176
Annual report and accounts April 2015 to March 2016

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 1
Annual report and accounts
April 2015 to March 2016
ARA2016_master 140616.indd 1 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 20162
Annual report and accounts
April 2015 to March 2016
ARA2016_master 140616.indd 2 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 3
Annual report and accounts
April 2015 to March 2016
Presented to Parliament pursuant
to Schedule 7, paragraph 25(4)(a)
of the National Health Service Act 2006
Norfolk and Suffolk NHS Foundation Trust
ARA2016_master 140616.indd 3 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 20164
© 2016 Norfolk and Suffolk NHS Foundation Trust
ARA2016_master 140616.indd 4 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 5
Contents
Chair’s report 6
Performance report, comprising:
Overview of performance 7
Performance analysis 10
Financial review 14
Environmental and social matters 17
Accountability report, comprising:
Directors’ report 19
Remuneration report 22
Staff report 33
NHS Foundation Trust Code of Governance 54
Regulatory ratings 75
Additional reporting 76
Quality report, comprising:
2015-16 Statements of Directors’ Responsibilities in Respect of the Quality Report 78
Independent auditor’s report to the Council of Governors of 79 Norfolk and Suffolk NHS Foundation Trust on the Quality Report
Statement from the Chief Executive 81
Priorities for Improvement in 2016-17 83
Statements of Assurance from the Board 86
Quality initiatives 93
National recognition 95
Quality indicators 96
Evaluation of patient safety 104
Evaluation of clinical effectiveness 107
Evaluation of patient experience 107
Commissioners and stakeholder comments 114
Key 121 Annual accounts, including: A1
Statement of accounting officer’s responsibilities A2
ARA2016_master 140616.indd 5 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 20166
I said in last year’s Annual Report that 2014-15 was “an incredibly challenging year” for the Trust. The last 12 months has continued to be very difficult with the demand for mental health services rising and the pressure on our finances showing no sign of letting up.
However, in spite of this, considerable progress has been made in addressing the issues identified by the Care Quality Commission (CQC) when they inspected the Trust in Autumn 2014. The CQC clearly acknowledged the caring nature of our clinical workforce and on my visits to all corners of the Trust over the last 12 months I have been enormously impressed by the compassion and dedication of our staff, working with some of the most vulnerable people across our two counties. It is not only the clinical staff that deserve our thanks; staff within our support functions have also worked incredibly hard and we have seen significant progress across all areas, including Human Resources and IT where the implementation of Lorenzo, a single electronic patient record, has been a massive undertaking. Whilst I know the introduction of Lorenzo has caused significant difficulties for staff, we are now beginning to see some of the benefits which will improve the safety and quality of our services.
Service user presentations to our Board have been valuable in highlighting some of the real life experiences of people using our services. Whilst we have heard of occasions where we haven’t got things right – which in itself is valuable in enabling us to learn lessons for the future – we have also heard some amazing stories of how we have cared for and supported people in their time of need. One regular feature has been the powerful impact that the Recovery College has had on enabling people to move forward with their lives. Some of these individuals have become Peer Support Workers, bringing people with lived experience into the front line of the provision of care. Recovery is at the heart of much of the clinical work that the Trust does and the Board remains fully committed to the principles of Implementing Recovery through Organisational Change (IMROC).
The Board has spent much of its time working with staff, carers, service users and other stakeholders to develop our strategy. The last 12 months has seen the launch of our Values: Working Together for Better Mental Health – Respectfully, Positively and Together. We have also launched our new Operational Strategy with three key elements:
• Improving quality and achieving financial sustainability
• Working as One Trust
• Increasing our focus on prevention, early intervention and recovery
This strategy is underpinned by our new Clinical Strategy and our Organisational Development and Workforce Strategy. The Trust now has a very clear sense of direction; we know where we are going and on that journey we will continue to be a champion for mental health in order to do everything we can to reduce stigma and get a better deal in terms of funding. We also understand that as an organisation, we need to continuously be learning lessons when things do not go right and also from looking at what other organisations are doing.
To enable us to continue to develop and improve services we need a sound financial base. We have continued to run a deficit in 2015-16, although we did achieve a result better than budget. We are forecasting an improved performance in 2016-17, but this will be dependent on the funding we receive and our ability to continue to find efficiencies.
I am proud to have been the Chair of this organisation working with some truly incredible people. I believe the Trust is in a much better place today than it was 12 months ago and I look forward to helping to drive our strategy forward for the benefit of those people that need our services.
Gary Page Chair
Chair’s report
ARA2016_master 140616.indd 6 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 7
Overview of performance
This report marks my first full year as Chief Executive of NSFT. I would like to thank my team of Executive Directors and all Board colleagues for their hard work and their support of me during this year.
But of course, it is each and every staff member who have delivered the services to the important people we serve. It is therefore pleasing to say that it is those staff that have generated our new organisational values in this year. Over 1,300 staff, together with service users and carers, generated the three values referred to in our Chair’s opening: Working together for better mental health… positively, respectfully, together. These values have become a touchstone to guide my activity during this year and, increasingly, that of the whole organisation.
The year has been marked by a focus on quality and quality improvement. The formal mechanism for this has been through my chairing of the Trust’s Transformation Board but it has been the activities of every staff member on the front line, which has delivered the improved service we seek for our service users. We know there have been many positive changes but, equally, we know where we still need to improve.
We completed the delivery of the final elements of our last strategic plan, bringing it to a close. This involved the reconfiguration of services in Great Yarmouth and Waveney, which was successfully completed without disruption to services and with minimal change for staff. We have also delivered our promise of a new style of management, which engages with staff, making changes, where necessary, but bringing people along. As we implement our three new strategic goals, we will continue to develop this engaging style of leadership and management.
‘Putting People First’ has been our motto for this year. This means we have listened to staff in new ways but also communicated outwards.
Finally, in 2015-16 we have delivered our financial targets for the year. At this time of financial pressure across all of the NHS we have delivered the financial plan that we agreed at the outset of the year. As we go into next year there will continue to be financial challenges but we are in a much better shape to meet them.
For us, this was an encouraging year in which our staff contributed to quality improvements and new strategic directions. I would like to take this opportunity to thank our staff and partners who have all been part of this.
Michael Scott Chief Executive
Performance report
ARA2016_master 140616.indd 7 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 20168
A134
Swaffham
CCG Boundaries
Felixstowe
GreatYarmouth
Wisbech
A47
Fakenham
NorthWalsham
Holt
Cromer
King’s Lynn
Wells next the seaHunstanton
Central NorfolkA140
A1065
A148
A11
Attleborough
Dereham
Aylsham
WymondhamWatton
A47
7
13
A47
A146
Southwold
Lowestoft
Aldeburgh
Gt Yarmouthand Waveney
A140Beccles
WoodbridgeWickham Market
Newmarket18
15 Bury StEdmunds
2
Stowmarket
IpswichSudbury
Haverhill9
10 11
19
East Suffolk
West SuffolkA134
A14
5
Diss
A143
Eye
FramlinghamA12
Halesworth
CarltonColville
20 Thetford
21
A10 Norwich
14
16
Issue date 18/05/16
6
8
3
Ipswich
Kesgrave
NewmarketSage Centre - CB8 7JG (Bury North IDT)
LothinglandAirey Close - NR32 3AXAllington Smith Close - NR32 3AX
10
11
The Hollies - IP3 8LS Mariner House - IP1 2GAWoodlands - IP4 5PDWalker Close - IP3 8LY Eccles Road - IP2 2RFChilton House - IP3 8LTFoxhall House - IP3 8LTEndeavour House - IP1 2BX
(Ipswich IDT)
(Coastal IDT)
15
13
LowestoftVictoria House - NR32 1PLMeridian House - NR32 1PLTennyson Centre - NR32 1PTBarley Way - NR33 7NHKirkley Cliff - NR33 ODF
King’s LynnChatterton House - PE30 5PDFermoy Unit - PE30 4ETChapel Street - PE30 1EG (NRP)
Grange Lodge - IP5 1JF
14
12
12
Bury Saint EdmundsBlomfield House - IP33 1HEChild Development Centre - IP33 3NDChild Health Centre - IP33 3NDWedgwood Unit - IP33 2QZ50 Barons Road - IP33 2JWHospital Road Site - IP33 3NR (Bury South IDT)
HaverhillHaverhill Health Clinic - CB9 8HF
Eye Hartismere Hospital - IP23 7BH
Gorleston
Felixstowe
Stepping Out - NR31 7QB
Grove Medical Centre - IP11 9JL
2
9
5
7
6
Great Yarmouth Northgate Hospital - NR30 1BU (NRP)
Carlton Colville Carlton Court - NR33 8AG
Attleborough Bickley Day Hospital - NR17 2QE
Dereham Springwell - NR19 1DL
Signpost House - NR20 3TL
4
8
3
1
1
StowmarketIpswich Street - IP14 1BBOld Fox Yard - IP14 1ABHaymills - IP14 1RF
SudburySt Leonards Hospital - CO10 2RQ
Thetford
Wickham Market
North Walsham
Thetford Healthy Living Centre - IP24 1JDThetford Business Centre - IP24 1BT (NRP)
Riverview - IP13 0TA
St Nicholas Court - NR28 9BY (NRP) The Atrium - NR28 9HZ
18
19
20
21
16
Norwich Hellesdon Hospital - NR6 5BE The Julian Hospital - NR2 3TD Mary Chapman House - NR2 4HN Norvic Clinic - NR7 0HT 80 St Stephen's Road - NR1 3RE
The Bure Centre - NR2 2PA 296 Drayton High Road - NR6 5BJ West Pottergate - NR2 4BX Genome Centre - NR4 7UH
(NRP)
WymondhamGateway House - NR18 0WF
17
22
4
22
17
DownhamMarket
West Norfolk
ARA2016_master 140616.indd 8 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 9
Purpose and activities
The Trust’s principal activities are to support and enable people with mental health problems to live fulfilling lives. We believe in recovery and wellbeing and understand the importance of good physical health, maintaining relationships and incorporating treatment into an active life.
Service users and carers are at the centre of all our work. We listen to their opinions and use their views and experiences to shape our services and enhance all aspects of our care. We want to be recognised in the local community for providing excellent advice and treatment, and for our friendly, flexible approach.
We are committed to research and innovation and our ambition is to become a national leader in the provision of high quality and cost-effective mental health services.
We provide a range of health and social care services specialising in mental health across Norfolk and Suffolk including: • Adult services
• Services for children, families and young people • Dementia and complexity in later life • Neurodevelopmental
• Wellbeing
• Low and medium secure services
• Alcohol and substance misuse services
We have inpatient facilities across Norfolk and Suffolk, with smaller bases in rural locations. Many of our services are offered in the community, enabling service users to receive the support they need in a familiar environment.
Brief history of the Trust and its statutory background
Norfolk and Suffolk NHS Foundation Trust was formed on 1 January 2012 by the merger of Norfolk and Waveney Mental Health NHS Foundation Trust and Suffolk Mental Health Partnership NHS Trust. Since the merger, the Trust has continued to evolve. The changing social care landscape, which has brought new statutory requirements, meant that in 2013-14 it was decided to end the Norfolk County Council
partnership (known as a S.75 agreement). This meant that there was clearer accountability for those aspects of social care for which Norfolk County Council is responsible. Staff carrying out these roles transferred to the employment of Norfolk County Council in 2014-15. The Suffolk S.75 agreement was not affected by this change. Under the Suffolk S.75 agreement Suffolk County Council staff mostly remained in the local authority’s employment.
The Trust now employs nearly 4,000 staff who work from sites across the two counties. We continue to develop strong working partnerships with social care, primary care, the police, the voluntary sector and, of course, all parts of the NHS.
Key issues and risks that could affect the Trust in delivering its objectives
During 2015-16 the top risks facing the Trust included a range of business, quality and financial risks, all of which were considered by the Board and its committees throughout the year. The key risks are identified as follows:
1. In February 2015 the Trust was placed into special measures with Monitor, following the CQC review of the Trust in October 2014. The Trust was rated as “inadequate” in the domains of well-led and safety and “requires improvement” in the domains of effectiveness and responsive. The Trust has developed a Quality Improvement Plan to address the concerns and recommendations. An improvement director has been appointed by Monitor to work with the Trust and the Board to ensure progress is made against the Plan. Progress against the Plan is reported to the Quality Governance Committee and to the Board of Directors on a monthly basis. The CQC is due to review the Trust in July.
2. As a result of the CQC concerns, Monitor identified governance issues, which led to an additional condition which requires the Trust to have an effectively functioning Board and Board committees; sufficient Board, management and leadership capacity and capability; and appropriate governance systems and processes. During 2015-16 the Board has developed its strategy, which was published in March 2016. This established our three goals of: improving quality and achieving financial sustainability; working as one Trust; and focusing on prevention, early intervention and promoting recovery.
ARA2016_master 140616.indd 9 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201610
3. The Trust established a Financial Recovery Plan to address its long-term financial sustainability. This provided a high-level plan to bring the Trust back to a surplus position by 2018-19. In 2015-16 the Trust improved on its financial plan resulting in a deficit of £8.9m by 31 March 2016. The Board is acutely aware of the need to ensure very tight financial control. The financial plan is monitored at the Finance Committee and at the Board on a monthly basis. This, along with quality, is a key focus of the Board.
4. Other key risks include: (i) Recruitment, retention and training of our staff. Our agency spend has reduced during the year and our vacancy rates have improved. However, there are still areas of high risk within the organisation where recruitment remains an issue. (ii) The implementation of a new electronic patient record, Lorenzo, supplied by CSC under a national contract, has been problematic. There have been system and network problems which the supplier has failed to resolve, as well as data quality issues which have led to significant additional work for our staff in resolving and training issues. The Board receives monthly updates on progress with the implementation. This continues to be a risk for the organisation in 2016-17.
Performance analysis
Performance reporting
Quality, service and financial compliance to national and locally commissioned targets are reported to the Board of Directors via the Business Performance Report. The performance management framework supports the organisational delivery and ensures delivery across all areas of performance.
For 2015-16 organisational accountability for performance was delivered via the Locality Performance Review Groups (PRG), which meets monthly to review the Integrated Performance Report (IPR). The IPR monitors key performance indicators across the following areas: • Organisational delivery • Quality, safety and experience • Workforce, development and effectiveness
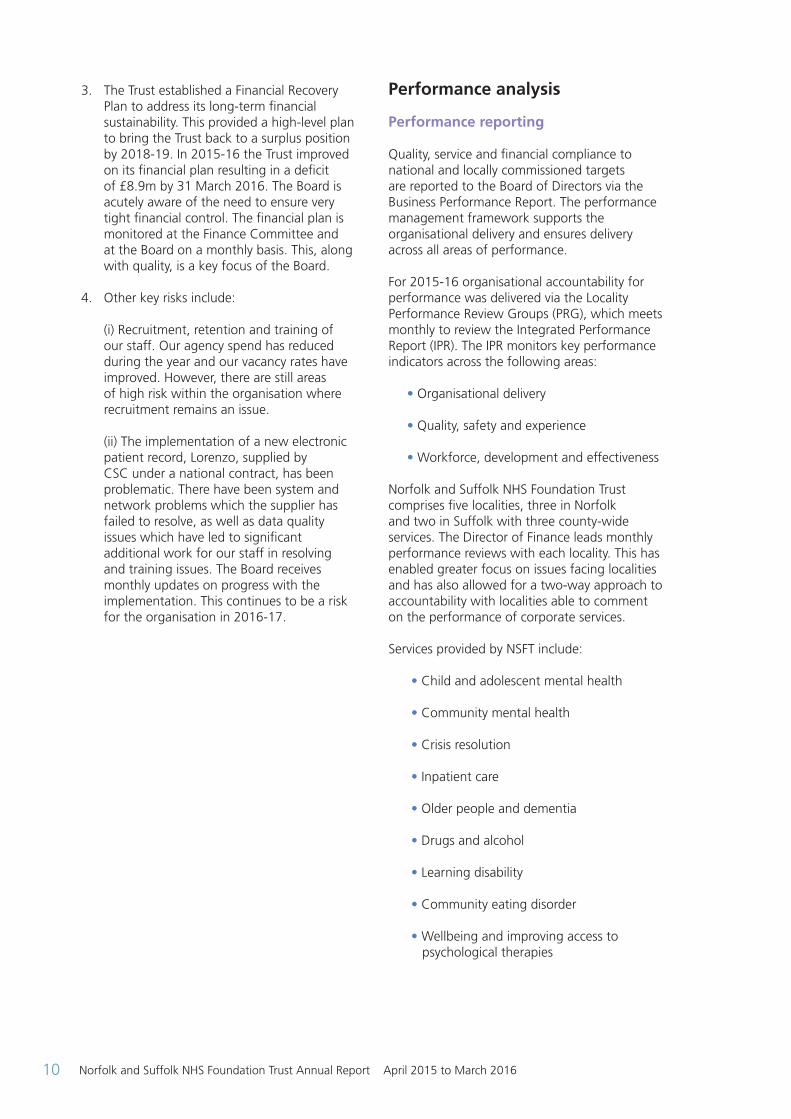
Norfolk and Suffolk NHS Foundation Trust comprises five localities, three in Norfolk and two in Suffolk with three county-wide services. The Director of Finance leads monthly performance reviews with each locality. This has enabled greater focus on issues facing localities and has also allowed for a two-way approach to accountability with localities able to comment on the performance of corporate services. Services provided by NSFT include:
• Child and adolescent mental health
• Community mental health
• Crisis resolution
• Inpatient care
• Older people and dementia
• Drugs and alcohol
• Learning disability
• Community eating disorder
• Wellbeing and improving access to psychological therapies
ARA2016_master 140616.indd 10 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 11
Monitor Compliance FrameworkThe Trust continues to be monitored against eight mental health targets and thresholds. Performance against these targets combines to provide the Trusts Governance Risk Rating (GRR).
(PA1)
2015-16
Target Threshold Qtr 1 Qtr 2 Qtr 3 Qtr 4
CPA patients receiving a follow-up within 7 days of discharge
95% 82% 83% 93% 97%
CPA patients having formal review within 12 months
95% N/A 79% 66% 69%
Minimising delayed transfers of care <7.5% 2.9% 4.3% 3.5% 3.5%
Admissions to inpatient services had access to CRHT teams
95% 43% 49% 62% 84%
Meeting commitment to service new psychosis cases by early intervention teams
95% 117% 137% 128% 118%
Data completeness: Identifiers 97% N/A 99% 99% 100%
Data completeness: Outcomes 50% N/A 59% 44% 32%
Self-certification against compliance regarding access to health care for people with a learning disability
6 6 6 6 6
People with common mental health conditions referred to the IAPT programme will be treated within 6 weeks of referral
75% N/A N/A 93% 94%
People with common mental health conditions referred to the IAPT programme will be treated within 18 weeks of referral
95% N/A N/A 95% 100%
Meeting commitment to serve new psychosis cases by early intervention teams NEW measure (scored from Q4 2015-16) Completed waits only
50% N/A N/A N/A 45%
Contract Targets
In 2015-16 the Trust operated within ‘block’ contract arrangements with Norwich CCG, North Norfolk CCG, South Norfolk CCG, West Norfolk CCG, Great Yarmouth and Waveney CCG, Ipswich and East Suffolk CCG and West Suffolk CCG, covering provision of mental health services for Child and Adolescent Mental Health (CAMHS), People of Working Age, Older People, and Substance Misuse. The Trust also provides Primary Care mental health services in the CCGs listed. The contracts include a range of agreed performance indicators. Please see below for the overall Trust performance.
ARA2016_master 140616.indd 11 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201612
(PA2)
Key Performance Indicator2014-15 Target
2014-15 Actual
2015-16 Target
2015-16 Actual
Percentage of patients with a valid MHCT assessment and care cluster
99% 97% 99% 94%
Percentage of long-term (over 12 months) inpatients who have received an annual health check
100% 94% 100% 100%
Percentage of referrals to CAMHS waiting within standard
80% 92% 80% 81%
Adult Acute Inpatient average length of stay 28 31 28 31
Contract target – Medium and Low Secure and CAMHS Tier 4 NHS England Specialised Commissioning
The Trust’s contract with the NHS England Specialised Commissioning Group for the provision of medium and low secure mental health services and a young people’s inpatient unit have identified bed occupancy as a key target. The medium and low secure bed occupancy threshold was set at 90%. The terms of the contract stipulated that occupancy levels below the thresholds would trigger a payback clause in the contract on a cost-per-day basis.
(PA3)
Key Performance Indicator2014-15 Target
2014-15 Actual
2015-16 Target
2015-16 Actual
Medium secure bed occupancy including leave days
90% 81% 90% 78%
Low secure bed occupancy including leave days
90% 87% 90% 86%
CAMHS T4 bed occupancy including leave days
90% 91% 90% 94%
Contract Target – Section 79 Suffolk
A Section 79 Agreement remains in place in Suffolk County Council.
ARA2016_master 140616.indd 12 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 13
Public Health contract Norfolk Public Health commission a substance misuse service in Norfolk. The Trust acts as a lead provider and has established partnerships with non-statutory services for the provision of the adult treatment service. This includes the psychosocial interventions for substance misuse within three Norfolk Prisons.
The substance misuse service has many key performance targets which map the service user journey through treatment and monitors the effectiveness of the service. The performance data is submitted to a national database (National Drug Treatment Monitoring System – NDTMS), which allows comparison of the targets achieved on a national basis. The progress of service users through their journey is measured by the completion of the Treatment Outcome
Profile (TOP), which is completed every three months. In regards to TOP completions at the start and end of treatment, the service achieves 100%; TOP reviews are regularly in the range of 95-98% (national target 80%, local target 90%).
The completion of sub modalities (the interventions that the service user receives during treatment) also has a compliance rate of 98%.
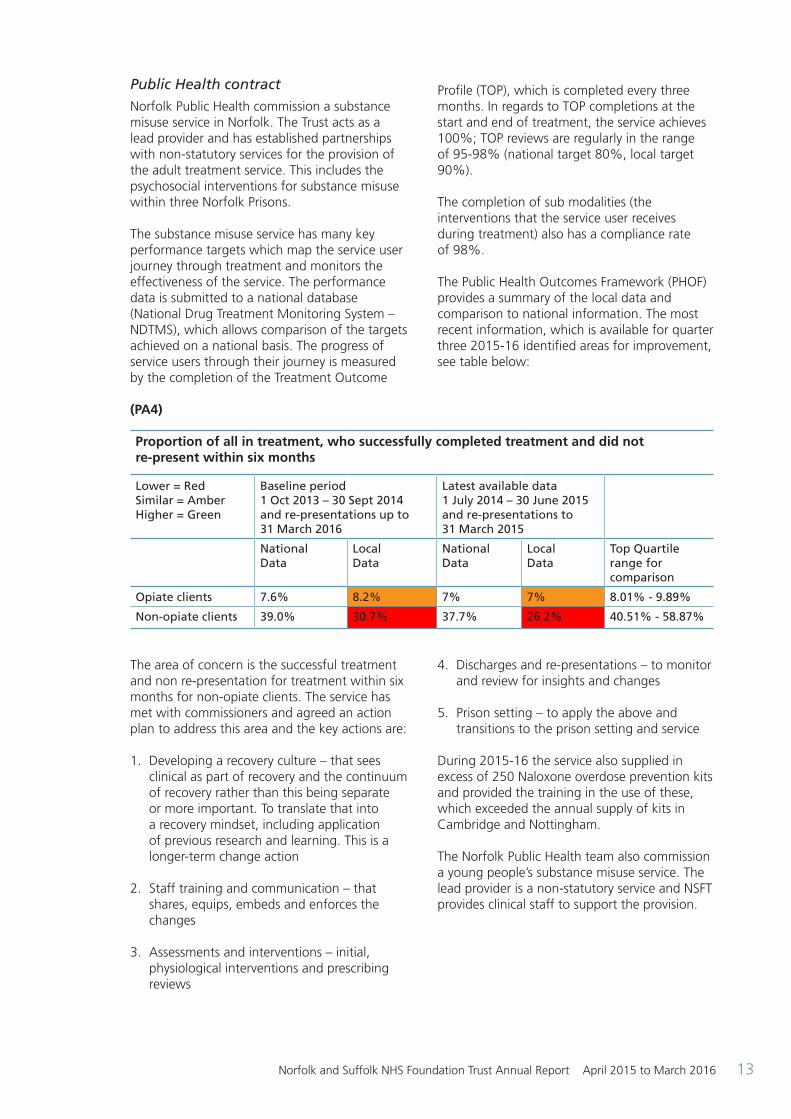
The Public Health Outcomes Framework (PHOF) provides a summary of the local data and comparison to national information. The most recent information, which is available for quarter three 2015-16 identified areas for improvement, see table below:
The area of concern is the successful treatment and non re-presentation for treatment within six months for non-opiate clients. The service has met with commissioners and agreed an action plan to address this area and the key actions are:
1. Developing a recovery culture – that sees clinical as part of recovery and the continuum of recovery rather than this being separate or more important. To translate that into a recovery mindset, including application of previous research and learning. This is a longer-term change action
2. Staff training and communication – that shares, equips, embeds and enforces the changes
3. Assessments and interventions – initial, physiological interventions and prescribing reviews
4. Discharges and re-presentations – to monitor and review for insights and changes
5. Prison setting – to apply the above and transitions to the prison setting and service
During 2015-16 the service also supplied in excess of 250 Naloxone overdose prevention kits and provided the training in the use of these, which exceeded the annual supply of kits in Cambridge and Nottingham.
The Norfolk Public Health team also commission a young people’s substance misuse service. The lead provider is a non-statutory service and NSFT provides clinical staff to support the provision.
Proportion of all in treatment, who successfully completed treatment and did not re-present within six months
Lower = Red Similar = Amber Higher = Green
Baseline period 1 Oct 2013 – 30 Sept 2014 and re-presentations up to 31 March 2016
Latest available data 1 July 2014 – 30 June 2015 and re-presentations to 31 March 2015
National Data
Local Data
National Data
Local Data
Top Quartile range for comparison
Opiate clients 7.6% 8.2% 7% 7% 8.01% - 9.89%
Non-opiate clients 39.0% 30.7% 37.7% 26.2% 40.51% - 58.87%
(PA4)
ARA2016_master 140616.indd 13 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201614
Financial review
This part of the Annual Report provides a review of the financial performance for the year ending 31 March 2016.
The Trust has experienced a very challenging year with a planned deficit of £9.4m. Against this target the Trust improved its performance with a resultant £8.9m deficit.
The need to maintain strong financial control and management of limited resources during a period of strict financial regulatory measures was a key focus in a period when the quality of care we provided was under scrutiny. However, the balance of quality of care and financial control was enforced and improved throughout the year. As a result of this, the Trust achieved a Financial Sustainability Risk Rating (FSRR) of 2 against the financial risk ratings metrics as implemented by Monitor (the Independent Regulator for Foundation Trusts). The financial information contained within this section is taken from the Trust accounts for the year ended 31 March 2016 which have been prepared in accordance with directions issued by Monitor, and comply with International Financial Reporting Standards and are designed to present a true and fair view of the Trust’s financial activities.
A full set of 2015-16 accounts are attached as part of the Annual Report at the end of this document.
Going concern
The Foundation Trust’s accounts have been prepared on a ‘going concern’ basis. This means that the Trust expects to operate into the future and that the balance sheet (assets and liabilities) reflects the on-going nature of the Trust’s activities.
After making enquiries, the Directors have a reasonable expectation that the NHS Foundation Trust has adequate resources to continue in operational existence for the foreseeable future. For this reason, they continue to adopt the going concern basis in preparing the accounts.
Summary of financial performance
As at 31 March 2016, the Trust had delivered the following performance:
• A year-end deficit of £8.9m
• A Financial Sustainability Risk Rating (FSRR)of 2 (which resulted in closer monitoring by Monitor in terms of assessing the Trust’s ability to comply with its continuity of services licence conditions
• Capital expenditure of £4.3m
• A cash balance of £8.5m at 31 March 2016, which was in line with plan
Income
The Trust’s total income (turnover) for the year was £211.8m, of which £197.4m was for the provision of patient care activities.
The NHS financial settlement for 2015-16 resulted in a 1.6% reduction (the deflation adjustment) on health care services contracts. This meant that the Trust received 1.6% less funding to deliver the same volume of patient care. The required saving was reflected in our internal cost reduction plans.
Research and Development and Education and Training income totalled £2.0m and £3.6m respectively and did not change significantly from the previous year. Funding for Education and Training is met by Health Education England and is given to NHS Trusts to support training placements for student and junior medical staff, nursing staff and other healthcare professionals.
Income associated with non-patient care services to other NHS bodies was £4.9m compared to £6.4m in 2014-15. This reduction was due to a one-off source of income from the Department of Health in 2014-15 to support the roll out of the Trust’s new single electronic patient record system across the Trust which was implemented during 2015-16. The Trust’s principal sources of income, as illustrated in the chart below, are from contracts for the provision of mental healthcare services to Clinical Commissioning Groups (CCGs) in Norfolk and Suffolk and for secure services (both medium and low secure) and CAMHS tier 4 for NHS England Specialised Services. These commissioners provided £179.9m, 85% of total turnover in the year.
ARA2016_master 140616.indd 14 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 15
The total income source for the Trust is shown in the table below:
(FR1)
Norfolk and Suffolk NHS Foundation TrustSources of Income 2015/16
1% 5%
34%
14%
8%
29%
4%
3%2%
Norfolk CCGs (North, Norwich, South and West)
Suffolk CCGs (Ipswich and East Suffolk and West)
NHS Great Yarmouth and Waveney CCG
NHS England
Other income
Clinical Partnerships
Other clinical income
Education and Training
Research and Development
Expenditure
Total operating expenditure during 2015-16 amounted to £215.8m which is summarised by type of spend in the chart below.
(FR2)
The total spend on staffing was £159.6m, 73% of total expenditure.
Norfolk and Suffolk NHS Foundation TrustAnalysis of Expenditure 2015/16
Pay (£159.6m)
Other costs (£14.6m)
Premises and rentals (£11.7m)
Depreciation (£6.9m)
Establishment (£3.8m)
Public Dividend Payment (£3.9m)
General supplies and services (£7m)
Drugs and clinical supplies (£4.3m)
Transport (£2.7m)
Out of Area placements (£2.6m)
Specialist placements (£2.2m)
Exceptional items (£0.3m)
73%
2%
1%1%
5%
2%
3%
1%
7%0% 3% 2%
ARA2016_master 140616.indd 15 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201616
The Trust delivered £7.9m savings during 2015-16. All schemes identified at the start of the financial year underwent a Quality Impact Assessment by the Trust’s medical and nursing directors to ensure that any planned savings did not adversely affect patient safety and service quality.
Financial Sustainability Risk Rating (FSRR)
The Trust achieved a year end FSRR of 2 under Monitor’s Risk Assessment Framework. This financial metric, against which the Trust is measured, represents a combined rating against some of the key financial performance metrics contained within the financial statements. The two metrics focus on debt service cover and liquidity, which assess the Trust’s ability to meet its operational cash and debt financing obligations.
Capital expenditure and investments
The Trust’s capital expenditure largely supports the buildings and facilities we provide. The Treasury has historically provided capital finance in the form of public dividend capital. As a result, the Trust is required to pay the Treasury dividends relating to that capital in September and March of each year. These dividends amounted to £3.9m in 2015-16.
The Foundation Trust has limited access to new public dividend capital as it is expected to finance capital expenditure from internally generated sources (i.e. from surplus and depreciation charges) or to agree an interest-bearing loan with either the Foundation Trust Financing Facility (FTFF) or a commercial lender.
The outstanding balance on loans from the FTFF was £12.2m as at 31 March 2016.
The following table summarises the Trust’s capital expenditure during 2015-16:
Capital expenditure category Total £m New Electronic Patient Record and associated IT 0.63 Patient safety improvements 0.23 Backlog maintenence 0.89 Information, Communication and Technology (ICT) 0.46 Estated rationalisation supporting service changes 2.11 Totals 4.31
The capital plans were reviewed and revised on a regular basis to ensure that emerging schemes in year, e.g. CQC compliance and patient safety requirements were prioritised over and above other original planned expenditure.
Asset disposals for the year realised £8.5m, which the Trust used to re-invest in the Trust. These related to four properties: St. Clements Hospital in Ipswich, Meadowlands in Norwich, Violet Hill Day Hospital in Stowmarket and Highlands in Norwich.
Private Finance Initiative (PFI)
The Trust currently provides services from one location developed as a Private Finance Initiative – the Wedgwood Unit on the West Suffolk Hospital site in Bury St Edmunds. This unit was opened in May 2002 and provides mental health inpatient services.
Liquidity and cash management
The Trust manages cash through the Government Banking Services arrangements. There is very little scope to invest in financial instruments outside of this arrangement due to the way in which Public Dividend Capital dividends are calculated.
Post balance sheet events
The Board of Directors confirms that there are no post balance sheet events applicable to the 2015-16 financial year.
Charitable funds
The Foundation Trust also administers the Norfolk and Suffolk NHS Foundation Trust Charitable Fund (Charity Number 1050441). This is a merged fund of the Norfolk and Waveney Mental Health NHS Foundation Trust Charitable Fund (Charity Number 1050441) and the Suffolk Mental Health Partnership NHS Trust Charitable Fund (Charity Number 1103563). These funds are used for the benefit of both patients and staff in accordance with the purpose for which the funds were either raised or donated. Such uses include equipment for wards and training for staff.
ARA2016_master 140616.indd 16 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 17
Political and charitable donations The Trust did not make any political or charitable donations from its exchequer funds in 2015-16.
Financial outlook for 2016-17
The Government Spending Review acknowledged the scale of the financial challenge facing the NHS and announced a £10billion increase in NHS funding by 2021. However, in return for this increase the NHS must deliver £22billion of efficiency savings over the same period. Addressing operational efficiencies, rationalising estates, improving workforce productivity and improving use of IT and access to electronic records will all be key components for the NHS efficiency plans.
Mental health accounts for 23% of NHS activity but spending on secondary mental health services is equivalent to less than 50% of this. Low prioritisation of mental health has led to underinvestment in the service nationally. The Five Year Forward View for Mental Health (Mental Health Taskforce report February 2016) sets out an ambition to deliver rapid improvements in outcomes by 2020-21 through ensuring that 1 million more people with mental health problems are accessing high quality care. The Taskforce identifies the need to invest an additional £1billion in 2020-21.
Whilst there is much positive commentary about the prioritisation of mental health services the pressures faced by the NHS are increasing in a time when significant savings are being required. The additional funding described by the Mental Health Taskforce will be a significant step to achieving parity of esteem but whatever the position on funding for mental health services, we will strive to improve the care we deliver to all our service users, carers and their families, whether or not the funding to improve access to mental health care is delivered.
Environmental and social matters
Environmental matters
We have delivered a number of benefits through implementation of our Sustainability Policy:
Furniture reuse scheme:
• Saves money by not ordering new
• Saves resources (metal, wood, plastic) by not using new products
• Saves emissions on production
• Saves on disposal cost
• Helps wards comply with CQC
Out-of-date medical equipment:
• Saves on disposal costs
• Provides Trust with opportunities for positive news stories
• Helps reuse items that are still useful in their intended state
• Enables us to work with external providers and charities (GCCG)
Sales of older items:
• Enables us to gain an income from items that would previously have been thrown away
• Helps to keep our sites free of items that clutter
• Demonstrates that we are seeking appropriate opportunities to take business decisions
• Saves the cost of disposal to landfill
Energy:
• Improved understanding of energy provision
• Tighter budget control alongside sharp account management
• Determined pursuit of refunds and reductions (Siemens contract savings of £6,000)
ARA2016_master 140616.indd 17 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201618
Waste:
• Recognising waste as an asset and reducing amounts produced
• Reduction leading to lower costs
• Obtaining free services such as battery collections
• Educating to help reduce incorrect use of waste streams, which also saves money
• More efficient Waste Transfer Station to ensure compliance and avoid possible breaches
Working with the local community:
• Releasing items that are needed in our local community (gym equipment, beds, curtains)
• Good news about our Trust
• Helps prevent situations where service users enter our system because of support that is not available elsewhere
Social, community and human rights issues With almost 4000 employees and a turnover of over £200m the Trust is a significant employer in Norfolk and Suffolk. We aim to go beyond the requirements of our contracts and contribute to the wellbeing of the communities we serve.
In 2015-16 we supported a wide variety of community events. These included support for black and minority ethnic (BME) community festivals and events, LGBT Pride, Transgender Memorial Day, Mental Health and Spirituality, dementia awareness and a wide range of wellbeing initiatives.
The Trust developed its work on equality and diversity considerably in 2015-16. Building on a local initiative with BME communities in Ipswich in 2014 called the Open Mind Project, the Trust is a partner in the BME NHS Network ‘reverse commissioning’ project which included a helpful analysis of patterns of service use. Along with a Suffolk Healthwatch partnership project, this work is leading to innovative service developments in Suffolk. This was recognised when the work was shortlisted as a finalist in the 2015 Mental Health Positive Practices Awards.
Once evaluated the service development will be rolled out across both counties.
The Council of Governors hosted two successful conferences for members and the wider public on children and young people’s mental health, and a further event highlighting progress in supporting people with dementia to live fulfilling lives. Altogether these three events were attended by nearly 400 people.
We evaluate the effectiveness of many of our events by asking for delegate feedback. The events received very high satisfaction ratings and feedback enables us to plan future initiatives.
Human rights
The Trust has an important role to play in protecting human rights through its administration of the Mental Health Act (1983) (MHA). The Trust has a specialist team who promote good practice in the use of the MHA across its services. During 2015-16 the team developed a ‘heat map’ to identify any inpatient areas requiring more support, particularly in making sure that detained patients understood their rights. The use of the MHA is monitored by the bi-monthly interagency Mental Health Law Forum which reports to the Quality Governance Committee.
ARA2016_master 140616.indd 18 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 19
Directors’ report Disclosures
Details of company directorships and other significant interests held by directors can be found on page 35-38.
The Trust has complied with the costing principles and standards set out in the Approved Costing Guidance issued by Monitor.
Details of the Better Payment Practice Code can be found on page A37.
Enhanced quality governance reporting The Trust has had regard to Monitor’s quality governance framework in arriving at its overall evaluation of the organisation performance, internal control and board assurance framework.
During the reporting period the Trust has strengthened its service quality governance arrangements.
Summary of action plans to improve the governance of quality
As part of a wholesale review of strategy and following extensive consultation, the Trust has refreshed its five-year strategic goals. The first of these is to improve quality and achieve financial stability. As every staff members’ objectives are aligned with the strategic goals, quality improvement is integral to the Trust’s governance arrangements. The Board of Directors has also reviewed the work of the Board committees, updating their terms of reference so as to clarify the focus on quality. The Board has introduced a Programme Management Office (PMO) which supports the delivery of Quality Improvement Plans, including improvements identified by the CQC inspection in 2014/15. The PMO reports to the Transformation Programme Board, chaired by the chief executive who in turn reports on progress to every Board meeting.
Developmental work has also taken place during the reporting year on a wide range of
quality related themes, including learning from incidents, risk management and the Board Assurance Framework.
Further details on arrangements to improve governance of quality can be found in the Annual Governance Statement starting on page A8 and within the Quality Account starting on page 78.
Patient care The Trust uses its foundation trust status to develop services and improve patient care through the work of the Council of Governors. Governors are involved in a wide range of initiatives. The role of the Council of Governors is to: • Represent the interests of local people in commenting on local service developments and on quality issues • Triangulate information on quality by reading reports and listening to service users, carers and the wider public
• Hold the non-executives to account for the performance of the Board of Directors
The Council of Governors’ Planning and Performance Subgroup scrutinises a wide range of Trust activites that impacts on quality. During the reporting period, the subgroup considered: the Trust’s annual plan, the new operating model, the impact of the Lorenzo IT and business process system, the reduction in use of restrictive practices, the Board development plan and the financial recovery plan.
Following feedback from governors, the Trust improved its complaints handling arrangements so as to ensure better quality assurance of responses. The complaints team provides an annual report to the Quality Governance Committee, which highlights themes and learning from complaints.
During the reporting period, the Trust has prioritised the improvement of accessible information for patients, particularly people with a learning disability and people who do not speak or read English.
Accountability report
ARA2016_master 140616.indd 19 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201620
Stakeholder relations
The Trust has well-established and valuable partnership arrangements with a wide range of statutory and voluntary sector organisations. By pooling funding, resources and skills the Trust is able to bring benefits to local people well beyond what it could achieve on its own. In addition to our joint working with local authorities’ social care services, our partnerships include:
Norfolk Recovery Partnership – the Trust works with The Matthew Project, Rehabilitation for Addicted Prisoners Trust (RAPt) and a wide range of other groups to help people with drug and alcohol dependence.
COMPASS – innovative education-based programmes supporting young people at risk of exclusion from school.
Connect Service – support for looked after children and their families and carers in Suffolk.
Police support – working in control rooms and street cars to provide the best possible response for people with mental health needs who come into contact with the police.
Criminal justice support – providing police and court liaison services so that people can access help when needed.
Wellbeing services – working with a wide range of partner organisations to help people with common mental health problems.
The Trust also supports joint policy and practice initiatives such as suicide reduction, autism awareness, and local Healthwatch projects.
Consultation with local groups and organisations / public and patient involvement activities
The Board of Directors has published a summary document describing its approach to consultation and involvement.
The relevant Trust documents / policies are:
• Our values…our behaviours…our future. Working together for better mental health (launched October 2015)
• Improving services together: Involvement and Engagement Strategy (launched October 2015)
• Membership Strategy (which is approved annually by the Council of Governors (CoG) and the Board of Directors (BoD)
Involvement of service users and carers Information about how to get involved is published on the Trust website: www.nsft.nhs.uk > Get involved > Service user and carer involvement
This section of the website explains the Trust’s policy on involvement. The website lists the wide variety of opportunities that there are for service users and carers to get involved.
It includes a link to the strategy, which was launched at the Trust’s AGM on 8 October 2015. Improving services together: Involvement and Engagement Strategy – 2015-2017. The strategy grew from the recognition that there are many ways for service users and carers to be meaningfully involved in their own care and in the development of local services. A ‘one size’ service user / carer council approach was insufficient to promote real involvement.
The strategy sets out the six commitments that the Trust has made:
1. Service users and carers will be able to have their say in Trust business.
2. There will be opportunities for service users and carers to use their skills and experiences to improve services.
3. We are changing the way we provide our services in line with our commitment to organisational change.
4. We will strengthen links and create partnerships with other agencies and service user and carer-led organisations.
5. We will reach out to diverse and other under-represented groups.
6. Service users and carers will ‘judge’ whether this strategy is being delivered.
For each commitment there is a list of ‘what you will see’. The level of involvement in care planning is also measured by the independently run annual service user survey.
ARA2016_master 140616.indd 20 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 21
Involvement of members and the wider community
Membership of the Trust is open to all residents of Suffolk and Norfolk aged 11 and over. Most members are interested in being kept informed about the work of the Trust and this takes place through Insight Magazine and a monthly Trust Matters email newsletter. Members who wish to be more involved can attend engagement events and also stand for election as governor (if aged 16 or over).
Member involvement (and involvement with the wider public) by governors is overseen by the governor-led Membership and Communications Subgroup which reports to the Council of Governors. The Trust has a full time membership and engagement officer who ensures Trust representation at community events.
In addition to representing the Trust at a wide range of community events and networks, the Council of Governors hosts two large member engagement events each year (one in each county) on a topical theme. In 2014 this was criminal justice and mental health, in 2015 it was young people’s mental health and in 2016 it is dementia.
The Trust Board of Directors reviews the way it engages and manages its stakeholder relationships. Consultation
The Trust aims to ensure proportionate meaningful consultation in line with S.242 of the NHS Act (2006) (‘the duty to consult’). In all cases the impact on people who share protected characteristics as defined by the Equality Act (2010) will be considered.
This means that for proposed changes that impact on local areas or services (for example changes to inpatient activity programmes) then consultation takes place via community / ward meetings so that those people affected are involved in decisions.
For proposals that involve changes to the configuration of services (for example, closing one service and opening a new one with a different focus as part of modernising services) then wider consultation is required, which takes into account the impact not just on people using services at the time but future services users and carers. Depending on the nature of the change, consultation may be led by the commissioners.
There are formal partnership arrangements with Staff Side to consult over changes that might impact on staff, largely via the Trust Partnership Meeting (TPM) and Local Negotiating Committee (LNC).
Interface with other consultative forums
Governors attend other consultative forums, including Health Overview and Scrutiny Committees (HOSC), Norfolk Heathwatch, Suffolk Healthwatch and Health and Wellbeing Boards. The roles of each of these groups are different and, whilst insights will inform governor deliberations, this exchange of information is a positive aspect.
The Trust’s constitution prohibits a member of the HOSC from also being a governor in order to avoid a conflict of interest.
Staff governors have a specific role description to ensure that the role of staff governor and that of staff / union representative are differentiated.
Statement of Disclosure to auditors (s418)
For each individual who is a director at the time that the report is approved:
So far as the director is aware, there is no relevant audit information of which the Trust’s auditor is unaware.
The director has taken all of the steps that they ought to have taken as a director in order to make themselves aware of any relevant audit information and to establish that the NHS foundation trust’s auditor is aware of that information.
Income disclosures required by Section 43(2A) of the NHS Act 2006
The Trust has met the requirements of the NHS Act that the income from the provision of goods and services for the purposes of the health service in England was greater than any income from the provision of goods and services for any other purpose.
Michael Scott Chief Executive
Date: 25 May 2016
ARA2016_master 140616.indd 21 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201622
Remuneration report – Annual statement on remuneration
Statement from Chair of Remuneration and Terms of Service Committee
During the financial year 2015-16 the Remuneration and Terms of Service Committee oversaw the appointment of the Director of Finance who took up her post on 1 December 2015. In the light of the benchmarking data presented to the committee on 25 June 2015 and given the market conditions, it was agreed to increase the salary for this post to £130k.
The structure of all other executive director remuneration remained unchanged with salaries near or below average.
There was no change to any other aspects of the remuneration arrangements for executive directors. The Trust does not operate a bonus or performance related payment scheme for executive directors.
Senior management remuneration policy
The Remuneration and Terms of Service Committee also considers senior management pay at the level below executive director. At its meeting on 7 September 2015 the committee noted that because executive director pay tends to be at or below average, senior management staff who are subject to Agenda for Change band 9 pay conditions can earn more than executive directors. In the light of this, the committee agreed that in future no new band 9 appointments would be made.
Gary Page Chair
Dated: 25 May 2016
ARA2016_master 140616.indd 22 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 23
Future policy table
The Trust does not operate a bonus or performance related payment scheme for senior managers and has no plans to do so at present.
Payments above £142,500 pa (Prime Minister’s ministerial and parliamentary salary level)
The Chief Executive is the only senior manager who is paid more than £142,500. The salary is set by the Remuneration and Terms of Service Committee. The committee took into account benchmarking information regarding CEO payment levels in Trusts of comparable size. The CEO salary is in line with the level of payment for Trusts with a similar turnover and there has been no increase in salary since appointment. There are no additional performance related pay or bonus arrangements.
Service contracts obligations
The Trust’s contracts of employment set out our obligations in regard to salary deductions in respect of tax, national insurance and pension contributions in accordance with legislation and pension scheme regulations.
Contracts set out circumstances in which a termination of employment may be triggered and obligations in regard to contractual notice payments and the payment of any outstanding annual leave.
Our contracts more generally set out contractual entitlements and obligations for such as:
• Maintaining and providing a safe place of work, free of hazards and risks, as per the health and safety at work act
• Statutory and occupational maternity, paternity and adoption leave, pay and other related rights
• Access to Statutory Sick Pay and Occupational Sick Pay for those meeting qualification criteria
Policy on payment for loss of office
Notice periods are set within our contracts of employment and are set following consultation with our recognised trade unions, with the exception of directors’ notice periods, which are set by the Remuneration Committee. With the exception of summary dismissal for which there is no notice entitlement, Band 8a and above managers are subject to a three-month notice period. Executive directors have a six-month notice period, as set by the Remuneration Committee.
Payments for loss of office are determined based on contractual entitlements (e.g. for redundancy). For all staff, excluding executive directors, this is based on NHS national terms and conditions. For executive directors, their contractual entitlements reflect those set out in Agenda for Change with the exception of notice entitlements (see above).
Performance is not relevant to the determination of payment for loss of office.
In the event of exceptional circumstances, any payments for loss of office outside contractual entitlement would be referred to Monitor / TDA for approval.
Statement of consideration of employment conditions elsewhere in the foundation trust
All senior managers within the Trust, with the exception of executive directors, are paid in accordance with Agenda for Change terms and conditions of employment. The remuneration for executive directors is reviewed by the Remuneration Committee on an annual basis taking account of external benchmarking information and the remuneration of staff directly reporting into the directors.
ARA2016_master 140616.indd 23 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201624
Annual report on remuneration
Remuneration and Terms of Service Committee
The Remuneration and Terms of Service Committee is a non-executive director committee that oversees the appointment, remuneration and appraisal of the Trust’s executive directors. It also reviews senior management pay. Senior managers’ pay below director level is set in line with the nationally negotiated Agenda for Change salary scales and therefore is not part of a separate negotiation or consultation process.
The Committee is chaired by the Trust Chair and is made up of all non-executive directors. Members for 2015-16 are shown in the attendance list.
The CEO is a member for the purpose of appointing executive directors and considering performance appraisal information (but is not party to discussions about CEO pay or performance).
Leigh Howlett (Director of Strategy and Resources), whose portfolio includes HR, attended part of the meeting held on 25 June 2015 to provide advice on senior management pay.
The Remuneration and Terms of Service Committee receives reports from the CEO on executive director performance and from the Chair on CEO performance.
During the year, the Committee referred to a benchmarking report by Capita (at a cost of £250) in order to assist in its review of salaries for executive directors.
Appointments
The Committee ensures that a robust and transparent process is followed in relation to executive director appointments.
During the review period the Committee oversaw the recruitment process for the Director of Finance / Deputy Chief Executive. The Committee appointed Odgers Berndtson as independent recruitment consultants to assist with this appointment.
Odgers Berndtson did not carry out any other work for the Trust in the reporting period and have no other connections with the organisation and were judged to be independent. The fee paid to Odgers Berndtson for this work was £21,637.
Executive director appointments are normally substantive, with notice periods and termination periods being limited to contractual minimums.
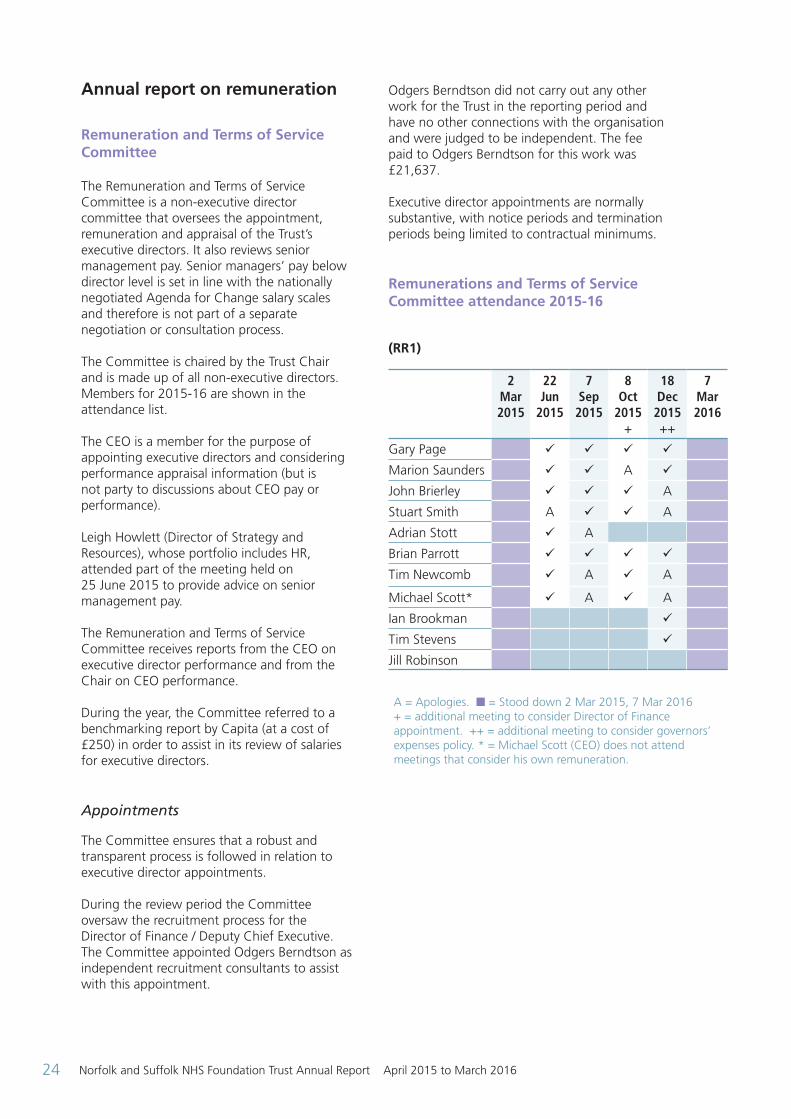
Remunerations and Terms of Service Committee attendance 2015-16
(RR1)
2 Mar 2015
22 Jun
2015
7 Sep
2015
8 Oct
2015 +
18 Dec
2015 ++
7 Mar 2016
Gary Page ü ü ü ü
Marion Saunders ü ü A ü
John Brierley ü ü ü A
Stuart Smith A ü ü A
Adrian Stott ü A
Brian Parrott ü ü ü ü
Tim Newcomb ü A ü A
Michael Scott* ü A ü A
Ian Brookman ü
Tim Stevens ü
Jill Robinson
A = Apologies. n = Stood down 2 Mar 2015, 7 Mar 2016 + = additional meeting to consider Director of Finance appointment. ++ = additional meeting to consider governors’ expenses policy. * = Michael Scott (CEO) does not attend meetings that consider his own remuneration.
ARA2016_master 140616.indd 24 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 25
Membership in 2015-16 consisted of:
Gary Page: Chair
Marion Saunders: Senior Independent Director
John Brierley: Non-executive Director
Brian Parrott: Non-executive Director
Tim Newcomb: Non-executive Director
Adrian Stott: Non-executive Director (stood down October 2015)
Stuart Smith: Non-executive Director (term ended 28 February 2016)
Ian Brookman: Non-executive Director (from 1 December 2015)
Tim Stevens: Non-executive Director (from 1 December 2015)
Jill Robinson: Non-executive Director (from 1 January 2016)
The Trust drew on an independent benchmarking report on executive pay provided by Capita (for a fee of £250) with a commentary by the Head of HR.
Nominations Committee
The Nominations Committee is a governor majority committee that oversees the appointment, remuneration and appraisal of the Trust’s Chair and non-executive directors. Non-executive directors are appointed for an initial three-year term and may, on satisfactory achievement of objectives, be offered a second three-year term. However, a third term would normally only be offered through an open competitive process. In all case the non-executive director must remain independent. The constitution also sets out how non-executive directors may be removed through a governor vote at a Council of Governors meeting.
It is chaired by the Senior Independent Director (SID) with the Lead Governor as vice-Chair.
During the financial year 2014-15 the Council of Governors agreed that there should be a core voting membership of the committee that included one governor from each constituency,
with other governors being able to be members of the committee on a non-voting basis.
The core voting governors during 2015-16 were:
• Guenever Pachent (Lead Governor)
• Dr Karen O’Sullivan (Staff Governor)
• Catherine Wells (Norfolk Public Governor)
• Jane Millar (Suffolk Public Governor)
• Mary Rose Roe (Norfolk Carer Governor)
• Kevin James (Norfolk Service User Governor)
• Sue Whitaker (Partner Governor)
Following the 2015-16 election, Howard Tidman took over from Dr Karen O’Sullivan who had come to the end of her term as staff governor.
Non-voting governor members consisted of:
• Stephen Fletcher (Norfolk Public Governor)
• Paddy Fielder (Suffolk Public Governor)
• Sheila Preston (Norfolk Public Governor)
During the year under review the nominations committee re-considered the core voting membership arrangement and agreed to bring forward a proposal to widen the membership during 2016-17.
Appointment and re-appointment processes
The committee ensures that a robust and transparent process is followed in relation to all appointments and re-appointments. During the review period the committee oversaw the NED recruitment process for three new NEDs and the re-appointment process for the Chair.
Three NED appointments were made by the Council of Governors on 30 October 2016, with Ian Brookman and Tim Stevens taking up their roles on 1 December 2015 and Jill Robinson taking up her role on 1 January 2016. The Trust used external recruitment consultants Gatenby Sanderson to assist in this process. The fee for this work was £25,981.84. Care was taken to advertise the positions widely in order to attract a wide range of candidates from all walks of life.
ARA2016_master 140616.indd 25 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201626
In line with the Nomination Committee’s policy of offering a second term where there has been positive performance against objectives, the Committee considered a proposal to re-appoint Gary Page for a second three-year term as Chair of the Trust. The Nominations Committee took into account Gary Page’s performance appraisals (which are carried out by the Senior Independent Director) and feedback from stakeholders. The Committee recommended the re-appointment to the Council of Governors on 18 February 2016. The Council of Governors approved the appointment with the new term of appointment starting on 2 April 2016.
The Committee also considered and recommended a proposal to extend the term of John Brierley from 9 November 2015 to 28 April 2016 so that, as Chair of the Audit and Risk Committee, there would be continuity for the end of the financial year. This was approved by the Council of Governors on 1 October 2015.
Remuneration
The Nominations Committee reviews the Chair and NED remuneration and expenses policies annually.
The Committee reviewed a benchmarking report on levels of remuneration for the Chair, NED, SID and Chair of Audit and Risk at its meeting on 27 July 2015.
The Chair, NED and SID levels of remuneration were found to be at or below average when compared to other NHS Trusts and so no changes were proposed. The Chair of the Audit and Risk Committee remuneration was found to be slightly above average and it was therefore agreed to reduce the payment (from £16k to £14.5k) for the new appointment, which took place later in the year.
