30,000incoverage,withsimplifiedmedicalunderwriting(onlyafewhealthquestions)forhigheramounts.
• EmployeemustelectCriticalIllnessbenefitsforthespousetobeeligibleforcoverage.
• Ratesarebasedontheemployee’sage.
Child Coverage• Allyourchildren,ages0-26,arecoveredat50%of
yourbenefitamount,atnoadditionalcost.• Childbenefitsareautomaticallyincludedin
existingemployeecoverage.
Dependent Child Illnesses Covered at 100% of Maximum Benefit• CysticFibrosis• CerebralPalsy• CleftLiporCleftPalate• Down Syndrome• SpinaBifida
Covered Critical Illnesses*Illnesses Covered Percentage of Face Amount• Heartattack 100%• Stroke 100%• Majororgantransplant 100%• Renalfailure(endstage) 100%• Internalcancer 100%• Coma 100%• Severeburns 100%• Paralysis 100%• Lossofsight,hearing,orspeech 100%• Carcinomainsitu 25%• Coronaryartery 25%• AdvancedAlzheimer’sdisease 25%
* A partial benefit (25%) is payable for carcinoma in situ and coronary artery bypass surgery. Payment of the partial benefit for carcinoma in situ will reduce the benefit for internal cancer. Payment of the partial benefit for coronary artery bypass surgery will reduce the benefit for a heart attack.

www.GaBreeze.ga.gov
2017 You Decide
25
First Occurrence BenefitAfterreceiptofwrittenproofofloss,aninsuredmayreceiveupto100%ofthebenefitselecteduponthefirstdiagnosisofeachcoveredcriticalillness.
Additional Occurrence BenefitIfaninsuredindividualcollectsfullbenefitsforacriticalillnessundertheplan,andlaterhasoneoftheremainingcoveredillnesses,thefullbenefitamountforanyadditionalillnesswillbepaid.Thetwodatesofdiagnosismustbeseparatedbyatleast90days(or,forcancer,afteratleast12monthstreatment-free).Additionalcriticalillnessescannotbecaused,orcontributedto,byacriticalillnessforwhichbenefitshavealreadybeenpaid.
Re-Occurrence BenefitOncebenefitsarepaidforacriticalillness,additionalbenefitsarepayableforaneweventofthesamecriticalillness,providedthereoccurrenceisdiagnosedatleast90daysfromthedateofinitialdiagnosis.
• Cancerreoccurrence:Theinsuredmustbetreatment-freefor12monthstoreceivetheReoccurrenceBenefitforacancerdiagnosis.
• Cancerthathasspread(metastasized),evenifthereisanewtumor,willnotbeconsideredanadditionaloccurrenceunlesstheinsuredhas beentreatment-freefor12months.
Health Screening BenefitsAcoveredemployeecanreceiveamaximumof$100for any single covered screening test per calendar year.Thisbenefitispaidregardlessoftheresultsofthetestandwillnotreducetheamountpayableforthediagnosisofacriticalillness.Thereisnolimittothenumberofyearsthecoveredemployeecanreceivethehealthscreeningbenefit;itwillbepaidaslongasthepolicyremainsinforce. Thecoveredhealthscreeningtestsinclude:
• Stress test on a bicycle or treadmill• Fastingbloodglucosetest,bloodtest
fortriglyceridesorserumcholesterol testtodeterminelevelofHDLandLDL
• Bonemarrowtesting• Breastultrasound• CA15-3(bloodtestforbreastcancer)• CA125(bloodtestforovariancancer)• CEA(bloodtestforcoloncancer)• Chestx-ray• Colonoscopy• Flexiblesigmoidoscopy• Hemocultstoolanalysis• Mammography• Papsmear• PSA(bloodtestforprostatecancer)• Serumproteinelectrophoresis
(bloodtestformyeloma)• Thermography
www.GaBreeze.ga.gov
2017 You Decide
26
Critical Illness Select Plus Plan
IncludesAccidentBenefitsforyouandyourfamily intheeventofanonoroffthejobaccidentalinjury.
• Indemnitybenefitspaidastheresultofanaccidentalinjury
• 24-hourcoverage• Over50accidentindemnitybenefitsincluded• Nomedicalunderwritingrequiredupto
GuaranteedIssueamount• Ratescannotbeindividuallyincreaseddueto
changeinage,healthorindividualclaim• Theplanisportable,subjecttocertain
stipulations,soyoumaybeabletotakeyourcoveragewithyouifyouleaveyourjob
• WellnessBenefitof$60
Plan Benefits SummaryPleaserefertoyourcertificateofcoverage fordefinitions,limitationsandexclusions
BenefitsInclude:• MedicalFees(PhysicianCharges,X-Rays,
EmergencyRoomServicesandSupplies)• HospitalFees(HospitalAdmission,DailyHospital
ConfinementandIntensiveCare)• AccidentalInjuries(Fractures/Dislocations,
Lacerations,Tendons/Ligaments,RupturedDisk,TornKneeCartilage,Burns,EyeInjuries)
• AccidentFollow-upBenefits(PhysicalTherapy, In-patientRehab,Follow-uptreatments)
• AdditionalBenefits(FamilyLodging,Transportation,GunshotWound,Paralysis,Prosthesis)
For a complete list of benefits and descriptions, please refer to the Critical Illness Select Plus PDF Brochure or your certificate of coverage
Premiums for the Critical Illness coverages in this section are paid on a post-tax basis – which allows you to receive benefits tax-free
www.GaBreeze.ga.gov
2017 You Decide
27
Legal InsuranceLegal Insurance with Hyatt Legal Plans
Whetheryou’rebuyinganewhome,drawingupawill,orjustneedsomelegaladvice,theHyattLegalPlancangiveyouaccesstoexperienced,localnetworkattorneysatanaffordablerate,throughpremiumstakenonapost-taxbasis.
