49
Annual Operating Plan 2015/16 Final 12 May 2015 (Subject to NHSE agreement)

Annual Operating Plan
2015/16
Final 12 May 2015
(Subject to NHSE agreement)

Operating Plan 2015/16 Subject to NHSE Agreement Page 1 of 48
CONTENTS
Introduction ............................................................................................................................... 2
Executive summary ......................................................................................................................... 3
A summary of our strategy .............................................................................................................. 4
Our successes ............................................................................................................................... 5
Developing our operating plan 2015/16 ........................................................................................... 6
Addressing health needs and inequalities ....................................................................................... 8
Improving quality and performance of services ............................................................................. 11
Transforming services ................................................................................................................... 17
Our programmes of delivery .......................................................................................................... 19
Enabling Transformation ............................................................................................................... 21
Risks to Delivery ........................................................................................................................... 25
Achieving financial balance ........................................................................................................... 27
Appendix 1 National outcomes framework indicators by domain progress .............................. 33
Appendix 2 National outcomes framework and outcomes by programme ............................... 34
Appendix 3 GP network profile summary ................................................................................ 35
Appendix 4 Commissioning levers .......................................................................................... 36
Appendix 5 NHS Constitution annual performance and plan ................................................... 39
Appendix 6 NHS Constitution trajectories ............................................................................... 42
Appendix 7 Quality, Innovation, Productivity and Prevention (QIPP) by Programme ............... 46
Appendix 8 Summary of patient and public involvement ......................................................... 47
Appendix 9 Programmes of delivery (see separate document) ............................................... 48

Operating Plan 2015/16 Subject to NHSE Agreement Page 2 of 48
Introduction Health in Croydon faces many challenges over the coming years inlcuding growth in our overall population numbers and our black and minority ethnic populations, variations in the quality of our services, as well as the significant financial challenges as a result of the inherited imbalance of resource allocation and need. We are determined that by implementing our transformation programme through better care provision and by working closely with our commissioning partners, NHS England, London CCGs, South West London Commissioning Collaborative, the London Borough of Croydon and our providers, alongside our increases in resource allocations, we will maximise the resources available to us to ensure that we can continue to strive to deliver high quality services and improve outcomes for the populations and patients we serve. We have developed our plans through continuous engagement with patients, the public and our partners, including the Health and Wellbeing Board and our plans reflect this feedback. We will continue to engage as we continue to develop our plans. Key themes which support our transformation agenda are: prevention, self-care and shared decision making; integration across health and social care and integrated commissioning structures. We are committed to the delivery of care in the most appropriate setting and developing and implementing outcomes based population commissioning which will span primary, community and secondary care boundaries in both acute and mental health services. Despite our financial deficit position, Croydon CCG will need to invest speculatively in order to deliver this ambitious transformation plan to improve quality and outcomes and release savings to improve its financial position in later years.

Operating Plan 2015/16 Subject to NHSE Agreement Page 3 of 48
Our strategic aims Maintaining and improving safety and quality of care Transforming the way care is delivered for the future Achieving financial sustainability
Executive summary Our strategy sets out a journey to deliver our ambition and we are pleased to reflect that we have made significant progress against last year’s operating plan.
GP leadership: Our GP leadership and networks have been instrumental in ensuring delivery against our vision and objectives. In 2014, for example: They have been integral in helping to design and roll out 18 new care pathways including;
Cardiology, Chronic Obstructive Pulmonary Disease (COPD) and Diabetes pathways. Through their commitment to working with provider clinicians, we have developed community
services through the Transforming Adult Community Services programme and more latterly the Better Care Fund. During 2015/16 we will continue to embed these services to gain maximum benefit.
Mental health services: In 2014/15, we invested in mental health services to increase access and we will need to further develop our mental health models of care and ensure we deliver on realistic targets for mental health services in Croydon. Older people: We have also implemented firm foundations for changing the way we commission services for older people; 2015/16 will be critical for establishing the model of care and procuring older people’s services, ready for 2017. Urgent care: During 2014/15 we saw pressures on A&E increase significantly during the winter months and, whilst we expect to see the benefits of a range of initiatives we have put in place, we must continue to work towards a resilient and sustainable model of emergency care in Croydon. Primary care: Co-commissioning primary care services with NHS England will form a key enabler in developing seamless, integrated, out of hospital services for local people. NHS England and South West London CCGs are establishing robust governance arrangements to manage co-commissioning in South West London. Equally, we must ensure we set out our plans to deliver a reduction in the variation in primary care. Again our GP networks are critical to drive this as they understand our population. Underpinning all of our work, are targeted initiatives to make a difference as a part of our prevention, self-care and shared decision making programme and we must establish our plans for this programme in 2015/16. Financial sustainability: We have also successfully delivered across our QIPP schemes and over the past two years have achieved a better financial position than planned. For 2015/16 our key areas of focus, to deliver our ambitious strategy, are:
Our focus for 2015/16 Prevention, self-care, shared decision making Improving access to mental health services Older people - Outcomes based commissioning Urgent and emergency care system resilience Transforming primary care

Operating Plan 2015/16 Subject to NHSE Agreement Page 4 of 48
A summary of our strategy
Health and social care face a number of challenges over the coming years. The overall population is growing. There is an expected increase in the number of younger people living in the borough, overall life expectancy is increasing and we have an ageing population which increases the demand on our services. Our population is also becoming more diverse, and so changing the health need in Croydon. There are variations in the quality and performance of our services, leading to varying experiences of care and outcomes for people. These challenges are set in the context of a significant financial challenge as a result of an imbalance between our resources and our population needs. Given these population needs and service challenges, our priority outcomes and subsequent indicators of delivery for the people of Croydon are: Reducing potential years of life lost through amenable disease Ensuring people are seen in the right place at the right time Children and young people reach their full potential Increased independence Positive patient experience Our changing population leads to a long term focus on: Cardiology Chronic Obstructive Pulmonary Disease (COPD) Diabetes Cancer Mental Health including Dementia Children and Young Adults The principles upon which we will deliver these and, indeed, all areas we commission are that: Prevention is better than cure but; When someone does become ill they are better able to manage their illness and; When a person does need treatment they are seen in the right place at the right time and; There is shared decision making between the patient and the health professional Ensuring we make the best use of our resources means we cannot continue delivering services in the same way. We require transformational change through: Prevention, self-care, shared decision making Outcomes based commissioning Transforming adult community services Improve integration of care Reducing unwarranted primary care variation Whole system redesign Our organisational objectives are:
‘Longer healthier lives for all the people in Croydon’
We will do this by working with the diverse community of Croydon, using our resources
wisely, to transform and provide safe, effective, high quality, patient centred services
To achieve financial balance
To develop as a mature membership organisation
To commission integrated, safe, high quality service in the right place at the right time
To have collaborative relationships to ensure integrated approach

Operating Plan 2015/16 Subject to NHSE Agreement Page 5 of 48
Our successes GP leadership and our GP networks have driven the development and implementation of our plans. As a result, we have achieved a range of service changes at a pace that would otherwise have not been possible.
Transforming the way we deliver care 18 new care pathways developed and implemented through the clinical networks
including, cardiology, COPD, diabetes, MSK and falls, meaning patients have fewer unnecessary appointments
Transforming Adult Community Services 20,500 people referred to the new 24/7 Integrated Single Point of Assessment
(SPA) have been triaged to the appropriate service
884 people referred to new 24/7 Rapid Response service to support unwell
patients to be cared for within the community
193 patients supported away from hospital through increased number of
Intermediate Care Bed from 6 to 12
800 patients supported through dedicated case management through joint GP-
led Primary, Community, Social Care and Mental Health Multi-Disciplinary
Teams (MDTs)
Better access for people with mental health problems with new and enhanced mental health services including, Home Treatment Crisis Service Enhancement, Dialectic Behavioural Therapy, Relapse Prevention.
496 patients undertaken diabetes management course as a result of GP practices having designate diabetes specialist nurse
Paediatric asthma service implemented
People with heart problems are seen and treated more quickly in the community at Community clinics: One Stop Heart Failure Clinic, Rapid Access Chest Pain Clinic
Improving Quality Highest performing CCG in South London for our quality premium indicators in
2013/14 A steady decline in the number of patients with new pressure ulcers as well as a
decrease in the number of falls Fewer venous thromboembolism (VTE) than planned Fewer Clostridium Difficile infections than planned Musculoskeletal (MSK) community service waiting times down from 28 weeks to 8
weeks Reduced number of fractured neck of femur through new falls prevention service Medication reviews in care homes 1 midwife to 28 births achieved
Achieving Financial Sustainability Delivered better than plan in the past two years £14m QIPP plan in 2013/14 and £11m in 2014/15

Operating Plan 2015/16 Subject to NHSE Agreement Page 6 of 48
Developing our operating plan 2015/16 Our operating plan for 2015/16 sets out year three of our strategy implementation. It also reflects implementation of emerging national, London and South West London priorities, as well as local service strategies such as: Prevention, Self-Care and Shared Decision Making Strategy Primary and Community Strategy Urgent and Emergency Care Strategy Mental Health Strategy Dementia Strategy Early Help Strategy Children’s and Family Partnerships Primary Prevention Plan Voluntary Sector Strategy All our strategies can be found at www.croydonccg.nhs.uk/strategies Our local plans continue to develop with the leadership of our six Clinical Leaders and through our six GP networks. By developing our networks we understand our population needs closer to where they live and are able to work towards delivering our priorities.
Key national priorities Overall there is a greater emphasis on: Public health prevention Parity of esteem for mental health including a range of new targets for Improving Access to
Psychological Therapies (IAPTs) and Early Intervention Services Extension of choice in mental health and maternity Use of different models of care for providers
National
Forward View
London
13 London programmes
South West London
SWL Commissioning Collaboration
Croydon CCG
Our Strategy
Networks
Network and practice challenges
Our Operating Plan reflects a number of
priorities

Operating Plan 2015/16 Subject to NHSE Agreement Page 7 of 48
The NHS Five Year Forward View sets out plans for CCGs to take on an increased role in the commissioning of primary care services. Co-commissioning with NHS England will enable CCGs to develop integrated out-of-hospital services, based around the needs of local population. NHS England is also developing a more collaborative approach to commissioning specialised services. As of April 2015, CCGs will be responsible for commissioning specialist wheelchair services and outpatient neurology activity in specialist neurology centres. During 2015/16 NHS England will also be reviewing whether it continues to commission specialist renal and morbid obesity services and responsibility may be devolved to CCGs in April 2016.
London priorities The development and commissioning of the London Quality Standards has led to improvements in services across London, and this remains a key priority (see Appendix 9). In addition in response to Better Health for London the London Commissioning System Design Group (LCSDG) has set out 13 priority programmes of additional London wide system reform, to improve health outcomes for Londoners.
Clinical programmes Enabler programmes
Cancer Primary Care
Children and young people Business intelligence and interoperability
Homeless healthcare services Estates
Mental health Engagement and personalisation
Prevention Payments and funding
Urgent and emergency care Specialised commissioning
Workforce
South West London priorities The South West London Commissioning Collaborative, made up of the six South West London CCGs, has a strategy that will ensure the ‘people in South West London can access the right health service when and where they need them’. The Collaborative has 7 Clinical Design Groups (CDGs) to deliver this:
Clinical programmes Enabler programmes
Cancer Primary care
Children Planned care
Integrated care Urgent and emergency care
Maternity Implementing the London Quality Standards
Mental health
In response to the challenges set out in the Case for Change in our 5 Year Strategic Plan the four acute providers in South West London have come together to form a Provider Collaborative. They will produce viable, but not site-specific, proposals that will improve the quality and financial sustainability of acute services in South West London.