The Nominations Committee also reviewed the mileage rate paid to the Chair and NEDs. Following consultation it was proposed to move from Agenda for Change rates to HMRC rates i.e. from 56ppm (to 3,500 miles then 20ppm) to 45ppm (to 10,000 miles then 25ppm), generating a modest saving.
These changes were approved by the Council of Governors on 1 October 2015.
Appraisals
The Committee received reports on the appraisals of the NEDs and Chair and provided assurance to the Council of Governors that the process followed had been robust. The Nominations Committee also comments on proposed objectives for the Chair and NEDs.
Other developmental work
On behalf of the Council of Governors the Nominations Committee oversees the Board development plan based on the external review carried out by Foresight Partnership in 2014-15.
The committee oversaw the process for the election of the Lead Governor in 2016.
Following a review of the terms of reference and work plan for the committee, a recommendation was made to move to four meetings a year (instead of six) for 2016.
(RR2) Nominations Committee attendance 2015-16
26 May 2015
28 July 2015
29 Sept 2015
24 Nov 2015
26 Jan
2016
Marion Saunders ü ü ü ü
Gary Page ü ü ü ü
Guenever Pachent ü A ü ü
Karen O’ Sullivan ü ü ü ü
Sue Whitaker ü ü A ü
Kevin James ü ü ü A
Catherine Wells ü ü ü ü
Mary Rose Roe ü A A ü
Paddy Fielder ü ü ü A
Stephen Fletcher A A A ü
Sheila Preston A ü A ü
Jane Millar A ü ü ü
A = Apologies. n = Stood down 29 Sept 2015
ARA2016_master 140616.indd 26 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 27
Membership in 2015-16 consisted of:
Marion Saunders: SID, Nom Ctte Chair
Gary Page: Chair
Core voting governors (one from each constituency plus lead):
Guenever Pachent: Lead Governor
Dr Karen O’Sullivan: Staff Governor
Catherine Wells: Norfolk Public Governor
Jane Millar: Suffolk Public Governor
Mary Rose Roe: Norfolk Carer Governor
Kevin James: Norfolk Service User Governor
Sue Whitaker: Partner Governor
Following the 2015-16 election, Howard Tidman took over from Dr Karen O’Sullivan who had come to the end of her term as staff governor Non-voting governors:
Stephen Fletcher: Norfolk Public Governor
Paddy Fielder: Suffolk Public Governor
Sheila Preston: Norfolk Public Governor
ARA2016_master 140616.indd 27 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201628
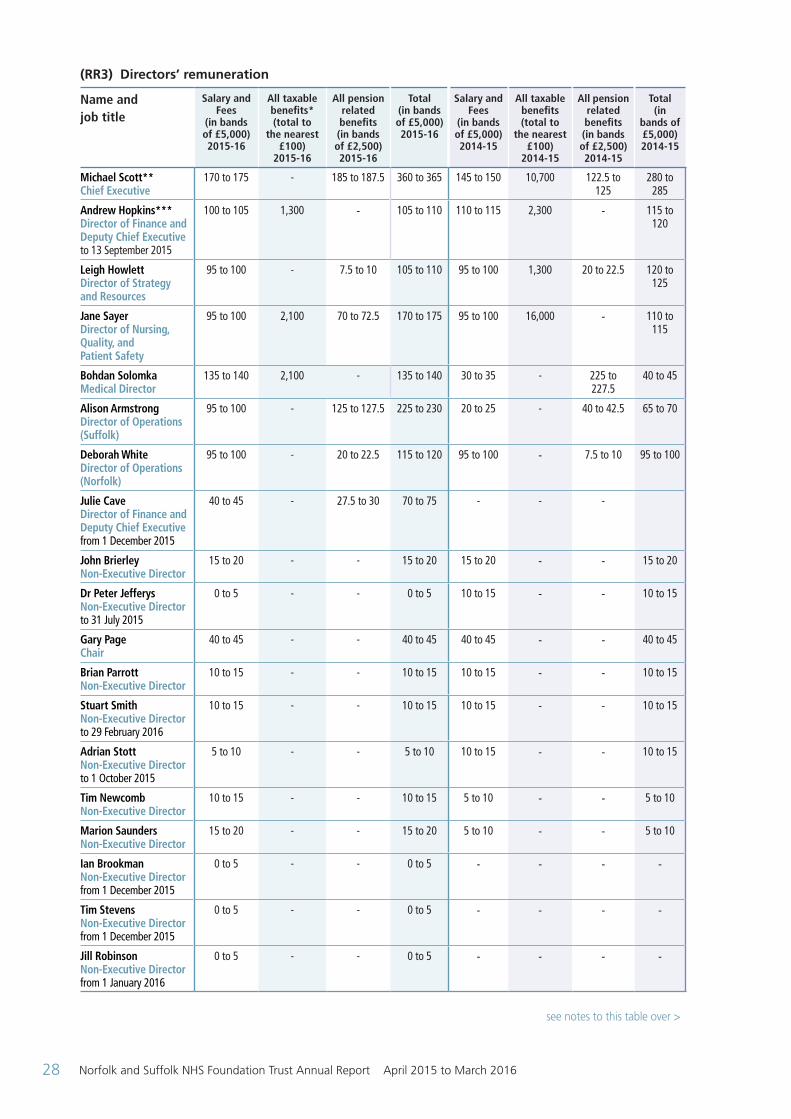
(RR3) Directors’ remuneration
Name andjob title
Salary and Fees
(in bands of £5,000) 2015-16
All taxable benefits* (total to
the nearest £100)
2015-16
All pension related benefits (in bands of £2,500) 2015-16
Total (in bands of £5,000) 2015-16
Salary and Fees
(in bands of £5,000) 2014-15
All taxable benefits (total to
the nearest £100)
2014-15
All pension related benefits (in bands of £2,500) 2014-15
Total (in
bands of £5,000) 2014-15
Michael Scott**Chief Executive
170 to 175 - 185 to 187.5 360 to 365 145 to 150 10,700 122.5 to 125
280 to 285
Andrew Hopkins***Director of Finance and Deputy Chief Executive to 13 September 2015
100 to 105 1,300 - 105 to 110 110 to 115 2,300 - 115 to 120
Leigh HowlettDirector of Strategy and Resources
95 to 100 - 7.5 to 10 105 to 110 95 to 100 1,300 20 to 22.5 120 to 125
Jane SayerDirector of Nursing, Quality, and Patient Safety
95 to 100 2,100 70 to 72.5 170 to 175 95 to 100 16,000 - 110 to 115
Bohdan SolomkaMedical Director
135 to 140 2,100 - 135 to 140 30 to 35 - 225 to 227.5
40 to 45
Alison ArmstrongDirector of Operations (Suffolk)
95 to 100 - 125 to 127.5 225 to 230 20 to 25 - 40 to 42.5 65 to 70
Deborah WhiteDirector of Operations (Norfolk)
95 to 100 - 20 to 22.5 115 to 120 95 to 100 - 7.5 to 10 95 to 100
Julie CaveDirector of Finance and Deputy Chief Executive from 1 December 2015
40 to 45 - 27.5 to 30 70 to 75 - - -
John BrierleyNon-Executive Director
15 to 20 - - 15 to 20 15 to 20 - - 15 to 20
Dr Peter JefferysNon-Executive Director to 31 July 2015
0 to 5 - - 0 to 5 10 to 15 - - 10 to 15
Gary PageChair
40 to 45 - - 40 to 45 40 to 45 - - 40 to 45
Brian ParrottNon-Executive Director
10 to 15 - - 10 to 15 10 to 15 - - 10 to 15
Stuart SmithNon-Executive Director to 29 February 2016
10 to 15 - - 10 to 15 10 to 15 - - 10 to 15
Adrian StottNon-Executive Director to 1 October 2015
5 to 10 - - 5 to 10 10 to 15 - - 10 to 15
Tim NewcombNon-Executive Director
10 to 15 - - 10 to 15 5 to 10 - - 5 to 10
Marion SaundersNon-Executive Director
15 to 20 - - 15 to 20 5 to 10 - - 5 to 10
Ian BrookmanNon-Executive Director from 1 December 2015
0 to 5 - - 0 to 5 - - - -
Tim StevensNon-Executive Director from 1 December 2015
0 to 5 - - 0 to 5 - - - -
Jill Robinson Non-Executive Director from 1 January 2016
0 to 5 - - 0 to 5 - - - -
see notes to this table over >
ARA2016_master 140616.indd 28 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 29
* Other remuneration includes the benefit in kind received relating to the provision of lease cars and relocation expenses.
** Michael Scott joined the Trust in May 2014, and so 2015-16 is the first full year of employment.
*** Andrew Hopkins received a contractual payment in lieu of notice of £55k.
Pensions (RR4)
Name andjob title
Real increase
in pension at pension age (bands of £2,500)
Real increase
in pension lump sum at pension age (bands of £2,500)
Total accrued
pension at pension age at
31 March 2016
(bands of £5,000)
Lump sum at pension age related to accrued penion at 31 March
2016 (bands of £5000)
Cash Equivalent
Transfer Value at 1 April 2015
(rounded to nearest
£000)
Real increase in Cash
Equivalent Transfer
Value (rounded to nearest
£000)
Cash Equivalent
transfer value at
31 March 2016
(rounded to nearest
£000)
Michael ScottChief Executive
7.5 to 10 25 to 27.5 65 tp 70 205 to 210 1,335 213 1,549
Andrew Hopkins*Director of Finance and Deputy Chief Executive to 13 September 2015
0 to (2.5) 0 to (2.5) 35 to 40 105 to 110 624 (9) 615
Leigh HowlettDirector of Strategy and Resources
0 to 2.5 2.5 to 5 35 to 40 105 to 110 649 24 673
Jane SayerDirector of Nursing, Quality and Patient Safety
2.5 to 5 10 to 12.5 35 to 40 115 to 120 600 68 669
Bohdan SolomkaMedical Director
(5) to (7.5) (17.5) to (20)
35 to 40 110 to 115 773 (103) 670
Alison ArmstrongDirector of Operations (Sfk)
5 to 7.5 17.5 to 20 40 to 45 125 to 130 736 135 671
Deborah WhiteDirector of Operations (Nfk)
0 to 2.5 2.5 to 5 30 to 35 100 to 105 579 32 611
Julie CaveDirector of Finance and Deputy Chief Executive from 1 December 2015
0 to 2.5 2.5 to 5 45 to 50 145 to 150 863 37 900
Pension benefits shown above relate to membership of the NHS Pension Scheme, which is available to all employees within the Foundation Trust. No additional pension payments are made by the Trust in relation to senior employees. As non-executive directors do not receive pensionable remuneration,
From 4 August to 30 November 2015 John Doyle was employed as interim Director of Finance. The Trust paid a total of £60-65k
NSFT currently has 27 governors out of a possible 31 in place – 18 of the 27 received expenses in the year, The aggregate expenses receive by governors for the financial year was £13,100 (2014-15 £16,200)
there will be no entries in respect of pension for non-executive members.
The value of pensions is at 31 March 2016 – A Hopkins left during the period but this valuation has not been undertaken at his leaving date.
ARA2016_master 140616.indd 29 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201630
Cash Equivalent Transfer Values
A Cash Equivalent Transfer Value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member’s accrued benefits and any contingent spouse’s pension payable from the scheme. A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
Real Increase in CETV This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses common market valuation factors for the start and end of the period.
ARA2016_master 140616.indd 30 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 31
Review of Tax Arrangements of Public Sector Appointees (not subject to audit)
As required by HM Treasury as per PES(2012)17, the Trust must disclose information regarding “off-payroll engagements”.
(RR5)
Number existing engagements as of 31 March 2016 21
Of which:
Number that have existed for less than one year at the time of reporting 15
Number that have existed for between one and two years at the time of reporting 5
Number that have existed for between two and three years at the time of reporting 1
Number that have existed for between three and four years at the time of reporting 0
Number that have existed for four or more years at the time of reporting 0
The existing off-payroll engagements, as outlined above, have been subject to a risk based assessment as to whether assurance is required that the individual is paying the right amount of tax and, where necessary, that assurance has been sought.
Number of new engagements, or those that reached six months 22 in duration between 1 April 2015 and 31 March 2016
Number of the above which include contractual clauses giving the trust the right to request assurance in relation to income tax and national insurance obligations 22
Number for whom assurance has been requested
Of which:
Number for whom assurance has been received 21
Number for whom assurance has not been received* 1
Number that have been terminated as a result of assurance not being received 0
Number of off-payroll engagements of Board members, and / or senior officials 1 with significant financial responsibility, during the financial year.
Number of individuals that have been deemed “Board members and/or senior officials with significant financial responsibility”. This figure should include both off-payroll and on-payroll engagements.
9
Details of the exceptional circumstances that led to each of these engagements
Whilst recruiting for a new Director of Finance, a secondment from Mersey Care NHS Trust was agreed with John Doyle to take up the post of Interim Director of Finance for the period 4 August to 31 October 2015. This then became an off-payroll engagement with Maycliffe Ltd from 1 to 30 November 2015.
*The individual from whom assurances have not been received is no longer working for NSFT.
ARA2016_master 140616.indd 31 14/06/2016 11:10
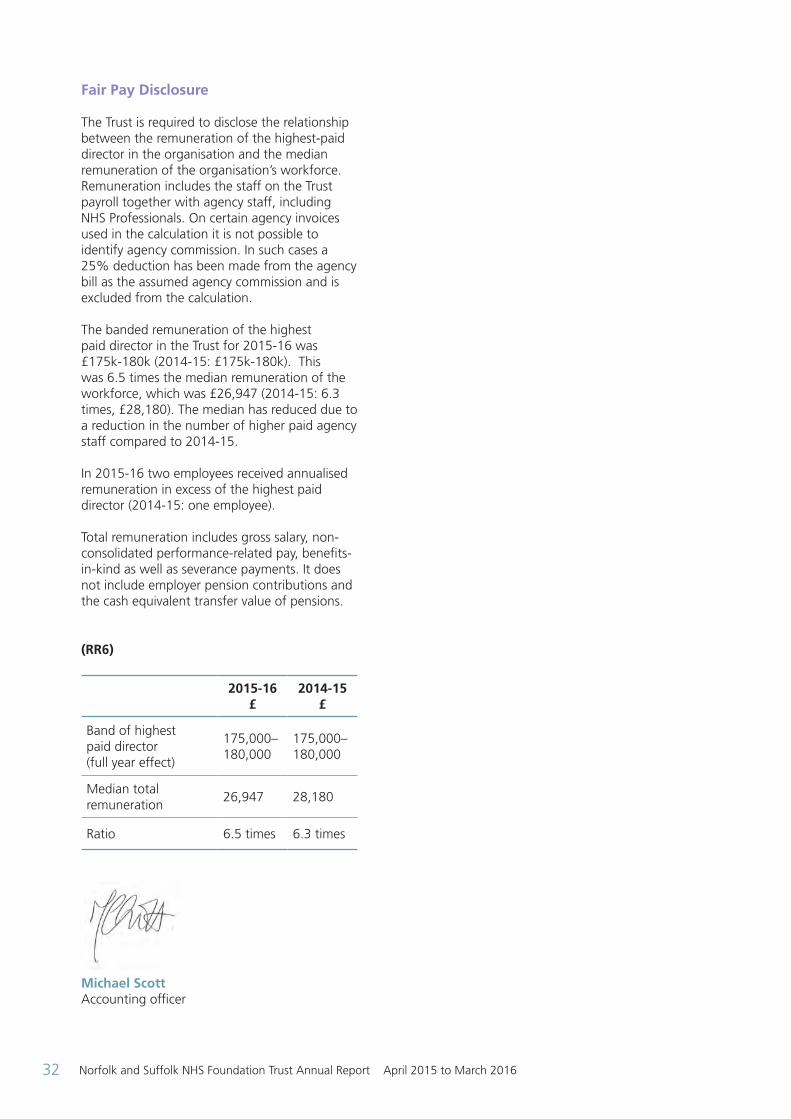
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201632
Fair Pay Disclosure
The Trust is required to disclose the relationship between the remuneration of the highest-paid director in the organisation and the median remuneration of the organisation’s workforce. Remuneration includes the staff on the Trust payroll together with agency staff, including NHS Professionals. On certain agency invoices used in the calculation it is not possible to identify agency commission. In such cases a 25% deduction has been made from the agency bill as the assumed agency commission and is excluded from the calculation.
The banded remuneration of the highest paid director in the Trust for 2015-16 was £175k-180k (2014-15: £175k-180k). This was 6.5 times the median remuneration of the workforce, which was £26,947 (2014-15: 6.3 times, £28,180). The median has reduced due to a reduction in the number of higher paid agency staff compared to 2014-15.
In 2015-16 two employees received annualised remuneration in excess of the highest paid director (2014-15: one employee).
Total remuneration includes gross salary, non-consolidated performance-related pay, benefits-in-kind as well as severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions.
(RR6)
2015-16 £
2014-15 £
Band of highest paid director (full year effect)
175,000–180,000
175,000–180,000
Median total remuneration
26,947 28,180
Ratio 6.5 times 6.3 times
Michael Scott Accounting officer
ARA2016_master 140616.indd 32 14/06/2016 11:10
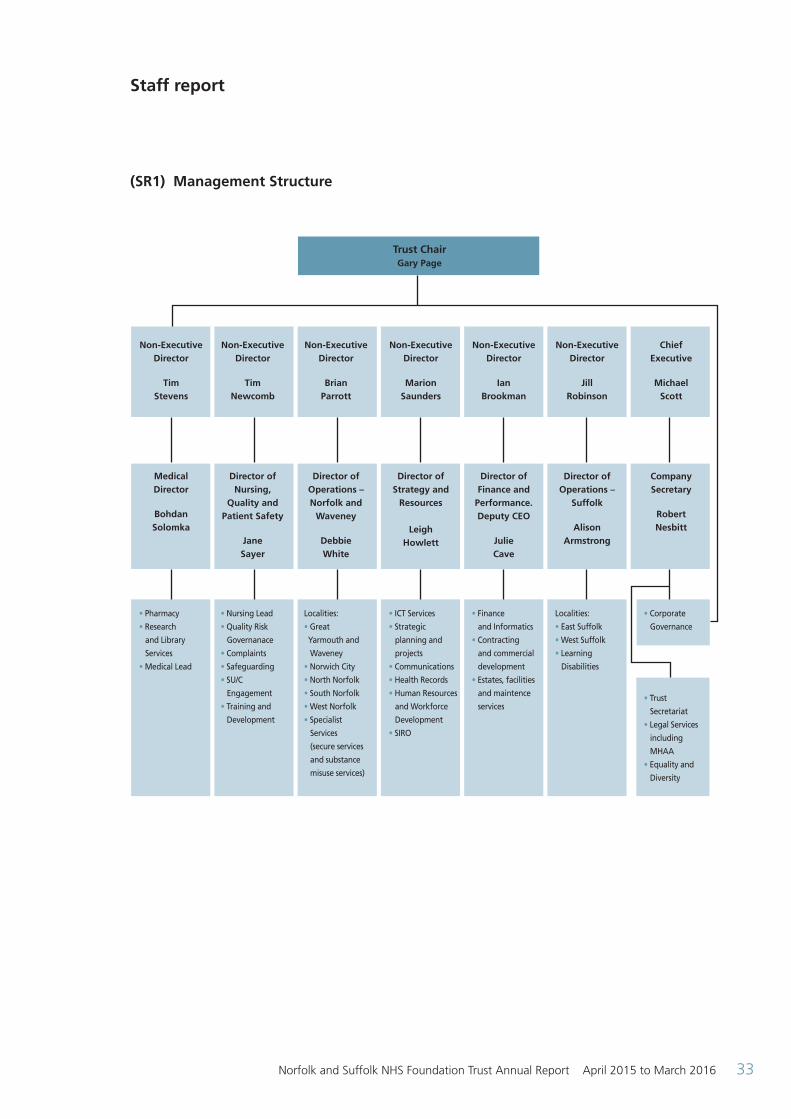
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 33
Staff report
(SR1) Management Structure
Trust Chair Gary Page
Non-Executive Director
Tim Stevens
Non-Executive Director
Tim Newcomb
Non-Executive Director
Brian Parrott
Non-Executive Director
Marion Saunders
Non-Executive Director
Ian Brookman
Non-Executive Director
Jill Robinson
Chief Executive
Michael Scott
Medical Director
Bohdan Solomka
Director of Nursing,
Quality and Patient Safety
Jane Sayer
Director of Operations – Norfolk and
Waveney
Debbie White
Director of Strategy and
Resources
Leigh Howlett
Director of Finance and
Performance. Deputy CEO
Julie Cave
Director of Operations –
Suffolk
Alison Armstrong
Company Secretary
Robert Nesbitt
• Pharmacy
• Research
and Library
Services
• Medical Lead
• Nursing Lead
• Quality Risk
Governanace
• Complaints
• Safeguarding
• SU/C
Engagement
• Training and
Development
Localities:
• Great
Yarmouth and
Waveney
• Norwich City
• North Norfolk
• South Norfolk
• West Norfolk
• Specialist
Services
(secure services
and substance
misuse services)
• ICT Services
• Strategic
planning and
projects
• Communications
• Health Records
• Human Resources
and Workforce
Development
• SIRO
• Finance
and Informatics
• Contracting
and commercial
development
• Estates, facilities
and maintence
services
Localities:
• East Suffolk
• West Suffolk
• Learning
Disabilities
• Corporate
Governance
• Trust
Secretariat
• Legal Services
including
MHAA
• Equality and
Diversity
ARA2016_master 140616.indd 33 14/06/2016 11:10
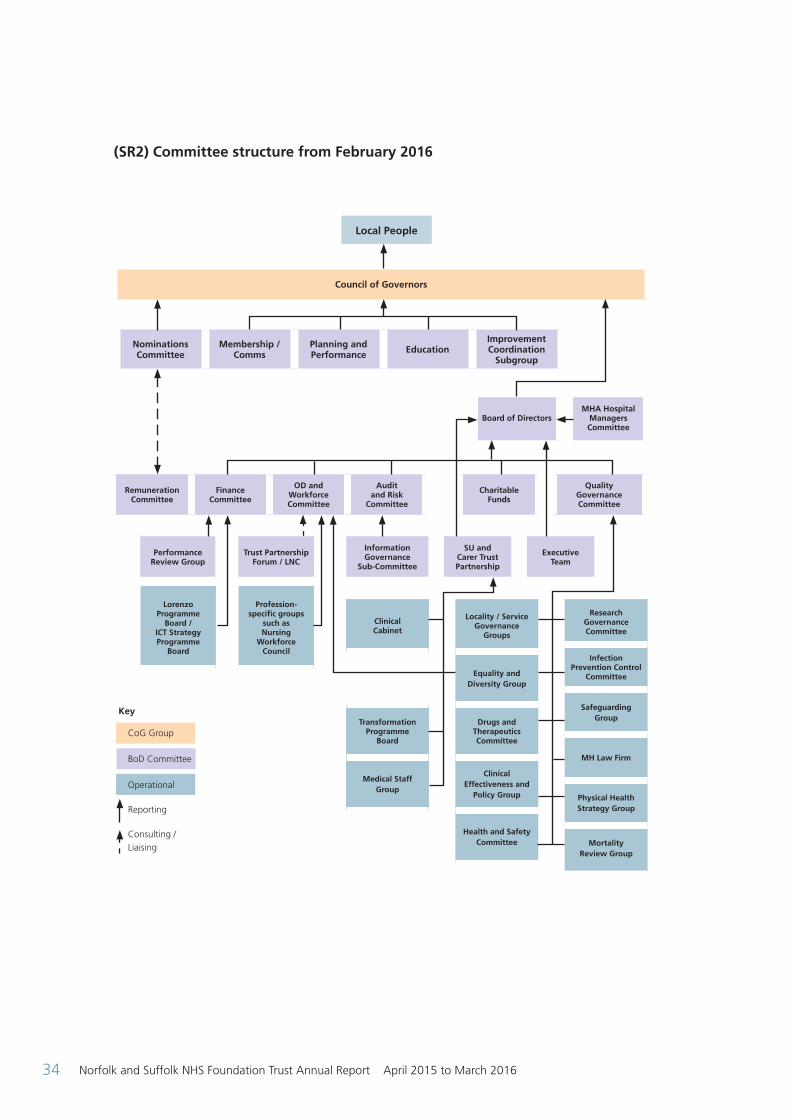
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201634
Nominations Committee
Membership / Comms
Planning and Performance Education
Improvement Coordination
Subgroup
Council of Governors
Remuneration Committee
Finance Committee
OD and Workforce Committee
Audit and Risk
Committee
Charitable Funds
Quality Governance Committee
Performance Review Group
Trust Partnership Forum / LNC
Information Governance
Sub-Committee
SU and Carer Trust Partnership
Executive Team
Board of DirectorsMHA Hospital
Managers Committee
Research Governance Committee
Infection Prevention Control
Committee
Safeguarding Group
MH Law Firm
Physical Health Strategy Group
Mortality Review Group
Locality / Service Governance
Groups
Equality and Diversity Group
Drugs and Therapeutics Committee
Clinical Effectiveness and
Policy Group
Health and Safety Committee
Clinical Cabinet
Transformation Programme
Board
Medical Staff Group
Profession- specific groups
such as Nursing
Workforce Council
Lorenzo Programme
Board / ICT Strategy Programme
Board
Local People
Key
CoG Group
BoD Committee
Operational
Reporting
Consulting / Liaising
(SR2) Committee structure from February 2016
ARA2016_master 140616.indd 34 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 35
Chair, NED, ED expertise and qualifications
Chair and NEDs
(SR3)
Experience and Skills Qualifications
Gary PageChair
• CEO Global Markets for ABNAMRO BANK NV (2006-08). Career in financial services from 1986
• Chair of Trustees for a school in East London for boys aged 11-16 with Social, Emotional and Behavioural Difficulties (2008-10)
• Chair of Trustees for the Hoffmann Foundation for Autism providing supported living and day services in North London for adults with Autism
• BA (Hons)
Marion Saunders • Non-Executive Director UIA Insurance Ltd• NMC Fitness to Practice Committee Member• IR and AAT Tribunals• CQC Specialist Adviser• Health and Social Care Consultancy• Former Independent Chair of Lewisham
Safeguarding Boards• Former Chair of Ealing PCT
• MSc HRD/OD• BA (Hons)• CQSW - registration with HCPC
Tim Newcomb 30 years in policing including:• 4yrs as Director of Intelligence –
managing covert operations• 2yrs as Divisional Commander for Eastern
Division - delivering mainstream community policing services
• 2yrs - Assistant Chief Constable in Essex Police
• Managed 2010 CSR Change Programme• Assistant Chief Constable in Suffolk
Constabulary 2012 to 2014• Hostage and Crisis Negotiator, including
Kidnap / Extortion training• Strategic Public Order and Firearms (Gold)
Commander Coach / Mentor
• Postgraduate Certificate in Business Excellence – Leeds University
• Diploma in applied Criminology and Policing – Cambridge University Mst Programme
• Level 5 Coaching Certificate
John Brierley • Formerly Director of own company• Formerly Executive Director of Norfolk
Learning Skills Council• Formerly Chief Executive of the Local Training
and Enterprise Council and City Treasurer of Norwich City Council
• Honorary Treasurer of local MIND
• Member of the Chartered Institute of Public Finance and Accountancy (CIPFA)
ARA2016_master 140616.indd 35 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201636
Brian Parrott • Former Director of Social Services and former Chair of small PCT
• Social Care (Adults and Children), Health and Local Government Consultancy
• Independent Chair, Safeguarding Adults Board – London Boroughs of Richmond and Tower Hamlets
• Former Co-Chair of Association of Directors of Social Services Associates Network
• Extensive experience of social services management and partnership working with NHS
• Certificate of Qualification in Social Work (currently registered)
Ian Brookman(from Dec 2015)
• Director of own accountancy and consultancy practice
• Chief Finance Officer – The Bell Foundation• Trustee and Chair of Audit Committee –
Ormiston Academy Trust• Formerly Finance Director – Ormiston Families• Formerly Managing Partner – regional
accountancy firm
• Fellow of the Institute of Chartered Accountants in England & Wales (ICAEW)
Tim Stevens(from Dec 2015)
• Diocesan Bishop of Leicester (1999 – 2015)• Previously Member of House of Lords with
Welfare Reform portfolio• Chair of Children’s Society (2004 and 2010)• Governor of De Montfort University
(2007 to 2010)• Former Chair of Leicester Faith Leaders’
Forum
• Cambridge MA• Oxford Dip Theol• Dip Mgt• Hon PhD Leicester University• Hon Phd De Montfort University
Dr. Jill Robinson (from Jan 2016)
• Currently Executive Dean for the Faculty of Health and Science and Professor of Healthcare Practice at University Campus Suffolk
• Formerly a Non Executive Director for an acute Trust
• Over 10 years senior leadership experience in health professional education and workforce development, stakeholder engagement, and quality improvement and assurance
• Successful track record of nationally funded research and publication in the fields of health professional education, practice and university governance
• PhD in Applied Educational Research • NMC Registered Mental Health Nurse
and Nurse Teacher• BABCP accredited Psychological
Therapist• Graduate Member of British
Psychological Society• Fellow of Higher Education Academy
Dr Peter Jeffreys(to 31 July 2015)
• Consultant Old Age Psychiatrist and former Medical Director of Harrow and Hillingdon Healthcare NHS Trust
• Former Lead Second Opinion Appointed Doctor for MHAC and CQC
• Former psychiatric advisor Parliamentary and Health Services Ombudsman
• Former member Mental Health Review Tribunals
• Chair Fitness to Practice Panels for GMC / MPTS and General Social Care Council
• Expert witness (mental capacity, unexpected death, homicide) recognised by High Court, Coroners and NHS England
ARA2016_master 140616.indd 36 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 37
Stuart Smith (to Feb 2016)
• Former director of business change programmes for Aviva and Norwich Union
• Over 20 years of change management and consulting experience in the UK and overseas
• Direction of complex change programmes• Delivery of UK wide property strategies• Direction of acquisition, merger, integration
and joint venture activity• Leading role in demutualisation and flotation
of Norwich Union• Partner in Stuart Smith Partners LLP, a
management consultancy organisation focused on complex change initiatives
• 35+ years in financial services as IT manager, management consultant and director of complex change programmes
Adrian Stott (to Oct 2015)
• Partner at investment bank Cazenove and managing director at JPMorgan Cazenove
• Governor of NSFT from February 2012 to October 2013
• Former trustee for a leading Christian charity• Trustee of the Mental Health Foundation• Lay member of the Board of the Faculty of
Public Health• Founder Trustee of MindEd Trust
• Cambridge University - BA (Hons) Securities Institute - Investment Analysis
CEO and Executive Directors (SR4)
Experience and Skills Qualifications
Michael Scott (Chief Executive)
• More than 30 years of experience across social care, the NHS and Department of Health, having worked in front line learning disability services, acute hospitals and commissioning organisations as well as mental health services
• Held a Chief Executive position for over 15 years
• Former chair of the NHS Confederation’s Community Health Services Forum
• BA Oxon• CSS
Julie Cave (Director of Finance / Deputy CEO from Dec 2015)
• 30 years’ experience in the NHS in acute hospitals, health authority and commissioning organisations as well as NSFT
• Held executive Director of Finance positions for 12 years
• Has delivered major transformational change, established new networks for health care and managed large-scale building projects to improve health care facilities
• BA (Hons)• Fellow of the Chartered Association
of Certified Accountants
Dr. Jane Sayer (Director of Nursing, Quality and Patient Safety)
• Extensive nursing leadership experience• Development of clinical career pathways• Research portfolio related to nursing workforce
• BA (Hons)• RMN• MSc• PhD
ARA2016_master 140616.indd 37 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201638
Debbie White (Director of Operations Norfolk and Waveney)
• Qualified as a Social Worker in 1995• Management of health and social care
services since 2002 including Locality Manager and Associate Director within NWMHFT
• Diploma in Social Work
Alison Armstrong (Director of Operations Suffolk)
• Previous commissioning roles and leadership of large scale transformation projects for both health and social care services in the London area
• Former Director of London-wide Programmes for mental health, offender health and substance misuse at NHS London
• Seconded to South West London and St George’s Mental Health NHS Trust and led a specialist services transformation project and taught a masters course on social policy
• RMN
Dr. Bohdan Solomka (Medical Director)
• Qualified as a doctor in 1988 and joined the Trust in October 1994 as Senior Registrar in Forensic Psychiatry
• Previously worked in Suffolk as a Consultant Forensic Psychiatrist from 1997 to 2007, then in Yarmouth and Waveney from 2007 to 2014 and the Women's Medium Secure Service from February 2014
• Lead Clinician in the Secure Service since January 2013
• Medical Director of the Trust in January 2015
• Member of the Royal• College of Psychiatrists
Leigh Howlett (Director of Strategy and Resources)
• Two previous director posts• Worked at Board level for 13 years• 30 years NHS experience across all areas of
health care provision and delivery
• Diploma in management studies• Significant professional
development in all areas of responsibility
Andrew Hopkins (Director of Finance to Sep 2015)
• Former Director of Finance and information at Huntingdonshire PCT
• Former consultant and auditor at KPMG• Previous chair of Eastern Branch of
Healthcare Financial Management Association
• Member of the Chartered• Institute of Public Finance and
Accountancy (CIPFA)
John Doyle (Interim Director of Finance from Aug 2015 to Nov 2015)
• 18 years experience as finance director 32 years NHS experience including 16 years in mental health
• Played significant role in organisations facing administration
• Fellow of the Chartered Institute of Management Accountants (CIMA)
The Nomination and Remuneration and Terms of Service Committee keep under review the balance and completeness of the skill and experience set for the board. Person specifications take into account the current and future Trust needs.
ARA2016_master 140616.indd 38 14/06/2016 11:10
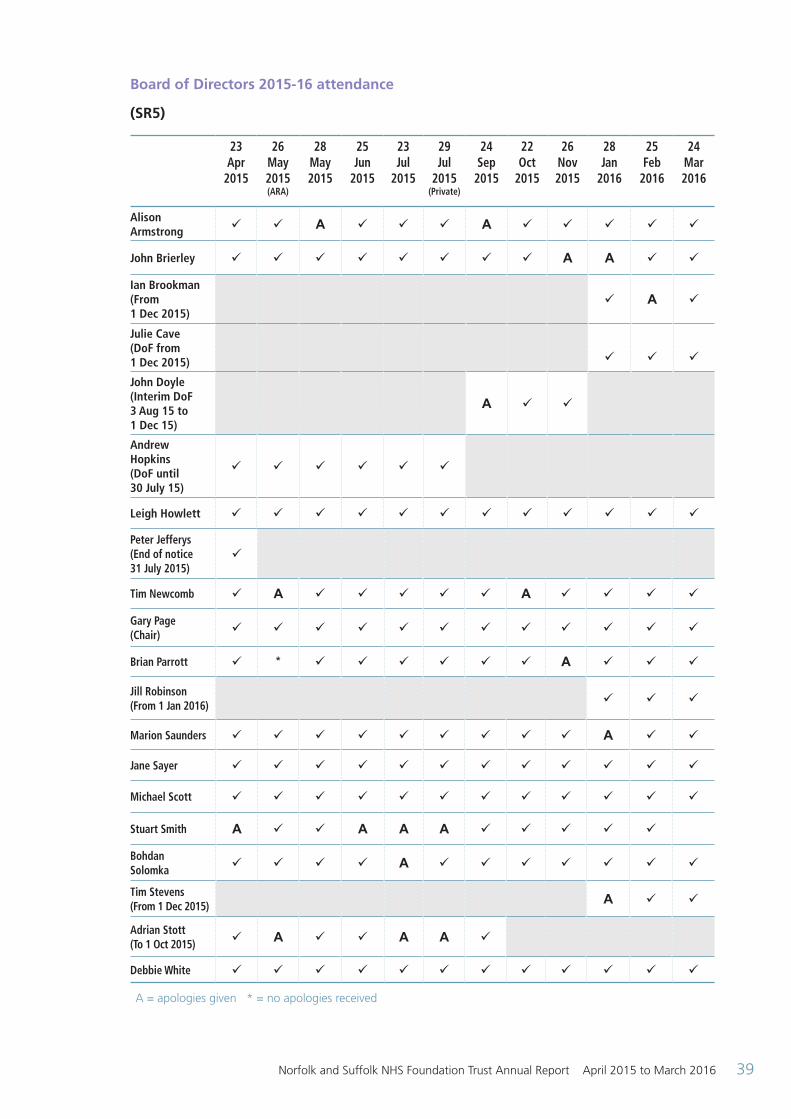
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 39
Board of Directors 2015-16 attendance
(SR5)
23 Apr
2015
26 May 2015 (ARA)
28 May 2015
25 Jun
2015
23 Jul
2015
29 Jul
2015 (Private)
24 Sep
2015
22 Oct
2015
26 Nov2015
28 Jan
2016
25 Feb
2016
24 Mar2016
Alison Armstrong ü ü A ü ü ü A ü ü ü ü ü
John Brierley ü ü ü ü ü ü ü ü A A ü ü
Ian Brookman (From 1 Dec 2015)
ü A ü
Julie Cave (DoF from 1 Dec 2015) ü ü ü
John Doyle (Interim DoF 3 Aug 15 to 1 Dec 15)
A ü ü
Andrew Hopkins (DoF until 30 July 15)
ü ü ü ü ü ü
Leigh Howlett ü ü ü ü ü ü ü ü ü ü ü ü
Peter Jefferys(End of notice 31 July 2015)
ü
Tim Newcomb ü A ü ü ü ü ü A ü ü ü ü
Gary Page(Chair) ü ü ü ü ü ü ü ü ü ü ü ü
Brian Parrott ü * ü ü ü ü ü ü A ü ü ü
Jill Robinson(From 1 Jan 2016) ü ü ü
Marion Saunders ü ü ü ü ü ü ü ü ü A ü ü
Jane Sayer ü ü ü ü ü ü ü ü ü ü ü ü
Michael Scott ü ü ü ü ü ü ü ü ü ü ü ü
Stuart Smith A ü ü A A A ü ü ü ü ü
Bohdan Solomka ü ü ü ü A ü ü ü ü ü ü ü
Tim Stevens(From 1 Dec 2015) A ü ü
Adrian Stott (To 1 Oct 2015) ü A ü ü A A ü
Debbie White ü ü ü ü ü ü ü ü ü ü ü ü
A = apologies given * = no apologies received
ARA2016_master 140616.indd 39 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201640
The Board of Directors meets ten times a year in public in Ipswich and Norwich. A small number of items of business are confidential or commercially sensitive and are dealt with in private. Governors receive copies of the private board papers. Details of meetings and board papers are available at www.nsft.nhs.uk.
The Board of Directors is satisfied that the non-executive directors who served on the Board for the period under review were independent. The Chair had no other significant commitments. A summary of the background of each of the directors along with their expertise is shown in the Directors’ Report.
Board committees report on their work to the next available board and include a review of performance against their terms of reference annually. Governors attend board committees as observers and provide feedback to the committee chair and to the Chair of the Board of Directors.
The executive directors are appraised by the CEO who reports to the remuneration committee. The CEO is appraised by the Chair.
The NEDs are appraised by the Chair and the Chair by the Senior Independent Director (SID). This is reported via the nominations committee to the Council of Governors.
The Work of the Council of Governors
The Health and Social Care Act (2012) clarified the general duties of the Council of Governors:
S.151 (4) “The general duties of the council of governors are:
(a) To hold the non-executive directors individually and collectively to account for the performance of the board of directors, and
(b) To represent the interests of the members of the corporation as a whole and the interests of the public.”
The main duties include:
• To appoint or remove the Chair and other non-executive directors
• To approve the appointment of the Chief Executive
• To decide the remuneration and allowances, and other terms and conditions of office, of the non-executive directors (delegated to the nominations committee)
• To appoint or remove the Trust’s auditor
Elections are held once a year with nominations opening in the autumn and the results being declared in December or January for governors to take up their seats from 1 February each year.
Governors canvass the opinions of Trust members and the wider public (including, for partner governors, the body they represent) in a wide range of ways. They use informal and formal networks, attend community and Trust events and take account of service user and carer experience. They feed these insights back to the Board of Directors through the Council of Governors’ issues log, by raising questions with directors and by attending the Board of Directors’ meeting. Governors use their insights to comment on the Trust’s forward plan, objectives and strategic priorities.
A summary of the business carried out by the Council of Governors is shown below.
The Council of Governors met on the following dates in 2015-16. At each meeting, governors present issues that they wish to highlight (often based on feedback from members and the wider public) and the Trust undertakes to respond to these issues as fully as possible. The agendas include other standing items, including the reports of the subgroups. In addition to these standing items the following business was conducted. A full set of papers for each meeting is available at www.nsft.nhs.uk.
ARA2016_master 140616.indd 40 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 41
Date of meeting Business covered
2 April 2015 NED recruitmentMembership strategyStrategic objectivesQuality improvement
2 July 2015 Workforce moraleService user and carer engagementFinancial recovery planQuality improvement
1 October 2015 Constitutional changesNED term extension
30 October 2015 Appointment of NEDs
7 January 2016 Joint working agreement between CoG and Board of DirectorsUpdates to Chair role profile and governor core documents (role descriptions and code of conduct)Financial recovery planQuality improvementCoG self-evaluation
18 February 2016 Re-appointment of the Chair Approval of substitute governor
Note: The meetings held on 30 October 2015 and 18 February 2016 were short business meetings with most of the day being given over to member engagement events.
There were also a number of developmental sessions including: representing the interests of members and the wider public, the work of the Trust, finance for governors, and holding to account skills.
Although the formal duties of the governors are discharged at full Council of Governor meetings, much work takes place in the subgroups.
The Planning and Performance Subgroup which meets six times a year has a particular focus on holding the non-executive directors to account and is normally attended by at least two non-executives. The Membership and Communications Subgroup also meets six times a year and has an overview on member recruitment and engagement. It also reviews the election publication materials. The Education Subgroup oversees training and development for governors. In addition, there is an annual Code of Conduct meeting that updates the Code and the role descriptions for governors and the lead governor. Governors also attended a wide range of community events across the two counties in 2015-16.
Summary of changes to the constitution approved by the Council of Governors in 2015-16
1. Amending the Board of Directors’ membership 2. Changing the arrangements for the election of substitute governors (when a governor stands down mid-term and the Council of Governors exercises its discretion to appoint the next governor from the election result list) 3. Changing the name ‘Board of Governors’ to ‘Council of Governors’ and the post title, ‘Trust Secretary’ to ‘Company Secretary’
Register of interests
All governors are required to declare any interests on the register at the time of their election or appointment and to keep this up-to-date. The full register is taken as an item at a public meeting once a year and is available for inspection by contacting Robert Nesbitt, Company Secretary at NSFT, Hellesdon Hospital, Drayton High Road, Norwich, NR6 5BE. Alternatively call: 01603 421 421 or email: [email protected].
(SR6)
ARA2016_master 140616.indd 41 14/06/2016 11:10
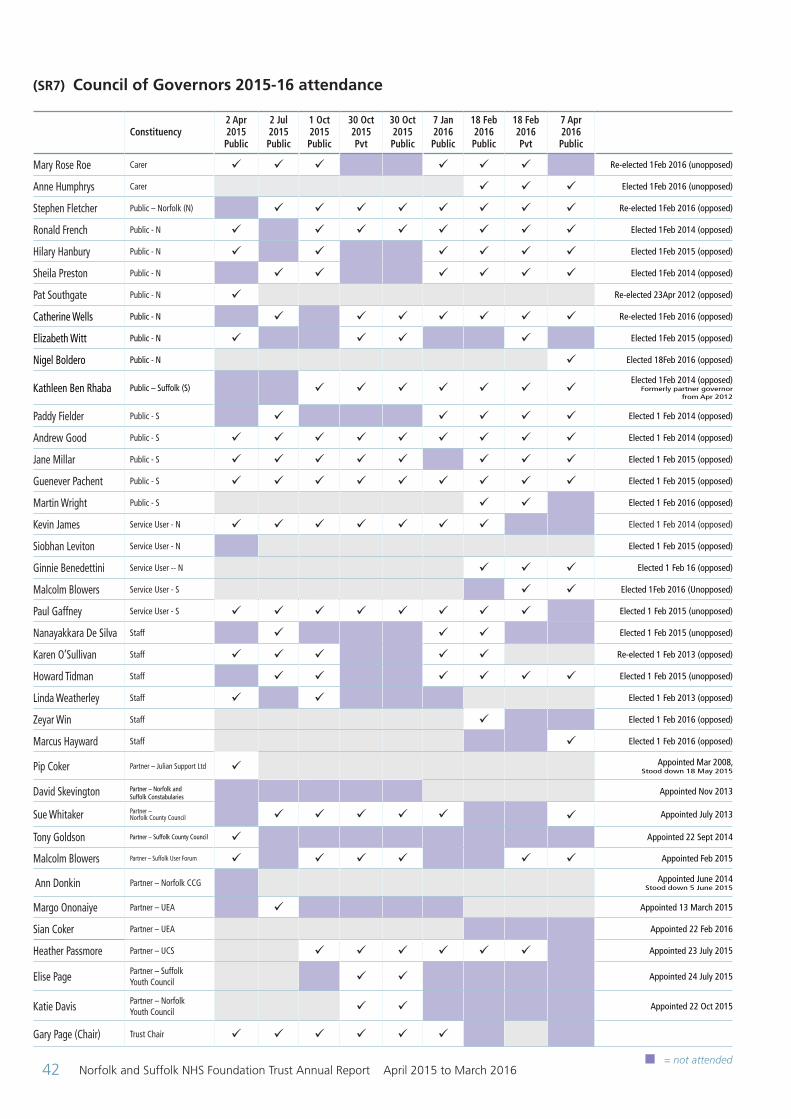
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201642
(SR7) Council of Governors 2015-16 attendance
Constituency2 Apr 2015 Public
2 Jul 2015 Public
1 Oct 2015 Public
30 Oct 2015 Pvt
30 Oct 2015 Public
7 Jan 2016 Public
18 Feb 2016 Public
18 Feb 2016 Pvt
7 Apr 2016 Public
Mary Rose Roe Carer ü ü ü ü ü ü Re-elected 1Feb 2016 (unopposed)
Anne Humphrys Carer ü ü ü Elected 1Feb 2016 (unopposed)
Stephen Fletcher Public – Norfolk (N) ü ü ü ü ü ü ü ü Re-elected 1Feb 2016 (opposed)
Ronald French Public - N ü ü ü ü ü ü ü ü Elected 1Feb 2014 (opposed)
Hilary Hanbury Public - N ü ü ü ü ü ü Elected 1Feb 2015 (opposed)
Sheila Preston Public - N ü ü ü ü ü ü Elected 1Feb 2014 (opposed)
Pat Southgate Public - N ü Re-elected 23Apr 2012 (opposed)
Catherine Wells Public - N ü ü ü ü ü ü ü Re-elected 1Feb 2016 (opposed)
Elizabeth Witt Public - N ü ü ü ü Elected 1Feb 2015 (opposed)
Nigel Boldero Public - N ü Elected 18Feb 2016 (opposed)
Kathleen Ben Rhaba Public – Suffolk (S) ü ü ü ü ü ü üElected 1Feb 2014 (opposed)
Formerly partner governor from Apr 2012
Paddy Fielder Public - S ü ü ü ü ü Elected 1 Feb 2014 (opposed)
Andrew Good Public - S ü ü ü ü ü ü ü ü ü Elected 1 Feb 2014 (opposed)
Jane Millar Public - S ü ü ü ü ü ü ü ü Elected 1 Feb 2015 (opposed)
Guenever Pachent Public - S ü ü ü ü ü ü ü ü ü Elected 1 Feb 2015 (opposed)
Martin Wright Public - S ü ü Elected 1 Feb 2016 (opposed)
Kevin James Service User - N ü ü ü ü ü ü ü Elected 1 Feb 2014 (opposed)
Siobhan Leviton Service User - N Elected 1 Feb 2015 (opposed)
Ginnie Benedettini Service User -- N ü ü ü Elected 1 Feb 16 (opposed)
Malcolm Blowers Service User - S ü ü Elected 1Feb 2016 (Unopposed)
Paul Gaffney Service User - S ü ü ü ü ü ü ü ü Elected 1 Feb 2015 (unopposed)
Nanayakkara De Silva Staff ü ü ü Elected 1 Feb 2015 (unopposed)
Karen O’Sullivan Staff ü ü ü ü ü Re-elected 1 Feb 2013 (opposed)
Howard Tidman Staff ü ü ü ü ü ü Elected 1 Feb 2015 (unopposed)
Linda Weatherley Staff ü ü Elected 1 Feb 2013 (opposed)
Zeyar Win Staff ü Elected 1 Feb 2016 (opposed)
Marcus Hayward Staff ü Elected 1 Feb 2016 (opposed)
Pip Coker Partner – Julian Support Ltd ü Appointed Mar 2008, Stood down 18 May 2015
David Skevington Partner – Norfolk and Suffolk Constabularies
Appointed Nov 2013
Sue Whitaker Partner – Norfolk County Council ü ü ü ü ü ü Appointed July 2013
Tony Goldson Partner – Suffolk County Council ü Appointed 22 Sept 2014
Malcolm Blowers Partner – Suffolk User Forum ü ü ü ü ü ü Appointed Feb 2015
Ann Donkin Partner – Norfolk CCG Appointed June 2014 Stood down 5 June 2015
Margo Ononaiye Partner – UEA ü Appointed 13 March 2015
Sian Coker Partner – UEA Appointed 22 Feb 2016
Heather Passmore Partner – UCS ü ü ü ü ü ü Appointed 23 July 2015
Elise Page Partner – Suffolk Youth Council ü ü Appointed 24 July 2015
Katie Davis Partner – Norfolk Youth Council ü ü Appointed 22 Oct 2015
Gary Page (Chair) Trust Chair ü ü ü ü ü ü
n = not attended
ARA2016_master 140616.indd 42 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 43
The Work of the Audit and Risk Committee
The Trust has a well-established Audit and Risk Committee which fulfi ls the responsibility of an audit committee on behalf of the Trust. The three members of the Committee are all non- executive directors. The Committee is chaired by John Brierley who is a qualifi ed accountant. The other members of the Committee, in the year ended 31 March 2016, were Marion Saunders (the senior independent director), Stuart Smith (from 1 June 2015 to 29 February 2016), Peter Jefferys (to 30 April 2015), Ian Brookman (with effect from 1 December 2015), Jill Robinson (with effect from 1 January 2016).
During the year, the Committee met on seven occasions. Governors were invited to attend the June meeting of the Committee when Annual Reports for the previous year and Annual Plans for the current year were considered and discussed. Governors could attend other meetings by request. The Committee has been observed by one of our governors as part of the monitoring arrangements approved by the Board of Directors.
Two members must be present for the meeting to be quorate. All meetings achieved this status during 2015-16.
The Trust has an Internal Audit service which is provided by the West Midlands Ambulance Trust. In 2015-16 the internal audit plan utilised 360 days which was considered to be sufficient by the Director of Finance and service provider to deliver an adequate service to the Trust. Internal Audit prepare and deliver a three-year, risk based, audit strategy which is translated into an internal audit plan each year. The service works in accordance with the Internal Audit Charter which incorporates public sector internal audit standards. Each year the Head of Internal Audit prepares a statement on the effectiveness of the systems of internal control. This is based around six domains of work. The internal audit strategies and plans are approved by the Audit and Risk Committee which also monitors progress and performance throughout the year. Any matters arising are reported to the Board of Directors by the Chair of the Committee. It is the Trust’s intention to subject internal audit to competitive bids during 2016-17. The Committee has assessed that the Trust received a reasonable and appropriate level of service during 2015-16.
The external audit of the Trust’s Annual Accounts and Annual Report, including the Quality Account is provided by KPMG, following a competitive tendering process in 2014. The contract term is for three years with an option to extend for a further two years. The contract value for 2015-16 was £64,400. During 2015-16 no non-audit services were provided by KPMG.
The Audit and Risk Committee worked throughout the year in accordance with its Terms of Reference and best practice guidance. The Terms of Reference was developed in accordance with Monitor’s Code of Governance for Audit Committees and Auditors. The Committee has a work programme for each fi nancial year. This programme covers:
• Annual Report and Accounts
• Governance, risk management and internal control
• Counter fraud work
• Internal audit work
• External audit
• Other assurance functions and work
• Management of the committee’s work
In discharging its responsibilities in respect of the Annual Report and Accounts, the Committee has reviewed:
• The Trust’s accounting policies, with particular reference to the adequacy and appropriateness of provisions
• Accounting for property, plant and equipment. The Committee has ensured that independent, professional advice has been obtained in valuing the Trust’s property portfolio
• The recognition of the Trust’s revenue by overseeing contracts and management processes designed to ensure that all revenue is properly recorded and is accounted for in accordance with the Trust’s accounting policies
• Management do not override the system of individual controls which are designed to deliver good governance and to ensure that good internal control practices are adopted or that weaknesses are identified and reported to the Board of Directors
ARA2016_master 140616.indd 43 14/06/2016 11:10
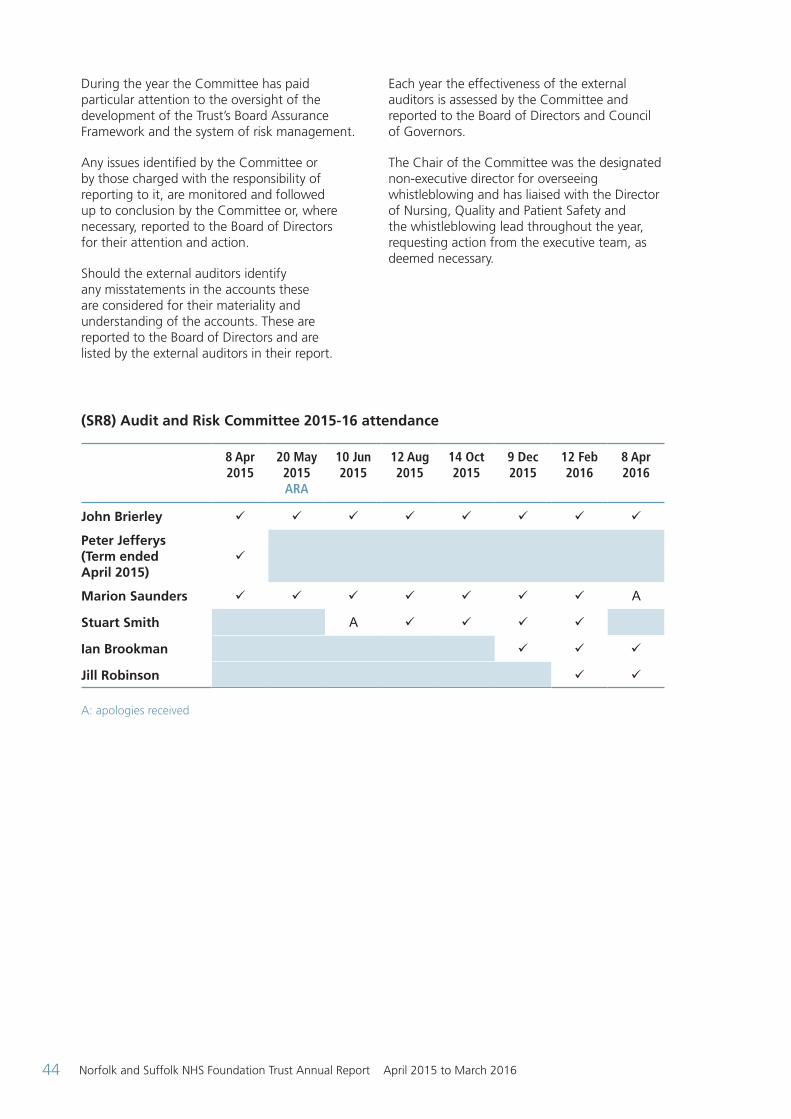
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201644
During the year the Committee has paid particular attention to the oversight of the development of the Trust’s Board Assurance Framework and the system of risk management.
Any issues identifi ed by the Committee or by those charged with the responsibility of reporting to it, are monitored and followed up to conclusion by the Committee or, where necessary, reported to the Board of Directors for their attention and action.
Should the external auditors identify any misstatements in the accounts these are considered for their materiality and understanding of the accounts. These are reported to the Board of Directors and are listed by the external auditors in their report.
(SR8) Audit and Risk Committee 2015-16 attendance
8 Apr 2015
20 May 2015ARA
10 Jun 2015
12 Aug 2015
14 Oct 2015
9 Dec 2015
12 Feb 2016
8 Apr2016
John Brierley ü ü ü ü ü ü ü ü
Peter Jefferys (Term ended April 2015)
ü
Marion Saunders ü ü ü ü ü ü ü A
Stuart Smith A ü ü ü ü
Ian Brookman ü ü ü
Jill Robinson ü ü
A: apologies received
Each year the effectiveness of the external auditors is assessed by the Committee and reported to the Board of Directors and Council of Governors.
The Chair of the Committee was the designated non-executive director for overseeing whistleblowing and has liaised with the Director of Nursing, Quality and Patient Safety and the whistleblowing lead throughout the year, requesting action from the executive team, as deemed necessary.
ARA2016_master 140616.indd 44 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 45
Membership strategy summary 2015-16
Members must be over 11 years of age and governors must be 16 or over.
We have consulted on and created the following membership constituencies:
• Public Constituency
– Norfolk
– Suffolk
• Service User and Family Carer Constituency
Anyone who has used our services within the last three years is eligible to become a service user member.
People who identify themselves as family carers of people who have been supported by our services are eligible to join as family carer members. The term family carer member is used to distinguish this group from paid carers. Family carers do not have to be related to the person they care for.
The constituency classes are:
• Service user (Norfolk)
• Service user (Suffolk)
• Carer (Norfolk)
• Carer (Suffolk)
• Staff
Permanent contracted staff are automatically granted membership (“opted-in”) although it is easy for any staff member to “opt out”, should they wish, by writing to the Company Secretary.
Members can only be a member of one constituency at a time. If they become ineligible to be a member of one constituency (e.g. they leave NSFT employment), they can opt to become a member of another constituency (e.g. a Public Member).
Eligible staff members are not permitted to join another constituency.