Legal BenefitsThelegalservicescoveredbytheplan,asdefinedbyyourSummaryPlanDescription(SPD),arefullycoveredwhenyouseeaParticipatingPlanAttorney.Youcanusetheplanasoftenasyouneedlegalrepresentation,withoutwaitingperiods,copayments,ordeductibles.
Access to Over 14,000 AttorneysTheHyattLegalPlanprovidesmemberswithaccesstoanationalnetworkofmorethan14,000PlanAttorneys.Ifyouprefer,youmayuseyourownattorneyandbereimbursedaccordingtoasetfeeschedule.IfyoufindyourselfinneedoflegalassistancewhiltetravelingwithintheU.S.,calltheHyattClientServiceCenterat800-821-6400,visit www.info.legalplans.com,ordownloadHyattLegalPlan’smobileapptolocateparticipatingattorneysinthearea.
Your Legal Benefit OptionsReviewthecoveragesbelowandonthefollowingpageandselecttheplanthatfitstheneedsofyouandyourfamily.Youcanenrollineitherplanwithsinglecoverageorcoverageforyouandyourdependents(uptoage26).
Select Plan
TheSelectoptionprovidesbenefitsforthe followingservices:
• Wills and codicils• Living wills• Powersofattorney• Unlimitedphoneandofficeadvice
andconsultations• Trafficticketdefense(noDUI)• Documentreview• Deeds• Mortgages• Promissorynotes• Elderlawmatters• Sale,purchaseandrefinancingofyour
primaryandsecondhome• Homeequityloansforyourprimary
andsecondhome• Debtcollectiondefense• Identitytheftdefense
www.GaBreeze.ga.gov
2017 You Decide
28
Select Plus Plan
TheSelectPlusoptionprovidesbenefitsforthefollowingservices:
• Wills and codicils• Living wills• Powersofattorney• Unlimitedphoneandofficeadvice
andconsultations• Probateproceedings• Consumerprotectionmatters• Debtcollectiondefense• Identitytheftdefense• Personalbankruptcy• Taxaudits• Civillitigationdefense• Administrativehearings• Incompetency defense• Changeorestablishmentofcustodyorder
orvisitationrights• Adoptionandlegitimization• Divorce*($1,000maximumforcontested)• Enforcementormodificationofsupportorder• Guardianship/conservatorship• Immigrationassistance• Trafficticketcefense(noDUI)• Sale,purchase,refinancingofyourprimaryand
secondhome• Evictionandtenantproblems(tenantonly)• Homeequityloansforprimaryandsecondhome• Namechanges
• Juvenilecourtdefense• Deeds,promissorynotes&mortgages• Documentreview• Elderlawmatters• Securitydepositassistance(tenant)• Protectionfromdomesticviolence
TheSelectPlusoptionoffersthesameservicesastheSelectPlan,plusadditionalservicesinfamilylaw,debtmatters,consumerprotection,tenantmatters,immigration,andcivillitigationdefense.
What Are the Exclusions?Thelegalplanexcludesappeals;classactionsandappeals;mattersthatHyattLegalPlansdeemfrivolous,non-meritorious,orunethical;farmandbusinessmatters;patent,trademark,andcopyrightmatters;costsandfines;mattersforwhichanattorney-clientrelationshipexistpriortoyourbecomingeligibleforplanbenefits,andanyemployment-relatedmatters.Foracompletelistofexclusions,visitwww.GaBreeze.ga.gov.
What if I have More Questions?Call1-800-821-6400MondaythroughFridayfrom8a.m.to7p.m.(EasternTime).AClientServiceRepresentativewillhelpyouunderstandcoverage,findaplanattorneyinthelocationmostconvenienttoyou,offerinformationaboutusinganout-of-networkattorney,andansweranyotherquestions.
Formoreinformation,downloadHyatt’smobileapporvisitthewebsitewww.info.legalplans.com. Enter theappropriateaccesscode,asfollows:
Select Plan7600001-EmployeeOnly7610001-Employeew/Dependents
Select Plus Plan7620001-EmployeeOnly7630001-Employeew/Dependents

www.GaBreeze.ga.gov
2017 You Decide
29
Spending AccountsTheSpendingAccountplansareadministeredbyADP.
