35
UNDERSTANDING ANTI- DEPRESSANT DRUGS By- Dr.Namrata Mohan Msc. Final Year
| Date post: | 07-Aug-2015 |
| Category: |
Documents |
| Upload: | vibhu-rathore |
| View: | 15 times |
| Download: | 1 times |
UNDERSTANDING ANTI-DEPRESSANT DRUGS
By- Dr.Namrata Mohan Msc. Final Year
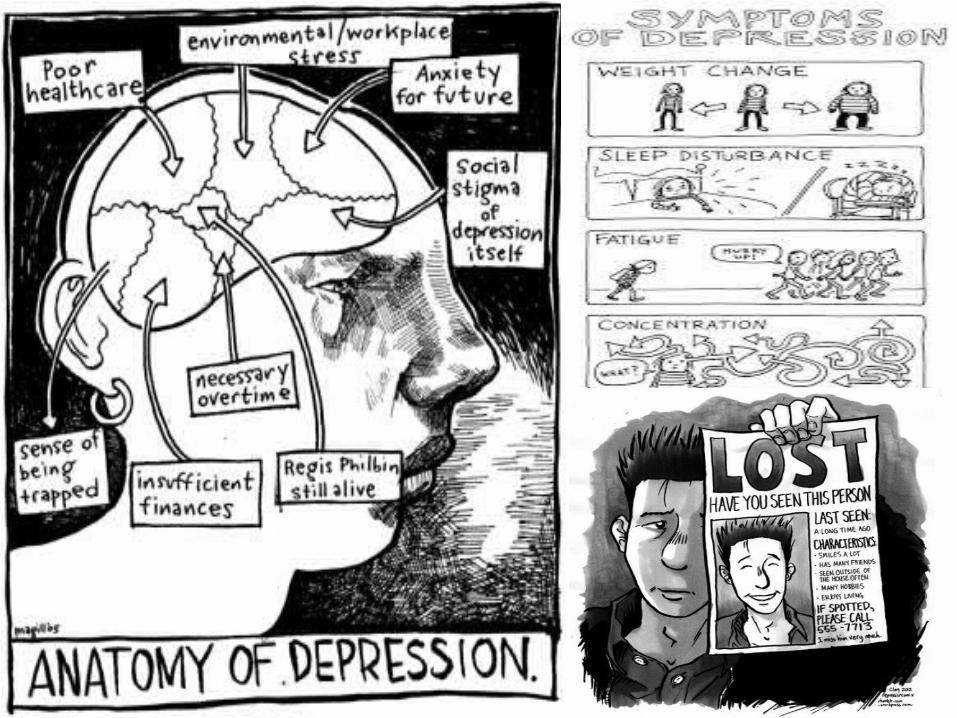
• Depression varies from person to person, but there are some common signs and symptoms. It’s important to remember that these symptoms can be part of life’s normal lows. But the more symptoms you have, the stronger they are, and the longer they’ve lasted—the more likely it is that you’re dealing with depression.