The total number of members is shown in the Membership Report. Membership has remained stable at around 13,000 (excluding staff) and our focus is on maintaining this level and building meaningful engagement. In common with other foundation trusts our membership has under-presentation of younger people and men and in 2016-17 we will continue to attempt to address this through targeted recruitment efforts. Representation of BME members has made good progress over recent years.
A full-time membership and engagement officer is in post and over the course of 2015-16 this has allowed us to have a presence at many community events across the two counties. These have included Ipswich Multi-cultural Day, the Ipswich Indian Mela, Transgender Memorial Day and a wide range of wellbeing events.
This year the Council of Governors has hosted successful member events on the topics of children and young people’s mental health and dementia.
Members who wish to contact the Trust’s governors may do so by emailing: [email protected] or by writing to Membership Office, NSFT, Hellesdon Hospital, Drayton High Road, Norwich NR6 5BE.
We strongly encourage members to receive information via email – about 90% of new members do so.
ARA2016_master 140616.indd 45 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201646
(SR9) Membership report 2015-16
Membership 2015-16 Population
Public constituency
As at start (1 April 2015) 11,551
New Members 222
Members leaving 429
At year end (31 March 2016) 11,344 1,497,295
Staff constituency
As at start (1 April 2015) 3,832
New Members 597
Members leaving 608
At year end (31 March 2016) 3,821
Patient constituency
As at start (1 April 2015) 1,491
New Members 99
Members leaving 66
At year end (31 March 2016) 1,524
Public constituency Number of members Population
Age (years)
0 - 16 4 109,318
17 - 21 80 79,379
22+ 9,523 1,308,598
Ethnicity
White 10,540 1,441,105
Mixed 79 19,913
Asian 143 22,988
Black 115 9,501
Other 24 3,788
Socio-economic groupings
AB 900 214,711
C1 6,333 325,775
C2 2,524 198,371
DE 1,421 380,116
Gender
Male 4,063 744,339
Female 7,169 752,956
Patient constituency Number of members
Age (years)
0 - 16 2
17 - 21 15
22+ 1,323
ARA2016_master 140616.indd 46 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 47
Staff demographic data
Analysis of average staff numbers
An analysis of average staff numbers employed during 2015-16 shows the following breakdown:
(SR10)
Staff Group Permanent Other* Total
Medical and dental 106.24 53.85 160.09
Administration and estates 826.97 100.44 927.41
Healthcare assistants and other support staff 801.07 44.6 845.67
Nursing, midwifery and health visiting staff 1090.81 41.67 1132.48
Scientific, therapeutic and technical staff 366.08 30.1 396.18
Social care staff 8.5 0 8.5
Total average numbers 3199.67 270.66 3470.33
* ’other staff’ include short-term contract staff and locum staff
Breakdown of male / female at year end
At the end of March 2016, 71.2% of the Trust’s total workforce was female. This decreases to 43.6% at senior management level, but rises to 66.7% at director level.
(SR11)
Staff Group Female MaleGrand
Total
Director 4 2 6
Other senior managers 17 22 39
Employees 2768 1106 3874
Total 2789 1130 3919
Sickness absence data
Annualised sickness absence data within the Trust shows a downward trend during 2015-16 to the lowest rate since the merger in 2012.
The largest known reason for sickness absence is due to ‘Anxiety / stress / depression / other psychiatric illnesses’, accounting for 26.8% of all absence. The top five reasons for absence are:
1. Anxiety / stress / depression / other psychiatric illnesses
2. Injury, fracture
3. Gastrointestinal problems
4. Other musculoskeletal problems
5. Cold, Cough, Flu - Influenza
Episodes of long-term absence (defined as being absence episodes of 28 days or more) decreased by 1.3% to 452 episodes when compared with 2014-15. Episodes of short-term absence (defined as being absence episodes of fewer than 28 days) decreased by 6.8% to 5,775 episodes when compared with 2014-15.
Staff policies and actions applied during the financial year
Action on working with disabled employees
In 2015-16 the Trust has been assessed and been re-awarded with the Government’s ‘Two Ticks - positive about disabled people’ symbol. The assessment confirms the Trust’s continued commitment to:
• Interview all disabled applicants who meet the minimum criteria for a job vacancy and to consider them on their abilities
• Discuss with disabled employees, at any time but at least once a year, what can be done to make sure they can develop and use their abilities
• Make every effort when employees become disabled to ensure they stay in employment
• Take action to ensure that all employees develop the appropriate level of disability awareness needed to make these commitments work
ARA2016_master 140616.indd 47 14/06/2016 11:10
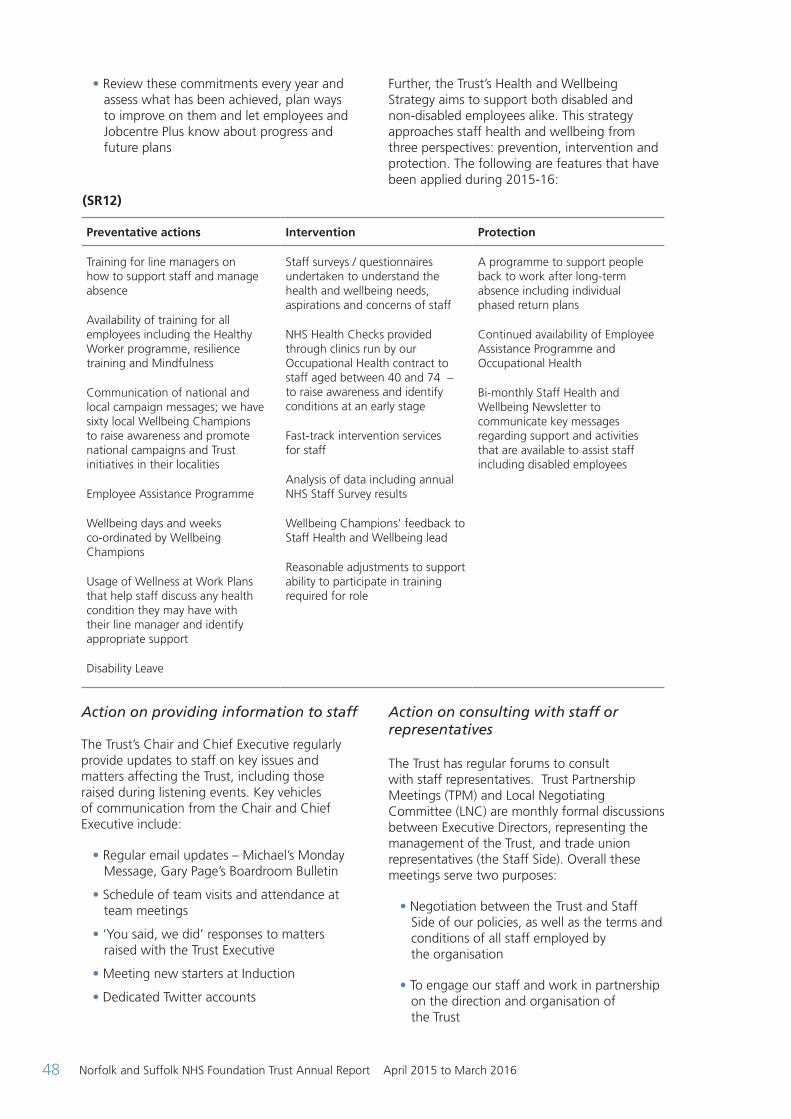
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201648
Action on providing information to staff The Trust’s Chair and Chief Executive regularly provide updates to staff on key issues and matters affecting the Trust, including those raised during listening events. Key vehicles of communication from the Chair and Chief Executive include:
• Regular email updates – Michael’s Monday Message, Gary Page’s Boardroom Bulletin
• Schedule of team visits and attendance at team meetings
• ‘You said, we did’ responses to matters raised with the Trust Executive
• Meeting new starters at Induction
• Dedicated Twitter accounts
Action on consulting with staff or representatives
The Trust has regular forums to consult with staff representatives. Trust Partnership Meetings (TPM) and Local Negotiating Committee (LNC) are monthly formal discussions between Executive Directors, representing the management of the Trust, and trade union representatives (the Staff Side). Overall these meetings serve two purposes:
• Negotiation between the Trust and Staff Side of our policies, as well as the terms and conditions of all staff employed by the organisation
• To engage our staff and work in partnership on the direction and organisation of the Trust
• Review these commitments every year and assess what has been achieved, plan ways to improve on them and let employees and Jobcentre Plus know about progress and future plans
Further, the Trust’s Health and Wellbeing Strategy aims to support both disabled and non-disabled employees alike. This strategy approaches staff health and wellbeing from three perspectives: prevention, intervention and protection. The following are features that have been applied during 2015-16:
Preventative actions Intervention Protection
Training for line managers on how to support staff and manage absence
Availability of training for all employees including the Healthy Worker programme, resilience training and Mindfulness
Communication of national and local campaign messages; we have sixty local Wellbeing Champions to raise awareness and promote national campaigns and Trust initiatives in their localities
Employee Assistance Programme
Wellbeing days and weeks co-ordinated by Wellbeing Champions
Usage of Wellness at Work Plans that help staff discuss any health condition they may have with their line manager and identify appropriate support
Disability Leave
Staff surveys / questionnaires undertaken to understand the health and wellbeing needs, aspirations and concerns of staff
NHS Health Checks provided through clinics run by our Occupational Health contract to staff aged between 40 and 74 – to raise awareness and identify conditions at an early stage
Fast-track intervention services for staff
Analysis of data including annual NHS Staff Survey results
Wellbeing Champions’ feedback to Staff Health and Wellbeing lead
Reasonable adjustments to support ability to participate in training required for role
A programme to support people back to work after long-term absence including individual phased return plans
Continued availability of Employee Assistance Programme and Occupational Health
Bi-monthly Staff Health and Wellbeing Newsletter to communicate key messages regarding support and activities that are available to assist staff including disabled employees
(SR12)
ARA2016_master 140616.indd 48 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 49
During 2015-16, TPM has ratified, amongst others, the following policies:
• Exit Interviews
• Medical Appraisal (Revalidation)
• Overpayment and Underpayment of Salary
• Long Service Award
• Engagement and Use of Temporary Workers
• Rostering (Clinical Teams)
• Retirement
• Long Service Award
Actions taken to encourage the involvement of employees in the Trust’s performance
During the financial year, the Trust held a series of events to encourage staff to become more aware of our overall financial performance. Staff were encouraged to submit ideas and plans to improve spending within the Trust to help meet Cost Improvement Plan targets. Many of those ideas are now being taken forward.
Internal performance review group meetings, chaired by the Director of Finance, are held monthly and encourage localities and staff to take responsibility for their performance.
Performance can be monitored using the Trust business intelligence system (Abacus). Abacus enables teams to examine their performance on a monthly basis against Monitor targets, check waiting lists and keep up to date with reviews and contacts. Performance is reported to localities on a monthly basis via an Integrated Performance Report.
Providing information relating to health and safety performance and occupational health
All localities have use of Datix dashboard, giving them up to the minute charts on incident reporting trends.
Work with Safer Care wards on Hammerton Court has produced regular data on the management and controls involved in issues such as patient falls and violence and aggression. This project has involved service users and carers in patient safety improvement.
On site health and safety and security inspections have taken place on 58 sites over the year with staff being offered the opportunity to talk with the Health and Safety Lead, Local Security Management Specialist and Union representatives on site.
All inpatient units had ligature audit reviews which were shared with the clinical team leads to discuss with staff. In addition, a bi-monthly patient safety newsletter has been produced by the Patient Safety Practitioner.
Safety folders were introduced to ensure staff had a central point of reference for inspection outcomes and the ligature control plans.
In terms of committees and meetings, the Health and Safety Committee are scheduled to meet three times a year, and staff and union representatives are asked to share information from attendance. The Trust’s Health and Safety Lead also attends the Trust’s the Wellbeing Group.
Providing information relating to countering fraud and corruption
A key aim of the work of the Trust’s Counter Fraud service over the course of 2015-16 has been to raise awareness of fraud and corruption.
The objective was to create a culture where staff feel they can readily raise their concerns without fear of victimisation, and that where this is necessary, they are clear on how to do this.
The following action has been delivered in relation to providing information relating to countering fraud and corruption:
• An e-learning module which is at 93% Trust compliance rate
• A dedicated page on the staff intranet
• A newsletter was issued in July and September 2015
• A survey to assess levels of fraud awareness and knowledge, and to identify improvements to the Counter Fraud service
ARA2016_master 140616.indd 49 14/06/2016 11:10
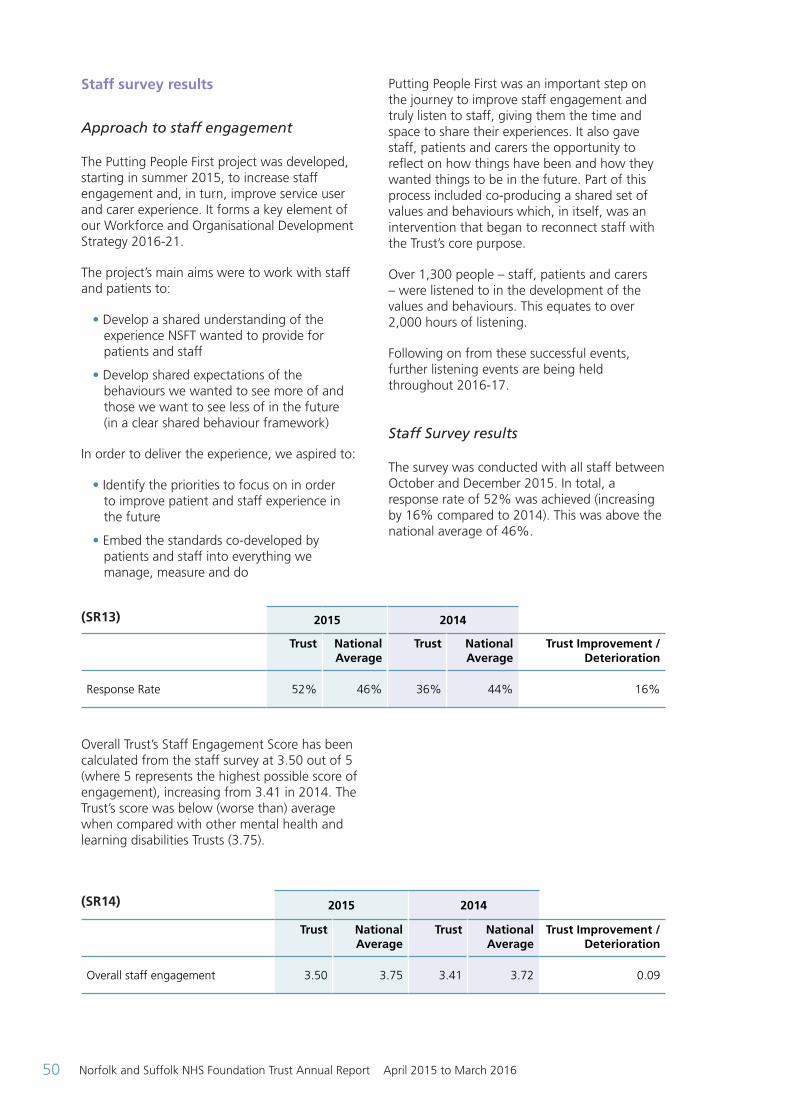
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201650
Staff survey results
Approach to staff engagement
The Putting People First project was developed, starting in summer 2015, to increase staff engagement and, in turn, improve service user and carer experience. It forms a key element of our Workforce and Organisational Development Strategy 2016-21.
The project’s main aims were to work with staff and patients to:
• Develop a shared understanding of the experience NSFT wanted to provide for patients and staff
• Develop shared expectations of the behaviours we wanted to see more of and those we want to see less of in the future (in a clear shared behaviour framework)
In order to deliver the experience, we aspired to:
• Identify the priorities to focus on in order to improve patient and staff experience in the future
• Embed the standards co-developed by patients and staff into everything we manage, measure and do
Overall Trust’s Staff Engagement Score has been calculated from the staff survey at 3.50 out of 5 (where 5 represents the highest possible score of engagement), increasing from 3.41 in 2014. The Trust’s score was below (worse than) average when compared with other mental health and learning disabilities Trusts (3.75).
Putting People First was an important step on the journey to improve staff engagement and truly listen to staff, giving them the time and space to share their experiences. It also gave staff, patients and carers the opportunity to reflect on how things have been and how they wanted things to be in the future. Part of this process included co-producing a shared set of values and behaviours which, in itself, was an intervention that began to reconnect staff with the Trust’s core purpose.
Over 1,300 people – staff, patients and carers – were listened to in the development of the values and behaviours. This equates to over 2,000 hours of listening.
Following on from these successful events, further listening events are being held throughout 2016-17.
Staff Survey results
The survey was conducted with all staff between October and December 2015. In total, a response rate of 52% was achieved (increasing by 16% compared to 2014). This was above the national average of 46%.
(SR13) 2015 2014
Trust National Average
Trust National Average
Trust Improvement /Deterioration
Response Rate 52% 46% 36% 44% 16%
(SR14) 2015 2014
Trust National Average
Trust National Average
Trust Improvement /Deterioration
Overall staff engagement 3.50 3.75 3.41 3.72 0.09
ARA2016_master 140616.indd 50 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 51
Out of 22 key findings that are directly comparable with the 2014 survey, seven of these had a statistically significant positive change. The Trust had no key scores that had a statistically significant negative change. The seven key findings with the statistically significant positive changes were:
• KF11. % Appraised in the last 12 months
• *KF17. % Suffering work related stress in the last 12 months
• *KF18. % Feeling pressure in the last 3 months to attend work when feeling unwell
• *KF28. % Witnessing potentially harmful errors, near misses or incidents in the last month
• KF1. Staff recommendation of the organisation has a place to work or receive treatment
• KF4. Staff motivation at work
• KF32. Effective use of patient / service user feedback
The Trust’s staff survey results benchmarked against other mental health and learning disabilities Trusts shows areas that the Trust compares most and least favourably.
The Trust only had one key finding that was ranked above (better than) average (KF24. % Reporting most recent experience of violence), while 26 of the 32 were ranked as being below (worse than) average.
The Trust had eight key findings which were ranked as being the lowest national scores attained for mental health and learning disability Trusts:
• KF1. Staff recommendation of the organisation as a place to work or receive treatment
• KF2. Staff satisfaction with the quality of work and care they are able to deliver
• KF5. Recognition and value of staff by managers and the organisation
• KF10. Support from immediate managers
• KF14. Staff satisfaction with resourcing and support
• KF3. Percentage of staff agreeing that their role makes a difference to patients / service users
• KF7. Percentage of staff able to contribute towards improvements at work
• KF11. Percentage of staff appraised in last 12 months
ARA2016_master 140616.indd 51 14/06/2016 11:10
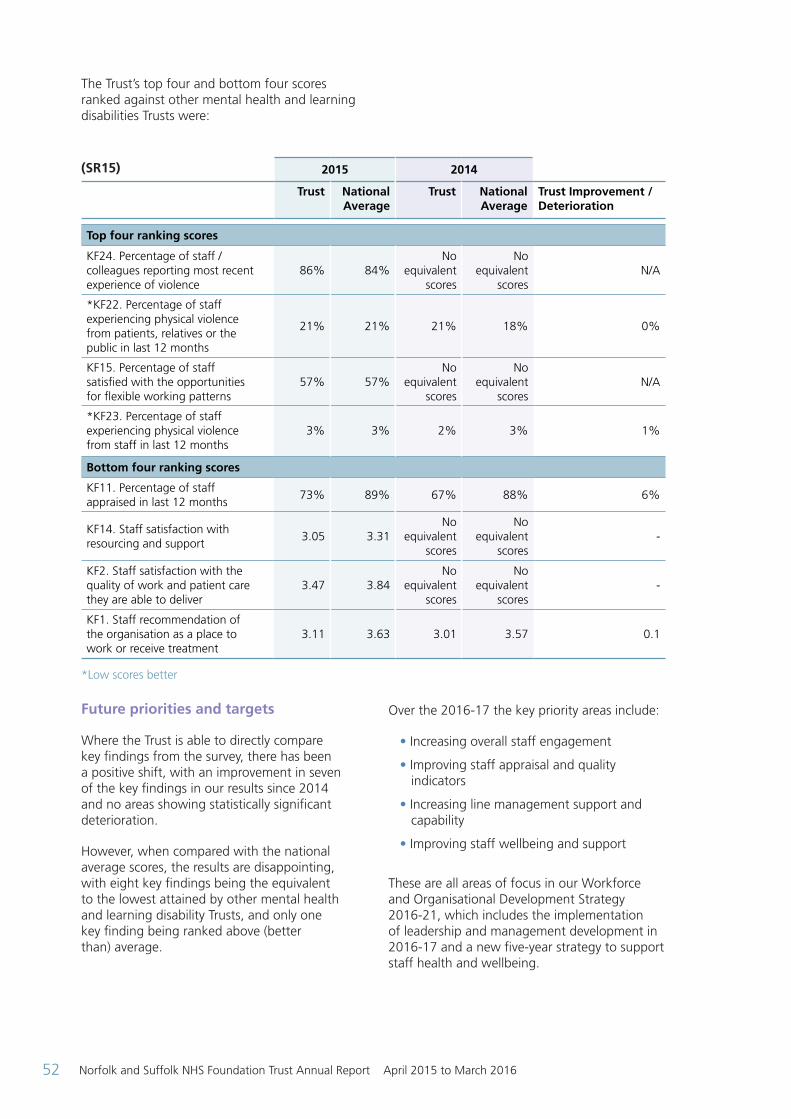
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201652
The Trust’s top four and bottom four scores ranked against other mental health and learning disabilities Trusts were:
(SR15) 2015 2014
Trust National Average
Trust National Average
Trust Improvement /Deterioration
Top four ranking scores
KF24. Percentage of staff / colleagues reporting most recent experience of violence
86% 84%No
equivalent scores
No equivalent
scores N/A
*KF22. Percentage of staff experiencing physical violence from patients, relatives or the public in last 12 months
21% 21% 21% 18% 0%
KF15. Percentage of staff satisfied with the opportunities for flexible working patterns
57% 57%No
equivalent scores
No equivalent
scores N/A
*KF23. Percentage of staff experiencing physical violence from staff in last 12 months
3% 3% 2% 3% 1%
Bottom four ranking scores
KF11. Percentage of staff appraised in last 12 months
73% 89% 67% 88% 6%
KF14. Staff satisfaction with resourcing and support
3.05 3.31No
equivalent scores
No equivalent
scores -
KF2. Staff satisfaction with the quality of work and patient care they are able to deliver
3.47 3.84No
equivalent scores
No equivalent
scores -
KF1. Staff recommendation of the organisation as a place to work or receive treatment
3.11 3.63 3.01 3.57 0.1
*Low scores better Future priorities and targets
Where the Trust is able to directly compare key findings from the survey, there has been a positive shift, with an improvement in seven of the key findings in our results since 2014 and no areas showing statistically significant deterioration.
However, when compared with the national average scores, the results are disappointing, with eight key findings being the equivalent to the lowest attained by other mental health and learning disability Trusts, and only one key finding being ranked above (better than) average.
Over the 2016-17 the key priority areas include:
• Increasing overall staff engagement
• Improving staff appraisal and quality indicators
• Increasing line management support and capability
• Improving staff wellbeing and support
These are all areas of focus in our Workforce and Organisational Development Strategy 2016-21, which includes the implementation of leadership and management development in 2016-17 and a new five-year strategy to support staff health and wellbeing.
ARA2016_master 140616.indd 52 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 53
Exit packages Reporting of compensation schemes - exit packages 2015/16
Number of compulsory redundancies
Number of other departures agreed
Total number of exit packages
Number Number Number
Exit package cost band (including any special payment element):
<£10,000 1 - 1
£10,001 - £25,000 3 2 5
£25,001 - 50,000 - - -
£50,001 - £100,000 - 2 2
£100,001 - £150,000 1 - 1
£150,001 - £200,000 - - -
>£200,000 - - -
Total number of exit packages by type 5 4 9
Total resource cost (£) £153,000 £140,000 £293,000
Reporting of compensation schemes - exit packages 2014/15
Number of compulsory redundancies
Number of other departures agreed
Total number of exit packages
Number Number Number
Exit package cost band (including any special payment element):
<£10,000 1 - 1
£10,001 - £25,000 3 3 6
£25,001 - 50,000 - - -
£50,001 - £100,000 1 1 2
£100,001 - £150,000 1 - 1
£150,001 - £200,000 - - -
>£200,000 - - -
Total number of exit packages by type 6 4 10
Total resource cost (£) £219,000 £97,000 £316,000
Exit packages: other (non-compulsory) departure payments
2015/16 2014/15
Payments agreed
Total value of agreements
Payments agreed
Total value of agreements
Number £000 Number £000
Voluntary redundancies including early retirement contractual costs
3 85 4 97
Mutually agreed resignations (MARS) contractual costs - - - -
Early retirements in the efficiency of the service contractual costs
- - - -
Contractual payments in lieu of notice 1 55 - -
Exit payments following Employment Tribunals or court orders
- - - -
Non-contractual payments requiring HMT approval - - - -
Total 4 140 4 97
Of which:
Non-contractual payments requiring HMT approval made to individuals where the payment value was more than 12 months’ of their annual salary
- - - -
ARA2016_master 140616.indd 53 14/06/2016 11:10
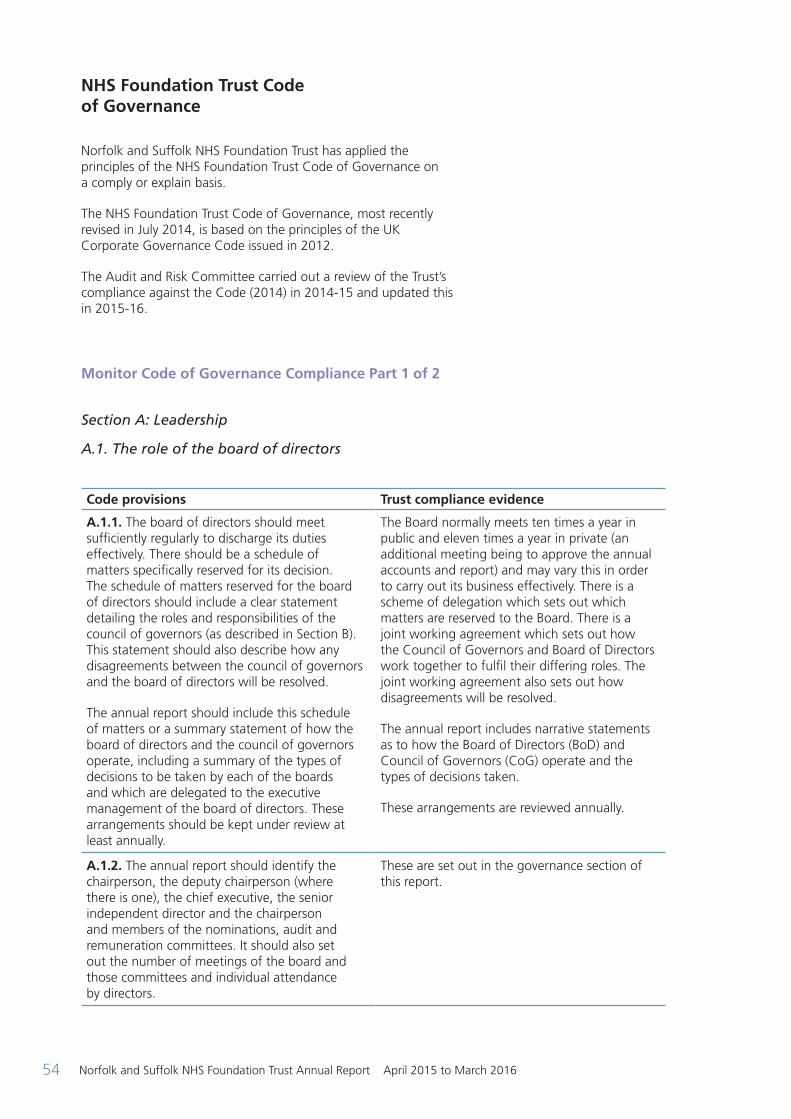
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201654
NHS Foundation Trust Code of Governance
Norfolk and Suffolk NHS Foundation Trust has applied the principles of the NHS Foundation Trust Code of Governance on a comply or explain basis.
The NHS Foundation Trust Code of Governance, most recently revised in July 2014, is based on the principles of the UK Corporate Governance Code issued in 2012.
The Audit and Risk Committee carried out a review of the Trust’s compliance against the Code (2014) in 2014-15 and updated this in 2015-16.
Monitor Code of Governance Compliance Part 1 of 2
Section A: Leadership
A.1. The role of the board of directors
Code provisions Trust compliance evidence
A.1.1. The board of directors should meet sufficiently regularly to discharge its duties effectively. There should be a schedule of matters specifically reserved for its decision. The schedule of matters reserved for the board of directors should include a clear statement detailing the roles and responsibilities of the council of governors (as described in Section B). This statement should also describe how any disagreements between the council of governors and the board of directors will be resolved.
The annual report should include this schedule of matters or a summary statement of how the board of directors and the council of governors operate, including a summary of the types of decisions to be taken by each of the boards and which are delegated to the executive management of the board of directors. These arrangements should be kept under review at least annually.
The Board normally meets ten times a year in public and eleven times a year in private (an additional meeting being to approve the annual accounts and report) and may vary this in order to carry out its business effectively. There is a scheme of delegation which sets out which matters are reserved to the Board. There is a joint working agreement which sets out how the Council of Governors and Board of Directors work together to fulfil their differing roles. The joint working agreement also sets out how disagreements will be resolved.
The annual report includes narrative statements as to how the Board of Directors (BoD) and Council of Governors (CoG) operate and the types of decisions taken.
These arrangements are reviewed annually.
A.1.2. The annual report should identify the chairperson, the deputy chairperson (where there is one), the chief executive, the senior independent director and the chairperson and members of the nominations, audit and remuneration committees. It should also set out the number of meetings of the board and those committees and individual attendance by directors.
These are set out in the governance section of this report.
(ref)
ARA2016_master 140616.indd 54 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 55
A.5. Governors
Code provisions Trust compliance evidence
A.5.3. The annual report should identify the members of the council of governors, including a description of the constituency or organisation that they represent, whether they were elected or appointed, and the duration of their appointments. The annual report should also identify the nominated lead governor. A record should be kept of the number of meetings of the council and the attendance of individual governors and it should be made available to members on request.
This information is reported in the governance and membership sections of this report.
The lead governor is Guenever Pachent (Public Governor Suffolk).
Section B: Effectiveness B.1. The composition of the board
Code provisions Trust compliance evidence
B.1.1. The board of directors should identify in the annual report each non-executive director it considers to be independent. The board should determine whether the director is independent in character and judgement and whether there are relationships or circumstances which are likely to affect, or could appear to affect, the director’s judgement. The board of directors should state its reasons if it determines that a director is independent despite the existence of relationships or circumstances which may appear relevant to its determination, including if the director:
• has been an employee of the NHS foundation trust within the last five years;
• has, or has had within the last three years, a material business relationship with the NHS foundation trust either directly, or as a partner, shareholder, director or senior employee of a body that has such a relationship with the NHS foundation trust;
• has received or receives additional remuneration from the NHS foundation trust apart from a director’s fee, participates in the NHS foundation trust’s performance-related pay scheme, or is a member of the NHS foundation trust’s pension scheme;
• has close family ties with any of the NHS foundation trust’s advisers, directors or senior employees;
• holds cross-directorships or has significant links with other directors through involvement in other companies or bodies;
All NEDs are considered independent.
None of the factors that might compromise independence in this list apply to the NEDs, other than the maximum six year term aspect. The nominations committee considers the question of independence in appointing and reappointing NEDs.
The Trust’s Constitution allows for NEDs to be appointed for up to nine years so long as they remain independent. Two NEDs have served more than six years or will have served more than six years by the end of their term. This situation will resolve from May 2016 as one of the longer term NEDs came to the end of their term in February 2016 and the other will leave at the end of April 2016.
This is set out in this annual report as part of the ‘comply or explain’ arrangement.
The Council of Governors has taken the view that the independence of NEDs is the primary concern and that this is not necessarily correlated with years’ service. For recent appointments, a second three-year term would normally be offered on the basis of satisfactory completion of objectives and then for the third three-year term, there would be market testing (with the incumbent being able to apply), unless there were over-riding factors why this would not be appropriate.
continued over >
ARA2016_master 140616.indd 55 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201656
• has served on the board of the NHS foundation trust for more than six years from the date of their first appointment; or
• is an appointed representative of the NHS foundation trust’s university medical or dental school.
B.1.4. The board of directors should include in its annual report a description of each director’s skills, expertise and experience. Alongside this, in the annual report, the board should make a clear statement about its own balance, completeness and appropriateness to the requirements of the NHS foundation trust. Both statements should also be available on the NHS foundation trust’s website.
Membership of the Board of Directors has been refreshed over the last 18 months with three new NEDs, a new Medical Director and Director of Finance. The Nominations Committee and Remuneration Committee consider the current and future needs of the Trust in drawing up person specifications and making appointments.
This annual report is downloadable from the Trust’s website.
B.2. Appointments of the board
Code provisions Trust compliance evidence
B.2.10. A separate section of the annual report should describe the work of the nominations committee(s), including the process it has used in relation to board appointments. The main role and responsibilities of the nominations committee should be set out in publicly available, written terms of reference.
Summaries of the work of the Nominations and Remunerations Committees are included in this annual report. The full ToRs are available on request.
B.3. Commitment
Code provisions Trust compliance evidence
B.3.1. For the appointment of a chairperson, the nominations committee should prepare a job specification defining the role and capabilities required including an assessment of the time commitment expected, recognising the need for availability in the event of emergencies. A chairperson’s other significant commitments should be disclosed to the council of governors before appointment and included in the annual report. Changes to such commitments should be reported to the council of governors as they arise, and included in the next annual report.
No individual, simultaneously whilst being a chairperson of an NHS foundation trust, should be the substantive chairperson of another NHS foundation trust.
This process was followed for the appointment of the Chair in 2013 and again for the proposed reappointment in 2016. There is an annual declaration of interests at both the BoD and CoG.
The Trust is compliant.
ARA2016_master 140616.indd 56 14/06/2016 11:10
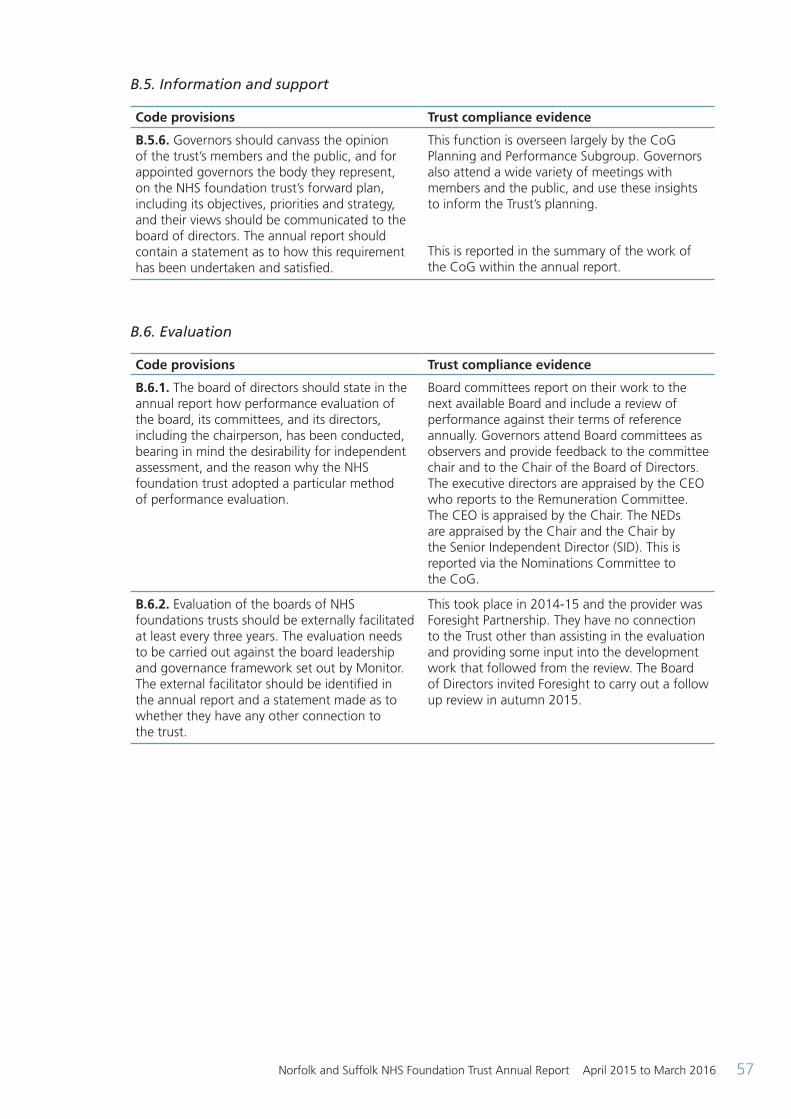
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 57
B.5. Information and support
Code provisions Trust compliance evidence
B.5.6. Governors should canvass the opinion of the trust’s members and the public, and for appointed governors the body they represent, on the NHS foundation trust’s forward plan, including its objectives, priorities and strategy, and their views should be communicated to the board of directors. The annual report should contain a statement as to how this requirement has been undertaken and satisfied.
This function is overseen largely by the CoG Planning and Performance Subgroup. Governors also attend a wide variety of meetings with members and the public, and use these insights to inform the Trust’s planning.
This is reported in the summary of the work of the CoG within the annual report.
B.6. Evaluation
Code provisions Trust compliance evidence
B.6.1. The board of directors should state in the annual report how performance evaluation of the board, its committees, and its directors, including the chairperson, has been conducted, bearing in mind the desirability for independent assessment, and the reason why the NHS foundation trust adopted a particular method of performance evaluation.
Board committees report on their work to the next available Board and include a review of performance against their terms of reference annually. Governors attend Board committees as observers and provide feedback to the committee chair and to the Chair of the Board of Directors. The executive directors are appraised by the CEO who reports to the Remuneration Committee. The CEO is appraised by the Chair. The NEDs are appraised by the Chair and the Chair by the Senior Independent Director (SID). This is reported via the Nominations Committee to the CoG.
B.6.2. Evaluation of the boards of NHS foundations trusts should be externally facilitated at least every three years. The evaluation needs to be carried out against the board leadership and governance framework set out by Monitor. The external facilitator should be identified in the annual report and a statement made as to whether they have any other connection to the trust.
This took place in 2014-15 and the provider was Foresight Partnership. They have no connection to the Trust other than assisting in the evaluation and providing some input into the development work that followed from the review. The Board of Directors invited Foresight to carry out a follow up review in autumn 2015.
ARA2016_master 140616.indd 57 14/06/2016 11:10
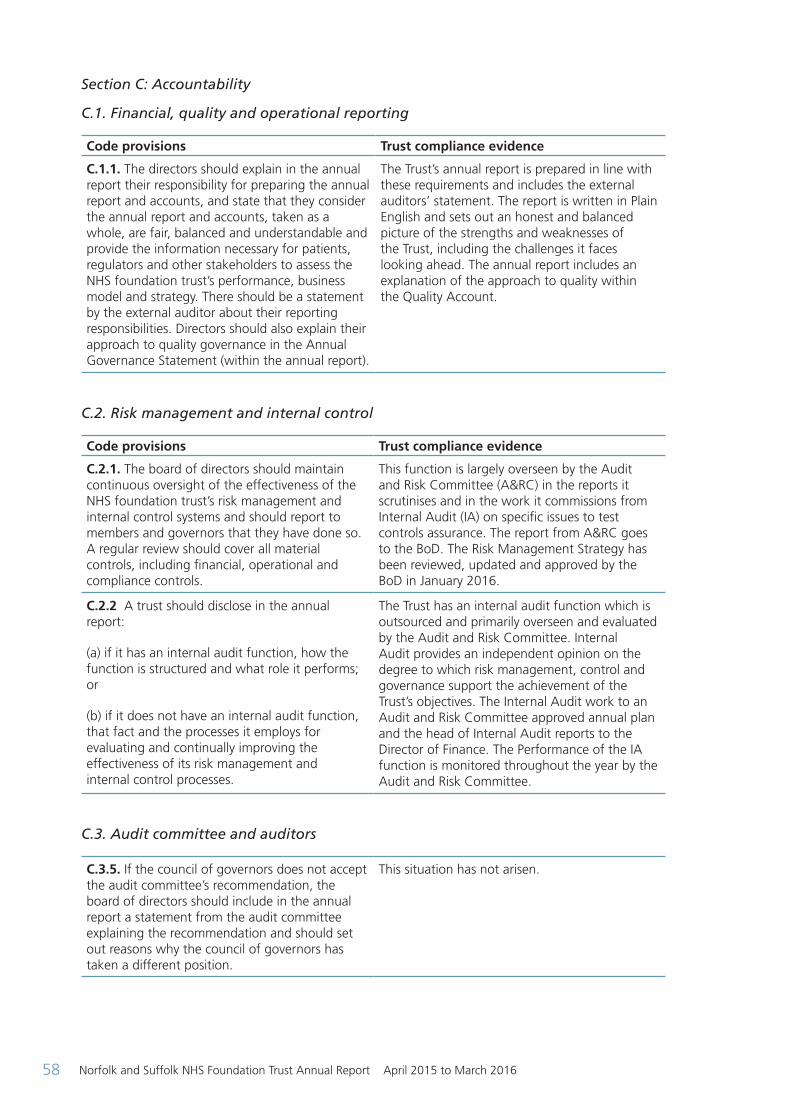
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201658
Section C: Accountability
C.1. Financial, quality and operational reporting
Code provisions Trust compliance evidence
C.1.1. The directors should explain in the annual report their responsibility for preparing the annual report and accounts, and state that they consider the annual report and accounts, taken as a whole, are fair, balanced and understandable and provide the information necessary for patients, regulators and other stakeholders to assess the NHS foundation trust’s performance, business model and strategy. There should be a statement by the external auditor about their reporting responsibilities. Directors should also explain their approach to quality governance in the Annual Governance Statement (within the annual report).
The Trust’s annual report is prepared in line with these requirements and includes the external auditors’ statement. The report is written in Plain English and sets out an honest and balanced picture of the strengths and weaknesses of the Trust, including the challenges it faces looking ahead. The annual report includes an explanation of the approach to quality within the Quality Account.
C.2. Risk management and internal control
Code provisions Trust compliance evidence
C.2.1. The board of directors should maintain continuous oversight of the effectiveness of the NHS foundation trust’s risk management and internal control systems and should report to members and governors that they have done so. A regular review should cover all material controls, including financial, operational and compliance controls.
This function is largely overseen by the Audit and Risk Committee (A&RC) in the reports it scrutinises and in the work it commissions from Internal Audit (IA) on specific issues to test controls assurance. The report from A&RC goes to the BoD. The Risk Management Strategy has been reviewed, updated and approved by the BoD in January 2016.
C.2.2 A trust should disclose in the annual report:
(a) if it has an internal audit function, how the function is structured and what role it performs; or
(b) if it does not have an internal audit function, that fact and the processes it employs for evaluating and continually improving the effectiveness of its risk management and internal control processes.
The Trust has an internal audit function which is outsourced and primarily overseen and evaluated by the Audit and Risk Committee. Internal Audit provides an independent opinion on the degree to which risk management, control and governance support the achievement of the Trust’s objectives. The Internal Audit work to an Audit and Risk Committee approved annual plan and the head of Internal Audit reports to the Director of Finance. The Performance of the IA function is monitored throughout the year by the Audit and Risk Committee.
C.3. Audit committee and auditors
C.3.5. If the council of governors does not accept the audit committee’s recommendation, the board of directors should include in the annual report a statement from the audit committee explaining the recommendation and should set out reasons why the council of governors has taken a different position.
This situation has not arisen.
ARA2016_master 140616.indd 58 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 59
C.3.9. A separate section of the annual report should describe the work of the committee in discharging its responsibilities. The report should include:
• the significant issues that the committee considered in relation to financial statements, operations and compliance, and how these issues were addressed;
• an explanation of how it has assessed the effectiveness of the external audit process and the approach taken to the appointment or re-appointment of the external auditor, the value of external audit services and information on the length of tenure of the current audit firm and when a tender was last conducted; and
• if the external auditor provides non-audit services, the value of the non-audit services provided and an explanation of how auditor objectivity and independence are safeguarded.
This is set out within the Audit and Risk Committee section of the annual report.
Section D: Remuneration
Code provisions Trust compliance evidence
D.1.3. Where an NHS foundation trust releases an executive director, for example to serve as a non-executive director elsewhere, the remuneration disclosures of the annual report should include a statement of whether or not the director will retain such earnings.
This has only arisen once in recent years when the Director of Operations for Norfolk and Waveney (Kathy Chapman) was seconded to a national role. The director received no additional remuneration.
Section E: Relations with stakeholders
E.1. Dialogue with members, patients and the local community
Code provisions Trust compliance evidence
E.1.4. The board of directors should ensure that the NHS foundation trust provides effective mechanisms for communication between governors and members from its constituencies. Contact procedures for members who wish to communicate with governors and / or directors should be made clearly available to members on the NHS foundation trust's website and in the annual report.
The main method of communication is through Insight magazine, and for members who have provided email addresses there is a monthly update which includes governor activities. The Trust coordinates member events on behalf of the governors to facilitate face-to-face discussions. As well as a members’ telephone contact number there is a [email protected] inbox monitored by the Membership and Engagement Office and Company Secretary to ensure that members are able to contact governors easily. This is made clear on the public website and in the annual report. Governors have access to a closed Facebook group for informal sharing of news, events and thoughts.
ARA2016_master 140616.indd 59 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201660
E.1.5 Describe the steps the board have taken to ensure members of the board, and in particular non-executive directors, develop an understanding of the views of governors and members about the FT.
The Council of Governors and Board of Directors have approved a joint agreement that sets out how non-executive directors work with governors to understand the views of members. Non-executive directors often attend Council of Governor meetings and are paired with link elected governors whom they meet informally. Non-executive directors also attend the Council of Governors’ Planning and Performance Subgroup where they discussion an agenda set by governors and on occasion carry out joint service visits with them. Governors raise issues on behalf of members and the wider public via an Issues Log which is taken in public at each full Council of Governors’ meeting. Directors often attend public facing events in the community or organised by governors and Trust officers.
E.1.6 The board of directors should monitor how representative the NHS Foundation Trust's membership is and the level and effectiveness of member engagement and report on this in the annual report.
The Board of Directors receives an annual report on membership which includes a demographic profile comparing membership to the population of Norfolk and Suffolk. The membership demographics are also reported in the annual report. The Trust’s Membership and Engagement Officer leads on recruitment and works with the Governors’ Membership and Communications Subgroup to promote membership to under-represented groups.
Monitor Code of Governance Compliance Part 2 of 2
Section A: Leadership
A.1. The role of the board of directors
Code provisions Trust compliance evidence
A.1.4. The board of directors should ensure that adequate systems and processes are maintained to measure and monitor the NHS foundation trust’s effectiveness, efficiency and economy as well as the quality of its health care delivery. The board should regularly review the performance of the NHS foundation trust in these areas against regulatory and contractual obligations, and approved plans and objectives
Monitoring of systems and processes, including regulatory compliance takes place through the scrutiny of business reports and through the work of internal and external audit functions. The Audit and Risk Committee takes an overview of risks to achievement of objectives. Finance, Investment and Quality Governance Committees have specific foci on quality and finance.
A.1.5. The board of directors should ensure that relevant metrics, measures, milestones and accountabilities are developed and agreed so as to understand and assess progress and delivery of performance. Where appropriate and, in particular, in high risk or complex areas, independent advice, for example, from the internal audit function, should be commissioned by the board of directors to provide an adequate and reliable level of assurance.
The Board receives performance information across the range of its activities, with more detailed reports on risk areas. The Board takes advice from the Audit and Risk Committee on use of audit functions where there is particular concern. Where appropriate, outcomes of IA reviews are reported to the Board by the Audit and Risk Committee.
ARA2016_master 140616.indd 60 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 61
A.1.6. The board of directors should report on its approach to clinical governance and its plan for the improvement of clinical quality in accordance with guidance set out by the DH, NHS England, the CQC and Monitor. The board should record where, within the structure of the organisation, consideration of clinical governance matters occurs.
The Board governance structure identifies the Quality Governance Committee as the main committee where clinical quality is considered, working closely with other committees, particularly Audit and Risk.
A.1.7. The chief executive as the accounting officer should follow the procedure set out by Monitor for advising the board of directors and the council of governors and for recording and submitting objections to decisions considered or taken by the board of directors in matters of propriety or regularity, and on issues relating to the wider responsibilities of the accounting officer for economy, efficiency and effectiveness.
On appointment, the CEO confirms their personal responsibilities as set out in the NHS Foundation Trust Accounting Officer Memorandum (March 2014).
A.1.8. The board of directors should establish the constitution and standards of conduct for the NHS foundation trust and its staff in accordance with NHS values and accepted standards of behaviour in public life, which includes the principles of selflessness, integrity, objectivity, accountability, openness, honesty and leadership (The Nolan Principles).
The Trust publishes a set of policies under the umbrella Business Conduct Policy which reference the Nolan Principles for public life. The Business Conduct Policy applies to all staff.
A.1.9. The board of directors should operate a code of conduct that builds on the values of the NHS foundation trust and reflect high standards of probity and responsibility. The board of directors should follow a policy of openness and transparency in its proceedings and decision-making unless this is in conflict with a need to protect the wider interests of the public or the NHS foundation trust (including commercial-in-confidence matters) and make clear how potential conflicts of interest are dealt with.
Board business is normally conducted in public although where there is confidential or commercial information this will be taken in private session.
The Board of Directors approved a code of conduct at its March 2016 meeting.
A.1.10. The NHS foundation trust should arrange appropriate insurance to cover the risk of legal action against its directors. Assuming the governors have acted in good faith and in accordance with their duties, and proper process has been followed, the potential for liability for the council should be negligible. Governors may have the benefit of an indemnity and/or insurance from the trust. While there is no legal requirement for trusts to provide an indemnity or insurance for governors to cover their service on the council of governors, where an indemnity or insurance policy is given, this can be detailed in the trust’s constitution.
Insurance cover is in place.
ARA2016_master 140616.indd 61 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201662
A.3. The chairperson
Code provision Trust compliance evidence
A.3.1. The chairperson should, on appointment by the council of governors, meet the independence criteria set out in B.1.1. A chief executive should not go on to be the chairperson of the same NHS foundation trust.
This requirement was met for the Chair on appointment in April 2013 and reappointment on 18 February 2016 (for three year term from April 2016). The Chair was not previously the Trust’s CEO.
A.4. Non-executive directors
Code provision Trust compliance evidence
A.4.1. In consultation with the council of governors, the board should appoint one of the independent non-executive directors to be the senior independent director (SID) to provide a sounding board for the chairperson and to serve as an intermediary for the other directors when necessary. The senior independent director should be available to governors if they have concerns that contact through the normal channels of chairperson, chief executive, finance director or Company Secretary has failed to resolve, or for which such contact is inappropriate. The senior independent director could be the deputy chairperson.
There is a SID (Marion Saunders) who is also the deputy chair, appointed in consultation with the Council of Governors (CoG), who is available to governors should the need arise.
A.4.2. The chairperson should hold meetings with the non-executive directors without the executives present. Led by the senior independent director, the non-executive directors should meet without the chairperson present, at least annually, to appraise the chairperson’s performance, and on other such occasions as are deemed appropriate.
There are regular NED (non-executive director) and Chair meetings without the EDs (executive directors) present (these take place before each Remuneration and Terms of Service committee meeting and via conference call).
There is a SID-led meeting of the NEDs without the Chair to discuss the Chair’s performance.
A.4.3. Where directors have concerns that cannot be resolved about the running of the NHS foundation trust or a proposed action, they should ensure that their concerns are recorded in the board minutes. On resignation, a director should provide a written statement to the chairperson for circulation to the board, if they have any such concerns.
The minutes will provide such a record should this situation arise. Minutes are checked for accuracy by the Board at the subsequent meeting.
A.5. Governors
Code provisions Trust compliance evidence
A.5.1. The council of governors should meet sufficiently regularly to discharge its duties. Typically the council of governors would be expected to meet as a full council at least four times a year. Governors should, where practicable, make every effort to attend the meetings of the council of governors. The NHS foundation trust should take appropriate steps to facilitate attendance.
The full CoG meets at least four times a year and holds two additional meetings (c. Feb and Nov), which are public facing and based around a specific theme (e.g. police liaison (2014), children and young people (2015), dementia (2016)).
Governors are reimbursed for all travel costs and may claim subsistence and other out of pocket expenses.
ARA2016_master 140616.indd 62 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 63
A.5.2. The council of governors should not be so large as to be unwieldy. The council of governors should be of sufficient size for the requirements of its duties. The roles, structure, composition, and procedures of the council of governors should be reviewed regularly as described in provision B.6.5
The full CoG composition was reviewed recently in 2011 prior to the merger when significant changes were made. Further changes have been made to keep the composition relevant.
A.5.4. The roles and responsibilities of the council of governors should be set out in a written document. This statement should include a clear explanation of the responsibilities of the council of governors towards members and other stakeholders and how governors will seek their views and keep them informed.
These responsibilities are set out in the Joint Working Agreement between the Board and the CoG that was agreed in October 2013.
A.5.5. The chairperson is responsible for leadership of both the board of directors and the council of governors (see A.3) but the governors also have a responsibility to make the arrangements work and should take the lead in inviting the chief executive to their meetings and inviting attendance by other executives and non-executives, as appropriate. In these meetings other members of the council of governors may raise questions of the chairperson or his/her deputy, or any other relevant director present at the meeting about the affairs of the NHS foundation trust.
The CEO normally attends all CoGs and EDs do so when their operational responsibilities allow. The minutes show that there is wide-ranging discussion on topics of concern to governors and members.
A.5.6. The council of governors should establish a policy for engagement with the board of directors for those circumstances when they have concerns about the performance of the board of directors, compliance with the new provider licence or other matters related to the overall wellbeing of the NHS foundation trust. The council of governors should input into the board’s appointment of a senior independent director (see A.4.1).
These engagement arrangements are set out in the Joint Working Agreement between the Board and the CoG that was agreed in October 2013 and reviewed in 2015-16.
The CoG inputs into the SID selection via the Nominations Committee.
A.5.7. The council of governors should ensure its interaction and relationship with the board of directors is appropriate and effective. In particular, by agreeing the availability and timely communication of relevant information, discussion and the setting in advance of meeting agendas and, where possible, using clear, unambiguous language.
The ways that information flows are set out in the Joint Working Agreement between the Board and the CoG that was agreed in October 2013 and reviewed in 2015-16. The use of clear language is encouraged in all Trust documents.
A.5.8. The council of governors should only exercise its power to remove the chairperson or any non-executive directors after exhausting all means of engagement with the board of directors. The council should raise any issues with the chairperson with the senior independent director in the first instance.
This situation has not arisen.
ARA2016_master 140616.indd 63 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201664
A.5.9. The council of governors should receive and consider other appropriate information required to enable it to discharge its duties, for example clinical statistical data and operational data.
The governor Planning and Performance subgroup requests and receives information including operational reports to enable it to assess the performance of the NEDs and the wider Board of Directors (BoD).
Section B: Effectiveness B.1. The composition of the board
Code provisions Trust compliance evidence
B.1.2. At least half the board of directors, excluding the chairperson, should comprise non-executive directors determined by the board to be independent.
The Trust has decided to have 7 NEDs, including the Chair and 7 EDs and to achieve the majority NED vote by allocating an additional vote to the Chair. This is set out in the Constitution.
B.1.3. No individual should hold, at the same time, positions of director and governor of any NHS foundation trust.
This is not possible under our Constitution.
B.2. Appointments of the board
Code provisions Trust compliance evidence
B.2.1. The nominations committee or committees, with external advice as appropriate, are responsible for the identification and nomination of executive and non-executive directors. The nominations committee should give full consideration to succession planning, taking into account the future challenges, risks and opportunities facing the NHS foundation trust and the skills and expertise required within the board of directors to meet them.
The person specifications for all BoD posts are reviewed as part of the process for recruitment to update them so as to take account of the future requirements of the organisation. The Nominations Committee Workplan includes future recruitment so that preparation is begun in good time.
B.2.2. Directors on the board of directors and governors on the council of governors should meet the “fit and proper” persons test (FPPT) described in the provider licence. For the purpose of the licence and application criteria, “fit and proper” persons are defined as those without certain recent criminal convictions and director disqualifications, and those who are not bankrupt (undischarged). Trusts should also abide by the updated guidance from the CQC regarding appointments to senior positions in organisations subject to CQC regulations.
Directors and governors are required to complete DBS checks and to declare that they are not undischarged bankrupts.
There is a FPPT checklist drawn from the CQC regulations for directors for use in appraisals from 2016.
ARA2016_master 140616.indd 64 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 65
B.2.3. There may be one or two nominations committees. If there are two committees, one will be responsible for considering nominations for executive directors and the other for non-executive directors (including the chairperson). The nominations committee(s) should regularly review the structure, size and composition of the board of directors and make recommendations for changes where appropriate. In particular, the nominations committee(s) should evaluate, at least annually, the balance of skills, knowledge and experience on the board of directors and, in the light of this evaluation, prepare a description of the role and capabilities required for appointment of both executive and non-executive directors, including the chairperson.
The Trust has a two committee structure. The Nominations Committee oversees NED appointments, and the Remuneration and Terms of Service Committee oversees ED appointments.
The CEO is invited to attend one Nominations Committee meeting a year, to consider the balance of skills around the BoD table.
Person specifications are set according to the wider Trust requirements and the specific gaps created by the individual’s departure.
B.2.4. The chairperson or an independent non-executive director should chair the nominations committee(s). At the discretion of the committee, a governor can chair the committee in the case of appointment of NEDs and the Chair.
The SID chairs the Nominations Committee and the lead governor is the deputy chair, and the Chair chairs the Remuneration and Terms of Service Committee. Governors are closely involved throughout the whole process of making NED and Chair appointments as well as being invited to sit on executive director appointment panels.