Operating Plan 2015/16 Subject to NHSE Agreement Page 8 of 48
Addressing health needs and inequalities By mid-2013, the resident population of Croydon was estimated to be 372,000. Croydon’s population is growing by about one percent per year, and is projected to reach 400,000 by 2021. Nationally, the population is ageing as life expectancy increases and the baby boomer generation approaches older age. Compared to other areas, however, Croydon has a relatively young population. The present high birth rate and effects of migration are expected to result in growth in some of the younger, as well as older age groups, in coming years. It is in everyone’s interest to ensure that people are able to maintain their independence and stay healthy throughout their lives. However, changes to the make-up of Croydon’s population and lifestyle trends are likely to lead to more people needing care in the future. People are living longer and our population is ageing; the latest projections suggest the number of people aged over 85 will increase by two thirds by 2030. This is an important trend because we know that older people generally have more health problems and need to use health and care services more than younger adults.
We have reviewed our progress against the national outcomes domain indicators (see Appendix 1 and 2) which shows ongoing improvement in years of life lost and in life expectancy. Unplanned hospital admissions for chronic ambulatory care, asthma, diabetes and epilepsy appear to be worsening. The CCG’s focus on these areas will support improvement over time.
Key facts Life expectancy for both men and women is higher than the average in England.
However, life expectancy is 9.1 years lower for men and 7.7 years lower for women in the most deprived areas of Croydon than in the least deprived areas
Deprivation in the borough is lower than average, however Croydon has become increasingly deprived in recent years at a faster rate than surrounding boroughs, and 21,500 (25.2%) children live in relative poverty
Croydon has a growing population with more people having mental health support needs
21% higher spend on mental health inpatient services than comparative boroughs
High numbers of looked after children including on average 400 unaccompanied asylum-seeking children
Over the last 10 years all-cause mortality rates have fallen. Early death rates
from cancer, heart disease and stroke have fallen. However, among under 75
year olds 27% of preventable deaths were due to cardio-vascular disease
(including heart disease and stroke), 40% were due to cancer and 8% were due
to respiratory disease
The prevalence of diabetes in Croydon is estimated to be 6.4% which is
significantly higher than in London (5.8%) and in England (6.0%).
An estimated 17% of adults smoke; there are 390 deaths from smoking each
year
An estimated 62% of adults are overweight or obese
There were 6,300 hospital stays for alcohol related harm in 2013/14;
Breast and cervical cancer screening rates are both significantly worse than the national average

Operating Plan 2015/16 Subject to NHSE Agreement Page 9 of 48
Circulatory diseases, cancers and respiratory diseases remain the causes for the majority of excess deaths which contribute to the gap in life expectancy between the most and least deprived quintiles by cause of death. Our focus in these areas will help address those inequalities. We are also tackling health inequalities by working with Public Health on the five most cost effective interventions as recommended by the National Audit Office (see Medicines Optimisation Programme Appendix 9)
In addition a key focus for 2015/16 is to ensure targeted engagement with those from black and minority ethnic groups. The GP network profiles (a summary of which is provided in Appendix 3) enable the CCG to understand the inequalities of health outcomes and primary care service variations by GP networks. GP networks are addressing key aspects through the Practice Development and Deliver Scheme. Each programme has also identified the priority challenges for each GP network to address, which are reflected in the ‘Programme of Delivery’ section (see page 17) The challenges set out above have led to us setting our priority areas below that will improve life expectancy and reduce health inequalities: Chronic Obstructive Pulmonary Disease (COPD) Cardiology Diabetes Cancer Mental Health including dementia Children and Young Adults
Five Most Cost Effective Interventions Increase uptake of drugs to control
blood pressure Increase uptake of drugs to reduce
cholesterol Increase smoking cessation services Increase anticoagulant therapy in
atrial fibrillation Improve blood sugar control in
diabetes
Equality and Diversity 2
We successfully completed the EDS2 review during 2014 and implemented our
Equality Objectives which we published in October 2013. In doing so the exercise
highlighted areas of good practice in:
Commissioning of the Diabetes Community Services and the Musculoskeletal
Services
Improved training and development opportunities for staff
Increased embedding of Equality and Diversity into the CCG’s operations
Improved and sustained engagement with more communities in Croydon
NHS Workforce Race Equality Standard
In January 2014, the CCG carried out a Staff Survey, the results of which were
used to complement actions of the Equality Objectives 2013-2014 Action Plan. An
action plan was developed including the development of a Staff Forum and specific
training for all CCG staff.

Operating Plan 2015/16 Subject to NHSE Agreement Page 10 of 48
Our GP Network Challenges
Selhurst
Woodside
South Norwood Thornton Heath
Ashburton
Norbury
Bensham Manor
West Thornton
Broad Green
Addiscombe
Upper Norwood
Shirley
Fairfield
Waddon
Croham Fieldway
Heathfield
New Addington
Coulsdon West
Selsdon & Ballards
Sanderstead
Purley
Coulsdon East
Kenley
Mayday
Patient experience
A&E attendance rates Emergency admission rates Diagnosis of atrial fibrillation
and epilepsy
Childhood immunisations Cancer screening
East Croydon
A&E attendances and emergency admissions particularly for over 65s
Prescribing indicators Diagnosis rates for diabetes,
depression, dementia and hypertension
Care and outcomes for diabetes, severe mental illness and Chronic Kidney Disease
Cancer screening
Purley
Flu vaccine uptake
Care and outcomes for diabetes and depression
Thornton Heath
Flu vaccine uptake
Emergency admissions for over 65s
GP referrals to A&E
Diagnosis rate for depression, CHD, atrial fibrillation, COPD and epilepsy
Care and outcomes for depression and rheumatoid arthritis
Breast and bowel screening Woodside and Shirley
Access and overall patient experience
Prescribing indicators Diagnosis rates for dementia
and CHD
Flu vaccine uptake
Childhood immunisations Care and outcomes for severe
mental illness and sexual health
High referral rates
New Addington and Selsdon
Breastfeeding; smoking during pregnancy
High emergency admission and A&E attendance rates in New Addington

Operating Plan 2015/16 Subject to NHSE Agreement Page 11 of 48
Improving quality and performance of services We strive to commission health services that are safe, that maintain or improve quality and offer information to inform patients’ choice on how, when and where they receive their health care services. We have effective quality assurance processes and have Clinical Quality Review meetings with our providers to ensure continued focus on improving quality. We also work with our providers to ensure that continuous improvement is made against the NHS Constitution measures. We have established weekly calls with providers to ensure risks are being mitigated. In addition, monthly System Resilience Group Meetings are held where the CCG monitors performance and reviews demand and capacity plans. The CCG Chief Officer leads fortnightly internal performance meetings.
Quality Improvement We continue to implement our Francis Report and Winterbourne action plans to ensure those that are most vulnerable receive the necessary high quality of care. Our focus is not only the national priorities but local priorities such as pressure ulcers and the quality of the provision in nursing homes. We will await the publication of the National Quality Board priorities to help us shape our quality agenda further.
We actively seek to reduce harm to patients. A review of a range of information enables us to address local issues for a range of providers including quality of care home provision. National priorities such as infection control or the new sepsis and acute kidney injury standards are managed locally with our providers. The 2015/16 contracts with acute providers include the national CQUINs on sepsis and acute kidney injury. We will continue our focus to reduce the use of antibiotics in primary care and the primary care Quality Premium target will be included in the 2015/16 Prescribing Incentive Scheme. We know that across a number of health services in Croydon, patients are reporting a poorer experience than those received elsewhere. In our local acute hospital, our community services, mental health services and patient experience services are below the national average (see Appendix 1). Satisfaction of our primary care services is just below the national average, although it has improved and is better than satisfaction across London.
Patient Safety – Reducing harm A steady decline in in the numbers of patients with new pressure ulcers as well as
the number of falls Fewer venous thromboembolism (VTE) than planned Fewer Clostridium Difficile infections than the 59 maximum planned for the year Reduced number of fractured neck of femur Medication reviews in care homes 1 midwife to 28 births achieved
Improving Patient Experience Rolling out Friends and Family Test in acute and mental health trusts and GP
practices Our Practice Development and Delivery Scheme include the requirement of
practices to demonstrate effective engagement with Patient Participation Groups as well as demonstrating learning and taking action from feedback
CQUIN initiatives for acute and community services to incentivise service improvements focused on urgent care access, including greater presence of emergency medicine consultants in ED, increased usage of out-of-hospital options and to facilitate earlier, safer discharge
18 new patient pathways that will mean patients are seen in the right place at the right time

Operating Plan 2015/16 Subject to NHSE Agreement Page 12 of 48
Joint commissioning of primary care services with NHS England means we are able to set our ambition for improvement with primary care. We will use the Friends and Family test, now being used in primary care, to help set this and to monitor progress. For our local acute, community and mental health services we continue to track progress and their developments for delivery. Our transformation plans also aim to improve the patient experience of the patient pathway.
We achieved the highest performance of all South London CCGs against delivering our 2013/14 quality premium, securing £1m for additional investment to improve quality. Whilst we have not met the national standard for IAPTs we are expected to have achieved against our local plans. The use of our £1m quality premiums money is set out in Appendix 4, as well as our plans for 2015/16. Francis and Berwick Reports The CCG has a Francis Report action plan which incorporates the findings of the Berwick Report, which is reviewed regularly by the Quality Committee. Each of the CCG’s main providers has a similar action plan in place. These are reviewed regularly by the Clinical Quality Review Groups, the CCG’s Quality Committee and the Health and Well-Being Board. Winterbourne View Report In 2011 there were 4 people in in-patient facilities - of that original group one remains in hospital. By 2015 there were 2 people in hospital wards (locked rehabilitation). There are no Learning Disability specific in-patient facilities in Croydon. If an admission is required it is via SLaM Adult Mental Health services or an out of area placement. We have begun a review of the full range of locally commissioned learning disability services including health and social care provision, delivered by statutory, voluntary sector and independent providers. As well as identifying where there may be gaps in provision a primary objective is to review the pathway for people with learning disabilities and complex behavioural needs to ensure that relevant services are in place to avoid unnecessary hospital placements. In addition we will consider the further guidance that the Department of Health is expected to publish soon. The number of individuals with the most complex needs who, at any one time, could benefit from these services will be relatively few in a particular health/Local Authority area. Therefore we will be
Our Quality Premium Achievements 2012/13 achievements Reducing avoidable emergency admissions Ensuring roll-out of the Friends and Family Test and improving patient experience
of hospital services Nine diabetes processes Multi-disciplinary team case management for people at home Reduction in numbers of admissions from care homes (nursing) Whilst we did not fully meet our plans for preventing healthcare associated infections and reducing potential years of lives lost through amenable mortality, we are expected to meet these for 2014/15. 2013/14 achievements Reducing avoidable emergency admissions Friends and Family Test (FFT) Improved reporting of medication-related safety incidents Increased referrals of people with diabetes diagnosed less in the past year to a
structured education programme

Operating Plan 2015/16 Subject to NHSE Agreement Page 13 of 48
working with our colleagues elsewhere in London or the surrounding area, to consider the appropriateness of shared commissioning options which would enable these services to be as close to home as possible for the individuals and their families. This could also offer significant benefits in relation to local monitoring of care as well as the opportunity to develop more effective relationships with the providers. Croydon’s services have traditionally benefited from having a strong and active Learning Disability Partnership (LDP) with representatives from service users and their carers, as well as from a variety of providers, local schools and advocacy organisations. People with a learning disability will continue to be involved in the service reviews and any proposals relating to commissioning changes. It should also be noted that reports have been made to the LDP on Winterbourne View and they will continue to be involved and updated on “Transforming Care”. Safeguarding: Adults and Children In order for the safeguarding team to provide assurance to the CCG that they are discharging their duty to safeguard, there are robust governance processes in place. The CCG Safeguarding Children and Adults Safeguarding Committee is chaired by the executive lead for safeguarding (chief nurse) and is held quarterly. This committee reports through an agreed line to the Governing Body and includes presentation of the six monthly safeguarding reports. It is the duty of the CCG to support improvement in the quality of primary medical care. In view of this, the safeguarding team has devised a model of case reflection (led by the deputy designated nurse) which provides an opportunity to consider cases of concern and develop practice with support from expert safeguarding leads. This has now been rolled out in 55 of our 58 practices. Each GP practice has an identified safeguarding lead for both children and adults. This is endorsed by GP quarterly safeguarding leads workshops, which also includes presentation from multi agency partners, in order to maintain awareness of local safeguarding processes and initiatives. Prevent Agenda: As members of the Community Safety Partnership Board (CSPB), the CCG has completed the Safeguarding Adults Board Audit Tool (NHSE), which included Prevent as part of the assurance. The Case Reflection model and GP Safeguarding Workshops has also helped to raise awareness in general practice.
Our safeguarding focus for 2015/16 Female Genital Mutilation (FGM) project: (funded through 2013/14 Quality
Premium monies - to invest £100k). This project will primarily focus on promoting the health and safety of women and girls affected by FGM in Croydon through collaborative work with the community and partners. The project will include the identification of a baseline, awareness raising through events and training and the development of relevant pathways
Review of the CCG Safeguarding Strategy in order to respond to new legislation, local and national initiatives
Finalisation of the work with the Integrated Commissioning Unit regarding the safeguarding element of contracts.
Further development of the relationship between the Integrated Commissioning Unit and the safeguarding team in order to ensure that safeguarding is considered in all levels of activity
Further development of quality assurance processes in order to have robust oversight of safeguarding activity and identify any areas of risk. These processes reflect the statutory requirements set out in s11 of the Children Act 2004 and s14 of the Care Act 2014
Collaborative work with the Local Authority and multi-agency partners in order to reduce the risk of harm to adults and children

