Anterior temporal lobectomy for epilepsy: success and shortcomings Dario J. Englot, visiting student Yale MD/PhD Program September 24, 2009 Department of Neurosurgery Department of Neurosurgery
Transcript
Anterior temporal lobectomy for epilepsy: success and shortcomings
Dario J. Englot, visiting student
Yale MD/PhD ProgramSeptember 24, 2009
Department of Neurosurgery
Department of Neurosurgery
61-year-old right-handed male with seizures for past 20 years per pt: daily “day dreaming” spells, losing touch with reality per wife: during seizures, face droops, clears throat, says
“okay” repeatedly, non responsive for ~30s no aura; somewhat confused for several minutes afterwards has failed management with multiple anti-epileptics:
PMH/PSH: retinal and shoulder surgeries Meds: levetiracetam, ASA, MVI NKDA SH: married engineer, no substance abuse FH: no epilepsy
Patient history
All vital signs in normal limits, and normal cardiopulmonary exam
Neurological exam: no deficits detected in mental status, cranial nerves, strength, sensation, reflexes, cerebellar function, or gait
Scalp EEG monitoring shows clinical episodes are associated with left temporal seizure activity
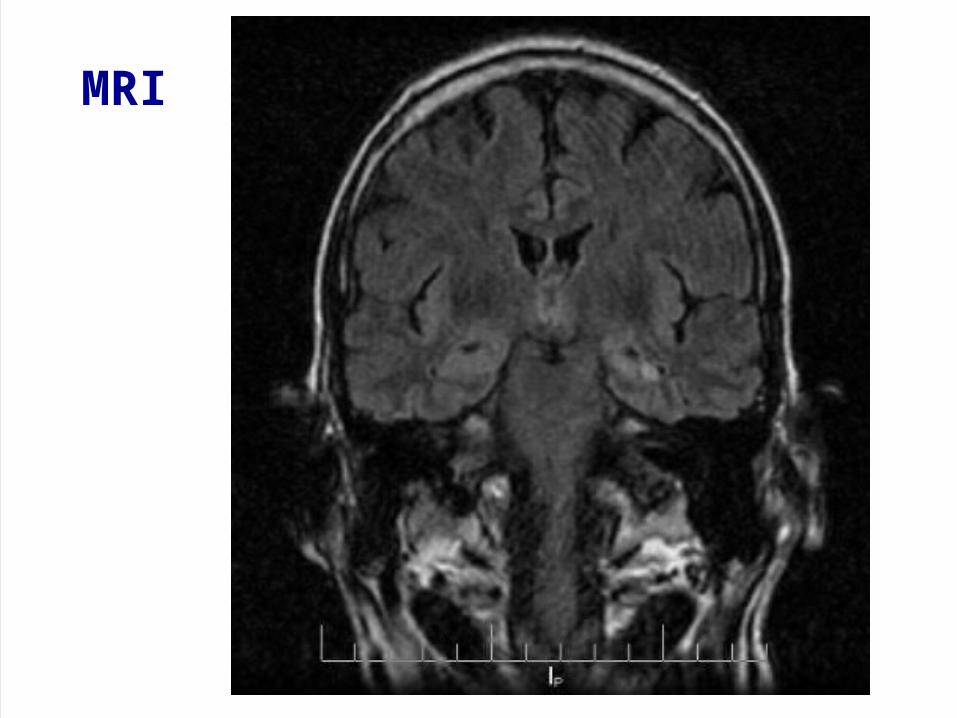
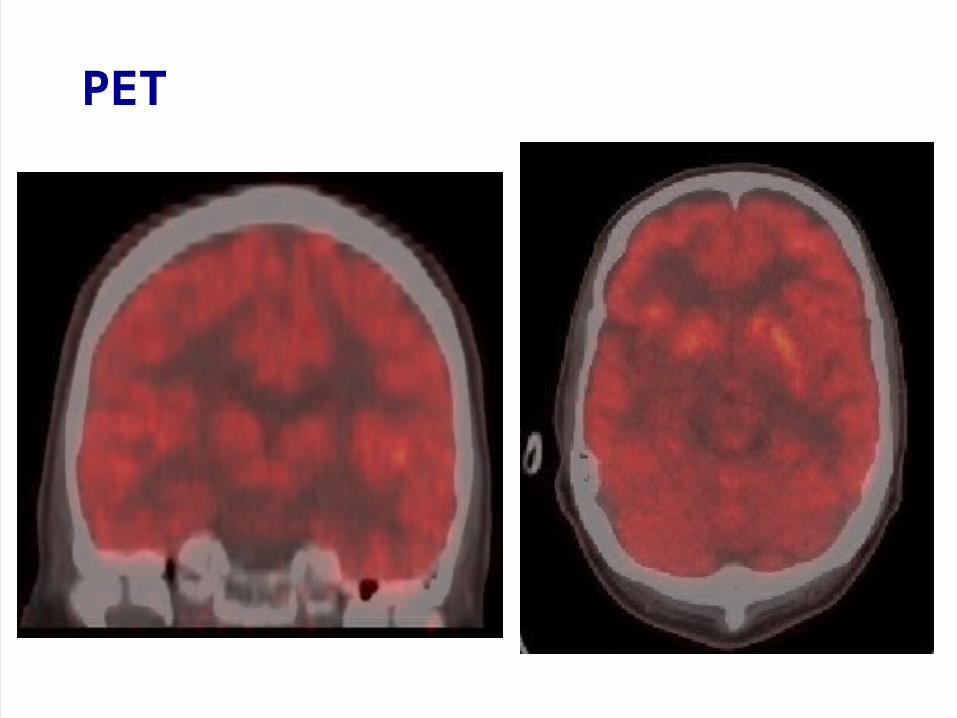
MRI, PET (outside hospital)
Physical exam and tests
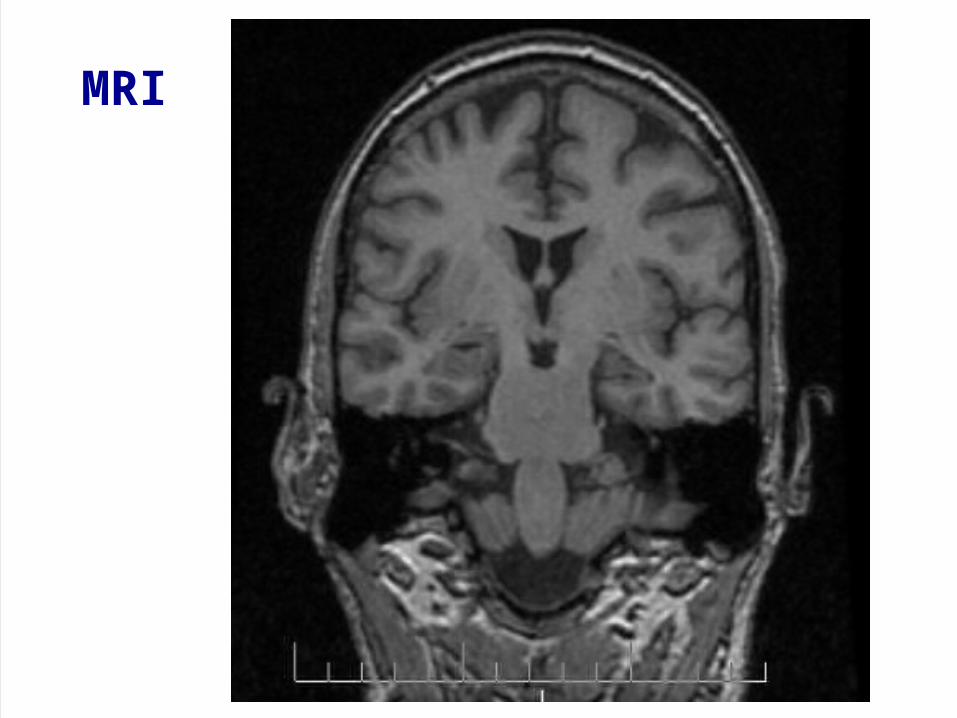
MRI
MRI
PET
Left anterior temporal lobectomy Dr. Emad Eskandar Assist: Dr. Jason Gerrard
Post-operatively expressive aphasia for a few hours urinary retention: treated full, uneventful recovery afterwards
