47
Arrhythmias and Anti- arrhythmics Alex F. Chen, MD, PhD, FAHA Alex F. Chen, MD, PhD, FAHA Professor and Dean Professor and Dean School of Pharmacy School of Pharmacy

Arrhythmias and Anti-arrhythmics
Alex F. Chen, MD, PhD, FAHAAlex F. Chen, MD, PhD, FAHAProfessor and DeanProfessor and DeanSchool of PharmacySchool of Pharmacy

Properties of cardiac muscle
ExcitabilityExcitability: action potential upon stimulation.: action potential upon stimulation.
AutomaticityAutomaticity: ability to initiate own activity via : ability to initiate own activity via
spontaneous depolarization.spontaneous depolarization.
ConductivityConductivity: ability to transmit impulses from : ability to transmit impulses from
cell to cell at appropriate rates.cell to cell at appropriate rates.
RefractorinessRefractoriness: ability to resist partially or : ability to resist partially or
completely to stimulation during repolarization .completely to stimulation during repolarization .

Pacemaker and non-pacemaker cells
Pacemaker Cells:Pacemaker Cells: Sino-atrial node (SA Sino-atrial node (SA node) and atrioventricular node (AV node).node) and atrioventricular node (AV node).
Nonpacemaker Cells:Nonpacemaker Cells: atrial and ventricular atrial and ventricular
myocytes, internodal tracks, AV bundle, myocytes, internodal tracks, AV bundle, Perkinje fibers, etc.Perkinje fibers, etc.

Specializations -- Electrical Conduction
Superior Vena Cava SA Node
AV Node Bundle of His
Purkinje Fibers
Left Bundle Branch
Right Ventricle
Tricuspid Valve
Left Atrium
Right BundleBranch
Right Atrium
Special Features: Automaticity, Rhythmicity, Syncytial Conduction
AV node: relay+delay
Left Ventricle

