39
Anorectal abscess on Anorectal abscess on call call Jim Hill Jim Hill Manchester Royal Manchester Royal Infirmary Infirmary
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | peregrine-holt |
| View: | 221 times |
| Download: | 0 times |

Anorectal abscess on callAnorectal abscess on call
Jim HillJim Hill
Manchester Royal InfirmaryManchester Royal Infirmary

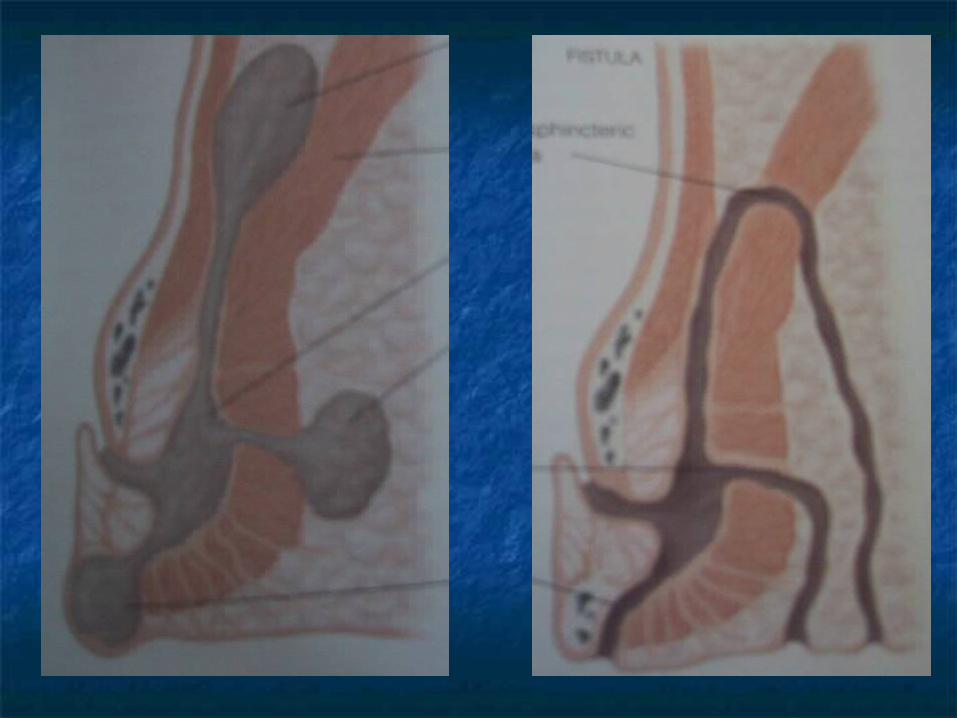
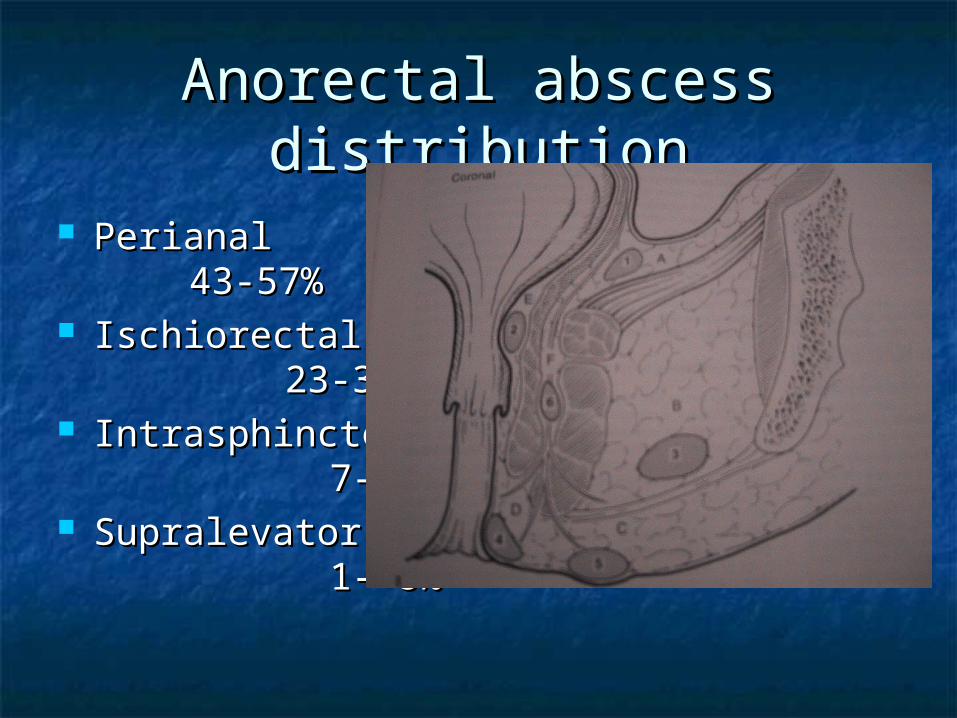
Anorectal abscess Anorectal abscess distributiondistribution
PerianalPerianal43-57%43-57%
IschiorectalIschiorectal23-34%23-34%
IntrasphinctericIntrasphincteric 7-21% 7-21%
SupralevatorSupralevator 1- 8% 1- 8%