Operating Plan 2015/16 Subject to NHSE Agreement Page 14 of 48
Performance Improvement The NHS Constitution sets out the national priority indicators. Throughout 2014/15 we actively managed performance with our providers and ensured progress in the delivery against these. Appendix 5 and 6 provides previous year’s performance as well as our plans for 2015/16. We will meet most of the national standards although there are some risks. Given the low baseline the CCG inherited we will be unable to meet the IAPTS access national standards during 2015/16. Urgent and Emergency Care Resilience A&E 4-hour waits – The target off 95% of patients waiting under 4 hours in A&E has
underperformed in 2014/15, with increased pressures due to a surge through the winter months, as well as perceived high acuity. For 2014/15 we expect to achieve 93.8% against 95% target.
The increased allocations for the CCG include winter resilience monies built into the baseline, facilitating earlier planning for winter. The System Resilience Group is developing an operational resilience strategy and plans for 2015/16. Given the current challenges the performance standard will be met on 2016/17 following the embedding of these plans. Plans include improving patient flow through the emergency department and the hospital, including effective discharge planning, developing innovative solution tackle workforce challenges, building intermediate care capacity and flex, facilitating discharges to nursing and care homes at weekends, enhancing therapies to ensure early rehabilitation on wards and follow up on discharge at the weekends, enhanced social care support at weekends and access to emergency services e.g. housing, staying put service and a more extensive social marketing campaign. Also see the Urgent and Emergency Care System Programme (see Appendix 9). Referral to Treatment (18 weeks) Overall Croydon CCG’s performance was compliant during 2014/15 although we had to actively
manage provider backlogs with planned dips in performance between July to November at CHS. St
George’s and Kings College Hospital backlog issues continue, which they expect to address by
quarter 2 at St George’s and from quarter 3 at King’s College Hospital. The CCG has prudently
assessed growth overall and reflected these increases in contracted activity, which will address
Referral to Treatment (RTT) delivery. We will monitor individual non hosted provider RTT activity
by speciality.
Cancer Waits We continue to deliver across the range of cancer waiting time indicators, with the exception of the 62-day standard for first GP-referrals, although performance has improved through the year. Croydon Health Services introduced a new Cancer Team, and implemented an action plan specifically to deal with improving the patient pathway and to prevent delays. The urology pathway redesign work will further improve performance during 2015/16, as well as the alignment with the South West London Commissioning Collaborative. The Cancer Programme (see Appendix 9) provides greater detail about plans for 2015/16.
Managing our challenges Sustainable four-hour A&E access target – delivered through the System
Resilience Group, through development and monitoring of the operational resilience plans
Being treated within 18 weeks (Referral to Treatment) – a focus on individual specialities and monitoring through the System Resilience Group
Cancer 62 day first GP referrals – a focus on individual specialities Improving Access to Psychological Therapies (IAPTS) indicators – a longer
term sustainable approach

Operating Plan 2015/16 Subject to NHSE Agreement Page 15 of 48
Mental Health Parity of Esteem The CCG inherited a position where mental health services started from a relatively low baseline with significant pressures. We committed to a steady journey over a number of years to stabilise services and transform community services to reduce inpatient need in the future and improve access. Following recent investment, including £5.2m during 2014/15, the CCG spend is now marginally above the average when benchmarked with similar CCGs. The full benefits to patients of this investment will be seen during 2015/16. In addition to this an additional £2.4m has been set aside for 2015/16 to increase the level of mental health provision further and to improve performance against existing and new national mental health standards. Subject to robust business cases this will be invested in Improving Access to Physiological Therapy Services, Early Intervention Service, Older People Community Services, Child and Adolescent Mental Health Services, Croydon Integrated Psychological Therapy Service Waiting Times, Assessment and Liaison Service, Crisis Line and the Perinatal Service.
All opportunities and models of care are being explored with SLaM and the voluntary sector to deliver economies of scale and efficiency. The mental health programme (Appendix 9) sets out our plans for 2015/16 on this journey to improve parity of esteem for mental health services. Increasing Access to Psychological Therapies (IAPTs) – national standard 15% -
Improving mental health services including the IAPTs roll out and new access targets, is a long term ambition, given we started from a low base. For 2015/16 we will achieve 8.16% (based on a prevalence of 42,245). This will increase to 11.5% in 2016/17 and 15% in 2017/18. (TBC)
Increasing Access to Psychological Therapies (IAPTs) Waiting Times – national standard 18 weeks 95%, 6 weeks 75% We will continue to meet both these standards from April 2015.
Dementia Diagnosis Rate (for over 65s) – national standard 66.7% - This is a new indicator specific to over 65s, and the data set is not available by age group at this time. We have estimated a target for 2015/16 based on national prevalence data and will achieve a diagnosis rate of 60% for 2015/16, and 66.7% in 2016/17. We expect an appropriate dataset to be published May 2015 and we will review these plans if necessary.
Choice: Maternity We continue to promote choice about where women deliver; monitoring the numbers that deliver in and out of borough. The CCG have set robust targets in ensuring that midwifery led care is the norm within Croydon. We have also set targets for the percentage of women with uncomplicated pregnancies who deliver at home. The maternity commissioner is part of the Maternity Services Liaison Committee (MSLC) which brings all stakeholders together to ensure that the views of expectant mothers and parents are heard and their views are embedded in service delivery and development. Choice: Mental Health The recently produced Mental Health Strategy 2014-2019 makes clear at the outset the CCG and Council’s commitments to service user choice and to personal budgets and the choices that a personal budget can facilitate. This is a clear driver to ensure there is a range of different providers and types of services to encourage and ensure genuine choice. Seven day services For 2015/16 we are working with our local care providers to further the achievements, cementing progress and incentivising further development where we feel that this is required in order to achieve the clinical standards for seven day working. We have planned for contractual Key Performance Indicators as wells as CQUINs to support this.

Operating Plan 2015/16 Subject to NHSE Agreement Page 16 of 48
Seven day services - Key Performance Indicators Emergency medicine consultant presence: emergency medicine consultants
deliver clinical care in the ED for 16 hours a day, seven days a week (ED2) Paediatric consultant peak time presence: a consultant paediatrician is readily
available during times of peak emergency activity – at a minimum up until 10pm, seven days a week (P4)
Quality of care for fractured neck of femur patients: all patients considered for pre-operative optimisation by critical care; and patients routinely offered fascia iliaca block post-admission
Seven day services – CQUINS Reduce emergency admission rates, which has been included as a CQUIN Inter-hospital transfer standards (LQS) – which includes full achievement of each
of the adult and paediatric inter-hospital transfer London Quality standards by the end of Q4 2015/16
7 day responsiveness of community services - increased presence of therapy staff on the wards on Sundays, to increase the number of discharges on Sundays

Operating Plan 2015/16 Subject to NHSE Agreement Page 17 of 48
Transforming services We have already described the challenges health and social care are facing. In order that we can address the needs that result from the changes in population, service quality and service performance we must fundamentally change how we commission, deliver and use health and care services. This is not about unnecessary structural change; it is about finding ways of doing things differently to ensure that services are sustainable for the future. Our transformational programme will mean we will work towards less reliance on hospital care through improved primary and community provision and continuing to develop our approach to prevention, self-care, and shared decision making. We will work with the South London Health Innovation Network to support the development of our plans for 2015/16 given their priorities of diabetes, alcohol, musculoskeletal, dementia and cancer. This is reflected in our delivery programmes (see Appendix 9). The diagram and table below set out how we will change the focus of health and health care over the next few years and our expected shifts in care settings.
A&E Urgent Care
A&E & Urgent
Care
NEL Maternity Total Elective
First OP All other OP
attend
Baseline: 2014/15 M11 FOT SUS
97,911 36,640 134,551 37,865 7,057 37,586 130,535 374,528
Growth 3,897 1,458 5,355 2,420 162 1,902 3,303 9,476
Less QIPP -7,984 6,718 -1,266 -3,002 - -476 -4,512 -14,068
Total Net -4,087 8,176 4,089 -582 162 1,426 -1,209 -4,592
Revised year on year growth (%)
3.98% 3.98% 3.98% 6.39% 2.30% 5.06% 2.53% 2.53%
2015/16 Activity 93,824 44,816 138,640 37,283 7,219 39,012 129,326 369,936
Growth in 2015/16 (%) -4.17% 22.32% 3.04% -1.54% 2.30% 3.79% -0.93% -1.23%
The planned growth/reduction in activity for 2015/16 has been built up based on the following elements for each point of delivery (POD): Projected population growth (1.1%) Projected additional growth in demand based on the last four years average annual growth Activity avoided through our clinically led QIPP schemes (aggregated from individual projects) We recognise that the assumptions around reducing non-elective care are challenging. Nevertheless, given our financial position and growth in short stay emergency admissions it is imperative our transformational plans and QIPP schemes achieve these. These are:

Operating Plan 2015/16 Subject to NHSE Agreement Page 18 of 48
Prevention, Self Care and Shared Decision Making
• Enabling residents and patients to take greater responsibility for their health
• Tackling self care for minor ailments; improving the appropriate use of health and care services; supporting self-management for people diagnosed with long-term conditions; increasing levels of shared decision making between patients and clinicians
• Focus for 2015/16 - diabetes, respiritory, musculoskeletall, urgent care, Effective Commissioning Initiatives
Transforming Care
•Croydon CCG aims to support people to commission their own care and support through Personal Health Budgets (PHB). From October 2014, those in receipt of NHS Continuing Healthcare have the right to a PHB, which will allow care and support to be organised that meets their needs
•Working with our local care providers to further develop 7 day working, as well as with the SWL Commissioning Collaborative. We have planned for contractual KPIs: emergency medicine consultant, paediatric consultant, fractured neck of femur. These will lead to reduced emergency admission rates which has been included as a CQUIN as well as inter-hospital transfer standards (LQS) and 7 day responsiveness of community services.
Outcomes Based Commissioning (OBC) for Older People Services
• Jointly with the Local Authority use new models of care to improve health and social care services for over 65
• Ensure services incentivise a focus on proactive care that keeps people healthy and at home
• Focus for 2015/16 - working with partners to consider the model of service
Better Care Fund (BCF) and Transforming Adult Community Services (TACS)
• Ensure integrated health and social care through a local single pooled budget to incentivise the NHS and local government to work more closely together around people
• Focus for 2015/16 - implementation of a roving GP service to provide GP response to patients with urgent care needs; improving clinical support and competencies in care homes; stream line existing ‘A&E Front of House’ services
Transforming Primary Care
• Co comissioning with NHS England, will enable us to develop integrated out-of-hospital services based around the needs of local populations
• Focus for 2015/16 - to establish governce arrangements
• Reducing variation - ensuring the reduction of unwarranted variations in primary care including diagnosis rates , referrals and health outcomes
• Focus for 2015/16 - to set specific targets for each network
Integrated Primary and Acute Care System (PACS)
• Collectively the health and social care economy to develop an integrated primary and community care system (PACS) including the model of enhanced health in care homes
• Focus for 2015/16 - to prototype a new risk stratified care model for the over 65 population that delivers person-centred, co-ordinated, holistic care that best meets the needs of patients and service users
Whole System Pathway Redesign
• Transforming the patient’s journey through the care pathway ensuring earlier identification of patients; decreased waiting times before appropriate treatment; a reduction in inappropriate referrals and treatment in secondary care; a reduction in complications; and better patient experience across a seamless pathway. In addition, it will increase efficiency within the system with significant savings.
• Focus for 2015/16 - embed 18 pathways initated in 2014/15 and identify new pathways focusing on planned care and the managment of long term conditions
Quality, Innovation, Productivity and Prevention (QIPP) (see Appendix 7)
•Ambitious plans to improve the quality of services whilst making them more efficient and cost effective
•Focus for 2015/16 - Delivery of £10.5m schemes to improve quality more effectively

