ANTERIOR CHAMBER FIBROUS MEMBRANE FORMATION FOLLOWING CORNEAL SURGERY * 1 Veena Raiji MD, MPH, 1 David A. Belyea MD, MBA, 1 Bryan D. Edgington MD, 2 Keith Wroblewski MD, 2 Kraig S. Bower MD 1 George Washington University Hospital, Washington DC 2 Walter Reed Army Medical Center, Washington DC *No financial interests
Transcript
ANTERIOR CHAMBER FIBROUS MEMBRANE FORMATION FOLLOWING CORNEAL SURGERY
*1Veena Raiji MD, MPH, 1David A. Belyea MD, MBA, 1Bryan D. Edgington MD, 2Keith Wroblewski MD, 2Kraig S. Bower MD
1George Washington University Hospital, Washington DC2Walter Reed Army Medical Center, Washington DC
*No financial interests
Objective
• We present 5 patients with visually significant retrocorneal membranes associated with corneal transplantation surgeries and glaucoma drainage implants
• Further histopathological studies will be used in these specimens to attempt to decipher the exact etiology of these membranes.
• Examples of these cases are presented here
Case 1-Courtesy of the Armed Forces Institute of Pathology, a thin pupillary membrane extending over the pupillary aperture.
Case 2-81 y/o male with advanced diabetes on dialysis, with a history of Baerveldt Glaucoma Implant and status-post penetrating keratoplasty for corneal edema. Patient underwent excision of fibrous anterior chamber membrane.
Pre- membrane excision clinical photo and optical coherence tomogram
Post- membrane excision clinical photo and optical coherence tomogram
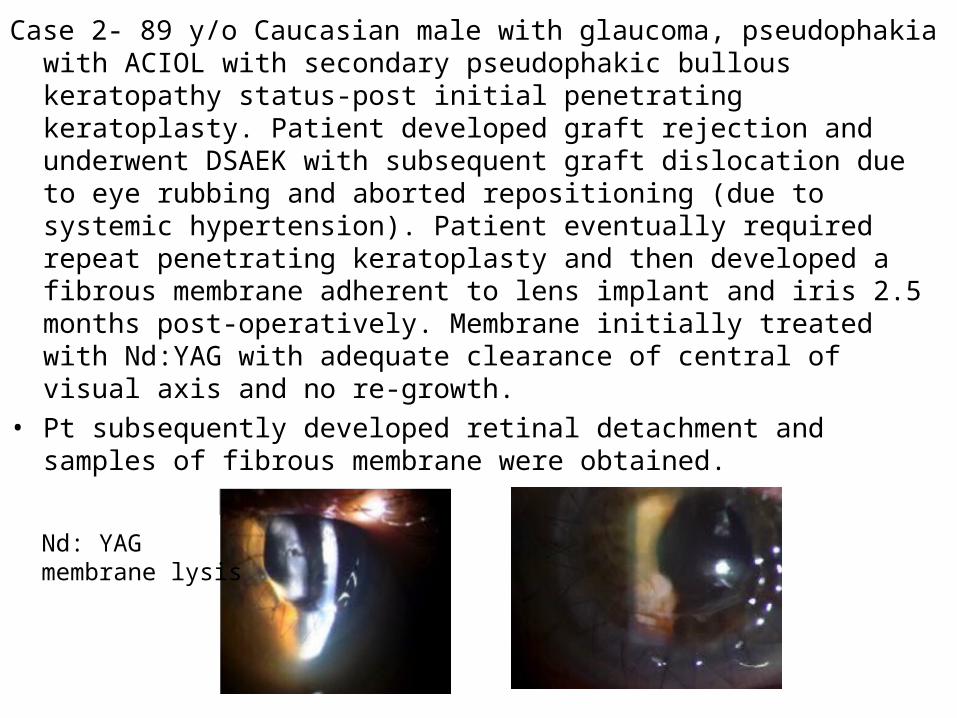
Case 2- 89 y/o Caucasian male with glaucoma, pseudophakia with ACIOL with secondary pseudophakic bullous keratopathy status-post initial penetrating keratoplasty. Patient developed graft rejection and underwent DSAEK with subsequent graft dislocation due to eye rubbing and aborted repositioning (due to systemic hypertension). Patient eventually required repeat penetrating keratoplasty and then developed a fibrous membrane adherent to lens implant and iris 2.5 months post-operatively. Membrane initially treated with Nd:YAG with adequate clearance of central of visual axis and no re-growth.