Basics of Cardiac Conductance
Resting PotentialResting Potential – – Voltage difference across the Voltage difference across the plasma membrane during the resting state of an excitable plasma membrane during the resting state of an excitable cell; cell interior is more negative than its exteriorcell; cell interior is more negative than its exterior
DepolarizationDepolarization – A change in membrane potential such – A change in membrane potential such that the cell interior becomes more positive than the cell that the cell interior becomes more positive than the cell exterior; transmitting from cell to cell and creating a wave exterior; transmitting from cell to cell and creating a wave or impulse of electrical activityor impulse of electrical activity
RepolarizationRepolarization – – A change in membrane potential A change in membrane potential returning to the initial resting (polarized) statereturning to the initial resting (polarized) state
Action PotentialAction Potential – – A rapid sequence of electrical A rapid sequence of electrical changes including depolarization and repolarization that changes including depolarization and repolarization that once initiated, is self-generatingonce initiated, is self-generating
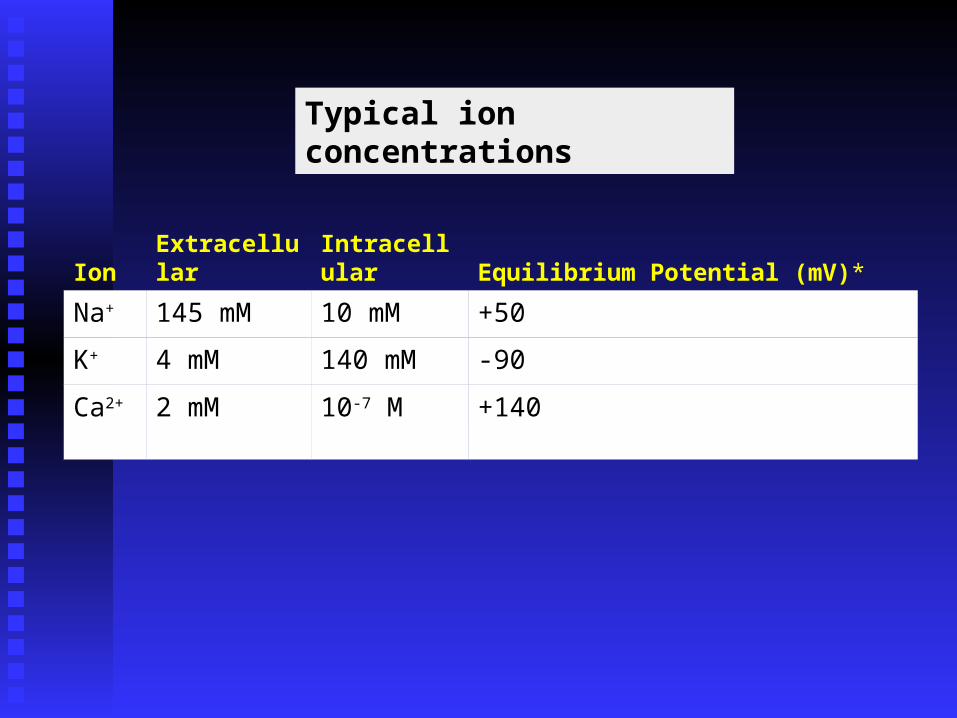
Typical ion concentrations
Ion Extracellular Intracellular Equilibrium Potential (mV)*
Na+ 145 mM 10 mM +50
K+ 4 mM 140 mM -90
Ca2+ 2 mM 10-7 M +140
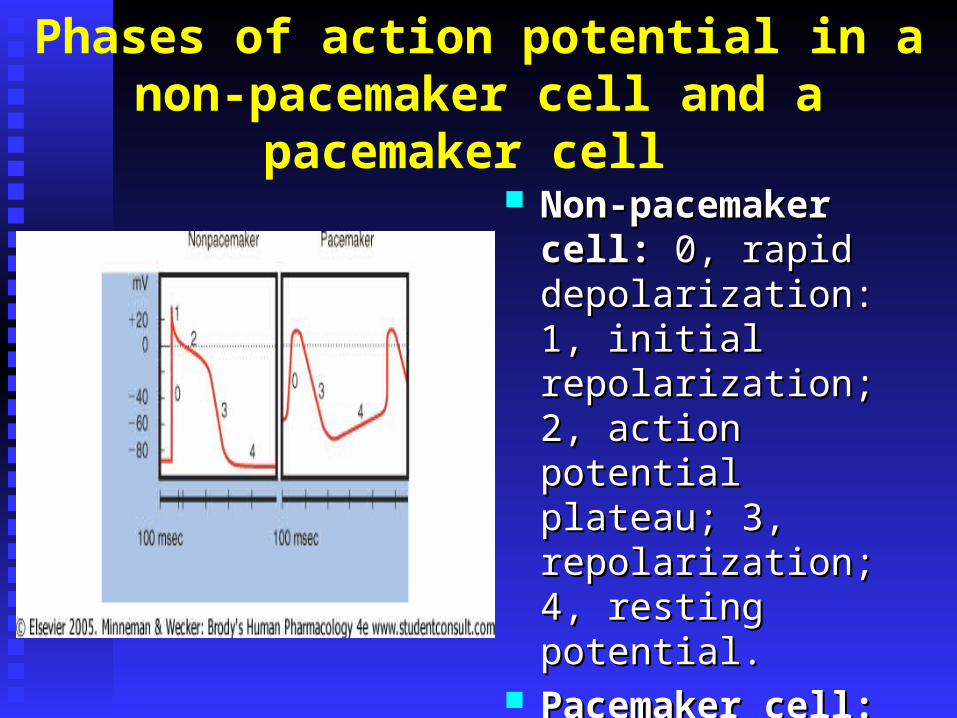
Phases of action potential in a non-pacemaker cell and a pacemaker cell
Non-pacemaker cell:Non-pacemaker cell: 0, 0, rapid depolarization: 1, rapid depolarization: 1, initial repolarization; 2, initial repolarization; 2, action potential plateau; action potential plateau; 3, repolarization; 4, 3, repolarization; 4, resting potential. resting potential.
Pacemaker cell:Pacemaker cell: 0, rapid 0, rapid depolarization; 3, plateau depolarization; 3, plateau and repolarization; 4, and repolarization; 4, slow diastolic slow diastolic depolarization.depolarization.