B.2.5. The governors should agree with the nominations committee a clear process for the nomination of a new chairperson and non-executive directors. Once suitable candidates have been identified the nominations committee should make recommendations to the council of governors.
This is the process followed by the CoG and Nominations Committee.
B.2.6. Where an NHS foundation trust has two nominations committees, the nominations committee responsible for the appointment of non-executive directors should consist of a majority of governors. If only one nominations committee exists, when nominations for non-executives, including the appointment of a chairperson or a deputy chairperson, are being discussed, there should be a majority of governors on the committee and also a majority governor representation on the interview panel.
The Trust has two committees and the NED appointment committee has a majority of governor members.
B.2.7. When considering the appointment of non-executive directors, the council of governors should take into account the views of the board of directors and the nominations committee on the qualifications, skills and experience required for each position.
Soundings are taken from the BoD in reviewing the person specification for NEDs.
B.2.8. The annual report should describe the process followed by the council of governors in relation to appointments of the chairperson and non-executive directors.
This is set out in the section on the work of the nominations committee.
B.2.9. An independent external adviser should not be a member of or have a vote on the nominations committee(s).
This is the case. External advisors on appointment panels are purely advisory and do not vote.
ARA2016_master 140616.indd 65 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201666
B.3. Commitment
Code provisions Trust compliance evidence
B.3.3. The board of directors should not agree to a full-time executive director taking on more than one non-executive directorship of an NHS foundation trust or another organisation of comparable size and complexity, nor the chairpersonship of such an organisation.
The Trust is compliant.
B.5. Information and support
Code provisions Trust compliance evidence
B.5.1. The board of directors and the council of governors should be provided with high-quality information appropriate to their respective functions and relevant to the decisions they have to make. The board of directors and the council of governors should agree their respective information needs with the executive directors through the chairperson.
The information for the boards should be concise, objective, accurate and timely, and it should be accompanied by clear explanations of complex issues.
The board of directors should have complete access to any information about the NHS foundation trust that it deems necessary to discharge its duties, including access to senior management and other employees.
Information requirements for the CoG and BoD are agreed locally and change over time and are overseen by the Chair. Governors may access all information presented to the BoD, including private BoD papers, on the basis of a confidentiality agreement.
The format and presentation of information is kept under review to ensure that the key elements are not obscured by detail.
This is the case.
B.5.2. The board of directors and in particular non-executive directors may reasonably wish to challenge assurances received from the executive management. They need not seek to appoint a relevant adviser for each and every subject area that comes before the board of directors, although they should, wherever possible, ensure that they have sufficient information and understanding to enable challenge and to take decisions on an informed basis. When complex or high-risk issues arise, the first course of action should normally be to encourage further and deeper analysis to be carried out in a timely manner, within the NHS foundation trust. On occasion, non-executives may reasonably decide that external assurance is appropriate.
The BoD minutes evidence challenge and requests for clarification / additional information in order to form a clear judgement or make a decision. NEDs are able to request external assurance on any appropriate matter.
ARA2016_master 140616.indd 66 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 67
B.5.3. The board should ensure that directors, especially non-executive directors, have access to the independent professional advice, at the NHS foundation trust’s expense, where they judge it necessary to discharge their responsibilities as directors. Decisions to appoint an external adviser should be the collective decision of the majority of non-executive directors. The availability of independent external sources of advice should be made clear at the time of appointment.
Access to external advice is available to all directors and NEDs. The NED appointment letter sets out the availability of external advice at the Trust’s expense.
B.5.4. Committees should be provided with sufficient resources to undertake their duties. The board of directors should also ensure that the council of governors is provided with sufficient resources to undertake its duties with such arrangements agreed in advance.
BoD, BoD committees and the CoG and CoG subgroups are supported by Trust officers so that they can undertake their duties. The arrangements are set out in the Joint CoG / BoD agreement.
B.6. Evaluation
Code provisions Trust compliance evidence
B.6.3. The senior independent director should lead the performance evaluation of the chairperson, within a framework agreed by the council of governors and taking into account the views of directors and governors.
This is in place and reports via the Nominations Committee to the CoG.
B.6.4. The chairperson, with assistance of the board secretary, if applicable, should use the performance evaluations as the basis for determining individual and collective professional development programmes for non-executive directors relevant to their duties as board members.
Individual development plans are developed following the Chair’s meetings with NEDs. These are informed by the external BoD evaluation and the collective BoD development plan.
B.6.5. Led by the chairperson, the council of governors should periodically assess their collective performance and they should regularly communicate to members and the public details on how they have discharged their responsibilities, including their impact and effectiveness on:
• holding the non-executive directors individually and collectively to account for the performance of the board of directors.
• communicating with their member constituencies and the public and transmitting their views to the board of directors; and
• contributing to the development of forward plans of NHS foundation trusts.
The council of governors should use this process to review its roles, structure, composition and procedures, taking into account emerging best practice. Further information can be found in Monitor’s publication: Your statutory duties: A reference guide for NHS foundation trust governors.
The CoG carries out a self-evaluation approximately every year. This includes all aspects of the governor’s role and the work of the CoG and its subgroups.
Communication to members is primarily via the Insight Magazine which is produced twice a year. This is complemented by an email newsletter and a governors’ email following each CoG setting out the work of governors.
The CoG self-evaluation is an annual process and informs discussions about its work, structures and processes. The Education Subgroup which oversees governor training and development uses the annual review to inform the annual development plan.
ARA2016_master 140616.indd 67 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201668
B.6.6. There should be a clear policy and a fair process, agreed and adopted by the council of governors, for the removal from the council of any governor who consistently and unjustifiably fails to attend the meetings of the council of governors or has an actual or potential conflict of interest which prevents the proper exercise of their duties. This should be shared with governors. In addition, it may be appropriate for the process to provide for removal from the council of governors where behaviours or actions of a governor or group of governors may be incompatible with the values and behaviours of the NHS foundation trust. Where there is any disagreement as to whether the proposal for removal is justified, an independent assessor agreeable to both parties should be requested to consider the evidence and determine whether the proposed removal is reasonable or otherwise.
This is set out in the Code of Conduct which is reviewed annually and which all governors sign. The sanction / removal process was updated in 2016.
B.8. Resignation of directors
Code provisions Trust compliance evidence
B.8.1. The remuneration committee should not agree to an executive member of the board leaving the employment of an NHS foundation trust, except in accordance with the terms of their contract of employment, including but not limited to service of their full notice period and / or material reductions in their time commitment to the role, without the board first having completed and approved a full risk assessment.
Executive directors leaving the Trust do so only in line with contractual requirements.
Section C: Accountability
C.1. Financial, quality and operational reporting
Code provisions Trust compliance evidence
C.1.3 At least annually and in a timely manner, the board should set out clearly its financial, quality and operating objectives for the NHS foundation trust and disclose sufficient information, both quantitative and qualitative, of the NHS foundation trust’s business and operation, including clinical outcome data, to allow members and governors to evaluate its performance.
The financial, quality and operating objectives are published annually as part of the business planning cycle in the public Board of Director papers. Financial and performance information is published monthly and additional information is shared with governors via the Planning and Performance subgroup where non-executive directors are held to account for the performance of the board. Clinical outcome data for mental health services is more challenging than in the acute sector but measures are reported through the Trust’s patient safety and quality report (four times a year) and the monthly business performance report. These are published on the Trust’s website and reviewed at the Trust’s Board meetings held in public.
ARA2016_master 140616.indd 68 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 69
C.1.4 a) The board of directors must notify Monitor and the council of governors without delay and should consider whether it is in the public’s interest to bring to the public attention, any major new developments in the NHS foundation trust’s sphere of activity which are not public knowledge, which it is able to disclose and which may lead by virtue of their effect on its assets and liabilities, or financial position or on the general course of its business, to a substantial change to the financial wellbeing, health care delivery performance or reputation and standing of the NHS foundation trust. b) The board of directors must notify Monitor and the council of governors without delay and should consider whether it is in the public interest to bring to public attention all relevant information which is not public knowledge concerning a material change in:
• the NHS foundation trust’s financial condition;
• the performance of its business; and / or
• the NHS foundation trust’s expectations as to its performance which, if made public, would be likely to lead to a substantial change to the financial wellbeing, health care delivery performance or reputation and standing of the NHS foundation trust.
C.3. Audit committee and auditors
Code provision Trust compliance evidence
C.3.1. The board of directors should establish an audit committee composed of at least three members who are all independent non-executive directors. The board should satisfy itself that the membership of the audit committee has sufficient skills to discharge its responsibilities effectively, including ensuring that at least one member of the audit committee has recent and relevant financial experience. The chairperson of the trust should not chair or be a member of the audit committee. He can, however, attend meetings by invitation as appropriate.
The Trust’s A&RC is constituted in line with this provision and is chaired by an appropriately qualified accountant. The Trust Chair is not a member of the A&R committee.
ARA2016_master 140616.indd 69 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201670
C.3.3. The council of governors should take the lead in agreeing with the audit committee the criteria for appointing, re-appointing and removing external auditors. The council of governors will need to work hard to ensure they have the skills and knowledge to choose the right external auditor and monitor their performance.
However, they should be supported in this task by the audit committee, which provides information to the governors on the external auditor’s performance as well as overseeing the NHS foundation trust’s internal financial reporting and internal auditing.
Last year the CoG appointed the external auditors with support from the Trust’s procurement team and the Audit and Risk Committe Chair. Two governors were nominated by the CoG to lead on this work, including setting the criteria in the specification and judging the applications.
C.3.6. The NHS foundation trust should appoint an external auditor for a period of time which allows the auditor to develop a strong understanding of the finances, operations and forward plans of the NHS foundation trust. The current best practice is for a three to five-year period of appointment.
The Trust follows this practice.
C.3.7. When the council of governors ends an external auditor’s appointment in disputed circumstances, the chairperson should write to Monitor informing it of the reasons behind the decision.
This situation has not arisen.
C.3.8. The audit committee should review arrangements that allow staff of the NHS foundation trust and other individuals where relevant, to raise, in confidence, concerns about possible improprieties in matters of financial reporting and control, clinical quality, patient safety or other matters.
The audit committee’s objective should be to ensure that arrangements are in place for the proportionate and independent investigation of such matters and for appropriate follow-up action.
This should include ensuring safeguards for those who raise concerns are in place and operating effectively.
Such processes should enable individuals or groups to draw formal attention to practices that are unethical or violate internal or external policies, rules or regulations and to ensure that valid concerns are promptly addressed.
These processes should also reassure individuals raising concerns that they will be protected from potential negative repercussions.
The Audit Committee oversees this work and approves the public interest disclosure (whistleblowing policy) and the Chair of the A&RC committee is also the lead NED for whistle-blowing. The policy and the communications that support it emphasise the safeguards in place to protect staff who raise concerns in good faith.
ARA2016_master 140616.indd 70 14/06/2016 11:10
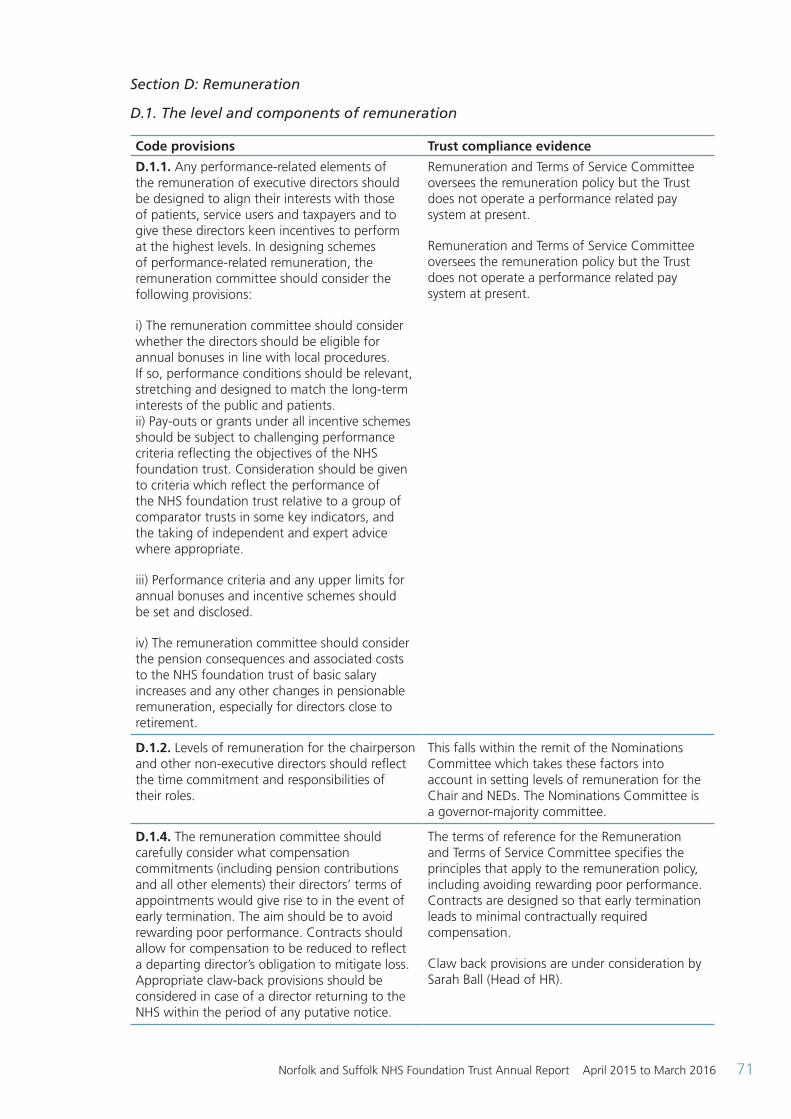
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 71
Section D: Remuneration
D.1. The level and components of remuneration
Code provisions Trust compliance evidence
D.1.1. Any performance-related elements of the remuneration of executive directors should be designed to align their interests with those of patients, service users and taxpayers and to give these directors keen incentives to perform at the highest levels. In designing schemes of performance-related remuneration, the remuneration committee should consider the following provisions:
i) The remuneration committee should consider whether the directors should be eligible for annual bonuses in line with local procedures. If so, performance conditions should be relevant, stretching and designed to match the long-term interests of the public and patients. ii) Pay-outs or grants under all incentive schemes should be subject to challenging performance criteria reflecting the objectives of the NHS foundation trust. Consideration should be given to criteria which reflect the performance of the NHS foundation trust relative to a group of comparator trusts in some key indicators, and the taking of independent and expert advice where appropriate.
iii) Performance criteria and any upper limits for annual bonuses and incentive schemes should be set and disclosed.
iv) The remuneration committee should consider the pension consequences and associated costs to the NHS foundation trust of basic salary increases and any other changes in pensionable remuneration, especially for directors close to retirement.
Remuneration and Terms of Service Committee oversees the remuneration policy but the Trust does not operate a performance related pay system at present.
Remuneration and Terms of Service Committee oversees the remuneration policy but the Trust does not operate a performance related pay system at present.
D.1.2. Levels of remuneration for the chairperson and other non-executive directors should reflect the time commitment and responsibilities of their roles.
This falls within the remit of the Nominations Committee which takes these factors into account in setting levels of remuneration for the Chair and NEDs. The Nominations Committee is a governor-majority committee.
D.1.4. The remuneration committee should carefully consider what compensation commitments (including pension contributions and all other elements) their directors’ terms of appointments would give rise to in the event of early termination. The aim should be to avoid rewarding poor performance. Contracts should allow for compensation to be reduced to reflect a departing director’s obligation to mitigate loss. Appropriate claw-back provisions should be considered in case of a director returning to the NHS within the period of any putative notice.
The terms of reference for the Remuneration and Terms of Service Committee specifies the principles that apply to the remuneration policy, including avoiding rewarding poor performance. Contracts are designed so that early termination leads to minimal contractually required compensation.
Claw back provisions are under consideration by Sarah Ball (Head of HR).
ARA2016_master 140616.indd 71 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201672
D.2. Procedure
Code provision Trust compliance evidence
D.2.2. The remuneration committee should have delegated responsibility for setting remuneration for all executive directors, including pension rights and any compensation payments. The committee should also recommend and monitor the level and structure of remuneration for senior management. The definition of senior management for this purpose should be determined by the board, but should normally include the first layer of management below board level.
This is set out in the terms of reference for the Remuneration and Terms of Service Committee and forms part of the work plan.
D.2.3. The council of governors should consult external professional advisers to market-test the remuneration levels of the chairperson and other non-executives at least once every three years and when they intend to make a material change to the remuneration of a non-executive.
The Nominations Committee takes account of benchmarking information (annually) in setting the remuneration levels for NEDs. This forms part of the work plan for the committee. Recommendations based on this information are then made to the CoG for decision.
Section E: Relations with stakeholders
E.1. Dialogue with members, patients and the local community
Code provisions Trust compliance evidence
E.1.2. The board of directors should clarify in writing how the public interests of patients and the local community will be represented, including its approach for addressing the overlap and interface between governors and any local consultative forums (e.g., Local Health watch, the Overview and Scrutiny Committee, the local League of Friends, and staff groups).
A paper setting out these arrangements was approved by the BoD at its meeting on March 2016.
E.1.3. The chairperson should ensure that the views of governors and members are communicated to the board as a whole. The chairperson should discuss the affairs of the NHS foundation trust with governors. Non-executive directors should be offered the opportunity to attend meetings with governors and should expect to attend them if requested by governors. The senior independent director should attend sufficient meetings with governors to listen to their views in order to help develop a balanced understanding of the issues and concerns of governors.
The Chair ensures that the views of governors and members are communicated to the Board through regular discussions, and the Chair meets with governors frequently to brief them on key topics and future developments. Non-executive directors meet with governors through a variety of channels. Directors are paired with elected governors, attend the governor Planning and Performance subgroup (usually at least two at each meeting), and the Council of Governors. The SID is available to all governors for informal discussions and attends the Council of Governors meetings. Some governors also take the opportunity to attend Board of Directors meetings and to talk informally before and after.
ARA2016_master 140616.indd 72 14/06/2016 11:10
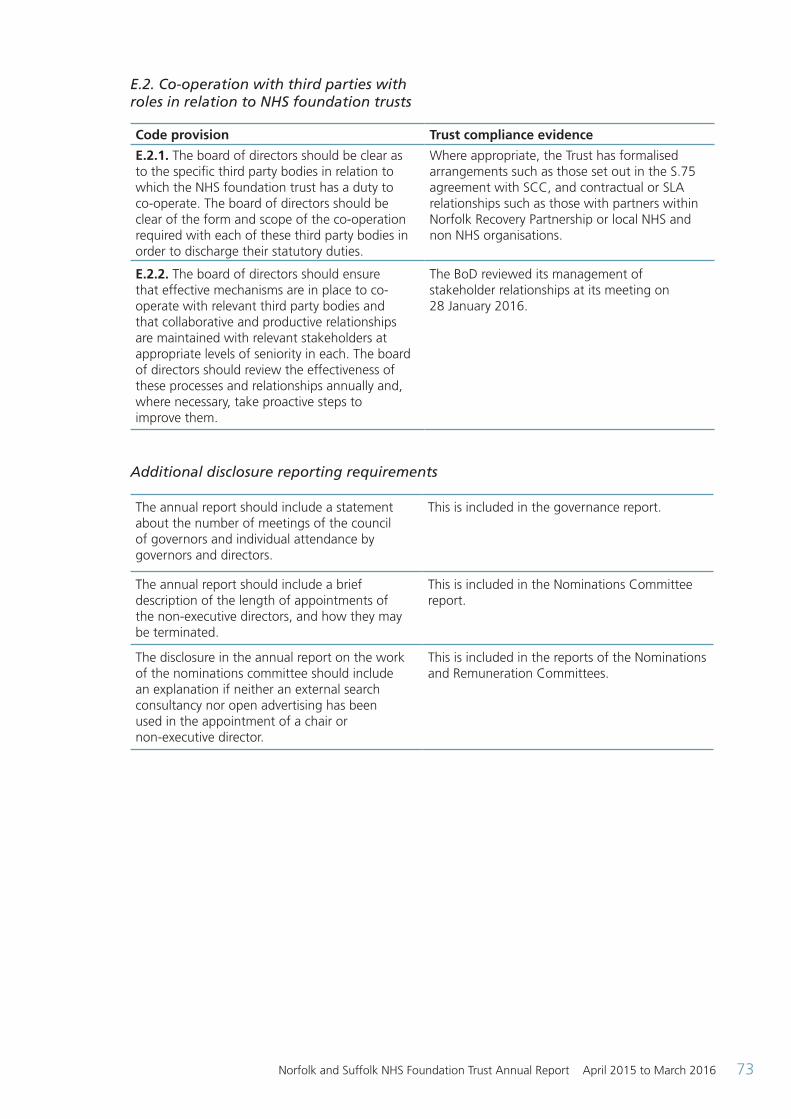
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 73
E.2. Co-operation with third parties with roles in relation to NHS foundation trusts
Code provision Trust compliance evidence
E.2.1. The board of directors should be clear as to the specific third party bodies in relation to which the NHS foundation trust has a duty to co-operate. The board of directors should be clear of the form and scope of the co-operation required with each of these third party bodies in order to discharge their statutory duties.
Where appropriate, the Trust has formalised arrangements such as those set out in the S.75 agreement with SCC, and contractual or SLA relationships such as those with partners within Norfolk Recovery Partnership or local NHS and non NHS organisations.
E.2.2. The board of directors should ensure that effective mechanisms are in place to co-operate with relevant third party bodies and that collaborative and productive relationships are maintained with relevant stakeholders at appropriate levels of seniority in each. The board of directors should review the effectiveness of these processes and relationships annually and, where necessary, take proactive steps to improve them.
The BoD reviewed its management of stakeholder relationships at its meeting on 28 January 2016.
Additional disclosure reporting requirements
The annual report should include a statement about the number of meetings of the council of governors and individual attendance by governors and directors.
This is included in the governance report.
The annual report should include a brief description of the length of appointments of the non-executive directors, and how they may be terminated.
This is included in the Nominations Committee report.
The disclosure in the annual report on the work of the nominations committee should include an explanation if neither an external search consultancy nor open advertising has been used in the appointment of a chair or non-executive director.
This is included in the reports of the Nominations and Remuneration Committees.
ARA2016_master 140616.indd 73 14/06/2016 11:10
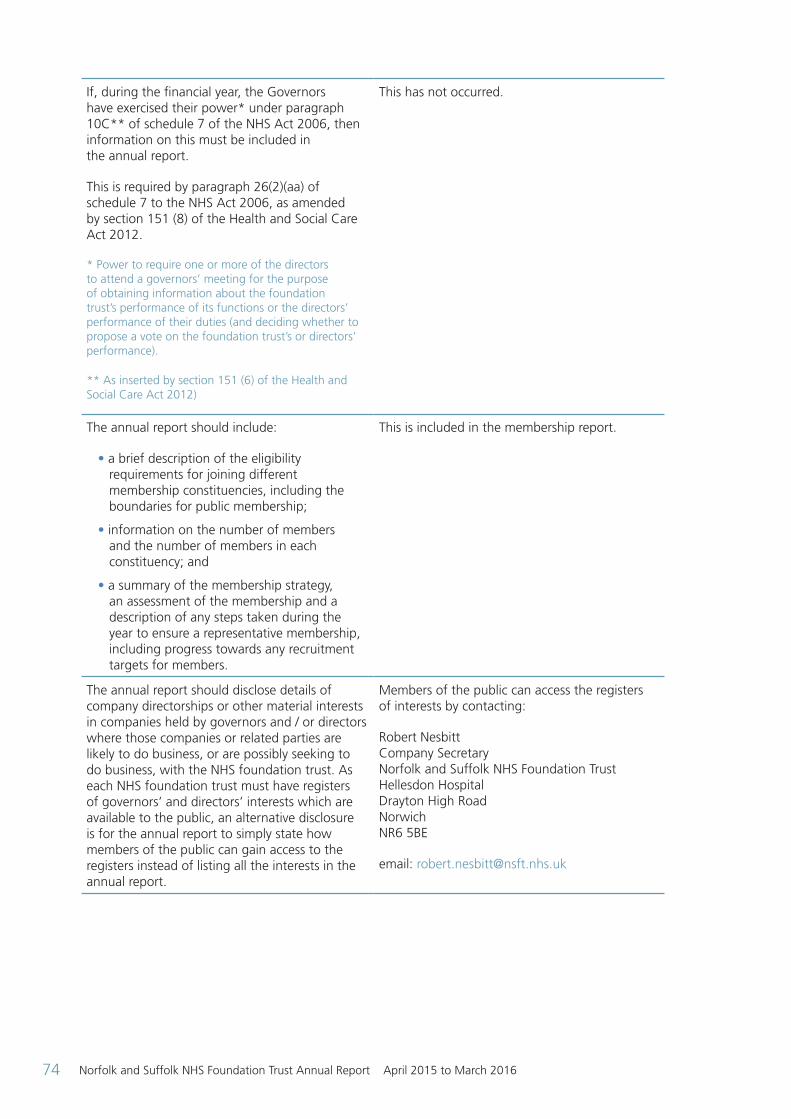
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201674
If, during the financial year, the Governors have exercised their power* under paragraph 10C** of schedule 7 of the NHS Act 2006, then information on this must be included in the annual report.
This is required by paragraph 26(2)(aa) of schedule 7 to the NHS Act 2006, as amended by section 151 (8) of the Health and Social Care Act 2012.
* Power to require one or more of the directors to attend a governors’ meeting for the purpose of obtaining information about the foundation trust’s performance of its functions or the directors’ performance of their duties (and deciding whether to propose a vote on the foundation trust’s or directors’ performance).
** As inserted by section 151 (6) of the Health and Social Care Act 2012)
This has not occurred.
The annual report should include:
• a brief description of the eligibility requirements for joining different membership constituencies, including the boundaries for public membership;
• information on the number of members and the number of members in each constituency; and
• a summary of the membership strategy, an assessment of the membership and a description of any steps taken during the year to ensure a representative membership, including progress towards any recruitment targets for members.
This is included in the membership report.
The annual report should disclose details of company directorships or other material interests in companies held by governors and / or directors where those companies or related parties are likely to do business, or are possibly seeking to do business, with the NHS foundation trust. As each NHS foundation trust must have registers of governors’ and directors’ interests which are available to the public, an alternative disclosure is for the annual report to simply state how members of the public can gain access to the registers instead of listing all the interests in the annual report.
Members of the public can access the registers of interests by contacting:
Robert Nesbitt Company Secretary Norfolk and Suffolk NHS Foundation Trust Hellesdon Hospital Drayton High Road Norwich NR6 5BE
email: [email protected]
ARA2016_master 140616.indd 74 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 75
Regulatory ratings
Monitor has a statutory role to ensure the continued provision of key NHS services, as identified by commissioners. They also have a statutory role in ensuring effective governance of NHS foundation trusts, which includes financial governance and managing finances in a way that is economic, efficient and effective. The risk assessment framework helps to detect early signs of any financial risks that could jeopardise an NHS foundation trust’s financial standing and so threaten the continuity of the key services it provides, or indicates a financial governance concern.
Monitor assesses foundation trusts against two key ratings to help determine that trusts are performing as expected and in keeping with their license to operate. These two ratings are the financial sustainability risk rating and the governance rating.
The financial sustainability risk rating is Monitor’s view of the level of financial risk a foundation trust faces to the ongoing delivery of key NHS services and its overall financial efficiency. The rating ranges from 1, the most serious risk, to 4, the lowest risk. A rating indicating serious risk does not necessarily represent a breach of the provider licence. Rather, it reflects the degree of financial concern Monitor have about a provider and consequently the frequency with which it will be monitored. Monitor has replaced the previously used ‘continuity of service risk rating’ with the ‘financial sustainability risk rating’.
The financial sustainability risk rating is calculated using the following measures:
Liquidity: days of operating costs held in cash or cash-equivalent forms, including wholly committed lines of credit available for drawdown.
Capital servicing capacity: the degree to which the organisation’s generated income covers its financial obligations.
Income and expenditure (I&E) margin: the degree to which the organisation is operating a surplus/deficit. The I&E margin is defined as surplus/(deficit)/total operating and non-operating income. Surplus/(deficit) should be calculated before impairments, transfers by absorption, gains / losses on asset disposal and restructuring costs.
Variance from plan in relation to I&E margin: variance between a foundation trust’s planning I&E margin in its annual forward plan and its actual I&E margin within the year.
The Trust’s FSRR was expected to fall to ‘1’ in 2015-16 as the Trust dealt with the impact of special measures and the financial investment necessary to address the quality issues. With slightly improved performance the FSRR of 2 was achieved. The COSRR rating in 2014-15 was 2, although the measure was of course different at the time.
(RR1) Q1 (YTD)
Q2 (YTD)
Q3 (YTD)
Q4 (YTD)2015-16 Annual Plan Full Year
Capital Service Cover 1 1 1 1 1 1
Liquidity 1 1 1 1 1 1
I&E Margin NA 1 1 1 1 1
I&E Margin from plan NA 4 4 4 4 4
FSRR overall rating 1 1 2 2 2 2
The governance rating is Monitor’s degree of concern about how the Trust is run. This provides an assessment of how well run the Trust is in terms of providing care to patients, meeting national quality standards and ensuring value for money. Trusts can be assessed as “green” meaning no concerns; “under investigation” where concerns are
being investigated; and “red” where issues have been identified and action is being taken.
The governance rating at 20 April 2016 is currently red with the comment ‘Subject to enforcement action, in special measures’. This rating is expected if a Trust is in special measures.
ARA2016_master 140616.indd 75 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201676
Additional reporting Sustainability reporting
Within NSFT, the Sustainability Manager has a key responsibility to support and enable the Trust to implement our Sustainability Policy, which covers all aspects of our environmental impact.
The government set NHS organisations a challenging target for 2015 which was to reduce carbon footprint by 10% from 2007 levels. So far we have exceeded that target by reaching 14% and we are now on track to reach the 2020 target of a 20% reduction of our 2007 levels.
We have made progress this year with the sale of energy from Grange Lodge PV panels back to the grid and the use of more LED lighting along with campaigns to educate all users of the need to conserve energy. The Trust continues to utilise framework pricing to achieve preferred rates across properties.
The Trust has made significant changes in recycling of stock and equipment that is no longer suitable for Trust requirements by investigating and building relationships with third parties who are able to reuse the items to both local and distant locations. This enables the Trust to help a variety of organisations, reduce our disposal costs and achieve a far more environmental option for disposal. We have recently commenced working with a charity that recycles electrical waste so that items can be bought at competitive prices by services users. Income has also been received through sales of items such as out-of-date furniture and equipment that the Trust is no longer able to use.
We have implemented a Trust-wide furniture reuse scheme that has seen significant cost avoidance savings through reallocation of items. The introduction of a control process for purchasing of these types of items has enabled a Trust-wide inventory to be introduced.
Waste management is closely managed with an increase in direct recycling to approximately 56% through extended recycling schemes across the Trust. The waste contractor has also contributed through a system of filtering the general waste for other recyclates with the remaining residue being bailed into pellets as fuel. This enables us to report confidently a recycling rate of over 90%. Currently, clinical waste is sent to a waste site which supports the
provision of energy for buildings at the Ipswich Hospital site, where Woodlands, one of our own facilities, is situated.
Supporting the Trust’s policy and staff welfare, regular updates regarding eating healthily and being proactive in taking exercise are circulated and to support this there is cycle scheme and lift share sites that are actively promoted.
The Trust has recently submitted the Good Corporate Citizenship report which shows an increase to 59% (2015-16) from 48% (2014-15) which means that NSFT is rapidly changing its effect on the environment both locally and nationally. The increased score has been brought about by a strong resilience policy and work with community organisations.
We have supported the development of ‘East of England Sustainability Managers forum’ working alongside HEFMA. We, as founder members, have been proactive in teaching, sharing best practice and giving support and guidance regarding our successful sustainable project options.
Equality reporting
Equality Act (2010) requirements:
The general duties are:
• Eliminate unlawful discrimination, harassment and victimisation and any other conduct prohibited by the Act
• Advance equality of opportunity between people who share a protected characteristic and people who do not share it
• Foster good relations between people who share a protected characteristic and people who do not share it
The specific duties are to:
• Publish information to show our compliance with the (general) Equality Duty, at least annually
• Set and publish equality objectives, at least every four years
The Trust complies with the Equality Act through the NHS Equality Delivery System (EDS). The main purpose of the EDS is to help local NHS organisations to meet obligations under the Equality Act (2010). It works by ensuring that all of the work of the Trust is benefitting all protected groups in different ways.
ARA2016_master 140616.indd 76 14/06/2016 11:10

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 77
The Board of Directors receives four reports a year on the Trust’s progress against its objectives. A full year report is published in April each year. For the reporting period the objectives were:
Objective 1: Governance, leadership and accountability
“To provide the trust with an assurance framework that equality and diversity is embedded in business as usual and that each directorate takes their part of responsibility implementing the EDS2 to achieve the Trust equality objectives.”
Rationale: In order for equality and diversity to be considered as an essential element across the organisation, leaders need to lead by example and act as role models to make sure we uphold the principles of fairness, respect, equality, dignity and autonomy in all our practices that relate to both our services and workforce.
Objective 2: Improving access and experience for service users with protected characteristics who are over and under-represented in our services
“To carry out equality analyses across all services and use qualitative and quantitative information to identify priorities for action.”
Rationale: In order to be able to remove potential barriers and be sensitive to individual needs, each of our services must understand the demographics of the population we serve and whether those that access services are reflective of our local diverse population. Furthermore, to improve our services we need to gather feedback from people who are from protected groups to better understand their experiences and where the inequalities are.
Objective 3: Staff to feel supported and treated fairly
“Managers are responsible in making sure that their staff are supported and treated fairly within the work place and furthermore need to understand the impact this has on the quality and safety of the service we provide. Their role in tackling discrimination and promoting equality of opportunity is essential.”
Rationale: In common with most NHS Trusts, the NHS staff survey 2014 identified that more needed to be done to address staff concerns regarding bullying, harassment and discrimination, particularly race discrimination.
Objective 4: Optimising training “To optimise the delivery of equality and diversity training so that it supports the Trust’s objectives.”
Rationale: The Trust’s approach, in comparison with other NHS organisations, offers only very basic training regarding equality and diversity.
Details of the Trust’s work on equality and diversity is published at: www.nsft.nhs.uk > About Us > Equality
ARA2016_master 140616.indd 77 14/06/2016 11:10
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201678
2015-16 Statements of Directors’ Responsibilities in Respect of the Quality Report.
The Directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each financial year.
Monitor has issued guidance to NHS Foundation Trust Boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that NHS Foundation Trust Boards should put in place to support the data quality for the preparation of the Quality Report.
In preparing the Quality Report, Directors are required to take steps to satisfy themselves that:
• The content of the Quality Report meets the requirements set out in the NHS Foundation Trust Annual Reporting Manual 2014/15 and supporting guidance
• The content of the Quality Report is not inconsistent with internal and external sources of information including:
– Board minutes and papers for the period April 2014 to April 2015 to May 2016
– Papers relating to Quality reported to the Board over the period April 2014 to April 2015 to May 2016
– Feedback from commissioners dated May 2016
– Feedback from governors dated May 2016
– Feedback from local Healthwatch organisations dated May 2016
– Feedback from Overview and Scrutiny Committee dated May 2016
– The Trust’s complaints report published under regulation 18 of the Local Authority Social Services and NHS Complaints Regulations 2009
– The national patient survey
– The national staff survey
– The Head of Internal Audit’s annual opinion over the Trust’s control environment dated May 2016
– CQC Intelligent Monitoring Report dated November 2014
• The Quality Report presents a balanced picture of the NHS Foundation Trust’s performance over the period covered
• The performance information reported in the Quality Report is reliable and accurate
• There are proper internal controls over the collection and reporting of the measures of performance included in the Quality Report, and these controls are subject to review to confirm that they are working effectively in practice
• The data underpinning the measures of performance reported in the Quality Report is robust and reliable, conforms to specified data quality standards and prescribed definitions, is subject to appropriate scrutiny and review, and
• The Quality Report has been prepared in accordance with Monitor’s annual reporting guidance (which incorporates the Quality Accounts regulations) (published at: www.monitor.gov.uk/annualreportingmanual) as well as the standards to support data quality for the preparation of the Quality Report (available at: www.monitor.gov.uk/annualreportingmanual)
The Directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the Quality Report.
By order of the Board
Gary Page Chairman Date: 25 May 2016
Michael Scott Chief Executive Date: 25 May 2016
Quality report
ARA2016_QA section 140616 post audit.indd 78 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 79
Independent auditor’s report to the Council of Governors of Norfolk and Suffolk NHS Foundation Trust on the Quality Report.
We have been engaged by the Council of Governors of Norfolk and Suffolk NHS Foundation Trust to perform an independent assurance engagement in respect of Norfolk and Suffolk NHS Foundation Trust’s Quality Report for the year ended 31 March 2016 (the ‘Quality Report’) and certain performance indicators contained therein.
Scope and subject matter
The indicators for the year ended 31 March 2016 subject to limited assurance consist of the following two national priority indicators (the indicators):
• 100% enhanced Care Programme Approach patients receiving follow-up contact within seven days of discharge from hospital; and
• minimising delayed transfers of care.
Respective responsibilities of the directors and auditors
The directors are responsible for the content and the preparation of the Quality Report in accordance with the criteria set out in the NHS Foundation Trust Annual Reporting Manual issued by Monitor.
Our responsibility is to form a conclusion, based on limited assurance procedures, on whether anything has come to our attention that causes us to believe that:
• the Quality Report is not prepared in all material respects in line with the criteria set out in the NHS Foundation Trust Annual Reporting Manual;
• the Quality Report is not consistent in all material respects with the sources specified in the Detailed Guidance for External Assurance on Quality Reports 2015/16 (‘the Guidance’); and
• the indicator in the Quality Report identified as having been the subject of limited assurance in the Quality Report are not reasonably stated in all material respects in accordance with the NHS Foundation Trust Annual Reporting Manual and the six dimensions of data quality set out in the Guidance.
We read the Quality Report and consider whether it addresses the content requirements of the NHS Foundation Trust Annual Reporting Manual and consider the implications for our report if we become aware of any material omissions.
We read the other information contained in the Quality Report and consider whether it is materially inconsistent with:
• board minutes and papers for the period April 2015 to May 2016;
• papers relating to quality reported to the board over the period April 2015 to May 2016;
• feedback from commissioners;
• feedback from governors;
• feedback from local Healthwatch organisations;
• feedback from Overview and Scrutiny Committee;
• the trust’s complaints report published under regulation 18 of the Local Authority Social Services and NHS Complaints Regulations 2009;
• the latest national patient survey;
• the latest national staff survey;
• the 2015/16 Head of Internal Audit’s annual opinion over the trust’s control environment; and
• the latest CQC Intelligent Monitoring Report.
We consider the implications for our report if we become aware of any apparent misstatements or material inconsistencies with those documents (collectively, the ‘documents’). Our responsibilities do not extend to any other information.
We are in compliance with the applicable independence and competency requirements of the Institute of Chartered Accountants in England and Wales (ICAEW) Code of Ethics. Our team comprised assurance practitioners and relevant subject matter experts.
This report, including the conclusion, has been prepared solely for the Council of Governors of Norfolk and Suffolk NHS Foundation Trust as a body, to assist the Council of Governors in reporting the NHS Foundation Trust’s quality agenda, performance and activities. We permit the disclosure of this report within the Annual Report for the year ended 31 March 2016, to enable the Council of Governors
ARA2016_QA section 140616 post audit.indd 79 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201680
to demonstrate they have discharged their governance responsibilities by commissioning an independent assurance report in connection with the indicator. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Council of Governors as a body and Norfolk and Suffolk NHS Foundation Trust for our work or this report, except where terms are expressly agreed and with our prior consent in writing.
Assurance work performed
We conducted this limited assurance engagement in accordance with International Standard on Assurance Engagements 3000 (Revised) – ‘Assurance Engagements other than Audits or Reviews of Historical Financial Information’, issued by the International Auditing and Assurance Standards Board (‘ISAE 3000’). Our limited assurance procedures included:
• evaluating the design and implementation of the key processes and controls for managing and reporting the indicator;
• making enquiries of management;
• testing key management controls;
• limited testing, on a selective basis, of the data used to calculate the indicator back to supporting documentation;
• comparing the content requirements of the NHS Foundation Trust Annual Reporting Manual to the categories reported in the Quality Report; and
• reading the documents.
A limited assurance engagement is smaller in scope than a reasonable assurance engagement. The nature, timing and extent of procedures for gathering sufficient appropriate evidence are deliberately limited relative to a reasonable assurance engagement.
Non-financial performance information is subject to more inherent limitations than financial information, given the characteristics of the subject matter and the methods used for determining such information.
The absence of a significant body of established practice on which to draw allows for the selection of different, but acceptable measurement techniques which can result in materially different measurements and can affect comparability. The precision of different measurement techniques may also vary. Furthermore, the nature and methods used to determine such information, as well as the measurement criteria and the precision of these criteria, may change over time. It is important to read the quality report in the context of the criteria set out in the NHS Foundation Trust Annual Reporting Manual.
The scope of our assurance work has not included governance over quality or the non-mandated indicator, which was determined locally by Norfolk and Suffolk NHS Foundation Trust.
Conclusion
Based on the results of our procedures, nothing has come to our attention that causes us to believe that, for the year ended 31 March 2016:
• the Quality Report is not prepared in all material respects in line with the criteria set out in the NHS Foundation Trust Annual Reporting Manual;
• the Quality Report is not consistent in all material respects with the sources specified in the Guidance; and
• the indicators in the Quality Report subject to limited assurance have not been reasonably stated in all material respects in accordance with the NHS Foundation Trust Annual Reporting Manual and the six dimensions of data quality set out in the Guidance.
KPMG LLP Chartered Accountants 100 Botanic House, Cambridge CB2 1AR 25 May 2016
ARA2016_QA section 140616 post audit.indd 80 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 81
Statement from the Chief Executive
This time last year I described to you the challenging 12 months NSFT had just faced. I addressed how our Trust had reached its turning point, and that the commitment of our Board was for 2015-16, and beyond, to be a time of improvement.
One year on…and I feel proud to say we have delivered on our promise to focus on quality and on improving the working lives of our staff, and that we are beginning to see the early results of that progress.
It may have been another tough year, but in that time our Board has moved from expressing its disappointment at being put in special measures to looking forward to our next Care Quality Commission (CQC) inspection in the summer of 2016.
This is not because we are complacent or that we fail to recognise improvements still need to be made; it is because we feel confident that NSFT is now moving forward, and in the right direction.
And we are keeping quality as our central focus as we move into 2016-17. We recently launched our Trust Strategy incorporating our three strategic goals, setting out the blueprint for our future. Its over-arching vision is to work together for better mental health, putting recovery at the heart of everything we do so that people can live the best life they can, with or without a mental health condition.
Our priorities clearly have a quality improvement focus and can be abridged as:
Improving quality and achieving financial sustainability… by developing our leadership and management capability and retaining a skilled and responsive workforce
Working as One Trust… by sharing best practice and learning across the Trust… and making sure our values are reflected in everything we do
Focusing on prevention, early intervention and promoting recovery… maximising face-to-face clinical time… developing evidence-based clinical strategies which improve outcomes and are co-produced with service users, carers and commissioners… working with other agencies to keep people well and to support recovery
So, how do we know we are improving quality? Recently, we commissioned our own mock CQC inspection to test how much we have improved and to enable us to check our quality improvement plan remained focused on the key priorities required to provide improved services.
It was conducted by more than 50 volunteers from our staff, service users, Clinical Commissioning Groups (CCGs), Healthwatch and our governors and more than 40 clinical areas or services were inspected to a similar set of criteria as those created by CQC.
Although using similar methodology to the CQC inspections, we decided to raise the threshold for our scoring to give a clearer understanding of areas for action. So this, in effect, was a tougher testing of our services.
We were really pleased to see that we have made some significant improvements in areas where our formal CQC report raised concerns, including reducing the use of restrictive practices, prone restraint and seclusion; safer staffing levels; greater evidence of crisis plans being put in place for our service users; and improvements in the rates of risk assessment.
A summary of our Mock CQC results are:
Safe our Trust scored 77% (amber)
Effective our Trust scored 75% (amber)
Responsive our Trust scored 83% (amber)
Well-led our Trust scored 75% (amber)
Caring our Trust scored 97% (green)
Overall rating our Trust scored 78% (amber)
We have achieved the improvements we have made so far by focusing throughout 2015-16 on enhancing safety, embedding learning across the organisation, engaging more effectively with staff and service users and ensuring all of our services are of the highest quality. We’ve made a number of changes to help us achieve those goals.
We’ve opened the new 12-bed Thurne Ward at Hellesdon Hospital, which has had a huge impact on reducing out of Trust placements by ensuring people with acute mental health needs can be treated closer to home. A total of £3.6m has been invested in additional staff for both our inpatient and community services, in turn helping us achieve safer staffing levels.
A priority for us as has been engaging fully with our service users, carers and staff.
ARA2016_QA section 140616 post audit.indd 81 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201682
We worked with 1,300 individuals to draw up a set of Trust values which cement the standards of behaviour people should expect when using our services, and have also developed a new strategy to better involve service user and carers in our work and development – Improving Services Together (www.nsft.nhs.uk/improving-services-together).
Safety has been another key focus. We’ve improved training and reviewed the way we work with people who may become aggressive, in turn reducing the number of times service users need to be restrained.
A new ‘safe wards’ programme has been introduced, which is helping inpatients stay calm and reducing the chances of violent behaviour. We’ve also brought in an early warning tool in our inpatient services, which alerts staff to potential problems with workforce or patient safety, for example, so that action can be taken before the issue develops.
We have also made some significant changes to our management team, recruiting new Directors and Non-Executive Directors who have now fully bedded-in and are playing an instrumental role in driving improvements across the Trust.
Our new electronic patient record ‘Lorenzo’ was introduced in May 2015. A commentary on the implementation and some of the challenges that have arisen are provided on page 93. The challenges have resulted in some cases to a deterioration in our Trust’s reporting position for some quality indicators such as seven day follow ups and CPA reviews. We are confident, however, that the figures are improving month on month as people become more familiar with the system and this is monitored through the quality dashboard.
All of our achievements so far are a testament to the commitment and professionalism of our staff. They have played a crucial role in driving through the improvements from which our service users are now benefiting. It has been no surprise to us that the mock CQC showed ‘caring’ was still our highest marker. On behalf of the Board I’d like to acknowledge their ongoing support and dedication.
So what does 2016-17 hold for us? Despite these improvements, we are not complacent and recognise there is still further work to be done to continue embedding the high quality standards to which we all aspire across all of our services and localities.
Of course, there’s still work to be done and our Quality Improvement Plan and the Quality Goals
outlined within this Quality Account will provide the framework for our continued progress.
We know what is important and these priorities will ensure we stay on track. Some of the things we will continue to focus on in 2016-17 will include:
• Further embedding learnings from serious incidents and evidencing this
• Improving clinical supervision and mandatory training rates
• Continuing to improve the potential of the Trust’s electronic patient record – Lorenzo – to better support effective clinical practice
• Further embedding the Trust’s vision and values to help improve the culture and working environment within NSFT
All of this will take time and it won’t be easy – especially in the face of unprecedented financial pressures and increasing demands for services – but we are determined to do what we can to get our own house in order.
Managing this demand has led to an increase in waiting times but we are confident that this is managed clinically, with those people at highest risk seen first and support offered to those waiting by the Wellbeing service and the ability to contact team duty workers for help and advice.
Key to delivering further improvements will be continuing our focus on addressing the mistakes of the past, while ensuring we learn from them in the future, for the benefit of everyone who uses our services. We will continue to listen, to learn, to improve and to raise the bar on quality through 2016-17 and beyond.
We thank you for your continued support while we achieve this.
Further information:
If you would like to read our Trust’s Five-Year Strategy in full log onto our website at: www.nsft.nhs.uk/five-year-strategy
Statement of Accuracy I confirm that to the best of my knowledge, the information contained in this document is accurate. Michael Scott Chief Executive
ARA2016_QA section 140616 post audit.indd 82 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 83
Priorities for improvement in 2016-17
This is the section of the Trust’s Quality Account that looks forward to 2016-17 and identifies our goals for improvement. The rationale for why these goals have been chosen and how progress will be monitored is described. Quality Priorities for 2016-17
As our Trust continues to implement quality improvement plans (QIP) in response to the Care Quality Commission (CQC) inspection in 2014, a number of quality priorities which support that plan have been agreed. These quality priorities are also reflected in the results of the service user survey, local and national clinical audits and local feedback, including complaints and serious incident investigations. Each of these priorities will be led by an Executive Director and monitored through the project management office (PMO) to ensure progress is made. Progress will be reported to our full Board of Directors (BoD) four times a year.
Patient safety: Aim: Staff will have the confidence and tools to manage service users who self-harm, improving the service user experience. This will be measured through the number of people who attend training, a staff survey and a patient reported outcome measure, which will be developed.
Background: People who self-harm are often struggling with distress and self-harming helps them to feel in control (www.rcpsych.ac.uk). This priority will aim to increase the skills and confidence of staff to deal with this service user group and improve the experience of the service user. Lead: The Director of Nursing, Quality and Patient Safety.
Aim: For our Trust to participate in regional initiatives and develop a five year target for suicide reduction in partnership with other services. Background: About 30% of people who take their own lives in Norfolk and Suffolk
are receiving mental health services. NSFT is committed to reducing this number and to work with partners to improve the wellbeing of our communities beyond those people in formal contact with our services. We can only do this by working with partners.
Lead: The Director of Nursing, Quality and Patient Safety.
Patient experience: Aim: To raise the number of people reporting in the mandatory service user survey that they were involved, or involved to some extent in decisions about their care to above 90% in 2017.
Background: Our Trust has identified a theme in feedback and complaints that service users and carers report not being involved in decisions about their care. This is reflected in the service user survey which has remained static for the past two years (88%). Lead: The Operations Directors.
Clinical effectiveness: Aim: To ensure that 95% of service users have their capacity to consent to treatment on admission, recorded in the electronic record. Background: Inspections of MHA compliance by the CQC frequently identify that capacity has not been recorded. Staff report that capacity is assessed informally but is not recorded. This needs to improve to evidence practice. Lead: The Medical Director. Aim: To ensure that section 17 leave is managed in accordance with the Code of Practice, monitored by the MHA administration team.
a) 95% of leave authorisations are signed by the Responsible Clinician or their nominated deputy
b) 95% of leave authorisations have the parameters of the leave clearly set out
c) 95% of service users granted leave have a specific risk assessment carried out
d) 95% of service users granted leave have been given a copy of the forms or it is documented that they refused a copy
ARA2016_QA section 140616 post audit.indd 83 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201684
e) 95% of carers will be offered a copy of the forms or it is documented that the service user has denied permission Background: The MHA sets out clear requirements for the management of detained patients who are granted leave from the ward. Inspections of MHA compliance by the CQC, frequently identify that section 17 leave forms are not completed in accordance with the code of practice. This failure may increase the level of risk for the service user if staff are not able to monitor the leave.
Lead: The Medical Director (a,b,c) / Company Secretary (d,e).
Feedback on Quality Priorities 2015-16
The Quality Account published in 2015 identified four quality targets. This section demonstrates the progress that has been made in the past 12 months.
Patient safety (Reference: Quality Improvement Plan SA4)
Seclusion and restrictive interventions Use of restrictive interventions will reduce to below the national benchmarking average by 1 April 2016.
Where we were: The ‘Positive and Proactive Care’ report was published in 2014 with the requirement that trusts reduce restrictive practices. Restrictive practice refers to the restraint of patients, restraints in the face down position (prone) and the use of seclusion.
The monthly mean average for each of the three indicators in 2014-15 was:
Number of occasions where restraint was used
219
Number of seclusion incidents 61
Number of occasions when prone restraint was used
76
Where we are now: After a full 12 months since project initiation, calculations for the full year 2015-2016 from March's Quality Dashboard report demonstrated:
1) The number of recorded prone restraints average 61 per month, which is a 20% (19.7) reduction (Average 76 per month 2014-2015)
2) The number of recorded seclusion events average 52 per month, which is a 15% (14.8) reduction (Average 61 per month 2014-2015)
3) The number of recorded physical restraints average 224 per month, which is a 2% (2.3) increase (Average 219 per month 2014-2015)
Prone restraint / seclusion reductions have achieved KPI targets for the year 2015-2016. An increase in recorded physical restraints during March have caused the overall 2015-2016 average to show an increase of 2% from 2014-2015 figures.
Until March 2016 figures were included in the calculation of full year figures, a 0.5 overall reduction from April 2015 to February 2016 was demonstrated. The quality dashboard indicates that the increase in use of restraint can be linked to a small number of indiviudals who were at risk of significant harm to themselves or others during this time.
With regard to the trend for general physical restraints not achieving the KPI target, this is considered to be due to the way that general restraints have been reported. For example, within NSFT we report in line with the definition of physical restraint which will include staff providing physical care and interventions, or gently guiding service users away from situations. The majority of these occur within older persons services, which are our highest reporting areas in the use of physical restraints.
Prevention and Management of Aggression (PMA) training has recently been reviewed to provide differing levels of interventions based on Primary, Secondary and Tertiary interventions.
Going forward, incidents will be recorded using this model to enable us to provide a clearer picture of the incidents recorded as described (physical care interventions, gentle guidance of service users away from situations) within older person’s services.
All restrictive interventions will continue to be monitored via the patient safety group meeting and reported to the Board on a quarterly basis. The PMA team also have established Datix dashboards and have a practitioner monitoring activity to follow up if emerging trends or themes are noted.
ARA2016_QA section 140616 post audit.indd 84 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 85
Physical health(Reference: Quality Improvement Plan SA4)
Physical Health Check 95% of service users admitted to a ward for more than 24 hours will receive a physical health check. This will be recorded on the service user (patient) record (Lorenzo) along with any action plan if a physical health need is identified. Where we were: Physical health is an important aspect of the care of people with mental illness as research demonstrates that people with severe mental health problems have a shortened life expectancy. (No Health Without Mental Health 2011) Where we are now: Evidence from the mock CQC inspection has shown that the physical health form is now being used and there are many examples of good practice. Work continues to roll out physiological workbook training and to ensure that all areas have the equipment required. An audit undertaken in February 2016 shows that currently 90% of service users admitted to the ward receive a physical health check. This priority will remain the focus of the physical health strategy group.
Patient experience(Reference: Quality Improvement Plan RE6)
Care Plan involvement Trust service users (with Care Programme Approach entitlements) will report that they were involved in their care plans at a level at or above the national benchmarking average when the 2016 results* are published. This will be measured via the Service User Survey – ‘Have you agreed with someone from NHS mental health services what care you will receive?’ Where we were: Patient survey results 2015 identified that there had been an increase in the overall score from 5.6 to 5.8 out of a possible score of 10. But patient feedback continues to identify lack of involvement in care planning as a general theme.
Where we are now: The final CQC report for the 2015 survey indicates that the NSFT final score of 5.8 has moved our Trust from the worst performing category in 2014 to the “as expected” category.
Data shows a polarised picture with the number of people reporting they had been involved increased from 48% to 54%. The number of people reporting that they were not involved but wanted to be, also increased from 6% to 12%. Action to improve will be included in a number of initiatives including the implementation of the service user and carer strategy as well as a specific action plan in response to the final survey results.
(*Due to the delay between the sample for the survey being drawn and the survey taking place, the 2016 survey will provide the most accurate assessment of progress made.)
Clinical effectiveness(Reference: Quality improvement Plan SA9)
Learning from incidents All locality governance groups will be able to demonstrate that learning from incidents has led to changes in practice by 1 October 2015. Where we were: The CQC report identified that clinical areas were not learning from incident reports and were therefore unable to prevent similar incidents being repeated. Where we are now: A number of initiatives have been put in place to enable clinical teams to learn from incidents. This includes the five key learning points poster*, patient safety top tips booklet and regular patient safety bulletins and updates. In addition, a reflective practice group has been set up in Suffolk with plans to roll this out across the Trust following evaluation. The mock CQC inspection held in November 2015 identified that some staff are still unable to articulate changes as a result of incident reviews and team leaders have been asked to ensure that these are discussed at both team meetings and handovers to ensure all staff are aware. (*The five key learning points poster was developed as a tool to ensure teams are sharing information and learning from incidents, SIs, complaints.)
ARA2016_QA section 140616 post audit.indd 85 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201686
Statements of Assurance from the Board
The wording in the following statements is required in the DoH regulations for producing Quality Accounts. The statements are required nationally to enable the public to compare the performance of individual trusts and are therefore common across all Quality Accounts. We have tried to provide some explanation of the terms used in the key, but if you would like any further explanation, please contact the Patient Advice and Liaison Service (PALS) on Freephone 0800 279 7257. Review of services
During 2015-16 NSFT provided and / or subcontracted eight NHS services: adult services, children’s services, drug and alcohol services, improving access to psychological therapies (IAPT), learning disability services and older people’s services. The Trust also provides forensic
and Tier 4 Child and Adolescent Mental Health Services (CAMHS) commissioned by NHS England rather than local CCGs. The Trust has reviewed all the data available on the quality of care in all of these services. The income generated by the NHS services reviewed in 2015-16 represents 93.2% of the total income generated from the provision of NHS services by the Trust for 2015-16. The quality of care the Trust has provided has been reviewed in a number of ways. This is via the collection of systematic performance data against Monitor, CQC and CCG quality targets as well as clinical audits, surveys, analysis of complaints and serious incident data, and informal feedback from service users and carers. However data is gathered, the Trust system of meetings ensures that it is reported, and that action plans for improvement are put in place where needed. Information is cascaded to all levels of the organisation via locality leadership and clinical and management supervision.
Data type Lead Reported to Action
Clinical Audit
Audit lead
Quality Governance Committee
Action plan developed and implemented by clinical team.
This is then monitored by the audit department and a re-audit undertaken as indicated to demonstrate that the plan has improved the service.
Locality governance dashboards incorporating audit compliance and audit results databases are updated monthly and shared with localities to enable them to compare their performance with other areas and to see, at a glance, where further action is required.
Complaints Complaints Manager
Quality Governance Committee
Action plan developed and implemented by relevant manager.