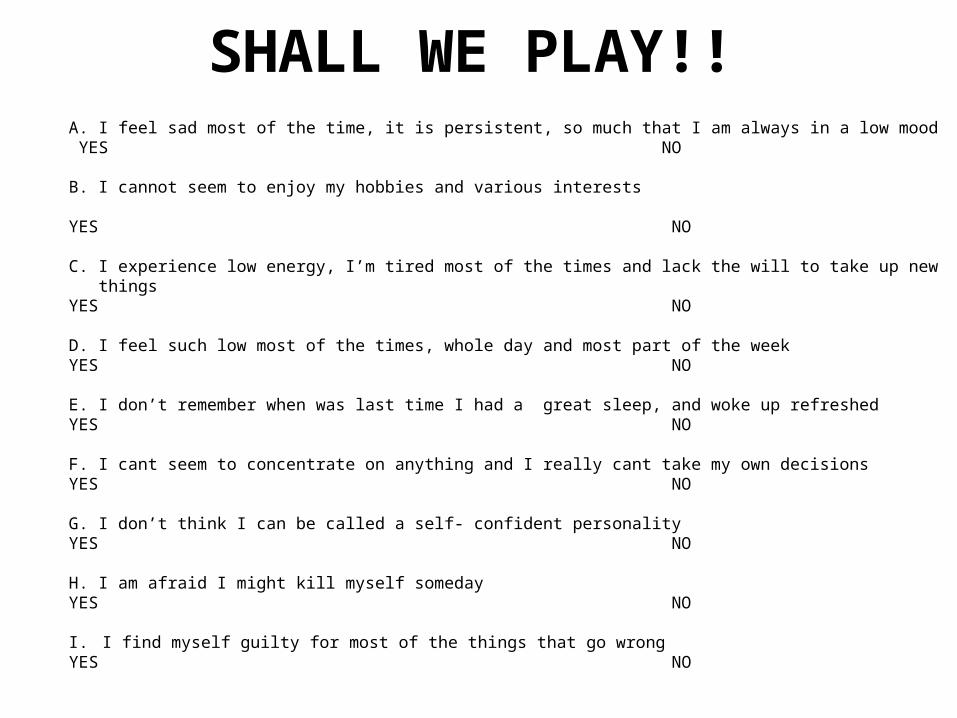
SHALL WE PLAY!!A. I feel sad most of the time, it is persistent, so much that I am always in a low mood YES NO
B. I cannot seem to enjoy my hobbies and various interests
YES NO
C. I experience low energy, I’m tired most of the times and lack the will to take up new thingsYES NO D. I feel such low most of the times, whole day and most part of the weekYES NO
E. I don’t remember when was last time I had a great sleep, and woke up refreshedYES NO
F. I cant seem to concentrate on anything and I really cant take my own decisionsYES NO
G. I don’t think I can be called a self- confident personalityYES NO
H. I am afraid I might kill myself somedayYES NO
I. I find myself guilty for most of the things that go wrongYES NO
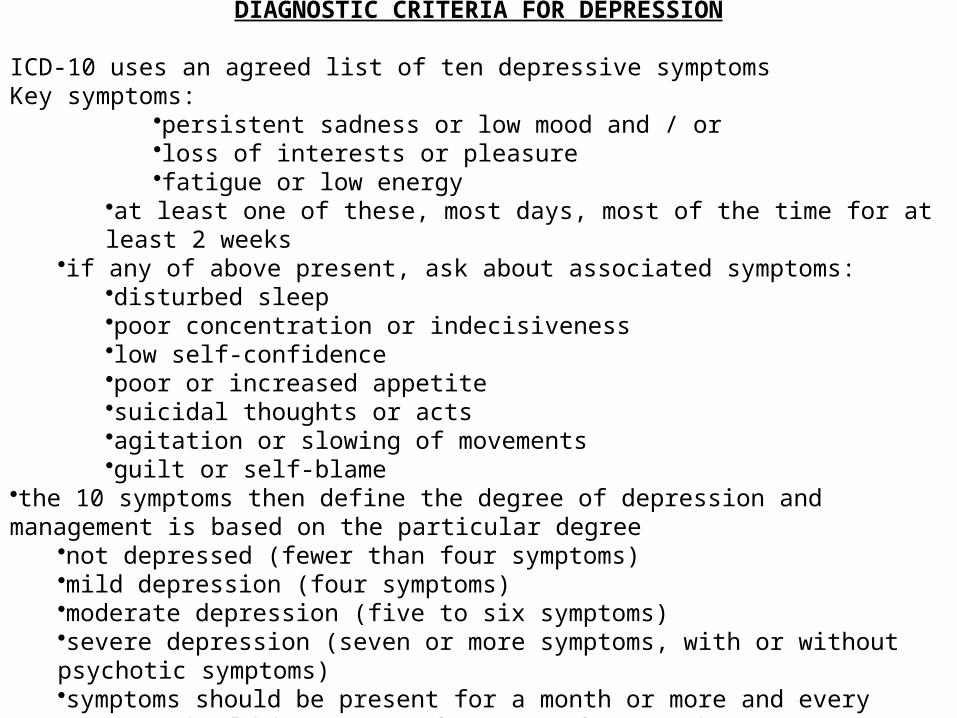
DIAGNOSTIC CRITERIA FOR DEPRESSION ICD-10 uses an agreed list of ten depressive symptomsKey symptoms:
•persistent sadness or low mood and / or•loss of interests or pleasure•fatigue or low energy
•at least one of these, most days, most of the time for at least 2 weeks•if any of above present, ask about associated symptoms:
•disturbed sleep•poor concentration or indecisiveness•low self-confidence•poor or increased appetite•suicidal thoughts or acts•agitation or slowing of movements•guilt or self-blame
•the 10 symptoms then define the degree of depression and management is based on the particular degree
•not depressed (fewer than four symptoms)•mild depression (four symptoms)•moderate depression (five to six symptoms)•severe depression (seven or more symptoms, with or without psychotic symptoms)•symptoms should be present for a month or more and every symptom should be present for most of every day
CAUSES 0F DEPRESSION
Like most of the Mental conditions, exact cause for depression is not known, but it is believed to be triggered by :•Biological differences•Brain Chemistry•Traumatic events•Family History
•Major depression
Major depression is characterized by the inability to enjoy life and experience pleasure. The symptoms are constant, ranging from moderate to severe. Left untreated, major depression typically lasts for about six months. Some people experience just a single depressive episode in their lifetime, but more commonly, major depression is a recurring disorder.