Forthe2017planyear,theannualamountsyou maycontributeare: Minimum Maximum DependentCare $120 $4,960HealthCare $120 $2,510
TheIRSrulesandtherulesoftheEmployeeBenefitsPlanCouncildesignateeligibleexpenses.TheEmployeeBenefitsPlanCouncilhastheresponsibilitytointerprettheserulesandmakealldecisionsastoanexpense’seligibility.
Important Information About Spending Accounts• Deductionsforspendingaccountsaremadeona
pre-taxbasiseverypayperiod.• Yourspendingaccountelectionsarebindingfor
theplanyear.Youmaybeabletomakelimitedchangesifyouhaveaqualifiedstatuschange.
• Youcannotcarryoverexpensesthatyouhaveincurredinoneplanyearintothenextplanyearforreimbursement.
• Youcannottransfermoneyfromoneaccount toanother.
• Claimsshouldbesubmittedonlyafterserviceshavebeenprovided.
• Youmaysubmitclaimsatanytimeforanyamount,butpaymentwillnotbemadeuntil yourclaimstotal$25ormore.Reimbursementmaybebycheckorbydirectdeposittoyourbankaccount.
• Duringtheyear,youreceivestatementsshowinghowmuchyouhaveineachaccount.
• Reimbursementsareissuedonadailybasis.• UnderIRSrules,anymoneyleftinyour
accounts,andnotclaimedforthepreviousplanyear’sexpensesbytheclaimfilingdeadline,isforfeited.Itisretainedbytheplanandusedforadministrativeexpenses.
TheHealthCareSpendingAccounthasagraceperiodthatcanhelpyouavoidlosingmoneyforunclaimedexpenses.Seepage31.
• Amonthlyadministrationfeeof$3.20isincludedinthetotalcontributionamountfortheHealthCareSpendingAccount.
Important Note:Pleasebeawarethatifyouarecurrentlycontributingtoaspendingaccount,yourannualallocationwillnotautomaticallycontinueintothenewplanyear.Youmustmakeanewelectionifyouwanttocontributetotheplansin2017.
ContactGaBreezeBenefitsCenterat1-877-342-7339formoreinformation.
Dependent Care Spending Account (DCSA)
TheDependentCareSpendingAccountprovidesyouwiththeopportunitytousetax-freedollarstopayforthecareofyourchildrenunderage13orotherIRS-eligibledependents(suchasadisabledchildofanyageoranelderlyparent)whileyouandyourspouseworkorattendschoolfulltime.

www.GaBreeze.ga.gov
2017 You Decide
30
Eligiblechildcareservicesmayincludeyourcosttosendachildtopreschool,afterschool,ornurseryschool.Also,expensesfordependentsofanyagewhoareunabletocareforthemselvesbecauseofaphysicalormentalhandicapareeligible.Apersonqualifyingforthistypeofcaremustspendatleasteighthoursadayinyourhome.Elderlydependentcaremayincludeyourcosttosendadependentparenttoaneldercarefacilityorhavesomeonecarefortheminyourhome.
Ifyouaremarried,bothyouandyourspousemustbeworking,orbeafull-timestudent,duringthetimethecareisreceived.Yourincometaxreturn(longandshortforms)willrequireyoutoincludeyourdependentcareprovider’snameandtaxnumberorSocialSecuritynumber.
Dependent Care Spending Account Exclusions ListTheseareafewexamplesofdependentcareexpensesthatarenoteligibleforreimbursement.• Activityandbookfees• Cleaningandcookingservicesnotprovided
bythecareprovider• Field trips• Food,clothing,andentertainment• Kindergarten• Overnightcamps• Sports lessons
• Transportationtoandfromthechildcareprovider• Tuitionforprivateschool
NOTE:YoushouldcarefullyreviewyouroptionsandconsultaqualifiedtaxadvisorforassistanceindeterminingusingtheDependentCareTaxCreditorusingtheDependentCareSpendingAccount.
Dependent Care Spending Account LimitsYoumaynotbeabletodepositthefull$4,992ifanyofthefollowingsituationsapplytoyou.• IfyourspouseworksfortheState,oranother
employerwhooffersasimilarplan,thetotalofyourfamily'scontributionstoadependentcarespendingaccountcannotexceed$4,992.
• Ifeitheryouoryourspouseearnslessthan$5,000ayear,youcandepositasmuchasthesmallerofyourtwoincomes.
• Ifyourspouseiseitherafull-timestudentorincapableofself-care,youmaydepositupto$3,000foronedependent,or$4,992fortwoormore dependents.
• Ifyouaremarriedbutfileaseparatefederalincometaxreturn,youmaydepositamaximumof$2,500toyourdependentcarespendingaccount.
• IfyouarehiredafterJanuary1,orhaveaqualifiedchangeinstatusduringtheplanyear(seeTermsandConditions),youmaycontributeupto$416permonthfortheremainderoftheplanyear.
www.GaBreeze.ga.gov
2017 You Decide
31
Health Care Spending Account (HCSA)
TheHealthCareSpendingAccount(HCSA)helpsyousavetaxdollarsonhealth-relatedproductsandservicesreceivedbyyouandyourfamily.