Operating Plan 2015/16 Subject to NHSE Agreement Page 19 of 48
Our programmes of delivery Given our ambitious long term strategy and the successful delivery of our plans to achieve this vision, our key focus of delivery for 2015/16 will be proportionate to current progress.
Delivery of our plans is underpinned by a robust programme management approach and effective contract management. We have aligned our contractual levers to support providers to stretch some of our ambitions, and this can be found in Appendix 4. Our clinical leaders have been integral to the development of implementation plans and our GP networks are integral to implementation. To support delivery of the plans, GP networks are aligned with the operating plan based on the networks population and service challenges. Set out below are areas our networks are considering. These will be finalised by June as part of the Practice Development and Delivery Schemes (see Primary Care Programme in Appendix 9)
GP Network Areas Being Considered (To be confirmed by June)
East Croydon Cancer Screening, Diabetes, Mental Health incl. Dementia, Nursing/Care Homes, COPD
Mayday Asthma, Diabetes, Cancer Screening, Obesity
New Addington / Selsdon Cancer Screening, Nursing/Care Homes, Mental health incl. Dementia, Musculoskeletal Referrals, Anticoagulation
Purley Care homes, Musculoskeletal Referrals, Dementia, Nursing Homes, Learning Disabilities
Thornton Heath Admissions, COPD, Cancer Screening
Woodside /Shirley Diabetes, Mental health incl. Dementia, Chronic Kidney Disease, Musculoskeletal Referrals
Appendix 9 provides an overview of each of our workstreams, and set out below are our key
service changes for 2015/16.
Embedding:
- 18 pathways
- Transforming Adult Community Services and Better Care Funds (plus 3 new services)
Further focus to ensure sustainability in:
- Mental health (IAPT’s, Older Adult Mental Health)
- Urgent and emergency care (system resilience)
Preparedness for:
- Urgent Care procurement - Outcomes Based Commissioning for Older People (incl. Primary and Community Care Model)
Significant focus on:
- Prevention, Self Care, Shared Decision Making (diabetes, respiratory, MSK, urgent care)
- Transforming Primary Care (Co-commissioning, primary care variation, support GP collaboration)
Our organisational focus for 2015/16 is proportionate to current progress

Operating Plan 2015/16 Subject to NHSE Agreement Page 20 of 48
2015/16 Priority Area Focus for 2015/16
Prevention, self-care, shared decision making
Diabetes, respiratory, MSK, urgent care and Effective Commissioning Initiative
Mental health
Older Adult Mental Health Services redesign Primary Care Liaison Services Early Intervention Service redesign Enhanced community teams Crisis Concordat implementation Improving Access to Psychological Services (IAPTs) mixed
model implementation
Older people
Outcomes based commissioning preparation for implementation
Urgent and emergency care system
System resilience development Urgent care model reviewed and procurement preparation
Primary care and primary care variation
Co commissioning implementation Primary care variation identified by network and plans in place
to reduce Integrated primary and acute care system (PACS) including
the model of enhanced health in care homes GP Collaboration facilitation
Other workstreams Focus for 2015/16
Adult community services GP roving service implemented Front House of A&E improvement through co-ordination of
services Nursing and Care Homes programme of review and enhanced
support
Community Intermediate Services
Review of all intermediate services
End of Life A named GP for all care homes
Integrated Cancer Services London pathways implementation of London Pathways
Planned care Effective Commissioning Initiative (ECI) review and further changes in year
Croydon Referral System and Assessment Service – implementation of review recommendations including Consultant to Consultant referrals and ECIs

Operating Plan 2015/16 Subject to NHSE Agreement Page 21 of 48
Enabling transformation
Organisational Development, Leadership and Innovation Leadership development is important to being able to deliver transformational change in financially challenged times. We have begun a significant organisational development programme to further develop our Governing Body, clinicians and managers. The CCG has five strategic organisational development priorities: 1. A CCG that is recognised by the community as having its interests at heart 2. An engaged and lively membership that believes it is part of the CCG and shaping its agenda 3. A strong and shared leadership with longer term succession 4. A commissioning organisation that integrates and that builds the experience and skills of staff
making the CCG a desirable place to work 5. A strong and durable partnership with the Local Authority in forging a new shared
commissioning agenda for outcomes Clinical leadership is a key component of our plans, empowering clinical leaders to bring about change supported by managers who back good ideas and turn clinical decisions into practice. To ensure the organisation is fit for purpose going forward we are developing an Organisational Development Plan for delivery during 2015/16, with senior leadership and programme management across a number of work streams.
Patient and Public Engagement We want to be an open and listening organisation that has the needs of local people at its heart and delivers real benefits through collaborative and partnership working. Croydon Clinical Commissioning Group (CCG) is dedicated to commissioning the best possible services for the people of Croydon. A key component of our work is ensuring that we communicate and engage with our patients, the wider health and social care community, and our local stakeholders. The CCG has established a framework for patient and public engagement that will ensure patient and community views are integral to the commissioning work of the CCG.
We continue to develop an infrastructure to ensure patient and community views are integral to our work, at corporate, community and practice levels.
We are delivering our engagement work plan 2014/15 and are working with patients to update the strategy and work plan for 2015/16. Our new engagement strategy will aim to strengthen and build upon the engagement work we have already done, and to help ensure patients, public and stakeholders.
Our organisational development plan Leadership and People Development and Vision Vision, Values, Behaviours, and Culture Communications and engagement Recruitment, Retention, Performance & Reward

Operating Plan 2015/16 Subject to NHSE Agreement Page 22 of 48
We hold a Patient and Public Forum open meeting each quarter at which we give an update on the latest developments and the key issues and have conversations to hear people’s views about specific topics of interest to inform the development of commissioning plans. We have a Patient and Public Involvement Reference Group through which we discuss priorities for, and approach to future engagement with representatives from Healthwatch, patient participation groups, other community groups and local stakeholders. Attached at Appendix 8 we set out the some of the engagement we will be taking forward during 2015/16.
Local Partnership Working Croydon health and social care have a good record working in partnership to improve health and well-being. Local stakeholders are an active partner in our transformation programme. Our Transformation Board leads the transformation agenda in Croydon overseeing the development and implementation of some of our transformational plans such as Transforming Adult Community Services. Jointly with the Local Authority, we have engaged with our main provider Croydon Health Services (CHS) about Outcomes based Commissioning for Older People. We have established a joint Quality, Innovation, Productivity and Prevention (QIPP) Group with CHS to support the development of ideas and implementation of plans. Our voluntary sector strategy means we have set out an approach to support the development of the voluntary sector and ensure commissioning recognises the benefits the voluntary sector can bring. Co – commissioning of primary care medical services with NHS England will further support our transformation programme enabling commissioning across all pathways. We will continue to seek new ways of working together to achieve better value for money and transform services, embedding a culture of efficiency within our respective organisations to enable the funding of new and changing service demands and expectations. To ensure we achieve greater commissioning efficiencies we have established with the Local Authority an Integrated Commissioning Unit, to ensure both our commissioning plans are aligned, where possible, to bring greater benefits to patients.
Our patient and public engagement plan Better engagement with more people from diverse communities Ensure that the views of public, patients, and carers are at the centre of every
decision that we make Work collaboratively with other groups and organisations Deliver engagement work that contributes effectively to improving the quality of
services
Our implementation focus for 2015/16 Ensure engagement is undertaken systematically throughout the commissioning
cycle Ensure targeted engagement with those from black and minority ethnic groups

Operating Plan 2015/16 Subject to NHSE Agreement Page 23 of 48
Transforming estates The CCG is not responsible for the health estate; however we have a role in ensuring we plan effectively for our estate to meet our commissioning needs. There are a number of housing developments in Croydon which will impact on the demand of health services. Our transformation programme means that we want to ensure care is closer to home, and we are aware that many GP practices are too small for their current registered population. Working in partnership with the NHS Property Service, NHS England and local providers, we will develop an estates strategy to ensure we understand our needs for the future and have a plan to address them.
Managing information and IT Information and IT management are recognised as key enablers to drive forward our commissioning strategy. We are in the process of finalising our Information and IT Strategy for primary care and for the CCG, which sets out our key objectives as: Make information more accessible to patients and staff Increase integration so that information is shared across care settings Improve data quality Use information to monitor health outcomes, support commissioning and measure patients’
experience of local services There are a number of themes in the draft strategy that address the key strategic objectives for Managing Information and IT and these will be reviewed and prioritised early in 2015/16.
Our implementation focus for 2015/16 Finalise the Information and IT Strategy by May 2015 Prioritise our focus for 2015/16
Clinical dashboard embedding risk stratification Integration and record sharing Patient Online – Patient Access to GP Systems Mobile Medicines – Medicine on the Move Primary Care Infrastructure Development Primary Care Pathway Decision Support
Our implementation focus for 2015/16 Outcomes Based Commissioning for Older People is further developed in
preparation for procurement in 2016/17 Development of joint commission of primary care medical services Review our voluntary sector contracts to ensure greatest benefits are achieved
Our implementation focus for 2015/16 Understand needs for the future Develop an estates strategy to address the needs

Operating Plan 2015/16 Subject to NHSE Agreement Page 24 of 48
Our providers of health services Our transformational programme requires providers to look differently at how services are provided. Transforming the health care system through transformational change will require fundamental changes to the way health services are provided. Health staff will need to be trained, recruited and deployed accordingly. Staff will be required to work in different and more flexible ways and to deliver new care pathways that will be predominantly in a community or primary care setting. Therefore, a planned shift of services and staff from acute to primary and intermediate care settings will be required with the creation of more joint roles across agencies.

Operating Plan 2015/16 Subject to NHSE Agreement Page 25 of 48
Risks to delivery There is an established method to identify, monitor, control and mitigate risks throughout the
organisation as part of and within the CCGs Risk Management Framework.
We have identified high level risks associated with the scale and pace of transformation required in
the plan period which are as follows. Specific financial risks are considered on page 32.
Risk S L R Mitigating actions S L R
Risks to implementation of initiatives:
Unable to increase transformation programme due to staff capacity, resources, capability
4 4 16 OD plan focused on developing and securing skills Recruitment campaign underway Lead Director: Director of Governance and Quality
4 3 12
Insufficient provider workforce staff capacity or capability
4 4 16 Upskilling current community workforce as part of initiative implementation
OBC will require providers to plan for a shift of staff from acute to primary and intermediate care settings with the creation of more joint roles across agencies
Working with Community Education Provider Network (CEPN) to develop range of primary care workforce
SWL Commissioning Collaborative working to develop community staffing approach
Health Education England will lead the implementation of the Shape of Training Review for the medical profession
Lead Director: Director of Commissioning
4 3 12
Risk of initiatives not having expected impact:
Innovative approaches not proven to be effective
4
4
16
Regular reviews of impact and plans revised as necessary
Pilot new approaches
Ensure evidence based decision making Lead Director: Director of Commissioning
4
3
12
Poor provider performance or failure to meet improvement plans/trajectories
4 4 16 Joint QIPP Group with CHS Use of performance levers e.g. improvement notices
in contract Use of short term action plans Service redesign and re-commissioning Lead Director: Director of Commissioning / Director of Finance
4 3 12
Risks from lack of interaction with stakeholders and partners:
Public opposition to service changes
4 3 12 Clinical leadership to make case for changing Extensive engagement and communications to
inform and build understanding Lead Director: Director of Commissioning
3 2 6
Old ways of delivery are retained by organisations / individuals
4
3
12
Clinical leadership to promote new ways All partner organisations on the Transformation
Programme Board Lead Director: Director of Commissioning
4
2
8
Lack of buy in to proposals due to diverse agendas,
4
4
16
Effective engagement and consultation processes, sharing learning and good practice
Exploring new and innovative initiatives with
4 2 8

Operating Plan 2015/16 Subject to NHSE Agreement Page 26 of 48
Risk S L R Mitigating actions S L R
financial constraints and expectations
stakeholders Lead Director: Director of Commissioning
S= severity, L=likelihood, R=Risk
The key impacts of these risks have been identified as being unable to: Achieve health improvement /disease management targets Achieve financial plans Address the longer term impacts on health and well being and potential future burden of
disease Realise the shift in activity from acute to community care through demand management,
planned care and other initiatives Achieve performance targets and national standards