•Dysthymia (recurrent, mild depression)Dysthmia is a type of chronic “low-grade” depression. More days than not, you feel mildly or moderately depressed, although you may have brief periods of normal mood. The symptoms of dysthymia are not as strong as the symptoms of major depression, but they last a long time (at least two years). Some people also experience major depressive episodes on top of dysthymia, a condition known as “double depression
also known as manic depression, is characterized by cycling mood changes. Episodes of depression alternate with manic episodes, which can include impulsive behavior, hyperactivity, rapid speech, and little to no sleep. Typically, the switch from one mood extreme to the other is gradual, with each manic or depressive episode lasting for at least several weeks. When depressed, a person with bipolar disorder exhibits the usual symptoms of major depression. However, the treatments for bipolar depression are very different. In fact, antidepressants can make bipolar depression worse.
•Bipolar Disorder: When Depression is Just One Side of the Coin
WHEN TO THINK OF ANTI-DEPRESSANTS
DEPRESSION & SUICIDE
•Depression is a major risk factor for suicide.•15% of people with such disorders show suicidal behaviours in their lifetime. •Thoughts of death or suicide are a serious symptom of depression, so take any suicidal talk or behaviour seriously. It's not just a warning sign that the person is thinking about suicide: it's a cry for help!!
ANTI-DEPRESSANTSBUT THEN THERE IS A GOOD NEWS-
WHAT ARE ANTI-DEPRESSANTSAntidepressants are drugs used for the treatment of major depressive disorder and other conditions, including dysthymia, anxiety disorders, obsessive compulsive disorder, eating disorders, chronic pain, neuropathic pain and, in some cases, dysmenorrhoea, snoring, migraines, attention-deficit hyperactivity disorder (ADHD), substance abuse and sleep disorders. They can be used alone or in combination with other medications.