Debit CardWhenyouenrollinaHealthCareSpendingAccount,you’llreceiveaVISA®SpendingAccountCardforpurchasesofeligiblehealthcareservices.Thiscardwillarrivefundedwithyourfull annual allocation. Youmayrequestuptofouradditionalcardswithyourspouseordependent’snameonit,forafeeof$5percard.Ifyourcardislostorstolen,youmayrequestanothercardforafeeof$15.Foradditionalcards,callADPat1-800-893-0763.
Keeping ReceiptsRemember,youmustkeepyourreceiptssincesometransactionsmayrequirevalidationbyADP.
Important Note: TheIRSdoesnotallowparticipationinbothHealthCareSpendingAccountsandHealthSavingsAccounts.
Examples of Eligible Expenses• Deductiblesandco-paymentsnotpaid
byanyhealthordentalinsuranceinwhichyouoryourfamilymembersparticipate
• Costsforproceduresnotcoveredor notcoveredfullybyahealth,dental, or vision plan
• Specializedequipmentfor disabled persons
• Preventativecarescreenings• Contact lens and glasses• Lasereyesurgery• Prescription• Mentalhealthservices• Physicaltherapy• CertainotherIRSapprovedexpenses
Examples of Ineligible Expenses • Cosmeticprocedures/drugs• Electrolysis• Hairtransplants• Herbalsupplements• Insurancepremiums• Nicotinepatchesandgum• Nutritionalsupplements• Teethwhitening/bonding• Vitamins• Over-the-countermedications
HCSA Grace Period of 2½ Months
UndertheHCSA,theIRSallowsyouagraceperiodtoavoidthe“UseItorLoseIt”provision.IfyouhaveanyHCSAfundsremainingonDecember31,youhaveanadditional2½months–throughMarch15ofthefollowingyear–todepleteyouraccount.Youcancontinuetouseyourdebitcard,orsubmitqualifiedexpensesforreimbursement,forproductsandservicespurchasedthroughMarch15th.You’llhaveuntilApril30thtosubmitsuchclaimstoADP.Remember,ifaclaimismailed,theenvelopemust bepostmarkedbyApril30th.Thefastestwayto getclaimstoADPistofaxthemat1-866-643-2219.
Tobesttakeadvantageofthisgraceperiod,fund onlythoseexpensesyouexpecttohaveduring the12-monthperiod.Ifyoudonotspendallof themoneyyoucontributed,duringtheplanyear, besuretouseitupduringthegraceperiod.

www.GaBreeze.ga.gov
2017 You Decide
32
EMPLOYEE CHECKLISTReview YOU DECIDEforvaluableinformationfor
eachoption,descriptionsofrequiredmedicalunderwritingrequirements,andTermsandConditions.
EnsureyouhaveyourIDandpasswordfortheGaBreeze website.
Checkwithyourentity'sHumanResources/PayrollOfficeforapplicabledeadlines.
ConfirmontheGaBreezewebsitetoseeifadditionaldocumentationrequired,suchasmedicalunderwritingforms.
ReviewyourConfirmationPageandreportdiscrepanciesimmediatelytoGaBreezeBenefitsCenter1-877-342-1339.Followuptoensurethatcorrectionsaremade.
Compareyourpaystub(s)againsttheoptionsyouselected.Contactyourpersonnel/payrollofficeifyoufindanydiscrepancies.
Reportanyincorrectinformationtoyourpersonnel/payrolloffice.
Additional Information
TheFlexibleBenefitsProgramattemptstobeasconsistentaspossiblewithStateHealthBenefitPlanrulesandregulations.Thisisnotalwayspossibleduetothevariationsinbenefitofferings.
ThisbookletsummarizesthebenefitsyoucanchoosethroughtheStateofGeorgiaFlexibleBenefitsProgram.AmoredetailedexplanationofbenefitprovisionsisprovidedineachBenefitSummaryPlanDescription.Everyattempthasbeenmadetoensurethattheinformationinthisbookletisaccurate.
TheStateofGeorgiaFlexibleBenefitsProgramisgovernedbylegaldocumentationandinsurancecontracts.However,intheeventthereareanyconflictsbetweenthisbookletandtheofficialplandescriptionsandcontracts,thetermsoftheofficialplandescriptionsandcontractswillprevail.
TheFlexibleBenefitsProgramisgovernedbycurrenttaxlawandissubjectto,andoperatedinaccordancewith,regulationsoftheInternalRevenueService(IRS).IfchangesintheFlexibleBenefitsProgramarenecessary,wewillmakeupdatestocomplywithappicableIRSregulations.
www.GaBreeze.ga.gov
2017 You Decide
33
HIPAA PRIVACY AND SECURITY NOTICETheHealthInsurancePortabilityandAccountabilityActof1996(HIPAA)requiresthatcoveredentities,includingstateagenciesthatdealwithProtectedHealthInformation(PHI),provideyouwiththisnoticeregardingprogramsadministeredbytheDepartmentofAdministrativeServices(DOAS)inwhichDOASmaymaintainvarioustypesofPHIaboutyou.DOASunderstandsthatinformationaboutyouandyourfamilyispersonal.Assuch,DOASiscommittedtosecuringandprotectingyourconfidentiality.