Phases of action potential in a non-pacemaker cell and a pacemaker cell
Non-pacemaker cell:Non-pacemaker cell: 0, 0, depolarization – depolarization – Na influxNa influx; 1, ; 1, repolarization - repolarization - ↓↓Na & K Na & K efflux; 2, plateau – Ca influx; efflux; 2, plateau – Ca influx; 3, repolarization - ↓Ca & K 3, repolarization - ↓Ca & K efflux; 4, resting potential - -efflux; 4, resting potential - -90 mV. 90 mV.
Pacemaker cell:Pacemaker cell: 0, 0, depolarization – depolarization – Ca influxCa influx; 3, ; 3, repolarization - ↓Ca & K repolarization - ↓Ca & K efflux; 4, slow diastolic efflux; 4, slow diastolic depolarization – K efflux & depolarization – K efflux & Na influx, -60 mV.Na influx, -60 mV.
Heartbeat and ECG
HeartbeatHeartbeat: in orderly sequence, contraction : in orderly sequence, contraction
of atria (atrial systole) followed by of atria (atrial systole) followed by
contraction of ventricles (ventricular systole) contraction of ventricles (ventricular systole)
and relaxation of all 4 chambers (diastole)and relaxation of all 4 chambers (diastole)
ECG or EKGECG or EKG: recording of fluctuations in : recording of fluctuations in
action potentials during the cardiac cycleaction potentials during the cardiac cycle

Waves of the ECG
P waveP wave - atrial depolarization - atrial depolarizationQRS complexQRS complex - ventricular depolarization - ventricular depolarizationST segmentST segment and and T waveT wave - ventricular repolarization - ventricular repolarization