Where there is learning for other areas, the action plan is shared through a variety of mechanisms, including access to the plan and the production of themes that are shared with all areas, policy amendments and adjustments to training packages.
Feedback from visits
Executive and Non-executive Directors
Modern Matrons and Ward Managers
Action plan developed to resolve any issues that arise.
Feedback
Head of Governance
Quality Governance Committee
Quality improvement visits carried out by clinicians, governors, commissioners and partner agency representatives.
(QA1) Quality of care review methods
ARA2016_QA section 140616 post audit.indd 86 14/06/2016 10:27
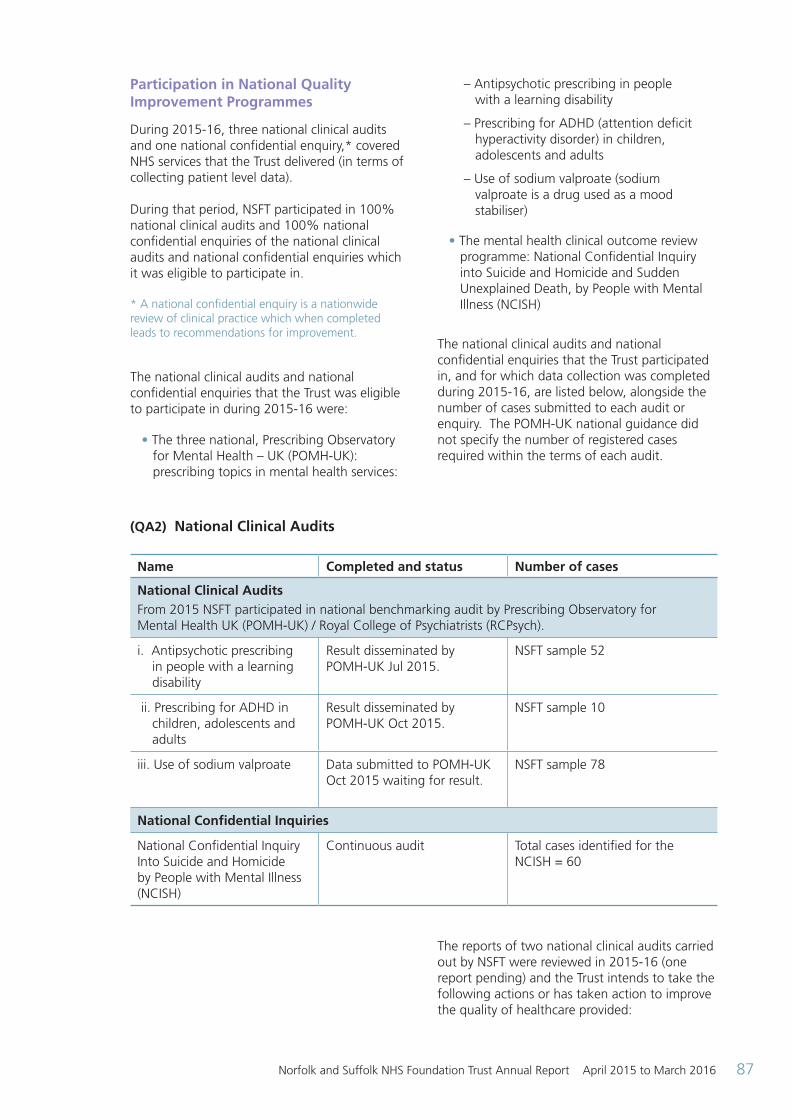
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 87
Participation in National Quality Improvement Programmes
During 2015-16, three national clinical audits and one national confidential enquiry,* covered NHS services that the Trust delivered (in terms of collecting patient level data). During that period, NSFT participated in 100% national clinical audits and 100% national confidential enquiries of the national clinical audits and national confidential enquiries which it was eligible to participate in. * A national confidential enquiry is a nationwide review of clinical practice which when completed leads to recommendations for improvement. The national clinical audits and national confidential enquiries that the Trust was eligible to participate in during 2015-16 were:
• The three national, Prescribing Observatory for Mental Health – UK (POMH-UK): prescribing topics in mental health services:
– Antipsychotic prescribing in people with a learning disability
– Prescribing for ADHD (attention deficit hyperactivity disorder) in children, adolescents and adults
– Use of sodium valproate (sodium valproate is a drug used as a mood stabiliser)
• The mental health clinical outcome review programme: National Confidential Inquiry into Suicide and Homicide and Sudden Unexplained Death, by People with Mental Illness (NCISH)
The national clinical audits and national confidential enquiries that the Trust participated in, and for which data collection was completed during 2015-16, are listed below, alongside the number of cases submitted to each audit or enquiry. The POMH-UK national guidance did not specify the number of registered cases required within the terms of each audit.
The reports of two national clinical audits carried out by NSFT were reviewed in 2015-16 (one report pending) and the Trust intends to take the following actions or has taken action to improve the quality of healthcare provided:
(QA2) National Clinical Audits
Name Completed and status Number of cases
National Clinical AuditsFrom 2015 NSFT participated in national benchmarking audit by Prescribing Observatory for Mental Health UK (POMH-UK) / Royal College of Psychiatrists (RCPsych).
i. Antipsychotic prescribing in people with a learning disability
Result disseminated by POMH-UK Jul 2015.
NSFT sample 52
ii. Prescribing for ADHD in children, adolescents and adults
Result disseminated by POMH-UK Oct 2015.
NSFT sample 10
iii. Use of sodium valproate Data submitted to POMH-UK Oct 2015 waiting for result.
NSFT sample 78
National Confidential Inquiries
National Confidential Inquiry Into Suicide and Homicide by People with Mental Illness (NCISH)
Continuous audit Total cases identified for the NCISH = 60
ARA2016_QA section 140616 post audit.indd 87 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201688
(QA3) Actions following Audit
Prescribing Observatory for Mental Health - UK: prescribing topics in mental health services (2015-16)
Audits reported in 2015 Actions in progress
i. Antipsychotic prescribing in people with a learning disability
NSFT performed above national average in 2 of total 5 parameters but required improvement in 3 - monitoring EPS*, obesity and hypertension. The Audit Lead, LD Consultant will be providing training and education to the team and raising awareness.
(*EPS = Extrapyramidal side effects, a group of side effects associated with antipsychotic medications.)
ii. Prescribing for ADHD in children, adolescents and adults
The Audit Lead will: • Feedback the results to the team
• Provide training and awareness to improve prescribing, a programme is being rolled out which will include postgraduate training and MDT (multi-disciplinary team)
• Monitoring potential adverse effects of the drugs prescribed
iii. Use of sodium valproate Results of the audit are expected in March 2016.
Trust Clinical Audit Programme
The reports of 70 local clinical audits were reviewed by the provider in 2015-16 and NSFT intends to take the following actions to improve the quality of healthcare provided in relation to the five audit topics selected:
(QA4) Actions following Audit
Audit Title Actions Taken
Antimicrobial Prescribing Prior to March 2015 NSFT did not meet the three required standards for antimicrobial prescribing. Following the audit in March 2015, an action plan was prepared to improve prescribing which included:
• Dissemination of the audit results with team / ward level data as widely as possible
• The results of the audit as well as importance of meeting prescribing standards was included in the mandatory doctors’ induction and medication update training, delivered by the pharmacy team
continued over >
ARA2016_QA section 140616 post audit.indd 88 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 89
The pharmacy led re-audit of antimicrobial prescribing in Nov 2015 showed significant improvement in the prescribing standards of antimicrobials and met all three key standards in over 75% of prescriptions. A programme of re-audit will monitor improvements in prescribing standards.
Delivering Planned Physical Health Care The baseline audit reported that 91% compliance was reached.
As a result the physical health team have:
• Developed long term conditions guidance notes that are available to support staff in completing a relevant intervention plan for chronic health conditions
• Locality physical health nurses, will focus on supporting staff to implement appropriate care plans
• A second round of audit in March 2016 to monitor efficacy of actions in achieving the 95% target as set in the Quality Priorities
Fundamental Aspects of Care – Quarterly Matrons’ Audit of Inpatient Care
Quarterly Modern Matrons’ audits monitor clinical areas to gain insight into compliance with key areas of ‘The Fundamental Aspect of Care’ (FAC). Results of these audits influence action planning and set priorities for improvement.
In 2015-16 Matrons focused on improving the documentation of patient engagement, including recording the physical health and physical observations of the patient on admission (using the Trust-wide standardised format).
Physiological workbook training is progressing with an anticipated completion date for inpatient staff of September 2016, and a completion date of January 2017 for community staff.
Monitoring of High-Dose Antipsychotic Therapy
The pharmacy team produced Trust guidelines on prescribing High-Dose Antipsychotic Therapy (HDAT) requiring:
• Physical health monitoring and regular reviews
• The use of ‘alert stickers’ on the drug charts
• HDAT discussion is now part of induction and mandatory training
• Wall poster from POMH-UK to all teams as a part of raising awareness
• The pharmacy team are collecting data this year between 7 and 18 March which will inform further actions
ARA2016_QA section 140616 post audit.indd 89 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201690
Medical Staff audits Medical staff have completed many audits throughout the year, and participated in Trust-wide audits.
Topics have included:
• Involving patients in decisions about prescribed medicines and supporting adherence
• Smoking cessation
• Monitoring obesity
• Memory clinic practice
• Driving and dementia
Each audit has resulted in relevant actions for improvement.
The Trust participates in the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness as previously documented, with excellent compliance scores. Should the Trust have a serious incident resulting in a child’s death or near miss, this would be referred to the Norfolk and Suffolk Safeguarding Children’s Boards for consideration under the Serious Case Review (SCR) guidance as outlined in Working Together to Safeguarding Children 2015, and be reported in the three-year national report. For the period being looked at there have been two SCRs involving children known to the Trust in Norfolk, and to which the Trust contributed as part of the management review. As a member of the Norfolk and Suffolk Safeguarding Child and Adult Boards, the Trust will take account of all recommendations arising from SCRs and Safeguarding Adult Reviews (SAR’s), regardless of whether or not Trust services were involved. The Trust participated in an Adult SAR involving two adults known to Suffolk services, and a further joint Suffolk and Norfolk Adult SAR related to a service user known to the Trust in both counties.
Research
420 patients receiving NHS services provided or sub-contracted by the Trust from April 2015 to March 2016 were recruited during that period to participate in research approved by a research ethics committee. NSFT Research was shortlisted in the HSJ Awards for ‘Clinical Research Impact’, which recognised the efforts of the Trust to embed research into clinical practice. Part of the initiatives developed include an online research referral resource, a research training and forum online centre, and a weekly e-newsletter ‘Research Matters’ which is
accessible by all staff. Through the training and opportunities for research in the Trust, multiple NSFT staff members have been accepted onto funded development pathways in research, including MScs in clinical research, research fellowships and PhDs. 2015 also saw the launch of NSFT’s research development programme, which will strategically develop new research and evaluation projects in key clinical services through a collaboration with academic, clinical, third-sector and service user and carer (inspire group) partners. The ultimate aim of the programme is to inform the quality of treatments and services through evidence-based practice and research.
Commissioning and Quality Innovation Goals (CQUIN) agreed with commissioners
A proportion of the Trust’s income in 2015-16 was conditional on achieving quality improvement and innovation goals agreed between the Trust and any person or body with which it entered into a contract, agreement, or arrangement for the provision of NHS services, through the Commissioning for Quality and Innovation (CQUIN) payment framework. The Trust has a contract with Central Norfolk* CCG, West Norfolk CCG, Ipswich and East Suffolk CCG, West Suffolk CCG and Cambridge and Peterborough CCG for the provision of mental health services to the population of Norfolk and Suffolk, and with NHS England (specialist) Commissioning Group for the provision of low and medium secure services and Tier 4 Child and Adolescent Mental Health Service.
ARA2016_QA section 140616 post audit.indd 90 14/06/2016 10:27
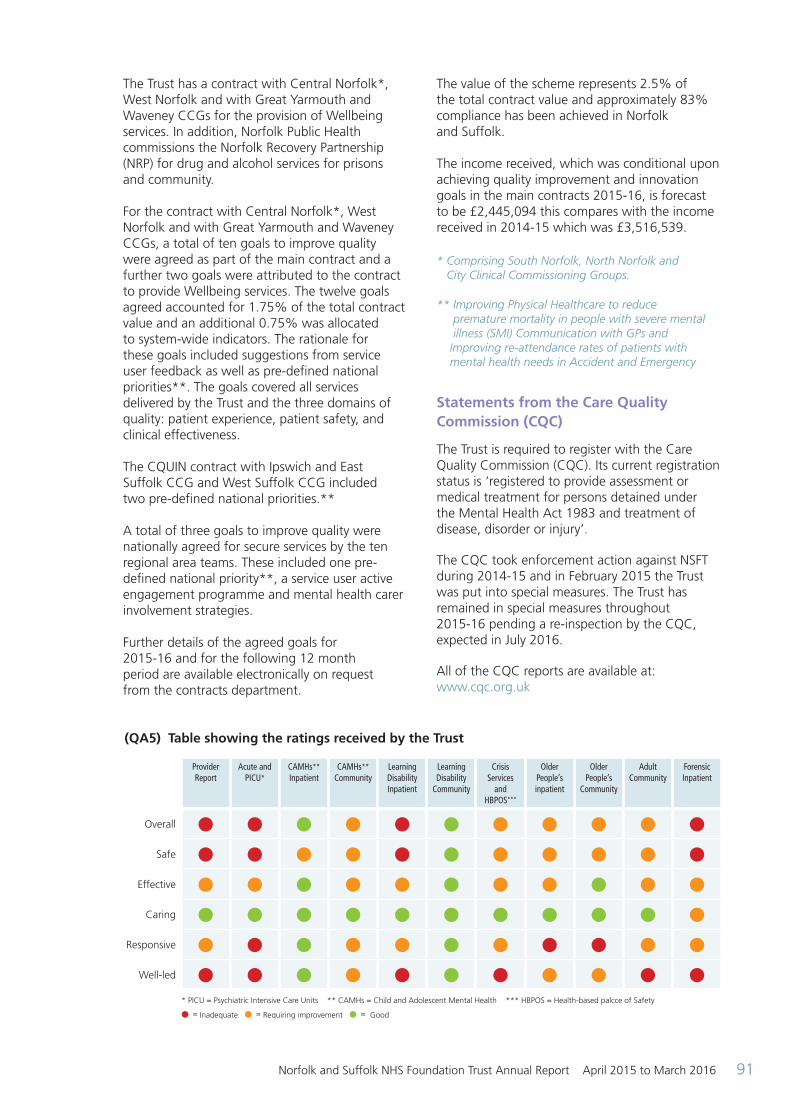
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 91
The Trust has a contract with Central Norfolk*, West Norfolk and with Great Yarmouth and Waveney CCGs for the provision of Wellbeing services. In addition, Norfolk Public Health commissions the Norfolk Recovery Partnership (NRP) for drug and alcohol services for prisons and community. For the contract with Central Norfolk*, West Norfolk and with Great Yarmouth and Waveney CCGs, a total of ten goals to improve quality were agreed as part of the main contract and a further two goals were attributed to the contract to provide Wellbeing services. The twelve goals agreed accounted for 1.75% of the total contract value and an additional 0.75% was allocated to system-wide indicators. The rationale for these goals included suggestions from service user feedback as well as pre-defined national priorities**. The goals covered all services delivered by the Trust and the three domains of quality: patient experience, patient safety, and clinical effectiveness. The CQUIN contract with Ipswich and East Suffolk CCG and West Suffolk CCG included two pre-defined national priorities.** A total of three goals to improve quality were nationally agreed for secure services by the ten regional area teams. These included one pre-defined national priority**, a service user active engagement programme and mental health carer involvement strategies. Further details of the agreed goals for 2015-16 and for the following 12 month period are available electronically on request from the contracts department.
The value of the scheme represents 2.5% of the total contract value and approximately 83% compliance has been achieved in Norfolk and Suffolk. The income received, which was conditional upon achieving quality improvement and innovation goals in the main contracts 2015-16, is forecast to be £2,445,094 this compares with the income received in 2014-15 which was £3,516,539. * Comprising South Norfolk, North Norfolk and City Clinical Commissioning Groups.
** Improving Physical Healthcare to reduce premature mortality in people with severe mental illness (SMI) Communication with GPs and Improving re-attendance rates of patients with mental health needs in Accident and Emergency
Statements from the Care Quality Commission (CQC)
The Trust is required to register with the Care Quality Commission (CQC). Its current registration status is ‘registered to provide assessment or medical treatment for persons detained under the Mental Health Act 1983 and treatment of disease, disorder or injury’.
The CQC took enforcement action against NSFT during 2014-15 and in February 2015 the Trust was put into special measures. The Trust has remained in special measures throughout 2015-16 pending a re-inspection by the CQC, expected in July 2016.
All of the CQC reports are available at: www.cqc.org.uk
(QA5) Table showing the ratings received by the Trust
Provider Report
Acute and PICU*
CAMHs** Inpatient
CAMHs** Community
Learning Disability Inpatient
Learning Disability
Community
Crisis Services
and HBPOS***
Older People’s inpatient
Older People’s
Community
Adult Community
Forensic Inpatient
Overall l l l l l l l l l l l
Safe l l l l l l l l l l l
Effective l l l l l l l l l l l
Caring l l l l l l l l l l l
Responsive l l l l l l l l l l l
Well-led l l l l l l l l l l l * PICU = Psychiatric Intensive Care Units ** CAMHs = Child and Adolescent Mental Health *** HBPOS = Health-based palcce of Safety
l = Inadequate l = Requiring improvement l = Good
ARA2016_QA section 140616 post audit.indd 91 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201692
A quality improvement plan was developed in response to the inspection findings and is being monitored by the Trust Board and reviewed at monthly meetings with Monitor* and the CQC. Regular updates are published on the NHS Choices website which demonstrates many actions are already complete. Some longer term actions are under way and will be complete within the next two to three months. Some examples are reported in the Quality Initiative section on page 93. The Trust has not been eligible for any special reviews or investigations by the CQC during 2015-16. During 2015-16, the CQC undertook a number of visits to the Trust to check compliance with the Mental Health Act for people detained. A number of themes were identified and these are being addressed as part of the QIP and monitored through the production of a ‘heatmap’ which shows areas of non-compliance. This shows:
• Improvements made in the recording of patients consent across all clinical areas
• Although the figures show an improving trend there are still concerns and ongoing issues with the reading of patient’s rights under the MHA and the documentation of these being revisited at timely intervals
• All areas score highly on Section 17 leave forms being valid and present, but these being signed by patients along with patients and nearest relative / carers receiving copies remain as issues to address
*Monitor is the regulator for Foundation Trusts
Data quality
NSFT will be taking the following actions to improve data quality. Excellent data quality is essential to the delivery of excellent quality care. NSFT will continue to ensure data quality improvements are made to support services through provision of easily accessible performance reporting through Abacus and MIS, the Trust’s business intelligence reporting systems, overseen by the Data Quality Group.
These systems provide daily updates which are accessed by business support staff. Any data quality issues can be passed to the appropriate staff member for correction. A monthly data quality meeting is held and attended by a wide range of staff to discuss data quality issues, new updates, where applicable, and Information Standards Board changes which may affect reporting and therefore data quality. Data quality is also mentioned in staff job descriptions, ensuring that staff are held accountable for the quality of the data that they submit. NSFT submitted records during 2015-16 to the Secondary Uses Service for inclusion in the Hospital Episode Statistics which are included in the latest published data. The percentage of records in the published data:
• Which included the patient’s valid NHS number was 98.66% for admitted patient care:
– Not applicable for outpatient care
– Not applicable for accident and emergency care
• Which included the patient’s valid General Medical Practice Code was 99.2% for admitted patient care:
– Not applicable for outpatient care
– Not applicable for accident and emergency care
NSFT information governance assessment reports the overall score for 2015-16, submitted in March 2016, was 84% and was graded ‘satisfactory’ under national information governance rules. Action plans are being developed with regards to those requirements that did not achieve Level 3. This is monitored at the Information Governance Group with the expectation that these improvements will be in place before the next submission due in March 2017. The Information Governance Risk Register, and also information governance related incidents that are reported through the Trust Datix reporting system, are continuously reviewed and reported quarterly to the Information Governance Committee for action.
ARA2016_QA section 140616 post audit.indd 92 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 93
The information quality and records management attainment levels assessed within the information governance toolkit provide an overall measure of the quality of data systems, standards and processes within an organisation. Further details on information governance can be found at: www.commissioningforhealth.nhs.uk The Trust was not subject to the payment by results clinical coding audit during 2015-16 by the Audit Commission.
Quality initiatives This section summarises quality information specific to Norfolk and Suffolk NHS Foundation Trust. Key performance and developments during 2015-16
This section allows our Trust to highlight quality matters from 2015-16 in more detail or that have not been addressed elsewhere in the report.
The examples are reported as part of the five domains measured by the CQC. n Safe
Seclusion Care Planning Tool
A Seclusion Care Planning Tool has been developed in response to the care planning needs of service users who have been secluded and the requirements of the MHA Code of Practice. This has been developed on Lark Ward, at the Woodlands Unit, in Ipswich, and made available to all staff via Lorenzo, our electronic patient record. This form prompts attention to particular areas of practice that protect the rights and wellbeing of service users who have been secluded and contributes to the management of restrictive practice. Ligature management
The CQC reports highlighted the number of ligatures in ward areas across NSFT. Our Trust has put in place a programme to remove ligatures and where that is not possible, to ensure staff know how to mitigate any remaining risks.
Safewards Safewards is a model developed by Len Bowers, Professor of Psychiatric Nursing at King’s College London. Its key principals are:
• Making psychiatric wards more peaceful places
• Better relationships between patients and staff
• Increasing safety, reducing coercion
• Fewer assaults, fewer injuries
• Less time spent on containment, more invested in engagement
As Safewards is a two-year national model, the 2015-16 CQUIN focused on the planning, preparation and organisational embedding of the model ahead of implementation in year two (2016-17). The Modern Matrons, supported by link staff throughout each participating service, have led this 2015-16 CQUIN.
Robust planning, as well as staff and service user engagement, will support the successful implementation of the model. The expected outcomes will provide an improved therapeutic environment, which should reduce conflict and have a positive impact on reducing incidents and improving patient experience. n Effective
Lorenzo
In May 2015 NSFT introduced Lorenzo – a single electronic patient record (EPR).
The introduction has been a significant challenge with the need for training and the change from a number of other electronic systems as well as paper records. There have also been a number of issues identified with the system performance and familiarisation with the new processes.
NSFT has expressed its dissatisfaction with the performance of the system to CSC, the system provider and both CSC and the HSCIC, a body that manages the contract on behalf of the Department of Health, have apologised for the poor service. Assurances have been given that they are working to resolve the issues and that this is a “top priority”.
ARA2016_QA section 140616 post audit.indd 93 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201694
Despite the issues that have affected the system nationally, Lorenzo is already helping to improve:
• Patient safety – reduced clinical risk of fragmented health records and staff have easy and timely access to all patient information
• Operational efficiency – reduced duplication of data entry
• Standardisation – there are now Trust-wide processes and procedures allowing best practice and guidance to be shared
• Reporting – whilst the team are addressing some of the data quality issues as part of the transition, a single data source will ultimately enable us to improve accuracy and to better support service design and performance / contractual management
• System management – replacing multiple systems with a single system is more cost effective and easier to maintain and support
• Mobile working – staff using Trust laptops now have direct access to clinical notes
n Caring
The Green Light Tool Kit
The Green Light Toolkit from the National Development Team for Inclusion is a guide to auditing and improving mental health services to meet the needs of people with learning disabilities (LD) and autism. The toolkit identifies 27 standards to ensure reasonable adjustments are in place to provide fair and equitable services.
The implementation of the Green Light standards will form the basis of the NSFT LD / Autism strategy. The strategy group re-launched in January 2016 will develop a strategy in line with Norfolk and Suffolk County Councils, CCGs and LD Partnership Boards.
For NTDi Green Light Toolkit information: http://www.ndti.org.uk/major-projects/current/green-light-toolkit-2013/
A ‘Green Light Champion’ in each team will promote best practice and ensure reasonable adjustments are in place within teams to meet service users’ needs. Champions will receive effective support through the Green Light Champions Network. As of February 2016, there are 48 Green Light Champions within the Trust.
Accessible information NSFT is obliged to comply with the new statutory NHS England ‘accessible information standards’ which means that all teams will be required to provide service users with information in a format they require, such as different languages, easy read or accessible versions. A task and finish group has been set up to ensure the requirements of the Green Light Toolkit are met and this will also ensure compliance with Monitor’s requirements, the Autism Act (2009) and Equality Act (2010). Work is underway to develop a policy, easy read appointment letters and easy read versions of Trust leaflets.
n Responsive
New recruits to the council of governors
A number of new people have joined our Trust’s Council of Governors and this includes two governors who ensure that young people’s voices are heard and their needs are taken into account when planning for the future. Female only lounges Building work has now started for completion in June, to provide female only lounges for Poppy and Avocet wards at the Woodlands site in Ipswich, to promote privacy and dignity. n Well-led
Visions and values The Putting People First (PPF) initiative set out to engage with staff, service users, and carers to develop the Trust values and behaviours (see ‘Positively... Respectfully... Together...’ graphic on page 95). Firstly, by holding a number of listening sessions throughout the Trust, 1,300 people shared their views. From these sessions the new NSFT values and behaviours were co-created. Currently the PPF team is undertaking the next phase, to work with key leaders and managers to embed the values at team level and influence a change in the culture of the organisation. Quality dashboard
NSFT has developed a quality dashboard which provides month on month statistics to demonstrate quality metrics. The dashboard provides an ‘at a glance’ position and is available on our Trust website.
ARA2016_QA section 140616 post audit.indd 94 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 95
National recognition
Psychiatric Liaison Accreditation Network (PLAN) The West Suffolk Psychiatric Liaison Team has achieved accreditation with PLAN.
The Team takes referrals from all inpatient departments of the West Suffolk Hospital and emergency referrals presenting via A&E, providing assessment, risk management and onward referrals for service users. The standards have helped develop and shape the team in addition to enhancing relationships with acute hospital colleagues. Accreditation assures patients, carers, frontline staff, commissioners, managers and regulators that the liaison service is of a good quality and that staff are committed to improving care. Meeting accreditation targets helps meet other priorities too, including national initiatives.
Open Mind initiative
The Open Mind initiative was recognised in the ‘equality and diversity in service delivery’ category of the National Positive Practice in Mental Health Awards 2015. NSFT was one of
just three trusts to be shortlisted for the award from a field of 14 entries. Open Mind’s aim has been to give diverse local communities a chance to make their voices heard so that services can be shaped to meet their specific needs, in turn helping to break down some of the inequalities which can make it more difficult for people to access care.
As part of the project, community and voluntary organisations and members of the BME (Black Minority Ethnic) community took part in workshops to help NSFT understand the issues which are important to carers and service users. This includes piloting cultural awareness training and development courses for staff which will then be evaluated to assess the impact this has on patient care. Other key concerns highlighted by the project, including service delivery, feedback and access to services will also be investigated further by the group.
Following its success in Suffolk, the next step will be to roll out the project across Norfolk.
Working together for better mental health
Be proactive... Look for solutions, think creatively and focus on what we can do
Take pride... Always do our best
Take responsibility... Plan ahead, be realistic and do what we say we will
Support people to set and achieve goals... And be the best they can
Recognise people... Their efforts and achievements, and say thank you
Value everyone... Acknowledge people’s unique experiences, skills and contribution
Step into other people’s shoes... Notice what’s actually happening
Take time to care... Be welcoming, friendly and support others
Be professional… Respect people’s time and beaware of our impact
Be effective... Focus on the purpose and keep it as simple as possible
Involve people... Make connections and learn from each other
Share... Knowledge, information and learning
Keep people updated... With timely, open and honest communication
Have two-way conversations... Listen and respond
Speak up... Seek, welcome and give feedback
Positively... Respectfully... Together...
ARA2016_QA section 140616 post audit.indd 95 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201696
Trust doctor shortlisted for national psychiatry award A senior specialist trainee in psychiatry at NSFT was shortlisted as one of four finalists for a national award in the Royal College of Psychiatrists Awards 2015. Dr Yasir Hameed, who is in specialist training in General Adult and Old Age Psychiatry at the Trust, was nominated for the Higher Psychiatric Trainee of the Year award, which recognises a high level of achievement over and above that expected for their grade.
NHS England e-Prescribing Digital Maturity NSFT along with a number of Trusts including those within the Carter Programme* have completed the e-Prescribing** digital maturity model.
NSFT ranked 8th place out of 45 participating trusts in its readiness for and uptake for e-Prescribing.
The mean average total maturity score was 17%, and NSFT scored 33%.
(*Carter Programme – From Lord Carter’s review of NHS acute hospitals, its recommendations include the 2018 deadline for trusts to have fully integrated systems for e-Rostering*** and e-Prescribing**). **e-Prescribing is a way for your prescribers (a doctor or other health professionals legally allowed to write prescriptions) to send your prescriptions electronically and directly to the pharmacy).
***e-Rostering supports management of clinical services aiding safer staffing levels. It also provides a mechanism for recording working hours, leave and absence for all staff including those in support areas such as HR, ICT and Finance.
Quality indicators Seven Day Follow Up This indicator is described as “The percentage of patients on CPA who are followed up within seven days after discharge from psychiatric inpatient care”.
NSFT considers that this data is as described for the following reasons:
• NSFT has robust systems in place to check the quality of data
• Data is submitted to commissioners where it is scrutinised and challenged where necessary
NSFT has taken the following actions to improve this percentage, and so the quality of its services, by:
• Business Support Managers check the systems and liaise with clinical staff to check any data that appears to be outside normal parameters
• Data is discussed at local management groups as well as Trust-wide performance groups
The latest available data produced by NHS England shows that the national average score for the period October to December 2015 was 96.9%. The highest performing area scored 100% and the lowest area scored 96.9%.
(QA6)
Prescribed information
Related NHS Outcomes framework domain
2013-14 2014-15 2015-16
The percentage of patients on CPA who were followed up within seven days after discharge from psychiatric inpatient care.
This is a national definition reported to Monitor.
Target 95%
Preventing people from dying prematurely.
Enhancing quality of life for people with long term conditions.
97.89% 98.57% 89.42%
ARA2016_QA section 140616 post audit.indd 96 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 97
Access to CRHT This indicator is described as “The proportion of inpatient admissions gate kept by the crisis resolution home treatment teams”. NSFT considers that this data is as described for the following reasons:
• NSFT has robust systems in place to check the quality of data
• Data is submitted to commissioners where it is scrutinised and challenged where necessary
The latest available data produced by NHS England shows that the national average score for the period October to December 2015 was 97.4%. The highest performing area scored 100% and the lowest area scored 24.6%.
Readmission rates
NSFT considers that this data is as described for the following reasons:
NSFT has taken the following actions to improve this percentage, and so the quality of its services, by:
• Business Support Managers check the systems and liaise with clinical staff to check any data that appears to be outside normal parameters
• Data is discussed at local management groups as well as Trust-wide performance groups
• NSFT has robust systems in place to check the quality of data
NSFT has taken the following actions to improve this percentage, and so the quality of its services by:
• Ensuring that discharge planning is robust and that the discharge policy is followed
• Ensuring patients receive a follow up visit within 7 days of discharge and telephone contact within 48 hours of discharge
(QA7)
Prescribed information Related NHS Outcomes framework domain
2013-14 2014-15 2015-16
The percentage of admissions to acute wards for which CRHT acted as gatekeeper.
This is a national definition reported to Monitor.
Target 95%
Enhancing quality of life for people with long term conditions.
99.69% 97.46% 60.62%
(QA8)
Prescribed information Related NHS Outcomes framework domain
2013-14 2014-15 2015-16
The percentage of patients
aged 0-15
16 or over
readmitted to a hospital which forms part of the Trust within 28 days of being discharged from a hospital which forms part of the Trust.
Helping people to recover from episodes of ill health or following injury.
5.9%**
5.3%
** The number of
readmissions refers to the specialist tier
4 CAMHS unit
No re-
admissions
7.87%
No re-
admissions
8.33%
ARA2016_QA section 140616 post audit.indd 97 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 201698
Staff Survey
The national NHS Staff Survey is a mandatory requirement for NHS organisations, with results being used by NSFT to understand the views of its staff and to inform improvements in the workforce arena. The most recent survey took place in September to October 2015, with results published on 23 February 2016.
(QA9)
Prescribed information Related NHS Outcomes framework domain
2013 2014 2015
Staff employed by, or under contract to, the Trust during the reporting period who would recommend the Trust as a place to work or receive treatment. National average: 3.63 Top scoring Trust: 4.04*
(The scores achieved are from a maximum possible score of five)
Ensuring that people have a positive experience of care.
3.06 3.01 3.11
NB: It should be noted that the question has changed slightly in 2015 and the scores reported in 2013 and 2014 have been adjusted to show the weighted scores, enabling comparison with other Trusts.
NSFT considers that this data is as described for the following reasons: • Building on the approach from last year, NSFT again undertook a survey of all staff in order to get feedback from as many staff as possible. This re-enforced the principle established within the ‘Putting People First’ project of actively listening and engaging with all staff. Overall, compared with last year, NSFT’s response rate increased from 36% to 52%. This increase is higher than the in-year national increase (2%) and higher than the overall national response rate of 46%
• Whilst recognising the poor results from last year, NSFT is again disappointed by the results, especially when compared with the national average scores. The results, however, do highlight that our Trust has improved in a number of key areas. Where we can directly compare year-on-year there is a positive shift in the right direction, with an improvement in seven of the key findings in our results since 2014
NSFT is taking the following actions to improve this percentage, and so the quality of its services, by:
• Engaging independent consultants to work with NSFT to find out more about our leadership climate that focuses on how it feels to be managed in our Trust so that the Trust can focus on in shaping a supportive and engaged leadership culture
• Reviewing its clinical strategy and actively pursuing responsibilities and accountabilities framework to support this
• A Trustwide workforce and organisational development strategy underpinned by three main pillars of activity:
1. Engaged Workforce
2. Skilled Workforce
3. Responsive Workforce
ARA2016_QA section 140616 post audit.indd 98 14/06/2016 10:27
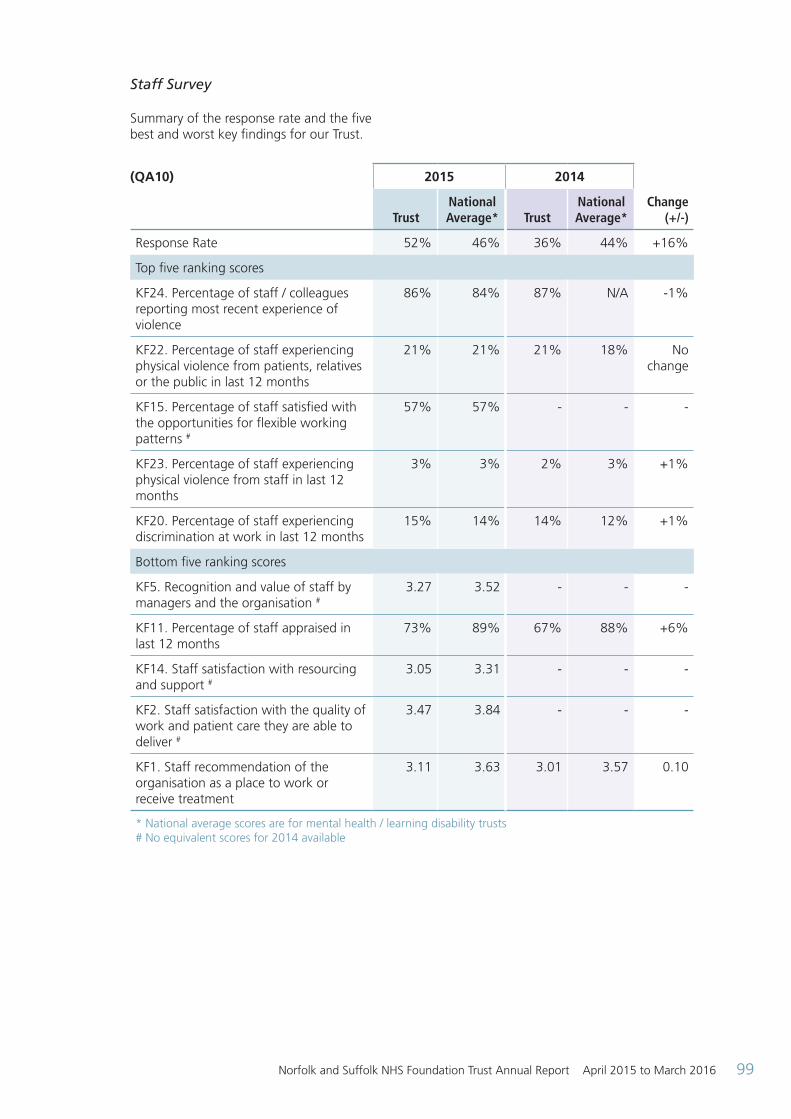
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 99
Staff Survey
Summary of the response rate and the five best and worst key findings for our Trust.
(QA10) 2015 2014
Change (+/-)Trust
National Average* Trust
National Average*
Response Rate 52% 46% 36% 44% +16%
Top five ranking scores
KF24. Percentage of staff / colleagues reporting most recent experience of violence
86% 84% 87% N/A -1%
KF22. Percentage of staff experiencing physical violence from patients, relatives or the public in last 12 months
21% 21% 21% 18% No change
KF15. Percentage of staff satisfied with the opportunities for flexible working patterns #
57% 57% - - -
KF23. Percentage of staff experiencing physical violence from staff in last 12 months
3% 3% 2% 3% +1%
KF20. Percentage of staff experiencing discrimination at work in last 12 months
15% 14% 14% 12% +1%
Bottom five ranking scores
KF5. Recognition and value of staff by managers and the organisation #
3.27 3.52 - - -
KF11. Percentage of staff appraised in last 12 months
73% 89% 67% 88% +6%
KF14. Staff satisfaction with resourcing and support #
3.05 3.31 - - -
KF2. Staff satisfaction with the quality of work and patient care they are able to deliver #
3.47 3.84 - - -
KF1. Staff recommendation of the organisation as a place to work or receive treatment
3.11 3.63 3.01 3.57 0.10
* National average scores are for mental health / learning disability trusts # No equivalent scores for 2014 available
ARA2016_QA section 140616 post audit.indd 99 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016100
Future Priorities and Targets
• As set out under the commentary on page 98 improving workforce engagement is one of the three strategic workforce priorities
• Supporting strategies for the Workforce and Organisational Development Strategy in regard to each of the priority areas: engaged workforce, skilled workforce and responsive workforce
• The focus areas for the staff engagement strategy are embedded above, which includes promoting a safe and healthy working environment
• In addition to the Trust-wide approach to improving staff engagement, existing Locality Workforce Plans will be reviewed to respond to area specific priorities highlighted by the staff survey results
• NSFT is committed to making improvements across all key findings as benchmarked against previous staff survey results and other mental health trusts. Progress will be monitored taking account of the measures set out under the commentary above
• Further information about the survey, and a full breakdown of results, can be accessed via a dedicated website on: http://www.nhsstaffsurveys.com
Community Service User Survey
NSFT considers that this data is as described for the following reasons:
• The Trust commissions an outside agency, Quality Health, which is an ‘approved provider’ to undertake the survey
NSFT has taken the following actions to improve this percentage, and so the quality of its services, by:
• Each locality analysing their data and identifying where issues are incorporated within their Quality Improvement Plans. Where issues are not covered in Quality Improvement Plans specific plans are to be developed to improve the service user experience. These action plans are monitored at locality governance meetings and the Quality Governance Committee
• It should be noted that the sample is drawn from service users accessing services before the results of the previous survey are known. We would therefore not expect to see any improvements as a result of the action plan in the next survey
(QA11)
Prescribed information Related NHS Outcomes framework domain
2013 2014 2015
The trust “patient experience of community mental health services” indicator score with regard to a patient’s experience of contact with a health or social care worker.
Enhancing quality of life for people with long-term conditions.
Ensuring that people have a positive experience of care.
8.6 7.5 7.4
Range of scores: 6.8-8.2 The scores achieved are from a maximum possible score of ten.
ARA2016_QA section 140616 post audit.indd 100 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 101
Incident reporting NSFT considers that this data is as described for the following reasons:
• NSFT is identified through the NRLS as one of the highest reporters of incidents which staff report via the Datix system
• All incident reports are reviewed by the risk management team and clinical managers are required to investigate and sign off each incident before closing the event
• Health, safety and security audits are carried out on all Trust premises which include a review of incident reporting trends
• These are subject to discussion at the Patient Safety Group and Health and Safety Committee meetings
NSFT has taken the following actions to improve this percentage, and so the quality of its services, by:
• Encouraging staff to report all incidents and continues to develop and roll out Datix dashboards to provide clinical managers with a live overview of the reported incidents in their area. This enables them to monitor for themes and trends and make early changes to practice where required
• Incidents are reviewed by the Patient Safety Group to identify themes and patterns, working with clinical areas and stakeholders, such as the Police, to implement changes where required
• Serious incidents are managed in accordance with national guidance
ARA2016_QA section 140616 post audit.indd 101 14/06/2016 10:27
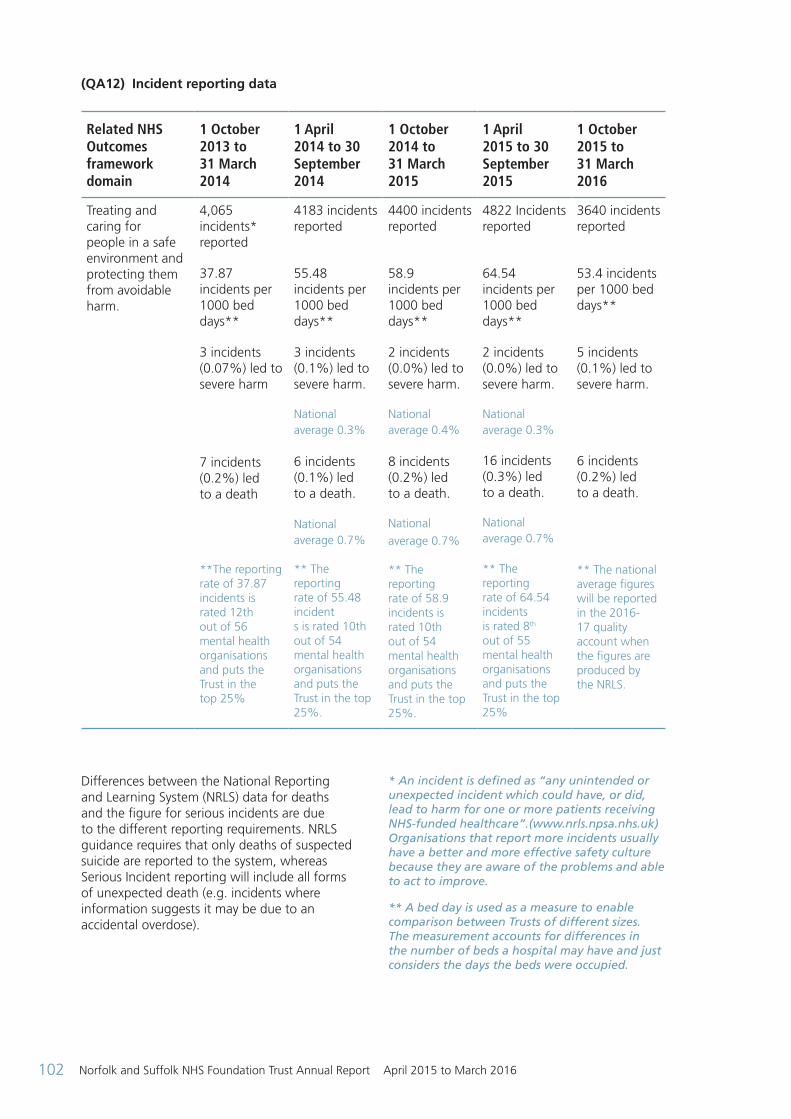
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016102
Differences between the National Reporting and Learning System (NRLS) data for deaths and the figure for serious incidents are due to the different reporting requirements. NRLS guidance requires that only deaths of suspected suicide are reported to the system, whereas Serious Incident reporting will include all forms of unexpected death (e.g. incidents where information suggests it may be due to an accidental overdose).
* An incident is defined as “any unintended or unexpected incident which could have, or did, lead to harm for one or more patients receiving NHS-funded healthcare”.(www.nrls.npsa.nhs.uk) Organisations that report more incidents usually have a better and more effective safety culture because they are aware of the problems and able to act to improve.
** A bed day is used as a measure to enable comparison between Trusts of different sizes. The measurement accounts for differences in the number of beds a hospital may have and just considers the days the beds were occupied.
(QA12) Incident reporting data
Related NHS Outcomes framework domain
1 October 2013 to 31 March 2014
1 April 2014 to 30 September 2014
1 October 2014 to 31 March 2015
1 April 2015 to 30 September 2015
1 October 2015 to 31 March 2016
Treating and caring for people in a safe environment and protecting them from avoidable harm.
4,065 incidents* reported
37.87 incidents per 1000 bed days**
3 incidents (0.07%) led to severe harm
7 incidents (0.2%) led to a death
**The reporting rate of 37.87 incidents is rated 12th out of 56 mental health organisations and puts the Trust in the top 25%
4183 incidents reported
55.48 incidents per 1000 bed days**
3 incidents (0.1%) led to severe harm.
National average 0.3% 6 incidents (0.1%) led to a death. National average 0.7% ** The reporting rate of 55.48 incident s is rated 10th out of 54 mental health organisations and puts the Trust in the top 25%.
4400 incidents reported
58.9 incidents per 1000 bed days**
2 incidents (0.0%) led to severe harm.
National average 0.4% 8 incidents (0.2%) led to a death.
National
average 0.7% ** The reporting rate of 58.9 incidents is rated 10th out of 54 mental health organisations and puts the Trust in the top 25%.
4822 Incidents reported
64.54 incidents per 1000 bed days**
2 incidents (0.0%) led to severe harm.
National average 0.3%
16 incidents (0.3%) led to a death.
National average 0.7% ** The reporting rate of 64.54 incidents is rated 8th out of 55 mental health organisations and puts the Trust in the top 25%
3640 incidents reported
53.4 incidents per 1000 bed days**
5 incidents (0.1%) led to severe harm.
6 incidents (0.2%) led to a death.
** The national average figures will be reported in the 2016-17 quality account when the figures are produced by the NRLS.
ARA2016_QA section 140616 post audit.indd 102 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 103
(QA13)
Key Performance Indicator 2012-13 2013-14 2014-15 2015-16
Patient Safety
Seven-day follow up of service users following their discharge from inpatient services. Target 95%
95.9% 97.89% 98.57% 89.42%
Absconsions of detained patients from Adult wards as a ratio of 100 detained patients. Target 4.1
7.61 7.31 5.72 8.16
Ratio of inpatient serious untoward incidents (e.g. suicide) per 10,000 occupied bed days. Target 3.8
2.74 2.74 4.19 3.40
Clinical Effectiveness
Access to crisis resolution and home treatment services. Target 95%
92.40% 99.69% 98.92% 60.62%
Delayed transfers of care, relating to other support needs (like housing) following discharge from hospital. Target <7.5%
4.55%
The increased numbers of
delayed transfers are attributable to a reduction
in capacity and funding in social care. The
number remains within target.
4.80% 4.61% 3.39%
Readmission rates
Age 0-15
Age 16+
No admissions
6.2%
5.9%*
5.3%
No readmissions
7.87%
No readmissions
8.33%
Patient Experience
CPA patients having formal review within 12 months. Target 95%
97.55% 98.05% 96.71% 69.24%
Waiting times. The number of people waiting 18 weeks or greater.
99 72 78 280
Number of under-18 year old admissions to adult acute ward.
15 17 12 5
Number of under-16 year old patients admitted to adult acute wards. Target 0
0 0 0 0
Meeting commitment to serve new psychosis cases by early intervention teams. Target 95%
137.65% 131.76% 118.24%
ARA2016_QA section 140616 post audit.indd 103 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016104
Evaluation of patient safety
NSFT continues to report all serious incidents on receipt of an initial report. This is reported as good practice by the National Patient Safety Agency.
The latest report from the National Reporting and Learning System for the period 1 April 2015 to 30 September 2015 shows that NSFT is the 8th highest reporter of all 55 mental health trusts in that period.
(QA14) Comparative reporting rate per 1,000 bed days for 55 MENTAL HEALTH organisations
Org
anis
atio
ns
Reporting Rate (per 1,000 bed days)n Your organisation’s report rate n Highest 25% of Reporters n Middle 50% of Reporters n Lowest 25% of Reporters
0 10 20 30 40 50 60 70 80 90
The median reporting rate for the is cluster is 38.62 incidents per 1,000 bed days. Organisations that report more incidents usually have a better and more effective safety culture. You can’t learn and improve if you don’t know what the problems are.
Are you actively encouraging reporting of incidents?
The comparative reporting rate summary shown below provides an overview of incidents reported by NHS organisations to the National Reportig and Learning System (NRLS) occuring between 01 April 2015 to 30 September 2015. Your organisation reported 4,822 incidents (rate of 64.54*) during this period.
Figure 1: Comparative reporting rate per 1,000 bed days for 56 MENTAL HEALTH organisations
ARA2016_QA section 140616 post audit.indd 104 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 105
Infection Prevention and Control (IPAC) activities
The IPAC annual work plan is devised to identify and implement activity which will deliver the priorities described in key documents and guidance, including: the Health and Social Care Act 2008 (rev.2010), CQC Regulation 12 objective 8, national best practice standards. The completion of the IPAC annual work plan is overseen by the IPAC Committee, the Quality Governance Committee and the Trust Board.
Key achievements resulting from implementation of the IPAC plan for 2015-16 have been:
• NSFT staff succeeded in maintaining a low rate of Health Care Acquired Infections (HCAI); there were no cases of methicillin resistant Staphylococcus aureus (MRSA) blood stream infection, one case of Clostridium difficile infection was attributed to our Trust. There have been no outbreaks of confirmed viral gastrointestinal infection during the period, although several potential clusters of cases were investigated.
• To support the IPAC team NSFT operates a system of link infection control practitioners known as Local Infection Prevention and Control Supporters (LIPACS). Eighty LIPACS attended the annual education and training programme to enable them to more effectively monitor and manage their environment and support local staff. The LIPACS have additionally completed a programme of audits to demonstrate compliance with key policies, and address deficits.
• The IPAC team has successfully introduced a new system of auditing for hand hygiene practice and theory.
• The IPAC team has continued to build on improvements in mandatory training compliance. A new bespoke e-learning package developed collaboratively with the University of East Anglia has been made available for inductees and existing staff throughout NSFT.
The priorities for the forthcoming year include: The service delivery arrangements for infection prevention and control were revised during
2015. The priority for the team is the effective delivery of a comprehensive annual programme.
Key areas of focus within the programme:
• Strengthening the role of the LIPACS within clinical teams to continue embedding good infection control practices into every aspect of NSFT
• Improving compliance with mandatory education in IPAC procedures through a range of learning and assessment opportunities
• To continue to work closely with staff in all settings regarding management of alert organisms with particular reference to MRSA, C. difficile, Norovirus and emerging antibiotic resistant organisms
• Improved focus to ensure actions identified by audit are implemented and completed
Physical health
Our Physical Health Strategy Group (PHSG), which includes representatives from all localities and staff groups within our Trust, aims to improve the focus on physical health throughout NSFT. The group reports to the Quality Governance Committee and to the Trust Board.
Key achievements this year have been:
• Completion of and implementation of Physical Health Observation RCN accredited training course and package of learning, delivering training to localities in both inpatient and community settings.
• Opportunities for all staff to undertake education and training appropriate to the needs of their service. Further supported by enhanced training by wound care and continence specialists.
• Commencement of simulation training to staff including doctors, utilising a simulation man funded by monies from Health Education East. A training room environment is in development ready for scenario training.
• The appointment of Physical Health Nurses in many localities and the introduction of Locality Physical Health groups in Suffolk East, Suffolk West, Great Yarmouth and Waveney and Secure Services discussing locality issues and influencing decisions on strategy through representation on the PHSG.
ARA2016_QA section 140616 post audit.indd 105 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016106
• Developed best practice care plans for patients with long-term conditions to ensure standardised care interventions, with recommended appropriate actions for patients with chronic diseases.
• Developed physical health forms for use with Lorenzo to improve data quality collection and the monitoring of health changes. Providing evidence of actions taken where physical health problems have been identified.
• Accessible standardised formularies for wound care and continence products to enhance and streamline appropriate effective use of clinical products.
• Engagement with community teams to support implementation of the national Rethink tool ‘My Physical Health’ as a document for raising and addressing physical health issues.
Sign Up to Safety plan
The Sign up to Safety campaign supports the ambition of the Secretary State for Health of halving avoidable harm in the NHS over the next three years. The campaign aims to incorporate three key principles to improve patient safety:
• Listen – to patients/carers and staff
• Learn – from what they say when things go wrong
• Act – take action to improve patient safety when things go wrong.
By making the commitment in Signing up to Safety NSFT will:
• Put safety first – committing to reduce avoidable harm within NSFT, making both the safety goals and plans available to the public
• Continually learn from safety incidents and share that learning to prevent similar occurrences – by developing a culture of learning and development that strengthen NSFT’s ability to safety and risk
• Promote an open and honest culture for those who work in our services and use our services – by being transparent with both those who use our services, work in our services and supporting people if something goes wrong
• Collaborate – with services and teams to ensure learning is shared
• Provide support to individuals to understand why things go wrong and how to put them right and also celebrate improvements
NSFT has identified five key initiatives to improve safety and have set the following ambitions for each of the priorities:
The five safety priorities
• Reduce the number of restrictive interventions used within NSFT by 25% by 2018
• Reduce the number of assaults by 25% within NSFT by 2018
• That no falls result in severe harm
• Provide an environment that reduces the risk of harm so that all inpatient areas comply with current same sex accommodation standards and all ligature points are removed or mitigating actions put in place
• To ensure NSFT embeds a safety culture based on openness, transparency and learning from previous incidents that have caused harm. This ensures that individuals feel supported and safe to report incidents and when things go wrong and improvements are made to prevent future occurrence
The safety improvement plans for each of these ambitions have been developed and align and cross reference to NSFT’s Quality Improvement Plan (QIP), and identify specific goals for years 1-3. While there is clear commitment, drive and energy to achieve the ambitions, the reality is that there will still be situations where things may go wrong. NSFT commits that in these cases, we will continue to utilise these experiences to learn and continuously improve services.
Positive and proactive care
In April 2014 the DoH published the report ‘Positive and Proactive Care’ focusing on the need to reduce the use of restrictive interventions (restraint) by staff in mental health trusts.
‘Restraint’ describes any restrictive intervention involving direct physical contact where the intervener’s intention is to prevent, restrict, or subdue movement of the body, or part of the body of another person.
NSFT has a positive reporting culture and reports approximately an average of 1358 incidents a
ARA2016_QA section 140616 post audit.indd 106 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 107
month and is consistently within the top quartile of Mental Health Trust reporting incidents via the NRLS system. See QA14 on page 104.
The graph below demonstrates the use of restraint across all localities and services for 2014-15 and this data has been used to establish a benchmark.
(QA15) Total restraints 2014/15
The benchmarking data has been used to establish a 25% reduction in the use of restraint within NSFT during the next three years. The target for 2015-16 is a reduction of 10% and this is reported on page 118.
Evaluation of clinical effectiveness
The implementation of NICE guidance and adopting nationally agreed best practice is central to ensuring good quality outcomes for patients.
NICE guidance published since April 2015 included:
• Medications – technology appraisals are discussed by our Drug and Therapeutics Committee to make sure that such medicines are available when recommended by the prescriber
• New guidance on medicines optimisation, challenging behaviour and learning disabilities, and antimicrobial stewardship
were reviewed with Trust leads, reported to Clinical Cabinet for consideration and actions agreed to implement where appropriate
• Violence, comprehensive review of new guidelines on the management of violence led to review of our rapid tranquillisation policy, the development of an e-learning tool as well as plans to monitor use of rapid tranquillisation across our wards and audit practice against NICE standards during 2016
NSFT is also now registered as a stakeholder in the development of several new NICE guidelines giving us the chance to be involved in their development.
The NSFT audit schedule includes audits that measure compliance against the NICE guidance and best practice, for example screening for delirium, psychological therapy for Post Traumatic Stress Disorder (PTSD) and prescribing for rapid tranquillisation. Where non-compliance is identified by the team, an action plan to improve is implemented. NSFT also participates in national POMH-UK audits which measure prescribing against NICE standards. All NICE audit reports are reviewed at Clinical Cabinet.
Monitor identifies a number of measures of clinical effectiveness including access to crisis resolution and home treatment teams before a person is admitted to hospital, and ensuring service users are followed up within seven days of discharge from an inpatient ward. These are reported to Monitor and NSFT is disappointed to report a reduction in performance this year. The quality dashboard continues to show a month on month improvement and it is hoped that our Trust will be able to demonstrate compliance in 2016-17 as staff become more familiar with the Lorenzo reporting system.
Evaluation of patient experience
Service user and carer involvement
NSFT values the role played by service users and carers who engage in a number of ways to provide feedback and contribute to improvements. NSFT has groups for adult mental health service users and carers across the region, in West Norfolk, City and South Norfolk, North Norfolk, Great Yarmouth and Waveney, East Suffolk and West Suffolk. The groups are open to people who are using or who have used mental health services and their carers.
n Suffolk Specialist Servicesn Secure Services n East Suffolk Locality n Central (Older Persons) n Central Cluster (Adult) n West Suffolk Locality
n Gt Yarmouth and Waveney (Older Persons) n Gt Yarmouth and Waveney (Adult) n West Norfolk (Adult) n Gt Yarmouth and Waveney (CAMHS) n West Suffolk (Older Persons)
600
400
200
0
No
of
rest
rain
ts
NSFT clinical teams
ARA2016_QA section 140616 post audit.indd 107 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016108
Service users and carers from our locality groups play an important role in influencing developments within our Trust and are actively involved in the interview process for appointing new staff.