Thisnoticetellsyou(a)howDOASusesanddisclosesinformationaboutyouand,(b)discussesyourrightsinkeepingthisinformationprivateandsecure.Pleasereviewthisnoticecarefully.
Overview
What is HIPAA?HIPAA,theHealthInsurancePortabilityandAccountabilityActof1996,isafederallawregardingtheconfidentialityandsecurityofProtectedHealthInformation(PHI).Itimposesrestrictionsonhowyourhealthinformationcanbeusedandshared,andconfirmsrightsforindividualsconcerningtheirhealthinformation.
What is PHI?PHI,ProtectedHealthInformation,isindividuallyidentifiablehealthinformationthatismaintainedortransmittedbyacoveredentity.Itisinformationrelatedtoaperson’shealth,provisionofcare,orpayment.ExamplesofitemscontainingPHIincludeabillforhealthservices,anexplanationofbenefitsstatement,receiptsforreimbursementfromahealth
carespendingaccount,oranylistshowingtheamountofbenefitspaidwithabreakdownbysocialsecuritynumber.Thisalsoincludesyouremployer(e.g.,stateagency,schoolsystem,authority)transmittinginformationaboutyoutoDOAS.Thisinformationmayincludeyourname,address,birthdate,socialsecuritynumber,employeeidentificationnumber,andcertainhealthinformation
How DOAS Uses and Discloses Protected Health InformationWhenservicesarecontracted,DOASmaydisclosesomeorallofyourinformationtothecompanytoperformthejobDOAShascontractedwiththemtodo.DOASrequiresthecompanytosafeguardyourinformationinaccordancewithfederalandstatelaw.
Privacy and Security Law RequirementsDOASisrequiredbylawto:• Maintaintheprivacyofyourinformation.• ProtectelectronicPHIbyimplementingreasonable
andappropriatephysicaladministrativeandtechnicalsafeguards.
• ProvidethisnoticeofDOAS’legaldutiesandprivacyandsecuritypracticesregardingtheinformationthatDOAShasaboutyou.
• Abidebythetermsofthisnotice.• Refrainfromusingordisclosinganyinformation
aboutyouwithoutyourwrittenpermission,exceptforthereasonsgiveninthisnotice.Youmayrevokeyourpermissionatanytime,inwriting.ThatrevocationwillnotapplytoinformationthatDOASdisclosedpriortoreceivingyourwrittenrequest.Ifyouareunabletogiveyourpermissionduetoanemergency,DOASmayreleaseinformation,ifitisinyourbestinterest.DOASmustnotifyyouassoonaspossibleafterreleasingtheinformation.

www.GaBreeze.ga.gov
2017 You Decide
34
Your Health Information RightsYouhavethefollowingrightsregardingthehealthinformationmaintainedbyDOASaboutyou:• Seeandobtainacopyofyourhealthinformation.
ThisrightwouldnotextendtoinformationneededforalegalactionrelatingtoDOAS.
• AskDOAStochangehealthinformationthatisincorrectorincomplete.DOASmaydenyyourrequestundercertaincircumstancesorrequestadditionaldocumentation.
• RequestalistofthedisclosuresthatDOAShasmadeofyourhealthinformationbeginninginApril2003.
• Requestarestrictiononcertainusesordisclosuresofyourhealthinformation.DOASisnotrequiredtoagreewithyourrequest.
• RequestthatDOAScommunicatewithyouaboutyourhealthinawayoratalocationthatwillhelpyoukeepyourinformationconfidential.
• RequestanothercopyofthisnoticefromDOAS,oryoumayobtainacopyfromtheDOASwebsite,www.doas.ga.gov(under“Privacy”).
For More Information and To Report a ProblemIfyouhavequestionsandwouldlikeadditionalinformationaboutProtectedHealthInformation(PHI)youmaycontactGaBreezeat1-877-342-7339MondaythruFriday8:00a.m.to5:00p.m.Youmayalso visit DOAS web site, www.doas.ga.gov.
DOASdoesnotdiscriminateonthebasisofdisabilityintheadmissionoraccessto,ortreatmentofemploymentinitsprogramsoractivities.IfyouhaveadisabilityandneedadditionalaccommodationstoparticipateinanyDOASprograms,pleasecontacttheDOASatthenumberslisted.ForTDDrelayserviceonly:1-800-255-0056(text-telephone)or1-800-255-0135(voice).
Ifyoubelieveyourprivacyorsecurityrightshavebeenviolated:• Youmayfileacomplaintinwritingtothe
DOASPrivacyUnitat: Department of Administrative Services
Attn: Privacy Officer 200 Piedmont Avenue SE West Tower, Suite 502 Atlanta, GA 30334-9010
• YoucanfileacomplaintwiththeSecretaryofHealthandHumanServicesbywritingto:SecretaryofHealthandHumanServices,200IndependenceAve.SW,Washington,DC20201.Foradditionalinformation,call1-877-696-6775.