Operating Plan 2015/16 Subject to NHSE Agreement Page 27 of 48
Achieving financial balance
Historic financial position On establishment in April 2013, Croydon CCG inherited, from its predecessor Croydon PCT, a significant recurrent financial short-fall between resources allocated and demand for health services (£33.9m recurrent deficit). The expenditure profile of Croydon CCG was benchmarked by external consultants in March 2013, concluding that the savings opportunity alone, even if delivered in full, would not address the financial position. It is of note that Croydon is one of the most cost effective prescribers in England, but also had below average investment in mental health services. Over the past two years since its inception, the CCG has successfully delivered better than plan:
Plan Outturn Variance
2013/14 £19.9m £18.2m £1.7m Fav
2014/15 £17.0m £14.7m £2.3m Fav
cumulative £36.9m £32.9m £4.0m Fav
The CCG has also successfully delivered a £14m QIPP plan in 2013/14 and £11m in 2014/15. This was over and above the QIPP achieved in the final two years of the PCT (£38.2m). The legacy of the inherited financial position has been under investment in community services and primary care, and under investment in mental health services. The CCG has not invested sufficiently in IAPT services and has long waiting list for CIPTs. A significant £4m cost pressure on acute mental health inpatient beds arose in 2013/14 as a consequence. During 2014/15, the CCG has taken steps to address this under investment and the following investments were made: Adult Mental Health - £5.2m (inclusive of £1.5m on Community) IAPT - £700k Community (Transforming Adult Community Services) - £2.4m
Programme allocations The 2013/14 funding gap (distance from target) between the CCG’s actual allocation (£392m) and target allocation (£432m) was assessed by NHS England (December 2013) as £42m (£10.3%). The allocations for 2014/15 and 2015/16 have confirmed additional “pace of change” funding to close the funding gap:
Actual Allocation
Target Allocation
Additional Funding
Growth Closing Distance from Target
2014/15 £406m £449m £13.9m 3.55% -9.61%
2015/16 £434m £466m £14.9m 6.94% -6.87%
It is anticipated that the CCG will receive an additional £8.7m in 2016/17 which would reduce its funding gap to £23m (5%). Included within the 2015/16 allocation is £2.2m funding for systems resilience which was previously received non-recurrently. The CCG is also anticipating non-recurrent allocations for primary care IT and the Quality Premium. These have not yet been factored into our plans.
Impact of allocations The CCG has received additional growth funding in 2015/16 of £14.9m above both local planning assumptions (£8.5m) and national average assumptions (£4.7m).

Operating Plan 2015/16 Subject to NHSE Agreement Page 28 of 48
The assumption on tariff deflator for 2015/16 (-0.5%) is worse than previous planning assumptions submitted in April 2014 (-1.1%) and factors in the majority of our acute providers accepting the Extended Tariff Offer consulted on by the Department of Health. This has resulted in a £1.4m cost pressure to the CCG. Whilst underlying planning assumptions on demographic and non-demographic growth have not changed materially, the CCG has found it necessary to increase its QIPP challenge to £10.5m (previously identified £9.5m) due to the significant cost and investment pressures on Mental Health as a result of Parity of Esteem (£2.4m) and changes to NETA as a result of the increase in the threshold from 30% to 70% (£4.8m). It should be noted that the expected benefit from the impact of the development of Outcomes Based Commissioning for Older People is profiled to impact from 2017/18. Work is continued to be progressed in this area. The table below summarises the overall impact of allocations, QIPP and cost pressures which move the CCG from a business rules deficit of £24.9m in 2013/14 to a business rules deficit of £21.1m in 2014/15 and £13.9m in 2015/16.
In-Year Cumulative
Recurrent Deficit
Return of Non
Recurrent Funding
Reported In-Year Position
Prior Year Deficit
Total Cumulative
Deficit
£m £m £m £m £m
2013/14 24.9 (6.7) 18.2 - 18.2
2014/15 FOT 21.1 (6.4) 14.7 18.2 32.9
2015/16 Plan* 13.9 - 13.9 32.9 46.8
* This draft plan is subject to further clarification re funding to support the choice exercised by providers regarding the 2015/16 tariff deflator and marginal rate for emergency activity (NETA).
Health economy position and strategic change The Croydon Health Economy has a significant financial challenge. For 2014/15, the CCG is forecasting a cumulative deficit of £32.9m and Croydon Health Services NHS Trust is forecasting a deficit of £23.4m. Croydon has both a growing and ageing population, placing increased pressures on the health and social care system. Over 65s represent nearly 13% of Croydon’s total population, and this number is growing - over the next five years, the number of over 65s living in Croydon will have grown by 10%. The pressures on the system from this age group will continue to grow over the next decade - the number of over 65s living in a care home, for example, is projected to have grown by nearly 24% by 2020. The initial priority of the CCG’s transformation strategy is frail and older people with long term conditions, with the approach outlined within the transformation strategy closely aligned with the values of an outcome based approach. A key focus is placed on integration and collaboration across the care economy, defined by a whole systems approach to service delivery which will have the benefit of alignment of the provider, commissioner and public goals. This will impact from 2017/18. The Strategic Resilience Group is developing an operational resilience strategy for 2015/16. The CCG has an allocation of £2.2m to support this in addition to the potential positive impact of the tariff change to the NETA and use of CQUIN against agreed outcomes. A number of new initiatives have been identified that will potentially require the additional funding of £2.2m. The detail of these plans is currently being developed. They include: building intermediate care capacity and flex, facilitating discharges to nursing and care home at weekends, enhancing therapies to

Operating Plan 2015/16 Subject to NHSE Agreement Page 29 of 48
ensure early rehabilitation on wards and follow up on discharge and at the weekends, enhanced social care support at weekends and access to emergency services e.g. housing, staying put service and a more extensive social marketing campaign. For 2015/16, the CCG has set aside £2.4m to deliver parity of esteem in Mental Health access targets. £1m of this is committed from 2014/15 developments. There is currently active dialogue with South London and the Maudsley Mental Health NHS Trust on a bottom up review of the investment required to achieve these targets.
Finance and activity plans The CCG and CHS NHS Trust are working together to agree the finance and activity plans by the 7 April. The financial baseline has been agreed in principle and the CCG QIPP plans have been shared with the Trust setting out the analysis of potential savings at HRG level. These savings have been modelled through the CCGs 2015/16 activity plans. The highest area of growth is in Non-Elective admissions, and this has been a focus of the 2015/16 QIPP plan, in line with the BCF plan, and the aim to reduce Non-Electivity Admissions. A breakdown of our growth and activity assumptions is set out below:
A&E Urgent Care
A&E and Urgent
Care
NEL Maternity Total Elective
First OP
All other OP attendances
Baseline: 2014/15 M11 FOT SUS
97,911 36,640 134,551 37,865 7,057 37,586 130,535
374,528
Growth 3,897 1,458 5,355 2,420 162 1,902 3,303 9,476
Less QIPP -7,984 6,718 -1,266 -3,002 - -476 -4,512 -14,068
Total Net -4,087 8,176 4,089 -582 162 1,426 -1,209 -4,592
Revised year on year growth (%)
3.98% 3.98% 3.98% 6.39% 2.30% 5.06% 2.53% 2.53%
2015/16 Activity 93,824 44,816 138,640 37,283 7,219 39,012 129,326
369,936
Growth in 2015/16 (%) -4.17% 22.32% 3.04% -1.54% 2.30% 3.79% -0.93% -1.23%
The CCG has a track record of owning and delivering against the quality and financial challenge in Croydon. There is a clinically led and quality based approach to driving efficiency and performance gains. In 2014/15, the CCG received £1m additional quality premium funding representing 56% performance against the quality standards, one of the highest in London. The CCG continues to operate its Project Management Office and QIPP Operational Board governance structure. Under this governance structure, the CCG has developed a QIPP programme of £11.4m (net) against a target of £10.5m for 2015/16. Approximately 56% of the QIPP schemes are rag assessed as GREEN or AMBER – this metric is expected to be continually developed as schemes are signed off, following further internal and external review. Key elements of the programme are (i) transforming community services, (ii) new care pathways (including musculoskeletal, Effective Commissioning Initiatives, End of Life, COPD, signed off by clinical leaders and (iii) further savings on prescribing and continuing care. The majority of PIDs had been signed off by 31 March 2015. The CCG is engaging further support to extend the QIPP programme and to support the operational and financial planning. The scope of this is covering (i) updated benchmarking on QIPP opportunity, (ii) supporting the refresh of our 3-5 year plan and (iii) external clinical review of the 2015/16 QIPP programme.

Operating Plan 2015/16 Subject to NHSE Agreement Page 30 of 48
Expenditure The expenditure model has been developed based on Month 9 forecast outturn for 2014/15, adjusted for non-recurrent items, followed by assumptions on tariff efficiency, inflation, growth, cost pressures and QIPP plans as outlined above.
The 2015/16 opening baseline is a £12.6m deficit after adjustment for non-recurrent items. In addition, the following cost pressures are reflected in the financial plans:
Cost Pressure 2015/16 Draft Plan (Feb 15)
£m
Better Care Fund transfers £3.7m
Non Elective Threshold Adjustments – Change in Marginal Rate relief £4.8m
London Ambulance Service – continuation of 2014/15 funding to support performance.
£0.7m
Mental Health Parity of Esteem £1.4m
Operational Resilience £2.2m
Learning Difficulties – increase in Step Down bed provision £0.5m
Non Elective Threshold Adjustments – Specialised and Service Transfers £0.5m
NHS111 £0.1m
Total £13.9m
Key Assumptions
2015/16 2016/17 2017/18 2018/19
Growth £ £28.0m £18.5m £9.0m £9.2m
Total £ £434.2m £452.6m £461.7m £470.9m
Growth % 6.90% 4.26% 1.99% 1.99%
Inflation 3.00% 4.20% 3.20% 3.20%
Efficiency -3.50% -3.80% -3.80% -3.80%
NET -0.50% 0.40% -0.60% -0.60%
Demographic Growth 1.10% 1.10% 1.10% 1.10%
Acute 3.60% 2.60% 2.60% 2.60%
Prescribing 3.90% 5.90% 5.90% 5.90%
Continuing Care 4.90% 4.90% 4.90% 4.90%
Non Acute 0.00% 2.00% 2.00% 2.00%
Contingency (0.5%) 0.50% 0.50% 0.50% 0.50%
Non Recurrent Funds (1.0%) 1.00% 0.75% 0.75% 0.75%
Transformation Funds 0.00% 0.00% 0.00% 0.00%
QIPP £10.5m £8.4m £6.9m £6.9m
OBC £0.0m £0.0m £1.5m £1.5m
% 2.42% 1.86% 1.82% 1.78%
Non
Demographic
Growth
Allocations
Deflator
Business Rules
Efficiency

Operating Plan 2015/16 Subject to NHSE Agreement Page 31 of 48
Reconciliation from the 2014/15 forecast outturn to the 2015/16 planned deficit is detailed below:
Better care fund In 2014/15 the s256 reablement allocation increased from £5.0m to £6.4m. This was payable direct by NHS England to the Local Authority. In 2015/16, the CCG will receive the £6.4m funding recurrently, and in turn the CCG will contribute £21.5m (including £15.1m of its own resources) to the Croydon Better Care Fund. This has resulted in a £3.7m cost pressure of which £0.8m has been identified to fund additional initiatives to deliver the 3.5% NEL admission reduction. The current QIPP programme is still in development

Operating Plan 2015/16 Subject to NHSE Agreement Page 32 of 48
and identifies a shift of 2.83% in NEL admissions (amounting to £6.7m gross QIPP) particularly in Transforming Adult Community Services, End of Life Care, Cardiology and Falls and Bones. The Better Care Fund was signed off by the Health & Wellbeing Board on 11 September 2014.
Key risks The following are the key risks facing Croydon CCG over the next year: Implications of the “tariff choice” offered to providers including impact on the deflator and
marginal rate on non-elective activity, Provider business cases on pricing and service developments. NHSE/TDA arbitration guidance on KPIs (£2.0m) LAS Deficit (second £0.7m) Application of 2015/16 PbR (£2.3m) Demand growth estimates (acute, prescribing) Transformation funds – LHC/SWL (£5.0m) Delivery of limited QIPP opportunity Development and implementation of outcomes based commissioning Key mitigations are: 0.5% mandatory contingency 0.5% SWL Risk Pool (access to £8m) Performance element of BCF (up to £1.8m) Delay MH investments (risk to patients) Restructure CCG to focus on primary care variation External support to strengthen QIPP delivery
Primary care co-commissioning NHSE invited proposals for co-commissioning primary care medical services with CCGs and we will now be co commissioning with NHS England which means we will be better able to set our ambition for improvement with primary care. Initial data that has been shared indicates current expenditure is circa £45m which is broadly in line (1.4% below) with needs based target allocations. For 2015/16 the resources and risk will remain with NHSE under potential Joint Commissioning arrangements.
New investments There are no new planned investments within the plan other than the funding earmarked for delivery of QIPP as part of the overall net QIPP programme and the funds earmarked for investment into the Mental Health parity of esteem access targets.