Service user and carer forums and meetings
These groups take place across NSFT and are open to people who have accessed or are accessing services, and their carers.The groups provide an opportunity for service users and carers to use their lived experiences in further developing services and working with locality staff to improve services locally.
It is important to note that in Great Yarmouth and Waveney our Trust delivers its service user and carer forum in conjunction with Feedback, a local service user led forum. Joint forums are held monthly and to date, services users have been able to hear about the new Wellbeing Service and the Recovery College.
Other service user and carers initiatives for 2015-16
• Service users and carers continue to be involved in the interview process for appointing new staff
• Service user and carer involvement in co-producing a new course for our Recovery College on an ‘Introduction to Involvement and Participation’
• Service users involved working with local CCGs on an asset-based community development project
Triangle of Care
Our Trust has been successful in attaining their first gold star in relation to work on the Triangle of Care.
NSFT joined the Triangle of Care membership scheme in 2014 and as a requirement in the first year inpatient services must begin to bench mark their services in relation to carer involvement. We were able to evidence this, along with action plans and were accredited with our star as evidence of better joined up working with carers.
Locality services are working with service users and carers to monitor the Triangle of Care implementation via local steering groups.
As part of NSFT’s ongoing work to implement the Triangle of Care:
• East Suffolk service users and carers involved in developing a carer awareness DVD for our staff teams to use to develop staff awareness with regard to carers support
• West Suffolk and Norfolk Central Acute Services have co-developed other training that is being delivered across our Trust to promote working with carers and effective communication. The training is delivered by our staff, service users and carers
• Carer lead posts recruited across NSFT to support carers needs and ensure their involvement
Service User and Carer Involvement Strategy A project group, incorporating representatives from our Trust-wide forums, service user and carer governors, members of the Board of Directors, NSFT staff and stakeholders, has developed a new service user and carer involvement strategy called ‘Improving Services Together’.
• A steering group, which has representation from carers, service users, governors and Healthwatch, has been formed to develop and explore ways in which the commitments of the strategy can be implemented. One locality has been identified as a pilot site to trial the new structure
• In parallel to the development of a structure, all six commitment work streams have begun to meet and consider the delivery of the detail specified in all of the actions
• Discussions have begun with members of the ABCD Project, to consider the integration of project work with the proposed structure. CCG have expressed a positive interest in how we begin integration
The above detail gives full consideration to the quality objectives specified in the service user and carer involvement strategy. The strategy was officially launched at the Trust’s Annual General Meeting (AGM) in October, where service users and a carer were able to talk about their experience of being involved in developing the strategy and the difference it will make to the services they use.
ARA2016_QA section 140616 post audit.indd 108 14/06/2016 10:27
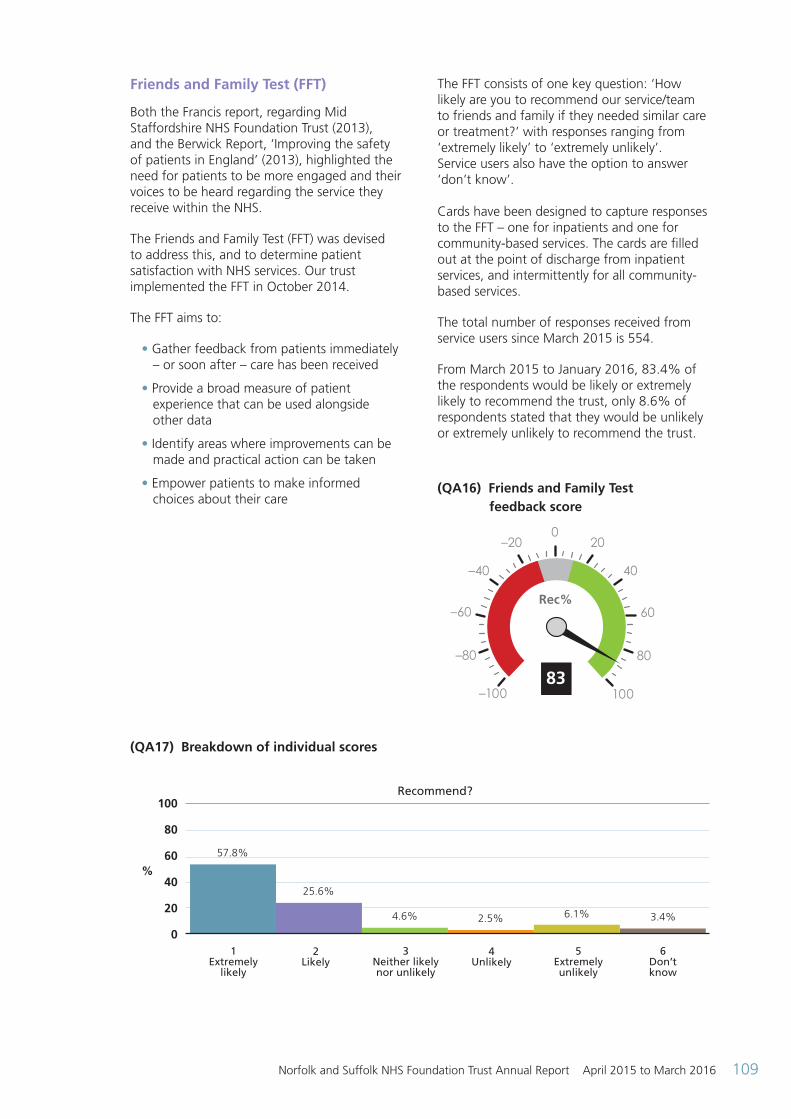
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 109
Friends and Family Test (FFT)
Both the Francis report, regarding Mid Staffordshire NHS Foundation Trust (2013), and the Berwick Report, ‘Improving the safety of patients in England’ (2013), highlighted the need for patients to be more engaged and their voices to be heard regarding the service they receive within the NHS.
The Friends and Family Test (FFT) was devised to address this, and to determine patient satisfaction with NHS services. Our trust implemented the FFT in October 2014.
The FFT aims to:
• Gather feedback from patients immediately – or soon after – care has been received
• Provide a broad measure of patient experience that can be used alongside other data
• Identify areas where improvements can be made and practical action can be taken
• Empower patients to make informed choices about their care
The FFT consists of one key question: ‘How likely are you to recommend our service/team to friends and family if they needed similar care or treatment?’ with responses ranging from ‘extremely likely’ to ‘extremely unlikely’. Service users also have the option to answer ‘don’t know’. Cards have been designed to capture responses to the FFT – one for inpatients and one for community-based services. The cards are filled out at the point of discharge from inpatient services, and intermittently for all community-based services.
The total number of responses received from service users since March 2015 is 554.
From March 2015 to January 2016, 83.4% of the respondents would be likely or extremely likely to recommend the trust, only 8.6% of respondents stated that they would be unlikely or extremely unlikely to recommend the trust.
(QA16) Friends and Family Test feedback score
83
Rec%
020–20
–40
–60
–80
–100 100
40
60
80
(QA17) Breakdown of individual scores
100
80
60
40
20
01
Extremely likely
2 Likely
3 Neither likely nor unlikely
4 Unlikely
5 Extremely unlikely
6 Don’t know
Recommend?
57.8%
25.6%
4.6% 2.5% 6.1% 3.4%
%
ARA2016_QA section 140616 post audit.indd 109 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016110
Some comments received:
“Staff are so caring, working hard to look after my father who has dementia – they are calm and reassuring”
“The people I have had contact with have been friendly, helpful and professional”
“The service is overwhelmed, which is a result of the 'open door' policy where any person can self-refer in”
“Painfully slow and inefficient from the first contact to triage to initial assessment onwards”
NSFT is disappointed with the low numbers of responses to the FFT and will explore ways of increasing the feedback. This is however only one source of feedback and the trust also reviews comments on NHS Choices, complaints and compliments and other feedback surveys to inform improvements.
The information being received from the FFT is being used as part of the wider Trust strategy to incorporate service user feedback into tangible changes to clinical services. Some examples of service user feedback having direct impact on service provision include:
Northgate acute ward Weekly community meeting is held on the ward where patient feedback is gathered, as a result the following changes have been made.
• More fresh fruit is made available throughout the day
• Laundry baskets are now provided in the laundry room
• Extra relaxation classes have been provided
• A discharge pack is currently being developed
Child Family and Youth Pathway (CFYP) - west Norfolk
Service users from CFYP surveyed the waiting area and recommended changes to the environment which have now been implemented. This includes:
• The door to be painted bright yellow
• New curtains and furnishings for the family therapy area
Waveney ward
Service users stated that the physical environment was drab and uninviting. Charitable funds were used to purchase some large pictures for the lounge area.
Hammerton Court
One patient noted that his bed was too narrow and it was confirmed that the beds are approximately 2” smaller than a standard divan. It was then arranged for this service user to trial a different type of bed.
Carer information booklet has been reviewed by carers and additional information included.
Secure Services
Following patient feedback regarding the décor and furnishings of the family room, new furniture has been ordered.
Serious incidents (SIs)
Our Trust continues to report serious incidents (SI) in accordance with national guidance.
From April 2015 to March 2016, 216 SIs (including seven which were voided following receipt of more information) were reported by NSFT. The SIs involved service users who were accessing a range of inpatient and community services across NSFT.
Our Trust uses Root Cause Analysis methodology to consider the timeline and factors that influenced an incident. Through group review the analysis identifies learning actions. A number of serious incidents have strengthened oversight through the engagement of Executive and Non-Executive Directors in setting the terms of the investigation and agreeing the final report.
Learning from serious incidents plays a critical role in developing services and was reported within the CQC inspection in 2015. Using this feedback our Trust has been developing ways to share learning through a number of actions. These include a bi-monthly Patient Safety Newsletter and Managers Bulletin to highlight key messages from Root Cause Analysis reports. In addition, NSFT has implemented ‘key learning’ and ‘top ten policy’ posters as practical ways for teams to influence
ARA2016_QA section 140616 post audit.indd 110 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 111
learning specific to their area. Locally, some community teams have introduced monthly protected time sessions for specific discussion on Serous Incidents and the learning taken from these.
Complaints
Our Trust is committed to using complaints to learn and improve our services. Our Trust considers complaints in an open and transparent way. At the time of reporting (April 2016), our Trust had received 592 complaints during April 2015 – March 2016 (608 in 2014-15). The majority of complaints related to “clinical treatment” (39 %), followed by “values and behaviours (of staff)” (17%).
At the time of reporting 526 complaints have been responded to. Of these complaints 19% were upheld, 40% were partially upheld and 41% were not upheld by our Trust. 14% of complaints were stood down for reasons including the service user not providing consent to a complaint being made on their behalf, complainant not confirming the details of their complaint and the complaint was found to refer to another agency.
NSFT has been informed that following the response to a complaint, 12 complainants requested review of their complaint by the Parliamentary and Health Service Ombudsman. The Ombudsman requested information from our Trust to assist their investigation.
During this year NSFT has recognised the time taken to respond to complaints can be in excess of our 30 working day target. With this in mind, a Complaints Manager has been appointed to further support all complaints to be responded to in a thorough and timely manner. Our Complaints Manager will also be providing all complaints investigators with refreshed complaints handling training, to support a consistent approach to dealing with complaints across our Trust.
NSFT’s Patient Advice and Liaison Service (PALS) continues to be available to provide support to service users, carers and members of the general public who seek to find information or to resolve their concerns without the desire or need to use the complaints procedure.
Duty of Candour
NSFT continues to apply the Duty of Candour in accordance with statutory and contractual direction. Promoting a greater openness and candour when safety incidents occur our Trust applies a number of actions including notifying an individual or their representative when an incident of moderate harm or above occurs. There follows a discussion of the incident with an apology for its occurrence. Where identified, further investigation is undertaken with the intention to maximise learning which is then confirmed with the individual or their representative. These actions are confirmed in writing. Staff training was offered during the implementation and a plan for training updates is being formulated to be delivered later this year.
Patient Led Assessments of the Care Environment (PLACE)
PLACE assessments take place annually, and results are reported publicly to help drive improvements in the care environment across the NHS and show how providers are performing against their peers both nationally and locally.
PLACE assessments were undertaken across nine inpatient sites and involved staff, current service users, ex-service users, carers, Healthwatch and Governors to assist with the audits.
NSFT performed as follows:
There are five main areas of assessment (Cleanliness; Food; Privacy Dignity and Wellbeing; Condition Appearance and Maintenance and Dementia Needs); however, the Food element has an overall score but is also split into Organisational Food, covering the general provision and food service, and Ward Food which covers the actual quality, taste, aroma and texture.
ARA2016_QA section 140616 post audit.indd 111 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016112
Criteria NSFT Score 2015 National Average Score 2015
Cleanliness 99.38% 97.57%
Food 92.90% 88.49%
Organisational Food 91.55% 87.21%
Ward Food 92.56% 89.27%
Privacy Dignity and Wellbeing 91.82% 86.03%
Condition Appearance and Maintenance 97.34% 90.11%
Dementia 78.49% 74.51% NSFT has scored above average in all domains
NSFT individual site scores attained were as follows:
(QA19) 2014 2015 2014 2015 2014 2015 2014 2015
Overall ward org
Overall ward org
Overall ward org
Overall ward org
Overall ward org
Overall ward org
Overall ward org
Overall ward org
LocationCleanliness Food Organisational
FoodWard Food
Wedgwood 99.94% 99.94% 86.7% 97.91% 95.14% 100%
Carlton Court 99.48% 99.69% 96.2% 93.55% 92.26% 94.34%
Fermoy Unit 99.03% 99.41% 90.0% 93.88% 89.52% 96.41%
Hellesdon Hospital 99.11% 99.30% 95.15% 93.80% 92.40% 94.54%
Woodlands 99.95% 99.75% 87.05% 86.11% 88.75% 83.95%
Foxhall House 100% 85.64% 94.04% 79.11%
The Julian Hospital 99.95% 98.78% 93.5% 96.17% 90.21% 99.60%
The Norvic Clinic 99.66% 98.76% 93.77% 91.25% 91.44% 91.15%
Northgate Hospital 99.06% 99.45% 95.06% 92.55% 90.21% 99.39%
Location
Privacy, Dignity and Wellbeing
Condition, appearance and
maintenance
Dementia
Wedgwood 85.85% 89.48% 90.35% 98.55% 97.00%
Carlton Court 92.06% 90.68% 99.62% 96.69% 97.88%
Fermoy Unit 81.67% 85.74% 98.36% 98.59%
Hellesdon Hospital 91.12% 91.99% 99.03% 97.87%
Woodlands 86.86% 93.69% 97.76% 93.41% 92.93%
Foxhall House 85.35% 93.55%
The Julian Hospital 91.83% 92.42% 99.35% 99.36% 95.31%
The Norvic Clinic 95.11% 94.29% 99.72% 98.28%
Northgate Hospital 87.38% 94.25% 99.18% 98.59%
(The blue sections identify areas not reported on in 2014-15)
(QA18)
ARA2016_QA section 140616 post audit.indd 112 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 113
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
0 1 2 3 4 5 6 7 8 9 10
It is worth noting that whilst we have scored well on food provision in most cases, we will always score lower with a cook chill food service because the scoring is weighted towards the NHS promotion of traditionally cooked food.
At individual site level, the scores indicate we have areas to improve on, around the quality of some food dishes, standards of cleaning, internal and external maintenance. These areas are being supported to ensure these are resolved and current standards maintained.
Service user survey The CQC requires trusts to undertake national service user surveys each year and this survey involved 55 mental health NHS trusts.
The 2015 survey questionnaire was substantially redeveloped and updated in order to reflect changes in policy, best practice and patterns of
service. New questions have been added to the questionnaire, and existing questions modified. This means that for all questions, the results from the 2015 survey are not comparable with the results from previous surveys.
Community survey
A response rate of 31% was achieved – the national average was 29%.
Further information about the survey can be accessed via the CQC website on http://www.cqc.org.uk/content/community-mental-health-survey-2015 or type ‘service user survey’ into the CQC website search box.
This national survey enables NSFT to be benchmarked against other mental health trusts. The survey questions are grouped into nine sections and the table below shows our Trust scores compared to other mental health trusts.
These results are subject to an action plan which was developed by the Senior Managers Forum, which will continue to monitor progress, and also locality-based action plans which will be monitored within the locality governance meeting.
(QA20) Section scores
♦ denotes the Trust’s position within the above ratings
Best performing trusts
About the same
Worst performing trusts
S1. Health and social care workers
S2. Organising care
S3. Planning care
S4. Reviewing care
S5. Changes in who people see
S6. Crisis care
S7. Treatments
S8. Other areas of life
S9. Overall views of care and services
S10. Overall experience
ARA2016_QA section 140616 post audit.indd 113 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016114
Commissioners and stakeholder comments
The comments received from commissioners and stakeholders are appreciated by the Trust and are used to inform and improve subsequent accounts. In some cases where minor changes are suggested, these have been incorporated for this year but in other cases, where more substantial changes are suggested, these have not been included but will inform change next year. It should also be noted that the Quality Account will be published separately and the layout will change accordingly.
NSFT Governors
The governors acknowledge receipt of Norfolk and Suffolk Foundation Trust’s 2015-2016 Quality Accounts. We appreciate the opportunity to review in detail the data for the quality of services and care provided by NSFT. We note that the Quality Accounts are presented in an easily accessible document which refers to data compiled around the safety and clinical effectiveness of services provided by NSFT together with recorded surveys about the experience of users of Trust services.
Inevitably, this year’s Quality Accounts focus, not only on mandatory data, but also on the requirements of CQC to improve quality in areas highlighted in last year’s inspection, and in preparation for CQC’s forthcoming inspection. The governors acknowledge that tremendous effort has been put into improving services within a challenging financial vista. We note the attention to eradicating ligature points, and providing same sex facilities. Also, Governors acknowledge the efforts in Commissioning Quality Innovation goals (CQUIN) alongside challenging cost improvement programmes (CIPs). We note the Trust’s efforts to improve quality and leadership by involving modern matrons in the design and management of services. Governors acknowledge the Trust has met targets to reduce the use of restrictive practices, including prone restraint, seclusion, and risk assessment. Also, we appreciate that the Trust is focusing on improving crisis planning for its service users. We support the continued emphasis on physical health for Trust service users and look forward to the Trust achieving its target in this area of 95 percent.
Of note is the continuing good work of staff in relation to ‘caring’ which has a ‘green’ rating in accordance with the CQC score board. We look forward to continuing improvements in the scores achieved in the realms of safety, effectiveness, responsiveness, and the leadership of the Trust, which received an amber rating in the Trust’s mock CQC results.
Governors are concerned that there has been a dip in seven-day followups after discharge. Waiting times still are a cause for concern. We are aware that in part this might be attributed to challenges from a Trust wide increase in referrals, a large proportion of which are do not meet the criteria for secondary care but still involve assessment time. We are pleased that the Trust is examining assessment criteria in Norfolk to bring it into line with those of Suffolk. The implementation of Lorenzo has not been problem free, but governors observe that the Trust is monitoring and working to improve Lorenzo’s usability and effectiveness, and future potential. The introduction of E-rostering has been a cause for concern among some staff.
Much effort has been put into Trust vision and values and improving staff morale with the initiative Putting People First but there is a perception that past operational upheavals continue to affect staff wellbeing.
We congratulate the efforts of staff to give of their best at all times, even though the staff survey results were disappointing. We accept the Trust is rebuilding trust gradually, attempting to increase job satisfaction and attract quality staff.
The Trust continues to struggle with commissioning and providing the required number of inpatient beds to make out of area placements unnecessary. The new 12 bed Thurne ward at Hellesdon has helped to reduce out of area placements. We acknowledge that the Trust has a constant battle juggling financial and human resources to provide adequate inpatient facilities and adequate safe care in the community.
We note the Trust’s five key learning messages on learning from issues of safety, effectiveness and serious incidents. Whilst the governors acknowledge that the Trust is amongst the highest reporter of serious incidents nationally, we look forward to receiving the external audit of local unexpected deaths.
ARA2016_QA section 140616 post audit.indd 114 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 115
Governors are monitoring the quality and implementation of the current service and carer engagement strategy, Improving Services Together. We appreciate that it is ambitious in its aims to involve a wide variety of users, external providers and voluntary organisations. As part of our governor role, we are monitoring implementation and effectiveness of the Trust’s communication with its users and the wider public. We are concerned that the pace of implementation of the service user / carer strategy is slow, and that involvement by current service users and carers has declined whilst waiting for a network of involvement to be put in place that will provide meaningful comment and co-production of service design and provision. We appreciate the implementation of the Triangle of Care. Governors note the encouraging results from the Friends and Family Test taken by patients and carers on wards and upon leaving inpatient facilities and the national patient experience survey. However, we would like to see greater communication with service users and carers of service users who form the majority of the mentally ill receiving Trust services and who live in the community.
Governors are aware of the challenges faced by the Trust and the priorities of improving quality within a finite budget. We are appreciative of the focus on early intervention and recovery but mindful of the needs of service users who are unable to take advantage of recovery initiatives due to the nature of their incurable enduring mental health conditions. We hope that there will be an increase in protected allocated time for staff to accompany service users to the Recovery College and that existing courses are enhanced, extended and more widely available.
Governors appreciate the time and effort that has been spent in producing the Quality Accounts and are assured of the authenticity of the data it contains.
Healthwatch Norfolk
Healthwatch Norfolk appreciates the opportunity to comment on the Quality Account 2015/16 which details the quality of services and care provided by the Norfolk and Suffolk NHS Foundation Trust (NSFT). We note that the Quality Accounts are presented in an accessible document (although we are not aware if it will be made available in other formats). It is noticeable that throughout the document there are clear explanations of the acronyms and technical terms used to help the lay reader have a clearer understanding. It would add to
ease of understanding if the percentages used in some of the tables / graphs could detail the total number of patients that the percentage refers to.
Priorities for forthcoming year are clearly laid out with an identified lead and commitment to reporting to NSFT Board four times a year. We also note that there are several areas where it is clear that NSFT have involved service users and carers in reviewing the service and helping to ensure ongoing improvements are effective e.g. involving service users and carers in the research development programme, improving the environment on the wards as a result of service user feedback, the launch of Improving Services Together. We will be monitoring the implementation and effectiveness of the Improving Services Together strategy. As an organisation whose statutory role is to represent service users we believe it is imperative to take into account such experiences and we were pleased to take part in the mock CQC inspection held earlier this year. The inclusion of young people’s voices through the Council of Governors is also welcomed by Healthwatch Norfolk.
We note there are a number of areas across the Trust that have recorded improvements during the year and acknowledge that these improvements have been put in place during a time of significant financial constraints across the health and social care sector. In particular we have noted:
• A reduction in out of hospital placements
• Improved focus on physical health check
• A reduction in the use of restrictive practices (although we note that the use of prone restraint amongst patients with Learning Disabilities is still above average)
• Further work to eradicate ligature points across the organisation
• Providing same sex facilities
• The implementation of easy read appointment letters/documentation (we trust that service users will be very much involved in this initiative)
However, we also note a number of areas of concern where we believe the Trust needs to make considerable effort to implement improvements:
• The reduction in the target for access to crisis resolution/home treatment (although we are aware the Trust is focusing to improve this)
ARA2016_QA section 140616 post audit.indd 115 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016116
• The correct process being implemented with regard to the Code of Practice for MHA Section 17 leave of absence, ensuring the safety of patients
• Increase the number of service users who agree that they are involved in their care plan
• Address the decrease in the seven-day follow up after discharge
• The significant increase in waiting times is of particular concern to Healthwatch Norfolk
• We look forward to there being information in the next Quality Account relating to the implementation of Safewards
• Whilst we are aware that the Trust has continued to make significant efforts to recruit, retain and support staff appropriately, it is disappointing to note the results of the staff survey. We trust that there will be a continued effort to ensure all staff are appraised regularly and that the outcome of the independent review of management in the Trust helps to improve staff morale
We will continue to work with the Trust to ensure that the views of patients, carers and their families are taken into account and to make recommendation for change where appropriate.
Healthwatch Suffolk
Patient safety
Physical Health Check: 95% of service users admitted to a ward for more than 24 hours will receive a physical health check.
Achieving ‘90% of service users admitted to a ward receiving a health check’ is positive although clearly more progress is needed to reach the 95% target. Physical health is a key issue for all of the Trust`s service uses, not just those admitted to wards.
A survey carried out by Healthwatch Suffolk and Suffolk User Forum during the last quarter of 2015 found that 1 in every 2 respondents were not asked about their physical health during
their assessment by the Access and Assessment service of the Trust. It is very desirable that progress is also made in this area given that people suffering from serious mental health problems also suffer from physical health problems that contribute 15-20 years’ loss of life in comparison with the general population.
Seclusion and restrictive interventions: Use of restrictive interventions will reduce to below the national benchmarking average by 1 April, 2016.
Some good progress seems to have been made in the area of prone restraints and seclusions but sustained staff training initiatives and efforts to increase staff awareness are needed to consolidate progress and to achieve better than average benchmarking on all aspects. Patient experience Care Plan involvement: Trust service users (with Care Programme Approach entitlements) will report that they were involved in their care plans at a level at or above the national benchmarking average when the 2016 results are published.
Feedback to Healthwatch Suffolk from service users has identified lack of care plan involvement by service users, as well as other aspects of care plan management, as a very key area of concern.
Evidence of improvement from the 2015 CQC Survey is limited at best and does not correspond to the findings of the Healthwatch Suffolk / Suffolk User Forum survey that found that two thirds of service users say that they were not involved in reviews of their care. We certainly agree that it is appropriate that the Trust continues to target this area in their 2016/17 Quality Priorities (see below).
Clinical effectiveness Learning from incidents: All locality governance groups will be able to demonstrate that learning from incidents has led to changes in practice by 1 October, 2015.
Clearly the findings of the Mock CQC inspection at the end of 2015 still give cause for concern in spite of various initiatives undertaken.
ARA2016_QA section 140616 post audit.indd 116 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 117
Healthwatch Suffolk – Feedback on proposed 2016/17 Quality Priorities
Patient Safety
Self-harm: Staff will have the confidence and tools to manage service users who self-harm, improving the service user experience. This will be measured through the number of people who attend training, a staff survey and a patient reported outcome measure, which will be developed.
Suicide Prevention: For the Trust to participate in regional initiatives and develop a five-year target for suicide reduction in partnership with other services.
Healthwatch Suffolk has received sustained feedback from service users, with lived experience, on the urgent need for better and more empathetic treatment of self harmers and for a Suicide Prevention Programme to match the ambition of efforts being carried out in other areas of England. We therefore welcome the Trust’s decision to focus on these issues. In the case of the Self Harm priority we trust that a co-production approach, involving service users with appropriate experience, will be adopted in the development of staff training, ‘the tools to manage service users’ and a ‘patient reported outcome measure’.
Participation in regional initiatives and the development of a five-year target for suicide reduction is clearly dependent on the decisions of other organisations. It is suggested therefore that the Trust articulates and targets an objective (or objectives) that it is confident would contribute to a wider regional or countywide initiative. Patient Experience
Care planning: To raise the number of people reporting in the mandatory service user survey that they were involved, or involved to some extent, in decisions about their care to above 90% in 2017.
The Healthwatch Suffolk view is that a range of aspects of care planning are problematic within the Trust, not just whether service users are involved or not in decisions about their care. The Healthwatch / Suffolk User Forum survey in late 2015 for example found that two in every five respondents would have liked their family
or friends involved in the review of their care but they were not, and some respondents even claimed to be unaware that they had a Care Plan at all. Key issues identified at a Workshop, involving service users, carers and Trust professionals, held to review the survey findings, highlighted significant concerns related to continuity of care and the need for a much more patient-centered approach to care planning.
In spite of these wider Care Planning issues, however, we support the Trust`s decision to continue to focus on the single item of service users being involved in decisions about their care. Getting this right will necessitate resolving issues that should be of general benefit to the wider aspects. In particular, achieving adequate continuity of care and the cultural change needed to ensure patient-centered care will be a key factor if success is to be achieved. Underpinning this will be the need for adequate resourcing to allow staff sufficient time on the job, and the training, to carry out their roles to the higher standard needed. Clinical Effectiveness
MHA Compliance on recording capacity to consent: To ensure that 95% of service users have their capacity to consent to treatment on admission, recorded in the electronic record.
MHA Compliance on recording Section 17 leave: To ensure that Section 17 leave is managed in accordance with the Code of Practice, monitored by the MHA administration team.
Healthwatch Suffolk fully supports the Trust`s aim to achieve critical compliance in these areas. General Comment on Structure / Content The document is not in its present form appropriate for service users, carers or the general public. While it is appreciated that the Trust is required to report within a certain format it is recommended that the Trust produce a shorter `easy read` version of the final Quality Account, specifically designed for service users and carers, in order to reach a wider stakeholder audience.
ARA2016_QA section 140616 post audit.indd 117 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016118
Health Overview and Scrutiny Committee ‘The Norfolk Health Overview and Scrutiny Committee has decided not to comment on any of the Norfolk provider Trusts’ Quality Accounts for 2015-16 and would like to stress that this should in no way be taken as a negative comment. The Committee has taken the view that it is appropriate for Healthwatch Norfolk to consider the Quality Accounts and comment accordingly.
South Norfolk Clinical Commissioning Group NHS South Norfolk Clinical Clinical Commissioning Group, as the coordinating commissioner for Norfolk and Suffolk Foundation Trust on behalf of the Central Norfolk CCGs (Norwich, North Norfolk and South Norfolk), supports the Trust in its publication of the 2015/16 Quality Account. Having reviewed the mandatory detail of the report, we are satisfied that the Quality Account incorporates the mandated elements required, based on available data. We recognise the challenges experienced by the Trust due to having been under special measures in 2015/16 and the pending CQC re-inspection in July 2016. The Trust continues to work collaboratively with a range of stakeholders and we hope that the extra support provided as part of special measures will continue to support the improvement of services. The CCG has and will continue to support the Trust through Clinical Quality Review Meetings (CQRM).
We support the key quality priorities for 2016/17 and will continue to work with the Trust to monitor and review progress on the areas identified:
Patient Safety
• The Trust will ensure that staff will have the confidence and tools to manage service users who self harm, improving the service user experience. This will be measured through the number of people who attend training, a staff survey and a patient reported outcome measure.
• The CCG asks that the Trust participates in regional initiatives in developing a strategy that supports a Zero Tolerance for suicide. The CCG expects this to include a stretched target of three years for suicide reduction in partnership with other services.
Patient Experience
• The Trust will raise the number of people reporting in the mandatory service user survey to above 90% by 31 March 2017. The Trust will develop a plan and agree a trajectory in partnership with the CCG to demonstrate how this will be delivered during the year – this will be monitored at CQRM.
Clinical Effectiveness
• The Trust will ensure that 95% of service users have their capacity to consent to treatment on admission recorded in the electronic record.
• The Trust will ensure that section 17 leave is managed in accordance with the Code of Practice, monitored by the Mental Health Act administration team.
The Trust continues to demonstrate good reporting of serious incidents, openness and transparency on all matters of patient safety. The Trust has fully implemented ‘Duty of Candour’ guidance and we hope this will continue to support learning and improvement of services. We are pleased that the Trust has developed a quality dashboard which provides a month on month ‘at a glance’ position and which supports the reviewing and monitoring of quality metrics. We are pleased to note that the Trust has put in place a programme to remove ligatures and where not possible, to ensure staff know how to mitigate any remaining risks.
Although incidents of physical restraint reported in 2015/16 are above the national average, the Trust has implemented a programme of work to achieve reduction of restrictive interventions. A reduction in prone restraint and seclusion was achieved in line with the Trust’s 10% target in 2015/16, compared to 2014/15. The Trust has placed more emphasis on creating an environment and atmosphere which reduces the risk of restrictive interventions by adopting the Safewards Model. The CCG has supported this work through a local Commissioning for Quality and Innovation (CQUIN) scheme for 2015-16 and the CQUIN is continued into 2016/17. The CCG will continue to work with the Trust to further reduce the number of physical restraints reported.
ARA2016_QA section 140616 post audit.indd 118 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 119
Commissioners have raised concerns over the functionality and performance of Lorenzo, a single electronic patient record (EPR) introduced by the Trust in May 2015, specifically around the assurance of patient safety. Whilst this remains a significant concern the CCG commends the Trust on their wide range of efforts to address the associated issues and we acknowledge that part of the problem resides with the provider of the system. Despite the identified concerns the CCG recognises that Lorenzo provides an opportunity to improve services especially by reducing risk of fragmented records.
We also commend the Trust for using a wide range of national and local audits, national and local key performance indicators (KPIs), surveys and other forms of feedback such as the Friends and Family Test (FFT) to gain feedback from service users and their families and to improve services. Whilst outcomes from some of these measures (for example, FFT response rates) were disappointing, the Trust continues to explore different ways of improving feedback and engagement. The CCGs will continue to monitor this at CQRM and will work with the Trust to increase the use of the FFT and the associated response rate.
The CCG notes that the Trust remains focused on improving access to their services, in particular for people with learning disabilities, by adopting the Green light Toolkit. Although staff survey results were disappointing, we note that the Trust has a number of initiatives to improve staff engagement, including Putting People First (PPF).
The CCG also notes the quality priorities identified for 2016-17 and are recommending that mandatory training should feature within these. The CCG has raised concerns over training compliance throughout 2015/16 and believes that safe and quality services can be assured by a well-trained workforce.
The CCG looks forward to continuing to working in a positive and collaborative manner with the Trust to continue improvements in patient care during the coming year.
Ipswich and East Suffolk Clinical Commissioning Group and West Suffolk Clinical Commissioning Group
Ipswich and East Suffolk Clinical Commissioning Group and West Suffolk Clinical Commissioning Group, as the commissioning organisations for Norfolk and Suffolk Foundation Trust,
confirm that the Trust has consulted and invited comment regarding the Quality Account for 2015/2016. This has occurred within the agreed timeframe and the CCGs are satisfied that the Quality Account incorporates all the mandated elements required.
The CCGs have reviewed the Quality Account data to assess reliability and validity and to the best of our knowledge consider that the data is accurate. The information contained within the Quality Account is reflective of both the challenges and achievements within the Trust over the previous 12 month period. The priorities identified within the account for the year ahead reflect and support local priorities.
Ipswich and East Suffolk Clinical Commissioning Group and West Suffolk Clinical Commissioning Group, are currently working with clinicians and manager from the Trust and with local service users to continue to improve services to ensure quality, safety, clinical effectiveness and good patient / care experience is delivered across the organisation.
This Quality Account demonstrates the commitment of the Trust to improve services. The Clinical Commissioning Groups endorse the publication of this account.
Great Yarmouth and Waveney Clinical Commissioning Group
Great Yarmouth and Waveney Clinical Commissioning Group as a commissioning organisation of NSFT supports the organisation in its publication of a Quality Account for 2015/16. We are satisfied that the Quality Account incorporates the mandated elements required based on available data. The information contained within the Quality Account is reflective of the Trust over the previous 12 month period.
In our review we have taken account of the clinical quality and safety improvement priorities identified for 2016/17 and support the identified improvement objectives in the quality and safety of care provided to Great Yarmouth and Waveney residents. The Trust will do this by:
Improving Patient Safety
The Trust Board will enable staff to have the confidence and requisite skills to care for service users who self-harm whilst improving service users’ experience. This will be measured by the
ARA2016_QA section 140616 post audit.indd 119 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016120
number of people who attend training, a staff survey and the implementation of a patient reported outcome measure.
The Trust Board will participate in regional initiatives and develop a five-year target for suicide reduction in partnership with other services to improve the well-being of our communities beyond those people in formal contact with the Trust’s services.
Improving Patient Experience
The Trust Board will improve the number of people saying that they involved, or involved to some extent in decisions about their care, to 90% or above in 2017 via the mandatory service user survey.
Improving Clinical Effectiveness
The Trust Board will ensure that 95% of service users have their capacity to consent to treatment on admission recorded in their electronic record in response to inspections of mental health act compliance by the Care Quality Commission.
The Trust Board will ensure that Section 17 leave is managed in accordance with the Mental Health Act which sets out clear requirements for the management of detained patients who are granted leave.
Great Yarmouth and Waveney CCG notes the quality priorities identified for 2015/16 and in particular the latest results from the national audit for restraint in August 2015 which showed that the Trust is still reporting above average rates of restraint and prone restraint overall. The CCG also notes that the Trust has implemented a programme of work to achieve a reduction in the number of prone restraints and to ensure that restraints are carried out safely.
The CCG notes the evidence from the mock CQC inspection which showed that 90% of service users admitted to a ward for more than 24 hours received a physical health check and that the Trust continues to rollout physiological workbook training to all staff.
The CCG is pleased to note that the Trust participated in the Prescribing Observatory for Mental Health clinical audit during 2015/16 and that the Trust’s performance was above the national average in two of the parameters for antipsychotic prescribing in people with a learning disability.
We recognise the actions that the Trust is taking to improve data quality, essential for the delivery of excellent patient care, and the Trust’s monitoring processes to identify data quality issues that require correction.
The CCG commends the Trust for its openness and honesty regarding Lorenzo, the electronic patient record, and is pleased to note that the organisations that manage the contract on behalf of the Department of Health have provided assurances that the continuing issues with the system are now being prioritised.
We acknowledge the challenge to the Trust of being in Special Measures throughout 2015/16 and the pending Care Quality Commission re-inspection scheduled for July 2016. The CCG commends the Trust for the continued commitment to making the required improvements detailed within the Quality Improvement Plan.
The CCG believes that the Annual Quality Account presents the Trust with an opportunity to share with service users the significant service changes that have occurred within 2015/16 and provide an update on how these service changes continue to be monitored.
The Great Yarmouth and Waveney Clinical Commissioning Group looks forward to working with the NSFT during 2016/17.
ARA2016_QA section 140616 post audit.indd 120 14/06/2016 10:27
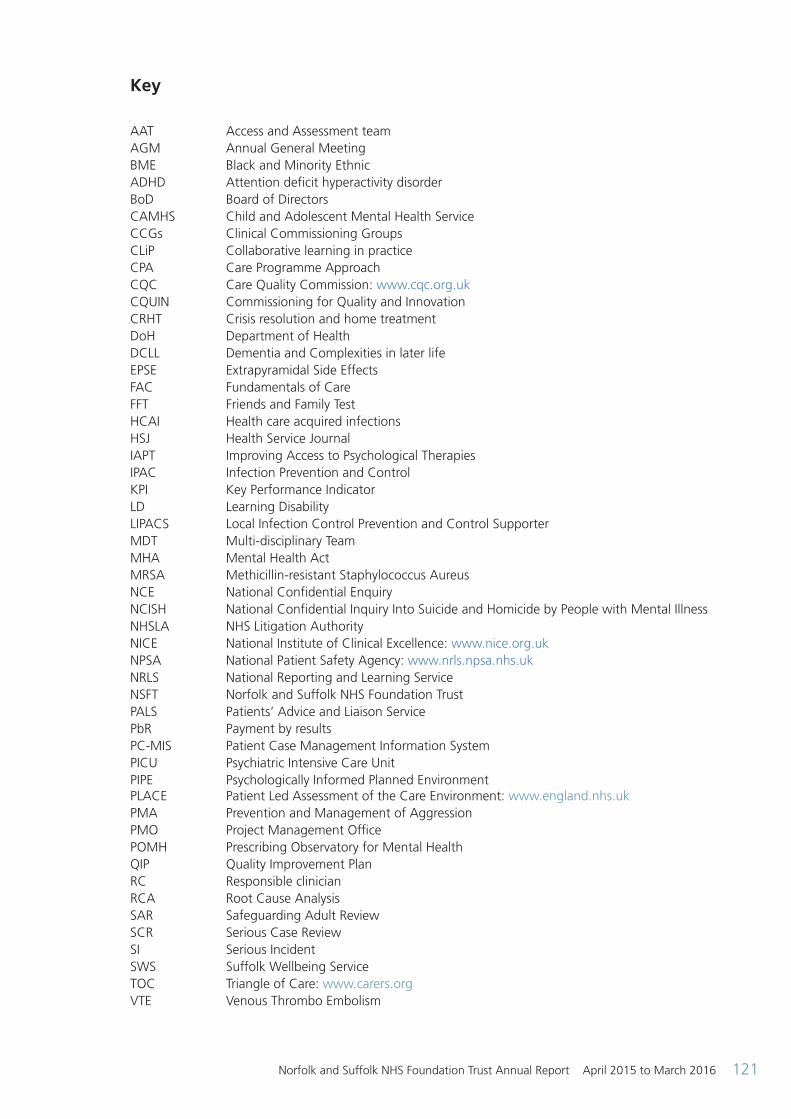
Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016 121
Key
AAT Access and Assessment teamAGM Annual General MeetingBME Black and Minority EthnicADHD Attention deficit hyperactivity disorderBoD Board of DirectorsCAMHS Child and Adolescent Mental Health ServiceCCGs Clinical Commissioning GroupsCLiP Collaborative learning in practiceCPA Care Programme ApproachCQC Care Quality Commission: www.cqc.org.ukCQUIN Commissioning for Quality and Innovation CRHT Crisis resolution and home treatment DoH Department of Health DCLL Dementia and Complexities in later lifeEPSE Extrapyramidal Side EffectsFAC Fundamentals of CareFFT Friends and Family TestHCAI Health care acquired infectionsHSJ Health Service JournalIAPT Improving Access to Psychological TherapiesIPAC Infection Prevention and ControlKPI Key Performance IndicatorLD Learning DisabilityLIPACS Local Infection Control Prevention and Control SupporterMDT Multi-disciplinary TeamMHA Mental Health ActMRSA Methicillin-resistant Staphylococcus AureusNCE National Confidential EnquiryNCISH National Confidential Inquiry Into Suicide and Homicide by People with Mental IllnessNHSLA NHS Litigation AuthorityNICE National Institute of Clinical Excellence: www.nice.org.ukNPSA National Patient Safety Agency: www.nrls.npsa.nhs.ukNRLS National Reporting and Learning ServiceNSFT Norfolk and Suffolk NHS Foundation TrustPALS Patients’ Advice and Liaison ServicePbR Payment by resultsPC-MIS Patient Case Management Information System PICU Psychiatric Intensive Care UnitPIPE Psychologically Informed Planned Environment PLACE Patient Led Assessment of the Care Environment: www.england.nhs.ukPMA Prevention and Management of AggressionPMO Project Management OfficePOMH Prescribing Observatory for Mental HealthQIP Quality Improvement PlanRC Responsible clinicianRCA Root Cause AnalysisSAR Safeguarding Adult ReviewSCR Serious Case ReviewSI Serious IncidentSWS Suffolk Wellbeing ServiceTOC Triangle of Care: www.carers.orgVTE Venous Thrombo Embolism
ARA2016_QA section 140616 post audit.indd 121 14/06/2016 10:27

Norfolk and Suffolk NHS Foundation Trust Annual Report April 2015 to March 2016122
ARA2016_QA section 140616 post audit.indd 122 14/06/2016 10:27
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A1
Annual accounts
for the year ended31 March 2016
ARA2016 - Acc Section 130616 post audit.indd 1 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A2
Statement of the Chief Executive’s responsibilities as the accounting officer of Norfolk and Suffolk NHS Foundation Trust
The NHS Act 2006 states that the chief executive is the accounting officer of the NHS foundation trust. The relevant responsibilities of the accounting officer, including their responsibility for the propriety and regularity of public finances for which they are answerable, and for the keeping of proper accounts, are set out in the NHS Foundation Trust Accounting Officer Memorandum issued by Monitor.
Under the NHS Act 2006, Monitor has directed Norfolk and Suffolk NHS foundation trust to prepare for each financial year a statement of accounts in the form and on the basis set out in the Accounts Direction. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of Norfolk and Suffolk NHS foundation trust and of its income and expenditure, total recognised gains and losses and cash flows for the financial year.
In preparing the accounts, the Accounting Officer is required to comply with the requirements of the NHS Foundation Trust Annual Reporting Manual and in particular to:
• observe the Accounts Direction issued by Monitor, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis;
• make judgements and estimates on a reasonable basis;
• state whether applicable accounting standards as set out in the NHS Foundation Trust Annual Reporting Manual have been followed, and disclose and explain any material departures in the financial statements;
• ensure that the use of public funds complies with the relevant legislation, delegated authorities and guidance; and
• prepare the financial statements on a going concern basis.
The accounting officer is responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the NHS foundation trust and to enable him to ensure that the accounts comply with requirements outlined in the above mentioned Act. The Accounting Officer is also responsible for safeguarding the assets of the NHS foundation trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in Monitor’s NHS Foundation Trust Accounting Officer Memorandum.
Signed:
Michael Scott Chief Executive
Date: 25 May 2016
ARA2016 - Acc Section 130616 post audit.indd 2 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A3
Independent Auditor’s Report to the Council of Governors of Norfolk And Suffolk NHS Foundation Trust
Opinions and conclusions arising from our audit 1. Our opinion on the financial statements is unmodified
We have audited the financial statements of Norfolk and Suffolk NHS Foundation Trust for the year ended 31 March 2016 set out on pages A16 to A51. In our opinion:
• the financial statements give a true and fair view of the state of the Trust’s affairs as at 31 March 2016 and of the Trust’s income and expenditure for the year then ended; and
• the financial statements have been properly prepared in accordance with the NHS Foundation Trust Annual Reporting Manual 2015/16.
2. Our assessment of risks of material misstatement
In arriving at our audit opinion above on the financial statements the risks of material misstatement that had the greatest effect on our audit were as follows:
Valuation of land and buildings – £133 million (land, buildings and dwellings); £0.7 million (assets held for sale) The risk level is (consistent) year on year Refer to page 10 (Audit Committee Report), page A21 and A22 (accounting policy) and pages A38 to A40 (financial disclosures).
The risk: Land and buildings are initially recognised at cost. Non-specialised property assets in operational use are subsequently recognised at current value in existing use. Specialised assets, where a market value is not readily ascertainable, are subsequently recognised at the depreciated replacement cost of a modern equivalent asset that has the same service potential as the existing property. There is significant judgment involved in determining the appropriate basis for each asset according to the degree of specialisation, as well as over the assumptions made in arriving at the valuation of the asset. Evaluations are performed every five years and interim valuations are undertaken every three years. A full valuation of land and buildings was performed as at 31 March 2015.
Assets that are transferred to ‘assets held for sale’ are transferred at market value. In 2015 St Clements Hospital was moved into this category. It has been identified that the valuation carried out at the time did not take into account the full amount of asbestos contained in the building. A prior period adjustment to the valuation has been made to reflect this cost which reduces the value by £3.2 million.
Our response: We evaluated and tested management’s arrangements for considering that the valuation of land and buildings as at 31 March 2016 were appropriate. We also evaluated the accounting treatment relating to the assets held for sale. In these area our audit procedures included:
• Assessing the basis of the factors relating to local land and building valuations to determine the risk that the assets are impaired by comparing to known benchmarks and indices;
• Reviewing management’s arrangements regarding the consideration for any impairments;
• Determining whether disclosures in relation to land and buildings complies with the requirements of the ARM; and
• Reviewing the accounting treatment and considering the adequacy of the disclosures in the notes to the accounts in regard to the prior-period adjustment.
ARA2016 - Acc Section 130616 post audit.indd 3 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A4
NHS Income Recognition - £189 million The risk level is (consistent) year on year Refer to page 11 (Audit Committee Report), page A20 (accounting policy) and pages A30 to A31 (financial disclosures).
The risk: The main source of income for the Trust is the provision of healthcare services to the public under contracts with NHS commissioners, which make up (93%) of income from activities. The Trust participates in the national Agreement of Balances (AoB) exercise for the purpose of ensuring that intra-NHS balances are eliminated on the consolidation of the Department of Health’s resource accounts. The AoB exercise identifies mismatches between receivable and payable balances recognised by the Trust and its commissioners, which will be resolved after the date of approval of these financial statements. For these financial statements the Trust identifies the specific cause, and accounts for the expected future resolution, of each individual difference. Mis-matches can occur for a number of reasons. Where there is a lack of agreement, mis-matches can also be classified as formal disputes and referred to NHS England Area Teams for resolution.
We do not consider NHS income to be at high risk of significant misstatement, or to be subject to a significant level of judgement. However, due to its materiality in the context of the financial statements as a whole NHS income is considered to be one of the areas which had the greatest effect on our overall audit strategy and allocation of resources in planning and completing our audit. Our response: Our methodology included:
• Evaluating and testing the accounting policy for revenue recognition to ensure that it is consistent with the requirements of the NHS Foundation Trust Annual Reporting Manual.
• Testing controls around the authorisation of sales invoices.
• For the commissioners’ revenue, obtaining and agreeing the revenue recognised to a signed contract and correspondence between the Trust and the commissioners.
• Reviewing the output from the National Agreement of Balances (AoB) exercise and agreeing any material mis-matches to supporting evidence.
• Reviewing invoices and credit notes raised around the year end date to ensure the recognition of income had fallen in the correct period.
3. Our application of materiality and an overview of the scope of our audit
The materiality for the financial statements was set at £3,300,000 (2014/15: £3,300,000), determined with reference to a benchmark of income from operations (of which it represents approximately 1.5% (2014/15: 1.5%). We consider income from operations to be more stable than a surplus-related benchmark. This is consistent with the prior year. We report to the Audit Committee any corrected and uncorrected identified misstatements exceeding £165,000 (2014/15: £165,000), in addition to other identified misstatements that warrant reporting on qualitative grounds. The Group has one component - the Trust. Our audit of the Trust was undertaken to the materiality level specified above and was performed at the Trust’s offices at Hellesdon Hospital. 4. Our opinion on other matters prescribed by the Audit Code for NHS Foundation Trusts is unmodified
In our opinion:
• the part of the Directors’ Remuneration Report to be audited has been properly prepared in accordance with the NHS Foundation Trust Annual Reporting Manual 2015/16; and
• the information given in the Performance Report and the Accountability Report for the financial year for which the financial statements are prepared is consistent with the financial statements.
ARA2016 - Acc Section 130616 post audit.indd 4 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A5
5. We have nothing to report in respect of the following matters on which we are required to report by exception
Under ISAs (UK&I) we are required to report to you if, based on the knowledge we acquired during our audit, we have identified other information in the Annual Report that contains a material inconsistency with either that knowledge or the financial statements, a material misstatement of fact, or that is otherwise misleading.
In particular, we are required to report to you if:
• we have identified material inconsistencies between the knowledge we acquired during our audit and the directors’ statement that they consider that the Annual Report and Accounts taken as a whole is fair, balanced and understandable and provides the information necessary for patients, regulators and other stakeholders to assess the Trust’s performance, business model and strategy; or
• the Audit Committee Report does not appropriately address matters communicated by us to the audit committee.
Under the Code of Audit Practice we are required to report to you if in our opinion:
• the Annual Governance Statement does not reflect the disclosure requirements set out in the NHS Foundation Trust Annual Reporting Manual 2015/16, is misleading or is not consistent with our knowledge of the Trust and other information of which we are aware from our audit of the financial statements.
In addition we are required to report to you if:
• any reports to the regulator have been made under Schedule 10(6) of the National Health Service Act 2006.
• any matters have been reported in the public interest under Schedule 10(3) of the National Health Service Act 2006 in the course of, or at the end of the audit.
We have nothing to report in respect of the above responsibilities. 6. Other matters on which we report by exception – adequacy of arrangements to secure value for money
Under the Code of Audit practice we are required to report by exception if we conclude that we are not satisfied that the Trust put in place proper arrangements to secure value for money in the use of resources for the relevant period.
In February 2015 Monitor issued an enforcement undertaking under section 106 of the Health and Social Care Act 2012.
Monitor stated that it had concerns with breaches of its conditions of licence, in particular:
• An inspection by the Care Quality Commission (CQC) found that the Trust was “inadequate” overall and highlighted specific concerns around services being safe and well-led;
• An independent governance review identified concerns including:
– Lack of effective Board-led strategy development and implementation; – Weaknesses in leadership; – Lack of effective governance structures; – Over centralised systems of control and lack of an effective system of control for monitoring the quality of care; – Lack of effective risk management arrangements; – Lack of effective response of staff escalation of issues.
ARA2016 - Acc Section 130616 post audit.indd 5 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A6
At this time Monitor noted that they believed the actions that the Trust had undertaken to take were actions required to secure the breaches did not continue or recur. The Trust’s Annual Governance Statement sets out progress made against the plan. As a result of these issues we are not able to conclude that the Trust has put in place proper arrangements for securing economy, efficiency and effectiveness in its use of resources. Certificate of audit completion
We certify that we have completed the audit of the accounts of Norfolk and Suffolk Hospital NHS Foundation Trust in accordance with the requirements of Schedule 10 of the National Health Service Act 2006 and the Code of Audit Practice issued by the National Audit Office. Respective responsibilities of the accounting officer and auditor
As described more fully in the Statement of Accounting Officer’s Responsibilities on page A2 the accounting officer is responsible for the preparation of financial statements which give a true and fair view. Our responsibility is to audit, and express an opinion on, the financial statements in accordance with applicable law and International Standards on Auditing (UK and Ireland). Those standards require us to comply with the UK Ethical Standards for Auditors. Scope of an audit of financial statements performed in accordance with ISAs (UK and Ireland)
A description of the scope of an audit of financial statements is provided on our website at www.kpmg.com/uk/auditscopeother2014. This report is made subject to important explanations regarding our responsibilities, as published on that website, which are incorporated into this report as if set out in full and should be read to provide an understanding of the purpose of this report, the work we have undertaken and the basis of our opinions. Respective responsibilities of the Trust and auditor in respect of arrangements for securing economy, efficiency and effectiveness in the use of resources
The Trust is responsible for putting in place proper arrangements to secure economy, efficiency and effectiveness in its use of resources, to ensure proper stewardship and governance, and to review regularly the adequacy and effectiveness of these arrangements.
Under Section 62(1) and Schedule 10 paragraph 1(d), of the National Health Service Act 2006 we have a duty to satisfy ourselves that the Trust has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources. We are not required to consider, nor have we considered, whether all aspects of the Trust’s arrangements for securing economy, efficiency and effectiveness in its use of resources are operating effectively. Scope of the review of arrangements for securing economy, efficiency and effectiveness in the use of resources
We have undertaken our review in accordance with the Code of Audit Practice, having regard to the guidance on the specified criterion issued by the Comptroller and Auditor General (C&AG), as to whether the Trust has proper arrangements to ensure it took properly informed decisions and deployed resources to achieve planned and sustainable outcomes for taxpayers and local people. The C&AG determined this criterion as necessary for us to consider under the Code of Audit Practice in satisfying ourselves whether the Trust put in place proper arrangements for securing economy, efficiency and effectiveness in its use of resources for the year ended 31 March 2016.
ARA2016 - Acc Section 130616 post audit.indd 6 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A7
We planned our work in accordance with the Code of Audit Practice. Based on our risk assessment, we undertook such work as we considered necessary to form a view on whether, in all significant respects, the Trust had put in place proper arrangements to secure economy, efficiency and effectiveness in its use of resources. The purpose of our audit work and to whom we owe our responsibilities
This report is made solely to the Council of Governors of the Trust, as a body, in accordance with Schedule 10 of the National Health Service Act 2006. Our audit work has been undertaken so that we might state to the Council of Governors of the Trust, as a body, those matters we are required to state to them in an auditor’s report and for no other purpose. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Council of Governors of the Trust, as a body, for our audit work, for this report or for the opinions we have formed.
Stephanie Beavis
for and on behalf of KPMG LLP, Statutory Auditor
Chartered Accountants Botanic House, 100 Hills Road, Cambridge CB2 1AR
25 May 2016
ARA2016 - Acc Section 130616 post audit.indd 7 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A8
1. Scope of responsibility
As Accounting Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the Norfolk and Suffolk NHS Foundation Trust’s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS foundation trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Foundation Trust Accounting Officer Memorandum.
2. The purpose of the system of internal control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of Norfolk and Suffolk NHS Foundation Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in Norfolk and Suffolk NHS Foundation Trust for the year ended 31 March 2016 and up to the date of approval of the annual report and accounts.
3. Capacity to handle risk
The Trust has implemented a robust structure for ensuring that risk management, control and review processes have been properly established and monitored. Firm and clear leadership has been provided to focus these processes in the following ways:
• Executive Director lead with responsibility for risk management
• Dedicated risk management team
• Board approved risk management strategy
• Board Assurance Framework in place that covers the risks to the Trust’s strategic objectives, controls and mitigation arrangements
• Regular monitoring of performance at a number of levels, including Audit and Risk Committee, Finance Committee, Transformation Programme Board, Quality Governance Committee, Senior Management Forum, Executive Directors, and Board of Directors
• Locality and Service Managers are each supported by a Lead Clinician who provides clinical leadership to managerial and governance processes
• All programmes and projects also maintain risk registers, which are managed by the respective programme and reported up the governance structure as appropriate
• Regular monitoring of risk action plans to ensure all reasonable steps taken to minimise risk
• All staff receive induction training that includes risk management, and key staff are further trained in root cause analysis and risk assessment
• All serious incidents are investigated using root cause analysis and the learning is disseminated across the organisation using a range of mechanisms including discussion at Quality Governance Committee, Senior Management Forum, and locality meetings. Learning from incidents is an area where we have focused on strengthening our practice and this is reflected in our Quality Improvement Plan
The Board of Directors regularly reviews its governance structures and systems against latest guidance and reports from national enquiries to ensure that assurance and performance management systems are working effectively.
Annual Governance Statement
ARA2016 - Acc Section 130616 post audit.indd 8 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A9
The Quality Governance Committee undertakes more detailed reviews of service governance issues with regular reports to the Audit and Risk Committee, including risk register and Care Quality Commission (CQC) reports.
