32
Anterior Knee Anterior Knee Pain Pain In In Adolescents Adolescents Johan Johan Myburgh Myburgh February February 2012 2012
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | alexandra-cameron |
| View: | 233 times |
| Download: | 0 times |

Anterior Knee PainAnterior Knee Pain InIn AdolescentsAdolescents
Johan MyburghJohan MyburghFebruary 2012February 2012
Anterior knee painAnterior knee pain
• Introduction• Case study• Discussion– history– physical examination– investigations
• Conditions• Growing skeleton
IntroductionIntroduction• One of the most common musculoskeletal
complaints - pediatric population• Differential diagnosis fairly extensive -
thorough history and physical examination• Special attention:– anatomic location of the pain– aggravating factors
• Assessment of growth and development • Exclude hip and lumbar disorders (all patients)
HistoryHistory
• 15 year old male• 2 month history anterior knee pain• Progressively worse• Aggravated by activity• Noticed swelling below knee• Karate – Provincial level• Pain preventing exercise and tournament
paticipation
Clinical ExaminationClinical Examination
• Observation: Swelling at the infrapatellar tendon attachment on the tibial tubercle.
• Palpation: Tenderness to same area.
• Flexibility: Hamstring tightness
• Normal hip and lumbar spine examination
BiomechanicalBiomechanical evaluationevaluation
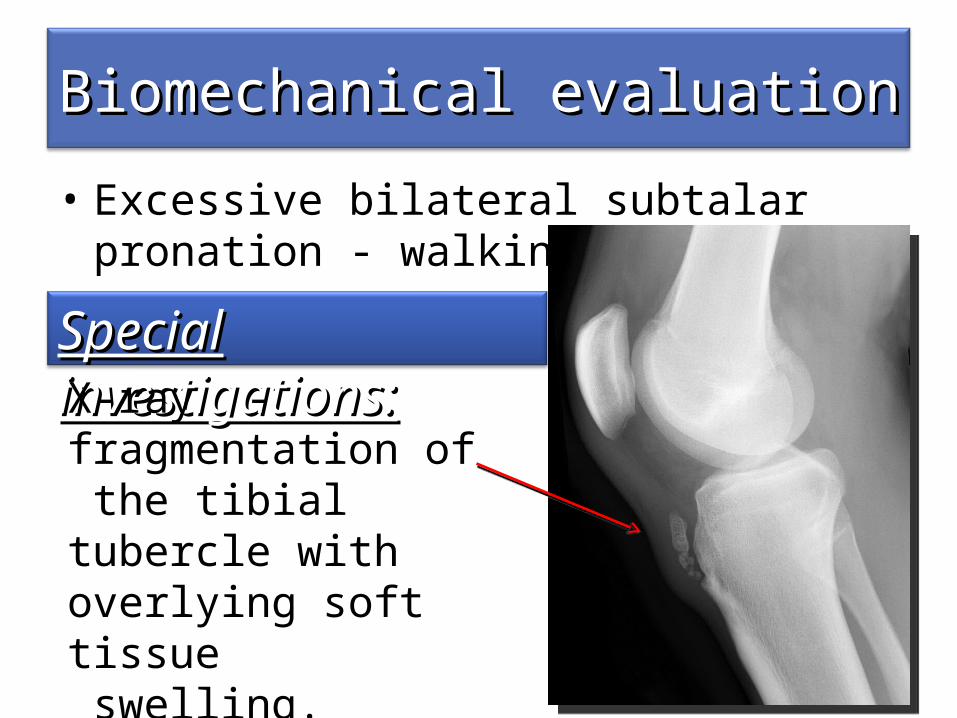
• Excessive bilateral subtalar pronation - walking
Special investigations:Special investigations:X-ray - fragmentation of the tibial tubercle with overlying soft tissue swelling.
Summary (3 stage)Summary (3 stage)
1. Clinical. Osgood-Schlatter disease– INTRINSIC FACTORS
• biomechanical abnormality• immature skeleton
– EXTRINSIC FACTORS• Kicking sport
– FITT • Overtraining ( preparing for tournament)
Summary (3 stage)Summary (3 stage)
2. Personal.Karate is his passion - can’t imagine being not able to do it for possibly months.3. Contextual Couch will not understand the chronic nature of his condition.