Normal cardiac rate:Normal cardiac rate:
Heart beat starts at SA node (normal Heart beat starts at SA node (normal sinus rhythm);sinus rhythm);
70 beats/min at rest; 70 beats/min at rest; bradycardia (at rest), bradycardia (at rest), tachycardia (emotion, exercise, fever, tachycardia (emotion, exercise, fever,
etc)etc) respirationrespiration
Arrhythmias (Dysrhythmias)
~80% with acute myocardial infarction ~80% with acute myocardial infarction (accompanied by some degree of left (accompanied by some degree of left ventricular failure).ventricular failure).
Resulting from: disturbances in impulse Resulting from: disturbances in impulse generation, conduction, or both.generation, conduction, or both.
Ischemia, hypoxia, acidosis or alkalosis, Ischemia, hypoxia, acidosis or alkalosis, electrolyte abnormalities, excessive electrolyte abnormalities, excessive catecholamine exposure, drug toxicity, catecholamine exposure, drug toxicity, overstretching of cardiac fibers, diseased tissue.overstretching of cardiac fibers, diseased tissue.
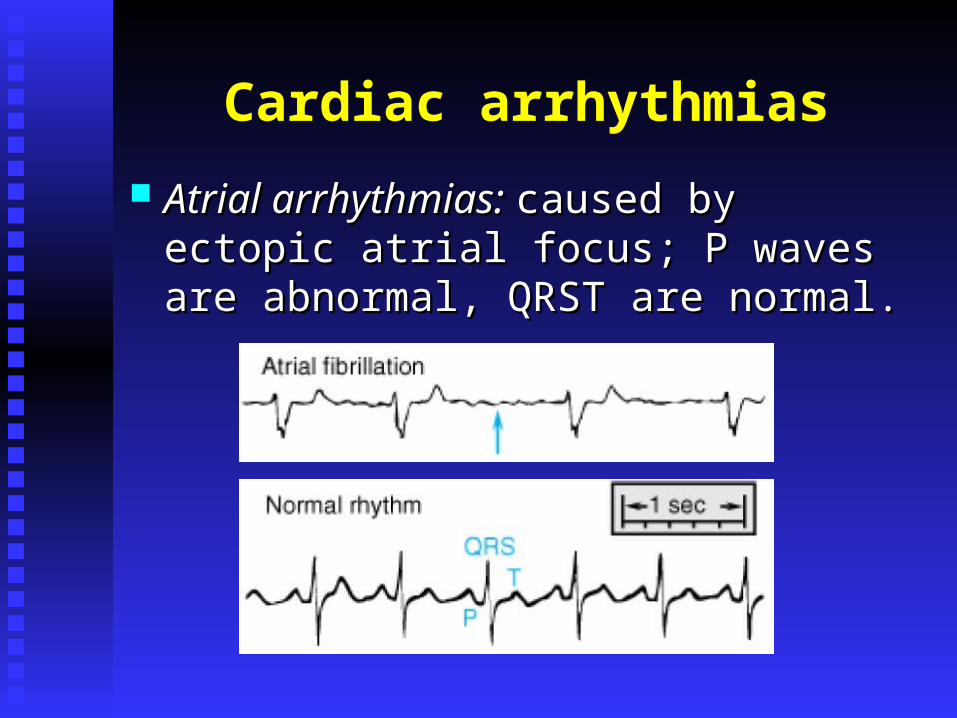
Cardiac arrhythmias
Atrial arrhythmias: Atrial arrhythmias: caused by ectopic atrial caused by ectopic atrial focus; P waves are abnormal, QRST are focus; P waves are abnormal, QRST are normal.normal.
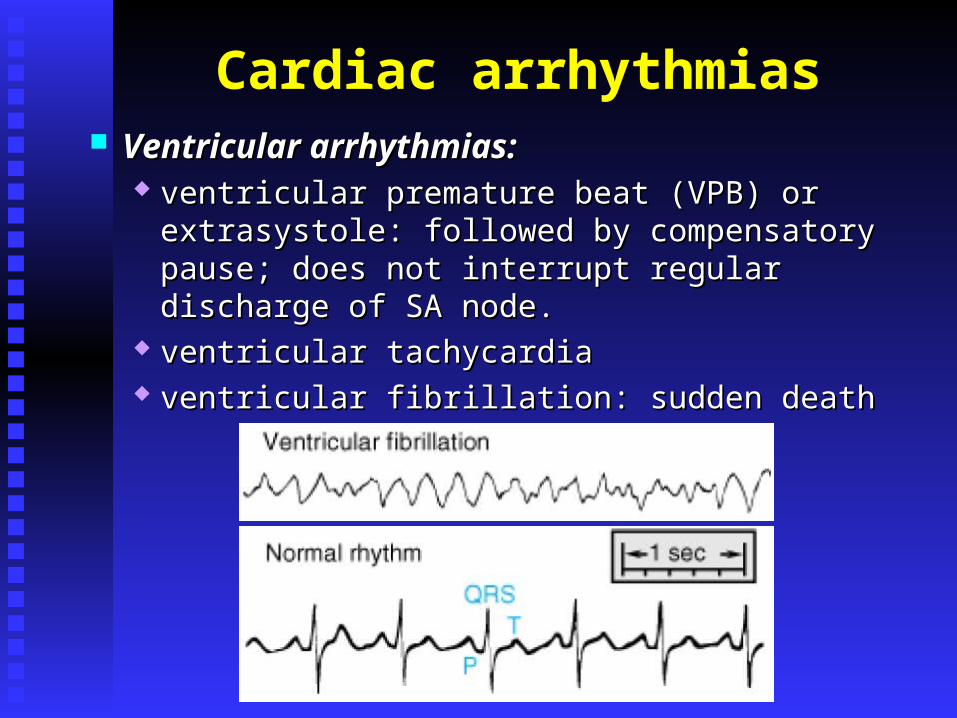
Cardiac arrhythmias Ventricular arrhythmias:Ventricular arrhythmias:
ventricular premature beat (VPB) or extrasystole: ventricular premature beat (VPB) or extrasystole: followed by compensatory pause; does not interrupt followed by compensatory pause; does not interrupt regular discharge of SA node.regular discharge of SA node.
ventricular tachycardiaventricular tachycardia ventricular fibrillation: sudden deathventricular fibrillation: sudden death