Anorectal abscess – de Pezzer Anorectal abscess – de Pezzer drainage – Isbister ANZJS 1987drainage – Isbister ANZJS 1987
Local anaestheticLocal anaesthetic 10% intolerable 10% intolerable
painpain 29% developed 29% developed
fistula in follow up fistula in follow up periodperiod

Anorectal abscess and fistula - Anorectal abscess and fistula - USA. A study of 1023 pts. USA. A study of 1023 pts. Abcarian et al Dis Colon Abcarian et al Dis Colon
Rectum 1984Rectum 1984 Regional anaesthesia, early Regional anaesthesia, early
aggressive treatment of low fistulaaggressive treatment of low fistula 35% internal opening (3% 35% internal opening (3%
sup/sphincteric)sup/sphincteric) 3.7% recurrence abscess only group3.7% recurrence abscess only group 1.8% recurrence primary fistulotomy 1.8% recurrence primary fistulotomy
groupgroup
Anorectal and fistula – UK. Anorectal and fistula – UK. Winslett at al Dis Col Rectum Winslett at al Dis Col Rectum
1988 1988 233 pts233 pts 5% internal opening5% internal opening 32% reoperation in incision and 32% reoperation in incision and
drainage categorydrainage category 12% occult disease12% occult disease

Anorectal abscess and fistula - Anorectal abscess and fistula - incidenceincidence
AbcarianAbcarian 35%35% GordonGordon 37%37% MazierMazier 69%69% WinslettWinslett 5% 5%

Primary fistulotomy-perianal Primary fistulotomy-perianal abscess – Seow-Choen et al Dis abscess – Seow-Choen et al Dis
Colon Rectum 1997Colon Rectum 1997
Randomised trial 52 consecutive patientsRandomised trial 52 consecutive patients Persistent fistulas Persistent fistulas
25% I&D group25% I&D group 0% Fistulotomy group 0% Fistulotomy group
No difference in continence or ARPSNo difference in continence or ARPS Operating time, hospital stay, wound Operating time, hospital stay, wound
healing no differenthealing no different

Early re-operation for anorectal Early re-operation for anorectal abscessabscess
Onaca et al Mayo Dis Colon Rectum 2001Onaca et al Mayo Dis Colon Rectum 2001500 consecutive patients, 627 procedures500 consecutive patients, 627 procedures7.6% (48 pts) re-operation rate – 10 days7.6% (48 pts) re-operation rate – 10 days23 incomplete drainage23 incomplete drainage19 missed loculations/abscess19 missed loculations/abscessHorseshoe abscess 50% failure rateHorseshoe abscess 50% failure rateSurgical error leading cause early Surgical error leading cause early failurefailure

Horseshoe abscessHorseshoe abscess
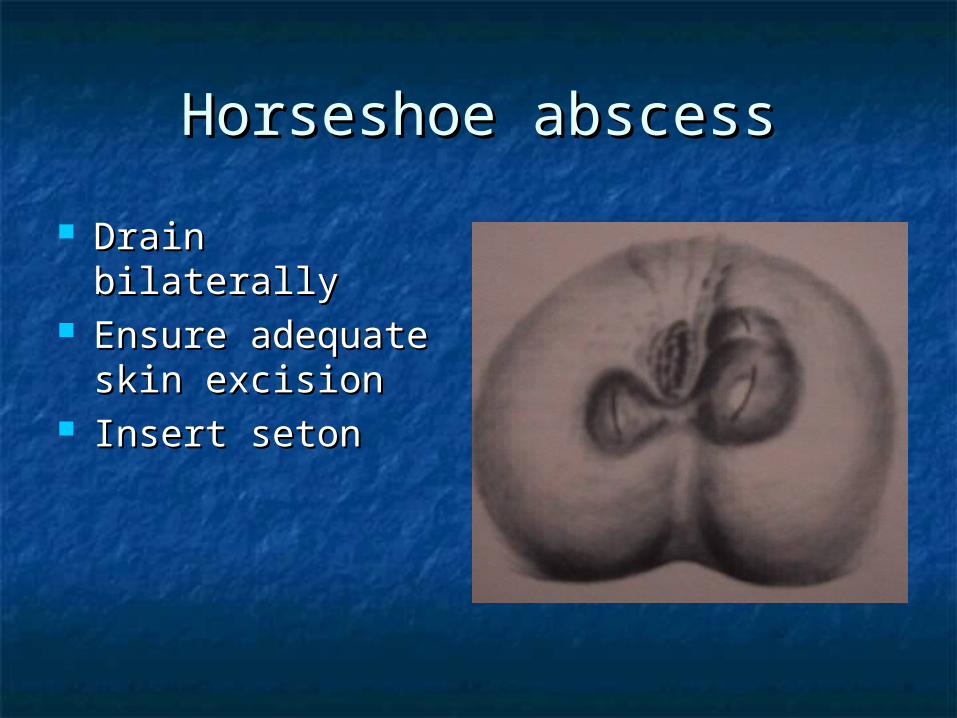
Horseshoe abscessHorseshoe abscess
Drain bilaterally Drain bilaterally Ensure adequate Ensure adequate
skin excisionskin excision Insert setonInsert seton