ProblemProblem listlist
• Active - Osgood-Schlatter disease
• Passive - Excessive bilateral subtalar overpronation
ManagementManagement planplan • Conservative
1. Regular icing of the area.2. Modifying activities - No pain causing activities
like jumping3. Physiotherapy to correct biomechanical
abnormalities and treat pain.• Progression: – physiotherapy and modified activity routine for 4
weeks– minor relapse of symptoms 2 weeks after
resuming sport specific activities, but he started his treatment regime and the pain resolved.
DISCUSSIONDISCUSSION
Anterior Knee Pain Anterior Knee Pain
HISTORYHISTORY• Pain characteristics – location, character, onset,
duration, change with activity or rest, aggravating and alleviating factors, and night pain.
• Trauma – acute major trauma, repetitive minor trauma.
• Mechanical symptoms – locking or extension block, instability
• Inflammatory symptoms – morning stiffness, swelling
• Bleeding disorders• Previous injury & treatments• Current level of functioning
HISTORYHISTORY
• Overuse knee injuries - report sensation of knee instability– Pseudo-giving way due to a neuromuscular
inhibition – Inhibition secondary to pain, muscle weakness
and patellar instability.
Physical ExaminationPhysical Examination• Complete knee examination (above and below
joints)– Examine - contralateral knee and the ipsilateral hip
joint.• Biomechanical examination - predisposing
factors. • Genetic predisposition includes excessive
stiffness, loose-jointedness and poor muscle tone.
• Knee joint swelling - suspicion of intra-articular pathology, synovitis
InvestigationsInvestigations
• Laboratory testing– infection suspected - CBC, ESR, CRP– arthritis is diagnosed - anti-CCP, ANA, RF and HLA-
B27 for classification and treatment.
• Imaging studies rarely used– Assist in diagnosis• Perthe’s and Slipped femoral capital epiphysis
– X-rays and MRI most commonly used.
Extensive differential diagnosisExtensive differential diagnosis
• Patellofemoral pain syndrome
• Patellofemoral instability and patellar subluxation
• Patellar tendinopathy (Jumper’s knee)
• Osteochondroses• Fat pad
irritation/impingement• Referred pain from the hip
and lumbar spine• Osteochondritis Dissecans
• Synovial plica• Quadriceps tendinopathy• Bipartite patella• Stress fracture of the
patella• Bursitis• Inflammatory disorders• Pain amplification
syndromes• Tumors
Patellofemoral Pain SyndromePatellofemoral Pain Syndrome
• most common cause of pediatric chronic anterior knee pain
• etiology– malalignment of the patella relative to the femoral
trochlea• result in articular cartilage damage
– peripatellar synovitis secondary to mechanical overloading• chemical irritation of local nerve endings
Patellofemoral Pain SyndromePatellofemoral Pain Syndrome• Risk factors
– malalignment of the lower limb– larger Q-angles– VMO weakness– muscle inflexibilities like tight quadriceps, gastrocnemius, hamstrings,
lateral retinaculum and IT band.• Classic Hx & Px• Quadriceps grinding test has a 96% sensitivity. • Management
– modification of activity, flexibility and strengthening exercises, patellar tracking exercises, icing, NSAIDS, patellar taping and shoe orthotics.
Other patellar pathology Other patellar pathology
• Patellofemoral instability and patellar subluxation– Clinically looks like patellofemoral pain syndrome - but
lateral dislocation may be elicited with palpation
• Patellar tendinopathy (Jumper’s knee)– common cause of infrapatellar knee pain– associated with osteochondroses and PFP – Rx activity modification and biomechanical rehabilitation – Progressive eccentric strengthening is essential.
OSTEOCHONDROSESOSTEOCHONDROSES
• adolescents during growth spurt • present with localized pain with activities , localized
tenderness and swelling• X-rays only if infection or bony tumors are suspected.• Self-limiting disorders - managed conservatively• Conservative management includes activity
modification, biomechanical rehabilitation, icing, NSAIDS, muscle strengthening and muscle flexibility exercises.