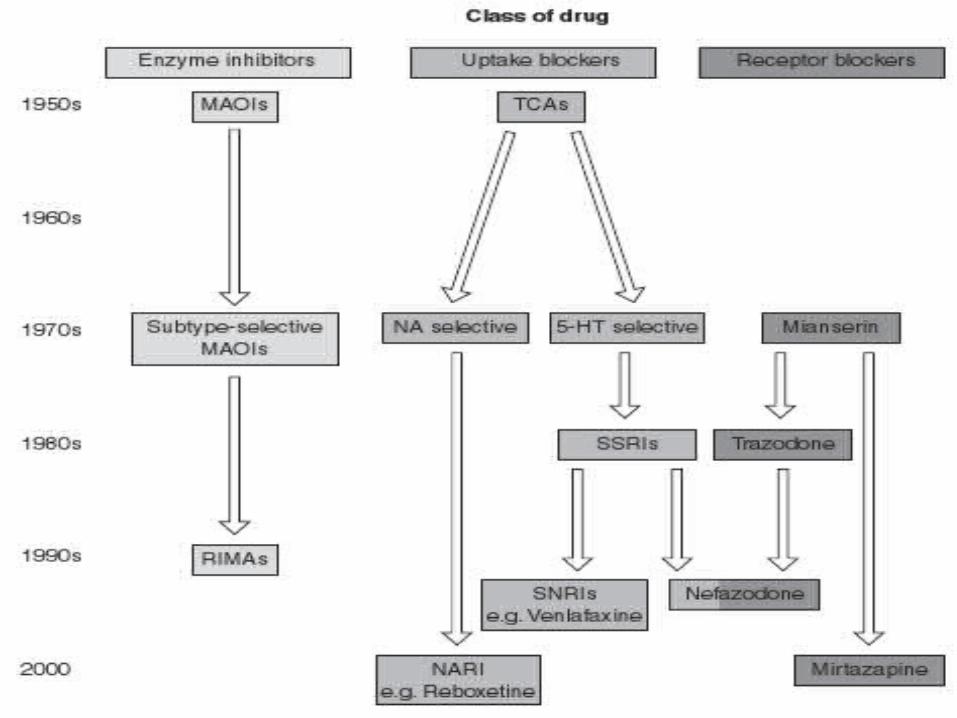
CLASSES OF ANTI-DEPRESSANTSThe most important classes are:
•SEROTONIN – NOREPINEPHRINE REUPTAKE INHIBITORS (SSRI’s & SNRI’s)
• TRICYCLIC ANTIDEPRESSANTS (TCA’s)• MONOAMINE OXIDASE INHIBITORS (MAOI’s)
• Other drugs include- buprenorphine, low dose antipsychotics, St.John Worts
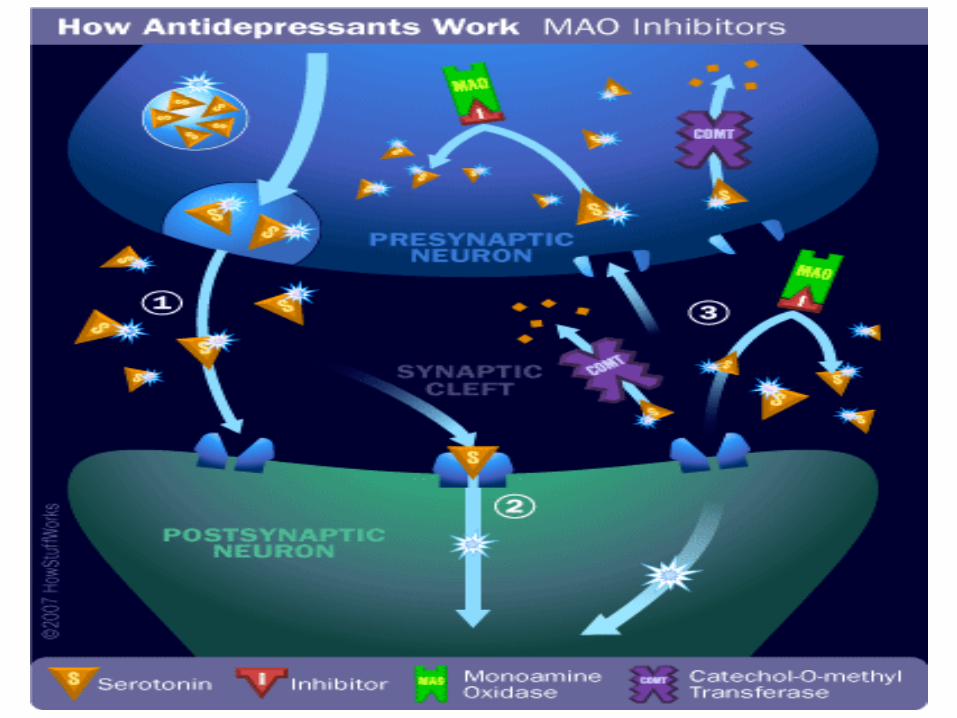
CLASS : MAO INHIBITORSMAO (Monoamine oxidase) is a Mitochondrial enzyme
involved in the oxidative de-amination of biogenic amines (Adr, NA, DA, 5-HT).