Operative course
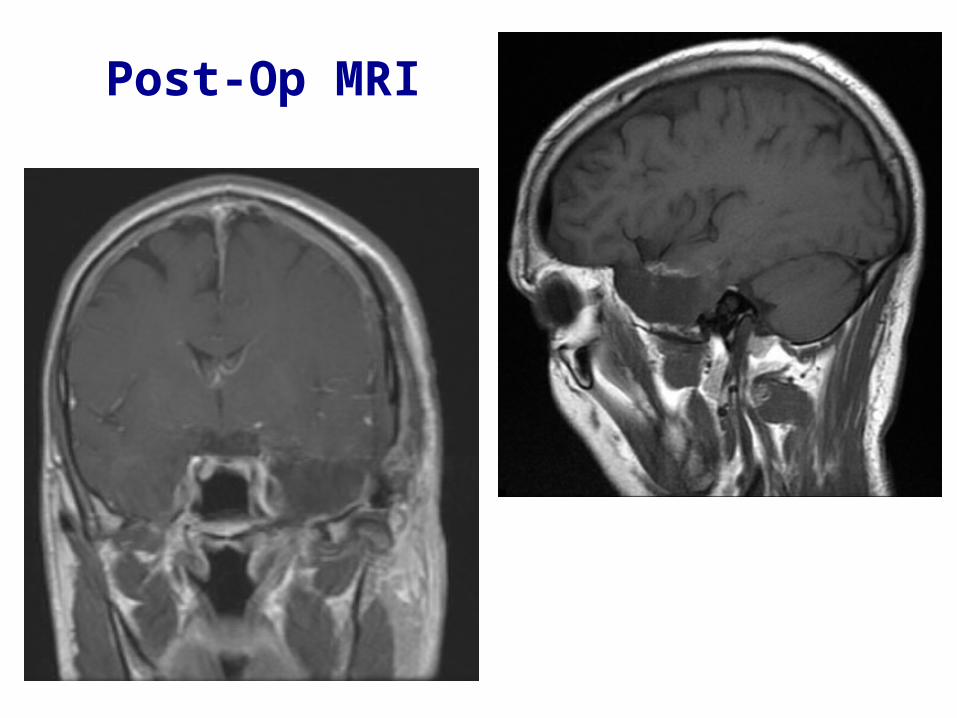
Post-Op MRI
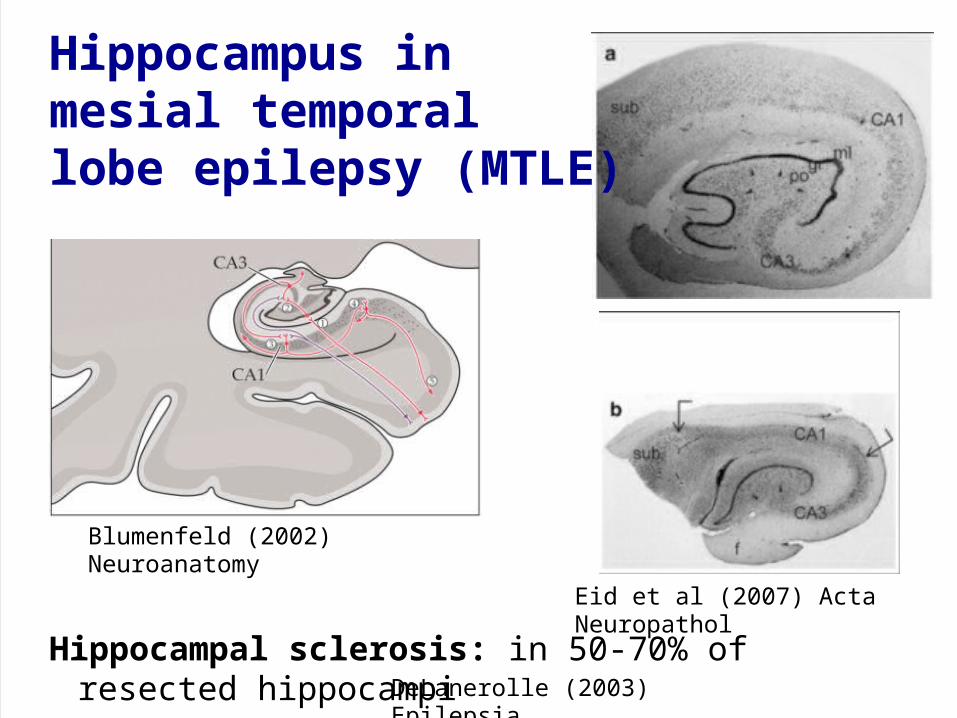
Blumenfeld (2002) Neuroanatomy
Hippocampal sclerosis: in 50-70% of resected hippocampi DeLanerolle (2003) Epilepsia
Eid et al (2007) Acta Neuropathol
Hippocampus in mesial temporal lobe epilepsy (MTLE)
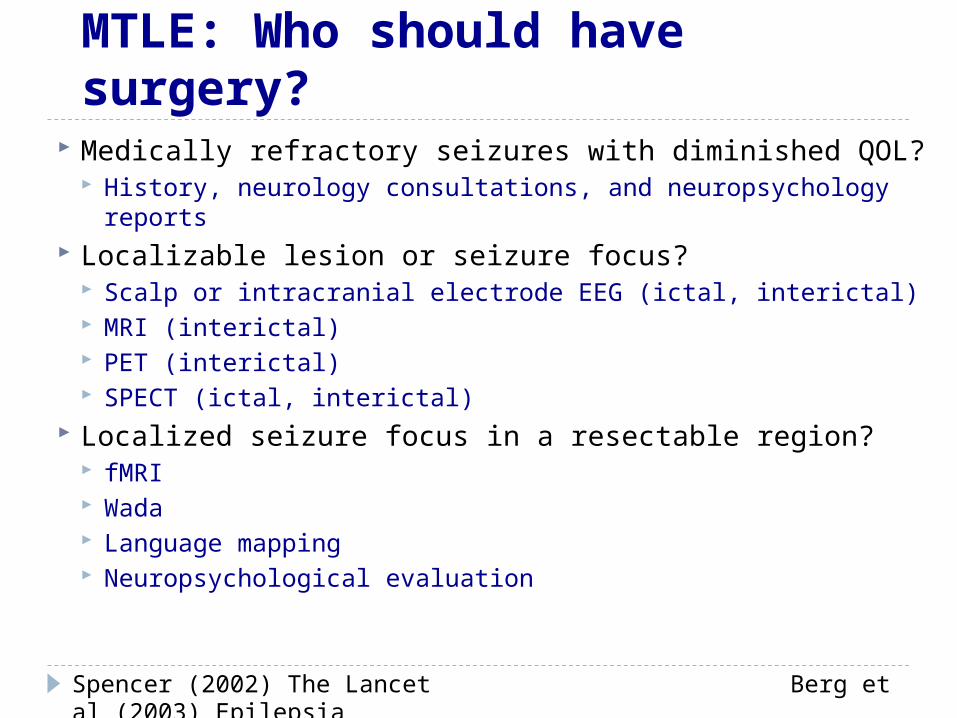
Medically refractory seizures with diminished QOL? History, neurology consultations, and neuropsychology
reports Localizable lesion or seizure focus?