• Pt subsequently developed retinal detachment and samples of fibrous membrane were obtained.
.
Nd: YAG membrane lysis
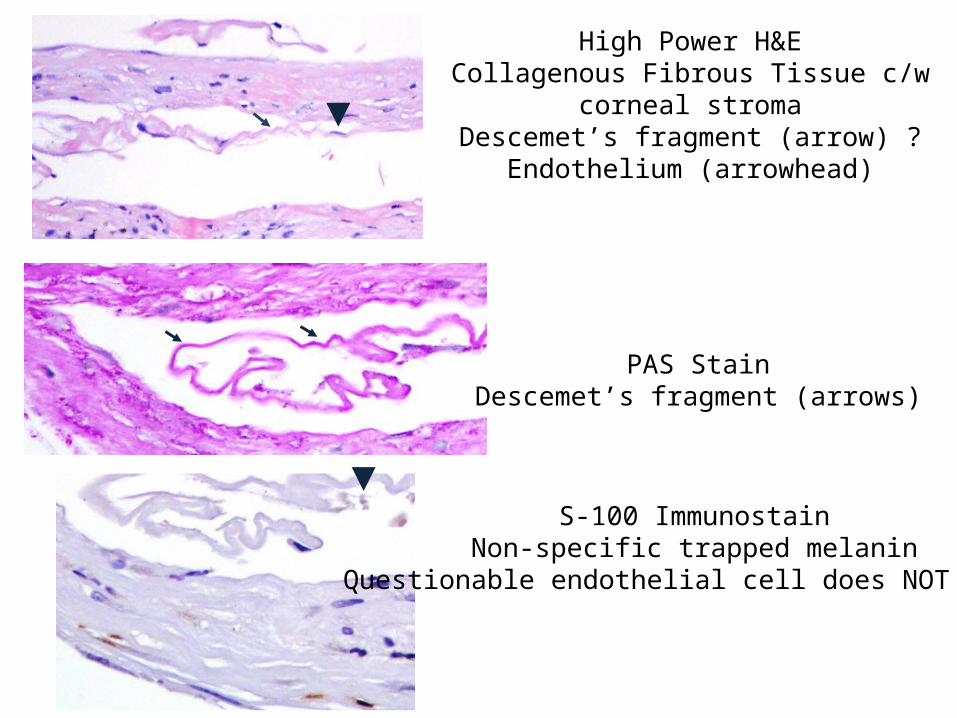
High Power H&ECollagenous Fibrous Tissue c/w corneal stroma
Descemet’s fragment (arrow) ?Endothelium (arrowhead)
PAS StainDescemet’s fragment (arrows)
S-100 ImmunostainNon-specific trapped melanin
Questionable endothelial cell does NOT stain
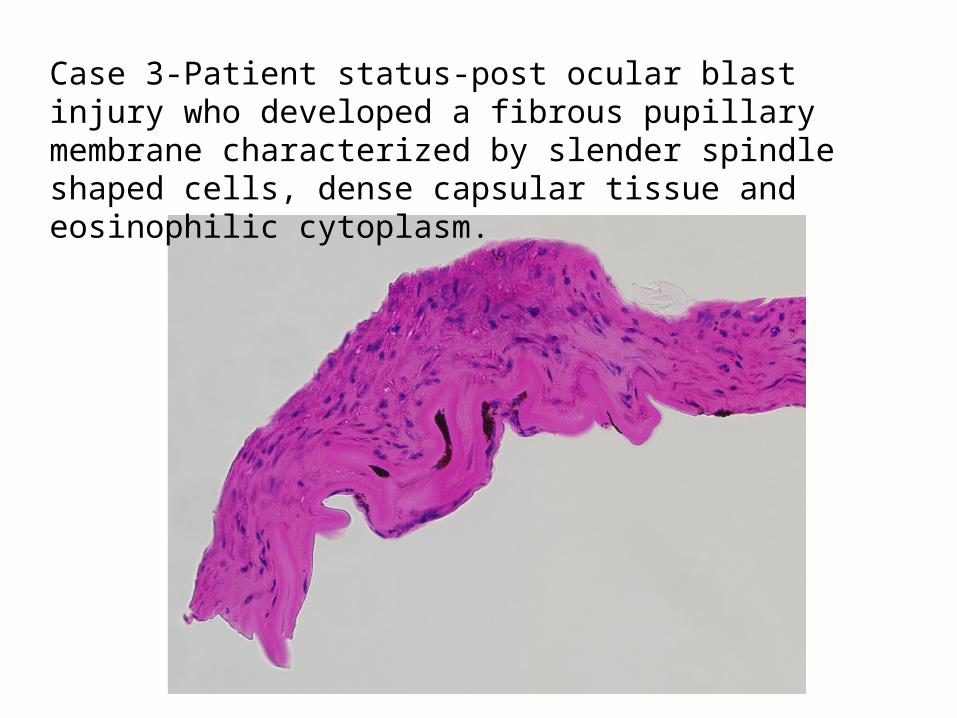
Case 3-Patient status-post ocular blast injury who developed a fibrous pupillary membrane characterized by slender spindle shaped cells, dense capsular tissue and eosinophilic cytoplasm.