• can last ≤ 24 months until skeleton matures.symptoms persist past skeletal maturity surgery indicated to excise the separated tibial tuberosity fragment.
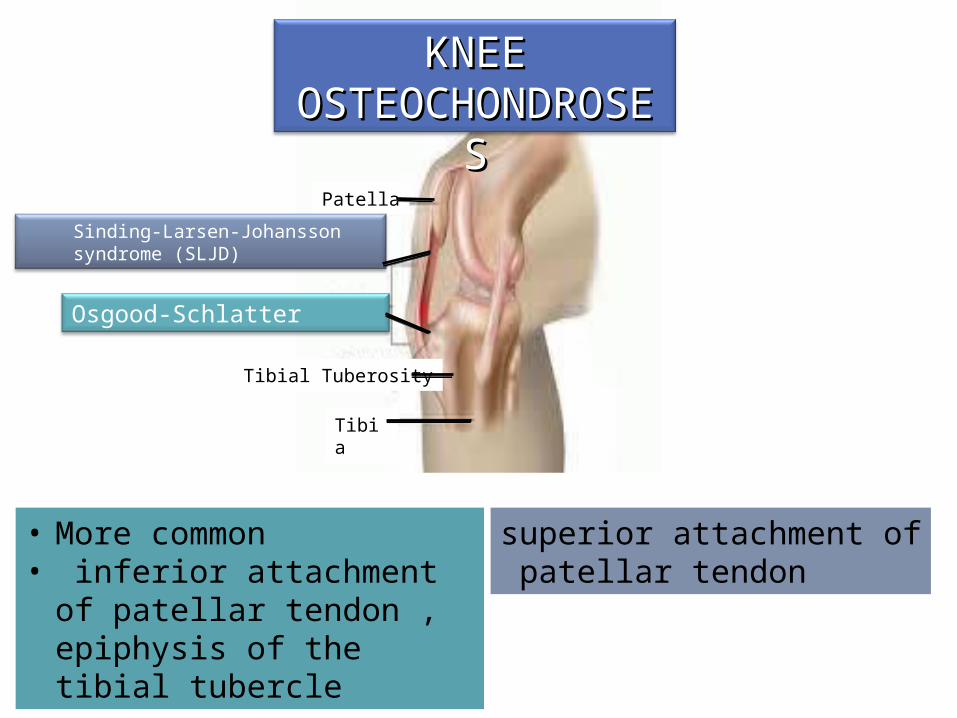
KNEE KNEE OSTEOCHONDROSESOSTEOCHONDROSES
Patella
Sinding-Larsen-Johansson syndrome (SLJD)
Tibial Tuberosity
Tibia
Osgood-Schlatter
• More common• inferior attachment of patellar
tendon , epiphysis of the tibial tubercle
superior attachment of patellar tendon
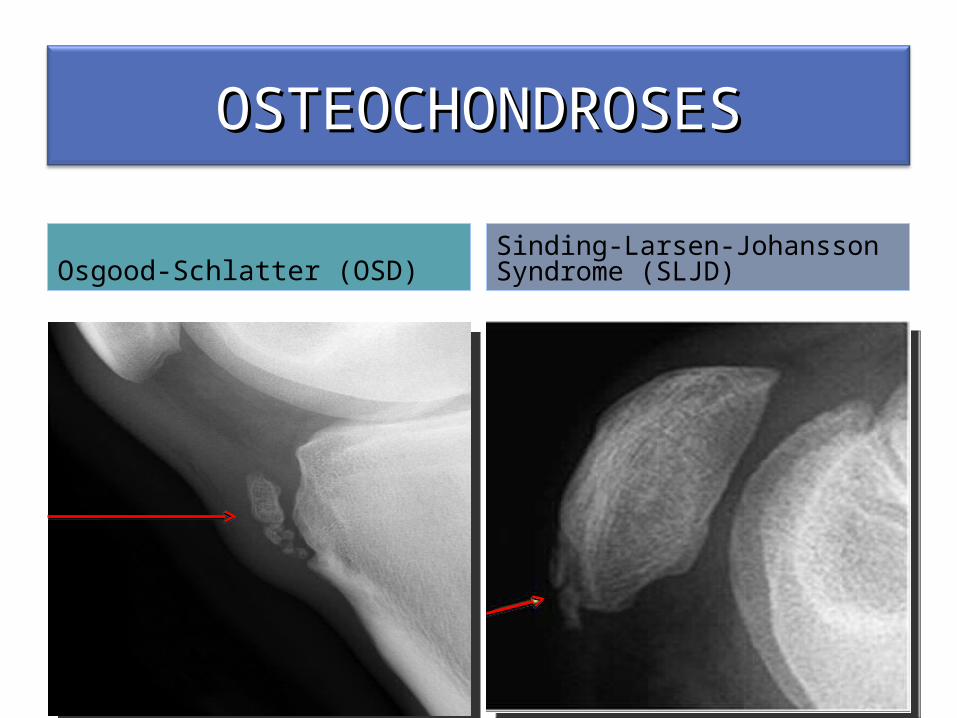
OSTEOCHONDROSESOSTEOCHONDROSES
Osgood-Schlatter (OSD)Sinding-Larsen-Johansson Syndrome (SLJD)
Osgood-Schlatter DiseaseOsgood-Schlatter Disease
• What’s new/controversial ?Journal Pediatrics July 2011Hyperosmolar Dextrose Injection for Recalcitrant
Osgood-Schlatter Disease– injection of the patellar tendon enthesis/tibial apophysis
with 12.5% dextrose (monthly x 3)– better 3,6,12 month outcome in pain score (NPPS—
Nirschl Pain Phase Scale) than usual care – Release several growth factors and neuropeptides
ConditionsConditions
• Fat pad irritation/impingement– Infrapatellar fat pad is a richly innervated area– Impingement occurs between the patella and femoral
condyle– Caused by direct trauma or a hyperextension injury
• Patellar tendinopathy, PFP and synovitis can cause chronic irritation.
• Referred pain from the hip and lumbar spine– Perthe’s disease or slipped capital femoral epiphysis may
present with knee pain.