Primary suture of anorectal Primary suture of anorectal abscess – Mortenson et al Dis abscess – Mortenson et al Dis
Col Rectum 1995Col Rectum 1995
Randomised trial 107 patientsRandomised trial 107 patients
Clindamycin vs clindamycin and gentacollClindamycin vs clindamycin and gentacoll
Any fistula detected layed openAny fistula detected layed open
Recurrence 17% vs 22%Recurrence 17% vs 22%
Instructions to the BSTInstructions to the BST Good News/low Good News/low
riskrisk Small abscessSmall abscess First abscessFirst abscess YoungYoung HealthyHealthy
Bad News/high riskBad News/high risk Large, bilateralLarge, bilateral Previous abscessPrevious abscess OldOld Cardiorespiratory Cardiorespiratory
diseasedisease Crohn’s diseaseCrohn’s disease FatFat ObeseObese ImmunosuppressionImmunosuppression

Debriding agentsDebriding agents
Systemic review Health Technology Systemic review Health Technology Assessment 2001Assessment 2001 No good trialsNo good trials All used autolytic methodsAll used autolytic methods Modern dressings (foam, alginate, Modern dressings (foam, alginate,
hydrocolloid) vs gauzehydrocolloid) vs gauze Suggestion better than gauze for healing, Suggestion better than gauze for healing,
pain, dressing performance and resource pain, dressing performance and resource useuse

Crohn’s diseaseCrohn’s disease
Abscess always associated with a Abscess always associated with a fistulafistula
Loose draining setons Loose draining setons Avoid fistulotomyAvoid fistulotomy Recurrence rates >50% at two yearsRecurrence rates >50% at two years Recurrence rates less in patients with Recurrence rates less in patients with
stomasstomas
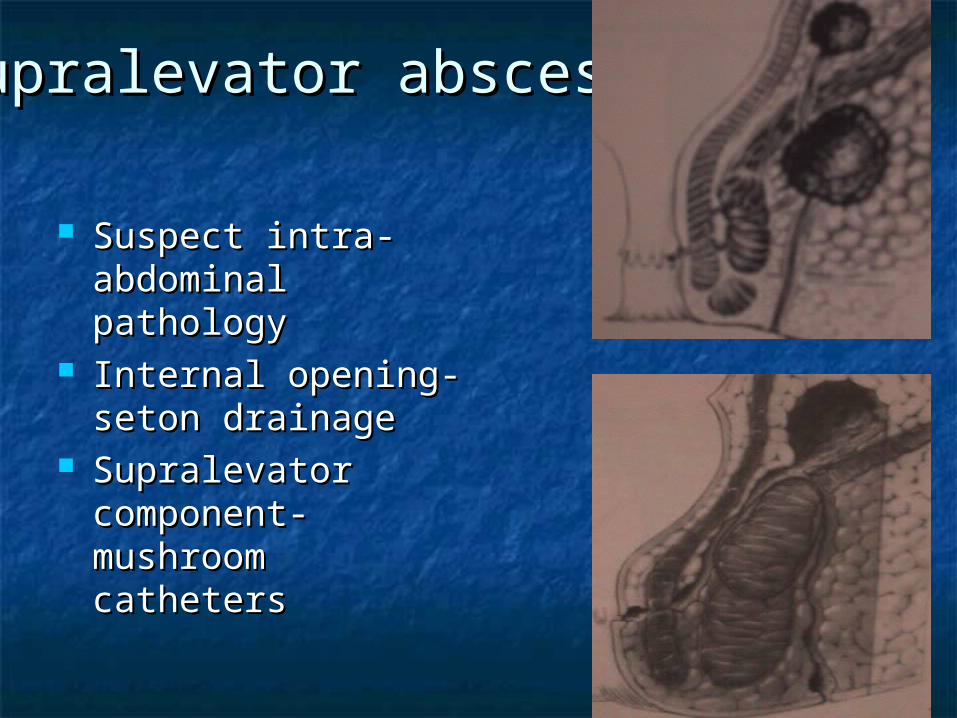
Supralevator abscessSupralevator abscess
Suspect intra-Suspect intra-abdominal abdominal pathologypathology
Internal opening-Internal opening-seton drainage seton drainage
Supralevator Supralevator component-component-mushroom mushroom catheterscatheters