• YoumayfileagrievancewiththeUnitedStatesOfficeforCivilRightsbycalling1-866-OCR-PRIV(1-866-627-7748)or1-886-788-4989TTY.
Therewillbenoretaliationforfilingacomplaintorgrievance.
IfDOASchangesitsprivacyorsecuritypracticessignificantly,DOASwillpostthenewnoticeonitsweb site at www.doas.ga.gov.
www.GaBreeze.ga.gov
2017 You Decide
35
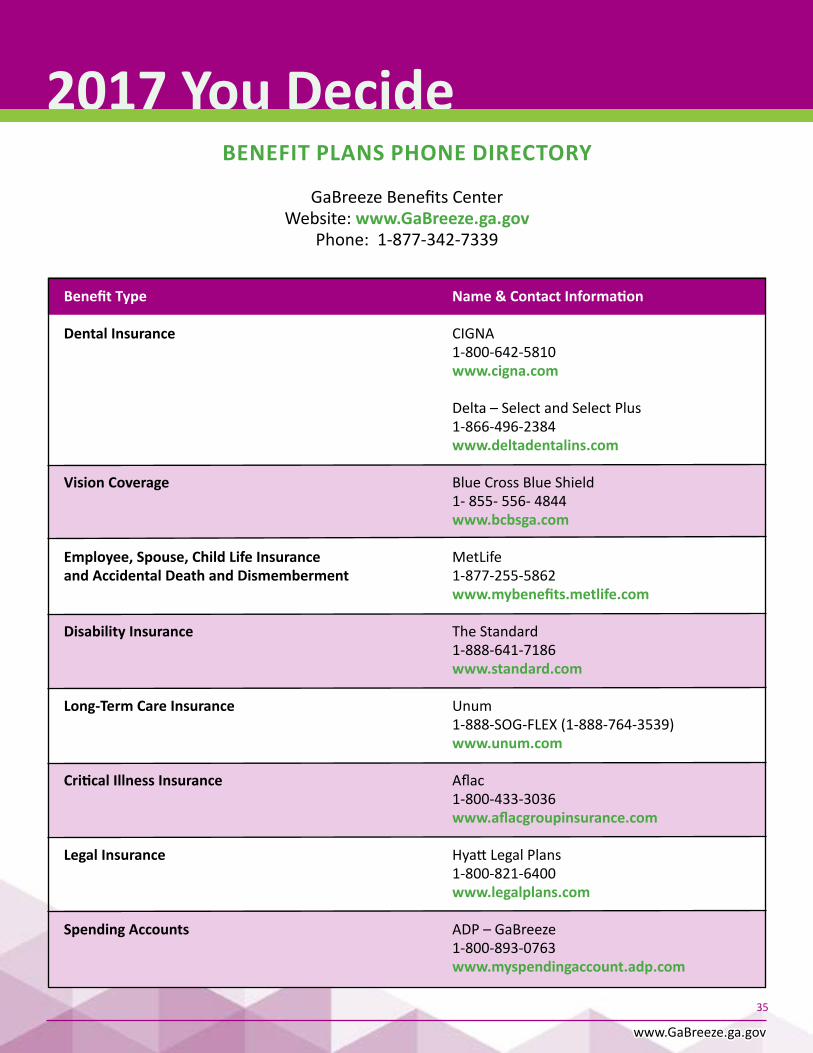
BENEFIT PLANS PHONE DIRECTORY
GaBreezeBenefitsCenterWebsite:www.GaBreeze.ga.gov
Phone:1-877-342-7339
Benefit Type Name & Contact Information
Dental Insurance CIGNA 1-800-642-5810 www.cigna.com
Delta–SelectandSelectPlus 1-866-496-2384 www.deltadentalins.com
Vision Coverage BlueCrossBlueShield 1-855-556-4844 www.bcbsga.com
Employee, Spouse, Child Life Insurance MetLife and Accidental Death and Dismemberment 1-877-255-5862 www.mybenefits.metlife.com
Disability Insurance TheStandard 1-888-641-7186 www.standard.com
Long-Term Care Insurance Unum 1-888-SOG-FLEX(1-888-764-3539) www.unum.com
Critical Illness Insurance Aflac 1-800-433-3036 www.aflacgroupinsurance.com
Legal Insurance HyattLegalPlans 1-800-821-6400 www.legalplans.com
Spending Accounts ADP–GaBreeze 1-800-893-0763 www.myspendingaccount.adp.com
www.GaBreeze.ga.gov
2017 You Decide
36
TERMS AND CONDITIONSTheFlexibleBenefitsProgramisofferedbytheEmployeeBenefitsPlanCouncilandparticipatingdepartmentsandauthorities.TheFlexibleBenefitsProgramisgovernedbytheInternalRevenueCode,section125,andrulesissuedbytheEmployeeBenefitsPlanCouncil.TheFlexibleBenefitsProgramprovidesyouwithamethodtohaveyouremployerpurchasebenefitswithmoneythatwouldhavebeenpaidtoyou.Youdonotreceivethepremiumamountsandcontributionsforthepre-taxoptionsyouselectastaxableincome(andthereforedonotpaytaxesonthatamount);youdoreceivethebenefitsasanemployerpaidbenefit.Theelectionisabindingsalaryagreement.FailuretocomplywithallcontractualandadministrativerequirementswillresultinanyexcesssalaryreductionsbeingretainedbythePlan.ThefollowingstatementsapplytothebenefitoptionslistedontheAnnualEnrollment web site.