Non-pharmacological therapy
Reentry arrhythmias, atrial flutter, some ventricular Reentry arrhythmias, atrial flutter, some ventricular tachycardiatachycardia Open heart surgeryOpen heart surgery radio-frequency energy delivered through radio-frequency energy delivered through
intracardiac catheter (radio-frequency ablation, intracardiac catheter (radio-frequency ablation, RFA)RFA)
Ventricular fibrillationVentricular fibrillation conventional defibrillators: “quick-look paddles”conventional defibrillators: “quick-look paddles” Implantable cardioverter-defibrillator (ICD)Implantable cardioverter-defibrillator (ICD)

Pharmacological therapy
Antiarrhythmic drugs act by altering the flux Antiarrhythmic drugs act by altering the flux
of ions across the membranes of cardiac of ions across the membranes of cardiac
excitable cells. excitable cells.
Vaughan-Williams classification: inhibition of Vaughan-Williams classification: inhibition of
Na channels (Class I), blockade of beta-Na channels (Class I), blockade of beta-
adrenergic receptors (Class II), inhibition of K adrenergic receptors (Class II), inhibition of K
channels (Class III), and inhibition of Ca channels (Class III), and inhibition of Ca
channels (Class IV).channels (Class IV).

Classification of antiarrhythmic agents
Class I (blockers of fast Na+ channels)
Class II (β-blockers)
Class III (blockers of K+ channels)
Class IV (blockers of Ca2+ channels)
IA Propranolol Bretylium Verapamil
Quinidine Metoprolol Amiodarone Diltiazem
Procainamide Nadolol Sotalol
Disopyramide Atenolol Dofetilide
IB Acebutolol Ibutilide
Lidocaine Pindolol
Phenytoin Sotalol
Tocainide Timolol
Mexiletine Esmolol
IC
Flecainide
Propafenone

CLASS I(Na+channel blockers)
local anesthetic action
slow conduction velocity automaticity of Na+-dependent tissue

Prototypes
Class IAClass IA: lengthen action potential duration : lengthen action potential duration QuinidineQuinidine, Procainamide, Procainamide
Class IBClass IB: shorten action potential duration : shorten action potential duration LidocaineLidocaine, Mexiletine, Tocainide, Phenytoin, Mexiletine, Tocainide, Phenytoin
Class ICClass IC: no effect or minimal : no effect or minimal in duration in duration FlecainideFlecainide
Interaction with NaInteraction with Na++channels:channels: Ib > Ia >IcIb > Ia >Ic
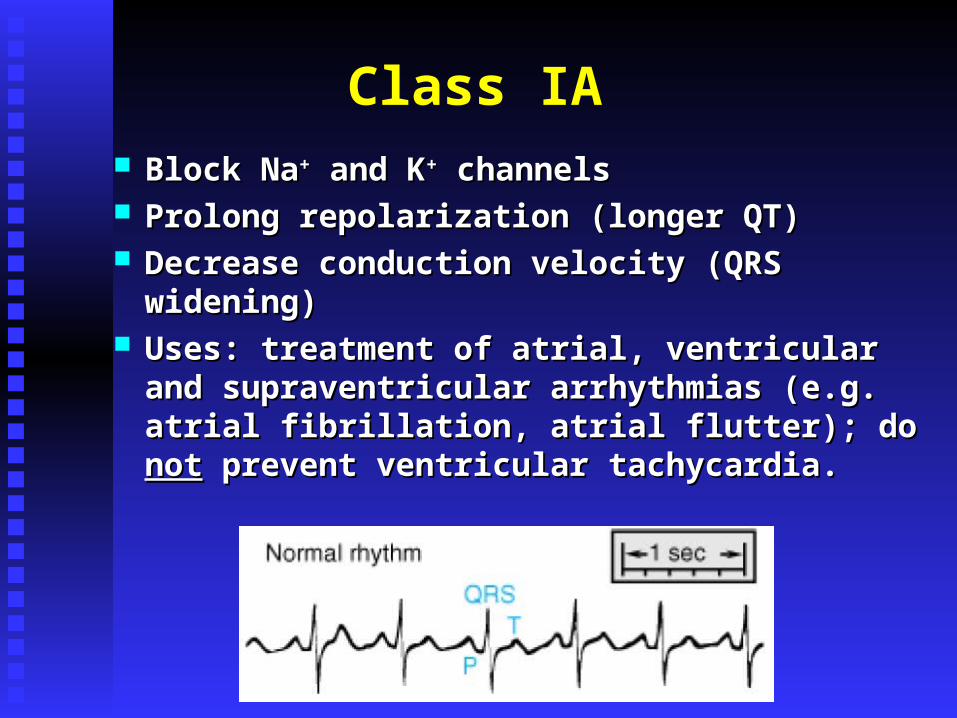
Class IA Block NaBlock Na++ and K and K++ channels channels Prolong repolarization (longer QT)Prolong repolarization (longer QT) Decrease conduction velocity (QRS widening)Decrease conduction velocity (QRS widening) Uses: treatment of atrial, ventricular and Uses: treatment of atrial, ventricular and
supraventricular arrhythmias (e.g. atrial supraventricular arrhythmias (e.g. atrial fibrillation, atrial flutter); do fibrillation, atrial flutter); do notnot prevent prevent ventricular tachycardia.ventricular tachycardia.