ConditionsConditions• Osteochondritis Dissecans
– Idiopathic bone necrosis – Acute, hemarthrosis and loose body ( locked knee)– Most common lateral aspect of the medial femoral condyle
• Synovial plica– Local synovitis caused by microtrauma– synovium trapped between the patella and the femoral condyle. – medial knee pain – a thickened band when pressed against the condyle
• Quadriceps tendinopathy– Uncommon
ConditionsConditions
• Bipartite patella– superolateral patella may show an accessory ossification
centre ( pain and swelling)
• Stress fracture of the patella– uncommon condition– jumping athletes– intense localized pain and swelling – X-ray chronic stress reaction (bone scan)
• Bursitis– Prepatellar bursa most commonly affected – Infrapatellar bursitis mimic tendinopathy
• Aspirate bursa if septic arthritis is suspected

ConditionsConditions• Inflammatory disorders– Juvenile inflammatory arthritis
• morning stiffness and gradual resolution of the pain with activity• monoarthritis • screen for asymptomatic uveitis • confused with OSD (morning symptoms differentiate)
• Pain amplification syndromes– Reflex sympathetic dystrophy, reflex neurovascular
dystrophy and complex regional pain syndrome• pain out of proportion with the amount of trauma• unwillingness to weight bear and allodynia (pain from a non-
painful stimulus) • signs of autonomic dysfunction • special investigations are not helpful.