• MAO is found bound to the outer membrane of most of the cell types of body.
• In humans there are two subtypes- MAO –A& MAO-B• Both are found in CNS (neurons & astroglia) - outside CNS:MAO-A : liver, pulmonary vascular endothelial, GI tract
and place
SIGNIFICANCE OF MAO
• MAO-A is, for which they display different specificities.
• Serotonin, melatonin, noradrenaline, and adrenaline are mainly broken down by MAO-A.
• Phenethylamine and benzylamine are mainly broken down by MAO-B.
• Both forms break down dopamine, tyramine, and tryptamine equally.
PHARMACOLOGY
• Because of the vital role that MAOs play in the inactivation of neurotransmitters, MAO dysfunction (too much or too little MAO activity) is thought to be responsible for a number of psychiatric and neurological disorders. For example, unusually high or low levels of MAOs in the body have been associated with schizophrenia, depression, attention deficit disorder, substance abuse, migraines and irregular sexual maturation .
• Monoamine oxidase inhibitors are one of the major classes of drug prescribed for the treatment of depression, although they are often last-line treatment due to risk of the drug's interaction with diet or other drugs. Excessive levels of catecholamines (epinephrine, norepinephrine, and dopamine) may lead to a hypertensive crisis, and excessive levels of serotonin may lead to serotonin syndrome.
• In fact, MAO-A inhibitors act as antidepressant and antianxiety agents, whereas MAO-B inhibitors are used alone or in combination to treat Alzheimer’s and Parkinson’s diseases.
SPHERE OF ACTION•CNS: MAO inhibitors elevate mood - Maximal inhibition occurs in 3-5 days - Mood elevating effect may take 3-4 weeks. - Markedly supress REM sleep in non-depressed. Corrective in depressed.•CVS: Cause fall in BP - due to ganglionic interference - decreasing central sympathetic outflow etc.
PHARMACOKINETICS
• Well absorbed orally• Hydrazine compounds generate some
metabolites more potent and irreversible inhibitors of MAO ,inactivated by acetylation
• “HIT & RUN” Drugs- themselves stay in the bosy for relatively short periods but their effects continue for 2-3 weeks of discontinuation.
COMMON MAO’s
NON-SELECTIVE
• Hydrazines• Phenelzine• Isocarboxacid• Non-Hydrazine• Tranylcypromine
ISOZYME SELECTIVE
MOA-A• Clorgiline• Moclobemide
MAO-B• Selegiline
(deprenyl)
INTERACTIONS & ADVERSE REACTIONS
Combining MAO inhibitors with foods or drinks containing tyramine can result in dangerously high blood pressure, which can lead to a stroke or heart attack. Because of this danger, MAOIs are not typically chosen as a first-line depression treatment, there has to careful monitoring of diet, with restrictions which may include cheese, beers, chocolates & wine
COMMON SIDE EFFECTS :
• Dizziness• Insomnia• Weight gain• Headaches• Sexual problems• Daytime sleepiness• Risk of Heart attack• Dry Mouth• Nausea
SELECTIVE SEROTONIN REUPTAKE INHIBITORS ( SSRIs)
• Capable of affecting a specific neural site of action (eg, uptake pumps, receptors) while avoiding effects on other site of action
• The SSRIs (selective serotonin reuptake inhibitors) are the most commonly prescribed class of antidepressants. They act on a chemical in the brain called serotonin.
• The SSRIs are preferred over older classes of antidepressants such as tricyclic antidepressants and MAOIs because their adverse effects are less severe.
• The SSRIs can also cause serious withdrawal symptoms if stopped abruplty.