NHS Croydon CCG Annual Operating Plan 2015-16 Page 33 of 48
Appendix 1 National outcomes framework indicators by domain progress
1 Preventing people from dying prematurely
Overarching indicators
National
Indicator Value
Croydon
Indicator Value
1a.iPotential Years of Life Lost (PYLL) from causes considered
amenable to healthcare - Adults (Male)3,167.8 3305.8
1a.iPotential Years of Life Lost (PYLL) from causes considered
amenable to healthcare - Adults (Female)2,470.0 2083.4
1a.ii Children and Young People (Males) 486.5No Data
Available
1a.ii Children and Young People (Females) 478.9No Data
Available
1b.i Life expectancy at 75 - Males 11.3 11.5
1b.ii Life expectancy at 75 - Females 13.0 13.3
Improvement Areas
1.1 Under-75 mortality rate from cardiovascular disease 76.6 78.2
1.2 Under-75 mortality rate from respiratory disease 33.2 31.4
1.3 Under-75 mortality rate from liver disease 17.7 15.8
1.4 Under-75 mortality rate from cancer 141.5 116.4
1.4.i One-Year survival from all cancers 68.2No Data
Available
1.4.ii Five-Year survival from all cancers 47.9No Data
Available
1.4.iii One-Year survival from breast, lung and colorectal cancer 69.5No Data
Available
1.4.iv Five-Year survival from breast, lung and colorectal cancer 51.4No Data
Available
1.5Excess under-75 mortality rate in adults with serious mental
illness347.2 326.4
1.6.i Infant mortality 4.0 3.9
1.6.ii Neo-natal mortality and stillbirths 7.6 9.1
1.6.iii Five-Year survival from all cancers in children 81.3No Data
Available
1.7Excess under-60 mortality rate in adults with a learning
disability
2 Preventing people from dying prematurely
Overarching indicators
National
Indicator Value
Croydon
Indicator Value
2Health-related quality of life for people with long-term
conditions0.743 0.748
Improvement Areas
2.1Proportion of people feeling supported to manage their
condition65.1 59.5
2.2 Employment of people with long-term conditions 13.2 0.8
2.3.iUnplanned hospitalisation for chronic ambulatory care
sensitive conditions (all ages)820.5 1011.6
2.3.iiUnplanned hospitalisation for asthma, diabetes and epilepsy
in under-19s340.6 425.1
2.4 Health-related quality of life for carers 0.804 0.803
2.5 Employment of people with mental illness 36.8 18.4
2.6.i Estimated diagnosis rate for people with dementia 48.7No Data
Available
2.6.iiA measure of the effectiveness of post diagnosis care in
sustaining independence and improving quality of life
3 Helping people to recover from episodes of ill health or following injury
Overarching indicators
National
Indicator Value
Croydon
Indicator Value
3aEmergency admissions for acute conditions that should not
usually require hospital admission (all ages)1204.3 1146.9
3bEmergency readmissions within 30 days of discharge from
hospital11.78 12.62
Improvement Areas
3.1.iTotal health gain as assessed by patients for elective
procedures - Hip replacement30,721
No Data
Available
3.1.iiTotal health gain as assessed by patients for elective
procedures - Knee replacement24,009
No Data
Available
3.1.iiiTotal health gain as assessed by patients for elective
procedures - Groin hernia5,837 266
3.1.ivTotal health gain as assessed by patients for elective
procedures - Varicose Veins2,256 80
3.1.vTotal health gain as assessed by patients for elective
procedures - Psychological Therapies
3.2Emergency admissions for children with lower respiratory
tract infections371.2 252.8
3.3 An indicator on recovery from injuries and trauma
3.4Proportion of stroke patients reporting an improvement in
activity/lifestyle on the Modified Rankin Scale at 6 months
3.5.iProportion of patients with a fragility fracture recovering to
their previous levels of mobility at 30 days24.0
No Data
Available
3.5.iiProportion of patients with a fragility fracture recovering to
their previous level of mobility at 120 days50.3
No Data
Available
3.6.iProportion of older people (65 and over) who were still at
home 91 days after discharge from hospital into 81.9 85.2
3.6.iiProportion offered rehabilitation following discharge from
acute or community hospital3.3 2.2
To be developed
To be developed
To be developed
5 Treating and caring for people in a safe environment & protecting them from avoidable harm
Overarching indicators
National
Indicator Value
Croydon
Indicator Value
5a Patient safety incidents reported - 5.9
5b Safety incidents involving severe harm or death - 0.13
5c Hospital deaths attributable to problems in care
Improvement Areas
5.1Deaths from VTE related events within 90 days post
discharge from hospital69.8
No Data
Available
5.2iIncidence of healthcare-associated infection - MRSA
bacteraemia862 3
5.2ii Incidence of healthcare-associated infection - C.difficile 13,361 14
5.3Incidence of newly acquired category 2, 3 & 4 pressure
ulcers
5.4 Incidence of medication errors causing serious harm 0.34No Data
Available
5.5 Admission of full-term babies to neonatal care 6.1No Data
Available
5.6 Incidence of harm to children due to 'failure to monitor' 1,242No Data
Available
To be developed
To be developed
NHS Outcomes Framework
2014 – 2015
NHS Croydon CCG vs National Position
Latest Data available February 2015
Please note the hospital activity data is up to 2 years
out of date. Our Transforming Adult Community
Services and pathway redesign is expected to impact
on much of the unplanned hospitalisation and
emergency admissions values
4 Ensuring that people have a positive experience of care
Overarching indicators National
Indicator Value Croydon
Indicator Value 4a.i Patient experience of primary care - GP services 85.7 83.3
4a.ii GP out-of-hours services 66.2 56.7
4a.iii NHS Dental services 84.2 82.9
4b Patient experience of hospital care 76.9 67.1
4c Friends and family test Improvement Areas
4.1 Patient experience of outpatient services 79.5 74.4
4.2 Responsiveness to inpatients' personal needs 68.7 54.4
4.3 Patient experience of A&E services 79.1 75.5
4.4i Access to GP services 74.6 73.4
4.4ii Access to NHS Dental services 94.8 94.6
4.5 Women's experience of maternity services 78.9 No Data Available
4.6 Bereaved carers' views on the quality of care in the last 3 months of life 75.9 No Data
Available
4.7 Patient experience of community mental health services 85.8 No Data Available
4.8 Improving children and young people's experience of healthcare
4.9 Improving people's experience of integrated care
To be developed
To be developed
To be developed

NHS Croydon CCG Annual Operating Plan 2015-16 Page 34 of 48
Appendix 2 National outcomes framework and outcomes by programme
NHS Outcomes Framework Domains
Seven Outcome Ambitions
1 2 3 4 5
1 2 3 4 5 6 7
Programmes Pre
ven
tin
g p
eo
ple
fro
m d
yin
g p
rem
atu
rely
Enh
anci
ng
qu
alit
y o
f lif
e f
or
pe
op
le w
ith
lon
g-te
rm c
on
dit
ion
s
He
lpin
g p
eo
ple
to
re
cove
r fr
om
ep
iso
de
s o
f ill
h
eal
th o
r fo
llow
ing
inju
ry
Ensu
rin
g th
at p
eop
le h
ave
a p
osi
tive
exp
erie
nce
of
care
Tre
atin
g an
d c
arin
g fo
r p
eo
ple
in a
saf
e
en
viro
nm
en
t an
d p
rote
ctin
g th
em f
rom
avo
idab
le h
arm
Secu
rin
g ad
dit
ion
al y
ear
s o
f lif
e f
or
the
pe
op
le o
f
Engl
and
wit
h t
reat
able
me
nta
l an
d p
hys
ical
h
eal
th c
on
dit
ion
s
Imp
rovi
ng
the
hea
lth
-re
late
d q
ual
ity
of
life
of
the
15
mill
ion
+ p
eo
ple
wit
h o
ne
or
mo
re lo
ng-
term
co
nd
itio
ns,
incl
ud
ing
me
nta
l he
alth
co
nd
itio
ns
Re
du
cin
g th
e a
mo
un
t o
f ti
me
pe
op
le s
pe
nd
av
oid
ably
in h
osp
ital
th
rou
gh b
ett
er
and
mo
re
inte
grat
ed
car
e in
th
e c
om
mu
nit
y o
uts
ide
of
ho
spit
al
Incr
eas
ing
the
pro
po
rtio
n o
f o
lde
r p
eop
le li
vin
g
ind
ep
en
de
ntl
y at
ho
me
fo
llow
ing
dis
char
ge f
rom
h
osp
ital
Incr
eas
ing
the
nu
mb
er o
f p
eo
ple
hav
ing
a
po
siti
ve e
xpe
rie
nce
of
ho
spit
al c
are
Incr
eas
ing
the
nu
mb
er o
f p
eo
ple
wit
h m
enta
l an
d
ph
ysic
al h
eal
th c
on
dit
ion
s h
avin
g a
po
siti
ve
exp
erie
nce
of
care
ou
tsid
e h
osp
ital
, in
ge
ne
ral
pra
ctic
e a
nd
in t
he
co
mm
un
ity
Mak
ing
sign
ific
ant
pro
gre
ss t
ow
ard
s e
limin
atin
g av
oid
able
de
ath
s in
ou
r h
osp
ital
s ca
use
d b
y
pro
ble
ms
in c
are
Integrated Cancer Service
Cardiology
Community
COPD
Children and Young People
Diabetes
End of Life Care
Learning Disabilities
Maternity
Mental Health
Older People
Planned Care (Acute)
Primary Care
Prevention, Self-Care, Self-Management, Shared Decision Making
Urgent and Emergency Care
Medicine's Optimisation