Class IA - Quinidine
pacemaker rate (ectopic); lengthens pacemaker rate (ectopic); lengthens refractory period and refractory period and excitability and excitability and conduction, prolongs action potentialconduction, prolongs action potential
longer QRS and QT interval (ECG) due longer QRS and QT interval (ECG) due to blockade of Kto blockade of K++ channels; channels;
reduction of reentry frequency, slowing reduction of reentry frequency, slowing tachycardia.tachycardia.
Class IA - Quinidine
Clinical indications:Clinical indications:
Most commonly used for atrial Most commonly used for atrial fibrillation;fibrillation;
Route of administration - IV or IM.Route of administration - IV or IM.

Class IA - Quinidine ToxicityToxicity::
Anti-muscarinic (vagolytic) action or Anti-muscarinic (vagolytic) action or atropine-like: atropine-like: sinus rate and AV sinus rate and AV conduction (conduction ( ventricular rate in atrial ventricular rate in atrial fibrillation or flutter)fibrillation or flutter)
Quinidine syncopeQuinidine syncope: lightheadedness and : lightheadedness and fainting, caused by polymorphic fainting, caused by polymorphic ventricular tachycardiaventricular tachycardia

Class IA - Procainamide
Similar effects to those of quinidineSimilar effects to those of quinidine Ganglion-blocking properties: Ganglion-blocking properties: peripheral peripheral
vascular resistance and hypotension vascular resistance and hypotension (infusion).(infusion).
2nd choice (after lidocaine) for sustained 2nd choice (after lidocaine) for sustained ventricular arrhythmias associated with ventricular arrhythmias associated with acute myocardial infarction.acute myocardial infarction.

Class IB Block NaBlock Na++channels channels onlyonly Shorten repolarization phaseShorten repolarization phase Decrease conduction velocityDecrease conduction velocity Negligible change in the ECGNegligible change in the ECG Indicated only for ventricular arrhythmiasIndicated only for ventricular arrhythmias Lidocaine: IV only; Mexiletine and Lidocaine: IV only; Mexiletine and
Tocainide: oral congeners.Tocainide: oral congeners.

Class IB- Lidocaine
abnormal automaticity, shortens action abnormal automaticity, shortens action potential;potential;
Agent of choice for ventricular tachycardia and Agent of choice for ventricular tachycardia and fibrillation;fibrillation;
IV bolus therapy during cardiac arrest, followed IV bolus therapy during cardiac arrest, followed by constant-rate infusion to reach the steady by constant-rate infusion to reach the steady state;state;
Not effective for supraventricular Not effective for supraventricular tachyarrhythmias.tachyarrhythmias.
Class IB- Lidocaine
Extensive first-pass effect in the liver;Extensive first-pass effect in the liver; Short half-life (tShort half-life (t1/21/2) – a few hours;) – a few hours;
Potent local anesthetic (blocks activated and Potent local anesthetic (blocks activated and inactivated Nainactivated Na++ channels); channels);
CNS side effects: seizures – diazepam CNS side effects: seizures – diazepam (Valium) as treatment.(Valium) as treatment.