MECHANISM OF ACTION OF SSRIs
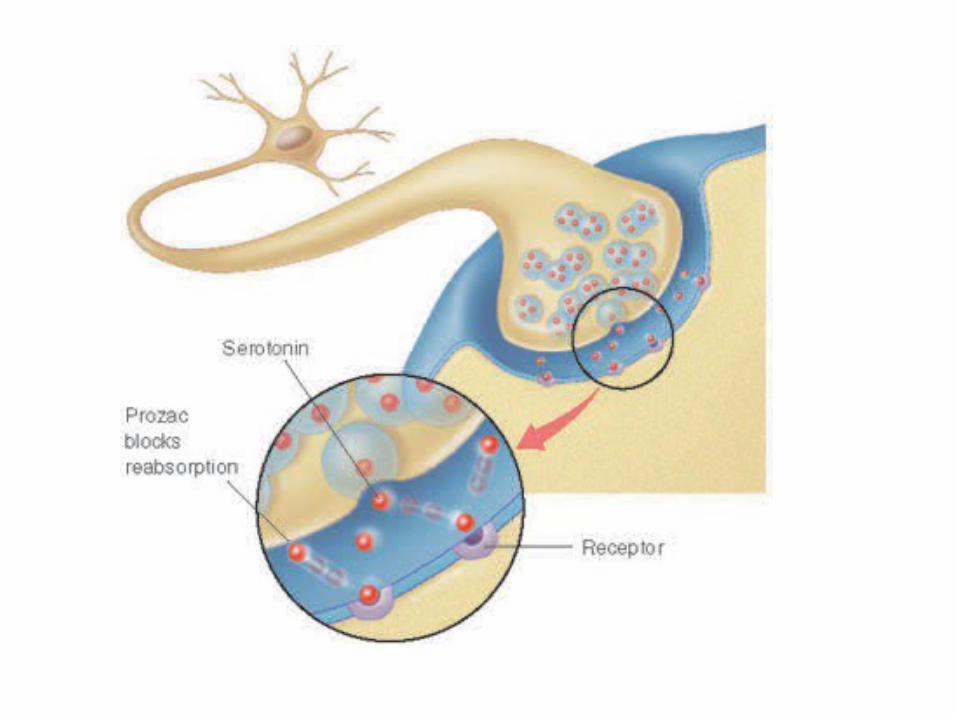
• All selective serotonin reuptake inhibitors have the same general mechanism of action. SSRIs seem to relieve symptoms of depression by blocking the reabsorption (reuptake) of serotonin by certain nerve cells in the brain. This leaves more serotonin available, which enhances neurotransmission and improves mood. SSRIs are called selective because they seem to affect serotonin significantly more than other neurotransmitters. Thus, the medications work by allowing the body to make the best use of the reduced amounts of serotonin that it has at the time. In due course, the levels of natural serotonin will rise again, and in some instances the SSRI can be reduced and withdrawn.
COMMON SSRI GENERIC NAMES
• Fluoxetine (Prozac)• Fluvoxamine (Luvox)• Sertraline (Zoloft)• Paroxetine (Praxil)• Escitalopram (Lexapro)• Citalopram (Celexa)
COMMON SIDE EFFECTS• Nausea• Insomnia• Dizziness• Weight gain or loss• Tremors• Sweating• Anxiety and restlessness• Decreased sex drive• Drowsiness or fatigue• Dry mouth• Diarrhea or constipation• Headaches
TRICYCLIC ANTIDEPRESSANTS• Imipramine (a diabenzapine- analogue of
phenothiazine in which sulphur atom of the central ring has been replaced by an ethylene bridge) was found during clinical trials in 1958.
• Since then a number of congeners have been added-:
• Tricyclic- Imipramine, Amitryptyline, Doxepin..• Tetracyclic- Mianserin, Amoxapine, Maprotiline• Atypical- Trazodone, Flouxetine
MECHANISM OF ACTION• They work by inhibiting the brain’s reuptake Of biogenic amines
NA, 5-HT and dopamine (partially) into their respective neurons. {they differ in selectivity and potency for different amines
• Because the tricyclics have such a broad mechanism of action, they tend to cause more side effects than the other classes of antidepressants. For this reason, the SSRIs and the atypical antidepressants are usually prescribed first.