1) YourparticipationintheFlexibleBenefitsProgramisvoluntary.Youarenotrequiredtochooseanyoftheoptions.Ifyoudonotwishtoparticipateinthesebenefits,select‘nocoverage’ineachbenefitcategory.
2) Somecoveragelevelsavailabletoyouandthepremiumamountforeachcoveragelevelmaybecalculatedusingyourretirementsalary,yourage,youreligibilityfordisabilityretirementbenefits,andFICAstatusonyourdateofhireortheBenefitCalculationDate,whicheverisdeemedappropriatebythePlanAdministrator.AnyadjustmentstotheAnnualBenefitBaseRate,withtheexceptionoferrors(asdeterminedbythePlanAdministratorshallbereflectedonthefollowingBenefitCalculationDate,tobeeffectiveforthefollowingplanyear.)Promotions,demotions,adjustmentsduetocertificationsarenotdeemedtobeerrors.Anyerrorsintheseitemsshouldbereportedtoyourpersonnelorpayrollofficeimmediately.
3) Thecalculationoftaxsavingsdoesnottakeintoconsiderationanyotherincomeearnedbyemployeeorfamilymembers,incomereductionprogramsuchasDeferredCompensationorTaxShelteredAnnuities,oranychangesyoumaymakeincoveragesfortheupcomingyear.
4) ByselectingcoveragesandindicatingcontributionstoSpendingAccounts,youareagreeingthatyouragencymayreduceyourtaxableincomebytheamountnecessarytopurchasethosecoveragesandmakethosecontributions.Exceptincertaincircumstances,theamountofincomereductionmaynotbechangeduntilthenextenrollmentperiod.
5) Fordependentand/orspousalcoverage,itisyourresponsibilitytonotifytheGaBreezeBenefitCenterifthepersonceasestobeeligibletoparticipateinthePlan.TherewillbenorefundofpremiumspaidintothePlan,whenatimelychangeisnotmade.
6) AfterthisenrollmentperiodyoumaybecomeaparticipantormakechangesinsomecoveragesonlyunderlimitedconditionsinaccordancewiththerulesoftheIRScode,theEmployeeBenefitsPlanCouncil.TheEmployeeBenefitsPlanCouncilhastheresponsibilitytointerprettheserulesandmakethefinaldecisionastowhetheryoumayenrollorchangeanycoverageoutsideoftheenrollmentperiod.Yourrequestforenrollmentorachangeoutsideoftheenrollmentperiodwillonlybeconsideredifyousubmittheproperdocumentationwithinthetimeframeallotted.
YourrequestforenrollmentorachangeincoverageundertheFlexibleBenefitsProgrammustbedonebycallingtheGaBreezeBenefitCenteroronthewebsitewithin30days.AlistofeventsthatmightpermityoutoenrollorchangeoneormorecoveragesundertheFlexibleBenefitsProgram:a) Yougainorloseaspouse;orb) Yougain(notimelimitifduetojudgment,decree
ororder)orloseaneligibledependent;orc) Yourspouseordependentbecomeseligiblefororloses
coverageunderanotheremployer’splan,COBRAoragovernmentalplan;or
d)Aneventcausesyourdependenttogainorloseeligibilityforcoverageunderyouremployer’splan;or
e) Yourchangeofresidencecausesyouoryourspouseordependentstogainorloseeligibilityforcoverageunderyourplanoranotheremployer’splan;or
f) Thecostofyourdependentcareincreasesordecreasessignificantlyandyourdependentproviderisnotrelatedtoyou,yourspouse,oryourdependent;or
g)Yourspouse’semployerincreases,decreasesorceasescoverage,orconductsopenenrollment.
7) Thissalaryagreementwillbeterminatedifyouchangetheagreementduringthenextenrollmentperiod.Ifyoudonotchangetheagreement,yourbenefitchoiceswillrolloverinthenextPlanyearordefaulttoaspecifiedcoveragewiththeexceptionoftheFlexibleSpendingAccounts.
8) IfyouareeligibletoparticipateinthePlan,youterminateandarerehiredwithin30daysduringthesameplanyear,youmustmaintainthesameoptions.
9) OptionsandcoverageundertheFlexibleSpendingAccountsaresetforthintheFlexibleBenefitPlanDocument.ForallotherbenefitsundertheFlexibleBenefitsProgram,theoptionsandcoveragelevelsofferedconformtopoliciesprovidedbytheinsurancecompanymakingtheoffer.Byselectinganoptionandcoveragelevelyouagreetoabidebythetermsandconditionsofthatpolicy.