Class IB- Mexiletine & Tocainide
Congeners of Lidocaine, resistant to 1st pass Congeners of Lidocaine, resistant to 1st pass effect = effect = oraloral
Effects similar to those of LidocaineEffects similar to those of Lidocaine Mexiletine – ventricular arrhythmias;Mexiletine – ventricular arrhythmias; Toxicity: neurological such as tremors, Toxicity: neurological such as tremors,
blurred vision, lethargy, etc.blurred vision, lethargy, etc.
Class IB- Phenytoin
Diphenylhydantoin, DilantinDiphenylhydantoin, Dilantin®®
Antiepileptic drug; inhibit NaAntiepileptic drug; inhibit Na+ + currents.currents. Digoxin-induced ventricular arrhythmias Digoxin-induced ventricular arrhythmias
(modulation of vagal efferent activity).(modulation of vagal efferent activity). Toxicity: Toxicity:
CNS: drowsiness, vertigo, nystagmus, CNS: drowsiness, vertigo, nystagmus, nausea.nausea.

Class IC
Block NaBlock Na++channels channels onlyonly No effect on repolarizationNo effect on repolarization Profoundly slow conduction velocity (QRS Profoundly slow conduction velocity (QRS
widening)widening) Atrial and ventricular arrhythmiasAtrial and ventricular arrhythmias

Class IC- Flecainide
Potent blocker of NaPotent blocker of Na++ and K and K++ channels channels No anti-muscarinic effectNo anti-muscarinic effect Used for supraventricular arrhythmias, oralUsed for supraventricular arrhythmias, oral Contraindicated in heart failure (significant Contraindicated in heart failure (significant
negative inotropic effect)negative inotropic effect) Neurologic toxicity: dizziness, visual Neurologic toxicity: dizziness, visual
abnormality.abnormality.

Differences among class I antiarrhythmic drugs
Class Phase O Depression Repolarization AP Duration
IA Moderate Prolonged Increased
IB Weak Shortened Decreased
IC Strong No effect No effect

CLASS II(beta blockers)
beta adrenergic antagonistsslow SA and AV conduction
heart rateNo change in QRS and QT intervals
Propranolol, Atenolol, Esmolol

Class II- -blockers
Used to slow supraventriculaer and Used to slow supraventriculaer and ventricular fibrillations;ventricular fibrillations;
Also used for hypertrophic Also used for hypertrophic cardiomyopathy;cardiomyopathy;
Can prevent recurrent infarction and Can prevent recurrent infarction and sudden death recovering from AMI;sudden death recovering from AMI;
Propranolol (oral/IP);Propranolol (oral/IP); Esmolol: IV infusion pump only; short-Esmolol: IV infusion pump only; short-
acting, acting, 11-selective.-selective.
Class II - -blockers
Side effects:Side effects: bradycardia, hypotension - CHFbradycardia, hypotension - CHFbronchospasm in asthmaticsbronchospasm in asthmaticsmay mask hypoglycemia in diabetesmay mask hypoglycemia in diabetes
CLASS III(AP-prolonging agents)
block K+ channels
prolong effective refractory periodprolong action potential
(repolarization)prolong QT intervals

Class III - Amiodarone
Complex effects on NaComplex effects on Na++, K, K++ and Ca and Ca+2+2 channels as channels as well as well as - and - and -adrenergic blocking properties. -adrenergic blocking properties. very effective blocker on inactivated Navery effective blocker on inactivated Na+ +
channels; channels; markedly prolongs AP duration (blocking of markedly prolongs AP duration (blocking of
KK+ + channels); channels); weak blocking of Caweak blocking of Ca+2+2 channels; channels; Non-competitive Non-competitive - and - and - blocking - blocking
properties: antianginal effects (+ blocking of properties: antianginal effects (+ blocking of CaCa+2 +2 influx) influx)

Class III- Amiodarone
Treat severe ventricular Treat severe ventricular arrhythmias;arrhythmias;
Extremely long tExtremely long t1/21/2 (13-103 d): 15-30 (13-103 d): 15-30
days to estimate drug’s efficacy, days to estimate drug’s efficacy, dosing controlled by response.dosing controlled by response.