NHS Croydon CCG Annual Operating Plan 2015-16 Page 35 of 48
Appendix 3 GP network profile summary Mayday Population:
77% Black, Asian and Minority Ethnic groups
High crime and overcrowded housing
High proportion of lone parent families
High prevalence of obesity and diabetes Achievements:
Prescribing indicators
Breastfeeding
Smoking
Diagnosis of CHD, heart failure and hypertension
Care and outcomes for mental health conditions, COPD and CKD
Challenges:
Patient experience
High A&E attendance rates
High emergency admission rates
Diagnosis of atrial fibrillation and epilepsy
Childhood immunisations
Cancer screening Significantly high referral rates: Endocrinology, direct
access ultrasound
Woodside / Shirley Population:
Demographics similar to Croydon average
51% Black, Asian and Minority Ethnic groups
High prevalence of smoking, adult obesity, and long-term conditions including depression, AF, COPD, asthma, CKD and rheumatoid arthritis
Achievements:
Low rates of A&E attendances
Diagnosis rates for adult obesity, diabetes, hypertension, atrial fibrillation, CKD and epilepsy
Care and outcomes for COPD Challenges:
Access and overall patient experience
Prescribing indicators
Diagnosis rates for dementia and CHD
Flu vaccine uptake
Childhood immunisations
Care and outcomes for severe mental illness and sexual health
High referral rates Significantly high referral rates (top 3): Orthopaedics /
musculoskeletal, ENT, paediatrics
East Croydon Population:
High proportion aged 25-44
High population growth in future years
57% Black, Asian and Minority Ethnic groups
Deprived area with high crime rate
High proportion of nursing home residents
High prevalence of smoking, severe mental illness, and drug and alcohol use
Achievements:
Diagnosis rates for atrial fibrillation, stroke/TIA, CKD and epilepsy
Care and outcomes for atrial fibrillation Challenges:
High rate of A&E attendances and emergency admissions particularly for over 65s
Prescribing indicators
Diagnosis rates for diabetes, depression, dementia and hypertension
Care and outcomes for diabetes, severe mental illness and CKD
Cancer screening Significantly high referral rates: Direct access US
Thornton Heath Population:
68% Black, Asian and Minority Ethnic groups
Deprived area with high unemployment
High proportion of lone parent families
High prevalence of smoking, diabetes and severe mental illness
Achievements:
Patient experience
Diagnosis rate for diabetes
Care and outcomes for atrial fibrillation Challenges:
Flu vaccine uptake
High rate of emergency admissions for over 65s
High rate of GP referrals to A&E
Diagnosis rate for depression, CHD, atrial fibrillation, COPD and epilepsy
Care and outcomes for depression and rheumatoid arthritis
Breast and bowel screening; cancer reviews Significantly high referral rates: Physiotherapy, direct
access MRI
Purley Population:
High proportion aged over 55
31% Black, Asian and Minority Ethnic groups
Affluent area
High proportion of care home residents
High prevalence of long-term conditions including depression, dementia, CVD, cancer and hypothyroidism
Achievements:
Patient experience
Low rate of A&E attendances and emergency admissions
Primary immunisations uptake
Cervical and bowel cancer screening coverage Challenges:
Flu vaccine uptake
Care and outcomes for diabetes and depression Significantly high referral rates (top 3):
Physiotherapy, cancer TWW, dermatology
New Addington / Selsdon Population:
29% Black, Asian and Minority Ethnic groups
Includes deprived and affluent areas
High proportion of older people living alone
High prevalence of smoking, adult obesity, circulatory diseases, cancer, COPD
Achievements:
Patient experience of access
Flu vaccine uptake (QOF indicators)
Support for stopping smoking
Care and outcomes for circulatory conditions, mental health conditions and CKD
Challenges:
Breastfeeding; smoking during pregnancy
High emergency admission and A&E attendance rates in New Addington
Significantly high referral rates (top 3):
Orthopaedics/musculoskeletal, paediatrics, cancer TWW

NHS Croydon CCG Annual Operating Plan 2015-16 Page 36 of 48
Appendix 4 Commissioning levers
COMMISSIONING LEVERS
Programmes Lever Totals
£10.839m
CQUINS (2015/16) £5.229m*
Quality Premium (2013/14 Investment)
£1.025m
Quality Premium
Better Care Fund (2015/16 New Schemes)
£800k
LIS - £1.435m** Practice Development and Delivery Scheme -
£2.35m
KPIs
Prevention/Self Care, Shared Decision Making
£350k Long-term conditions (eg Prevention, self-care) (£350k)
Reducing potential years of lives lost through causes considered amenable to healthcare (10%)
Immunisations (DES)
LTC – Diabetes £147k LIS - Diabetes (£147k)
LTC - Cardiology £48k
LIS – ECG (£48k Current Spend)
LTC – Cancer £1.7k Loc - Cancer: early detection (10%)
LIS – MGUS/CLL (£1.7k
current spend)
LTC – Mental Health
£957.4k
(MHNat and MH4B
CQUINs value is £557k)
MH Loc – Adult Mental
Health Service Redesign (£46.5k)
MH Loc – Integrated
Adult MH service model (£46.5k)
MH 4B – CAMHS GP
Access and Therapeutic Assessment (£TBC)
MH 4B – Outcomes
framework (£TBC)
MH 4B – Improve
inpatient experience – (£TBC)
MH Nat – Improve
Physical Health (£TBC)
Crisis Care Concordat Co-ordinator (£18k)
Mental Health Focused
Discharge Planning (£249k)
Enhanced Competency
Cultural Training
Nat/Loc - Reduction in the number of people with severe mental illness who are currently smokers (30%) Loc - % of people with severe mental illness who have received a list of physical checks (10%)
LIS - Mental Health
(£40.4k)
Extended hours and learning disabilities
enhanced services (DES)
LTC Dementia £364k Nat - Dementia (£364k) Dementia (DES)
Maternity £320k Loc – Maternity (£302k)
Older People £139.5k MH Loc – MH Older
Adults managed in the Care Homes

NHS Croydon CCG Annual Operating Plan 2015-16 Page 37 of 48
COMMISSIONING LEVERS
Programmes Lever Totals
£10.839m
CQUINS (2015/16) £5.229m*
Quality Premium (2013/14 Investment)
£1.025m
Quality Premium
Better Care Fund (2015/16 New Schemes)
£800k
LIS - £1.435m** Practice Development and Delivery Scheme -
£2.35m
KPIs
community (£93) MH Loc – MH OA
readmission rates (£46.5k)
Planned Care £1.4k
Nat – Kidney injury
(£364k) SWL - LQS – Inter-
hospital transfer standards (£192k) Lo c - Diagnostic Waits
(£271k) MH Loc –Reduction in IP beds (£64k)
Epilepsy and Convulsions (£200k) Special School Nursing (£49k) FGM (£100k) ‘Hear Us’ Link worker (£29k)
LIS – Barrett’s
Oesophagus (£17.3k) LIS – Complex Leg
Ulcer, Secondary Care Wound Management (Basket) – (£292k) LIS – Coeliacs (£8.2k) LIS – Minor Surgery
(£104k) LIS – Phlebotomy
(£327.1k) LIS – Pre-op hernia
(£10.9k) LIS – Spirometry
(£100.2k) LIS – Urology (£30.3k)
Internally generated Referrals - Consultant to Consultant Threshold for Outpatients 14% Outpatient First to Follow-up ratios against agreed ratios Outpatient surgical procedures Excess Bed Days
Primary Care £2.7m Nat - Sepsis (£364k)
A named, accountable GP for all patients (incl children) (DES) PDDS1. Engagement
and Participation - £n/a PDDS2. Practice Plans
£293k PDDS3. Practice
Assurance Report £293k PDDS4. Use of Available
Services £1.06m PDDS5. Prescribing
£313k PDDS6. Financial
Balance - £391k
Community Care / Transforming Adult Community Services
£150.1k Comm – 7 day
responsiveness
LIS – GP Care homes
(£150.1k)
Urgent Care £2.1m
(includes Nat - Urgent and
emergency care
Nat/Loc - Increase in the proportion of discharges
Consolidation of A&E Front of House
Avoiding unplanned admissions (DES)
Excess Bed Days

NHS Croydon CCG Annual Operating Plan 2015-16 Page 38 of 48
COMMISSIONING LEVERS
Programmes Lever Totals
£10.839m
CQUINS (2015/16) £5.229m*
Quality Premium (2013/14 Investment)
£1.025m
Quality Premium
Better Care Fund (2015/16 New Schemes)
£800k
LIS - £1.435m** Practice Development and Delivery Scheme -
£2.35m
KPIs
£800k BCF funding)
Loc – A&E Conversion
Rate (£1.3m) MH Loc – Reduced
inappropriate referrals (£46.5k)
of non-elective patients at weekends (30%)
Roving GP
Emergency Medicine Consultant presence Paediatric Consultant peak time presence Quality of care for fractured neck of femur
Medicines Management
£253k Loc – Medicines
Management (x3) (£96k)
Improving antibiotic prescribing in primary and secondary care (10%)
LIS – Shared Care
Prescribing, Zoladex/Prostrap (Basket) – (£157k)
Quality Improvement
£643k
Loc – Patient Safety
Mortality Rate (£73k) Loc – Safe Staffing
(£607k)
Pressure Ulcers (£29k)
Other £304k
Comm – Community
Minimum Dataset (£176k) SWL - Strategy Dataset
(£128k)
*CQUINS
Nat = £1.092m SWL = £319k Local = £2.9m MH = £929k
**Local Incentive Scheme (LIS) figures are based on M9 FOT 14-15

NHS Croydon CCG Annual Operating Plan 2015-16 Page 39 of 48
Appendix 5 NHS Constitution annual performance and plan Actuals Plan
Area Measure 12/13 Year
End Position
13/14 Year End Position
14/15 Forecast Year End Position
2015/16
Plan
2015/16 National Standard
A&E waits Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department – Croydon Health Services
94.5% 95.3% 93.8% 94.15% 95%
Cat A Ambulance Calls
Category A calls resulting in an emergency response arriving within 8 minutes - Red 1
77.8% 77.4% 67.2% 75% 75%
Category A calls resulting in an emergency response arriving within 8 minutes - Red 2
76.3% 75.3% 59.7% 75% 75%
Category A calls resulting in an ambulance arriving at the scene within 19 minutes
98.2% 97.9% 92.0% 95% 95%
Referral To Treatment waiting times for non-urgent consultant-led treatment
Admitted patients to start treatment within a maximum of 18 weeks from referral
90.7% 91.5% 89.4% 90% 90%
Non-admitted patients to start treatment within a maximum of 18 weeks from referral
97.2% 96.4% 95.4% 95% 95%
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
90.7% 93.3% 94.2% 92% 92%
Diagnostic test waiting times
Patients waiting for a diagnostic test should have been waiting less than 6 weeks from referral
99.1% 96.8% 94.3% 99% 99%
Mixed Sex Accommodation
Minimise breaches - 32 4 0 0
Cancer waits - two-week wait
Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
95.8% 95.8% 95.6% 93% 93%
Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
96.2% 95.9% 97.8% 93% 93%
Cancer waits - 31 days
Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers
98.2% 98.7% 98.3% 96% 96%
Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen
99.7% 100% 98.6% 98% 98%
Maximum 31-day wait for subsequent treatment where that treatment is surgery
98.5% 97.9% 97.8% 94% 94%

NHS Croydon CCG Annual Operating Plan 2015-16 Page 40 of 48
Actuals Plan
Area Measure 12/13 Year
End Position
13/14 Year End Position
14/15 Forecast Year End Position
2015/16
Plan
2015/16 National Standard
Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy
96.4% 99.4% 97.9% 94% 94%
Cancer waits - 62 days
Maximum two-month (62-day) wait from urgent GP referral to first definitive treatment for cancer
82.4% 82.0% 76.4% 85% 85%
Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
90.6% 91.7% 98.8% 90% 90%
Maximum 62-day wait for first definitive treatment following a consultant's decision to upgrade the priority of the patient (all cancers)
83.3% 76.2% 80.2% Not set Not set
Infection Number of C. Difficile infections 61 51 56 55 55
Care Programme Approach (CPA)
The proportion of people under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period
93.6% 97.3% 97.5% 95% 95%
Dementia Percentage diagnosis rate 59.2%* 66.7% 66.7%
IAPT
IAPT Access proportion * (To Be Confirmed) 2.8% 3.76% 6.1%
(Local 5%) 8.16% (Local)
15%
IAPT Recovery Rate 40.8% 44% 42.9% 50% 50%
Mental Health Access
Proportion of patients waiting 6 weeks from referral to entering a course of IAPT treatment
- - 75% 75% 75%
By Apr-16
Proportion of patients waiting 18 weeks from referral to entering a course of IAPT treatment
- - 95% 95% 95%
By Apr-16
Direct Commissioning Primary Care
Satisfaction with the quality of consultation at the GP practice 401.65 401.43 398.96 402.9 Not set
Satisfaction with the overall care received at the surgery 84.0% 83.4% 82.8% 83.6% Not set
Satisfaction with accessing primary care 74.9% 73.5% 72.6%
73.3% Not set
*Based on revised DDR based estimate of 65 and overs on the dementia register (prior to revised estimate 51.8%)

NHS Croydon CCG Annual Operating Plan 2015-16 Page 41 of 48
*Achieving the national standards
Plan
Area Measure 2015/16
Plan 2016/17
Plan 2017/18
Plan
2015/16 National Standard
IAPT IAPT Access proportion (To Be Confirmed) 8.16% 11.5% 15% 15%