ConditionsConditions
• Tumors– rare cause on anterior knee pain– local osteosarcoma, leukemia and metastasis from
neuroblastoma
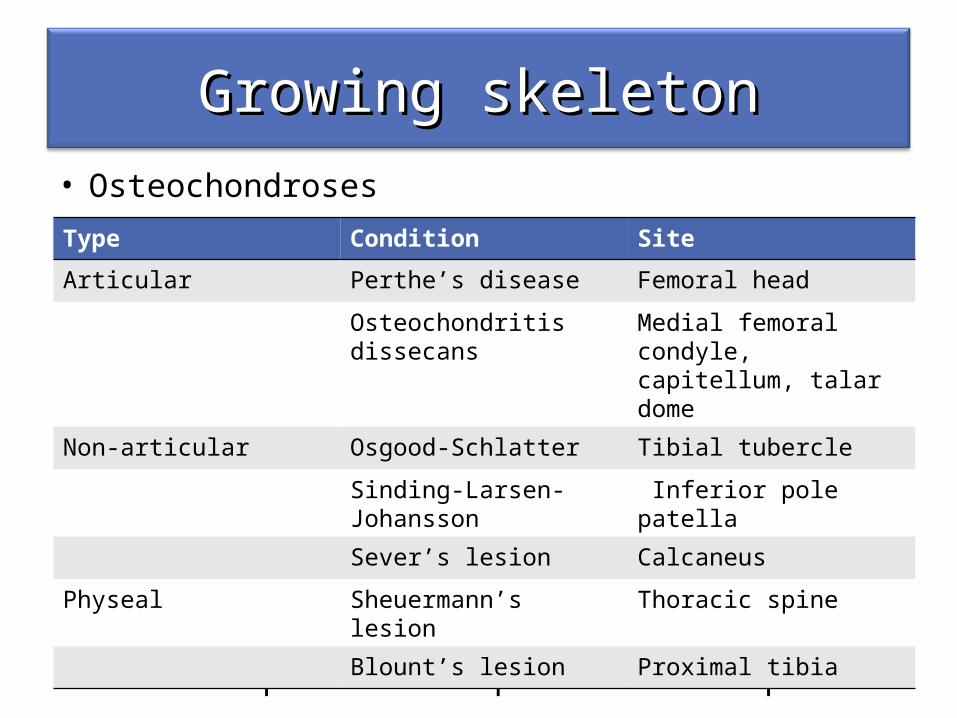
Growing skeletonGrowing skeleton• Osteochondroses
• Referred pain from the hip and lumbar spine
• Referred pain form hip and lumber spine
Type Condition Site
Articular Perthe’s disease Femoral head
Osteochondritis dissecans Medial femoral condyle, capitellum, talar dome
Non-articular Osgood-Schlatter Tibial tubercle
Sinding-Larsen-Johansson Inferior pole patella
Sever’s lesion Calcaneus
Physeal Sheuermann’s lesion Thoracic spine
Blount’s lesion Proximal tibia
ConclusionConclusion• Anterior knee pain - common in the pediatric
population• Thorough history and physical examination
necessary, often enough to make an accurate diagnosis.
• Patellofemoral joint and the extensor mechanism of the knee - most common areas affected
• Conditions unique to the growing skeleton like hip diseases (Perthe’s and SCFE) and osteochondroses
• Systemic diseases (inflammatory disease and malignancies) should be in differential diagnosis
ReferencesReferences• Cassas KJ. Childhood and adolescent sports-related overuse
injuries. Am Fam Physician. Mar 2006; 73(6): 1014-22.• Patel DR. Musculoskeletal injuries in sports. Prim Care. Jun 2006;
33(2): 545-79. • Mercier LR. Osgood-Schlatter disease. Ferri’s Clinical Advisor:
Instant Diagnosis and Treatment. 9th ed. St. Louis, Mo: Mosby; 2009:593
• D Caine, J DiFiori, and N Maffulli. Physeal injuries in children's and youth sports: reasons for concern?, Br J Sports Med. 2006 September; 40(9): 749–760
• Houghton KM. Review for the generalist: evaluation of anterior knee pain. Pediatric Rheumatology 2007, 5:8
• Gastón Andrés Topol, MD, Leandro ArielPodesta, MD, Kenneth Dean Reeves, MD, Marcelo Francisco Raya, PT, Bradley Dean Fullerton, MD,and Hung-wen Yeh, PhD: Journal Pediatrics July 2011
• Brukner and Khan Revised 3rd edition

Thank you

