Class IV(Ca+2 channel blockers)
Ca+2 channel antagonists decrease cardiac output
slow conduction (SA and AV nodes)prolong effective refractory period
prolong QT intervals antianginal agents

Class IV - Verapamil
Blocks both activated and inactivated Blocks both activated and inactivated CaCa+2+2 channels; channels;
Used for supraventricular tachycardia, Used for supraventricular tachycardia, atrial fibrillation and flutter;atrial fibrillation and flutter;
Counters digitalis-induced ventricular Counters digitalis-induced ventricular arrhythmias;arrhythmias;
Adverse effects:Adverse effects: hypotension, ventricular fibrillation hypotension, ventricular fibrillation negative inotropic effectnegative inotropic effect not used with not used with ββ-blockers-blockers

Class IV - Diltiazem
Diltiazem (IV form): less frequent Diltiazem (IV form): less frequent hypotension and bradyarrhythmia hypotension and bradyarrhythmia when used in atrial fibrillation.when used in atrial fibrillation.
CardizemCardizem®®, Dilacor, Dilacor®® (oral, (oral, parenteral): Diltiazem.parenteral): Diltiazem.
More frequently used than More frequently used than verapamil.verapamil.

Classification of antiarrhythmic agents
Class I (blockers of fast Na+ channels)
Class II (β-blockers)
Class III (blockers of K+ channels)
Class IV (blockers of Ca2+ channels)
IA Propranolol Bretylium Verapamil
Quinidine Metoprolol Amiodarone Diltiazem
Procainamide Nadolol Sotalol
Disopyramide Atenolol Dofetilide
IB Acebutolol Ibutilide
Lidocaine Pindolol
Phenytoin Sotalol
Tocainide Timolol
Mexiletine Esmolol
IC
Flecainide
Propafenone

Miscellaneous agents

Atropine
Muscarinic receptor antagonistMuscarinic receptor antagonist Treats sinus bradycardia and sinus Treats sinus bradycardia and sinus
arrest, also used in anesthesiaarrest, also used in anesthesia PO or IPPO or IP Side effects: vagolytics – constipation, Side effects: vagolytics – constipation,
dry mouse, etc.dry mouse, etc.

Isoproterenol
ββ1 and 1 and ββ2 adrenoceptor agonist;2 adrenoceptor agonist; Increases sinus node rate;Increases sinus node rate; Short-term treatment of dogs with sick Short-term treatment of dogs with sick
sinus syndrome or third-degree AV sinus syndrome or third-degree AV block;block;
First pass effect – IV infusion;First pass effect – IV infusion; Side effects: hypotension and Side effects: hypotension and
tachyarrhymias.tachyarrhymias.
Adenosine
Endogenous purine nucleoside; tEndogenous purine nucleoside; t1/21/2 = 10 = 10
sec, rapid IV bolus;sec, rapid IV bolus; KK+ + conductance and inhibits cAMP-conductance and inhibits cAMP-
induced calcium influx, resulting in induced calcium influx, resulting in hyperpolarization and hyperpolarization and ↓action potential↓action potential;;
Drug of choiceDrug of choice to convert reentrant to convert reentrant supraventricular arrhythmias (SVA) to supraventricular arrhythmias (SVA) to sinus rhythm involving ventricles.sinus rhythm involving ventricles.

Question: The use of propranolol as an antiarrhythmic agent is contraindicated with:
A. Severe AV node blockA. Severe AV node block B. Uncompensated heart failureB. Uncompensated heart failure C. Bronchial asthmaC. Bronchial asthma D. None of the aboveD. None of the above E. a, b, and c.E. a, b, and c.

