Scalp or intracranial electrode EEG (ictal, interictal) MRI (interictal) PET (interictal) SPECT (ictal, interictal)
Localized seizure focus in a resectable region? fMRI Wada Language mapping Neuropsychological evaluation
MTLE: Who should have surgery?
Spencer (2002) The Lancet Berg et al (2003) Epilepsia
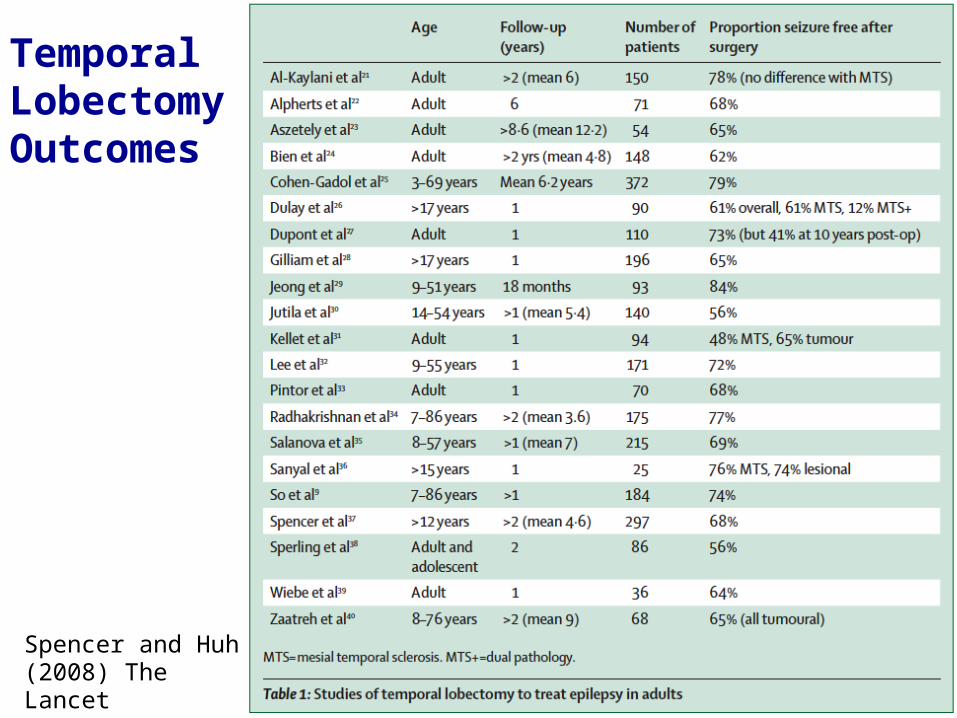
Spencer and Huh (2008) The Lancet
Temporal LobectomyOutcomes
Identifiable lesions and consistent imaging and electrophysiological findings improve outcomes
Some “good” surgical candidates, including those with unilateral temporal lobe sclerosis, nevertheless have recurrence post-operatively
Pathogenesis: Incomplete resection of epileptogenic lesions vs. new epileptogenicity
Why does surgery sometimes fail?
Extent of resection: anterior lobectomy vs. selective amygdalohippocampectomy Cohort study,100 patients (50 each surgery),
followed 5 yr: no statistical difference in recurrence rates1
Demographics: age, sex, or duration of epilepsy Retrospective chart review, 105 patients,
followed up to 3 yr: no relationship between factors & recurrence2
1) Tanriverdi et al (2008) J Neurosurg 2) Ramos et al (2009) J Neurosurg
Why does surgery sometimes fail?