• Tricyclic antidepressants typically take around two weeks to provide symptom relief. Drowsiness is a highly common side effect, particularly in the first few weeks after starting the medication.
• The tricyclics cause withdrawal symptoms when discontinued abruptly. Tricyclic antidepressants can also cause an abnormal heart rhythm, so they are not recommended if patient has heart problems or seizures.
PHARMACOKINETICS
• The oral absorption is good, though slow.• Highly bound to plasma & tissue protiens • Extensively metabolized in liver.• Inactivation occurs by oxidation and
gulcouronide conjugation.• Metabolites excreted in urine over 1-2 weeks.• Plasma t1/2 is between 16-24 hours for
amitriptyline, imipramine etc.
TRICYCLIC- COMMON & GENERIC NAMES
• Amitriptyline (Elavil)• Clomipramine (Anafranil)• Desipramine (Norpramin)• Doxepin (Sinequan)• Imipramine (Tofranil)• Nortriptyline (Pamelor, Aventyl)• Protriptyline (Vivactil)• Trimipramine (Surmontil)
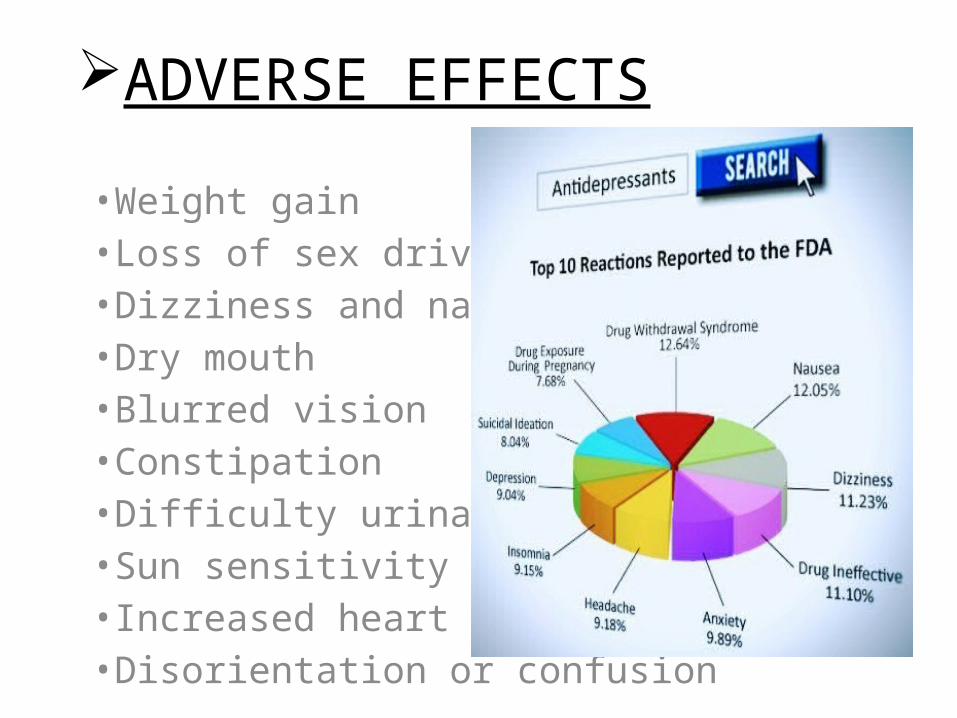
ADVERSE EFFECTS
•Weight gain•Loss of sex drive•Dizziness and nausea•Dry mouth•Blurred vision•Constipation•Difficulty urinating•Sun sensitivity•Increased heart rate•Disorientation or confusion
CHEAT CODES To remember names Tricyclic
ADD’s• "I have to hide, the CIA is
after me":ClomipramineImipramineAmitrptyline· If want the next 3 worth knowing, the DND is also after me:DesipramineNorrtriptylineDoxepin
TCA‘S side effects:
ThrombocytopeniaCardiac (arrhymia, MI, stroke)Anticholinergic (tachycardia, urinary retention, etc)Seizures
THANK YOU FOR A PATIENT HEARING

