NHS Croydon CCG Annual Operating Plan 2015-16 Page 42 of 48
Appendix 6 NHS Constitution trajectories
Area Measure Target 2015/16 Plan
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E waits Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department
95% 91.8% 95.8% 94.8% 94.2%
Cat A Ambulance Calls
Category A calls resulting in an emergency response arriving within 8 minutes – Red 1
75%
Category A calls resulting in an emergency response arriving within 8 minutes – Red 2
75%
Category A calls resulting in an ambulance arriving at the scene within 19 minutes
95%
Referral To Treatment waiting times for non-urgent consultant-led treatment
Admitted patients to start treatment within a maximum of 18 weeks from referral
90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
Non-admitted patients to start treatment within a maximum of 18 weeks from referral
95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
92% 92% 92% 92% 92% 92% 92% 92% 92% 92% 92% 92% 92%
Diagnostic test waiting times
Patients waiting for a diagnostic test should have been waiting less than 6 weeks from referral
99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%
Cancer waits - two-week wait
Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
93% 93% 93% 93% 93%
Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
93% 93.0% 93.0% 93.0% 93.0%
Cancer waits - 31 days
Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers
96% 96.0% 96.0% 96.0% 96.0%
Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen
98% 98.0% 98.0% 98.0% 98.0%
Waiting plans from Brent CCG

NHS Croydon CCG Annual Operating Plan 2015-16 Page 43 of 48
Area Measure Target 2015/16 Plan
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Maximum 31-day wait for subsequent treatment where that treatment is surgery
94% 94.0% 94.0% 94.0% 94.0%
Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy
94% 94.0% 94.0% 94.0% 94.0%
Cancer waits - 62 days
Maximum two-month (62-day) wait from urgent GP referral to first definitive treatment for cancer
85% 85.0% 85.0% 85.0% 85.0%
Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
90% 90% 90% 90% 90%
Maximum 62-day wait for first definitive treatment following a consultant's decision to upgrade the priority of the patient (all cancers)
Not set 82.5% 82.5% 82.5% 82.5%
Infection Number of C. Difficile infections 55 4 5 4 5 4 4 5 5 5 5 4 5
Dementia Percentage diagnosis rate (over 65s) 66.7% 59.2%
59.9%
60.6%
61.3%
61.9%
62.6%
63.3%
64.0%
64.7%
65.4%
66.0%
66.7%
IAPT
IAPT Access proportion (To Be Confirmed) 8.16% (Local)
2.04% 2.04% 2.04% 2.04%
IAPT Recovery Rate 50% 50.1% 50.1% 50.1% 50.1%
Mental Health Access
Proportion of patients waiting 6 weeks from referral to entering a course of IAPT treatment
75% By Apr-16
75% 75% 75% 75%
Proportion of patients waiting 18 weeks from referral to entering a course of IAPT treatment
95% By Apr-16
95% 95% 95% 95%
Direct Commissioning Primary Care
Satisfaction with the quality of consultation at the GP practice
- 402.9
Satisfaction with the overall care received at the surgery
- 83.6%
Satisfaction with accessing primary care - 73.3%

NHS Croydon CCG Annual Operating Plan 2015-16 Page 44 of 48
Areas that need planning for during 2015/16 for delivery in 2016/17 or beyond are set out below:
Mental Health
Mental health Care Programme Approach (CPA): The proportion of people under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period - 95%
*New* Mental health access waits
The proportion of people that wait 18 weeks or less from referral to their first IAPT treatment appointment against the number of people who enter treatment in the reporting period
The proportion of people that wait 6 weeks or less from referral to their first IAPT treatment appointment against the number of people who enter treatment in the reporting period
Early Intervention in Psychosis
More than 50% of people experiencing a first episode of psychosis will be treated with a NICE approved care package within two weeks of referral (in development) - >50% by April 2016
Liaison Psychiatry % of acute trusts with an effective model of liaison psychiatry (all ages, appropriate to the size, acuity and specialty of the hospital) (in development) - 100% by 2020
Operational *New* Mental health access waits
Number of ended referrals in the reporting period that received a course of treatment against the number of ended referrals in the reporting period that received a single treatment appointment
Average number of treatment sessions
Re-focusing service provision on less severe cases (in development)
*New* Transforming care
Total number of patients in in-patient beds for mental and/or behavioural healthcare who have either learning disabilities and/or autistic spectrum disorder (including Asperger's syndrome)
Numbers of admissions to in-patient beds for mental and/or behavioural healthcare who have either learning disabilities and/or autistic spectrum disorder (including Asperger's syndrome).

NHS Croydon CCG Annual Operating Plan 2015-16 Page 45 of 48
Numbers of patients discharged to community settings
Patients without a care coordinator
Patients not on the register
Patients without a review in the last 26 weeks
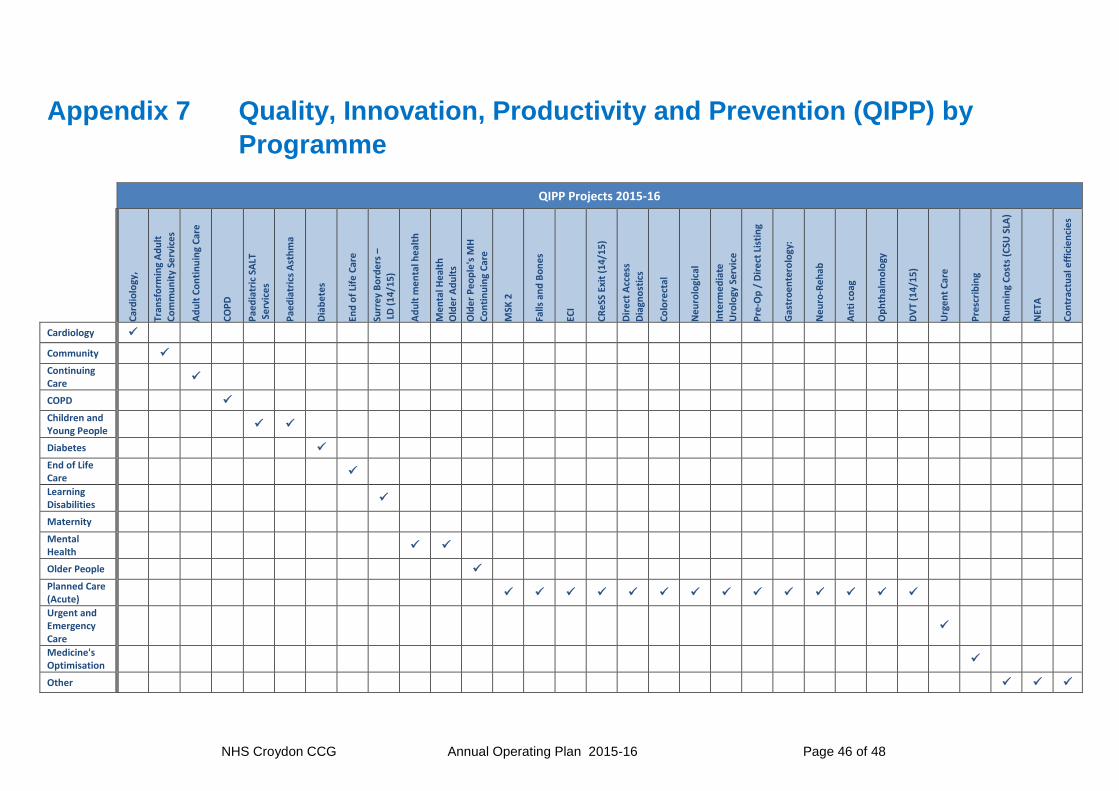
NHS Croydon CCG Annual Operating Plan 2015-16 Page 46 of 48
Appendix 7 Quality, Innovation, Productivity and Prevention (QIPP) by
Programme
QIPP Projects 2015-16
Car
dio
logy
,
Tran
sfo
rmin
g A
du
lt
Co
mm
un
ity
Serv
ice
s
Ad
ult
Co
nti
nu
ing
Car
e
CO
PD
Pae
dia
tric
SA
LT
Se
rvic
es
Pae
dia
tric
s A
sth
ma
Dia
be
tes
End
of
Life
Car
e
Surr
ey
Bo
rde
rs –
L
D (
14
/15
)
Ad
ult
me
nta
l he
alth
Me
nta
l He
alth
O
lde
r A
du
lts
Old
er
Peo
ple
's M
H
Co
nti
nu
ing
Car
e
MSK
2
Falls
an
d B
on
es
ECI
CR
eSS
Exi
t (1
4/1
5)
Dir
ect
Acc
ess
Dia
gno
stic
s
Co
lore
ctal
Ne
uro
logi
cal
Inte
rme
dia
te
Uro
logy
Ser
vice
Pre
-Op
/ D
ire
ct L
isti
ng
Gas
tro
en
tero
logy
:
Ne
uro
-Re
hab
An
ti c
oag
Op
hth
alm
olo
gy
DV
T (1
4/1
5)
Urg
en
t C
are
Pre
scri
bin
g
Ru
nn
ing
Co
sts
(CSU
SLA
)
NET
A
Co
ntr
actu
al e
ffic
ien
cie
s
Cardiology
Community
Continuing Care
COPD
Children and Young People
Diabetes
End of Life Care
Learning Disabilities
Maternity
Mental Health
Older People
Planned Care (Acute)
Urgent and Emergency Care
Medicine's Optimisation
Other

NHS Croydon CCG Annual Operating Plan 2015-16 Page 47 of 48
Appendix 8 Summary of patient and public involvement
Programme Engagement Plans
Cancer Engage a range of patient and community representatives to ensure that the strategy and the actions planned will improve the patient experience
Cardiology Evaluation of ECG service in primary care. Patient and Friends survey across all pathways Responses regarding hot clinic and cardiac rehab pilots to guide full implementation
Children and Young Children
Engage with children and families as part of commissioning and service reviews and build a requirement for the provider to engage into service specifications.
Chronic Obstructive Pulmonary Rehab
Engage patients in service redesign through Patient Forums, at Croydon Old Peoples Network meetings, consulting members of Breathe Easy Croydon, the British Lung Foundation, Older Peoples Health Forum and Age UK. Existing patients at the Pulmonary Rehabilitation, Hot Clinics and on Wards
Community Services (TACS)
Using patient Friends and Family Test feedback on services and service user stakeholder events to inform and support service redesign and/or development Undertaking patient/carer feedback/stakeholder events in developing new services Working with services to develop and implement patient reported outcome measures that inform and support service redesign and/or development
Diabetes Diabetes UK will be part of the Steering Group going forward to support with PPI input as the service continues to implement and develop Improving access for BME groups - use of the South London Health Innovation Network to support this
End of Life Involve range of groups to enable implement a service fit for purpose in Croydon: Patient Groups, Healthwatch, Health / Social care providers, GPs/CCG/LA staff, Other Stakeholders and Faith Groups

NHS Croydon CCG Annual Operating Plan 2015-16 Page 48 of 48
Programme Engagement Plans
Learning Disabilities Involve and engage people with Learning Disability in any change proposal, and also ensure engagement with family carers. Well-established networks and groups are active in Croydon - e.g. through the LD partnership, through Croydon People First (and other voluntary sector organisations or support groups) and via the resident/user forum.
Maternity Through Maternity Service Liaison Committee continue to deliver actions against improvement plan
Older People Involve range of groups to commission a service fit for purpose in Croydon: Patient Groups, HealthWatch, Health / Social care providers, GPs/CCG/LA staff, Other Stakeholders and Faith Groups
Engage with patients and care agency providers to develop the domiciliary service Continued Outcome Based Commissioning for Older People engagement
Planned care Procurement of dermatology intermediate service Annual survey of patient experience in intermediate services
Prevention, Self-Care, Shared Care
Engagement in three areas (diabetes, respiratory and MSK) to develop prevention, self-care, shared care making commissioning requirements and guidelines
Primary Care Support practices in development of PPGs and regular patient surveys Engage with patient groups at practice level to support implementation of clinical target areas Develop programme of regular patient feedback to the CCG on primary care services
Urgent Care and Emergency Care
Wide engagement in the development of the urgent and emergency care model to be procured by March 2017
Appendix 9 Programmes of delivery (see separate document)
The details of each of our programmes of delivery are provided in a separate document.













![BOXPARK CROYDON - Bars€¦ · BOXPARK CROYDON. INTRODUCTION [03] THE CONCEPT [05] BXPARKO SHOREDITCH [07] CROYDON [16] BXPARKO CROYDON [20] DETAILS [31] CONTENTs. ELUTIONTH EvO Of](https://static.documents.pub/doc/80x56/5f105a3e7e708231d448afca/boxpark-croydon-bars-boxpark-croydon-introduction-03-the-concept-05-bxparko.jpg)