Haematological Haematological malignancies 1malignancies 1
Incidence 7-10%Incidence 7-10% Neutrophil count significant prognostic Neutrophil count significant prognostic
factorfactor Mortality 20-50%Mortality 20-50% Organisms same as non-Organisms same as non-
immunocompromised patientsimmunocompromised patients Pus can form even in patients with Pus can form even in patients with
severe neutropaeniasevere neutropaenia
Haematological Haematological malignancies -2malignancies -2
Evaluate rectal pain and fever carefullyEvaluate rectal pain and fever carefully Start broad spectrum antibioticsStart broad spectrum antibiotics Beware rapid progression to Fournier’sBeware rapid progression to Fournier’s Incision and drainage when fluctuation Incision and drainage when fluctuation
presentpresent Role of surgery uncertain in non-Role of surgery uncertain in non-
resolving cellulitisresolving cellulitis

HIV and perianal abscessHIV and perianal abscess
Anorectal pathology not impacted by Anorectal pathology not impacted by highly active antiviral therapyhighly active antiviral therapy
Disturbed wound healing more common Disturbed wound healing more common (4-34%) and related to low CD4(4-34%) and related to low CD4++ counts counts (< 200 x10(< 200 x1066))
Serious septic complications higher (15%)Serious septic complications higher (15%) Idiopathic anal canal ulcer commonly Idiopathic anal canal ulcer commonly
associated with inter-sphincteric abscessassociated with inter-sphincteric abscess

Acute pilonidal abscess – Acute pilonidal abscess – incision and drainageincision and drainage
Br J Surg 1988 Jensen and HarlingBr J Surg 1988 Jensen and Harling 73 pts all had symptoms resolved73 pts all had symptoms resolved 58% healed primarily in 10 weeks58% healed primarily in 10 weeks 12% later recurrence12% later recurrence 45% healed overall45% healed overall
Increased recurrence rates in those with Increased recurrence rates in those with more pits and lateral sinusmore pits and lateral sinus

Pilonidal abscess – primary Pilonidal abscess – primary closure with antibiotic coverclosure with antibiotic cover
Eur J Surg 1993Eur J Surg 1993 56 patients one or four days 56 patients one or four days
ampicillin/flagylampicillin/flagyl 30% recurrence30% recurrence No difference with antibiotic regimesNo difference with antibiotic regimes

Perianal hidradenitisPerianal hidradenitis

SummarySummary
Train the BSTTrain the BST Send pus and skinSend pus and skin High risk cases High risk cases
Assess preoperativelyAssess preoperatively Be present in theatre Be present in theatre
Low fistulas can be dealt with safelyLow fistulas can be dealt with safely Use modern dressingsUse modern dressings



MCQMCQ
Which of the following statements with haematological Which of the following statements with haematological malignancies and anal infections is truemalignancies and anal infections is trueA. The development of a perianal abscess is A. The development of a perianal abscess is independent from the granulocyte countindependent from the granulocyte countB. The most common causative agent is candidaB. The most common causative agent is candidaC. The overall prognosis for the haematological cancer C. The overall prognosis for the haematological cancer is independent from the prescence of septic is independent from the prescence of septic complicationscomplicationsD. The pus found at the time of the incision and D. The pus found at the time of the incision and drainage is identical to pus drained from common drainage is identical to pus drained from common perianal abscessesperianal abscessesE. Fever is an important element in the clinical E. Fever is an important element in the clinical presentation of such casespresentation of such cases






Horseshoe abscessHorseshoe abscess



Horseshoe abscessHorseshoe abscess
Bilateral drainageBilateral drainage Insertion of seton Insertion of seton
through internal through internal openingopening
RadiologyRadiology
US scanning US scanning 63% accuracy relation abscess and Park’ 63% accuracy relation abscess and Park’
classificationclassification 28% accuracy locating internal opening28% accuracy locating internal opening




![A Rare Case of Anorectal Abscess due to Foreign Ingested ...A].pdf · the patient’s perianal abscess was drained. Due to the presence of gaseous, purulent drainage from the perianal](https://static.documents.pub/doc/80x56/60858a3928e9e201eb61b9d8/a-rare-case-of-anorectal-abscess-due-to-foreign-ingested-apdf-the-patientas.jpg)