4. The risk and control framework
The Trust takes seriously its responsibilities for risks and control through a fully integrated approach to governance and risk. This is supported by a Trust-wide Risk Management Strategy, which provides the framework for the management of risk that covers processes relating to, clinical risk, health and safety risk and organisational (corporate and strategic) risk. The key elements of the Risk Management Strategy encompass a strategic intent by the Trust to develop a risk management culture that engages all staff. The Board of Directors is committed to ensuring risk management forms an integral part of its philosophy, practices and business plans. It also proves that the Trust is open with stakeholders, receptive to challenges and keen to learn. All identified risks are evaluated using a 5x5 scoring matrix that calculates risks, and change in risk by measuring likelihood and severity of consequences. Each locality and service assesses their services on a monthly basis and records a risk profile in the risk register. Each profile is scrutinised and monitored through the governance and risk department, who facilitate recording and reporting. The risk matrix is consistently used throughout the organisation:
• Low risks (green 1-3) and moderate risks (yellow 3-6) are held at local level
• Significant risks (amber 8-12) and above are reported and monitored monthly through the Trust’s Quality Governance Committee and Audit and Risk Committee
• High risks (red 15-25) are reported to the Executive Team and the Board of Directors
The risk management policy and strategy describes the risk management process and provides clear lines of accountability to ensure that all risks are appropriately managed with action plans to mitigate against occurrence. The Trust has empowered staff to make sound judgments and decisions concerning the management of risk and risk taking. All services
assess their own risk profiles, which are reported and recorded through to the Trust’s risk register. All significant risks are entered onto the Trust risk register with an action plan to eliminate or reduce risks of all kinds. The Governance Team monitors individual risk registers with review by the Audit and Risk Committee. This includes the setting of target risk scores, which is the level of risk the organisation is prepared to accept and once achieved, the risk would no longer be reported as such.
During 2015-16 the Board continued to develop the format and structure of the Board Assurance Framework (BAF). The Trust’s Risk Manager meets with the Trust Secretary quarterly to cross-reference the Trust’s Risk Register with the BAF. The Trust has established an Assurance Framework, which is designed and operating to meet the requirements of the Annual Governance Statement and provides the necessary weight of evidence that an effective system of control operates within the Trust. This Framework includes the following items:
• Board Assurance Framework that considers risks to strategic objectives
• Regular review of longer-term corporate and strategic risks by the Executive Team and Board of Directors
• Results of the Care Quality Commission specific reviews and outcomes from site visits, including Mental Health Act reviews
• Comprehensive live risk register that includes strategic, corporate, financial, clinical and other non-clinical risks
• Regular reviews of risk register by the Board of Directors, Audit and Risk Committee, Quality Governance committee and Executive Directors’ formal meeting
• A regular programme of visits (including unannounced) to clinical areas by both Executive and Non-Executive Board Members
• Feedback from external bodies, including Monitor, Care Quality Commission, National Patient Safety Agency and NHS Litigation Authority (NHSLA)
• Root Cause Analysis reports to include learning from patient safety issues and these are included in reports to the Board of Directors
ARA2016 - Acc Section 130616 post audit.indd 9 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A10
A wide range of communication and consultation mechanisms also exists with relevant stakeholders, both internal and external, which includes the use of external assessors, where appropriate, to assist in determining the extent of a particular risk.
The Health and Social Care Act (2012) places a duty on the Board as a whole and directors individually to act with a view to promote the success of the Trust and maximise the benefits for members and the public. In relation to risk and control, the Board fulfils this duty through the governance structures of the Board and its committees. This structure is complemented by a policy and procedure framework that covers risk assessment and management, the scheme of delegation, standing financial instructions and the allocation of responsibility to specified post holders across the organisation.
The lines of reporting which show how accountability flows between the executive team, the Board of Directors committees and the Board are shown in the diagram in the Trust Governance section of this report.
Board of Director Committees consisted in the year of:
• Audit and Risk Committee
• Quality Governance Committee (formerly Service Governance Committee)
• Finance Committee
• Charitable Funds Committee
• Mental Health Act Hospital Managers Committee
• Remuneration and Terms of Service Committee (which acts as a nominations committee for executive director posts)
• Organisational Development and Workforce Committee
The Audit and Risk Committee provides the Board of Directors (and the Council of Governors) with objective assurance on the governance arrangements across the Trust including its internal controls for the management of risk. A report is made to the next Board of Directors’ meeting following each committee meeting.
The Quality Governance Committee is chaired by the Trust Chair. A report is made to the
next Board of Directors meeting following each committee meeting. There are close links between the Audit and Risk and Quality Governance Committees and all committees cross-refer issues, where appropriate.
The Finance Committee is responsible for ensuring the effective management of all of the Trust’s affairs, including management of the Trust’s cost and finance base, significant investment decisions, and overall performance. This committee has the capacity to scrutinise Trust performance and escalates areas of concern to the Board of Directors. It receives reports from Performance Review Group meetings as well as overseeing key programmes. The committee monitors the Trust’s cost improvement programmes and provides oversight of the organisation’s integrated performance management systems. A report is made to the next Board of Directors meeting following each committee meeting.
The Transformation Programme Board is responsible for providing assurance to the Board on the successful delivery of the Quality Improvement Plan and Financial Recovery Plan. The Board ensures that a framework exists for robust governance and accountability arrangements for the implementation of the Transformation Programme.
The Charitable Funds committee now consists of one fund. The purpose of the committee is to ensure that charitable funds are properly collected, invested and allocated in line with overarching statutory and policy requirements and in accordance with any specific requirements attached to individual funds or bequests. The Committee acts to ensure the Trust meets its obligations as a corporate trustee as set out by the Charities Act and other related legislation and regulations. It acts as a host for other NHS Trust charitable funds. A report is made to the next Board of Directors’ meeting following each committee meeting.
As a mental health FT, the Trust sometimes needs to detain and treat patients against their will under the Mental Health Act (1983). Within this statutory framework there is a requirement for hospital managers (who are not employed by the Trust, and who are independent of the Trust’s management) to review detentions and decide whether they continue to be required. The MHA Hospital Managers’ committee serves this function and is chaired by a non-executive director. An annual report from this committee is reviewed by the Board of Directors.
ARA2016 - Acc Section 130616 post audit.indd 10 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A11
The Remuneration and Terms of Service Committee oversees the appointment and remuneration of executive directors, as well as providing assurance on the process for setting objectives and performance appraisal. The committee also oversees succession planning and Board skill mix. A report is made to the next Board of Directors meeting following each Remuneration and Terms of Service Committee meeting. The Nominations Committee is primarily a Council of Governors committee that oversees recruitment and appraisal of the Chair and non-executive directors.
The Trust’s Equalities and Engagement Manager supports staff in equality assessment arrangements in line with the Equality Act (2010). Guidance is now available for staff carrying out service based equality assessments and policy equality assessments and where service plans change assessments are updated. In order to support the implementation of equality assessment plans the Trust has developed several key documents based on the Equality Act’s protected characteristics. These include practice guidelines on supporting lesbian, gay and bisexual service users, spiritual and pastoral care guidelines and guidance on challenging racist and discriminatory behaviours. Compliance with human rights legislation is supported through the work of the Equalities and Engagement Manager and the Safeguarding Team, as well as the Mental Health Law Forum which oversees policy and practice in relation to the Mental Capacity and Mental Health legislation.
A wide range of communication and consultation mechanisms also exists with relevant stakeholders, both internal and external, which includes the use of external assessors, where appropriate, to assist in determining the extent of a particular risk.
The Trust manages its information risks by undertaking an annual information governance audit using the NHS toolkit provided for this purpose and seeking to improve year on year. The Trust has undertaken the 2015 assessment (submitted in March 2016) and is 84% compliant (an improvement from 80% last year). Action is being undertaken to embed the policies and procedures throughout the Trust.
As an employer with staff entitled to membership of the NHS Pension Scheme control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary,
employer’s contributions and payments in to the Scheme are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations.
The Trust has undertaken to produce risk assessments and Carbon Reduction Delivery Plans in accordance with emergency preparedness and civil contingency requirements, based on UKCIP 2009 weather projects and the ‘Under the Weather’ guidance from the NHS Sustainable Development Unit, to ensure that this Trust’s obligations under the Climate Change Act and the Adaptation Reporting requirements are complied with.
Control measures are in place to ensure that all the organisation’s obligations under equality, diversity and human rights legislation are complied with.
Further information is given in the Strategic Review section of the Annual Report.
5. Review of economy, efficiency and effectiveness of the use of resources
The Executive Team is responsible for overseeing the day-to-day operations of the Trust and for ensuring the economic, efficient and effective deployment of resources. The Executive Team works as part of the wider senior management team, whose membership includes all senior locality and directorate managers. This Team receives regular monthly financial and performance reports that highlight any areas of concern.
The Transformation Programme Board is responsible for overseeing the development and implementation of strategic cost improvement plans. These are subject to full risk and quality assessment, and resources are deployed as appropriate to ensure plans are achieved.
Internal Audit undertakes a review of the Trust’s internal control systems as part of the Annual Audit Plan (approved by the Audit and Risk Committee).
The Trust participates in a number of processes designed to secure better value for money from its use of resources. These include the use of shared financial services, a competitive tendering approach and membership and participation in the Eastern Collaborative Procurement Hub,
ARA2016 - Acc Section 130616 post audit.indd 11 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A12
which is designed to ensure non-pay expenditure, is incurred as efficiently as possible. The Trust is also a member of the Audit Commission’s Mental Health Benchmarking Club.
In October 2014 the Trust was inspected by the Care Quality Commission with the report being published in February 2015. The inspection found that the Trust was rated ‘inadequate’ in the domains of well-led, safe and responsive and ‘requires improvement’ in the domain of effectiveness. This means that the Trust is not compliant with the registration requirements of the CQC.
Following the CQC review the Trust was deemed by Monitor to be in breach of License conditions FT4(2), FT4(4)(a–c), FT4(5)(b–c). FT4(5)(e–f) and FT4(6) (a–f) and the Trust was placed into “special measures”. The Trust has been required to draw up and implement a Quality Improvement Plan to address the CQC concerns and to ensure the Trust improves quality of care and returns to compliance with all health care standards.
The Trust has accepted and embraced the findings of the external reviews and has developed a plan to address the quality improvement issues identified in the CQC report and the independent review of corporate governance report (see page 12). Good progress has been made against the CQC recommendations and details are available on the Trust website. The QIP is managed and monitored by the Project Management Office (PMO) with executive sponsors for each action. The Trust reported a financial deficit in the year of £8.9m and achieved a Financial Sustainability risk rating of 2.
6. Information Governance “During this IG year, we had two Level 2 incidents that required reporting to the Information Commissioner’s Office (ICO) via the IG Toolkit Incident Reporting Tool. In addition, one other incident was self-referred. In all three incidents, the ICO determined that no further action was required beyond the action that had already been put into place.
We have undertaken an operational restructure of IG during this year. The IG Committee has been also restructured into a strategic IG Group (chaired by the SIRO) and an operational IG Sub
Group (chaired by the IG Manager). This new approach has been reviewed and deemed to be successful. IG Services have been created as an independent service having been moved from being part of ICT.
7. Annual Quality Report
The directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations 2010 (as amended) to prepare Quality Accounts for each financial year. Monitor has issued guidance to NHS foundation trust boards on the form and content of annual Quality Reports which incorporate the above legal requirements in the NHS Foundation Trust Annual Reporting Manual.
The Trust has produced an Annual Quality Account for 2015-16. The information contained in this report draws on information from the same systems that underpin the Trust’s normal reporting processes, including activity management, performance management and risk and governance systems. The Report is developed through the Governance Team and all data is validated for accuracy and completeness by the referral of performance and activity data from the Trust’s central information team back to the clinical teams for checking.
8. Review of effectiveness
As Accounting Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, clinical audit and the executive managers and clinical leads within the NHS Foundation Trust who have responsibility for the development and maintenance of the internal control framework. I have drawn on the content of the quality report attached to this Annual Report and other performance information available to me. My review is also informed by comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, the Audit and Risk Committee, Internal Audit and Counter Fraud and a plan to address weaknesses and ensure continuous improvement of the system is in place.
• Reports from external audit
ARA2016 - Acc Section 130616 post audit.indd 12 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A13
• Substantial assurance provided through the Head of Internal Audit’s Opinion on the effectiveness of internal control
• Inspection reports on the Trust’s services by the CQC
• Results from clinical audit reviews, comprehensive clinical audit programmer for suicide prevention for inpatients, clinical suicide audit and an audit of the effectiveness of the reviews on unexpected deaths; and
• Reports from external assessors as regards the financial and clinical governance systems and procedures within the Trust
I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the:
• Board of Directors
• Audit and Risk Committee
• Quality Governance Committee
• Operational Risk Management Group
• Executive Directors and Trust Management Team, and
• Internal Audit, Clinical Audit and Counter Fraud
The Head of Internal Audit Opinion for the period 1 April 2015 to 31 March 2016 states:
“Substantial Assurance can be given that there is a generally sound system of internal control, designed to meet the organisation’s objectives, and that controls are generally being applied consistently. However, there are weaknesses in the design and/or inconsistent application of controls put the achievement of particular objectives at risk”
The Audit and Risk Committee and the Board of Directors regularly receive risk management reports that incorporate information from all the above sources. Particular attention is paid to those risks with a higher impact / higher probability of occurring.
The ongoing development of the Board Assurance Framework (BAF) ensures that the Board of Directors is fully aware of the risks associated with the Trust meeting its strategic objectives. The BAF is cross-referenced to the Trust Risk Register and updated quarterly.
In October 2014 a board effectiveness review was commissioned from Foresight Partnership. The review identified significant development areas and these formed the basis of an action plan. Since then changes have been implemented and in autumn 2015 Foresight Partnership updated their review and reported significant improvements.
The Trust’s key policies and procedures are subject to annual review and the relevant committee and the Executive Team undertake this process, before taking the revised policy to the Board of Directors for final approval.
All of this work is linked to the Trust’s risk register, which is updated for risks pertaining to compliance with CQC registration standards, Controls Assurance and Board Assurance Framework, but which is also updated on an everyday basis as new risks become apparent. This process enables staff to report incidents and concerns in a way that can be investigated and added to the risk register where appropriate so that remedial action can be taken.
The Quality Governance Committee assesses compliance with standards and other compliance matters/declarations, which includes the development of action plans to meet any shortfalls or gaps in meeting these standards. The work of this Committee is designed to ensure that assurance can be drawn from the arrangements within the Trust for ensuring compliance with CQC standards. These arrangements have improved throughout the year based on the feedback from the CQC in 2015. The success of the new arrangements will be part of the CQC assessment in July 2016.
“he Trust is subject to an enforcement notice from Monitor reflecting the findings of the 2014 CQC report referred to earlier. This identified the Trust was inadequate in two clinical governance domains and required improving in two. Monitor identified the following governance issues with the Trust:
The lack of effective Board-led strategy development and implementation:
• Weakness in leadership, including an inexperienced Executive Team and unclear
ARA2016 - Acc Section 130616 post audit.indd 13 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A14
division of roles and responsibilities between Executive and Non-Executive positions
• The lack of effective governance structures to support effective accountability, including Board Committees and differing operating models
• Overly centralised systems of control and a lack of an effective system of control for monitoring the quality of care
• The lack of effective risk management arrangements; and
• The lack of effective response to staff escalation of issues
As a result of these findings, the Trust has had an additional condition imposed on license FT(4), which requires the Trust to ensure that it has in place:
• An effectively functioning board and board committees
• Sufficient and effective board, management and clinical leadership capacity and capability; and
• Appropriate governance systems and processes
An Improvement Director has been appointed by Monitor to work with the Trust and the Board to ensure progress is made with the Quality Improvement Plan and related areas of work. The Trust has also entered into a “buddying arrangement” with Nottinghamshire Healthcare NHS FT, which facilitates the sharing of good practice and provides learning opportunities for NSFT.
A Transformation Programme Board was established in the 2014/15 financial year, which is chaired by the Chief Executive to drive and monitor the delivery of the Performance Improvement Plan. Monthly updates on progress are shared at Progress Review meetings with Monitor and other key stakeholders. Progress with the plan is also shared on the NHS Choices website.
As part of the Trust’s continued surveillance of quality we identified a possible increase in unexpected deaths and commissioned a review from an external body, Verita. The outcome of the review will be reported to a public board in line with our commitment to transparency and accountability.
9. Conclusion
To the best of my knowledge and belief, based on the above processes, there are control issues for the Trust relating to the following areas:
• The quality of care provided, resulting in the CQC report
• A lack of sufficiently robust governance systems, structures and processes at board, management and operational levels
However, although the Trust remains in special measures significant improvement has been made ahead of the CQC visit in July 2016.
Signed:
Michael Scott Chief Executive
Date: 25 May 2016
ARA2016 - Acc Section 130616 post audit.indd 14 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A15
These accounts, for the year ended 31 March 2016, have been prepared by Norfolk and Suffolk NHS Foundation Trust in accordance with paragraphs 24 & 25 of Schedule 7 within the National Health Service Act 2006.
Signed:
Michael Scott Chief Executive
Date: 25 May 2016
Foreword to the accounts as the accounting officer of Norfolk and Suffolk NHS Foundation Trust
ARA2016 - Acc Section 130616 post audit.indd 15 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A16
Statement of Comprehensive Income for the year ended 31 March 2016
2015/16 2014/15 restated
Note £000 £000
Operating income from patient care activities 3 197,352 195,335
Other operating income 3.3 14,424 17,496
Total operating income from continuing operations 211,776 212,831
Operating expenses 4 (215,846) (214,850)
Operating deficit from continuing operations (4,070) (2,019)
Finance income 9 32 62
Finance expenses 10, 20 (962) (1,042)
PDC dividends payable (3,911) (3,876)
Net finance costs (4,841) (4,856)
Deficit for the year from continuing operations (8,911) (6,875)
Deficit for the year (8,911) (6,875)
Other comprehensive income
Will not be reclassified to income and expenditure:
Impairments 12.5 (372) (1,331)
Revaluations 12.4 (5) 19,370
Total comprehensive income/(expense) for the period (9,288) 11,164
ARA2016 - Acc Section 130616 post audit.indd 16 14/06/2016 10:25
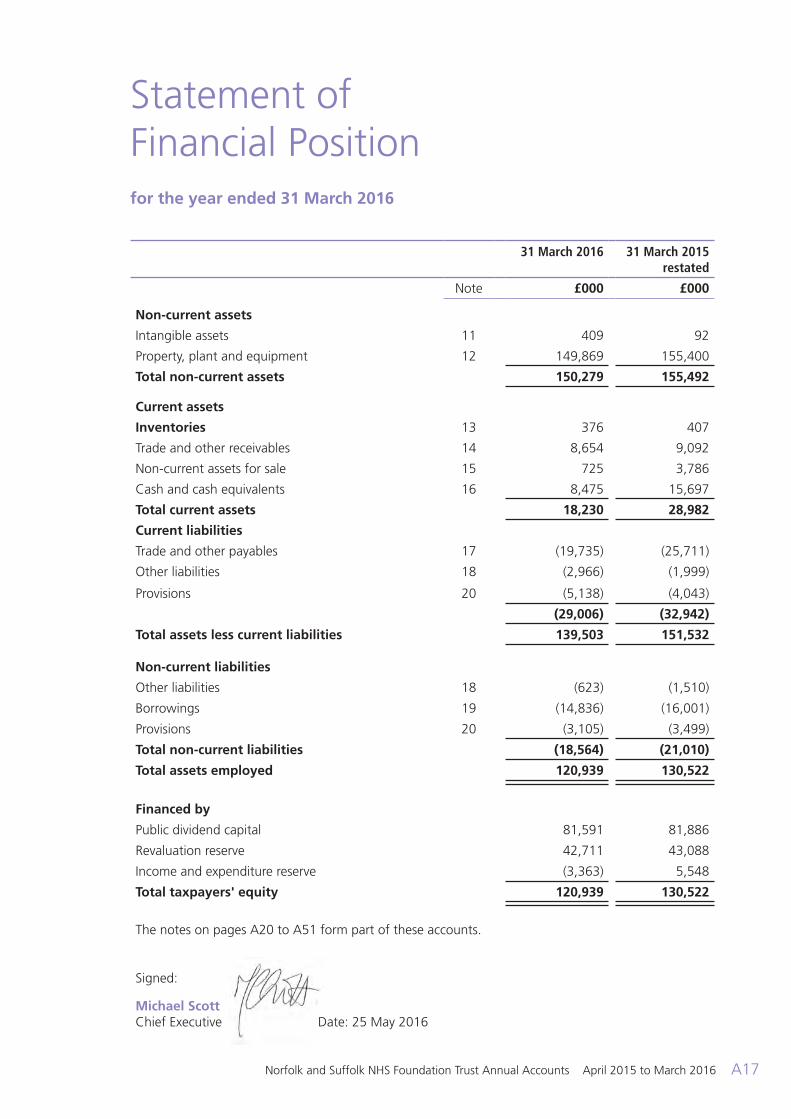
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A17
Statement of Financial Position for the year ended 31 March 2016
31 March 2016 31 March 2015 restated
Note £000 £000
Non-current assets
Intangible assets 11 409 92
Property, plant and equipment 12 149,869 155,400
Total non-current assets 150,279 155,492
Current assets
Inventories 13 376 407
Trade and other receivables 14 8,654 9,092
Non-current assets for sale 15 725 3,786
Cash and cash equivalents 16 8,475 15,697
Total current assets 18,230 28,982
Current liabilities
Trade and other payables 17 (19,735) (25,711)
Other liabilities 18 (2,966) (1,999)
Provisions 20 (5,138) (4,043)
(29,006) (32,942)
Total assets less current liabilities 139,503 151,532
Non-current liabilities
Other liabilities 18 (623) (1,510)
Borrowings 19 (14,836) (16,001)
Provisions 20 (3,105) (3,499)
Total non-current liabilities (18,564) (21,010)
Total assets employed 120,939 130,522
Financed by
Public dividend capital 81,591 81,886
Revaluation reserve 42,711 43,088
Income and expenditure reserve (3,363) 5,548
Total taxpayers' equity 120,939 130,522
The notes on pages A20 to A51 form part of these accounts.
Signed: Michael Scott Chief Executive Date: 25 May 2016
ARA2016 - Acc Section 130616 post audit.indd 17 14/06/2016 10:25
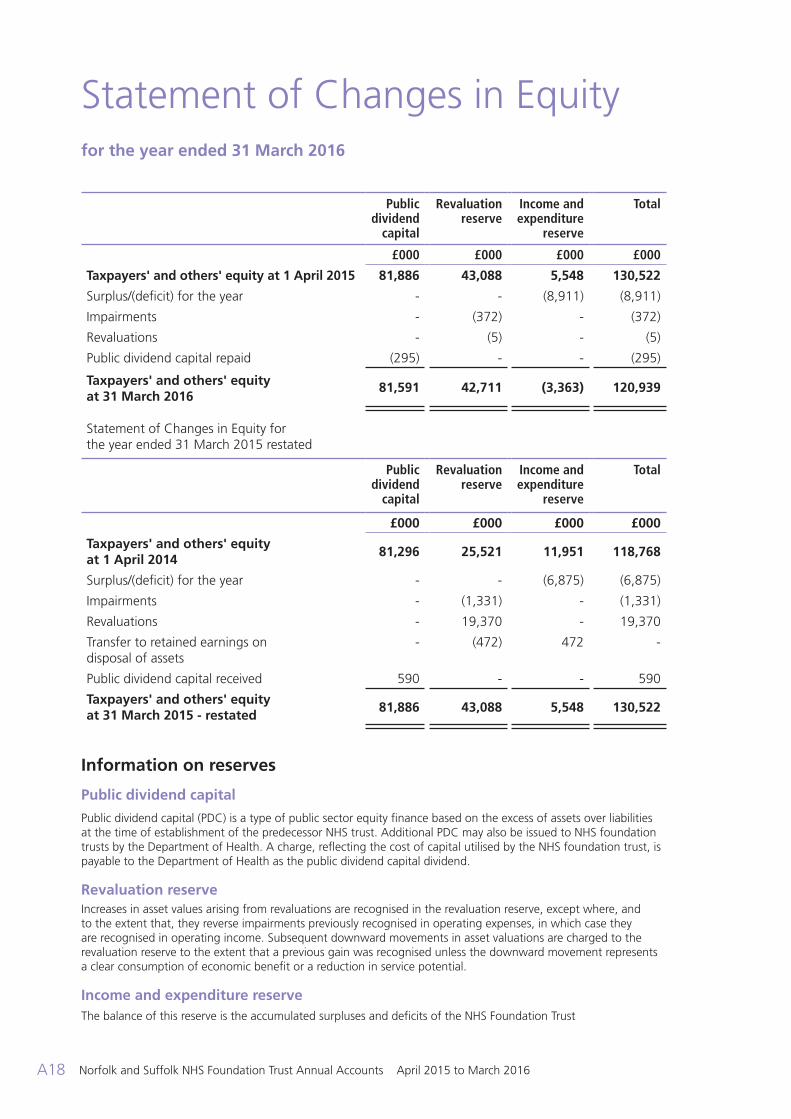
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A18
Statement of Changes in Equity for the year ended 31 March 2016
Public dividend
capital
Revaluation reserve
Income and expenditure
reserve
Total
£000 £000 £000 £000
Taxpayers' and others' equity at 1 April 2015 81,886 43,088 5,548 130,522
Surplus/(deficit) for the year - - (8,911) (8,911)
Impairments - (372) - (372)
Revaluations - (5) - (5)
Public dividend capital repaid (295) - - (295)
Taxpayers' and others' equity at 31 March 2016
81,591 42,711 (3,363) 120,939
Statement of Changes in Equity for the year ended 31 March 2015 restated
Public dividend
capital
Revaluation reserve
Income and expenditure
reserve
Total
£000 £000 £000 £000
Taxpayers' and others' equity at 1 April 2014
81,296 25,521 11,951 118,768
Surplus/(deficit) for the year - - (6,875) (6,875)
Impairments - (1,331) - (1,331)
Revaluations - 19,370 - 19,370
Transfer to retained earnings on disposal of assets
- (472) 472 -
Public dividend capital received 590 - - 590
Taxpayers' and others' equity at 31 March 2015 - restated
81,886 43,088 5,548 130,522
Information on reserves
Public dividend capital Public dividend capital (PDC) is a type of public sector equity finance based on the excess of assets over liabilities at the time of establishment of the predecessor NHS trust. Additional PDC may also be issued to NHS foundation trusts by the Department of Health. A charge, reflecting the cost of capital utilised by the NHS foundation trust, is payable to the Department of Health as the public dividend capital dividend. Revaluation reserve Increases in asset values arising from revaluations are recognised in the revaluation reserve, except where, and to the extent that, they reverse impairments previously recognised in operating expenses, in which case they are recognised in operating income. Subsequent downward movements in asset valuations are charged to the revaluation reserve to the extent that a previous gain was recognised unless the downward movement represents a clear consumption of economic benefit or a reduction in service potential. Income and expenditure reserve The balance of this reserve is the accumulated surpluses and deficits of the NHS Foundation Trust
ARA2016 - Acc Section 130616 post audit.indd 18 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A19
Statement of Cash Flows for the year ended 31 March 2016
2015/16 2014/15
Note £000 £000
Cash flows from operating activities
Operating surplus/(deficit) (4,070) (2,019)
Non-cash income and expense:
Depreciation and amortisation 4.1 6,982 6,555
Impairments and reversals of impairments 5 - 3,308
(Gain)/loss on disposal of non-current assets 3.3 (33) (202)
(Increase)/decrease in receivables and other assets 324 1,086
(Increase)/decrease in inventories 31 (115)
Increase/(decrease) in payables and other liabilities (4,902) 2,211
Increase/(decrease) in provisions 701 (2,642)
Tax (paid)/received 34 (110)
Net cash generated from/(used in) operating activities (933) 8,072
Cash flows from investing activities
Interest received 32 62
Purchase of property, plant, equipment and investment property
(5,290) (7,355)
Sales of property, plant, equipment and investment property 5,213 1,208
Net cash generated from/(used in) investing activities (45) (6,085)
Cash flows from financing activities
Public dividend capital received - 590
Public dividend capital repaid (295) -
Movement on loans from the Department of Health
(1,056) (1,057)
Capital element of PFI, LIFT and other service concession payments
(132) (122)
Interest paid on PFI, LIFT and other service concession obligations
(554) (553)
Other interest paid (410) (440)
PDC dividend paid (3,797) (3,862)
Net cash generated from/(used in) financing activities (6,244) (5,444)
Increase/(decrease) in cash and cash equivalents (7,222) (3,457)
Cash and cash equivalents at 1 April 15,697 19,154
Cash and cash equivalents at 31 March 16.1 8,475 15,697
ARA2016 - Acc Section 130616 post audit.indd 19 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A20
Note 1 Accounting policies and other information
Basis of preparation
Monitor is responsible for issuing an accounts direction to NHS foundation trusts under the NHS Act 2006. Monitor has directed that the financial statements of NHS foundation trusts shall meet the accounting requirements of the FT ARM which shall be agreed with the Secretary of State. Consequently, the following financial statements have been prepared in accordance with the FT ARM 2015/16 issued by Monitor. The accounting policies contained in that manual follow IFRS and HM Treasury’s FReM to the extent that they are meaningful and appropriate to NHS foundation trusts. The accounting policies have been applied consistently in dealing with items considered material in relation to the accounts.
Accounting convention
These accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment, intangible assets, inventories and certain financial assets and financial liabilities.
Going concern
These accounts have been prepared on a going concern basis. Whilst there are control issues for the Trust relating to the quality of the care provided and the governance system structures and processes at board management and operation levels (please refer to the Annual Governance Statement), the Trust Board considers that there is sufficient assurance that there will be a continuation of the provision of services in the future. This decision has been made with reference to future financial plans, and the action plans being developed for the issues noted in the Annual Governance Statement.
Critical accounting judgements and key sources of estimation uncertainty
In the application of the Trust’s accounting policies, management is required to make
judgements, estimates and assumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from those estimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both current and future periods. Where significant accounting judgements have been made, further detail is included in the relevant note e.g. provisions.
Note 1.1 Income
Income in respect of services provided is recognised when, and to the extent that, performance occurs and is measured at the fair value of the consideration receivable. The main source of income for the trust is contracts with commissioners in respect of health care services.
Where income is received for a specific activity which is to be delivered in a subsequent financial year, that income is deferred.
Income from the sale of non-current assets is recognised only when all material conditions of sale have been met, and is measured as the sums due under the sale contract.
Note 1.2 Expenditure on employee benefits Short-term employee benefits
Salaries, wages and employment-related payments are recognised in the period in which the service is received from employees. The cost of annual leave entitlement earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that employees are permitted to carry-forward leave into the following period.
Notes to the Accounts
ARA2016 - Acc Section 130616 post audit.indd 20 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A21
Pension costs
NHS Pension Scheme
Past and present employees are covered by the provisions of the NHS Pension Scheme. The scheme is an unfunded, defined benefit scheme that covers NHS employers, general practices and other bodies, allowed under the direction of Secretary of State, in England and Wales. It is not possible for the NHS foundation trust to identify its share of the underlying scheme liabilities. Therefore, the scheme is accounted for as a defined contribution scheme.
Employer’s pension cost contributions are charged to operating expenses as and when they become due.
Additional pension liabilities arising from early retirements are not funded by the scheme except where the retirement is due to ill-health. The full amount of the liability for the additional costs is charged to the operating expenses at the time the trust commits itself to the retirement, regardless of the method of payment.
Note 1.3 Expenditure on other goods and services
Expenditure on goods and services is recognised when, and to the extent that they have been received, and is measured at the fair value of those goods and services. Expenditure is recognised in operating expenses except where it results in the creation of a non-current asset, such as property, plant and equipment.
Note 1.4 Property, plant and equipment
Recognition
Property, plant and equipment is capitalised where:
• It is held for use in delivering services or for administrative purposes
• It is probable that future economic benefits will flow to, or service potential be provided to, the trust
• It is expected to be used for more than one financial year and
• The cost of the item can be measured reliably.
Where a large asset, for example a building, includes a number of components with significantly different asset lives, eg, plant and equipment, then these components are treated as separate assets and depreciated over their own useful economic lives.
Measurement
Valuation
All property, plant and equipment assets are measured initially at cost, representing the costs directly attributable to acquiring or constructing the asset and bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management.
All assets are measured subsequently at valuation. An item of property, plant and equipment which is surplus with no plan to bring it back into use is valued at fair value under IFRS 13, if it does not meet the requirements of IAS 40 of IFRS 5.
Land and buildings used for the Trust’s services or for administrative purposes are stated in the statement of financial position at their revalued amounts, being the fair value at the date of revaluation less any accumulated depreciation and impairment losses. Fair values are determined as follows:
• Land and non-specialised buildings – market value for existing use
• Specialised buildings – depreciated replacement cost
Non property assets that have short lives and/or their values are low are held at depreciated historic cost.
Revaluations are performed with sufficient regularity to ensure that carrying amounts are not materially different from those that would be determined at the end of the reporting period.
Subsequent expenditure Subsequent expenditure relating to an item of property, plant and equipment is recognised as an increase in the carrying amount of the asset when it is probable that additional future economic benefits or service potential deriving from the cost incurred to replace a component of such item will flow to the enterprise and the cost of the item can be determined reliably.
ARA2016 - Acc Section 130616 post audit.indd 21 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A22
Where a component of an asset is replaced, the cost of the replacement is capitalised if it meets the criteria for recognition above. The carrying amount of the part replaced is de-recognised. Other expenditure that does not generate additional future economic benefits or service potential, such as repairs and maintenance, is charged to the Statement of Comprehensive Income in the period in which it is incurred.” Depreciation Items of property, plant and equipment are depreciated over their remaining useful economic lives in a manner consistent with the consumption of economic or service delivery benefits.
Freehold land is considered to have an infinite life and is not depreciated. For all other assets depreciation is charged to write off the costs or valuation of property, plant and equipment and intangible non-current assets, less any residual value, over their estimated useful lives, in a manner that reflects the consumption of economic benefits or service potential of the assets.
The estimated useful life of an asset is the period over which the Trust expects to obtain economic benefits or service potential from the asset. This is specific to the Trust and may be shorter than the physical life of the asset itself. Estimated useful lives and residual values are reviewed each year-end, with the effect of any changes recognised on a prospective basis.
Property, plant and equipment which have been reclassified as ‘Held for Sale’ cease to be depreciated upon the reclassification.
Assets in the course of construction and residual interests in off-Statement of Financial Position PFI contract assets are not depreciated until the asset is brought into use or reverts to the trust, respectively.
Revaluation gains and losses Revaluation gains are recognised in the revaluation reserve, except where, and to the extent that, they reverse a revaluation decrease that has previously been recognised in operating expenses, in which case they are recognised in operating income.
Revaluation losses are charged to the revaluation reserve to the extent that there is an available balance for the asset concerned, and thereafter are charged to operating expenses.
Gains and losses recognised in the revaluation reserve are reported in the Statement of Comprehensive Income as an item of ‘other comprehensive income’.
Impairments
In accordance with the FT ARM, impairments that arise from a clear consumption of economic benefits or of service potential in the asset are charged to operating expenses. A compensating transfer is made from the revaluation reserve to the income and expenditure reserve of an amount equal to the lower of (i) the impairment charged to operating expenses; and (ii) the balance in the revaluation reserve attributable to that asset before the impairment.
An impairment that arises from a clear consumption of economic benefit or of service potential is reversed when, and to the extent that, the circumstances that gave rise to the loss is reversed. Reversals are recognised in operating income to the extent that the asset is restored to the carrying amount it would have had if the impairment had never been recognised. Any remaining reversal is recognised in the revaluation reserve. Where, at the time of the original impairment, a transfer was made from the revaluation reserve to the income and expenditure reserve, an amount is transferred back to the revaluation reserve when the impairment reversal is recognised.
Other impairments are treated as revaluation losses. Reversals of ‘other impairments’ are treated as revaluation gains.
De-recognition
Assets intended for disposal are reclassified as ‘held for sale’ once all of the following criteria are met:
• The asset is available for immediate sale in its present condition subject only to terms which are usual and customary for such sales
• The sale must be highly probable ie:
- Management are committed to a plan to sell the asset
- An active programme has begun to find a buyer and complete the sale
- The asset is being actively marketed at a reasonable price
- The sale is expected to be completed within 12 months of the date of classification as ‘held for sale’; and
ARA2016 - Acc Section 130616 post audit.indd 22 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A23
- The actions needed to complete the plan indicate it is unlikely that the plan will be dropped or significant changes made to it
Following reclassification, the assets are measured at the lower of their existing carrying amount and their ‘fair value less costs to sell’. Depreciation ceases to be charged. Assets are de-recognised when all material sale contract conditions have been met.
Property, plant and equipment which is to be scrapped or demolished does not qualify for recognition as ‘held for sale’ and instead is retained as an operational asset and the asset’s economic life is adjusted. The asset is de-recognised when scrapping or demolition occurs.
Donated, government grant and other grant funded assets
Donated and grant funded property, plant and equipment assets are capitalised at their fair value on receipt. The donation/grant is credited to income at the same time, unless the donor has imposed a condition that the future economic benefits embodied in the grant are to be consumed in a manner specified by the donor, in which case, the donation / grant is deferred within liabilities and is carried forward to future financial years to the extent that the condition has not yet been met.
The donated and grant funded assets are subsequently accounted for in the same manner as other items of property, plant and equipment.
Private Finance Initiative (PFI) transactions
Private Finance Initiative (PFI) transactions
PFI transactions which meet the IFRIC 12 definition of a service concession, as interpreted in HM Treasury’s FReM, are accounted for as “on-Statement of Financial Position” by the Trust. In accordance with IAS 17, the underlying assets are recognised as property, plant and equipment at their fair value, together with an equivalent finance lease liability. Subsequently, the assets are accounted for as property, plant and equipment and / or intangible assets, as appropriate.
The annual unitary payment is separated into the following component parts, using
appropriate estimation techniques where necessary:
• Payment for the fair value of services received
• Payment for the PFI asset, including finance costs; and
• Payment for the replacement of components of the assets during the contract “lifecycle replacement”
Services received
The fair value of services received in the year is recorded under the relevant expenditure headings within “operating expenses”.
PFI asset
The PFI assets are recognised as property, plant and equipment, when they come into use. The assets are measured initially at fair value in accordance with the principles of IAS 17. Subsequently, the assets are measured at fair value, which is kept up to date in accordance with the Trust’s approach for each relevant class of asset in accordance with the principles of IAS 16.
PFI liability
A PFI liability is recognised at the same time as the PFI assets are recognised. It is measured initially at the same amount as the fair value of the PFI asset and is subsequently measured as a finance lease liability in accordance with IAS 17.
An annual finance cost is calculated by applying the implicit interest rate in the lease on the operating lease liability for the period, and is charged to “Finance Costs” within the Statement of Comprehensive Income.
The element of the annual unitary payment that is allocated as a finance lease rental is applied to meet the annual finance cost and to repay the lease liability over the contract term. An element of the annual unitary payment increase due to cumulative indexation is allocated to the finance lease. In accordance with IAS 17, this amount is not included in the minimum lease payments, but is instead treated as contingent rent and is expensed as incurred. In substance, this amount is a finance cost in respect of the liability and the expense is presented as a contingent finance cost in the Statement of Comprehensive Income.
ARA2016 - Acc Section 130616 post audit.indd 23 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A24
Lifecycle replacement
Lifecycle costs are maintenance costs spread over the term of the contract and form part of the operating expense.
Assets contributed by the Trust to the operator for use in the scheme.
There were no assets contributed by the Trust.
Useful economic lives of property, plant and equipment
Useful economic lives reflect the total life of an asset and not the remaining life of an asset. The range of useful economic lives are shown in the table below:
Min life Max life Years Years
Buildings, excluding dwellings 15 80 Dwellings 30 45 Plant and machinery 5 15 Transport equipment 5 7 Information technology 3 5 Furniture and fittings 5 15
Finance-leased assets (including land) are depreciated over the shorter of the useful economic life or the lease term, unless the FT expects to acquire the asset at the end of the lease term in which case the assets are depreciated in the same manner as owned assets above.
Note 1.5 Intangible assets
Recognition
Intangible assets are non-monetary assets without physical substance which are capable of being sold separately from the rest of the trust’s business or which arise from contractual or other legal rights. They are recognised only where it is probable that future economic benefits will flow to, or service potential be provided to, the trust and where the cost of the asset can be measured reliably.
Software
Software which is integral to the operation of hardware, eg an operating system, is capitalised as part of the relevant item of property, plant
and equipment. Software which is not integral to the operation of hardware, eg application software, is capitalised as an intangible asset. Measurement
Intangible assets are recognised initially at cost, comprising all directly attributable costs needed to create, produce and prepare the asset to the point that it is capable of operating in the manner intended by management.
Subsequently intangible assets are measured at current value in existing use. Where no active market exists, intangible assets are valued at the lower of depreciated replacement cost and the value in use where the asset is income generating. Revaluations gains and losses and impairments are treated in the same manner as for property, plant and equipment. An intangible asset which is surplus with no plan to bring it back into use is valued at fair value under IFRS 13, if it does not meet the requirements of IAS 40 of IFRS 5.
Intangible assets held for sale are measured at the lower of their carrying amount or “fair value less costs to sell”.
Amortisation
Intangible assets are amortised over their expected useful economic lives in a manner consistent with the consumption of economic or service delivery benefits.
Useful economic life of intangible assets
Useful economic lives reflect the total life of an asset and not the remaining life of an asset. The range of useful economic lives are shown in the table below:
Min life Max life Years Years Intangible assets - internally generated
Information technology 3 5 Development expenditure 3 5 Other 3 5
Intangible assets - purchased
Software 3 5 Licences and trademarks 3 5 Patents - - Other - - Goodwill - -
ARA2016 - Acc Section 130616 post audit.indd 24 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A25
Note 1.6 Revenue government and other grants
Government grants are grants from government bodies other than income from commissioners or NHS trusts for the provision of services. Where a grant is used to fund revenue expenditure it is taken to the Statement of Comprehensive Income to match that expenditure.
Note 1.7 Inventories
Inventories are valued at the lower of cost and net realisable value. The cost of inventories is measured using the First In, First Out (FIFO) method.
Note 1.8 Cash and cash equivalents
Cash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents are investments that mature in three months or less from the date of acquisition and that are readily convertible to known amounts of cash with insignificant risk of change in value.
In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an integral part of the Trust’s cash management.
Note 1.9 Financial instruments and financial liabilities
Recognition
Financial assets and financial liabilities which arise from contracts for the purchase or sale of non-financial items (such as goods or services), which are entered into in accordance with the trust’s normal purchase, sale or usage requirements, are recognised when, and to the extent which, performance occurs, ie, when receipt or delivery of the goods or services is made.
De-recognition
All financial assets are de-recognised when the rights to receive cash flows from the assets have expired or the trust has transferred substantially all of the risks and rewards of ownership.
Financial liabilities are de-recognised when the obligation is discharged, cancelled or expires.
Classification and measurement
Financial assets are categorised as “fair value through income and expenditure”, loans and receivables.
Financial liabilities are classified as “fair value through income and expenditure” or as “other financial liabilities”.
Financial assets and financial liabilities at “fair value through income and expenditure”
Financial assets and financial liabilities at “fair value through income and expenditure” are financial assets or financial liabilities held for trading. A financial asset or financial liability is classified in this category if acquired principally for the purpose of selling in the short-term.
Derivatives are also categorised as held for trading unless they are designated as hedges.
Loans and receivables
Loans and receivables are non-derivative financial assets with fixed or determinable payments which are not quoted in an active market. They are included in current assets.
The Trust’s loans and receivables comprise: cash and cash equivalents, NHS receivables, accrued income and “other receivables”.
Loans and receivables are recognised initially at fair value, net of transactions costs, and are measured subsequently at amortised cost, using the effective interest method. The effective interest rate is the rate that discounts exactly estimated future cash receipts through the expected life of the financial asset or, when appropriate, a shorter period, to the net carrying amount of the financial asset.
Interest on loans and receivables is calculated using the effective interest method and credited to the Statement of Comprehensive Income. Loans from the Department of Health are not held for trading and are measured at historic cost with any unpaid interest accrued separately.
ARA2016 - Acc Section 130616 post audit.indd 25 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A26
Available-for-sale financial assets
Available-for-sale financial assets are non-derivative financial assets which are either designated in this category or not classified in any of the other categories. They are included in long-term assets unless the Trust intends to dispose of them within 12 months of the Statement of Financial Position date.
Available-for-sale financial assets are recognised initially at fair value, including transaction costs, and measured subsequently at fair value, with gains or losses recognised in reserves and reported in the Statement of Comprehensive Income as an item of “other comprehensive income”. When items classified as “available-for-sale” are sold or impaired, the accumulated fair value adjustments recognised are transferred from reserves and recognised in “Finance Costs” in the Statement of Comprehensive Income.
Other financial liabilities
All other financial liabilities are recognised initially at fair value, net of transaction costs incurred, and measured subsequently at amortised cost using the effective interest method. The effective interest rate is the rate that discounts exactly estimated future cash payments through the expected life of the financial liability or, when appropriate, a shorter period, to the net carrying amount of the financial liability. They are included in current liabilities except for amounts payable more than 12 months after the Statement of Financial Position date, which are classified as long-term liabilities.
Interest on financial liabilities carried at amortised cost is calculated using the effective interest method and charged to Finance Costs. Interest on financial liabilities taken out to finance property, plant and equipment or intangible assets is not capitalised as part of the cost of those assets.
Note 1.10 Leases
Finance leases
Where substantially all risks and rewards of ownership of a leased asset are borne by the NHS foundation trust, the asset is recorded as property, plant and equipment and a corresponding liability is recorded. The value at which both are recognised is the lower of the fair value of the asset or the present value of the minimum lease payments, discounted using the interest rate implicit in the lease.
The asset and liability are recognised at the commencement of the lease. Thereafter the asset is accounted for an item of property plant and equipment.
The annual rental is split between the repayment of the liability and a finance cost so as to achieve a constant rate of finance over the life of the lease. The annual finance cost is charged to Finance Costs in the Statement of Comprehensive Income. The lease liability, is de-recognised when the liability is discharged, cancelled or expires.
Operating leases
Other leases are regarded as operating leases and the rentals are charged to operating expenses on a straight-line basis over the term of the lease. Operating lease incentives received are added to the lease rentals and charged to operating expenses over the life of the lease.
Leases of land and buildings
Where a lease is for land and buildings, the land component is separated from the building component and the classification for each is assessed separately.
Note 1.11 Provisions
The NHS foundation trust recognises a provision where it has a present legal or constructive obligation of uncertain timing or amount; for which it is probable that there will be a future outflow of cash or other resources; and a reliable estimate can be made of the amount. The amount recognised in the Statement of Financial Position is the best estimate of the resources required to settle the obligation. Where the effect of the time value of money is significant, the estimated risk-adjusted cash flows are discounted using the discount rates published and mandated by HM Treasury.
Clinical negligence costs
The NHS Litigation Authority (NHSLA) operates a risk pooling scheme under which the NHS foundation trust pays an annual contribution to the NHSLA, which, in return, settles all clinical negligence claims. Although the NHSLA is administratively responsible for all clinical negligence cases, the legal liability remains with the NHS foundation trust. The total value of clinical negligence provisions carried by the NHSLA on behalf of the NHS foundation trust is disclosed at note 19.1 but is not recognised in the NHS foundation trust’s accounts.
ARA2016 - Acc Section 130616 post audit.indd 26 14/06/2016 10:25
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A27
Non-clinical risk pooling
The NHS foundation trust participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the trust pays an annual contribution to the NHS Litigation Authority and in return receives assistance with the costs of claims arising. The annual membership contributions, and any “excesses” payable in respect of particular claims are charged to operating expenses when the liability arises.
Note 1.12 Contingencies Contingent assets (that is, assets arising from past events whose existence will only be confirmed by one or more future events not wholly within the entity’s control) are not recognised as assets, but are disclosed where an inflow of economic benefits is probable.
Contingent liabilities are not recognised, but are disclosed, unless the probability of a transfer of economic benefits is remote.
Contingent liabilities are defined as:
• possible obligations arising from past events whose existence will be confirmed only by the occurrence of one or more uncertain future events not wholly within the entity’s control; or
• present obligations arising from past events but for which it is not probable that a transfer of economic benefits will arise or for which the amount of the obligation cannot be measured with sufficient reliability
Note 1.13 Public dividend capital Public dividend capital (PDC) is a type of public sector equity finance based on the excess of assets over liabilities at the time of establishment of the predecessor NHS trust. HM Treasury has determined that PDC is not a financial instrument within the meaning of IAS 32.
A charge, reflecting the cost of capital utilised by the NHS foundation trust, is payable as public dividend capital dividend. The charge is calculated at the rate set by HM Treasury (currently 3.5%) on the average relevant net assets of the NHS foundation trust during the financial year. Relevant net assets are calculated as the value of all assets less the value of all liabilities, except for (i) donated assets (including lottery funded assets), (ii) average daily cash
balances held with the Government Banking Services (GBS) and National Loans Fund (NLF) deposits, excluding cash balances held in GBS accounts that relate to a short-term working capital facility, and (iii) any PDC dividend balance receivable or payable. In accordance with the requirements laid down by the Department of Health (as the issuer of PDC), the dividend for the year is calculated on the actual average relevant net assets as set out in the “pre-audit” version of the annual accounts. The dividend thus calculated is not revised should any adjustment to net assets occur as a result the audit of the annual accounts.
Note 1.14 Value added tax
Most of the activities of the NHS foundation trust are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
Note 1.15 Corporation tax The Trust has determined that there is no corporation tax liability.
Note 1.16 Foreign exchange The functional and presentational currencies of the trust are sterling.
A transaction which is denominated in a foreign currency is translated into the functional currency at the spot exchange rate on the date of the transaction.
Where the trust has assets or liabilities denominated in a foreign currency at the Statement of Financial Position date:
• Monetary items (other than financial instruments measured at “fair value through income and expenditure”) are translated at the spot exchange rate on 31 March
• Non-monetary assets and liabilities measured at historical cost are translated using the spot exchange rate at the date of the transaction; and
ARA2016 - Acc Section 130616 post audit.indd 27 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A28
• non-monetary assets and liabilities measured at fair value are translated using the spot exchange rate at the date the fair value was determined.
Exchange gains or losses on monetary items (arising on settlement of the transaction or on re-translation at the Statement of Financial Position date) are recognised in income or expense in the period in which they arise.
Exchange gains or losses on non-monetary assets and liabilities are recognised in the same manner as other gains and losses on these items.
Note 1.17 Third party assets
Assets belonging to third parties (such as money held on behalf of patients) are not recognised in the accounts since the NHS foundation trust has no beneficial interest in them. However, they are disclosed in a separate note to the accounts in accordance with the requirements of HM Treasury’s FReM.
Note 1.18 Losses and special payments
Losses, and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way that individual cases are handled. Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis, including losses which would have been made good through insurance cover had NHS foundation trusts not been bearing their own risks (with insurance premiums then being included as normal revenue expenditure).
However the losses and special payments note is compiled directly from the losses and compensations register which reports on an accrual basis with the exception of provisions for future losses.
Note 1.19 Early adoption of standards, amendments and interpretations No new accounting standards or revisions to existing standards have been early adopted in 2015/16.
Note 1.20 Prior Period Adjustment
In 2015 a valuation of St Clements Hospital was undertaken which did not take account of the full amount of asbestos within the building. As such the value of the hospital did not include the cost of removal of the asbestos and consequently the impaired value of the hospital was not reflected in the accounts at that time. In accordance with IAS 8 the cost of removal of the asbestos is now reflected in the prior period.
As such the following adjustments are required:
Note 4.1 Operating expenses – Impairments increased by £3,169k to £3,308kNote 15 Non Current Assets held for sale – Impairment of £3,169k includedStatement of Comprehensive Income – Deficit for the year increased to £(6,875)kStatement of Financial Position – Non Current assets for sale and Income and expenditure reserve reduced by £3,169k – Total taxpayers equity reduced to £130,522k
Other related disclosure notes are amended to reflect these changes.
Note 1.21 Standards, amendments and interpretations in issue but not yet effective or adopted
The following table lists changes to standards issued by the International Accounting Standards Board (IASB) which have not yet been adopted herein.
ARA2016 - Acc Section 130616 post audit.indd 28 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A29
Change published Published by IASB Financial year for which the change first applies
IFRS 11 (amendment) – acquisition of an interest in a joint operation
May-14 Not yet EU adopted. Expected to be effective from 2016/17.
IAS 16 (amendment) and IAS 38 (amendment) – depreciation and amortisation
May-14 Not yet EU adopted. Expected to be effective from 2016/17.
IAS 16 (amendment) and IAS 41 (amendment) – bearer plants
Jun-14 Not yet EU adopted. Expected to be effective from 2016/17.
IAS 27 (amendment) – equity method in separate financial statements
Aug-14 Not yet EU adopted. Expected to be effective from 2016/17.
IFRS 10 (amendment) and IAS 28 (amendment) – sale or contribution of assets
Sep-14 Not yet EU adopted. Expected to be effective from 2016/17.
IFRS 10 (amendment) and IAS 28 (amendment) – investment entities applying the consolidation exception
Dec-14 Not yet EU adopted. Expected to be effective from 2016/17.
IAS 1 (amendment) – disclosure initiative
Dec-14 Not yet EU adopted. Expected to be effective from 2016/17.
IFRS 15 Revenue from contracts with customers
May-14 Not yet EU adopted. Expected to be effective from 2017/18.
Annual improvements to IFRS: 2012-15 cycle
Sep-14 Not yet EU adopted. Expected to be effective from 2017/18.
IFRS 9 Financial Instruments Jul-14 Not yet EU adopted. Expected to be effective from 2018/19.
* This reflects the EU-adopted effective date rather than the effective date in the standard.
Note 2 Operating segments
Financial information reported to the Board is at a Trust-wide level, and not reported segmentally. Individual locality issues will be reported on an exceptions basis.
Income from healthcare activities is included at note 3.1 Income from patient care activities - provision of health care services. Income balances with a single external customer that amount to a material proportion of income are disclosed in note 26 to the accounts, Related Party Transactions.
ARA2016 - Acc Section 130616 post audit.indd 29 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A30
Note 3 Operating income from patient care activities
Note 3.1 Income from patient care activities (by nature)
2015/16 2014/15
£000 £000
Mental health services
Block contract income 180,657 176,224
Clinical partnerships providing mandatory services (including S75 agreements)
9,536 11,421
Clinical income for the secondary commissioning of mandatory services
2,235 2,238
Other clinical income from mandatory services 4,910 5,363
All services
Other clinical income 14 89
197,352 195,335
Note 3.2 Income from patient care activities (by source)
2015/16 2014/15
£000 £000
Income from patient care activities received from:
CCGs and NHS England 183,867 179,312
Local authorities 11,136 14,607
Department of Health 295 -
Other NHS foundation trusts 542 273
NHS trusts 207 225
NHS other - 15
Non NHS: other 1,305 903
Total income from activities 197,352 195,335
ARA2016 - Acc Section 130616 post audit.indd 30 14/06/2016 10:25
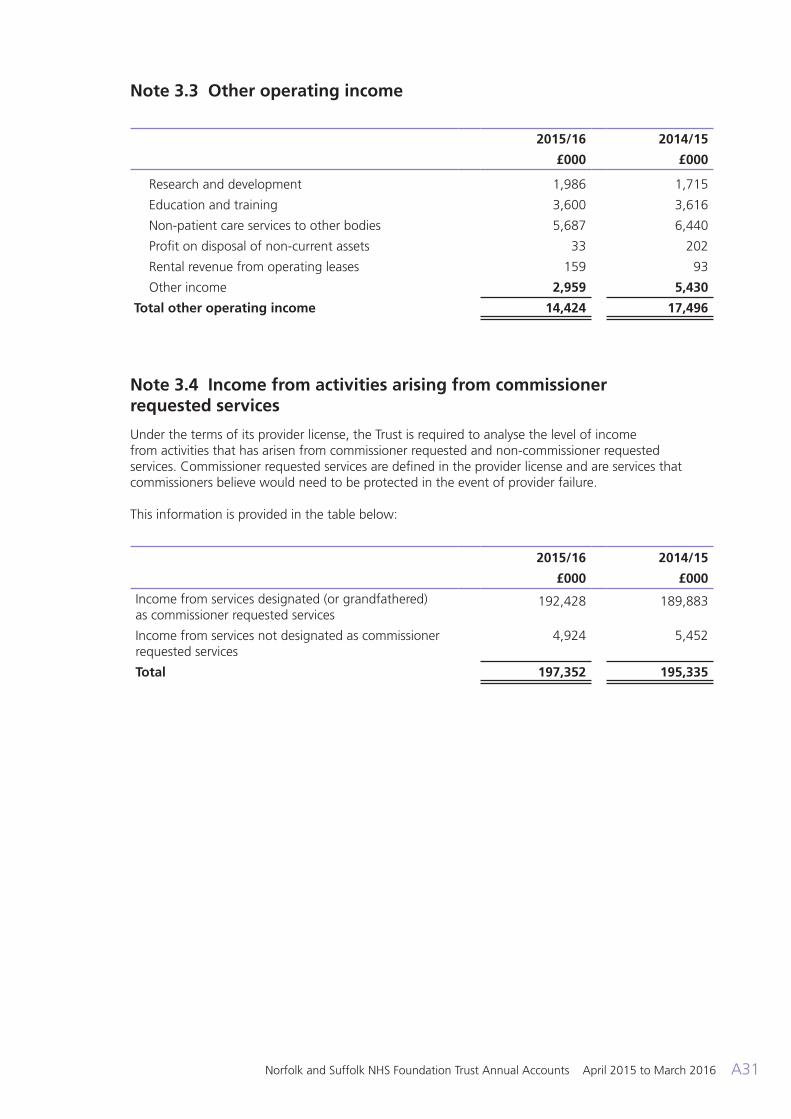
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A31
Note 3.3 Other operating income
2015/16 2014/15
£000 £000
Research and development 1,986 1,715
Education and training 3,600 3,616
Non-patient care services to other bodies 5,687 6,440
Profit on disposal of non-current assets 33 202
Rental revenue from operating leases 159 93
Other income 2,959 5,430
Total other operating income 14,424 17,496
Note 3.4 Income from activities arising from commissioner requested services
Under the terms of its provider license, the Trust is required to analyse the level of income from activities that has arisen from commissioner requested and non-commissioner requested services. Commissioner requested services are defined in the provider license and are services that commissioners believe would need to be protected in the event of provider failure. This information is provided in the table below:
2015/16 2014/15
£000 £000
Income from services designated (or grandfathered) as commissioner requested services
192,428 189,883
Income from services not designated as commissioner requested services
4,924 5,452
Total 197,352 195,335
ARA2016 - Acc Section 130616 post audit.indd 31 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A32
Note 4.1 Operating expenses
2015/16 2014/15
£000 £000
Services from NHS foundation trusts 1,647 1,356
Services from NHS trusts 219 494
Services from CCGs and NHS England 15 -
Services from other NHS bodies 83 16
Purchase of healthcare from non NHS bodies 11,314 11,595
Employee expenses - executive directors 1,170 955
Remuneration of non-executive directors 139 146
Employee expenses - staff 158,292 158,545
Supplies and services - clinical 924 725
Supplies and services - general 7,073 5,592
Establishment 3,846 4,068
Research and development - 37
Transport 2,671 2,603
Premises 8,478 7,540
Increase/(decrease) in provision for impairment of receivables
752 (36)
Increase/(decrease) in other provisions 1,865 -
Drug costs 3,425 3,612
Rentals under operating leases 3,206 2,942
Depreciation on property, plant and equipment 6,819 6,370
Amortisation on intangible assets 163 185
Impairments - 3,308
Audit fees payable to the external auditor
audit services - statutory audit 82 83
Clinical negligence 290 299
Legal fees 73 366
Consultancy costs 229 248
Internal audit costs 171 149
Training, courses and conferences 1,239 1,481
Patient travel 205 475
Car parking & security 144 271
Redundancy 281 317
Hospitality 24 40
Insurance 220 340
Other services, eg external payroll 215 306
Losses, ex gratia & special payments 60 65
Other 512 357
Total 215,846 214,850
ARA2016 - Acc Section 130616 post audit.indd 32 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A33
Note 4.2 Limitation on auditor’s liability
The limitation on auditors’ liability for external audit work is £1m (2014/15: £1m).