Pre-op electrophysiology and imaging results Retrospective review, 118 pts, followed 1 yr:
similar data with/without recurrence1 (also found in previously mentioned study2)
Historical risk factors: head trauma, tuberous sclerosis, VP shunts, AVMs, CNS infection, global hypoxia, febrile seizures, status epilepticus 118 patients followed 1 yr: only status epilepticus
showed prediction (p = 0.0276) of a higher recurrence rate1
Why does surgery sometimes fail?
1) Hardey et al (2003) Epilepsia 2) Ramos et al (2009) J Neurosurg
Discontinuation of antiepileptic drugs (AEDs) 6 retrospective clinical studies each with > 5 patients
taken off meds (total N = 54-210 per study) Sironi et al (1983) Riv Neurol; Murro et al (1991) J Epilepsy;
Schiller et al (2000) Neurology; Van Veelan (2001) Ned Tijdschr Geneeskd; Al-Kaylani (2002) Epilepsia; Lachhwani (2003) Neurology
Relapse rate after AEDs D/Ced: 32-36% (f/u 1-6 yr) Relapse rate with AEDs onboard: 7-17% (f/u 1-5
yr) No benefit of waiting to attempt AED D/C after 2
yr in adults and 1 yr childrenReviewed in: Hardey et al (2003) Epilepsia
Why does surgery sometimes fail?
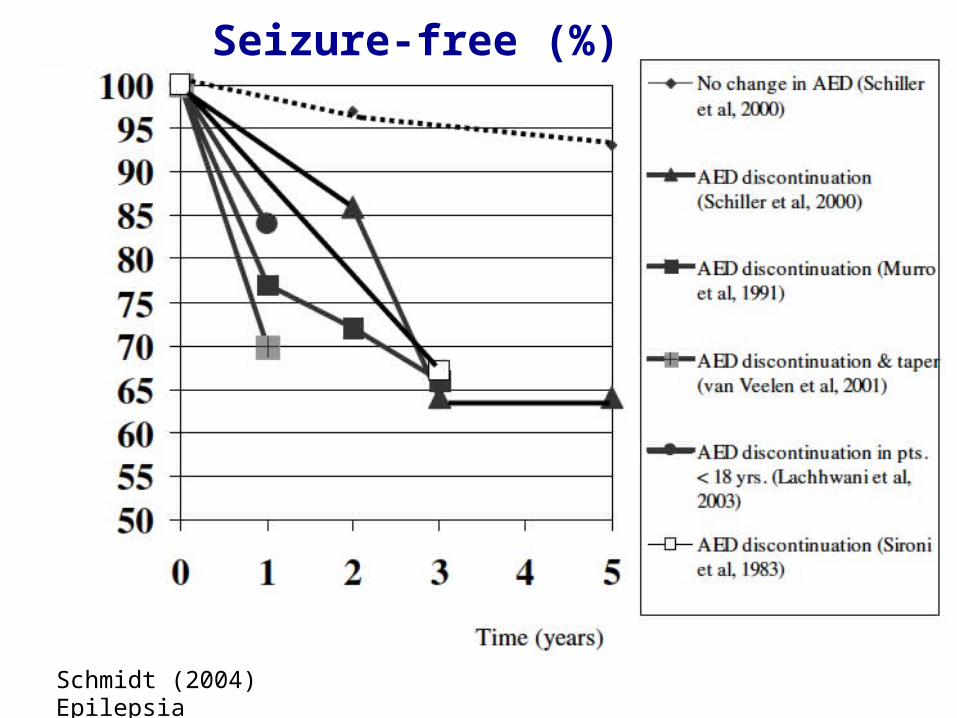
Schmidt (2004) Epilepsia
Seizure-free (%)
Limitation: possible selection bias with retrospective observations
Further study: need randomized, double-blind, placebo-controlled trial of AED continuation vs. discontinuation 2 yr post-op
AED discontinuation after temporal lobectomy
Hardey et al (2003) Epilepsia (review); Sironi et al (1983) Riv Neurol; Murro et al (1991) J Epilepsy; Schiller et al (2000) Neurology; Van Veelan (2001) Ned