10) ContributionstoSpendingAccountsarevoluntary.YoushouldnotparticipateinSpendingAccountsuntilyouthoroughlyreadthesectionsoftheEnrollmentBookletrelatedtoSpendingAccounts.BychoosingtocontributemoneytooneormoreSpendingAccountsyouareagreeingtoabidebytheRulesoftheEmployeeBenefitsPlanCouncilrelatedtoSpendingAccounts.Inparticular,youareagreeingtothefollowingprovisions:a) MoneycontributedtotheHealthCareSpendingAccount
cannotbeusedtopayclaimsfortheDependentCareexpenses.MoneycontributedtotheDependentCareSpendingAccountcannotbeusedtopayclaimsfortheHealthCareexpenses.
b)Ingeneral,theamountcontributedforaDependentCareAccountcannotbegreaterthantheearnedsalaryofyouoryourspouse,whicheverisless.
c)Ifyouaremarriedfilingseparately,theamountcontributedforaDependentCareAccountcannotbegreaterthan$2,500.
d)ThevalidityofaclaimagainstaSpendingAccountisdeterminedinaccordancewiththePlan,InternalRevenueCode,andIRSregulationsasinterpretedbytheAdministratorsubjecttotheappealprovisionsofthePlan.

www.GaBreeze.ga.gov
2017 You Decide
37
e)AnymoneynotreimbursabletoyouwillbeforfeitedtotheFlexibleBenefitsProgram.Forfeitedmoneywillnotbereturnedorpaidtotheemployeebutwillbeusedtoreducethecostsassociatedwithprovidingthisbenefit.NOTE:Thisruleisintendedtoensureyouallocateonlythoseexpensesyouexpecttoincur.Seep.31forinformationaboutthegraceperiodthatcanhelpyouavoidhavingtoforfeitHealthCareSpendingAccountfunds.
f) FortheSpendingAccounts,eligibleexpenseswillbereimbursedinaccordancewiththeRulesoftheEmployeeBenefitsPlanCouncilandtheIRScode.
g)FortheDependentCareSpendingAccount,youwillnotbereimbursedformorethanthePlanhasreceivedfromyourdepartmentonyourbehalf.
h)IfyoudecidetoactivateandusetheSpendingAccountdebitcard,youagreetoabidebyallrequirementsasindicatedinthecardholder’sagreementreceivedwiththecard.
11) ByselectingtheCriticalIllnessBenefit,youareagreeingtothefollowing:a)Iamassertingthattothebestofmyknowledgeandbelief,
theanswerstothequestionsontheapplicationaretrueandcomplete.TheyareofferedtoContinentalAmericanInsuranceCompanyasthebasisforanyinsuranceissued.ItisunderstoodandagreedthatcoveragewillnotbecomeeffectiveunlessIamactivelyatworkonthedateofenrollmentandtheeffectivedateofcoverage.
b)Iunderstandandagreethatnobenefitsarepayableforlossstartingoroccurringwithin12monthsoftheeffectivedateofcoveragewhichiscausedby,contributedtoby,duetoorresultingfromaPre-existingcondition,unlessIhavegone12monthswithoutmedicalcare,treatmentorsuppliesforthePre-existingcondition.
c) Irealizethatanyfalsestatementormisrepresentationmayresultinlossofcoverageunderthecertificate.Iunderstand
thatnoinsurancewillbeineffectuntilapprovedbyContinentalAmericanInsuranceCompanyandthenecessarypremiumispaid.Anypersonwho,withintenttodefraudorknowingthatheisfacilitatingfraudagainstaninsurer,submitsanapplicationorfilesaclaimcontainingafalseordeceptivestatementmaybeguiltyofinsurancefraud.
d)IauthorizemyemployertodeducttheappropriateamountfrommyearningsandtodeductandpayContinentalAmericanInsuranceCompanythepremiumrequiredthereaftereachmonthformyinsurance.
12) Othertermsandconditions:a)Ifyouchoosenottoparticipateorchoosenottocontinue
coverages,yourabilitytoenrollatalaterdatewillbesubjecttocontractualprovisions,whichmayincludemedicalproofofinsurabilityorlimitedcoverages.
b)Ifyoufailedtoenrollinoptionsrequiringmedicalunderwritingwhenfirsteligibleandyouchooseneworincreasedlevelsofcoverage,youmustcompletethemedicalunderwritingprocess and be approved.
c)IfyouchoosecoverageundertheLifeInsuranceoptionsandtheAccidentalDeathandDismembermentoptions,thesameBeneficiaryelectioninformationwillbeused.Ifabeneficiaryisnotnamed,thebeneficiarywillfollowtheorderstatedinthepolicy.
d) Ifyouselectmorethan$50,000undertheLifeInsuranceoption,youmaychoosetopaythepremiumwithpost-taxdollarstoavoidhavingtopayimputedincome;thiswilleliminateanytaxsavingsonthelifeinsurancepremium.
13) IntheeventofanadministrativeerrorwithrespecttotheFlexibleBenefitsProgram,decisionswillbemadeinaccordancewiththeInternalRevenueCode,andtheRulesoftheEmployeeBenefitPlanCouncilfortheFlexibleBenefitsProgram.