Note 5 Impairment of assets
2015/16 2014/15£000 £000
Net impairments charged to operating surplus / deficit resulting from:
Changes in market price - 3,308
Total net impairments charged to operating surplus / deficit - 3,308
Impairments charged to the revaluation reserve 372 1,331
Total net impairments 372 4,639
Note 6 Employee expenses
The aggregate amounts payable to directors were:
2015/16 2014/15Permanent Other Total Total
£000 £000 £000 £000
Salaries and wages 112,531 1,523 114,054 111,835
Social security costs 8,205 - 8,205 8,732
Employer's contributions to NHS pensions 14,505 - 14,505 14,163
Termination benefits 281 - 281 317
NHS Professional bank - 7,956 7,956 8,188
Agency/contract staff - 14,742 14,742 16,582
Total staff costs 135,522 24,221 159,743 159,817
Note 6.1 Retirements due to ill-health
During 2015/16 there were 4 early retirements from the trust agreed on the grounds of ill-health (13 in the year ended 31 March 2015). The estimated additional pension liabilities of these ill-health retirements is £338k (£586k in 2014/15).
The cost of these ill-health retirements will be borne by the NHS Business Services Authority - Pensions Division.
ARA2016 - Acc Section 130616 post audit.indd 33 14/06/2016 10:25
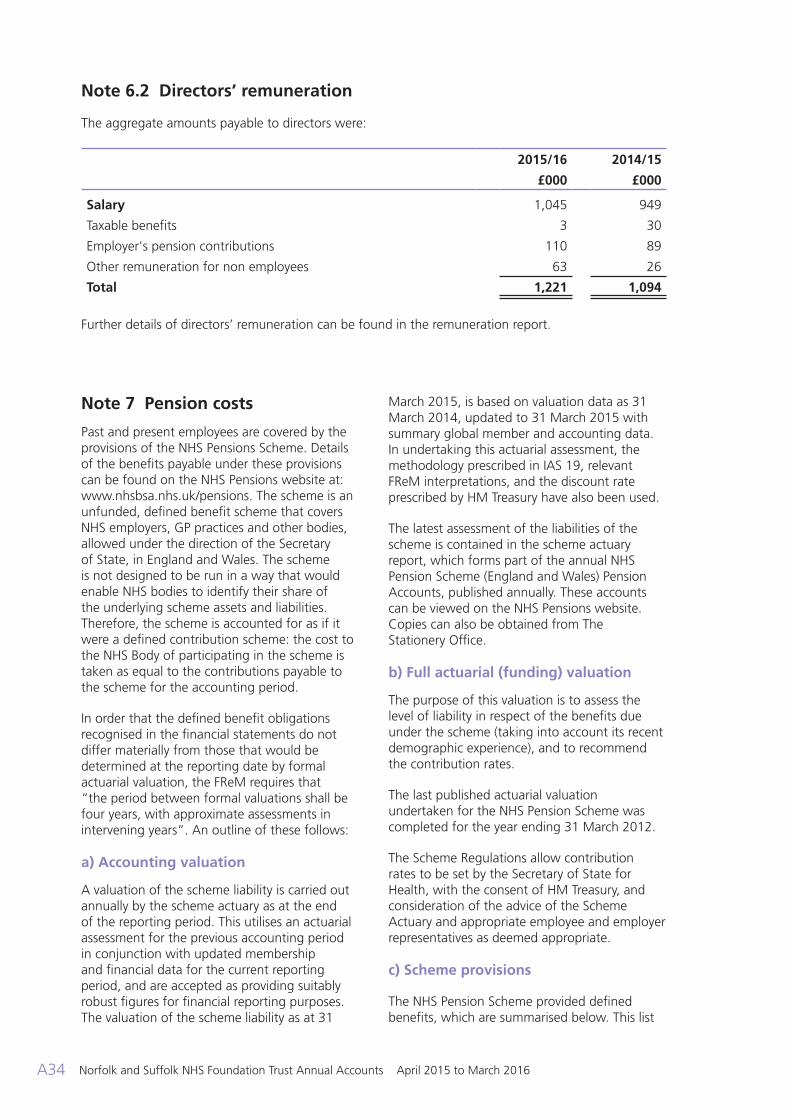
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A34
Note 6.2 Directors’ remuneration
The aggregate amounts payable to directors were:
2015/16 2014/15
£000 £000
Salary 1,045 949
Taxable benefits 3 30
Employer's pension contributions 110 89
Other remuneration for non employees 63 26
Total 1,221 1,094
Further details of directors’ remuneration can be found in the remuneration report.
Note 7 Pension costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. Details of the benefits payable under these provisions can be found on the NHS Pensions website at: www.nhsbsa.nhs.uk/pensions. The scheme is an unfunded, defined benefit scheme that covers NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS Body of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period.
In order that the defined benefit obligations recognised in the financial statements do not differ materially from those that would be determined at the reporting date by formal actuarial valuation, the FReM requires that “the period between formal valuations shall be four years, with approximate assessments in intervening years”. An outline of these follows:
a) Accounting valuation
A valuation of the scheme liability is carried out annually by the scheme actuary as at the end of the reporting period. This utilises an actuarial assessment for the previous accounting period in conjunction with updated membership and financial data for the current reporting period, and are accepted as providing suitably robust figures for financial reporting purposes. The valuation of the scheme liability as at 31
March 2015, is based on valuation data as 31 March 2014, updated to 31 March 2015 with summary global member and accounting data. In undertaking this actuarial assessment, the methodology prescribed in IAS 19, relevant FReM interpretations, and the discount rate prescribed by HM Treasury have also been used.
The latest assessment of the liabilities of the scheme is contained in the scheme actuary report, which forms part of the annual NHS Pension Scheme (England and Wales) Pension Accounts, published annually. These accounts can be viewed on the NHS Pensions website. Copies can also be obtained from The Stationery Office.
b) Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the scheme (taking into account its recent demographic experience), and to recommend the contribution rates.
The last published actuarial valuation undertaken for the NHS Pension Scheme was completed for the year ending 31 March 2012.
The Scheme Regulations allow contribution rates to be set by the Secretary of State for Health, with the consent of HM Treasury, and consideration of the advice of the Scheme Actuary and appropriate employee and employer representatives as deemed appropriate.
c) Scheme provisions
The NHS Pension Scheme provided defined benefits, which are summarised below. This list
ARA2016 - Acc Section 130616 post audit.indd 34 14/06/2016 10:25
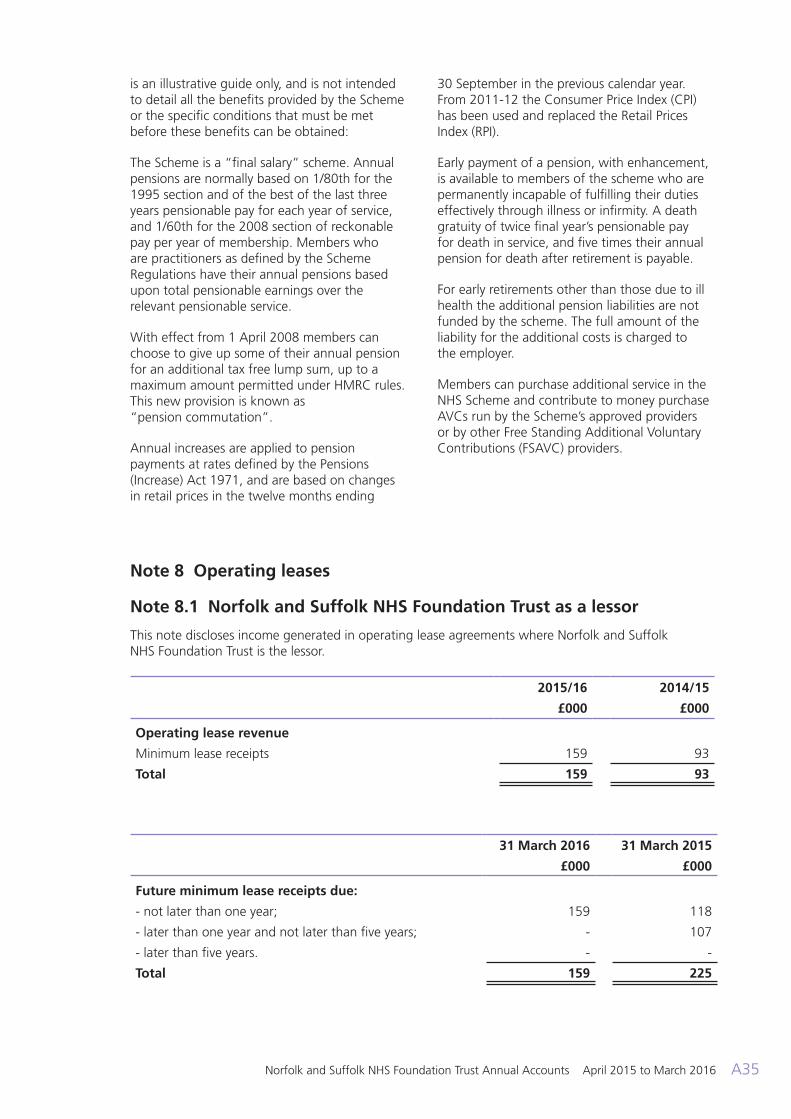
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A35
is an illustrative guide only, and is not intended to detail all the benefits provided by the Scheme or the specific conditions that must be met before these benefits can be obtained:
The Scheme is a “final salary” scheme. Annual pensions are normally based on 1/80th for the 1995 section and of the best of the last three years pensionable pay for each year of service, and 1/60th for the 2008 section of reckonable pay per year of membership. Members who are practitioners as defined by the Scheme Regulations have their annual pensions based upon total pensionable earnings over the relevant pensionable service.
With effect from 1 April 2008 members can choose to give up some of their annual pension for an additional tax free lump sum, up to a maximum amount permitted under HMRC rules. This new provision is known as “pension commutation”.
Annual increases are applied to pension payments at rates defined by the Pensions (Increase) Act 1971, and are based on changes in retail prices in the twelve months ending
30 September in the previous calendar year. From 2011-12 the Consumer Price Index (CPI) has been used and replaced the Retail Prices Index (RPI).
Early payment of a pension, with enhancement, is available to members of the scheme who are permanently incapable of fulfilling their duties effectively through illness or infirmity. A death gratuity of twice final year’s pensionable pay for death in service, and five times their annual pension for death after retirement is payable.
For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to the employer.
Members can purchase additional service in the NHS Scheme and contribute to money purchase AVCs run by the Scheme’s approved providers or by other Free Standing Additional Voluntary Contributions (FSAVC) providers.
Note 8 Operating leases
Note 8.1 Norfolk and Suffolk NHS Foundation Trust as a lessor
This note discloses income generated in operating lease agreements where Norfolk and Suffolk NHS Foundation Trust is the lessor.
2015/16 2014/15
£000 £000
Operating lease revenue
Minimum lease receipts 159 93
Total 159 93
31 March 2016 31 March 2015
£000 £000
Future minimum lease receipts due:
- not later than one year; 159 118
- later than one year and not later than five years; - 107
- later than five years. - -
Total 159 225
ARA2016 - Acc Section 130616 post audit.indd 35 14/06/2016 10:25
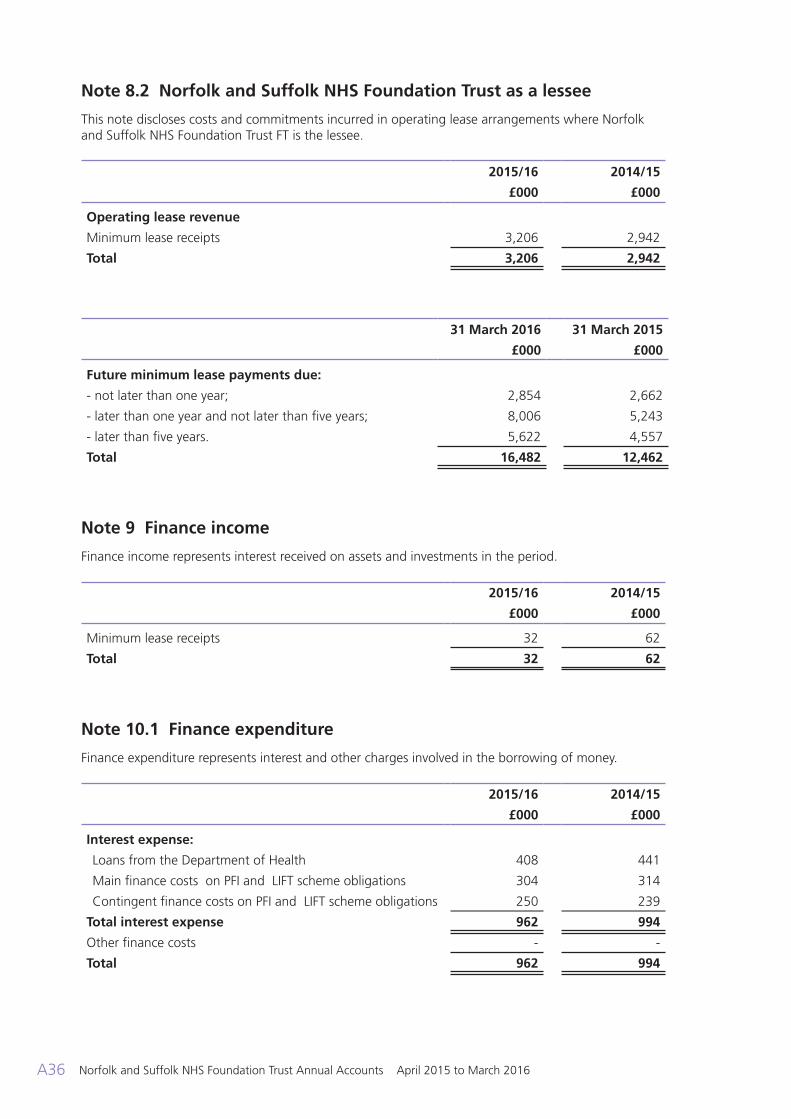
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A36
Note 8.2 Norfolk and Suffolk NHS Foundation Trust as a lessee
This note discloses costs and commitments incurred in operating lease arrangements where Norfolk and Suffolk NHS Foundation Trust FT is the lessee.
2015/16 2014/15
£000 £000
Operating lease revenue
Minimum lease receipts 3,206 2,942
Total 3,206 2,942
31 March 2016 31 March 2015
£000 £000
Future minimum lease payments due:
- not later than one year; 2,854 2,662
- later than one year and not later than five years; 8,006 5,243
- later than five years. 5,622 4,557
Total 16,482 12,462
Note 9 Finance income
Finance income represents interest received on assets and investments in the period.
2015/16 2014/15
£000 £000
Minimum lease receipts 32 62
Total 32 62
Note 10.1 Finance expenditure
Finance expenditure represents interest and other charges involved in the borrowing of money.
2015/16 2014/15
£000 £000
Interest expense:
Loans from the Department of Health 408 441
Main finance costs on PFI and LIFT scheme obligations 304 314
Contingent finance costs on PFI and LIFT scheme obligations 250 239
Total interest expense 962 994
Other finance costs - -
Total 962 994
ARA2016 - Acc Section 130616 post audit.indd 36 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A37
Note 10.2 Better Payment Practice Code
2015/16 2014/15Number Value Number Value
£000 £000
Total Non-NHS trade invoices paid in the year 27,170 69,016 34,057 69,774
Total Non-NHS trade invoices paid within target 22,818 59,235 29,103 60,278
84% 86% 85% 86%
Total NHS trade invoices paid in the year 771 5,681 1,081 6,193
Total NHS trade invoices paid within target 573 4,183 859 4,846
Percentage paid within target 74% 74% 79% 78%
Note 11.1 Intangible assets - 2015/16
Software licences
Total
£000 £000
Valuation/gross cost at 1 April 2015 564 564
Reclassifications 480 480
Gross cost at 31 March 2016 1,044 1,044
Amortisation at 1 April 2015 472 472
Provided during the year 163 163
Amortisation at 31 March 2016 635 635
Net book value at 31 March 2016 409 409
Net book value at 1 April 2015 92 92
Note 11.2 Intangible assets - 2014/15
Software licences
Total
£000 £000
Valuation/gross cost at 1 April 2014 1,461 1,461
Reclassifications (897) (897)
Valuation/gross cost at 31 March 2015 564 564
Amortisation at 1 April 2014 1,184 1,184
Provided during the year 185 185
Reclassifications (897) (897)
Amortisation at 31 March 2015 472 472
Net book value at 31 March 2015 92 92
Net book value at 1 April 2014 277 277
ARA2016 - Acc Section 130616 post audit.indd 37 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A38
Note 12.1 Property, plant and equipment - 2015/16
Land Buildings excluding dwellings
Dwellings Assets under
construction
Plant and machinery
Transport equipment
Information technology
Furniture and
fittings
Total
£000 £000 £000 £000 £000 £000 £000 £000 £000
Valuation/ gross cost at 1 April 2015
21,044 115,793 4,523 9,475 5,045 319 10,242 3,171 169,612
Additions - - - 4,297 - - - - 4,297
Impairments - (372) - - - - - - (372)
Reclassifications - 6,214 - (10,046) 256 - 2,930 165 (481)
Re-presentation of historical balances
37 (2,734) - (201) (324) 6 (2,625) (718) (6,559)
Transfers to / from assets held for sale
(1,164) (1,008) - - (16) - - - (2,188)
Valuation / gross cost at 31 March 2016
19,917 117,893 4,523 3,525 4,961 325 10,547 2,618 164,309
Accumulated depreciation at 1 April 2015
- 2,860 - 138 2,610 319 6,499 1,786 14,212
Provided during the year
- 4,267 123 - 472 4 1,600 353 6,819
Reclassifications 37 (5,590) - (344) (646) 4 (5,458) (1,123) (13,120)
Revaluations - 5 - - - - - - 5
Re-presentation of historical balances
- 2,860 - 138 326 (2) 2,833 405 6,560
Transfers to / from assets held for sale
- (24) - - (12) - - - (36)
Accumulated depreciation at 31 March 2016
37 4,378 123 (68) 2,750 325 5,474 1,421 14,440
Net book value at 31 March 2016
19,880 113,515 4,400 3,593 2,211 - 5,073 1,197 149,869
Net book value at 1 April 2015
21,044 112,933 4,523 9,337 2,435 - 3,743 1,385 155,400
ARA2016 - Acc Section 130616 post audit.indd 38 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A39
Note 12.2 Property, plant and equipment - 2014/15
Land Buildings excluding dwellings
Dwellings Assets under
construction
Plant and machinery
Transport equipment
Information technology
Furniture and
fittings
Total
£000 £000 £000 £000 £000 £000 £000 £000 £000
Valuation/gross cost at 1 April 2014
23,616 106,560 3,212 7,956 5,812 326 10,416 6,533 164,431
Additions - - - 7,563 - - - - 7,563
Impairments (217) (411) (703) - - - - - (1,331)
Reclassifications 92 2,086 762 (6,044) 1,071 (7) 473 (2,773) (4,340)
Revaluations 867 11,801 1,252 - - - - - 13,920
Transfers to/ from assets held for sale
(3,314) (4,078) - - (5) - - - (7,397)
Disposals / derecognition
- (165) - - (1,833) - (647) (589) (3,234)
Valuation/gross cost at 31 March 2015
21,044 115,793 4,523 9,475 5,045 319 10,242 3,171 169,612
Accumulated depreciation at 1 April 2014
- 4,282 98 (1) 3,093 326 7,909 5,181 20,888
Provided during the year
- 4,144 117 - 494 6 1,278 331 6,370
Impairments - - - 139 - - - - 139
Reclassifications - - - - 858 (13) (2,048) (3,137) (4,340)
Revaluations - (5,235) (215) - - - - - (5,450)
Transfers to/ from assets held for sale
- (160) - - (2) - - - (162)
Disposals / derecognition
- (171) - - (1,833) - (640) (589) (3,233)
Accumulated depreciation at 31 March 2015
- 2,860 - 138 2,610 319 6,499 1,786 14,212
Net book value at 31 March 2015
21,044 112,933 4,523 9,337 2,435 - 3,743 1,385 155,400
Net book value at 1 April 2014
23,616 102,278 3,114 7,957 2,719 - 2,507 1,352 143,543
ARA2016 - Acc Section 130616 post audit.indd 39 14/06/2016 10:25
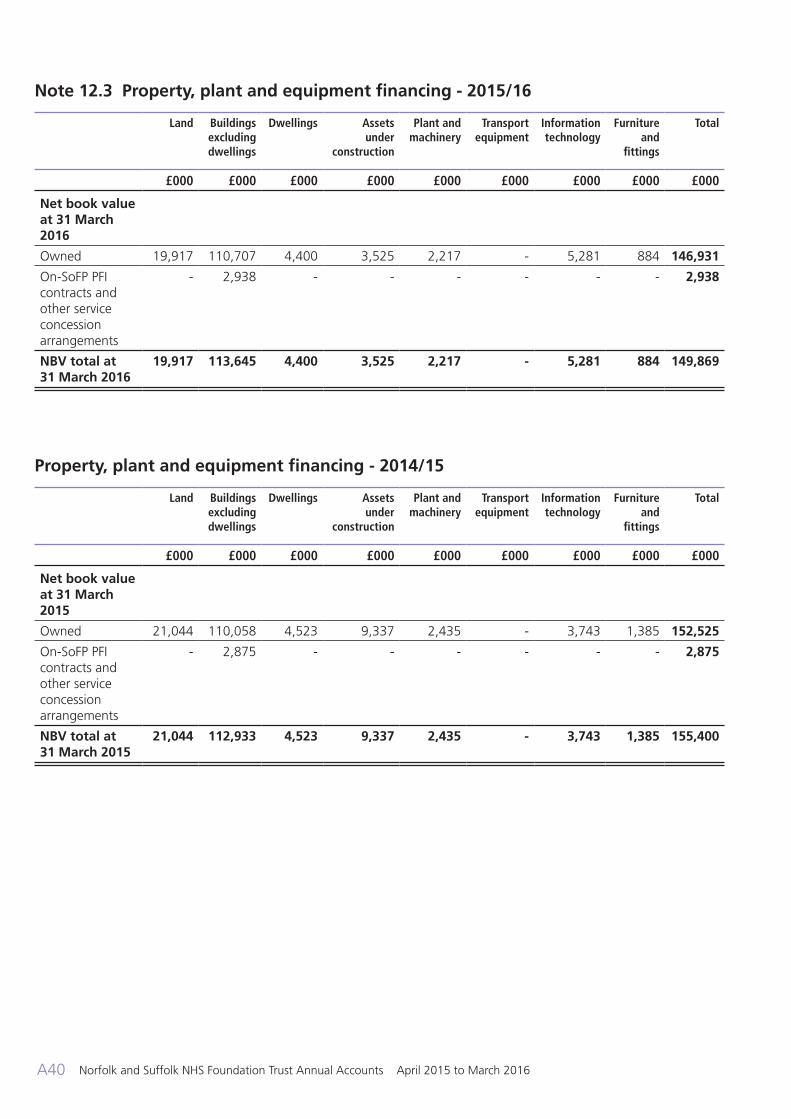
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A40
Note 12.3 Property, plant and equipment financing - 2015/16
Land Buildings excluding dwellings
Dwellings Assets under
construction
Plant and machinery
Transport equipment
Information technology
Furniture and
fittings
Total
£000 £000 £000 £000 £000 £000 £000 £000 £000
Net book value at 31 March 2016
Owned 19,917 110,707 4,400 3,525 2,217 - 5,281 884 146,931
On-SoFP PFI contracts and other service concession arrangements
- 2,938 - - - - - - 2,938
NBV total at 31 March 2016
19,917 113,645 4,400 3,525 2,217 - 5,281 884 149,869
Property, plant and equipment financing - 2014/15
Land Buildings excluding dwellings
Dwellings Assets under
construction
Plant and machinery
Transport equipment
Information technology
Furniture and
fittings
Total
£000 £000 £000 £000 £000 £000 £000 £000 £000
Net book value at 31 March 2015
Owned 21,044 110,058 4,523 9,337 2,435 - 3,743 1,385 152,525
On-SoFP PFI contracts and other service concession arrangements
- 2,875 - - - - - - 2,875
NBV total at 31 March 2015
21,044 112,933 4,523 9,337 2,435 - 3,743 1,385 155,400
ARA2016 - Acc Section 130616 post audit.indd 40 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A41
Note 12.4 Revaluations of property, plant and equipment
The last full valuation of all land and buildings was undertaken as at 31 March 2015 on the basis set out in the accounting policies. Valuations are carried out by professionally qualified valuers in accordance with the Royal Institute of Chartered Surveyors (RICS) Appraisal and Valuation Manual, in so far that these terms are consistent with the agreed requirements of the Department of Health and HM Treasury at that time. The revaluation was performed by Boshier and Company Chartered Surveyors. A full valuation is undertaken every five years, and interim valuations are undertaken every three years. The next interim revaluation will take place in 2017/18.
Impairment reviews are undertaken annually to ensure that the carrying values reflect fair values. £372k of impairments have been have been recognised in the 2015/16 financial year (£1,331k - 2014/15).
The Trust is the lessor of assets on operating leases. These leases are immaterial in value and relate to the renting of a small part of an owned asset (e.g. part of a building, space on a roof) and therefore this is not accounted for separately to the overall asset in terms of depreciation and impairments.
Reclassifications included above also include assets under construction reclassified as intangible assets.
Note 13 Inventories
31 March 2016 31 March 2015
£000 £000
Drugs 376 407
Total inventories 376 407
Inventories recognised in expenses for the year were £1,304k (2014/15: £105k). Write-down of inventories recognised as expenses for the year were £0k (2014/15: £0k).
Note 14.1 Trade receivables and other receivables
31 March 2016 31 March 2015
£000 £000
Current
Trade receivables due from NHS bodies 3,027 2,801
Other receivables due from related parties 388 1,100
Provision for impaired receivables (864) (118)
Prepayments (non-PFI) 1,513 2,060
Accrued income 806 750
PDC dividend receivable - 114
VAT receivable 423 400
Other receivables 3,361 1,985
Total current trade and other receivables 8,654 9,092
ARA2016 - Acc Section 130616 post audit.indd 41 14/06/2016 10:25
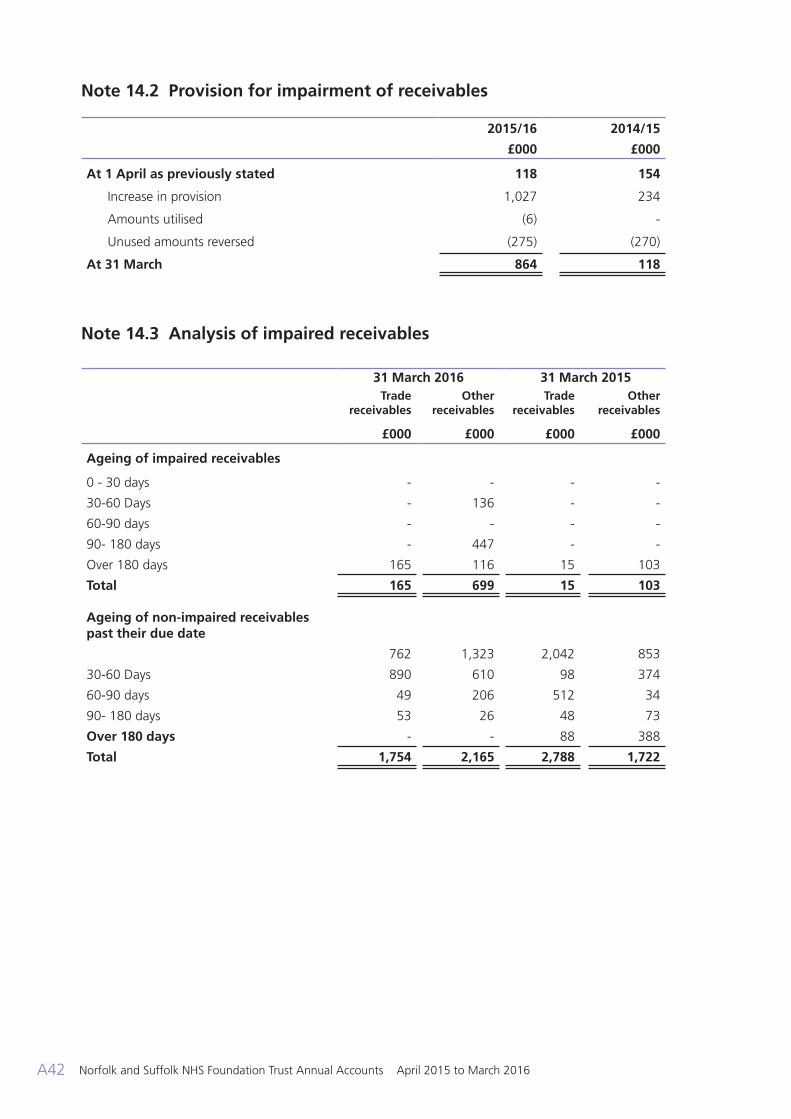
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A42
Note 14.2 Provision for impairment of receivables
2015/16 2014/15
£000 £000
At 1 April as previously stated 118 154
Increase in provision 1,027 234
Amounts utilised (6) -
Unused amounts reversed (275) (270)
At 31 March 864 118
Note 14.3 Analysis of impaired receivables
31 March 2016 31 March 2015Trade
receivablesOther
receivablesTrade
receivablesOther
receivables
£000 £000 £000 £000
Ageing of impaired receivables
0 - 30 days - - - -
30-60 Days - 136 - -
60-90 days - - - -
90- 180 days - 447 - -
Over 180 days 165 116 15 103
Total 165 699 15 103
Ageing of non-impaired receivables past their due date
762 1,323 2,042 853
30-60 Days 890 610 98 374
60-90 days 49 206 512 34
90- 180 days 53 26 48 73
Over 180 days - - 88 388
Total 1,754 2,165 2,788 1,722
ARA2016 - Acc Section 130616 post audit.indd 42 14/06/2016 10:25
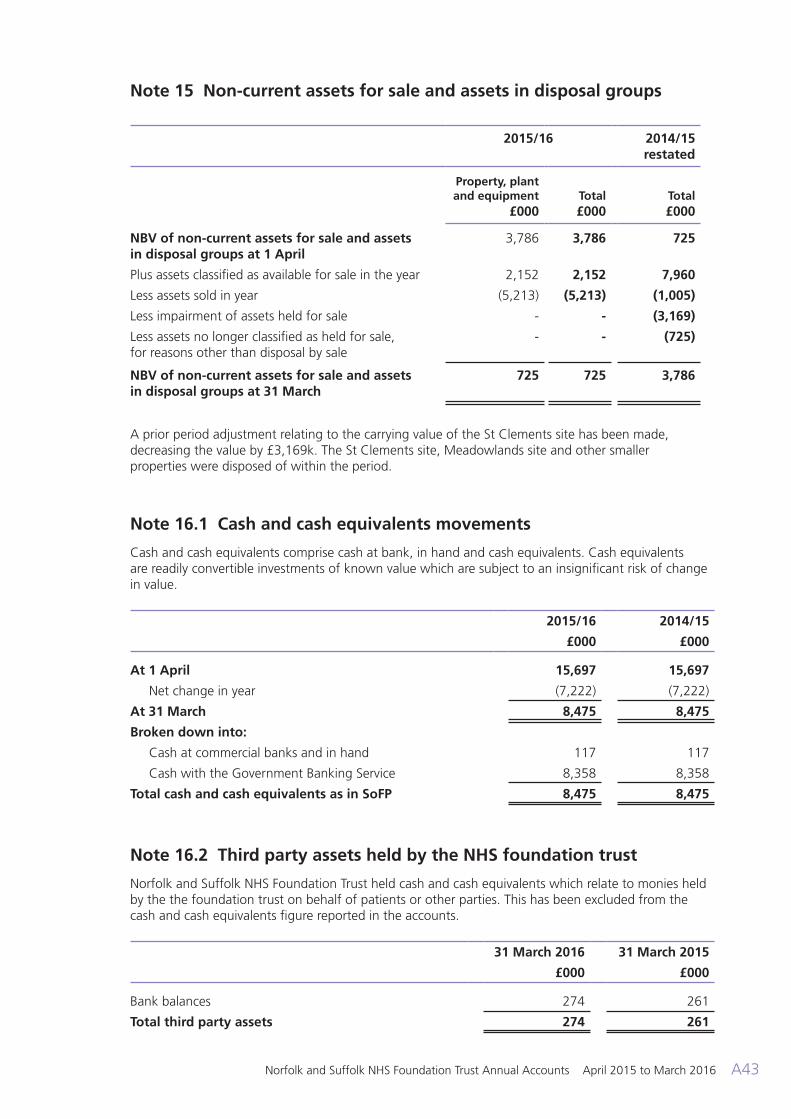
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A43
Note 15 Non-current assets for sale and assets in disposal groups
2015/16 2014/15 restated
Property, plant and equipment
£000Total £000
Total £000
NBV of non-current assets for sale and assets in disposal groups at 1 April
3,786 3,786 725
Plus assets classified as available for sale in the year 2,152 2,152 7,960
Less assets sold in year (5,213) (5,213) (1,005)
Less impairment of assets held for sale - - (3,169)
Less assets no longer classified as held for sale, for reasons other than disposal by sale
- - (725)
NBV of non-current assets for sale and assets in disposal groups at 31 March
725 725 3,786
A prior period adjustment relating to the carrying value of the St Clements site has been made, decreasing the value by £3,169k. The St Clements site, Meadowlands site and other smaller properties were disposed of within the period.
Note 16.1 Cash and cash equivalents movements
Cash and cash equivalents comprise cash at bank, in hand and cash equivalents. Cash equivalents are readily convertible investments of known value which are subject to an insignificant risk of change in value.
2015/16 2014/15
£000 £000
At 1 April 15,697 15,697
Net change in year (7,222) (7,222)
At 31 March 8,475 8,475
Broken down into:
Cash at commercial banks and in hand 117 117
Cash with the Government Banking Service 8,358 8,358
Total cash and cash equivalents as in SoFP 8,475 8,475
Note 16.2 Third party assets held by the NHS foundation trust
Norfolk and Suffolk NHS Foundation Trust held cash and cash equivalents which relate to monies held by the the foundation trust on behalf of patients or other parties. This has been excluded from the cash and cash equivalents figure reported in the accounts.
31 March 2016 31 March 2015
£000 £000
Bank balances 274 261
Total third party assets 274 261
ARA2016 - Acc Section 130616 post audit.indd 43 14/06/2016 10:25
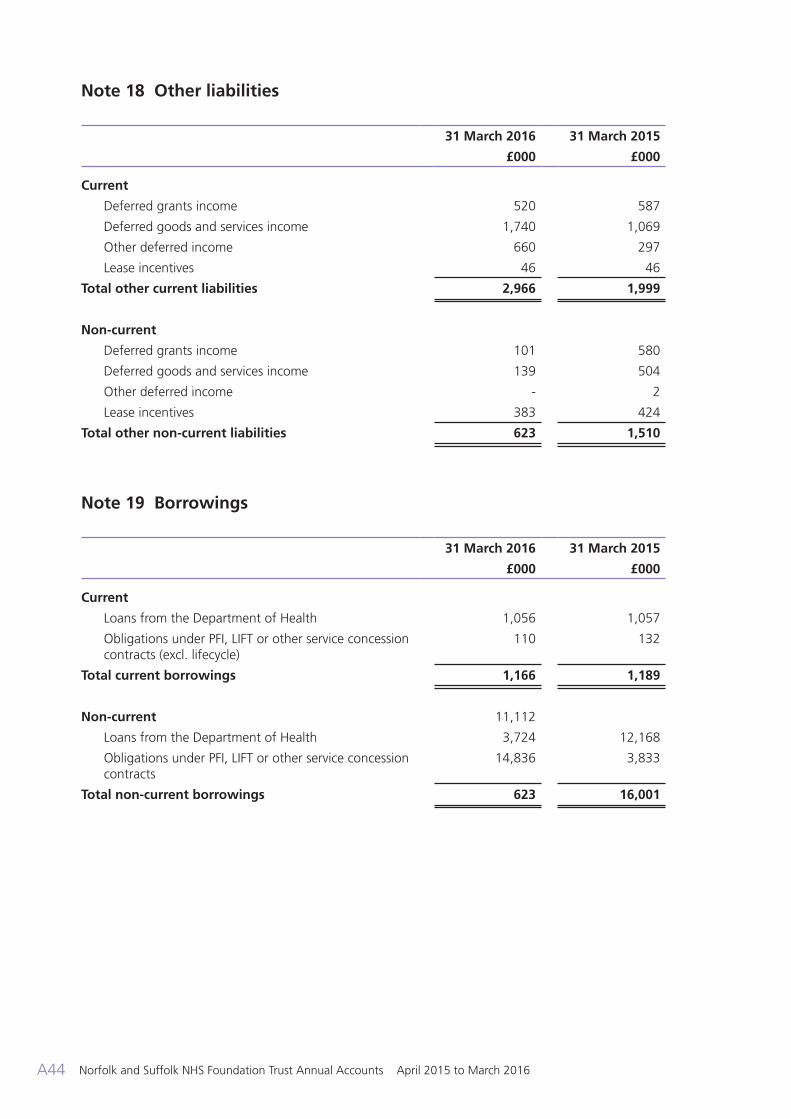
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A44
Note 18 Other liabilities
31 March 2016 31 March 2015
£000 £000
Current
Deferred grants income 520 587
Deferred goods and services income 1,740 1,069
Other deferred income 660 297
Lease incentives 46 46
Total other current liabilities 2,966 1,999
Non-current
Deferred grants income 101 580
Deferred goods and services income 139 504
Other deferred income - 2
Lease incentives 383 424
Total other non-current liabilities 623 1,510
Note 19 Borrowings
31 March 2016 31 March 2015
£000 £000
Current
Loans from the Department of Health 1,056 1,057
Obligations under PFI, LIFT or other service concession contracts (excl. lifecycle)
110 132
Total current borrowings 1,166 1,189
Non-current 11,112
Loans from the Department of Health 3,724 12,168
Obligations under PFI, LIFT or other service concession contracts
14,836 3,833
Total non-current borrowings 623 16,001
ARA2016 - Acc Section 130616 post audit.indd 44 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A45
Note 20 Provisions for liabilities and charges analysis
Pensions - other staff
Other legal
claims
Redundancy Other Total
£000 £000 £000 £000 £000
At 1 April 2015 1,958 481 364 4,739 7,542 Arising during the year - 250 652 3,428 4,330
Utilised during the year (260) (145) (391) (368) (1,164)
Reversed unused - (130) - (2,335) (2,465)
At 31 March 2016 1,698 456 625 5,464 8,243
Expected timing of cash flows:
- not later than one year; 259 456 625 3,798 5,138
- later than one year and not later than five years;
476 - - 495 971
- later than five years. 963 - - 1,171 2,134
Total 1,698 456 625 5,464 8,243
The pensions’ provision relates to the NHS Pensions Agency in respect of early retirement awards, payable to former employees of the Trust is calculated using actuarial information on named individuals and is reviewed on a quarterly basis.
The provision for legal claims relates to unresolved claims arising from tribunal hearings, equal pay claims, clinical negligence claims, and other legal matters. Other provisions include £1,802k in respect of Injury Benefits awards. Other provisions have been made for service redesign and other potential liabiltiies
The value and expected timings of the injury benefit provisions are calculated by reference to information available at the balance sheet date, provided by the Trust’s advisors. As new evidence comes to light, the value of the provision can change either up or down. Similarly, new evidence can affect the expected timings of cashflows.
Note 20.1 Clinical negligence liabilites
At 31 March 2016, £3,277k was included in provisions of the NHSLA in respect of clinical negligence liabilities of Norfolk and Suffolk NHS Foundation Trust (31 March 2015 £1,879k).
Note 20.2 Contractual capital commitments
As at 31 March 2016, the Trust had entered into contract to purchase property plant and equipment for £1,241k (31 March 2015 £403k). These commitments are expected to be settled in the following financial year.
ARA2016 - Acc Section 130616 post audit.indd 45 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A46
Note 21.1 Imputed finance lease obligations
The trust has the following obligations in respect of the finance lease element of on-Statement of Financial Position PFI and LIFT schemes:
31 March 2016 31 March 2015
£000 £000
Gross PFI, LIFT or other service concession liabilities 12,053 13,753
Of which liabilities are due
- not later than one year; 695 694
- later than one year and not later than five years; 2,872 2,924
- later than five years. 8,486 10,135
Finance charges allocated to future periods (8,219) (9,788)
Net PFI, LIFT or other service concession arrangement obligation
3,834 3,965
- not later than one year; 110 132
- later than one year and not later than five years; 694 644
- later than five years. 3,030 3,189
Note 21.2 Total on-SoFP PFI, LIFT and other service concession arrangement commitments
The trust’s total future obligations under these on-SoFP schemes are as follows:
31 March 2016 31 March 2015
£000 £000
Total future payments committed in respect of the PFI, LIFT or other service concession arrangements
32,753 34,608
Of which liabilities are due:
- not later than one year; 1,855 1,855
- later than one year and not later than five years; 7,664 7,664
- later than five years 23,234 25,089
ARA2016 - Acc Section 130616 post audit.indd 46 14/06/2016 10:25
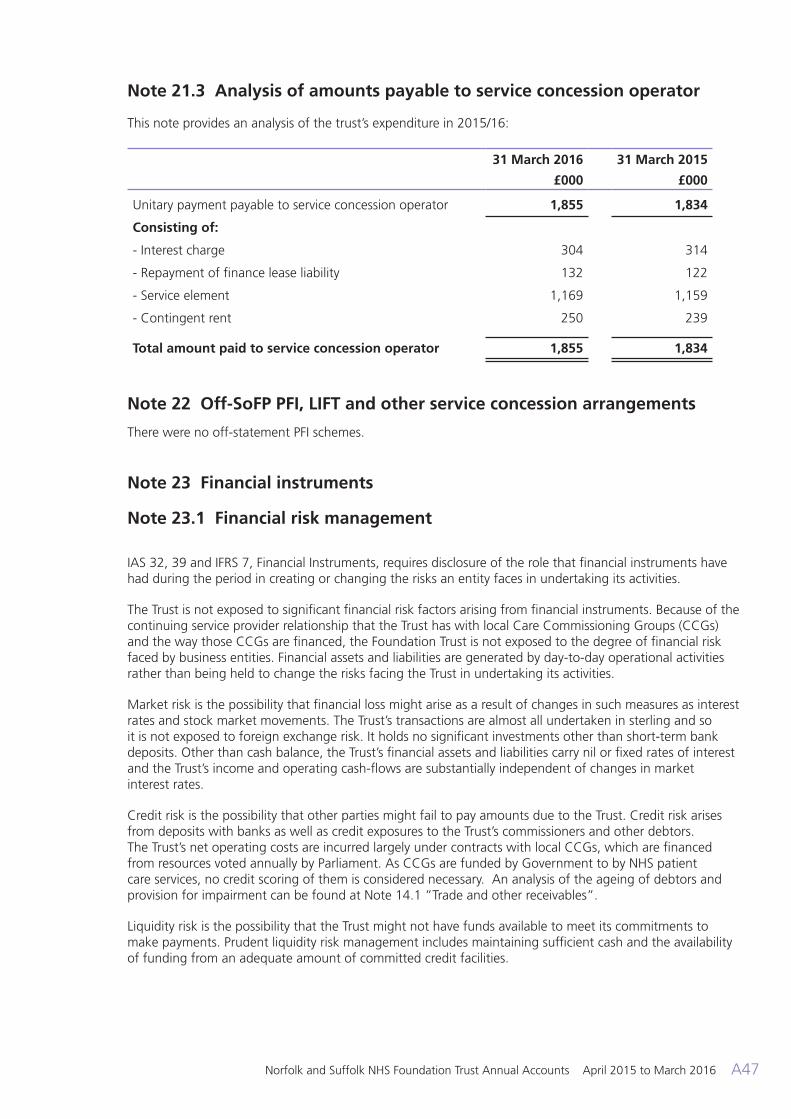
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A47
Note 21.3 Analysis of amounts payable to service concession operator
This note provides an analysis of the trust’s expenditure in 2015/16:
31 March 2016 31 March 2015
£000 £000
Unitary payment payable to service concession operator 1,855 1,834
Consisting of:
- Interest charge 304 314
- Repayment of finance lease liability 132 122
- Service element 1,169 1,159
- Contingent rent 250 239
Total amount paid to service concession operator 1,855 1,834
Note 22 Off-SoFP PFI, LIFT and other service concession arrangements
There were no off-statement PFI schemes.
Note 23 Financial instruments Note 23.1 Financial risk management
IAS 32, 39 and IFRS 7, Financial Instruments, requires disclosure of the role that financial instruments have had during the period in creating or changing the risks an entity faces in undertaking its activities.
The Trust is not exposed to significant financial risk factors arising from financial instruments. Because of the continuing service provider relationship that the Trust has with local Care Commissioning Groups (CCGs) and the way those CCGs are financed, the Foundation Trust is not exposed to the degree of financial risk faced by business entities. Financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the Trust in undertaking its activities.
Market risk is the possibility that financial loss might arise as a result of changes in such measures as interest rates and stock market movements. The Trust’s transactions are almost all undertaken in sterling and so it is not exposed to foreign exchange risk. It holds no significant investments other than short-term bank deposits. Other than cash balance, the Trust’s financial assets and liabilities carry nil or fixed rates of interest and the Trust’s income and operating cash-flows are substantially independent of changes in market interest rates.
Credit risk is the possibility that other parties might fail to pay amounts due to the Trust. Credit risk arises from deposits with banks as well as credit exposures to the Trust’s commissioners and other debtors. The Trust’s net operating costs are incurred largely under contracts with local CCGs, which are financed from resources voted annually by Parliament. As CCGs are funded by Government to by NHS patient care services, no credit scoring of them is considered necessary. An analysis of the ageing of debtors and provision for impairment can be found at Note 14.1 ”Trade and other receivables”.
Liquidity risk is the possibility that the Trust might not have funds available to meet its commitments to make payments. Prudent liquidity risk management includes maintaining sufficient cash and the availability of funding from an adequate amount of committed credit facilities.
ARA2016 - Acc Section 130616 post audit.indd 47 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A48
Note 23.2 Financial assets
Loans and receivables
Total
£000 £000
Assets as per SoFP as at 31 March 2016
Trade and other receivables excluding non financial assets 5,885 5,885
Cash and cash equivalents at bank and in hand 8,475 8,475
Total at 31 March 2016 14,360 14,360
Assets as per SoFP as at 31 March 2015
Trade and other receivables excluding non financial assets
4,533 4,533
Cash and cash equivalents at bank and in hand 15,697 15,697
Total at 31 March 2015 20,230 20,230
Note 23.3 Financial liabilities
Other financial liabilities
Total
£000 £000
Liabilities as per SoFP as at 31 March 2016
Borrowings excluding finance lease and PFI liabilities 12,168 12,168
Obligations under PFI, LIFT and other service concession contracts
3,834 3,834
Trade and other payables excluding non financial liabilities 19,198 19,198
Total at 31 March 2016 35,200 35,200
Other financial liabilities
Total
£000 £000
Liabilities as per SoFP as at 31 March 2015
Borrowings excluding finance lease and PFI liabilities 13,225 13,225
Obligations under PFI, LIFT and other service concession contracts
3,965 3,965
Trade and other payables excluding non financial liabilities 24,180 24,180
Total at 31 March 2015 41,370 41,370
ARA2016 - Acc Section 130616 post audit.indd 48 14/06/2016 10:25
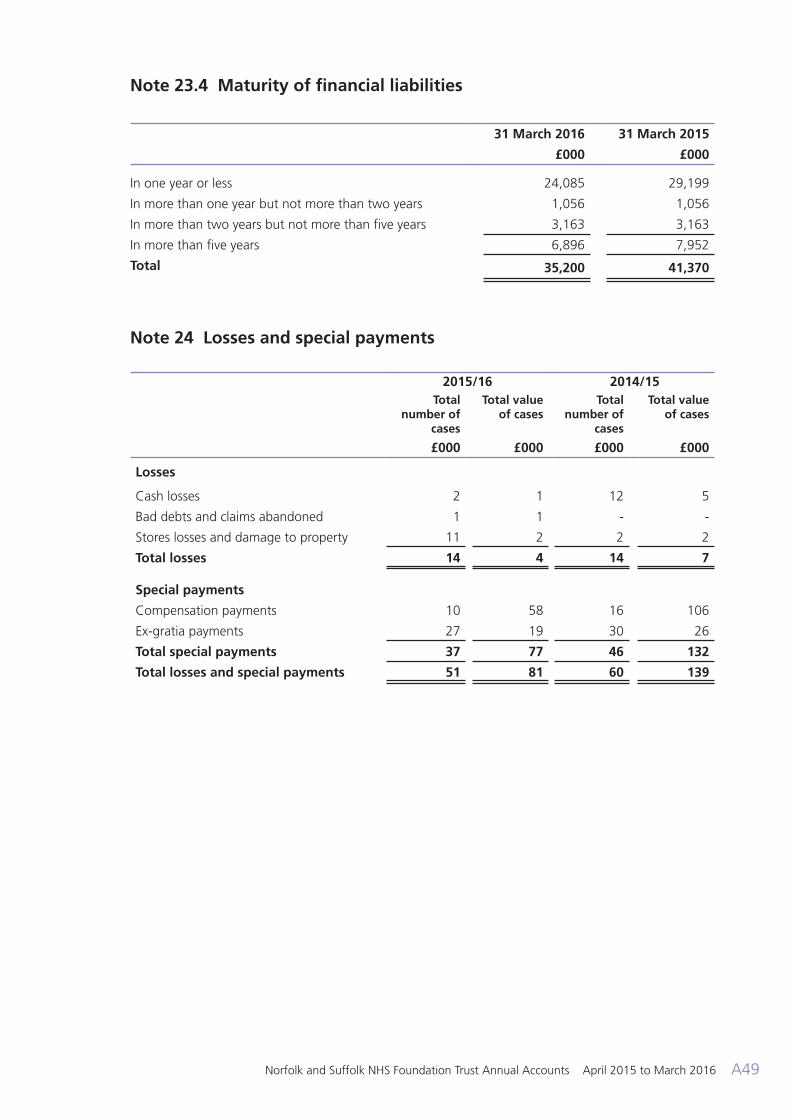
Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A49
Note 23.4 Maturity of financial liabilities
31 March 2016 31 March 2015
£000 £000
In one year or less 24,085 29,199
In more than one year but not more than two years 1,056 1,056
In more than two years but not more than five years 3,163 3,163
In more than five years 6,896 7,952
Total 35,200 41,370
Note 24 Losses and special payments
2015/16 2014/15Total
number of cases
Total value of cases
Total number of
cases
Total value of cases
£000 £000 £000 £000
Losses
Cash losses 2 1 12 5
Bad debts and claims abandoned 1 1 - -
Stores losses and damage to property 11 2 2 2
Total losses 14 4 14 7
Special payments
Compensation payments 10 58 16 106
Ex-gratia payments 27 19 30 26
Total special payments 37 77 46 132
Total losses and special payments 51 81 60 139
ARA2016 - Acc Section 130616 post audit.indd 49 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A50
Note 25 Prior period adjustments
A prior period adjustment in regards to an impairment has been made to the 2014-15 financial position. The impact of this is summarised below.
Statement of Comprehensive Income 2014/15 Impairment adjustment
2014/15 restated
£000 £000 £000
Total operating income from continuing operations 212,831 212,831
Operating expenses (211,681) (3,169) (214,850)
Operating surplus/(deficit) from continuing operations 1,150 (3,169) (2,019)
Net finance costs (4,856) - (4,856)
Surplus/(deficit) for the year (3,706) (3,169) (6,875)
Total comprehensive income/(expense) for the period 14,333 (3,169) 11,164
Statement of Financial Position 2014/15 Impairment adjustment
2014/15 restated
£000 £000 £000
Total non-current assets 155,492 - 155,492
Total current assets 32,151 (3,169) 28,982
Total current liabilities (32,942) - (32,942)
Total assets less current liabilities 154,701 (3,169) 151,532
Total non-current liabilities (21,010) - (21,010)
Total assets employed 133,691 (3,169) 130,522
Financed by
Public dividend capital 81,886 - 81,886
Revaluation reserve 43,088 - 43,088
Income and expenditure reserve 8,717 (3,169) 5,548
Total taxpayers' equity 133,691 (3,169) 130,522
ARA2016 - Acc Section 130616 post audit.indd 50 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A51
Note 26 Related parties
Norfolk and Suffolk NHS Foundation Trust is a body corporate established by order of the Secretary of State for Health. During the year none of the board members or members of the key management staff or parties related to them has undertaken any material transactions with the Trust (2014/15 - £nil).
The Department of Health is regarded as a related party. During the year Norfolk and Suffolk NHS Foundation Trust has had a significant number of material transactions with the Department, and with other entities for which the Department is regarded as the parent Department. The Trust also had transactions with a number of Clinical Commissioning Groups (CCGs) including Norwich CCG, South Norfolk CCG, West Norfolk CCG, North Norfolk CCG, Ipswich and East Suffolk CCG and West Suffolk CCG.
The Trust also had £14,463k of expenditure with NHS Professionals for temporary staff costs (2014- £16,261k). In addition, the Trust had a significant number of material transactions with other Government bodies, namely Norfolk County Council and Suffolk County Council.
The Trust is the corporate trustee of the Norfolk and Suffolk NHS Foundation Trust Charitable Funds. The members of the Trust Board of Directors act on behalf of the Trust in its capacity as corporate trustee. During the year none of the Trustees or members of the key management staff or parties related to them has undertaken any material transactions with the Charitable Trust.
Board Members (and other senior staff) take decisions both on Charity and Exchequer matters but endeavour to keep the interests of each discrete and do not seek to benefit personally from such decisions. Declarations of personal interest have been made in both capacities and are available to be inspected by the public.
Receivables Payables31 March
201631 March
201531 March
201631 March
2015£000 £000 £000 £000
Department of Health 50 343 180 372
NHS England 572 21 16 53
NHS Foundation Trusts 275 292 509 513
NHS Trusts 114 267 275 462
Care Commissioning Groups (CCGs) - 1,808 694 237
Health Education England 62 666 694 705
Other NHS bodies 2,340 337 236 30
Local Government and other WGA bodies 811 1,100 5,712 4,871
Total 4,224 4,834 8,316 7,243
Income Expenditure2015/16 2014/15 2015/16 2014/15
£000 £000 £000 £000
Department of Health 1,410 2,519 - -
NHS England 17,959 19,147 344 3
NHS Foundation Trusts 1,082 1,387 2,970 2,809
NHS Trusts 542 507 1,219 1,408
Care Commissioning Groups (CCGs) 168,150 163,573 691 366
Health Education England 4,652 4,216 3 4
Other NHS bodies 1,128 1,070 947 823
Local Government and other WGA bodies 11,839 15,202 31,479 25,539
Total 206,762 207,621 37,653 30,952
ARA2016 - Acc Section 130616 post audit.indd 51 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A52
© M
ay 2
016.
Nor
folk
and
Suf
folk
NH
S Fo
unda
tion
Trus
t. G
FX:4
000
ARA2016 - Acc Section 130616 post audit.indd 52 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016 A53
ARA2016 - Acc Section 130616 post audit.indd 53 14/06/2016 10:25

Norfolk and Suffolk NHS Foundation Trust Annual Accounts April 2015 to March 2016A54
Norfolk and Suffolk NHS Foundation Trust values and celebrates the diversity of all the communities we serve. We are fully committed to ensuring that all people have equality of opportunity to access our service, irrespective of their age, gender, ethnicity, race, disability, religion or belief, sexual orientation, marital or civil partnership or social and economic status.NSFTrust
@NSFTtweets
nsft.nhs.uk
01603 421421Trust Headquarters: Hellesdon HospitalDrayton High RoadNorwich NR6 5BE
Patient Advice and Liaison Service (PALS)
NSFT PALS provides confidential advice, information and support, helping you to answer any questions you have about our services or about any health matters.
If you would like this leaflet in large print, audio, Braille, alternative format or a
different language, please contact PALS and we will do our best to help. Email: [email protected] call PALS Freephone 0800 279 7257
ARA2016 - Acc Section 130616 post audit.indd 54 14/06/2016 10:25

