Results
• We report 5 cases of anterior chamber fibrous membrane formation following penetrating keratoplasty (PKP) or Descemet Stripping Endothelial Keratoplasty (DSEK).
• Histopathology and ocular coherence tomography confirm fibrous membrane formation and anterior segment involvement.
• Four of the five of the patients in our series have glaucoma, and three had pre-existing Baerveldt shunts in place prior to corneal surgery.
• Two of the five patients had severe diabetic disease.
Conclusions
• The etiology of these pupillary membranes is unclear but may be related to the proliferation of residual anterior capsular epithelial cells after the insertion of the glaucoma drainage implants and subsequent formation of an epithelial-like plaque.
• A small amount of blood breakdown products in the anterior chamber as a result of the drainage tube may allow these cells to undergo fibrous metaplasia and form the scaffold that allows adjacent cells to migrate over the pupillary aperture. Underlying cells may lose their ability to receive oxygen and nutrient supply and undergo metaplasia and become spindle-like fibroblasts which eventually opacify.
• Since a majority of these cases occurred in combination of penetrating keratoplasty and glaucoma drainage implant, the change in the morphology or perhaps anterior chamber alignment may lead to this scaffold formation.
Conclusions
• Cockerham and Hidayat reported the high incidence of retrocorneal membranes with myofibroblasts after perforating injury and the mechanism may be similar.
• Jakobiec, in a series of 28 retrocorneal membranes, showed that the majority of subtypes were fibrous keratocytic and stained positively for vimentin and alpha-smooth muscle actin and the other significant group was endothelial derived and stained positively for CK7, alpha-smooth muscle actin and vimentin.
• Calabrese et al. showed a 45% histopathologic incidence of retrocorneal membranes in 371 grafts sustaining graft failure at the University of Erlangen –Nurnberg which is similar to the work of Kremer et al.
• In suspected cases, tissue samples should be stained with S-100, PAS, vimentin, CK7 and alpha-smooth muscle actin to better understand the etiology of these membranes.
References• Cockerham GC, Hidayat AA. Retrocorneal membrane with myofibroblasts after after
perforating injury: an immunohistochemical and ultrastructural study of 11 cases. Cornea 1999; 18: 700-706.
• Jakobiec F, Bhat P. Retrocorneal Membranes: A Comparative Immunohistochemical Analysis of Keratocytic, Endothelial and Epithelial Origins. Am J Ophthalmol 2010; 150: 230-242.
• Calabrese S, Wenkel H, Rummelt H et al. Histopathology of Retrocorneal Membranes after Keratoplasty. Klin Monatsbl Augenheilkd 2010; 227: 815-818.
• Kremer I, Rapuano CH, Cohen Ej et al. Retrocorneal fibrous membranes in failed corneal grafts. Am J Ophthalmol 1993; 115: 478-484.
• Shulman J et al. Failed descemet-stripping automated endothelial keratoplasty grafts: a clinicopathologic analysis. Am J Ophthalmol. 2009 Nov;148(5):752-759
• Bansal R et al. Intracorneal epithelial ingrowth after Descemet stripping endothelial keratoplasty and stromal puncture. Cornea. 2009 Nov; 28(3):334-337
• Young AL et al. Case of post Descemet stripping endothelial keratoplasty retrocorneal fibrous membrane. Clin Experiment Ophthalmol. 2009 May;37(4):418-9